SET Facility







Archived Revised Rates of Hospital Charges All India Institute of Medical Sciences New Delhi, India
Blood Clinical Chemistry
ABO & RH Grouping 50
| Sr. No. | Radio Diagnosis | OPD/General Ward | Private Ward |
|---|---|---|---|
| 1 | Plain X-Ray (per film)
|
|
|
| 2 | Gastro Intestinal & Hepatobiliary
|
|
|
| 3 | Urinary
|
|
|
| 4 | Mammography
|
|
|
| 5 | Miscellaneous
|
|
|
| 6 | Ultrasound
|
|
|
| 7 | CT and CT Guided Interventions
|
|
|
| ANTI HCV HEPATITIS C | 0 |
| ANTI-HBc IgM ANTIBODY | 0 |
| ANTI-HBs ANTIBODY | 0 |
| Name of the Test | AIIMS OPD Patients | AIIMS Pvt. Ward & Other Pvt. Hospital | Overseas Patient |
|---|---|---|---|
| I.Serology based | - | - | - |
| HLA B 27 | 500/- | 800/- | 1000/- |
| HLA -ABC | 800/- | 1500/- | 3000/- |
| HLA-DR.DQ | 800/- | 1500/- | 3000/- |
| HLA-ABC &DR/DQ | 1200/- | 2500/- | 5000/- |
| Cross Matching(serology) | 300/- | 500/- | 1000/- |
| PRA | 500/- | 1500/- | 2000/- |
| Flowcytometric(cross matching) | 500/- | 1500/- | 1500/- |
| II.Paternity/Immigratilon cases | - | - | - |
| HLA-DNA Class-I&DRBI low resolution | 10000/- | 10000/- | 15000/- |
| HLA DQ Alpha | 4000/- | - | - |
| III.Molecular Biology Test | - | - | - |
| HLA-Class I | 3000/- | 4000/- | 6000/- |
| HLA- Class II(low resolution) DRBI DR 52, DR53 | 3000/- | 4000/- | 6000/- |
| HLA Class II (high resolution)( DRBI B3, B4, 5) | 3000/- | 4000/- | 7000/- |
| HLA-DQ Beta | 3000/- | 4000/- | 6000/- |
PCR for CMV 600
PCR for HSV (1&2) 600
RT-PCR for enteroviruses 900
RT-PCR for HCV 1500
Diagnostic Seriological assays For syphilis 50
Diagnostic Seriological assays 50 For Anti-streptolysine O Antibodies
| S.No. | Type of Investigation &Category of patients. | Fee Rs. |
|---|---|---|
| 1. | Plain MRI OPD/Indoor (Pvt. Wards) | 3000/- Plus >Rs.500/- (for films) |
| 2. | Plain MRI Indoor (General Wards) | 2500/- Plus Rs.500/- (for films) |
| 3. | Plain MRI Outside (Medico-legal cases and other exceptional cases) | 3500/- (with films) |
| 4. | Additional clinical studies like MRA, MRS and/or additional parts being scanned during the same sitting. Additional payment is required. (applicable to each category of S.N. 1,2 &3) | 1500/- |
| 5. | Extra cost for contrast MRI. Applicable to each category of S.N. 1,2 3 &4. | A) 2600 For patients of age 12 years and above B) 1500 For children less than 12 years of age |
| 6. | MRS for research | 3000/-(no films will be issued) |
Ability Assessment : 100.00
Aptitude Assessment : 100.00
Interest Assessment : 100.00
Memory Function test : 100.00
Organic Brain Damage Battery : 100.00
Personality Assessment (Full) : 100.00
Projective test (single) : 100.00
Questionnaire test (single) : 100.00
Test for Attention and concentration : 100.00
Test for Intelligence : 100.00
Test for thinking function : 100.00
Amniotic fluid AFP assay : 300.00
Amniotic fluid or urine 2 D :750.00
Blood/Bone marrow for chromosomes : 750.00
Buccal Smear for Sex Chromatin : 25.00
CVS for sexing for X-linked disease : 1500.00
Carrier Screening for thalassemia Nestroff and Hb A2 : 300.00
Carrier detection of DMD/Hemophillia/DNA diagnosis : 6000.00
Chemical test in urine : 150.00
Chromosomal study of blood/bone marrow : 500.00
Chromosomes from CVS by culture, or by amninotic culture : 3500.00
DNA based mutation Detection in thalassemia : 3500.00
DNA based mutation detection on DMD or other diseases : 3500.00
Electronic Cell Count : 150.00
Electrophoresis for MPS Amniotic fluid acetyle : 750.00
Galactosemia quantitative enzyme assay : 750.00
Galactosemia screening : 300.00
Genetic Karyotyping : 500.00
Leucocyte enzyme assay Arylsulfatase A, Hemosamindase : 750.00
MPS 24 Hrs,estimation with creatinine : 300.00
MPS spot test on urine : 150.00
Maternal serum AFP assay : 300.00
Maternal serum HCG assay : 300.00
Plasma/urine Quantitative Aminoscids : 1500.00
Prenatal diagnosis of Ataxia Telengiectasia or Fragile X : 6000.00
Prenatal diagnosis of thalassemia DMD Hemophilia, or Enzyme : 4500.00
Urine/plasma aminoacid screening : 300.00
Miscellaneous tests sent abroad
Miscellaneous - special diet / Drug / Injection.
| D-xylose &24 hour Fecal Fat Diagnosis Test : 50.00 |
| Aminoacid chromatography of urine/ plasma : 200.00 |
| Amniotic fluid or urine 2D for MPS : 750.00 |
| Chemical Test in urine : 75.00 |
| Glactosemia screening (Beutler spot fluorescence test) : 300.00 |
| Leucocyte enzyme assay (with control enzymes) : 500.00 |
| MPS spot test on urine : 75.00 |
| Triple marker screen (antenatal) : 850.00 |
| Prenatal diagnosis by enzyme assay : 500.00 |
| Leucocyte enzyme assay for Hurler (MPS) : 1000.00 |
| Celaic Serology : 500.00 |
| DNA based mutation detection in Thalassemia : 2000.00 |
| Prenatal diagnosis of Thalassemia :2000.00 |
| Xmm Polymorphism study : 1000.00 |
| Deletion studies in DMD : 2000.00 |
| Prenatal diagnosis of DMD by deletion studies : 2000.00 |
| Carrier screening by linkage studies in DMD : 2000.00 |
| DNA studies in SMA : 1500.00 |
| Prenatal diagnosis of SMA : 1500.00 |
| Carrier detection of Hemophilia A/B : 2000.00 |
| Prenatal diagnosis of Hemophilia A/B : 2000.00 |
| Fragile X PCR study : 1000.00 |
| 4 connexin 26 mutations : 1000.00 |
| Rh genotyping of Blood /AF : 1000.00 |
| Prenatal diagnosis of cord blood sampling : 750.00 (Karyotyping + Klehaur’s tests |
| Chromosomal study of blood Karyotyping : 500.00 |
| Chromosomes from CVS culture : 2500.00 |
| Chromosomes from Abortus tissue : 2500.00 |
B.M. Test for Eustachian Tube Function : 50.00
Bekesy Audiometry : 50.00
Caloric Test : 50.00
Electrogenstometry : 50.00
Olfactometry : 50.00
AFP : 450.00
Beta Heg : 450.00
CEA : 450.00
Estrogen receptor : 900.00
Progestron receptor : 900.00
T3 : 200
T4 : 200
TSH : 200
LH : 225
FSH : 225
Prolactin : 225
Estradiol : 225
Progesterone : 225
Alpha FP : 225
Testosterone : 225
HCG : 225
PSA : 275
DHEA : 300
DHEA-S : 300
Cortisol : 225
CA-125 : 500
b HCG : 250
Routine Semen Analysis : 40
Seminal Fructose (Quantitative) : 40 (Qualitative) : 20
Seminal Citric Acid : 25
Hypoosmatic Swelling Test (HOS) : 20
Acrosome intactness : 50
Sperm nuclear chromatin decondensation : 50
Sperm Mitochondrial Activity index : 50
Sperm Glyceryl Phosphoryl choline (GPC) : 250
Immunobead test IgG : 615
Complete sperm morphology : 50
T3 : 200
T4 : 200
TSH : 200
LH : 225
FSH : 225
PROLACTIN : 225
TESTOSTERONE : 225
DHEA-S : 300
CORTISOL : 225
INSULIN : 225
C PEPTIDE : 300
G H : 250
IGF-I : 1000
ISLET CELL ANTIBODY : 1000
MICRO ALBUMIN : 300
ANDROSTEREDIONE : 300
DHT : 1000
ACTH + CORTISOL : 1000
ALDOSTERONE : 400
17-OHP : 400
PTH-C TERMINAL with Calcium : 1000
VIT. D 25, OH : 1000
THYROID ANTIBODY (TPO) : 300
Embalming of ordinary (non-autopsied) bodies : 2000
Embalming of autopsied bodies : 4000
Prenatal Diagnostic services for Chromosomal abnormalities using amniotic cultures and conventional Karyotyping : 7000
Fluoride Test : 25
Conventioal Cytogenetics : 500
FISH (Molecular Cytogenetics) : 4000
| Single site study | 400 |
| Two sites study | 600 |
| Three sites study | 800 |
| Whole body study | 1000 |
| ANTISMOOTH MUSCLE ANTIBODY BY IMMUNOFLUORESCENCE METHOD | 0 |
| Agl - I gG | 100 |
| Agl - I gM | 100 |
| ANTI ds DNA | 100 |
| ANCA | 50 |
| ANA (HEP-2) | 100 |
| ANTI-LKM-1 | 200 |
| ANTINUCLEAR ANTIBODY TEST | 50 |
| ANTITHYROID ANTIBODY TEST | 50 |
| APCR | 300 |
| AT III | 400 |
| BETA 2 GLYCOPROTEIN | 0 |
| C-3 QUANTIFICATION IN SERUM/ OTHER FLUIDS | 50 |
| CARRIER DETECTION HAEMOPHILLIA | 2000 |
| CARRIER DETECTION PRENATAL | 2000 |
| CRP &PCT FOR SEPSIS- CRP QUALITATIVE KIT | 0 |
| CRP &PCT FOR SEPSIS -CRP QUANTITATIVE KIT | 0 |
| CRYOGLOBULINS | 50 |
| D-XYLOSE &24 HR FECAL FAT ESTIMATION | 0 |
| FACTOR ASSAY | 1200 |
| HEPARIN ASSAY | 250 |
| HEPATITIS ANTIGEN TEST | 50 |
| HOMOCYSTEIN | 0 |
| HPLC | 300 |
| IMMUNOELECTROPHORESIS PER ANTIBODY | 0 |
| IMMUNOPHLOROSCENCE ASSAY(IFA)&TTG ELISA FOR DIAGNOSIS OF - CELIAC DISEASE | 0 |
| IMMUNNOGLOBULINS A | 100 |
| IMMUNNOGLOBULINS G | 100 |
| IMMUNNOGLOBULINS M | 100 |
| IMMUNOTYPING FIVE ANTIBODY | 0 |
| IMMUNOTYPING ONE ANTIBODY | 0 |
| LATEX RHEUMTOID FACTOR TEST | 50 |
| MOLECULAR GENETIC STUDIES BY RQ –RT PCR | 3000 |
| MUTATION DETECTION F V LAIDEN | 0 |
| MUTATION DETECTION MTHFR | 0 |
| MUTATION DETECTION P 20210 | 0 |
| NITRO BLUE TETRAZOLIUM TEST FOR CHRONIC GRANULOMATOUS - DISEASE | 0 |
| PCT QUANTITATIVE KIT | 0 |
| PRO C GLOBAL | 500 |
| PROTEIN C CLOTTING | 0 |
| PROTEIN C ELISA | 0 |
| PROTEIN S CLOTTING | 0 |
| PROTEIN S ELISA | 0 |
| RA | 0 |
| RISTOCETIN | 0 |
| VWD | 0 |
| IGMACL | 100 |
Pulmonary Function Test 250
Supply of one unit Blood (Pvt. Ward) 250.00
Abscess incision : 250.00
Acrylic Full Crown : 100.00
Activator : 250.00
All extractions in one Jaw : 250.00
Alveolectomy : 250.00
Apical Curettage : 250.00
Biopsy : 250.00
Cast Inlay per tooth (Non-precious alloy) : 100.00
Complete Denture Acrylic - One jaw : 500.00
Complete Denture Acrylic - both jaws : 1000.00
Complete Denture with metal basis-both jaws : 2000.00
Condylectomy : 1000.00
Cysectomy : 250.00
Definitive Obturator with teeth : 500.00
Dental Restoration Class-I with AG amalgam/composite : 50.00
Dental Restoration Class-II with AG amalgam composite : 100.00
Expansion plate (excluding screw to be brought by patient : 250.00
Extraction per tooth : 25.00
Fistula closure : 250.00
Fistulectomy : 250.00
Fixation of Fracture of Jaw : 1000.00
Fixed Appliances both jaw : 1000.00
Fixed Applicances one jaw : 500.00
Fixed Partial Denture 3 units with Porcelain : 250.00
Fixed Partial Denture 3 units with : 2000.00
porcelain veenering - Non-precious alloy
Fixed Partial Denture per additional tooth with : 250.00
porcelain veenering - semi precious alloy
Fixed partial denture - 3 units with acrylic veneering : 1000.00
Fixed partial denture 3 units in gold alloy (excluding gold : 500.00
Fixed partial denture per additional tooth in gold alloy : 250.00
Fixed partial denture per additional unit with acrilic : 500.00
Fracture Jaws closed reduction : 500.00
Fracture Jaws open reduction : 1000.00
Frenectomy :rown (Nickel Chrome) : 200.00
Gingivectomy full mouth : 1000.00
Gingivectomy per segment : 250.00
Growth removal : 250.00
Head Gear (excluding sctraps to be brought by patients : 250.00
Inclined plane/repair of plane : 100.00
Mandibulectomy : 2000.00
Nasal/Auricular/Orbital Prosthesis : 250.00
Orthodontic Appliance, Bite plates, Retraction plate : 250.00
Osteotomy : 1000.00
Pericoronotomy : 150.00
Peripheral Neurectomy : 500.00
Porcelain Full Crown : 250.00
Porcelain to metal crown : 500.00
Pulpotomy : 250.00
Removable Acrylic Partial Denture per additional tooth : 50.00
Removable Acrylic Partial Denture with one tooth : 100.00
Removable Cast Partial Denture (Chromecobalt) per additional : 50.00
Removable Cast Partial Denture (Chromecobalt) with one tooth : 500.00
Removal of Impaction : 250.00
Repairing/ Relining Denture : 100.00
Resection of jaw : 2000.00
Rochett's (Maryland) Bridge 3 units : 250.00
Root Planning : 250.00
Root amputation : 250.00
Root canal treatment : 250.00
Segmental resection of jaw : 1000.00
Sequestrectomy : 250.00
Sialolithotomy : 250.00
Silver cast splint per dental arch : 250.00
Single Jacket Crown/Dowel crowh in non precious alloy with : 250.00
Single three quarter crown (Nickel - Chrome) : 250.00
Surgical Obturator/Intermediate obturator (without teeth) : 100.00
Total extraction both jaws : 1000.00
Tumour Excision : 1000.00
Veneering - Non precious alloy : 1000.00
Abscess Drainage under G.A. : 250.00
Aspiration of cold abscess/cysts : 250.00
Biopsy (Punch/ Excision/ Cervical cone/Endometrial : 250.00
Bone Tumor/Testicular--)
Cervical sympathectomy : 2000.00
Circumcision : 250.00
Colostomy closure : 5000.00
Excision and skin graft of contracture : 1000.00
Excision benign breast lumps : 250.00
Excision of cheek cancer : 2000.00
Excision of Small tumour : 250.00
Excision of rectum : 2000.00
Feeding Jejunostomy/ Gastrostomy : 250.00
Fissurectomy : 250.00
Fistulectomy : 250.00
Fractional Curettage : 500.00
Haemorrhoids : 250.00
Hemicollectomy : 5000.00
Incision & Drainage : 250.00
Injection of keloids : 250.00
Intestinal biopsy : 250.00
Kidney transplant : 8000.00
Laceration suture abscess drainage under local anaesthesia :100.00
Laparoscopy : 500.00
Laprotomy + Additional procedure : 2000.00
Oopherectomy : 2000.00
Operation for gall stones : 2000.00
Operations for Intestinal obstruction : 5000.00
Operations for pancreas : 5000.00
Operations for peptic ulcer/ stomach cancer : 5000.00
Operations for surgical jaundice : 2000.00
Operations for tuberculosis cancer of the Bowel : 2000.00
Partial Amputation Penis : 250.00
Preparation and transfer of tube pedicles and flap : 250.00
Radical Amputation Penis : 2000.00
Radical mastectomy : 2000.00
Repair of External Hernia : 1000.00
Repair of facial fracture : 1000.00
Sequestrectomy : 250.00
Simple mastectomy : 1000.00
Surgery for portation : 8000.00
Thyroidectomy : 5000.00
Trachectomy : 1000.00
Tracheostomy : 500.00
Undescended testis operative procedure : 1000.00
A.V. Shunt : 1000.00
CAPD (Tenkoff) Cathetre implantation : 1000.00
CAVH : 2000.00
CAVHD : 2000.00
CVVH : 2000.00
CVVHD : 2000.00
Femoral Vein cathetrisation : 500.00
Haemodialysis on keil dialyser : 2000.00
Insertion of A.V. Canula for Acute Haemodialysis : 500.00
Peritoneal dialysis cathetrisation (intermittent) : 1000.00
Plasmapheresis : 1000.00
Subclavian vein perm cathetre implantation : 1000.00
Abdominal perineal Ext.Hysterectomy : 2000.00
Abdominal perineal neo construction Cx+Uteria+Vagina : 5000.00
Caesaerian Hysterectomy : 2000.00
Cervical Biopsy : 250.00
Colopotomy : 500.00
Colpollaisis/Colporrhophy : 2000.00
Cone Biopsy Cervix : 500.00
Cryosurgery : 250.00
D & C : 500.00
Deliveries Normal : 2000.00
Dilatation of Cervix : 250.00
Electro Cauterization : 250.00
Endometrial Biopsy : 250.00
Evacuation : 500.00
Fractional Curettage : 500.00
Gynaecography : 1000.00
H/C V.V.F. & R.V.F. : 2000.00
Hydrotubation : 250.00
Hymenectomy : 250.00
Hysterectomy (Abdominal) : 2000.00
Hysterectomy (Wertheims) : 5000.00
Normal R/o Placenta : 1000.00
Operation for stress incontinence : 2000.00
Ovarion Cystectomy : 2000.00
Ovaritomy : 2000.00
Pelvic Exenteration : 5000.00
Plastic Operation on uterus : 2000.00
Radical Vulvectomy : 5000.00
Repair of Perineal Tear : 250.00
Salpingectomy : 1000.00
Salpingostomy : 1000.00
Schauha's Operation : 5000.00
Tubal Insufflation : 250.00
Tuboplasty : 5000.00
Vaginal Hysterectomy : 2000.00
Vagino Plasty : 2000.00
Wedge Resection of Ovary : 1000.00
Wertheim's Hysterectomy : 5000.00
Amputations :-
Amputations through Arm/Forearm : 2000.00
Amputations through Hand/Foot : 1000.00
Amputations through Thigh/Leg : 2000.00
Disarticulation through major joints of the limb : 2000.00
Disarticulation through small joints of Hand/Foot : 500.00
Excision of supernumery digit : 500.00
Fore Quarter amputation : 5000.00
Hind Quarter amputation : 5000.00
Arthrodesis:-
Arthrodesis of large joints : 2000.00
(Hip, Knee, Shoulder, Ankle, Wrist)
Arthrodesis of small joints of hand/foot : 1000.00
Arthroscopy:-
Arthroscopic surgery
lavage : 2000.00
menisectomy (partial/total) : 2000.00
ligament reconstruction : 2000.00
Removal of loose body : 2000.00
Synovial biopsy : 2000.00
Diagnostic arthroscopy of large joints : 500.00
Diagnostic arthroscopy of small joints : 500.00
Biopsy
C.T. Guided biopsy : 1000.00
Excisional biopsy : 1000.00
Needle biopsy : 500.00
Open biopsy : 500.00
Bone Grafting:-
(To be added up with any operation of internal or external
fixation)
Composite grafting : 2000.00
Fibular/tibial grafting : 1000.00
Iliac crest grafting : 1000.00
Phemester grafting : 2000.00
Rib grafting : 1000.00
Dressings, Debridement:-
Debridement & Repair : 250.00
Fasciectomy : 250.00
Sloughectomy : 250.00
Wound inspection : 250.00
Excision of bone
Patellectomy (Partial/total) : 1000.00
Talectomy : 1000.00
Excision of Accessory bone (Navicular) : 1000.00
Proximal row carpectomy : 1000.00
Fibulectomy : 1000.00
Excisional arthroplasty of:-
Elbow : 2000.00
Hip : 2000.00
Small joints of hand/foot : 2000.00
TM joint : 2000.00
External fixation of fractures:-
External fixation with soft tissue Reconstruc. : 5000.00
procedures
Mini Fixator : 2000.00
Pin and Plaster application : 2000.00
Ring fixator : 5000.00
Tubular external fixator : 2000.00
Internal Fixation of fractures:-
Interlocking nailing : 2000.00
K. Wire fixation : 2000.00
Meyer's Procedure : 5000.00
Nailing : 2000.00
Neck Reconstruction : 5000.00
Plating : 2000.00
Screw fixation : 5000.00
Special plating procedures : 5000.00
S.P. Nail plate : 5000.00
Dynamic Hip Screw : 5000.00
Dynamic Compression Screw : 5000.00
Condylar blade plate :5000.00
Tension Band Wiring : 1000.00
Joint replacements:-
Partial (Hemi) hip replacement : 5000.00
Replacement of small joints of Hand or foot : 5000.00
Total Hip replacement : 8000.00
Total Knee replacement : 8000.00
Total Shoulder/Elbow replacement : 5000.00
Limb lengthening:-
Femoral lengthening : 5000.00
Humeral Lengthening : 5000.00
Metacarpal/Phalangeal lengthening : 5000.00
Tibial lengthening : 5000.00
Manipulations:-
Closed reductions of fractures and : Dislocations : 1000.00
Correction of deformities : 1000.00
Manipulation under G.A. : 1000.00
Muscle/Tendon transfer
Steindler's flexoroplasty : 1000.00
Tendon transfers (Hand &foot):-
Oponensplasty : 1000.00
Egger's procedure : 1000.00
Trapezius transfer : 2000.00
Nerve repair/grafting : 5000.00
Open reduction/dislocations:-
Open reduction of C.D.H. (Cong. Dis. Hip) : 1000.00
Open reduction of C.D.H. with Osteotomy : 2000.00
Open reduction of dislocation : 1000.00
Operations for infection:-
Sequestrectomy : 500.00
Saucerization : 500.00
Sinus tract excision : 50.00
Orthoses/Splints:-
Body jacket (PVC) : 500.00
Cast brace : 500.00
Floor reaction orthosis (FRO) : 1000.00
Hand Splints : 250.00
Osteotomy:-
Corrective osteotomy of long bones : 2000.00
Corrective osteotomy of small bones : 2000.00
French Osteotomy : 2000.00
High tibial osteotomy : 2000.00
MC Murray's Osteotomy
Osteotomy of the pelvis (Salter's
Chiary, pembertion) : 2000.00
Valgus/Varus Osteotomy : 2000.00
Replantation : 8000.00
Skeletal traction:-
Halo Traction/Distraction : 2000.00
Skull Traction : 500.00
Traction through tibia, femur, olecranon, Calcaneum : 250.00
Skin Coverage:-
Abdomenal flap : 2000.00
Cross finger flap : 2000.00
Cross leg flap : 2000.00
Free flap : 5000.00
Full thickness skin grafting : 500.00
Groin flap : 2000.00
Myocutaneous flap : 2000.00
Myoplasty with/without skin grafting : 2000.00
Redicled flap : 2000.00
Rotation flap : 2000.00
Split thickness skin grafting : 500.00
Soft tissue reconstructive procedures:-
Anterior transposition of ulnar nerve : 2000.00
Bankart's operation : 2000.00
Bristwo's operation : 2000.00
Joint Debridement : 2000.00
Ligament reconstruction of the knee,elbow, ankle : 2000.00
Mc Bride procedure : 2000.00
Neurolysis : 2000.00
Putti plat operation : 2000.00
Reconstruction surgery of the hand : 2000.00
(for post-traumatic &Congenital anomalies/deformities) : 2000.00
Synovectomy : 2000.00
Soft tissue release Operations:-
Carpal tunnel release : 1000.00
Defatting operation : 1000.00
Dequervam's release : 1000.00
Dupuytren's soft tissue release : 1000.00
Max page release : 1000.00
Postero medial soft tissue release : 1000.00
Soutter's and younts soft tissue release : 1000.00
Steindler's release : 1000.00
Subcutaneous tenotomy : 1000.00
Syndactyly release : 1000.00
T.A. lengthening : 1000.00
Tenotomy-open : 1000.00
Torticollis release : 1000.00
Trigger finger/thumb release : 1000.00
Wilson's Soft tissue release : 1000.00
Z-plasty for contractures : 1000.00
Spine:-
Anteriorolateral decompression : 5000.00
Anterior loosening : 8000.00
Anterior loosening with instrumentation : 8000.00
Anterior Spinal fusion : 5000.00
Discetomy : 5000.00
Excision of diastematomyelia : 8000.00
Laminectomy : 5000.00
Posterolateral Spinal fusion : 5000.00
Posterior Spinal fusion with instrumentation : 5000.00
Posterolateral Spinal fusion with instrumentation : 5000.00
Spinal fusion (posterior) : 5000.00
Spinal instrumentation (Without fusion) : 5000.00
Transthoracic decompression : 8000.00
Tendon repair/grafting : 2000.00
Tumour Surgery:-
Curettage : 500.00
Curettage with bone grafting : 1000.00
Curettagre with bone cement : 1000.00
Debulking of the tumour : 2000.00
Excision of the tumours of the hand or foot : 1000.00
Radical resection of the large tumour : 2000.00
Resection Arthrodesis (with internal or external fixation) : 5000.00
Adenoidectomy : 500.00
Antral Biopsy : 500.00
Antrum Wash : 250.00
Audiometry : 250.00
Aural Polypectomy : 250.00
Block Dissection of neck : 5000.00
Bronchoscopy : 500.00
C.W.L.(Rt) (Minor) : 1000.00
Caldwell Luc's Operation : 500.00
Direct Laryngoscopy : 500.00
Ethmoidectomy : 2000.00
Excision of Temporal Bone : 5000.00
Foreign Body ear and nose removal : 250.00
Frontal Sinus Operation : 2000.00
Intranasal Antrostomy : 250.00
Laryngectomy : 5000.00
Laryngofissure : 2000.00
Laryngophayryngectomy : 5000.00
Laryngoscopy : 500.00
Lateral Pharyngotomy : 2000.00
Lateral Rhinotomy : 2000.00
Mastoidectomy : 2000.00
Maxillectomy : 2000.00
Meatoplasty : 500.00
Microlaryngoscopy : 500.00
Myringoplasty : 500.00
Myringotomy : 250.00
Nasal Cautery : 250.00
Nasal Polypectomy : 500.00
Oesphagoscopy : 500.00
Ossioloplasty : 2000.00
Partial Glossectomy : 5000.00
Pinnaplasty : 2000.00
Plastopharyngoplasty for Rhinolalia Absenta : 5000.00
R.N.D.: 5000.00
Rhinoplasty (M.R.M.) : 2000.00
Septoplasty : 500.00
Stapedectomy : 5000.00
Submucus Resection of Septum : 500.00
Tonsillectomy : 500.00
Trachesostomy : 500.00
Transpalatal Operation : 2000.00
Turbinectomy : 250.00
Tympanoplasty : 5000.00
Abdominoperineal pull through : 5000.00
Anoplasty for imperforate anus : 2000.00
Appendicectomy : 1000.00
Biopsy of Ulcer : 250.00
Brachial sinus excision : 1000.00
Change of suprapubic cystostomy tube : 100.00
Circumcision : 250.00
Cleft lip (complete repair) : 5000.00
Cleft palate repair : 5000.00
Colonic transplant : 5000.00
Corn excision : 100.00
Corrective procedure for biliary atresia : 5000.00
Cysto panendoscopy : 500.00
Cystolithotomy : 1000.00
Cystostomy : 250.00
Drainage of an abscess suturing of minor laceration under : 250.00
Electrocoagulation : 250.00
Epispadias repair : 1000.00
Examination under G.A. : 250.00
Excision of omphalomesentric duct : 2000.00
Excision of posterior uretheral valve : 2000.00
Excision of rectal polyp : 1000.00
Excision of small cysts Ganglia etc. : 250.00
Gastrostomy : 1000.00
Gut back operation for imperforate anus : 1000.00
Hemihepatectomy : 5000.00
Hydrocortisone Injection of Peyronies disease : 250.00
Ileal or colon conduct : 5000.00
Intercostal drainage : 250.00
Intussusception : 2000.00
Laparotomy with additional procedures like resection &ana : 2000.00
Ligation of umblical polyp : 250.00
Lymphnode Biopsy : 250.00
Meatotomy under G
.A. : 250.00
Minor correction of repaired lip or palate : 250.00
Minor urethroplasty : 250.00
Nephrectomy : 2000.00
Nephrostomy tube change : 250.00
Oesophagostomy : 2000.00
Orchectomy and Orchiopexy : 1000.00
Parotid fistula closure : 1000.00
Pelvic osteotomy : 1000.00
Perineal urethrostomy : 1000.00
Preauricular sinus excision : 1000.00
Prepucial advancement and chorde correction : 1000.00
Prepucial dilatation : 250.00
Primary reconstruction for extrophy of Bladder : 5000.00
Pyelolithotomy : 2000.00
Pyeloplasty : 2000.00
Pyeloroplasty with or without vagotomy : 2000.00
Pyloromyotomy : 2000.00
Repair of hiatus hernia : 2000.00
Repair of partial cleft lip : 1000.00
Retrograde seminal vesiculography : 250.00
Revision/dilatation of ileostomy/colostomy : 250.00
Rib resection and drainage : 1000.00
Scar excision under G.A. : 250.00
Secondary procedure for extrophy of the bladder : 1000.00
Sigmodioscopy under G.A. : 500.00
Skin tag excision under G.A. : 250.00
Spleenectomy : 2000.00
Stitch removal under G.A. : 250.00
Surgical separation of conjoined siamese twins : 8000.00
Syndactyle : 250.00
Tapping of hydrocele : 250.00
Testicular biopsy : 250.00
Thyroglossal duct excision : 1000.00
Thyroglossal sinus and fistula excision : 1000.00
Total correction of extrophy of urinary bladder : 5000.00
Tracheo-oesophageal fistula with Oesophagealatresia : 5000.00
Transposition of anus for ectopic anus : 2000.00
Ureterostomy or ureters sigmoidostomy : 5000.00
Urethroplasty for penile or penoscrotal type hypospadias : 5000.00
Urinary diversion e.g. cutaneous : 2000.00
Ventriculoatrial shunt : 2000.00
Cystolithotripsy Endoscopic : 2000.00
Davis intubated ureterostomy : 2000.00
Dilatation of Urethra : 250.00
ESWL Procedure (Lithotripsy) : 9000.00
Endoscopic Basketing : 1000.00
Excision of Renal Cyst : 2000.00
Excision of Stricture : 2000.00
Excision of Suprapubic Fistula : 2000.00
Excision of adrenal cyst : 2000.00
Excision of pheochromocytoma or Adrenal tumours : 5000.00
Excision of suprapubic fitula : 1000.00
Exploration of Kidney : 2000.00
Fulguration of bladder tumour : 2000.00
Ileal loop diversion : 5000.00
Internal ureterotomy : 1000.00
Nephrectomy : 2000.00
Nephrolithotomy : 2000.00
Nephrostomy : 1000.00
Radical Prostatectomy : 5000.00
Retrograde Pyelography : 1000.00
Retropublic prostatectomy : 2000.00
Suprapublic transvesical bladder neck Resection : 2000.00
Supreapubic transvesical excision of bladder tumour : 2000.00
Supreapublic transvesical prostatectomy : 2000.00
Total cystotomy : 5000.00
Total uretherectomy with pelvic exentiration : 5000.00
Transurethral resection of bladder neck : 2000.00
Transurethral resection of bladder tumour : 2000.00
Ureterolithotomy : 2000.00
Ureteroneocystostomy : 5000.00
Ureterorolysis : 2000.00
Vaginal cystolithotomy : 5000.00
Vesicoepidydimal anastomosis :5000.00
Archived Revised Rates of Hospital Charges All India Institute of Medical Sciences New Delhi, India
Blood Clinical Chemistry
ABO & RH Grouping 50
| Sr. No. | Radio Diagnosis | OPD/General Ward | Private Ward |
|---|---|---|---|
| 1 | Plain X-Ray (per film)
|
|
|
| 2 | Gastro Intestinal & Hepatobiliary
|
|
|
| 3 | Urinary
|
|
|
| 4 | Mammography
|
|
|
| 5 | Miscellaneous
|
|
|
| 6 | Ultrasound
|
|
|
| 7 | CT and CT Guided Interventions
|
|
|
| ANTI HCV HEPATITIS C | 0 |
| ANTI-HBc IgM ANTIBODY | 0 |
| ANTI-HBs ANTIBODY | 0 |
| Name of the Test | AIIMS OPD Patients | AIIMS Pvt. Ward & Other Pvt. Hospital | Overseas Patient |
|---|---|---|---|
| I.Serology based | - | - | - |
| HLA B 27 | 500/- | 800/- | 1000/- |
| HLA -ABC | 800/- | 1500/- | 3000/- |
| HLA-DR.DQ | 800/- | 1500/- | 3000/- |
| HLA-ABC &DR/DQ | 1200/- | 2500/- | 5000/- |
| Cross Matching(serology) | 300/- | 500/- | 1000/- |
| PRA | 500/- | 1500/- | 2000/- |
| Flowcytometric(cross matching) | 500/- | 1500/- | 1500/- |
| II.Paternity/Immigratilon cases | - | - | - |
| HLA-DNA Class-I&DRBI low resolution | 10000/- | 10000/- | 15000/- |
| HLA DQ Alpha | 4000/- | - | - |
| III.Molecular Biology Test | - | - | - |
| HLA-Class I | 3000/- | 4000/- | 6000/- |
| HLA- Class II(low resolution) DRBI DR 52, DR53 | 3000/- | 4000/- | 6000/- |
| HLA Class II (high resolution)( DRBI B3, B4, 5) | 3000/- | 4000/- | 7000/- |
| HLA-DQ Beta | 3000/- | 4000/- | 6000/- |
PCR for CMV 600
PCR for HSV (1&2) 600
RT-PCR for enteroviruses 900
RT-PCR for HCV 1500
Diagnostic Seriological assays For syphilis 50
Diagnostic Seriological assays 50 For Anti-streptolysine O Antibodies
| S.No. | Type of Investigation &Category of patients. | Fee Rs. |
|---|---|---|
| 1. | Plain MRI OPD/Indoor (Pvt. Wards) | 3000/- Plus >Rs.500/- (for films) |
| 2. | Plain MRI Indoor (General Wards) | 2500/- Plus Rs.500/- (for films) |
| 3. | Plain MRI Outside (Medico-legal cases and other exceptional cases) | 3500/- (with films) |
| 4. | Additional clinical studies like MRA, MRS and/or additional parts being scanned during the same sitting. Additional payment is required. (applicable to each category of S.N. 1,2 &3) | 1500/- |
| 5. | Extra cost for contrast MRI. Applicable to each category of S.N. 1,2 3 &4. | A) 2600 For patients of age 12 years and above B) 1500 For children less than 12 years of age |
| 6. | MRS for research | 3000/-(no films will be issued) |
Ability Assessment : 100.00
Aptitude Assessment : 100.00
Interest Assessment : 100.00
Memory Function test : 100.00
Organic Brain Damage Battery : 100.00
Personality Assessment (Full) : 100.00
Projective test (single) : 100.00
Questionnaire test (single) : 100.00
Test for Attention and concentration : 100.00
Test for Intelligence : 100.00
Test for thinking function : 100.00
Amniotic fluid AFP assay : 300.00
Amniotic fluid or urine 2 D :750.00
Blood/Bone marrow for chromosomes : 750.00
Buccal Smear for Sex Chromatin : 25.00
CVS for sexing for X-linked disease : 1500.00
Carrier Screening for thalassemia Nestroff and Hb A2 : 300.00
Carrier detection of DMD/Hemophillia/DNA diagnosis : 6000.00
Chemical test in urine : 150.00
Chromosomal study of blood/bone marrow : 500.00
Chromosomes from CVS by culture, or by amninotic culture : 3500.00
DNA based mutation Detection in thalassemia : 3500.00
DNA based mutation detection on DMD or other diseases : 3500.00
Electronic Cell Count : 150.00
Electrophoresis for MPS Amniotic fluid acetyle : 750.00
Galactosemia quantitative enzyme assay : 750.00
Galactosemia screening : 300.00
Genetic Karyotyping : 500.00
Leucocyte enzyme assay Arylsulfatase A, Hemosamindase : 750.00
MPS 24 Hrs,estimation with creatinine : 300.00
MPS spot test on urine : 150.00
Maternal serum AFP assay : 300.00
Maternal serum HCG assay : 300.00
Plasma/urine Quantitative Aminoscids : 1500.00
Prenatal diagnosis of Ataxia Telengiectasia or Fragile X : 6000.00
Prenatal diagnosis of thalassemia DMD Hemophilia, or Enzyme : 4500.00
Urine/plasma aminoacid screening : 300.00
Miscellaneous tests sent abroad
Miscellaneous - special diet / Drug / Injection.
| D-xylose &24 hour Fecal Fat Diagnosis Test : 50.00 |
| Aminoacid chromatography of urine/ plasma : 200.00 |
| Amniotic fluid or urine 2D for MPS : 750.00 |
| Chemical Test in urine : 75.00 |
| Glactosemia screening (Beutler spot fluorescence test) : 300.00 |
| Leucocyte enzyme assay (with control enzymes) : 500.00 |
| MPS spot test on urine : 75.00 |
| Triple marker screen (antenatal) : 850.00 |
| Prenatal diagnosis by enzyme assay : 500.00 |
| Leucocyte enzyme assay for Hurler (MPS) : 1000.00 |
| Celaic Serology : 500.00 |
| DNA based mutation detection in Thalassemia : 2000.00 |
| Prenatal diagnosis of Thalassemia :2000.00 |
| Xmm Polymorphism study : 1000.00 |
| Deletion studies in DMD : 2000.00 |
| Prenatal diagnosis of DMD by deletion studies : 2000.00 |
| Carrier screening by linkage studies in DMD : 2000.00 |
| DNA studies in SMA : 1500.00 |
| Prenatal diagnosis of SMA : 1500.00 |
| Carrier detection of Hemophilia A/B : 2000.00 |
| Prenatal diagnosis of Hemophilia A/B : 2000.00 |
| Fragile X PCR study : 1000.00 |
| 4 connexin 26 mutations : 1000.00 |
| Rh genotyping of Blood /AF : 1000.00 |
| Prenatal diagnosis of cord blood sampling : 750.00 (Karyotyping + Klehaur’s tests |
| Chromosomal study of blood Karyotyping : 500.00 |
| Chromosomes from CVS culture : 2500.00 |
| Chromosomes from Abortus tissue : 2500.00 |
B.M. Test for Eustachian Tube Function : 50.00
Bekesy Audiometry : 50.00
Caloric Test : 50.00
Electrogenstometry : 50.00
Olfactometry : 50.00
AFP : 450.00
Beta Heg : 450.00
CEA : 450.00
Estrogen receptor : 900.00
Progestron receptor : 900.00
T3 : 200
T4 : 200
TSH : 200
LH : 225
FSH : 225
Prolactin : 225
Estradiol : 225
Progesterone : 225
Alpha FP : 225
Testosterone : 225
HCG : 225
PSA : 275
DHEA : 300
DHEA-S : 300
Cortisol : 225
CA-125 : 500
b HCG : 250
Routine Semen Analysis : 40
Seminal Fructose (Quantitative) : 40 (Qualitative) : 20
Seminal Citric Acid : 25
Hypoosmatic Swelling Test (HOS) : 20
Acrosome intactness : 50
Sperm nuclear chromatin decondensation : 50
Sperm Mitochondrial Activity index : 50
Sperm Glyceryl Phosphoryl choline (GPC) : 250
Immunobead test IgG : 615
Complete sperm morphology : 50
T3 : 200
T4 : 200
TSH : 200
LH : 225
FSH : 225
PROLACTIN : 225
TESTOSTERONE : 225
DHEA-S : 300
CORTISOL : 225
INSULIN : 225
C PEPTIDE : 300
G H : 250
IGF-I : 1000
ISLET CELL ANTIBODY : 1000
MICRO ALBUMIN : 300
ANDROSTEREDIONE : 300
DHT : 1000
ACTH + CORTISOL : 1000
ALDOSTERONE : 400
17-OHP : 400
PTH-C TERMINAL with Calcium : 1000
VIT. D 25, OH : 1000
THYROID ANTIBODY (TPO) : 300
Embalming of ordinary (non-autopsied) bodies : 2000
Embalming of autopsied bodies : 4000
Prenatal Diagnostic services for Chromosomal abnormalities using amniotic cultures and conventional Karyotyping : 7000
Fluoride Test : 25
Conventioal Cytogenetics : 500
FISH (Molecular Cytogenetics) : 4000
| Single site study | 400 |
| Two sites study | 600 |
| Three sites study | 800 |
| Whole body study | 1000 |
| ANTISMOOTH MUSCLE ANTIBODY BY IMMUNOFLUORESCENCE METHOD | 0 |
| Agl - I gG | 100 |
| Agl - I gM | 100 |
| ANTI ds DNA | 100 |
| ANCA | 50 |
| ANA (HEP-2) | 100 |
| ANTI-LKM-1 | 200 |
| ANTINUCLEAR ANTIBODY TEST | 50 |
| ANTITHYROID ANTIBODY TEST | 50 |
| APCR | 300 |
| AT III | 400 |
| BETA 2 GLYCOPROTEIN | 0 |
| C-3 QUANTIFICATION IN SERUM/ OTHER FLUIDS | 50 |
| CARRIER DETECTION HAEMOPHILLIA | 2000 |
| CARRIER DETECTION PRENATAL | 2000 |
| CRP &PCT FOR SEPSIS- CRP QUALITATIVE KIT | 0 |
| CRP &PCT FOR SEPSIS -CRP QUANTITATIVE KIT | 0 |
| CRYOGLOBULINS | 50 |
| D-XYLOSE &24 HR FECAL FAT ESTIMATION | 0 |
| FACTOR ASSAY | 1200 |
| HEPARIN ASSAY | 250 |
| HEPATITIS ANTIGEN TEST | 50 |
| HOMOCYSTEIN | 0 |
| HPLC | 300 |
| IMMUNOELECTROPHORESIS PER ANTIBODY | 0 |
| IMMUNOPHLOROSCENCE ASSAY(IFA)&TTG ELISA FOR DIAGNOSIS OF - CELIAC DISEASE | 0 |
| IMMUNNOGLOBULINS A | 100 |
| IMMUNNOGLOBULINS G | 100 |
| IMMUNNOGLOBULINS M | 100 |
| IMMUNOTYPING FIVE ANTIBODY | 0 |
| IMMUNOTYPING ONE ANTIBODY | 0 |
| LATEX RHEUMTOID FACTOR TEST | 50 |
| MOLECULAR GENETIC STUDIES BY RQ –RT PCR | 3000 |
| MUTATION DETECTION F V LAIDEN | 0 |
| MUTATION DETECTION MTHFR | 0 |
| MUTATION DETECTION P 20210 | 0 |
| NITRO BLUE TETRAZOLIUM TEST FOR CHRONIC GRANULOMATOUS - DISEASE | 0 |
| PCT QUANTITATIVE KIT | 0 |
| PRO C GLOBAL | 500 |
| PROTEIN C CLOTTING | 0 |
| PROTEIN C ELISA | 0 |
| PROTEIN S CLOTTING | 0 |
| PROTEIN S ELISA | 0 |
| RA | 0 |
| RISTOCETIN | 0 |
| VWD | 0 |
| IGMACL | 100 |
Pulmonary Function Test 250
Supply of one unit Blood (Pvt. Ward) 250.00
Abscess incision : 250.00
Acrylic Full Crown : 100.00
Activator : 250.00
All extractions in one Jaw : 250.00
Alveolectomy : 250.00
Apical Curettage : 250.00
Biopsy : 250.00
Cast Inlay per tooth (Non-precious alloy) : 100.00
Complete Denture Acrylic - One jaw : 500.00
Complete Denture Acrylic - both jaws : 1000.00
Complete Denture with metal basis-both jaws : 2000.00
Condylectomy : 1000.00
Cysectomy : 250.00
Definitive Obturator with teeth : 500.00
Dental Restoration Class-I with AG amalgam/composite : 50.00
Dental Restoration Class-II with AG amalgam composite : 100.00
Expansion plate (excluding screw to be brought by patient : 250.00
Extraction per tooth : 25.00
Fistula closure : 250.00
Fistulectomy : 250.00
Fixation of Fracture of Jaw : 1000.00
Fixed Appliances both jaw : 1000.00
Fixed Applicances one jaw : 500.00
Fixed Partial Denture 3 units with Porcelain : 250.00
Fixed Partial Denture 3 units with : 2000.00
porcelain veenering - Non-precious alloy
Fixed Partial Denture per additional tooth with : 250.00
porcelain veenering - semi precious alloy
Fixed partial denture - 3 units with acrylic veneering : 1000.00
Fixed partial denture 3 units in gold alloy (excluding gold : 500.00
Fixed partial denture per additional tooth in gold alloy : 250.00
Fixed partial denture per additional unit with acrilic : 500.00
Fracture Jaws closed reduction : 500.00
Fracture Jaws open reduction : 1000.00
Frenectomy :rown (Nickel Chrome) : 200.00
Gingivectomy full mouth : 1000.00
Gingivectomy per segment : 250.00
Growth removal : 250.00
Head Gear (excluding sctraps to be brought by patients : 250.00
Inclined plane/repair of plane : 100.00
Mandibulectomy : 2000.00
Nasal/Auricular/Orbital Prosthesis : 250.00
Orthodontic Appliance, Bite plates, Retraction plate : 250.00
Osteotomy : 1000.00
Pericoronotomy : 150.00
Peripheral Neurectomy : 500.00
Porcelain Full Crown : 250.00
Porcelain to metal crown : 500.00
Pulpotomy : 250.00
Removable Acrylic Partial Denture per additional tooth : 50.00
Removable Acrylic Partial Denture with one tooth : 100.00
Removable Cast Partial Denture (Chromecobalt) per additional : 50.00
Removable Cast Partial Denture (Chromecobalt) with one tooth : 500.00
Removal of Impaction : 250.00
Repairing/ Relining Denture : 100.00
Resection of jaw : 2000.00
Rochett's (Maryland) Bridge 3 units : 250.00
Root Planning : 250.00
Root amputation : 250.00
Root canal treatment : 250.00
Segmental resection of jaw : 1000.00
Sequestrectomy : 250.00
Sialolithotomy : 250.00
Silver cast splint per dental arch : 250.00
Single Jacket Crown/Dowel crowh in non precious alloy with : 250.00
Single three quarter crown (Nickel - Chrome) : 250.00
Surgical Obturator/Intermediate obturator (without teeth) : 100.00
Total extraction both jaws : 1000.00
Tumour Excision : 1000.00
Veneering - Non precious alloy : 1000.00
Abscess Drainage under G.A. : 250.00
Aspiration of cold abscess/cysts : 250.00
Biopsy (Punch/ Excision/ Cervical cone/Endometrial : 250.00
Bone Tumor/Testicular--)
Cervical sympathectomy : 2000.00
Circumcision : 250.00
Colostomy closure : 5000.00
Excision and skin graft of contracture : 1000.00
Excision benign breast lumps : 250.00
Excision of cheek cancer : 2000.00
Excision of Small tumour : 250.00
Excision of rectum : 2000.00
Feeding Jejunostomy/ Gastrostomy : 250.00
Fissurectomy : 250.00
Fistulectomy : 250.00
Fractional Curettage : 500.00
Haemorrhoids : 250.00
Hemicollectomy : 5000.00
Incision & Drainage : 250.00
Injection of keloids : 250.00
Intestinal biopsy : 250.00
Kidney transplant : 8000.00
Laceration suture abscess drainage under local anaesthesia :100.00
Laparoscopy : 500.00
Laprotomy + Additional procedure : 2000.00
Oopherectomy : 2000.00
Operation for gall stones : 2000.00
Operations for Intestinal obstruction : 5000.00
Operations for pancreas : 5000.00
Operations for peptic ulcer/ stomach cancer : 5000.00
Operations for surgical jaundice : 2000.00
Operations for tuberculosis cancer of the Bowel : 2000.00
Partial Amputation Penis : 250.00
Preparation and transfer of tube pedicles and flap : 250.00
Radical Amputation Penis : 2000.00
Radical mastectomy : 2000.00
Repair of External Hernia : 1000.00
Repair of facial fracture : 1000.00
Sequestrectomy : 250.00
Simple mastectomy : 1000.00
Surgery for portation : 8000.00
Thyroidectomy : 5000.00
Trachectomy : 1000.00
Tracheostomy : 500.00
Undescended testis operative procedure : 1000.00
A.V. Shunt : 1000.00
CAPD (Tenkoff) Cathetre implantation : 1000.00
CAVH : 2000.00
CAVHD : 2000.00
CVVH : 2000.00
CVVHD : 2000.00
Femoral Vein cathetrisation : 500.00
Haemodialysis on keil dialyser : 2000.00
Insertion of A.V. Canula for Acute Haemodialysis : 500.00
Peritoneal dialysis cathetrisation (intermittent) : 1000.00
Plasmapheresis : 1000.00
Subclavian vein perm cathetre implantation : 1000.00
Abdominal perineal Ext.Hysterectomy : 2000.00
Abdominal perineal neo construction Cx+Uteria+Vagina : 5000.00
Caesaerian Hysterectomy : 2000.00
Cervical Biopsy : 250.00
Colopotomy : 500.00
Colpollaisis/Colporrhophy : 2000.00
Cone Biopsy Cervix : 500.00
Cryosurgery : 250.00
D & C : 500.00
Deliveries Normal : 2000.00
Dilatation of Cervix : 250.00
Electro Cauterization : 250.00
Endometrial Biopsy : 250.00
Evacuation : 500.00
Fractional Curettage : 500.00
Gynaecography : 1000.00
H/C V.V.F. & R.V.F. : 2000.00
Hydrotubation : 250.00
Hymenectomy : 250.00
Hysterectomy (Abdominal) : 2000.00
Hysterectomy (Wertheims) : 5000.00
Normal R/o Placenta : 1000.00
Operation for stress incontinence : 2000.00
Ovarion Cystectomy : 2000.00
Ovaritomy : 2000.00
Pelvic Exenteration : 5000.00
Plastic Operation on uterus : 2000.00
Radical Vulvectomy : 5000.00
Repair of Perineal Tear : 250.00
Salpingectomy : 1000.00
Salpingostomy : 1000.00
Schauha's Operation : 5000.00
Tubal Insufflation : 250.00
Tuboplasty : 5000.00
Vaginal Hysterectomy : 2000.00
Vagino Plasty : 2000.00
Wedge Resection of Ovary : 1000.00
Wertheim's Hysterectomy : 5000.00
Amputations :-
Amputations through Arm/Forearm : 2000.00
Amputations through Hand/Foot : 1000.00
Amputations through Thigh/Leg : 2000.00
Disarticulation through major joints of the limb : 2000.00
Disarticulation through small joints of Hand/Foot : 500.00
Excision of supernumery digit : 500.00
Fore Quarter amputation : 5000.00
Hind Quarter amputation : 5000.00
Arthrodesis:-
Arthrodesis of large joints : 2000.00
(Hip, Knee, Shoulder, Ankle, Wrist)
Arthrodesis of small joints of hand/foot : 1000.00
Arthroscopy:-
Arthroscopic surgery
lavage : 2000.00
menisectomy (partial/total) : 2000.00
ligament reconstruction : 2000.00
Removal of loose body : 2000.00
Synovial biopsy : 2000.00
Diagnostic arthroscopy of large joints : 500.00
Diagnostic arthroscopy of small joints : 500.00
Biopsy
C.T. Guided biopsy : 1000.00
Excisional biopsy : 1000.00
Needle biopsy : 500.00
Open biopsy : 500.00
Bone Grafting:-
(To be added up with any operation of internal or external
fixation)
Composite grafting : 2000.00
Fibular/tibial grafting : 1000.00
Iliac crest grafting : 1000.00
Phemester grafting : 2000.00
Rib grafting : 1000.00
Dressings, Debridement:-
Debridement & Repair : 250.00
Fasciectomy : 250.00
Sloughectomy : 250.00
Wound inspection : 250.00
Excision of bone
Patellectomy (Partial/total) : 1000.00
Talectomy : 1000.00
Excision of Accessory bone (Navicular) : 1000.00
Proximal row carpectomy : 1000.00
Fibulectomy : 1000.00
Excisional arthroplasty of:-
Elbow : 2000.00
Hip : 2000.00
Small joints of hand/foot : 2000.00
TM joint : 2000.00
External fixation of fractures:-
External fixation with soft tissue Reconstruc. : 5000.00
procedures
Mini Fixator : 2000.00
Pin and Plaster application : 2000.00
Ring fixator : 5000.00
Tubular external fixator : 2000.00
Internal Fixation of fractures:-
Interlocking nailing : 2000.00
K. Wire fixation : 2000.00
Meyer's Procedure : 5000.00
Nailing : 2000.00
Neck Reconstruction : 5000.00
Plating : 2000.00
Screw fixation : 5000.00
Special plating procedures : 5000.00
S.P. Nail plate : 5000.00
Dynamic Hip Screw : 5000.00
Dynamic Compression Screw : 5000.00
Condylar blade plate :5000.00
Tension Band Wiring : 1000.00
Joint replacements:-
Partial (Hemi) hip replacement : 5000.00
Replacement of small joints of Hand or foot : 5000.00
Total Hip replacement : 8000.00
Total Knee replacement : 8000.00
Total Shoulder/Elbow replacement : 5000.00
Limb lengthening:-
Femoral lengthening : 5000.00
Humeral Lengthening : 5000.00
Metacarpal/Phalangeal lengthening : 5000.00
Tibial lengthening : 5000.00
Manipulations:-
Closed reductions of fractures and : Dislocations : 1000.00
Correction of deformities : 1000.00
Manipulation under G.A. : 1000.00
Muscle/Tendon transfer
Steindler's flexoroplasty : 1000.00
Tendon transfers (Hand &foot):-
Oponensplasty : 1000.00
Egger's procedure : 1000.00
Trapezius transfer : 2000.00
Nerve repair/grafting : 5000.00
Open reduction/dislocations:-
Open reduction of C.D.H. (Cong. Dis. Hip) : 1000.00
Open reduction of C.D.H. with Osteotomy : 2000.00
Open reduction of dislocation : 1000.00
Operations for infection:-
Sequestrectomy : 500.00
Saucerization : 500.00
Sinus tract excision : 50.00
Orthoses/Splints:-
Body jacket (PVC) : 500.00
Cast brace : 500.00
Floor reaction orthosis (FRO) : 1000.00
Hand Splints : 250.00
Osteotomy:-
Corrective osteotomy of long bones : 2000.00
Corrective osteotomy of small bones : 2000.00
French Osteotomy : 2000.00
High tibial osteotomy : 2000.00
MC Murray's Osteotomy
Osteotomy of the pelvis (Salter's
Chiary, pembertion) : 2000.00
Valgus/Varus Osteotomy : 2000.00
Replantation : 8000.00
Skeletal traction:-
Halo Traction/Distraction : 2000.00
Skull Traction : 500.00
Traction through tibia, femur, olecranon, Calcaneum : 250.00
Skin Coverage:-
Abdomenal flap : 2000.00
Cross finger flap : 2000.00
Cross leg flap : 2000.00
Free flap : 5000.00
Full thickness skin grafting : 500.00
Groin flap : 2000.00
Myocutaneous flap : 2000.00
Myoplasty with/without skin grafting : 2000.00
Redicled flap : 2000.00
Rotation flap : 2000.00
Split thickness skin grafting : 500.00
Soft tissue reconstructive procedures:-
Anterior transposition of ulnar nerve : 2000.00
Bankart's operation : 2000.00
Bristwo's operation : 2000.00
Joint Debridement : 2000.00
Ligament reconstruction of the knee,elbow, ankle : 2000.00
Mc Bride procedure : 2000.00
Neurolysis : 2000.00
Putti plat operation : 2000.00
Reconstruction surgery of the hand : 2000.00
(for post-traumatic &Congenital anomalies/deformities) : 2000.00
Synovectomy : 2000.00
Soft tissue release Operations:-
Carpal tunnel release : 1000.00
Defatting operation : 1000.00
Dequervam's release : 1000.00
Dupuytren's soft tissue release : 1000.00
Max page release : 1000.00
Postero medial soft tissue release : 1000.00
Soutter's and younts soft tissue release : 1000.00
Steindler's release : 1000.00
Subcutaneous tenotomy : 1000.00
Syndactyly release : 1000.00
T.A. lengthening : 1000.00
Tenotomy-open : 1000.00
Torticollis release : 1000.00
Trigger finger/thumb release : 1000.00
Wilson's Soft tissue release : 1000.00
Z-plasty for contractures : 1000.00
Spine:-
Anteriorolateral decompression : 5000.00
Anterior loosening : 8000.00
Anterior loosening with instrumentation : 8000.00
Anterior Spinal fusion : 5000.00
Discetomy : 5000.00
Excision of diastematomyelia : 8000.00
Laminectomy : 5000.00
Posterolateral Spinal fusion : 5000.00
Posterior Spinal fusion with instrumentation : 5000.00
Posterolateral Spinal fusion with instrumentation : 5000.00
Spinal fusion (posterior) : 5000.00
Spinal instrumentation (Without fusion) : 5000.00
Transthoracic decompression : 8000.00
Tendon repair/grafting : 2000.00
Tumour Surgery:-
Curettage : 500.00
Curettage with bone grafting : 1000.00
Curettagre with bone cement : 1000.00
Debulking of the tumour : 2000.00
Excision of the tumours of the hand or foot : 1000.00
Radical resection of the large tumour : 2000.00
Resection Arthrodesis (with internal or external fixation) : 5000.00
Adenoidectomy : 500.00
Antral Biopsy : 500.00
Antrum Wash : 250.00
Audiometry : 250.00
Aural Polypectomy : 250.00
Block Dissection of neck : 5000.00
Bronchoscopy : 500.00
C.W.L.(Rt) (Minor) : 1000.00
Caldwell Luc's Operation : 500.00
Direct Laryngoscopy : 500.00
Ethmoidectomy : 2000.00
Excision of Temporal Bone : 5000.00
Foreign Body ear and nose removal : 250.00
Frontal Sinus Operation : 2000.00
Intranasal Antrostomy : 250.00
Laryngectomy : 5000.00
Laryngofissure : 2000.00
Laryngophayryngectomy : 5000.00
Laryngoscopy : 500.00
Lateral Pharyngotomy : 2000.00
Lateral Rhinotomy : 2000.00
Mastoidectomy : 2000.00
Maxillectomy : 2000.00
Meatoplasty : 500.00
Microlaryngoscopy : 500.00
Myringoplasty : 500.00
Myringotomy : 250.00
Nasal Cautery : 250.00
Nasal Polypectomy : 500.00
Oesphagoscopy : 500.00
Ossioloplasty : 2000.00
Partial Glossectomy : 5000.00
Pinnaplasty : 2000.00
Plastopharyngoplasty for Rhinolalia Absenta : 5000.00
R.N.D.: 5000.00
Rhinoplasty (M.R.M.) : 2000.00
Septoplasty : 500.00
Stapedectomy : 5000.00
Submucus Resection of Septum : 500.00
Tonsillectomy : 500.00
Trachesostomy : 500.00
Transpalatal Operation : 2000.00
Turbinectomy : 250.00
Tympanoplasty : 5000.00
Abdominoperineal pull through : 5000.00
Anoplasty for imperforate anus : 2000.00
Appendicectomy : 1000.00
Biopsy of Ulcer : 250.00
Brachial sinus excision : 1000.00
Change of suprapubic cystostomy tube : 100.00
Circumcision : 250.00
Cleft lip (complete repair) : 5000.00
Cleft palate repair : 5000.00
Colonic transplant : 5000.00
Corn excision : 100.00
Corrective procedure for biliary atresia : 5000.00
Cysto panendoscopy : 500.00
Cystolithotomy : 1000.00
Cystostomy : 250.00
Drainage of an abscess suturing of minor laceration under : 250.00
Electrocoagulation : 250.00
Epispadias repair : 1000.00
Examination under G.A. : 250.00
Excision of omphalomesentric duct : 2000.00
Excision of posterior uretheral valve : 2000.00
Excision of rectal polyp : 1000.00
Excision of small cysts Ganglia etc. : 250.00
Gastrostomy : 1000.00
Gut back operation for imperforate anus : 1000.00
Hemihepatectomy : 5000.00
Hydrocortisone Injection of Peyronies disease : 250.00
Ileal or colon conduct : 5000.00
Intercostal drainage : 250.00
Intussusception : 2000.00
Laparotomy with additional procedures like resection &ana : 2000.00
Ligation of umblical polyp : 250.00
Lymphnode Biopsy : 250.00
Meatotomy under G
.A. : 250.00
Minor correction of repaired lip or palate : 250.00
Minor urethroplasty : 250.00
Nephrectomy : 2000.00
Nephrostomy tube change : 250.00
Oesophagostomy : 2000.00
Orchectomy and Orchiopexy : 1000.00
Parotid fistula closure : 1000.00
Pelvic osteotomy : 1000.00
Perineal urethrostomy : 1000.00
Preauricular sinus excision : 1000.00
Prepucial advancement and chorde correction : 1000.00
Prepucial dilatation : 250.00
Primary reconstruction for extrophy of Bladder : 5000.00
Pyelolithotomy : 2000.00
Pyeloplasty : 2000.00
Pyeloroplasty with or without vagotomy : 2000.00
Pyloromyotomy : 2000.00
Repair of hiatus hernia : 2000.00
Repair of partial cleft lip : 1000.00
Retrograde seminal vesiculography : 250.00
Revision/dilatation of ileostomy/colostomy : 250.00
Rib resection and drainage : 1000.00
Scar excision under G.A. : 250.00
Secondary procedure for extrophy of the bladder : 1000.00
Sigmodioscopy under G.A. : 500.00
Skin tag excision under G.A. : 250.00
Spleenectomy : 2000.00
Stitch removal under G.A. : 250.00
Surgical separation of conjoined siamese twins : 8000.00
Syndactyle : 250.00
Tapping of hydrocele : 250.00
Testicular biopsy : 250.00
Thyroglossal duct excision : 1000.00
Thyroglossal sinus and fistula excision : 1000.00
Total correction of extrophy of urinary bladder : 5000.00
Tracheo-oesophageal fistula with Oesophagealatresia : 5000.00
Transposition of anus for ectopic anus : 2000.00
Ureterostomy or ureters sigmoidostomy : 5000.00
Urethroplasty for penile or penoscrotal type hypospadias : 5000.00
Urinary diversion e.g. cutaneous : 2000.00
Ventriculoatrial shunt : 2000.00
Cystolithotripsy Endoscopic : 2000.00
Davis intubated ureterostomy : 2000.00
Dilatation of Urethra : 250.00
ESWL Procedure (Lithotripsy) : 9000.00
Endoscopic Basketing : 1000.00
Excision of Renal Cyst : 2000.00
Excision of Stricture : 2000.00
Excision of Suprapubic Fistula : 2000.00
Excision of adrenal cyst : 2000.00
Excision of pheochromocytoma or Adrenal tumours : 5000.00
Excision of suprapubic fitula : 1000.00
Exploration of Kidney : 2000.00
Fulguration of bladder tumour : 2000.00
Ileal loop diversion : 5000.00
Internal ureterotomy : 1000.00
Nephrectomy : 2000.00
Nephrolithotomy : 2000.00
Nephrostomy : 1000.00
Radical Prostatectomy : 5000.00
Retrograde Pyelography : 1000.00
Retropublic prostatectomy : 2000.00
Suprapublic transvesical bladder neck Resection : 2000.00
Supreapubic transvesical excision of bladder tumour : 2000.00
Supreapublic transvesical prostatectomy : 2000.00
Total cystotomy : 5000.00
Total uretherectomy with pelvic exentiration : 5000.00
Transurethral resection of bladder neck : 2000.00
Transurethral resection of bladder tumour : 2000.00
Ureterolithotomy : 2000.00
Ureteroneocystostomy : 5000.00
Ureterorolysis : 2000.00
Vaginal cystolithotomy : 5000.00
Vesicoepidydimal anastomosis :5000.00
Heart is a muscular pump, made up of specialized muscles. The right half of the heart receives impure (deoxygenated) blood from the body and pumps it into the lungs. The left half of the heart receives pure (oxygenated) blood and pumps it to the rest of the body. The left half of the heart is stronger and thicker.
In order to function, the heart needs nourishment. The nourishment comes to the heart via blood which is supplied to the heart through two major coronary arteries : left and right coronary arteries. The left coronary artery again divides into two major branches (left anterior descending and left circumflex arteries), from which several smaller branches arise and supply the heart. Thus, there are three major arteries : left anterior descending artery, left circumflex artery and right coronary artery.
Principle :In CABG, a new route of blood flow is created by using a piece of blood vessel (graft). One end of the graft is attached to the aorta or one of its branches and the other end of the graft is attached to the diseased coronary artery beyond the blockage. Thus, the obstruction is bypassed.
Types of Graft :The graft may be an artery or a vein. Arterial grafts are considered superior as these remain patent for a longer period. Commonly used arterial grafts are :
Among the vein grafts, long saphenous vein is used most frequently. It is obtainedfrom leg and thigh of the patient. Selection of the grafts is based upon the nature of blockage, condition of coronary arteries and function of the heart.
Approaches and techniques :The traditional the and commonly used technique involves an incision down the front of the chest through the breastbone or sternum. This incision is called a “median sternotomy”. Sometimes a smaller incision is used on the left side of the chest. This technique is referred to as “Minimally invasive coronary artery bypass” or MICAB. In MICAB, it is expected that patient will have less pain and faster recovery. Most commonly, the patient is attached to the heart lung machine and the heart is stopped during CABG. In selected cases, the heart lung machine is not used and CABG is performed on a beating heart
Risks and complications:Though CABG is a safe operation, about 5% patients develop some form of complications. It is a major operation and depending upon the condition of the patient, there is a small but definite risk to the life. Other potential complications of CABG include bleeding or infection, stroke (which is primarily related to age and history of previous stroke), kidney failure (related in large measure to the kidney function before the surgery), and heart attack during or after the surgery. The risk of complications generally depends upon age, general health, smoking history, specific medical conditions, and most importantly, the heart function.
The outcome of surgery and long term success:The operation abolishes angina in almost all patients and minimizes the risk of future heart attacks. However, some patients may have residual angina even after CABG, but it is of lesser severity. CABG is also known to prolong the expected survival (life-span) in a specific subgroups of patients. One should understand clearly that CABG does not abolish or retard the process of coronary artery disease. It only provides a remedy for the harmful effects of the disease. Thus, it is possible that a patient may develop symptoms again, either due to progression of coronary artery disease or due to involvement of the grafts in the disease process. Vein grafts are particularly susceptible for involvement in the disease process and about 50% of the vein grafts may be blocked by 10 years.
CABG is not the permanent cure of your coronary artery disease. It is a palliative procedure and your coronary arteries and grafts may get involved in the disease in future as a result of progression of atherosclerotic process. This progression can not be entirely prevented, but with careful lifestyle and proper drug therapy, the rate of atherosclerotic progression can be slowed down. Thus, after surgery, it is important to follow the suggested guidelines. There are several risk factors which you can modify and thus reduce the risk of recurrence of the problem.
Smoking: Quit smoking. It not only damages your lungs and causes cancer, it also accelerates the process of atherosclerosis and coronary artery disease. Smoking increases the risk of graft blockade, subsequent myocardial infarction and death.
Sedentary life style and lack of exercise: Change your life style. Physical exercises play a great role in your life. Perform regular exercises. For elderly people, brisk walking is the ideal exercise. You can perform light ‘Yoga’ under supervision. Exercise reduces ‘fat levels, in the blood and also increases circulation to heart muscles and other parts of body.
Diet : Diet rich in fats and carbohydrates may contribute to obesity, high fat levels in blood and thus to development of coronary artery disease. Consume low calorie, fat free diet which is rich in minerals, vitamins, proteins and antioxidants. Antioxidants are substances which reduce progression of atherosclerosis. Fresh fruits, green vegetables and sprouted seeds are important sources of antioxidants. You are advised to use a cooking medium that contains Rice bran oil (Sundrop Heart). You mau avoid salt if you have high blood pressure and sweets if you have diabetes.
High fat levels in blood: Increased level of cholesterol predisposes to development of atherosclerosis. A balanced diet and regular physical exercise are required to keep cholesterol level under control. However, sometimes drugs are also required to keep the cholesterol level in check.
Diabetes mellitus: Diabetics is an important predisposing factor in development of coronary artery disease. Thus, proper management of diabetes is essential. Regular physical exercise and dietary regulation help in great way to control the diabetes. Follow your doctor’s advice for diabetes control and maintain regular check-up.
Hypertension : Proper control of hypertension is essential to retard the progression of coronary artery disease. Decreased intake of salt, weight reduction and avoidance of stressful life also helps in control of high blood pressure. Regular and closely monitored drug therapy is essential for the management of hypertension.
Stress: Stress is an important risk factor. Change your life style. Stress reducing exercises and meditation help in reducing the stress.
Thus to sum up:
You have been unfortunate to have this disease, but this is not an end of life. With your experience and knowledge, you can save your friends and relatives from the clutches of this disease. Tell them about your sufferings and also tell them the ways of prevention Encourage them to adopt an healthy, stress-free life style. Campaign against smoking and introduce the people to the hazards of smoking. Make the people understand that the prevention is always better than the cure, and also that there is no real cure.
You have been unfortunate to have this disease, but this is not an end of life. With your experience and knowledge, you can save your friends and relatives from the clutches of this disease. Tell them about your sufferings and also tell them the ways of prevention Encourage them to adopt an healthy, stress-free life style. Campaign against smoking and introduce the people to the hazards of smoking. Make the people understand that the prevention is always better than the cure, and also that there is no real cure.
CABG is not the permanent cure of your coronary artery disease. It is a palliative procedure and your coronary arteries and grafts may get involved in the disease in future as a result of progression of atherosclerotic process. This progression can not be entirely prevented, but with careful lifestyle and proper drug therapy, the rate of atherosclerotic progression can be slowed down. Thus, after surgery, it is important to follow the suggested guidelines. There are several risk factors which you can modify and thus reduce the risk of recurrence of the problem.
Smoking: Quit smoking. It not only damages your lungs and causes cancer, it also accelerates the process of atherosclerosis and coronary artery disease. Smoking increases the risk of graft blockade, subsequent myocardial infarction and death.
Sedentary life style and lack of exercise: Change your life style. Physical exercises play a great role in your life. Perform regular exercises. For elderly people, brisk walking is the ideal exercise. You can perform light ‘Yoga’ under supervision. Exercise reduces ‘fat levels, in the blood and also increases circulation to heart muscles and other parts of body.
Diet : Diet rich in fats and carbohydrates may contribute to obesity, high fat levels in blood and thus to development of coronary artery disease. Consume low calorie, fat free diet which is rich in minerals, vitamins, proteins and antioxidants. Antioxidants are substances which reduce progression of atherosclerosis. Fresh fruits, green vegetables and sprouted seeds are important sources of antioxidants. You are advised to use a cooking medium that contains Rice bran oil (Sundrop Heart). You mau avoid salt if you have high blood pressure and sweets if you have diabetes.
High fat levels in blood: Increased level of cholesterol predisposes to development of atherosclerosis. A balanced diet and regular physical exercise are required to keep cholesterol level under control. However, sometimes drugs are also required to keep the cholesterol level in check.
Diabetes mellitus: Diabetics is an important predisposing factor in development of coronary artery disease. Thus, proper management of diabetes is essential. Regular physical exercise and dietary regulation help in great way to control the diabetes. Follow your doctor’s advice for diabetes control and maintain regular check-up.
Hypertension : Proper control of hypertension is essential to retard the progression of coronary artery disease. Decreased intake of salt, weight reduction and avoidance of stressful life also helps in control of high blood pressure. Regular and closely monitored drug therapy is essential for the management of hypertension.
Stress: Stress is an important risk factor. Change your life style. Stress reducing exercises and meditation help in reducing the stress.
Thus to sum up:
Principle :In CABG, a new route of blood flow is created by using a piece of blood vessel (graft). One end of the graft is attached to the aorta or one of its branches and the other end of the graft is attached to the diseased coronary artery beyond the blockage. Thus, the obstruction is bypassed.
Types of Graft :The graft may be an artery or a vein. Arterial grafts are considered superior as these remain patent for a longer period. Commonly used arterial grafts are :
Among the vein grafts, long saphenous vein is used most frequently. It is obtainedfrom leg and thigh of the patient. Selection of the grafts is based upon the nature of blockage, condition of coronary arteries and function of the heart.
Approaches and techniques :The traditional the and commonly used technique involves an incision down the front of the chest through the breastbone or sternum. This incision is called a “median sternotomy”. Sometimes a smaller incision is used on the left side of the chest. This technique is referred to as “Minimally invasive coronary artery bypass” or MICAB. In MICAB, it is expected that patient will have less pain and faster recovery. Most commonly, the patient is attached to the heart lung machine and the heart is stopped during CABG. In selected cases, the heart lung machine is not used and CABG is performed on a beating heart
Risks and complications:Though CABG is a safe operation, about 5% patients develop some form of complications. It is a major operation and depending upon the condition of the patient, there is a small but definite risk to the life. Other potential complications of CABG include bleeding or infection, stroke (which is primarily related to age and history of previous stroke), kidney failure (related in large measure to the kidney function before the surgery), and heart attack during or after the surgery. The risk of complications generally depends upon age, general health, smoking history, specific medical conditions, and most importantly, the heart function.
The outcome of surgery and long term success:The operation abolishes angina in almost all patients and minimizes the risk of future heart attacks. However, some patients may have residual angina even after CABG, but it is of lesser severity. CABG is also known to prolong the expected survival (life-span) in a specific subgroups of patients. One should understand clearly that CABG does not abolish or retard the process of coronary artery disease. It only provides a remedy for the harmful effects of the disease. Thus, it is possible that a patient may develop symptoms again, either due to progression of coronary artery disease or due to involvement of the grafts in the disease process. Vein grafts are particularly susceptible for involvement in the disease process and about 50% of the vein grafts may be blocked by 10 years.
Heart is a muscular pump, made up of specialized muscles. The right half of the heart receives impure (deoxygenated) blood from the body and pumps it into the lungs. The left half of the heart receives pure (oxygenated) blood and pumps it to the rest of the body. The left half of the heart is stronger and thicker.
In order to function, the heart needs nourishment. The nourishment comes to the heart via blood which is supplied to the heart through two major coronary arteries : left and right coronary arteries. The left coronary artery again divides into two major branches (left anterior descending and left circumflex arteries), from which several smaller branches arise and supply the heart. Thus, there are three major arteries : left anterior descending artery, left circumflex artery and right coronary artery.
Patient ID Card
Patient ID Card
Oral anticoagulants (Acitrom) is prescribed to prevent blood clot formation on and around the mechanical valve. This drug must be taken carefully and under supervision. If the level of drug is not enough. Blood clot may form on the valve and can clog the valve or can produce a stroke. Excess level of this drug can cause bleeding, both externally and internally.
Your doctor will determine the level of anticoagulant that is right for you. To maintain proper levels of anticoagulation, take your medication as prescribed and follow up with blood tests as scheduled. The dosage will be closely monitored by blood tests. The blood tests include a PT or INR.
Some important points of anticoagulant therapy are:
In cases of young female patients, if pregnancy is anticipated in future, it should be discussed with the cardiac surgeon, even before surgery. If pregnancy is anticipated, valve repair, bioprosthesis, homografts or autografts are preferred options because use of oral anticoagulants during pregnancy may cause neurological or skeletal/facial abnormalities in the fetus. Also it may increase the chances of fetal loss and bleeding at the time of child birth.
Inform your doctor urgently, if you develop any of the following:
Anticoagulation related bleeding
Patient ID Card
Patient ID Card
Oral anticoagulants (Acitrom) is prescribed to prevent blood clot formation on and around the mechanical valve. This drug must be taken carefully and under supervision. If the level of drug is not enough. Blood clot may form on the valve and can clog the valve or can produce a stroke. Excess level of this drug can cause bleeding, both externally and internally.
Your doctor will determine the level of anticoagulant that is right for you. To maintain proper levels of anticoagulation, take your medication as prescribed and follow up with blood tests as scheduled. The dosage will be closely monitored by blood tests. The blood tests include a PT or INR.
Some important points of anticoagulant therapy are:
In cases of young female patients, if pregnancy is anticipated in future, it should be discussed with the cardiac surgeon, even before surgery. If pregnancy is anticipated, valve repair, bioprosthesis, homografts or autografts are preferred options because use of oral anticoagulants during pregnancy may cause neurological or skeletal/facial abnormalities in the fetus. Also it may increase the chances of fetal loss and bleeding at the time of child birth.
Inform your doctor urgently, if you develop any of the following:
Anticoagulation related bleeding
Make regular visits to your doctor. It is essential for proper regulation of your medicines.
Proper dental hygiene is very important. Infection from teeth may involve your valve.
Treat all minor infections vigorously. Consult the local doctor for skin infections, respiratory tract, urinary tract or similar infections.
Avoid hazardous life-style. Your wounds will bleed excessively. In case of minor cuts or abrasion, prolong pressure is required to stop the bleeding.
Take medicines carefully. ‘Do not practice self medication’ Do not take drugs, especially pain killers without the advice of a doctor. In case of an ailment, inform the doctor that you are taking oral anticoagulants.
For all minor surgical procedures, you need hospitalization and switching over from oral anticoagulants to heparin. All such minor procedures should be performed under antibiotic cover.
All patients who have rheumatic heart disease, require Penicillin therapy till the age of 45 years. Always receive penicillin injection with disposable syringe and needle. In case of allergy to penicillins, inform your doctor.
Carry an identify card with you which, in case of emergency, may inform the hospital personnel that you have undergone a valve replacement and that you are receiving oral anticoagulants.
Stop smoking. Alcohol may affect the level of anticoagulation, better avoid it.
Avoid diet which is rich in Vitamin K. (spinach (palak), cabbage(Patta Gobhi), lettuce, broccoli(Green-Gobhi), cauliflower(Phool-Gobhi), tomatoes(Tamatar), carrots(Gajar), butter(Makhan), olive(Jaitun ) or corn oil and eggs(Anda)).
Make regular visits to your doctor. It is essential for proper regulation of your medicines.
Proper dental hygiene is very important. Infection from teeth may involve your valve.
Treat all minor infections vigorously. Consult the local doctor for skin infections, respiratory tract, urinary tract or similar infections.
Avoid hazardous life-style. Your wounds will bleed excessively. In case of minor cuts or abrasion, prolong pressure is required to stop the bleeding.
Take medicines carefully. ‘Do not practice self medication’ Do not take drugs, especially pain killers without the advice of a doctor. In case of an ailment, inform the doctor that you are taking oral anticoagulants.
For all minor surgical procedures, you need hospitalization and switching over from oral anticoagulants to heparin. All such minor procedures should be performed under antibiotic cover.
All patients who have rheumatic heart disease, require Penicillin therapy till the age of 45 years. Always receive penicillin injection with disposable syringe and needle. In case of allergy to penicillins, inform your doctor.
Carry an identify card with you which, in case of emergency, may inform the hospital personnel that you have undergone a valve replacement and that you are receiving oral anticoagulants.
Stop smoking. Alcohol may affect the level of anticoagulation, better avoid it.
Avoid diet which is rich in Vitamin K. (spinach (palak), cabbage(Patta Gobhi), lettuce, broccoli(Green-Gobhi), cauliflower(Phool-Gobhi), tomatoes(Tamatar), carrots(Gajar), butter(Makhan), olive(Jaitun ) or corn oil and eggs(Anda)).

The heart acts as a pump. It is divided in to a right and left portion. The right portion receives blood (which is impure) from the body and pumps the same to the lungs for purification (oxygenation). The impure blood enters the heart from two large veins called the superior and inferior vena cava. The blood from these veins enters the right upper chamber known as the Right Atrium. This chamber also receives impure blood from the heart veins through the coronary sinus. The right atrium pumps this blood into the Right Ventricle or the right lower chamber through the Tricuspid Valve. The tricuspid valve prevents blood from flowing from the right ventricle to the right atrium. The right ventricle pumps blood into the Pulmonary Artery. The Pulmonary Valve prevents blood from leaking back into the right ventricle. The pulmonary artery carries impure blood to the right and left lungs. The left half of the heart collects and pumps pure (oxygenated) blood from the lungs to all parts of the body. The blood from the lungs enters the heart from four veins called the Pulmonary Veins. These veins bring the blood into the left upper chamber called the Left Atrium. The left atrium pumps blood through the Mitral Valve into the left ventricle or left lower chamber.
The mitral valve prevents blood from leaking back from the left ventricle to the left atrium. The left ventricle pumps the blood into the Aorta, which circulates to all parts of the body. The Aortic Valve prevents blood from leaking back into the left ventricle. The four valves in the heart are the Mitral and Aortic valves on the left side and Tricuspid and Pulmonary valves on the right side.
The heart acts as a pump. It is divided in to a right and left portion. The right portion receives blood (which is impure) from the body and pumps the same to the lungs for purification (oxygenation). The impure blood enters the heart from two large veins called the superior and inferior vena cava. The blood from these veins enters the right upper chamber known as the Right Atrium. This chamber also receives impure blood from the heart veins through the coronary sinus. The right atrium pumps this blood into the Right Ventricle or the right lower chamber through the Tricuspid Valve. The tricuspid valve prevents blood from flowing from the right ventricle to the right atrium. The right ventricle pumps blood into the Pulmonary Artery. The Pulmonary Valve prevents blood from leaking back into the right ventricle. The pulmonary artery carries impure blood to the right and left lungs. The left half of the heart collects and pumps pure (oxygenated) blood from the lungs to all parts of the body. The blood from the lungs enters the heart from four veins called the Pulmonary Veins. These veins bring the blood into the left upper chamber called the Left Atrium. The left atrium pumps blood through the Mitral Valve into the left ventricle or left lower chamber.
The mitral valve prevents blood from leaking back from the left ventricle to the left atrium. The left ventricle pumps the blood into the Aorta, which circulates to all parts of the body. The Aortic Valve prevents blood from leaking back into the left ventricle. The four valves in the heart are the Mitral and Aortic valves on the left side and Tricuspid and Pulmonary valves on the right side.

Hostel Rules and regulations are framed and should be followed diligently. A copy is available with the Hostel Office. It is expected that all hostellers would conduct themselves in a disciplined manner befitting the honour, tradition, and respectability of the institution and the profession. No form of ragging is permitted in the hostels. Hostellers are required to clear all dues in time. Rooms are to be vacated according to rules and within ten days after completion of tenure or resignation or termination whichever is earlier, according to hostel rules so that the next batch may be accommodated.
In case of any problem or complaints regarding the hostels, the concerned warden or the hostel office or the Superintendent of Hostels should be contacted.
All hostellers are required to look after their rooms and hostel property properly. Water and electricity should be consumed as needed and not wasted. Use of electrical gadgets and machinery without prior permission is strictly prohibited. General cleanliness of the Hostels and toilets is done by the institution.
Rooms are allotted according to the waiting list prepared by the Hostel Section. This is on date of joining / date of completion of application basis. All entrants are therefore advised to apply for hostels as soon as they join in case they are interested in such accommodation. Proof of marriage is required for considering allotment to Married Hostels. There is a waiting list for some of the Undergraduate Hostels, Postgraduate Hostels and the Married accommodation. Students are given alternate transit accommodation in two seater & three seater rooms until further accommodation is available. The wait list is updated every month for sharing accommodation, single accommodation & married accommodation. Trainees and other similar category of applicants are accommodated depending on the availability of seats.
The residential areas of All India Institute of Medical Sciences are spread over five campuses within a radius of around 3 kilometers, of which hostel accommodation is available in two.
| S.No. | Campus | Location and Accommodation |
|---|---|---|
| 1. | Ansari Nagar (East) | The main campus that houses the institution and hospitals, residential quarters and most of the hostels. |
| 2. | Ansari Nagar (West) | A smaller residential area just across and to the West of the hospital on Aurobindo Marg, adjacent to the Safdarjung Hospital. |
| 3. | Masjid Moth | A sister campus adjacent to the Ansari Nagar (East) less than a kilometer away has hostels and residential quarters. |
| 4. | Ayurvigyan Nagar | This campus is on the Khel Gaon Marg adjacent to the HUDCO Complex that houses the Ansal Plaza and has residential quarters and transit accommodation. |
| 5. | Asiad Village | On the Khel Gaon Marg, this has few houses for the Faculty only. There are no hostels in this campus. |
Transport department provides transportation facility to B.Sc & M.Sc Nursing female students to and from Masjid Moth & AIIMS campus. A subsidized fee is charged for this purpose. The transport Department should be contacted for details.
| FROM MASJID MOTH | FROM A.I.I.M.S. |
|---|---|
| 7.10 AM (Trauma Centre) from November 2023 Onwards | 12.30 PM (Trauma Centre) |
| 7.20 AM | 12.30 PM |
| 1.45 PM | 4.50 PM / 5.00 PM |
| On Saturday | |
| 7.20 AM | 1.00 PM |
| 8.30 AM | |
| A.I.I.M.S. TO BALLABHGARH | 7.30 am (Monday) 12.30 pm (Friday) [Return after one week] |
| BALLABHGARH TO A.I.I.M.S. | |
| A.I.I.M.S. TO DAYALPUR | 7.30 am (Monday to Friday) |
| DAYALPUR TO A.I.I.M.S. | 12.30 pm (Monday to Friday) |
| A.I.I.M.S. TO AMBEDKAR NAGAR | 9.30 am (Monday to Friday) |
| AMBEDKAR NAGAR TO A.I.I.M.S. | 12.30 pm (Monday to Friday) |
There are a total of twenty different halls of residence and dwellings that are regarded as hostel accommodation. Of these, thirteen are in the Ansari Nagar (East) campus and accommodates all undergraduates (except lady nursing students) and single postgraduates and resident doctors. These are the older hostels. These nine hostels for gentlemen have derived their names from the Ayurveda, and are a tribute to those who have laid the foundations for medicine and surgery, relevant even today. The four hostels for ladies are named after Goddesses, Laxmi, Parvati, Saraswati and Akshara. [However the hostels are invariably known as numbers]. There is no married accommodation in the Ansari Nagar (East) campus.
| S.No. | Hostel | Location | Category | Gender | Type of Room |
|---|---|---|---|---|---|
| 1. | Hostel No. 1 (Charak Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Single rooms |
| 2. | Hostel No. 2 (Jivak Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Single rooms |
| 3. | Hostel No. 3 (Sushruta Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Single rooms |
| 4. | Hostel No. 4 (Madhava Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Single rooms |
| 5. | Hostel No. 5 (Nagarjuna Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Single rooms |
| 6. | Hostel No. 6 (Vagbhatta Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Single rooms |
| 7. | Hostel No. 7 (Ashwini Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Double seater |
| 8. | Hostel No. 8 (Bharadwaj Hostel) | Gents Hostel Ansari Nagar (East) | Postgraduates | Gents | Single rooms |
| 9. | Hostel No. 9 (Parvati Hostel) | Ladies Hostel Ansari Nagar (East) | Undergraduates Postgraduates | Ladies | Single / Double seater |
| 10. | Hostel No. 10 (Saraswati Hostel) | Ladies Hostel Ansari Nagar (East) | Undergraduates | Ladies | Single rooms |
| 11. | Hostel No. 11 (Akshara Hostel) C2 Flats | Ladies Hostel Ansari Nagar (East) | Undergraduates | Ladies | Double / Triple seater |
| 12. | Hostel No. 12 (Dhanwantri Hostel) RPC I | Gents Hostel Ansari Nagar (East) | Postgraduates | Gents | Single rooms |
| 13. | Hostel No. 13 (Laxmi Hostel) RPC II | Ladies Hostel Ansari Nagar (East) | Undergraduates | Ladies | Single / Six seater |
| 14. | Hostel No. 14 (Atreya Hostel) | Masjid Moth Campus | Postgraduates | Ladies Single, Gents Single & Married | Single rooms & One Bed room set for married |
| 15. | Hostel No. 15 (Medha Hostel) | Masjid Moth Campus | Undergraduates Postgraduates | Ladies | Single / Double / Triple / Four seater |
| 16. | Hostel No. 16 (Agnivesa Hostel) | Masjid Moth Campus | Postgraduates | Gents Single & Married | Single rooms & One room set / One Bed room set for married |
| 17. | Hostel No. 17 (Ambuja Hostel) | Masjid Moth Campus | Postgraduates | Married | One Bed room set for married |
| 18. | Hostel No. 18 (Kashyap Hostel) | Masjid Moth Campus | Undergraduates Postgraduates | Gents | Single / Double / Triple seater |
| 19. | Hostel No. 19 (Patanjali Hostel) | Masjid Moth Campus | Postgraduates | Ladies | Single rooms / Double seater |
| 20. | JPNATC Hostel | Raj Nagar | Postgraduates | Gents Single & Married | Single rooms & One Bed room set for married |
These hostels have a total capacity of about 2700 seats approx. The majority of the accommodation is for a single student / resident / family. Attached toilets are only available in married accommodation and in JPNATC Hostel, Hostel No. 18 (Kashyap Hostel) and Hostel No. 19 (Patanjali Hostel). Otherwise toilets and bathrooms are shared.
FURNISHINGS
Most single rooms are modestly furnished with a cot, almirah, table, chair and bookshelf (in some hostels). The married accommodation is also furnished accordingly. All hostellers are advised to check the inventory while occupying and vacating the rooms.
The Director, AIIMS is the highest authority that oversees the functioning of the hostels. To supervise the hostel section, members of the Faculty are appointed by the Director to work in the capacities of the Superintendent and Deputy Superintendents. The Superintendent of Hostels is the overall in-charge of the hostels. The Hostel Section looks after the day-to-day functioning with the Senior Warden overseeing all the hostels. The Senior Warden is supported by Wardens, Deputy Wardens, Assistant Wardens and Junior Wardens who look after individual hostels along with other staff. You should check and know the respective Warden in charge of your hostel.
There is a Hostel Advisory Committee that oversees various aspects of the functioning of the hostels and includes not only members of the faculty (Superintendent and Deputy Superintendents), the Warden, but also representatives of different students’ bodies such as AIIMS Students Association, Student Nurses Association, Resident Doctors Association and the Society of Young Scientists. Other members from the administration, finance, engineering services and security also contribute to run and maintain various services in the hostels.
The Hostel Section is on the First Floor of Hostel No. VII (first hostel on the right as you enter Gents Hostel). In addition most of the hostels (except Hostels 1-8) have small offices in their premises.
There are several hostel offices. The Hostel Section deals with most matters related to hostellers of all hostels. In addition the smaller offices deal with allotments, vacation and immediate problems that may arise.
| Office | Location | In-charge of Hostels | Duties |
|---|---|---|---|
| Hostel Section and Masjid Moth Hostel Office | Hostel No. 7 (Ashwini Hostel), First Floor, Gents Hostel and Hostel No. 14 (Atreya Hostel), Room No. 002, Ground Floor. | Mr. Mohan Kumar Sharma | Supervision of Hostel Section & Masjid Moth Hostels under the direct control of Superintendent of Hostels. |
| Ladies Hostel Office | Hostel No. 10 (Saraswati Hostel), Room No. 7, Ground Floor. | Ms. Seema Pruthi | Supervision of Allotment Division-II Hostel No. 9 (Parvati Hostel) Hostel No. 10 (Saraswati Hostel) Hostel No. 11 (Akshara Hostel) C2 Flats Hostel No. 13 (Laxmi Hostel) RPC-II |
| Hostel Section | Hostel No. 7 (Ashwini Hostel), First Floor, Gents Hostel. | Ms. Suchita Kumari | Supervision of Allotment Division-III & H.No.1 to 8. Organize Hostel Committee Meeting, Prepare the minutes of the meeting & Compile the Annual Report etc. |
| Masjid Moth Hostel Office | Hostel No. 18 (kashyap Hostel), Room No. 009, Ground Floor. | Mr. Sukhpal Malik | Supervision of Allotment Division-I Hostel No. 18 (Kashyap Hostel) |
| Masjid Moth Hostel Office | Hostel No. 15 (Medha Hostel), Ground Floor. | Ms. Tripta Sharma | Allotment of Nurses Hostel (U.G. & P.G.) with the help of Ms. Sonia D.E.O. Hostel No. 15 (Medha Hostel) |
| Masjid Moth Hostel Office | Hostel No. 19 (Patanjali Hostel), Room No. 005, Ground Floor. | Ms. Rani Varghese | Hostel No. 19 (Patanjali Hostel) |
| Hostel Section | Hostel No. 7 (Ashwini Hostel), First Floor, Gents Hostel. | Mr. Ankit Dogra | To reply of official letters and documents related to Hostel Section. Currently working as a reliever in Hostel No. 7 (Ashwini Hostel), Hostel No. 8 (Bharadwaj Hostel), Hostel No. 12 (Dhanwantri Hostel) RPC-I & JPNATC Hostel. |
| RPC I Hostel Office and JPNATC Hostel Office | Hostel No. 12 (Dhanwantri Hostel) RPC-I, Ground Floor and JPNATC Hostel, Room No. 05, Ground Floor. | Mr. Babu Lal Meena | Hostel No. 12 (Dhanwantri Hostel) RPC-I JPNATC Hostel |
| Masjid Moth Hostel Office | Hostel No. 16 (Agnivesa Hostel), Room No. 14, Ground Floor and Hostel No. 17 (Ambuja Hostel), Room No. 103, Ground Floor. | Mr. Dinesh Desai | Hostel No. 16 (Agnivesa Hostel) Hostel No. 17 (Ambuja Hostel) |
| Hostel Section | Hostel No. 7 (Ashwini Hostel), First Floor, Gents Hostel. | Ms. Nirmala Barthwal | Hostel No. 4 (Madhava Hostel) Management of duties of Group ‘D’ staff. Maintenance of C.L.,E.L. Records. |
| Hostel Section | Hostel No. 7 (Ashwini Hostel), First Floor, Gents Hostel. | Mr. Rajesh Rawat | Hostel No. 7 (Ashwini Hostel) Hostel No. 8 (Bharadwaj Hostel) |
| Hostel Section | Hostel No. 7 (Ashwini Hostel), First Floor, Gents Hostel. | Ms. Sunil Devi | Hostel No. 1 (Charak Hostel) Hostel No. 2 (Jivak Hostel)
Hostel No. 3 (Sushruta Hostel) Hostel No. 6 (Vagbhatta Hostel)
|
| Masjid Moth Hostel Office | Hostel No. 14 (Atreya Hostel), Room No. 002, Ground Floor. | Ms. Asha | Hostel No. 14 (Atreya Hostel) |
| S.No. | Designation | Name |
|---|---|---|
| 1. | Superintendent of Hostels (Chairman) | Prof. Sanjay Kumar Rai |
| 2. | Deputy Superintendent of Hostel | Prof. Neerja Bhatla |
| 3. | Deputy Superintendent of Hostel | Prof. Tanuj Dada |
| 4. | Deputy Superintendent of Hostel | Prof. Raj Kumar Yadav |
| 5. | Deputy Superintendent of Hostel | Prof. Rakesh Kumar |
| 6. | Deputy Superintendent of Hostel | Prof. K.H. Reeta |
| 7. | Deputy Superintendent of Hostel | Prof. Vijay Sharma |
| 8. | Deputy Superintendent of Hostel | Dr. Harshal Ramesh Salve Additional Professor |
| 9. | Deputy Superintendent of Hostel | Ms. Cecilia M.S. Associate Professor |
| 10. | Deputy Superintendent of Hostel | Ms. Bhupinder Kaur Deputy Nursing Superintendent |
| 11. | Administrative Officer (Hostels) | Mr. Uttam Chand |
| 12. | Senior Financial Advisor or his Nominee | - |
| 13. | Superintendent Engineer or his Nominee | - |
| 14. | Senior Warden | Mr. Mohan Kumar Sharma |
| 15. | R.D.A. President or his Nominee | Special invitee |
| 16. | S.Y.S. Chairman or his Nominee | Special invitee |
| 17. | A.S.A. President or his Nominee | Special invitee |
| 18. | S.N.A. President or her Nominee | Special invitee |
| 19. | Co-opted Members | As desired by Chairman |
All major decisions of mutual interest to the administration and the students regarding the functioning of the hostels are taken by the Hostel Advisory Committee and wherever necessary, duly approved by the Director and / or other competent authorities / bodies of the institution.
| Designation | Name | Department |
|---|---|---|
| Superintendent of Hostels | Prof. Sanjay Kumar Rai | Professor, Department of Centre for Community Medicine |
| Deputy Superintendent of Hostel (Ladies Hostels) | Prof. Neerja Bhatla | Professor & H.O.D. Obst. & Gynae. |
| Deputy Superintendent of Hostel | Prof. Tanuj Dada | Professor, Department of Ophthalmology |
| Deputy Superintendent of Hostel | Prof. Raj Kumar Yadav | Professor, Department of Physiology |
| Deputy Superintendent of Hostel | Prof. Rakesh Kumar | Professor, Department of E.N.T. |
| Deputy Superintendent of Hostel (Ladies Hostels) | Prof. K.H. Reeta | Professor, Department of Pharmacology |
| Deputy Superintendent of Hostel (Trauma Centre) | Prof. Vijay Sharma | Professor, Department of Orthopedics |
| Deputy Superintendent of Hostel (CRHSP, Ballabgarh) | Dr. Harshal Ramesh Salve | Additional Professor, Department of C.C.M. |
| Deputy Superintendent of Hostel (Nursing Students) | Ms. Cecilia M.S. | Associate Professor, College of Nursing |
| Deputy Superintendent of Hostel (Nursing Staff) | Ms. Bhupinder Kaur | D.N.S., Main Hospital |
| Designation | Name | Duties |
|---|---|---|
| Senior Warden | Mr. Mohan Kumar Sharma | Supervision of Hostel Section & Masjid Moth Hostels under the direct control of Superintendent of Hostels. |
| Warden | Ms. Seema Pruthi | Supervision of Allotment Division-II Hostel No. 9 (Parvati Hostel) Hostel No. 10 (Saraswati Hostel) Hostel No. 11 (Akshara Hostel) C2 Flats Hostel No. 13 (Laxmi Hostel) RPC-II |
| Deputy Warden | Ms. Suchita Kumari | Supervision of Allotment Division-III & H.No.1 to 8. Organize Hostel Committee Meeting, Prepare the minutes of the meeting & Compile the Annual Report etc. |
| Deputy Warden | Mr. Sukhpal Malik | Supervision of Allotment Division-I Hostel No. 18 (Kashyap Hostel) |
| Assistant Warden | Ms. Tripta Sharma | Allotment of Nurses Hostel (U.G. & P.G.) with the help of Ms. Sonia D.E.O. Hostel No. 15 (Medha Hostel) |
| Assistant Warden | Ms. Rani Varghese | Hostel No. 19 (Patanjali Hostel) |
| Assistant Warden | Mr. Ankit Dogra | To reply of official letters and documents related to Hostel Section. Currently working as a reliever in Hostel No. 7 (Ashwini Hostel), Hostel No. 8 (Bharadwaj Hostel), Hostel No. 12 (Dhanwantri Hostel) RPC-I & JPNATC Hostel. |
| Junior Warden | Mr. Babu Lal Meena | Hostel No. 12 (Dhanwantri Hostel) RPC-I JPNATC Hostel |
| Junior Warden | Mr. Dinesh Desai | Hostel No. 16 (Agnivesa Hostel) Hostel No. 17 (Ambuja Hostel) |
| Junior Warden | Ms. Nirmala Barthwal | Hostel No. 4 (Madhava Hostel) Hostel No. 5 (Nagarjuna Hostel) Management of duties of Group ‘D’ staff. Maintenance of C.L.,E.L. Records. |
| Junior Warden | Mr. Rajesh Rawat | Hostel No. 7 (Ashwini Hostel) Hostel No. 8 (Bharadwaj Hostel) |
| Junior Warden | Ms. Sunil Devi | Hostel No. 1 (Charak Hostel) Hostel No. 2 (Jivak Hostel) Hostel No. 3 (Sushruta Hostel) Hostel No. 6 (Vagbhatta Hostel) |
| Store Keeper | Mr. Pankaj Kumar | Hostel Store |
| Store Keeper (Drugs) | Mr. Ravi Ukhardya Dhanap | Hostel Store |
| Junior Administrative Officer | Ms. Harisha Suri | Hostel Section |
| Senior Administrative Assistant | Ms. Sameena Parveen | Hostel Cashier |
| Senior Administrative Assistant | Mr. Sunil Kumar Sarwan | RTI & All Administrative Matters |
| Junior Administrative Assistant | Mr. Vijendra | Hostel Guest room booking & Hostel fee |
| Junior Administrative Assistant | Ms. Asha | Hostel No. 14 (Atreya Hostel) |
| Junior Administrative Assistant | Mr. Dharam Dutt | Hostel Shops & Establishments |
| Name | Location | Internal | |
|---|---|---|---|
Prof. Sanjay Kumar Rai Superintendent of Hostels | Department of Centre for Community Medicine | 4416 | drsanjay.aiims@gmail.com |
Prof. Neerja Bhatla Deputy Superintendent of Hostel | Department of Obst. & Gynae. | 4991 | neerja.bhatla07@gmail.com |
Prof. Tanuj Dada DeputySuperintendent of Hostel | Department of Ophthalmology | 3001 | tanujdada@gmail.com |
Prof. Raj Kumar Yadav Deputy Superintendent of Hostel | Department of Physiology | 6461 | raj3kr@gmail.com |
Prof. Rakesh Kumar Deputy Superintendent of Hostel | Department of E.N.T. | 3443 | winirk@hotmail.com |
Prof. K.H. Reeta Deputy Superintendent of Hostel | Department of Pharmacology | 3247 | reetakh@gmail.com |
Prof. Vijay Sharma Deputy Superintendent of Hostel | Department of Orthopaedics, JPNATC | 26731160 | drvijaysharmatrauma@gmail.com |
Dr. Harshal Ramesh Salve Additional Professor Deputy Superintendent of Hostel | Department of C.C.M. | 3366 | harshalsalve@ymail.com |
Ms. Cecilia M.S. Associate Professor Deputy Superintendent of Hostel | College of Nursing | 4457 | cecilia.aiims@gmail.com |
Ms. Bhupinder Kaur Deputy Superintendent of Hostel | Main Hospital C.N.O. Office | 4705 | bhupinderkaur65@gmail.com |
Mr. Mohan Kumar Sharma Senior Warden | Hostel Section | 4633 6661 3487 4954(M.M.H.) | mohansharma276@gmail.com |
Mondays to Fridays: 9:30 AM to 5:15 PM with a short lunch break from 1:00 PM to 1:30 PM.
Saturdays: 9:30 AM to 1:15 PM.
Note: Payments are accepted by the hostel cashier between 9:30 AM to 1:00 PM & 1:30PM to 5:00 PM on week days and between 9:30 AM to 1:00 PM on Saturdays.
| S.NO. | COURSE | POT FUND (Per Month) | HOSTEL RENT (Per Month) | ELECTRICITY (Per Month) | GYMKHANA (Per Month) | TOTAL HOSTEL FEES/ CHARGES |
|---|---|---|---|---|---|---|
| 1. | MD/MS/MDS (3 Years) | NIL | NIL | Rs. 7/- | Rs. 3/- | Rs. 360/- |
| 2. | M.Ch. (6 Years) | NIL | NIL | Rs. 7/- | Rs. 3/- | Rs. 720/- |
3.
| MD/MS/MDS (Sponsored) (3 Years) | Rs. 20/- | Unmarried Rs. 450/- Married Rs. 650/- | Rs. 7/- | Rs. 3/- | Hostel Fees Rs. 1080/- Hostel Rent Unmarried (+)Rs. 16200/- |
| Total Rs. 17280/- | ||||||
Hostel Fees Rs. 1080/- Hostel Rent Married (+) Rs. 23400/- | ||||||
| Total Rs. 24480/- | ||||||
| 4. | DM/M.Ch. (3 Years) | NIL | NIL | Rs. 7/- | Rs. 3/- | Rs. 360/- |
| 5. | DM/M.Ch. (Sponsored) (3 Years) | Rs. 20/- | Unmarried Rs. 450/- Married Rs. 650/- | Rs. 7/- | Rs. 3/- | Hostel Fees Rs. 1080/- Hostel Rent Unmarried (+)Rs. 16200/- |
| Total Rs. 17280/- | ||||||
Hostel Fees Rs. 1080/- Hostel Rent Married (+) Rs. 23400/- | ||||||
| Total Rs. 24480/- | ||||||
| 6. | Ph.D. (5 Years) | Rs. 20/- | Rs. 30/- | Rs. 7/- | Rs. 3/- | Rs. 3600/- |
| 7. | MBBS 51/2 Years (Including Internship) | Rs. 20/- | Rs. 15/- | Rs. 3/- | Rs. 220/- (51/2 Years) | Rs. 2728/- |
| 8. | M.Sc. Nursing (2 Years) | Rs. 20/- | NIL | Rs. 10/- | Rs. 3/- | Rs. 792/- |
| 9. | M.Sc. Other Courses (2 Years) | Rs. 20/- | NIL | Rs. 10/- | Rs. 3/- | Rs. 792/- |
| 10. | B.Sc. Nursing (4 Years) | Rs. 20/- | Rs. 10/- | NIL | NIL | Rs. 1440/- |
| 11. | B.Sc. (Opthal) (4 Years) (Including Internship) | Rs. 20/- | NIL | NIL | NIL | Rs. 960/- |
| 12. | B.Sc. (Dental Hygiene Course) (31/2 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 840/- |
| 13. | B.Sc. (Dental Operation Room Assistant) (4 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 960/- |
| 14. | B.Sc. (Operation Theatre Technology) (31/2 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 840/- |
| 15. | B.Sc. (MRIT) (31/2 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 840/- |
HOSTEL SECURITY Rs. 1000/- (REFUNDABLE) DEPOSITED AT THE TIME OF SUBMISSION OF APPLICATION FOR THE HOSTEL ACCOMMODATION.
Payments may be required at the time of placing an order or at intervals (monthly) or in advance (in Student run messes) depending on the type of boarding. Current charges for four meals (breakfast, lunch, evening tea, and dinner) in the format of fixed menu is around Rs. 3500.00 per month in most messes, but in the Student run messes this may vary between Rs. 3500.00 to Rs. 4500.00 per month. Boarders are however free to order for other dishes and pay extra. Each mess has its different methods of predetermined service and charge accordingly. The rate-list is available with each mess / café and should be checked.
Actuals to be paid in the mess / café etc. All boarders are required to make payments in time.
Penal Rent is levied in case of unauthorized occupation of hostels (e.g. beyond the period of allotment such as, according to current rules, after ten days of completion of tenure).
All Students / Residents are requested to submit their penal rent recovery challan or other challan on the following working days:
Monday to Friday from 11.00 AM to 2.00 PM
Saturday 10.00 AM to 11.30 AM
Challan will not be received by the cashier cell on the last working day of the every month.
| Hostel Category | Hostels / Accommodation | Penal Rent (Per Month) | Penal Rent (Per day) | Normal Rent (Per Month) | Normal Rent (Per day) |
|---|---|---|---|---|---|
Undergraduates Gents & Ladies Hostels (Single rooms) | Hostel No. 1 Charak Hostel (Gents), Hostel No. 2 Jivak Hostel (Gents), Hostel No. 3 Sushruta Hostel (Gents), Hostel No. 4 Madhava Hostel (Gents), Hostel No. 5 Nagarjuna Hostel (Gents), Hostel No. 6 Vagbhatta Hostel (Gents), Hostel No. 10 Saraswati Hostel (Ladies), Hostel No. 13 Laxmi Hostel (RPC-II ) (Ladies), Hostel No. 15 Medha Hostel (Ladies) | Rs. 23,500.00 P.M. | Rs. 783.00 Per day | Rs. 470.00 P.M. | Rs. 16.00 Per day |
Undergraduates Gents & Ladies (Double seater) | Hostel No. 7 Ashwini Hostel (Gents), Hostel No. 9 Parvati Hostel (Ladies), Hostel No. 15 Medha Hostel (Ladies) | Rs. 23,500.00 P.M. | Rs. 783.00 Per day | Rs. 470.00 P.M. | Rs. 16.00 Per day |
Undergraduates Ladies (Double seater) | Hostel No. 11 Akshara Hostel C2 Flats (Ladies)
| Rs. 33,000.00 P.M | Rs. 1100.00 Per day | Rs. 660.00 P.M. | Rs. 22.00 Per day |
Undergraduates Gents & Ladies (Triple seater) | Hostel No. 11 Akshara Hostel C2 Flats (Ladies), Hostel No. 15 Medha Hostel (Ladies), Hostel No. 18 Kashyap Hostel (Gents) | Rs. 23,500.00 P.M. | Rs. 783.00 Per day | Rs. 470.00 P.M. | Rs. 16.00 Per day |
Undergraduates Ladies (Four seater) | Hostel No. 15 Medha Hostel (Ladies) | Rs. 33,000.00 P.M | Rs. 1100.00 Per day | Rs. 660.00 P.M. | Rs. 22.00 Per day |
Undergraduates Ladies (Six seater) | Hostel No. 13 Laxmi Hostel RPC-II (Ladies) | - | - | - | - |
Postgraduates Gents & Ladies Hostels (Single rooms) | Hostel No. 8 Bharadwaj Hostel (Gents), Hostel No. 9 Parvati Hostel (Ladies), Hostel No. 12 Dhanwantri Hostel (RPC-I) (Gents), Hostel No. 14 Atreya Hostel (Gents & Ladies), Hostel No. 16 Agnivesa Hostel (Gents), Hostel No. 18 Kashyap Hostel (Gents), Hostel No. 19 Patanjali Hostel (Ladies), JPNATC Hostel (Gents) | Rs. 23,500.00 P.M. | Rs. 783.00 Per day | Rs. 470.00 P.M. | Rs. 16.00 Per day |
| Postgraduates Gents & Ladies (Double seater) | Hostel No. 9 Parvati Hostel (Ladies), Hostel No. 15 Medha Hostel (Ladies), Hostel No. 18 Kashyap Hostel (Gents), Hostel No. 19 Patanjali Hostel (Ladies) | Rs. 33,000.00 P.M. | Rs.1100.00 Per day | Rs. 660.00 P.M. | Rs. 22.00 Per day |
Postgraduates (Married) | Hostel No. 14 Atreya Hostel, JPNATC Hostel | Rs. 33,000.00 P.M. | Rs. 1100.00 Per day | Rs. 660.00 P.M | Rs. 22.00 Per day |
Hostel No. 16 Agnivesa Hostel, Hostel No. 17 Ambuja Hostel | Rs. 45,500.00 P.M. | Rs. 1517.00 Per day | Rs. 910.00 P.M. | Rs. 31.00 Per day |
Complaints that would improve the hostels.
Never feel hesitant to make a complaint. Unsolicited and frivolous complaints should be avoided. Whenever the hosteller wishes the names shall not be disclosed.
Depending on the nature of complaint, the complaint may be addressed to the appropriate authority.
For day to day matters - Complain to the Junior Warden or the Concerned Hostel Offices.
Engineering services / repairs in the room - Enquiry offices are available in all hostels / compounds. These offices are open 24 hours. Boards displaying the names of Engineers are displayed at these offices.
Security - Every hostel has security guards round the clock. In case of complaints these may be directed to the guards or the Security Officers any time of the day or night.
Sanitation and Cleanliness - Complaints regarding sanitation and cleanliness may be directed to the Junior / Concerned Wardens who will coordinate with the appropriate authorities.
Shops & Establishments - It is mandatory for all commercial establishments to keep a complaint book. Hostellers may lodge their complaints regarding quality of service, food and other grievances. Mess complaint book is checked regularly by Senior Warden (Hostels) & shops complaint book is checked by Estate Section and appropriate action (such as imposition of fines) is taken.
Other matters - Depending on the gravity and nature of complaint, hostellers may write or meet the Senior Warden or the Deputy Superintendents or the Superintendent without any hesitation.
Suggestions for hostel web pages
Suggestions and criticisms of this web site are welcome from all hostellers. We would like to thank Drs. Shree Gopal Sharma, Nidhi Aggarwal, Anup Das and Bal Chander for the photographs that you see.
रेजीडेन्ट/विधार्थी द्वारा वचनवंध-Undertaking by the Resident/Student
Eligible for Postgraduates
MALE
Initial Allotment of Unmarried Male in Hostel No. 8 (Bharadwaj Hostel), Hostel No. 12 (Dhanwantri Hostel) RPC I, Hostel No. 14 (Atreya Hostel) & JPNATC Hostel on the basis of Date of Joining, Date of Completion of Application and Receipt no. of security slip for the hostel, respectively.
(Ratio 2:1:1:1:1)
2 Senior Resident, 1 Junior Resident, 1 Senior Resident (AIIMSONION), 1 Junior Resident (AIIMONSION), 1 PHD, Every 4th PHD is AIIMSONION PHD, According to waiting list.
Up gradation for unmarried Male in Hostel No. 18 (Kashyap Hostel), Seniority is given on the basis of Date of Allotment / Date of Application.
MARRIED
Allotment of Married Hostel’s in Hostel No. 14 (Atreya Hostel), Hostel No. 16 (Agnivesa Hostel), Hostel No. 17 (Ambuja Hostel) & JPNATC Hostel, According to waiting list.
Ratio in Married Accommodation
-
(Ratio 3:2:1)
3 Resident (2 Senior Resident & 1 Junior Resident), 2 AIIMSONION Resident (1 Senior Resident & 1 Junior Resident), 1 PHD, Every 4th PHD is AIIMSONION PHD, According to waiting list.
FEMALE
Initial Allotment of Unmarried Female in Hostel No. 9 (Parvati) & Hostel No. 14 (Atreya Hostel) on the basis of Date of Joining, Date of Completion of Application and Receipt no. of security slip for the hostel, respectively.
-
(Ratio 2:1:1:1:1)
2 Senior Resident, 1 Junior Resident, 1 Senior Resident (AIIMSONION), 1 Junior Resident (AIIMONSION), 1 PHD, Every 4th PHD is AIIMSONION PHD, According to waiting list.
Up gradation for unmarried Female in Hostel No. 19 (Patanjali Hostel), Seniority is given on the basis of Date of Allotment / Date of Application.
For Married & Unmarried Accommodation waiting list is updated once a month. 1st week of the every month new list is generated.
If a Resident is given offer / allotment & he / she refuses to take the room than he / she will be debarred from the waiting list for 6 months.
MALE
Allotment of unmarried male in Hostel No. 18 (Kashyap Hostel) on the basis of Date of Joining, Date of Completion of Application and Receipt no. of security slip for the hostel, respectively.
(Ratio)
There is no ratio for B.Sc. Paramedical Students. 36 Seats are reserved for B.Sc. Paramedical Students.
FEMALE
Allotment of Unmarried Female in Hostel No. 9 (Parvati Hostel)& Hostel No. 13 (Laxmi Hostel) RPC II on the basis of Date of Joining, Date of Completion of Application and Receipt no. of security slip for the hostel, respectively.
(Ratio)
There is no ratio for B.Sc. Paramedical Students. 17 seats are reserved for B.Sc. Paramedical students.
These seats are given according to the date of vacation of room, According to waiting list.
For Unmarried Accommodation waiting list is updated once a month. 1st Week of the every month new list is generated.
If a Student is given allotment & he / she refuses to take the room he / she will be debarred from the waiting list for 6 months.
Authority letter for Parcel-Courier/पार्सल-कोरियर्स के लिए अधिकार पत्र
Hostel no dues form(Nursing Female)/छात्रावास बेबाकी प्रपत्र (नर्सिग महिला)
Application for allotment of Hostel Accommodation/छात्रावास आवास के आबंटन हेतु आवेदन
Application for Married Accommodation/विवाहित आवास हेतु आवेदन
Application for Grant of House Rent Allowances/मकान किराया-भत्ता का प्रदान करने के लिए आवेदन
Application for purpose of Residence Proof/निवास प्रमाण के अभिप्राय हेतु आवेदन
| Service | Location | Internal | External | |
|---|---|---|---|---|
| Casualty | AIIMS | Screening | 3887 | - |
| Emergency 1 | 4084 4085 | - - | ||
| New Emergency Ward | 4405 4591 3415 | 26594405 - - | ||
| Surgery | 4255 4706 | - - | ||
| Duty Officer | AIIMS | 3308 3574 | 26593308 26593574 | |
| Security Control Room | AIIMS | 4780 3333 4444 | 26594780 - - | |
| Police | AIIMS Post | 3345 | 26593345 | |
| Control Room | - | 112 | ||
| Defence Colony | - | 26253402 | ||
| Hauz Khas | - | 26867878 | ||
| Sarojini Nagar | - | 24671281 | ||
| Fire (PC Block) | AIIMS | 3661 | 26593661 | |
| Masjid Moth Hostels | 4950 | 26594950 | ||
| Delhi Fire Service | - | 101 | ||
| J.E. (Electrical) | Gents Hostels | 6614 | 26596614 | |
| Electrical Enquiry | Gents Hostels | 3424 | 26593424 | |
| J.E. (Electrical) | Ladies Hostels | 3777 | 26593777 | |
| Electrical Enquiry | Ladies Hostels | 6324 | 26596324 | |
| J.E. (Electrical) | RPC Hostels | 3777 | 26593777 | |
| Electrical Enquiry | RPC Hostels | 6324 | 26596324 | |
| J.E. (Electrical) | Masjid Moth Hostels | 6715 | 26546715 | |
| Electrical Enquiry | Masjid Moth Hostels | 4233 | 26594233 | |
| J.E. (Electrical) | JPNATC Hostel | 1208 1285 | 26731208 26731285 | |
| Electrical Enquiry | JPNATC Hostel | 1210 | 26731210 | |
| NDMC, Kidwai Nagar | - - | 24104748 24106892 | ||
| J.E. (Civil) | Gents Hostels | 3656 | 26593656 | |
| Civil Enquiry | Gents Hostels | 4054 | 26594054 | |
| J.E. (Civil) | Ladies Hostels | 6419 | 26596419 | |
| Civil Enquiry | Ladies Hostels | 3065 | 26593065 | |
| J.E. (Civil) | RPC Hostels | 6419 | 26596419 | |
| Civil Enquiry | RPC Hostels | 3065 | 26593065 | |
| J.E. (Civil) | Masjid Moth Hostels | 4959 | 26544959 | |
| Civil Enquiry | Masjid Moth Hostels | 4959 | 26544959 | |
| J.E. (Civil) | JPNATC Hostel | 1209 | 26731209 | |
| Civil Enquiry | JPNATC Hostel | 1199 | 26731199 | |
| Name | Location | Internal | External |
|---|---|---|---|
Prof. Sanjay Kumar Rai Superintendent of Hostels | Department of Centre for Community Medicine | 4416 | 26594416 |
Prof. Neerja Bhatla Deputy Superintendent of Hostel | Department of Obst. & Gynae. | 4991 | 26594991 |
Prof. Tanuj Dada Deputy Superintendent of Hostel | Department of Ophthalmology | 3001 | 26593001 |
Prof. Raj Kumar Yadav Deputy Superintendent of Hostel | Department of Physiology | 6461 | 26546461 |
Prof. Rakesh Kumar Deputy Superintendent of Hostel | Department of E.N.T. | 3443 | 26593443 |
Prof. K.H. Reeta Deputy Superintendent of Hostel | Department of Pharmacology | 3247 | 26593247 |
Prof. Vijay Sharma Deputy Superintendent of Hostel | Department of Orthopedics JPNATC | - | 26731160 |
Dr. Harshal Ramesh Salve Additional Professor Deputy Superintendent of Hostel | Department of C.C.M. | 3366 | 26593366 |
Ms. Cecilia M.S. Associate Professor Deputy Superintendent of Hostel | College of Nursing | 4457 | 26594457 |
Ms. Bhupinder Kaur D.N.S. Deputy Superintendent of Hostel | Main Hospital C.N.O. Office | 4705 | 26594705 |
Mr. Uttam Chand Administrative Officer (Hostels) | Examination Section | 6422 | 26596422 |
Mr. Yatender Meena Store Officer (Hostels) | Store Section (CNC) | 4704 | 26594704 |
Mr. Amit Kumar Accounts Officer (Hostels) | Cash Section | 3687 | 26593687 |
Mr. Mohan Kumar Sharma Senior Warden (Hostels) | Hostel Section | 4633 6661 3487 4954(M.M.H.) | 26594633 26546661 26593487 26594954 |
| Name | Location | Internal | External |
|---|---|---|---|
| Hostel Section | Gents Hostels Hostel No. 7 (Ashwini Hostel) Ansari Nagar (East) | 4633 6661 3487 | 26594633 26546661 26593487 |
| Ladies Hostels | Ladies Hostels Hostel No. 10 (Saraswati Hostel) Ansari Nagar (East) | 3096 4578 4306 | 26593096 26594578 26594306 |
| Hostel No. 12 (Dhanwantri Hostel) RPC I | RPC Gents Hostel Ansari Nagar (East) | 3320 | 26593320
|
| Hostel No. 14 (Atreya Hostel) | Masjid Moth Campus | 4951 4952 4954 | 26594951 26594952 26594954 |
| Hostel No. 15 (Medha Hostel) | Masjid Moth Campus | 4961 | 26594961 |
| Hostel No. 16 (Agnivesa Hostel) | Masjid Moth Campus | 4154 | 26594154 |
| Hostel No. 17 (Ambuja Hostel) | Masjid Moth Campus | 3249 | 26593249 |
| Hostel No. 18 (Kashyap Hostel) | Masjid Moth Campus | 4960 | 26594960 |
| Hostel No. 19 (Patanjali Hostel) | Masjid Moth Campus | 3865 | 26593865 |
| JPNATC Hostel | Raj Nagar | - | 26731225 |
| Name | Location | Internal | External |
|---|---|---|---|
| Hostel No. 1 (Charak Hostel) | Gents Hostels (U.G.) | 4377 3393 | 26594377 26593393 |
| Hostel No. 2 (Jivak Hostel) | Gents Hostels (U.G.) | 3592 | 26593592 |
| Hostel No. 3 (Sushruta Hostel) | Gents Hostels (U.G.) | 3593 | 26593593 |
| Hostel No. 4 (Madhava Hostel) | Gents Hostels (U.G.) | 3594 | 26593594 |
| Hostel No. 5 (Nagarjuna Hostel) | Gents Hostels (U.G.) | 4554 | 26594554 |
| Hostel No. 6 (Vagbhatta Hostel) | Gents Hostels (U.G.) | 4634 | 26594634 |
| Hostel No. 7 (Ashwini Hostel) | Gents Hostels (U.G.) | - | - |
| Hostel No. 8 (Bharadwaj Hostel) | Gents Hostels (P.G.) | 4475 | 26594475 |
| Hostel No. 9 (Parvati Hostel) | Ladies Hostels (U.G. & P.G.) | 4640 | 26594640 |
| Hostel No. 10 (Saraswati Hostel) | Ladies Hostels (U.G.) | 4578 | 26594578 |
| Hostel No. 11 (Akshara Hostel) C2 Flats | Ladies Hostels (U.G.) | 4241 | 26594241 |
| Hostel No. 12 (Dhanwantri Hostel) RPC I | Gents Hostels Near RP Centre (P.G.) | 3080 | 26593080 |
| Hostel No. 13 (Laxmi Hostel) RPC II | Ladies Hostels (U.G.) | 3081 | 26593081 |
| Hostel No. 14 (Atreya Hostel) | Masjid Moth Campus Ground Floor Reception (P.G.) | 4950 | 26594950 |
| Hostel No. 15 (Medha Hostel) | Masjid Moth Campus Ground Floor Reception (U.G. & P.G.) | 4964 4965 | 26594964 26594965 |
| Hostel No. 16 (Agnivesa Hostel) | Masjid Moth Campus (P.G.) | 4152 | 26594152 |
| Hostel No. 17 (Ambuja Hostel) | Masjid Moth Campus (P.G.) | 3249 | 26593249 |
| Hostel No. 18 (Kashyap Hostel) | Masjid Moth Campus (U.G. & P.G.) | 4959 | 26594959 |
| Hostel No. 19 (Patanjali Hostel) | Masjid Moth Campus (P.G.) | 3866 3867 | 26593866 26593867 |
| JPNATC Hostel | Raj Nagar (P.G.) | - | 26731204 |
Letters should be addressed to the Superintendent of Hostels. In case of official letters, these should be routed through the Head of the Department or the Registrar (in the case of Undergraduates and Trainees) or the Principal College of Nursing (for Nursing Students). Letters should be handed over to the Hostel Office (in the Gents Hostels) and a receipt obtained if delivered by hand. In case of any complaints these should be handed over in sealed envelopes whenever confidentiality is to be maintained.
E-MAIL: You may e-mail the Superintendent of Hostels at hostels@aiims.edu for any questions or complaints. Strict confidentiality will be maintained in all these e-mails since access is only available to the Hostel Superintendent. Unsolicited mails shall not be entertained.
Please do feel free to contact us for any queries or doubts, we try to be a helpful bunch!
Since by and large only those who are in an academic course or training are accommodated in the hostels, applications are received after the applicant has formally been offered the position and has joined the institution.
For undergraduate students, generally, the admission procedure for the hostels is arranged along with the admission formalities for the course. The entire process is completed in one of the rooms in the teaching block with the staff from the academic section and the hostel office. Therefore it may not be necessary to go to the hostel office under such circumstances.
Application Forms are to be submitted in the following offices, unless collected otherwise (as mentioned in the case of undergraduates):
Click here for Procedure To Apply For Hostel Accommodation Online (for Post Graduate).
Click here for Procedure To Apply For Hostel Accommodation Online (for Under Graduate).
IF ANY QUERY ABOUT HOSTEL APPLICATION PLEASE CONTACT HOSTEL SECTION.
Very few documents are required. You are required to submit the application form duly forwarded by the Head of the Department and the Registrar (or only the Registrar in the case of undergraduate students). Also enclose a copy of the Appointment Letter , Joining letter duly forwarded by registrar and two recent passport sized photographs, one of which is to be pasted on the application form. You should have made the necessary payments (including the Hostel security Deposit).
Kindly note the receipt number since this will help you track your allotment position, if wait-listed.
Click here for Documents Required For Hostel Accommodation Application.
Every user has different experimental needs. Some users might want to do quantifications/data analyses and making image panels themselves. We are happy to provide all the required support andassistance in terms of offline processing, data quantification and making image panels on a case-to-case basis.
Click here for Documents Required For Hostel Accommodation Application.
PEvery room is provided with a bed, study table, chair, bookshelf (in some hostels), steel almirah / wooden in built cupboard. In addition you will be provided with a ceiling fan, bulb holder fitting and tubelight fitting. There is a three-pin plug point in every room. Additional beds / double bed, dining table and chairs are provided in married accommodation.
Please check and sign the inventory before shifting into a room / accommodation.
STATEMENT OF HOSTEL FEES STRUCTURE
| S.NO. | COURSE | POT FUND (Per Month) | HOSTEL RENT (Per Month) | ELECTRICITY (Per Month) | GYMKHANA (Per Month) | TOTAL HOSTEL FEES/ CHARGES |
|---|---|---|---|---|---|---|
| 1. | MD/MS/MDS (3 Years) | NIL | NIL | Rs. 7/- | Rs. 3/- | Rs. 360/- |
| 2. | M.Ch. (6 Years) | NIL | NIL | Rs. 7/- | Rs. 3/- | Rs. 720/- |
3.
| MD/MS/MDS (Sponsored) (3 Years) | Rs. 20/- | Unmarried Rs. 450/- Married Rs. 650/- | Rs. 7/- | Rs. 3/- | Hostel Fees Rs. 1080/- Hostel Rent Unmarried (+)Rs. 16200/- |
| Total Rs. 17280/- | ||||||
Hostel Fees Rs. 1080/- Hostel Rent Married (+) Rs. 23400/- | ||||||
| Total Rs. 24480/- | ||||||
| 4. | DM/M.Ch. (3 Years) | NIL | NIL | Rs. 7/- | Rs. 3/- | Rs. 360/- |
| 5. | DM/M.Ch. (Sponsored) (3 Years) | Rs. 20/- | Unmarried Rs. 450/- Married Rs. 650/- | Rs. 7/- | Rs. 3/- | Hostel Fees Rs. 1080/- Hostel Rent Unmarried (+)Rs. 16200/- |
| Total Rs. 17280/- | ||||||
Hostel Fees Rs. 1080/- Hostel Rent Married (+) Rs. 23400/- | ||||||
| Total Rs. 24480/- | ||||||
| 6. | Ph.D. (5 Years) | Rs. 20/- | Rs. 30/- | Rs. 7/- | Rs. 3/- | Rs. 3600/- |
| 7. | MBBS 51/2 Years (Including Internship) | Rs. 20/- | Rs. 15/- | Rs. 3/- | Rs. 220/- (51/2 Years) | Rs. 2728/- |
| 8. | M.Sc. Nursing (2 Years) | Rs. 20/- | NIL | Rs. 10/- | Rs. 3/- | Rs. 792/- |
| 9. | M.Sc. Other Courses (2 Years) | Rs. 20/- | NIL | Rs. 10/- | Rs. 3/- | Rs. 792/- |
| 10. | B.Sc. Nursing (4 Years) | Rs. 20/- | Rs. 10/- | NIL | NIL | Rs. 1440/- |
| 11. | B.Sc. (Opthal) (4 Years) (Including Internship) | Rs. 20/- | NIL | NIL | NIL | Rs. 960/- |
| 12. | B.Sc. (Dental Hygiene Course) (31/2 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 840/- |
| 13. | B.Sc. (Dental Operation Room Assistant) (4 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 960/- |
| 14. | B.Sc. (Operation Theatre Technology) (31/2 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 840/- |
| 15. | B.Sc. (MRIT) (31/2 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 840/- |
HOSTEL SECURITY Rs. 1000/- (REFUNDABLE) DEPOSITED AT THE TIME OF SUBMISSION OF APPLICATION FOR THE HOSTEL ACCOMMODATION.
In case you are eligible to draw house rent allowance, then according to the prevailing rules you cannot claim House Rent Allowance (HRA) if you stay in the hostel.
In case your spouse is eligible to draw House Rent Allowance (HRA) then both you and your spouse cannot claim the allowance if you stay in the hostels. This is applicable if the allotment is either in the name of the husband or the wife. Please check for further details with the Finance / Accounts Section regarding the rules and regulations. Note: It is a serious offence if you do not disclose your marital status and the office of employment of your spouse during your tenure in the institution.
Please check for further details with the Finance / Accounts Section regarding the rules and regulations. Note: It is a serious offence if you do not disclose your marital status and the office of employment of your spouse during your tenure in the institution.
In case both the husband and wife are government employees (including one or both being Junior / Senior Residents of AIIMS) and do not reside in any government accommodation (including AIIMS hostels) then both are eligible to draw house rent allowance. This is not applicable if either one has a government accommodation. In other cases the appropriate rules shall apply. Please check for further details with the Finance / Accounts Section regarding the rules and regulations.
A certificate is given on request to those Resident Doctors who do not stay in the hostels so that this is submitted to the Accounts Section for payment of House Rent Allowance (HRA). It is mandatory to submit this certificate.
Ragging in any form is strictly prohibited anywhere within the institutional campus including the hostels. Individual or collective ragging constitutes gross indiscipline and will be dealt with severely with punitive measures that includes rustication.
Ragging shall ordinarily mean any act or conduct by an individual or group of individuals by which the dominant status or power of senior students is brought to bear upon the students who are in any way considered to be junior or inferior to them. Some acts that are included in this definition are:
No junior student should be taken into the room of a senior student or found in the room of a senior student till the ‘freshers’ welcome party is over. In case this is reported or found it shall be considered as ‘ragging’ unless otherwise proven.
An Anti-Ragging Committee is constituted every year for the purpose of surveillance, to ensure that acts of ragging do not occur and look into specific instances of ‘ragging’. Students are requested to bring all acts of ragging to the notice of the committee or authorities concerned. This will help in making new students comfortable and allow them to settle into an entirely new atmosphere. Many of the undergraduates leave the secure precincts of their home for the first time and the seniors are expected to realize this and conduct themselves accordingly.
Yes, a music system or a television set may be kept in the married room provided this does not exceed the sanctioned electrical load and does not in any way disturb fellow-hostellers. All hostels have facilities for cable connection at predetermined fixed-rates. Further there are TV Rooms where one may watch television programmes.
Yes you may keep a computer in your room.
No, installation of air-conditioners and similar electrical gadgets are strictly prohibited. These gadgets draw power far in excess of the sanctioned load and are not only illegal but also jeopardize the power supply of the campus and pose a serious fire-hazard.
According to current rules you are permitted to stay in the hostels for a maximum period of ten days after you have completed your tenure / examinations / course as scheduled in the academic calendar or as appointed. Ph.D. Scholars are permitted to stay for a maximum period of five years / thesis submission whichever is earlier. Resignations, discontinuations, termination of service and rustication shall be considered as completion of tenure / course.
The schedules in AIIMS are followed strictly and every Student / Resident Doctor / Ph.D. Scholar is aware of the probable date of completion (as defined above) literally at the time of joining. The Hostel Office is not obliged to intimate students of this date. This is the responsibility of every hosteller. Any delay in vacation of the room shall constitute a violation of hostel rules and invite appropriate penalty. All hostellers are therefore required to plan their departure accordingly. This would help in accommodating new batch of hostellers, many of whom come from different parts of the country and overseas and do not have relatives, friends or place to stay in Delhi.
Hostellers are not encouraged to change their allotted room. In exceptional circumstances the room can be changed on written request to the Hostel Superintendent giving the reasons for this request.
The mutual exchange is provided in the same type or at par hostel accommodation only once in the entire tenure subject to the following condition:-
For fresh offer - 7 working days (excluding Sunday and Gazetted Holiday), For fresh allotment - 10 working days (excluding Sunday and Gazetted Holiday), For change offer - 3 working days (excluding Sunday and Gazetted Holiday) and For change allotment - 7 working days (excluding Sunday and Gazetted Holiday).The allotment letter is provided to every hosteller through the Head of the Department. He / she have to contact the Hostel Office and intimate whether he / she is interested in the accommodation. In case he / she does not contact the office it is presumed that the person is not interested and has refused the allotment and he / she will be debarred from the waiting list for 6 months.
If you do not shift into the allotted room, the person next in the priority list is offered the room. You are then debarred for a period of six month from further allotment.
Hostellers are discouraged from overstaying. Strict action is taken against defaulters. However if there is a dire need then an written application is to be submitted to the Superintendent of Hostels, duly forwarded and recommended by the Head of the Department citing the reasons for extending the stay. Each case is evaluated on individual merit and decided accordingly. In general, extensions are extraordinary and refusals are to be expected.
Exceeding the period of stay is a serious offence. In case the hostel is not vacated, ‘no dues’ certificate is not issued. Without this certificate the last pay and benefits are withheld and the degree certificate is not released. Further penal rent is imposed. The room may be double-locked and necessary eviction proceedings are instituted.
Visitors are permitted in the hostels. However visitors are to make the necessary entries in the registers. Hostellers are not encouraged to take visitors into their rooms.
Proof of Residence Certificate is issued on the basis of an application in the form available in the Hostel Website. The application is to be forwarded through the Head of the Department or the Registrar (in the case of undergraduate students). The reason for which this certificate is required must be clearly indicated. Normally it takes one weekto issue this certificate.
You may choose one or several options available. There are cooperative messes run by hostellers for which the membership is limited. In addition there are contractor run messes where boarding charges may be paid monthly or for each meal. In addition there are Cafes that serve dishes that are to be ordered and paid for every time. You should check and discover what suits you best. Your seniors would guide you. A list of the messes and Cafes are available with the Hostel Office.
It is mandatory for every commercial establishment in the Hostels to maintain and produce on demand a Complaint Book. These complaints are checked periodically and fine imposed or appropriate action taken after verification. In case the Complaint Book is not available or you are not satisfied please do meet the Senior Warden and the Superintendent of Hostels.
Consumption of alcohol is prohibited in the hostels.
Vehicles belonging to hostellers may be parked within the hostel compound. However all hostellers are required to register their vehicles with the Security Officer (near the Central admission Office and Railway reservation Counter opposite the Emergency Entry Gate) and display the AIIMS Vehicle Pass Sticker (oval, blue coloured). If the approved sticker is not displayed the vehicle is liable to towed away.
Visitors are requested to park their vehicles in the designated parking lots outside the hostels.
Please note : this call center exclusively manages OPD appointments. We are unable to assist with any general hospital inquiries or other services."
11-26589141, 26589142, 26589143, 26589144
Timing for OPD booking on this Telephone is from 8:30 AM to 4:30 PM on Monday to Friday ( all working days). On Saturday (working day), the timing for OPD appointment booking is from 8:30 AM to 1:00 PM.
011-26589141, 26589142, 26589143, 26589144
"The appointment for new case is available for one month (depending upon the availability of OPD slots) from the date of applying for appointment and for the follow-up, the appointment is available for three months (also depending upon the availability of OPD slots) from the date of applying for the appointment".
Mobile App: The AIIMS App has been removed from the Google Play store due to issues with the app rendering it non-functional. Users who had installed that app should remove it from their devices.
For effective follow-up of post operative cardiac surgical patients at CTVS -OPD services, dedicated Helpline & Whatsapp numbers: 9999635940, 9999635425 will be active from 2:00pm to 6:00pm on Monday, Wednesday and Friday (i.e. otherwise usual OPD hours)/CTVS –OPD
Note:- If appointments are not available on O.R.S portal, then please do not call the call centre, as appointment through ORS portal and phone is from same pool.
Letters should be addressed to the Superintendent of Hostels. In case of official letters, these should be routed through the Head of the Department or the Registrar (in the case of Undergraduates and Trainees) or the Principal College of Nursing (for Nursing Students). Letters should be handed over to the Hostel Office (in the Gents Hostels) and a receipt obtained if delivered by hand. In case of any complaints these should be handed over in sealed envelopes whenever confidentiality is to be maintained.
E-MAIL: You may e-mail the Superintendent of Hostels at hostels@aiims.edu for any questions or complaints. Strict confidentiality will be maintained in all these e-mails since access is only available to the Hostel Superintendent. Unsolicited mails shall not be entertained.
Please do feel free to contact us for any queries or doubts, we try to be a helpful bunch!
| Name | Location | Internal | External |
|---|---|---|---|
| Hostel No. 1 (Charak Hostel) | Gents Hostels (U.G.) | 4377 3393 | 26594377 26593393 |
| Hostel No. 2 (Jivak Hostel) | Gents Hostels (U.G.) | 3592 | 26593592 |
| Hostel No. 3 (Sushruta Hostel) | Gents Hostels (U.G.) | 3593 | 26593593 |
| Hostel No. 4 (Madhava Hostel) | Gents Hostels (U.G.) | 3594 | 26593594 |
| Hostel No. 5 (Nagarjuna Hostel) | Gents Hostels (U.G.) | 4554 | 26594554 |
| Hostel No. 6 (Vagbhatta Hostel) | Gents Hostels (U.G.) | 4634 | 26594634 |
| Hostel No. 7 (Ashwini Hostel) | Gents Hostels (U.G.) | - | - |
| Hostel No. 8 (Bharadwaj Hostel) | Gents Hostels (P.G.) | 4475 | 26594475 |
| Hostel No. 9 (Parvati Hostel) | Ladies Hostels (U.G. & P.G.) | 4640 | 26594640 |
| Hostel No. 10 (Saraswati Hostel) | Ladies Hostels (U.G.) | 4578 | 26594578 |
| Hostel No. 11 (Akshara Hostel) C2 Flats | Ladies Hostels (U.G.) | 4241 | 26594241 |
| Hostel No. 12 (Dhanwantri Hostel) RPC I | Gents Hostels Near RP Centre (P.G.) | 3080 | 26593080 |
| Hostel No. 13 (Laxmi Hostel) RPC II | Ladies Hostels (U.G.) | 3081 | 26593081 |
| Hostel No. 14 (Atreya Hostel) | Masjid Moth Campus Ground Floor Reception (P.G.) | 4950 | 26594950 |
| Hostel No. 15 (Medha Hostel) | Masjid Moth Campus Ground Floor Reception (U.G. & P.G.) | 4964 4965 | 26594964 26594965 |
| Hostel No. 16 (Agnivesa Hostel) | Masjid Moth Campus (P.G.) | 4152 | 26594152 |
| Hostel No. 17 (Ambuja Hostel) | Masjid Moth Campus (P.G.) | 3249 | 26593249 |
| Hostel No. 18 (Kashyap Hostel) | Masjid Moth Campus (U.G. & P.G.) | 4959 | 26594959 |
| Hostel No. 19 (Patanjali Hostel) | Masjid Moth Campus (P.G.) | 3866 3867 | 26593866 26593867 |
| JPNATC Hostel | Raj Nagar (P.G.) | - | 26731204 |
| Name | Location | Internal | External |
|---|---|---|---|
| Hostel Section | Gents Hostels Hostel No. 7 (Ashwini Hostel) Ansari Nagar (East) | 4633 6661 3487 | 26594633 26546661 26593487 |
| Ladies Hostels | Ladies Hostels Hostel No. 10 (Saraswati Hostel) Ansari Nagar (East) | 3096 4578 4306 | 26593096 26594578 26594306 |
| Hostel No. 12 (Dhanwantri Hostel) RPC I | RPC Gents Hostel Ansari Nagar (East) | 3320 | 26593320
|
| Hostel No. 14 (Atreya Hostel) | Masjid Moth Campus | 4951 4952 4954 | 26594951 26594952 26594954 |
| Hostel No. 15 (Medha Hostel) | Masjid Moth Campus | 4961 | 26594961 |
| Hostel No. 16 (Agnivesa Hostel) | Masjid Moth Campus | 4154 | 26594154 |
| Hostel No. 17 (Ambuja Hostel) | Masjid Moth Campus | 3249 | 26593249 |
| Hostel No. 18 (Kashyap Hostel) | Masjid Moth Campus | 4960 | 26594960 |
| Hostel No. 19 (Patanjali Hostel) | Masjid Moth Campus | 3865 | 26593865 |
| JPNATC Hostel | Raj Nagar | - | 26731225 |
| Name | Location | Internal | External |
|---|---|---|---|
Prof. Sanjay Kumar Rai Superintendent of Hostels | Department of Centre for Community Medicine | 4416 | 26594416 |
Prof. Neerja Bhatla Deputy Superintendent of Hostel | Department of Obst. & Gynae. | 4991 | 26594991 |
Prof. Tanuj Dada Deputy Superintendent of Hostel | Department of Ophthalmology | 3001 | 26593001 |
Prof. Raj Kumar Yadav Deputy Superintendent of Hostel | Department of Physiology | 6461 | 26546461 |
Prof. Rakesh Kumar Deputy Superintendent of Hostel | Department of E.N.T. | 3443 | 26593443 |
Prof. K.H. Reeta Deputy Superintendent of Hostel | Department of Pharmacology | 3247 | 26593247 |
Prof. Vijay Sharma Deputy Superintendent of Hostel | Department of Orthopedics JPNATC | - | 26731160 |
Dr. Harshal Ramesh Salve Additional Professor Deputy Superintendent of Hostel | Department of C.C.M. | 3366 | 26593366 |
Ms. Cecilia M.S. Associate Professor Deputy Superintendent of Hostel | College of Nursing | 4457 | 26594457 |
Ms. Bhupinder Kaur D.N.S. Deputy Superintendent of Hostel | Main Hospital C.N.O. Office | 4705 | 26594705 |
Mr. Uttam Chand Administrative Officer (Hostels) | Examination Section | 6422 | 26596422 |
Mr. Yatender Meena Store Officer (Hostels) | Store Section (CNC) | 4704 | 26594704 |
Mr. Amit Kumar Accounts Officer (Hostels) | Cash Section | 3687 | 26593687 |
Mr. Mohan Kumar Sharma Senior Warden (Hostels) | Hostel Section | 4633 6661 3487 4954(M.M.H.) | 26594633 26546661 26593487 26594954 |
| Service | Location | Internal | External | |
|---|---|---|---|---|
| Casualty | AIIMS | Screening | 3887 | - |
| Emergency 1 | 4084 4085 | - - | ||
| New Emergency Ward | 4405 4591 3415 | 26594405 - - | ||
| Surgery | 4255 4706 | - - | ||
| Duty Officer | AIIMS | 3308 3574 | 26593308 26593574 | |
| Security Control Room | AIIMS | 4780 3333 4444 | 26594780 - - | |
| Police | AIIMS Post | 3345 | 26593345 | |
| Control Room | - | 112 | ||
| Defence Colony | - | 26253402 | ||
| Hauz Khas | - | 26867878 | ||
| Sarojini Nagar | - | 24671281 | ||
| Fire (PC Block) | AIIMS | 3661 | 26593661 | |
| Masjid Moth Hostels | 4950 | 26594950 | ||
| Delhi Fire Service | - | 101 | ||
| J.E. (Electrical) | Gents Hostels | 6614 | 26596614 | |
| Electrical Enquiry | Gents Hostels | 3424 | 26593424 | |
| J.E. (Electrical) | Ladies Hostels | 3777 | 26593777 | |
| Electrical Enquiry | Ladies Hostels | 6324 | 26596324 | |
| J.E. (Electrical) | RPC Hostels | 3777 | 26593777 | |
| Electrical Enquiry | RPC Hostels | 6324 | 26596324 | |
| J.E. (Electrical) | Masjid Moth Hostels | 6715 | 26546715 | |
| Electrical Enquiry | Masjid Moth Hostels | 4233 | 26594233 | |
| J.E. (Electrical) | JPNATC Hostel | 1208 1285 | 26731208 26731285 | |
| Electrical Enquiry | JPNATC Hostel | 1210 | 26731210 | |
| NDMC, Kidwai Nagar | - - | 24104748 24106892 | ||
| J.E. (Civil) | Gents Hostels | 3656 | 26593656 | |
| Civil Enquiry | Gents Hostels | 4054 | 26594054 | |
| J.E. (Civil) | Ladies Hostels | 6419 | 26596419 | |
| Civil Enquiry | Ladies Hostels | 3065 | 26593065 | |
| J.E. (Civil) | RPC Hostels | 6419 | 26596419 | |
| Civil Enquiry | RPC Hostels | 3065 | 26593065 | |
| J.E. (Civil) | Masjid Moth Hostels | 4959 | 26544959 | |
| Civil Enquiry | Masjid Moth Hostels | 4959 | 26544959 | |
| J.E. (Civil) | JPNATC Hostel | 1209 | 26731209 | |
| Civil Enquiry | JPNATC Hostel | 1199 | 26731199 | |
Since by and large only those who are in an academic course or training are accommodated in the hostels, applications are received after the applicant has formally been offered the position and has joined the institution.
For undergraduate students, generally, the admission procedure for the hostels is arranged along with the admission formalities for the course. The entire process is completed in one of the rooms in the teaching block with the staff from the academic section and the hostel office. Therefore it may not be necessary to go to the hostel office under such circumstances.
Application Forms are to be submitted in the following offices, unless collected otherwise (as mentioned in the case of undergraduates):
Click here for Procedure To Apply For Hostel Accommodation Online (for Post Graduate).
Click here for Procedure To Apply For Hostel Accommodation Online (for Under Graduate).
IF ANY QUERY ABOUT HOSTEL APPLICATION PLEASE CONTACT HOSTEL SECTION.
Very few documents are required. You are required to submit the application form duly forwarded by the Head of the Department and the Registrar (or only the Registrar in the case of undergraduate students). Also enclose a copy of the Appointment Letter , Joining letter duly forwarded by registrar and two recent passport sized photographs, one of which is to be pasted on the application form. You should have made the necessary payments (including the Hostel security Deposit).
Kindly note the receipt number since this will help you track your allotment position, if wait-listed.
Click here for Documents Required For Hostel Accommodation Application.
Every user has different experimental needs. Some users might want to do quantifications/data analyses and making image panels themselves. We are happy to provide all the required support andassistance in terms of offline processing, data quantification and making image panels on a case-to-case basis.
Click here for Documents Required For Hostel Accommodation Application.
PEvery room is provided with a bed, study table, chair, bookshelf (in some hostels), steel almirah / wooden in built cupboard. In addition you will be provided with a ceiling fan, bulb holder fitting and tubelight fitting. There is a three-pin plug point in every room. Additional beds / double bed, dining table and chairs are provided in married accommodation.
Please check and sign the inventory before shifting into a room / accommodation.
STATEMENT OF HOSTEL FEES STRUCTURE
| S.NO. | COURSE | POT FUND (Per Month) | HOSTEL RENT (Per Month) | ELECTRICITY (Per Month) | GYMKHANA (Per Month) | TOTAL HOSTEL FEES/ CHARGES |
|---|---|---|---|---|---|---|
| 1. | MD/MS/MDS (3 Years) | NIL | NIL | Rs. 7/- | Rs. 3/- | Rs. 360/- |
| 2. | M.Ch. (6 Years) | NIL | NIL | Rs. 7/- | Rs. 3/- | Rs. 720/- |
3.
| MD/MS/MDS (Sponsored) (3 Years) | Rs. 20/- | Unmarried Rs. 450/- Married Rs. 650/- | Rs. 7/- | Rs. 3/- | Hostel Fees Rs. 1080/- Hostel Rent Unmarried (+)Rs. 16200/- |
| Total Rs. 17280/- | ||||||
Hostel Fees Rs. 1080/- Hostel Rent Married (+) Rs. 23400/- | ||||||
| Total Rs. 24480/- | ||||||
| 4. | DM/M.Ch. (3 Years) | NIL | NIL | Rs. 7/- | Rs. 3/- | Rs. 360/- |
| 5. | DM/M.Ch. (Sponsored) (3 Years) | Rs. 20/- | Unmarried Rs. 450/- Married Rs. 650/- | Rs. 7/- | Rs. 3/- | Hostel Fees Rs. 1080/- Hostel Rent Unmarried (+)Rs. 16200/- |
| Total Rs. 17280/- | ||||||
Hostel Fees Rs. 1080/- Hostel Rent Married (+) Rs. 23400/- | ||||||
| Total Rs. 24480/- | ||||||
| 6. | Ph.D. (5 Years) | Rs. 20/- | Rs. 30/- | Rs. 7/- | Rs. 3/- | Rs. 3600/- |
| 7. | MBBS 51/2 Years (Including Internship) | Rs. 20/- | Rs. 15/- | Rs. 3/- | Rs. 220/- (51/2 Years) | Rs. 2728/- |
| 8. | M.Sc. Nursing (2 Years) | Rs. 20/- | NIL | Rs. 10/- | Rs. 3/- | Rs. 792/- |
| 9. | M.Sc. Other Courses (2 Years) | Rs. 20/- | NIL | Rs. 10/- | Rs. 3/- | Rs. 792/- |
| 10. | B.Sc. Nursing (4 Years) | Rs. 20/- | Rs. 10/- | NIL | NIL | Rs. 1440/- |
| 11. | B.Sc. (Opthal) (4 Years) (Including Internship) | Rs. 20/- | NIL | NIL | NIL | Rs. 960/- |
| 12. | B.Sc. (Dental Hygiene Course) (31/2 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 840/- |
| 13. | B.Sc. (Dental Operation Room Assistant) (4 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 960/- |
| 14. | B.Sc. (Operation Theatre Technology) (31/2 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 840/- |
| 15. | B.Sc. (MRIT) (31/2 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 840/- |
HOSTEL SECURITY Rs. 1000/- (REFUNDABLE) DEPOSITED AT THE TIME OF SUBMISSION OF APPLICATION FOR THE HOSTEL ACCOMMODATION.
In case you are eligible to draw house rent allowance, then according to the prevailing rules you cannot claim House Rent Allowance (HRA) if you stay in the hostel.
In case your spouse is eligible to draw House Rent Allowance (HRA) then both you and your spouse cannot claim the allowance if you stay in the hostels. This is applicable if the allotment is either in the name of the husband or the wife. Please check for further details with the Finance / Accounts Section regarding the rules and regulations. Note: It is a serious offence if you do not disclose your marital status and the office of employment of your spouse during your tenure in the institution.
Please check for further details with the Finance / Accounts Section regarding the rules and regulations. Note: It is a serious offence if you do not disclose your marital status and the office of employment of your spouse during your tenure in the institution.
In case both the husband and wife are government employees (including one or both being Junior / Senior Residents of AIIMS) and do not reside in any government accommodation (including AIIMS hostels) then both are eligible to draw house rent allowance. This is not applicable if either one has a government accommodation. In other cases the appropriate rules shall apply. Please check for further details with the Finance / Accounts Section regarding the rules and regulations.
A certificate is given on request to those Resident Doctors who do not stay in the hostels so that this is submitted to the Accounts Section for payment of House Rent Allowance (HRA). It is mandatory to submit this certificate.
Ragging in any form is strictly prohibited anywhere within the institutional campus including the hostels. Individual or collective ragging constitutes gross indiscipline and will be dealt with severely with punitive measures that includes rustication.
Ragging shall ordinarily mean any act or conduct by an individual or group of individuals by which the dominant status or power of senior students is brought to bear upon the students who are in any way considered to be junior or inferior to them. Some acts that are included in this definition are:
No junior student should be taken into the room of a senior student or found in the room of a senior student till the ‘freshers’ welcome party is over. In case this is reported or found it shall be considered as ‘ragging’ unless otherwise proven.
An Anti-Ragging Committee is constituted every year for the purpose of surveillance, to ensure that acts of ragging do not occur and look into specific instances of ‘ragging’. Students are requested to bring all acts of ragging to the notice of the committee or authorities concerned. This will help in making new students comfortable and allow them to settle into an entirely new atmosphere. Many of the undergraduates leave the secure precincts of their home for the first time and the seniors are expected to realize this and conduct themselves accordingly.
Yes, a music system or a television set may be kept in the married room provided this does not exceed the sanctioned electrical load and does not in any way disturb fellow-hostellers. All hostels have facilities for cable connection at predetermined fixed-rates. Further there are TV Rooms where one may watch television programmes.
Yes you may keep a computer in your room.
No, installation of air-conditioners and similar electrical gadgets are strictly prohibited. These gadgets draw power far in excess of the sanctioned load and are not only illegal but also jeopardize the power supply of the campus and pose a serious fire-hazard.
According to current rules you are permitted to stay in the hostels for a maximum period of ten days after you have completed your tenure / examinations / course as scheduled in the academic calendar or as appointed. Ph.D. Scholars are permitted to stay for a maximum period of five years / thesis submission whichever is earlier. Resignations, discontinuations, termination of service and rustication shall be considered as completion of tenure / course.
The schedules in AIIMS are followed strictly and every Student / Resident Doctor / Ph.D. Scholar is aware of the probable date of completion (as defined above) literally at the time of joining. The Hostel Office is not obliged to intimate students of this date. This is the responsibility of every hosteller. Any delay in vacation of the room shall constitute a violation of hostel rules and invite appropriate penalty. All hostellers are therefore required to plan their departure accordingly. This would help in accommodating new batch of hostellers, many of whom come from different parts of the country and overseas and do not have relatives, friends or place to stay in Delhi.
Hostellers are not encouraged to change their allotted room. In exceptional circumstances the room can be changed on written request to the Hostel Superintendent giving the reasons for this request.
The mutual exchange is provided in the same type or at par hostel accommodation only once in the entire tenure subject to the following condition:-
For fresh offer - 7 working days (excluding Sunday and Gazetted Holiday), For fresh allotment - 10 working days (excluding Sunday and Gazetted Holiday), For change offer - 3 working days (excluding Sunday and Gazetted Holiday) and For change allotment - 7 working days (excluding Sunday and Gazetted Holiday).The allotment letter is provided to every hosteller through the Head of the Department. He / she have to contact the Hostel Office and intimate whether he / she is interested in the accommodation. In case he / she does not contact the office it is presumed that the person is not interested and has refused the allotment and he / she will be debarred from the waiting list for 6 months.
If you do not shift into the allotted room, the person next in the priority list is offered the room. You are then debarred for a period of six month from further allotment.
Hostellers are discouraged from overstaying. Strict action is taken against defaulters. However if there is a dire need then an written application is to be submitted to the Superintendent of Hostels, duly forwarded and recommended by the Head of the Department citing the reasons for extending the stay. Each case is evaluated on individual merit and decided accordingly. In general, extensions are extraordinary and refusals are to be expected.
Exceeding the period of stay is a serious offence. In case the hostel is not vacated, ‘no dues’ certificate is not issued. Without this certificate the last pay and benefits are withheld and the degree certificate is not released. Further penal rent is imposed. The room may be double-locked and necessary eviction proceedings are instituted.
Visitors are permitted in the hostels. However visitors are to make the necessary entries in the registers. Hostellers are not encouraged to take visitors into their rooms.
Proof of Residence Certificate is issued on the basis of an application in the form available in the Hostel Website. The application is to be forwarded through the Head of the Department or the Registrar (in the case of undergraduate students). The reason for which this certificate is required must be clearly indicated. Normally it takes one weekto issue this certificate.
You may choose one or several options available. There are cooperative messes run by hostellers for which the membership is limited. In addition there are contractor run messes where boarding charges may be paid monthly or for each meal. In addition there are Cafes that serve dishes that are to be ordered and paid for every time. You should check and discover what suits you best. Your seniors would guide you. A list of the messes and Cafes are available with the Hostel Office.
It is mandatory for every commercial establishment in the Hostels to maintain and produce on demand a Complaint Book. These complaints are checked periodically and fine imposed or appropriate action taken after verification. In case the Complaint Book is not available or you are not satisfied please do meet the Senior Warden and the Superintendent of Hostels.
Consumption of alcohol is prohibited in the hostels.
Vehicles belonging to hostellers may be parked within the hostel compound. However all hostellers are required to register their vehicles with the Security Officer (near the Central admission Office and Railway reservation Counter opposite the Emergency Entry Gate) and display the AIIMS Vehicle Pass Sticker (oval, blue coloured). If the approved sticker is not displayed the vehicle is liable to towed away.
Visitors are requested to park their vehicles in the designated parking lots outside the hostels.
Authority letter for Parcel-Courier/पार्सल-कोरियर्स के लिए अधिकार पत्र
Hostel no dues form(Nursing Female)/छात्रावास बेबाकी प्रपत्र (नर्सिग महिला)
Application for allotment of Hostel Accommodation/छात्रावास आवास के आबंटन हेतु आवेदन
Application for Married Accommodation/विवाहित आवास हेतु आवेदन
Application for Grant of House Rent Allowances/मकान किराया-भत्ता का प्रदान करने के लिए आवेदन
Application for purpose of Residence Proof/निवास प्रमाण के अभिप्राय हेतु आवेदन
Eligible for Postgraduates
MALE
Initial Allotment of Unmarried Male in Hostel No. 8 (Bharadwaj Hostel), Hostel No. 12 (Dhanwantri Hostel) RPC I, Hostel No. 14 (Atreya Hostel) & JPNATC Hostel on the basis of Date of Joining, Date of Completion of Application and Receipt no. of security slip for the hostel, respectively.
(Ratio 2:1:1:1:1)
2 Senior Resident, 1 Junior Resident, 1 Senior Resident (AIIMSONION), 1 Junior Resident (AIIMONSION), 1 PHD, Every 4th PHD is AIIMSONION PHD, According to waiting list.
Up gradation for unmarried Male in Hostel No. 18 (Kashyap Hostel), Seniority is given on the basis of Date of Allotment / Date of Application.
MARRIED
Allotment of Married Hostel’s in Hostel No. 14 (Atreya Hostel), Hostel No. 16 (Agnivesa Hostel), Hostel No. 17 (Ambuja Hostel) & JPNATC Hostel, According to waiting list.
Ratio in Married Accommodation
-
(Ratio 3:2:1)
3 Resident (2 Senior Resident & 1 Junior Resident), 2 AIIMSONION Resident (1 Senior Resident & 1 Junior Resident), 1 PHD, Every 4th PHD is AIIMSONION PHD, According to waiting list.
FEMALE
Initial Allotment of Unmarried Female in Hostel No. 9 (Parvati) & Hostel No. 14 (Atreya Hostel) on the basis of Date of Joining, Date of Completion of Application and Receipt no. of security slip for the hostel, respectively.
-
(Ratio 2:1:1:1:1)
2 Senior Resident, 1 Junior Resident, 1 Senior Resident (AIIMSONION), 1 Junior Resident (AIIMONSION), 1 PHD, Every 4th PHD is AIIMSONION PHD, According to waiting list.
Up gradation for unmarried Female in Hostel No. 19 (Patanjali Hostel), Seniority is given on the basis of Date of Allotment / Date of Application.
For Married & Unmarried Accommodation waiting list is updated once a month. 1st week of the every month new list is generated.
If a Resident is given offer / allotment & he / she refuses to take the room than he / she will be debarred from the waiting list for 6 months.
MALE
Allotment of unmarried male in Hostel No. 18 (Kashyap Hostel) on the basis of Date of Joining, Date of Completion of Application and Receipt no. of security slip for the hostel, respectively.
(Ratio)
There is no ratio for B.Sc. Paramedical Students. 36 Seats are reserved for B.Sc. Paramedical Students.
FEMALE
Allotment of Unmarried Female in Hostel No. 9 (Parvati Hostel)& Hostel No. 13 (Laxmi Hostel) RPC II on the basis of Date of Joining, Date of Completion of Application and Receipt no. of security slip for the hostel, respectively.
(Ratio)
There is no ratio for B.Sc. Paramedical Students. 17 seats are reserved for B.Sc. Paramedical students.
These seats are given according to the date of vacation of room, According to waiting list.
For Unmarried Accommodation waiting list is updated once a month. 1st Week of the every month new list is generated.
If a Student is given allotment & he / she refuses to take the room he / she will be debarred from the waiting list for 6 months.
Rooms are allotted according to the waiting list prepared by the Hostel Section. This is on date of joining / date of completion of application basis. All entrants are therefore advised to apply for hostels as soon as they join in case they are interested in such accommodation. Proof of marriage is required for considering allotment to Married Hostels. There is a waiting list for some of the Undergraduate Hostels, Postgraduate Hostels and the Married accommodation. Students are given alternate transit accommodation in two seater & three seater rooms until further accommodation is available. The wait list is updated every month for sharing accommodation, single accommodation & married accommodation. Trainees and other similar category of applicants are accommodated depending on the availability of seats.
Hostel Rules and regulations are framed and should be followed diligently. A copy is available with the Hostel Office. It is expected that all hostellers would conduct themselves in a disciplined manner befitting the honour, tradition, and respectability of the institution and the profession. No form of ragging is permitted in the hostels. Hostellers are required to clear all dues in time. Rooms are to be vacated according to rules and within ten days after completion of tenure or resignation or termination whichever is earlier, according to hostel rules so that the next batch may be accommodated.
In case of any problem or complaints regarding the hostels, the concerned warden or the hostel office or the Superintendent of Hostels should be contacted.
All hostellers are required to look after their rooms and hostel property properly. Water and electricity should be consumed as needed and not wasted. Use of electrical gadgets and machinery without prior permission is strictly prohibited. General cleanliness of the Hostels and toilets is done by the institution.
रेजीडेन्ट/विधार्थी द्वारा वचनवंध-Undertaking by the Resident/Student
Suggestions for hostel web pages
Suggestions and criticisms of this web site are welcome from all hostellers. We would like to thank Drs. Shree Gopal Sharma, Nidhi Aggarwal, Anup Das and Bal Chander for the photographs that you see.
Complaints that would improve the hostels.
Never feel hesitant to make a complaint. Unsolicited and frivolous complaints should be avoided. Whenever the hosteller wishes the names shall not be disclosed.
Depending on the nature of complaint, the complaint may be addressed to the appropriate authority.
For day to day matters - Complain to the Junior Warden or the Concerned Hostel Offices.
Engineering services / repairs in the room - Enquiry offices are available in all hostels / compounds. These offices are open 24 hours. Boards displaying the names of Engineers are displayed at these offices.
Security - Every hostel has security guards round the clock. In case of complaints these may be directed to the guards or the Security Officers any time of the day or night.
Sanitation and Cleanliness - Complaints regarding sanitation and cleanliness may be directed to the Junior / Concerned Wardens who will coordinate with the appropriate authorities.
Shops & Establishments - It is mandatory for all commercial establishments to keep a complaint book. Hostellers may lodge their complaints regarding quality of service, food and other grievances. Mess complaint book is checked regularly by Senior Warden (Hostels) & shops complaint book is checked by Estate Section and appropriate action (such as imposition of fines) is taken.
Other matters - Depending on the gravity and nature of complaint, hostellers may write or meet the Senior Warden or the Deputy Superintendents or the Superintendent without any hesitation.
Penal Rent is levied in case of unauthorized occupation of hostels (e.g. beyond the period of allotment such as, according to current rules, after ten days of completion of tenure).
All Students / Residents are requested to submit their penal rent recovery challan or other challan on the following working days:
Monday to Friday from 11.00 AM to 2.00 PM
Saturday 10.00 AM to 11.30 AM
Challan will not be received by the cashier cell on the last working day of the every month.
| Hostel Category | Hostels / Accommodation | Penal Rent (Per Month) | Penal Rent (Per day) | Normal Rent (Per Month) | Normal Rent (Per day) |
|---|---|---|---|---|---|
Undergraduates Gents & Ladies Hostels (Single rooms) | Hostel No. 1 Charak Hostel (Gents), Hostel No. 2 Jivak Hostel (Gents), Hostel No. 3 Sushruta Hostel (Gents), Hostel No. 4 Madhava Hostel (Gents), Hostel No. 5 Nagarjuna Hostel (Gents), Hostel No. 6 Vagbhatta Hostel (Gents), Hostel No. 10 Saraswati Hostel (Ladies), Hostel No. 13 Laxmi Hostel (RPC-II ) (Ladies), Hostel No. 15 Medha Hostel (Ladies) | Rs. 23,500.00 P.M. | Rs. 783.00 Per day | Rs. 470.00 P.M. | Rs. 16.00 Per day |
Undergraduates Gents & Ladies (Double seater) | Hostel No. 7 Ashwini Hostel (Gents), Hostel No. 9 Parvati Hostel (Ladies), Hostel No. 15 Medha Hostel (Ladies) | Rs. 23,500.00 P.M. | Rs. 783.00 Per day | Rs. 470.00 P.M. | Rs. 16.00 Per day |
Undergraduates Ladies (Double seater) | Hostel No. 11 Akshara Hostel C2 Flats (Ladies)
| Rs. 33,000.00 P.M | Rs. 1100.00 Per day | Rs. 660.00 P.M. | Rs. 22.00 Per day |
Undergraduates Gents & Ladies (Triple seater) | Hostel No. 11 Akshara Hostel C2 Flats (Ladies), Hostel No. 15 Medha Hostel (Ladies), Hostel No. 18 Kashyap Hostel (Gents) | Rs. 23,500.00 P.M. | Rs. 783.00 Per day | Rs. 470.00 P.M. | Rs. 16.00 Per day |
Undergraduates Ladies (Four seater) | Hostel No. 15 Medha Hostel (Ladies) | Rs. 33,000.00 P.M | Rs. 1100.00 Per day | Rs. 660.00 P.M. | Rs. 22.00 Per day |
Undergraduates Ladies (Six seater) | Hostel No. 13 Laxmi Hostel RPC-II (Ladies) | - | - | - | - |
Postgraduates Gents & Ladies Hostels (Single rooms) | Hostel No. 8 Bharadwaj Hostel (Gents), Hostel No. 9 Parvati Hostel (Ladies), Hostel No. 12 Dhanwantri Hostel (RPC-I) (Gents), Hostel No. 14 Atreya Hostel (Gents & Ladies), Hostel No. 16 Agnivesa Hostel (Gents), Hostel No. 18 Kashyap Hostel (Gents), Hostel No. 19 Patanjali Hostel (Ladies), JPNATC Hostel (Gents) | Rs. 23,500.00 P.M. | Rs. 783.00 Per day | Rs. 470.00 P.M. | Rs. 16.00 Per day |
| Postgraduates Gents & Ladies (Double seater) | Hostel No. 9 Parvati Hostel (Ladies), Hostel No. 15 Medha Hostel (Ladies), Hostel No. 18 Kashyap Hostel (Gents), Hostel No. 19 Patanjali Hostel (Ladies) | Rs. 33,000.00 P.M. | Rs.1100.00 Per day | Rs. 660.00 P.M. | Rs. 22.00 Per day |
Postgraduates (Married) | Hostel No. 14 Atreya Hostel, JPNATC Hostel | Rs. 33,000.00 P.M. | Rs. 1100.00 Per day | Rs. 660.00 P.M | Rs. 22.00 Per day |
Hostel No. 16 Agnivesa Hostel, Hostel No. 17 Ambuja Hostel | Rs. 45,500.00 P.M. | Rs. 1517.00 Per day | Rs. 910.00 P.M. | Rs. 31.00 Per day |
| S.NO. | COURSE | POT FUND (Per Month) | HOSTEL RENT (Per Month) | ELECTRICITY (Per Month) | GYMKHANA (Per Month) | TOTAL HOSTEL FEES/ CHARGES |
|---|---|---|---|---|---|---|
| 1. | MD/MS/MDS (3 Years) | NIL | NIL | Rs. 7/- | Rs. 3/- | Rs. 360/- |
| 2. | M.Ch. (6 Years) | NIL | NIL | Rs. 7/- | Rs. 3/- | Rs. 720/- |
3.
| MD/MS/MDS (Sponsored) (3 Years) | Rs. 20/- | Unmarried Rs. 450/- Married Rs. 650/- | Rs. 7/- | Rs. 3/- | Hostel Fees Rs. 1080/- Hostel Rent Unmarried (+)Rs. 16200/- |
| Total Rs. 17280/- | ||||||
Hostel Fees Rs. 1080/- Hostel Rent Married (+) Rs. 23400/- | ||||||
| Total Rs. 24480/- | ||||||
| 4. | DM/M.Ch. (3 Years) | NIL | NIL | Rs. 7/- | Rs. 3/- | Rs. 360/- |
| 5. | DM/M.Ch. (Sponsored) (3 Years) | Rs. 20/- | Unmarried Rs. 450/- Married Rs. 650/- | Rs. 7/- | Rs. 3/- | Hostel Fees Rs. 1080/- Hostel Rent Unmarried (+)Rs. 16200/- |
| Total Rs. 17280/- | ||||||
Hostel Fees Rs. 1080/- Hostel Rent Married (+) Rs. 23400/- | ||||||
| Total Rs. 24480/- | ||||||
| 6. | Ph.D. (5 Years) | Rs. 20/- | Rs. 30/- | Rs. 7/- | Rs. 3/- | Rs. 3600/- |
| 7. | MBBS 51/2 Years (Including Internship) | Rs. 20/- | Rs. 15/- | Rs. 3/- | Rs. 220/- (51/2 Years) | Rs. 2728/- |
| 8. | M.Sc. Nursing (2 Years) | Rs. 20/- | NIL | Rs. 10/- | Rs. 3/- | Rs. 792/- |
| 9. | M.Sc. Other Courses (2 Years) | Rs. 20/- | NIL | Rs. 10/- | Rs. 3/- | Rs. 792/- |
| 10. | B.Sc. Nursing (4 Years) | Rs. 20/- | Rs. 10/- | NIL | NIL | Rs. 1440/- |
| 11. | B.Sc. (Opthal) (4 Years) (Including Internship) | Rs. 20/- | NIL | NIL | NIL | Rs. 960/- |
| 12. | B.Sc. (Dental Hygiene Course) (31/2 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 840/- |
| 13. | B.Sc. (Dental Operation Room Assistant) (4 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 960/- |
| 14. | B.Sc. (Operation Theatre Technology) (31/2 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 840/- |
| 15. | B.Sc. (MRIT) (31/2 Years) | Rs. 20/- | NIL | NIL | NIL | Rs. 840/- |
HOSTEL SECURITY Rs. 1000/- (REFUNDABLE) DEPOSITED AT THE TIME OF SUBMISSION OF APPLICATION FOR THE HOSTEL ACCOMMODATION.
Payments may be required at the time of placing an order or at intervals (monthly) or in advance (in Student run messes) depending on the type of boarding. Current charges for four meals (breakfast, lunch, evening tea, and dinner) in the format of fixed menu is around Rs. 3500.00 per month in most messes, but in the Student run messes this may vary between Rs. 3500.00 to Rs. 4500.00 per month. Boarders are however free to order for other dishes and pay extra. Each mess has its different methods of predetermined service and charge accordingly. The rate-list is available with each mess / café and should be checked.
Actuals to be paid in the mess / café etc. All boarders are required to make payments in time.
Mondays to Fridays: 9:30 AM to 5:15 PM with a short lunch break from 1:00 PM to 1:30 PM.
Saturdays: 9:30 AM to 1:15 PM.
Note: Payments are accepted by the hostel cashier between 9:30 AM to 1:00 PM & 1:30PM to 5:00 PM on week days and between 9:30 AM to 1:00 PM on Saturdays.
| S.No. | Designation | Name |
|---|---|---|
| 1. | Superintendent of Hostels (Chairman) | Prof. Sanjay Kumar Rai |
| 2. | Deputy Superintendent of Hostel | Prof. Neerja Bhatla |
| 3. | Deputy Superintendent of Hostel | Prof. Tanuj Dada |
| 4. | Deputy Superintendent of Hostel | Prof. Raj Kumar Yadav |
| 5. | Deputy Superintendent of Hostel | Prof. Rakesh Kumar |
| 6. | Deputy Superintendent of Hostel | Prof. K.H. Reeta |
| 7. | Deputy Superintendent of Hostel | Prof. Vijay Sharma |
| 8. | Deputy Superintendent of Hostel | Dr. Harshal Ramesh Salve Additional Professor |
| 9. | Deputy Superintendent of Hostel | Ms. Cecilia M.S. Associate Professor |
| 10. | Deputy Superintendent of Hostel | Ms. Bhupinder Kaur Deputy Nursing Superintendent |
| 11. | Administrative Officer (Hostels) | Mr. Uttam Chand |
| 12. | Senior Financial Advisor or his Nominee | - |
| 13. | Superintendent Engineer or his Nominee | - |
| 14. | Senior Warden | Mr. Mohan Kumar Sharma |
| 15. | R.D.A. President or his Nominee | Special invitee |
| 16. | S.Y.S. Chairman or his Nominee | Special invitee |
| 17. | A.S.A. President or his Nominee | Special invitee |
| 18. | S.N.A. President or her Nominee | Special invitee |
| 19. | Co-opted Members | As desired by Chairman |
All major decisions of mutual interest to the administration and the students regarding the functioning of the hostels are taken by the Hostel Advisory Committee and wherever necessary, duly approved by the Director and / or other competent authorities / bodies of the institution.
| Designation | Name | Department |
|---|---|---|
| Superintendent of Hostels | Prof. Sanjay Kumar Rai | Professor, Department of Centre for Community Medicine |
| Deputy Superintendent of Hostel (Ladies Hostels) | Prof. Neerja Bhatla | Professor & H.O.D. Obst. & Gynae. |
| Deputy Superintendent of Hostel | Prof. Tanuj Dada | Professor, Department of Ophthalmology |
| Deputy Superintendent of Hostel | Prof. Raj Kumar Yadav | Professor, Department of Physiology |
| Deputy Superintendent of Hostel | Prof. Rakesh Kumar | Professor, Department of E.N.T. |
| Deputy Superintendent of Hostel (Ladies Hostels) | Prof. K.H. Reeta | Professor, Department of Pharmacology |
| Deputy Superintendent of Hostel (Trauma Centre) | Prof. Vijay Sharma | Professor, Department of Orthopedics |
| Deputy Superintendent of Hostel (CRHSP, Ballabgarh) | Dr. Harshal Ramesh Salve | Additional Professor, Department of C.C.M. |
| Deputy Superintendent of Hostel (Nursing Students) | Ms. Cecilia M.S. | Associate Professor, College of Nursing |
| Deputy Superintendent of Hostel (Nursing Staff) | Ms. Bhupinder Kaur | D.N.S., Main Hospital |
| Designation | Name | Duties |
|---|---|---|
| Senior Warden | Mr. Mohan Kumar Sharma | Supervision of Hostel Section & Masjid Moth Hostels under the direct control of Superintendent of Hostels. |
| Warden | Ms. Seema Pruthi | Supervision of Allotment Division-II Hostel No. 9 (Parvati Hostel) Hostel No. 10 (Saraswati Hostel) Hostel No. 11 (Akshara Hostel) C2 Flats Hostel No. 13 (Laxmi Hostel) RPC-II |
| Deputy Warden | Ms. Suchita Kumari | Supervision of Allotment Division-III & H.No.1 to 8. Organize Hostel Committee Meeting, Prepare the minutes of the meeting & Compile the Annual Report etc. |
| Deputy Warden | Mr. Sukhpal Malik | Supervision of Allotment Division-I Hostel No. 18 (Kashyap Hostel) |
| Assistant Warden | Ms. Tripta Sharma | Allotment of Nurses Hostel (U.G. & P.G.) with the help of Ms. Sonia D.E.O. Hostel No. 15 (Medha Hostel) |
| Assistant Warden | Ms. Rani Varghese | Hostel No. 19 (Patanjali Hostel) |
| Assistant Warden | Mr. Ankit Dogra | To reply of official letters and documents related to Hostel Section. Currently working as a reliever in Hostel No. 7 (Ashwini Hostel), Hostel No. 8 (Bharadwaj Hostel), Hostel No. 12 (Dhanwantri Hostel) RPC-I & JPNATC Hostel. |
| Junior Warden | Mr. Babu Lal Meena | Hostel No. 12 (Dhanwantri Hostel) RPC-I JPNATC Hostel |
| Junior Warden | Mr. Dinesh Desai | Hostel No. 16 (Agnivesa Hostel) Hostel No. 17 (Ambuja Hostel) |
| Junior Warden | Ms. Nirmala Barthwal | Hostel No. 4 (Madhava Hostel) Hostel No. 5 (Nagarjuna Hostel) Management of duties of Group ‘D’ staff. Maintenance of C.L.,E.L. Records. |
| Junior Warden | Mr. Rajesh Rawat | Hostel No. 7 (Ashwini Hostel) Hostel No. 8 (Bharadwaj Hostel) |
| Junior Warden | Ms. Sunil Devi | Hostel No. 1 (Charak Hostel) Hostel No. 2 (Jivak Hostel) Hostel No. 3 (Sushruta Hostel) Hostel No. 6 (Vagbhatta Hostel) |
| Store Keeper | Mr. Pankaj Kumar | Hostel Store |
| Store Keeper (Drugs) | Mr. Ravi Ukhardya Dhanap | Hostel Store |
| Junior Administrative Officer | Ms. Harisha Suri | Hostel Section |
| Senior Administrative Assistant | Ms. Sameena Parveen | Hostel Cashier |
| Senior Administrative Assistant | Mr. Sunil Kumar Sarwan | RTI & All Administrative Matters |
| Junior Administrative Assistant | Mr. Vijendra | Hostel Guest room booking & Hostel fee |
| Junior Administrative Assistant | Ms. Asha | Hostel No. 14 (Atreya Hostel) |
| Junior Administrative Assistant | Mr. Dharam Dutt | Hostel Shops & Establishments |
| Name | Location | Internal | |
|---|---|---|---|
Prof. Sanjay Kumar Rai Superintendent of Hostels | Department of Centre for Community Medicine | 4416 | drsanjay.aiims@gmail.com |
Prof. Neerja Bhatla Deputy Superintendent of Hostel | Department of Obst. & Gynae. | 4991 | neerja.bhatla07@gmail.com |
Prof. Tanuj Dada DeputySuperintendent of Hostel | Department of Ophthalmology | 3001 | tanujdada@gmail.com |
Prof. Raj Kumar Yadav Deputy Superintendent of Hostel | Department of Physiology | 6461 | raj3kr@gmail.com |
Prof. Rakesh Kumar Deputy Superintendent of Hostel | Department of E.N.T. | 3443 | winirk@hotmail.com |
Prof. K.H. Reeta Deputy Superintendent of Hostel | Department of Pharmacology | 3247 | reetakh@gmail.com |
Prof. Vijay Sharma Deputy Superintendent of Hostel | Department of Orthopaedics, JPNATC | 26731160 | drvijaysharmatrauma@gmail.com |
Dr. Harshal Ramesh Salve Additional Professor Deputy Superintendent of Hostel | Department of C.C.M. | 3366 | harshalsalve@ymail.com |
Ms. Cecilia M.S. Associate Professor Deputy Superintendent of Hostel | College of Nursing | 4457 | cecilia.aiims@gmail.com |
Ms. Bhupinder Kaur Deputy Superintendent of Hostel | Main Hospital C.N.O. Office | 4705 | bhupinderkaur65@gmail.com |
Mr. Mohan Kumar Sharma Senior Warden | Hostel Section | 4633 6661 3487 4954(M.M.H.) | mohansharma276@gmail.com |
The Director, AIIMS is the highest authority that oversees the functioning of the hostels. To supervise the hostel section, members of the Faculty are appointed by the Director to work in the capacities of the Superintendent and Deputy Superintendents. The Superintendent of Hostels is the overall in-charge of the hostels. The Hostel Section looks after the day-to-day functioning with the Senior Warden overseeing all the hostels. The Senior Warden is supported by Wardens, Deputy Wardens, Assistant Wardens and Junior Wardens who look after individual hostels along with other staff. You should check and know the respective Warden in charge of your hostel.
There is a Hostel Advisory Committee that oversees various aspects of the functioning of the hostels and includes not only members of the faculty (Superintendent and Deputy Superintendents), the Warden, but also representatives of different students’ bodies such as AIIMS Students Association, Student Nurses Association, Resident Doctors Association and the Society of Young Scientists. Other members from the administration, finance, engineering services and security also contribute to run and maintain various services in the hostels.
The Hostel Section is on the First Floor of Hostel No. VII (first hostel on the right as you enter Gents Hostel). In addition most of the hostels (except Hostels 1-8) have small offices in their premises.
There are several hostel offices. The Hostel Section deals with most matters related to hostellers of all hostels. In addition the smaller offices deal with allotments, vacation and immediate problems that may arise.
| Office | Location | In-charge of Hostels | Duties |
|---|---|---|---|
| Hostel Section and Masjid Moth Hostel Office | Hostel No. 7 (Ashwini Hostel), First Floor, Gents Hostel and Hostel No. 14 (Atreya Hostel), Room No. 002, Ground Floor. | Mr. Mohan Kumar Sharma | Supervision of Hostel Section & Masjid Moth Hostels under the direct control of Superintendent of Hostels. |
| Ladies Hostel Office | Hostel No. 10 (Saraswati Hostel), Room No. 7, Ground Floor. | Ms. Seema Pruthi | Supervision of Allotment Division-II Hostel No. 9 (Parvati Hostel) Hostel No. 10 (Saraswati Hostel) Hostel No. 11 (Akshara Hostel) C2 Flats Hostel No. 13 (Laxmi Hostel) RPC-II |
| Hostel Section | Hostel No. 7 (Ashwini Hostel), First Floor, Gents Hostel. | Ms. Suchita Kumari | Supervision of Allotment Division-III & H.No.1 to 8. Organize Hostel Committee Meeting, Prepare the minutes of the meeting & Compile the Annual Report etc. |
| Masjid Moth Hostel Office | Hostel No. 18 (kashyap Hostel), Room No. 009, Ground Floor. | Mr. Sukhpal Malik | Supervision of Allotment Division-I Hostel No. 18 (Kashyap Hostel) |
| Masjid Moth Hostel Office | Hostel No. 15 (Medha Hostel), Ground Floor. | Ms. Tripta Sharma | Allotment of Nurses Hostel (U.G. & P.G.) with the help of Ms. Sonia D.E.O. Hostel No. 15 (Medha Hostel) |
| Masjid Moth Hostel Office | Hostel No. 19 (Patanjali Hostel), Room No. 005, Ground Floor. | Ms. Rani Varghese | Hostel No. 19 (Patanjali Hostel) |
| Hostel Section | Hostel No. 7 (Ashwini Hostel), First Floor, Gents Hostel. | Mr. Ankit Dogra | To reply of official letters and documents related to Hostel Section. Currently working as a reliever in Hostel No. 7 (Ashwini Hostel), Hostel No. 8 (Bharadwaj Hostel), Hostel No. 12 (Dhanwantri Hostel) RPC-I & JPNATC Hostel. |
| RPC I Hostel Office and JPNATC Hostel Office | Hostel No. 12 (Dhanwantri Hostel) RPC-I, Ground Floor and JPNATC Hostel, Room No. 05, Ground Floor. | Mr. Babu Lal Meena | Hostel No. 12 (Dhanwantri Hostel) RPC-I JPNATC Hostel |
| Masjid Moth Hostel Office | Hostel No. 16 (Agnivesa Hostel), Room No. 14, Ground Floor and Hostel No. 17 (Ambuja Hostel), Room No. 103, Ground Floor. | Mr. Dinesh Desai | Hostel No. 16 (Agnivesa Hostel) Hostel No. 17 (Ambuja Hostel) |
| Hostel Section | Hostel No. 7 (Ashwini Hostel), First Floor, Gents Hostel. | Ms. Nirmala Barthwal | Hostel No. 4 (Madhava Hostel) Management of duties of Group ‘D’ staff. Maintenance of C.L.,E.L. Records. |
| Hostel Section | Hostel No. 7 (Ashwini Hostel), First Floor, Gents Hostel. | Mr. Rajesh Rawat | Hostel No. 7 (Ashwini Hostel) Hostel No. 8 (Bharadwaj Hostel) |
| Hostel Section | Hostel No. 7 (Ashwini Hostel), First Floor, Gents Hostel. | Ms. Sunil Devi | Hostel No. 1 (Charak Hostel) Hostel No. 2 (Jivak Hostel)
Hostel No. 3 (Sushruta Hostel) Hostel No. 6 (Vagbhatta Hostel)
|
| Masjid Moth Hostel Office | Hostel No. 14 (Atreya Hostel), Room No. 002, Ground Floor. | Ms. Asha | Hostel No. 14 (Atreya Hostel) |
There are a total of twenty different halls of residence and dwellings that are regarded as hostel accommodation. Of these, thirteen are in the Ansari Nagar (East) campus and accommodates all undergraduates (except lady nursing students) and single postgraduates and resident doctors. These are the older hostels. These nine hostels for gentlemen have derived their names from the Ayurveda, and are a tribute to those who have laid the foundations for medicine and surgery, relevant even today. The four hostels for ladies are named after Goddesses, Laxmi, Parvati, Saraswati and Akshara. [However the hostels are invariably known as numbers]. There is no married accommodation in the Ansari Nagar (East) campus.
| S.No. | Hostel | Location | Category | Gender | Type of Room |
|---|---|---|---|---|---|
| 1. | Hostel No. 1 (Charak Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Single rooms |
| 2. | Hostel No. 2 (Jivak Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Single rooms |
| 3. | Hostel No. 3 (Sushruta Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Single rooms |
| 4. | Hostel No. 4 (Madhava Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Single rooms |
| 5. | Hostel No. 5 (Nagarjuna Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Single rooms |
| 6. | Hostel No. 6 (Vagbhatta Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Single rooms |
| 7. | Hostel No. 7 (Ashwini Hostel) | Gents Hostel Ansari Nagar (East) | Undergraduates | Gents | Double seater |
| 8. | Hostel No. 8 (Bharadwaj Hostel) | Gents Hostel Ansari Nagar (East) | Postgraduates | Gents | Single rooms |
| 9. | Hostel No. 9 (Parvati Hostel) | Ladies Hostel Ansari Nagar (East) | Undergraduates Postgraduates | Ladies | Single / Double seater |
| 10. | Hostel No. 10 (Saraswati Hostel) | Ladies Hostel Ansari Nagar (East) | Undergraduates | Ladies | Single rooms |
| 11. | Hostel No. 11 (Akshara Hostel) C2 Flats | Ladies Hostel Ansari Nagar (East) | Undergraduates | Ladies | Double / Triple seater |
| 12. | Hostel No. 12 (Dhanwantri Hostel) RPC I | Gents Hostel Ansari Nagar (East) | Postgraduates | Gents | Single rooms |
| 13. | Hostel No. 13 (Laxmi Hostel) RPC II | Ladies Hostel Ansari Nagar (East) | Undergraduates | Ladies | Single / Six seater |
| 14. | Hostel No. 14 (Atreya Hostel) | Masjid Moth Campus | Postgraduates | Ladies Single, Gents Single & Married | Single rooms & One Bed room set for married |
| 15. | Hostel No. 15 (Medha Hostel) | Masjid Moth Campus | Undergraduates Postgraduates | Ladies | Single / Double / Triple / Four seater |
| 16. | Hostel No. 16 (Agnivesa Hostel) | Masjid Moth Campus | Postgraduates | Gents Single & Married | Single rooms & One room set / One Bed room set for married |
| 17. | Hostel No. 17 (Ambuja Hostel) | Masjid Moth Campus | Postgraduates | Married | One Bed room set for married |
| 18. | Hostel No. 18 (Kashyap Hostel) | Masjid Moth Campus | Undergraduates Postgraduates | Gents | Single / Double / Triple seater |
| 19. | Hostel No. 19 (Patanjali Hostel) | Masjid Moth Campus | Postgraduates | Ladies | Single rooms / Double seater |
| 20. | JPNATC Hostel | Raj Nagar | Postgraduates | Gents Single & Married | Single rooms & One Bed room set for married |
These hostels have a total capacity of about 2700 seats approx. The majority of the accommodation is for a single student / resident / family. Attached toilets are only available in married accommodation and in JPNATC Hostel, Hostel No. 18 (Kashyap Hostel) and Hostel No. 19 (Patanjali Hostel). Otherwise toilets and bathrooms are shared.
FURNISHINGS
Most single rooms are modestly furnished with a cot, almirah, table, chair and bookshelf (in some hostels). The married accommodation is also furnished accordingly. All hostellers are advised to check the inventory while occupying and vacating the rooms.
The residential areas of All India Institute of Medical Sciences are spread over five campuses within a radius of around 3 kilometers, of which hostel accommodation is available in two.
| S.No. | Campus | Location and Accommodation |
|---|---|---|
| 1. | Ansari Nagar (East) | The main campus that houses the institution and hospitals, residential quarters and most of the hostels. |
| 2. | Ansari Nagar (West) | A smaller residential area just across and to the West of the hospital on Aurobindo Marg, adjacent to the Safdarjung Hospital. |
| 3. | Masjid Moth | A sister campus adjacent to the Ansari Nagar (East) less than a kilometer away has hostels and residential quarters. |
| 4. | Ayurvigyan Nagar | This campus is on the Khel Gaon Marg adjacent to the HUDCO Complex that houses the Ansal Plaza and has residential quarters and transit accommodation. |
| 5. | Asiad Village | On the Khel Gaon Marg, this has few houses for the Faculty only. There are no hostels in this campus. |
Transport department provides transportation facility to B.Sc & M.Sc Nursing female students to and from Masjid Moth & AIIMS campus. A subsidized fee is charged for this purpose. The transport Department should be contacted for details.
| FROM MASJID MOTH | FROM A.I.I.M.S. |
|---|---|
| 7.10 AM (Trauma Centre) from November 2023 Onwards | 12.30 PM (Trauma Centre) |
| 7.20 AM | 12.30 PM |
| 1.45 PM | 4.50 PM / 5.00 PM |
| On Saturday | |
| 7.20 AM | 1.00 PM |
| 8.30 AM | |
| A.I.I.M.S. TO BALLABHGARH | 7.30 am (Monday) 12.30 pm (Friday) [Return after one week] |
| BALLABHGARH TO A.I.I.M.S. | |
| A.I.I.M.S. TO DAYALPUR | 7.30 am (Monday to Friday) |
| DAYALPUR TO A.I.I.M.S. | 12.30 pm (Monday to Friday) |
| A.I.I.M.S. TO AMBEDKAR NAGAR | 9.30 am (Monday to Friday) |
| AMBEDKAR NAGAR TO A.I.I.M.S. | 12.30 pm (Monday to Friday) |
The present building of Centre for Dental Education and Research (CDER) is a continuation of erstwhile Department of Dental Surgery established in 1960 with single dental surgeon. The department saw significant progress from non-teaching to teaching and subsequently starting Post-graduation in Orthodontics and Dentofacial Orthopedics in 1984, Maxillofacial Prosthodontics in 1995, Conservative Dentistry and Endodontics in 2003 and Oral and Maxillofacial Surgery in 2005. The Governing Body of the Institute approved in principle establishment of post graduate dental specialty centre in 1999 and the foundation stone for this building was laid in May 2003. As on now this centre is one of the outstanding specialized centres of AIIMS and carries on the tradition of providing excellent patient care, post graduate education and research. The fifth specialty Pediatric and Preventive Dentistry post graduate courses started in year 2017 and it is envisaged to start post-graduation in several other subjects, PhD and fellowships in other branches of dentistry.
The CDER has been actively providing policy and program support to the Govt by advising and participating in various technical and scientific work of Govt of India. The erstwhile Department of Dental Surgery was named as nodal agency for implementation of pilot project on National Oral Health Care Program in the country in year 1999. Subsequently, the Centre developed the implementation strategies for National Oral Health Care Program and developed several demonstration programs and guidelines for oral disease prevention. The Centre also developed several IEC materials, manuals, educative film on Oral health and chapters for NCERT books on oral health awareness and disease prevention. The Centre also conducted several training programmes for dental surgeons, health workers, nurses, school teachers and NGOs on primary prevention of oral diseases and effective tobacco cessation counselling. The Centre has been involved in several projects of Ministry of Health and Family Welfare, Indian Council for Medical Research, Department of Science & Technology, Department of Biotechnology, CSIR and WHO. The Centre provides essential treatment at AIIMS outreach centres at Mid-town Rotary Hospital at Trilokpuri, and CRHSP, Ballabhgarh. The Centre was the Nodal agency for National Oral Health Care Programme (1999-2005).
The Centre was given the status of National Centre of Excellence for Implementation of National Oral Health Program in February 2014 and WHO CC for Oral Health Promotion in May 2014. The faculty from the Centre have been instrumental in development of operational guidelines for National Oral Health Program, Regional Oral Health Strategy, Draft National Oral Health Policy and guidelines for dental screening under Rashtriya Bal Swasthya Karyakram (RBSK).
As part of National Oral Health Program, CDER has also developed a web portal and app named EDantSeva for use as informative and educative electronic resource for public on oral health issues as well as data for dental. Professionals.
The faculty from the Centre is providing leadership role in various technical and professional organizations at key positions and are publishing a significant number of scientific articles in journals of repute.
Email: cmetaiims@gmail.com
Website Coordinator :
Dr. Rakesh Garg
Mobile: 9810394950
Email: drrgarg@hotmail.com
K.L. WIG CENTRE FOR MEDICAL EDUCATION & TECHNOLOGY
AIIMS, ANSARI NAGAR, NEW DELHI –110029, INDIA
Phone : 91-11- 26588500, 26588700 Ext. 3392, 3258
Fax : 91-11-26588641, 26588663
Email: cmetaiims@gmail.com
Office bearers:
| Name | Designation | Telephone | |
|---|---|---|---|
| Prof. Peush Sahni | Chief | 26592445 | |
| Dr Anurag Srivastav | Professor-In-Charge (Surgical Disciplines) | 26494560 Int. 4560 | dranuragsrivasta@gmail.com |
| Dr. A.K. Deorari | Professor-in-Charge (Faculty Development of Clinical Faculty of Medicine) | 26594998 | |
| Dr. K.K. Deepak | Professor-in-Charge (Basic Sciences) | 26593583 Int. 3583 | kkdeepak@gmail.com |
| Mr. Yogesh Kumar | Educational Media Generalist | Int. 3258, 3392 | yogesh.anju@gmail.com |
The unprecedented change in educational and information technology over the past decade has resulted in a situation where Faculty development is vital for keeping in touch with recent trends and launching innovations in the field of education. From its inception, KL Wig CMET has initiated a process of organizing workshops at the institutional, National and international levels. The areas addressed in these workshops are Assessment Strategies in medical education, The Role of Media in Education Problem-Based Learning, production of Learning Resource Materials and Computer Assisted Learning, Scientific Writing, 'How to make good slides?' and Multiple Choice Questions (MCQs) etc. AIIMS has popularized the use of MCQs and the Objective Structured Clinical Examination (OSCE) to assess theory and clinical skills, respectively, which have influenced the quality of training.
CMET workshops are collective efforts in which the in-house faculty members come together to organize the activities.
Globalization, free market courses, changing needs and expectations of society, and rapid technology change, besides the knowledge explosion, have driven Medical Education worldwide. The medical schools are striving for skill enhancement of their residents with inbuilt flexibility in terms of scope for self-directed learning. The availability and access to information technology have opened the window for adopting new education strategies. Capacity building of Residents has become the buzzword.
| S.No. | Name | Designation |
|---|---|---|
| 01 | Dr. Kalpana Luthra | Prof. & Chief, CMETi |
| 02 | Dr. Rakesh Garg | Officer-In-Charge, Store, CMETi |
| 03 | Mr. Devi Prasaad | Administrative officer |
| 04 | Mrs. Rita Luthra | Private Secretary |
| 05 | Mr. Sanjay Sharma | Sr. Photographer |
| 06 | Mr. Dinesh Kr. Santoshi | Sr. Photographer |
| 07 | Mrs. Sheeja Siyad | Data Entry operator Gd. A |
| 08 | Mr. Anil Kumar | Jr. Photographer |
| 09 | Mr. Rajesh Saini | Jr. Photographer |
| 10 | Mr. Vijay Kumar | Senior Administrative Assistant |
| 11 | Mr. Dinesh Sharma | Data Entry Operator ( On Contract) |
| 12 | Mrs. Mamta Paswan | Data Entry Operator ( On Contract) |
| 13 | Mr. Radhe Shyam | Office Attendant |
| 14 | Ms. Rekha Kumari | Hospital attendant |
| Name | Designation | Contact No. |
|---|---|---|
| Dr. Kalpana Luthra | Prof. & Chief, CMETi | 26594483/*8462/3258 |
| Dr. A. Shariff | Professor In-charge (For Faculty Development of Basic Sciences) | 26593660 |
| Dr. Rakesh Lodha | Professor In-charge (For Faculty Development & Medical Sciences) | 26594622 |
| Dr. Rashmi Ramachandran | Professor In-charge (For skill and simulation-based learning) | 26594022 |
| Dr. Ambuj Roy | Head, Set Facility | 26598252 |
| Dr. Rakesh Garg | Member | 26595107 |
| Dr. Tushar Aggarwal | Member | |
| Dr Anu Sachdeva | Member | 26597326 |
| Dr. Mohit Joshi | Member & Faculty Coordinator, Clinical Sciences | 26551819 |
| Dr. Uma Kanga | Member & Faculty Coordinator, Basic Sciences Immunogenetics | 26594638 |
AIIMS is responsible for developing teaching patterns in undergraduate and postgraduate medical education in all its branches to demonstrate a high standard of medical education to all medical colleges and other health professional institutions in India. Although the Institute has brought about significant changes in its curricula, the overall standard of Medical Education at a national level has remained static since 1947. Teachers in most medical colleges in India have remained uninfluenced by modern educational theories and advanced educational technology. Our health planners increasingly felt that urgent, competent and comprehensive action was needed to make medical education more relevant to our national needs. AIIMS has been exploring the possibility of establishing an inter-institutional link with the Centre for Medical Education at the University of Dundee in the United Kingdom for quite some time. A proposal was mooted 1977 to establish a Centre for Medical Education and Technology at AIIMS. However, it was in 1989 that the Government of India accorded formal approval to the tripartite agreement between AIIMS, Overseas Development Agencies (ODA), the United Kingdom and Govt. of New Zealand to set up a Centre with a view to elevate the standards of Medical and Health Personnel Education by improving the methods of teaching learning and rationalising the educational strategy. The Centre has been named after Prof. K.L. Wig, the second Director of AIIMS and a doyen of Medical Education.
Following a tripartite agreement between AIIMS and the UK and New Zealand governments, a faculty development program was organised for a core faculty and technical staff at the Dundee Institute of Educational Technology, United Kingdom. The Government of New Zealand provided the equipment for a fully fledged media production centre.
"To be a leader in medical education by fostering a culture of continuous learning, innovation and excellence and prepare a new generation of healthcare professionals who are clinically proficient, scientifically informed, and deeply committed to compassion, ethics, and patient-centred care."
Prof. K.L. Wig
"To be a leader in medical education by fostering a culture of continuous learning, innovation and excellence and prepare a new generation of healthcare professionals who are clinically proficient, scientifically informed, and deeply committed to compassion, ethics, and patient-centred care."
Prof. K.L. Wig
In medical photography, CMETi provides technical support to the AIIMS faculty, residents,and other health professionals. This department not only photographs the modern state-of-the-art videography but also edits work. The services of CMET are being used in the following areas, which are later used for educational purposes.
Poster designing and printing for conferences/workshops, etc.
| S.NO | Topic | Duration | Te DD | No. of Participants | Faculty Coordinator |
|---|---|---|---|---|---|
| 01 | Curriculum design and framing of objectives (For SRs) | Half Day (2.00-5.00 pm) | 08th March 2025 | 40 | Dr. Nasreen, Dr. Tony |
| 02 | Basic Course in Medical Education (For Faculty) | Three Full Days | 27-29thMarch 2025 | 40 | Dr. Rakesh Garg, Dr. Mohit Joshi |
| 03 | Microteaching Workshop Batch 1 (For SRs) | Half Day (2.00-5.00 pm) | 05thApril 2025 | 15 | Dr. Akshay Dr. Ritu Sehgal |
| 04 | First Aid in Common Emergencies (For undergraduate students) | Full Day | 12th April 2025 | 50 | Dr. Rakesh Garg |
| 05 | Basic Course in Medical Education (For SRs) | 2 days (One Saturday post lunch+ Sunday full day + following Saturday post-lunch One and Half Days (1 1/2 days) | April 13th (full day); 19th (2.00-5.00 pm)& 20th April (Full day) 2025 | 40 | Dr. Rakesh Garg, Dr. Mohit Joshi |
| 06 | Assessment in Medical Education (For Faculty) | Full Day | 01stMay 2025 | 25 | Dr Anu Sachdeva |
| 07 | Microteaching Workshop Batch 2 (For post SRs, Scientists interested in academic careers) | Half Day | 3rd May 2025 | 15 | Dr. Ritu Sehgal, Dr. Asmita Patil |
| 08 | Assessment in Medical Education (For Scientists and SRs) | Full Day | 8thMay 2025 | 25 | Dr Anu Sachdeva |
| 09 | First Aid in Common Emergencies (For undergraduate students) | Full Day | 31st May 2025 | 50 | Dr. Rakesh Garg |
| S.NO | Date | Target Group | Duration |
|---|---|---|---|
| 01 | 21.01.2025 | Residents Doctors | Full Day |
| 02 | 21.02.2025 | Nursing Officers | Half Day |
| 03 | 18.03.2025 | Resident Doctors | Full Day |
| 04 | 22.04.2025 | Nursing Officers | Half Day |
| 05 | 13.05.2025 | Resident Doctors | Full Day |
| 06 | 22.07.2025 | Nursing Officers | Half Day |
| S.No. | Past Workshops |
|---|---|
| 1 | Workshop for Undergraduate Students Workshop Title: First Aid in Common Emergencies Date: 06thAugust 2024 Faculty Coordinator: Dr Rakesh Garg |
| 2. | Basic Course in Medical Education for Faculty Date : 28-31 August 2024 Faculty Coordinator: Dr. Mohit Joshi |
| 3. | Curriculum Design & Framing of Objectives for Senior Residents Date: 05th October 2024 Faculty Coordinator: Dr. Mohit Joshi & Dr. Nasreen |
| 4. | Microteaching Workshop for Senior Residents Date: 19th October 2024 Faculty Coordinator: Dr. Mohit Joshi & Dr.Tony |
| 5. | How to frame MCQs Workshop for Senior Residents Date: 26th October 2024 Faculty Coordinator : Dr. Kalpana Luthra & Dr. Ritu Sehgal |
| S. No | Topic | Date | Coordinator |
|---|---|---|---|
| 01 | Information Retrieval in Health Sciences | 11/10/2024 | Dr. Rakesh Garg |
| 02 | Tool for scientific writing in health science | 18/10/2024 | Dr. Tony |
| 03 | Designing pamphletsand poster | 25/10/2024 | Dr. Abhishek Nagarjappa |
| 04 | Animation in PowerPoint | 01/11/2024 | Dr. Rishi Nayyar |
| 05 | Creativity | 08/11/2024 | Dr. Abhishek Nagarjappa |
| 06 | Information Retrieval in Health Science | 22/11/2024 | Dr Vivek Gupta |
| 07 | Tool for Scientific Writing in Health Science | 29/11/2024 | Dr. Suman Das |
| 08 | Media in Education | 06/12/2024 | Dr Karthikeyan |
The unprecedented change in educational and information technology over the past decade has resulted in a situation where Faculty development is vital for keeping in touch with recent trends and launching innovations in the field of education. From its inception, KL Wig CMET has initiated a process of organizing workshops at the institutional, National and international levels. The areas addressed in these workshops are Assessment Strategies in medical education, The Role of Media in Education Problem-Based Learning, production of Learning Resource Materials and Computer Assisted Learning, Scientific Writing, 'How to make good slides?' and Multiple Choice Questions (MCQs) etc. AIIMS has popularized the use of MCQs and the Objective Structured Clinical Examination (OSCE) to assess theory and clinical skills, respectively, which have influenced the quality of training.
CMET workshops are collective efforts in which the in-house faculty members come together to organize the activities.
Globalization, free market courses, changing needs and expectations of society, and rapid technology change, besides the knowledge explosion, have driven Medical Education worldwide. The medical schools are striving for skill enhancement of their residents with inbuilt flexibility in terms of scope for self-directed learning. The availability and access to information technology have opened the window for adopting new education strategies. Capacity building of Residents has become the buzzword.
Lt. Sh. Ganguly
Lt. Sh. M.L.Bhalla

Sh. M L Dhawan

Lt. Sh. M K Sharma

Lt. Sh. Asha Ram
Lt. Sh. B.D.Ghosh
Sh. A K Panjanani

Sh. Roshan Lal

Sh. K.C.Kapoor

Lt. Sh. Mohar Singh

Sh. S.C.Mehta

Sh. S C Sharma

Dr. B V Adkoli

Sh. Yogeshwar Nath

Sh. Yogesh Kumar
| S.No. | Name | Designation |
|---|---|---|
| 01 | Dr. Kalpana Luthra | Prof. & Chief, CMETi |
| 02 | Dr. Rakesh Garg | Officer-In-Charge, Store, CMETi |
| 03 | Mr. Devi Prasaad | Administrative officer |
| 04 | Mrs. Rita Luthra | Private Secretary |
| 05 | Mr. Sanjay Sharma | Sr. Photographer |
| 06 | Mr. Dinesh Kr. Santoshi | Sr. Photographer |
| 07 | Mrs. Sheeja Siyad | Data Entry operator Gd. A |
| 08 | Mr. Anil Kumar | Jr. Photographer |
| 09 | Mr. Rajesh Saini | Jr. Photographer |
| 10 | Mr. Vijay Kumar | Senior Administrative Assistant |
| 11 | Mr. Dinesh Sharma | Data Entry Operator ( On Contract) |
| 12 | Mrs. Mamta Paswan | Data Entry Operator ( On Contract) |
| 13 | Mr. Radhe Shyam | Office Attendant |
| 14 | Ms. Rekha Kumari | Hospital attendant |
Waiting List of students enrolled in various courses
| Year | Students Waiting List | |
| Senior Res. | Junior Res. | |
| 2013 | ( Non- Acad) January Session ( Non- Acad) July Session
| |
| 2014 | (Non Acad) Januaey Session | |
| Name | Designation | Contact No. |
|---|---|---|
| Dr. Kalpana Luthra | Prof. & Chief, CMETi | 26594483/*8462/3258 |
| Dr. A. Shariff | Professor In-charge (For Faculty Development of Basic Sciences) | 26593660 |
| Dr. Rakesh Lodha | Professor In-charge (For Faculty Development & Medical Sciences) | 26594622 |
| Dr. Rashmi Ramachandran | Professor In-charge (For skill and simulation-based learning) | 26594022 |
| Dr. Ambuj Roy | Head, Set Facility | 26598252 |
| Dr. Rakesh Garg | Member | 26595107 |
| Dr. Tushar Aggarwal | Member | |
| Dr Anu Sachdeva | Member | 26597326 |
| Dr. Mohit Joshi | Member & Faculty Coordinator, Clinical Sciences | 26551819 |
| Dr. Uma Kanga | Member & Faculty Coordinator, Basic Sciences Immunogenetics | 26594638 |
AIIMS is responsible for developing teaching patterns in undergraduate and postgraduate medical education in all its branches to demonstrate a high standard of medical education to all medical colleges and other health professional institutions in India. Although the Institute has brought about significant changes in its curricula, the overall standard of Medical Education at a national level has remained static since 1947. Teachers in most medical colleges in India have remained uninfluenced by modern educational theories and advanced educational technology. Our health planners increasingly felt that urgent, competent and comprehensive action was needed to make medical education more relevant to our national needs. AIIMS has been exploring the possibility of establishing an inter-institutional link with the Centre for Medical Education at the University of Dundee in the United Kingdom for quite some time. A proposal was mooted 1977 to establish a Centre for Medical Education and Technology at AIIMS. However, it was in 1989 that the Government of India accorded formal approval to the tripartite agreement between AIIMS, Overseas Development Agencies (ODA), the United Kingdom and Govt. of New Zealand to set up a Centre with a view to elevate the standards of Medical and Health Personnel Education by improving the methods of teaching learning and rationalising the educational strategy. The Centre has been named after Prof. K.L. Wig, the second Director of AIIMS and a doyen of Medical Education.
Following a tripartite agreement between AIIMS and the UK and New Zealand governments, a faculty development program was organised for a core faculty and technical staff at the Dundee Institute of Educational Technology, United Kingdom. The Government of New Zealand provided the equipment for a fully fledged media production centre.
"To be a leader in medical education by fostering a culture of continuous learning, innovation and excellence and prepare a new generation of healthcare professionals who are clinically proficient, scientifically informed, and deeply committed to compassion, ethics, and patient-centred care."
Prof. K.L. Wig
"To be a leader in medical education by fostering a culture of continuous learning, innovation and excellence and prepare a new generation of healthcare professionals who are clinically proficient, scientifically informed, and deeply committed to compassion, ethics, and patient-centred care."
Prof. K.L. Wig
जल्द आ रहा है
| Department | Name | AIIMS Email-Id | Alternate Email-Id |
|---|---|---|---|
| Director | Dr M. Srinivas | director[at]aiims[dot]gov[dot]in | - |
| Dean (Academic) | Dr. Kaushal kr. Verma | dean.acad[at]aiims[dot]gov[dot]in | - |
| Medical Superintendent | Dr. Nirupam Madaan | ms.main[at]aiims[dot]gov[dot]in | - |
| Additional Director (Administration) | Sh. Karan Singh | dd[at]aiims[dot]gov[dot]in | - |
| Dean (Research) | Dr. Nikhil Tandon | dean.research[at]aiims[dot]gov[dot]in | - |
| Prof. In Charge (Computer Facility) | Dr. Pooja Gupta | piccf[at]aiims[dot]gov[dot]in | - |
| Dean (Examinations) | Dr. | dean.exam[at]aiim[dot]gov[dot]in | - |
| Associate Dean (Academics) | Dr. Rakesh Lodha | associatedeanacad[at]aiims[dot]edu | - |
| Associate Dean (Research) | Dr. Vineet Ahuja | assodeanres[at]aiims[dot]gov[dot]in | researchsectionaiims[at]gmail[dot]com |
| Associate Dean (Examinations) | Dr. Naval K Vikram | assodean.exam[at]aiims[dot]gov[dot]in | - |
| Registrar | Dr. Girija Pd. Rath | registrar[at]aiims[dot]gov[dot]in | aiims.reg[at]gmail[dot]com |
| Asstt. Controller of Examinations | Sh. Manoj Kr. Singh | - | - |
अखिल भारतीय आयुर्विज्ञान संस्थान
अंसारी नगर, नई दिल्ली - 110029
बोर्ड संख्या : +91-11-26588500 / 26588700
फैक्स : +91-11-26588663 / 26588641
एम्स में महत्वपूर्ण ई -मेल पते
एम्स अस्पताल गाजियाबाद
Prof. Sandeep Chauhan, Chief, Cardio-Thoracic Sciences Centre
Prof. P. RAJASHEKAR Addl. Medical Superintendent
हृदय पक्ष केन्द्र के संस्थापक और प्रथम प्रमुख, प्रो. नागारूर गोपीनाथ का शोक पत्र
हृदय वक्ष विज्ञान केंद्र ने 1982 में नए भवन में कार्य शुरू किया। केंद्र में विशेष रूप से सभी हृदय रोगों के लिए व्यापक देखभाल के लिए आवश्यक सभी सहायक सुविधाओं के साथ कार्डियोलॉजी और हृदय शल्य चिकित्सा के लिए 200 बिस्तर उपलब्ध हैं। 1986 में केंद्र ने सरकार पूरी तरह से स्वतंत्र होने के बाद अपनी नई 7 मंजिला इमारत से पूरी तरह से कार्य करना आरंभ किया। हृदय वक्ष विज्ञान केंद्र में निम्नलिखित विभाग हैं।
प्रोफेसर एन गोपीनाथ हृदय वक्ष विज्ञान केंद्र के संस्थापक और पहले प्रमुख थे। उनके बाद क्रमश: प्रोफेसर एम. एल. भाटिया, प्रोफेसर आर टंडन, प्रोफेसर पी. वेणुगोपाल द्वारा पद ग्रहण किया गया था और वर्तमान में प्रोफेसर ए संपत कुमार कार्यरत हैं।
There are eight fully equipped operating rooms with the state-of-art technology to carry out all kinds of complex cardiothoracic and vascular procedures 24X7 through out the year accessible and affordable to everyone. Total bed capacity (136) under CTVS in General ward is distributed in 1st, 4th, 5th and 6thfloors of Cardiothoracic sciences center of which
| नाम | ई-मेल आईडी | पद |
|---|---|---|
| डॉ. ए.के. बिसोई | drakbisoi[at]gmail[dot]com | अपर प्रोफेसर |
| डॉ. वी. देवगुरू | vdeva[at]hotmail[dot]com | सहायक प्रोफेसर |
| डॉ.सचिन तलवार | sachintalwar[at]hotmail[dot]com, drsachintalwar[at]gmail[dot]com | सहायक प्रोफेसर |
| Dr. P. RAJASHEKAR | praja[at]aiims[dot]edu | Professor (CTVS) |
| डॉ. ए.के. बिसोई | drakbisoi[at]gmail[dot]com | अपर प्रोफेसर |
| Dr. MANOJ SAHU | drmanojsahu[at]gmail[dot]com | Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SARVESH PAL SINGH | sarveshpalsingh[at]gmail[dot]com | Additional Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. P.RAMESH MENON | rpmpgi[at]gmail[dot]com | Additional Professor Pediatrics (Neonatalogy) in CTVS |
| Dr. PRADEEP RAMAKRISHNAN | pradeep[dot]r[dot]reddy85[at]gmail[dot]com | Associate Professor (CTVS) |
| Dr. UMMED SINGH | drusd[at]yahoo[dot]com | Associate Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SUSHAMA GAYATRI B | sushama[dot]gayatri[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. NAVNITA KISKU | navnita[dot]kisku[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. AMITABH SATSANGI | indiactvs[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. MAYANK YADAV | drmayankctvs[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr.BHARATH.V | drbharathv[at]gmail[dot]com | Assistant Professor (CTVS) |
List of Faculty Members in the Department of Cardiology
| नाम | पद | ई-मेल आईडी |
|---|---|---|
| डॉ. नीति मखीजा | एसोसिएट प्रोफेसर | 9868398102 |
| डॉ संदीप चौहान | प्रोफेसर | 9868398101 |
| डॉ. पूनम मल्होत्रा | एसोसिएट प्रोफेसर | 9868398103 |
| डॉ. मिनाती चौधरी | एसोसिएट प्रोफेसर | 9868398104 |
| डॉ. एस. एन. दास | सहायक प्रोफेसर | 9868398105 |
| डॉ. पराग घारडे | सहायक प्रोफेसर | 9868398106 |
| Dr. Suruchi Hasija | Professor | 9868398107 |
| Dr. Arindam Choudhury | Professor | 9868398107 |
| नाम | पद |
|---|---|
| डॉ. रूमा रे | प्रोफेसर |
| Dr. Sudheer Kumar A | Professor |
| नाम | पद | संपर्क नं. / ई-मेल |
|---|---|---|
| डॉ प्रिया जगिया | सहायक प्रोफेसर | 9868398117 |
| डॉ. संजीव शर्मा | प्रोफेसर और विभागाध्यक्ष | - |
| Dr. Niraj N.Pandey | Asstt. Prof. | - |
| नाम | पद |
|---|---|
| डॉ. आर लक्ष्मी | सहायक प्रोफेसर |
| नाम | पद |
|---|---|
| डॉ. आरती विज (ओआरबीओ) | अपर प्रोफेसर |
| नाम | पद |
|---|---|
| डॉ. आरती विज | अपर प्रोफेसर |
| Dr. Mede Charan Raj | Asstt. Professor |
| नाम | पद |
|---|---|
| डॉ. चेतन पटेल | सहायक प्रोफेसर |
Prof. Sandeep Chauhan, Chief, Cardio-Thoracic Sciences Centre
Prof. P. RAJASHEKAR Addl. Medical Superintendent
हृदय पक्ष केन्द्र के संस्थापक और प्रथम प्रमुख, प्रो. नागारूर गोपीनाथ का शोक पत्र
हृदय वक्ष विज्ञान केंद्र ने 1982 में नए भवन में कार्य शुरू किया। केंद्र में विशेष रूप से सभी हृदय रोगों के लिए व्यापक देखभाल के लिए आवश्यक सभी सहायक सुविधाओं के साथ कार्डियोलॉजी और हृदय शल्य चिकित्सा के लिए 200 बिस्तर उपलब्ध हैं। 1986 में केंद्र ने सरकार पूरी तरह से स्वतंत्र होने के बाद अपनी नई 7 मंजिला इमारत से पूरी तरह से कार्य करना आरंभ किया। हृदय वक्ष विज्ञान केंद्र में निम्नलिखित विभाग हैं।
प्रोफेसर एन गोपीनाथ हृदय वक्ष विज्ञान केंद्र के संस्थापक और पहले प्रमुख थे। उनके बाद क्रमश: प्रोफेसर एम. एल. भाटिया, प्रोफेसर आर टंडन, प्रोफेसर पी. वेणुगोपाल द्वारा पद ग्रहण किया गया था और वर्तमान में प्रोफेसर ए संपत कुमार कार्यरत हैं।
There are eight fully equipped operating rooms with the state-of-art technology to carry out all kinds of complex cardiothoracic and vascular procedures 24X7 through out the year accessible and affordable to everyone. Total bed capacity (136) under CTVS in General ward is distributed in 1st, 4th, 5th and 6thfloors of Cardiothoracic sciences center of which
| नाम | ई-मेल आईडी | पद |
|---|---|---|
| डॉ. ए.के. बिसोई | drakbisoi[at]gmail[dot]com | अपर प्रोफेसर |
| डॉ. वी. देवगुरू | vdeva[at]hotmail[dot]com | सहायक प्रोफेसर |
| डॉ.सचिन तलवार | sachintalwar[at]hotmail[dot]com, drsachintalwar[at]gmail[dot]com | सहायक प्रोफेसर |
| Dr. P. RAJASHEKAR | praja[at]aiims[dot]edu | Professor (CTVS) |
| डॉ. ए.के. बिसोई | drakbisoi[at]gmail[dot]com | अपर प्रोफेसर |
| Dr. MANOJ SAHU | drmanojsahu[at]gmail[dot]com | Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SARVESH PAL SINGH | sarveshpalsingh[at]gmail[dot]com | Additional Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. P.RAMESH MENON | rpmpgi[at]gmail[dot]com | Additional Professor Pediatrics (Neonatalogy) in CTVS |
| Dr. PRADEEP RAMAKRISHNAN | pradeep[dot]r[dot]reddy85[at]gmail[dot]com | Associate Professor (CTVS) |
| Dr. UMMED SINGH | drusd[at]yahoo[dot]com | Associate Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SUSHAMA GAYATRI B | sushama[dot]gayatri[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. NAVNITA KISKU | navnita[dot]kisku[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. AMITABH SATSANGI | indiactvs[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. MAYANK YADAV | drmayankctvs[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr.BHARATH.V | drbharathv[at]gmail[dot]com | Assistant Professor (CTVS) |
List of Faculty Members in the Department of Cardiology
| नाम | पद | ई-मेल आईडी |
|---|---|---|
| डॉ. नीति मखीजा | एसोसिएट प्रोफेसर | 9868398102 |
| डॉ संदीप चौहान | प्रोफेसर | 9868398101 |
| डॉ. पूनम मल्होत्रा | एसोसिएट प्रोफेसर | 9868398103 |
| डॉ. मिनाती चौधरी | एसोसिएट प्रोफेसर | 9868398104 |
| डॉ. एस. एन. दास | सहायक प्रोफेसर | 9868398105 |
| डॉ. पराग घारडे | सहायक प्रोफेसर | 9868398106 |
| Dr. Suruchi Hasija | Professor | 9868398107 |
| Dr. Arindam Choudhury | Professor | 9868398107 |
| नाम | पद |
|---|---|
| डॉ. रूमा रे | प्रोफेसर |
| Dr. Sudheer Kumar A | Professor |
| नाम | पद | संपर्क नं. / ई-मेल |
|---|---|---|
| डॉ प्रिया जगिया | सहायक प्रोफेसर | 9868398117 |
| डॉ. संजीव शर्मा | प्रोफेसर और विभागाध्यक्ष | - |
| Dr. Niraj N.Pandey | Asstt. Prof. | - |
| नाम | पद |
|---|---|
| डॉ. आर लक्ष्मी | सहायक प्रोफेसर |
| नाम | पद |
|---|---|
| डॉ. आरती विज (ओआरबीओ) | अपर प्रोफेसर |
| नाम | पद |
|---|---|
| डॉ. आरती विज | अपर प्रोफेसर |
| Dr. Mede Charan Raj | Asstt. Professor |
| नाम | पद |
|---|---|
| डॉ. चेतन पटेल | सहायक प्रोफेसर |
Few selected recent publications
Few selected recent publications
There is a PhD program in Cardiac Biochemistry. Currently three students are pursuing PhD in the department
The department has collaboration with several clinical departments and involved in several MD/DM thesis work
The department is actively involved in research in the following areas:
Located at: Room No.11, CN center
Located at R.No.53, CN center
Testing done in the following areas:
The Department of Psychiatry had informal beginning in 1958, when Dr. Luvia Taylor Gregg, Honorary Consultant in Psychiatry, began formal teaching in psychiatry for the first batch of MBBS students. Dr Gregg planned to introduce 100 hours of teaching in psychiatry in MBBS curriculum. Prof KL Wig, the then Head, Department of Medicine (later Director, AIIMS) was instrumental in integrating teaching of psychiatry throughout the clinical posting in medicine, so that the exposure to psychiatry was spread to all the 3 years on weekly basis. DrVimlaVirmani, who later headed the Department of Neurology, also worked as clinical tutor in the initial years of the Department history.
Dr AS Mahal joined as Assistant Professor in 1962 and Dr D Satyanand as Professor and Head in Aug 1963. Regular MD Psychiatry programme in psychiatry, the first in the country was started in 1964 by DrSatyanand. During 1967-1968, Dr Erna Hoch, a Swiss psychiatrist, who had migrated to India, headed the Department as Honorary Professor and Head for about one and half year. She was followed by Dr JS Neki, who joined in Sept 1968 as Professor and Head.
The Department of Psychiatry had a number of firsts in India besides being a pioneer in establishing postgraduate training in psychiatry in general hospital setting. The department gave a stature to psychiatry as medical discipline in a medical institution in India. Another path braking contribution of the department of psychiatry was initiating rural mental health services, through the Indian Council of Medical Research funded mental health project at the Ballabgarh Community Centre in 1964. The department has also the credit of starting the first Child Guidance Clinic in Delhi in 1964 and De Addiction Centre in 1988 which got the status of the National Drug Dependence Treatment Centre (NDDTC) in 1988. NDDTC is also a WHO Collaborating Centre on Substance Abuse.
The Department of Psychiatry has been a pioneer in providing mental health services in a General Hospital Setting. The department runs regular out-patient and in-patient services and multiple Specialty clinics along with Community services, Consultation liaison services and Emergency psychiatric services. In addition to medical management, psychological treatments, modified electro convulsive therapy (MECT), rTMS, tDCS and biofeedback are routinely provided. During the year 2017-18, the department provided out-patient consultation services to a total of 17,204 new cases and 66,333 follow up cases. The department is at the forefront of medical education with courses for MBBS, B.Sc/M.Sc nursing, MD (Psychiatry) and PhD (Clinical Psychology). The department undertakes regular collaborative research with national and international agencies like World Health Organization (WHO), University of California, National Institute of Health Research (UK), ICMR, and organizes year round public educational events for awareness and promotion of mental health.
Currently primary mandate of the department is to develop highly trained manpower, curriculum and techniques for undergraduate and postgraduate medical education. Funded research on epidemiology of substance abuse along with general mental health morbidity has been the main focus. The postgraduates are trained through outpatient, inpatient, community based and family centred mental health care
The general facility of the AIIMS CCRF houses multiple molecular biology equipment. Major instruments which has been installed (till now) in General Facility are mentioned below
Details of Major services and equipment provided by General Facility at CCRF.

Ultra-Centrifuge
(Model:.Optima XPN-100, Beckman Coulter)

Polymerase Chain Rection machine
(Model:SureCycler 8800 Thermal Cycler; Agilent Technologies)

Polymerase Chain Rection machine
(Model: C1000 Touch Thermal Cycler; BioRad)

Multimode microplate Reader
(Model:Cytation1; Biotek)

Electroporation system
(Model:.Gene Pulser Xcell system; Biorad)
Gel Documentation System
(Model: G:Box-Chemi-XX9, Company, Syngene)

Multipurpose Centrifuge
Model: Sorvall ST4 Plus
Centrifuge, Thermo Scientific

Refrigerated-Centrifuges
(Model: Heraeus™ Fresco™ 17 Microcentrifuge; Thermo scientific)

Homogenizer
(Supplier:JSR)

Agarose gel electrophoresis set-up
(Supplier:Biorad)

Protein and Western Blot (semi-dry) Apparatus

ElISA washer and ELlSA reader
(Make: Biorad)

Lyophilizer ( Seltis)

Laminar Hood (M/s Haier)

MilliQ and RO water system

Oven and Incubator

The SET Facility is an example of the vision of the institute’s leadership for continuous innovation in the field of medical education.
The facility has a Dry Skill Lab equipped to impart several basic and advanced medical skills through in-house developed modules. It has a Wet Lab hosting cadaveric and other surgical skill development workshops in various surgical specialties. In addition, there are three modern studios with capability to link with over 50 medical institutions across India. The SET (Skills, e-Learning, Telemedicine) Facility is a state of art facility set uptoinnovate medical education using simulation-based skill learning and e-learning methods to improve current teaching at the institute. The SET facility is a shared facility for use by different departments to impart simulation-based skills for undergraduate and postgraduate students for better patient care in addition to the traditional training methods. The simulation-based skill learning of medical undergraduates, postgraduates and nursing staff helps them be better prepared when managing patients in wards and clinics. The facility has active involvement of faculty members from various clinical and non-clinical departments who develop the training modules and teaching content and impart hands-on teaching to the students. The skill lab provides a stress-free environment to learn skills. The other aspects of the facility are to develop e-learning modules and to impart education through Tele-education linkages with medical colleges and hospitals across India. The Facility also serves as the National Resource Centre (NRC) of the National Medical College Network (NMCN), a MOHFW in initiative for tele-education networking across India.

Director, AIIMS
Chairman, SET Management Committee

Dean (Academics)
Co-Chairman, SET Management Committee

Head, SET Facility

Prof-In-Charge E-Learning

Prof. In-Charge (Skill and Simulation)

Prof. In-Charge (Tele-medicine)
Email: aiims[dot]setfacility[at]gmail[dot]com

Mobile: 9810394950
drrgarg[at]hotmail[dot]com




The department organized “64th Annual National Conference of Indian Public Health Association (IPHA)” at AIIMS, New Delhi from February 28 to March 2, 2020 that was attended by more than 1100 national and international public health delegates.

Plantation drive was conducted in SDH, Ballabgarh and both the PHCs on June 5, 2022, as a part of the world environment day.
At NCI patients are managed by single window DMG mode. A group of experts from relevant departments attend DMG to discuss all cases and plan the course of treatment.

जैव सांख्यिकी में अल्पावधि प्रशिक्षण (छ: माह की अवधि तक) पाने वाले स्नातकोत्तर / सेवारत प्रायोजित प्रत्याशियों को 1000 रु. प्रति माह का शुल्क प्रदान किया जाता है।
विभाग में पीएच.डी कार्यक्रम जनवरी 1988 में आरंभ किया गया था। अब तक इस कार्यक्रम में तेरह छात्रों का प्रवेश किया गया है, जिसमें से दस को डॉक्टरेट की डिग्री प्रदान की गई।
पीएच.डी. के तहत प्रवेश के नियमों के बारे में कार्यक्रम
कम से कम 60% अंक के साथ जैव सांख्यिकी / सांख्यिकी में मास्टर डिग्री।
इस लिखित परीक्षा के बाद विभागीय मूल्यांकन किया जाएगा। इसे केवल दिल्ली में ही जनवरी और जुलाई में एक वर्ष में दो बार आयोजित किया जाएगा।
चयन की विधि :पीएचडी के लिए चयन पंजीकरण के रूप में निम्नानुसार दो चरण प्रदर्शन मूल्यांकन के माध्यम से किया जाएगा
लिखित परीक्षा में 90 मिनट की अवधि सहित 80 अंक होंगे। प्रश्न पत्र में बहु विकल्प प्रश्न (एमसीक्यू) और लघु उत्तर प्रश्न (एसएक्यू) होंगे जो जैव सांख्यिकी पर आधारित होंगे।
जो प्रत्याशी लिखित परीक्षा (चरण-1) में कम से कम 50 प्रतिशत अंक प्राप्त करते हैं उन्हें विभागीय आकलन के लिए बुलाया जाएगा (20 अंक सहित)।
पीएच. डी. पाठ्यक्रम में प्रवेश मान्यता प्राप्त निधिकरण एजेंसियों से मिलने वाली अनुसंधान निधि / अध्येतावृत्ति / अनुदान की उपलब्धता के अधीन या जैव सांख्यिकी विभाग, एम्स में अनुसंधान परियोजनाओं की उपलब्धता के अधीन होगी। पीएच. डी पाठ्यक्रम के लिए संस्थान में कोई अध्येतावृत्ति नहीं है।
3-5 वर्ष
Field of Research: Immunology of Autoimmune and Inflammatory (Cardiovascular and skin) diseases
Publications: Refer to below Pubmed link:
https://pubmed.ncbi.nlm.nih.gov/?term=tembhre+m+k&sort=date
Current Work: Research is focused on skin diseases (e.g. Vitiligo, Psoriasis, Pemphigus, Alopecia areata, allergy etc.) and Cardiovascular diseases (e.g. Cardiomyopathy, Rheumatoid Heart Diseases, Heart Failure, CHD, CAD etc. with main focus on understanding the cardiac homeostasis) using various in vivo (Human subjects and animal models) and in vitro studies. Understanding the fundamentals of cell death (Apoptosis, Necroptosis) pathways, autophagy, mitochondrial dynamics, Immune regulations via T cells (Tregs & Th17 cells), macrophages, Neutrophil extracellular trap formation and alarmins in driving cardiovascular and skin homeostasis are key aspects of research in our lab. Lab is also having research collaborations in multidisciplinary areas (neurological disorders, Tumor Immunobiology, Human Microbiota etc.) and is open for collaboration in similar or diverse fields. Lab encouraged the highly motivated student to join the PhD programme of the department. Department is having Research facilities like qPCR (BioRad), Western Blot platform (BioRad), Flow Cytometer (BD-Lyrics), HPLC and other equipments.
Lab members:
PhD students:
Ms. Shipra (UGC-JRF)-2020
Ms. Priyanka Solanki (DBT-JRF)-2022
Project Research Fellow
Mr. Ritesh Raj (ICMR-Senior Research Fellow, PhD (Amity University))-2021

Email ID : manojkt143[at]gmail[dot]com
manoj_kt143[at]yahoo[dot]com
manojkt143[at]aiims[dot]edu
Mobile:+918800502994
Telephone -011-26594201

Email ID : ransijob[at]gmail[dot]com
Mobile:+919911716130
Telephone - 011-26594426
Publications: Refer to below pubmed link https://www.ncbi.nlm.nih.gov/myncbi/ransi.abraham.1/bibliography/public/
विभाग के प्रमुख फोकस में प्रोटीन अणुओं की त्रि-आयामी संरचना निर्धारण, संरचना-कार्य संबंध स्थापित करने के लिए, उनकी जैविक भूमिकाओं में विस्तृत अंतर्दृष्टि प्राप्त करने के लिए और तर्कसंगत संरचना-आधारित दृष्टिकोण का उपयोग करके नई दवा अणुओं को डिजाइन करने के लक्ष्य के रूप में प्रासंगिक प्रोटीन संरचनाओं का उपयोग करना शामिल है। हमारी प्रयोगशालाओं में, आणविक जीव विज्ञान तकनीकों का उपयोग करते हुए, नए प्रोटीन को प्रोटीन रसायन विज्ञान के उपकरणों का उपयोग करके प्राकृतिक स्रोतों से अलग किया जाता है और साथ ही उन्हें अधिक परिणाम देने हेतु उत्पादित किया जाता है।
संरचनाएं एक्स-रे क्रिस्टलोग्राफिक विधियों का उपयोग करके परमाणु विवरण पर निर्धारित की जाती हैं। सफल संरचना निर्धारण के बाद, नए प्रोटीन सिलवटों को प्रकट करने और कार्यात्मक तंत्र स्थापित करने के लिए संरचनाओं का बड़े विवरण में विश्लेषण किया जाता है। प्रोटीन की गतिशीलता और तह में अंतर्दृष्टि की भी व्याख्या की गई है।
विभाग प्रोटिओमिक्स के तरीकों का उपयोग करके नए प्रोटीन की पहचान और लक्षण वर्णन में भी शामिल है। बाध्यकारी अध्ययनों का उपयोग करते हुए, प्रिसाईस-लिगैंड इंटरैक्शन किया जाता है। नए संरचनात्मक रूप से विशिष्ट पेप्टाइड्स का डिज़ाइन तैयार किया जाता है और फिर मैनुअल और स्वचालित दोनों तरीकों का उपयोग करके संश्लेषित किया जाता है।

ashutosh[dot]bansal0408[at]gmail[dot]com

UGC-JRF
shipra9goel[at]gmail[dot]com

DBT-JRF
priyankasolanki367[at]gmail[dot]com

Professor In-charge
lakshmy_ram[at]yahoo[dot]com
Contact no. 26594659
Expertise/Research interests
Pubmed link for publications in the last five years: https://pubmed.ncbi.nlm.nih.gov/?term=ramakrishnan%20Lakshmy&filter=datesearch.y_5&sort=date
The department of cardiac biochemistry under the Cardiothoracic center (CTC) caters to the inpatients and outpatients of Cardiology and CTVS. In addition to patient care services the department is active in research in the area of developmental origin of adult chronic diseases, telomere biology, endothelial progenitor cells and trans fatty acids.
The department under one roof does testing in the areas of clinical chemistry, hematology, coagulation, hormones, cardiac drugs, lipids, catecholamine, marker of heart transplant evaluation, markers of inflammation and in addition assessment of novel risk factors for CAD like homocysteine, lipoprotein(a), apolipoproteins A1 and B. The department has excellent infrastructure and most of the investigations are carried out on automated instruments. Facilities for doing genetic analysis are also available. On an average 250 patients samples are analyzed in the lab every day.
The cardiac biochemistry lab is externally validated through quality assessment scheme (UKNEQAS) accredited to BIRMINGHAM, UK and RIQAS (Randox external quality assessment scheme) and has shown a consistently good performance.
Following facilities are available in the department:
| S.No | Facilities | Address | Telephone |
|---|---|---|---|
| 1 | X-Ray (Portable & OPD services) | Room no. 35 Ground floor CNC | 011-26593552 |
| 2 | Ultrasound | Room no.34 Ground floor CNC | . 011-26546539 |
| 3 | Dual energy 384 slice CT Scanner | Room no. 56 Ground floor CNC | 011-26593311 |
| 4 | MRI Scan | NMR Building | Ext. 3346, 4133 |
| 5 | Fluoroscopy | Room no. 29 Ground floor CNC | 01126593331 |
| 6 | DSA Lab | Cath lab 5 Ground floor CNC | 01126593270 |
| 7. | ABI Machine | Room no. 29 Ground floor CNC | 01126593331 |
The department was established in 1985 to develop a comprehensive program in Cardiovascular Imaging and Endovascular Interventions with clinical, educational and research components. The department has since evolved from basic radiographic and cardiac angiographic examinations to all types of current, state-of-the-art cardiovascular imaging and endovascular interventions. The department currently caters to clinical requirements of the entire CT Centre and other allied departments at AIIMS as well as conducts:

Professor
Workshop on "Practical Implications of Haemodynamic Monitoring
Teaching Programmes for the period January 2009 is as
| Annual Workshop on ECMO | Organized in YEAR 2012,2013,2014 |
| MSc Perfusion course started | From 2005 |
| Workshop on perioperative evaluation by TEE | Organized in Nov 9th & 10 th 2013 |
Woman Of the year 2000” by American Biographical Institute, USA.
T.N.Jha Award by Indian Society of Anaesthesia.
21st Century Award for the contribution in Medicine and Spirituality by International Biographical Institute.
Best paper Award in 2003 in International Paediatric Anaesthesia Conference.
Best Free paper award 2004, Cochin IACTA.
Best poster award 2006 ISA, Delhi.
Poster awarded for Best Free Paper 2007 IACTA.
Dr. Kop’s Award 1998.
Dr. Kop’s Award 2002.
Dr. Kop’s Award 2003.
Dr. Kop’s Award 2005.
ISACON Award 2003 & 2005.
Free paper Award IACTA 2007.
| Prof. Usha Kiran, Prof. & HOD | -Fellow of Indian College of Anaesthesia 2012. - Fellow IACTA in 2011. - Life time achievement award in preventive cardiology by Hon’ble President of India – 2008. - Rastriya Gaurav Award 0 2007 |
| Prof Sandeep Chauhan | Fellow IACTA |
| Prof. Neeti Makhija |
|
| Dr. Sambhunath Das |
|
| Dr. Arindam Choudhury | Best paper award in Echocardiography workshop at PGIMCR, chandigarh-2013. |
| Dr Suruchi Hashija | First prize in VA Punoose Award in Delhi & NCR branch of cardiac anaesthesia conference August-2014 |
| S. No. | Name | Designation |
|---|---|---|
| 1. | Dr. S. V. S. Deo (1991) | Senior Resident |
| 2. | Dr. Sumeet Goyal | Senior Resident |
| 3. | Dr. Kislay Kumar Thakur | Senior Resident |
| 4. | Dr. Rajesh Nanda | Senior Resident |
| 5. | Dr. Shantivardhan | Senior Resident |
| 6. | Dr. Arun Goel | Senior Resident |
| 7. | Dr. V Seenu | Senior Resident |
| 8. | Dr. Deepak Routray | Senior Resident |
| 9. | Dr. Rajesh Srivastava | Senior Resident |
| 10. | Dr. J Kishore | Senior Resident |
| 11. | Dr. Murali babu | Senior Resident |
| 12. | Dr. Niranjan | Senior Resident |
| 13. | Dr. Dinesh Kadam | Senior Resident |
| 14. | Dr. Rashmi | Senior Resident |
| 15. | Dr. Madhabanand Kar | Senior Resident |
| 16. | Dr. G. Srinivas | Senior Resident |
| 17. | Dr. Sonal Asthana | Senior Resident |
| 18. | Dr. D Sridhar | Senior Resident |
| 19. | Dr. Diganta K das | Senior Resident |
| 20. | Dr. Joydeep Purkayastha | Senior Resident |
| 21. | Dr. Sunil Kumar | Senior Resident |
| 22. | Dr. Rajiv Saran | Senior Resident |
| 23. | Dr Mittal | Senior Resident |
| 24. | Dr Neeraj Saxena | Senior Resident |
| 25. | Dr Charak | Senior Resident |
| 26. | Dr. Atul Samaiya | Senior Resident |
| 27. | Dr. Sidharth Hazarika | Senior Resident |
| 28. | Dr. Ajay Saha | Senior Resident |
| 29. | Dr. M. Om Prakask | Senior Resident |
| 30. | Dr. Gaurav Jain | Senior Resident |
| 31. | Dr. Majid | Senior Resident |
| 32. | Dr. Prashant Khullar | Senior Resident |
| 33. | Dr. Rajive | Senior Resident |
| 34. | Dr. Manish Verma | Senior Resident |
| 35. | Dr. Archit Pandit | Senior Resident |
| 36. | Dr. Mandeep Singh | Senior Resident |
| 37. | Dr. Hemant Goyal | Senior Resident |
| 38. | Dr. Deepak Jha | Senior Resident |
| 39. | Dr. Jeevan Ram | Senior Resident |
| 40. | Dr. Jitender | Senior Resident |
| 41. | Dr. Ashwin Kalayanpur | Senior Resident |
| 42. | Dr. Balasubramaniam | Senior Resident |
| 43. | Dr. Amrita | Senior Resident |
| 44. | Dr. Shubham | Senior Resident |
| 45. | Dr. Subi | Senior Resident |
| 46. | Dr. Debashish | Senior Resident |
| 47. | Dr. Shubham Garg | Senior Resident |
| 48. | Dr. Vaitheeswaran | Senior Resident |
| 49. | Dr. Amruta Nikhil Beke | Senior Resident |
| 50. | Dr. Mamraj Gupta | Senior Resident |
| 51. | Dr. Rakesh Sakiya | Senior Resident |
| 52. | Dr. Tapan Singh Chouhan | Senior Resident |
| 53. | Dr. Shivam Vatsal | Senior Resident |
| 54. | Dr. Dharma Kumar K G | Senior Resident |
| 55. | Dr. Subrat Kumar | Senior Resident |
| 56. | Dr. Anjay Kumar | Senior Resident |
| 57. | Dr. Murali A | Senior Resident |
| 58. | Dr. Sarees Kumar MK | Senior Resident |
| 59. | Dr. Praveen Yadav | Senior Resident |
| 60. | Dr. Jitendra Kumar Nangal | Senior Resident |
| 61. | Dr. Majid Ahmed Talikoti | Senior Resident |
| 62. | Dr. Ramesh | Senior Resident |
| 63. | Dr. Niju Pegu | Senior Resident |
| 64. | Dr. Aravind S Kapali | Senior Resident |
| 65. | Dr. Ankit Dhiman | Senior Resident |
| 66. | Dr. Tejas Prakash Vispute | Senior Resident |
| 67. | Dr. Amar Prem | Senior Resident |
| 68. | Dr. Bhupendra Saini | Senior Resident |
| 69. | Dr. Nishant | Senior Resident |
| 70. | Dr. Neha Mishra | Senior Resident |
| 71. | Dr. Durgesh Wankhede | Senior Resident |
| 74. | Dr. Arvind Kumar Koslia | Senior Resident |
| 75. | Dr. Vineet Goel | Senior Resident |
| 76. | Dr. Rajeev Sharma | Senior Resident |
| 77. | Dr. Kumar S S | Senior Resident |
| 78. | Dr. B Ravindra Babu | Senior Resident |
| 79. | Dr. Vivek Gupta | Senior Resident |
| 80. | Dr. Amit Attam | Senior Resident |
| 81. | Dr. Saurabh Kalia | Senior Resident |
| 82. | Dr. Saarat Chandra Pingali | Senior Resident |
| 83. | Dr. Prashant Khullar | Senior Resident |
| 84. | Dr. Om Prakash M | Senior Resident |
| 85. | Dr. Neha Mishra | Senior Resident |
| 86. | Dr. Durgesh Wankhede (NCI) | Senior Resident |
| 87. | Dr. Arvind Kumar Koslia | Senior Resident |
| 88. | Dr. Rahul Saini | Senior Resident |
| 90. | Dr. Dinesh Mohan | Senior Resident |
| 92. | Dr. Saurabh Singh (NCI) | Senior Resident |
| 93. | Dr. Akotkar Shravika Suresh | Senior Resident |
| S. No. | Name | Designation | D.O.J. | D.O. Completion | Email ID |
|---|---|---|---|---|---|
| 1. | Dr. Dillip Kumar Muduly | Senior Resident (Academic) | 04.07.12 | 03.07.15 | dillipmuduly@gmail.com |
| 2. | Dr. Manjunath NML | Senior Resident (Academic) | 20.07.12 | 19.07.15 | nmlmanjunath@gmail.com |
| 3. | Dr. R M Palaniappan | Senior Resident (Academic) | 02.01.13 | 02.01.16 | fruitfather@gmail.com |
| 4. | Dr. Ashish Jakhetiya | Senior Resident (Academic) | 03.01.13 | 02.01.16 | jakashish@gmail.com |
| 5. | Dr. Pankaj Kumar Garg | Senior Resident (Academic) | 30.01.13 | 31.01.16 | dr.pankajgarg@gmail.com |
| 6. | Dr. Paras Khanna | Senior Resident (Academic) | 01.07.13 | 30.06.16 | paraskhanna@gmail.com |
| 7. | Dr. Jyoti Sharma | Senior Resident (Academic) | 01.07.13 | 30.06.16 | drjyoti27@yahoo.co.in |
| 8. | Dr. Mahesh Sultania | Senior Resident (Academic) | 01.01.14 | 31.12.16 | drmaheshsultania@gmail.com |
| 9. | Dr. Mahendra Pal Singh | Senior Resident (Academic) | 01.01.14 | 31.12.16 | drmahi_cool@yahoo.com |
| 10. | Dr. Sandeep K Boriwal | Senior Resident (Academic) | 01.01.14 | 31.12.16 | drsandeepbhoriwal@gmail.com |
| 11. | Dr. Vinaya Kumar JR | Senior Resident (Academic) | 01.07.14 | 30.06.17 | jrvk85@gmail.com |
| 12. | Dr. Mokkapati Praveen Royal | Senior Resident (Academic) | 01.07.14 | 30.06.17 | mpraveenroyal@gmail.com |
| 13. | Dr. Bharat Bhushan Khurse | Senior Resident (Academic) | 01.01.15 | 31.12.17 | dr.bharatbhushankhurse@gmail.com |
| 14. | Dr. Raj Mohan | Senior Resident (Academic) | 01.01.15 | 31.12.17 | drrajmohan_2005@yahoo.co.in |
| 15. | Dr. Seema Singh | Senior Resident (Academic) | 01.01.15 | 29.06.18 | seemasingh5jan@gmail.com |
| 16. | Dr. Ashutosh Mishra | Senior Resident (Academic) | 01.07.15 | 30.06.18 | drashutoshmishra11@gmail.com |
| 17. | Dr. P. Naveen | Senior Resident (Academic) | 13.07.15 | 12.07.18 | drnaveenp.in@gmail.com |
| 18. | Dr. Parmesh S | Senior Resident (Academic) | 01.01.16 | 31.12.18 | sparroww6@gmail.com |
| 19. | Dr. Manoj Gowda S | Senior Resident (Academic) | 01.01.16 | 31.12.18 | drmanojsg@gmail.com |
| 20. | Dr. Rashpal Singh | Senior Resident (Academic) | 14.07.16 | 13.07.19 | rashpalcallingrashpal@gmail.com |
| 21. | Dr. Babul Bansal | Senior Resident (Academic) | 02.07.16 | 01.07.19 | babulbansal@yahoo.com |
| 22. | Dr. Naveen Kumar | Senior Resident (Academic) | 01.07.16 | 30.06.19 | dr.naveenms@gmail.com |
| 23. | Dr. Prakash Bhagat | Senior Resident (Academic) | 09.01.17 | 08.01.20 | prakashbhagat@hotmail.com |
| 24. | Dr. Areendam Barua | Senior Resident (Academic) | 08.02.17 | 07.02.20 | drareendam@gmail.com |
| 25. | Dr. Navin Kumar | Senior Resident (Academic) | 01.07.17 | 30.06.20 | navin2k1@gmail.com |
| 26. | Dr. Raghuram K | Senior Resident (Academic) | 01.07.17 | 30.06.20 | dr_raghummc@yahoo.co.in |
| 27. | Dr. Sudhakar G | Senior Resident (Academic) | 01.01.18 | 31.12.20 | sudhakar2k4@gmail.com |
| 28. | Dr. Prashant Gupta | Senior Resident (Academic) | 04.01.18 | 03.01.21 | drprashant42@gmail.com |
| 29. | Dr. Amitabha Mandal | Senior Resident (Academic) | 02.07.18 | 01.07.21 | amitabha.doc@gmail.com |
| 30. | Dr. Pallabika Mandal | Senior Resident (Academic) | 02.07.18 | 01.07.21 | pallabika86@gmail.com |
| 31. | Dr. Kunal Dhall | Senior Resident (Academic) | 02.07.18 | 01.07.21 | kunaldhall@gmail.com |
| 32. | Dr. Manish Gaur | Senior Resident (Academic) | 02.01.19 | 01.01.22 | manish.gr1@gmail.com |
| 33. | Dr. Sourabh Nandi | Senior Resident (Academic) | 01.01.19 | 31.12.21 | saurav337@gmail.com |
| 34. | Dr. Premanand N | Senior Resident (Academic) | 28.01.19 | 30.06.22 | dr.premanandmmc1989@gmail.com |
| 35. | Ajit Singh Oberoi | Senior Resident (Academic) | 01.07.19 | 30.06.22 | ajitaiimsz@gmail.com |
| 36. | Dr. Jaya Kumar P | Senior Resident (Academic) | 11.07.19 | 10.07.22 | jk151986@gmail.com |
Department of Surgical Oncology is active at several national and international forums and has conducted numerous conferences and cadaveric workshops. In last few years, the department has conducted several events, a few worth mentioning being







| 1 | Pattern of care and survival studies in breast, head &neck and cervical cancer. |
| 2 | Evaluation of Diffusion Weighted Magnetic Resonance Imaging for assessment of response to Neo Adjuvant Chemotherapy in advanced Squamous cell carcinoma of oral cavity |
| 3 | Role of Fibrin sealant in Ilio Inguinal Block Dissection to reduce the rate of lymphatic drainage and seroma formation, thereby morbidity |
| 4 | Role of Fibrin sealant in Ilio Inguinal Block Dissection to reduce the rate of lymphatic drainage and seroma formation, thereby morbidity |
| 5 | A randomized controlled trial comparing single dose versus three doses of antibiotic prophylaxis in surgical oncology patients with clean wounds. |
| 6 | Role of PET– CT Scan ( Positron Emission Tomography and CT Scan ) in the Staging of Locally Advanced / Recurrent Breast Cancer as a Single modality in Comparison to Multiple Organ Directed Conventional Investigations (C.I) A prospective Study. |
| 7 | Low cost, low dose, oral, neoadjuvant chemotherapy protocol in locally advanced borderline oral cancers - Feasibility study. |
| 8 | Analysis of a computerized prospective database of patients with uncommon sites of oral cancer presenting to IRCH, AIIMS. |
| 9 | Analysis of a prospective computerized database of colon cancer patients presenting to IRCH-AIIMS. |
| 10 | Prospective analysis the role of Positron emission tomography in preoperative evaluation of resectable soft tissue sarcoma and correlation with histo-pathological grading |
| 11 | Analysis of a prospective computerized database of esophageal cancer patients presenting to IRCH-AIIMS. |
| 12 | Clinical profiles and patterns of palliative surgery in cancer patients: An ambispective Study. |
| 13 | Analysis of a prospective computerized database of Gastric cancer patients presenting to IRCH-AIIMS. |
| 14 | A prospective study of Assessment of Breast anthropometry in Indian breast cancer patients. |
| 15 | Peri operative morbidity after complete cytoreduction and HIPEC |
| 16 | River Flow’ Incision for decreasing morbidity of Ilio-Inguinal Dissection |
| 17 | Pre-operative short course radiotherapy Vs NACT- long term radiotherapy in the management of locally advanced rectal cancer |
| 18 | Analysis of a computerized prospective database of patients with early breast cancer. |
| 19 | A prospective study evaluating incidence of DVT in patients undergoing surgery for thoracic and abdomino-pelvic malignancies. |
| 20 | Review of clinic-pathological, epidemiological, imaging accuracy, treatment outcomes and prognostic factors of operable pulmonary metastases in Department of Surgical Oncology, IRCH, AIIMS. |
| 21 | Role of PET– CT Scan ( Positron Emission Tomography and CT Scan ) in the Staging of Locally Advanced / Recurrent Breast Cancer as a Single modality in Comparison to Multiple Organ Directed Conventional Investigations (C.I) |
| 22 | Retrospective Analysis of A prospective computerized data base of patients with Early Tongue cancer. |
| 23 | Analysis of a Prospective computerized clinical database of Soft Tissue Sarcomas |
| 24 | A Prospective Study evaluating role of Ultrasound and Ultrasound guided FNAC in the assessment of cervical node metastasis in Oral Cancer |
| 25 | Molecular profiling (BRAF and K-RAS gene mutation) in differentiated thyroid cancer (DTC) in Indian patients operated at BRA IRCH AIIMS . |
| 26 | A prospective and Retrospective study of complex Breast conservation therapy. |
| 27 | A prospective study to validate the role of Integrated Positron Emission Tomography-Computed Tomography and Endobronchial Ultrasound and guided Transbronchial needle aspiration in the mediastinal staging of resectable Non small cell lung cancer |
| 28 | Standardizing Surgico-pathological evaluation of oral squamous cell carcinomas specimens - A prospective study |
| 29 | A prospective study to validate the role of PET CT and EBUS in the staging of resectable Non Small Cell Lung Cancer” |
| 30 | Efficacy of Neoadjuvant chemotherapy in carcinoma esophagus- A pilot study comparing Cisplatin+5-FU with Paclitaxel + Carboplatin |
| 31 | A prospective randomized control trial comparing intracostal with pericostal throractomy closure to evaluate post thoracotmy pain syndromes |
| 32 | Complex breast conservation therapy for breast cancer patient selection criteria clinical profile and outcomes |
| 33 | Patterns of care and survival studies on cancer in childhood, lymphoid and hematopoietic malignancies, other gynecological malignancies |
| 34 | Immuno-phenotypic profile of tumor infiltrating cells of the immune system & expression of PDL1 in triple negative/Her-2 neu positive breast cancer patients and their correlation with response to neoadjuvant chemotherapy |
| 35 | Comparative Sphingolipid profiling of breast cancer cell and tissue types for identification of Potential Metastatic Biomarkers |
| 36 | Development of Standard Operating Procedures (SOP) of Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in peritoneal surface malignancies for Government set up in India. |
| 37 | Clinical significance of cell-free DNA in intraoperative pleural lavage fluid and plasma in patients with non-small cell lung cancer (NSCLC): A pilot study |
| 38 | Role of T-regulatory cells (Tregs) and their clinical correlation in epithelial ovarian cancer. |
| 39 | Evaluation of peritoneal cancer index (PCI) in primary advanced ovarian epithelial carcinoma amongst Indian population. |
| 40 | A prospective observational study comparing CT scan vs PET CT scan in carcinoma ovary for determining the pre-operative disease burden and resectability |
| 41 | Efficacy of Neoadjuvant chemotherapy protocol in locally advanced, carcinoma oral cavity- A randomized, pilot study comparing Cisplatin+5-FU with Paclitaxel + Carboplatin |
| 42 | A study of young colorectal cancer patients - Clinical profile, treatment and relapse patterns, learning basic laboratory techniques of molecular biology for miRNA extraction in colon cancer patients. |
| 43 | Clinical Utility of cell-free DNA in intraoperative pleural lavage fluid and plasma for patients with resectable primary pulmonary malignancies – A pilot study |
| 44 | Awareness and Knowledge of Indian Breast Cancer patients pertaining to genetic aspect of Breast cancer |
| 45 | Prospective study to evaluate the accuracy of axillary staging using Ultrasound guided FNAC in early breast cancer |
| 46 | Comparison of pulmonary metastasis detected with PET-CT vs NCCT chest with surgical pathology |
| 47 | Evaluation of Indocyanine green dye-based navigation surgery in optimizing axillary management of carcinoma breast. |
| 48 | Learning Basic Lab Techniques and Analysis of Colorectal cancer data base. |
| 49 | Prevalence of sarcopenia in patients with upper gastrointestinal and lung malignancy undergoing surgical resection and its impact on immediate postoperative outcomes: A prospective observational study |
| 50 | Patterns of Care and Survival Studies on Gall Bladder Cancer under ICMR- National Cancer Registry Programme (NCRP) |
| 51 | Validation of role of PET-CT and Diagnostic Laparoscopy in the gall bladder cancer patients – A prospective study. |
| 52 | Feasibility study of dual technique- blue dye and fluorescence imaging for detection of sentinel node in oral cavity cancer – a prospective validation study |
| 53 | Prospective assessment of quality indicators of perioperative outcomes in major oncological surgeries at a high-volume tertiary care center |
| 54 | A prospective comparative study between HIPEC and EPIC and a Retrospective analytic survey of HIPEC patients. |
| 55 | SURAKHA – Breast Cancer Genetic awareness and risk Assessment |
| 56 | Predicting the response to neo-adjuvant chemotherapy by analysis of exome and transcriptome in squamous cell carcinoma of esophagus |
| 57 | Breast and Ovarian cancer awareness |
| 58 | Role of heavy metals As etiology for carcinoma of the gallbladder |
| 59 | Hospital Based Cancer Registry at National Cancer Institute (NCI)-AIIMS |
| 60 | Functional recovery and Return to work after Thoracic surgery in patients with Malignant thoracic Diseases: A Prospective study |
| 61 | A pilot study to assess role of preoperative chemoradiotherapy in locally advanced / recurrent extremity soft tissue sarcoma & audit of soft tissue sarcoma database. |
| 62 | Prospective study of in person versus online cancer genetic counseling and ambispective evaluation of patients undergoing risk reducing surgery. |
| 63 | A study to evaluate time trends of clinical profile and risk factors among breast cancer patients and learning basic laboratory techniques of breast cancer lipidomics |
| 64 | Prospective evaluation of diagnostic imaging methods and its impact on surgical decision-making algorithm in the management of nodal disease in recurrent differentiated thyroid cancer and audit of the thyroid cancer database for evaluation of clinical and surgical spectrum and outcomes |
| 65 | A study evaluating MIS for of colorectal cancer patients and learning basic laboratory techniques of molecular biology for miRNA extraction in colon and rectal cancer patients |
| 66 | Prospective study on the expression of cancer-testis antigen (CT45) in the patients of advanced epithelial ovarian cancer undergoing Hyperthermic Intraperitoneal Chemotherapy and its correlation with response to platinum-based chemotherapy |
| 67 | Pilot study to evaluate the role of Toluidine Blue Dye and Narrow Band Imaging for assessment of malignant and potentially malignant disorders in oral cavity and update and analysis of Oral Cancer Database |
| 68 | Clinical spectrum, patterns of care and outcomes of Indian cancer patients treated by Multidisciplinary team management |
| 69 | Understanding the impact of gut microbiome dysbiosis and metabolic alterations in the pathogenesis of early onset (EOCRC) Colorectal Cancer (CRC) |
| 70 | Evaluation of tumor derived exosomes in blood during pre and post treatment of pancreatic cancer patients |
| 71 | Role of Circulating Tumor DNA (ctDNA) As A Surrogate Marker in Ovarian Cancer - A Pilot Study |
| 72 | Assessment of cell free DNA (cfDNA) as a biomarker in common gastrointestinal track cancers |
| 73 | POCSS for PBCR -Head &Neck, Breast and Cervix cancers |
| 74 | Prospective evaluation of diagnostic imaging methods and its impact on surgical decision-making algorithm in the management of nodal disease in recurrent differentiated thyroid cancer and audit of the thyroid cancer database for evaluation of clinical and surgical spectrum and outcomes |
| 1 | Diversity of Oral microbiome of smokeless tobacco induced oral cancer patients as compared to tobacco chewers and non tobacco chewer healthy individuals- A metagenomic approach” |
| 2 | Metallic tumor markers for breast cancer. Design, development and clinical implications. |
| 3 | Evaluation of circulating cell free DNA as a prognostic marker in breast cancer |
| 4 | A study of Promoter Methylation of PTEN in Sporadic BREAST Cancer from North India |
| 5 | Analyzing FGFR2 and candidate genes affecting Its Downstream Signaling In Breast Cancer |
| 6 | A comprehensive analysis of mammalian target of rapamycin (mTOR) and mitogen activated protein (MAP) Kinase signaling pathways in non- small cell lung carcinoma |
| 7 | Role of Multiparametric MRI in Evaluation of Locally Advanced Rectal Cancer. |
| 8 | Circulating microRNAs as biomarkers for testicular germ cell tumors: A pilot study |
| 9 | Randomized control trial of combined EBRT plus HD brachy therapy boost versus EBRT alone with IMRT in intermediate & high risk prostate cancer. |
| 10 | Functional status and co morbidities of older patients with cancer |
| 11 | Molecular analysis of LIFR and YAP genes in Indian Breast Cancer patients |
| 12 | Molecular Analysis of lats2 and Fosp³ genes in Indian Breast Cancer patients |
| 13 | Expression studies of FOXO gene family in Indian Breast Cancer Patients |
| 14 | A study to assess the effectiveness of an educational package on knowledge regarding post-operative care of oral cancer patient’s relatives following discharge. |
| 15 | A study to assess the level of fatigue and presence of functional deficit in adult patients undergoing upfront surgery for solid tumors in pre and post-surgical phase in AIIMS |
| 16 | Differentiating inflammatory and metastatic mediastinal lymphadenopathy on 18-FDG- PET/CT in lung cancer: Role of steroid suppression |
| 17 | Etiology of oral cancer in Indian population younger than 30 years |
| 18 | Evaluation of HE4 level in epithelial ovarian cancer for diagnosis & monitoring of therapy |
| 19 | An economic analysis of alternative treatment methods of ovarian cancer in India: An appraisal of economic burden, quality of life and mortality risk. |
| 20 | Evaluation of Human Epididymis Protein 4 (HE4) level in the diagnosis of ovarian cancer |
| 21 | Bio-statistical Models for Evaluation of Lymph Node involvement among oral cancer patients |
| 22 | Role of Real Time Ultrasonography fused with PET-CT for image guidance and intervention: A nodal approach in management of Thyroid cancer” |
| 23 | Evaluation of the effect of Prosthodontic Rehabilitation on quality of Life and Psychological distress in Maxillectomy patients – A preliminary study |
| 24 | To evaluate whether a predictive microRNA signature from TCGA acts as a biomarker in Indian colorectal cancer (CRC) patients” |
| 25 | Dosimetric study in children and young adults with differentiated Thyroid cancer undergoing radioiodine (¹³¹I-Na) therapy” |
| 26 | Isolation Identification and characterization of cancer stem cells from different histopathological grades of colorectal carcinoma” |
| 27 | Association of HIPEC treatment with expression of T regulatory cells (FOXP3) in epithelial ovarian cancer and its clinical significance |
| 28 | Determining Surgical Resection Margin of Cancer by Rapid Molecular Assessment Using Mass Spectrometric Imaging |
| 29 | Hyperthermia and immune modulation in homologous recombination stratified epithelial ovarian cancer: Development of targeted therapeutic approaches |
| 30 | The phase 2 study of HIPEC and the proposed phase 3 RCT comparing between HIPEC and IP chemotherapy. |
| 31 | A prospective study to elucidate molecular genetic risk factors of gallbladder carcinoma in Indian Population |
| 32 | Role of nuclear receptors in pathogenesis of carcinoma gall bladder |
| 33 | Molecular and Genetic Analysis of TNBC |
| 34 | Hyperthermia and immune modulation in homologous recombination stratified epithelial ovarian cancer: Development of targeted therapeutic approaches |
| 35 | The phase 2 study of HIPEC and the proposed phase 3 RCT comparing between HIPEC and IP chemotherapy. |
| 36 | Role of nuclear receptors in pathogenesis of carcinoma gall bladder |
| 37 | Study of a Surrogate Panel of Immunohistochemical and Molecular Markers to Classify Human Colorectal Carcinomas as per the Consensus Molecular Subtypes and Clinical Correlation |
Department of Surgical Oncology has four state of art major operation theatres for performing various kinds of major cancer surgeries. An operation theatre is capable of instituting Intra-operative Radiotherapy (IOHDR). This technique involves delivery of precise radiation beams to the tumor bearing area during the surgery after tumor removal. All the major operation theatres are well equipped with a range of modern and contemporary machinery and equipment required to perform various types of complex cancer surgeries involving various organ systems viz. intra-operative fluorescence imaging, gamma cameras, intra-operative nerve monitoring, HIPEC machines, ILP machine, laparoscopic units, modular OT tables, operating microscope, argon plasma coagulator etc. Robotic units are under the due process of procurement and will soon be operational.
The special surgical programs being provided for in the major OT are Robotic and Minimally Access Surgery, Palliative Surgery, Peritoneal Surface Malignancies, Microvascular Reconstruction, Risk Reducing Surgery and Intra-operative Radiation Therapy.

The department has a separate Minor O.T complex in the ground floor of IRCH for wound care and minor operations.
Minor operative procedures:
Patients of Gastro-intestinal, Genitourinary, Gynaecological, Thoracic and Head and Neck cancers require endoscopy procedure for confirmation and evaluation of cancer. The department of Surgical oncology is offering the following Endoscopy services for cancer patients at IRCH.
Diagnostic Endoscopy :
Therapeutic Endoscopy :
| Year | Census | ||
|---|---|---|---|
| Major OT procedure | Minor OT & Endoscopic Procedures | TOTAL | |
| 2008-09 | 632 | 6019 | 6651 |
| 2009-10 | 648 | 5569 | 6217 |
| 2010-11 | 706 | 5627 | 6333 |
| 2011-12 | 782 | 5303 | 6085 |
| 2012-13 | 1014 | 5811 | 6825 |
| 2013-14 | 1190 | 6411 | 7601 |
| 2014-15 | 1388 | 6814 | 8202 |
| 2015-16 | 1978 | 8372 | 10350 |
| 2016-17 | 1390 | 7908 | 9298 |
| 2017-18 | 1547 | 8782 | 10329 |
| 2018-19 | 1592 | 10477 | 12069 |
| 2019-20 | 1374 | 10493 | 11867 |
| 2020-21 | 977 | 3344 | 3221 (COVID) |
| 2021-22 | 1697 | 5843 | - |
Dr. BRA-IRCH, AIIMS, New Delhi has a dedicated ICU setup (6 beds) with state of art equipment and highly trained manpower – managed by Department of Onco-anesthesia.
NCI-AIIMS, Jhajjar campus presently has 25 operational ICU beds during Phase 1.
Dr. BRA-IRCH, AIIMS, New Delhi is a 182 bedded hospital and Surgical Oncology services cater to a total of 48 beds (including 5 private ward beds) and 4 dedicated OTs.
National Cancer Institute (NCI-AIIMS), Jhajjar campus – The surgical oncology services will have 200 beds and 18 OTs once completed. Presently the project is operationalizing in phase 1 (80 beds and 9 OTs).
| Day | Morning (9 AM – 1 PM) | Room | Afternoon (2 PM – 5 PM) | Room |
|---|---|---|---|---|
| Monday | - | - | Breast Cancer Clinic (BCC) | Board Room |
| Head & Neck Cancer Clinic (A) | Room 5 | |||
| Tuesday | Surgical Oncology OPD | Board Room | - | - |
| Genitourinary- Gynecology (GUG) Cancer Clinic | Room 59 | |||
| Wednesday | Thoracic Oncology Clinic | Room 5/7 | Gastro-intestinal Cancer (GIC) Clinic | Room 5 |
| Thursday | Surgical Oncology OPD (9am – 12 noon) | Board Room | Bone & Soft Tissue (B&ST) | Board Room |
| Friday | Genitourinary-Gynecology (GUG) Cancer & Peritoneal Surface Malignancy (PSM) Clinic | Room 59 | Breast Cancer Clinic | Board Room |
| Head & Neck Cancer Clinic (A) | Room 5 | |||
| Hepatobiliary & Pancreatic (HPB) Cancer Clinic | Room 6/7 | |||
| Saturday | Surgical Oncology Rehabilitation & Physiotherapy/Ostomy Care Clinic | Board Room/Minor OT 9B | - | - |
| Cancer Genetics Clinic | Room 6 | - | - |
Department of Surgical Oncology offers following opportunities for training
For Rules and Regulations –
For Enquiry regarding Training & Observerships – Contact
Prof SVS Deo
Head of Department
Department of Surgical Oncology
011-29575234
svsdeo@yahoo.co.in
For Enquiry - Contact :
Dean / Registrar ,AIIMS ,Ansari Nagar ,New Delhi -110029, India
Or
Prof. N.K. Shukla
Head of Department, Surgical Oncology
BRA-IRCH,
AIIMS
New Delhi -110029, India
GRID COVID-19 Study Group. Combating the COVID-19 pandemic in a resource-
constrained setting: insights from initial response in India. BMJ Glob Health.2020 Nov;5(11):e003416.

Preventive oncology clinic:
Friday: 2pm-5pm
Saturday: 9am-1pm
Contact number for appointment:
Establishment of Hospital Based Registries and Patterns of care and survival studies on Cancer Breast, Cancer Cervix and Head & Neck Cancers
Population Based Survival studies on Cancer Breast, Cancer Cervix and Head & Neck Cancers
Textbook of Radiation Oncology: Principles and Practice. G.K. Rath and B.K. Mohanti (eds). New Delhi: BI Churchill Livingstone, 2000 (ISBN 81-7042-166-7); Elsevier, 2003 (Reprint)
As part of AIIMS New Delhi, the department plays a pivotal role in training future oncologists. It offers:
Research is a key component of the department’s activities. It focuses on:
The department collaborates with national and international cancer research institutes, ensuring that it remains at the cutting edge of oncology advancements.
RT ward : 32 beds
Patients and their relatives are educated through pamphlets, frequent interactions etc. regarding the status of their disease, intended treatment, care and precautions to be taken during treatment and expected outcome.
The department offers comprehensive radiation oncology services, catering to a vast number of cancer patients from across India. It is equipped with modern radiotherapy techniques, including:
The department works closely with Medical Oncology, Surgical Oncology, Pathology, Radiology, Nuclear Medicine and Palliative Care to provide a holistic and patient-centric approach to cancer treatment. Multidisciplinary disease site clinics ensure that every patient receives an individualized treatment plan based on evidence-based protocols.
Clinics
The faculty is involved in various interdepartmental research projects and thesis work. We are also involved in a research project being conducted in collaboration with IIT, Delhi.
The Radiology unit provides following diagnostic services - X-ray, ultrasound, CT scan, mammography, fluoroscopic procedures like barium and contrast studies and diagnostic Angiography. X-rays are done immediately during working hours, without any waiting. Other investigations are performed with prior appointment which can be obtained at counter no. 12, ground floor, Dr BRAIRCH.
Interventional radiological services include ultrasound and CT guided biopsy, FNAC and drainage procedures. Palliative care procedures like percutaneous nephrostomy (PCN) and percutaneous transhepatic biliary drainage (PTBD) with stenting and therapeutic vascular interventions including transarterial chemo embolization are also performed. MRI facility is not available in the unit and this service is provided by centralized facility of department of NMR.
We also review outside imaging studies of patients being treated at BRAIRCH. We also engage in collaborative image guided procedures with other departments. These include intra-operative ultrasound, radio-frequency ablation of tumors and interventional pain management procedures.
A radiographer is on duty on 24x7 basis to provide emergency x-rays, including portable bedside x-rays in wards, ICU and OT.
We conduct interdepartmental clinic-radiological conferences with all clinical departments of BRAIRCH six days a week. In this, the imaging studies are discussed and compared. This is an important teaching as well as patient care activity of the department. In addition, faculties of the department regularly take classes for students of MD Radio-diagnosis, MD, Radiotherapy, DM Medical oncology and M Ch Surgical oncology. They also participate in teaching of undergraduate students of MBBS.

The Indian Cancer Genetics and Genomics Conference-2020
The Indian Cancer Genetics and Genomics Conference-2020 (ICGGC-2020) was organized on a hybrid-virtual platform on the 24th and 25th of November 2020. This was organised by the Department of Medical Oncology, AIIMS, New Delhi in association with the Indo-UK Genetic Education Forum, under the aegis of the Research and Education Society of medical Oncology (RESMO).
Genetics and genomics are playing an ever-increasing role in deciding the management of cancers, be it the diagnosis, prognosis, precision therapeutic management or precision prevention. The role of genomics and genetics in oncology is evolving at an extremely fast pace and it is prudent to keep abreast of it. Precision prevention, particularly identifying the high-risk families and unaffected relatives has a tremendous potential for preventing cancers and altering the natural history of the disease. With this intent in mind, this conference was planned to present the current state-of -the art management in Clinical Cancer Genetics. It was an educational event targeted to the residents training in medical, surgical, radiation oncology and gynaecological and breast surgery in different institutes all over the country.
The conference had a galaxy of esteemed faculty, including renowned clinicians and geneticists from the United kingdom, the United Sates, leading academic institutes across the length and breadth of India including AIIMS-New Delhi, Tata Memorial Hospital-Mumbai, PGIMER-Chandigarh, JIPMER-Puducherry, Cancer Institute-Adyar, Chennai.
The first day was dedicated to Hereditary breast and ovarian cancers and the speakers explained the current concepts and the state- of – the art practice. Important data from European and Indian studies were presented and discussed. Panel discussion explaining the important aspects of clinical management was organised. The second day was dedicated was Lynch syndrome, Li Fraumeni, Retinoblastoma and other miscellaneous cancers. The laboratory principles, technical details of reporting, genetic counselling etc were addressed.
The event was attended online and appreciated by more than 800 viewers all over the world. The videos of the event, both days 1 & 2 are available at the link on the institute website.
navdeepaiims@yahoo.com
| S. No. | Name | Passing Year | Email Address |
|---|---|---|---|
| 1 | Dr ATUL SHARMA | 1998 | atul1@hotmail.com |
| 2 | Dr MANISHA BHUTANI | 1999 | manishabhutani@hotmail.com |
| 3 | Dr VIKAS GUPTA | 1999 | vikas71@hotmail.com |
| 4 | Dr JYOTI WADHWA | 1999 | jyotiwadhwa@hotmail.com |
| 5 | Dr SUSHREE PARIDA | 2000 | sushreeparida@gmail.com |
| 6 | Dr SUDEEP GUPTA | 2000 | sudeepgupta04@gmail.com |
| 7 | Dr PRATAP KISHORE DAS | 2000 | - |
| 8 | Dr HARINDER PAL SINGH | 2000 | - |
| 9 | Dr PRAKASH N P | 2001 | - |
| 10 | Dr AMIT AGARWAL | 2002 | - |
| 11 | Dr RAJEEV BEDI | 2002 | - |
| 12 | Dr SHAWGI S | 2002 | - |
| 13 | Dr HARI K GOYAL | 2003 | - |
| 14 | Dr AMISH D VOHRA | 2003 | tellamish@yahoo.com |
| 15 | Dr DEVINDER SINGH | 2003 | devinderaiims@hotmail.com |
| 16 | Dr BRIJESH KUMAR | 2003 | - |
| 17 | Dr HARI MENON V G | 2003 | menontata@yahoo.in |
| 18 | Dr GANESSAN K | 2004 | ganessan.kichenadase@gmail.com |
| 19 | Dr NAVIN KHATTRY | 2005 | nkhattry@gmail.com |
| 20 | Dr GULL MOHD BHAT | 2005 | drgull81250@yahoo.com |
| 21 | Dr NILESH LOKESHWAR | 2005 | nileshlok@yahoo.com |
| 22 | Dr B SURENDRA | 2006 | - |
| 23 | Dr JOSEPH FRANSIS DOMINIC | 2006 | josephdominic75@gmail.com |
| 24 | Dr MANJU SENGAR | 2006 | manju.sengar@gmail.com |
| 25 | Dr J LAIRINSANGA PAUTA | 2006 | - |
| 26 | Dr RAVI SHANKAR PATNAIK | 2006 | ravipatnaik@gmail.com |
| 27 | DR K H MEDHI | 2006 | mediaiims@gmail.com |
| 28 | Dr NAVDEEP SINGH | 2007 | - |
| 29 | Dr SATYAPAL KATARIA | 2007 | - |
| 30 | Dr AJAY GUPTA | 2008 | ajayajaygupta2002@rediffmail.com |
| 31 | Dr JAYA GHOSH | 2008 | archana_jaya_ghosh@yahoo.co.in |
| 32 | Dr AMIT DUTT DWARY | 2008 | amitdwary@gmail.com |
| 33 | Dr S BHATTACHARYA | 2008 | shibashishbhattacharya@ymail.com |
| 34 | Dr PRABRAJYAN NARAYAN MOHAPATRA | 2008 | prabrajya.mohapatra@rediffmail.com |
| 35 | DR JYOTI BAJPAI | 2009 | dr_jyotibajpai@yahoo.co.in |
| 36 | Dr DEEPAK GUPTA | 2009 | drdeepakgupta@yahoo.co.in |
| 37 | Dr DEEPAK DEBKARA | 2009 | deepakdabkara@yahoo.com |
| 38 | Dr PRASHANTH G. | 2009 | pg1980@gmail.com |
| 39 | DR INDERNEEL | 2010 | dr.indraghosh@gmail.com |
| 40 | Dr MANISH SINGHAL | 2010 | singhaloncocare@yahoo.co.in |
| 41 | DR SUSHIL MANDHANIYA | 2010 | sushilmandhania@gmail.com |
| 42 | DR DIPANJAN PANDA | 2010 | dipanjan.panda@gmail.com |
| 43 | Dr GAURAV PRAKASH | 2011 | drgp@gmail.com |
| 44 | DR VENKAT | 2011 | venkymd@gmail.com |
| 45 | DR RAM PRABHU | 2011 | ramprabu_1979@yahoo.co.in |
| 46 | Dr. AJAY GOGIA | 2011 | >ajaygogia@gmail.com |
| 47 | Dr ANUJ KUMAR BANSAL | May-12 | anujkumarbansal2003@gmail.com |
| 48 | Dr PRABHAT S MALIK | May-12 | drprabhatsm@gmail.com |
| 49 | Dr TVS TILAK | Dec-12 | drtilaktvs@gmail.com |
| 50 | Dr SMITA KAYAL | Dec-12 | kayalsmita@rediffmail.com |
| 51 | Dr ANKUR BEHL | Dec-12 | drankurbahl@gmail.com |
| 52 | Dr RK BIKRAM SINGH | Dec-12 | bikramsana@gmail.com |
| 53 | Dr SONU CYRIAC | May-13 | sunucyriac@rediffmail.com |
| 54 | Dr SIDHARATH | May-13 | dr.sid22@gmail.com |
| 55 | Dr VIBHAS BISWAS | May-13 | bivasbiswas@gmail.com |
| 56 | Dr RANJIT K SAHOO | Dec-13 | drranjitmd@gmail.com |
| 57 | DR. PRASHANT MEHTA | Dec-14 | prashantcipher@yahoo.co.in |
| 58 | DR. SAPHALTA BAGHMAR | Dec-14 | drbsaphalta@gmail.com |
| 59 | DR. VIJAY NATARAJ | Dec-14 | vimurugan@yahoo.co.in |
| 60 | DR. NIDA IQBAL | May-15 | nida.iqbal55@yahoo.com |
| 61 | DR. PRIYA TIWARI | May-15 | pluto_2k3@yahoo.co.in |
| 62 | DR. ATUL BATRA | Dec-15 | batraatul85@gmail.com |
| 63 | DR. HARISH P | Dec-15 | harishnharry@gmail.com |
| 64 | DR. BOYA RAKESH REDDY | May-16 | drrakeshreddyboya@yahoo.com |
| 65 | DR. RAJA PRAMANIK | May-16 | drrajapramanik@gmail.com |
| 66 | DR. RAMAN KAIN | Dec-16 | drramankain@gmail.com |
| 67 | DR. CHANDAN KRUSHNA DAS | Dec-16 | ckdasneo@yahoo.com |
| 68 | DR. B. SAINATH | Dec-16 | bsainath101@yahoo.co.in |
| 69 | DR. PAI ROHIT RAMESH | May-17 | docrohitpai@gmail.com |
| 70 | DR. AMOL NANDKUMAR PATEL | May-17 | dr.amolpatel@gmail.com |
| 71 | DR. VINEET GOVINDA | Dec -17 | vineetgovindagupta@gmail.com |
| 72 | DR. DEEPAM PUSHPAM | Dec -17 | deepampushpam@gmail.com |
| 73 | DR. AKASH KUMAR | May- 18 | akashjha08@gmail.com |
| 74 | DR. SUSHANT KUMAR PAIKRAY | May- 18 | drskppgi@gmail.com |
| 75 | DR. AJAY YADAV | May- 18 | ajayalwar01@gmail.com |
| 76 | DR. AKASH TIWARI | Dec- 18 | akash07tiwari@gmail.com |
| 77 | DR. MUKESH PATEKAR | Dec- 18 | drmukeshpatekar@gmail.com |
| 78 | DR. ATUL SHARMA | Dec- 18 | dratulsharma@gmail.com |
| 79 | DR. ABHISHEK RAJ | May-19 | 316.raj@gmail.com |
| 80 | DR. VINOD SHARMA | May-19 | vinod_mbbs4u@yahoo.co.in |
| 81 | DR. ILAVARASI VANIDASSANE | May-19 | docila12@gmail.com |
| 82 | DR. ARUN GARG | May-19 | arungarg1512@gmail.com |
| 83 | DR. MANISH SHARMA | May-19 | - |
| 84 | DR. BABITA KATARIA | Dec-19 | dr.babita.lhmc@gmail.com |
| 85 | DR. APARNA SHARMA | Dec-19 | aparna96@gmail.com |
| 86 | DR. RAMAVATH DEV | Dec-19 | devaiims2012@gmail.com |
| 87 | DR. VIRAJ NEVREKAR | Dec-19 | vn1351@yahoo.co.in |
| 88 | DR. SUKESH NAIR | May-20 | sukesh2529@yahoo.com |
| 89 | DR. HARISH KANCHARLA | May-20 | harik486@gmail.com |
| 90 | DR. SUNIL SHARMA | May-20 | ss463581@gmail.com |
| 91 | DR. NARESH GUNDU | May-20 | nareshcamry@gmail.com |
| 92 | DR. PRIYANSHU CHOUDHARY | Dec- 20 | drpriyanshu17@gmail.com |
| 93 | DR. SATYAJIT PAWAR | Dec- 20 | dr.sj156@gmail.com |
| 94 | DR. SURYA PRAKASH VADLAMANI | Dec- 20 | vadlamanisuryaprakash@gmail.com |
| 95 | DR. SANTOSH CHELLAPURAM | Dec- 20 | Santosh.chellapuram@gmail.com |
| 96 | DR. VIKAS GARG | May- 21 | vg18007@gmail.com |
| 97 | DR. ABHENIL MITTAL | May- 21 | drabhenil@gmail.com |
| 98 | DR. KAUSHAL KALRA | May- 21 | kaushalkalra@yahoo.com |
| 99 | DR. SAURAV VERMA | May- 21 | sauravverma4327@gmail.com |
| 100 | DR. ANKUR VARSHNEY | Dec- 21 | drankurvarshney@gmail.com |
| 101 | DR. RAKESH SHARMA | Dec- 21 | rakesh28k9@gmail.com |
| 102 | DR. ROHIT REDDY | Dec- 21 | rohitreddy915@gmail.com |
| 103 | DR. AZGAR ABDUL RASHEED | Dec- 21 | azgarar@gmail.com |
| 104 | DR. SHALABH ARORA | Dec- 21 | dr.shalabharora@gmail.com |
| 105 | DR. ANNIE K BAA | May- 22 | anniekbaa@gmail.com |
| 106 | DR. GHAZAL TANSIR | May- 22 | ghzl_complique@yahoo.com |
| 107 | DR. NEHA PATHAK | May- 22 | drneha1pathak@gmail.com |
| 108 | DR. SUDHIR KIRAR | May- 22 | sudhirkirar@gmail.com |
| 109 | Dr. Rupak Kr. Giri | Dec.-22 | zeemelgiri@gmail.com |
| 110 | Dr. Sindhu Chitikela | Dec.-22 | drcsindhu@gmail.com |
| 111 | Dr. Anshul Gupta | Dec.-22 | anshul_dr@yahoo.co.in |
| 112 | Dr. Shuvadeep Ganguly | Dec.-22 | ganguly.shuvadeep@gmail.com |
| 113 | Dr. Kapil Goyal | Dec.-22 | kapil207goyal@gmail.com |
| S.No | Names | Month &Year of PhD Awarded | |
|---|---|---|---|
| 1 | Dr. Gottemukkala Muralik Raju | February-1999 | |
| 2 | Dr. Ashutosh Pathak | May-2002 | |
| 3 | Dr. Pratibha Sharma | January-2010 |  |
| 4 | Dr. Rashmi Bhardwaj | September-2010 |  |
| 5 | Dr. Rakesh Verma | March-2011 |  |
| 6 | Dr. Nitin Mathur | February-2012 |  |
| 7 | Dr. Surender Kumar Sharawat | May-2013 |  |
| 8 | Dr. Nivedita Pathak | September-2013 |  |
| 9 | Dr. Minakshi Mann | February 2014 – July 2020 |  |
| 10 | Dr. Anudishi Tyagi | January 2013 - February 2019 |  |
| 11 | Dr. Shivali Jasrotia | August 2011 - July 2019 |  |
| 12 | Dr. Mohsin Maqbool | February 2010 - December 2018 |  |
| 13 | Dr. Shilpi Chaudhary | February 2016- October 2021 |  |
| 14 | Dr. Anjali Mookerjee | February 2015 - December 2021 | |
| 15 | Dr. Luxmi Devi | February 2015- February 2022 |  |
| S.no | Publication | Year Published |
|---|---|---|
| 1 | Kumar A, Bhatnagar S. Cancer; Mental Health-Gender Difference. Hospital Today Vol V1 NO. 8 : August 2000. | 2000 |
| 2 | Kumar A, Bhatnagar S. Cancer; Mental Health-Gender Difference. Hospital Today Vol V1 NO. 8 : August 2000. | 2000 |
| 3 | Deo SVS, Shukla NK, Srinivas G, Raina V, Mohanti BK,Rath GK.Colorectal cancers-Experience at a regional Cancer center in India. Tropical Gastroenterology,2001;22:83-86. | 2001 |
| 4 | Agrawal S, Guleria S, Dinda A, Kumar L. and Tarique S. Embryonal sarcoma of liver mimicking hydatid cyst in an adult. Trop Gastroenterol 2001 | 2001 |
| 5 | Asthana S, Deo SVS, Shukla NK, Raina V and Kumar L. Persistent mullerian duct syndrome presenting with bilateral intra-abdominal gonaldal tumours and obstructive uropathy. Clin oncol 2001; 13:304-306. | 2001 |
| 6 | Asthana S, Deo SVS, Shukla NK, Raina V.Carcinoma breast metastatic to hand and foot .Austalasian Radiology,2001; 45(3);380-382. | 2001 |
| 7 | Bimla N, Kumar L, Thulkar S, Bal S and Dawar R. Primary malignant melanoma in ovarian cystic teratoma. Gynecol Oncol 2001; 82:380-383 | 2001 |
| 8 | Chaudhary R, Mathur P, Dhawan B and Kumar Lalit. Emergenge of metronidazole – resistant bacteroides fragilis, Emerging Infectious Dis 2001;7:485-6. | 2001 |
| 9 | Deo SVS, Mohanti BK, Shukla NK, Chawla S, Raina V, Julka PK, Rath GK. Attitudes and treatment outcome of breast conservation therapy for stage I & II breast cancer using peroperative iridium-192 implant boost to the tumor bed. Australasian Radiol. 45:35-38, 2001 | 2001 |
| 10 | Pathy S, Mohanti BK, Sharma A, Bahadur S, Sharma DN, Wadhwa MK. Giant cell reparative granuloma maxilla-A case report. Oncology Forum 2001;4:9-11. | 2001 |
| 11 | Pathy S, Mohanti BK, Sharma A, Bahadur S, Sharma DN, Wadhwa MK. Giant Cell reparative Granuloma of the Maxilla. Oncology Forum 2001: 4; 9-12 | 2001 |
| 12 | Prakash J, Gupta SK, Kochupillai V, Singh N, Gupta SK and Joshi S. Chemopreventive activity of Withania somnifera in experimentally induced firbosarcoma tumours in Swiss albino mice. Phytother Res 2001,15:240-244 | 2001 |
| 13 | Sengupta S, Tyagi P, Chandra S, Kochupillai V, Gupta SK. Encapsulation in cationic liposomes enhances antitumor efficacy and reduces the toxicity of etoposide, a topo-isomerase II inhibitor. Pharmacology 62:163-171, 2001. | 2001 |
| 14 | Sharma A, Raina V, Gujral S, Kumar R, Tandon R, Jain P Burkitt's lymphoma of stomach: A case report and review of literature. Am J Hematol. 2001 May;67(1):48-50. | 2001 |
| 15 | Sharma DN, Chander S, Gairola M, Kumar L, Parida DK, Pathy S. Medical disorders associated with endometrial carcinoma. JAPI 2001; 49:630-633. | 2001 |
| 16 | Wadhwa J, Kumar L and Kochupillai V. VAD followed by VMCP. An alternative regimen for multiple myeloma. Medical Oncology Vol 19(No.2):2002 | 2002 |
| 17 | Bhutani M, Kumar L, Seth A, Thulkar S, Vijayraghwan M & Kochupillai V. Germ cell tumours of testis : Clinical features, treatment outcome and prognostic factors. Nat Med J India 2002;15:18-21 | 2002 |
| 18 | Mathur P, Chaudhary R, Dhawan B and Kumar Lalit. Anaerobic bacterimia in patients of hematological malignancies. Med & Paed Oncology 2002;38:147 | 2002 |
| 19 | Agrawal A,Raina V,Shukla NK, Deo SVS, Rath GK, Sharma A,Mohanti BK. Retrospective analysis of locally advanced breast cancer(LABC) seen at All India Institute of Medical Sciences,New-Delhi, India (1993-1988). Proc Am Soc Clin Oncol 2002;21 ;62b. | 2002 |
| 21 | Bhutani M, Vora A, Kumar L, Kochupillai V. Lympho-hematopoietic malignancies in India: Medical Oncology, 2002; 19 (3): 141-50. | 2002 |
| 22 | Bhutani M, Kumar L, Vora A, Bhardwaj N, Pathak AK, Singh R and Kochupillai V. Randomised study comparing 4’- epidoxorubicin (Epirubicin) Versus doxorubicin as a part of Induction treatment in adult acute lymphoblastic leukemia. Am. J. Haematol, 2002; 71 (4): 241-247 | 2002 |
| 23 | Deo SVS, Shukla NK, Raina V Bhutani M, Joydeep P, Rath GK .A prospective randomized trial comparing preoperative versus no preoperative chemotherapy in operable locally advanced breast cancer (T4bN0-2M0). International J of Cancer, 2002 (Supplement 13 ) ;199 (abstract P 182 ). | 2002 |
| 24 | Kumar L, Kumari M and Menon H. STI-571 (Gleevec) in the treatment of chronic myeloid leukemia. Nat Med J India, 2002; 15: 298 (IF, 0. 617). | 2002 |
| 25 | Kumar P, Rehani MM, Kumar L, Sharma R, Bhatla N, Singh R, Sundaram KR. Potential of CT scan based tumor volume as a response indicator in chemotherapy of advanced epithelial ovarian cancer. Med Sci Monit, 2002; 8(10): CR667-674 | 2002 |
| 26 | Mathur P, Chouchary R, Kumar L, Kapil A, Dhawan B. A study of bacterimia in febrile neutropenic patients at a tertiary – care hospital with special reference to anerobes. Med Oncol, 2002; 19: 267-272 (IF, 1.318). | 2002 |
| 27 | Pathak AK, Singh N, Khanna N, Reddy VG, Prasad KN and Kochupillai V. Potentiation of the effect of paclitaxel and carboplatin by antioxidant mixture on human lung cancer H520 cells. J Am Coll Nutr, 2002; 21 (5): 416-425. | 2002 |
| 28 | Raina V, Sharma A, Vora A, Bedi R, Shukla NK, Rath GK, Deo SVS,. Non –Hodgkin lymphoma of the gastrointestinal tract . Is chemotherapy alone an effective modality ? International J of Cancer, 2002 (Supplement 13 );401 (abstract P845). | 2002 |
| 29 | Rath GK, Deo SVS, Shukla NK, Raina V, Mohani BK. .Multimodality management of squamous anal cancer using sequential chemoradiation. International J of Cancer, 2002 (Supplement 13 );219 (abstract P246). | 2002 |
| 30 | Sharma A, Raina V, Shukla NK, Mohanti BK, Deo SVS, Rath GK, Kochupillai V. Oxaliplatin, folinic acid and 5 flurouracil in advanced/unresectable adenocarcinoma of gall bladder: a pilot study. Proc Am Soc Clin Oncol 2002;21:142 b. | 2002 |
| 31 | Shukla NK, Das DK, Deo SVS, Raina V – An analysis of long-term venous access catheters in cancer patients : experience from a tertiary care centre in India. Journal of Postgraduate medicine 2002, 48:21-24. | 2002 |
| 32 | Shukla NK, Deo SVS, Asthana S, Raina V, Dronamaraju SS. Neodaduqvant chemotherapy in advanced gastric cancer-results of a pilot study. Tropical Gastroenterology 2002, 23:94-96. | 2002 |
| 33 | Vohra A, Raina V, Sharma A, Bedi R, Shukla NK, Rath GK, Deo SVS. Primary gastro intestinal non Hodgkins lymphoma (GINHL). Does it behaves like nodal NHL? Is chemotherapy alone sufficient to cure GINHL? Blood 2002:100 (11):303b (abst). | 2002 |
| 34 | Wadhwa J, Kumar L and Kochupillai V. VAD followed by VMCP. An alternative regimen for multiple myeloma. Medical Oncology, 2002; 19 (2) : 105-108. | 2002 |
| 35 | Kar M, Deo SVS, Shukla NK, Asthana S, Mohanti BK, Bijlani L. Malignant peripheral nerve sheath tumor (MPNST)-clinical profile and management at a regional cancer centre. International J of Cancer, 2002 (Supplement 13); 302 (Abstract P517). | 2002 |
| 36 | Anand M, Kumar R, Jain P, Gupta R, ghosal N, Sharma A, Agarwal A, Sharma MC. Metastatic anaplastic oligodendroglioma simulating acute leukemia: a case report. Acta Cytologica 2003; 47(3): 467-469. | 2003 |
| 37 | Anand M, Kumar R, Kumar L, Barge S, Singh S. Chronic myeloid leukemia presenting with absence of basophils and marked dyspoiesis. Ind J Cancer. 2003; 40: 144-7. | 2003 |
| 38 | Anand M, Kumar R, Jain P, Gupta R, Majumdar N, Sharma A, Agarwal A, Sharma MC. Metastatic Anaplastic Oligodendroglioma Stimulating Acute Leukemia: A Case Report. Acta Cytologica, 2003; 47: 467-469. | 2003 |
| 39 | Kumar L, Raju GMK, Ganessan K, Shawgi S, Menon H, Wadhwa J, Sharma A, Singh R and Kochupillai V. High dose chemotherapy followed by autologous stem cell transplantation in multiple myeloma. Nat Med J India, 2003; 16: 16-20 | 2003 |
| 41 | Deo SVS, Purkayastha J, Shukla NK, Raina V, Asthana S, Das DK, Rath GK. Intent of therapy in metastatic breast cancer with isolated ipsilateral supraclavicular lymph node spread; A therapeutic dilemma. JAPI, 2003;51:272-275. | 2003 |
| 42 | Bakhshi S, Arya LS. Etiopathophysiology of disseminated intravascular coagulation. JAPI 2003;51:796-800. | 2003 |
| 43 | Bakhshi S, Kabra M, Iyer V, Arya LS. Immune thrombocytopenic purpura as a presenting manifestation of childhood tubercular lymphadenitis. Indian J Pediatr 2003;70:993-994. | 2003 |
| 44 | Bakhshi S, Arya LS. Diagnosis and treatment of disseminated intravascular coagulation. Ind Pediatr 2003;40:721-730. | 2003 |
| 45 | Bakhshi S, Abella E. Candida parapsilosis on peripheral blood smear. Ind Pediatr 2003;40:903-904. | 2003 |
| 46 | Bedi R, Kumar L, Kochupillai V. Autologous peripheral blood stem cell transplantation : predictors for haemopoietic reconstitution. Nat Med J India 2003;16:209-213. | 2003 |
| 47 | Bedi R, Kumar L, Bhutani M, Sharma A, Kochupillai V, and Mohanti S. Autologous peripheral blood stem cell transplantation : Engraftment Kinetics. Ind Jn Med & Paed Oncology 2003;24: 9-14. | 2003 |
| 48 | Bhatia M, Kumar A, Bhardwaj NK, Pandey RM and Kochupillai V. Electrophysiological evaluation of Sudarshan Kriya: EEG, BAER and P-300 study. Ind J Physiol Pharmacol 2003;47 (2):157-163. | 2003 |
| 50 | Deo SV, Bhutani M, Shukla NK, Raina V, Rath GK, Purkayasth J. Randomized trial comparing neo-adjuvant versus adjuvant chemotherapy in operable locally advanced breast cancer (T4bN0-2M0). J Surg Oncol. 2003; 84 (4): 192-197. | 2003 |
| 51 | Deo SV, Purkayastha J, Shukla NK, Raina V, Asthana S, Das DK, Rath GK. Intent of therapy in metastatic breast cancer with isolated ipsilateral supraclavicular lymph node spread--a therapeutic dilemma. J Assoc Physicians India. 2003; 51: 272-275 | 2003 |
| 52 | Deo SV, Sridhar D, Purkayastha J, Bhutani M, Shukla NK, Raina V. Theapuetic controversies in bilateral breast cancer. Clin Oncol (R Coll Radiol) 2003; 15(5): 297-8 | 2003 |
| 53 | Deo SV,Bhutani M,Shukla NK,Raina V,Rath GK,Purkayasth J. Randomised trial comparing neo-adjuvant chemotherapy versus adjuvant chemotherapy in operable locally advanced breast cancer (T4bN0-2 M0). J Surg Oncol.2003;84(4):192-7. | 2003 |
| 54 | Ganessan K, Kumar L, Sharma A, & Kochupillai V. Waldenstrom’s Macroglobulinemia : Report of 8 cases. Ind J Med & Paed Oncology 2003;24:9-12. | 2003 |
| 55 | Jain P, Kumar R, Anand M, Asthana S, Deo SV, Gupta R, Bhutani M, Karak AK, Shukla NK. Touch imprint cytology of axillary lymph nodes after neoadjuvant chemotherapy in patient with breast carcinoma. Cancer. 2003; 25: 99(6): 346-51. | 2003 |
| 56 | Jain P. Kumar R, Anand M, Asthana S, Seo SVS, Gupta R, Bhutani M, Karak AK, Shukla NK. Touch imprint cytology of axillary lymph nodes after neoadjuvant chemotherapy in patients with breast cancer. Cancer Cytopathology 2003; 99: 346-351 | 2003 |
| 57 | Jain V, Bakhshi S, Chan MY, Arya LS. Acute myeloid leukemia presenting simultaneously in two siblings. Ind Pediatr 2003;40:1191-1194. | 2003 |
| 58 | Jeremy LP and Kumar L. Selected summary . Nat Med J India 2003;16:150-151. | 2003 |
| 59 | Kumar L, Barge S, Mahapatra AK, Thulkar S, Rath GK, Kumar S, Mishra R, Dawar R and Singh R. Central nervous system metastases from primary epithelial ovarian cancer. Can Control 2003;10: 244-253. | 2003 |
| 60 | Kumar L, Janga D, Berge S, Gupta S, Kumar S, Bhatla N and Kochupillai V. neoadjuvant chemotherapy in stage III & IV epithelial ovarian carcinoma (EOC). J Ind Med Sci. Acad. 2003;16:89-92. | 2003 |
| 61 | Kumar L, Kumari M, Kumar S, and Kochupillai V. Chronic myelogenous leukemia (CML). Ind J Hematol & Trans Medicine 2003;21:21-26 | 2003 |
| 62 | Kumar L, Barge S, Mahapatra AK, Thulkar, S, Rath GK. Central nervous system metastases from primary epithelial ovarian cancer. Can Control 2003; 10 (3): 244-253. | 2003 |
| 63 | Mohanty S, Bakshi S, Kapil A, Gupta AK, Arya LS, Das BK. Venous thrombosis with Salmonella infection: report of a case and review of literature. Ind J Med Sci 2003;57:199-203 | 2003 |
| 64 | Raina V, Sharma A, Mohanty BK, Kumar R, Dawar R, Rath GK Etoposide, vinblastine, adriamycin and prednisolone(EVAP) combination chemotherapy as first line treatment for Hodgkin’s disease. The Nat Med J India. 2003; 16: 199-203. | 2003 |
| 65 | Raina V, Sharma A, Mohanti BK, Kumar R, Dawar R, Rath GK. Etposide, Vinblastine, Adriamycin and Prednisolone (EVAP) combination chemotherapy as first-line treatment for Hodgkin’s disease. Natl Med J India 2003; 16 (3): 199-203 | 2003 |
| 66 | Raju GM, Guha S, Mukhopadhyay A, Kumar L, Kale VP, Mittal S, Deka D, Mohanty S, Kochupillai V. Colony-stimulating activity of fetal liver cells: synergistic role of stem cell factor in bone marrow recovery from aplastic anemia. J Hematother Stem Cell Res 2003; 12(5):491-7. | 2003 |
| 67 | Sharma A, Agarwal A , Sharma MC, Anand M, Agarwal S, Raina V. Bone Marrow Metastasis in Anaplastic Oligodendroglioma. Intl. J Clin Practice 2003; 57(4): 351-352 | 2003 |
| 68 | Sharma A, Singh D, Raina V, Mohanti VK, Bahadur S, Shukla NK. Second Primary Cancer From And To Head And Neck Area: Report Of 2 Cases. Otorinolaringologia 2003; 53: 67-69. | 2003 |
| 69 | Sharma A, Raina V. Current Status of Bone Marrow and Stem Cell Transplantation in Breast cancer: A Review. Indian J Med and Ped Oncol , 2003; 24: 13-18 | 2003 |
| 70 | Sharma H, Sen S, Singh A, Bhardwaj NK, Kochupillai V and Singh N. Sudarshan Kriya practitioners exhibit better antioxidant status and lower blood lactate levels. Biol. Psychol. 2003; 63: 281-291 | 2003 |
| 71 | Singh D, Sharma A, Mohanti BK, Thulkar S, Bahadur S, Sharma SC, Gupta SD. Multiple Extranodal Sites at Presentation in non-Hodgkin’s Lymphoma. Am J Hematol 2003; 74(1): 74-77. | 2003 |
| 72 | Singh D, Wadhwa J, Kumar L, Raina V, Agarwal A, and Kochupillai V. POEMS syndrome : Experience with fourteen cases. Leuk & Lymphoma 2003;44:1749-1752. | 2003 |
| 73 | Tomar S, Bakhshi S, Kabra SK, Arya LS. Pancreatic pseudocyst complicating treatment of acute lymphoblastic leukemia. Ind Pediatr 2003;40:670-672. | 2003 |
| 74 | Singh D, Sharma A, Mohanti BK, Thulkar S, Bahadur S, Sharma SC, Gupta SD. Multiple extra nodal sites at presentation in non-Hodgkin's lymphoma. Am J Hematol. 2003; 74 (1): 75-77 | 2003 |
| 75 | Khaitan A, Gupta NP, Goel A, Safaya R & Kumar L. Primary non-Hodgkin’s lymphoma of urinary bladder. Report of a case and review of literature. Urol Int 2004;72: 82-4. | 2003 |
| 76 | Anand M, Kumar R, Kumar L, Barge S and Singh S. Chronic myeloid leukemia presenting with absence of basophils and marked dyspoiesis. Ind J Cancer 2004;40:144-7. | 2004 |
| 77 | Arora B, Kumar L, Sharma A, Wadhwa J, & Kochupillai V. Pigmentary changes in chronic myeloid leukemia patients treated with imatinib mesylate. Ann Oncol 2004;15:358-359. | 2004 |
| 78 | Bakhshi S, Hamre MR. Neuroblastoma in chromosomal breakage syndromes. Cancer Genet and Cytogenet 2004;148:85. | 2004 |
| 79 | Gupta R, Jain P, Deo SVS, Sharma A. Flow cytometric analysis of CD5 positive B- cells: a frame of reference for minimal residual disease analysis in chronic lymphocytic leukemia. Am J Clin Pathol 2004; 121: 368-372. | 2004 |
| 80 | Gupta R, Jain P, Deo SV,Sharma A. Flow cytometric analysis of CD5+ B cells: a frame of reference for minimal residual disease analysis in chronic lymphocytic leukemia. Am J Clin Pathol. 2004 Mar; 121(3):368-72. | 2004 |
| 81 | Seth T, Vora A, Bhutani M, Jain P, Kumar R, Kochupillai V. Acute basophilic leukemia with translocation t(8; 21) as sole cytogenetic abnormality. Leuk Lymphoma 2004; 45 (3): 605-608 | 2004 |
| 82 | Singh D, Kumar L, Sharma A, Vijayraghwan M, Thulkar S & Tandon N. Adrenal involvement in non Hodgkin’s lymphoma : Four cases and review of literature. Leuk & Lymphoma 2004;45:789-794. | 2004 |
| 83 | Anand M, Ghara N, Kumar R, Singh Sarika, Sengar M, Panikar N, Raina V, Sharma A. Myeloperoxidase cytochemical negativity: An unexpected but intrinsic property of blasts of all phases of Chronic Myeloid Leukemia. Annals of Hematology (Online published 1st July 2005)84; 767-770 | 2005 |
| 84 | Dutta T, Sharma H, Kumar L, Dinda AK, Kumar S, Bhatla N & Singh N. Neoadjuvant chemotherapy for epithelial ovarian cancer – role of apoptosis. Cancer Chemother Pharmacol 2005; 56:427-35. | 2005 |
| 85 | Gupta DK, Suri A, Mahapatra AK, Mehta VS, Sarkar C & Kumar L. When an unusual lesion occurs in an odd place. Spine J 2005;5(4):471-2. | 2005 |
| 86 | Kochupillai V, Kumar P, Singh D, Aggarwal Dhiraj, Bhardwaj N, Bhutani M & Das S. Effect of rhythmic breathing (Sudarshan kriya and Pranayam) on immune functions and tobacco addiction. Annals New York Acad of Sciences. 2005;1-11. | 2005 |
| 87 | Lokeshwar N, Kumar L & Kumari M. Severe bone marrow aplasia following imatinib mesylate in a patient with chronic myelogenous leukemia. Leuk & Lymph2005;46:781-784. | 2005 |
| 88 | Raina V, Lokeshwar N, A Sharma, G Bhatt, R Kumar. Whole blood collected after 4 days of filgrastim and reinfused after high dose myeloablative chemotherapy for various cancers is a safe and cost effective method of stem cell rescue.. Journal of Clinical Oncology 2005: 23 (16S); --- ( abstr ) | 2005 |
| 89 | Singh D & Kumar L. Myelomatous ascitis in multiple myeloma. Leuk & Lymphoma2005;46:631-632 (letter). | 2005 |
| 90 | Sharma A, Raina V, Lokeshwar N, Deo SV, Shukla NK, Rath GK. Multifractionated cisplatin, etoposide, and paclitaxel, (CEP) in unresectable gastric/ gastro esophageal (GE) cancer: Phase II study.. Journal of Clinical Oncology 2005: 23 (16S); 4203 ( abstr ) | 2005 |
| 91 | Arora B, Kumar L, Kumaru M, Sharma A, Wadhwa J & Kochupillai V. Therapy with imatinib mesylate for chronic myeloid leukemia. Ind J Med & Paed Oncology2005;26:5-18 | 2005 |
| 92 | Bakhshi S, Pautu JL. EBV associated hemophagocytic lymphohistiocytosis with spontaneous regression. Indian Pediatr 2005;42:1253-5. | 2005 |
| 93 | Bakhshi S, Sethuraman G, Singh MK, Arya LS. Atypical pyoderma gangrenosum as manifestation of childhood acute lymphoblastic leukemia. Pediatr Dermat 2005;22:543-5. | 2005 |
| 94 | Hariprasad R & Kumar L. Secondary surgical cytoreduction for advanced Ovarian Carcinoma. Ind J Med & Paed Oncology . 2005;26:28-30 (selected summary). | 2005 |
| 95 | Jain TP, Thulkar S, Saha S, Bakhshi S, Dominic J. Extensive pneumothorax, pneumomediastinum and surgical emphysema as a complication of bleomycin therapy. Pediatr Radiol 2005;35:1227-1229. | 2005 |
| 96 | Kotwal A, Thakur R, Seth T. Correlates of Tobacco Use pattern amongst adolescents in two schools of New Delhi, India. Indian Journal of Medical Sciences. June 2005; 59 (6): 243-253. | 2005 |
| 97 | Kumar L, Gangadharan VP, Raghunadha Rao D, Saikia T, Shah S, Malhotra H , Bapsy PP, Singh K & Rao R. study on the safety and efficacy of an indigenous recombinant interferon alpha-2b in chronic myeloid leukemia patients : results of a multicentric trial from India. Nat Med J India 2005. 18:66-70. | 2005 |
| 98 | Manju S, Bhutani M, Aggarwal D & Kochupillai V. Cancer Treatment: Role of Yoga, Naturopathy and Prayer. Ind Soc Health Admn. (ISHA), Vol. XVII:, No.1: 151-157, 2005. | 2005 |
| 99 | Mohan A, Guleria R, Pathak A, Bhutani M, Hemraj P, Mohan C, and Kochupillai V. Quality of life measures in lung cancer. Ind. J Cancer. Vol. 42, 125-132, 2005. | 2005 |
| 100 | Prasad R & Kumar L. Secondary surgical cytoreduction for advanced ovarian carcinoma. Ind J Med & Paed Oncology 2005; 26: 28-30 (selected summary). | 2005 |
| 101 | Raina V, Bhutani M, Bedi R, Sharma A, Deo SV, Shukla NK, Mohanti BK, Rath GK. Clinical features and prognostic factors of early breast cancer at a major cancer center in North India.. Indian J Cancer.2005 Jan-Mar;42(1):40-45. | 2005 |
| 102 | Sharma P, Mohanty S and Kumar L. A vaccine for chronic myeloid leukemia NatMed J India 2005;18:146-7. (selected summary ). | 2005 |
| 103 | Sharma A, Nilesh Lokeshwar. Febrile neutropenia in hematological malignancies. Journal of Post Graduate Medicine 2005; 51:S 42-48 (suppl). | 2005 |
| 104 | Uppal G, Raina V. Sharma A, Kumar R, Anand M, Khaitan BK, Grover JK. Use of simple hematological and biochemical and clinical parameters to monitor response of Multiple Myeloma Patients on High Dose Thalidomide therapy.. Indian Journal of Cancer2005;42(1) 46-50 | 2005 |
| 105 | Vimla N, Kumar L, Kumar S, Vijayraghwan M, Bhatla N, & Hariprasad R. granulosa cell tumours of ovary : variables affecting prognosis. Ind Jn Med & Paed Oncology 2005;26:12-19. | 2005 |
| 106 | Arya LS, Dinand V, Thavaraj V, Bakhshi S, Dawar R, Singh R, Vats TS. Hodgkin’s disease in Indian children: outcome with chemotherapy alone. Pediatr Blood Cancer 2006;46:26-34. | 2006 |
| 107 | Bakhshi S, Singh D, Karak AK, Thakur S. Childhood primary mesenteric seminoma. Ind. J. Pediatr. 2006; 73: 241-3. | 2006 |
| 108 | Bakhshi S, Joenje H, Schindler D, Oostra A, Mohamed AN, Madgy D, Ravindranath Y, Abella E. A case report of a patient with microcephaly, facial dysmorphism, mitomycin-c-sensitive lymphocytes, and susceptibility to lymphoma. Cancer Genet Cytogenet 2006;164:168-71. | 2006 |
| 109 | Medhi K, Kumar L, Sharma A, Raina V, Kochupillai V, Dawar R & Sreedhar E. Hairy cell leukemia: Experience at a Tertiary Cancer Centre in Northern India. Ind . J Med. & Paed. Onc. 2006; 27; 8-14. | 2006 |
| 110 | Kumar L, Vikram P & Kochupillai V. Recent advances in the management of multiple myeloma. The Nat. Med. J Ind. 2006: 19; 80-89. | 2006 |
| 111 | Bhutani M, Pathak AK, Mohan A, Guleria R, Kochupillai V. Extensive stage Small cell lung cancer: An update on chemotherapy. Ind. J Chest Dis Allied Sci. Vol. 48: 49-58, 2006 | 2006 |
| S.no | Name of the Project & Principal Investigator | Description of the Project |
|---|---|---|
| 1 | Fetal liver infusion: Further studies on the role of action of fetal liver cells on the regeneration of adult bone marrow: In vitro evaluation | Earlier studies conducted in our lab. demonstrated that fetal liver conditioned medium (FLCM) supported the colony growth of normal bone marrow as well as aplastic marrow. This suggested the presence of growth stimulatory cytokines in FLCM. Eliza studies revealed the presence of stem cell factor in 50% of FLCM samples. Subsequent studies revealed that Flt3 and IL-6 were also present in substantial number of FLCM samples. |
| 2 | Evaluation of thermal camera to detect early cancer: Collaborative project with Moscow | Russian scientists have produced a Camera which measures thermal changes in the body. Thermal changes occurring in superficial parts of body may be indicative of cancer. DST has identified IRCH, AIIMS as one of the centres where this camera could be evaluated to see, if cancer can be detected in its early stages. Two doctor team from IRCH, AIIMS has already visited Moscow and seen this camera. Now IRCH has procured this camera and has initiated the required work. |
| 3 | Effect of breathing techniques: Sudarshan Kriya in normal individuals and those with cancer in remission | Sudarshan kriya (SK) is a rhythmic breathing process, where 3 rhythms of breath are followed in cyclical fashion. This process has been introduced by H.H. Sri Sri Ravi Shankar. Studies conducted so far have shown that regular practice of Sudershan Kriya (SK) and Pranayam(P) introduces changes in electroencephalogram (EEG) consistent with the achievement of state of relaxed alertness. Fall in blood lactate in those practicing SK & P further confirms that state of relaxation is achieved. Also natural killer (NK) cells and antioxidant defence increases in the body This would raise the possibility that age related diseases may be reduced with these practices. Gene expression profiling revealed that process of scenescence may get delayed and risk of cancer may be less. Patients with breast cancer had fewer side effects to chemotherapy, better quality of life and better immune status. |
| 4 | Antioxidant Vitamins in lung cancer: | Current therapies for lung cancer are unsatisfactory. Despite using multiple chemotherapy combinations, response rates have been less than 40%; survival less than 10 months and one year survival often less than 40%. In vitro study carried out by us demonstrated increase in apoptosis when antioxidants were added to Carboplatin/Paclitaxel combination. Clinical study also showed improved response rates and longer survival although statistical difference could not be demonstrated. |
| 5 | “Common cancers: Perception and determinants of community behavior”. – Terry Fox Project | Description:- Under this project 10 focused group discussion (FGD) have been organized with community members, para medical workers, health workers and medical officers. These were organized in four districts of Delhi. Individual interviews with community members, para medical workers, health workers is also conducted in the same district. Interviews with medical officers, senior medical administrative officers and program planners is likely to finish in near future |
| 6 | Population screening programme for cancer of cervix, breast and oral cavity to (i) Determine the level of knowledge and skill of health workers in the use of low cost screening techniques for the detection of common cancers in the community (ii) Assess the effectiveness of training of health workers in the use of low cost screening techniques and (iii) Determine the supervisory and monitoring factors in a programme on the use of low cost screening techniques by health workers. | Description:- Under this project training program on awareness and cancer screening technique for common cancers i.e cervix, breast and oral cavity is being organized for the medical officers, para medical workers and health workers of CGHS and ESI. So far theoretical and practical training has been provided to 200 personnel. Program is on and target is to cover all personnel of above organization. Screening for cancer cervix is being run in association with various NGO’s. |
| 7 | Randomized study comparing upfront surgery followed by chemotherapy versus upfront chemotherapy followed by interval debulking surgery in previously untreated epithelial ovarian cancer stage III C and stage IV (pleural effusion only). | Between Oct. 2001 and Aug. 2006, 118 previously untreated patients of Stage IIIC & IV were randomized into two arms; Arm A (n=62) consisted of upfront debulking surgery followed by 6 cycles of Paclitaxel and Carboplatin. Arm B; upfront 3 cycles of chemotherapy followed by interval debulking surgery. Results: Patients in neoadjuvant arm had higher optimum debulking rate (p<0.001) and decreased blood loss. There was good correlation between CAT Scan findings and suboptimal debulking. Quality of life score (QOL) was higher in arm B. |
| 8 | Alpha interferon vs low dose Thalidomide as maintenance therapy following autologous stem cell transplant in patients with multiple myeloma: A randomized study | To reduce the risk of relapse, after autolo stem cell transplant we are performing a prospective ,study in which patients are randomized to receive either IFN- a 3 mU SC thrice a week for => one year or low dose thalidomide, 50 mg daily for =>one year. Between October 2002 and June 2004, 17 patients have been entered into the study (IFN- a - 8, thalidomide- 9). Therapy was started within 12 weeks of transplant. Patients are being followed regularly for any toxicity to above therapy and relapse. In one patient randomized to IFN-a arm , treatment could not be started due to low counts >3 months post transplant. In another patient IFN-a had to be stopped after 12 weeks due to intolerance. The major side effects to thalidomide were- constipation, drowsiness and mild neuropathy and skin rash in one patient. In IFN arm, - flu like symptoms were seen in almost all patients within first 2 to 6 weeks, followed by myelosuppression (grade I-II). All 17 patients continue to be alive till date. |
| 9 | Concomitant chemoradiation protocol for advanced and or unresectable squanous cell carcinoma of oropharynx and nasopharynx | The head and neck cancers constitute 5% of all cancers worldwide and 15% of all cancers in developing countries. Most of these patients present in advanced stages. There are areas in the head and neck region e.g. Nasopharynx and Oropharynx where surgery is not technically feasible or it is difficult and these cancers are treated with radical or palliative radiotherapy which is often supplemented with chemotherapy. A number of trials including meta analyses are available in the literature giving conflicting results whether addition of chemotherapy definitely adds to the improvement in survival or not. There is lack of published literature from India in this particular field. In the proposed study we, plan to study the safety and efficacy of chemoradiation (concomitant using single agent cispaltin) in unresectable squamous cell carcinoma of oropharynx and nasopharynx and to compare it with radical radiotherapy in a randomized fashion. |
| 10 | Efficacy and Adverse effects of Thalidomide and Prednisone in Hormone refractory prostate cancer | Prostate cancer is an important and increasing public health problem. In India incidence of prostate cancer is 4.5/ 1,00,000. However, it is the 3rd commonest cancer in males in Delhi. During the course of disease once the cancer becomes androgen independent or refractory there are limited options available. Angiogenesis has been identified as a key pathophysiological process that is important in growth, local invasiveness and metastasis of malignant tumors. Therefore, anti-angiogenic therapy represents one of the promising new approaches to anticancer therapy. Thalidomide is one such drug available in oral formulation and have limited side effects except teratogenecity. In this trial 50 hormone refractory metastatic prostate cancer patients will be recruited. |
| 11 | Gemcitabine, and Oxaliplatin in advanced/Unrespectable Adenocarcinoma of Gall Bladder: A phase II study | Gall bladder cancer is one of the commonest cancer in females in this part of country. Majority of these patients present in advanced and unresectable stage. Currently these patients of unresectable/ metastatic gall bladder cancer are treated with palliative RT, chemotherapy or just with analgesics. There are some initial reports about efficacy of Gemcitabine, and Oxaliplatin in these patients. The drugs are also available in India. As majority of our patients present with advanced stage it will be meaningful to test combination of Gemcitabine and Oxaliplatin as first line therapy in advanced/ unresectable adenocarcinoma of gall bladder. |
| 12 | In vitro expansion and establishment of human fetal liver hematopoietic stem cell line. | Fetal liver is the predominant site of hematopoiesis during mid gestation. Fetal liver infusion has been used to treat certain disorders like aplastic anemia (AA), acute myeloid leukemia (AML) and immunodeficiency syndrome., In previous study we have demonstrated the presence of putative growth factors (cytokines), such as stem cell factor (SLF), IL-6 and fms – like tyrosine kinase – (FLt-3) in fetal liver conditioned media. In the present project we plan to isolate fetal liver hematopoietic stem cells (FLHSC) expand these cells under in vitro culture condition and establish transformed and non-transformed cell lines. |
| 13 | An invitro study of antiproliferative and apoptotic effects of gefitinib on lung cancer cell lines. | Lung cancer is the leading cause of cancer death across the globe. Nearly 60% of people diagnosed with lung cancer die within one year and >75% within 2 years of their diagnosis. Recent data from the combination of newer agents plus platinum has shown a modest increase in survival for patients with advanced lung cancer. We plan to examine the effects of gefitinib alone and in combination with various chemotherapeutic drugs on the cell cycle. Cytotoxicity and apoptosis in lung cancer cell line. |
| 14 | Antioxidant as adjunct to chemotherapy of lung cancer: in vitro study. | In this study, we want to see the effects of antioxidants (Vitamin C, E & beta-carotene) in conjunction with standard chemotherapeutic agents in a number of lung cancer cell lines. As earlier in our study we have demonstrated that a mixture of antioxidants significantly enhance the apoptotic effect of chemotherapeutic agents paclitaxel and carboplatin on human lung cancer cell line. |
| 15 | Resistance to Imatinib Phositive Indian leukemia patients: Molecular mechanism. | Imatinib mesylate is a tyrosine kinase inhibitor that has now become the standard drug therapy for chronic myeloid leukemia in all phases of disease. But a cohort of patients either do not achieve a significant level of response or looses their best response.. In this project we aim to study what are the changes occurring at molecular level that are responsible for this type of resistance to Imatinib. |
| 16 | Expansion of adult human bone marrow and cord blood stem cells for reconstituting marrow and for reprogramming into hepatocytes. | With discovery of transdifferentiation ability of hematopoietic stem cells, cellular therapy is expected to become relatively simpler and versatile. Patient’s own born marrow cells can be utilized for the therapy avoiding immune rejection. It would be exciting to explore the possibility of candidates stem cell expansion, then ex vivo reprogramming them to partially different target cells and transporting into the hose (nude mice in our project). Beside bone marrow, cord blood is an excellent candidate for adult stem cells having primitive phenotype (CD 34+, CD38-, HLA-DR); has the potential for ex vivo expansion and cell therapy. In this project we target both cord blood and born marrow as a source of multipotent adult progenitor cells (MAPC). Characterization of MAPC, its ex vivo expansion and differentiation into hepatocytes will provide possible insight for transdifferentiation. In vivo experiments using nude mice will provide evidence of stem cell potential for homing engraftment and differentiation into hepatocytes |
| 17 | Treatment and characterization of acute lymphoblastic leukemia in children, adolescents and young adults | Enrolling patients of ALL <25 years age for diagnosis, immunophenotyping, treatment protocol and to study their biology using molecular markers. |
| 18 | G-CSF mobilized peripheral blood progenitor cell transplantation(allogeneic or autologous: A multicentric study. | Role of G-CSF in mobilization of stem cell in both autologous and allogeneic stem cell setting. So far 8 patients have been recruited. Initial results confirm the role of G-CSF (grastim) in mobilization of CD34 +ve cells. |
| 19 | Randomized comparison of ABVD with EVAP in newly diagnosed cases of Hodgkin’s lymphoma-protocol p-0402 | Most of Hodgkin’s Lymphoma (Disease) patients require combination chemotherapy. The available chemotherapy regimens include doxorubicin (adriamycin), bleomycin, vinblastine, decarbazine (ABVD) which is considered gold standard; COPP< MOPP-ABV etc. Whereas, the ABVD is one of the most effective combination majority of our patients find it difficult to afford. Alkylating based regimen like MOPP and COPP are usually associated with sterility in significant number of cases together with risk of secondary leukemia (malignancy). Hence, there is a need for a new regimen which may be as effective as ABVD, devoid of late side effects of alkylators and yet cheaper. Earlier we have shown effectiveness of etoposide, vinblastine, adriamycin, and prednisolone (EVA). Therefore, we plan to compare effectiveness of EVAP vis a vis ABVD in a prospective randomized fashion in newly diagnosed cases of Hodgkin’s lymphoma. Study was started in September 2004 and we are likely to complete accrual of 100 by October 2006. |
| 20 | Role of arsenic trioxide with ascorbic acid in treatment of multiple myeloma – a pilot study. | A Phase II study of role of arsenic trioxide with ascorbic acid in treatment of relapsed/refractory multiple myeloma is underway, a total of eight patients have been recruited and their evaluation is underway. A total 20 patients are intended for recruitment. |
| S.No | Name | Details |
|---|---|---|
| 1 | Bone marrow transplantation | Bone marrow transplantation is routinely being done at IRCH AIIMS since 1995. So far 350 transplants have been done. Primary indication for allogeneic BMT includes – CML and severe Aplastic anemia. For autologous stem cell transplant, major indications include – myeloma and Lymphomas. |
| S.No | Name of the Lab | Test done | Details & Rates | Cost |
|---|---|---|---|---|
| 1 | Medical Oncology | RT-PCR / Quantitative PCR | For BCR Abl translocation (p210, p190) | Rs. 2200/ test |
| Cytogenetics | For Philadelphia Chromosome | Rs. 500/ test | ||
| Haemogram | Complete blood counts | Rs. 30/ test | ||
| Flow cytometeric analysis | CD 34 counts | Rs. 1200 / test | ||
| Harvesting and cryopreservation | Storage of stem cells at 80°C | Rs. 32000/ Cycle | ||
| Harvesting and cryopreservation | Storage of stem cells at 196°C | Rs. 38000 / Cycle | ||
| ELISA for galactomannan | - | NIL |
| S.No | Unit | No. of Beds |
|---|---|---|
| 1 | Medical Oncology | 30 |
| 2 | DayCare | 30 |
| 3 | BMT | 8 |
| S.No | Name of the OPD/Unit | Day/Time |
|---|---|---|
| 1 | Chemotherapy Evaluation | Monday 9AM onwards
Wednesday 9AM onwards
Thursday 9AM onwards
Friday 9AM onwards |
| 2 | LL Clinic (Lymphoma/Leukemia) | Wednesday 2 PM onwards
Thursday 2 PM onwards |
| 3 | Breast Clinic | Monday 2 PM onwards
Friday 2 PM onwards |
| 4 | GE Clinic | Wednesday 2 PM onwards |
| 5 | H & N clinic | Monday 2 PM onwards Friday 2 PM onwards |
| 6 | Gynae. Cancer Clinic | Wednesday 2 PM onwards
Saturday 9AM onwards |
| 7 | Ophthalmic tumour Clinic | Thursday 3.30 PM onwards |
| 8 | BMT Clinic | Friday 9 AM onwards |
| 9 | Bone & Soft Tissue Clinic | Thursday 2 PM onwards |
| 10 | Urology Clinic | Thursday 11 AM onwards |
| 11 | Pediatric Surgery clinic | Thursday 2 PM onwards |
| 12 | Lung Cancer Clinic | Tuesday & Friday 9 AM to 1 PM |
| S.N | Name of the Course | Details of Admission |
|---|---|---|
| 1 | Ph.D Medical Oncology | All India Open Entrance Examination |
| 2 | DM Medical Oncology | All India Open Entrance Examination |
The focus area of research is medical image optimisation, radiation safety, quality assurance in imaging, imaging services and total quality management. We are working on Dual Energy CT based characterisation and also development of new thermoluminescent and optically stimulated luminescent phosphor so that accurate radiation dosimetry may be accomplished in patients, staff and public.
| S. No | Name | Detail |
|---|---|---|
| 1 | Blood Bag Irradiation Facility | Blood and blood products are irradiated before transfusion to prevent Transfusion-related Graft versus Host Disease (TA-GVHD). The patients with bone marrow transplantation, hematologic cancer, high-dose chemotherapy are at risk of TA-GVHD besides certain other non-oncologic settings (congenital immunodeficiency, Cardiac surgery, etc.) |
| 2 | Quality Assurance Gadgets | Various medical imaging equipment need periodic quality assurance checks and radiation safety measurements. We conduct, train, and carry out research in QA and radiation protection aspects of units like radiography, CT, mammography, DEXA, c-arm, fluoroscopy, US, etc. |
| 3 | Radiation Dosimetry Equipment | Thermoluminescence and Optical Stimulated Luminescence Radiation Dosimetry, other radiation dosimetry and radiation detection gadgets. |
| S. No | Computer Programs Developed | Description |
|---|---|---|
| 1 | Information modules for cancer patients | Computer-based general and cancer-specific multimedia modules have been developed which give all the relevant information to the public and cancer patients. It can be run in patient waiting areas, on the web, home, or corporate offices. |
| 2 | RADPREG | This menu-based educational program deals with a variety of aspects on the effects of radiation on early conception, organogenesis, carcinogenic effects, mental development & so on, dose-effect relationships, accidental exposure in pregnancy, female radiation workers and pregnancy. The program has been written in BASIC language. |
| 3 | RISKEST | A program for calculation of somatic & genetic risk probability after exposure to a known amount of radiation dose. The program has been written in Quick Basic. |
| 4 | FETAL DOSE | Program for calculation of radiation dose to uterus or fetus in routine diagnostic radiological procedure. The dose can be calculated for individual cases. Written in FOXPRO. |
| 5 | PT DOSE | Educational program for inferring the radiation doses in diagnostic procedures expressed in multiple chest x-rays risk estimate. Written in Story Board. |
| 6 | PT RISK | Program for calculation of somatic & genetic risk in diagnostic exposure. Written in BASIC and FOXPRO. |
| S. No | Name of Training | Details for Admission |
|---|---|---|
| 1 | Comprehensive training programme in Diagnostic Medical Physics | Maximum duration two months, Forms available from registrar, AIIMS. Open throughout the year. Training fee = Rs. 1000. Medical Physicists, Radiologists and Imaging technologists are eligible. No accommodation provided. For details contact: Medical Physics Unit, IRCH, AIIMS |
| 2 | MD Radiology | Basics of Radiation Physics and its application to radiology. |
| 3 | B.Sc. (Hons.) Radiography | Radiation Physics, Radiation protection and Image Quality. Details in Dept. of Radiology |
| S. No | Name of Course | Details for Admission |
|---|---|---|
| 1 | Ph.D (Medical Physics) | Eligibility: M.Sc (physics) or M.Sc. (Medical Physics) with relevant exposure to Diagnostic Medical Physics. Entrance exam is conducted by AIIMS twice in a year (Jan. & July). |
11th TCS Annual Meeting and Workshop 2018 (October 30-31st, 2018 & November 1, 2018)
Since its inception in 2005, The Cytometry Society-India (TCS) has been actively involved in dissemination of knowledge and updation of state-of-the-art flow cytometry technology by interactive sessions with international and national experts and organized hands-on-training. Laboratory Oncology Unit, Dr BRA IRCH, AIIMS, New Delhi takes pride for hosting the 11th TCS annual conference and workshop, 2018. In this upcoming 4 days multidimensional and multifaceted flow cytometry conference, both the basic and clinical faculty will share valuable insights from application-oriented translational and applied research as well as the use of this technology at diagnostic front. The flow cytometry workshop will include hands-on-training in MRD analysis, transplant Immunology, multi-parametric flow cytometry and cell sorting for young researchers and faculty.
CME series on Hemato-Oncopathology , July 23-24, 2016
The Laboratory Oncology Unit organized the CME on recent advances in Hemato-Oncopathology. This program provided a unique platform for medical practitioners to meet and exchange ideas and information on the most recent innovations, trends, and concerns with the experienced faculty of internationally recognized authorities in the fields of hematology and oncopathology. This meeting provided an opportunity for better understanding and management of leukemia, lymphoma, and plasma cell myeloma. The guidelines, recommendations, and expert opinions presented here were an amalgamation of the current information with the pre-existing knowledge.
7th Annual TCS meeting and 15th Indo-US Clincal Cytometry Workshop, 2014
The focus of this workshop was to update the participants on their knowledge in flowcytometry. The topics varied from basic sciences and multi-color clinical flow cytometry with emphasis on detection of minimal residual disease in acute leukemia.
2nd National CME cum Workshop in Hemato-oncopathology 2002
The Laboratory Oncology Unit organized the second CME cum Workshop in Hemato-oncopathology from October 3-5, 2002 with an aim to improve the diagnostic skill and awareness of pathologists and hematologists in the field of hematological malignancies. One hundred and forty delegates from almost every state of the country registered for the program. On the first two days the emphasis was on practical approach to diagnosis of leukemias and lymphomas. Gray areas in hemato-oncopathology were illustrated with suitable case studies. On the third day basic principles of flow cytometry were discussed in detail and case studies incorporating morphology, cytochemistry and flow cytometry were discussed with all participants.
1st National CME cum Workshop in Hemato-oncopathology 1998
The workshop was aimed at hematopathologists working in peripheral medical colleges, the objective being to introduce them to the setting up of a myeloma laboratory and also to discuss a few common hematological conditions that are commonly misdiagnosed. For the former, some 60 electrophoresis and immunofixation plates (each with 8 serum/urine samples) were shown and individually discussed with all the participants. For the latter several peripheral blood or bone marrow slides exemplifying each of the three conditions were first seen by all participants. They were then discussed threadbare with all participants by means of projection slides.
Alam MT, Ali MS, Goel H, Singh J, Chatterjee B, Bose S, Hadda V, Chopra A. Expression Profile, Molecular Association, and Clinical Significance of POLD4 in Glioblastoma. Cell Mol Neurobiol. 2023;43:3753-3765.
Anticancer Agents Med Chem. 2023 Sep 8.
Choudhary S, Ganguly S, Palanichamy JK, Singh A, Pradhan D, Bakhshi R, Chopra A, Bakhshi S. Mitochondrial gene expression signature predicts prognosis of pediatric acute myeloid leukemia patients. Frontiers in Oncology. 2023;13:1109518.
Controlled Trials. J Pediatr Hematol Oncol. 2023 Oct 1;45(7):361-369. doi: 10.1097/MPH.0000000000002737. Epub 2023 Aug 3. PMID: 37539996.
Harshita Dubey, Amar Ranjan, Anil Sharma, Swati Gupta, Khushi Tanwar, Saransh Verma, Leena Gupta, Pranay Tanwar, Anita Chopra, Arvind Kumar, Harsh Goel, Diagnostic role of TTF1 expression in a case of carcinoma of unknown primary, Am. J. Transl. Res. Accepted on March 01, 2023, IF 2.52, Cite Score 3.0.
hotspot mutation by droplet digital PCR in breast cancer among Indian population. Cancer Cell Int. 2023 Oct 11;23(1):236.
Rawal N, Awasthi S, Dash NR, Kumar S, Das P, Ranjan A, Chopra A, Khan MA, Saluja S, Hussain S, Tanwar P. Prognostic relevance of PDL1 and CA19-9 expression in gall bladder cancer vs inflammatory lesions. Curr Oncol. 2023;30:1571-1584.
receptor-like factor 2 in pediatric B-lineage acute lymphoblastic leukemia. Am J Cancer Res. 2023 Jun 15;13(6):2452-2470. PMID: 37424808; PMCID: PMC10326580
Ongoing funded Extramural/Intramural projects P
The IRCH laboratory Oncology Unit accepts referrals for detailed work-up of leukemia and myeloma from not only IRCH but also the AIIMS main hospital. To facilitate the work of clinical residents, there is only one referral form (white) for all specializedhematological investigations, which can be obtained from Room No. 8, ground floor, IRCH. This form must be sent with every sample (except hemogram) and should be complete with patient registration and clinical details. Clarification and reports can be readily had over the telephone.
The Laboratory Oncology Unit accepts referrals for detailed work-up of leukemia and myeloma from not only IRCH but also the AIIMS main hospital. To facilitate the work of clinical residents, there is only one referral form (white) for all specialized hematological investigations. Some of the investigations that are available from this laboratory include the following: Complete blood counts, peripheral blood smear, bone marrow aspiration and touch smear examination with cytochemistry, High resolution serum and urine protein electrophoresis, immunofixation studies, serum free light chain assay, Tumour markers, molecular studies for hemato-lymphoid malignancies, multiparametric flow cytometry of blood, bone marrow and body fluids with minimal residual disease estimation and testing for high-risk HPV.
| Year | Name | |
|---|---|---|
| - | Dr. T R Kannan | - |
| - | Dr. Joytsana | - |
| - | Dr. Manas Panigrahai | - |
| - | Dr. Seema Mishra | - |
| - | Dr. Asootosh | - |
| - | Dr. Amit Singhal | - |
| - | Dr. Anirbhan Chowdhary | - |
| - | Dr. Girija Prasad Rath | - |
| - | Dr. Mohan Gurjar | - |
| - | Dr. Rajeev Ranjan | - |
| - | Dr. Anurag Aggarwal | - |
| - | Dr. Prashant Nasa | - |
| - | Dr. Prem | - |
| 2007 | Dr. Deepak Gupta | andg@rediffmail.com |
| 2007 | Dr. Madhu | - |
| 2008 | Dr. Himanshu Chauhan | drhimanshuchauhan@gmail.com |
| 2008 | Dr. Surjya Prasad Upadhyay | run77in@yahoo.com |
| 2008 | Dr. Roopesh Jain | mdroopesh@yahoo.com |
| 2008 | Dr. Himanshu Khurana | himanshuuzz@doctor.com |
| 2008 | Dr. Gaurav N Goyal | drgauravgoyal@rediffmail.com |
| 2008 | Dr. Sanjeev Kumar | sanjivkumarsharma@hotmail.com |
| 2008 | Dr. Ravi Agrawal | swatiraviagrawal@yahoo.com |
| 2008 | Dr. Rajnish Kumar | drraj76pmch@yahoo.co.in |
| 2008 | Dr. Prakash | pkcd@yahoomail.com |
| 2008 | Dr. Shiv Pratap Singh Rana | sps_rana2k@yahoo.com |
| 2008 | Dr. Siddharth Sharma | sidds_docin@rediffmail.com |
| 2008 | Dr. Daksha Bhaiya | sushilnagpur001@yahoo.co.in |
| 2009 | Dr. Arif Ahmed | drarifahmed1978@gmail.com |
| 2009 | Dr. Sandeep Khanna | - |
| 2009 | Dr. Roshni | - |
| 2009 | Dr. Deepa Khurana | drdeepa.khurana@gmail.com |
| 2009 | Dr. Charu | canbera21@gmial.com |
| 2010 | Dr. Rahul Gupta | rahulgupta.md@gmail.com |
| 2010 | Dr. Mahmood | syedmehmood2k8@gmail.com |
| 2010 | Dr. Alka Bhatnagar | dralkabhatnagar@gmail.com |
| 2010 | Dr. Frenny N Philip | frennyp@gmail.com |
| 2010 | Dr. Vikas Gogia | vikasgogs@yahoo.com |
| 2011 | Dr. Saurabh Joshi | soshijo@gmail.com |
| 2011 | Dr. Irfanul Haque | mdirfanulhaque@gmail.com |
| 2012 | Dr. Gaurav Chanana | icydoc@gmail.com |
| 2012 | Dr. Vivek Shrivasatava | vivek_dr999@yahoo.co.in |
| 2012 | Dr. Megha Pruthi | dr.meghapruthi@gmail.com |
| 2013 | Dr. Komal Joshi | drkomaljoshi@gmail.com |
| 2013 | Dr. Vidhi Mahendru | vidhimahendru1@gmail.com |
| 2013 | Dr. Megha Sharma | dr.sharmamegha@yahoo.com |
| 2013 | Dr. Komal | drkomaljoshi@gmail.com |
| 2009 | Dr. Deepa Khurana | drdeepa.khurana@gmail.com |
| 2009 | Dr. Charu | canbera21@gmial.com |
| 2010 | Dr. Rahul Gupta | rahulgupta.md@gmail.com |
| 2010 | Dr. Mahmood | syedmehmood2k8@gmail.com |
| 2010 | Dr. Alka Bhatnagar | dralkabhatnagar@gmail.com |
| 2010 | Dr. Frenny N Philip | frennyp@gmail.com |
| 2010 | Dr. Vikas Gogia | vikasgogs@yahoo.com |
| 2011 | Dr. Saurabh Joshi | soshijo@gmail.com |
| 2011 | Dr. Irfanul Haque | mdirfanulhaque@gmail.com |
| 2012 | Dr. Gaurav Chanana | icydoc@gmail.com |
| 2012 | Dr. Vivek Shrivasatava | vivek_dr999@yahoo.co.in |
| 2012 | Dr. Megha Pruthi | dr.meghapruthi@gmail.com |
| 2013 | Dr. Komal Joshi | drkomaljoshi@gmail.com |
| 2013 | Dr. Vidhi Mahendru | vidhimahendru1@gmail.com |
| 2013 | Dr. Megha Sharma | dr.sharmamegha@yahoo.com |
| 2013 | Dr. Komal | drkomaljoshi@gmail.com |
| 2014 | Dr. Prasanna Vani | prasna.vani@gmail.com |
| 2014 | Dr. Shalini Saini | drshalinisaini28@gmail.com |
| 2014 | Dr. Kalpajit Dutta | kalpajit.dutta@gmail.com |
| 2015 | Dr. Anuja Pandit | anujapandit@yahoo.co.in |
| 2015 | Dr. Ambika Bairwa | doc_ambika@yahoo.co.in |
| 2015 | Dr. Sofia Batool | batoolsofia@gmail.com |
| 2015 | Dr. Rohini Dattatri | rdattatri2@gmial.com |
| 2015 | Dr. Anuradha Bansal | bansal.a.1988@gmail.com |
| 2015 | Dr. Anuradha Patel | patelanuradha20@gmail.com |
| 2015 | Dr. Mahima Gupta | mahhima@gmail.com |
| 2015 | Dr. Siddharth | sidharth_doc@yahoo.co.in |
| 2015 | Dr. Silvy Anna Varughese | drsilvyann@gmail.com |
| 2015 | Dr. Kinshuki | dockinshukijain@gmail.com |
| 2015 | Dr. Prashant Sirohiya | s_prasant22@yahoo.com |
| 2015 | Dr. Wasimul Huda | wasu077@gmail.com |
| 2016 | Dr. Rudranil Nandi | drrudranilnandi@gmail.com |
| 2016 | Dr. Richa Prabhakar | pathakricha@yahoo.co.in |
| 2016 | Dr. Praneeth Suvvari | praneethsuv@gmail.com |
| 2016 | Dr. Nandan Choudhary | drnandanchy@gmail.com |
| 2016 | Dr. Nupur Abrol | nupur.abrol@gmail.com |
| 2016 | Dr. Manoj Kumar Ray | ray4manoj@gmail.com |
| 2016 | Dr. Anupama Tomer | dr.anupama.tomer@gmail.com |
| 2016 | Dr. Shagun | shagunchahal123@gmail.com |
| 2016 | Dr. Chandan Sahu | dr.sahuchandan@gmail.com |
| 2016 | Dr. Vishnu Garg | drvishnugarg7686@gmail.com |
| 2017 | Dr. Varnika | varnika.mihas@yahoo.in |
| 2017 | Dr. Kokila | kokila.chinnathambi@gmail.com |
| 2017 | Dr. Anuradha Patel | patelanuradha20@gmail.com |
| 2017 | Dr. Dimple Pandey | truegemini21@gmail.com |
| 2017 | Dr. Astha | koolestastha@gmail.com |
| 2017 | Dr. Ajisha Abubakker | aaji.008@gmail.com |
| 2017 | Dr. Shikhar More | shikharmore@gmail.com |
| 2017 | Dr. Sakshi Thakore | drsakshiarora88@gmail.com |
| 2017 | Dr. Priodarshi | dr.priodarshi@gmail.com |
| 2017 | Dr. Gautam Modak | gautam.modak312@gmail.com |
| 2017 | Dr. Manisha Pandey | manishapandey29122015@gmail.com |
| 2017 | Dr. Preeti | preetielegant2004@gmail.com |
| 2017 | Dr. Kritika Agrawal | krikika.agrawal.4@gmail.com |
| 2017 | Dr. Rahul D Arora | xerxes85@ymail.com |
| 2016 | Dr. Nandan Choudhary | drnandanchy@gmail.com |
| 2016 | Dr. Nupur Abrol | nupur.abrol@gmail.com |
| 2016 | Dr. Manoj Kumar Ray | ray4manoj@gmail.com |
| 2016 | Dr. Anupama Tomer | dr.anupama.tomer@gmail.com |
| 2016 | Dr. Shagun | shagunchahal123@gmail.com |
| 2016 | Dr. Chandan Sahu | dr.sahuchandan@gmail.com |
| 2016 | Dr. Vishnu Garg | drvishnugarg7686@gmail.com |
| 2017 | Dr. Varnika | varnika.mihas@yahoo.in |
| 2017 | Dr. Kokila | kokila.chinnathambi@gmail.com |
| 2017 | Dr. Anuradha Patel | patelanuradha20@gmail.com |
| 2017 | Dr. Dimple Pandey | truegemini21@gmail.com |
| 2017 | Dr. Astha | koolestastha@gmail.com |
| 2017 | Dr. Ajisha Abubakker | aaji.008@gmail.com |
| 2017 | Dr. Shikhar More | shikharmore@gmail.com |
| 2017 | Dr. Sakshi Thakore | drsakshiarora88@gmail.com |
| 2017 | Dr. Priodarshi | dr.priodarshi@gmail.com |
| 2017 | Dr. Gautam Modak | gautam.modak312@gmail.com |
| 2017 | Dr. Manisha Pandey | manishapandey29122015@gmail.com |
| 2017 | Dr. Preeti | preetielegant2004@gmail.com |
| 2017 | Dr. Kritika Agrawal | krikika.agrawal.4@gmail.com |
| 2017 | Dr. Rahul D Arora | xerxes85@ymail.com |
| 2017 | Dr. Shilpi Agarwal | drshilpi87@gmail.com |
| 2017 | Dr. Rohini Dattatri | rdattatri2@gmail.com |
| 2017 | Dr. Mahima Gupta | mahima@gmail.com |
| 2017 | Dr. Abhity Gulia | drabhity.mamc@gmil.com |
| 2018 | Dr. Alka Yadav | alkayadava@gmail.com |
| 2018 | Dr. Ankita | ankita2090@gmail.com |
| 2018 | Dr. Himanshu Prince Yadav | drhimanshuprince@gmail.com |
| 2018 | Dr. Swarnbala Solanki | drswarnbalasolanki@gmail.com |
| 2018 | Dr. Goyir Gangkak | goyir.gangkak@gmail.com |
| 2018 | Dr. Tuhin Mistry | tm.tuhin807@gmail.com |
| 2018 | Dr. Akansha Sangwan | akansha_sangwan@yahoo.com |
| 2018 | Dr. Aditya | adi.gatsby@hotmail.com |
| 2018 | Dr. Deepti Ahuja | deeptiahuja2252@gmail.com |
| 2018 | Dr. Sapna Singla | sapnasingla08@gmail.com |
| 2018 | Dr. Aditi Suri | aditisuri18@gmail.com |
| 2018 | Dr. Shruti Garolia | shrutigarolia@gmail.com |
| 2018 | Dr. Kiran Mahendru | kiranmahendru.aol@gmail.com |
| 2019 | Dr. Amrit Kaur | kauramrit.25@gmail.com |
| 2016 | Dr. Nandan Choudhary | drnandanchy@gmail.com |
| 2016 | Dr. Nupur Abrol | nupur.abrol@gmail.com |
| 2016 | Dr. Manoj Kumar Ray | ray4manoj@gmail.com |
| 2016 | Dr. Anupama Tomer | dr.anupama.tomer@gmail.com |
| 2016 | Dr. Shagun | shagunchahal123@gmail.com |
| 2016 | Dr. Chandan Sahu | dr.sahuchandan@gmail.com |
| 2016 | Dr. Vishnu Garg | drvishnugarg7686@gmail.com |
| 2017 | Dr. Varnika | varnika.mihas@yahoo.in |
| 2017 | Dr. Kokila | kokila.chinnathambi@gmail.com |
| 2017 | Dr. Anuradha Patel | patelanuradha20@gmail.com |
| 2017 | Dr. Dimple Pandey | truegemini21@gmail.com |
| 2017 | Dr. Astha | koolestastha@gmail.com |
| 2017 | Dr. Ajisha Abubakker | aaji.008@gmail.com |
| 2017 | Dr. Shikhar More | shikharmore@gmail.com |
| 2017 | Dr. Sakshi Thakore | drsakshiarora88@gmail.com |
| 2017 | Dr. Priodarshi | dr.priodarshi@gmail.com |
| 2017 | Dr. Gautam Modak | gautam.modak312@gmail.com |
| 2017 | Dr. Manisha Pandey | manishapandey29122015@gmail.com |
| 2017 | Dr. Preeti | preetielegant2004@gmail.com |
| 2017 | Dr. Kritika Agrawal | krikika.agrawal.4@gmail.com |
| 2017 | Dr. Rahul D Arora | xerxes85@ymail.com |
| 2017 | Dr. Shilpi Agarwal | drshilpi87@gmail.com |
| 2017 | Dr. Rohini Dattatri | rdattatri2@gmail.com |
| 2017 | Dr. Mahima Gupta | mahima@gmail.com |
| 2017 | Dr. Abhity Gulia | drabhity.mamc@gmil.com |
| 2018 | Dr. Alka Yadav | alkayadava@gmail.com |
| 2018 | Dr. Ankita | ankita2090@gmail.com |
| 2018 | Dr. Himanshu Prince Yadav | drhimanshuprince@gmail.com |
| 2018 | Dr. Swarnbala Solanki | drswarnbalasolanki@gmail.com |
| 2018 | Dr. Goyir Gangkak | goyir.gangkak@gmail.com |
| 2018 | Dr. Tuhin Mistry | tm.tuhin807@gmail.com |
| 2018 | Dr. Akansha Sangwan | akansha_sangwan@yahoo.com |
| 2018 | Dr. Aditya | adi.gatsby@hotmail.com |
| 2018 | Dr. Deepti Ahuja | deeptiahuja2252@gmail.com |
| 2018 | Dr. Sapna Singla | sapnasingla08@gmail.com |
| 2018 | Dr. Aditi Suri | aditisuri18@gmail.com |
| 2018 | Dr. Shruti Garolia | shrutigarolia@gmail.com |
| 2018 | Dr. Kiran Mahendru | kiranmahendru.aol@gmail.com |
| 2019 | Dr. Amrit Kaur | kauramrit.25@gmail.com |
| 2019 | Dr. Shreya Das Adhikari | drshreyadasadhikari@gmail.com |
| 2019 | Dr. Niyati Arora | drnitiarora@gmil.com |
| 2019 | Dr. Gayanendra Kumar | Gyanenkumar@yahoo.com |
| 2019 | Dr. Pradeep Parmar | drpksparmar@yahoo.com |
| 2019 | Dr. Nitish Thakur | nitishthakur@outlook.com |
| 2019 | Dr. Raunak Chakraborty | raunaq.chakraborty@gmail.com |
| 2019 | Dr. Swati Choudhary | drswati90@gmail.com |
| 2020 | Dr. Ankita | anki.dhir08@yahoo.co.in |
| 2020 | Dr. Meet Minarey | drmeetminarey@rediffmail.com |
| 2020 | Dr. Amit Kumar | amit2007kr@gmail.com |
| 2020 | Dr. Jadhav Ramanand Vijayanand | rvj4me@gmail.com |
| 2020 | Dr. Kanika Rustagi | drkanika1@gmail.com |
| 2020 | Dr. Vikram | vps1907@gmail.com |
| 2020 | Dr. Manisha | manishapandey29122015@gmail.com |
| 2020 | Dr. Preeti | preetielegant2004@gmail.com |
| 2021 | Dr. Deepti Ahuja | deeptiahuja2252@gmail.com |
| 2021 | Dr. Abhishek Kumar | abhishekk73102@gmail.com |
| 2021 | Dr. Aditi Suri | aditisuri18@gmail.com |
| 2021 | Dr. Shweta | drshweta2309@gmail.com |
| 2021 | Dr. Sapna Singla | sapnasingla08@gmail.com |
| 2021 | Dr. Aditya | adi.gatsby@hotmail.com |
| 2021 | Dr. Vishnu Panwar | vishnupanwar6767@gmail.com |
| 2021 | Dr. Swati Choudhary | drswati90@gmail.com |
| 2021 | Dr. Nidhi Gupta | nidhi790@gmail.com |
| 2021 | Dr. Neha Singh | nehasingh140792@gmail.com |
| 2021 | Dr. Bhanu Pratap | bhanumaurya9@gmail.com |
| 2021 | Dr. Neethu Susan Abraham | neethu.march30@gmail.com |
| 2021 | Dr. Swagta Biswas | manibiswas58@gmail.com |
| 2022 | Dr. Alka Yadav | alkayadava@gmail.com |
| 2022 | Dr. Jitender Sirohiya | dr.jitendersirohiya@gmail.com |
| 2022 | Dr. Priyanka Dixit | pridixit1005@gmail.com |
| 2022 | Dr. Ayushi Agarwal | ayushiagarwaldr@gmail.com |
| 2022 | Dr. Shallu Goel | goel.shallu90@gmail.com |
| 2022 | Dr. Madhu Smita | madhusmita.gmc@gmail.com |
| 2022 | Dr. Surjyendu Ghosh | surja.rgkmch@gmail.com |
| 2022 | Dr. Bora Hemalatha | borahemalatha@gmail.com |
| 2022 | Dr. Jasmeet Gill | jess.scorpio@gmail.com |
| 2022 | Dr. Raghav Gupta | raghavgupta88@gmail.com |
| 2022 | Dr. Sonal | lanos.yadav1027@gmail.com |
| 2022 | Dr. Renoxy Bansal | renoxybansal@gmail.com |
| 2022 | Dr. Karthik P. Vasist | karthikpvasist@gmail.com |
| 2022 | Dr. Pavneet Kochar | neet.kochar7555@gmail.com |
| 2022 | Dr. Puneet Rathore (PM) | puneet.spmc@gmail.com |
| 2022 | Dr. Krishan Priya | krishnapriyasreelakam1992@gmail.com |
| 2022 | Dr. Bhawesh | bhawesh.pangaria@gmail.com |
| 2022 | Dr. Sanjeev Kumar | strongindians@gmail.com |
| 2022 | Dr. Vasudha Ahuja | vasudha.ahuja26@gmail.com |
| 2022 | Dr. Rabiya Abdu Razak | rabiya.malayil@gmail.com |
| 2022 | Dr. Khushboo Pandey | khushboo0411@gmail.com |
| 2022 | Dr. Ruchi Singh | instantruchi@gmail.com |
| 2022 | Dr. Bikash Anand | bikash.jovial@gmail.com |
| 2022 | Dr. Mahajan Jitendra Subhash | jitendrassm@gmail.com |
| 2023 | Dr. Pratishtha Yadav | Pratishthayadav88@gmail.com |
| 2023 | Dr. Prateek Kumar Maurya | zprateekmaurya@gmail.com |
| 2023 | Dr. Ankit Sharma | ankitmame@gmail.com |
| 2023 | Dr. Ajit Raj Verma | ajitrajverma99@gmail.com |
| 2023 | Dr. Nengneivahh Haokip | vahsyzongku@gmail.com |
| 2023 | Dr. Alice | dralicethankachan@gmail.com |
| 2023 | Dr. Pratyasa Padhi | pratyasa95@gmail.com |
| 2023 | Dr. Anurag Sarkar | dr.anuragsarkar@gmail.com |
| S. No. | Name | Batch | Chief guide Name | Thesis Title |
|---|---|---|---|---|
| 1. | Dr. Nandan Choudhary | July, 2016-19 | Dr. Seema Mishra | "Prevalence of breakthrough cancer pain and its impact on quality of life in cancer patients at regional cancer center, India: A cross-sectional study. |
| 2. | Dr. Puneet | July, 2016-19 | Dr. Sushma Bhatnagar | "To study and analyze the pattern of symptoms of patients presenting in palliative care ward at regional cancer center of india. |
| 3. | Dr. Astha Koolwal | January, 2017-20 | Dr. Seema Mishra | "Assessment of Pallivtive care outcome in patients of multiple myeloma attending the palliative care clinic of a tertiary care centre: A prospective observational study. |
| 4. | Dr. Ajisha P.A | January, 2017-20 | Dr. Sushma Bhatnagar | Prevalence and factors affecting dyspnoea in advanced cancer patients attending tertiary cancer hospital in india. |
| 5. | Dr. Vikram | July, 2017-20 | Dr. Seema Mishra | "Assessment of palliative care outcome in patients of gastro intestinal malignancies attending the palliative care clinic of a tertiary care centre: A prospective observational study. |
| 6. | Dr. Manisha | January, 2017-20 | Dr. Sushma Bhatnagar | "Comparison of intervention with analgesics versus analgesics alone in patients with head and neck malignancy in terms of pain relief and quality of life at 3 months follow up: A prospective randomized study |
| 7. | Dr. Neha Singh | January, 2018-21 | Dr. Seema Mishra | "Assessment of symptom burden and quality of Life in patient of advanced breast cancer in india population: A cross-sectional study |
| 8. | Dr. Bhanu Pratap | January, 2018-21 | Dr. Sushma Bhatnagar | "End of life care practices at tertiary cancer centre in india: An observational study. |
| 9. | Dr. Neethu Susan Abraham | July, 2018- | Dr. Seema Mishra | "Quality of life and symptom burden inpatients with hematological malignancies receiving Hematopoietic stem cell transplantation:A Prospective Observational Study |
| 10. | Dr. Rabiya Abdu Razak | July, 2018- | Dr. Sushma Bhatnagar | "A clinical correlations between COPN with deficiency to vitamin B12 D 3 and calcium. |
| 11. | Dr. Bikash Anand | January, 2019- | Dr. Sushma Bhatnagar | "Assessment of symptom burden and QOL in patient of Malignant bowel obstruction in tertiary care center: Observastion study |
| 12. | Dr. Krishan Priya | January, 2019- | Dr. Sushma Bhatnagar | "Pattern of patients presenting with malignant spinal cord comressionin palliative care unit. |
| 13. | Dr. Bhawesh | January, 2019- | Dr. Seema Mishra | "Symptom assessment in pediatric malignancies ina tertiary care centre in india. |
| 14. | Dr. Sanjeev Kumar | July, 2019- | Dr. Seema Mishra | "Assessment of Symptom Burden and quality of Life in Patients of Lung Cancer attending the palliative care clinic of a tertiary care centre: A Prospectice observational study. |
| 15. | Dr. Ajit Raj Verma | January, 2020- | Dr. Seema Mishra | "Assessment of symptom burden and quality of life in patients of advanced head and neck cancer receiving palliative care at tertiary care centre, India: A prospective observational study. |
| 16. | Dr. Nengneivah Haokip | January, 2020- | Dr. Sushma Bhatnagar | "To study the effect of oral morphine prescribed for dyspnoca in cancer patients presenting to the departments of Onco-anaesthesia and palliative medicine and pulmonary medicine and sleep disorders in a tertiary care hospital in india: A prospective abservational study. |
| 17. | Dr. Alice | January, 2020- | Dr. Rakesh Garg | "Palliative care needs, symptom burden and quality of life in advanced sarcoma patients presenting to palliative medicine clininc- A cross sectional study. |
| 18. | Dr. Pratyasa Padhi | July, 2020- | Dr. Vinod Kumar | "Assessment of symptom burden and quality of life in Patients of primary brain tumor, attending palliative care unite of a tertiary care center: A prospective observation study. |
| 19. | Dr. Anurag Sarkar v | July, 2020- | Dr. Sachidanand Jee Bharati | "Impact of intravenous iron therapy on fatigue and quality of life in cancer patient receiving palliative care: A prospective interventional study |
| 20. | Dr. Himanshu Varshney | July, 2020- | Dr. Nishkarsh Gupta | "Early integration of best supportive care inaddition to standard care in patients with breast cancer: A Randomised Controlled Trial". |
| 21. | Dr. Karanvir Singh Matharoo | January, 2021- | Dr. Sushma Bhatnagar | "Symptom burden, Quality of life assessment and Incidence of Anxiety, Depression in Covid-19 positive Mucormycosis patient." |
| 22. | Dr. Shunmuga Priya.I.C | January, 2021- | Dr. Sachidanand Jee Bharati | "POCUS on Patient admitted for palliative care in tertiary hospital: cross sectional study. |
| 23. | Dr. Saruadarshi Saraswata Mahapatra | January , 2021 | Dr. Vinod Kumar | "Psychological distress and quality of life in non-small cell lung cancer patients receiving vhemotherapy":- A prospective observational study. |
| 24. | Dr. Abhinav Mishra | January, 2021- | Dr. Nishkarsh Gupta | "Assessment of Quality of Life in CoVid-19 Patients after discharge from hospital: A Prospective Observational Study." |
| 25. | Dr.Bishnu Prasad Shrestha | January, 2021- | Dr. Rakesh Garg | "Effect of dietary modifications and education tool on morphine induced constipation in addition to routine morphine prescriptions in cancer patients: A randomized control trial". |
| 26. | Dr.Revathy Vijaya kumar | January, 2021- | Dr. Sushma Bhatnagar | "Palliative care needs of patients with life-limiting illnesses presenting to the Emergency Department. |
| 27. | Dr. Mangaleswari.V | January, 2021- | Dr. Seema Mishra | "Symptom Burden and Quality of Life Assessment in Advanced Cervical Cancer Patients Presenting to the Palliative Care Department in a Tertiary Care Centre: A Prospective Observational Study". |
| 28. | Dr. Suhana Sulfiker | July, 2021- | Dr. Seema Mishra | "Caregiver burden and qualit of life of parents of children with cancer in a tertiary care centre in india- A cross sectional study. |
| 29. | Dr. Prateek Gandhi | July, 2021- | Dr. Rakesh Garg | "Needs Assessment of Palliative Care in Geriatrics |
| 30. | Dr. Arknil | July, 2021- | Dr. Sushma Bhatnagar | "To Asseess the factors Responsible for delayed presentation of cancer patients to tertiary centre: And its implication in patient care. |
| 31. | Dr. Vishnu charanthiriveedhi | January, 2022- | Dr. Sushma Bhatnagar | "Unmet Palliative care needs assessment in patients suffering from End-Stage Lung Disease [Chronic ostructive pulmonary disease(COPD)/Interstitial lung disease (ILD)]: A prospective Study" |
| 32. | Dr. Devina Juneja | January, 2022- | Dr. Vinod Kumar | "Analysis of symptom burden and quality of life in patients undergoing haemodialysis at tertiary care centre: A Prospective observational study". |
| 33. | Dr. Khushboo Mandal | January, 2022- | Dr.SachidanandJee | "Insomnia, Anxiety and Depression in newly diagnosed lung cancer patients". |
| 34. | Dr. Pooja | January, 2022- | Dr.Nishkarsh Gupta | "Effect of opioids on cognition among cancer patients". |
| S. No. | Title of the project |
|---|---|
| 1. | An Exploratory CrossSectional study to identify the social contents of pain in cancer patients. |
| 2. | Development of tool to assess total pain in cancer patients. |
| 3. | A Randomized Control Trial to Evaluate The Efficacy Of Scrambler Therapy In The Management of Pain Due To Cancers Of Head, Neck And Thoracic origin. |
| 4. | A prospective randomized study to assess the analgesic efficacy of SAP block (SAP) for modified radical mastectomy under general anesthesia. |
| 5 | A comparison between lignocaine-fentanyl intravenous infusion and ropivacaine-fentanyl epidural infusion as perioperative analgesia technique in patients undergoing major abdominal oncosurgery. |
| 6 | A prospective, randomized, double blinded comparison of intranasal Dexmedetomidine vs intranasal ketamine for efficacy of sedation in preschool children undergoing radiotherapy procedures |
| 7. | Prevalence of breakthrough cancer pain and its impact on quality of life in cancer patients at regional cancer centre, India: A Cross-sectional Study. |
| 8 | To study and analyze the pattern of symptoms of patients presenting in Palliative care wards at Regional Cancer Centre of India. |
| 9 | A prospective randomized study to assess the analgesic efficacy of Serratus anterior plane block for modified radical mastectomy with axillary dissection under general anaesthesia |
| 10 | A comparison of two techniques of postoperative analgesia: lignocaine-fentanyl intravenous infusion and ropivacaine-fentanyl epidural infusion in patients undergoing major abdominal oncosurgery- a randomized control trial. |
| 11 | Predicting difficult laryngoscopy in oral cancer patients by clinical and radiological parameters- a prospective, observational study |
| 12 | A prospective, randomized, double blinded comparison of intranasal Dexmedetomidine vs intranasal ketamine for efficacy of sedation in preschool children undergoing radiotherapy procedures. |
| 13 | To assess the correlation between nutritional status and quality of life in Indian adult palliative cancer patients. |
| 14 | To assess the role of Respiratory physiotherapy in the effectiveness of pleurodesis in adult patients with malignant pleural effusion. |
| 15 | To evaluate relation between sleep quality and cancer pain in patients admitted in palliative care unit -an observational study. |
| 16 | Comparative evaluation of Nasotracheal intubation with GlidescopeVideolaryngosocope and conventional Macintosh laryngoscope using cuff inflation technique in patients undergoing head and neck cancer surgeries: A prospective randomized study |
| 17 | Comparison of two techniques (bolus morphine vs. morphine infusion) of analgesic titration with intravenous morphine in palliative cancer patient - a prospective randomized study. |
| 18 | To study the impact of nutritional intervention in delaying the progression of cachexia to refractory cachexia in female cancer patients: A study based in India |
| S. No. | Title of the project |
|---|---|
| 1. | Spiritual problems and concerns faced by Indian palliative care patientsfunded byICMR Rs. 13, 2538 |
| 2. | Prevalence and factors associated with cancer related neuropathic pain in India: A cross sectional studyKindly reimburse as per rule funded by ICMR Rs. 10,00,000 |
| 3. | Molecular Determinates of Response to opioids in cancer patients: Indian Scenariofunded by ICMR Rs. 28,00,000. |
| S. No. | Title of the project |
|---|---|
| 1. | A prospective randomized control trial comparing intracostal with pericostal thoracotomy closure to evaluate post thoracotomy pain syndromes(paint) collaborating with Surgical Oncology |
| 2. | Prediction of infection in postoperative cases of gastrointestinal malignancy by analysis of thrombopoetin collaborating with Laboratory Oncology |
| 3. | Safety and efficacy of neoadjuvant chemotherapy in stage IIB and IIIA NSCLC: Single arm phase II study collaborating with Medical Oncology |
| S. No. | Title of the project |
|---|---|
| 1. | Prevalence and factors associated with cancer related neuropathic pain in India: A cross sectional study |
| 2. | Validation of an Indian Palliative Care Spiritual Distress Scale |
| 3. | Pattern of presentation of breast cancer related lymphedema and its impact on quality of life of breast cancer patients attending pain and palliative care clinic. |
| 4. | A cross-sectional survey of medical professionals in India toassess their prescription practices, knowledge, attitude, and barrierstowards opioid analgesic prescriptions |
| 5 | A survey of medical professionals in an apex tertiary care hospital to assess awareness, interest, practices and knowledge in palliative care : A descriptive cross-sectional study. |
| 6 | Asian patient’s perspective regarding oncology awareness, care and health (APPROACH). |
| 7. | Effectiveness of the Certificate Course in Essentials of Palliative Care programme on the knowledge in palliative care among the participants: A cross-sectional interventional study |
| 8 | Incidence and risk factors for post operative nausea vomiting in cancer surgeries : a prospective observational study |
| 9 | Effects of physiotherapy on neck and shoulder movements and mouth opening in patients operated for oral cancer and their quality of life. A Pilot Study. |
| 10 | Palliative Care: Promoting Access & International Cancer Experience in India Collaborative (PC-PAICE India Collaborative) |
| 11 | An observational study to elucidate the reasons for non compliance to home treatment for breast cancer related lymphedema in a tertiary care hospital |
| 12 | Title: Comparison of WHO step 2 analgesic drug versus step 3 analgesic drug in Stage 4 opioid-naive lung cancer patients presenting to pain clinic with moderate to severe pain in terms of pain relief and quality of life at 3 weeks follow up: A randomized prospective study |
| 13 | A double blind, double-dummy, randomized, prospective, two arm, parallel, multicenter, phase iv clinical trial to evaluate efficacy and safety of gaba-nt (fixed-dose combination of gabapentin and nortriptyline) in comparison with gabapentin in patients with neuropathic pain |
| 14 | To study the impact of nutritional intervention in delaying the progression of cachexia to refractory cachexia in female cancer patients: A study based in India |
| S. No. | Title of the project |
|---|---|
| 1. | Spiritual problems and concerns faced by Indian palliative care patients funded by ICMR Rs. 1,32,538. |
| 2. | Prevalence and factors associated with cancer related neuropathic pain in India: A cross sectional study” Kindly reimburse as per rule funded by ICMR Rs. 10,00,000. |
| 3. | Molecular Determinates of Response to opioids in cancer patients: Indian Scenario funded by ICMR Rs. 28,00,000. |
| S.No. | Title of the Project |
|---|---|
| 1 | Prevalence and factors associated with cancer related neuropathic pain in India: A cross sectional study |
| 2 | Validation of an Indian Palliative Care Spiritual Distress Scale |
| 3 | Pattern of presentation of breast cancer related lymphedema and its impact on quality of life of breast cancer patients attending pain and palliative care clinic. |
| 4 | A cross-sectional survey of medical professionals in India to assess their prescription practices, knowledge, attitude, and barriers towards opioid analgesic prescriptions |
| 5 | A survey of medical professionals in an apex tertiary care hospital to assess awareness, interest, practices and knowledge in palliative care : A descriptive cross-sectional study. |
| 6 | Asian patient’s perspective regarding oncology awareness, care and health (APPROACH) |
| 7 | Effectiveness of the Certificate Course in Essentials of Palliative Care programme on the knowledge in palliative care among the participants: A cross-sectional interventional study |
| 8 | Incidence and risk factors for post operative nausea vomiting in cancer surgeries : a prospective observational study |
| 9 | Effects of physiotherapy on neck and shoulder movements and mouth opening in patients operated for oral cancer and their quality of life. A Pilot Study. |
| 10 | Palliative Care: Promoting Access & International Cancer Experience in India Collaborative (PC-PAICE India Collaborative) |
| 11 | An observational study to elucidate the reasons for non compliance to home treatment for breast cancer related lymphedema in a tertiary care hospital |
| 12 | Comparison of WHO step 2 analgesic drug versus step 3 analgesic drug in Stage 4 opioid-naive lung cancer patients presenting to pain clinic with moderate to severe pain in terms of pain relief and quality of life at 3 weeks follow up: A randomized prospective study |
| 13 | A double blind, double-dummy, randomized, prospective, two arm, parallel, multicenter, phase IV clinical trial to evaluate efficacy and safety of gaba-nt (fixed-dose combination of gabapentin and nortriptyline) in comparison with gabapentin in patients with neuropathic pain |
| S.No. | Title of the Project | Funding Source & Amount |
|---|---|---|
| 1 | Spiritual problems and concerns faced by Indian palliative care patients | ICMR - Rs. 13,258 |
| 2 | Prevalence and factors associated with cancer related neuropathic pain in India: A cross sectional study | ICMR - Rs. 10,00,000 |
| 3 | A Double Blind, Double-Dummy, Randomized, Prospective, Two Arm, Parallel, Multicenter, Phase IV Clinical Trial To Evaluate Efficacy And Safety Of Gaba-NT (Fixed-Dose Combination Of Gabapentin And Nortriptyline) In Comparison With Gabapentin In Patients With Neuropathic Pain | Rs. 3,00,000 |
| 4 | Molecular Determinants of Response to Opioids in Cancer Patients: Indian Scenario | ICMR - Rs. 28,00,000 |
| S.No. | Title of the Project |
|---|---|
| 1 | Comparison between C-arm fluoroscopic guided posterior versus Percutaneous Ultrasound-guided anterior approach for celiac plexus neurolysis in patients with upper abdominal cancer in terms of pain relief and quality of life - A Prospective randomized comparative study |
| 2 | The Journey Of Cancer Patients From Symptom Onset To The Beginning Of Treatment In A Cancer Hospital In India |
| 3 | Prevalence of Pain Among Inpatients at All India Institute of Medical Sciences - New Delhi |
| 4 | Assessment of quality of life in breast cancer patients receiving hormonal therapy |
| 5 | Palliative Care Needs Assessment in Patients Suffering from Advanced Chronic Obstructive Pulmonary Disease (COPD)/ Interstitial Lung Disease (ILD): A Prospective Study |
| 6 | A Prospective Observational Study to Assess the Effect of Palliative Care Consultation on the Palliative Care Needs of Patients Suffering from Advanced Lung Cancer, in a Tertiary Care Hospital in India |
| 7 | Early pain intervention in cancer pain patients improves quality of pain relief, decreases analgesic requirement and thus improves quality of life |
| 8 | Association of Vitamin D deficiency with opioid consumption, quality of life and progression free survival in metastatic breast cancer patients: An Observational descriptive prospective study |
| 9 | To compare the effectiveness of Duloxetine vs Gabapentin on neuropathic pain intensity in patients with chemotherapy-induced peripheral neuropathy: A double-blind randomized controlled trial |
| 10 | Prevalence and factors associated with cancer related neuropathic pain in India: A cross sectional study |
| 11 | Validation of an Indian Palliative Care Spiritual Distress Scale |
| 12 | Pattern of presentation of breast cancer related lymphedema and its impact on quality of life of breast cancer patients attending pain and palliative care clinic |
| 13 | A cross-sectional survey of medical professionals in India to assess their prescription practices, knowledge, attitude, and barriers towards opioid analgesic prescriptions |
| 14 | A survey of medical professionals in an apex tertiary care hospital to assess awareness, interest, practices and knowledge in palliative care: A descriptive cross-sectional study |
| 15 | Asian patient’s perspective regarding oncology awareness, care and health (APPROACH) |
| 16 | Effectiveness of the Certificate Course in Essentials of Palliative Care programme on the knowledge in palliative care among the participants: A cross-sectional interventional study |
| 17 | Incidence and risk factors for post operative nausea vomiting in cancer surgeries: A prospective observational study |
| 18 | Effects of physiotherapy on neck and shoulder movements and mouth opening in patients operated for oral cancer and their quality of life. A Pilot Study |
| 19 | Palliative Care: Promoting Access & International Cancer Experience in India Collaborative (PC-PAICE India Collaborative) |
| 20 | An observational study to elucidate the reasons for non compliance to home treatment for breast cancer related lymphedema in a tertiary care hospital |
| 21 | Comparison of WHO step 2 analgesic drug versus step 3 analgesic drug in Stage 4 opioid-naive lung cancer patients presenting to pain clinic with moderate to severe pain in terms of pain relief and quality of life at 3 weeks follow up: A randomized prospective study |
| S.No. | Title of the Project |
|---|---|
| 1 | Comparison between C-arm fluoroscopic guided posterior versus Percutaneous Ultrasound-guided anterior approach for celiac plexus neurolysis in patients with upper abdominal cancer in terms of pain relief and quality of life - A Prospective randomized comparative study |
| 2 | The Journey of Cancer Patients From Symptom Onset To The Beginning Of Treatment In A Cancer Hospital In India |
| 3 | Prevalence of Pain Among Inpatients at All India Institute of Medical Sciences - New Delhi |
| 4 | Assessment of quality of life in breast cancer patients receiving hormonal therapy |
| 5 | Palliative Care Needs Assessment in Patients Suffering from Advanced Chronic Obstructive Pulmonary Disease (COPD)/ Interstitial Lung Disease (ILD): A Prospective Study |
| 6 | A Prospective Observational Study to Assess the Effect of Palliative Care Consultation on the Palliative Care Needs of Patients Suffering from Advanced Lung Cancer, in a Tertiary Care Hospital in India |
| 7 | Early pain intervention in cancer pain patients improves quality of pain relief, decreases analgesic requirement and thus improves quality of life |
| 8 | Association of Vitamin D deficiency with opioid consumption, quality of life and progression free survival in metastatic breast cancer patients: An Observational descriptive prospective study |
| 9 | To compare the effectiveness of Duloxetine vs Gabapentin on neuropathic pain intensity in patients with chemotherapy-induced peripheral neuropathy: A double-blind randomized controlled trial |
| 10 | Prevalence and factors associated with cancer related neuropathic pain in India: A cross sectional study |
| 11 | Validation of an Indian Palliative Care Spiritual Distress Scale |
| 12 | Pattern of presentation of breast cancer related lymphedema and its impact on quality of life of breast cancer patients attending pain and palliative care clinic |
| 13 | A cross-sectional survey of medical professionals in India to assess their prescription practices, knowledge, attitude, and barriers towards opioid analgesic prescriptions |
| 14 | A survey of medical professionals in an apex tertiary care hospital to assess awareness, interest, practices and knowledge in palliative care: A descriptive cross-sectional study |
| 15 | Asian patient’s perspective regarding oncology awareness, care and health (APPROACH) |
| 16 | Effectiveness of the Certificate Course in Essentials of Palliative Care programme on the knowledge in palliative care among the participants: A cross-sectional interventional study |
| 17 | Incidence and risk factors for post operative nausea vomiting in cancer surgeries: A prospective observational study |
| 18 | Effects of physiotherapy on neck and shoulder movements and mouth opening in patients operated for oral cancer and their quality of life. A Pilot Study |
| 19 | Palliative Care: Promoting Access & International Cancer Experience in India Collaborative (PC-PAICE India Collaborative) |
| 20 | An observational study to elucidate the reasons for non compliance to home treatment for breast cancer related lymphedema in a tertiary care hospital |
| 21 | Comparison of WHO step 2 analgesic drug versus step 3 analgesic drug in Stage 4 opioid-naive lung cancer patients presenting to pain clinic with moderate to severe pain in terms of pain relief and quality of life at 3 weeks follow up: A randomized prospective study |
| S.No. | Title of the Project |
|---|---|
| 1 | Spiritual problems and concerns faced by Indian palliative care patients funded by ICMR Rs. 1,32,538 |
| 2 | Study of Pain attributes to Design a Pain Measurement Device for the cancer and injured Patients funded by DRDO Rs. 24,88,100 |
| 3 | Clinical Validation of Iontophoretic Delivery of Lidocaine as an Alternative to EMLA Cream funded by AIIMS Intramural Rs. 5,00,000 |
| S.No. | Title of the Project |
|---|---|
| 1 | Comparison between C-arm fluoroscopic guided posterior versus Percutaneous Ultrasound-guided anterior approach for celiac plexus neurolysis in patients with upper abdominal cancer in terms of pain relief and quality of life-A Prospective randomized comparative study |
| 2 | The Journey of Cancer Patients From Symptom Onset To The Beginning Of Treatment In A Cancer Hospital In India |
| 3 | Prevalence of Pain Among Inpatients at All India Institute of Medical Sciences- New Delhi |
| 4 | Assessment of quality of life in breast cancer patients receiving hormonal therapy |
| 5 | Palliative Care Needs Assessment in Patients Suffering from Advanced Chronic Obstructive Pulmonary Disease (COPD)/ Interstitial Lung Disease (ILD): A Prospective Study. |
| 6 | A Prospective Observational Study to Assess the Effect of Palliative Care Consultation on the Palliative Care Needs of Patients Suffering from Advanced Lung Cancer, in a Tertiary Care Hospital in India |
| 7 | Early pain intervention in cancer pain patients improves quality of pain relief, decreases analgesic requirement and thus improves quality of life |
| 8 | Association of Vitamin D deficiency with opioid consumption, quality of life and progression free survival in metastatic breast cancer patients: An Observational descriptive prospective study |
| 9 | To compare the effectiveness of Duloxetine vs Gabapentin on neuropathic pain intensity in patients with chemotherapy-induced peripheral neuropathy: A double-blind randomized controlled trial |
| 10 | Prevalence and factors associated with cancer related neuropathic pain in India: A cross sectional study |
| 11 | Validation of an Indian Palliative Care Spiritual Distress Scale |
| 12 | Pattern of presentation of breast cancer related lymphedema and its impact on quality of life of breast cancer patients attending pain and palliative care clinic. |
| 13 | A cross-sectional survey of medical professionals in India to assess their prescription practices, knowledge, attitude, and barriers towards opioid analgesic prescriptions |
| 14 | A survey of medical professionals in an apex tertiary care hospital to assess awareness, interest, practices and knowledge in palliative care: A descriptive cross-sectional study. |
| 15 | Asian patient’s perspective regarding oncology awareness, care and health (APPROACH). |
| 16 | Effectiveness of the Certificate Course in Essentials of Palliative Care programme on the knowledge in palliative care among the participants: A cross-sectional interventional study |
| 17 | Incidence and risk factors for post-operative nausea vomiting in cancer surgeries: a prospective observational study |
| 18 | Effects of physiotherapy on neck and shoulder movements and mouth opening in patients operated for oral cancer and their quality of life. A Pilot Study. |
| 19 | Palliative Care: Promoting Access & International Cancer Experience in India Collaborative (PC-PAICE India Collaborative) |
| 20 | An observational study to elucidate the reasons for non-compliance to home treatment for breast cancer related lymphedema in a tertiary care hospital |
| 21 | Comparison of WHO step 2 analgesic drug versus step 3 analgesic drug in Stage 4 opioid-naive lung cancer patients presenting to pain clinic with moderate to severe pain in terms of pain relief and quality of life at 3 weeks follow up: A randomized prospective study |
| 1. | Calculating 95% effective dose (ED 95) of hyperbaric bupivacaine for intracavitary radiotherapy under sub-arachnoid block in patients with carcinoma cervix: A sequential allocation study |
| 2. | To assess the impact of advanced airway imaging (3D CT reconstruction and virtual endoscopy of airway) on airway management in adult patients undergoing head and neck cancer surgeries under general anaesthesia: Prospective randomized study |
| 3. | To evaluate the effect of implementation of Enhance Recovery After Surgery (ERAS) protocol in adult patients undergoing head and neck cancer surgery under general anesthesia on length of hospital stay: A prospective interventional study. |
| 4. | To assess the palliative care needs, symptom burden and quality of life in geriatrics patients attending a tertiary care centre in India- a cross sectional observational study |
| 5. | To assess the impact of respiratory physiotherapy on the effectiveness of pleurodesis after ultrasound guided pigtail catheter insertion in adult patients with malignant pleural effusion: a prospective randomized interventional study |
| 6. | Effect of Regional Anaesthesia on immune response, recurrence, and metastasis in breast cancer surgery: a prospective randomized control study. |
| 7. | Muscle activity during intubation in a difficult airway |
| 8. | Effect of early integration of palliative care on QOL in patients with CA breast |
| 9. | Effect of COVID-19 on quality of life of patients |
| 11. | Implementing Telemedicine in preanesthesia clinic at a tertiary cancer care center: A Prospective randomized comparative study. |
| 12. | Smartphone based telemedicine service for symptoms assessment in patients attending palliative care unit: A cross sectional study at a tertiary care cancer hospital |
| 13. | Prevalence and risk factors of acute neuropathic pain following oncological surgeries: a prospective study at a tertiary cancer center |
| 14. | Prospective Evaluation of Social Support, Depression and Quality of Life in Advanced Cancer Patients Attending The Palliative Care Clinic Of A Tertiary Care Centre |
| 15. | Knowledge, attitude and perception regarding morphine use in Indian cancer patients. |
| 16. | To evaluate the comparative efficacy and safety of Gabapentin, Duloxetine and Pregabalin in patients with Chemotherapy Induced Painful Neuropathy (CIPN): A Randomized Controlled Pilot trial. |
| 17. | Prevalence and predictors of insomnia in cancer patients presented to palliative care unit of a tertiary care center in India |
| 18. | Strong opioids and its impact on QOL in chemotherapy induced oral mucositis: A prospective observational study |
| 19. | Cardiopulmonary exercise testing as a predictor of morbidity after major gastrointestinal cancer surgeries in patients at nutritional risk: A prospective observational pilot study |
| 20. | Prevalence and predictors of postoperative fatigue and its impact on the quality of life patients after gastrointestinal cancer surgeries: A prospective observational study |
| 21. | A randomized control trial to evaluate the comparative efficacy of ultrasound guided supraclavicular brachial plexus block with triamcinolone and oral morphine in the management of upper extremity pain due to cancer |
| 22. | To evaluate the comparative efficacy and safety of Gabapentin, Duloxetine and Pregabalin in patients with Chemotherapy Induced Painful Neuropathy (CIPN): A Randomized Controlled Pilot trial. |
| 23. | Prevalence of chemotherapy induced peripheral neuropathy in a palliative care setup and its impact on the quality of life of cancer patients. |
| 24. | Prevalence of postoperative morbidity in patients undergoing elective major thoraco-abdominal oncosurgery and their correlation with anaesthetic technique. |
| 25. | Effect of patient controlled epidural analgesia (PCEA) and intravenous patient-controlled analgesia (IVPCA) on postoperative inflammatory response and cancer recurrence in patients undergoing abdominal oncosurgery - a prospective randomized controlled trial. |
| 26. | Validation of the Hindi version of the EORTC QLQ–C15–PAL questionnaire for the evaluation of quality of life of advanced cancer patients at tertiary care center, India.” |
| 27. | Concerns of health care professionals managing non‐COVID patients during the COVID‐19 pandemic: A descriptive cross‐sectional study. |
| 28. | Palliative Care Needs Assessment in Patients Suffering from Advanced Chronic Obstructive Pulmonary Disease (COPD)/ Interstitial Lung Disease (ILD): A Prospective Study |
| 29. | A Prospective Observational Study to Assess the Effect of Palliative Care Consultation on the Palliative Care Needs of Patients Suffering from Advanced Lung Cancer, in a Tertiary Care Hospital in India |
| 30. | Dexmedetomidine versus Midazolam for Sedation during Medical Thoracoscopy: A Pilot Randomized Controlled Trial (RCT): Journal of Bronchology and Interventional Pulmonology |
| 31. | Pain Management Policy formulation at a tertiary care teaching institute in India: A prospective observational study. |
| 32. | Feasibility of ERAS (Enhanced Recovery after Surgery) protocol in patients undergoing gastrointestinal cancer surgeries in tertiary care. |
| 33. | Role of Perioperative Vitamin C supplementation in reduction of surgical stress and inflammatory markers following head and neck oncosurgeries- A Prospective double blinded randomized trial. |
| 34. | To see the effects of implementation of ERAS protocol in adult patients undergoing head and neck cancer surgery under general anaesthesia on length of hospital stays. |
| 35. | Effect of anesthetic technique on anti-tumor immunity and clinical outcomes in patients undergoing surgery for oral cancer: A prospective randomized comparative study. |
| 36. | A Prospective Randomized Control Trial To Compare Post-Operative Pain And Complications After Colorectal Cancer Surgery Under Different AnaesthesticTechniques; Intraoperative Total Intravenous Anaesthesia (TIVA) With Propofol Versus Sevoflurane Based Anaesthesia |
| 37. | Comparison of macintosh laryngoscope with various video laryngoscopes with respect to upper limb muscular activity and perceived workload using surface electromyography (SEMG) during intubation in a manikin with simulated difficult airway: A prospective randomized cross over trial. |
| 38. | A comparison of two techniques of postoperative analgesia: multimodal intravenous analgesic technique and epidural infusion of ropivacaine in patients undergoing oncological abdominal surgeries – prospective randomized trial" |
| 39. | Impact of advanced airway imaging (3 D CT reconstruction and virtual endoscopy) on airway management in patients undergoing head and neck cancer surgeries :Prospective randomized study. |
| 40. | To compare the efficacy of continuous bilateral quadratus lumborum block with continuous epidural block for providing effective analgesia and perioperative outcome in patients undergoing exploratory laparotomy for colorectal cancer surgery: A non-inferiority randomized controlled trial |
| 41. | Effect of anesthetic technique on anti-tumor immunity and its markers in patients undergoing surgery for Gall Bladder Cancer: A prospective randomized comparative study. |
| 42. | Impact of individualised PEEP in patients undergoing one lung ventilation: a Randomised control trial |
| 43. | Comparison of different video laryngoscopes for Nasotracheal intubation in manikin with difficult airway by experienced anesthesiologists: A randomized, self-controlled, crossover trial |
| 44. | To compare the efficacy of opioid free general anesthesia with opioid based general anesthesia on post-operative morphine consumption in patients undergoing breast cancer surgery: a prospective randomized control study. |
| 45. | Comparison of lung aeration loss in open abdominal oncologic surgeries after ventilation with Electrical Impedance Tomography guided PEEP versus conventional PEEP – a pilot randomized control trial. |
| 46. | Effect of dietary modifications and education tool on morphine induced constipation in addition to routine morphine prescriptions in cancer patients: A randomized control trial". |
| 47. | Palliative care needs of patients with life-limiting illnesses presenting to the Emergency Department. |
| 48. | Caregiver burden and qualit of life of parents of children with cancer in a tertiary care centre in India- A cross sectional study. |
| 49. | Needs Assessment of Palliative Care in Geriatrics Symptom Burden and Quality of Life Assessment in Advanced Cervical Cancer Patients Presenting to the Palliative Care Department in a Tertiary Care Centre: A Prospective Observational Study. |
| 50. | To Assess the factors Responsible for delayed presentation of cancerpatients to tertiary centre: And its implication in patient care. Palliative care needs of patients with life-limiting illnesses presenting to the Emergency Department |
| 51. | Psychological distress and quality of life in Lung cancer patients receiving chemotherapy: - A prospective observational study |
| 52. | Role of Intravenous iron therapy on fatigue and quality of life in patients of palliative care: a prospective interventional study. |
| 53. | Assessment of Symptom Burden and “Quality of Life” in Patients of Primary brain tumors receiving palliative care at a tertiary care centre, India: A Prospective Observational Study. |
| 54. | Effect of early integration of best supportive care in addition to standard care in patients with breast cancer: a randomized controlled trial |
| 55. | To assess the palliative care needs, symptom burden and quality of life in advanced sarcoma patients presenting to a palliative medicine clinic of tertiary cancer centre- a cross-sectional study |
| 56. | Assessment Of Symptom Burden and Quality of Life in Paediatric Cancer Patients in A Tertiary Care Centre In India: A prospective study. |
| 57. | To study the clinical correlation between chemotherapy induced peripheral neuropathy (CIPN) and deficiency of vitamin b12, vitamin d3, calcium and omega 3 fatty acids. |
| 58. | Smartphone‐based telemedicine service at palliative care unit during nationwide lockdown: Our initial experience at a tertiary care cancer hospital. |
| 59. | Effect of nation‐wide lockdown on palliative care services in a tertiary care centre in India: A retrospective observational study. |
| 60. | Opioid dispensing patterns from a tertiary care cancer hospital during the nationwide lockdown in COVID‐19 pandemic |
| 61. | Palliative Care Needs Assessment in Patients Suffering from Advanced Chronic Obstructive Pulmonary Disease (COPD)/ Interstitial Lung Disease (ILD): A Prospective Study. |
| 62. | Effect of adding dexamethasone to ropivacaine on ultrasound guided serratus anterior plane block for modified radical mastectomy: A Prospective randomized controlled study. |
| 63. | Perioperative anaesthesia management for brachytherapy in cancer patients: A retrospective observational study. |
| 64. | To compare the efficacy of opioid free anaesthesia with opioid based anaesthesia on post-operative opioid consumption in patients undergoing open thoracotomy surgeries: a prospective randomized control trial. |
| 66. | Correlation of oxygenation, ventilatory parameters and optic nerve sheath diameter (ONSD) to intra-operative mechanical ventilation in abdominal surgeries, comparison of recruitment maneuver with conventional ventilation. A pilot randomized controlled trial. |
| 67. | To evaluate the effect of two ventilatory strategies (conventional bag mask ventilation and manual jet ventilation) on peak inspiratory pressures and dynamic compliance using electrical impedance tomography after interventional rigid bronchoscopy for malignant central airway obstruction. |
| 68. | Comparison of total intravenous anaesthesia and inhalational anesthesia for development of postoperative pulmonary complications in oral cancer resection surgery with pectoralis major myocutaneous (PMMC) flap reconstruction: a prospective, randomized control trial. |
| 69. | A comparison of two techniques of postoperative analgesia: lignocaine-fentanyl intravenous infusion and ropivacaine-fentanyl epidural infusion in patients undergoing cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) – prospective randomized control study. |
| 70. | A Prospective Randomized Control Trial of Goal directed Vs Standard Fluid Therapy in Cytoreductive Surgery with Hyperthermic Intraperitoneal Chemotherapy.” |
| 71. | Assessment of Symptom Burden and “Quality of Life” in Patients of Primary brain tumours receiving palliative care at a tertiary care centre, India: A Prospective Observational Study. |
| 72. | Assessment of Symptom Burden and Quality of Life in Patients of advanced head and neck cancer receiving palliative care at tertiary care centre, India: A Prospective Observational Study. |
| 73. | To study the effect of oral morphine prescribed for dyspnoea in cancer patients presenting to the Departments of Onco-Anaesthesia and Palliative Medicine and Pulmonary Medicine and Sleep Disorders in a tertiary care hospital in India: A prospective observational study. |
| 74. | Assessment of Symptom Burden And Quality Of Life in Patients Of Lung Cancer Attending The Palliative Care Clinic Of A Tertiary Care Centre: Prospective |
| 75. | Comparison of intervention with analgesics versus analgesics alone in patients with Head and Neck malignancy in terms of pain relief and quality of life at 3 months follow up: A Prospective randomized study |
| 76. | Assessment of Symptoms Burden and Quality of Life in Patients of Malignant Bowel Obstruction Presenting in Palliative Care Unit at Tertiary Cancer Centre in India. |
| 77. | Pattern of Patients Presenting with Malignant Spinal cord Compression in Palliative Care Unit at a Tertiary Care Centre of India-An Observational Study”. |
| 78. | Quality of life and symptom burden in patients with hematological malignancies receiving hematopoietic stem cell transplantation- a prospective observational study |
| 79. | End of Life care practice at a Tertiary Cancer Centre in India: An Observational study.” |
| 80. | Assessment of Symptom Burden And Quality of Life in Patients of Advanced Breast Cancer in Indian Population: A Cross-Sectional study.” |
| 81. | Assessment of palliative care outcomes in patients of gastro intestinal malignancies attending the palliative care clinic of a tertiary care centre: a prospective observational study. |
| 82. | Comparison of Mc Grath-MAC and C-MAC video laryngoscopes for intubation in a COVID simulated mannequin by novice users wearing face protective gear: a randomized crossover trial |
| 83. | To evaluate the effect of two ventilatory strategies (conventional bag mask ventilation and manual jet ventilation) on peak inspiratory pressures and dynamic compliance using electrical impedance tomography after interventional rigid bronchoscopy for malignant central airway obstruction |
| 84. | A comparison of two techniques of postoperative analgesia: lignocaine-fentanyl intravenous infusion and ropivacaine-fentanyl epidural infusion in patients undergoing cytoreductive cancer surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) - prospective randomized control study. |
| 85. | Perioperative anaesthetic management in cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC): a retrospective analysis in a single tertiary care cancer centre |
| 86. | Comparison of kind vision Videolaryngoscopechanneled and non-channeled blades with direct Laryngoscope for intubation in mannequin by medical students: a randomized mannequin study. Funded AIIMS Undergraduate research project |
| 87 | To compare the efficacy of opioid free general anesthesia with opioid based general anesthesia on post-operative morphine consumption in patients undergoing breast cancer surgery: a prospective randomized control study. |
| 88. | Nasotracheal intubation in patients with oropharyngeal carcinoma under general anaesthesia: A comparative evaluation between fibreoptic bronchoscope and C-MAC D blade videolaryngoscope |
| 89. | Comparison of two different doses of hyperbaric bupivacaine for intracavitary radiotherapy in patients with carcinoma cervix: A Randomized control trial. |
| 90. | An assessment of need for palliative care in patients with rheumatoid arthritis using SF36, DAS28, DASS and HAQ-DI questionnaires |
| 91. | Comparison of kind vision Videolaryngoscopechanneled and non-channeled blades with direct Laryngoscope for intubation in mannequin by medical students: a randomized mannequin study. Funded AIIMS Undergraduate research project |
| 92. | Comparison of Mc Grath-MAC and C-MAC video laryngoscopes for intubation in mannequin by donned anesthesiologists using an intubation box during COVID-19: pandemic: a prospective randomized study. |
| 93. | Comparison of Mc Grath-MAC and C-MAC video laryngoscopes for intubation in patients with normal airway by donned anesthesiologists using an intubation box during COVID-19: pandemic: a prospective randomized study. |
| 94. | A comparison of effect of Desflurane vs Sevoflurane on arterial oxygenation during one lung ventilation for thoracotomies in oncosurgical patients: - a randomized control trial.” |
| 95. | Comparison of analgesic efficacy of Ultrasound guided thoracic Paravertebral block versus surgeon guided Serratus Anterior Plane block for acute postoperative pain in patients undergoing thoracotomy for lung surgery-A prospective randomized study |
| 96. | Comparison of efficacy of Ultrasound guided Paravertebral Block versus Erector Spinae Plane block for Postoperative Analgesia in Modified Radical Mastectomy: A Randomized Controlled Trial. |
| 97. | Cardiopulmonary exercise testing as a predictor of postoperative outcome in patients undergoing esophageal cancer surgery following neoadjuvant chemotherapy - A prospective observational study. |
| 98. | Cardiopulmonary exercise testing as an early predictor of chemotherapy induced cardiac dysfunction in carcinoma breast patients receiving neo-adjuvant chemotherapy and to compare their early post-operative recovery with the carcinoma breast patients posted for upfront surgery: A Prospective Observational Study |
| 99. | Comparison of lung aeration loss in open abdominal oncologic surgeries after ventilation with Electrical Impedance Tomography guided PEEP versus conventional PEEP – a pilot randomized control trial. |
| 100. | Comparison of efficacy of ultrasound guided paravertebral block versus complete anterior thoracic block for postoperative analgesia in modified radical mastectomy: a randomized controlled trial |
| S.No. | Title of the Project | Funding Agency & Amount |
|---|---|---|
| 1 | To determine the impact of latent tuberculosis on severity and outcomes in patients with suspected SARS-COV-19 infection | Intramural, AIIMS, New Delhi Rs. 4,54,000 |
| 2 | Development of homeopathic nosode from Covid-19, its evaluation and efficacy against Covid-19 infections in humans | Central Council for Research in Homeopathy (CCRH), Ministry of AYUSH, Government of India Rs. 10,00,000 |
| 3 | Phase2, randomized, controlled, open label multi-center study to assess efficacy and safety of DFV890 for the treatment of SARS-CoV-2 infected patients with COVID-19 pneumonia and impaired respiratory function | Norartis Pvt. Ltd. Rs. 5,00,000 |
| 4 | Comparison between C-MAC and King Vision video laryngoscope (channeled blade) for tracheal intubation in aerosol-prevention intubation box for COVID-19 patients | Intramural, AIIMS, New Delhi Rs. 5,00,000 |
| 5 | Effect Of Intraoperative Single Dose Ketorolac On Release Of Vegf And Tgf-Β In Patients Undergoing Breast Cancer Resection – A Prospective Randomized Trial | Intramural, AIIMS, New Delhi Rs. 4,54,000 |
| 6 | Clinical Validation of Iontophoretic Delivery of Lidocaine as an Alternative to EMLA Cream | Intramural, AIIMS, New Delhi Rs. 10,00,000 |
| 7 | Homoeopathy as an adjuvant to standard treatment protocol in management of corona virus infection - a randomized, placebo controlled, open label study | Central Council for Research in Homeopathy (CCRH), Ministry of AYUSH, Government of India Rs. 14,31,135 |
| 8 | Development of homeopathic nosode from Covid-19, its evaluation and efficacy against Covid-19 infections in humans | Central Council for Research in Homeopathy (CCRH), Ministry of AYUSH, Government of India Rs. 9,83,220 |
| S.No. | Title of the Project |
|---|---|
| 1 | Novel Video Laryngoscope for Endotracheal Intubation in Patients with Reduced Mouth Opening approved for AIIMS-IIT project funding (ongoing) collaboration with IIT Delhi |
| 2 | An RCT to compare the effectiveness of mobile app-based prescription vs conventional prescription of analgesics and adjuvant adherence on selected variables in patients receiving palliative care at tertiary care centre collaboration with College of Nursing |
| 3 | A prospective randomized control trial comparing intracostal with pericostal thoracotomy closure to evaluate post thoracotomy pain syndromes (paint) collaboration with Surgical Oncology |
| 4 | Safety and efficacy of neoadjuvant chemotherapy in stage IIB and IIIA NSCLC: Single arm phase II study collaboration with Medical Oncology |
Physiotherapy
WHO Collaborating Centres / Centres of Excellence etc
WHO CC Reference Number - IND-163
Operating Rooms
ICU
Palliative Care Ward
| Day | OT 1 | OT 2 | OT 3 | NCI | ICU/RT/CT/Selectron/GF OT | OPD/PCU | Academic Day | On call | |
|---|---|---|---|---|---|---|---|---|---|
| Mon | Dr. Vinodkumar | Dr. Rakesh Garg | Dr. Vinod Kumar (1st& 3rd /Dr. Rakesh Garg (2nd& 4th ) | Dr.SachidanandJee Bharati
| Dr.Nishkarsh Gupta/*Dr.SachidanandJee Bharati
| Dr. Seema Mishra/Dr.Nishkarsh Gupta
| Dr. Sushma Bhatnagar
| Dr. Rakesh Garg
| |
Tues
| Dr. Seema Mishra
| Dr.Nishkarsh Gupta | Dr. Rakesh Garg/ Dr.NishkarshGupta | Dr. Sushma Bhatnagar/ Dr.Rakesh Garg | Dr. Vinod Kumar/ Dr.SachidanandJeeBharati | Dr. Seema Mishra | |||
Wed
| Dr. Sushma Bhatnagar
| Dr. Vinod Kumar
| Dr, Seema Mishra/ Dr. Vinod Kumar | Dr.SachidanandJee Bharati/ Dr. Seema Mishra | Dr.Nishkarsh Gupta/ Dr. Rakesh Garg | Dr. Vinod Kumar
| |||
Thurs
| Dr. Vinod Kumar
| Dr.Nishkarsh Gupta
| Dr.SachidanandJee Bharati
| Dr. Seema Mishra
| Dr. Rakesh Garg
| Dr. Sushma Bhatnagar/ Dr. Rakesh Garg | Dr. Seema Mishra/
| Dr.Nishkarsh Gupta | |
| Fri | Dr.Nishkarsh Gupta (1st & 3rd ) Dr.SachidanandJee Bharati (2nd & 4th )/ Dr. Rakesh Garg* | Dr.SachidanandJee Bharati | Dr.Nishkarsh Gupta | Dr. Rakesh Garg | Dr. Seema Mishra | Dr. Vinod Kumar/ Dr. Sushma Bhatnagar | -- | Dr.SachidanandJee Bharati | |
Sat/ Sun | OT and OPD-Week end consultant on call Round- All consultants | ||||||||
Current Issues in Pain Management for the Primary Care Clinician
International Association for the Study of Pain Pain Definitions
The Resource Center of the American Alliance of Cancer Pain Initiatives
For details kindly visit
| S. No | Name of Event | Date | City |
|---|---|---|---|
| 1 | IAPC certificate course in Palliative Care | July and Jan 2021 | Dr. B.R.A IRCH, AIIMS, Virtually |
| 2 | World Hospice Day | 9th October, 2021 | Dr. B.R.A IRCH, AIIMS, Virtually |
Preventive Oncology plays a pivotal role in cancer prevention and early detection, offering both clinical and outreach services to diverse populations. Through its academic endeavors, it also contributes to the training of healthcare professionals and advances research in cancer prevention strategies. It functions as an essential part of a multidisciplinary approach to cancer control, working closely with other departments, public health organizations, and communities. The department focuses on various cancers, especially those that are preventable, and offers both clinical and outreach services. Additionally, it plays a crucial role in academics, contributing to the training of healthcare professionals and the dissemination of cancer prevention knowledge.

The Department of Radiation Oncology at the All India Institute of Medical Sciences (AIIMS), New Delhi, is a premier centre for cancer treatment, research, and education in India. Established with the mission to provide state-of-the-art radiation oncology services, the department has been at the forefront of cancer care, integrating advanced technology with cutting-edge research and high-quality patient care
| S.No. | Name | Year of Passing |
|---|---|---|
| 1 | Brahm Prakash | 1968 |
| 2 | B.S. Das | 1970 |
| 3 | Ravi Bhatia | 1971 |
| 4 | Jawahar Dar | 1972 |
| 5 | H. N. Agarwal | 1974 |
| 6 | S. Mohanty | 1974 |
| 7 | A.K. Reddy | 1975 |
| 8 | B. N. Acharya | 1977 |
| 9 | N.R. Nanda | 1979 |
| 10 | Dr. R.K. Navlakha | 1980 |
| 11 | Dr. M.A.Wani | 1980 |
| 12 | Dr. S.P. Agarwal | 1980 |
| 13 | Dr. Ved Prakash | 1980 |
| 14 | Dr. Laxman Das | 1981 |
| 15 | Dr. V.S.Mehta | 1981 |
| 16 | Dr A. K . Mahapatra | 1982 |
| 17 | Dr. S.K. Sogani | 1983 |
| 18 | Dr. B.K. Misra | 1983 |
| 19 | Dr. Sudhir S Pai | 1983 |
| 20 | Dr. S.B. Ali | 1985 |
| 21 | Dr. Sanjeev Bhatia | 1985 |
| 22 | Dr. G.B. Bhatty | 1986 |
| 23 | Dr. Avinash Prasad | 1986 |
| 24 | Dr. Karam Chand | 1986 |
| 25 | Dr. Ranganatham | 1986 |
| 26 | Dr. R.V.P.Singh | 1987 |
| 27 | Dr. V.P.Singh | 1987 |
| 28 | Dr. H.K. Pal | 1989 |
| 29 | Dr. Rana Patir | 1989 |
| 30 | Dr. Jitendra Kumar | 1989 |
| 31 | Dr. Sandeep Sood | 1989 |
| 32 | Dr. S.N. Iyengar | 1990 |
| 33 | Dr. V.K. Rajoria | 1990 |
| 34 | Dr. Abhay Verma | 1990 |
| 35 | Dr. A.K. Dubey | 1991 |
| 36 | Dr. Dhirendra Prasad | 1991 |
| 37 | Dr. A.K. Verma | 1992 |
| 38 | Dr. S.N. Chaudhary | 1992 |
| 39 | Dr. Rakesh Gupta | 1993 |
| 40 | Dr. Anoop Chakraborty | 1993 |
| 41 | Dr. Raj Kumar | 1993 |
| 42 | Dr. Ajay K Sinha | 1993 |
| 43 | Dr. P.K. Sahoo | 1994 |
| 44 | Dr. Ashish K Srivastav | 1994 |
| 45 | Dr. Anuj K Singh | 1994 |
| 46 | Dr. Dipankar Nandi | 1995 |
| 47 | Dr. S.S.Kale | 1996 |
| 48 | Dr. Sandeep Vaishya | 1996 |
| 49 | Dr. A.S. Randhawa | 1996 |
| 50 | Dr. Sanjay Bansal | 1996 |
| 51 | Dr. Charu Varma | 1997 |
| 52 | Dr. Raj Kamal | 1997 |
| 53 | Dr. B.S. Walia | 1997 |
| 54 | Dr. Kalpesh C Jain | 1997 |
| 55 | Dr. Ajay Agarwal | 1997 |
| 56 | Dr. Sudheer Kumar Tyagi | 1997 |
| 57 | Dr. Navanil Barua | 1997 |
| 58 | Dr. Ajay Bakshi | 1997 |
| 59 | Dr. Anupam Jindal | 1998 |
| 60 | Dr.Ashish Suri | 1998 |
| 61 | Dr. Aditya Gupta | 1999 |
| 62 | Dr. B.K. Ojha | 1999 |
| 63 | Dr. Tushar Arora | 2000 |
| 64 | Dr. Pankaj Kr. Jha | 2000 |
| 65 | Dr. Ashish Kr. Khandwey | 2000 |
| 66 | Dr. Arun Naik | 2000 |
| 67 | Dr. Pradeep Kr. Jain | 2000 |
| 68 | Dr. Somil Kansal | 2001 |
| 69 | Dr. Gurru Dutta Satyarthee | 2001 |
| 70 | Dr Vijay Shankar Jha | 2002 |
| 71 | Dr. Manmohan Singh | 2002 |
| 72 | Dr. Ravinder Pal Singh Chhabra | 2002 |
| 73 | Dr. Subodh Raju | 2002 |
| 74 | Dr. Rajinder Kumar | 2002 |
| 75 | Dr. G.V. Ramdas | 2002 |
| 76 | Dr. K.I. Mathai | 2002 |
| 77 | Dr. Awadhesh Kr.Jaiswal | 2002 |
| 78 | Dr. Paritosh Pandey | 2002 |
| 79 | Dr. Manish Singh Sharma | 2002 |
| 80 | Dr. T.S. Vasan | 2003 |
| 81 | Dr. Deepak Agrawal | 2003 |
| 82 | Dr. Ashish Tandon | 2003 |
| 83 | Dr. Sujoy Kumar. Sanyal | 2003 |
| 84 | Dr. Deepak Kumar Gupta | 2004 |
| 85 | Dr. Deepinder Singh | 2004 |
| 86 | Dr. S. Dwarkanath | 2004 |
| 87 | Dr. Pralay Kishore Nayak | 2004 |
| 88 | Dr. Ajay Kurve | 2004 |
| 89 | Dr. Sumit Sinha | 2005 |
| 90 | Dr. S.A. Jaleel Kirmani | 2005 |
| 91 | Dr. T. Ramesh | 2005 |
| 92 | Dr. S.S Dhandapani | 2005 |
| 93 | Dr. N.A. Sai Kiran | 2005 |
| 94 | Dr. Shyam Kishore Mishra | 2006 |
| 95 | Dr. Dhruv Chaturvedi | 2006 |
| 96 | Dr. Karanjit Singh | 2006 |
| 97 | Dr. Faiz Uddin Ahmed | 2006 |
| 98 | Dr.Pradyot Kumar | 2007 |
| 99 | Dr.Mahinder Singh Chouhan | 2007 |
| 100 | Dr. Arun Kumar Srivastva | 2007 |
| 101 | Dr. Om Prakash | 2007 |
| 102 | Dr M Sriniwas | 2007 |
| 103 | Dr Girish Rajpal | 2007 |
| 104 | Dr. Ravinder Srivastava | 2008 |
| 105 | Dr. Gaurav Bansal | 2008 |
| 106 | Dr. K. B. Shanker | 2008 |
| 107 | Dr. Rohit Kumar Goel | 2008 |
| 108 | Dr. R.G. Prasad | 2008 |
| 109 | Dr. Anuj Tripathi | 2008 |
| 110 | Dr. Manish Kasliwal | 2008 |
| 111 | Dr. Anil Garg | 2008 |
| 112 | Dr. Vamsi K Y | 2009 |
| 113 | Dr.Shashank Ramdurg | 2009 |
| 114 | Dr. Amit Srivastava | 2009 |
| 115 | Dr.Rakesh K Singh | 2009 |
| 116 | Dr.Pankaj Singh | 2009 |
| 117 | Dr.Shailesh Jain | 2009 |
| 118 | Dr.Nilesh Kurwale | 2009 |
| 119 | Dr.Amit Thapa | 2009 |
| 120 | Dr.Shashwat Mishra | 2009 |
| 121 | Dr.Hitesh K G | 2009 |
| 122 | Dr.Gopal Sedain | 2009 |
| 123 | Dr. Vivek Tandon | 2009 |
| 124 | Dr Vikas Naik | 2010 |
| 125 | Dr Gaurav Jaiswal | 2010 |
| 126 | Dr Shameem Ahmed | 2010 |
| 127 | Dr Amit Dagar | 2010 |
| 128 | Dr Sachin Anil Borkar | 2010 |
| 129 | Dr Pankaj Ailawadhi | 2011 |
| 130 | Dr Ajit Singh | 2011 |
| 131 | Dr Vipin Kumar Gupta | 2011 |
| 132 | Dr Pankaj Dawar | 2011 |
| 133 | Dr Noufal Basheer | 2011 |
| 134 | Dr Deva Kumar Borgohain | 2011 |
| 135 | Dr Amandeep Jagdevan | 2011 |
| 136 | Dr Yashpal Singh Rathore | 2011 |
| 137 | Dr Anand Gupta | 2012 |
| 138 | Dr Sumit Bansal | 2012 |
| 139 | Dr Utkarsh Bhagat | 2012 |
| 140 | Dr Anand V.K | 2012 |
| 141 | Dr Ashutosh Khandelwal | 2012 |
| 142 | Dr Laxmiprasad | 2012 |
| 143 | Dr Prashant Gunawat | 2012 |
| 144 | Dr Ajay bisht, | 2012 |
| 145 | Dr Harshit Mishra | 2012 |
| 146 | Dr Mansukh Sangani | 2012 |
| 147 | Dr Avijit Sarkari | 2012 |
| 148 | Dr Siddharth Sahoo | 2012 |
| 149 | Dr Shejoy P Joshua | 2012 |
| 150 | Dr Saurabh Sharma | 2012 |
| 151 | Dr Akash Mishra | 2012 |
| 152 | Dr Manoj Phalak | 2013 |
| 153 | Dr Kanwaljeet Garg. | 2013 |
| 154 | Dr Saquib Azad Siddiqui | 2013 |
| 155 | Dr Gaurang Vaghani | 2013 |
| 156 | Dr Amitabha Das | 2013 |
| 157 | Dr Nishant Goyal | 2013 |
| 158 | Dr Amol Raheja | 2014 |
| 159 | Dr Nityanand Pandey | 2014 |
| 160 | Dr Dattaraj Sawarkar | 2014 |
| 161 | Dr Pradeep Chouksey | 2014 |
| 162 | Dr Rajvir Singh Garrsa | 2014 |
| 163 | Dr Nandish Gowda | 2014 |
| 164 | Dr Chinmaya Dash | 2014 |
| 165 | Dr Ratandeep Bose | 2014 |
| 166 | Dr Mayank Garg | 2014 |
| 167 | Dr Satyashiva Munjal | 2014 |
| 168 | Dr Ankit Bansal | 2015 |
| 169 | Dr Sukanto Das | 2015 |
| 170 | Dr Satish Verma | 2015 |
| 171 | Dr M D Sudhan | 2015 |
| 172 | Dr SP Manik Prabhu | 2015 |
| 173 | Dr Dipankar Singh Mankotia | 2015 |
| 174 | Dr Vivek Shete | 2015 |
| 175 | Dr Anil K Kothiwala | 2015 |
| 176 | Dr Nitin Verma | 2015 |
| 177 | Dr Anutosh Singh | 2015 |
| 178 | Dr Shashi Pratap Singh | 2015 |
| 179 | Dr Shantanu Bora | 2015 |
| 180 | Dr Ribhav Pasricha | 2016 |
| 181 | Dr Venkat Koyalmantham | 2016 |
| 182 | Dr Anil K. Gaur | 2016 |
| 183 | Dr Raghav Singla | 2016 |
| 184 | Dr Gopal Krishna | 2016 |
| 185 | Dr Surya Prakash Gora | 2016 |
| 186 | Dr Saraj Kumar Singh | 2016 |
| 187 | Dr Ashutosh Agarwal | 2017 |
| 188 | Dr Mohit Agrawal | 2017 |
| 189 | Dr Skanda Moorthy | 2017 |
| 190 | Dr Ashwani Kumar | 2017 |
| 191 | Dr Bhoopendra Singh | 2017 |
| 192 | Dr Anirudha Mohite | 2017 |
| 193 | Dr Soubam Parkinson Singh | 2017 |
| 194 | Dr Mahalangikar Raman Ashok | 2017 |
| 195 | Dr Jaskaran Singh | 2017 |
| 196 | Dr Ambuj Kumar | 2017 |
| 197 | Dr Raghavendra Kumar Sharma | 2017 |
| 198 | Dr Hardik Sardana | 2018 |
| 199 | Dr Varshney Gaurav Chandrapal | 2018 |
| 200 | Dr Mayanglambam Amitkumar | 2018 |
| 201 | Dr Suveen Janmatti | 2018 |
| 202 | Dr Satyajit Panda | 2018 |
| 203 | Dr Harish. C | 2018 |
| 204 | Dr Raghu Samala | 2018 |
| 205 | Dr Vijaykumar Harshad Chipde | 2018 |
| 206 | Dr Krishnveer Singh Choudhary | 2018 |
| 207 | Dr Simranjeet Singh | 2018 |
| 208 | Dr Gaurav Singh | 2018 |
| 209 | Nitish Agarwal | 2019 |
| 210 | Hitesh Inder Singh Rai | 2019 |
| 211 | Suresh Kanasani | 2019 |
| 212 | Chandra Kumar Thounoujam | 2019 |
| 213 | Ravi Sharma | 2019 |
| 214 | Sanjeev A Srinivasan | 2019 |
| 215 | Atmaranjan Dash | 2019 |
| 216 | Meher Thej Boorgula | 2020 |
| 217 | Faiz Akram Siddiqui | 2020 |
| 218 | Ankit Jain | 2020 |
| 219 | Dibyajyoti Mahakul | 2020 |
| 220 | Surya Sri Krishna Gour | 2020 |
| 221 | Varidh Katiyar | 2020 |
| 222 | Devasheesh Kamra | 2020 |
| 223 | Ajay Kumar Nayak | 2020 |
| 224 | Arvinder Kumar Dhayal | 2020 |
| 225 | Dipanshu Narula | 2020 |
| 226 | Vaibhav Vij | 2020 |
| 227 | Mukesh Bisht | 2020 |
| 228 | Prashant Kumar Sharma | 2020 |
The department of Neurosurgery is organizing
HOD 1965-1988
HOD 1995-2006
HOD 2006 -2012, currently on deputation as Director, AIIMS, Bhubaneshwar
Spine Surgery Fellowship, Tampa, Florida, USA 2002-2003
BOYS CAST Fellowship, DST 2005-2006.
The Department has always been in the forefront in the areas of research and academic activities. Taken together, since 1965, when the Department was still in its infancy, we have contributed more than 500 scientific publications in various national and international journals. This is probably the largest number of publications by any neurosurgical centre in India.
The department of Neurosurgery has remained a centre point of research in the country. There has been research on evidence based clinical practice and laboratory based work. The department has been involved with several multi-centric national and international studies.
The Department of Neurosurgery at the All India Institute of Medical Sciences, New Delhi started the “Experimental Microneurosurgery Laboratory” in 1971 through the efforts of Prof. P.N. Tandon and Prof. A.K. Banerji (Emeritus Professors, Department of Neurosurgery).
The training laboratory was expanded and renovated into a full fledged training facility named as Neurosurgery Skills Training Facility and Experimental Laboratory with the support of Department of Science and Technology (DST), Ministry of Science and Technology, Govt. of India, Department of Biotechnology (DBT) Indo-German Collaboration, Ministry of Science and Technology, Govt. of India, and Department of Health Research (DHR-ICMR), Ministry of Health and Family Welfare, Govt. of India for hands on skills training of M.Ch and DNB neurosurgery residents and trained /trainee Neurosurgeons from India and abroad.
The Neurosurgery Skills Training Facility and Experimental Laboratory is equipped with the state-of-the-art equipment, which simulates a modern Neurosurgery Operation Room environment. The training imparted is aimed at development of Neurosurgical skills and techniques.
The training imparted in the form of quarterly workshops, short term training programs and daily skills training sessions is focused on formulation of a new curriculum of neurosurgical skills development and imparting hands-on practice on synthetic/semi synthetic models, live anesthetized animals and cadaver parts using highly advanced equipment and technology creating a neurosurgical operation room environment.
The inpatient services of department of Neurosurgery are located in Cardiothoracic and Neurosciences Centre (C N Centre) and C N Tower at AIIMS.
There are two Neurosurgical units in the department located on 2nd and 3rd floor of C N Centre better known as NS-2 and NS-3 wards. Each ward has bed strength of 35. The C N Tower has 25 special rooms dedicated for neurosciences patients. There are two Intensive Care Units ICU-B and ICU-C, situated on the 1st floor of C N Centre and have bed strength of 25. Each ICU is equipped with state of the art equipment viz. electro-hydraulic beds, latest ventilators for each bed, central monitor for each bed, blood gas analyzer, blood coagulation parameter analyzer, cardiac defibrillators, infusion pumps, dialysis machine and transcranial doppler etc. The nurse to patient ratio in ICU is 1:1.
There are 7 neurosurgical operation theaters situated in the CN Centre and CN Tower. Operation theaters are equipped with the state of the art modern amenities and equipments e.g. laminar flow, intra-operative MRI, electro hydraulic operating tables, latest operating microscopes, CUSA, image intensifiers, intra-operative ultrasound, intra-operative vascular doppler machine, intra-operative neuro-navigation (Treon-from Medtronic), intra-operative EEG, intra-operative cell saver (to recycle blood loss during surgery), intra-operative trans-esophageal echocardiography, intra-operative evoked potential recording, nerve stimulators etc. Along with this each operation theater is equipped with state of the art anesthesia equipment and monitoring systems. The department of neurosurgery has back up of most modern sister departments of Neuro-radiology and Neuro-pathology. The neuro-radiology department is equipped with state of the art biplane DSA machine, multi-slice CT machine, 1.5 tesla MRI machine and ultra-sound machine.
Apart from this, the department has Gamma Knife unit equipped with Leksell Gamma Knife machine which treats various intracranial lesions non-invasively.
The department specializes in various fields of Neurosurgery i.e.
The Department of Neurosurgery runs OPD in Cardiothoracic and Neurosciences Centre (CN Centre Ground Floor) for four days in a week i.e. on Monday, Tuesday, Thursday and Friday.
| Day | Time | Faculty |
|---|---|---|
Monday NS Unit –I | 9 a.m. to 1 pm | Prof B S Sharma Dr P Sarat Chandra Dr Manmohan Singh Dr Guru D Satyarthee Dr Deepak Agarwal Dr Pankaj Kr Singh Dr Hitesh Kumar |
Tuesday NS Unit –II | 9 am to 1 pm | Dr S. S. Kale Dr Ashish Suri Dr Rajender Kumar Dr Deepak Gupta Dr Sumit Sinha Dr Sachin A Borkar Dr Vivek Tandon |
Thursday NS Unit –I | 2 pm to 6 pm | Prof B S Sharma Dr P Sarat Chandra Dr Manmohan Singh Dr Guru D Satyarthee Dr Deepak Agarwal Dr Pankaj Kr Singh Dr Hitesh Kumar |
Friday NS Unit –II | 9 am to 1 pm | Dr S. S. Kale Dr Ashish Suri Dr Rajender Kumar Dr Deepak Gupta Dr Sumit Sinha Dr Sachin A Borkar Dr Vivek Tandon |
The department has created a forum to support, coordinate and enhance efforts to generate scientific information useful to Neurosurgical trainees and specialists. http://aiimsnets.org/neurosurgeryeducation.asp
The department is committed for advancement and promotion of neurosurgery in the country. The department regularly organizes the “ANNUAL AIIMS MICRO NEUROSURGERY WORKSHOP” in the month of February every year. Two eminent faculties of National and International repute along with AIIMS faculty demonstrate their surgical skills. There is live telecast of operations and the delegates directly communicate with operating surgeons.
The visiting international faculty during the annual micro neurosurgery workshop also delivers the prestigious “SARVESHWARI MEMORIAL ORATION”.
Over the years the department has organized the following national and international conferences:
| 1975 | Micro Neurosurgery Workshop |
| 1981 | National Seminar on CNS Infection |
| 1982 and 1983 | Micro Neurosurgery Workshop |
| 1986 | 1. Standardization of neurosurgical training in India (under the aegis of NSI) 2. Endoscopic choroid plexus fulguration |
| 1989 | 1. 9th World Congress of Neurological Surgeons 2. First National Conference on Skull Base Surgery |
| 1991- | Endoscopic Disc Surgery |
| 1992 | Cadaver Skull Base Workshop |
| 1994 | 1. One day Conference of Gamma Knife 2. Midas Rex Hands on Workshop (two courses) |
| 1995 | 1. Micro neurosurgery Workshop 2. Skull Base Workshop – both live surgery and cadaver dissection |
| 1996 | Skull Base Workshop – Live demonstration of surgery |
| 1997 | Skull Base Workshop – Live demonstration and cadaver dissection |
| 1998 | Neurosciences Update by Neurosciences Centre |
| 2002- | Mid-Neurocon under NSI |
| 2004- | 2nd Indo-Japanese Neurosurgery Conference |
| 1999-2012 | Annual AIIMS Micro Neurosurgery Workshop |
| 2007- | 1. First National Radiosurgery update 2. 9th Annual Conference of Skull Base Surgery Society of India, International Skull Base CME, WFNS Microsurgery and Endoscopy Skull Base Cadaver Workshop from 24th-28th October, 2007 at AIIMS. |
| 2009 | 1. Annual Conference of Delhi Neurological Society (DNACON 2009) 2. Ist Live surgery and Cadaveric Hands on Workshop on Minimal Access Spinal Surgery 23rd-25th July 2009, at Jai Prakash Narain Apex Trauma Center, All India Institute of Medical Sciences, New Delhi. |
| 2011 | 1th Annual Conference of the Indian Society of Cerebro-vascular Surgery, International Cerebrovascular CME & Pre-conference Live AIIMS Neurosurgery, Neuro-intervention and Radiosurgery Workshop. Dates: 6th to 9th October, 2011 |
| 2016 | PROFESSOR, NEUROSURGERY & GAMMA-KNIFE (1 November 2016 -PRESENT) Department of Neurosurgery, JPNATC, Neurosciences & Gamma Knife Centre, All India Institute of Medical Sciences, Ansari Nagar, New Delhi, India-110029 |
| 2014 | ADDITIONAL PROFESSOR, NEUROSURGERY & GAMMA-KNIFE (1 JULY 2012 -30 OCTOBER 2016) Department of Neurosurgery, JPNATC, Neurosciences & Gamma Knife Centre, All India Institute of Medical Sciences, Ansari Nagar, New Delhi, India-110029 JULY 8, 2014 ASSOCIATE PROFESSOR, NEUROSURGERY & GAMMA-KNIFE (1 JULY 2009 -30 JUNE 2012) Department of Neurosurgery, JPNATC, Neurosciences & Gamma Knife Centre, All India Institute of Medical Sciences, Ansari Nagar, New Delhi, India-110029 JULY 8, 2014 |
| 2006 | ASSISTANT PROFESSOR, NEUROSURGERY & GAMMA-KNIFE (26 SEPTEMBER 2005-30 JUNE 2009) Department of Neurosurgery, Neurosciences & Gamma Knife Centre, All India Institute of Medical Sciences, Ansari Nagar, New Delhi, India-110029 SEPTEMBER 28, 2006 |
| 2005 | CLINICAL FELLOW, PEDIATRIC & ENDOSCOPIC NEUROSURGERY, (AUG 2004-SEPTEMBER 2005) Department of Neurosurgery, British Columbia children’s Hospital, 4480 Oak street, Vancouver, Canada SEPTEMBER 15, 2005 |
| 2004 | SENIOR RESEARCH FELLOW, NEUROSURGERY (OCTOBER 2003-JULY 2004) Department of Neurosurgery, Neurosciences & Gamma Knife Centre, All India Institute of Medical Sciences, Ansari Nagar, New Delhi, India-110029 JUNE 30, 2004
|
 |  |  |  |  |
ATLS Instructor Have successfully done the ATLS provider and instructor course and am a qualified ATLS instructor | AUTLS Course Director Is director of AIIMS Ultrasound Trauma Life support Course which is held in 4 countries | AIIMS-KISS Program Director Program Director of ‘AIIMS- Keep it Simple Sonography for Neurosurgeons’: Have held the workshop in India & Nepal | AIIMS- REAP Program Director Program Director of AIIMS- Research Ethics and Presentation Course held for Doctors & nurses | AIIMS-PDCP Program Director Program director of AIIMS-Personality development, communication & Presentation skills workshop held regularly all over India |
 |  |  |  |  |  |
| BEST POSTER AWARD BY NEUROTRAUMA SOCIETY OF INDIA | CERTIFICATION FOR TRAINING IN ETHICS BY JOHN HOPKINS | CERTIFICATE OF ACHIEVEMENT BY ASIAN CONGRESS OF NEUROLOGICAL SURGEONS | ATLS INSTRUCERTIFICATION | BEST PRESENTATION AWARD BY ASSOCIATION OF SURGEONS OF INDIA | Dr Deepak Agrawal won the coveted 'Dynamic CIO of health care of the year -2016' by jury in the 5th Annual Healthcare Summit held from 13-14 May 2016 in Delhi. |
Guidelines for Short-Term/Long-Term Training/Visiting Fellow in respect of Indian and Foreign National candidates
The Department of Neurosurgery at the All India Institute of Medical Sciences, New Delhi started the “Experimental Microneurosurgery Laboratory” in 1971 through the efforts of Prof. P.N. Tandon and Prof. A.K. Banerji (Emeritus Professors, Department of Neurosurgery).
The training laboratory was expanded and renovated into a full fledged training facility named as Neurosurgery Skills Training Facility and Experimental Laboratory with the support of Department of Science and Technology (DST), Ministry of Science and Technology, Govt. of India, Department of Biotechnology (DBT) Indo-German Collaboration, Ministry of Science and Technology, Govt. of India, and Department of Health Research (DHR-ICMR), Ministry of Health and Family Welfare, Govt. of India for hands on skills training of M.Ch and DNB neurosurgery residents and trained /trainee Neurosurgeons from India and abroad.
The Neurosurgery Skills Training Facility and Experimental Laboratory is equipped with the state-of-the-art equipment, which simulates a modern Neurosurgery Operation Room environment. The training imparted is aimed at development of Neurosurgical skills and techniques.
The training imparted in the form of quarterly workshops, short term training programs and daily skills training sessions is focused on formulation of a new curriculum of neurosurgical skills development and imparting hands-on practice on synthetic/semi synthetic models, live anesthetized animals and cadaver parts using highly advanced equipment and technology creating a neurosurgical operation room environment.
http://aiimsnets.org/workshops.asp
NATIONAL CANCER INSTITUTE (Jhajjar Campus), AIIMS
The department offers course in neurosurgery to award degree of
MCh (NEUROSURGERY)
There are two streams of neurosurgery course in the department
For further information contact Examination Cell, AIIMS
The candidates selected in 3 year stream work as Senior Residents in the department. They are supposed to do all clinical work of wards, ICU’s, emergency and assist cases in operation theaters under supervision. The candidate is given increasing responsibility for independent surgical work. The candidate is expected to maintain a log book of all surgical experience. They are supposed to write two dissertations (one prospective and one retrospective study) to qualify to appear in final MCh exam. The final MCh examination to award the degree takes place after the end of 3rd year.
The candidates selected in 6 year MCh course, spend first 3 years as Junior Residents. During this period they are posted for 1 year in General Surgery on rotation. After completing 3 years, they work as Senior Residents in the department for next 3 years. During these three years they have similar responsibilities as that of a senior resident from the 3 year stream. They also have to write two dissertations (one prospective and one retrospective study) to qualify to appear in final MCh exam. The candidates of 6 year stream appear for their final MCh exam after the end of 5 years. During the 6th year they work in the department as chief residents.
The final examination to award the degree of MCh consists of following steps
Pit and Fissure Sealant Training Workshop 1 May 2017

Prof. OP Kharbanda welcoming ShriLavAgarwal, JS Health

Inaugural Ceremony

ShriLavAgarwal delivering the Welcome Address

Prof. OP Kharbanda

Dr. L Swasticharan, CMO

Shri.Ziley Singh Vical, Deputy Secretary

Prof. Neeraj Gugnani, Resource Person

Prof. RM Pandey, Resource Person

Dr. Harsh Priya, Resource Person

Dr. UtkalMohanty, Resource Person

Delegates at the Training Workshop

Group Photograph
The CBCT facility in room No. 514, 5th floor CDER, was inaugurated by Director AIIMS New Delhi, Prof. Randeep Guleria in the presence of Chief CDER, Dean Academics, Dean Research and other faculty members of AIIMS, on 1st January 2018.
The CBCT machine is capable of both 2D and 3D imaging and reconstruction of oral and maxillofacial structures by using a specialized projection geometry and algorithm resulting in a significant reduction of radiation exposure to the patient as compared to conventional CT machines. This facility is now available to all patients seeking treatment at AIIMS at a very subsidized cost.
CBCT allows visualization of sub-millimetre sections with no magnification making linear and angular measurements accurate for high precision applications like implant placement and endodontics.
CBCT will open up new vistas for advanced imaging which will enhance diagnosis, treatment planning and management of patients with complex oral and maxillofacial pathology, trauma, and deformities. Its applications can be further enhanced by coupling it with 3D scanners and 3D printers for creating life- size models, making it an excellent tool for patient education, training and research.
The “Staff Cafeteria” at ground floor, centre for Dental Education and Research, AIIMS, New Delhi was inaugurated by Prof. Randeep Gulleria, Director, AIIMS, New Delhi in presence of Prof O.P. Kharbanda, Chief , CDER, AIIMS on 1st January, 2018. They were accompanied by Prof Chitra Sarkar, Dean Research, AIIMS and Prof Y.K. Gupta, Dean Academic, AIIMS and other esteemed faculty members of AIIMS.
Report on Oral Health Promotion Drive on International Childhood Cancer Day 2017 – 8th February 2017 (Wednesday)
Centre for Dental Education and Research participated in the event organised by the Department of Paediatrics on 8th February 2017 commemorating the International Childhood Cancer Day on 15th February 2017 at the Jawaharlal Nehru Auditorium, AIIMS New Delhi. An Oral Health Promotion Drive for the Paediatric cancer patients was also done. Oral hygiene methods were demonstrated to the children suffering from cancer using animated video and brushing models. Also a comic story was circulated among the children and their caregivers regarding the oral health. The comic demonstrated various oral conditions that might happen during their Chemotherapy and radiotherapy and ways to combat them. Also 100 badges were distributed to the children carrying various oral health messages emphasising the need of brushing twice daily, healthy eating and avoid snacking. Posters providing educational information on oral health in children were displayed. The participating team in the event was
AIIMS Employee cancer awareness and Screening (Aug 22 to Sep 2, 2022)
Workshop on Cancer Awareness and Early Detection and Cancer screening camp at India International Center, New Delhi (28th May, 2022)

Tobacco Symposium:
Tobacco cessation Interventions in Oncology Practice (11th March, 2020)

World Cancer Day
Feb 4th 2020 “Role of Nurses in Cancer Prevention and Control.” Training for Nurses

Preventive oncology clinic
3rd Floor, B-Wing OPD Block, NCI-Jhajjar
Monday to Friday, 9am to 1PM
For appointments: 8929042745
| S.No. | Name of course | Admission criteria |
|---|---|---|
| 1. | Ph.D. | M.Sc (Physics) or M.Sc. (Medical Physics) with relevant exposure to Diagnostic Medical Physics or the relevant qualification according to the running project. Admission through entrance examination conducted by AIIMS twice in a year (Jan. & July) |
| 2. | Training in radiation safety and quality in imaging | Personnel working in the relevant area or desirous to have exposure in the said course. Application to be routed through the Registrar, AIIMS. |
| S.No | Name of the Tumor Board/ conference | Day/Time |
|---|---|---|
| 1 | Head and Neck Oncology Tumour Board | Monday and Friday 4pm onwards |
| 2 | GastroIntestinal Tumor Board Clinic | Saturday 12-1 pm |
| 3 | Lung Cancer Tumour Board | Wednesday 9:30 am |
| 4 | Sarcoma Tumor Board | Wednesday 1 pm |
| 5 | Surgical Oncology Conference | Monday and Friday 9-10:30 am |
| 6 | Medical and Gynaecology Oncology Conference | Tuesday 830 am onwards |
| 7 | Radiation Oncology Conference | Wednesday 9 am |
| 8 | Oncoanesthesia and palliative medicine | Saturday 9 am |
Email: irchradiology@gmail.com
The Department of Head and Neck Oncology at the National Cancer Institute, Jhajjar, strives to offer affordable and quality service to patients with head and neck cancer. The department currently provides daily outpatient services (Monday to Friday), including various office-based procedures. We ensure optimal and quality clinical in-patient services in the current 20-bedded ward on the 5th floor. Additionally, we run a multidisciplinary disease management group twice a week (Tuesday and Friday) and a swallowing clinic with a facility for Functional endoscopic evaluation of swallowing (FEES) for appropriate rehabilitation of the patients after surgery in the OPD setting. Emergency services (management of airway and bleeding in relation to head and neck cancers) are offered round the clock. We are equipped with nasal endoscopy and fiberoptic laryngoscopy for clinical oncologic examination.
The department runs eight operation theaters weekly (Monday to Friday). It offers surgical treatment of cancer related to the domain of Otorhinolaryngology (maxillectomy, laryngectomy, neck dissection, glossectomy, thyroidectomies, mandibulectomy, etc.) for early and advanced oral, laryngeal, and other head and neck cancers.
In addition to clinical care, the department has also been playing a prominent role in academic and research activities. Residents training (MS {ENT} and MCh {Head and Neck Cancer Surgery}) is being undertaken with an emphasis on clinical care, research, and teaching aspects. The teaching courses in the subspecialties of Head and neck oncology are being conducted regularly.
| S. No. | Name | Designation |
|---|---|---|
| 1. | Dr. S. V. S. Deo (1991) | Senior Resident |
| 2. | Dr. Sumeet Goyal | Senior Resident |
| 3. | Dr. Kislay Kumar Thakur | Senior Resident |
| 4. | Dr. Rajesh Nanda | Senior Resident |
| 5. | Dr. Shantivardhan | Senior Resident |
| 6. | Dr. Arun Goel | Senior Resident |
| 7. | Dr. V Seenu | Senior Resident |
| 8. | Dr. Deepak Routray | Senior Resident |
| 9. | Dr. Rajesh Srivastava | Senior Resident |
| 10. | Dr. J Kishore | Senior Resident |
| 11. | Dr. Murali babu | Senior Resident |
| 12. | Dr. Niranjan | Senior Resident |
| 13. | Dr. Dinesh Kadam | Senior Resident |
| 14. | Dr. Rashmi | Senior Resident |
| 15. | Dr. Madhabanand Kar | Senior Resident |
| 16. | Dr. G. Srinivas | Senior Resident |
| 17. | Dr. Sonal Asthana | Senior Resident |
| 18. | Dr. D Sridhar | Senior Resident |
| 19. | Dr. Diganta K das | Senior Resident |
| 20. | Dr. Joydeep Purkayastha | Senior Resident |
| 21. | Dr. Sunil Kumar | Senior Resident |
| 22. | Dr. Rajiv Saran | Senior Resident |
| 23. | Dr Mittal | Senior Resident |
| 24. | Dr Neeraj Saxena | Senior Resident |
| 25. | Dr Charak | Senior Resident |
| 26. | Dr. Atul Samaiya | Senior Resident |
| 27. | Dr. Sidharth Hazarika | Senior Resident |
| 28. | Dr. Ajay Saha | Senior Resident |
| 29. | Dr. M. Om Prakask | Senior Resident |
| 30. | Dr. Gaurav Jain | Senior Resident |
| 31. | Dr. Majid | Senior Resident |
| 32. | Dr. Prashant Khullar | Senior Resident |
| 33. | Dr. Rajive | Senior Resident |
| 34. | Dr. Manish Verma | Senior Resident |
| 35. | Dr. Archit Pandit | Senior Resident |
| 36. | Dr. Mandeep Singh | Senior Resident |
| 37. | Dr. Hemant Goyal | Senior Resident |
| 38. | Dr. Deepak Jha | Senior Resident |
| 39. | Dr. Jeevan Ram | Senior Resident |
| 40. | Dr. Jitender | Senior Resident |
| 41. | Dr. Ashwin Kalayanpur | Senior Resident |
| 42. | Dr. Balasubramaniam | Senior Resident |
| 43. | Dr. Amrita | Senior Resident |
| 44. | Dr. Shubham | Senior Resident |
| 45. | Dr. Subi | Senior Resident |
| 46. | Dr. Debashish | Senior Resident |
| 47. | Dr. Shubham Garg | Senior Resident |
| 48. | Dr. Vaitheeswaran | Senior Resident |
| 49. | Dr. Amruta Nikhil Beke | Senior Resident |
| 50. | Dr. Mamraj Gupta | Senior Resident |
| 51. | Dr. Rakesh Sakiya | Senior Resident |
| 52. | Dr. Tapan Singh Chouhan | Senior Resident |
| 53. | Dr. Shivam Vatsal | Senior Resident |
| 54. | Dr. Dharma Kumar K G | Senior Resident |
| 55. | Dr. Subrat Kumar | Senior Resident |
| 56. | Dr. Anjay Kumar | Senior Resident |
| 57. | Dr. Murali A | Senior Resident |
| 58. | Dr. Sarees Kumar MK | Senior Resident |
| 59. | Dr. Praveen Yadav | Senior Resident |
| 60. | Dr. Jitendra Kumar Nangal | Senior Resident |
| 61. | Dr. Majid Ahmed Talikoti | Senior Resident |
| 62. | Dr. Ramesh | Senior Resident |
| 63. | Dr. Niju Pegu | Senior Resident |
| 64. | Dr. Aravind S Kapali | Senior Resident |
| 65. | Dr. Ankit Dhiman | Senior Resident |
| 66. | Dr. Tejas Prakash Vispute | Senior Resident |
| 67. | Dr. Amar Prem | Senior Resident |
| 68. | Dr. Bhupendra Saini | Senior Resident |
| 69. | Dr. Nishant | Senior Resident |
| 70. | Dr. Neha Mishra | Senior Resident |
| 71. | Dr. Durgesh Wankhede | Senior Resident |
| 74. | Dr. Arvind Kumar Koslia | Senior Resident |
| 75. | Dr. Vineet Goel | Senior Resident |
| 76. | Dr. Rajeev Sharma | Senior Resident |
| 77. | Dr. Kumar S S | Senior Resident |
| 78. | Dr. B Ravindra Babu | Senior Resident |
| 79. | Dr. Vivek Gupta | Senior Resident |
| 80. | Dr. Amit Attam | Senior Resident |
| 81. | Dr. Saurabh Kalia | Senior Resident |
| 82. | Dr. Saarat Chandra Pingali | Senior Resident |
| 83. | Dr. Prashant Khullar | Senior Resident |
| 84. | Dr. Om Prakash M | Senior Resident |
| 85. | Dr. Neha Mishra | Senior Resident |
| 86. | Dr. Durgesh Wankhede (NCI) | Senior Resident |
| 87. | Dr. Arvind Kumar Koslia | Senior Resident |
| 88. | Dr. Rahul Saini | Senior Resident |
| 90. | Dr. Dinesh Mohan | Senior Resident |
| 92. | Dr. Saurabh Singh (NCI) | Senior Resident |
| 93. | Dr. Akotkar Shravika Suresh | Senior Resident |
| S. No. | Name | Designation | D.O.J. | D.O. Completion | Email ID |
|---|---|---|---|---|---|
| 1. | Dr. Dillip Kumar Muduly | Senior Resident (Academic) | 04.07.12 | 03.07.15 | dillipmuduly@gmail.com |
| 2. | Dr. Manjunath NML | Senior Resident (Academic) | 20.07.12 | 19.07.15 | nmlmanjunath@gmail.com |
| 3. | Dr. R M Palaniappan | Senior Resident (Academic) | 02.01.13 | 02.01.16 | fruitfather@gmail.com |
| 4. | Dr. Ashish Jakhetiya | Senior Resident (Academic) | 03.01.13 | 02.01.16 | jakashish@gmail.com |
| 5. | Dr. Pankaj Kumar Garg | Senior Resident (Academic) | 30.01.13 | 31.01.16 | dr.pankajgarg@gmail.com |
| 6. | Dr. Paras Khanna | Senior Resident (Academic) | 01.07.13 | 30.06.16 | paraskhanna@gmail.com |
| 7. | Dr. Jyoti Sharma | Senior Resident (Academic) | 01.07.13 | 30.06.16 | drjyoti27@yahoo.co.in |
| 8. | Dr. Mahesh Sultania | Senior Resident (Academic) | 01.01.14 | 31.12.16 | drmaheshsultania@gmail.com |
| 9. | Dr. Mahendra Pal Singh | Senior Resident (Academic) | 01.01.14 | 31.12.16 | drmahi_cool@yahoo.com |
| 10. | Dr. Sandeep K Boriwal | Senior Resident (Academic) | 01.01.14 | 31.12.16 | drsandeepbhoriwal@gmail.com |
| 11. | Dr. Vinaya Kumar JR | Senior Resident (Academic) | 01.07.14 | 30.06.17 | jrvk85@gmail.com |
| 12. | Dr. Mokkapati Praveen Royal | Senior Resident (Academic) | 01.07.14 | 30.06.17 | mpraveenroyal@gmail.com |
| 13. | Dr. Bharat Bhushan Khurse | Senior Resident (Academic) | 01.01.15 | 31.12.17 | dr.bharatbhushankhurse@gmail.com |
| 14. | Dr. Raj Mohan | Senior Resident (Academic) | 01.01.15 | 31.12.17 | drrajmohan_2005@yahoo.co.in |
| 15. | Dr. Seema Singh | Senior Resident (Academic) | 01.01.15 | 29.06.18 | seemasingh5jan@gmail.com |
| 16. | Dr. Ashutosh Mishra | Senior Resident (Academic) | 01.07.15 | 30.06.18 | drashutoshmishra11@gmail.com |
| 17. | Dr. P. Naveen | Senior Resident (Academic) | 13.07.15 | 12.07.18 | drnaveenp.in@gmail.com |
| 18. | Dr. Parmesh S | Senior Resident (Academic) | 01.01.16 | 31.12.18 | sparroww6@gmail.com |
| 19. | Dr. Manoj Gowda S | Senior Resident (Academic) | 01.01.16 | 31.12.18 | drmanojsg@gmail.com |
| 20. | Dr. Rashpal Singh | Senior Resident (Academic) | 14.07.16 | 13.07.19 | rashpalcallingrashpal@gmail.com |
| 21. | Dr. Babul Bansal | Senior Resident (Academic) | 02.07.16 | 01.07.19 | babulbansal@yahoo.com |
| 22. | Dr. Naveen Kumar | Senior Resident (Academic) | 01.07.16 | 30.06.19 | dr.naveenms@gmail.com |
| 23. | Dr. Prakash Bhagat | Senior Resident (Academic) | 09.01.17 | 08.01.20 | prakashbhagat@hotmail.com |
| 24. | Dr. Areendam Barua | Senior Resident (Academic) | 08.02.17 | 07.02.20 | drareendam@gmail.com |
| 25. | Dr. Navin Kumar | Senior Resident (Academic) | 01.07.17 | 30.06.20 | navin2k1@gmail.com |
| 26. | Dr. Raghuram K | Senior Resident (Academic) | 01.07.17 | 30.06.20 | dr_raghummc@yahoo.co.in |
| 27. | Dr. Sudhakar G | Senior Resident (Academic) | 01.01.18 | 31.12.20 | sudhakar2k4@gmail.com |
| 28. | Dr. Prashant Gupta | Senior Resident (Academic) | 04.01.18 | 03.01.21 | drprashant42@gmail.com |
| 29. | Dr. Amitabha Mandal | Senior Resident (Academic) | 02.07.18 | 01.07.21 | amitabha.doc@gmail.com |
| 30. | Dr. Pallabika Mandal | Senior Resident (Academic) | 02.07.18 | 01.07.21 | pallabika86@gmail.com |
| 31. | Dr. Kunal Dhall | Senior Resident (Academic) | 02.07.18 | 01.07.21 | kunaldhall@gmail.com |
| 32. | Dr. Manish Gaur | Senior Resident (Academic) | 02.01.19 | 01.01.22 | manish.gr1@gmail.com |
| 33. | Dr. Sourabh Nandi | Senior Resident (Academic) | 01.01.19 | 31.12.21 | saurav337@gmail.com |
| 34. | Dr. Premanand N | Senior Resident (Academic) | 28.01.19 | 30.06.22 | dr.premanandmmc1989@gmail.com |
| 35. | Ajit Singh Oberoi | Senior Resident (Academic) | 01.07.19 | 30.06.22 | ajitaiimsz@gmail.com |
| 36. | Dr. Jaya Kumar P | Senior Resident (Academic) | 11.07.19 | 10.07.22 | jk151986@gmail.com |

Department of Surgical Oncology is active at several national and international forums and has conducted numerous conferences and cadaveric workshops. In last few years, the department has conducted several events, a few worth mentioning being
| 1 | Pattern of care and survival studies in breast, head &neck and cervical cancer. |
| 2 | Evaluation of Diffusion Weighted Magnetic Resonance Imaging for assessment of response to Neo Adjuvant Chemotherapy in advanced Squamous cell carcinoma of oral cavity |
| 3 | Role of Fibrin sealant in Ilio Inguinal Block Dissection to reduce the rate of lymphatic drainage and seroma formation, thereby morbidity |
| 4 | Role of Fibrin sealant in Ilio Inguinal Block Dissection to reduce the rate of lymphatic drainage and seroma formation, thereby morbidity |
| 5 | A randomized controlled trial comparing single dose versus three doses of antibiotic prophylaxis in surgical oncology patients with clean wounds. |
| 6 | Role of PET– CT Scan ( Positron Emission Tomography and CT Scan ) in the Staging of Locally Advanced / Recurrent Breast Cancer as a Single modality in Comparison to Multiple Organ Directed Conventional Investigations (C.I) A prospective Study. |
| 7 | Low cost, low dose, oral, neoadjuvant chemotherapy protocol in locally advanced borderline oral cancers - Feasibility study. |
| 8 | Analysis of a computerized prospective database of patients with uncommon sites of oral cancer presenting to IRCH, AIIMS. |
| 9 | Analysis of a prospective computerized database of colon cancer patients presenting to IRCH-AIIMS. |
| 10 | Prospective analysis the role of Positron emission tomography in preoperative evaluation of resectable soft tissue sarcoma and correlation with histo-pathological grading |
| 11 | Analysis of a prospective computerized database of esophageal cancer patients presenting to IRCH-AIIMS. |
| 12 | Clinical profiles and patterns of palliative surgery in cancer patients: An ambispective Study. |
| 13 | Analysis of a prospective computerized database of Gastric cancer patients presenting to IRCH-AIIMS. |
| 14 | A prospective study of Assessment of Breast anthropometry in Indian breast cancer patients. |
| 15 | Peri operative morbidity after complete cytoreduction and HIPEC |
| 16 | River Flow’ Incision for decreasing morbidity of Ilio-Inguinal Dissection |
| 17 | Pre-operative short course radiotherapy Vs NACT- long term radiotherapy in the management of locally advanced rectal cancer |
| 18 | Analysis of a computerized prospective database of patients with early breast cancer. |
| 19 | A prospective study evaluating incidence of DVT in patients undergoing surgery for thoracic and abdomino-pelvic malignancies. |
| 20 | Review of clinic-pathological, epidemiological, imaging accuracy, treatment outcomes and prognostic factors of operable pulmonary metastases in Department of Surgical Oncology, IRCH, AIIMS. |
| 21 | Role of PET– CT Scan ( Positron Emission Tomography and CT Scan ) in the Staging of Locally Advanced / Recurrent Breast Cancer as a Single modality in Comparison to Multiple Organ Directed Conventional Investigations (C.I) |
| 22 | Retrospective Analysis of A prospective computerized data base of patients with Early Tongue cancer. |
| 23 | Analysis of a Prospective computerized clinical database of Soft Tissue Sarcomas |
| 24 | A Prospective Study evaluating role of Ultrasound and Ultrasound guided FNAC in the assessment of cervical node metastasis in Oral Cancer |
| 25 | Molecular profiling (BRAF and K-RAS gene mutation) in differentiated thyroid cancer (DTC) in Indian patients operated at BRA IRCH AIIMS . |
| 26 | A prospective and Retrospective study of complex Breast conservation therapy. |
| 27 | A prospective study to validate the role of Integrated Positron Emission Tomography-Computed Tomography and Endobronchial Ultrasound and guided Transbronchial needle aspiration in the mediastinal staging of resectable Non small cell lung cancer |
| 28 | Standardizing Surgico-pathological evaluation of oral squamous cell carcinomas specimens - A prospective study |
| 29 | A prospective study to validate the role of PET CT and EBUS in the staging of resectable Non Small Cell Lung Cancer” |
| 30 | Efficacy of Neoadjuvant chemotherapy in carcinoma esophagus- A pilot study comparing Cisplatin+5-FU with Paclitaxel + Carboplatin |
| 31 | A prospective randomized control trial comparing intracostal with pericostal throractomy closure to evaluate post thoracotmy pain syndromes |
| 32 | Complex breast conservation therapy for breast cancer patient selection criteria clinical profile and outcomes |
| 33 | Patterns of care and survival studies on cancer in childhood, lymphoid and hematopoietic malignancies, other gynecological malignancies |
| 34 | Immuno-phenotypic profile of tumor infiltrating cells of the immune system & expression of PDL1 in triple negative/Her-2 neu positive breast cancer patients and their correlation with response to neoadjuvant chemotherapy |
| 35 | Comparative Sphingolipid profiling of breast cancer cell and tissue types for identification of Potential Metastatic Biomarkers |
| 36 | Development of Standard Operating Procedures (SOP) of Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in peritoneal surface malignancies for Government set up in India. |
| 37 | Clinical significance of cell-free DNA in intraoperative pleural lavage fluid and plasma in patients with non-small cell lung cancer (NSCLC): A pilot study |
| 38 | Role of T-regulatory cells (Tregs) and their clinical correlation in epithelial ovarian cancer. |
| 39 | Evaluation of peritoneal cancer index (PCI) in primary advanced ovarian epithelial carcinoma amongst Indian population. |
| 40 | A prospective observational study comparing CT scan vs PET CT scan in carcinoma ovary for determining the pre-operative disease burden and resectability |
| 41 | Efficacy of Neoadjuvant chemotherapy protocol in locally advanced, carcinoma oral cavity- A randomized, pilot study comparing Cisplatin+5-FU with Paclitaxel + Carboplatin |
| 42 | A study of young colorectal cancer patients - Clinical profile, treatment and relapse patterns, learning basic laboratory techniques of molecular biology for miRNA extraction in colon cancer patients. |
| 43 | Clinical Utility of cell-free DNA in intraoperative pleural lavage fluid and plasma for patients with resectable primary pulmonary malignancies – A pilot study |
| 44 | Awareness and Knowledge of Indian Breast Cancer patients pertaining to genetic aspect of Breast cancer |
| 45 | Prospective study to evaluate the accuracy of axillary staging using Ultrasound guided FNAC in early breast cancer |
| 46 | Comparison of pulmonary metastasis detected with PET-CT vs NCCT chest with surgical pathology |
| 47 | Evaluation of Indocyanine green dye-based navigation surgery in optimizing axillary management of carcinoma breast. |
| 48 | Learning Basic Lab Techniques and Analysis of Colorectal cancer data base. |
| 49 | Prevalence of sarcopenia in patients with upper gastrointestinal and lung malignancy undergoing surgical resection and its impact on immediate postoperative outcomes: A prospective observational study |
| 50 | Patterns of Care and Survival Studies on Gall Bladder Cancer under ICMR- National Cancer Registry Programme (NCRP) |
| 51 | Validation of role of PET-CT and Diagnostic Laparoscopy in the gall bladder cancer patients – A prospective study. |
| 52 | Feasibility study of dual technique- blue dye and fluorescence imaging for detection of sentinel node in oral cavity cancer – a prospective validation study |
| 53 | Prospective assessment of quality indicators of perioperative outcomes in major oncological surgeries at a high-volume tertiary care center |
| 54 | A prospective comparative study between HIPEC and EPIC and a Retrospective analytic survey of HIPEC patients. |
| 55 | SURAKHA – Breast Cancer Genetic awareness and risk Assessment |
| 56 | Predicting the response to neo-adjuvant chemotherapy by analysis of exome and transcriptome in squamous cell carcinoma of esophagus |
| 57 | Breast and Ovarian cancer awareness |
| 58 | Role of heavy metals As etiology for carcinoma of the gallbladder |
| 59 | Hospital Based Cancer Registry at National Cancer Institute (NCI)-AIIMS |
| 60 | Functional recovery and Return to work after Thoracic surgery in patients with Malignant thoracic Diseases: A Prospective study |
| 61 | A pilot study to assess role of preoperative chemoradiotherapy in locally advanced / recurrent extremity soft tissue sarcoma & audit of soft tissue sarcoma database. |
| 62 | Prospective study of in person versus online cancer genetic counseling and ambispective evaluation of patients undergoing risk reducing surgery. |
| 63 | A study to evaluate time trends of clinical profile and risk factors among breast cancer patients and learning basic laboratory techniques of breast cancer lipidomics |
| 64 | Prospective evaluation of diagnostic imaging methods and its impact on surgical decision-making algorithm in the management of nodal disease in recurrent differentiated thyroid cancer and audit of the thyroid cancer database for evaluation of clinical and surgical spectrum and outcomes |
| 65 | A study evaluating MIS for of colorectal cancer patients and learning basic laboratory techniques of molecular biology for miRNA extraction in colon and rectal cancer patients |
| 66 | Prospective study on the expression of cancer-testis antigen (CT45) in the patients of advanced epithelial ovarian cancer undergoing Hyperthermic Intraperitoneal Chemotherapy and its correlation with response to platinum-based chemotherapy |
| 67 | Pilot study to evaluate the role of Toluidine Blue Dye and Narrow Band Imaging for assessment of malignant and potentially malignant disorders in oral cavity and update and analysis of Oral Cancer Database |
| 68 | Clinical spectrum, patterns of care and outcomes of Indian cancer patients treated by Multidisciplinary team management |
| 69 | Understanding the impact of gut microbiome dysbiosis and metabolic alterations in the pathogenesis of early onset (EOCRC) Colorectal Cancer (CRC) |
| 70 | Evaluation of tumor derived exosomes in blood during pre and post treatment of pancreatic cancer patients |
| 71 | Role of Circulating Tumor DNA (ctDNA) As A Surrogate Marker in Ovarian Cancer - A Pilot Study |
| 72 | Assessment of cell free DNA (cfDNA) as a biomarker in common gastrointestinal track cancers |
| 73 | POCSS for PBCR -Head &Neck, Breast and Cervix cancers |
| 74 | Prospective evaluation of diagnostic imaging methods and its impact on surgical decision-making algorithm in the management of nodal disease in recurrent differentiated thyroid cancer and audit of the thyroid cancer database for evaluation of clinical and surgical spectrum and outcomes |
| S.no | Research Topics |
|---|---|
| 1 | Diversity of Oral microbiome of smokeless tobacco induced oral cancer patients as compared to tobacco chewers and non tobacco chewer healthy individuals- A metagenomic approach” |
| 2 | Metallic tumor markers for breast cancer. Design, development and clinical implications. |
| 3 | Evaluation of circulating cell free DNA as a prognostic marker in breast cancer |
| 4 | A study of Promoter Methylation of PTEN in Sporadic BREAST Cancer from North India |
| 5 | Analyzing FGFR2 and candidate genes affecting Its Downstream Signaling In Breast Cancer |
| 6 | A comprehensive analysis of mammalian target of rapamycin (mTOR) and mitogen activated protein (MAP) Kinase signaling pathways in non- small cell lung carcinoma |
| 7 | Role of Multiparametric MRI in Evaluation of Locally Advanced Rectal Cancer. |
| 8 | Circulating microRNAs as biomarkers for testicular germ cell tumors: A pilot study |
| 9 | Randomized control trial of combined EBRT plus HD brachy therapy boost versus EBRT alone with IMRT in intermediate & high risk prostate cancer. |
| 10 | Functional status and co morbidities of older patients with cancer |
| 11 | Molecular analysis of LIFR and YAP genes in Indian Breast Cancer patients |
| 12 | Molecular Analysis of lats2 and Fosp³ genes in Indian Breast Cancer patients |
| 13 | Expression studies of FOXO gene family in Indian Breast Cancer Patients |
| 14 | A study to assess the effectiveness of an educational package on knowledge regarding post-operative care of oral cancer patient’s relatives following discharge. |
| 15 | A study to assess the level of fatigue and presence of functional deficit in adult patients undergoing upfront surgery for solid tumors in pre and post-surgical phase in AIIMS |
| 16 | Differentiating inflammatory and metastatic mediastinal lymphadenopathy on 18-FDG- PET/CT in lung cancer: Role of steroid suppression |
| 17 | Etiology of oral cancer in Indian population younger than 30 years |
| 18 | Evaluation of HE4 level in epithelial ovarian cancer for diagnosis & monitoring of therapy |
| 19 | An economic analysis of alternative treatment methods of ovarian cancer in India: An appraisal of economic burden, quality of life and mortality risk. |
| 20 | Evaluation of Human Epididymis Protein 4 (HE4) level in the diagnosis of ovarian cancer |
| 21 | Bio-statistical Models for Evaluation of Lymph Node involvement among oral cancer patients |
| 22 | Role of Real Time Ultrasonography fused with PET-CT for image guidance and intervention: A nodal approach in management of Thyroid cancer” |
| 23 | Evaluation of the effect of Prosthodontic Rehabilitation on quality of Life and Psychological distress in Maxillectomy patients – A preliminary study |
| 24 | To evaluate whether a predictive microRNA signature from TCGA acts as a biomarker in Indian colorectal cancer (CRC) patients” |
| 25 | Dosimetric study in children and young adults with differentiated Thyroid cancer undergoing radioiodine (¹³¹I-Na) therapy” |
| 26 | Isolation Identification and characterization of cancer stem cells from different histopathological grades of colorectal carcinoma” |
| 27 | Association of HIPEC treatment with expression of T regulatory cells (FOXP3) in epithelial ovarian cancer and its clinical significance |
| 28 | Determining Surgical Resection Margin of Cancer by Rapid Molecular Assessment Using Mass Spectrometric Imaging |
| 29 | Hyperthermia and immune modulation in homologous recombination stratified epithelial ovarian cancer: Development of targeted therapeutic approaches |
| 30 | The phase 2 study of HIPEC and the proposed phase 3 RCT comparing between HIPEC and IP chemotherapy. |
| 31 | A prospective study to elucidate molecular genetic risk factors of gallbladder carcinoma in Indian Population |
| 32 | Role of nuclear receptors in pathogenesis of carcinoma gall bladder |
| 33 | Molecular and Genetic Analysis of TNBC |
| 34 | Hyperthermia and immune modulation in homologous recombination stratified epithelial ovarian cancer: Development of targeted therapeutic approaches |
| 35 | The phase 2 study of HIPEC and the proposed phase 3 RCT comparing between HIPEC and IP chemotherapy. |
| 36 | Role of nuclear receptors in pathogenesis of carcinoma gall bladder |
| 37 | Study of a Surrogate Panel of Immunohistochemical and Molecular Markers to Classify Human Colorectal Carcinomas as per the Consensus Molecular Subtypes and Clinical Correlation |
NCI-AIIMS, Jhajjar campus presently has 25 operational ICU beds during Phase 1. The capacity will be expanded to 50 beds. The ICU is equipped with state of art machines and is managed by specialist doctors (Department of Onco-anesthesia), dedicated nursing officers and technicians.
Dr. BRA-IRCH, AIIMS, New Delhi has a dedicated 6 bedded ICU setup.

Department of Surgical Oncology has 8 state of art major operation theatres for performing various kinds of major cancer surgeries. In addition, one emergency operation theatre is dedicated for emergency surgeries.
All the major operation theatres are well equipped with a range of modern and contemporary machinery and equipment required to perform various types of complex cancer surgeries involving various organ systems viz. intra-operative fluorescence imaging, gamma cameras, intra-operative nerve monitoring, HIPEC machines, ILP machine, laparoscopic units, modular OT tables, operating microscope, argon plasma coagulator etc. Robotic units are under the due process of procurement and will soon be operational. An operation theatre designed to institute Intra-operative Radiotherapy (IOHDR) will be operational in phase 2.
The special surgical programs being provided for in the major OT are Robotic and Minimally Access Surgery, Palliative Surgery, Peritoneal Surface Malignancies, Microvascular Reconstruction, Risk Reducing Surgery and Intra-operative Radiation Therapy.

State-of-the-art Modular Operation Theatres

Former MOHFW Shri JP Nadda visiting the Operation Theatres

First surgery at NCI-AIIMS, Jhajjar being performed by Prof. SVS Deo
The department has a Minor O.T complex in the Hospital Block at NCI. Post-operative care is provided in the OPD block.
Minor operative procedures:
Biopsies for confirmation of cancer including Core needle, punch, incision or excision biopsy & FNAC.
Removal of small superficial cancers under local anesthesia.
Placement of long term venous access devices for chemotherapy (Hickman catheters/Chemoport)
Patients of Gastro-intestinal, Genitourinary, Gynaecological, Thoracic and Head and Neck cancers require endoscopy procedure for confirmation and evaluation of cancer. The department of Surgical oncology is offering the following Endoscopy services for cancer patients at NCI-AIIMS, Jhajjar.
Diagnostic Endoscopy :
Therapeutic Endoscopy :

National Cancer Institute (NCI-AIIMS), Jhajjar campus – The surgical oncology services is presently providing patient care on 80 beds. The department will eventually have 200 beds and 18 OTs in subsequent phases
Dr. BRA-IRCH, AIIMS, New Delhi is a 182 bedded hospital and Surgical Oncology services cater to a total of 48 beds (including 5 private ward beds) and 4 dedicated OTs.

Schedule of OPD & Clinics
| Day | Morning (9 AM – 1 PM) | Room | Afternoon (2 PM – 5 PM) | Room |
|---|---|---|---|---|
| Monday | - | - | Breast Cancer Clinic (BCC) | Board Room |
| Head & Neck Cancer Clinic (A) | Room 5 | |||
| Tuesday | Surgical Oncology OPD | Board Room | - | - |
| Genitourinary- Gynecology (GUG) Cancer Clinic | Room 59 | |||
| Wednesday | Thoracic Oncology Clinic | Room 5/7 | Gastro-intestinal Cancer (GIC) Clinic | Room 5 |
| Thursday | Surgical Oncology OPD (9am – 12 noon) | Board Room | Bone & Soft Tissue (B&ST) | Board Room |
| Friday | Genitourinary-Gynecology (GUG) Cancer & Peritoneal Surface Malignancy (PSM) Clinic | Room 59 | Breast Cancer Clinic | Board Room |
| Head & Neck Cancer Clinic (A) | Room 5 | |||
| Hepatobiliary & Pancreatic (HPB) Cancer Clinic | Room 6/7 | |||
| Saturday | Surgical Oncology Rehabilitation & Physiotherapy/Ostomy Care Clinic | Board Room/Minor OT 9B | - | - |
| Cancer Genetics Clinic | Room 6 | - | - |
Department of Surgical Oncology offers following opportunities for training –
For Rules and Regulations–
For Enquiry regarding Training & Observerships – Contact
Prof SVS Deo
Head of Department
Department of Surgical Oncology
011-29575234
svsdeo@yahoo.co.in
| S.no | Name | Details |
|---|---|---|
| 1 | Stem cell transplantation | Stem cell transplantation is routinely being done at IRCH AIIMS since 1995. Primary indication for allogeneic BMT includes – Acute leukemia and severe Aplastic anemia for autologous stem cell transplant, major indications include – myeloma and Lymphomas |
| Test done | Details & Rates | Cost |
|---|---|---|
| RT-PCR | Quantitative PCR For BCR Abl translocation (p210, p190) | Rs. 2200/ test |
| Cytogenetics | For Philadelphia Chromosome | Rs. 500/ test |
| Haemogram | Complete blood counts | NIL |
| Flow cytometeric analysis | CD 34 counts | Rs. 1200 / test |
| Harvesting and cryopreservation | Storage of stem cells at 80 C | Rs. 32000/ Cycle |
| Harvesting and cryopreservation | Storage of stem cells at 196 C | Rs. 38000 / Cycle |
| ELISA for galactomannan | - | NIL |
| Serum Magnesium | - | NIL |
| S.no | Unit | No. of Beds |
|---|---|---|
| 1 | Medical Oncology | 30 |
| 2 | DayCare | 30 |
| 3 | BMT | 8 |
| S.No | Name of the OPD/Unit | Day/Time |
|---|---|---|
| 1 | Chemotherapy Evaluation | Monday 9AM onwards Wed. 9AM onwards Thursday 9AM onwards Friday 9AM onwards |
| 2 | LL Clinic (Lymphoma/Leukemia) | Wednesday 2 PM onwards Thursday 2 PM onwards |
| 3 | Breast Clinic | Monday 2 PM onwards Friday 2 PM onwards |
| 4 | GE Clinic | Wednesday 2 PM onwards |
| 5 | H & N clinic | Monday 2 PM onwards Friday 2 PM onwards |
| 6 | Gynae. Cancer Clinic | Wednesday 2 PM onwards Saturday 9AM onwards |
| 7 | Ophthalmic tumour Clinic | Thursday 3.30 PM onwards |
| 8 | BMT Clinic | Friday 9 AM onwards |
| 9 | Bone & Soft Tissue Clinic | Thursday 2 PM onwards |
| 10 | Urology Clinic | Thursday 11 AM onwards |
| 11 | Pediatric Surgery clinic | Thursday 2 PM onwards |
| 12 | Lung Cancer Clinic | Tuesday & Friday 9 AM to 1 PM |
| S.No. | Name of the Course | Details of Admission |
|---|---|---|
| 1 | Ph.D Medical Oncology | All India Open Entrance Examination |
| 2 | DM Medical Oncology | All India Open Entrance Examination |
The department of medical oncology was established in 1984 and since its inception, it has excelled in clinical, teaching, and research activities.
The department provides its services in adult and pediatric hematological and solid malignancies, and runs several clinics, including, but not limited to leukemia, myeloma and lymphoma, head and neck cancers, breast cancer, lung cancer, gastrointestinal cancers, pediatric cancers, genitourinary cancers, gynecological cancers, ophthalmic cancers, bone and soft tissue cancers, and brain tumors. Several daycare procedures including bone marrow aspirate, biopsy, thoracocentesis, pleurocentesis, intrathecal chemotherapy, etc are performed Clinics are run on all working days, providing consults to over 15,000 patients annually. In addition, state-of-art stem cell transplant services are provided that includes autologous, matched sibling, haploidentical, umbilical cord, and matched unrelated transplants in a dedicated stem cell transplant ward.
Medical Oncology department runs a DM and a PhD programme, for which a national competitive exam is held every six months.
This department proudly owns its laboratory where RT- PCR, FISH, cytogenetics, tissue culture, and Flowcytometry etc. have already been standardized. Stem cell storage is carried out routinely; and blood component therapy is provided with the help of cell separator.
Medical Oncology has been actively working with various NGO’s to increase cancer awareness in schools and in the communities. Medical oncology faculty has been participating in many Continuing education programs/workshops/symposia conducted by Medical Oncology on various topics regularly over the last several years including hemato-oncology, cancer screening and awareness, lung cancer, cancer team management, colorectal cancers, hematopoietic stem cell transplants etc.
The department has published several research articles in high-indexed peer-reviewed scientific journals, including Journal of Clinical Oncology, Annals of Oncology, European Journal of Cancer, etc.
(2020-2022)
| Year | Name | Duration | |
|---|---|---|---|
| 2015 | Dr. Anuja Pandit | anujapandit@yahoo.co.in | (2015-18) |
| 2015 | Dr. Brajesh Kumar Ratre | brajesh.ratre@gmail.com | (2015-2019) |
| 2015 | Dr. Shweta Arun Bhopale | dr.shweta610ab@gmail.com | (2015-2019) |
| 2015 | Dr. Rohini Dattatri | rdattatri2@gmial.com | - |
| 2015 | Dr. Anuradha Patel | patelanuradha20@gmail.com | - |
| 2015 | Dr. Mahima Gupta | mahhima@gmail.com | - |
| 2015 | Dr. Kinshuki Jain | dockinshukijain@gmail.com | (2016-20) |
| 2015 | Dr. Wasimul Huda | wasu077@gmail.com | - |
| 2016 | Dr. Rudranil Nandi | drrudranilnandi@gmail.com | (2016-20) |
| 2016 | Dr. Swati Bhan | swatibhan6@gmail.com | (2016-19) |
| 2016 | Dr. Saurarbh Vig | saurabh377@yahoo.com | (2016-19) |
| 2016 | Dr. Prashant Sirohiya | sirohiyaprashant@gmail.com | (2016-19) |
| 2016 | Dr. Ram Singh | dr.ram2001@gmail.com | (2016-19) |
| 2016 | Dr. Praneeth Suvvari | praneethsuv@gmail.com | (2016-20) |
| 2016 | Dr. Anuja Pandit | anujapandit@yahoo.co.in | (2016-18) |
| 2016 | Dr. Punit | punit.spmc@gmial.com | (2016-19) |
| 2016 | Dr. Nandan Choudhary | drnandanchy@gmail.com | (2016-19) |
| 2017 | Dr. Anuradha Patel | patelanuradha24@gmail.com | (2017-20) |
| 2017 | Dr. Astha | koolestastha@gmail.com | (2017-20) |
| 2017 | Dr. Ajisha Abubakker | aaji.008@gmail.com | (2017-20) |
| 2017 | Dr. Shikhar More | shikharmore@gmail.com | (2017-20) |
| 2017 | Dr. Manisha Pandey | manishapandey29122015@gmail.com | (2017-20) |
| 2017 | Dr. Rahul D Arora | xerxes85@ymail.com | (2017-20) |
| 2017 | Dr. Shilpi Agarwal | drshilpi87@gmail.com | (2017-20) |
| 2017 | Dr. Rohini Dattatri | rdattatri2@gmail.com | (2017-20) |
| 2017 | Dr. Mahima Gupta | mahima@gmail.com | (2017-20) |
| 2017 | Dr. Vikram Pratap Singh | vps1907@gmail.com | (2017-20) |
| 2017 | Dr. Abhity Gulia | drabhity.mamc@gmil.com | (2017-20) |
| 2018 | Dr. Neha Singh | nehasingh140792@gmail.com | (2018-21) |
| 2018 | Dr. Himanshu Prince Yadav | drhimanshuprince@gmail.com | (2018-20) |
| 2018 | Dr. Swarnbala Solanki | drswarnbalasolanki@gmail.com | - |
| 2018 | Dr. Goyir Gangkak | goyir.gangkak@gmail.com | (2018-19) |
| 2018 | Dr. Akansha Sangwan | akansha_sangwan@yahoo.com | (2018-20) |
| 2018 | Dr. Aditya | adi.gatsby@hotmail.com | (2018-21) |
| 2018 | Dr. Vishnu Panwar | vishnupanwar6767@gmail.com | (2018-21) |
| 2018 | Dr. Deepti Ahuja | deeptiahuja2252@gmail.com | (2018-21) |
| 2018 | Dr. Sapna Singla | sapnasingla08@gmail.com | - |
| 2018 | Dr. Balbir Kumar | drbalbir10@gmail.com | (2018-19) |
| 2018 | Dr. Aditi Suri | aditisuri18@gmail.com | (2018-21) |
| 2018 | Dr. Shruti Garolia | shrutigarolia@gmail.com | (2018-21) |
| 2018 | Dr. Abhishek Kumar | abhishekk73102@gmail.com | (2018-21) |
| 2018 | Dr. Kiran Mahendru | kiranmahendru.aol@gmail.com | (2018-21) |
| 2018 | Dr. Riniki Sarma | riniki_rs@hotmail.com | (2018-21) |
| 2018 | Dr. Swagata Biswas | manibiswas58@gmail.com | (2018-21) |
| 2019 | Dr. Ruchi Singh | instantruchi@gmail.com | (2019-22) |
| 2019 | Dr. Karthik.AR. | arkarthik1234@yahoo.com | (2019-22) |
| 2019 | Dr. Khushboo Pandey | khushboo0411@gmail.com | (2019-22) |
| 2019 | Dr. Mahajan Jitendra Subhash | jitendrassm@gmail.com | (2019-22) |
| 2020 | Dr. Pratishtha Yadav | pratishthayadav88@gmail.com | (2019-22) |
| 2018 | Dr. Bhanu Pratap Singh | bhanumaurya9@gmail.com | (2018-21) |
| 2018 | Dr. Neethu Susain Abrahim | neethu.march30@gmail.com | (2018-21) |
| 2018 | Dr. Raghav Gupta | raghavgupta88@gmail.com | (2018-21) |
| 2018 | Dr. Amrit Kaur | kauramrit.25@gmail.com | (2018-19) |
| 2019 | Dr. Shreya Das Adhikari | drshreyadasadhikari@gmail.com | (2018-20) |
| 2019 | Dr. Nitish Thakur | nitishthakur@outlook.com | (2019-20) |
| 2019 | Dr. Alka Yadav | alkayadava@gmail.com | (2019-22) |
| 2019 | Dr. Bikash Anand | bikash.govial@gmail.com | (2019-22) |
| 2019 | Dr. Rajeshwari R | (2019-19) | |
| 2019 | Dr. Krishan Priya | krishnapriyasreelakam1992@gmal.com | (2019-22) |
| 2019 | Dr. Bhawesh Pangaria | bhawesh.pangaria@gmail.com | (2019-22) |
| 2019 | Dr. Ruparna Khurana | ruparna@gmail.com | (2019-2022) |
| 2019 | Dr. Raunak Chakarborty | raunaq.chakraborty@gmail.com | (2019-20) |
| 2019 | Dr. Swati Choudhary | drswati90@gmail.com | (2019-21) |
| 2019 | Dr. Karthik AR | arkarthik1234@yahoo.com | (2019-22) |
| 2019 | Dr. Swagata Biswas | manibiswas58@gmail.com | (2019-22) |
| 2019 | Dr. Ruparna Khurana | ruparna@gmail.com | (2019-22) |
| 2019 | Dr. Priyanka Dixit | pridixit1005@gmail.com | (2019-22) |
| 2019 | Dr. Tuhin Mistry | tm.tuhin87@gmail.com | (2019-2019) |
| 2019 | Dr.Gyanendra kumar | Gyanekumar@yahoo.com | - |
| 2019 | Dr.Pradeep parmar | drpksparmar@yahoo.com | (2019-2019) |
| 2019 | Dr.Jitender Sirohiya | dr.jitendersirohioya@gmail.com | (2019-2022) |
| 2019 | Dr.Sanjeev Kumar | strongindians@gmail.com | (2019-2022) |
| 2020 | Dr.Rumit Sood | rumitsood111@gmail.com | (2020-2023) |
| 2020 | Dr. Manisha | manishapandey29122015@gmail.com | (2020-2023) |
| 2021 | Dr. Neha Singh | nehasingh140792@gmail.com | (2021) |
| 2021 | Dr. Bhanu Pratap singh | bhanumaurya9@gmail.com | (2021) |
| 2021 | Dr. Neethu Susan | neethu.march30@gmail.com | (2021) |
| 2020 | Dr. Ankita | anki.dhir08@yahoo.co.in | (2020-2023) |
| 2020 | Dr. Meet Minarey | drmeetminarey@rediffmail.com | (2020-20) |
| 2020 | Dr. Amit Kumar | amit2007kr@gmail.com | - |
| 2022 | Dr.Nengneivah Haokip | vahsyzongku@gmail.com | (2022-2023) |
| 2022 | Dr. Nengneivah Haokip | vahsyzongku@gmail.com | (2022-2023) |
| 2020 | Dr. Alice | dralicethankachan@gmail.com | (2020-2023) |
| 2020 | Dr. Pratyasa Padhi | pratyasa95@gmail.com | (2020-2023) |
| 2022 | Dr. Anurag Sarkar | dr.anuragsarkar@gmail.com | (2020-2023) |
| 2020 | Dr. Himanshu Varshney | docvarshney.in@gmail.com | (2020-2023) |
| 2021 | Dr. Karanvir Singh Matharoo | singhkaranvir328@gmail.com | (2021) |
| 2021 | Dr. Shunmuga Priya.I.C | priyamaanaveeran@gmail.com | (2021) |
| 2021 | Dr. Saruafrashi Saraswata Mahapatra | satyaswayam@gmail.com | (2021) |
| 2021 | Dr. Abhinav Mishra | abhiharvis619@gmail.com | (2021) |
| 2021 | Dr. Bishnu Prasad Shrestha | bipeeshrestha@gmail.com | (2021) |
| 2021 | Dr.Revathy Vijaya kumar | revu2rahul@gmail.com | (2021) |
| 2021 | Dr. Mangaleswari.V | mangaleswariv.994@gmail.com | (2021) |
| 2021 | Dr. Suhana Sulfiker | suhanasulfiker@gmail.com | (2021) |
| 2021 | Dr. Prateek Gandhi | prateek8265@outliik.com | (2021) |
| 2021 | Dr. Arknil | docgainarkanil@gmail.com | (2021) |
| 2020 | Dr. Jadhav Ramanand Vijayanand | rvj4me@gmail.com | - |
| 2020 | Dr. Kanika Rustagi | drkanika1@gmail.com | (2017-20) |
| 2020 | Dr. Shallu Goel | goel.shallu90@gmai.com | - |
| 2020 | Dr. Shweta | drshweta2309@gmail.com | (2020-21) |
| 2021 | Dr. Jasmeet Gill | jess.scorpio@gmail.com | (2021-21) |
| 2021 | Dr. Nidhi Gupta | nidhi790@gmail.com | (2021-21) |
| 2021 | Dr. Ayushi Agarwal | ayushiagarwaldr@gmail.com | (2021-22) |
| 2021 | Dr.Madhu Smita | madhusmita.gmc@gmail.com | (2021) |
| 2021 | Dr. Surjyendu Ghosh | surja.rgkmch@gmail.com | (2021-2022) |
| 2021 | Dr.Bora Hemalatha | borahemalatha@gmail.com | (2021) |
| 2021 | Dr.Raghav Gupta | raghavgupta88@gmail.com | (2021) |
| 2021 | Dr.Sonal | lanos.yadav1027@gmail.com | (2021) |
| 2021 | Dr.Renoxy Bansal | renoxybansal@gmail.com | (2021-2022) |
| 2021 | Dr.Karthik.p.Vasist | karthikpvassist@gmail.com | (2021) |
| 2022 | Dr.Aanchal Malik | aanchalmalik955@gamil.com | (2022) |
| 2022 | Dr.pavneet Kochar | neet.kochar7555@gmail.com | (2022) |
| 2022 | Dr.Sonam Patel | 2009mhhs.sonam@gmail.com | (2022) |
| 2022 | Dr.Vasudha Ahuja | vasudha.ahuja26@gmail.com | (2022) |
| 2022 | Dr.Akhila Swarnakumar | akhilaicg@gmail.com | (2022) |
| 2022 | Dr. Vishnu Charan Thiriveedhi | visitvishnucharan@gmail.com | (2022) |
| 2022 | Dr. Dervina Juneja | juneja.devina1995@gmail.com | (2022) |
| 2022 | Dr. Khushboo Mandal | khushboo697@gmail.com | (2022) |
| 2022 | Dr. Pooja | poojakrishna.sajeev@gamil.com | (2022) |
The following Academic Courses are being conducted under the department:
The Services of Onco-Anaesthesia, Intensive Care, Pain and Palliative Medicine are an integral part of National Cancer Institute, Jhajjar, All India Institute of Medical Sciences. The Department works alongside the department of Onco-Anaesthesia and Palliative Medicine, Dr.BRAIRCH under the able headship of Dr (Prof) Sushma Bhatnagar. The department provide services to anesthesiology, intensive care, pain and palliative care and emergency medicine as well. All of them are professionally qualified anesthesiologists and critical care physicians and have gained experience as palliative care personnel in the advanced cancer patients referred for pain and other symptom management. They have many years of teaching experience as well.
The mission of the Department is to provide state-of-art and comprehensive care for patients with cancer with both curative and palliative intent. It includes services for various diagnostic interventions, surgical procedures, pain and palliative procedures. The department has a 24-bedded palliative care ward for providing inpatient palliative care of oncology patients which provides round the clock services for acute and chronic pain management as well. The ward has well trained nursing staff and physiotherapist for improving the quality of life for cancer palliative care. The department also manages one operation theatre dedicated for interventions in palliative care patients for symptom and pain management.
The department has 25-bedded intensive care unit which provides care for critically ill patients from surgical oncology, medical oncology and radiation oncology departments. The ICU is well equipped with state-of-art technology and well-trained manpower.
The department provides comprehensive care for the surgical procedures. It has pre-anaesthetic clinic for preoperative evaluation and optimization for surgical interventions. The operating rooms are well equipped with state-of-art infrastructure including anesthesia workstations and other ancillary equipments like invasive monitoring devices, intubating fiberscope, ultrasound machines etc. The centre has well equipped recovery area providing immediate care to postsurgical patients. All surgical patients receives acute pain management services round the clock supervised by the faculty. The department provides point of care technology with ultrasound for diagnostic (vascular access, nerve blocks, volume responsiveness assessment, and for therapeutic purposes (pleurocentesis, optimization of cardiovascular function in various types of shock) in the operating room, palliative care ward and Intensive care
The department provide emergency services including airway management and ventilatory support to patients admitted with other specialties like surgical oncology, medical oncology and radiation oncology. The services for management of pain due to chemotherapy or radiation therapy are also provided to these departments round the clock.
We also run OPDs 5 days in a week where we examine and treat cancer pain patients and admit patients if required to the palliative care. In theses OPDs we also see patients for pre anesthesia check ups.
Via NH48:
Via Dwarka Expressway
Train to Jhajjar:
State Transport Buses:
Bus from Tilak Nagar terminal (Bus No. 827)
Haryana Roadways Bus from Gurugram.
Metro to Dwarka Sector 21 (Blue line):
Metro Blue line to Dwarka metro station then Grey line to Najafgarh
Prof Alok Thakar
Prof Sunil Kumar
Past Event:
Photo:
Past events:
Past conferences
The hostel facilities at the National Cancer Institute (NCI) in Jhajjar are strategically located away from the hustle and bustle of the city, providing a serene environment that is close to nature. This tranquil setting helps create a calming atmosphere, which is especially beneficial for patients and their families during treatment.
Here are some key aspects of the hostel's location:
This emphasis on a nature-focused environment complements the comprehensive care approach at the NCI.
Amenities available in the hostel rooms:
Basic Amenities
Cafeteria Facilities
Bathroom Facilities
Connectivity
Safety and Security
Additional Facilities
The staff residential quarters at NCI Jhajjar provide accommodation for employees and their families. These quarters are designed to offer a comfortable living environment with various amenities. At NCI Jhajjar, the staff residential quarters typically include different types of accommodations, such as:
Types of Accommodations
Facilities Available
Application Process
At the National Cancer Institute (NCI) in Jhajjar, free e-vehicle transport facility is provided for patients. This service facilitate access to healthcare services.
Patient accommodation at the National Cancer Institute (NCI) in Jhajjar typically includes a range of facilities designed to provide comfort and support for patients undergoing treatment. Here are some key aspects:
At NCI patients are managed by single window DMG mode. A group of experts from relevant departments attend DMG to discuss all cases and plan the course of treatment.
Common symptoms of cancer can vary depending on the type and location, but some general signs to watch for include:
While not all cancers can be prevented, many can be reduced through certain lifestyle choices and preventive measures. Here are some key strategies:
Several types of cancer have established screening protocols to help detect them early. Here are some common ones:
There are vaccines that can help prevent certain types of cancer:
Cancer treatment typically involves several main modalities, often used in combination. Here are the primary treatment options:
Cancer can have a genetic component, but it's not solely determined by genetics. Here’s a breakdown:
Alternative treatments for cancer are often used alongside conventional therapies, but their effectiveness can vary. Here’s an overview:
Overall, it's crucial to approach cancer treatment with a well-informed and collaborative strategy, incorporating evidence-based practices while considering individual preferences. Always consult with a healthcare professional before making treatment decisions.
A long delay in treatment can be detrimental to cancer patients' outcomes for several reasons:
If there are concerns about delays in treatment, it's important for patients to communicate openly with their healthcare team to explore all options and strategies for timely intervention.
The National Cancer Institute (NCI) in Jhajjar, India, offers a range of comprehensive cancer treatment facilities, including:

Head of NCI
Prof Alok Thakar, MS
Prof and Head
Department of H&N Oncology
Message of the Head
As we continue our fight against cancer, I want to take a moment to reflect on our collective efforts and the progress we’ve made. The journey is challenging, but our commitment to advancing research, improving patient care, and enhancing public awareness remains steadfast.
Our dedicated team at the National Cancer Institute is working tirelessly to develop innovative treatment options and to make cutting-edge therapies accessible to all. We are also prioritizing education and outreach to empower individuals with knowledge about prevention and early detection.
Collaboration is key to our success. I encourage each of you to continue fostering partnerships within the medical community and beyond. Together, we can make significant strides toward reducing the burden of cancer.
Thank you for your unwavering dedication and support. Let’s remain united in our mission to improve lives and conquer cancer.
Warm regards
One of the principal goals of the institute is the education and training of the next generation of stem cell researchers and the physicians who will practice regenerative medicine. The institute fosters this goal through graduate education, post-doctoral employment, and medical school coursework.
The Stem Cell Facility offers an interdisciplinary doctoral program in stem cell biology and regenerative medicine. The program integrates studies in basic and clinical sciences to create a doctoral program designed to foster a translational approach to biomedical research.
| Sr. Residents | 2 nos. |
| Jr. Residents | 10 Nos. |
Er. Deepak Bhutale is incumbent Superintending Engineer of AIIMS, New Delhi & its associated Centers & sub-centers except National Cancer Institute (NCI), Jhajjar which is being presently headed by Er. Pradeep Kumar. Under each Superintending Engineer there are mainly three sections of engineering i.e. Civil, Electrical, and AC&R. Further, these sections are divided into various divisions headed by Executive Engineers, and all the Divisions have their own setup of Engineers, staff (Regular/outsourced) for effectively running the infrastructure of AIIMS.
Er. Deepak Bhutale Superintending Engineer, ESD, AIIMS, New Delhi & its allied Centres & sub-centres Email: supdt.engg.aiims@aiims.edu Tel:- 26594782 | |||
| Executive Engineer | Assistant Engineer | Junior Engineer | Allotted Area |
CIVIL DIVISION-I (Er. Anuj Agrawal) Email: anuj.a@aiims.gov.in anujag69@gmail.com Tel:- 26594731 | Er. R.N. Deogam Phone: 9958178586 | Er. Zeeshan Athar Phone: 8826600550 | Main Hosp, Ward block, Emergency, CCSD, Medical Store, Manifold Old RAK OPD. |
Er. Haider Ali Phone: 9991206632 | Old RAK OPD (under the guidance of Er. Zeeshan Athar) | ||
Er. Dilip Gurjar Phone: 9868396991 | PC & Teaching Block, PMR, NMR, Convergence Block, J. L. Auditorium, Nurses Lecture Theater, CMET, B.B.D. Library, Admin Block. | ||
Er. Rajesh Mann Phone: 9868397876 | Er. Mohd. Naem Phone: 9868397857 | Biotech, CAF, Transport, Store (DO), Gymkhana, Laundry, CWC, Mortuary, Hostel (1-8). | |
Er. Ashish kr. Verma {ASW-II} Phone: 7007997726 | Girls Hostel (9, 10, 11) & RPC Hostel (12, 13). | ||
Er. Atir Hasan Saifi Phone: 9811396992 | Hostel (14-19) | ||
Er. Dinesh Kumar (Circle planning) Phone: 9868397872 | Er. Munesh Kr. Meena Phone: 9694635401 | Residences @ East Ansari Nagar, Director bungalow, Community Centre, Guest house | |
Er. Guddu Paswan Phone: 8210811880 | Circle planning, Residences @ West Ansari Nagar, Rajgharia & Sai Vishram Sadans. | ||
Er. Abdesh Kumar (new) Phone: 8955261660 | I-type qtrs & West Ansari Nagar under the guidance of Er. Guddu Paswan | ||
Er. Rakesh Kumar Phone: 9992068041 | Residences @ Masjid Moth. | ||
Er. Shadab Ali Phone: 9868397871 | Er. Shubham Sharma Phone: 9914093364 | CRHSP Ballabhgarh | |
Er. Rakesh Kumar Phone: 9992068041 | NDDTC Ghazibad | ||
CIVIL DIVISION-II & Circle Planning, ESD (Er. Devender Kumar) Email: devenderkr@aiims.gov.in dkaiims.esd@gmail.com deven_kumar@hotmail.com Tel:- 26594869 | Er. Sanjeev Kumar Phone: 9868398030 | Er. Kuljeet Dhiya Phone: 8168764125 | CDER, Dr. BRAIRCH. |
Er. Md. Modassir Phone: 9868397850 | CNC, CN Tower. | ||
Er. Narayan Karmarkar Phone: 9868397859 | Dr. RPC, NPW, PW-III, Old OT, CCM, College of Nursing. | ||
Er. Anil Kumar Sharma Email: anilsharma.jpnatc@gmail.com Phone: 9868397974 | Er. Ravinder Kumar Phone: 9467871269 | External Services | |
Er. Satish Kumar Phone: 9868397877 | External Services | ||
| Er. Narender | Horticulture | ||
Er. Sanjay Jain Phone: 9868397875 | Er. Ritvik Mishra Phone: 9811169563 | New RAK OPD, MCH; UG Parking. | |
Er. Harsh Tiwari Phone: 9911571764 | NCA, Surgical Block | ||
Er. Raj Priyadarshan Phone: 8051428699 | (ASW-II) | ||
| - | RKAK Guest House, Shimla. | ||
Er. Pankaj Gupta Phone: 9868397873 | Er. Rahul Kumar Phone: 9868396994 9990767350 | Residences @ A.V. Nagar. | |
Er. Sahil Yadav Phone: 7015189669 | Residences @ FTA & Asiad Village. | ||
Er. Sunil Mehra Phone: 9711444523 | Er. Suraj Phone: 8799736799 | (Circle Planning) | |
CIVIL DIVISION-III & Appellate Authority, ESD (Er. Deepak Bhutale) Email: deepak.bhutale@aiims.gov.in Tel:- 26594820 | Er. Sanjay Kumar Jain Phone: 9868397884 | Er. Jatin Singh Phone: 9868396994 | Trauma Centre campus, Power Grid Vishram Sadan, External. |
Er. K.D. Biswal Phone: 9868397870 | Er. Sadiq Qamar Phone: 9868396990 | Divisional Planning ASW-I (CD-III & CD-IV). | |
CIVIL DIVISION-IV (Er. Sunil Kumar) Email: sunil.kumar@aiims.gov.in Tel:- 26731206 | Er. Sanjay Kumar Jain Phone: 9868397884 | Er. Suraj Phone: 8799736799 | Burns & Plastic Block. |
ELECTRIC DIVISION-I & CPIO, ESD
(Er. Pradeep Kumar) Email: eeelect1aiims@gmail.com pradeep.kumar2@aiims.gov.in Tel:- 26594894 | Er. Manoj Kumar (Circle Planning) Phone: 9868397889 | Er. Zulfikar Ali Phone: 9868397860 | Main hosp, PC & Teaching Block, PMR, NMR, Convergence, Admin. Block. |
Er. Kumar Saurabh Phone: 9868397861; 9873607761 | Ward Block & old private ward. | ||
Er. Deepak Kumar Phone: 9315346783 (Divisional Plann) | Old RAK OPD; DG sets & Lifts of (Main Hosp., Old RAK OPD, PC & Teaching Block). | ||
| - | Shimla Guest Hous> | ||
Er. Kamaldeep Phone: 7988364845 (Divisional Plann) | Under supervision of JE Deepak Kumar | ||
Er. Satbir Kumar Phone: 9868397892 | Er. Sharat Kumar Rana (Circle Planning .) Phone: 9868398036 |
Dr. RPC, CNC, C.N. Tower. | |
Er. Sandeep Phone:- 8527368655
| Dr. BRAIRCH. | ||
Er. Gaurav Kumar Phone: 9868396997 | CDER,CRHSP Ballabhgarh & associated Centres. | ||
Er. Ravi Kumar Meena Phone: 7891164772 | NDDTC Ghazibad, Trilokpuri, NPW, old OT, CCM, Nursing College. | ||
Er. Mahender Singh Phone: 9868397843 | Er. Anand Kumar Phone: 9868397896 | All Hostels in MM Campus (11-19). | |
Er. Prateek Verma Phone: 9068884916 | All Hostels in East Ansari Nagar Campus (1-10). | ||
ELECTRIC DIVISION-II & Divisional Planning (Elect.) (Er. Dinesh Kr. Jhakhad) Email:dinesh.j@aiims.gov.in dkjaiims@gmail.com Tel: 26593666 | Er. Rajneesh Kumar Phone: 9868398031 | Er. Uma Shankar Phone:9868396996; 8059771087 | New RAK OPD, Surgical Block. |
Er. Kumar Vivekanand Phone: 9667330935 | MCH; NCA; 2MLD STP. | ||
Er. Amit Phone: 8295116056 | Private Ward-III. | ||
Er. Sanjeev Godwin (Telephone Services; Divisional Planning Elect) Phone: 9868397871 | Er. Prashant Kumar Phone: 9868396998 | JPNATC, Vertical Expansion. | |
Er. Chintala Himagiri Phone: 9642120545 | Burns & Plastic Block, Power Grid Vishram Sadan. | ||
Er. Vijay Singh Phone: 9868397995; 8929919735 | Er. Prem Dutt Phone: 9868398033; 9871968687 | (AV Nagar, FTA & Asiad Village) residential Campus. | |
Er. Himanshu Ranjan Phone: 8920671678 | MM Residential Campus; UGP; Bio-Tech; Animal House; Transport Garage; Gas plant; Main STP; Laundry Cum Workshop; Mortuary. | ||
Er. Vimal Kumar Pabri Phone: 9024481748 | Eastern-Western residential Campus; Street lights, External Services; Rajgarhia Vishram Sadan 1&2 & Sai Vishram Sadan, Cent. Store (E). | ||
AC&R DIVISION (Er. D. Vijayaraghavan) Email: d.vijay@aiims.gov.in raghavanaiims@gmail.com Tel: 26594819 | Er. Inderjeet Singh Phone: 9868397997 | Er. Mohit Kumar Phone: 9855324092 | Main institute, PC & Teaching Block, Ward Block, Emergency Medical store, Foyer, Old RAK OPD, Convergence Block, Admin Block, BB Diksit library, NPW, NPW-III, Old OT, Nursing College, CCM, CMET, Bio-tech, CAF, Mortuary, CWC, Laundry. |
Er. Subhash Chand Phone:- 9868397993 | Er. N. Moize Phone: 8860648815 | Dr. R.P. Centre, C.N.Centre, C.N. Tower, Dr. BRAIRCH & CDER, expansion projects etc. | |
Er. Sudhesh Jain Phone: 9868397897 | Er. Dinesh Kr. Meena Phone: 9950169171 | New RAK OPD, MCH, Surgical Block, NCA, Underground Parking, Hostels (1-19), EAC, coordination of Division office. | |
Er. Dinesh Pal Phone: 9868397893 | Er. Satya Prakash Phone: 9911067743 | Trauma Centre, Burns & Plastic Block, allied Vishram Sadans & external services of East & West Campus, A.V. Nagar, Asiad Village; CRHSP Ballabgarh, NDDTC Ghaziabad including associated sub-centers, Divisional Planning (AC&R) | |
Er. Pradeep Kumar Superintending Engineer, NCI, Jhajjar Email: se.nci@aiims.gov.in Tel: 012-51274026 | |||
| Executive Engineer | Assistant Engineer | Junior Engineer | Allotted Area |
CIVIL DIVISION (Er. Sunil Kumar) Phone: 9868397878 | Er. Sunil Mehra Phone: 9711444523 | Er. Gauri Shakar Phone: 8929643699 | Capital Works hosp. & residential area |
Er. Deepak Yadav Phone: 9996956888 | Preventive maintenance hosp. & residential area | ||
Er. Mohd. Talib Phone: 9467792147 | Preventive maintenance of Outreach OPD | ||
ELECTRIC DIVISION (Er. Dinesh Pal) Email: dineshaiims84@yahoo.com Tel: 01251-274957 | Er. Pravin Patharbe Phone: 9711708802 | Er. Shudansu Gautam Phone: 8929643702 | Residential & Outreach OPD area-Capital & preventive maintenance |
Er. Ravi Kumar Pandit Phone: 8929723042 | Capital & preventive maintenance hosp. | ||
AC&R DIVISION (Er. Sudhesh Jain) Email:exengg.acnr@aiims.gov.in sudhesh_jainy@yahoo.co.in Tel: 01251-275016 | - | Er. Pushpender Kumar Phone: 9458660626; 8929900159 | Entire NCI, Jhajjar |
# Tele-Exchange No- 011-26594900.
*For Tender procedures visit our website: www.tenderwizard.com/AIIMS
CSSD is under the administrative control of Medical Superintendent, All India Institute of medical Sciences, New Delhi.
Dr. Nirupam Madaan is the Officer Incharge of the central sterile services department, who is looking after the routine administrative work of the CSSD.
Central Sterile Services
CSSD is currently been manned by the following staff
| S. No. | Post | No. of Posts |
|---|---|---|
| 1 | Technical Officer | 1 |
| 2 | Nursing Officer | 3 |
| 3 | Technical Assistant | 1 |
| 4 | OT Technician | 6 |
| 5 | Lab Technician | 1 |
| 6 | OTA | 4 |
| 7 | Hospital Attendant | 28 |
| 8 | Sanitary Attendant | 1 |
The Set facility has provided a robust platform for conduct of research related to teaching and training. Many projects have been completed and many are ongoing.
| S.No. | Date | Name |
|---|---|---|
| 1 | - | October,2023 |
| 2 | - | August,2023 |
| S.No. | Date | Name |
|---|---|---|
| 1 | - | October,2023 |
| 2 | - | August,2023 |
Award of certificate of appreciation for contribution to various academic activities at the SET Facility by Director, AIIMS.
| Sl No. | Faculty Name | Departments |
|---|---|---|
| 01 | Dr. Rashmi Ramachandran | Anaesthesiology, Pain Medicine and Critical Care |
| 02 | Dr. Thilaka Muthiah | Anaesthesiology, Pain Medicine and Critical Care |
| 03 | Dr. Manpreet Kaur | Anaesthesiology, Pain Medicine and Critical Care |
| 04 | Dr. Devalina Goswami | Anaesthesiology, Pain Medicine and Critical Care |
| 05 | Dr. Nishkarsh Gupta | Department of Onco Anaesthesiology |
| 06 | Dr. Rakesh Garg | Department of Onco Anaesthesiology |
| 07 | Dr. Gyanendra Pal Singh | Department of Neuro Anaesthesiology |
| 08 | Dr. Prabhjot Singh | Department of Urology |
| 09 | Dr. Prabudh Goel | Department of Paediatrics Surgery |
| 10 | Dr. Anu Sachdeva | Department of Paediatrics |
| 11 | Dr. K. Aparna Sharma | Department of Obstetrics & Gynecology |
| 12 | Dr. Jhuma Sankar | Department of Paediatrics |
| 13 | Dr. Juhi Bharti | Department of Obstetrics & Gynecology |
| 14 | Dr. Jyoti Meena | Department of Obstetrics & Gynecology |
| 15 | Dr. Vidushi Sinha | Department of Obstetrics & Gynecology |
| 16 | Dr. Ravneet Kaur | Centre for Community Medicine |
| 17 | Dr. Harshal Salve | Centre for Community Medicine |
| 18 | Dr. Suhani | Surgical Disciplines |
| 19 | Dr. Mohit Joshi | Surgical Disciplines |
| 20 | Dr. Kamlesh Kumari Sharma | College of Nursing |
| 21 | Dr. Smita Das | College of Nursing |
| 22 | Dr. Arvind Kumar | Department of Medicine |
| 23 | Dr. Ranveer Singh Jadon | Department of Medicine |
The Set facility has provided a robust platform for conduct of research related to teaching and training. Many projects have been completed and many are ongoing.
| S.No. | Date | Activity |
|---|---|---|
| 1 | Feb.-2025 | WET LAB |
| 2 | Jan.-2025 | WET LAB |
| 3 | Dec.-2024 | WET LAB |
| 4 | Nov.-2024 | WET LAB |
| 5 | Sep.-2024 | WET LAB |
| 6 | Oct.-2024 | WET LAB |
| 7 | Aug.-2024 | WET LAB |
| 8 | July-2024 | WET LAB |
| 9 | June-2024 | WET LAB |
| 10 | May-2024 | WET LAB |
| 11 | April-2024 | WET LAB |
| 12 | March-2024 | WET LAB |
| 13 | Feb.-2024 | WET LAB |
| 14 | Jan.-2024 | WET LAB |
| 15 | Dec.-2023 | WET LAB |
| 16 | Nov.-2023 | WET LAB |
| 17 | Oct.-2023 | WET LAB |
| 18 | Sept.-2023 | WET LAB |
| 19 | Aug.-2023 | WET LAB |
| 20 | July-2023 | WET LAB |
| 21 | June-2023 | WET LAB |
| 22 | May-2023 | WET LAB |
| 23 | April-2023 | WET LAB |
| 24 | March-2023 | WET LAB |
| 25 | Feb.-2023 | WET LAB |
| 26 | Jan.-2023 | WET LAB |
| 27 | Dec.-2022 | WET LAB |
| 28 | Nov.-2022 | WET LAB |
| 29 | Oct.-2022 | WET LAB |
Ocular Surface Reconstruction
Peripheral vascular disease
Myocardial infarction
Dilated cardiomyopathy
Biliary Atresia
Vitiligo
Stroke
Spinal Cord injury
Age related Macular Regeneration
Retinitis Pigmentosa
Heart Surgery Forum; 2007
Neurosurgery. 2012
Journal of American College of Cardiology,2010
Journal of Cardiovascular Magnetic Resonance, 2011
Indian Journal of Nuclear Medicine; 2014
Pediatr Srgu Int. 2011 Cornea ; 2011
IOVS , 2011 World Journal of Retina and Vitreous;2012,5-13
HTML
| S. No. | Title of the project | Funding Agency | Year | Duration (years) |
|---|---|---|---|---|
| 1. | Role of mesenchymal stem cell in animal model of hypoxic induced brain injury: implications for translation: HIBI initiative” | DBT | 2017 | 3 |
| 2. | Understanding the therapeutic role of adult stem..... induced neurodegenerative disease | DBT | 2017 | 3 |
| 3. | Immunomodulatory property of human mesenchymal stem cell: assessment of their therapeutic potential in gvhd model | DST | 2017 | 3 |
| 4. | A double-blind randomized trial of transplantation of cultured melanocytes from outer root sheath of plucked hair follicles vs. cultured melanocytes from epidermis | DBT | 2017 | 3 |
| 5. | Comparative evaluation of efficacy of conjunctival stem cell transplantation with cultivated oral mucosal epithelial transplantation in patients with bilateral cicatrizing ocular surface diseases (i.e. stevensjohnson syndrome & chemical burns) | DBT | 2017 | 3 |
| 6. | Development of a carrier dressing capable of supporting the transfer of melanocytes & keratinocytes onto an in vitro wound bed model | DBT | 2017 | 3 |
| 7. | DBT- Centre of Excellence for Stem Cell Research: Basic and Translational (phase-ii) | DBT | 2017 | 3 |
| 8. | Assessment of the effect of various storage media on viability, proliferative ability and differentiation potential of human periodontal ligament stem cells (hpdlscs): an in-vitro study. | AIIMS | 2016 | 1 |
| 9. | Utilization of intra-arterial injections of autologous bone-marrow derived mononuclear cells for treatment of spinal injury | AIIMS | 2016 | 1 |
| 10. | Evaluation of autologous bone marrow derived stem cells in dry age related macular degeneration-a comprehensive study” | ICMR | 2016 | 3 |
| 11. | Comparison of autologous cultured limbal stem cells on amniotic membrane transplant versus limballenticule transplantation alone in the management total limbal stem cell deficiency due to ocular burns: a randomized controlled clinical trial | DST | 2016 | 3 |
| 12. | Targeting telomerase reverse transcriptase (tert) gene to immortalize peripheral blood mononuclear cells of patients with coronary artery disease | ICMR | 2015 | 3 |
| 13. | Isolation and expansion of MSCs from human bone marrow umbilical clod blood and evaluation of its cardiomyogenic and neurogenic differentiation potential” | AIIMS | 2015 | 1 |
| 14. | Study of paracrine mechanism of autologous intravenous stem cell transplantation in stroke using bio functional markers | DST | 2015 | 3 |
| 15. | Sculpturing corneal constructs using micro-patterned surface and decellularized corneas | DBT | 2014 | 3 |
| 16. | To compare the differentiation potential of MSCs derived from different sources into cardiomyocytes using 5-aza and tgfb1 as inducer | AIIMS | 2014 | 1 |
| 17. | Isolation and characterization of mesenchymal stem cells from amniotic fluid and Wharton jelly | AIIMS | 2014 | 1 |
| 18. | Role of mouse embryonic fibroblast and human foreskin fibroblast feeder cell in maintaining self-renewal of embryonic stem cell: role of Tgf-βand igf ii | UGC | 2013 | 2 |
| 19. | Cell sheet engineering for assembling human corneal construct | IIT-D | 2012 | 2 |
| 20. | To study the association of cardiac specific genes towards generation of functionally active cardiomyocytes derived from human bone marrow MSCs | ICMR | 2012 | 3 |
| Course | Application Procedure | Duration |
|---|---|---|
| PhD | PhD Entrance Examination of AIIMS | 3 – 5 Years |
| Name of the training | Application Procedure | Duration |
|---|---|---|
| Short term training for the graduate, post-graduate and post doctoral students | Apply to the Registrar through the respective institutions | 1 month – 3 months |
| S No. | Title of the talk | Name of the CME/ Conference | Date | Venue | City |
|---|---|---|---|---|---|
| 1. | Mesenchymal Stem Cells: The New Immunomodulatory Agents | 43rd Annual Conference of Indian Immunology Society (IIS) “IMMUNOCON 2016” | 16th-18th Feb 2017 | GITAM University | Vishakhapatnam |
| 2. | Realizing the potential of Stem Cell Research | DBT-NER Hands on training Workshop on “Stem Cell Biology” | 13th Feb 2017 | ACTREC-Tata Memorial Centre | Mumbai |
| 3. | Stem Cells and Regeneration: Role of Mitochondria | International Conference on Mitochondria in Health and Disease | 10th -11th Feb 2017 | Jawaharlal Nehru University | Delhi |
| 4. | Stem Cell Therapy: Current Status | 14th Annual Meeting of International Society for Heart Research | 27th -29th Jan 2017 | CSIR-IGIB | Delhi |
| 5. | Mesenchymal Stem Cell biology and hypoxia | Seminar on “Current Research Trends in Hypoxia Research | 18th Jan 2017 | JNU | Delhi |
| 6. | Experience with Stem Cell Research | 2nd French-Indian (FAM- ANM- AIIMS) Public and Medical Innovation Forum Conference | 17th -18th Nov 2016 | Paris | France |
| 7. | Application of Mesenchymal Stem Cells: Bench to Bedside | 1st Malaysian Society for Stem Cell Research and TherapySymposium on “Stem Cell” | 11th Oct 2016 | Institute of Medical Research | Malaysia |
| 8. | Stem Cells: Their Role & Clinical Implications In Dentistry | National CDE Program on “Regenerative Endodontics | 9th Apr 2016 | Maulana Azad Institute of Dental Sciences | Delhi |
| CLET and AM regulations, availability and accessibility issues | Doscon 2016: Ophthalmic Panorama | 15th -17th Apr 2016 | Hotel Ashok | Delhi |
| S No. | Title of the talk | Name of the CME/ Conference | Date | Venue | City |
|---|---|---|---|---|---|
| 1. | Emerging Role of Stem Cells in Dentistry | 28th Annual ISDR Conference | 22nd November, 2016 | R-Ahmed Auditorium, I.T.S Centre for Dental Studies & Research | Ghaziabad |
| 2. | Translational Stem Cell Research: Present Status and Future Prospectus | International Conference on Translational Medicine | 20th February, 2016 | Amity University | Gurgaon |
| 3. | Trends in Translational Stem Cell Research | 5th Annual Meeting of Indian Academy of Biomedical Sciences | 27th February, 2016 | Indian Habitat Centre | Delhi |
| 4. | Trends in Stem Cell Research and Future | Lecture Series in Molecular Medicine & Biotechnology | 22nd March, 2016 | AIIMS | Delhi |
| 5. | Stem Cell Research: Current Scenario and Translational Aspect | Fourth International Conference of Pharmacoeconomics & Outcomes Research | 31st October, 2015 | Delhi Institute of Pharmaceutical Sciences and Research | New Delhi |
| 6. | Stem cells Therapy in TBI and SCI: Overview | 3rd AIIMS Neurotrauma Conference | 29th October, 2015 | AIIMS | Delhi |
| 7. | Stem Cell: Current Concepts | Medical Biotechnology | 13th October, 2015 | Miranda house, Delhi University | Delhi |
| 8. | Technology bridging India and Japan in Corneal Regeneration and beyond | Niche-In-Centre for Regenerative Medicine | 10th October, 2015 | Hotel Savera, Chennai | Chennai |
| 9. | Stem Cell Therapy: Scope and Historical Aspects | Indian Academy of Neurology; Expert Group Meeting on Stem Cell Treatment in Neurology | 22nd August, 2015 | Westin Hotel, Gurgaon | Gurgaon |
National Poisons Information Centre (NPIC) in Department of Pharmacology, AIIMS, New Delhi initiated an outreach project with a theme BE CAUTIOUS, BE POISON SAFE. This theme aims to increase awareness towards poisons and poisoning among general public including Children, Parents and Occupational Workers. It also intends to increase knowledge regarding poisons and poisonous substances and disseminate knowledge of poison prevention measures that can be practiced to reduce the risk of accidental poisonings. It also advocates to adopt safe practices and enforce effective poison control measures.
Awareness activities organized in the past by National Poisons Information Centre (NPIC), AIIMS, New Delhi
| S.No. | Date | Monthly Activity |
|---|---|---|
| 1 | Jan.-2025 | Skill Lab |
| 2 | Dec.-2024 | Skill Lab |
| 3 | Nov.-2024 | Skill Lab |
| 4 | Oct.-2024 | Skill Lab |
| 5 | Aug.-2024 | Skill Lab |
| 6 | July-2024 | Skill Lab |
| 7 | June-2024 | Skill Lab |
| 8 | May-2024 | Skill Lab |
| 9 | April-2024 | Skill Lab |
| 10 | March-2024 | Skill Lab |
| 11 | Feb.-2024 | Skill Lab |
| 12 | Jan.-2024 | Skill Lab |
| 13 | Dec.-2023 | Skill Lab |
| 14 | Nov.-2023 | Skill Lab |
| 15 | Oct.-2023 | Skill Lab |
| 16 | Sept.-2023 | Skill Lab |
| 17 | Aug.-2023 | Skill Lab |
| 18 | July-2023 | Skill Lab |
| 19 | June-2023 | Skill Lab |
| 20 | May-2023 | Skill Lab |
| 21 | April-2023 | Skill Lab |
| 22 | March-2023 | Skill Lab |
| 23 | Feb.-2023 | Skill Lab |
| 24 | Jan.-2023 | Skill Lab |
| 25 | Dec.-2022 | Skill Lab |
| 26 | Nov.-2022 | Skill Lab |
| 27 | Oct.-2022 | Skill Lab |
| S.N. | Name | Designation |
|---|---|---|
| 1 | Prof. Ambuj Roy | Head of SET Facility |
| 2 | Prof. Kalpana Luthra | Prof. In-Charge (E-Learning) |
| 3 | Prof. Rashmi Ramachandran | Prof. In-Charge (Skill and Simulation) |
| 4 | Prof. Vijay Prakash Mathur | Prof. In-Charge (Tele-medicine) |
| 5 | Prof. Nishkarsh Gupta | Officer In-Charge Store |
| 6 | Gyan Chand | Administrative Officer |
| 7 | Adarsh Kumar Sharma | Chief Technical Officer |
| 8 | Ram Pal Singh | Assistant Store Officer |
| 9 | Vikram Singh Choudhary | Senior Nursing Officer |
| 10 | Deepesh Piliwal | Nursing Officer |
| 11 | Dragpal | Nursing Officer |
| 12 | Fahad PT | Nursing Officer |
| 13 | Ashok Kumar | Nursing Officer |
| 14 | Pradeep Kumar | Nursing Officer |
| 15 | Susen Kumar Barik | D.E.O. G-‘B’ |
| 16 | Chandan | Junior Photographer |
| 17 | Brijesh Kumar | Junior Administrative Assistant |
| 18 | Ravi Ukhardya Dhanap | Store Keeper |
| 19 | Bobby Kumar | Office Attendant |
| 20 | Surender Pal | MTS |

Faculty and Staff at SET facility activities
The SET Facility is an example of the vision of the institute’s leadership for continuous innovation in the field of medical education.
The facility has a Dry Skill Lab equipped to impart several basic and advanced medical skills through in-house developed modules. It has a Wet Lab hosting cadaveric and other surgical skill development workshops in various surgical specialties. In addition, there are three modern studios with capability to link with over 50 medical institutions across India. The SET (Skills, e-Learning, Telemedicine) Facility is a state of art facility set uptoinnovate medical education using simulation-based skill learning and e-learning methods to improve current teaching at the institute. The SET facility is a shared facility for use by different departments to impart simulation-based skills for undergraduate and postgraduate students for better patient care in addition to the traditional training methods. The simulation-based skill learning of medical undergraduates, postgraduates and nursing staff helps them be better prepared when managing patients in wards and clinics. The facility has active involvement of faculty members from various clinical and non-clinical departments who develop the training modules and teaching content and impart hands-on teaching to the students. The skill lab provides a stress-free environment to learn skills. The other aspects of the facility are to develop e-learning modules and to impart education through Tele-education linkages with medical colleges and hospitals across India. The Facility also serves as the National Resource Centre (NRC) of the National Medical College Network (NMCN), a MOHFW in initiative for tele-education networking across India.
Director, AIIMS
Chairman, SET Management Committee
Dean (Academics)
Co-Chairman, SET Management Committee
Head, SET Facility
Prof-In-Charge E-Learning
Prof. In-Charge (Skill and Simulation)
Prof. In-Charge (Tele-medicine)
Email: aiims[dot]setfacility[at]gmail[dot]com
Mobile: 9810394950
drrgarg[at]hotmail[dot]com
Telephone: 26593011 and 26593402
Email: aiimstransport@gmail.com
Postal Address: Transport Office (Main Garage),AIIMS Ansari Nagar ,New Delhi 110608
To download requisition form for kindly click on the links as per the requirement of the type of vehicles:
Requisition for institute vehicles for official duties:
Requisition form for special drop facility at night (9.30 PM and 10.30 PM) from AIIMS to Masjid Moth Hostel: Please click here.
How to avail facility: All female doctors and students finishing work late in the evening are welcome. For the purpose of records a requisition form is to be filled.
Various types of vehicles being run on contract basis and their existing contracts are as follows:
Faculty and officers of the AIIMS can request a vehicle when deputed by AIIMS for official duties outside AIIMS. Procedure for the same is as follows:
Special arrangements have been made by the AIIMS authorities to facilitate female Resident Doctors and students finishing their work late in the evening.
Drop facilitiy from AIIMS to Masjid Moth Hostel
Frequency: Daily (Except Thursdays) at 9.30 PM and 10.30 PM
Start point: AIIMS near Private Ward.
Route: AIIMS Old Private Ward - General Raj School
Green Park - Gulmohar
Park-Gautam Nagar Taxi Stand - Gautam Nagar Shiv Mandir Gate - Father
Agnel School Gate No.2 - Masjid Moth Hostel and lastly to AIIMS.
How to avail facility: All female doctors and students finishing work late in the evening are welcome. For the purpose of records a requisition form is to be filled. It can be downloaded by click here
The Transport Section of AIIMS is also known as the "Main Garage." It provides transport services to the AIIMS. However, the transport services of various centers under AIIMS and the Hospital Section are catered separately.
The section has its own fleet of buses and cars augmented by some vehicles hired on contract basis, for various requirements of the AIIMS. Presntly the fleet consists of Cars : 15
Buses (different capacities) : 6
Mobile Clinic Van : 1
The number of hired vehicles is variable and dependent on the requirements from time to time.
ABOUT NPIC | |
The National Poisons Information Centre (NPIC) was established in February 1995 in the Department of Pharmacology, All India Institute of Medical Sciences (AIIMS), New Delhi. The Centre provides round-the-clock information on management of poisonings to Health Care Professionals and the general public. Toll Free No. - 1800 116 117 Tel No. - 011-2658 9391, 011-2659 3677 E-mail: npicaiims2010@gmail.com |
 | Name: Dr. Madhuri Gupta Designation: Scientist Qualification: M.Sc., Ph.D. Area of Interest: Analytical chemistry & pesticides Phone: 011-26593677, 26589391 Email: madhurijaswal71@ymail.com |
 | Name: Dr. Sunder S. Samuel Designation: Scientist Qualification: M.Sc., Ph.D. Area of Interest: Cardio & neurotoxicology Phone: 011-26593677, 26589391 Email: sunder_sam@yahoo.co.uk |
 | Name: Dr. Swati Sharma Designation: Scientist Qualification: M.Sc., Ph.D. Area of Interest: Pharmacogenomics & bioinformatics Phone: 011-26593677, 26589391 Email: mail_swati84@yahoo.co.in / drswati2107@gmail.com |
 | Name: Dr. Devendra Singh Designation: Scientist Qualification: M.Phamr, Ph.D. Area of Interest: Neuropharmacology, Ischemic Stroke, Alzheimer’s Disease, Preclinical research Phone: 011-26593677, 26589391 Email: dvndr.singh@gmail.com |
 | Name: Dr. Ajay Godwin Potnuri Designation: Scientist Qualification: M.S (Pharm), Ph.D. Area of Interest: Cardiovascular Pharmacology and toxicology with a special emphasis on hypertensive heart disease and vascular biology Email: dr.ajaygodwin.p@gmail.com |
 | Name: Dr. Jyoti Designation: Scientist Qualification: M.Sc., Ph.D. Area of Interest: Endocrinology, Neurosciences Email: jyotiswarup11@gmail.com |
Through Cheque Donation
Donations for poor & indigent patients undergoing treatment at AIIMS (Main Hospital) can be made by Bank Draft/ Cheque drawn in favor of “AIIMS POOR FUND ACCOUNT”. Donations made in favor of AIIMS Poor Fund Account are eligible for deduction U/S 80G of Income Tax Act, 1961 The Bank Draft/ Cheque along with a Covering Letter could also be directly sent by post to Medical Superintendent, All India Institute of Medical Sciences, Ansari Nagar, New Delhi-110029.
The name of the patients for whom the donations is being made should also be written on the backside of the Bank Draft/Cheque along with the O.P.D. registration number/ C.R. Number”.
In Service To Nation Since 1995
Department Of Pharmacology
All India Institute Of Medical Sciences (AIIMS)
New Delhi-110029

Toll Free No. : 1800 116 117
Tel No. : 011-2658 9391, 011-2659 3677
Mail : npicaiims2010[at]gmail[dot]com
Students of Social Work from different educational institutions come to Medical Social Welfare Unit for:
Short-term Observership Training
(To apply for Short-term Observership Training through Academic Section – AIIMS kindly see the information - https://www.aiims.edu/en/academic_section_training.html)
Concurrent Field-Work
Orientation Visit
To apply for Concurrent Field-Work/ Orientation Visit, please send an email to: mswunitaiims@gmail.com)
Scientist-II Confocal Microscopy Facility - CCRF ,Room No. 8A, Convergence Block, Ground Floor (along the Department of Anatomy hallway)
For queries, sample preparation and bookings email us at: microscopy.ccrf@aiims.edu & saumitra.d.c@aiims.edu
Telephone: +91-11-26549261 (Extension: 8561)
To see Patient Welfare Services in AIIMS Citizen Charter, click on the link:
https://www.aiims.edu/en/citizen-charter/79-about-aiims/13722-patient-welfare-services_12-09-22.html
| Working Monday, Wednesday, Thursday & Friday | |
| (Morning OPD) | (Evening OPD) |
| 08:30 – 10:30 AM | 04:30 – 5:30 PM |
| Working Tuesday | |
| 08:30 – 11:30 AM | Closed |
| Working Saturday | |
| 08:30 – 10:30 AM | Closed |
| Sunday | |
| 09:30 – 10:30 AM | Closed |
| Month | Male | Female | Boy | Girl | Total |
|---|---|---|---|---|---|
| Jan | 6444 | 6078 | 882 | 748 | 14152 |
| Feb | 6387 | 6398 | 900 | 708 | 14393 |
| Mar | 6579 | 6301 | 805 | 618 | 14303 |
| Apr | 6656 | 6416 | 902 | 708 | 14682 |
| May | 6812 | 6582 | 972 | 741 | 15107 |
| Jun | 6094 | 5752 | 839 | 699 | 13384 |
| Jul | 7350 | 6851 | 1067 | 861 | 16129 |
| Aug | 6491 | 6308 | 896 | 682 | 14377 |
| Sep | 6971 | 6741 | 1001 | 745 | 15458 |
| Oct | 7182 | 6805 | 1049 | 793 | 15829 |
| Nov | 6926 | 6616 | 915 | 700 | 15157 |
| Dec | 6529 | 6225 | 911 | 802 | 14467 |
| Total | 80421 | 77073 | 11139 | 8805 | 177438 |
| Month | Male | Female | Boy | Girl | Total |
|---|---|---|---|---|---|
| Jan | 6048 | 5665 | 853 | 596 | 13162 |
| Feb | 6034 | 5750 | 986 | 673 | 13443 |
| Mar | 6238 | 5969 | 940 | 776 | 13923 |
| Apr | 5584 | 5170 | 884 | 667 | 12305 |
| May | 6513 | 6258 | 898 | 693 | 14362 |
| Jun | 5436 | 5236 | 888 | 649 | 12209 |
| Jul | 6096 | 5814 | 991 | 718 | 13619 |
| Aug | 6275 | 5914 | 877 | 674 | 13740 |
| Sep | 7179 | 6860 | 993 | 773 | 15805 |
| Oct | 6724 | 6449 | 957 | 727 | 14857 |
| Nov | 6395 | 6073 | 909 | 747 | 14124 |
| Dec | 6157 | 5882 | 944 | 770 | 13753 |
| Total | 74679 | 71040 | 11120 | 8463 | 165302 |
It was in the year 1956, when the vision of comprehensive healthcare inclusive of preventive, promotive and curative came into existence with the establishment of AIIMS, New Delhi as an autonomous institution of national importance. To serve as a nucleus for nurturing excellence in all aspect of health care, Medical Social Welfare Services in AIIMS were initiated and the first Medical Social Worker was appointed in the hospital in 1960.
Since the advent of Medical Social Welfare Services, it has gained much needed support from Hospital Administration and its leadership. The services to the underprivileged and impoverished catered socio-economic challenges and psycho-social assessment through specific designed interventions by the Medical Social Work professionals. Henceforth, the professional development of Social Welfare Services never looked back and the post of MSW eventually developed into a cadre of Medical Social Service Officer (MSSO) increasing the strength of officers to 58 at present.
At present the Medical Social Welfare Unit, Main Hospital has 14 Medical Social Service Officers taking care of OPDs and Wards of 19 significant departments. The Medical Social Welfare Unit (main hospital) comes under the Medical Superintendent, Main Hospital (Dr. D. K. Sharma), the day-to-day activities are supervised by the Chief MSSO (B. R. Shekhar).
In addition to the Medical Social Welfare Unit, AIIMS has other Medical Social Services Officers placed in different departments and centers. They are working directly under the Chief/HOD of the concerned department.
Due to the professional efforts, sincerity & hard work of Medical Social Service Officers and the visionary support of the superior authorities, AIIMS has become the only institution in India with the biggest strength of Medical Social Workers in a Hospital setting.
| Sr. No. | Office | Address | Phone No. |
|---|---|---|---|
| 1 | Office of Chief MSSO mswunitaiims[at]gmail[dot]com | Room No. C-613, 6th floor – C wing, RAK OPD, AIIMS | 011-29576392 Ext : 2879 |
| 2 | MSSO Office - RAK OPD | Room no. 9, Ground floor – C wing, RAK OPD, AIIMS | 011-29576031 Ext : 2531/2532 |
| 3 | MSSO Office – Main hospital | Room No. 9, In front of Emergency, AIIMS | 011-26594242/4815 |
| 4 | MSSO Office – Emergency | Room No. 9-A, Emergency -1, AIIMS | 011-26546428 |
| 5 | MSSO Office – ABPMJAY | Ayushman Bharat Office, Near gate no. 1, AIIMS | 011-26593251 |
| 6 | MSSO Office – BPS | Room no. 111, 1st Floor, Burn & Plastic Surgery Block, AIIMS | 011-26739567 |
| Sr. No. | Name | Designation | Telephone No. | |
|---|---|---|---|---|
| 1 | Dr. (Prof.) Rima Dada | Prof. In-charge, Media Cell | 011-26549131, 9811783318 | picmedia[at]aiims[dot]gov[dot]in |
| 2 | Dr. (Prof.) Asmita Patil | Addl. Spokesperson | 9971870338 | drasmita[at]aiims[dot]gov[dot]in |
| 3 | Dr. Manpreet kaur, (Assoc. Prof.) | Addl.Spokesperson | 9868551276 | manpreet[dot]aiims[at]aiims[dot]edu |
| 4 | MR. Rajeev Maikhuri | Medical Social Welfare Officer/Media Coordinator | 9868563105 | rajeevmaikhuri[at]aiims[dot]gov[dot]in |
| 1 | Mr. Yogesh Prabhakar, Receptionist | Room no. 10, Ground floor, Convergence Block, Near Gate No. 2 of AIIMS mediaprotocolaiims[at]gmail[dot]com | ||
| 2 | Mr. Manoj Kumar, D.E.O. | |||
| 3 | Mr. Tushar Saini, D.E.O. | |||
| Sr. No. | Name | Designation | Telephone No. | Email ID | |
|---|---|---|---|---|---|
| 1 | Dr. (Prof.) Nand Kumar | Professor In-Charge Protocol Division | 011-26549131 | picprotocolaiims[at]aiims[dot]gov[dot]in mediaprotocolaiims[at]gmail[dot]com | |
| 2 | Mr. Sushil Kumar | PRO (Offctg.) | 011-26543400/3514,+91 8929638517 | mediaprotocolaiims[at]gmail[dot]com | |
| 3 | Mr. Bishwanath Acharya | Asst. PRO | 011-26549131 | mediaprotocolaiims[at]gmail[dot]com | |
| 4 | Mr. Sudhir Sharma | JRO | 011-26543400/3514 | mediaprotocolaiims[at]gmail[dot]com | |
| 5 | Mr. Aditya Kumar | JRO | 011-26543400/3514 | mediaprotocolaiims[at]gmail[dot]com | |
Office Address | |||||
| 1 | Mr. Bharpur Mehra | Receptionist | 1. Room No. 09, Ground floor, Convergence Block, Near Gate No. 02 of AIIMS 2. Protocol Division, 1st floor, JL Auditorium, Contact details : 011-26549131, 011-26593400, 011-26593514 mediaprotocolaiims[at]gmail[dot]com | ||
| 2 | Mr. Sachin Tomar | Program Asst. (PA) | |||
| 3 | Mr. Gautam Kumar Jha | DEO | |||
In response to a request made by the Ministry of Health and Family Welfare, a study was commissioned by the WHO-SEARO to evaluate the WHO fellowship program in India for a period of two biennium, viz., 1994-95, 1996-97. The objectives of this study were to categorize the Fellows selected for training, to assess the relevance of training received, and the extent of utilization of the training in their local setting. Methodology consisted of questionnaire survey and document analysis. Results indicated a disproportionate allotment of fellowships to various health professionals, and problems in the implementation of the knowledge, skills learnt in their local situation. Suggestions have been given for strengthening the fellowship program.
Email: cmetaiims@gmail.com
Website Coordinator :
Dr. Rakesh Garg
Mobile: 9810394950
Email: drrgarg@hotmail.com
K.L. WIG CENTRE FOR MEDICAL EDUCATION & TECHNOLOGY
AIIMS, ANSARI NAGAR, NEW DELHI –110029, INDIA
Phone : 91-11- 26588500, 26588700 Ext. 3392, 3258
Fax : 91-11-26588641, 26588663
Email: cmetaiims@gmail.com
Office bearers:
| Name | Designation | Telephone | |
|---|---|---|---|
| Prof. Peush Sahni | Chief | 26592445 | |
| Dr Anurag Srivastav | Professor-In-Charge (Surgical Disciplines) | 26494560 Int. 4560 | dranuragsrivasta@gmail.com |
| Dr. A.K. Deorari | Professor-in-Charge (Faculty Development of Clinical Faculty of Medicine) | 26594998 | |
| Dr. K.K. Deepak | Professor-in-Charge (Basic Sciences) | 26593583 Int. 3583 | kkdeepak@gmail.com |
| Mr. Yogesh Kumar | Educational Media Generalist | Int. 3258, 3392 | yogesh.anju@gmail.com |
During 1987-95, AIIMS, in partnership with three more leading medical schools in India (Institute of Medical Sciences, B.H.U., Varanasi, C.M.C., Vellore, JIPMER, Pondicherry) and Department of Medical Education, University of Illinois, Chicago, USA, launched a major WHO Project of forming a Consortium of Medical Institutions for Reform of Medical Education.
The Consortium Institutions adopted “Inquiry-driven Strategies for Innovations in Medical Education”. This included use of a common protocol, viz., inquiry into the deficiencies by collecting a data base, identifying innovations and implementing these innovations. The study was conducted by an interdisciplinary core group in each institution, especially involving clinical faculty. A series of workshops were held at CMC, Vellore, JIPMER, Pondicherry, Institute of Medical Sciences, BHU, Varanasi, in addition to Delhi for collecting a database, identifying deficiencies and initiating some innovations in undergraduate medical education. Though initially started with four institutes, the consortium was gradually extended to cover 16 medical colleges across the country. Some of the deliberations of the consortium include:
CMET/AIIMS was involved in a WHO-SEARO Multi-centric research project entitled “Teaching and Application of Health Ethics in South East Asia (India, Bangladesh, Nepal, Indonesia, Myanmar, Sri Lanka). The objective of this study was to identify the ethical dilemma faced by the clinicians and to examine the ethical issues involved in patient - doctor relationship and allocation of resources. This study involved qualitative design, viz., in-depth interview of a cross section of faculty members from various clinical specialties and a questionnaire survey using simulated case scenario. The study revealed a wide variation in the perception of doctors regarding kind of ethical dilemma they faced and the manner in which they attempted to resolve the same. A variation in the pattern is also noticed across different countries depending upon their socio-cultural ethos. The study brought out the need for developing training modules for the teachers to effectively deal with ethical problems.
CMET was integral part of Faculty Development Program conducted at AIIMS, New Delhi. The main function was to evolve in need oriented, self reliant plan for improvement of Medical Education in India with emphasis on development indigenous educational technology. CMET played a major role in organizing various national level program on Medical Education with special emphasis on curricular design, improving teaching methods, innovative objective methods of evaluation and assessment for undergraduate and postgraduate teaching programs. The list of such programs are enumerated below:
| S.No. | Date | Topic |
|---|---|---|
| 1. | 11 -17 Jan, 1989 | Seminar on: · Curriculum models in Medical Education. · Knowledge Learning & Design · Teaching & Learning in Medical Education |
| 2. | 17 April -30 June, 1989 | Twelve week course on Principles of Instructional Design, Teaching & Learning styles, Assessment methods and innovations. |
| 3. | 29-31 March, 1990 | National workshop on Assessment Strategies in undergraduate Medical Education |
| 4. | 29-31, March 1990 | Assessment Strategies in Medical Education |
| 5. | 23-25, April, 1990 | The use of “Inquiry Driven Strategies for innovation in Medical Education: National Conference organized by AIIMS |
| 6. | 30 April-2 May 1992 | Consortium workshop “Inquiry Driven Strategies for innovation in Medical Education Action plan workshop |
| 7. | 8-10, October 1992; | Medical Education Assessment Strategies |
| 8. | 12-14 April, 1993 | Consortium workshop “Inquiry Driven Strategies for innovation in Medical Education – North-North workshop |
| 9. | 10-12 November 1993; | Assessment Strategies in Medical Education |
| 10. | 22-24, March 1993 | Media in Medical Education |
| 11. | 20-22, October 1994 | Media in Medical Education |
| 12. | 22-24 February 1995 | Strategies for Assessment in Medical Education |
| 13. | 10-14, February 1997 | WHO-SEARO Workshop General Principles of Health Professional Education |
| 14. | 10-12, October 1997 | Production of Learning Resource Materials |
| 15. | 2-7 November, 1998 | WHO-SEARO Workshop General Principles of Health Professional Education |
| 16. | 15-17 September, 2003 | National workshop on Ethical issues in biomedical research held in collaboration with ICMR |
| 17. | 23-25 November, 2006 | Emerging Trends in Medical Education |
| 18. | 15-17 November, 2007 | National Conference on Medical Education-NCME 2007 |
| 19. | 10-12 November, 2008 | Teaching Learning Methods in Health Professions Education |
| 20. | 21st Feb., 2012 | Promises and Pitfalls (PBL) |
The unprecedented change in the educational and information technology over the past decade has resulted in a situation where Faculty development is vital for keeping in touch with the recent trends and also launching new innovations in the field of education. Right from its inception , KL Wig CMET has initiated a process of organizing workshops at the institutional, National and international levels. The areas addressed in these workshops are: Assessment Strategies in medical education, The Role of Media in education Problem Based Learning , production of Learning Resource Materials, and Computer Assisted Learning , Scientific Writing , 'How to make good slides?' and Multiple Choice Questions (MCQs) etc. AIIMS has popularized the use of MCQs and the Objective Structured Clinical Examination (OSCE) for the assessment of theory and clinical skills respectively, which have influenced the quality of training.
CMET workshops are largely collective efforts in which the in-house faculty members come together and organize the activities.
| Sr No | Mode | Topic |
|---|---|---|
| 1. | Workshop | Scientific writing, literature search, tips for publishing |
| 2. | Workshop | MCQs and Item Analysis |
| 3. | Lecture | Leadership and management of change |
| 4. | Workshop | Assessment Strategies in medical education |
| 5. | Workshop | Microteaching |
| 6. | Lecture | Challenges in Medical Education |
| 7. | Lecture | Concept of item analysis, question bank and computerization |
| 8. | Workshop | Teaching in Clinical Environment |
| 9. | Workshop | OSPE & OSCE |
| 10. | Workshop | Writing a Research Paper |
Medical Education across the world has been driven by the courses of globalization, free market courses, changing needs and expectations of the society rapid change of technology besides knowledge explosion. The medical schools are striving for skill enhancement of its residents with inbuilt flexibility in terms of scope for self directed learning. The availability and access to the information technology has opened the window for adopting new education strategies. Capacity building of Residents has become the buzz word. Through regular conduction of these Skill Enrichment activities honest efforts are being made to enhance the all-round development of the residents.
| Sr No | Mode | Topic |
|---|---|---|
| 1 | Workshop | Information Retrieval using Internet & Bibliography Management |
| 2 | Workshop | Effective use of media and e-learning |
| 3 | Workshop | Tools for Scientific writing in MS word |
| 4 | Workshop | Designing Effective Presentation |
| 5 | Workshop | Animation in Power Point |
| 6 | Workshop | Writing a Research Paper |
| 7 | Lecture | Management of Stress |
| 8 | Workshop | Introduction to Medical Photography |
| 9 | Workshop | Workshop on “Organizing a Workshop” |
| 10 | Workshop | Designing posters and pamphlets |
| 11 | Lecture | E-learning & Smart Phone in Learning |
As per the recommendations of Valiathan Committee Human Resource Development Cell (HRD Cell) has been set up at AIIMS in the year 2012. To cater the training needs of the AIIMS staff this cell is taking various initiatives under the aegis of CMET. The training programme is being conducted on regular basis so that each and every employee can develop the required skills to perform their task more effectively and efficiently. Various behavioural and attitudinal training programme are also being conducted throughout the year.
| Sr No | Mode | Topic |
|---|---|---|
| 1 | Workshop | Media in Medical Education |
| 2 | Workshop | Designing Effective Presentation |
| 3 | Workshop | Presentation Skills |
| 4 | Workshop | Animation in Power point |
| 5 | Workshop | Tool for scientific writing in health sciences |
| 6 | Workshop | Information Retrieval in Health Sciences |
| 7 | Workshop | Designing Pamphlet and Poster |
| 8 | Workshop | Creativity |
| 9 | Workshop | Workshop on workshop |
| 10 | Workshop | Introduction to Digital Photography |
| Sr No | Mode | Topic |
|---|---|---|
| 1 | Training | Orientation programme of Multi Tasking Staff (MTS) |
| 2 | Training | Noting and Drafting |
| 3 | Training | Working in a team |
| 4 | Training | Effective Communication |
| 5 | Training | Stress Management |
| 6 | Training | Application of MS Office |
| 7 | Training | Nursing Induction Programme |
KL Wig CMET is undertaking short courses and training for Medical students, Nursing and Research scholars in English and Communication Skills. The objectives are to undertake self –analysis and identify factors that could bridge the communication gap in health settings. Further, Medical professionals should be equipped with strong communication skills as they need to communicate to patients/fellow medical professionals from all over the world. It includes effective speaking, active listening, paraphrasing- summarizing, empathy and appreciation when dealing with patients and other health professionals.
In the field of Medical Photography CMET provides the technical support to the AIIMS faculty, residents & other health professionals. Not only photography, the modern state of the art videography, editing work is also being carried out by this department. The services of CMET are being used in the following areas, which are later used for educational purpose.
Details of Media Production for the year 2012-2013
| Particulars | 2012-2013 |
|---|---|
| Clinical Photography | 5069 |
| X-ray scan & A4 printing, slide scan | 5634 |
| Photographic colour prints, scanning of images and documents | 637 |
| Video recording and editing | 192 |
| Designing/printing of large format posters | 1794 + 481 small prints (A4, A3 size) |
In addition to that CMET extends its media photography & videography support to conduct the Convocation & Institute Day celebrations. During Institute Day CMET prepares more than 200 educational posters for the general public, which is really a commendable task.
AIIMS is responsible for developing patterns of teaching in undergraduate and postgraduate medical education in all its branches so as to demonstrate a high standard of medical education to all medical colleges and other health professional institutions in India. Although the Institute has brought about significant changes in its curricula, the overall standard of Medical Education at a national level has remained rather static since 1947. By and large teachers in most of medical colleges of India had remained uninfluenced by the modern educational theories and advanced in educational technology. In fact it was being increasingly felt by our health planners that an urgent, competent and comprehensive action was needed to make medical education to more relevant our national needs. For quite some time AIIMS had been exploring the possibility of establishing an inter-institutional link with the Centre for Medical Education at the University of Dundee in United Kingdom. A proposal was mooted in 1977 for the establishment of a Centre for Medical Education and Technology at AIIMS. However it was in 1989 that the Government of India accorded formal approval to the tripartite agreement between AIIMS, Overseas Development Agencies (ODA), United Kingdom and Govt. of New Zealand to set up a Centre with a view to elevate the standards of Medical and Health Personnel Education by improving the methods of teaching learning and rationalizing the educational strategy. The Centre has been named after Prof. K.L. Wig, the second Director of AIIMS, and a doyen of Medical Education.
Following a tripartite agreement between AIIMS, Governments of UK and New Zealand, a Faculty Development Program was organized for a core group of faculty and technical staff at the Dundee Institute of Educational Technology, United Kingdom. The equipments required for setting up a fully fledged media production centre were provided by the Government of New Zealand. The centre was formally inaugurated by Hon’ble Shri K.R. Narayanan, the- then Vice- President of India, in 1993.
Keeping in mind the overall vision of AIIMS, the future vision of CMET is to develop as a Centre of Excellence in Medical and Health Professional education in the country and the South Asian Region in response to the emerging needs in this field.
Within the institute CMET is focussing on capacity building of all categories of staff by engaging in training through in-house workshops and other activities.
In the field of Medical Photography CMET provides the technical support to the AIIMS faculty, residents & other health professionals. Not only photography, the modern state of the art videography, editing work is also being carried out by this department. The services of CMET are being used in the following areas, which are later used for educational purpose.
| Particulars | 2012-2013 |
|---|---|
| Clinical Photography | 5069 |
| X-ray scan & A4 printing, slide scan | 5634 |
| Photographic colour prints, scanning of images and documents | 637 |
| Video recording and editing | 192 |
| Designing/printing of large format posters | 1794 + 481 small prints (A4, A3 size) |
In addition to that CMET extends its media photography & videography support to conduct the Convocation & Institute Day celebrations. During Institute Day CMET prepares more than 200 educational posters for the general public, which is really a commendable task.
Providing the data & other investigating results of medicines in various diseases to Jr. Residents & Sr. Residents for their research purposes
Engineering is found in every nook & corner & in every domain of this universe. It is the backbone of any infrastructure and is no less important in a medical institution/hospital. All India Institutes of Medical Sciences (AIIMS), New Delhi is a Premier Medical Institution in the world not only known for Health Services but also for the state-of-the-art Architecture and Structural Design among the other Health Institutions. AIIMS has got its own Engineering Services Department (ESD) with team of Core Engineers. They are providing best ergonomics & optimization to handle the huge patients load for smooth functioning of hospital services etc. and keeping the Institute’s dignity ever high since many decades. The ESD have been maintaining the entire infrastructure and providing a wide range of services and supports for variety of end users round ‘O’ clock efficiently for more than six decades. ESD also involved in expansion of AIIMS infrastructure by coordinating with the consultant and deals every engineering aspect to meet the optimum user’s requirement while designing and executions of new projects. Last 10 years has been unprecedented in developing & expansion of AIIMS infrastructure by building many new Centers & Departments. Besides the routine maintenance, the team of Engineers is also involved in cleanliness, beautifications, horticultures, landscaping, infection controls, environment safety etc. ESD has been working hand in hand with medical team and their cumulative efforts made the AIIMS won first prize for Kayakalp campaign most of the times.
The mission of Engineering Services Department is to provide uninterrupted operation of the vital utilities of the institute, ensuring reliable operation of utilities through effective and efficient operation & maintenance of facilities. It aims to provide sustainable development & optimal use of resources in order to secure our future generations. In coordination with Sanitation, ESD is striving to make AIIMS, CLEAN & GREEN ever before which is also one of the objectives of incumbent hon. Director, Prof. M. Srinivas.
In recent times many new blocks/hostels/buildings/Waiting lounge have been or is being constructed at AIIMS, New Delhi especially at Masjid Moth Campus which is unprecedented in the history of AIIMS.
Newly constructed/is being constructed key blocks/hostels/buildings/Waiting lounge are:-
Educating the Patients regarding preventive , promotive and curative health.
EHS has one Injection Room which provides the following facilities:
The central sterile services department (CSSD) performs sterilization of medical devices, equipment and consumables and select laundry items for subsequent use in aseptic procedures performed in the operating theatres, ICUs, general wards of the hospital. The operations of a central sterile services department consist of the reprocessing, that is cleaning, disinfecting and sterilizing of reusable medical equipment. The CSSD at AIIMS was set up in the 1960s to cater to 801 beds. Eventually, the Institute expanded such that there was a marked increase in not only the bed strength but also the Operation theatres and the ICU beds. Subsequently, it has taken the load of the expanded bed strength of the main hospital, along with that of the centers which have come up subsequently. Today, the CSSD caters to approximately 1900 beds.

Rural Electrification Corporation Limited (REC), A Govt. of India Navratna Enterprise, extended financial assistance of Rs. 13.02 crore under its CSR initiative to All India Institute of Medical Sciences (AIIMS), New Delhi for the project, renovation and provision of equipment for Central Sterile Supply Department (CSSD) of AIIMS along with procurement of new steam sterilizers, on turn-key basis.
Services provided include provision of the following types of sterile supplies to the Main Hospital, CDER, CN centre, Dr. BRAIRCH, Dr. RPCOS:
Providing practical training to 10 Jr. Residents.
E.H.S. (Dept. of Family Medicine) was established on pattern of Central Govt. Health Services at AIIMS to take care of preventive, promotive and curative aspects of health care of institute employees and their dependents.
The out patient care is taken care by a team of doctors. There is an injection room, dressing room, treatment room and a day care room. In the day care room patients undergoing short medical and surgical procedures are kept under observation. For the indoor patients of EHS there are 52 beds spread across different wards Year- marked for them. There are private rooms which are also ear marked for these patients.
Email-id: generalfacility.ccrf@gmail.com
Ph. No.: 011-26549373
The general facility of the AIIMS CCRF houses multiple molecular biology equipment. Major instruments which has been installed (till now) in General Facility are mentioned below
Details of Major services and equipment provided by General Facility at CCRF.
Ultra-Centrifuge
(Model:.Optima XPN-100, Beckman Coulter)
Polymerase Chain Rection machine
(Model:SureCycler 8800 Thermal Cycler; Agilent Technologies)
Polymerase Chain Rection machine
(Model: C1000 Touch Thermal Cycler; BioRad)
Multimode microplate Reader
(Model:Cytation1; Biotek)
Electroporation system
(Model:.Gene Pulser Xcell system; Biorad)
Gel Documentation System
(Model: G:Box-Chemi-XX9, Company, Syngene)
Multipurpose Centrifuge
Model: Sorvall ST4 Plus
Centrifuge, Thermo Scientific
Refrigerated-Centrifuges
(Model: Heraeus™ Fresco™ 17 Microcentrifuge; Thermo scientific)
Homogenizer
(Supplier:JSR)
Agarose gel electrophoresis set-up
(Supplier:Biorad)
Protein and Western Blot (semi-dry) Apparatus
ElISA washer and ELlSA reader
(Make: Biorad)
Lyophilizer ( Seltis)
Laminar Hood (M/s Haier)
MilliQ and RO water system
Oven and Incubator
The General Facility (GF) of the centralized core research facility (CCRF) is set up with the major aim to provide basic and advanced molecular instrumentation services to the faculty, researchers, and students of AIIMS to facilitate research work and to empower the faculty in AIIMS to set up their individual research work. The General facility will organize regular training workshops to provide hands-on training to faculty, MD/DM/MCh, PhD scholars, MSc, M-Biotech students in basic research/molecular methods, and has recently organized and conducted a workshop in the month of February 2020 as detailed below. In addition, the GF will support the functioning of other sub-facilities of CCRF (including Proteomics/ Genomics/ Bio-analytics and Confocal microscopy facility).

The facility regularly conducts various training sessions, workshops, webinars, and other educational activities for researchers working in the area of flow cytometry. Recent activities at the facility include:

BD FACS Symphony A5, 35 colors, 5 LASERS

BD FACS Aria Fusion Sorter-18 colors, 5 LASERS
You may download the booking form here
FACS Facility is located on the 9th floor under centralized core research facility (CCRF) at convergence block.
For any further detail and information please contact us on:
E-mail: facs.ccrf@gmail.com
Ext No. 011-2654-9292/8652

B1) BD FACS Aria Fusion Sorter-18 color, 5 LASERS

BD FACS Symphony A5, 35 color, 5 LASERS
Acknowledgement is mandatory for any publications, reports and scientific content resulting from the use of the Confocal, the Airyscan or the Image processing systems in CCRF. This helps us to track how well the system has been utilized for publication purposes. The standard sentence to be used is: “We acknowledge the Microscopy and Imaging Facility, CCRF, AIIMS New Delhi for help with image acquisition and analyses.” Please get in touch with the scientist in-charge to get details on the microscope model, details of the objectives, N.A., etc. before writing the Materials and Methods section of your paper.
Authorship in a manuscript is subjective and depends on the effort, time, inputs for the experimental design, troubleshooting, image processing, quantification and statistical analyses including help with writing up specific section(s) of the manuscript that the scientist has contributed to. This should be discussed upfront and depending on how much help is required from the facility/ scientist, a consensus can be reached on whether authorship is warranted.
For general authorship guidelines, please refer the following:
International Committee of Medical Journal Editors Guidelines
Zeiss Webinar: LSM880 with Airyscan – Revolutionize your Confocal Imaging
What is a Confocal Microscope – Webinar [Leica Microsystems]
Confocal Microscopy: Peeping into Lives of Cells [Prof. S.C. Lakhotia,
Acknowledgement is mandatory for any publications, reports and scientific content resulting from the use of the Confocal, the Airyscan or the Image processing systems in CCRF. This helps us to track how well the system has been utilized for publication purposes. The standard sentence to be used is “We acknowledge the Microscopy and Imaging Facility, CCRF, AIIMS New Delhi for help with image acquisition and analyses.” Please get in touch with the scientist in-charge to get details on the microscope model, details of the objectives, N.A., etc. before writing the Materials and Methods section of your paper.
Authorship in a manuscript is subjective and depends on the effort, time, inputs for the experimental design, troubleshooting, image processing, quantification and statistical analyses including help with writing up specific section(s) of the manuscript that the scientist has contributed to. This should be discussed upfront and depending on how much help is required from the facility/ scientist, a consensus can be reached on whether authorship is warranted.
how much help is required from the facility/ scientist, a consensus can be reached on whether authorship is warranted.
For general authorship guidelines, please refer the following:
International Committee of Medical Journal Editors Guidelines
Webinar on Confocal Microscopy, Specifications and Applications of the Zeiss LSM980 System
Demonstration of Zeiss LSM980 Confocal System installed in CCRF
Demonstration of Zeiss Airyscan 2 Semi Super-Resolution Module installed in CCRF
The first step is to fill out the Basic User and Sample Information Form followed by the second step which is to Book your Appointment for the Confocal or Book your Appointment for Image Analysis/ Processing from the available slots in the calendar. The third step is to fill out the Payment Challan(common for all CCRF sub-facilities and available on the CCRF home page) and make the necessary payment. Charges are flexible depending on the experiment and usage. Kindly refer to the CCRF homepage to see the approved charges.
Also, do write to us at microscopy.ccrf@aiims.edu regarding your samples, purpose of analysis, the experiments and protocols that you may want to run and the dates that would suit you best. We will get back to you with the necessary instructions regarding your sample preparation, the best method to execute your protocol and the date and time.

The available LSM980 Confocal system comes with an inverted Axio Observer 7 microscope and is equipped with 7 laser lines of excitation wavelengths: 405 nm, 445 nm, 488 nm, 514 nm, 561 nm, 594 nm and 639 nm. Images are acquired using the Zen 3.1 Blue software. The system can be used to image samples on glass slides mounted on coverslips, glass-bottom multi-well plates, glass-bottom 35 mm petri-dishes and Labtek chamber slides. Cells and thin tissue sections stained with standard fluorophores can be viewed. With the confocal system, one can obtain a lateral resolution of 200 nm and axial resolution of 500 nm. For optimal results, it is advisable to have section thickness of less than 50 µm. Samples on multi-well plates and petri-dishes made of plastic or other polymers cannot be viewed in this microscope. Only confocal grade glass slides, cover slips, plates and dishes are to be used; cover slips mandatorily must be of 1 or 1.5 number with approximately 0.17 mm thickness.

Airyscan 2 is available with the LSM980 Confocal system for semi super-resolution imaging. With the Airyscan 2 system, one can obtain a lateral resolution of around 140 nm and axial resolution of around 400 nm. This module is not to be used for any routine fluorescence/ confocal imaging but only for capturing high quality representative images. The sample preparation protocol remains the same as that for confocal imaging. The laser lines and the sample types that can be imaged remain the same.

Live-cell imaging at present can be performed only with cells grown on 35 mm glass-bottom dishes. The temperature and gas modules enable setting of the desired temperature and gas concentrations – CO2 and N2 (for hypoxia) experiments. With future system upgrades, it will be possible to perform live-imaging on 6, 12, 24, 48 and 96-well glass bottom plates.

The off-line image processing system has the Zen (Blue) and Fiji (ImageJ) softwares installed. At present, only images acquired on the LSM980 confocal system can be processed. The facility is in the process of procuring image analysis softwares that can be used to analyze images captured on other confocal or super-resolution systems.
A picture is worth a thousand words and hence ‘Imaging’ is an essential component of most research and reporting using tissues and cells. The morphology of cells and tissues vary with different physiological and pathological states. This can be observed with different methods of staining or labelling with fluorophore labelled anti-bodies that can localize to regions of interest. But cells are much larger than the organelle and tubules contained within themselves. Therefore, it becomes essential to draw extremely thin sections as is done for transmission electron microscopy. This can be done effectively by optical sectioning using confocal imaging technology. Today it is even possible to reconstruct stacks of confocal images into a three-dimensional model that provides more information that can be analysed with relevance to the condition of the cells and their organelles etc. than a two-dimensional picture. Hence, at the Centralized Core Research Facility at AIIMS, where cutting edge research technology is used to answer relevant questions regarding the health of the Indian population, we have an imaging platform that provides various imaging methods such as single photon/multiphoton fluorescence or imaging with UV lasers in simultaneous or sequential mode with a possibility to image live cells with and without labeling (by Coherent anti-Stokes Raman Scattering that visualizes vibrational contrast between different molecules in the cells).
LASER Confocal Microscopy with Airyscan Semi Super-Resolution and Live-cell Imaging
The Microscopy and Imaging Facility at CCRF has been established to cater to the high-resolution imaging needs of researchers at AIIMS. With the Zeiss LSM980 system in place, one can now image samples with high spatio-temporal resolution. This state-of-the-art confocal system is equipped with a temperature and gas-controlled incubation chamber for live imaging applications. Whether you are looking for high-resolution protein localization within the cell or want to capture high-speed ion flux in an organelle, this system can perform these tasks. The confocal system has also been upgraded to semi super-resolution capability with the inclusion of Airyscan2.
The facility also has an offline ZEN image processing system that can be used for data analyses, quantifications, and 3D reconstruction. This is separate from the image acquisition system and ensures that the online confocal system is not blocked for data processing. The facility will support researchers with data quantification and suggest the type of analyses that might be required to make conclusions from the acquired data. There is help at hand for performing high quality imaging for thesis submissions, manuscript publications, etc.
As per the vision and mandate of CCRF, the Microscopy and Imaging Facility is also committed to training researchers and making them aware of the latest trends in microscopy and imaging techniques. Along this line, webinars, workshops and research talks will be conducted regularly. The users are encouraged to talk, discuss, and seek help in designing their experiments with the personnel in the facility. We look forward to seeing you with your samples at our Microscopy and Imaging facility.

Bioinformatics Facility - CCRF, Convergence Block, Ninth Floor, AIIMS
E-mail: bioinformatics.ccrf@aiims.edu, bioinformatics.ccrf.aiims@gmail.com
Phone: 011-26549361
Learning resources designed for workshop/training program or software available at Bioinformatics Facility would be updated here.

| Multi-Omics, molecular modeling and AI based data analytics services | |
|---|---|
| Whole-genome sequencing (WGS) | Metataxonomics (16S rRNA gene sequencing) |
| Whole-exome sequencing (WES) | Noncoding RNA sequencing (lncRNA and circRNA) |
| Somatic and germline single-nucleotide variants (SNVs) | Targeted-gene sequencing/panels (TGPs) |
| Copy number variants (CNVs) | Microarray (Affymetrix, Agilent, and Illumina) |
| Single-cell RNA sequencing (scRNA-seq) | Pan-genome analysis (core genome and accessory genome) |
| RNA sequencing (RNA-seq) | Genome assembly (de novo and reference-based) and annotation |
| Gene fusions from RNA sequencing data | Phylogenetic analysis (sequence identity, wgMLST and SNP-based) |
| Small RNA sequencing (sRNA-seq) | Genotypic characterization of antibiotic-resistant in bacteria |
| Ribosome sequencing (Ribo-seq) | Gene ontology and pathway analysis (GSEA, ORA and GSVA) |
| Methylation sequencing (Methyl-seq) | Interaction network (generic PPI, gene-disease association, gene-miRNA) |
| Illumina Bead Chip Array (HumanMethylation450/EPIC) | Molecular docking and simulation |
| Metagenomics (whole shotgun metagenomic sequencing) | Artificial intelligence (ML-DL model) in health care |
You may download the booking form from here
Big data analysis has become a central component of scientific discovery. In order to store, retrieve, process, and analyze very large amounts of data, it is necessary to have centralized computational support. The Bioinformatics facility has a high-performance computing facility (CCRF-Bioinformatics-HPC) consisting of high-end servers and storage systems. CCRF-Bioinformatics-HPC is regularly updated according to the latest scientific tools and pipelines required for large-scale biological and clinical data analysis. This facility works closely with other core facilities (such as genomics, proteomics, metabolomics, etc.) by providing continuous and seamless data storage, access, and analysis of the large volumes of data generated by these facilities.
High performance Computing Cluster - 01

| Component | Specification |
|---|---|
| Node | 10 |
| Intel® Xeon® Gold Processors | 10 * 48 = 480 (3.0 GHz) |
| NVIDIA A100 Tensor Core GPU | 40 GB * 4 = 160 GB |
| TruDDR4 Memory | 3.4 PB |
| Centralized PFS Storage | 1 PB usable (20 % SSD, 40 % SAS, 40 % NL-SAS) |
| Internal Server Storage | 300 TB |
Workstations (01) and All in One Desktops (10)
Proteomics Facility, Convergence Block, 9th Floor, AIIMS
Phone No.: 26549275 Extn. – 212, 213, 214, 215, 216
Email id:proteomics.ccrf@aiims.edu
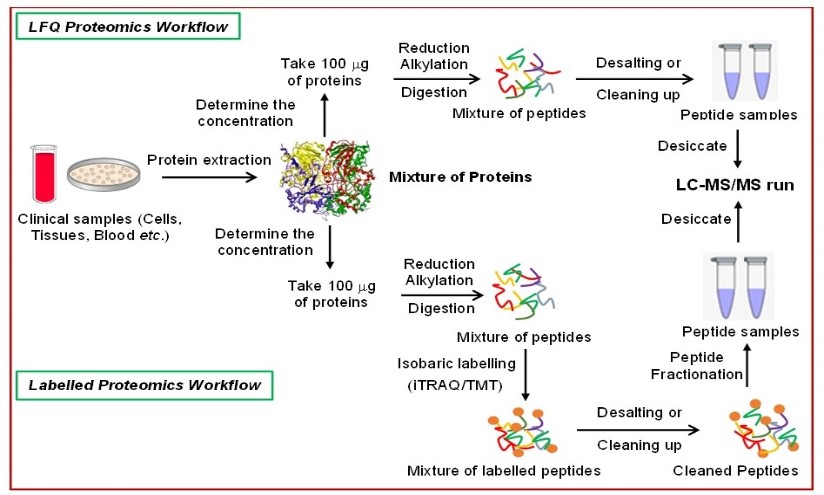
| Instrument | Prime Applications |
|---|---|
Rehydration Chamber (Cytiva)
| Iso-electric focusing (IEF) strip Rehydration
|
EttanPHOR IPG (Cytiva)
| Iso-electric focusing (IEF)
|
TE 22 Mini Tank Transfer Unit (Cytiva)
| Protein transfer for blotting
|
2D Ruby apparatus (Cytiva)
| Run denaturing second dimension electrophoresis of proteins on acrylamide gels
|
Amersham Imager 680 (Cytiva)
| Amersham Imager 680 is a blot and gel imager for sensitive, publication-quality imaging of DNA and protein gels. It has both chemiluminescence and fluorescence imaging facilities. Illumination options in Amersham Imager 680 Chemiluminescence: Use with any blot that incorporates chemiluminescence labeling. Colorimetric Epi-White: Take real-color images and use this with chemiluminescence mode to generate images for gel documentation or combine chemiluminescence with automatic color-marker overlay for easy molecular weight identification. Colorimetric Trans-White: Factory calibrated system for quantitative OD measurement for Coomassie Brilliant Blue stained and silver stained gels. Fluorescence Trans-UV: Use with ethidium bromide or other UV fluorescent stains. Fluorescence Epi-RGB: Use for multiplex, quantitative Western blotting applications. |
Amersham Typhoon Scanner (Cytiva)
|
|
DeCyder Software (Cytiva)
| Data analysis
|
LC-MS/MS Proteomics data analysis
| S. No. | Workshop/Webinar conducted by Proteomics Sub-facility | Lectures delivered by Faculty and Scientists | Date | Number of candidates attended |
|---|---|---|---|---|
| 1 | Webinar on “Practical Approach to Proteomic Experiments” |
| 07/09/20 | 109 |
| 2 | Workshop on “Targeted multi-omics - Hands-on workshop using LC-MS/MS (Targeted Proteomics, Metabolomics and Lipidomics)” |
| 21/12/23 | 122 |
| S. No. | Workshop conducted by Proteomics Sub-facility | Hands-on training provided by Faculty and Scientists | Sessions | Date | Number of candidates attended |
|---|---|---|---|---|---|
| 1 | Targeted multi-omics - Hands-on workshop using LC-MS/MS (Targeted Proteomics, Metabolomics and Lipidomics) Afternoon hands-on session |
|
|
|
|
Proteomics is a high throughput or large-scale comprehensive study of proteome which can be best described as the entire set of proteins that can be expressed by a genome, cell, tissue, or organism at a certain time. The proteomics study can provide information on protein’s differential regulations (for biomarker discovery), variations and modifications, enrichment processes, interacting partners in a network and possible drug target to control a disease.
The Proteomics sub-facility at CCRF, AIIMS provides two different platforms of proteomics experiments –
Both approaches are known as bottom-up proteomics approach where digestion of proteins using proteolytic enzymes (like trypsin) are required prior to the Mass Spectrometry (MS) analysis. The facility looks to help researchers and clinicians to learn and conduct proteomic experiments that can help to answer research questions associated with human diseases and therapeutics. The cutting-edge Liquid Chromatography coupled tandem mass spectrometry (LC-MS/MS) technology platforms will be used which can deliver high-throughput and high-sensitive proteome information.
The facility has four major objectives:
Genomics Facility- CCRF
9th floor, Convergence Block , AIIMS, New Delhi-110029,For queries and further details
Will have a booking calendar
Genomics core facility offers state-of-the-art technology platforms to equip the researchers to generate data for genomic analyses. The aim of the facility is to foster an environment of innovation and efficiency by enhancing investigators' capabilities to accelerate discovery and translation. The facility provides consultation and technical expertise to the faculty and student researchers of the institute to translate their research from ‘idea to impact’.
Centralized Core Research Facility (CCRF) at AIIMS is a cutting-edge research hub dedicated to advancing knowledge in genomics, proteomics, immunology, infection biology, and bioinformatics. By providing access to state-of-the-art technologies and expert support, CCRF empowers researchers to conduct high-quality research in these high-priority areas and positions AIIMS as a global leader in biomedical research.
CCRF was inaugurated by Prof. Venki Ramakrishnan, recipient of the 2009 Nobel Prize in Chemistry and the 62nd President of The Royal Society (Chief Guest) and Prof. Krishnaswamy VijayRaghavan, Principal Scientific Adviser, Government of India (Guest of Honour) on 24 January 2020. The facility re-dedicated Prof. David Julius, Nobel Laureate (2021) recipient of Nobel Prize in Physiology on 18 January 2024.


Confocal Microscopy Facility - CCRF
Room No. 8A, Convergence Block, Ground Floor
(along the Department of Anatomy hallway)
For queries, sample preparation and bookings email us at: confocal.ccrf.aiims@gmail.com & saumitra.d.c@aiims.edu
Acknowledgement is mandatory for any publications, reports and scientific content resulting from the use of the confocal system in CCRF. This helps us to track how well the system has been utilized for publication purposes. The standard sentence to be used is “We acknowledge the Confocal Microscopy Facility, CCRF, AIIMS New Delhi for help with image acquisition and analyses.” Please get in touch with the scientist in-charge to get details on the microscope model, details of the objectives, N.A., etc. before writing the Materials and Methods section of your paper.
Authorship in a manuscript is subjective and depends on the effort, time, inputs for the experimental design, troubleshooting, image processing, quantification and statistical analyses including help with writing up specific section(s) of the manuscript that the scientist has contributed to. This should be discussed upfront and depending on how much help is required from the facility/ scientist, a consensus can be reached on whether an authorship is warranted.
For general authorship guidelines, please refer the following:
Kindly share with us your methods/protocols (sample preparation, image acquisition parameters, useful tips, etc.) that you have followed while acquiring images with the LSM980 confocal system at CCRF-AIIMS. This will be an important resource for future users.
A facile 3D bio-fabrication of customized tubular scaffolds using solvent-based extrusion printing for tissue-engineered tracheal grafts
Kandi R, Sachdeva K, Choudhury SD, Pandey PM, Mohanty S.
| J Biomed Mater Res A.| October 2022 | doi: 10.1002/jbm.a.37458 |
PMID: 36210769 |
Kindly share with us details (PMID, DOI, etc.) of any manuscript you publish using the LSM980 confocal system at CCRF-AIIMS for us to showcase in our website.
Zeiss Webinar: LSM880 with Airyscan – Revolutionize your Confocal Imaging
What is a Confocal Microscope – Webinar [Leica Microsystems]
Confocal Microscopy: Peeping into Lives of Cells [Prof. S.C. Lakhotia, BHU, Varanasi]
Please fill out the Google form at this link:
Also, do write to us at confocal.ccrf.aiims@gmail.com regarding your samples, purpose of analysis, the experiments and protocols that you may want to run and that the dates that would suit you best. We will get back to you with the necessary instructions regarding your samples, their preparation, the best method to execute your protocol and the date and time.
Webinar on Confocal Microscopy, Specifications and Applications of the Zeiss LSM980 System
Demonstration of Zeiss LSM980 Confocal System installed in CCRF
Demonstration of Zeiss Airyscan 2 Semi Super-Resolution Module installed in CCRF
Presently, the confocal system can be accessed free of charge for a reasonable period of usage. Please keep visiting this site for further updates.
A picture is worth a thousand words and hence ‘Imaging’ is an essential component of most research and reporting using tissues and cells. The morphology of cells and tissues vary with different physiological and pathological states. This can be observed with different methods of staining or labelling with fluorophore labelled anti-bodies that can localize to regions of interest. But cells are much larger than the organelle and tubules contained within themselves. Therefore, it becomes essential to draw extremely thin sections as is done for transmission electron microscopy. This can be done effectively by optical sectioning using confocal imaging technology. Today it is even possible to reconstruct stacks of confocal images into a three-dimensional model that provides more information that can be analysed with relevance to the condition of the cells and their organelles etc. than a two-dimensional picture. Hence, at the Core Research Facility at AIIMS, where cutting edge research technology would be used to answer relevant questions regarding the health of the Indian population we have an imaging platform that provides various imaging methods such as single photon/multiphoton fluorescence or imaging with UV lasers in simultaneous or sequential mode with a possibility to image live cells with and without labeling (by Coherent anti-Stokes Raman Scattering that visualizes vibrational contrast between different molecules in the cells).
The Confocal Microscopy Facility at CCRF has been established to cater to the high-resolution imaging needs of researchers at AIIMS. With the Zeiss LSM980 system in place, one can now image samples with high spatio-temporal resolution. This state-of-the-art confocal system is equipped with a temperature and gas-controlled incubation chamber for live imaging applications. Whether you are looking for high-resolution protein localization within the cell or want to capture high-speed ion flux in an organelle, this system is capable of performing these tasks.
The facility also has an offline ZEN image processing system that can be used for data analyses, quantifications, and 3D reconstruction. This is separate from the image acquisition system and ensures that the online confocal system is not blocked for data processing. The facility will support researchers with data quantification and suggest the type of analyses that might be required to make conclusions from the acquired data. There is help at hand for performing high quality imaging for thesis submissions, manuscript publications, etc.
As per the vision and mandate of CCRF, the Microscopy Facility is also committed to training researchers and making them aware of the latest trends in microscopy and imaging techniques. Along this line, webinars, workshops and research talks will be conducted regularly. The users are encouraged to talk, discuss, and seek help in designing their experiments with the personnel in the facility. We look forward to seeing you with your samples at our microscopy facility.
The Computer Facility was created at AIIMS in 1988 in view of the increasing demands and pressing needs of the institute for the computerization of Patient Care System, academics, administration and library etc. The computer Facility has ever since been responsible for established of a local Area Network catering to more than 6500 nodes supporting the Institute, its hospital, Centers, the establishment, finance and the library... It is responsible for the application of computerization in academics where computational needs of the departments is assessed, developed and installed for the requirement of technology for research and teaching. The network management unit of Computer Facility is responsible for maintenance of network, its ever expanding needs, implementation of stat -of -art technology for higher speeds, development and installation of networks and network hardware. The Computer Facility has already established internet site hosted on server at the aiims.edu
The Computer Facility's internet and intranet unit takes care of maintenance of its proxy Mail and HTTP server for AIIMS, up gradation of internet services, development of the web site and the contents creation and management of the latest information of the departments at its web site. The management support unit of Computer Facility looks after the development and software and its maintenance for all the computational needs of the establishment, recruitment, audit, accounts and other administrative units of the AIIMS.
Computer Facility has undertaken the task of implementation of ehospital software along with NIC for AIIMS main hospital and related centres
The Institute is connected on to the Wide Area Network through the high speed dedicated link provided by NKN and NIC. The library network of the Institute is highly advanced and it is being upgraded to be available through web browsing so that readers may avail of the services form anywhere on the network.
The Computer Facility had also initiated certain teaching programme like Computer in Nursing (B.Sc.), Biotechnology, Human Biology. Certain other programs providing regular courses in Medical Informatics at Diploma in Postgraduate level which have been proposed by the Computer Facility are currently under consideration of the Institute.
To cope up with the increased cost of dietary items & other element for the maintenance of different laboratory animals. It has been decided in Experimental Animal Welfare Committee (EAWC) meeting was held on 17th October, 2018 at 3.30 PM in the seminar room of the Central Animal Facility, All India Institute of Medical Sciences (AIIMS), New Delhi-29 increase the by the competent Authority to increase the rate of procurement and maintenance of different laboratory animals (Institute and outside Institute) as per given below w.e.f. 1st May, 2019.
| For Institute(AIIMS) | For Outsiders | ||||
|---|---|---|---|---|---|
| S. No. | Animal | Rate | S. No. | Animal | Rate |
| 1. | Swiss albino Mice | 40/- | 1. | Swiss albino Mice | 100/- |
| 2. | Balb/c-57 (Black& White) | 75/- | 2. | Balb/c-57 (Black& White) | 125/- |
| 3. | Rat | 50/- | 3. | Rat | 125/- |
| 4. | Hamster | 75/- | 4. | Hamster | 150/- |
| 5. | Guinea Pig | 100/- | 5. | Guinea Pig | 200/- |
| 6. | Rabbit | 200/- | 6. | Rabbit | 350/- |
| S. No. | Animal | Rate |
|---|---|---|
| 1. | Swiss albino Mice | 3/- |
| 2. | Balb/c-57 (Black& White) | 3/- |
| 3. | Rat | 5/- |
| 4. | Hamster | 5/- |
| 5. | Guinea Pig | 7/- |
| 6. | Rabbit | 10/- |
(Dr. P.K. Yadav)
Sr. Veterinary Officer, CAF & Member Secretary EAWC
Breeding Programme:
The breeding of rodents like Rats, Mice, Guinea Pigs and Rabbits is done by the Central Animal Facility to fulfill the requirement of the investigators for teaching, diagnostic and research purposes of the various departments of the Institute.
Surgical and Clinical procedures:
The surgical procedures and radiological investigations were performed by various departments on small animals in the Central Animals Facility of the Institute.
The following laboratory facilities are provided by the Central Animal Facility to various investigators viz vacuum drying of sera, and storage of serum samples, blood sample collection, Microscope and X-ray Facility.
Experimental Surgery:
Surgical procedures and radiological investigations were performed by various departments, small and large animals in the Central Animals Facility of the Institute.
The Institutional Animal Ethics Committee (I.A.E.C.) cleared projects on small animals (Rodents) of various investigators of Institute and large animal’s projects cleared by CPCSEA (Committee for Purpose of Control and Supervision of Experiments on Animals) through IAEC. The above committee periodically meets to clear the ethical clearance of various research projects sanctioned under extra mural scheme.
The Institutional Animal Ethics Committee has provided the permission to maintain the departmental animals for Department of Physiology and Pharmacology, Dr. R.P. Centre, AIIMS.
All small animals of rodents colony are maintained by us in the Central Animal facility, AIIMS.
The various activities of this unit are categorized as follows.
The averages of the following rodents animals/month (24.07.18 to 23.08.18) have been maintained.
1. Rats (Wistar) - 1351
2. Rats (Sprague Dawley) - 357
3. Mice (Swiss) - 700
4. Mice Biopsy - 320
5. Mice C57BL/6 - 290
6. Rabbits (New Zealand) - 130
7. Guinea Pigs (Dunken Hartley) - 62
The Institutional Animal Ethics Committee (I.A.E.C.) periodically meets to cleared projects on laboratory animals (Rat, Mice, Rabbit, Guinea Pig and Hamster) of various investigators of the different departments of Institute.
The Institutional Animal Ethics Committee has provided the permission to maintain the experimental departmental laboratory animals for Physiology, Pharmacology and Ocular Pharmacology and Pharmacy, AIIMS.
All small animals of rodents colony are maintained by us in the Central Animal facility, AIIMS.
The various activities of this unit are categorized as follows :
The averages of the following rodent animals/month (01.10.2024 to 31.10.2024) have been maintained.
We are maintaining the departmental experimental wing of the rodents of the various departments of the Institute like Rat, Mice, Rabbit, Guinea Pig and Hamster (Outbreed & Inbred).
| Sl. No. | Investigator Name | Department | Rat | Mice | Rabbit | G. Pig | Hamster |
|---|---|---|---|---|---|---|---|
| 1 | Dr. Lalit Dhar | Microbiology | - | - | - | 2 | - |
| 2 | Dr. T.C. Nag | Anatomy | 7 | - | - | - | - |
| 3 | Dr. Jyotirmoy Banerjee | Biophysics | 27 | - | - | - | - |
| 4 | Dr. Ashish Suri | Neurosurgery | 11 | - | - | - | - |
| 5 | Dr. Vikram Saini | Biotechnology | - | 97 | - | - | - |
| 6 | Dr. Sujata Mohanty | Stem Cell Facility | 30 | 25 | - | - | - |
| 7 | Dr. Ranjeet Kr. Sahoo | Medical Oncology | - | 3 | - | - | - |
| 8 | Dr. Manoj KT | Cardiac BioChem | - | 8 | - | - | - |
| 9 | Dr. Krishna.K. Inampudi | Biophysics | - | 7 | - | - | - |
| 10 | Dr. Rupesh K. Shrivastava | BioTech | - | 36 | - | - | - |
| 12 | Surbhi Gupta | Rep. Biology | - | 13 | - | - | - |
| 13 | Pardeep Sharma | Biophysics | - | 16 | - | - | - |
| 14 | Dr. Kalapana Luthra | Bio-Chemistry | - | 10 | - | - | - |
| 15 | Dr. Sumit Rathore | Biotechnology | - | 13 | - | - | - |
| 16 | Dr. Avtar Singh Meena | Biotechnology | - | 28 | - | - | - |
| Sl. No. | Investigator Name | Department | Rat | Mice | Rabbit | G. Pig | Hamster |
|---|---|---|---|---|---|---|---|
| 1. | Dr. Ajay Singh 370/IAEC-1/2022 | Physiology | 03 | - | - | - | - |
| 2. | Gunjan Sharma 310/IAEC-I/2024 | Physiology | 16 | - | - | - | - |
| 4. | Shivangi 395/IAEC-I/2022 | Physiology | 07 | - | - | - | - |
| Sl. No. | Investigator Name | Department | Rat | Mice | Rabbit | G. Pig | Hamster |
|---|---|---|---|---|---|---|---|
| 1. | Swarnabha Sarkar 262/IAEC-1/2021 | Physiology | 03 | - | - | - | - |
| 2. | Dr. Ankita Nandi 262/IAEC-1/2020 | Physiology | 12 | - | - | - | - |
| Sl. No. | Investigator Name | Department | Rat | Mice | Rabbit | G. Pig | Hamster |
|---|---|---|---|---|---|---|---|
| 1. | Ms. Preeti 341/IAEC-1/2021 | Physiology | 04 | - | - | - | - |
| 2. | Dr. Yashaswee 262/IAEC-1/2020 | Physiology | 06 | - | - | - | - |
| 3. | Ms. Mansi 465/IAEC-I/2024 | Physiology | 14 | - | - | - | - |
| 4. | Dr. Binney Sharma | Physiology | 03 | - | - | - | - |
| 5. | Bhanu Teja | Physiology | 03 | - | - | - | - |
| Sl. No. | Investigator Name | Department | Rat | Mice | Rabbit | G. Pig | Hamster |
|---|---|---|---|---|---|---|---|
| 1. | 452/IAEC-1/2023 | Pharmacology | - | 30 | - | - | - |
| Sl. No. | Investigator Name | Department | Rat | Mice | Rabbit | G. Pig | Hamster |
|---|---|---|---|---|---|---|---|
| 1. | 460/IAEC-1/2023 | Pharmacology | 25 | - | - | - | - |
| Sl. No. | Investigator Name | Department | Rat | Mice | Rabbit | G. Pig | Hamster |
|---|---|---|---|---|---|---|---|
| 1. | Sumit | Pharmacology | 30 | - | - | - | - |
| Sl. No. | Investigator Name | Department | Rat | Mice | Rabbit | G. Pig | Hamster |
|---|---|---|---|---|---|---|---|
| 1. | 458/IAEC-I/2024 | Pharmacology | 22 | - | - | - | - |
| Sl. No. | Investigator Name | Department | Rat | Mice | Rabbit | G. Pig | Hamster |
|---|---|---|---|---|---|---|---|
| 1. | 481/IAEC-1/2023 | Pharmacology | 39 | - | - | - | - |
| 2. | 482/IAEC-1/2024 | Pharmacology | 37 | - | - | - | - |
| Sl. No. | Investigator Name | Department | Rat | Mice | Rabbit | G. Pig | Hamster |
|---|---|---|---|---|---|---|---|
| 1. | Dr. T. Velpandian 313/IAEC-I/2021 | Ocular Pharmacology | - | - | 14 | - | - |
| 2. | Dr. T. Velpandian 436/IAEC-1/2023 | Pharmacology | 13 | - | - | - | - |
As per the act passed by the Ministry of Environment and Forests in 1986 & notified the Bio Medical Waste (Management and Handling) Rules in July 1998, it is the duty of every “occupier”, (in the case of AIIMS, the Director, AIIMS) i.e. a person who has the control over the institution or its premises, to take all steps to ensure that waste generated is handled without any adverse effect to human health and environment.
The biomedical waste management policy followed at AIIMS is as per the Biomedical Waste Management Rules 2016, notified by the Ministry of Environment, Forest and Climate Change, Government of India as per the gazette notification dated 28th March 2016. Prior to this notification, AIIMS had been following the Bio-medical Waste (Management & Handling) Rules 1998 notified by the same ministry. At present, the biomedical waste management at AIIMS has been outsourced to a common biomedical waste management facility, M/S Biotic Waste Solutions Pvt. Ltd..
Hospital waste refers to all waste, biological or non‐ biological that is discarded and not intended for further use.
Bio-medical waste means any waste, which is generated during the diagnosis, treatment or immunization of human beings or animals or in research activities pertaining thereto or in the production or testing of biologicals, and including categories mentioned in Schedule I, of the BMW rules, 2016.
The major salient features of BMW Management Rules, 2016 include the following :
Authorization Of AIIMS Under Bio Medical Waste Management Rules
Renewal Of Authorization Of AIIMS Under Bio Medical Waste Management Rules-2016.
Biomedical Waste Management: Status Review The Laboratory Waste Perspective
Biomedical Waste Management Rules 2016: Overview, Salient Features Implication
Bio Medical Waste Management Lecture For Healthcare Workers: english
Bio Medical Waste Management Lecture For Healthcare Worker: Hindi
Delhi Pollution Control Committee Guide On Bio Medical Waste Management
Current Agreement : under finalization
Mode of disposal of Biomedical waste : Through CBWTF
Name and Address of the CBWTF:
Biotic Waste Solutions Pvt. Ltd.
46-47, SSI Industrial Area,
G.T. Karnal Road, Delhi-110033
Ph:+91-11-47528106/07
Nodal Officer
Dr. Vijaydeep Siddharth : Asstt. Professor, Dept. of Hospital Administration, AIIMS
Contact no.: Landline: 011-26593323
Sanitation Officer :Mr. R.D. Munda:
Contact No. :
Mobile No. - 9868023974
Landline - 011-26593369, 011-26594367 (available 24 X 7)
| Sr. No. | Title | Document |
|---|---|---|
| 1 | AIIMS, New Delhi Guidance document on Preparedness for Infection Prevention & Control including Biomedical Waste Management during Public Health Emergencies- 2024 | |
| 2 | AIIMS Infection Control Manual |
Chief N.S. Centre
Centre for Dental Education and Research (CDER), AIIMS, New Delhi was declared as the National Centre of Excellence for Implementation of National Oral Health Programme (NOHP) on 21st August 2014. During which, there has been panoramic coverage of the activities undertaken by CDER through National Oral Health Programme which has given oral health an outstanding visibility at national level and motivated the various professionals to work towards the motto of Oral Health for All.
To reduce morbidity from oral diseases by strengthening existing healthcare delivery system and ensure access to affordable, quality, patient centered care
CDER has empowered various health care professionals through training activities, oral health promotion for masses and development of eDantSeva website and application. The eDantSeva portal is the standalone government oral health website for promoting oral health awareness making it also easy for users to operate it. NOHP has initiated lateral integration with many national health programmes, conducted review meetings with state nodal officers and circulated advisory on oral health promotion.
Prof. (Dr.) Ritu Duggal
Chief- CDER
Ms. Pratibha Talreja PS to Chief | Email: ppschiefcder@gmail.com |
Office Address: Chief Office, First floor, Centre for Dental Education and Research, All India institute of Medical Sciences, Ansari Nagar, New Delhi - 110029 | Phone Nos. 011-2654 2304 011-2654 2305 |
| S.NO. | Name of Department | Name Of Faculty | Days (OPD) |
|---|---|---|---|
| 1. | Oral Medicine and Radiology | Dr. Shalini Gupta | Daily |
| 2. | Oral & Maxillofacial Surgery | Dr. Ajoy Roychoudhury | Monday/Friday |
| Dr. Ongkila Bhutia | Wednesday/Saturday | ||
| Dr. Rahul Yadav | Tuesday/Thursday | ||
| Dr. Krushna Vasant Kumar Bhatt | Tuesday/Thursday | ||
| 3. | Maxillofacial Prosthodontics | Dr. Veena Jain | Wednesday/Saturday |
| Dr. Dheeraj Kumar Koli | Monday/Thursday | ||
| Dr. Aditi Nanda | Tuesday/Friday | ||
| All Faculty | Monday/Thursday (2pm) | ||
| 4. | Conservative Dentistry & Endodontics | Dr. Ajay Logani | All days except Friday |
| Dr. Vijay Kumar | Wed/Sat | ||
| Dr. Amrita Chawla | Tue/Fri | ||
| Dr. Sidhartha Sharma | Mon/Thur | ||
| 5. | Orthodontics and Dentofacial Deformities | Dr. Ritu Duggal | Wed/Thur/Fri/Sat |
| Dr. Vilas D. Samrit | Tue/Wed/Fri/Sat | ||
| Dr. Prabhat Kumar Chaudhari | Mon/Wed/Thu/Fri | ||
| 6. | Periodontics | Dr. Kunaal Dhingra | Mon/Tue/Thur/Fri |
| Dr. Vikender Singh | Tue/Wed/Fri/Sat | ||
| Dr. Anika Dawar | Mon/Wed/Thu/Sat | ||
| 7. | Pedodontics and Preventive Dentistry | Dr. Vijay P. Mathur | Wed/Fri/Sat |
| Dr. Kalpana Bansal | Tue/Thu/Sat | ||
| Dr. Nitesh Tiwari | Mon/Wed/Fri/Sat | ||
| Dr. Rahul G. Morankar | Mon/Tue/Thur/Sat | ||
| 8. | Public Health Dentistry | Dr. Harsh Priya | Monday to Saturday |
| Dr. Bharathi M. Purohit | Monday to Saturday |
Intricacies and advances in management of traumatic dental injuries in growing children
Oral Health Promotion Drive on International Childhood Cancer Day
Pit and Fissure Sealant Training Workshop for Dental Professionals
International Symposium on Management of Complex Malocclusion and Canted Occlusal Plane
BOOKS, MONOGRAPHS, CHAPTERS, LEARNING MODULES AND IEC MATERIALS
Grimm WD, Benlidayi M, Didenko N, Dhingra K, Dolgalev A, et al. Isolation of skeletal muscle-derived cells modeling neural crest-derived stem cells for therapeutic use in regenerative periodontology. Dent Adv Res. 2021;6(1): 178. doi: 10.29011/2574-7347.100078.
Km S, Koli DK, Jain V, Pruthi G, Nanda A. Comparison of ridge resorption and patient satisfaction in single implant-supported mandibular overdentures with conventional complete dentures: A randomised pilot study. J Oral Biol Craniofac Res. 2021;11(1):71-77. doi:10.1016/j.jobcr.2020.11.014
Mishra D, Thippeswamy SH, Singh P, Santosh BS, Kumawat RM. Atypical Pyogenic granuloma of gingiva with exuberant proliferation of myofibroblasts- A case report. J Oral Maxillofac Surg Med Pathol. 2021;33(1):103-106.
Tewari N, Atif, Rahul M, Kaur A. New vistas in oral biology and regenerative medicine using immortalized odontogenic cell lines: a systematic review. Polymorph. 2021;6:33-48.
Jose A, Yadav P, Roychoudhury A, Bhutia O, Millo T, Pandey RM. Cadaveric Study of Topographic Anatomy of Temporal and Marginal Mandibular Branches of the Facial Nerve in Relation to Temporomandibular Joint Surgery. J Oral Maxillofac Surg. 2021;79(2):343.e1-343.e11. doi:10.1016/j.joms.2020.09.029
Tewari N, Mathur VP, Kaur A, et al. Evidence mapping and quality assessment of systematic reviews in dental traumatology. Dent Traumatol. 2021;37(1):17-36. doi:10.1111/edt.12606
Bansal A, Yadav P, Bhutia O, Roychoudhury A, Bhalla AS. Comparison of outcome of open reduction and internal fixation versus closed treatment in pediatric mandible fractures-a retrospective study. J Craniomaxillofac Surg. 2021;49(3):196-205. doi:10.1016/j.jcms.2020.12.013
Jose A, Nagori SA, Rawat A, Singh S, Roychoudhury A. Facial Reanimation by Modified Intraoral Temporalis Tendon Transfer With Ancillary Procedures. J Craniofac Surg. 2021;32(2):626-628. doi:10.1097/SCS.0000000000006971
Koli B, Chawla A, Logani A, Kumar V, Sharma S. Combination of Nonsurgical Endodontic and Vital Pulp Therapy for Management of Mature Permanent Mandibular Molar Teeth with Symptomatic Irreversible Pulpitis and Apical Periodontitis. J Endod. 2021;47(3):374-381. doi:10.1016/j.joen.2020.10.010
Krois J, Garcia Cantu A, Chaurasia A, et al. Generalizability of deep learning models for dental image analysis. Sci Rep. 2021;11(1):6102. Published 2021 Mar 17. doi:10.1038/s41598-021-85454-5
Mandal J, Bhutia O, Roychoudhury A, Yadav R, Adhikari M, Chaudhary G. Does the Retromandibular Transparotid Approach Provide Quicker Access to Fracture of Mandibular Subcondyle Compared With the Retromandibular Transmasseteric Anterior Parotid Approach?. J Oral Maxillofac Surg. 2021;79(3):644-651. doi:10.1016/j.joms.2020.10.008
Rao TN, Goswami D, Roychoudhury A, Bhutia O, Baidya DK, Trikha A. Efficacy of Local Anesthetic Wound Infiltration in Temporomandibular Joint Ankylosis Surgery for Control of Postoperative Pain: A Prospective, Randomized Controlled, and Double-Blinded Trial. J Oral Maxillofac Surg. 2021;79(3):559.e1-559.e11. doi:10.1016/j.joms.2020.10.034
Ambereen A, Bhutia O, Roychoudhury A, Yadav R, Khakhla DH, Vishwakarma K. Is coronoidectomy superior to coronoidotomy for improving maximum incisal opening in patients with oral submucous fibrosis?. J Oral Maxillofac Surg. 2021;79(4):863.e1-863.e7. doi:10.1016/j.joms.2020.11.009
Darlong V, Kalaiyarasan R, Baidya DK, et al. Effect of airway device and depth of anesthesia on intra-ocular pressure measurement during general anesthesia in children: A randomized controlled trial. J Anaesthesiol Clin Pharmacol. 2021;37(2):226-230. doi:10.4103/joacp.JOACP_55_19
Gupta SR, Xess I, Singh G, et al. Therapeutic implications of candida phenotypes, virulence factors and antifungal sensitivity in oral leukoplakia. J Oral Biol Craniofac Res. 2021;11(2):354-360. doi:10.1016/j.jobcr.2021.03.006
Nisar S, Yousuf P, Masoodi T, et al. Chemokine-cytokine networks in the head and neck tumor microenvironment. Int J Mol Sci. 2021;22(9):4584. Published 2021 Apr 27. doi:10.3390/ijms22094584
Purohit BM, Singh A, Dwivedi A, Purohit A. Oral health as predictors of family functioning: A cross-cultural adaptation and validation of Hindi version of family impact scale. A cross-sectional study. Pediatr Dent J. 2021;31(1):92-99.
Tabiyar K, Logani A. The Apical Extent of Mineral Trioxide Aggregate Apical Barrier Does not Influence the Treatment Outcome in a Nonvital Immature Permanent Anterior Tooth: A Split-Mouth Clinical Study. Eur Endod J. 2021;6(1):44-49. doi:10.14744/eej.2020.08760
Tewari N, Johnson RM, Mathur VP, et al. Global status of knowledge for prevention and emergency management of traumatic dental injuries in sports persons and coaches: A systematic review. Dent Traumatol. 2021;37(2):196-207. doi:10.1111/edt.12629
Rahul M, Sultan F, Tewari N, Mathur V. Orofacial characteristics and dental management in a child with moyamoya disease. BMJ Case Rep. 2021;14(5):e241211. Published 2021 May 21. doi:10.1136/bcr-2020-241211
Rahul M, Tewari N, Mathur V, Goel S, Jain G. Evidence mapping and quality analysis of published dental literature on COVID-19 - A systematic review. Natl J Maxillofac Surg. 2021;12(2):139-161. doi:10.4103/njms.NJMS_237_20
Siddiqui HP, Sennimalai K, Samrit VD, Duggal R, Yadav R. Adjunctive orthodontic therapy for prosthetic rehabilitation in a growing child with Axenfeld-Rieger syndrome: A case report. Spec Care Dentist. 2021;41(3):423-430. doi:10.1111/scd.12579
Sood A, Nayyar V, Mishra D, Kakkar A, Priya H. Post-COVID mucormycosis: Ascertainment of the pathological diagnostic approach. J Oral Maxillofac Pathol. 2021;25(2):219-222. doi:10.4103/0973-029X.325117
Agarwal B, Yadav P, Roychoudhury A, Bhutia O, Goswami D, Shukla G. Does bilateral gap arthroplasty increase the severity of obstructive sleep apnea in patients with temporomandibular joint ankylosis?. J Oral Maxillofac Surg. 2021;79(6):1344.e1-1344.e11. doi:10.1016/j.joms.2021.01.015
Adhikari M, Bhatt K, Yadav R, Mandal J, Bhutia O, Roychoudhury A. Fixation of subcondylar fractures of the mandible: a randomized clinical trial comparing one trapezoidal plate with two miniplates. Int J Oral Maxillofac Surg. 2021;50(6):756-762. doi:10.1016/j.ijom.2020.10.009
Chawla A, Gill S, Sharma S, Kumar V, Logani A. Endodontic implications of a patient with arteriovenous malformation: a case report and literature review. Int Endod J. 2021;54(6):975-987. doi:10.1111/iej.13473
Rathod PK, Yadav R, Bhutia O, Roychoudhury A, Bhatt K, Kaur K. Is zygomatic osteotomy a viable option to achieve symmetry and stability in post-traumatic residual deformity of the zygomaticomaxillary complex? J Oral Maxillofac Surg. 2021;79(6):1328.e1-1328.e13. doi:10.1016/j.joms.2021.01.017
Singh A, Purohit BM. ABO blood groups and its association with oral cancer, oral potentially malignant disorders and oral submucous fibrosis- A systematic review and meta-analysis. Asian Pac J Cancer Prev. 2021;22(6):1703-1712. Published 2021 Jun 1. doi:10.31557/APJCP.2021.22.6.1703
Sinha H, Maitra S, Anand RK, et al. Epidemiology and prognostic utility of cellular components of hematological system in sepsis. Indian J Crit Care Med. 2021;25(6):660-667. doi:10.5005/jp-journals-10071-23874
Aripirala M, Bansal K, Mathur VP, Tewari N, Gupta P, Logani A. Comparative evaluation of diode laser and simvastatin gel in pulpotomy of primary molars: A randomized clinical trial. J Indian Soc Pedod Prev Dent. 2021;39(3):303-309. doi:10.4103/jisppd.jisppd_60_21
Dhillon H, Chaudhari PK, Dhingra K, et al. Current applications of artificial intelligence in cleft care: A scoping review. Front Med (Lausanne). 2021;8:676490. Published 2021 Jul 28. doi:10.3389/fmed.2021.676490
Duggal R, Goswami R, Xess I, Duggal I, Talwar A, Mathur VP. Prevalence of species-specific candidiasis and status of oral hygiene and dentition among diabetic patients: A hospital-based study. Indian J Dent Res. 2021;32(3):292-298. doi:10.4103/ijdr.IJDR_827_20
Kalra G, Mathur VP. COVID-19 Third wave: A concern for pediatric dentists? J South Asian Assoc Pediatr Dent. 2021;4(2):71–72.
Lekshmi MS, Sharma S, Gupta SR, et al. Prevalence and radiological characteristics of palatogingival groove: A retrospective cone-beam computed tomography study in an Indian cohort. J Conserv Dent. 2021;24(4):359-363. doi:10.4103/jcd.jcd_36_21
Maitra S, Baidya DK, Goswami D, Muthiah T, Ramachandran R, Subramanian R. Optimum time of LMA ProSeal removal in adult patients undergoing isoflurane anesthesia: A randomized controlled trial. J Anaesthesiol Clin Pharmacol. 2021;37(3):354-359. doi:10.4103/joacp.JOACP_238_19
Malik AK, Baidya DK, Anand RK, Subramaniam R. A new ICU delirium prevention bundle to reduce the incidence of delirium: A randomized parallel group trial. Indian J Crit Care Med. 2021;25(7):754-760. doi:10.5005/jp-journals-10071-23881
Roychoudhury A, Yadav P, Bhutia O, et al. Alloplastic total joint replacement in management of temporomandibular joint ankylosis. J Oral Biol Craniofac Res. 2021;11(3):457-465. doi:10.1016/j.jobcr.2021.05.006
Selvaraj U, Koli DK, Jain V, Nanda A. Evaluation of the wear of glazed and polished zirconia crowns and the opposing natural teeth: A clinical pilot study. J Prosthet Dent. 2021;126(1):52-57. doi:10.1016/j.prosdent.2020.04.007
Yadav VS, Kamra P, Deepti, Singh N, Bhatia A, Yadav R. Treatment of multiple lingual gingival recession defects in mandibular incisors with modified coronally advanced tunnel technique and connective tissue graft: A case series. J Int Acad Periodontol. 2021;23(3):282-288.
Kaur A, Kumar V, Logani A. Accidental avulsion of a recently traumatised maxillary anterior tooth during rubber dam application. BMJ Case Rep. 2021;14(8):e241872. Published 2021 Aug 17. doi:10.1136/bcr-2021-241872
Kaur K, Kakkar A, Manchanda S, et al. Sinonasal IgG4-related disease: a rare and emerging entity broadening the differential diagnosis in the sinonasal universe. Eur Arch Otorhinolaryngol. 2021;278(8):2883-2890. doi:10.1007/s00405-020-06564-w
Purohit A, Singh A, Purohit B, Shakti P, Shah N. Is aromatherapy associated with patient's dental anxiety levels? A systematic review and meta-analysis. J Dent Anesth Pain Med. 2021;21(4):311-319. doi:10.17245/jdapm.2021.21.4.311
Rahul M, Atif M, Tewari N, Mathur V. Cancer-related radiation therapy in early childhood leading to root abnormality in multiple permanent teeth. BMJ Case Rep. 2021;14(8):e244770. Published 2021 Aug 19. doi:10.1136/bcr-2021-244770
Rzhepakovsky I, Anusha Siddiqui S, Avanesyan S, et al. Anti-arthritic effect of chicken embryo tissue hydrolyzate against adjuvant arthritis in rats (X-ray microtomographic and histopathological analysis). Food Sci Nutr. 2021;9(10):5648-5669. Published 2021 Aug 18. doi:10.1002/fsn3.2529
Singh A, Purohit B. Is malocclusion associated with dental caries among children and adolescents in the permanent dentition? A systematic review. Community Dent Health. 2021;38(3):172-177. Published 2021 Aug 31. doi:10.1922/CDH_00340Singh06
Tewari N, Jonna I, Mathur VP, et al. Global status of knowledge for the prevention and emergency management of traumatic dental injuries among non-dental healthcare professionals: A systematic review and meta-analysis. Injury. 2021;52(8):2025-2037. doi:10.1016/j.injury.2021.06.006
Yadav VS, Deepti NF, Kamra P, Singh N, Yadav R, Bhatia A. A novel approach of combining the tunnel technique with a double papilla flap or a coronally positioned flap for the treatment of multiple adjacent gingival recessions: report of two cases. Int J Esthet Dent. 2021;16(3):338-348.
Alagarsamy R, Roychoudhury A, Bhutia O, Lal B, Yadav R, Bhalla AS. Evaluation of fit feasibility of stock total joint replacement in temporomandibular joint ankylosis patients. Br J Oral Maxillofac Surg. 2021;59(7):792-797. doi:10.1016/j.bjoms.2020.11.016
Aravind A, Kumar V, Sharma S, Chawla A, Logani A. Influence of preoperative degree of tooth loosening and thickness of wire on the rigidity of wire composite splint. J Conserv Dent. 2021;24(5):451-456. doi:10.4103/jcd.jcd_259_21
Chaudhari PK, Kharbanda OP, Chaudhry R, et al. Factors Affecting High Caries Risk in Children With and Without Cleft Lip and/or Palate: A Cross-Sectional Study. Cleft Palate Craniofac J. 2021;58(9):1150-1159. doi:10.1177/1055665620980206
Hegde MN, Parmar G, Logani A, et al. Dental practice management during COVID-19 times-Now and beyond. Int J Clin Pract. 2021;75(9):e14251. doi:10.1111/ijcp.14251
Jaiswal AA, Siddiqui HP, Samrit VD, Duggal R, Kharbanda OP, Rajeswari MR. Comparison of the efficacy of two-time versus one-time micro-osteoperforation on maxillary canine retraction in orthodontic patients: A split-mouth randomized controlled clinical trial. Int Orthod. 2021;19(3):415-424. doi:10.1016/j.ortho.2021.06.003
Jose A, Singh S, Roychoudhury A, Kholakiya Y, Arya S, Roychoudhury S. Current Understanding in the Pathophysiology of SARS-CoV-2-Associated Rhino-Orbito-Cerebral Mucormycosis: A Comprehensive Review. J Maxillofac Oral Surg. 2021;20(3):373-380. doi:10.1007/s12663-021-01604-2
Kaur H, Mishra D, Bhutia O. Extensive lymphoid proliferation in syndromic multiple odontogenic keratocysts- A unique finding. J Oral Maxillofac Surg Med Pathol. 2021;33(5):568-571.
Lal B, Alagarsamy R, Agarwal B, Bhutia O, Roychoudhury A. Patient-specific three-dimensional printed template for halo frame pin placement for multiple skull bone defects after cranioplasty. Br J Oral Maxillofac Surg. 2021;59(7):847-849. doi:10.1016/j.bjoms.2020.09.034
Lal B, Kumar RD, Alagarsamy R, Shanmuga Sundaram D, Bhutia O, Roychoudhury A. Role of Carnoy's solution as treatment adjunct in jaw lesions other than odontogenic keratocyst: a systematic review. Br J Oral Maxillofac Surg. 2021;59(7):729-741. doi:10.1016/j.bjoms.2020.12.019
Mathur VP, Gowthaman K, Shrivstava N, et al. An Insight into Systematic Review and Meta-Analysis of Nonvital Pulp Therapy for Primary Teeth. Pediatr Dent. 2021;43(5):338-339.
Mishra D, Kaur H, Bhalla AS, et al. Ameloblastic Fibroodontoma of Mandible Causing Tumor Induced Osteomalacia: A Case Report with Review of 88 Phosphaturic Oral Neoplasms. Head Neck Pathol. 2021;15(3):975-988. doi:10.1007/s12105-020-01267-4
Qureshi T, Duggal R, Chaudhari PK. Correlation between chronological age and skeletal maturity in different malocclusions: A retrospective study. Int Orthod. 2021;19(3):453-461. doi:10.1016/j.ortho.2021.06.007
Srivastav S, Duggal I, Duggal R, Tewari N, Chaudhari PK, Pandey RM. Parental response to the feeding behavior problems in children with cleft lip and palate: A systematic review. Spec Care Dentist. 2021;41(5):559-571. doi:10.1111/scd.12604
Yadav P, Bhutia O, Bansal A, Lakshmanan S, Roychoudhury A. Does closed treatment of paediatric mandibular condyle fractures result in restitutional remodelling?. Br J Oral Maxillofac Surg. 2021;59(7):798-806. doi:10.1016/j.bjoms.2021.01.016
Yadav P, Roychoudhury A, Bhutia O. Strategies to reduce re-ankylosis in temporomandibular joint ankylosis patients. Br J Oral Maxillofac Surg. 2021;59(7):820-825. doi:10.1016/j.bjoms.2021.02.007
Yadav VS, Mir RA, Bhatia A, et al. Metallothionein levels in gingival crevicular fluid, saliva, and serum of smokers and non-smokers with chronic periodontitis. J Periodontol. 2021;92(9):1329-1338. doi:10.1002/JPER.20-0314
Bhattacharyya A, Subramaniam R, Baidya DK, Aggarwal P, Wig N. Effect of Early Administration of Vitamin D on Clinical Outcome in Critically Ill Sepsis Patients: A Randomized Placebo-controlled Trial. Indian J Crit Care Med. 2021;25(10):1147-1154. doi:10.5005/jp-journals-10071-23993
Chaudhari PK, Dhingra K, Zere E. Digital Presurgical Infant Orthopedics in COVID-19 Crisis. Cleft Palate Craniofac J. 2021;58(10):1331-1334. doi:10.1177/1055665620980230
Goswami D, Singh A, Yadav P, Roychoudhury A. Challenges during bilateral total temporomandibular joint replacement for ankylosis in ankylosing spondylitis patient-a case report. J Oral Biol Craniofac Res. 2021;11(4):544-546. doi:10.1016/j.jobcr.2021.07.010
Kumar N, Koli DK, Jain V, Nanda A. Stress distribution and patient satisfaction in flexible and cast metal removable partial dentures: Finite element analysis and randomized pilot study. J Oral Biol Craniofac Res. 2021;11(4):478-485. doi:10.1016/j.jobcr.2021.06.004
Mathur VP, Kalra G, Dhillon JK. Can dental caries be defined as a pandemic? J South Asian Assoc Pediatr Dent. 2021;4(3):163–164.
Qureshi T, Duggal R, Kharbanda OP, Rajeswari MR. Expression of circulating cell-free nucleic acids around miniscrew implant during orthodontic tooth movement-a prospective study. Prog Orthod. 2021;22(1):33. Published 2021 Oct 18. doi:10.1186/s40510-021-00378-0
R R, Aravind A, Kumar V, Sharma S, Chawla A, Logani A. Influence of occlusal and proximal caries on the outcome of full pulpotomy in permanent mandibular molar teeth with partial irreversible pulpitis: A prospective study. Int Endod J. 2021;54(10):1699-1707. doi:10.1111/iej.13588
Yadav P, Roychoudhury A, Bhutia O, Kaur K, Balachandran R. Does no-intraoperative correction of chin deviation prevent costochondral graft overgrowth in pediatric temporomandibular joint ankylosis management - an intermediate outcome study. J Oral Biol Craniofac Res. 2021;11(4):541-543. doi:10.1016/j.jobcr.2021.07.011
Bansal K, Saji S, Mathur VP, Rahul M, Tewari N. A Survey of Self-perceived Physical Discomforts and Health Behaviors Related to Personal Protective Equipment of Indian Dental Professionals during COVID-19 Pandemic. Int J Clin Pediatr Dent. 2021;14(6):784-789. doi:10.5005/jp-journals-10005-2061
Bhadauria US, Priya H, Purohit B, et al. Effectiveness of an oral health training program for nursing professionals in India: An interventional study. Public Health Nurs. 2021;38(6):1135-1139. doi:10.1111/phn.12953
Bhatia A, Yadav VS, Tewari N, Kumar A, Sharma RK. Efficacy of modified coronally advanced flap in the treatment of multiple adjacent gingival recessions: a systematic review and meta-analysis. Acta Odontol Scand. 2021;79(8):562-572. doi:10.1080/00016357.2021.1908594
Chowdhury AR, Subramanian R, Maitra S, Bhattacharjee S, Lakshmy R, Baidya DK. Intraoperative lung protective ventilation in peritonitis patients undergoing emergency laparotomy: A randomised controlled trial. Indian J Anaesth. 2021;65(11):798-805. doi:10.4103/ija.ija_573_21
Gupta SR, Gupta N, Sharma A, Xess I, Singh G, Mani K. The association of Candida and antifungal therapy with pro-inflammatory cytokines in oral leukoplakia. Clin Oral Investig. 2021;25(11):6287-6296. doi:10.1007/s00784-021-03927-3
Nangia D, Saini A, Sharma S, et al. Treatment outcome of regenerative endodontic procedures in mature permanent teeth compared to nonsurgical endodontic treatment: A systematic review and meta-analysis. J Conserv Dent. 2021;24(6):530-538. doi:10.4103/jcd.jcd_535_21
Chaudhari PK, Dhillon H, Dhingra K, Alam MK. 3D printing for fostering better dental education [published correction appears in Evid Based Dent. 2022 Mar;23(1):5]. Evid Based Dent. 2021;22(4):154-155. doi:10.1038/s41432-021-0217-8
Dhingra K, Grimm WD, Chaudhari PK, Verma F. Does periodontal disease elevate the risk of Alzheimer's disease and mild cognitive impairment? [published correction appears in Evid Based Dent. 2022 Mar;23(1):5]. Evid Based Dent. 2021;22(4):123-125. doi:10.1038/s41432-021-0214-y
Gagnani SP, Yadav P, Roychoudhury A, Bhutia O, Jaryal AK. Longitudinal electromyographic changes in masseter and anterior temporalis muscle before and after temporomandibular joint arthroplasty in ankylosis patients. J Stomatol Oral Maxillofac Surg. 2021;122(6):573-577. doi:10.1016/j.jormas.2020.09.015
Nair PR, Haritha D, Behera S, et al. Comparison of high-flow nasal cannula and noninvasive ventilation in acute hypoxemic respiratory failure due to severe COVID-19 pneumonia. Respir Care. 2021;66(12):1824-1830. doi:10.4187/respcare.09130
Rahul M, Gowthaman K, Tewari N, Mathur V. Dental manifestations of pseudo-vitamin-D deficiency rickets in a paediatric patient. BMJ Case Rep. 2021;14(12):e244517. Published 2021 Dec 30. doi:10.1136/bcr-2021-244517
Roychoudhury A, Yadav P, Bhutia O, Kaur K, Dekyi T, Pandey RM. Growth outcome and jaw functions are better after gap arthroplasty plus costochondral graft reconstruction than gap arthroplasty alone in pediatric temporomandibular joint ankylosis patients: A cluster randomized controlled trial. J Oral Maxillofac Surg. 2021;79(12):2548-2561. doi:10.1016/j.joms.2021.08.164
Yadav P, Roychoudhury A, Kumar RD, Bhutia O, Bhutia T, Aggarwal B. Total alloplastic temporomandibular joint replacement. J Maxillofac Oral Surg. 2021;20(4):515-526. doi:10.1007/s12663-021-01628-8
Alam MK, Alfawzan AA, Akhter F, Alswairki HJ, Chaudhari PK. Evaluation of Lip Morphology and Nasolabial Angle in Non-Syndromic Cleft Lip and/Palate and Non-Cleft Individuals. Appl. Sci. 2022:12(1):357.
Angel SL, Samrit VD, Kharbanda OP, et al. Effects of submucosally administered platelet-rich plasma on the rate of tooth movement. Angle Orthod. 2022;92(1):73-79. doi:10.2319/011221-40.1
Aravind A, R R, Sharma R, et al. Response to pulp sensibility tests after full pulpotomy in permanent mandibular teeth with symptomatic irreversible pulpitis: A retrospective data analysis. J Endod. 2022;48(1):80-86. doi:10.1016/j.joen.2021.10.005
Dhillon JK, Kalra G, Mathur VP. Nitrous oxide oxygen inhalation as safe and effective tool for behavior management in pediatric dentistry. J South Asian Assoc Pediatr Dent. 2022;5(1):1–2.
Dhingra K, Dinda AK, Kottarath SK, Chaudhari PK, Verma F. Mucoadhesive silver nanoparticle-based local drug delivery system for peri-implantitis management in COVID-19 era. Part 1: antimicrobial and safety in-vitro analysis. J Oral Biol Craniofac Res. 2022;12(1):177-181. doi:10.1016/j.jobcr.2021.11.007
Goswami D, Yadav P, Bhatt R, Lakshmanan S, Roychoudhury A, Bhutia O. Comparison of efficacy of Dexmedetomidine and Clonidine infusion to produce hypotensive anesthesia in patients undergoing orthognathic surgery: A randomized controlled trial. J Oral Maxillofac Surg. 2022;80(1):55-62. doi:10.1016/j.joms.2021.06.035
Gupta C, Jain V, Pruthi G. Influence of socioeconomic status on psychological distress and treatment satisfaction levels among patients undergoing prosthetic rehabilitation following maxillectomy: An observational study. Natl J Maxillofac Surg. 2022;13(1):54-59. doi:10.4103/njms.njms_320_21
Gupta V, Kaur H, Mishra D, Yadav VS, Kala S. Distribution of biopsied gingival lesions according to the proceedings from the 2017 World Workshop classification: A three-year retrospective study. Dent Med Probl. 2022;59(1):105-110. doi:10.17219/dmp/141555
Moidu NP, Sharma S, Chawla A, Kumar V, Logani A. Deep learning for categorization of endodontic lesion based on radiographic periapical index scoring system. Clin Oral Investig. 2022;26(1):651-658. doi:10.1007/s00784-021-04043-y
Priya H, Purohit B, Priyanka R. Future scope of virtual reality and augmented reality in tobacco control. Cancer Research, Statistics and Treatment. 2022;5(1):173-174.
Rahul M, Goyal A, Kapur A, Singh SK, Oswal S, Tewari N. Replantation of a Iatrogenically Avulsed Mandibular Premolar Undergoing Orthodontic Therapy: A 5 Year Follow-Up. J Clin Pediatr Dent. 2022;46(1):20-23. doi:10.17796/1053-4625-46.1.4
Rahul M, Shrivastava N, Tewari N, Mathur V. Dentofacial manifestations of fetal warfarin syndrome in a paediatric patient. BMJ Case Rep. 2022;15(1):e243890. Published 2022 Jan 17. doi:10.1136/bcr-2021-243890
Sehgal T, Nanda A, Prakash S, Subramanian A. Use of modified-citrate tube to rectify spurious coagulopathy in smoker's polycythaemia: medical resolution of a dentist's dilemma. BMJ Case Rep. 2022;15(1):e246102. Published 2022 Jan 17. doi:10.1136/bcr-2021-246102
Yadav VS, Singh N, Bhatia A, Kamra P, Yadav R. A Modified suturing protocol for tripod stabilization of connective tissue graft and coronal advancement of tunnel flap for treatment of isolated gingival recession. Int J Periodontics Restorative Dent. 2022;42(1):e9-e14. doi:10.11607/prd.4782
Agarwal D, Ravi P, Purohit B, Priya H. The effect of energy and fat content labeling on food consumption pattern: a systematic review and meta-analysis. Nutr Rev. 2022;80(3):453-466. doi:10.1093/nutrit/nuab035
Gupta SR, Rajiv B, Yadav A, Sharma S. Binder's phenotype with ankyloglossia: Report of a rare inherited association in an Indian female. J Oral Maxillofac Pathol. 2022;26(Suppl 1):S5-S11. doi:10.4103/jomfp.jomfp_143_21
Prasad K, Dwivedi SN, Kant S, et al. Cohort Profile: The LoCARPoN-a population-based prospective cohort study in middle-aged and older adults in India. Int J Epidemiol. 2022;51(1):29-30m. doi:10.1093/ije/dyab078
Tewari N, Tamchos R, Chaurasia B, et al. Comparison of three protocols for the management of re-fracture of teeth with uncomplicated crown fractures. Dent Traumatol. 2022;38(1):71-76. doi:10.1111/edt.12709
Verma D, Kumar A, Rathee G, Dhingra K, Mukherjee M, Solanki P. Prospects of Nanomaterial based Biosensors: A Smart Approach for Bisphenol-A Detection in Dental Sealants. J Electrochem Soc. 2022;169: 027516. doi: 10.1149/1945-7111/ac
Yadav V, Sharma S, Kumar V, Chawla A, Logani A. cone beam computed tomographic cone beam computed tomographic characterization of short root anomaly in chloroquine-induced Stevens-Johnson Syndrome - a case report. Folia Med (Plovdiv). 2022;64(1):169-175. doi:10.3897/folmed.64.e58178
Dhingra K. Is periodontal disease a risk factor for oral cancer?. Evid Based Dent. 2022;23(1):20-21. doi:10.1038/s41432-022-0245-z
Jain RA, Gupta R, Verma M, Nanda A, Gill S, Mehra R. Comparative evaluation of load-bearing capacity and fracture analysis of PEEK and zirconia three-unit fixed dental prostheses: An in vitro study. Int J Prosthodont. 2022;35(2):225-232. doi:10.11607/ijp.7469
Kaur H, Gupta V, Mishra D, Yadav VS. Fibrosarcoma: Origin, differential diagnosis, and report of a case in the mandible. J Indian Soc Periodontol. 2022;26(2):169-177. doi:10.4103/jisp.jisp_188_21
Kv N, Jain V, Koli DK, Kumar S, Nanda A. Comparative Evaluation of Osteocalcin in Peri-implant Crevicular Fluid and Radiographic Bone Loss in Immediate Loading and Delayed Loading Protocols: A Preliminary Split-Mouth Randomized Controlled Trial. Int J Prosthodont. 2022;35(2):174-180. doi:10.11607/ijp.7489
Nayyar V, Bhutia O, Kakkar A, Mishra D. Primary intraosseous oncocytic mucoepidermoid carcinoma of the jaw: First case report. Oral Oncol. 2022;126:105732. doi:10.1016/j.oraloncology.2022.105732
Pandey S, Yadav P, Roychoudhury A, Bhutia O, Goswami D. A randomized controlled trial to compare functional, combined rigid and functional and rigid fixation in double mandibular fractures. J Oral Biol Craniofac Res. 2022;12(2):233-237. doi:10.1016/j.jobcr.2022.02.003
Purohit BM, Kharbanda OP, Priya H. Universal oral health coverage - Perspectives from a developing country. Int J Health Plann Manage. 2022;37(2):610-618. doi:10.1002/hpm.3361
Teh MT, Ma H, Liang YY, et al. Molecular signatures of tumour and its microenvironment for precise quantitative diagnosis of oral squamous cell carcinoma: An international multi-cohort diagnostic validation study. Cancers (Basel). 2022;14(6):1389. Published 2022 Mar 9. doi:10.3390/cancers14061389
Atif M, Mathur VP, Tewari N, Bansal K, Rahul M, Bakhshi S. Long-Term Effect of Anticancer Therapy on Dentition in Childhood Cancer Survivors: An Observational, Cross-Sectional Study. Indian J Pediatr. 2022;89(4):327-332. doi:10.1007/s12098-021-03818-1
Jot K, Roychoudhury A, Bhalla AS, Mishra D. Rare case of primary giant cell rich osteosarcoma in mandible. Oral Oncol. 2022;127:105784. doi:10.1016/j.oraloncology.2022.105784
Kumar V, Kumar A, Kumar M, Lone MR, Mishra D, Chauhan SS. NFκB (RelA) mediates transactivation of hnRNPD in oral cancer cells. Sci Rep. 2022;12(1):5944. Published 2022 Apr 8. doi:10.1038/s41598-022-09963-7
Mathur VP, Atif M, Duggal I, Tewari N, Duggal R, Chawla A. Reporting guidelines for in-silico studies using finite element analysis in medicine (RIFEM). Comput Methods Programs Biomed. 2022;216:106675. doi:10.1016/j.cmpb.2022.106675
Samrit VD, Wadhawan N, Kharbanda OP, Duggal R. Interdisciplinary management of complicated case of bilaterally impacted maxillary canines and missing lateral incisors with canine-premolar transposition–A 10-year follow-up. AJO-DO Clinical Companion. 2022;2(2): 180-191.
Yadav VS, Gupta V, Chawla A, Tewari N, Yadav R. Successful management of a large mucosal fenestration at 18-months follow-up. J Esthet Restor Dent. 2022;34(3):445-450. doi:10.1111/jerd.12855
Batra P, Kaur H, Dawar A, Mehta V. The threshold of acceptability of excessive gingival display by laypersons: a systematic review. Int J Esthet Dent. 2022;(2):216-235.
Qureshi T, Chaudhari PK. Successful 2 phase treatment of growing skeletal Class III malocclusion based upon cephalometric prognostic factor: A case report. J Orthod Sci. 2022;11:29. Published 2022 May 4. doi:10.4103/jos.jos_160_21
Rahul M, Atif M, Ganguly S, et al. Long-term effects of chemotherapy and radiation received during early childhood on the developing dentition of pediatric cancer patients [published online ahead of print, 2022 May 23]. Spec Care Dentist. 2022;10.1111/scd.12730. doi:10.1111/scd.12730
Virkhare A, Lakshmanan S, Bhutia O, Roychoudhury A, Mehta N, Pandey S. Does evoked electromyography detect the injured facial nerve recovery earlier than clinical assessments? J Oral Maxillofac Surg. 2022;8(5):814-821. doi:10.1016/j.joms.2021.12.010
Agarwal D, Purohit B, Ravi P, Priya H, Kumar V. Effectiveness of topical fluorides in prevention of radiation caries in adults: A systematic review and meta- analysis. Oral Oncol. 2022;129:105869. doi:10.1016/j.oraloncology.2022.105869
Dawar A, Kamra P, Anand D, Nayyar V, Mishra D, Pandey S. Oral mesotherapy technique for the treatment of physiologic gingival melanin hyperpigmentation using locally injectable vitamin C: a clinical and histologic cases series. Quintessence Int. 2022;53(7):580-588. doi:10.3290/j.qi.b3044857
Shahbaz Alam M, Dhiman A, Jain V, Bhutia O, Pruthi G. Vertical Bone Implant Contact Around Anterior Immediate Implants and Their Stability After Using Either Alloplast or L-PRF or Both in Peri-Implant Gap: A Prospective Randomized Trial. J Maxillofac Oral Surg. 2022;21(2):533-541. doi:10.1007/s12663-020-01426-8
Thapa P, Singh V, Bhatt S, et al. Development of multimodal micro-endoscopic system with oblique illumination for simultaneous fluorescence imaging and spectroscopy of oral cancer. J Biophotonics. 2022;15(6):e202100284. doi:10.1002/jbio.202100284
Tewari N, Goel S, Srivastav S, et al. 'CARE compliance' of case reports published in Dental Traumatology in the past two decades: A bibliometric analysis. Dent Traumatol. 2022;38(3):175-184. doi:10.1111/edt.12738
Jha S, Balachandran R, Sharma S, Kumar V, Chawla A, Logani A. A Novel Approach to Repositioning and Stabilization of a Luxated Tooth With Displacement Using a 3D Printed Guide. J Endod. 2022;48(7):936-942. doi:10.1016/j.joen.2022.03.014
Barbi W, Purohit BM. Serum Lactate Dehydrogenase Enzyme as a Tumor Marker in Potentially Malignant Disorders: A Systematic Review and Meta-Analysis. Asian Pac J Cancer Prev. 2022;23(8):2553-2559. Published 2022 Aug 1. doi:10.31557/APJCP.2022.23.8.2553
Lokade A, Tewari N, Goel S, Mathur VP, Srivastav S, Rahul M. Comparative evaluation of fragment reattachment protocols for the management of teeth with crown-root fractures. Dent Traumatol. 2022;38(4):319-324. doi:10.1111/edt.12745
Nangia D, Saini A, Krishnan A, et al. Quality and accuracy of patient-oriented Web-based information regarding tooth avulsion. Dent Traumatol. 2022;38(4):299-308. doi:10.1111/edt.12741
Nethan ST, Lakshmi K, Ralhan R, et al. Assessment of the Prevalence and Relationship of Tobacco Use and Associated Oral Lesions in an Urban Population of New Delhi: a Cross-Sectional Study. Indian J Surg. 2022;84(4):720–728. https://doi.org/10.1007/s12262-021-03055-y
Department of Conservative Dentistry and Endodontics
Department of Orthodontics and Dentofacial Deformities
Department of Pediatric and Preventive Dentistry
Prof. OP Kharbanda Total 100 +
| S.No. | Title of the Project | PI | Funding Agency |
|---|---|---|---|
| 1 | Treatment of temporomandibular joint disorders based on Vienna concept of functional occlusion | Dr. Ritu Duggal | Austria-Scientific & Technological Cooperation, Department of Science and Technology, Government of India |
| 2 | Effectiveness of training on best mercury hygiene practices in improving the knowledge regarding Minamata Convention among dental professionals | Dr. Ritu Duggal | Under National Oral Health Program |
| 3 | Efficacy of a teacher training program on role of sugars on oral health: A mixed-method study | Dr. Ritu Duggal | Under National Oral Health Program |
| 4 | Effectiveness of an oral health training program among Navodaya Vidyalaya Samiti staff nurses | Dr. Ritu Duggal | Under National Oral Health Program |
| 5 | Effectiveness of an oral health training program among Kendriya Vidyalaya Sangathan school teachers on the role of sugars in oral health and general health | Dr. Ritu Duggal | Under National Oral Health Program |
| 6 | Fluoride and sugar levels for the commercially available baby food supplements | Dr. Ritu Duggal | AIIMS Intramural |
| 7 | HLA related genetic propensity for manifestation of oral submucous fibrosis among North Indians | Dr. Ritu Duggal | AIIMS Intramural |
| 8 | Evaluation of the efficacy of tooth movement with Alignwise Clear Aligner System. | Dr. Vilas Samrit | Alignwise Smile Technologies |
| 9 | 3D printed aligners as a state of the art smile designing appliance for its integration in Indian public hospitals | Dr. Prabhat Kumar Chaudhari | Science and Engineering Research Board, Government of India |
| 10 | Automatic diagnosis and monitoring for orthodontic invisible appliance cases using artificial neural network | Dr. Prabhat Kumar Chaudhari | India-Taiwan programme of co-operation [Department of Science and Technology (DST), Government of India] |
| 11 | Finite Element Analysis and development of Miniscrew Implant Supported Bi-helix Appliance (MISBA) for true asymmetric maxillary expansion | Dr. Prabhat Kumar Chaudhari | AIIMS, New Delhi & IIT-Delhi |
| 12 | Evaluation of the effect of newer simplified protocols for fabrication of complete denture on denture quality, patient satisfaction, and nutritional status | Dr. Aditi Nanda | AIIMS Intramural |
| 13 | Evaluation of osteocalcin and metalloproteinase 8 levels in the periimplant crevicular fluid (PICF) around immediate dental implant placed with socket shield technique (SST) and conventional technique (CT) in maxillary anterior region- A randomized controlled pilot study | Dr. Dheeraj Kumar Koli | AIIMS Intramural |
| 14 | A Prospective Pilot study to evaluate the clinical success of a Tooth Colored metal free Self-Curing Resin-based material as an alternate to silver amalgam for Class-II Posterior Restoration | Dr. Amrita Chawla | AIIMS Intramural |
| 15 | Low intensity pulsed ultrasound (LIPUS) as a therapeutic adjunct to enhance periodontal healing subsequent to luxation dental injuries | Dr. Vijay Kumar | AIIMS Intramural |
| 16 | The role of novel self-assembling peptides in prevention of post radiation caries in head and neck cancer patients: a randomised controlled trial | Dr. Vijay Kumar | ICMR |
| 17 | Development and testing of 3D printed tooth prototype with anatomic complexity for pre-clinical endodontic training | Dr. Sidhartha Sharma | AIIMS Intramural |
| 18 | Fabrication and in-vivo (rat model) evaluation of novel local drug delivery system based on polymer nanocomposite for treatment of periodontitis | Dr. Kunaal Dhingra | ICMR |
| 19 | A randomized controlled trial evaluating subepithelial connective tissue graft and injectable platelet-rich fibrin with or without enamel matrix derivative for treating multiple gingival recessions in smokers | Dr. Kunaal Dhingra | AIIMS Intramural |
| 20 | Clinical, histomorphometric and 3-dimensional cone beam computed tomographic analysis of autogenous tooth bone graft mixed with injectable platelet rich fibrin for ridge preservation | Dr. Vikender Singh | AIIMS Intramural |
| 21 | Serum and saliva metabolomic profiling and identification of potential biomarkers in periodontitis by nuclear magnetic resonance spectroscopy | Dr. Anika Dawar | AIIMS Intramural |
| 22 | Development of the mobile app for prevention of dental diseases in children | Dr. Kalpana Bansal | AIIMS Intramural |
| 23 | Development and validation of Dental Trauma Awareness Tool for school teachers | Dr. Nitesh Tewari | ICMR |
| 24 | Comparative evaluation of module for sports dental injury prevention (MSIP) and combination of MSIP with custom-fabricated mouth-guard for prevention of traumatic dental injuries in 10-18 years old Kabaddi Players of Delhi-NCR region in a sports season: a cluster randomized controlled trial | Dr. Nitesh Tewari | ICMR |
| 25 | Cytotoxicity of intracanal medicaments used for root canal disinfection and their effect on proliferation and differentiation potentials of Stem Cells from Apical Papilla-An in-vitro study | Dr. Morankar Rahul | AIIMS Intramural |
| 26 | The detection of current and persistent oral HPV infection using non- invasive method in oral potentially malignant disorders with their clinical and molecular characteristics | Dr. Shalini Gupta | ICMR |
| 27 | To determine the concentration of betel nut alkaloids and catechin in current and past betel nut users and their association with pro- oncogenic cytokines and oral potentially malignant disorders | Dr. Shalini Gupta | AIIMS Intramural |
| 28 | Multi region sequencing to unveil the intra tumoral heterogeneity and novel biomarkers in oral squamous cell carcinoma in an Indian population: Case Control Study | Dr. Deepika Mishra | ICMR |
| 29 | Investigate the use of fluorescence based micro endoscopy, developing image repository and artificial intelligence based deep learning to detect oral squamous cell carcinoma and dysplasia in Indian population. | Dr. Deepika Mishra | Non funded |
| 30 | Explore the novel use of florescence based micro endoscopy and Raman spectroscopy for detection of oral cancer and dysplasia | Dr. Deepika Mishra | AIIMS-IIT-Delhi Inter Institutional Collaborative Research Grant |
| 31 | Retrospective study of oral pathology specimens: incisional vs excisional specimens and cytopathology vs histopathology | Dr. Deepika Mishra | Non funded |
| 32 | Molecular and immunological characterization of fibro-osseous lesions affecting oral and maxillofacial region | Dr. Deepika Mishra | AIIMS Intramural |
| 33 | Impact of simulation based teaching on knowledge of performer, actual conduct of aerosol generating procedures and self-confidence while handling patients with COVID-19 | Dr. Devalina Goswami | AIIMS Intramural |
| SL. NO | Title of the project | Collaborating Department/Institution |
|---|---|---|
| 1 | A Population based prospective cohort study to unravel the causes of stroke and cognitive decline: A cross cultural perspective | Neurology – Clinical Epidemiology, AIIMS, New Delhi |
| 2 | Functionalized Collagen nanoparticle impregnated silk nanoceramic composite 3D matrices for flat bone regeneration | IIT Guwahati |
| 3 | NLRP3 Inflammasome gene polymorphisms and their expression in Periodontitis- a genetic study in North Indian population | Dept. of Biochemistry, AIIMS, New Delhi |
| 4 | A prospective, active controlled, randomised, double blind, multicentre, phase III study to compare the safety and efficacy of biosimilar denosumab of Enzine Biosciences Limited Versus innovator denosumab in the treatment of postmenopausal osteoporosis, as Co-PI | Orthopedics, Endocrinology, Radiology, AIIMS, New Delhi |
| 5 | Childhood Cancer Survivorship Program (CCSP) Program comprised effects of cancer related chemotherapy, radiotherapy and bone marrow transplantation of dentofacial and oral structures as Co-Investigator (Interdisciplinary collaborative project with IRCH department | Department of Medical Oncology IRCH AIIMS NEW DELHI |
| 6 | A descriptive study to evaluate the extracutaneous and systemic involvement in children with inherited epidermolysis bullosa. | Dermatology and Venereology, AIIMS, New Delhi |
| 7 | Assessment of Quality of Life Among Adult Survivors of Head and Neck Ewing Sarcoma Family of Tumours | Department of Medical Oncology IRCH AIIMS NEW DELHI |
| 8 | Dental conditions and co morbidities in an elderly Population in North India | Department of Geriatric Medicine, AIIMS, New Delhi |
| 9 | Development and testing of 3D printed tooth prototype with anatomic complexity for pre-clinical endodontic training | Conservative and Endodontics CDER |
| 10 | Clinical, histomorphometric and 3- Dimensional Cone Beam Tomographic analysis of Autogenous Tooth Bone Graft mixed with Injectable Platelet Rich Fibrin for ridge preservation | Periodontics CDER |
| 11 | Subepithelial connective tissue graft and injectable platelet –rich fibrin with or without enamel matrix derivative for treating multiple gingival recessions in smokers: a randomized clinical trial | Periodontics CDER |
| 12 | Immunoexpression of HLA class II antigen system in Oral Submucous Fibrosis- study of genetic propensity among North Indians | Public Health dentistry CDER |
| 13 | A study to examine dependence, harm perception and motivation to quit amongst Indian areca nut users and pilot test an intervention module. | PSYCHIATRY & NDDTC AIIMS |
| 14 | Elucidating the cellular functions and clinical significance of Dipeptidyl Peptidase III (DPP III) in oral cancer. | Dept of Biochemistry, AIIMS and Div of Oral Pathology and Microbiology, CDER. |
| 15 | A pilot study to evaluate flourescence UV imaging for assessment of malignant and potentially malignant disorders in oral cavity and update and analysis of tongue cancer database. | Dept of Surgical Oncology, IRCH and Div of Oral Pathology and Microbiology, CDER. |
| 16 | An observational study to evaluate bone healing and recurrence rate within one year after topical application of 5 fluorouracil in the treatment of odontogenic keratocyst | Div of Oral and maxillofacial Surgery and Div of Oral Pathology and microbiology, CDER, AIIMS |
| 17 | Role of human Heterogeneous Nuclear Ribonucleoprotein D (hnRNPD) in oral cancer. | Dept of Biochemistry and Div of Oral Pathology and Microbiology, CDER AIIMS |
| 18 | Role of Negative Regulators of EGFR in Malignant Transformations of Oral Dysplasia | Dept of Biochemistry, AIIMS and Div of Oral Pathology and Microbiology, CDER |
| 19 | A phase III randomised controlled study comparing xerostomia after tubarial salivary gland sparing IMRT versus standard IMRT in patients with locally advanced oropharyngeal squamous cell carcinoma. | Radiation Oncology, AIIMS and Div of Oral Pathology and Microbiology, CDER |
| 20 | Evaluation of two rehydration protocols for Fractured tooth fragments in terms of depth of penetrations of resin tags in dentin using confocal laser scanning microscopy. | Div of Pedodontics and Div of Oral Pathology and Microbiology, CDER |
| 21 | Multi-Model Autofluorescence, fluorescence, Polarization, Micro endoscopy and Spectroscopy based detection of common cancers of mouth, breast, Gut, respiratory tract, skin and female genital tract. | Department of General Surgery and Div of Oral Pathology and Microbiology, CDER. |
| 22 | Tumors and cysts of jaw: Evaluation by dual energy computed tomography with limited MRI correlation. | Department of Radiodiagnosis and Div of Oral Pathology and Microbiology CDER, AIIMS. |
| 23 | European Society Of Intensive Care Medicine Covid-19 Project (Unite-Covid-19) | European Society of Intensive Care Medicine |
| 24 | Comparison of 5 factor modified fraility index and ASA classification to predict morbidity and mortality in patients undergoing arthroplasty – A prospective observational study | Dept. of Orthopedics |
| 25 | Role of Parecoxib, A Selective Cyclooxygenase-2 Inhibitor, for Reduction of Severity of Acute Pancreatitis: A Randomized Controlled Trial | Dept. of Gastroenterology and Human Nutrition |
| 26 | Effect of Timing of Biliary Drainage (Urgent versus Early) in Patients with Severe Acute Cholangitis on 30 days Mortality: A Randomized controlled trial (ACT trial) | Dept. of Gastroenterology and Human Nutrition |
| 27 | Randomized controlled trial to assess the efficacy of swallowing exercise on dysphagia among post extubated patients admitted in ICU of AIIMS | College of Nursing |
| 28 | Development and preliminary validation of a novel pain assessment scale based on pulpal symptoms | Conservative Dentistry and Endodontics, CDER |
| S.NO. | Name of Department | Name Of Faculty | Days (OPD) |
|---|---|---|---|
| 1 | Oral Medicine and Radiology | Dr. Shalini Gupta | Daily |
| 2 | Oral & Maxillofacial Surgery | Dr. Ajoy Roychoudhury | Monday/Friday |
| Dr. Ongkila Bhutia | Wednesday/Saturday | ||
| Dr. Rahul Yadav | Tuesday/Thursday | ||
| Dr. Krushna Vasant Kumar Bhatt | Tuesday/Thursday | ||
| 3 | Maxillofacial Prosthodontics | Dr. Veena Jain | Wednesday/Saturday |
| Dr. Dheeraj Kumar Koli | Monday/Thursday | ||
| Dr. Aditi Nanda | Tuesday/Friday | ||
| All Faculty | Monday/Thursday (2pm) | ||
| 4 | Conservative Dentistry & Endodontics | Dr. Ajay Logani | All days except Friday |
| Dr. Vijay Kumar | Wed/Sat | ||
| Dr. Amrita Chawla | Tue/Fri | ||
| Dr. Sidhartha Sharma | Mon/Thur | ||
| 5 | Orthodontics and Dentofacial Deformities | Dr. Ritu Duggal | Wed/Thur/Fri/Sat |
| Dr. Vilas D. Samrit | Tue/Wed/Fri/Sat | ||
| Dr. Prabhat Kumar Chaudhari | Mon/Wed/Thu/Fri | ||
| 6 | Periodontics | Dr. Kunaal Dhingra | Mon/Tue/Thur/Fri |
| Dr. Vikender Singh | Tue/Wed/Fri/Sat | ||
| Dr. Anika Dawar | Mon/Wed/Thu/Sat | ||
| 7 | Pedodontics and Preventive Dentistry | Dr. Vijay P. Mathur | Wed/Fri/Sat |
| Dr. Kalpana Bansal | Tue/Thu/Sat | ||
| Dr. Nitesh Tiwari | Mon/Wed/Fri/Sat | ||
| Dr. Rahul G. Morankar | Mon/Tue/Thur/Sat | ||
| 8 | Public Health Dentistry | Dr. Harsh Priya | Monday to Saturday |
| Dr. Bharathi M. Purohit | Monday to Saturday |
| Name of course | Duration | Application procedure |
|---|---|---|
| B. Sc. (Dental Hygiene) | Three years | Through entrance examination held by All India Institute of Medical Sciences, New Delhi |
| B. Sc. (Dental Operating Room Assistance) | Three years |
| Name of course | Duration | Application procedure |
|---|---|---|
| M.D.S. (Orthodontics and Dentofacial Orthopedics) | Three years | Through entrance examination held by All India Institute of Medical Sciences, New Delhi www.aiimsexams.ac.in |
| M.D.S. (Prosthodontics) | Three years | |
| M.D.S. (Conservative Dentistry and Endodontics) | Three years | |
| M.D.S. (Oral and Maxillofacial Surgery) | Three years | |
| M.D.S. (Pedodontics and Preventive Dentistry) | Three years |
| Name of course | Duration | Application procedure |
|---|---|---|
| Cleft and Craniofacial Orthodontics | Two years | Through entrance examination held by All India Institute of Medical Sciences, New Delhi www.aiimsexams.ac.in |
The present building of Centre for Dental Education and Research (CDER) is a continuation of erstwhile Department of Dental Surgery established in 1960 with single dental surgeon. The department saw significant progress from non-teaching to teaching and subsequently starting Post-graduation in Orthodontics and Dentofacial Orthopedics in 1984, Maxillofacial Prosthodontics in 1995, Conservative Dentistry and Endodontics in 2003 and Oral and Maxillofacial Surgery in 2005. The Governing Body of the Institute approved in principle establishment of post graduate dental specialty centre in 1999 and the foundation stone for this building was laid in May 2003. As on now this centre is one of the outstanding specialized centres of AIIMS and carries on the tradition of providing excellent patient care, post graduate education and research. The fifth specialty Pediatric and Preventive Dentistry post graduate courses started in year 2017 and it is envisaged to start post-graduation in several other subjects, PhD and fellowships in other branches of dentistry.
The CDER has been actively providing policy and program support to the Govt by advising and participating in various technical and scientific work of Govt of India. The erstwhile Department of Dental Surgery was named as nodal agency for implementation of pilot project on National Oral Health Care Program in the country in year 1999. Subsequently, the Centre developed the implementation strategies for National Oral Health Care Program and developed several demonstration programs and guidelines for oral disease prevention. The Centre also developed several IEC materials, manuals, educative film on Oral health and chapters for NCERT books on oral health awareness and disease prevention. The Centre also conducted several training programmes for dental surgeons, health workers, nurses, school teachers and NGOs on primary prevention of oral diseases and effective tobacco cessation counselling. The Centre has been involved in several projects of Ministry of Health and Family Welfare, Indian Council for Medical Research, Department of Science & Technology, Department of Biotechnology, CSIR and WHO. The Centre provides essential treatment at AIIMS outreach centres at Mid-town Rotary Hospital at Trilokpuri, and CRHSP, Ballabhgarh. The Centre was the Nodal agency for National Oral Health Care Programme (1999-2005).
The Centre was given the status of National Centre of Excellence for Implementation of National Oral Health Program in February 2014 and WHO CC for Oral Health Promotion in May 2014. The faculty from the Centre have been instrumental in development of operational guidelines for National Oral Health Program, Regional Oral Health Strategy, Draft National Oral Health Policy and guidelines for dental screening under Rashtriya Bal Swasthya Karyakram (RBSK).
As part of National Oral Health Program, CDER has also developed a web portal and app named EDantSeva for use as informative and educative electronic resource for public on oral health issues as well as data for dental. Professionals.
The faculty from the Centre is providing leadership role in various technical and professional organizations at key positions and are publishing a significant number of scientific articles in journals of repute.
Prof. Sandeep Chauhan, Chief, Cardio-Thoracic Sciences Centre
Prof. P. RAJASHEKAR Addl. Medical Superintendent
Obituary of Prof. Nagarur Gopinath, founder & first chief of Cardiothoracic Sciences Center
Cardiothoracic Sciences Centre began functioning in the new building in 1982. The Centre has 200 beds exclusively for Cardiology and Cardiovascular Surgery with all the ancilliary facilities required for comprehensive care for all cardiovascular disorders. In 1986 the Centre became fully independent and functioned entirely from the new 7 floor building. The Cardiothoracic Sciences Centre has the following departments.
Professor N. Gopinath was the founder and first Chief of Cardiothoracic Centre. He was followed by Professor M.L. Bhatia, Professor R. Tandon , Professor P. Venugopal, Professor A. Sampath Kumar, Professor Balram Airan and Professor Vinay Kumar Bahl.
There are eight fully equipped operating rooms with the state-of-art technology to carry out all kinds of complex cardiothoracic and vascular procedures 24X7 through out the year accessible and affordable to everyone. Total bed capacity (136) under CTVS in General ward is distributed in 1st, 4th, 5th and 6thfloors of Cardiothoracic sciences center of which
| Name | E-mail add | DESIGNATION |
|---|---|---|
| Dr. A.K.BISOI | drakbisoi[at]gmail[dot]com | Prof. & HOD (CTVS) |
| Dr. V.DEVAGOUROU | vdeva[at]hotmail[dot]com | Professor (CTVS) |
| Dr. SACHIN TALWAR | sachintalwar[at]hotmail[dot]com, drsachintalwar[at]gmail[dot]com | Professor (CTVS) |
| Dr. P. RAJASHEKAR | praja[at]aiims[dot]edu | Professor (CTVS) |
| Dr. A.K.BISOI | drakbisoi[at]gmail[dot]com | Prof. & HOD (CTVS) |
| Dr. MANOJ SAHU | drmanojsahu[at]gmail[dot]com | Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SARVESH PAL SINGH | sarveshpalsingh[at]gmail[dot]com | Additional Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. P.RAMESH MENON | rpmpgi[at]gmail[dot]com | Additional Professor Pediatrics (Neonatalogy) in CTVS |
| Dr. PRADEEP RAMAKRISHNAN | pradeep[dot]r[dot]reddy85[at]gmail[dot]com | Associate Professor (CTVS) |
| Dr. UMMED SINGH | drusd[at]yahoo[dot]com | Associate Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SUSHAMA GAYATRI B | sushama[dot]gayatri[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. NAVNITA KISKU | navnita[dot]kisku[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. AMITABH SATSANGI | indiactvs[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. MAYANK YADAV | drmayankctvs[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr.BHARATH.V | drbharathv[at]gmail[dot]com | Assistant Professor (CTVS) |
List of Faculty Members in the Department of Cardiology
| Name | Designation | Contact No/Email |
|---|---|---|
| Dr. Neeti Makhija | Professor & HOD | 9868398102 |
| Dr. Sandeep Chauhan | CHIEF, CTC | - |
| Dr. Poonam Malhotra kapoor | Professor | 9868398103 |
| Dr. Minati Choudhury | Professor | 9868398104 |
| Dr.Sambhnath Das | Professor | 9868398105 |
| Dr. Parag Gharde | Professor | 9868398106 |
| Dr. Suruchi Hasija | Professor | 9868398107 |
| Dr. Arindam Choudhury | Professor | 9868398107 |
| Name | Designation |
|---|---|
| Dr. Ruma Ray | Professor |
| Dr. Sudheer Kumar A | Professor |
| Name | Designation | Contact No/Email |
|---|---|---|
| Dr. Priya Jagia | Prof. & HOD | 9868398117 |
| Dr. Sanjeev Kumar | Additional Prof. | - |
| Dr. Niraj N.Pandey | Asstt. Prof. | - |
| Name | Designation |
|---|---|
| Dr. R. Lakshmy | Professor |
| Name | Designation |
|---|---|
| Dr. Sujata Mohanty(Stem Cell) | Professor |
| Name | Designation |
|---|---|
| Dr. Aarti Vij | Professor |
| Dr. Mede Charan Raj | Asstt. Professor |
| Name | Designation |
|---|---|
| Dr. Chetan Patal | Professor |
Attended National Conference on Govt. Procurement being organised by Indian Institute of Materials and Management at New Delhi
Programme co-ordinator, training programme on Hospital Management and Administration for Medical Superintendents, GDMOs non specialists of Coal India at IICM and CME on Clinical issues during field visit to AIIMS in January, 2009.
The laboratory is NABL accredited, fully equipped to offer complete diagnostic services for diagnosis of tuberculosis (TB), Non-tubercular Mycobacteria (NTM), and drug resistance to various anti-tubercular drugs by molecular as well as conventional methods. The laboratory offers microscopy, culture (both liquid and solid), PCR and Gene-Xpert for diagnosis of TB and NTM. In addition, the conventional drug sensitivity testing in liquid and solid culture media, Gene-Xpert, Line Probe Assay are available for detecting resistance to both first line and second line drugs. The laboratory is equipped with state of art molecular typing techniques for TB. All the techniques are quality assured.
The laboratory carries out research under several funded schemes (Extramural funding support for Whole Genome Sequencing, Early Bactericidal Activity, Therapeutic Drug Monitoring, Point of Care tests (Aptamer based), Novel biomarkers, Rapid molecular drug resistance detection, Molecular Epidemiology of MDR-TB).
| S. no | Test performed | Product/material of the test (Sample) |
|---|---|---|
| 1 | AFB Smear (Ziehl Neelsen Staining) | Pulmonary & Extrapulmonary samples |
| 2 | Fluorescent staining for M. tuberculosis | Pulmonary & Extrapulmonary samples |
| 3 | MGIT 960 Mycobacteria Liquid Cultures. | Pulmonary & Extrapulmonary samples |
| 4 | Lowenstein Jensen Solid Culture for Mycobacteria | Pulmonary & Extrapulmonary samples |
| 5 | Drug Susceptibility Test – MGIT 960 Liquid Culture DST first line and second line drugs | Pulmonary & Extrapulmonary samples |
| 6 | Drug Susceptibility Test – Lowenstein Jensen Solid first line and second line drugs | Pulmonary & Extrapulmonary samples |
| 7 | Drug Susceptibility Test for NTM | Pulmonary & Extrapulmonary samples |
| 8 | Gene Xpert MTB/Rif | Pulmonary & Extrapulmonary samples |
| 9 | Polymerase Chain Reaction targeting Mpt64 gene | Pulmonary & Extrapulmonary samples |
| 10 | TRUNAT-MTB-RIF detection | Pulmonary & Extrapulmonary samples |
| 11 | Line Probe Assay (Hain’s) | Pulmonary & Extrapulmonary samples |
The Mycology Laboratory, Department of Microbiology, AIIMS, New Delhi has been designated as the ‘Advanced Mycology Diagnostic and Research Centre’ by ICMR.
List of investigations available:
| S. no | Test performed | Product/material of the test (Sample) |
|---|---|---|
| 1 | Direct KOH mount (with calcofluor white) | Respiratory samples, Tissues, Pus, Sterile fluids etc. |
| 2 | Conventional Culture for fungi | All Samples (Except Blood) |
| 3 | Gram’s stain | All Samples (Except Blood) |
| 4 | Giemsa stain | Samples for suspected deep mycoses (Histoplamosis etc.) |
| 5 | Automated Culture for fungi by BACTEC | Blood & sterile fluids |
| 6 | Modified ZN stain and culture for Nocardia | All Samples (Except Blood) |
| 7 | India ink preparation | CSF |
| 8 | Galactomannan antigen by ELISA test every Tuesday and Friday | Serum, BAL & CSF |
| 9 | Galactomannan antigen by LFA | On request |
| 10 | Beta-D-Glucan | Serum |
| 11 | Histoplasma urinary antigen | Urine |
| 12 | Aspergillus specific antibodies (IgG-IgM) by LFA | Serum |
| 13 | Cryptococcal antigen detection | Serum & CSF |
| 14 | Therapeutic drug monitoring for Voriconazole, Itraconazole and Posaconazole | Serum (Trough levels) |
| 15 | Drug Susceptibility Testing (DST) of Yeast (By VITEK and Microbroth dilution test) | Performed for all yeasts isolated from sterile sites |
| 16 | Drug Susceptibility Testing (DST) of Filamentous fungi (By Microbroth dilution test ) | On request |
| 17 | PCR for Aspergillus, Mucorales, Pan-fungal etc. | On request |
The National HIV/AIDS Reference Laboratory provides diagnostic and monitoring services to patients with HIV/AIDS which includes OPD as well as indoor patients. It is the first laboratory at AIIMS to receive NABL accreditation which has been continuously maintained.
| S. no | Test performed | Product/material of the test (Sample) |
|---|---|---|
| Absolute CD4 T-Lymphocytes Count | WHOLE BLOOD | |
| HIV 1+2 Antibodies | Serum | |
| HIV 1+2 Antibodies | Serum | |
| HIV 1+2 Antibodies | Serum |
Specimen from the STD clinics and Gynaecology Department are received for screening for the reproductive tract infection (RTI) or the bacterial STDs. The direct smears for Bacterial Vaginosis or vaginitis are screened. Microscopy and cultures for N. gonorrhoeae and the antibiotic resistance monitoring is undertaken. Besides the semen specimen are cultured in case any bacterial infection are suspected. PCR for N. gonorrhoeae and C. trachomatis for uro-genital and extra-genital samples is also available. Culture for T. vaginalis is also available.
| S.No. | Test name | Sample |
|---|---|---|
| 1. | Gram’s stain for GNDC | Urethral Swab / Discharge |
| Endocervical swab / Discharge | ||
| Rectal swab | ||
| Oro pharyngeal swab | ||
| 2. | Gram’s stain for Nugents scoring | Vaginal Discharge/swab |
| 3. | Culture and AST forNeisseria gonorrhoeae | Urethral Swab / Discharge |
| Endocervical swab / Discharge | ||
| Rectal swab | ||
| Oro pharyngeal swab | ||
| 4. | Routine Bacterial Culture and Susceptibility testing | EPS |
| Semen | ||
| HVS | ||
| Vaginal discharge | ||
| Endometrial aspirate | ||
| 5. | Culture forTrichomonas vaginalis | Vaginal discharge /swab |
| Urethral Discharge/swab | ||
| Urine | ||
| 6. | PCR forNeisseria gonorrhoeae | Urethral Swab / Discharge |
| Endocervical swab / Discharge | ||
| Rectal swab | ||
| Oro pharyngeal swab | ||
| 7. | PCR forChlamydia trachomatis | Urethral Swab / Discharge |
| Endocervical swab / Discharge | ||
| Rectal swab | ||
| Oro pharyngeal swab |
For Online OPD appointment please visit
For physical New Appointment please visit at New Raj Kumari Amirit Kaur OPD at 8.00 am to 10.00 am
For online Laboratory report visit
For tracing lab reports visit Hematology OPD 5th Floor, New Raj Kumari Amirit Kaur OPD
PhD
Dr. A.K. Karak, 1986
Dr. Sanjana Dayal, 1995
Dr. Sandeep, 2000
Long term trainees for two years :
| Candidate | Tenure | Current Address | Email ID |
|---|---|---|---|
| Dr. Venkatesan | Jul 2012 | Assistant Professor, AFMC Pune | ltcolsvenkatesan@gmail.com |
| Dr. Abhishek | Jan 2012 | Mahaveer Cancer Institute, Jaipur | garcon007@yahoo.com; |
| Dr. Narender Tejwani | Jan 2011 | Jay Pee Hospital, Noida | mbbsnt@gmail.com |
| Dr. Mrinalini | July 2010 | Associate Professor, UCMS and GTB hospital, Delhi | mrinalini.kotru@gmail.com |
| Dr. Sonal Jain Malhotra | Jan 2010 | Rajeev Gandhi Cancer research, Rohini, New Delhi | sonalmalhotra80@gmail.com |
| Gurmeet singh | Jul 2009 | Bhilai Steel Plant | vicky.gurmeet@gmail.com |
| Dr. Jasmita Dass | Jan 2009 | Sir Ganga Ram Hospital, New Delhi | drjasmita@gmail.com |
| Dr. JM Khunger | Jan 2009 | Professor, Safdarjung Hospital, New Delhi | drjmkhunger@rediffmail.com; |
| Dr. Monica Sharma | Jan 2009 | Professor, Safdarjung Hospital, New Delhi | monica_sharmamd@hotmail.com; |
| Dr. Anita Chopra | Jan 2008 | Dept. of Medical Oncology; AIIMS, New Delhi | chopraanita2005@gmail.com |
| Dr. Prashant Sharma | Jan 2007 | PGI Chandigarh | prashant.sh@gmail.com; |
| Dr. Sanjeev Gupta | July 2007 | Dept. of Medical Oncology; AIIMS, New Delhi | drskgupta@rediffmail.com |
| Dr. Bhushan Asthana | July 2006 | Associate Professor, R & R hospital, New Delhi | bhushanasthana@yahoo.com |
| Dr. Rakhee Kar | Jan 2006 | Associate Professor, JIPMER, Poducherry | rakhee_kar@rediffmail.com; |
| Dr. Jyoti Bajaj | Jan 2005 | GCRI Ahmedabad, Gujarat | jo_bajaj@yahoo.com |
| Dr. Shyamali Dutta | Consultant, Dept. of Hematology, NRS Medical College, Kolkata | ankilaanu@yahoo.co.in drshyamalidutta@gmail.com | |
| Dr. U. Sriniwas | Jan 2004 | Consultant, hematology, Hyderabad | upendra.srinivas@relianceada.com; upendra_srinivas@yahoo.co.in; |
| Dr. Pankhi Dutta | Jan 2003 | Hospital 7 hills, Mumbai | pankhidutta@gmail.com; pankhi_dutta@yahoo.co.in; |
| Dr. T Chatterjee | Jan 2002 | Consultant & HOD dept. of transfusion medicine, AFMC Pune | ctathagat@hotmail.com; |
| Candidate | Year of joining | Current address | Email ID |
|---|---|---|---|
| Dr. Ashish Dixit | 2001 July | Dr. Ashish Dixit Consultant in Clinical Hematology and Blood & Marrow Transplant Department of Hematology, Medical Oncology and Transplant Comprehensive Cancer Center Manipal Hospital Bangalore, Karnataka (India) | adxt001@gmail.com; |
| Dr. Maitreyee Bhattacharyya | 2002 Jan | Professor & Head, Hematology, dept., NRS Medical College, Kolkata | mbhattyacharyya@yahoo.co.in; |
| Dr. Dharma Choudhary | 2003 Jan | Consultant, BL Kapoor Hospital, Delhi | dharmahemat@gmail.com; drdharma@hotmail.com; dr_drchoudhary@yahoo.com; |
| Dr. Pravas Mishra | 2003 June | Addl. Professor, Dept. of Hematology, AIIMS, New Delhi | pmishra.aiims@gmail.com |
| Dr. Jena Bhattacharyya (Jina Bhattacharyya) | 2003 June | Associate Professor, Department of Clinical Hematology, GMCH, Guwahati | drjinabhattacharyya@yahoo.in; |
| Laxmi Pillai | 2004 Jan | UK | lakspillai@yahoo.com; |
| Narender AMVR | 2004 Jan | Consultant, Nizam’s Institute Hyderabad | naren.anukonda@gmail.com; paddu_naren@yahoo.co.in; paddunaren@gmail.com; |
| Shruti Prem | 2004 Jan | Kerala | shrutiprem@gmail.com; |
| Shyam Rathi | July 2005 | Bombay Hospital, Mumbai | drshyamrathi@yahoo.com; |
| Niranjan Rathod | July 2005 | Kokilaben Hospital | drniranjanrathod@gmail.com; |
| Prantar Chakrabarti | 2005 | Consultant institute of Immunohematology, Kolkata | |
| Rahul Naithani | 2006 july | Consultant, Max Healthcare Saket, New Delhi | |
| Rahul Bhargava | July 2006 | Medanta Medicity, Gurgaon | dr_rahul6@hotmail.com; bhargava777@gmail.com; bhargava777@rediffmail.com; |
| Tuphan Kanti Dolai | July 2006 | NRS, Kolkata | tkdolai@hotmail.com; |
| Tarun Verma | Jan 2007 | Command hospital, Lucknow | sonalitarun@yahoo.co.in; |
| Rajan Kapoor | Jan 2008 | Associate Army Hospital R&R New Delhi | majrkapoor@gmail.com |
| Nitin Gupta | Jan 2008 | BL Kapoor | docnitingupta@gmail.com |
| Narender Agarwal | Jan 2009 | Rajeev Gandhi Cancer Institute, Rohini | narendra_ag1@rediffmail.com |
| Sanjeev Sharma | July 2009 | BL Kapoor | sksanjeev13@yahoo.com; |
| Suman Pramanik | Jan 2010 | Command Hospital, Kolkata | suman.surendra@gmail.com; |
| Sunil Gupta | July 2010 | Action Balaji, Paschim Vihar, New Delhi | sunilkumaraiims@yahoo.co.in; |
| Avinash Kr Singh | July 2010 | avinash.pmch@gmail.com | |
| Anirudh Dayama | Jan 2011 | Artemas Gurgaon | dayama@gmail.com; |
| Pawan Kumar Singh | Jan 2012 | Jay Pee Hospital, Noida | pawan2809@gmail.com; |
| Mukul Agarwal | July 2012 | Rajiv Gandhi Hospital | mukulmamc@gmail.com |
| Rajeev | July 2011 | Assistant Professor, Army Hospital R&R | pooja_rajeev@rediffmail.com |
| Sudhir | July 2011 | PGI Rohtak | ssmantri74@yahoo.com |
Dr. R Saxena received the following awards
Dr HP PATI
Dr M Mahapatra
Dr Pravas Mishra
CMEs/Workshops/Symposia/National and International Conferences
2019: The department organized 60th Annual Conference of Indian Society of Hematology and Blood Transfusion (HAEMATOCON 2019) dated 7-10 November 2019. More than 1500 delegates participated in the conference. It also organized three workshops on 7 November 2019 as part of the conference. These workshops were on:
2020: The department had organized a workshop on “Role of RTPCR in Haematology” on 20 November 2020 as a part of 61st Annual Conference of Indian Society of Haematology and Blood Transfusion (ISHBT) - HEMATOCON 2020 in the virtual mode.
The department of hematology provided consultative services to patients of thalassemia, in coordination with National Thalassemia Welfare Society. Care to hemophilia was provided in coordination with Hemophilia Federation of India.
Dr. R. Saxena became an invited Member of Reach the World Forum of International society of Thrombosis and Hemostasis 2009 onwards. She was elected as the President Elect, Indian Society of Hematology and Transfusion Medicine 2008-09. She was appointed Member Secretary - Institution Ethics Committee, AIIMS w.e.f. August 2008. She continues to be Executive member Indian society of Hematology and Transfusion medicine 2006-2008, Member, Medical Advisory Board, HFI, 2005, Member, ICMR project review committee for Genetics, hematology, anatomy2005, Coordinator ISHTM-IIMS EQAP. Since 2003, Member: Subject expert committee for technical evaluation of proposals under women scientist scheme, Department of Science and Technology, Government of India. June 2005, Member, Technical Specification for single bid equipment, Chairman, Technical Specification Committee for computer stationery
Dr. H Pati was elected Honorary secretary of India Society of Hematology & Transfusion Medicine for 3 years 2008- 2011.
Dr. M Mahapatra continued as an Executive member of Indian Society of Hematology and Transfusion Medicine (ISHTM), was selected as the Organizing Secretary of golden jubilee conference of Indian society of Hematology and Transfusion medicine (ISHTM). He became a fellow of University of British Columbia after completing one year fellowship in Leukemia and Bone Marrow Transplant at Vancouver, Canada
STEM CELL TRANSPLANTATION (Bone marrow transplant, peripheral blood transplant)
Hematology services are available on the outpatient basis and in specialty clinics for hemophilia, thrombophilia, stem cell transplantation, thalassemia and leukemias. All patients are managed on predetermined protocols after detailed investigations. Department has specialized laboratories, which perform extensive state of the art investigations for leukemias, bleeding disorders, hemoglobinopathies and anemias.
INDOOR
In Patient Treatment
The hematology department has treated an increasing number of patients of leukemias, aplastic anemia, idiopathic thrombocytopenic purpura, lymphomas, myelodysplastic syndrome, hemophilia, multiple myeloma and various other hematological disorders as indoor patients. In the past year, 20 allogeneic transplants were performed successfully. The department also has a Day Care Centre for chemotherapy, procedures and blood product transfusions for hematological patients.
Inpatients census
General ward patients 547 (C2, Hematology ward and others)
Private ward patients 378
TOTAL 925
DAY CARE CENTER
Department has a six bedded day care unit to provide blood transfusion support for all hematology patients such as aplastic anemia, thalassemia and myelodysplastic syndrome and Factor therapy for hemophilia patients, platelet support and fresh frozen plasma/ cryoprecipitate for patients with platelet function defects and rare factor deficiencies.
In addition bone marrow aspirate, biopsies, intra-thecal and intravenous chemotherapy are given in the daycare to leukemia and lymphoma patients. Monoclonal antibody therapy, growth factor support, minor procedures like central line placement, removal etc are performed here. Other important hematological procedures like phlebotomy for polycythemia vera, chelation for iron overload are undertaken here on a daily basis.
Census of April 2008 to March 2009 of Hematology Day Care Centre
| Month | Blood Transfusions | Bone Biopsy & Bone Marrow Aspirates | Chemo therapy | IT | Other procedures | Total Admission |
|---|---|---|---|---|---|---|
| April | 362 | 82 | 76 | 16 | 55 | 441 |
| May | 251 | 92 | 130 | 16 | 94 | 498 |
| June | 362 | 103 | 78 | 12 | 95 | 564 |
| July | 217 | 120 | 118 | 12 | 64 | 473 |
| August | 133 | 91 | 92 | 21 | 73 | 344 |
| September | 350 | 93 | 112 | 22 | 113 | 589 |
| October | 104 | 112 | 104 | 15 | 24 | 359 |
| November | 221 | 106 | 125 | 22 | 24 | 498 |
| December | 292 | 68 | 101 | 19 | 74 | 487 |
| January | 256 | 87 | 147 | 8 | 95 | 507 |
| February | 255 | 94 | 145 | 19 | 115 | 524 |
| March | 256 | 126 | 151 | 10 | 125 | 555 |
| TOTAL | 3059 | 1174 | 1379 | 191 | 1365 | 5939 |
Clinical Apheresis Procedures
Single Donor Platelets (SDP) 870
Peripheral blood stem cell (PBSC) collection 19
Plasma pheresis 2
The department runs its out patient department on the third floor of the main Amrit Kaur OPD block. Regular Hematology OPD is on Monday/Wednesday/Friday from 9:30 am to 6.00 pm. Oncology patients are seen in the Monday in the Hemato-oncology clinic (HO). The Monday morning clinic is for chronic myeloid leukemia and chronic myeloproliferative disorders such as PV, MF, ET etc
| Monday ( MORNING) | Monday (AFTERNOON) |
|---|---|
| CML | Leukemia, lymphoma, multiple myeloma |
| CMPD | Myelodysplastic syndrome |
| Wednesday | Friday |
| Immune Thrombocytopenia, Hemolytic Anemia, Other Anemias | Aplastic anemia |
The department conducts specialty care clinics e.g. Hematopoietic Stem Cell Transplant clinic on Tuesday morning, Hemostasis Clinic (HC) on Thursday morning and a Long Term Leukemia survivor Clinic on Saturday mornings
Special clinics are conducted on Tuesday/Thursday and Saturday for patients with special problems and those who need integrated management.
| Tuesday | Thursday | Saturday |
|---|---|---|
| Transplant clinic | Hemostasis and thrombosis clinic | Long term follow up clinic |
| Patients planned for or post hematopoietic stem cell transplantation | Patients with hemophilia, deep vein thrombosis and other inherited or acquired bleeding problems | Leukemia, lymphoma patients off therapy, in remission, evaluation for long term sequelae |
| General Hematology | Special clinics | Grand Total | ||||||||||
| Male | Female | Total (H) | ||||||||||
| HO | HC | HA | CML | HS | HT | HL | ||||||
| Old cases | 16240 | 7202 | 23442 | 10000 | 3400 | 2042 | 3300 | 2000 | 1500 | 1200 | 46884 | |
| Male | Female | Total (H) | HO | HC | HA | CML | HS | HT | HL | Grand total | ||
| New Cases | 2222 | 1200 | 3422 | 1320 | 660 | 440 | 223 | 197 | 30 | 65 | 5278 | |
MBBS:
Faculty from the department of Hematology deliver lectures and practical sessions to MBBS students in Semester –IV and final year. The teaching covers pathology and clinical hematology lectures. This includes a combination of didactic lectures, interactive case sessions, practical demonstrations and discussions.
MD courses:
MD (Pathology), MD (Laboratory medicine and MD (Transfusion Medicine) residents are trained during routine posting in the Hematology laboratory posting. MD (Pediatrics) and MD (Internal Medicine) residents are trained in Clinical Hematology postings. Seminars, case studies and morphology sessions are conducted every week.
DM courses:
The department offers DM (Clinical Hematology) and DM (Hematopathology) courses with intake every 6 months. This involves comprehensive training in various aspects of Haematology specialty for 3 years. Seminars, case studies, microteaching sessions, journal club sessions form part of active teaching sessions conducted twice a week. The department participates in Clinical Case Rounds and Clinical Grand rounds attended by entire AIIMS faculty and resident doctors. DM candidates of Pediatric Oncology specialty are trained as part of their rotation in the department.
Short term Training/Visitorship/Observership
Short term training in Hematology for 3 months is offered to interested candidates. The Department offers following types of training programs:
(A) DM Hematopathology:
Duration: 3 years
(B) DM Clinical Hematology:
Duration: 3 years
(C) Ph.D and PDF:
The Department has PhD Hematology program. PDF and research associate positions are available after PhD.
| S. no | Test performed | Product/material of the test (Sample) |
|---|---|---|
| 1 | Gram’s stain for Bacteria | Sputum, BAL, mini-BAL, Endotracheal aspirate, Sterile body fluids (pleural, peritoneal, synovial etc), Urine, Tissues, Pus, Swabs, CSF, Bone marrow |
| 2 | Culture and susceptibility test: Culture identification (conventional methods and MALDI TOF) and susceptibility testing by disk diffusion method | Blood and bone marrow, Sputum/BAL/miniBAL/Endotracheal aspirate (Respiratory samples), Swab/Pus/ drain fluid/aspirate/catheter tip/biopsy/ urine/PCN/ CSF/sterile body fluids/stool |
| 3 | Culture: Automated microbial detection system | Blood, Bone marrow, CSF, Respiratory Sample Sputum, BAL, mini BAL, Endotracheal aspirate), Swab, Pus, Drain fluid, Aspirates, catheter tip, Biopsy, Urine, Percutaneous nephrostomy, Sterile body fluids(Ascitic fluid, Pericardial fluid, Synovial fluid, CSF, Peritoneal fluid, Pleural fluid), Stool. |
| 4 | Antimicrobial susceptibility testing by automated system | Blood and bone marrow, Sputum/BAL/miniBAL/Endotracheal aspirate (Respiratory samples), Swab/Pus/ drain fluid/aspirate/catheter tip/biopsy/ urine/PCN/ CSF/Ascitic Fluid, Cerebrospinal Fluid, Pericardial Fluid, Pleural Fluid, Synovial Fluid, Peritoneal fluid /stool |
| 5 | Hanging drop for darting motility of Vibrio Cholerae | Stool |
| S. no | Test performed | Product/material of the test (Sample) |
|---|---|---|
| 1 | Latex agglutination of CSF for Antigen detection of S. pneumoniae, H. influenzae, N. meningitidis, E. coli, S. agalactiae | CSF |
| 2 | Multiplex PCR from CSF for detection of pathogen of Acute Bacterial Meningitis | CSF |
| S. no | Test performed | Product/material of the test (Sample) |
|---|---|---|
| 1 | Anti-Streptolycin O | Serum |
| 2 | Venereal disease research laboratory test (VDRL) | Serum |
| 3 | Human Treponema Pallidum Antibodies Test (TPHA) | Serum |
| 4 | WIDAL | Serum |
| 5 | Brucella Antibody Standard Agglutination Test (SAT) | Serum |
| 6 | Helicobacter pylori (H.pylori) IgG Antibody detection | Serum |
| 7 | Helicobacter pylori (H.pylori) Antigen detection | Stool |
| 8 | Serum Procalcitonin Concentration | Serum |
Hospital Infection Control Laboratory: This section is involved with the surveillance of health care associated infections in the Institute. The number of health care associated infections including BSI (CLABSI), UTI (CAUTI), SSI, VAP, Hand hygiene compliance is recorded and infection rates determined. Environmental sampling is done to monitor effective decontamination and disinfecting procedures carried out in the hospital.
Central Sterile Supply Department (CSSD) autoclaves are monitored by Biological indicators to check for the functioning of the autoclaves. The sterility of the fluids or pre-sterile articles purchased is tested on the request of the Medical Supply Stores. Monitoring of antimicrobial resistance is done by keeping a record of the resistance pattern of the bacteria causing infections in our hospital. The change in the infection rates and outbreaks are identified and the concerned unit informed in time to take timely control measures. Surveillance of the staff to detect any carrier state in outbreaks is undertaken.
This section also involves with carrying out teaching activities and sensitization of all new health care staff to hospital infection activities.
Anaerobic and Special Bacterial Pathogen Laboratories are catering to the diagnostic needs as the nodal centre for many teaching and non-teaching hospitals across the country. The laboratory offers NABL accredited investigations for a wide spectrum of rare and neglected bacterial pathogens (including anaerobes and rickettsia).
| S. no | Test performed | Product/material of the test (Sample) |
|---|---|---|
| 1 | Anaerobic culture | Aortic Valve, Ascitic fluid, Bile, Blood, Bone marrow, Broncho-alveolar lavage, CSF, Drain Fluid, Endometrial Culture, Mitral Valve, Ocular fluid, Pericardial fluid, Pleural fluid, Pulmonary Valve, Pus, Stool, Subgingival pocket plaque, Synovial fluid, Tissue Biopsy, Tricuspid Valve, Urine (Suprapubic aspirate) |
| 2 | Toxin detection for Clostridioides difficile toxin A & B by ELISA and PCR | Stool |
| 3 | Enterotoxigenic Bacteroides fragilis detection by culture and PCR | Stool |
| 4 | Enterotoxigenic Clostridium perfringens detection by culture and PCR | Stool |
| 5 | Leptospira spp detection by Dark Ground Microscopy | Blood and urine |
| 6 | Detection of IgM antibodies against Leptospira spp | Serum |
| 7 | Detection of Leptospira spp by culture & PCR | Blood and urine |
| 8 | Detection of IgM antibodies for Scrub Typhus infection | Serum |
| 9 | Detection of Scrub Typhus by PCR | Blood, tissue biopsy (eschar) |
| 10 | Detection of IgM antibodies for Rickettsial infection | Serum |
| 11 | Detection of Rickettsial infection by PCR | Blood |
| 12 | Detection of IgM antibodies for Mycoplasma pneumoniae infection | Serum |
| 13 | Detection of Mycoplasma pneumonia by culture and PCR | Broncho alveolar lavage, Endotracheal aspirate, Nasopharyngeal aspirate, Throat swab |
| 14 | Detection of IgM antibodies for Legionella pneumophila infection | Serum |
| 15 | Detection of Legionella pneumophila by PCR | Broncho alveolar lavage, Nasopharyngeal aspirate, Pleural fluid, Sputum, Throat swab, Urine |
| 16 | Detection of IgM antibodies for Chlamydia pneumoniae infection | Serum |
| 17 | Detection of Bartonella infection by culture | Blood, tissue biopsy |
| 18 | Detection of IgG and IgM antibodies for Bartonella infection by IFA | Serum |
| 19 | Detection of Bartonella infection by PCR | Blood, tissue biopsy |
| 20 | Detection of IgG and IgM antibodies for Lyme disease infection | Serum and CSF |
| 21 | Detection of Lyme Disease infection by PCR | Blood and CSF |
The laboratory is NABL accredited, fully equipped to offer complete diagnostic services for diagnosis of tuberculosis (TB), Non-tubercular Mycobacteria (NTM), and drug resistance to various anti-tubercular drugs by molecular as well as conventional methods. The laboratory offers microscopy, culture (both liquid and solid), PCR and Gene-Xpert for diagnosis of TB and NTM. In addition, the conventional drug sensitivity testing in liquid and solid culture media, Gene-Xpert, Line Probe Assay are available for detecting resistance to both first line and second line drugs. The laboratory is equipped with state of art molecular typing techniques for TB. All the techniques are quality assured.
The laboratory carries out research under several funded schemes (Extramural funding support for Whole Genome Sequencing, Early Bactericidal Activity, Therapeutic Drug Monitoring, Point of Care tests (Aptamer based), Novel biomarkers, Rapid molecular drug resistance detection, Molecular Epidemiology of MDR-TB).
| S. no | Test performed | Product/material of the test (Sample) |
|---|---|---|
| 1 | AFB Smear (Ziehl Neelsen Staining) | Pulmonary & Extrapulmonary samples |
| 2 | Fluorescent staining for M. tuberculosis | Pulmonary & Extrapulmonary samples |
| 3 | MGIT 960 Mycobacteria Liquid Cultures. | Pulmonary & Extrapulmonary samples |
| 4 | Lowenstein Jensen Solid Culture for Mycobacteria | Pulmonary & Extrapulmonary samples |
| 5 | Drug Susceptibility Test – MGIT 960 Liquid Culture DST first line and second line drugs | Pulmonary & Extrapulmonary samples |
| 6 | Drug Susceptibility Test – Lowenstein Jensen Solid first line and second line drugs | Pulmonary & Extrapulmonary samples |
| 7 | Drug Susceptibility Test for NTM | Pulmonary & Extrapulmonary samples |
| 8 | Gene Xpert MTB/Rif | Pulmonary & Extrapulmonary samples |
| 9 | Polymerase Chain Reaction targeting Mpt64 gene | Pulmonary & Extrapulmonary samples |
| 9 | TRUNAT-MTB-RIF detection | Pulmonary & Extrapulmonary samples |
| 10 | Line Probe Assay (Hain’s) | Pulmonary & Extrapulmonary samples |
[Note: Some tests are not performed routinely, but only after discussion with the treating physicians/faculty]
Section of Parasitology, Department of Microbiology, is the first dedicated laboratory that provides investigations for diseases caused by parasites. The laboratory has received NABL accreditation. Investigations are available for the diseases caused by various medically important protozoa, helminths and arthropod agents. Many of these diseases are of immense public health importance and include malaria, visceral leishmaniasis, lymphatic filariasis, and intestinal parasitic infections. Microscopic techniques such as direct microscopic examination of unstained preparations of clinical specimens, examination of stained smears and special investigations such as Quantitative Buffy Coat (QBC) assay and immunochromatography test (ICT) are routinely used for some of the diseases. Rapid diagnostic tests are used for diagnosis of different parasitic infections of public health importance and includes antigen detection for malaria (pLDH & HRP-II) and lymphatic filariasis, and antibody detection assays such as, rK 39 test for visceral leishmaniasis, Enzyme Linked Immuno-Sorbent Assay (ELISA) for toxoplasmosis, amoebic liver abscess, cystic hydatid disease, strongyloidiasis, toxocariasis, etc. are being carried out. The section also conducts molecular diagnostic investigations including Multiplex PCR assay for human malaria, and PCR assays for Pneumocystis jiroveci, Microsporidia & free living amoeba.
| S.no. | Test Name | Sample |
|---|---|---|
| 1 | BLOOD (CITRATE) FOR EXAMINATION FOR MICROFILARIA Acridine orange staining for microfilaria (microscopy) Giemsa staining for microfilaria (microscopy) Quantitative buffy coat assay (microscopy) Direct & Concentration mount for microfilaria (microscopy) Filarial Antigen detection test | BLOOD (CITRATE) |
| 2 | BLOOD (EDTA) FOR MALARIA WORKUP Acridine orange staining for Malaria parasite (microscopy) Giemsa staining for Malaria parasite (microscopy) Quantitative buffy coat assay for Malaria parasite (microscopy) Malaria parasite antigen detection test | BLOOD (EDTA) |
| 3 | MULTIPLEX PCR ASSAY FOR HUMAN MALARIA | BLOOD (EDTA) |
| 4 | BLOOD (EDTA) FOR MICROSCOPY FOR PARASITES (OTHER THAN MALARIA) | BLOOD (EDTA) |
| 5 | BONE MARROW FOR MICROSCOPIC EXAMINATION FOR LD BODIES (KALA AZAR) Acridine orange staining for LD bodies Giemsa staining for LD bodies | BONE MARROW (EDTA/SMEAR) |
| 6 | BONE MARROW FOR MICROSCOPY FOR PARASITES (OTHER THAN KALA AZAR) | BONE MARROW (EDTA/SMEAR) |
| 7 | BRONCHO-ALVEOLAR LAVAGE FOR MICROSCOPIC EXAMINATION FOR Pneumocystis jiroveci (PCP) | BRONCHO-ALVEOLAR LAVAGE FLUID |
| 8 | BRONCHO-ALVEOLAR LAVAGE - PCR FOR Pneumocystis jiroveci (PCP) | BRONCHO-ALVEOLAR LAVAGE FLUID |
| 9 | BRONCHO-ALVEOLAR LAVAGE FOR MICROSCOPY FOR PARASITES (OTHER THAN Pneumocystis jiroveci/PCP) | BRONCHO-ALVEOLAR LAVAGE FLUID |
| 10 | C.S.F FOR DIRECT MICROSCOPY FOR FREE LIVING AMOEBAE | C.S.F |
| 11 | C.S.F FOR MICROSCOPY FOR PARASITES (OTHER THAN FREE LIVING AMOEBAE) | C.S.F |
| 12 | DUODENAL ASPIRATE FOR MICROSCOPY FOR PARASITES | DUODENAL ASPIRATE |
| 13 | LIVER ABSCESS ASPIRATE FOR MICROSCOPY FOR AMOEBIASIS | LIVER ABSCESS ASPIRATE |
| 14 | LIVER ABSCESS ASPIRATE FOR MICROSCOPY FOR PARASITES (OTHER THAN AMOEBIC LIVER ABSCESS) | LIVER ABSCESS ASPIRATE |
| 15 | LYMPH NODE ASPIRATE FOR MICROSCOPIC EXAMINATION FOR LD BODIES Acridine orange staining for LD bodies Giemsa staining for LD bodies | LYMPH NODE ASPIRATE |
| 16 | LYMPH NODE ASPIRATE FOR MICROSCOPY FOR PARASITES (OTHER THAN LEISHMANIASIS) | LYMPH NODE ASPIRATE |
| 17 | PROSTATIC SECRETION FOR MICROSCOPY FOR Trichomonas vaginalis | PROSTATIC SECRETION |
| 18 | SERUM FOR ELISA FOR AMOEBIASIS | SERUM |
| 19 | SERUM FOR ELISA FOR CYSTIC ECHINOCOCCOSIS | SERUM |
| 20 | SERUM FOR ELISA FOR TOXOPLASMOSIS | SERUM |
| 21 | SERUM FOR ANTI-Strongyloides IgG ELISA | SERUM |
| 22 | SERUM FOR ANTI-Toxocara canis IgG ELISA | SERUM |
| 23 | SERUM FOR ANTI-Taenia solium IgG ELISA | SERUM |
| 24 | SERUM FOR rK 39 ANTIBODY DETECTION FOR LEISHMANIASIS | SERUM |
| 25 | SIGMOIDOSCOPY ASPIRATE FOR MICROSCOPY FOR PARASITES | SIGMOIDOSCOPY ASPIRATE |
| 26 | SPLENIC ASPIRATE FOR MICROSCOPY FOR LD BODIES (KALA AZAR) | SPLENIC ASPIRATE |
| 27 | SPUTUM FOR MICROSCOPY FOR PARASITES (OTHER THAN Pneumocystis jiroveci/PCP) | SPUTUM |
| 28 | STOOL EXAMINATION FOR PARASITES (TROPHOZOITES/CYSTS/OOCYSTS OF COCCIDIA/OVA/LARVAE) Stool direct/concentration mounts microscopy Modified acid-fast staining for coccidian parasites (Cryptosporidium spp./Cyclospora cayetanensis/Cystoisospora belli) | STOOL |
| 29 | URETHRAL DISCHARGE FOR MICROSCOPY FOR Trichomonas vaginalis | URETHRAL DISCHARGE |
| 30 | URINE FOR MICROSCOPY FOR PARASITES | URINE |
| 31 | IDENTIFICATION OF MEDICALLY IMPORTANT ARTHROPODS | ARTHROPOD SPECIMEN |
| 32 | IDENTIFICATION OF PARASITIC SEGMENTS/WORMS | SEGMENT/WORM SPECIMEN |
| 33 | SPUTUM FOR MICROSCOPIC EXAMINATION FOR Pneumocystis jiroveci (PCP) GMS staining for Pneumocystis jiroveci | SPUTUM |
| 34 | SPUTUM FOR PCR FOR Pneumocystis jiroveci (PCP) | SPUTUM |
| 35 | STOOL FOR in vitro CULTURE FOR HOOKWORM | STOOL |
| 36 | STOOL FOR MICROSCOPIC EXAMINATION FOR MICROSPORIDIA Calcofluor white staining for microsporidia Modified trichrome staining for microsporidia | STOOL |
served as Chairman/Member of various intra- as well as extra mural policy making and decision making committees of AIIMS as well as other organizations including Ministry of Health & Family Welfare, Central Pollution Control Board, Govt. of NCT of Delhi etc. Invited as Chief Guest/ Guest of honour/ Guest faculty etc. in various National and International symposia, workshops and conferences. Nominated as Chairman/Principal Member of various Committees of Bureau of Indian Standards (BIS), India on hospital planning, medical equipments, surgical instruments, disposables and dressings
The Department of Hospital Administration organised the following Conferences/ CMEs/Workshops/Training Programme:
The Department of Hospital Administration has been involved in conducting various public lectures relevant in our health set up. The following public lectures were organised :
Actively involved in teaching and training hospital administration residents and delivering lectures in various training programmes/workshops organized by the department sponsored by Ministry of Health, HRD, personnel etc. Also been invited by various govt. and public sector organizations and professional associations to deliver lectures on various topics in the specialty of Hospital Administration.
HTML
Attended National Conference on Govt. Procurement being organised by Indian Institute of Materials and Management at New Delhi
Programme co-ordinator, training programme on Hospital Management and Administration for Medical Superintendents, GDMOs & non specialists of Coal India at IICM and CME on Clinical issues during field visit to AIIMS in January, 2009.
Lathwal Amit, Sharma D.K., Madan Nirupam, Sharma N.K. – Management of Dengue Outbreak by AIIMS : A Case Study,Journal of the Indian Hospital Association, Vol. XXXXIV & XXXXV (1 to 4), no. 46-54.
Pathni RK, Satpathy S, Kailash S. Need for Tele follow-up : a study at a public sector Quaternary referral hospital in India (Manuscript ID:JTT-08-12-006.R1) accepted for publication in Journal of Tele medicine and Tele care (in press).
Dr. I.B. Singh, Mr.I.B. Singh, S. Laxmibai Devi, S.Denabai Devi – “Robotics for Human Welfare – Application in Health Care” – Journal of Hospital Administration – Official Journal of Indian Hospital Association, New Delhi, Volume XXXXIV & XXXXV – March, 2007 to Decmber, 2008, pg. 36-44.
served as Chairman/Member of various intra- as well as extra mural policy making and decision making committees of AIIMS as well as other organizations including Ministry of Health & Family Welfare, Central Pollution Control Board, Govt. of NCT of Delhi etc. Invited as Chief Guest/ Guest of honour/ Guest faculty etc. in various National and International symposia, workshops and conferences. Nominated as Chairman/Principal Member of various Committees of Bureau of Indian Standards (BIS), India on hospital planning, medical equipments, surgical instruments, disposables and dressings
The Department of Hospital Administration organised the following Conferences/ CMEs/Workshops/Training Programme:
following public lectures were organised :
The Department of Hospital Administration is running a 2 year postgraduate programme viz. MHA (Masters in Hospital Administration) which entered its 43rd year after inception. It was officially started in February, 1966, for the first time in India and has since been recognized as a distinct post-graduate discipline. The Residency Programme in Hospital Adminstration focuses on “hands on” training, where Resident Administrators man the “Control Room” of hospital, round the clock as “Duty Officers”, and coordinate all the hospital activities after duty hours.
The Department introduced a paradigm shift in the Academic programme by launching Integrated Learning Modules for the residents of Department of Hospital Administration from 1st January, 2008. This includes lectures, discussions, problem based learning, case studies, journal club etc. from 8.00 am to 9.00, 12.00 to 1.00 pm and and 4.00 – 5.00 pm everyday. Each faculty member is assigned “Moderator” for a specific period. Various guest lectures were organised in the Department so as to increase the horizon of teaching.
The Department of Hospital Administration became 1st department in AIIMS hospital to be ISO certified, receiving the prestigious ISO 9001:2000 certification in the month of October, 2008.
Faculty members conducted several training programmes for the doctors working in various organization including Central & State Governments, Paramilitary Forces and in various PSUs such as IICM, Ranchi & also private sector management institutes.
Masters of Hospital Administration – Two Years Programme
The department runs a two year post graduate course in Hospital Administration leading to award of degree of Masters in Hospital Administration (MHA) for both sponsored and open candidates. Resident Administrators man the Control Room round the clock as Duty Officers, and coordinate various hospital activities. They also assist the faculty in hands-on management of various hospital activities and in turn gain valuable experience of hospital management. Ph.D. program in hospital administration is also conducted. Our alumni hold top administrative positions in various organizations of national and international importance. Many of them are also serving as independent consultants in Hospital Administration in the corporate sector.
Admission to the MHA program is through a competitive exam conducted twice a year. An advertisement is placed in national dailies in the month of August and January for sessions beginning December and July respectively. For details of admission procedure, form etc please visit www.aiims.edu.
Long & Short Term Trainings
Various long and short term trainings are provided under following categories:
Details of the training, fee, schedule etc can be obtained from the academic section of the institute or from the institute website www.aiims.edu.
Training to students from different institutes has also been carried out throughout the year 2008-2009
Publications are given in the respective personal profile of the faculty
| S. No. | Title of the project | Name of Principal Investigator | Funded by (Name of funding agency) | Duration (years) | Start year–End year | Total funds sanctioned (Rs) |
|---|---|---|---|---|---|---|
| 1 | Evaluation of the role of vitamin D receptors (VDR) polymorphisms on the efficacy of calcitriol therapy in stage 3-5 chronic kidney disease (CKD): A prospective double-blind study | Dr. Sudip Kr. Datta | ICMR | 3Yrs | 2021-2024 | Rs. 53,97,494/- (Fifty three lakhs ninety seven thousand four hundred and ninety four rupees only) |
| 2 | Long Term Effects of COVID-19 on endocrine system, semen quality and sperm proteome | Dr. Sudip Kr. Datta | AIIMS – IMRG Collaborative Research Project | 3Yrs | 2021-2023 | Rs. 20,00,000/- (Twenty lakhs only) |
| 3 | Development of Opto-electronic sensor for point-of-care diagnostics of micro-albumin in urine sample | Dr. Sudip Kr. Datta | AIIMS – IIT Delhi Collaborative Research Project | 2Yrs (Extended for 6 months) | 2019-2022 | Rs. 20,00,000/- (Twenty lakhs only) overall |
| 4 | Characterization and expression of transfer RNA derived small RNAs as a circulating biomarker for disease diagnosis and prognosis in NAFLD | Dr. Shyam Prakash | ICMR | 3 Years | 2022-2025 | Rs. 55.5 Lakh |
| 5 | Molecular interaction of iron trafficking gene variants with mitochondrial dysfunction in metabolically associated fatty liver disease | Dr. Shyam Prakash | ICMR | 3 Years | 2022-2025 | Rs. 52.5 Lakhs |
| 6 | Molecular coordination of T-regulatory cells and Prokineticins in obesity and their clinical correlation in obesity associated inflammation in non alcoholic fatty liver disease and metabolic syndrome | Dr. Shyam Prakash | ICMR | 2 years | 2021-2023 | Rs. 52.5 Lakh |
| 7 | An expensive and rapid diagnostic method for detection of SARS COV-2 and COVID-19 RNA by loop mediated isothermal amplification (LAMP) | Dr. Shyam Prakash | Intramural AIIMS | 2 years | 2020-2022 | Rs. 10 Lakh |
| 8 | Rapid diagnostic evaluation of Micro PCR for Hepatitis B virus DNA quantitation | Dr. Shyam Prakash | BigTech Bangalore | 5 Years | 2017-2022 | Rs. 40.0 Lakh |
| 9 | Development and validation of Standalone meter for non invasive salivary glucose quantification | Dr. Shyam Prakash | BIRAC (DST) | 2 years | 2021-2022 | Rs. 10.0 Lakh |
| 10 | Saliva as an alternate specimen source for SARs-COV-2 in symptomatic patients using Cepheid Xpert Xpress SARS-COV-2 in an outpatient setting | Dr. Suneeta Meena | AIIMS, DELHI | 1.5 years | 2020-2022 | Rs. 8,80,000 |
| 11 | Triacetylfusarinine C (TAFC) as a potential biomarker for early diagnosis of invasive aspergillosisin patients with haematological malignancy | Dr. Suneeta Meena | AIIMS, DELHI | 2 years | 2021-2023 | Rs. 4.40,000 |
| 12 | Evaluation of Artificial neural network for differentiating Iron deficiency anemia and β-Thalassemia trait in comparison to the conventional methods | Dr. Tushar Sehgal | ICMR, INDIA | 2 years | 2022-2023 | Rs. 22,87,766 |
| 13 | Evaluation of Extended inflammatory parameters of activated neutrophils (NEUT-RI, NEUT-GI), immature granulocytes (IG), reactive lymphocytes (RE-LYMP) and T cell-independent plasma cells (AS-LYMP) in Pyrexia of unknown origin and its correlation with functional imaging and conventional inflammatory parameters | Dr. Tushar Sehgal | SYSMEX, INDIA | 1 year | 2022-2023 | Rs. 13,36,500 |
Hospital Services: The reports of investigations done in the Department are available on eHospital portal and also through the website: www.ors.gov.in
Faculty In-charge: Dr. Shyam Prakash
STOs: Mr. Shaukat Ali, Mr. Rajeev Sharma, Ms. Reena Lazarus
Location: Room No. 27, Ground floor, in the foyer of the Old Rajkumari Amrit Kaur OPD block of AIIMS & New RAK OPD
Extension Numbers: 4278, 2857
Collection of blood from outpatients having valid AIIMS UHID & OPD card test prescription
| Timings of Blood Collection Centre (Central Collection facility)Lab No. 27 & 28 | |||
|---|---|---|---|
| Old RAK OPD | Monday to Friday | 8.00 am to 6.30 pm | Collection of fasting samples 8.00 am to 11.30 am |
| Old RAK OPD | Saturday | 8.00 am to 3.30 pm | Collection of fasting samples 8.00 am to 11.30 am |
| New RAK OPD | Monday to Friday | 8.00 am to 6.30 pm | Collection of fasting samples 8.00 am to 11.30 am |
| New RAK OPD | Saturday | 8.00 am to 3.30 pm | Collection of fasting samples 8.00 am to 11.30 am |
Spot investigations for outpatients: BT, CT test
Workload: Available at AIIMS website (https://www.aiims.edu/en/about-us/annual-reports.html)
Faculty In-charge: Dr. Tushar Sehgal
STOs: Mr. Kuldeep Singh, Mr. Subodh Jha
Location: Room No. 22 & 23, 2nd floor, Dept. of Lab Medicine
Extension Numbers: 6429
Investigations done
| Hematology (EMERGENCY AND WARD 24X7) | ||||
| Bar code series | Test Profile | Investigations | Cost | Sample collection tube |
| HMW | Complete blood count with differential cell count | Free | Violet capped (EDTA Blood) | |
| - | Hb% | |||
| - | Hematocrit | |||
| - | RBC count | |||
| - | WBC count | |||
| - | Platelet count | |||
| - | MPV | |||
| - | MCV | |||
| - | MCH | |||
| - | MCHC | |||
| - | RDW | |||
| - | RDW-CV | |||
| - | Neutro% | |||
| - | Lympho% | |||
| - | Eosino% | |||
| - | Mono% | |||
| - | Baso% | |||
| - | Neutro - Abs | |||
| - | Lympho- Abs | |||
| - | Eosino - Abs | |||
| - | Mono - Abs | |||
| - | Baso - Abs | |||
| Peripheral blood film | - | Free | ||
| PS for Hemoparasites | PS for Hemoparasites | |||
| PS for Schistocytes/hemolysis | PS for Schistocytes/hemolysis | |||
| PS for Atypical cells | PS for Atypical cells | |||
Reticulocyte count
| - | Free | ||
Manual platelet count
| - | Free | ||
| HMW-E | ESR
| - | Free | |
| Body fluid analysis for cell counts (EMERGENCY AND WARD 24X7) | ||||
| HFL | CSF Peritoneal Fluid Pleural Fluid Synovial Fluid | TLC count DLC count Atypical cell, if any | Free | Penicillin sample collection vial / sterile screw capped container |
| Coagulation (EMERGENCY AND WARD 24X7) | ||||
| HPT | PT/INR | - | Free | Blue capped (Citrate Blood) |
| APTT | - | |||
| Fibrinogen | - | |||
| D-dimer | - | |||
| Disseminated intravascular profile (DIC Profile) | PT, APTT, INR, D Dimer, Fibrinogen | |||
| Platelet function analysis(with appointment) | Platelet function tests | |||
Reports are uploaded on E-Hospital the same day
Workload: Available at AIIMS website (https://www.aiims.edu/en/about-us/annual-reports.html)
Faculty In-charge: Dr. Shyam Prakash
STOs: Mr. A. Karmakar, Mr. Sudhanshu S. Prasad
Location: Room No. 20 & 21, 2nd floor, Dept. of Lab Medicine
Extension Numbers: 4279, 4469
Investigations done
Clinical Biochemistry(EMERGENCY AND WARD 24X7) 2nd Floor, Main Department | ||||
| Bar code series | Test Profile | Investigations | Cost | Sample Collection tube |
| WC | - | - | Free | Yellow capped (Serum) |
| LFT | Bilirubin (Total) | |||
| - | Bilirubin (Direct) | |||
| - | Bilirubin (Indirect) | |||
| - | ALT | |||
| - | AST | |||
| - | ALP | |||
| - | Total protein | |||
| - | Albumin | |||
| - | Globulin (calculated) | |||
| - | A/G ratio (calculated) | |||
| RFT | Urea | |||
| - | Creatinine | |||
| - | Uric Acid | |||
| - | Calcium | |||
| - | Phosphorus | |||
| - | Sodium | |||
| - | Potassium | |||
| - | Chloride | |||
| Lipid Profile | Total Cholesterol | |||
| - | Triglycerides | |||
| - | VLDL - C (calculated) | |||
| - | LDL-C | |||
| - | dLDL | |||
| - | HDL | |||
| - | CHOL/HDL ratio | |||
| - | LDL/HDL ratio | |||
| Thyroid Profile | TSH | |||
| - | T3 | |||
| - | T4 | |||
| - | FT3 | |||
| - | FT4 | |||
| Total Amylase | - | |||
| Lipase | - | |||
| Cortisol | - | |||
| Vitamin D3 Total | - | |||
| Intact PTH | - | |||
| CK | - | |||
| CK-MB (activity) | - | |||
| LDH | - | |||
| AFP | - | |||
| Total PSA | - | |||
| ADA | - | |||
| βHCG | - | |||
| Serum Chromogranin A | - | |||
| Ionized Calcium | - | |||
| CEA | - | |||
| CA 19.9 | - | |||
| CA 125 | - | |||
| EMB | Arterial blood gas (ABG) (Room No. 2) | PH | Free | Heparinized Syringe |
| PO2 | ||||
| PCO2 | ||||
| HCO3 A | ||||
| HCO3 S | ||||
| BB | ||||
| BE | ||||
| BE ECF | ||||
| TCO2 | ||||
| O2 CT | ||||
| O2 SAT | ||||
| AADO2 | ||||
| WG-F | Plasma Glucose-F | - | Grey Capped (Fluoride Blood) | |
| WG- P | Plasma Glucose-PP | - | ||
| WG- R | Plasma Glucose-R | - | ||
| WG-0 | OGTT-Fasting | - | ||
| WG-1 | OGTT-1hr | - | ||
| WG-2 | OGTT-2hr | - | ||
| WGH | HbA1c (HPLC) | - | Free | Violet capped (EDTA Blood) |
WFU | U ACR | - |
Free |
Urine (Spot) |
| U Albumin | - | |||
| U Creatinine | - | |||
| U Protein | - | |||
| U Urea | - | |||
| U Calcium | - | |||
| U Phosphate | - | |||
| U Uric Acid | - | |||
| U Sodium | - | |||
| U Potassium | - | |||
| U Chloride | - | |||
| U Lipase | - | |||
| U Amylase | - | |||
| WFD | U 24 Albumin | - | Free | Urine (24 hour) |
| U 24 Protein | - | |||
| U 24 Creatinine | - | |||
| U 24 Uric Acid | - | |||
| U 24 Calcium | - | |||
| U 24 Urea | - | |||
| U 24 Phosphate | - | |||
| U 24 Sodium | - | |||
| U 24 Potassium | - | |||
| U 24 Chloride | - | |||
| WFC | CSF Protein | - | Free | Cerebrospinal fluid |
| CSF Glucose | - | |||
| CSF LDH | - | |||
| CSF Sodium | - | |||
| CSF Potassium | - | |||
| CSF Chloride | - | |||
| WFP | Pleural fluid Glucose | - | Free | Pleural fluid |
| Pleural fluid Protein | - | |||
| Pleural fluid Albumin | - | |||
| Pleural fluid ADA | - | |||
| Pleural fluid Amylase | - | |||
| Pleural fluid Lipase | - | |||
| WFA | Ascitic fluid Glucose | - | Free | Ascitic fluid |
| Ascitic fluid Protein | - | |||
| Ascitic fluid Albumin | - | |||
| Ascitic fluid Amylase | - | |||
| Ascitic fluid Lipase | - | |||
| WFH | Pericardial fluid Glucose | - | Free | Pericardial fluid |
| Pericardial fluid Protein | - | |||
| Pericardial fluid Albumin | - | |||
| Pericardial fluid Amylase | - | |||
| WFS | Synovial fluid Glucose | - | Free | Synovial fluid |
| Synovial fluid Protein | - | |||
| WFE | Drainage Fluid Triglyceride | - | Free | Drainage Fluid |
| Drainage Fluid Amylase | - | |||
| Drainage Fluid Lipase | - | |||
| - | - | |||
Reports are uploaded on E-Hospital the same day
Workload: Available at AIIMS website (https://www.aiims.edu/en/about-us/annual-reports.html)
Faculty In-charge: Dr. Sudip Kr. Datta
STOs: Mr. Ramji Rai, Ms. Anjoo Kher
Location: Basement, New RAK Building
Extension Numbers: 2526, 011-29576516 (sample receiving)
Investigations done:
| SMART LAB (24x7) | ||||
| Bar code series | Test Profile | Investigations | Cost | Sample collection tube |
| LC | LFT | - | Free | Yellow capped (Serum)
|
| - | Bilirubin (Total) | |||
| - | Bilirubin (Direct) | |||
| - | Bilirubin (Indirect) | |||
| - | ALT | |||
| - | AST | |||
| - | ALP | |||
| GGT | GGT | Free | ||
| Serum Proteins | - | Free
| ||
| - | Total protein | |||
| - | Albumin | |||
| - | Globulin (calculated) | |||
| - | A/G ratio (calculated) | |||
| Total Amylase | Total Amylase | Free | ||
| Lipase | Lipase | Free | ||
| Lipid Profile | - | Free | ||
| - | Total Cholesterol | Free | ||
| - | Triglycerides | Free | ||
| - | VLDL - C (calculated) | |||
| - | LDL-C (calculated) | |||
| - | HDL -C | |||
| - | CHOL/HDL ratio | |||
| - | LDL/HDL ratio | |||
| RFT | - | Free
| ||
| - | Urea | |||
| - | Creatinine | |||
| - | Uric Acid | |||
| - | Calcium | |||
| - | Phosphorus | |||
| - | Sodium | |||
| - | Potassium | |||
| - | Chloride | |||
| Magnesium | Magnesium | Free | ||
| Thyroid Profile | - | Free | ||
| - | TSH (ultrasensitive) | |||
| - | T3 | |||
| - | T4 | |||
| FT3 | FT3 | Free | ||
| FT4 | FT4 | Free | ||
| FSH | FSH | Free | ||
| LH | LH | Free | ||
| Prolactin | Prolactin | Free | ||
| Testosterone | Testosterone | Free | ||
| Cortisol | Cortisol | Free | ||
| Estradiol | Estradiol | Free | ||
| Progesterone | Progesterone | Free | ||
| Insulin | Insulin | Free | ||
| Vitamin D3 Total | Vitamin D3 Total | Free | ||
| Intact PTH | Intact PTH | Free | ||
| Iron | Iron | Free | ||
| Transferrin | Transferrin | Free | ||
| Ferritin | Ferritin | Free | ||
| TIBC | TIBC | Free | ||
| Vitamin B12 | Vitamin B12 | Free | ||
| Serum Folate | Serum Folate | Free | ||
| CK | CK | Free | ||
| CK-MB (mass) | CK-MB (mass) | Free | ||
| Troponin T - hs | Troponin T - hs | Free | ||
| Myoglobin | Myoglobin | Free | ||
| Homocysteine | Homocysteine | 500 | ||
| LDH | LDH | Free | ||
| AFP | AFP | Free | ||
| Total PSA | Total PSA | Free | ||
| Free PSA | Free PSA | Free | ||
| Beta HCG | Beta HCG | Free | ||
| CRP | CRP | Free | ||
| hs CRP | hs CRP | Free | ||
| ASO | ASO | Free | ||
| RA Factor | RA Factor | Free | ||
| Complement C3 | Complement C3 | Free | ||
| Complement C4 | Complement C4 | Free | ||
| IgG | IgG | Free | ||
| IgA | IgA | Free | ||
| IgM | IgM | Free | ||
| Carbamazepine | Carbamazepine | Free | ||
| Valproic acid | Valproic acid | Free | ||
| HIV Combo (HIV 1& HIV 2) | HIV Combo (HIV 1& HIV 2) | Free
| ||
| Anti HAV IgM | Anti HAV IgM | |||
| HBs Ag | HBs Ag | |||
| Anti HBs | Anti HBs | |||
| IgM Anti HBc | IgM Anti HBc | |||
| Anti HCV Ab | Anti HCV Ab | |||
| LG-F | Plasma Glucose-F | Plasma Glucose-F | Free
| Grey Capped (Fluoride Blood) |
| LG-P | Plasma Glucose-PP | Plasma Glucose-PP | ||
| LG-R | Plasma Glucose-R | Plasma Glucose-R | ||
| LG-F | OGTT-Fasting | OGTT-Fasting | ||
| LG-1 | OGTT-1hr | OGTT-1hr | ||
| LG-2 | OGTT-2hr | OGTT-2hr | ||
| LGH | HbA1c | HbA1c | Free | Violet capped (EDTA Blood)
|
| LH | CBC | - | Free
| Violet capped (EDTA Blood)
|
| - | Hb% | |||
| - | Hematocrit | |||
| - | RBC count | |||
| - | WBC count | |||
| - | Platelet count | |||
| - | MPV | |||
| - | MCV | |||
| - | MCH | |||
| - | MCHC | |||
| - | RDW | |||
| - | RDW-CV | |||
| - | Neutro% | |||
| - | Lympho% | |||
| - | Eosino% | |||
| - | Mono% | |||
| - | Baso% | |||
| - | Neutro - Abs | |||
| - | Lympho- Abs | |||
| - | Eosino - Abs | |||
| - | Mono - Abs | |||
| - | Baso - Abs | |||
| LH | PS for Hemoparasites | PS for Hemoparasites | Free
| |
| PS for Schistocytes | PS for Schistocytes | |||
| PS for Atypical cells | PS for Atypical cells | |||
Reticulocyte count
| Reticulocyte count - Abs | Free Free | ||
| - | Corrected Reticulocyte % | |||
| LE | ESR | ESR | Free | |
| LB | PT-INR | - | Free | Blue capped (Citrate Blood) |
| - | PT | -- | ||
| - | INR | -- | ||
| APTT | APTT | Free | ||
| TT | TT | Free | ||
| D Dimer | D Dimer | Free | ||
| Fibrinogen | Fibrinogen | Free | ||
| Protein C | Protein C | Free | ||
| Anti-thrombin | Anti-thrombin | Free | ||
Lupus anticoagulant
| Lupus anticoagulant screen | Free | ||
| - | Lupus anticoagulant confirm | -- | ||
| CHF | CSF Peritoneal Fluid Pleural Fluid Synovial Fluid | Total protein Albumin Sugar Amylase On request, Triglycerides and Bilirubin | Free
| Penicillin sample collection vial / Sterile container
|
| LUS | Spot Urine | Protein Albumin Phosphorous Uric acid Na+/K+ | Free
| Wide mouthed clean container |
| LUD | 24 hours Urine | Protein Albumin Phosphorous Uric acid Na+/K+ | Free
| Wide mouthed clean container |
Reports are uploaded on E-Hospital the same day
Workload: Available at AIIMS website (https://www.aiims.edu/en/about-us/annual-reports.html)
Faculty In-charge: Dr. Suneeta Meena
STOs: Mr. Rajendra Kumar
Location: Room No. 28, Ground floor, Dept. of Lab Medicine
Extension Numbers: 4397, 3546
Investigations done:
Clinical Microbiology: collection timing 8:00 am to 6:30 pm (Monday to Friday) and 8:00am to 3:30pm (Saturday) | ||||
| Bar code series | Test Profile | Investigations | Cost | Sample collection tube |
URM- Old RAK OPD, URN- New RAK OPD CUR- Ward | Urine: Routine/ Microscopy | pH | Free | Wide mouthed clean container |
| - | Specific gravity | |||
| - | Protein | |||
| - | Sugar | |||
| - | Acetone | |||
| - | Bile salts | |||
| - | Bile pigments | |||
| - | Urobilinogen | |||
| - | RBC | |||
| - | WBC | |||
| - | Epithelial Cells | |||
| - | CASTS | |||
| - | Crystals | |||
| - | Bacteria | |||
| - | Yeast | |||
| Bence Jones Protein | Bence Jones Protein | |||
| Myoglobinuria | Myoglobinuria | |||
| Urine for fat globules | Fat globules | |||
| CUC | Urine Culture and sensitivity testing | Urine Culture and sensitivity testing | Free | Wide mouthed sterile screw capped container |
| CST | Stool : Routine/ Microscopy | Routine/ Microscopy | Free | Wide mouthed clean container |
| - | Ova/ Cyst Ova/ Cyst | |||
| - | RBC | |||
| - | WBC | |||
| - | Yeast | |||
| Occult blood in stool | Occult blood in stool | |||
| Fat globules | Fat globules | |||
| CSP | Special stains for stool: Z-N stain, Modified | Special stains for stool: Z-N stain, Modified | Free | Sterile screw capped container |
| CSE | Semen analysis | Free | Sterile screw capped container | |
| - | Reaction/pH | |||
| - | Liquefaction | |||
| - | Viscosity | |||
| - | Motility | |||
| - | Count | |||
| - | Fructose | |||
| - | Bacteria/ yeast/ others | |||
| CSP | Sputum for AFB (ZN stain) | Sputum for AFB (ZN stain) | Free | Sterile screw capped container |
| Sputum MTB Culture | Sputum MTB Culture | |||
| CUA | Urine for AFB (ZN stain) | Urine for AFB (ZN stain) | Free | |
| Urine MTB Culture | Urine MTB Culture | |||
| GeneXpert MTB/RIF | GeneXpert MTB/RIF Urine MTB Culture AFB (ZN stain)
| Free | Penicillin sample collection vial/ Sterile screw capped container :BAL, Pleural fluid, Ascitic fluid, CSF, tissue sample and other fluids | |
| rK 39 (Leishmania) | rK 39 | Free | Yellow capped (Serum)
| |
| CTP | TORCH Profile | Free | Yellow capped (Serum)
| |
| Toxoplasma gondii IgG | Toxoplasma gondii IgG | |||
| Toxoplasma gondii IgM | Toxoplasma gondii IgM | |||
| Rubella IgG | Rubella IgG | |||
| Rubella IgM | Rubella IgM | |||
| Cytomegalo virus IgG | Cytomegalo virus IgG | |||
| Cytomegalo virus IgM | Cytomegalo virus IgM | |||
| Cytomegalo virus IgG Avidity | Cytomegalo virus IgG Avidity | |||
| Herpes Simplex virus IgG | Herpes Simplex virus IgG | |||
| Herpes Simplex virus 2 IgG | Herpes Simplex virus 2 IgG | |||
| Herpes Simplex virus (1+2) IgM | Herpes Simplex virus (1+2) IgM | |||
| Measeles IgG | ||||
| Mumps IgG | ||||
| Varicella IgG | ||||
| Varicella IgM | ||||
| CVM | Viral markers | Free | Yellow capped (Serum)
| |
| HAV IgM | HAV IgM | |||
| HBsAg | HBsAg | |||
| HBc IgM | HBc IgM | |||
| HBeAg | HBeAg | |||
| Anti HBe | Anti HBe | |||
| Anti HBs | Anti HBs | |||
| Anti HCV antibody | Anti HCV antibody | |||
| HEV IgM | HEV IgM | |||
| HIV- 1& 2 | HIV | |||
CPC
| HBV DNA | HBV DNA | Free | Violet capped (EDTA Blood)
|
| HCV RNA | HCV RNA | |||
| CMV PCR | CMV PCR | |||
| SARS CoV-2 Antibody (Quantitative) | SARS CoV-2 Antibody (Quantitative) | Free | Yellow capped (Serum)
| |
| S.No. | Name of the Training | Details of Admission |
|---|---|---|
| 1 | Short term training for outsiders in various aspects of Laboratory Medicine | Placement: As per rules of AIIMS Requires:
Duration: 4 weeks, 3 months, 6 months, 1year Sponsorship: Indian and Foreign Universities ,Dept. of Biotechnology , Govt. of India ,W.H.O Qualification:
Number: As per AIIMS rule. |
| S.No. | Name of the Course | Details of Admission |
|---|---|---|
| 1 | MD | Candidate has to qualify in the postgraduate entrance examination held by AIIMS Examination Cell twice a year. Total Number of approved seats: 11 + 3 (sponsored) |
| 2 | Ph.D | Candidate has to qualify in the Theory of Ph.D Entrance Examination held every 6 months by the Examination section of AIIMS and then qualify in viva-voice examination held by the Department. Candidate is advised to consult the concerned faculty before applying for Ph.D from this department. Candidates who have their own fellowship are given preference. Time period: 3-5 years Number: As per AIIMS rules |
| 3 | - | Department facilitates hands-on lab training of PG Residents from Dept. of Pathology, Biochemistry and Transfusion Medicine |
The Department organized an awareness programme on the occasion of World Sleep Day on 14th March 2014. The topic of discussion was “Role of sleep in health and disease”. The talk was organized at the seminar room of the Department of Medicine and was well attended with undergraduate students, nursing staff and postgraduate students of various disciplines among the audience. Various issues including need for sleep, normal duration of sleep, sleep debt, sleep hygiene, insomnia, jet lag, obstructive sleep apnea, restless leg syndrome, etc were highlighted. The presentation was followed by an interactive session and a quiz.
Publications are available on their respective profile
Dr. S. K. Sharma
Indian Council of Medical Research
Medical Council of India
Ranbaxy Research Award
Research Grants from Department of Biotechnology, Ministry of Science & Technology, Government of India
| S.No | Name of the Project |
|---|---|
| 1 | Principal Investigator & National Coordinator Efficacy and safety of immunomodulator (Mycobacterium w) as an adjuvant therapy in Category II pulmonary tuberculosis patients along with immunological investigations (A multicenter study with a total cost of Rs. 526.54/- Lakhs) Project registered with National Institute of Health (NCT00265226) |
| 2 | Principal Investigator & Coordinator Efficacy and safety of immunomodulator Mw as an adjunct therapy in Category I Pulmonary Tuberculosis along with assessment of immunological parameters (Double-blind, Randomized, Placebo-Controlled, Clinical Trial) Project registered with National Institute of Health (NCT00341328) |
| 3 | Principal Investigator Efficacy of oral zinc administration as an adjunct therapy in Category I Pulmonary Tuberculosis along with assessment of immunological parameters (Double-blind, Randomized, Placebo-Controlled, Multicenter Clinical Trial) Project registered with National Institute of Health (NCT00698386) |
| 4 | Principal Investigator Role of oral vitamin D as an adjunct therapy in Category I Pulmonary Tuberculosis along with assessment of immunological parameters (Double-blind, Randomized, Placebo-Controlled, Clinical Trial) Project registered with National Institute of Health (NCT00507000) |
| 5 | Principal Investigator Impact of HIV infection on latent TB among patients with HIV-TB co-infection (The site has been designated as National Facility) |
Dr. Sanjeev Sinha
Department of Medicine, All India Institute of Medical Sciences, New Delhi-110029
Phone: 91-11-26594440 (Off), 91-11-26181858 (Resi.)
Cell: 9868397242
Fax: 91-11-26588866
E-mail: drsanjeevsinha2002@yahoo.com
Residence address : E-26, Ansari Nagar (west), AIIMS campus, New Delhi-110029
Membership of Editorial boards of indexed international journals/Review committees of National bodies and Institutions:
Member of Editorial board of “Cases Journal”.
Dr. Anant Mohan
| Name of Faculty | Designation | Contact No. | |
|---|---|---|---|
| Dr Anant Mohan | Associate Professor | 26593006 | anant_mohan@rediff.com |
Dr. Anant Mohan, MD, MAMS
Current position: Associate Professor of Medicine
Office: room No. 3098, Third Floor, teaching Block
Honours /Distinctions:
Awarded UK Commonwealth Fellowship 2008-2009 in Chest Medicine at the Royal Preston Hospital Lancashire Teaching Hospitals NHS Trust, UK
Academic achievements:
Current research interests:
Chief Investigator and Co-Investigator of many funded projects.
Pulmonary and Critical Care Medicine (especially Lung Cancer, Chronic Obstructive Pulmonary Disease) and Interventional Pulmonology
Medicine Outpatient: Tuesday and Friday , 9:00 AM till 1:00 PM, Room No. 33, Medical OPD
Chest Clinic: Every Friday afternoon from 2 PM to 5 PM; Room No. 27
| Project Title | Funding Agency | Budget (Rs) | Duration & Status |
|---|---|---|---|
| Effect of feeding pectin on antioxidant status in patients with type 2 diabetes. | AIIMS | 1.65 lakhs | 2005-2007 (Completed) |
| Study of the prevalence of respiratory virus infections in hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease and their impact on morbidity and mortality. | Indian Council for Medical Research | 14.0 lakhs | 2007-2010 |
| Prognostic utility of various acute phase reactants in acute exacerbation of chronic obstructive pulmonary disease | AIIMS | 2.0 lakhs | 2007-09 (ongoing) |
| Mitochondrial DNA Mutations in Lung Cancer | Department of Biotechnology | 19.2 lakhs | 2008-2011 (ongoing) |
| Study of the variability in systemic inflammation in patients with chronic obstructive pulmonary disease due to smoking and non-smoking related causes. | ICMR, New Delhi | 28.0 lakhs | 2009-2012 (ongoing) |
| S.No | Project Title | Funding Agency | Budget (Rs) | Duration & Status |
|---|---|---|---|---|
| 1 | Assessment of nutritional and antioxidant enzyme status in mechanically ventilated critically ill patients. Effect on mortality and strategies to improve nutritional support. | Department of Science and Technology | 22.0 lakhs | 2006-2009 (Ongoing) |
| 2 | Serum leptin, nutritional status, and inflammatory markers in chronic obstructive pulmonary disease: Relationship with dyspnea and disease severity | ICMR, New Delhi | 21.01 lakhs | 2007-2010 (Ongoing) |
| 3 | A randomized, double-blind, placebo controlled, exploratory study to assess the safety and efficacy of multiple doses of ACZ885 in COPD | Novartis | 12.4 lakhs | Nov. 2008-Nov 2009 (Ongoing) |
| 4 | An Interventional Nutritional Study in subjects with newly diagnosed active tuberculosis | Glaxo SmithKline | 12.83 lakhs | 21.01.2008-20.07.2009 (Completed) |
| 5 | Genetic Metabolic and Hormonal Profile in Obstructive Sleep Apnea Syndrome | Department of Science and Technology | 24.0 lakhs | 1.4.2008-31.03.2011 |
| 6 | To evaluate the efficacy and safety of fixed dose combination of formoterol and fluticasone dry powder inhaler in partly controlled asthma | Ranbaxy | 1.5 lakhs | 1.11.2008-Till Date (Ongoing) |
I am particularly interested in the diagnostics of lung cancer, especially to explore the possibility of developing reliable screening tools and early diagnostic markers. I am also working on quality of life measures of lung cancer and COPD. I have been independently performing fiberoptic bronchoscopies since almost four years, and have done more than 300 procedures till date. I also perform transbronchial needle aspirations for diagnostic purposes. In addition, I routinely perform other pulmonary diagnostic procedures such as ultrasound guided needle aspirations and trucut biopsies of lung masses, as well as pleural biopsies. I propose to gain expertise in and initiate techniques of interventional bronchology in my Institution.
| Laboratory Facility | Location |
|---|---|
| ADA & ACE laboratory | Room 19, Cross Wing, Third floor, Department of Medicine, Teaching Block |
| Biochemistry Laboratory | Room 19, Cross Wing, Third floor, Department of Medicine, Teaching Block |
| Bronchoscopy Laboratory (Video-fiberoptic bronchoscopy) | Room No 16, D-II Ward, Second Floor |
| BSL 3 Facility | Room Nos 3,4,5 Cross Wing, Third floor, Department of Medicine, Teaching Block |
| Cold Room | Room 23, Cross Wing, Third floor, Department of Medicine, Teaching Block |
| Mtb Culture & DST Lab (solid and culture) | Room 15, Cross Wing, Third floor, Department of Medicine, Teaching Block |
| DNA sequencing | Room 19, Cross Wing, Third floor, Department of Medicine, Teaching Block |
| 2D Gel Electrophoresis | Room 37, Cross Wing, Third floor, Department of Medicine, Teaching Block |
| Flow Cytometer Facility | Room 21, Cross Wing, Third floor, Department of Medicine, Teaching Block |
| GeneXpert Lab | Room Nos 3,4,5 Cross Wing, Third floor, Department of Medicine, Teaching Block |
| Immunology Laboratory | Room No 4076 and Room No 4093, Fourth Floor, Teaching Block |
| Line Probe Assay Lab | Room 12, Cross Wing, Third floor, Department of Medicine, Teaching Block |
| Microscopy Room, LED, Fluorescence | Room 36, Cross Wing, Third floor, Department of Medicine, Teaching Block |
| Polysomnography Laboratory (Sleep Laboratory), Actigraphy | Room No 1, C-II ward, Second floor |
| Respiratory laboratory [Cardio-Pulmonary Exercise Testing (CPET)] | Room No 30, Medical OPD |
| Sleep Laboratory with Continuous Ambulatory BP Monitoring Facility | Room No 14, CII Ward, Second Floor |
| Ziehl Neelsen (ZN) microscopy facility | Room 36, Cross Wing, Third floor, Department of Medicine, Teaching Block |
*Department of Medicine has Intermediate Reference Laboratory (IRL) of RNTCP for Delhi State
| I | 8-bedded ICU |
| II | Actigraphy device |
| III | Advanced critical care beds with facilities of prevention of pulmonary complications like VAP |
| IV | Airway scope |
| V | Ambulatory Pressure cum Polysomnography studies |
| VI | Arterial blood gas analyzers |
| VII | Bedside ECHO facility |
| VIII | Blood Pressure Monitoring (Invasive) |
| IX | Central Cardiac Monitoring system with invasive pressure measurements, etCO2 measurement |
| X | CVP measurement |
| XI | Defibrillators |
| XII | Fibreoptic bronchoscope |
| XIII | High Frequency Oscillation Ventilators (HFOV) |
| XIV | Incentive Spirometry |
| XV | Infusion pumps |
| XVI | Intermittent Pneumatic Compression Device (IPCD) |
| XVII | Neurally Adjusted Ventilator Assist (NAVA ventilator) |
| XVIII | Non-invasive arterial BP monitor |
| XIX | Non-invasive ventilation |
| XX | Portable PSG machine |
| XXI | Sheath Bronchoscopy |
| XXII | Ultrasound machines |
| I | Ventilators |
| II | Non-invasive ventilators |
| III | Cardiac monitors |
| IV | Portable PSG machine (Type 2 and Type 3) |
| V | Incentive Spirometry |
Medicine Ward is located inside C2 & D2 ward with:
General Ward Beds
C2 – Bed 1-10 and Bed 24 and 25
Isolations Beds - C2 - 22 and 23 and D2 41
D2 – Bed 1 to 41
C2 ICU - 8
| S.No. | Title of the project | Name of Principal Investigator | Funded by (Name of funding agency) | Duration (years) | Start year | End year | Total funds Sanctioned (Rs) |
|---|---|---|---|---|---|---|---|
| 1. | Regional Virus Research and Diagnostic Laboratory (RL-VRDL) | Dr. Lalit Dar | Department of Health Research (DHR) | 10 years (extendable) | 2019 | Continuous | ~ 5 crore |
| 2. | External Quality Assurance Scheme (EQAS) of National HIV/AIDS Reference Laboratory, AIIMS, Delhi | Dr. Bimal Kr. Das | NACO | Continuous | 2005 | Continuous | Approx. 14 lacs/annum |
| 3. | HIV integrated counseling and testing (ICTC) | Dr. Bimal Kr. Das | NACO | Continuous | 2005 | Continuous | Kits are provided by NACO and the rest is taken care of under EQAS budget |
| 4. | CD4 testing program | Dr. Bimal Kr. Das | NACO | Continuous | 2005 | Continuous | Testing kits provided by NACO, Rs. 50,000/- for Consumables |
| 5. | Evaluation of NF- κB based reactivation of latency in HIV infected individuals who are on antiretroviral therapy for more than 15 years: A Quest for Cure. | Dr. Shesh Prakash Maurya (under mentorship of Bimal Kumar Das). | Funded by DHR (HRD scheme) | 3 years | 2022 | 2025 | Rs. 50,92,497/- |
| 6. | Evaluation of role of B-1 cells in modulating the response of T cells in HIV infected patients pre and post antiretroviral therapy: cohort study. | Dr. Bimal Kumar Das | Funded by ICMR | 3 years | 2022 | 2025 | Rs. 50,40,572/- |
| 7. | Nodal coordinating center for surveillance network of antimicrobial resistance in salmonella enterica serotype Typhi and Paratyphi | Dr. Bimal Kumar Das | Funded by ICMR | 2 YEAR | 2018 | 2024 | 2,39, 22,040 |
| 8. | Detection of salmonella serovars and their associated resistance marker directly from blood specimen using paper based DNA biosensor | Dr. Bimal Kumar Das | Funded by ICMR | 2 YEAR | 2024 | 2026 | 1,35,68,808 |
| 9. | Proteomics study of Giardia intestinalis isolates to associate with different clinical spectrum and extrapolate its invasive potential | Dr. B.R Mirdha | ICMR | 3 years | Sept, 2023 | August, 2026 | 48 lakhs |
| 10. | Characterization of human antibody responses to Plasmodium vivax in India”. (Through Inspire faculty programme) | Dr. B.R Mirdha | Department of Science and Technology | 5 years | August , 2023 | 2028 | More than 5 Cr. |
| 11. | ICMRs: Advanced Mycology Diagnostic and Research Centre (AMDRC) | Prof Immaculata Xess | ICMR | 5 years | 2022 | 2027 | 250 lakhs |
| 12. | Multi-centric study on prevalence of Mycoplasma genitalium and its resistance markers in the high–risk group (MSM and FSW) attending sexually transmitted disease cclinics in North India. | Benu Dhawan | ICMR | 3 years | December 2021 | December 2024 | 28.65 Lakhs |
| 13. | Towards point of care test development for Bacterial Vaginosis, a polymicrobial infection. | Dr. Seema Sood | ICMR | 3 years | 2020 | 2023 | 51 Lakhs |
| 14. | Exploring SELEX technology for potential POCT development for Genital Chlamydia trachomatis. | Dr. Seema Sood | ICMR | 3 years | 2022 | 2025 | 50 Lakhs |
| 15. | Point-of-care test development for Bacterial Vaginosis (BV): Bench to bedside (Clinical validation of proof-of-concept). | Dr. Seema Sood | ICMR | 3 years | 2024 | 2027 | 75 Lakhs |
| 16. | Mapping hotspots of MDR-TB in Assam, Sikkim and Tripura using Genomics approaches | Dr. Urvashi B. Singh | DBT-NER | 3 years | 2018 | 2024 | ~ 4 Cr |
| 17. | Epidemiological impact and intersection of the COVID-19 and Tuberculosis Pandemics in Brazil, Russia, India and South Africa | Dr. Urvashi B. Singh | DST | 2 years | 2021 | 2023 | 1.72 Cr |
| 18. | Validation of Indigenously Developed Diagnostic kit based on Detection of Proteomic markers from Urine for Diagnosis of Pulmonary and Extra-pulmonary Tuberculosis | Dr. Urvashi B. Singh | ICMR | 3 years | 2022 | 2025 | 1.4 cr |
| 19. | Operational Feasibility and performance of indigenous phenotypic kit for detection of multidrug resistant tuberculosis and extensively drug resistant tuberculosis in field setting under the National Tuberculosis Elimination program | Dr. Urvashi B. Singh | ICMR | 3 years | 2022 | 2025 | 14 lakhs |
| 20. | Development of Surface Plasmon Resonance Array Biosensor for Rapid Molecular Drug Resistance Detection for MDR and XDR TB | Dr. Urvashi B. Singh | ICMR | 2 years | 2023 | 2025 | 40 Lakhs |
| 21. | Development of Surface Enhanced Raman Scattering (SERS) Based Biosensor for Rapid Detection of oligonucleotides in MDR and XDR-TB. | Dr. Urvashi B. Singh | AIIMS-IITD | 2 years | 2022 | 2024 | 10 Lakhs |
| 22. | A Preclinical Study to evaluate synergistic action of Rifampicin with Faropenem and Cefdinir on persister Mycobacterium tuberculosis bacilli in mouse model. | Dr. Urvashi B. Singh | AIIMS-THSTI | 2 years | 2023 | 2025 | 10 Lakhs |
| 23. | To determine the prevalence of common virulence determinants associated with Uropathogenic Escherichia coli from community-setting at different geographical regions of India using phenotypic and genotypic methods | Dr. Sarita Mohapatra | ICMR | 3 year | 2022 | 2025 | Rs553400.00 |
| 24. | Platform for discovery of novel therapeutic monoclonal antibodies against MDR and XDR Klebsiella pneumoniae | Sarita Mohapatra (Co-PI) | DBT-BIRAC | 3 years | 2023 | 2026 | Rs. 4,88,840.00 |
| 25. | Micro-nano structured urinary catheter to minimize catheter-associated urinary tract infection | Sarita Mohapatra (Co-PI) | MoE-STARS | 3 years | 2023 | 2026 | Rs 32.6 lacs |
| 26. | National Program for the Surveillance of Viral Hepatitis | Dr. Aashish Choudhary | Ministry of Health & Family Welfare (MoHFW) | 5 years (extendable) | 2020 | Continuous | ~ 1.3 crore |
| 27. | NACO Regional Reference Laboratory for HIV viral load (VL) | Dr. Aashish Choudhary | National AIDS Control Organization (NACO) | No fixed duration | 2019 | Continuous | ~ 51 lakhs |
| 28. | NACO Regional Reference Laboratory for HIV early infant diagnosis (EID) | Dr. Aashish Choudhary | National AIDS Control Organization (NACO) | No fixed duration | 2012 | Continuous | ~ 93 lakhs |
| 29. | Whole genome sequencing of the SARS-CoV-2 novel coronavirus strains at a tertiary care center in Delhi. | Dr. Aashish Choudhary | AIIMS Delhi (Intramural grant) | 2 years | 2020 | 2023 | ~ 11 lakhs |
| 30. | Molecular Epidemiology and In-Vitro Antifungal Susceptibility of Cryptic Aspergillus species from Clinical and Environment samples | Dr. Gagandeep Singh | ICMR | 3 years | 2022 | 2025 | 35 lakhs |
| 31. | Genomic profiling of invasive and hospital acquired Escherichia coli pathotypes from different clinical samples to identify the virulence and antimicrobial resistance markers | Dr. Hitender Gautam | Science & Engineering Research Board SERB (Under DST) | 2 years 6 months | Mar 2022 | Sept 2024 | 45,45,816/- |
| 32. | Site-specific biomarkers to differentiate infection from either colonization or aseptic inflammation in ICU | Dr. Hitender Gautam | ICMR | 3 years | Jan 2023 | Dec 2025 | 73,39,362/- |
| 33. | Molecular Characterization of diarrheagenic Escherichia coli among children with acute diarrhea: Association of virulence and adherence genes. | AIIMS Site PI: Dr. Hitender Gautam | Department of Health Research (DHR) | 3 years | Jan 2024 | Dec 2026 | 20,42,367/- |
| 34. | Platform for enhanced pathogen detection for meningitis and sepsis: Rapid, portable, and field-deployable diagnostics. IIRPIG-2023-0001405 | AIIMS Site PI: Dr. Hitender Gautam | ICMR | 4 years | Mar 2024 | Feb 2027 | 93,46,030/- |
| 35. | Detection of viable but non-culturable (VBNC) Gram-negative bacteria in sepsis and meningitis: Clinical significance in AMR stewardship | AIIMS Site PI: Dr. Hitender Gautam | AIIMS-THSTI Collaborative Project | 2 years | Dec 2023 | Dec 2025 | 10 Lakhs |
| 36. | Antimicrobial susceptibility patterns of pathogens isolated in bloodstream infections vis a vis antibiotic prescribing practices and genotypic clonality of Acinetobacter baumannii in various patient care units/areas | Dr. Hitender Gautam | Inter-Disciplinary AIIMS IMRG. | 1 year | Jan 2024 | Jan 2025 | 4,90,350/- |
| 37. | Clinical and epidemiological study of Lyme disease: a multi-centric taskforce study in India | Dr. Nishant Verma | ICMR | 3 | 2020 | 2023 | 3,86,71,240/- |
| 38. | Proteomics study of Giardia intestinalis isolates to associate with different clinical spectrum and extrapolate its invasive potential | Dr. Nishant Verma | ICMR | 3 | 2023 | 2026 | 48,69,222 |
| 39. | Expanded viral etiological investigation of genital ulcer disease with phenotyping and genotyping for antiviral drug resistance in herpes simplex viruses | Dr. Megha Brijwal | ICMR | 3 years | 2023 | 2026 | ~ 59 lakhs |
| 40. | Strengthening Capacity for Genomic Sequencing of Outbreak Prone Respiratory Pathogens like Influenza and Other Respiratory Viruses | Dr. Megha Brijwal | CDC & APHL, USA | 5 months | 2023 | 2023 | ~ 40 lakhs |
| 41. | Quantification of JC polyomavirus in CSF in patients with suspected progressive multifocal leukoencephalopathy (PML) by digital PCR | Dr. Megha Brijwal | AIIMS Delhi (Intramural grant) | 1 year | 2023 | 2024 | ~ 5 lakhs |
| 42. | Non-tubercular mycobacteria responsible for pulmonary disease and infections in procedures involving prosthetic devices, laparoscopy or following other interventions. | Dr. Kiran Bala | AIIMS, Intramural | 1 year | 2023 | 2024 | 4.95 Lakhs |
| 43. | Detection of Mycoplasma pneumoniae infections in acute exacerbation of Chronic Obstructive Pulmonary Disease | Dr. Tanu Sagar | AIIMS Intramural | 2 years | 2024 | 2026 | 9.8 Lakhs |
| S.No. | Title of the project | Name of Principal Investigator | Funded by (Name of funding agency) | Duration (years) | Start year | End year | Total funds Sanctioned (Rs) |
|---|---|---|---|---|---|---|---|
| 1 | Comparison of diagnostic accuracy of Real time PCR versus Nugent’s scoring in Indian women with and without Bacterial Vaginosis (BV). Award of SRFship | Dr. Seema Sood | ICMR | 3 years | 2019 | 2022 | 16.6 Lakhs |
| 2 | Early Bactericidal Activity (EBA) of Rifampicin and Feropenem in Tuberculosis (Rifampicin Susceptible)- | Dr. Urvashi B. Singh | ICMR | 2 Years | 2019 | 2022 | 70 Lakhs |
| 3 | Early Bactericidal Activity (EBA) and Pk/Pd Study of Rifampicin Feropenem Cefdinir with Clavulanate vs Standard of Care in Newly Diagnosed Smear Positive Rifampicin Susceptible TB | Dr. Urvashi B. Singh | ICMR | 2 Years | 2019 | 2023 | 70 Lakhs |
| 4 | Rapid Molecular Drug Resistance Detections for MDR and XDR-TB and Molecular Typing of Mycobacterium Tuberculosis From Ziehl-Neelsen’s Stained Microscopic Slides From Delhi State. | Dr. Urvashi B. Singh | ICMR | 3 Years | 2018 | 2022 | ~ 60 Lakhs |
| 5 | Diagnosis of Pulmonary And Extra-Pulmonary Tuberculosis Patients Using Differentially Expressed Proteins As Potential Biomarkers: An Approach Towards Development Of Point Of Care Test. | Dr. Urvashi B. Singh | ICMR | 3 Years | 2018 | 2022 | 60 lakhs |
| 6 | Crohn’s Disease in India: A multicenter study from a country where intestinal tuberculosis as well as Johne’s disease is endemic. | Dr. Urvashi B. Singh | ICMR/DHR | 5 Years | 2016 | 2022 | 35 lacs |
| 7 | In vitro susceptibility of Cefiderocol against carbapenem-resistant gram-negative bacilli from patients with blood stream infection/sepsis, urinary tract infection or pneumonia | Dr. Sarita Mohapatra | Funded (Intramural) | 2yr | 2021 | 2023 | 9.7lacs |
| 8 | Implementation of An Institutional Antifungal Stewardship Program (AFSP) On The Appropriate Use Of Antifungal Therapy And Outcomes In Patients With Invasive Fungal Infections. | Dr. Gagandeep Singh | ICMR | 3 years | 2020 | 2023 | 48 lakhs |
| 9 | Study of hyaline non-sporulating moulds isolated from clinical samples of tertiary care respiratory hospital in Delhi | Dr. Gagandeep Singh | ICMR | 3 years | 2021 | 2024 | 27 lakhs |
| 10 | Magnitude of asymptomatic malaria infections in pregnant women in a community hospital | Dr. Nishant Verma | AIIMS, New Delhi | 1 | 2018 | 2019 (work continued in previous year too) | 4,98,000/- |
| 11 | A prospective study of viral infections in hematopoietic stem cell transplant recipients at a tertiary care hospital in India | Dr. Megha Brijwal | ICMR | 3 years | 2019 | 2023 | 45 lakhs |
| 12 | Point of care Urinary Lipoarabinomannan antigen (LAM) detection as a diagnostic tool for Extra-pulmonary tuberculosis. | Dr. Kiran Bala | AIIMS, Intramural | 2 year | 2021 | 2023 | 4.94 Lakhs |
| 13 | Changing epidemiology of tuberculosis among SARS CoV-2 pandemics. | Dr. Kiran Bala | AIIMS, Intramural | 2 year | 2021 | 2023 | 7.14 Lakhs |
Anaerobic-bacteriology, Special Bacterial Pathogen Laboratory and Metagenomics Laboratory
Microbiology III Semester Teaching Schedule 16th Aug 24 to 22nd Dec 24
| Mobile No. | Faculty Email I.D. | Faculty Name | Day | Start Date | Subject | Topic Name | Lecture Name | Venue | Type of Lecture | From | AM/PM | To | AM/PM |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 9818137078 | lalitdaraiims@gmail.com | Dr. L. Dar | Thursday | 22.08.24 | Microbiology | Introduction to Microbiology and its role in medicine | Introduction to Microbiology and its role in medicine | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9717315286 | tezpur.bimal@gmail.com | Dr. B. K. Das | Thursday | 22.08.24 | Microbiology | Introduction to Bacteriology: Classification & Structure | Introduction to Bacteriology: Classification & Structure | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9810225523 | seemalsood@gmail.com | Dr. S. Sood | Thursday | 22.08.24 | Microbiology | Microscopy & Micrometry | Microscopy & Micrometry | LT-4/UG LAB | Lecture/Practical | 2 | PM | 4 | PM |
| 7065226016 | dr.priyambatra@gmail.com | Dr. P Batra | Thursday | 29.08.24 | Microbiology | Bacterial staining & cultivation | Bacterial staining & cultivation | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9311106715 | dhawanb@gmail.com | Dr. B. Dhawan | Thursday | 29.08.24 | Microbiology | Standard Precautions | Standard Precautions | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9810726220 | drsarita2005@gmail.com | Dr. S. Mohapatra | Thursday | 29.08.24 | Microbiology | Direct demonstration of bacteria by staining (Gram’s/Albert’s/ZN) (demo) | Direct demonstration of bacteria by staining (Gram’s/Albert’s/ZN); common media (demo) | UG Lab | Practical | 2 | PM | 4 | PM |
| 9810726220 | drsarita2005@gmail.com | Dr. S. Mohapatra | Thursday | 05.09.24 | Microbiology | Common culture media | Common culture media | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9311106715 | dhawanb@gmail.com | Dr. B. Dhawan | Thursday | 05.09.24 | Microbiology | Common tests for bacterial identification & their principles | Common tests for bacterial identification & their principles | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9911188824 | drhitender@gmail.com | Dr. H. Gautam | Thursday | 05.09.24 | Microbiology | Revision of staining methods, hanging drop preparation; Common media & biochemical tests (demo) | Revision of staining methods, hanging drop preparation; Common media & biochemical tests (demo) | UG Lab | Practical | 2 | PM | 4 | PM |
| 9717315286 | tezpur.bimal@gmail.com | Dr. B. K. Das | Thursday | 12.09.24 | Microbiology | Bacterial Genetics | Bacterial Genetics | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9911188824 | drhitender@gmail.com | Dr. H. Gautam | Thursday | 12.09.24 | Microbiology | Antibiotic susceptibility testing | Antibiotic susceptibility testing | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9911188824 | drhitender@gmail.com | Dr. H. Gautam | Thursday | 12.09.24 | Microbiology | Antibiotic susceptibility testing (demo) | Antibiotic susceptibility testing (demo) | UG Lab | Practical | 2 | PM | 4 | PM |
| 9871455655 | aashishpath@yahoo.co.in | Dr. A choudhary | Thursday | 19.09.24 | Microbiology | Introduction to Virology: Structure & classification | Introduction to Virology: Structure & classification | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9868994329 | megha.brijwal@yahoo.com | Dr. M. Brijwal | Thursday | 19.09.24 | Microbiology | Laboratory diagnosis of viral infections | Laboratory diagnosis of viral infections | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9868994329 | megha.brijwal@yahoo.com | Dr. M. Brijwal | Thursday | 19.09.24 | Microbiology | Laboratory diagnosis of viral infections | Laboratory diagnosis of viral infections | UG Lab | Practical | 2 | PM | 4 | PM |
| 9818268181 | immaxess@gmail.com | Dr. I. Xess | Thursday | 26.09.24 | Microbiology | Introduction to Mycology: Structure & classification | Introduction to Mycology: Structure & classification | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9878370024 | drgagandeep@gmail.com | Dr. G. Singh | Thursday | 26.09.24 | Microbiology | Laboratory diagnosis of fungal infections | Laboratory diagnosis of fungal infections | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9878370024 | drgagandeep@gmail.com | Dr. G. Singh | Thursday | 26.09.24 | Microbiology | KOH preparation & Gram’s staining for fungi; culture methods (demo) | KOH preparation & Gram’s staining for fungi; culture methods (demo) | UG Lab | Practical | 2 | PM | 4 | PM |
| 9899679399 | mirdhabraiims@gmail.com | Dr. B. R. Mirdha | Thursday | 03.10.24 | Microbiology | Introduction to Parasitology & Classification of Parasites | Introduction to Parasitology & Classification of Parasites | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9868068001 | drnishant2k@yahoo.co.in | Dr. N. Verma | Thursday | 03.10.24 | Microbiology | Laboratory diagnosis of parasitic infections | Laboratory diagnosis of parasitic infections | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9717315286 | tezpur.bimal@gmail.com | Dr. B.K.Das (Moderator) Dr. S Mohapatra,Dr. G Singh, Dr. N. Verma, Dr. M. Brijwal | Thursday | 03.10.24 | Microbiology | Collection and transport of samples | Collection and transport of samples | LT-4 | Lecture | 2 | PM | 4 | PM |
| 3rd Mid semester exam from 07.10.24 to 15.10.24 | |||||||||||||
| 9911188824 | drhitender@gmail.com | Dr. H. Gautam | Thursday | 17.10.24 | Microbiology | General principles of immunity against microbes (I) | General principles of immunity against microbes (I) | LT-4 | Lecture | 8 | AM | 9 | AM |
| 7065226016 | dr.priyambatra@gmail.com | Dr. P Batra | Thursday | 17.10.24 | Microbiology | Immunodiagnostic tests | Immunodiagnostic tests | LT-4 | Lecture | 9 | AM | 10 | AM |
| 7065226016 | dr.priyambatra@gmail.com | Dr. P Batra | Thursday | 17.10.24 | Microbiology | Immunodiagnostic tests | Immunodiagnostic tests | UG Lab | Practical | 2 | PM | 4 | PM |
| 9911188824 | drhitender@gmail.com | Dr. H. Gautam | Thursday | 24.10.24 | Microbiology | General principles of immunity against microbes (II) | General principles of immunity against microbes (II) | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9810225523 | seemalsood@gmail.com | Dr. S. Sood | Thursday | 24.10.24 | Microbiology | Sterilization & Disinfection | Sterilization & Disinfection | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9810225523 | seemalsood@gmail.com | Dr. S. Sood | Thursday | 24.10.24 | Microbiology | Sterilization & Disinfection | Sterilization & Disinfection | UG Lab | Practical | 2 | PM | 4 | PM |
| 9818137078 | lalitdaraiims@gmail.com | Dr. L. Dar | Thursday | 07.11.24 | Microbiology | Viral Genetics | Viral Genetics | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9650822811 | drkiran.dks@gmail.com | Dr. K. Bala | Thursday | 07.11.24 | Microbiology | Molecular biology techniques II | Molecular biology techniques II | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9650822811 | drkiran.dks@gmail.com | Dr. K. Bala | Thursday | 07.11.24 | Microbiology | Molecular biology techniques (Demo) | Molecular biology techniques (Demo) | UG Lab | Practical | 2 | PM | 4 | PM |
| 9717315286 | tezpur.bimal@gmail.com | Dr. B. K. Das | Thursday | 14.11.24 | Microbiology | Introduction to Enterobacteriaceae | Introduction to Enterobacteriaceae | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9311106715 | dhawanb@gmail.com | Dr. B. Dhawan | Thursday | 14.11.24 | Microbiology | Bacillary dysentery | Bacillary dysentery | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9911188824 | drhitender@gmail.com | Dr. H. Gautam | Thursday | 14.11.24 | Microbiology | Enterobacteriaceae | Enterobacteriaceae | UG Lab | Practical | 2 | PM | 4 | PM |
| 9911188824 | drhitender@gmail.com | Dr. H. Gautam | Thursday | 21.11.24 | Microbiology | Cholera | Cholera | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9717315286 | tezpur.bimal@gmail.com | Dr. B. K. Das | Thursday | 21.11.24 | Microbiology | E.coli diarrhoea | E.coli diarrhoea | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9311106715 | dhawanb@gmail.com | Dr. B. Dhawan | Thursday | 21.11.24 | Microbiology | Exam. of stool- pus cells/RBC/motility, Culture media for Stool samples, Demonstration: Shigella,E.coli, Vibrio | Exam. of stool- pus cells/RBC/motility, Culture media for Stool samples, Demonstration: Shigella,E.coli, Vibrio | UG Lab | Practical | 2 | PM | 4 | PM |
| 7065226016 | dr.priyambatra@gmail.com | Dr. P Batra | Thursday | 28.11.24 | Microbiology | Bacterial food poisoning (toxic) | Bacterial food poisoning (toxic) | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9810726220 | drsarita2005@gmail.com | Dr. S. Mohapatra | Thursday | 28.11.24 | Microbiology | Bacterial food poisoning (infective) | Bacterial food poisoning (infective) | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9810726220 | drsarita2005@gmail.com | Dr. S. Mohapatra | Thursday | 28.11.24 | Microbiology | Lab. Diagnosis of food poisoning (incl. lab. diag. of Staph) | Lab. Diagnosis of food poisoning (incl. lab. diag. of Staph) | UG Lab | Practical | 2 | PM | 4 | PM |
| 9899679399 | mirdhabraiims@gmail.com | Dr. B. R. Mirdha | Thursday | 05.12.24 | Microbiology | Amoebiasis | Amoebiasis | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9868068001 | drnishant2k@yahoo.co.in | Dr. N. Verma | Thursday | 05.12.24 | Microbiology | Giardiasis and Intestinal Coccidiosis | Giardiasis and Intestinal Coccidiosis | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9868068001 | drnishant2k@yahoo.co.in | Dr. N. Verma | Thursday | 05.12.24 | Microbiology | Stool examination for ova and cyst | Stool examination for ova and cyst | UG Lab | Practical | 2 | PM | 4 | PM |
| 9868068001 | drnishant2k@yahoo.co.in | Dr. N. Verma | Thursday | 12.12.24 | Microbiology | Intestinal infection by Nematodes -I | Intestinal infection by Nematodes -I | LT-4 | Lecture | 8 | AM | 9 | AM |
| 9878370024 | drgagandeep@gmail.com | Dr. G. Singh | Thursday | 12.12.24 | Microbiology | Intestinal infection by Nematodes -II | Intestinal infection by Nematodes -II | LT-4 | Lecture | 9 | AM | 10 | AM |
| 9868068001 | drnishant2k@yahoo.co.in | Dr. N. Verma | Thursday | 12.12.24 | Microbiology | Stool examination for ova and cyst | Stool examination for ova and cyst | UG Lab | Practical | 2 | PM | 4 | PM |
| 3rd End semester exam from 13.12.24 to 22.12.24 | |||||||||||||
| Winter Vacation from 22.12.24 to 10.01.25 | |||||||||||||
| Name | Date of Joining |
|---|---|
| Dr Awasthi | 1-Jan-69 |
| Dr. Das Gupta | 14-Dec-74 |
| Dr. D S Rana | 15-Jun-77 |
| Dr. Manoj Parashar | 10-Feb-78 |
| Dr. R K Sharma | 4-May-79 |
| Dr. Ashok Kumar Gupta | 1-May-83 |
| Dr. D P Rathi | 1-May-83 |
| Dr. L C Sharma | 15-Nov-83 |
| Dr. Amit Gupta | 1-May-84 |
| Dr. S K Agarwal | 1-May-85 |
| Dr. R S Ahlawat | 15-Aug-87 |
| Dr. Rajesh Agarwal | 1-Sep-87 |
| Dr. D K Gupta | 18-Jan-88 |
| Dr. Dinesh Mittal | 4-May-90 |
| Dr. K D Sadhwani | 24-Jul-90 |
| Dr Ravinder Mittal | 26-May-91 |
| Dr. Rashmi Saxena | 20-Jan-92 |
| Dr. R K Hotchandani | 1-May-92 |
| Dr. U C Arora | 9-Jun-92 |
| Dr Shyamsunder | 21-Jan-93 |
| Dr. PM Jairaj | 23-Jan-93 |
| Dr. Sharad Agarwal | 7-Jul-93 |
| Dr. Sunil Prakash | 8-Jul-93 |
| Dr. Rajan Isaac | 14-Jan-94 |
| Dr. Sanjay Gupta | 24-Jan-94 |
| Dr. Sanjeev Mittal | 12-Jul-94 |
| Dr Yogesh Bhargava | 14-Jul-94 |
| Dr. (Col). H S Gill | 5-Jan-95 |
| Dr RP Mathur | 4-Jul-95 |
| Dr. AK Barman | 17-Jan-96 |
| Dr DS Ray | 18-Feb-96 |
| Dr. Gopesh Modi | 10-Oct-96 |
| Dr. Deepak Jain | 10-Oct-96 |
| Dr. Debashish Saha | 28-Jan-97 |
| Dr. BS Solanki | 31-Jan-97 |
| Dr. NK Mohanty | 1-Jul-97 |
| Dr. S Padmanabhan | 1-Jul-97 |
| Dr. (Col) A Hooda | 1-Jan-98 |
| Dr. (Col) Rajshree Ramasethu | 7-Jan-99 |
| Dr. DSB Raju | 1-Jul-99 |
| Dr. Sanjay Vikrant | 1-Jul-99 |
| Dr. Sandeep Mahajan | 1-Jul-99 |
| Dr Sugeet Baveja | 1-Jul-99 |
| Dr. K Abirami | 27-Jan-00 |
| Dr. Rajesh Bharani | 31-Jan-00 |
| Dr. Vikram kalra | 3-Jul-00 |
| Dr. Muzaffar Wani | 24-Jul-00 |
| Dr. Rajesh Khanduja | 23-Oct-00 |
| Dr. SM Shiva Prasad | 24-Jan-02 |
| Dr. Gulshan Mukhia | 2-Jul-02 |
| Dr. Ravi Bansal | 4-Jul-02 |
| Dr. Prashant Bendre | 6-Jan-03 |
| Dr. Sandeep Saxena | 10-Jan-03 |
| Dr. Tajamul Mir | 7-Jul-03 |
| Dr. Umesh Gupta | 9-Jul-03 |
| Dr. Manjuri Sharma | 21-Jan-04 |
| Dr. Himanshu Sekhar Mahapatra | 15-Jul-04 |
| Dr. Ashok Kumar Panda | 1-Jul-05 |
| Dr. (Col) Ranjit Kumar Nair | 1-Jul-05 |
| Dr. Vijay Gupta | 1-Jul-05 |
| Dr. Soumita K Bagchi | 1-Jul-05 |
| Dr. Amber Khera | 2-Jan-06 |
| Dr. BK Upadhyaya | 2-Jan-06 |
| Dr Suman Lata | 1-Jul-06 |
| Dr. Om Prakash rathi | 2-Jan-07 |
| Dr. Avinash ignatius | 2-Jan-07 |
| Dr. Pranabjyoti Mahanta | 10-Jan-07 |
| Dr. Ankur Gupta | 1-Jun-07 |
| Dr. Bakshish Singh | 9-Jan-08 |
| Dr. Satish mandonca | 9-Jan-08 |
| Dr. Anil K Bhatt | 1-Jul-08 |
| Dr. Charanjeet lal | 1-Jul-08 |
| Dr. Sheel jain | 1-Jan-09 |
| Dr. Mitul Bora | 1-Jan-09 |
| Dr. P M Dogra | 10-Jan-09 |
| Dr. Yasir Rizvi | 1-July-09 |
| Dr Amit Gupta | 1-Jan-10 |
| Dr Shivaramakrishnan R | 1-Jan-10 |
| Dr Mudit Gupta | 1-July-10 |
| Dr Sanjiv Mahajan | 5-Jul-10 |
| Dr Amit Kumar | 1-Jan-11 |
| Dr T Murari | 6-Jan-11 |
| Dr Akansha Agrawal | 1-July-11 |
| Dr Madhu Shankar | 1-July-11 |
| Dr Raj Kanwar Yadav | 7-July-11 |
| Dr Amritaksha Deb | 1-Jan-12 |
| Dr Yogesh Chaabra | 1-Jan-12 |
| Dr Sanjay Panda | 1-July-12 |
| Dr Sudeep Singh | 1-July-12 |
| Dr Muthu Kumar | 1-Jan-13 |
| Dr Sucheta Yadav | 1-July-13 |
| Dr Vikraman G | 1-July-13 |
| Dr Vijoy Kumar Jha | 1-Jan-14 |
| Dr Pramod Mittal | 1-Jan-14 |
| Dr Atul Kumar Srivastava | 1-Jan-14 |
| Dr Arun Kumar S | 1-July-14 |
| Dr Mamidi Pranith Ram | 1-July-14 |
| Dr Himanshu Sharma | 1-July-14 |
| Dr Navinath M | 1-Jan-15 |
| Dr N Rajkanna | 1-Jan-15 |
| Dr Shreepriya Mangalgi | 1-July-15 |
| Dr Vineet Behera | 1-Jan-16 |
| Dr A Kishore Kumar | 6-Jan-16 |
| Dr Nishita Mohan Philip | 4-July-16 |
| Dr Mohd Aslam | 4-Jan-17 |
| Dr Deepak Kumar Panigrahi | 6-Jan-17 |
| Dr Sukhwinder Sangha | 1-July-17 |
| Dr Kristin George | 3-July-17 |
| Dr Asheesh Kumar | 11-Aug-17 |
| Dr Sumita Bhogal | 1-Jan-18 |
| Dr Sachin Srivastava | 1-Jan-18 |
| Dr Anitha S | 3-Jan-18 |
| Dr Sana Shadab | 2-July-18 |
| Dr Dheeraj Singh | 2-July-18 |
| Dr Arpit Gupta | 22-Jan-19 |
| Dr Bhupesh Saini | 31-Jan-19 |
| Dr Timitrov P | 01-Jan-20 |
| Dr Indradip Maity | 29-Jan-20 |
| Dr Sambit Sundarray | 31-Jan-20 |
| Dr Nehal Agarwal | 11-Jan-21 |
| Dr Priyanka Verma | 11-Jan-21 |
The department is committed to increasing the awareness of the general public regarding various kidney diseases including their causes, prevention and available treatment modalities. Towards this end the department periodically conducts the following:
The Department of Nephrology conducts the following outpatient clinics/OPD
Monday, Tuesday, Thursday and Friday 9.00 am onwards
Monday and Thursday afternoon: All consultants
Monday, Tuesday, Thursday and Friday 9.00 am onwards
Wednesday 9-10 am
Patients are admitted as per availability of beds
The department is active in teaching of
Email ID : fetalmedicineaiims@gmail.com
The services provided by the division of MFM consists of the following:
Dr. Vatsla Dadhwal, Dr. Anubhuti Rana: Monday & Thursday
Dr. K. Aparna Sharma, Dr Rinchen Zangmo: Wednesday & Saturday
The Division of Maternal Fetal medicine (Department of Obstetrics and Gynaecology) at All India Institute of Medical Sciences New Delhi is known for its excellent team, respectful patient care and state of the art infrastructure with advanced ultrasound machines, LASER therapy and Radiofrequency ablation therapy. It was established under the leadership of Professor Dipika Deka. Over the years the division has grown keeping pace with the ever-increasing advances in the field of Fetal Medicine. In addition to providing quality care to the patients, the division is also actively involved in advanced research in fetal diagnostic and therapeutic procedures. We aim to serve all sections of the society with equal respect and care keeping medical etiquettes and ethics in mind. Our team believes in continuously auditing and introspecting our own management so as to give the best services to our patients and also engrave the idea of quality care in our trainees. We continuously update ourselves in the latest developments in the field by conducting continuous CMEs, Webinars and seminars. We have published over 60 research papers in indexed international and national journals. We have teamed up with the Division of Medical Genetics (Department of Pediatrics) AIIMS for counseling of the parents and for prenatal genetic testing so as to provide best possible care to expecting couples for a healthy baby. We offer one-year fellowship programme and long term observership programme based on eligibility criteria and an entrance examination. As many as 30 candidates have completed fellowship and observership from our centre and are providing services in the field of Fetal Medicine in different parts of the country.
ART Centre,
Department of Obst. And Gynaecolgy,
Third Floor, Main Hospital,
AIIMS, Ansaari Nagar, N.Delhi-110029
Tel.No. 011-26593450
E.Mail Address : -
| Batch | Name |
|---|---|
| 2016 | Dr. Arun Prashanth K |
| 2017 | Dr. Meghana Prabhu S, Dr. Dhritiman Chakraborty, Dr. K. Sreenivasa Reddy, Dr. Saurabh Arora |
| 2018 | Dr. Abhishek Behra, Dr. Avinash Tupalli |
| 2019 | Dr. Mangu Bharadwaj |
| 2020 | Dr. Shobhana, Dr. Chandra Teja Reddy, Dr. Sai Moulika |
| Batch | Name |
|---|---|
| 1997 | Dr. Senthil Kumar |
| 1998 | Dr. Gopal V. Punjabi, Dr. Sukanta Barai, Dr. Atul Marwah |
| 1999 | Dr. Bharati Dashan J, Dr. Hentok Phom |
| 2000 | Dr. Chandrasekhar N, Dr. Saikat K. Choudhury, Dr. Thomas E.J. |
| 2001 | Dr. Naveen K, Dr. Mohiuddin Hadi |
| 2002 | Dr. Srabani Sen, Dr. Murali Nadig R., Dr. Dhanapathi Halanaik |
| 2003 | Dr. Tarun Singhal |
| 2004 | Dr. Shamim A. Shamim, Dr. Tushar K. Mohapatra, Dr. B. Vijay Babu |
| 2005 | Dr. Nishikant A. Damle |
| 2006 | Dr. Niraj Naswa, Dr. Amburanjan Santra |
| 2007 | Dr. Gona Rama Mohan Reddy, Dr. Punit Sharma, Dr. Rajender Kumar, Dr. Suhas Singla |
| 2008 | Dr. Sagar Maharjan, Dr. Abhishek Kumar, Dr. Sellam Karunanithi |
| 2009 | Dr. Aftab H. Nazar, Dr. Harmandeep Singh, Dr. Parveen Kundu, Dr. Sunil Jeph |
| 2010 | Dr. Ramya S, Dr. Manish Patnecha, Dr. Kalpa J. Das, Dr. Khangembam Bangkim Chandra, Dr. Abhinav Singhal, Dr. Varun Singh Dhull, Dr. Sudhir Kc, Dr. Krishankant Agarwal, Dr. Manas K. Sahoo |
| 2011 | Dr. Sachin Jain, Dr. Ajiv K. Mishra, Dr. Tarun Kumar Jain |
| 2012 | Dr. Girish K. Parida, Dr. Sumeet S. Malapure, Dr. Anirban Mukherjee, Dr. Saurabh Arora, Dr. Partha Sarathi Chakraborty |
| 2013 | Dr. Ganesh Kumar M, Dr. Averilicia Passah, Dr. Ravi Kant Gupta, Dr. Kunal Kumar, Shambo Guha Roy, Dr. Satyavrat Verma |
| 2014 | Dr. Abhishek Behera, Dr. Anshul Sharma, Dr. Shruti Tulsyan, Dr. Pragati Jha |
| 2015 | Dr. Arun Raj ST, Dr. Vivek Baghel, Dr. Sarthak Tripathy, Dr. Divya Yadav |
| 2016 | Dr. Harish Goyal, Dr. Harish N |
| 2017 | Dr. Shreya Datta Gupta, Dr. Prateek Kaushik, Dr. Shobhana Raju, Dr. Jasim Jaleel, Dr. Tejesh P. Singh, Dr. T. Kishan Sibudhi, Dr. Roma |
| 2018 | Dr. Angel Hemrom, Dr. Arunav Kumar, Dr. Nikhil Mohan, Dr. Dikhra Khan, Dr. Sambit Sagar, Dr. Thayumanavan T, Dr. Sneha Prakash |
| 2019 | Dr. Suraj Kumar, Dr. Kritin Shankar, Dr. Ritwik Nitin Wakankar, Dr. Althaf K M, Dr. Sulochana Saraswat |
| 2020 | Dr. Siva Shankar, Dr. Ashok, Dr. Simran,Dr. Yamini,Dr. Anushna,Dr. Aparna, Dr. Dharvesh,Dr. Saurav, Dr. Vaibhav |
| 2021 | Dr. John, Dr. Sumit, Dr. Shubha, Dr. Aditi |
| Batch | Name |
|---|---|
| 2003 | Rajeev Kumar, Dhananjay, Sanjiv Saw, Sarika Kumari |
| 2004 | Parul Thakral, Santosh Gupta, Sarita, Sushma |
| 2005 | Praveen Kumar, Manjesh, Amit, Amarjeet |
| 2006 | Geetanjali Arora, Smriti, Archana, Durgesh K. Dwivedi, Himanshu, Ajay |
| 2007 | Priyanka Gupta, Sunil, Alok |
| 2008 | Arun, Jyotsna |
| 2009 | Sanjana Ballal, Ranjeet, Santosh, Abhishek, Sanjiv |
| 2010 | Ashwathi, Shekhar, Devender, Pankaj, Sumit Varshney |
| 2011 | Madhav Yadav |
| 2013 | Ridhima, Binish, Manoj |
| 2014 | Deepak, Jayprakash, Manoranjan, Rajesh Mishra, Preeti Singh |
| 2015 | Kartik Saroha H, Dhirendra Jaiswal, Mahesh, Mukesh, Umesh, Manish, Varsha |
| 2016 | Pankaj, Vaishali Dhiman, Chandan, Ashish, Priyanka, Praveen, Anukriti, Anand, Ghazala, Garima |
| 2017 | Bhola, Jahangir, Vanjul, Vikash, Deepak, Harpreet, Satnam, Sundarlal |
| 2018 | Lavanya, Shashwat, Kanaklata, Shweta, Naresh, Yaishwariya, Ajay |
| 2019 | Samta, Apoorva, Deepak, Navneet, Sunil, Tabassum, Shweta, Priyanka |
| 2020 | Shreya,Nicky, Shweta, Sonu Kumar, Navneet, Sachin, Satya, Jagriti, Roopal, Sakshi, Hashim, Jyoti, Sonu Sahu |
| 2021 | Gagandeep, Adibaa, Gagandeep, Beena, Priya, Anshika, Suman, Sonu Katala, Parvind, Nikhil, Prashant, Ravi, Rohit |
54th Annual Conference of the Society of Nuclear Medicine (India) SNMICON 2022 (Theme: Theranostics – The Dawn of a New Era), 8 – 11 December 2022; AIIMS, New Delhi.
| S.No | Procedure | Charges |
|---|---|---|
| 1. | IVF(In-Vitro-Fertilization) Package | Rs.60000/-(Sixty thousand only) |
| 2. | IVF- ICSI (In-Vitro-Fertilization with Intera-Cytoplasmic Sperm Insemination) Package | Rs.65000/-(Sixty five thousand only) |
| 3. | IUI (Intera-Uterine Insemination) | Rs.4000/-(four thousand only )per cycle with medicines and Consumables for one month |
| 4. | Embryo Freezing | Rs.5000/-(five thousand only)for one year |
| 5. | Frozen Embryo Replacement | Rs.5000/-/-(five thousand only) per Cycle |
| 6. | Assisted Hatching | Rs.2000/-/-(two thousand only) per cycle |
| 7. | Extended Blastocyst Culture | Rs.5000/-/-(five thousand only) per cycle |
Details of prior research publications are available in the annual reports available on the institute’s website. Please visit the AIIMS website and go to “About Us Annual Reports”.
Department is equipped with 5 Gamma cameras including 3 dual head SPECT systems. All types of nuclear medicine investigation are performed in these imaging systems.
Thyroid uptake probe, gamma ray spectrometers, Liquid Scintillation Counter are available for in-vivo and in-vitro studies.
Department has 11 MeV cyclotron (CTI Inc.) for the production of positron emitters (such as 18F, 15O,13N,11C) and well equipped Radio chemistry laboratory for producing positron emitting radiopharmaceuticals.
State of the art PET/CT (Biograph) imaging facility is now available in the department at AIIMS. The most widely used PET radiopharmaceutical 18F-FDG is being routinely used at our centre. The CT not only provides the high contrast anatomical images but also provides attenuation map for attenuation correction in PET imaging. This modality has its role in Oncology, cardiology and neurology with more than 80% application in oncology for staging, monitoring treatment response, in differentiating benign and malignant lesion and restaging. It also has a role for radio therapy treatment planning.
All the patients are now getting the advantage of this new and emerging imaging modality. More than 2400 patients have already been investigated on this new imaging facility till September 2006.
Other PET radiopharmaceuticals using 15O, 13N, and 11C are be used in near future.
Department has recently procured 68Ga-68Ge generators for preparing other positron emitting radio pharmaceuticals.
Department has been providing radionuclide therapy facility to patients of thyrotoxicosis and cancer thyroid with 131I. There is a specifically designed isolation ward/beds for cancer thyroid patients duly approved by BARC/AERB. Other radionuclide therapy include bone pain palliation with 89Sr, 153Sm, Radiation synovectomy with 90Y and treatment of inoperable hepato cellulat carcinoma (HCC) with 188Re-lipiodol.
Lab Services :
Other facilities : 7 Gamma Cameras including 2 Single Head, 4 Dual Head with 2 having SPECT/CT facilities.
Non Imaging : RAIU & GFR
A facility for indoor admission of patients undergoing Radionuclide Therapy is available in ward D1. The department has been providing radionuclide therapy to patients with thyrotoxicosis and thyroid cancer with 131-I. There is a specifically designed isolation ward/beds for thyroid cancer patients duly approved by BARC/AERB. Other radionuclide therapies include bone pain palliation, Radiation synovectomy, PRRT, PSMA therapy, FAPi therapy, treatment of inoperable hepatocellular carcinoma (HCC) with 188Re-lipiodol etc.
The department is equipped with 6 Gamma cameras including 3 dual head SPECT/CT systems. All types of nuclear medicine imaging procedures are performed in these imaging systems.
Thyroid uptake probe, gamma ray spectrometers, and Liquid Scintillation Counter are available for in-vivo and in-vitro studies such as RAIU, GFR.
The department has one 11 MeV cyclotron for the production of positron emitters (such as 18F, 15O,13N, and 11C) and a well-equipped Radiochemistry laboratory for producing positron-emitting radiopharmaceuticals.
Two state-of-the-art PET/CT systems are available in the department. The most widely used PET radiopharmaceutical, 18F-FDG, is being routinely produced and utilized in the department. This modality has a tremendous role in oncology, cardiology, neurology, etc. with more than 80% application in oncology for staging, monitoring treatment response, differentiating benign and malignant lesions, and restaging. It also has a role in radiotherapy treatment planning. The department also has 68Ge-68Ga generators for preparing other positron-emitting radiopharmaceuticals.
Nuclear Medicine Therapy OPD is held daily. The following consultants are available as per their designated days:
| Days | Nuclear Medicine Therapy Clinic |
|---|---|
| Monday | Prof. C.S. Bal |
| Tuesday | Dr. Shamim A. Shamim |
| Wednesday | Prof. C.S. Bal |
| Thursday | Prof. Rakesh Kumar |
| Friday | Dr. Nishikant A. Damle |
| Saturday | Dr. Madhavi Tripathi |
Nursing Superintendent is responsible to the C.N.O. for planning organisation and development of nursing services in the hospital in consultation with Medical Supdt./Chief of centres.
Deputy Nursing Superintendent is responsible to the Nursing Supdt. and assist her in the administration of nursing services in the hospital.
Asstt. Nursing Supdt, is responsible to Deputy Nursing Supdt. for the total nursing care of patients, management and development of the unit assigned to her :
Degree Awarded : None.
Duration : From a few days to Two Years.
Degree Awarded : None.
What is it : Tailored to the needs of the trainees sponsored by government institutions from India and abroad.
How to apply : Please visit the AIIMS website and go to "Academic Section" - "Courses and Training" offered. Duly filled application forms available on the website are to be duly forwarded by the head of the respective institutions.
The department has been conducting the following courses:
The duration of DM (Therapeutic Nuclear Medicine) and MD (Nuclear Medicine) courses is 3 years whereas the MSc (Nuclear Medicine Technology) course is two years duration. The PhD candidate can submit his/her thesis after 3 years of registration with the approval of the doctoral committee. Normally it takes 3-5 years in completing PhD.
This Programme was started under the leadership of Dr J B Sharma . Fellowship in Urogynecology and Pelvic Reconstructive Surgery was started from 2017 in the department of Obstetrics and Gynaecology. Till now we have trained four fellows. This fellowship has a tenure of 2 years. Various OPD and IPD services are offered to patients. We have specialty Urogynecology clinic on every Wednessday 2pm. In this clinic we are providing services for the patients of complaints with- Urinary and Fecal Incontinence, Diagnosis and conservative management of various pelvic floor disorders, Pelvic Floor Muscle Training, Pelvic floor ultrasound, treatment of recurrent urinary tract infection, Awareness and education regarding perineal care, Female Urodynamics, Painful bladder syndrome, Chronic pelvic pain, Cystoscopy. Apart from theses we are doing dedicated surgeries in our department like Sling surgeries, Burch colposuspension, Tension free tape transobturator tape, Tension free transvaginal tape, Vaginal hysterectomy, Non descent hysterectomy, Anterior colporrhaphy, Posterior colporrhaphy, Perineoplasty, Vaginoplasty, Urogenital fistula repair, Complete perineal tear, Sacrospinous fixation, Sacro colpopexy, Sacro hysteropexy and burch surgeries.
Assisted Reproductive center, All India Institute of Medical Sciences, New Delhi
“Achieving motherhood is right of every woman”
Since the inception of an idea of medical institute of national importance and excellence, the foundation of All India Institute of Medical Sciences has provided relief to millions of patients suffering from various ailments. Keeping up with the world pace in research and modern teaching, the institute in-houses state of art Assisted reproductive center (ART) center with comprehensive facilities providing safe and advanced treatments options to infertility issues.
Since 2007, thousands of distressed couples have achieved their dream of parenthood. The staff of renowned clinicians and reproductive specialists are passionate and dedicated towards their work and caters to the individual needs in their fertility journey. The years of experience promotes evidence-based medicine and encourages personalized treatment for every patient as each provide a unique learning opportunity.
The ART center has revolutionized the patient care by providing cost effective and easily accessible amenities to millions of grief-stricken couples. It caters to the need of entire north India and receives several referrals from various remote regions of adjoining states.
The multidisciplinary team is led by experienced consultants (Reproductive specialists) with Fellows, Senior residents, Embryologists, nurses, OT and Laboratory technicians, Nurses, Counselor each essential to the team function. Our center offers an array of infertility procedures including ovulation induction, Intra-uterine insemination (IUI), Semen analysis, Intracytoplasmic sperm injection (ICSI), surgical retrieval of sperms, assisted hatching, cryopreservation, fertility preservation, fertility enhancing surgeries, and now Embryoscope, which is latest incorporation at our center. The trailblazing does not end here as we are in process of performing Pre-implantation genetic testing for our patients.
The institute is well renowned for being premier in education and training. This is the pioneer institute in introducing super-specialty courses in field of reproductive medicine. The highly qualified faculty has a niche in training the next generation of reproductive specialists. The curriculum is comprehensive and believes in hands on training and learning. Our commitment towards patient care and continuing medical education & research is reflected by production of skilled trained doctors at par with international standards.
Research is elemental and essential part of continuing medical education. Our centre has international reputation in research and innovation with hundreds of publications in peer -reviewed indexed journals. Under the mentorship of the senior consultants, the trainees develop critical appraisal, analytical thinking and metier in biomedical research.
Excellence comes with planning. What we see today as a premier institute was the vision of Jawaharlal Nehru. Continuing on his envisioned dream, the Department of Obstetrics and Gynaecology was established in the year 1958 under the aegis of Dr P K Malkani.
Since then our mission is to provide comprehensive, evidence based but patient-centred care to overall improve the well being of women through all stages of life. Our didactic and trained faculties aim at continuing medical education and maximizing the learning potential of their residents and students in a stimulated environment. We believe and advocate hands on skill training and strive to create an environment where residents from diverse backgrounds gain skills and experiences from all realms of this multifaceted field. Furthermore, our team of intellectually curious and highly motivated individuals aims at pioneering in innovative research so as to contribute in transforming the way we see medicine.
The department has a state of the art set up and expertise in the fields ranging from managing high-risk pregnancies, maternal-fetal medicine, gynaecologic oncology, reproductive medicine, urogynaecology, and minimally invasive surgery. Therefore the department offers three years of super-speciality residency in Reproductive Medicine and Gynecologic Oncology and run a fellowship program in Fetal Medicine, Minimally Invasive Surgery, and Uro-gynecology.
Over the years, the gynaecologic surgery has evolved from primary abdominal approach to the current focus on minimally invasive gynaecological surgery. It is one of the greatest surgical innovations revolutionizing the management of many gynae operative cases endoscopically. The Minimally Invasive Gynaecological Surgery division of AIIMS, New Delhi is currently being led by senior Professor and unit head Dr K. K. Roy. We have a dedicated, hard-working team of expert gynae endoscopic surgeons who strive to provide a safer and an effective alternative to traditional open surgery. With the availability of wide range of endoscopic instruments, equipments and electrosurgical generators, we are able to provide the best care to the patients. Surgeries performed range from simple office hysteroscopy to operative hysteroscopy and diagnostic minilaparoscopy to all major laparoscopic surgeries including malignancies. Around 150-170 endoscopic surgeries are performed in each month. Minimally invasive surgeries offer various advantages to patients like reduced pain, less bleeding, shorter hospital stay and early postoperative recovery. Patients undergoing diagnostic procedures are discharged after two hours of the procedure and those undergoing operative procedures are usually discharged on the second or third day of surgery depending upon the surgical procedures. We keep ourselves updated with the latest research and regularly conduct workshops and CMEs. Various research studies are done every year pertaining to minimally invasive gynae surgery. The division is being credited with more than 200 publications in indexed national and international journals.
A two years fellowship program is offered in the domain through an entrance exam of AIIMS conducted twice in a year (January and July), Admission is based on a two-stage evaluation process i.e. written test and departmental clinical/practical assessment. MD/MS in Obstetrics and Gynaecology with 3 years teaching experience is the eligibility criteria for fellowship. It is a comprehensive academic program and squarely covers the clinical, research and surgical aspects related to the domain. A research project is undertaken by the selected candidate during his/her tenure. Our goal is to further develop the skills of budding gynae endo-surgeons. Five candidates have completed fellowship so far and are serving different parts of the country. Our further goal is to achieve more advanced endoscopic surgery in the same roof for excellent patient care in Minimally invasive gynae surgical procedure.
The services provided by the division of Minimally invasive gynaecological surgery includes:
Hysteroscopic surgeries:
Office hysteroscopy/ diagnostic hysteroscopy
Operative hysteroscopy: myomectomy, polypectomy, septal resection, embedded Cu T removal etc.
Laparoscopic surgeries:
Diagnostic laparoscopy
Operative laparoscopy: hysterectomy, myomectomy, surgeries for endometriosis, cystectomy, abdominal cerclage, ovarian drilling, surgery for ectopic pregnancy, surgeries for MRKH etc.
Maternal Fetal medicine program within the Department of Obstetrics and Gynaecology, at All India Institute of Medical Sciences New Delhi is known for its excellent team, respectful patient care and state of the art infrastructure with advanced ultrasound machines, LASER therapy and Radiofrequency ablation therapy. We reported the first case of intrauterine laser surgery for fetal bronchopulmonary sequestration successfully performed in India. It was established under the leadership of Professor Kamal Buckshee. Over the years the division has grown keeping pace with the ever-increasing advances in the field of Fetal Medicine. In addition to providing quality care to the patients, the division is also actively involved in advanced research in fetal diagnostic and therapeutic procedures. We aim to serve all sections of the society with equal respect and care keeping medical etiquettes and ethics in mind. Our team believes in continuously auditing and introspecting our own management to give the best services to our patients and engrave the idea of quality care in our trainees. We continuously update ourselves in the latest developments in the field by conducting continuous CMEs, Webinars, and seminars. We have published over 60 research papers in indexed international and national journals. We have teamed up with the Division of Medical Genetics (Department of Pediatrics) AIIMS for counselling of the parents and for prenatal genetic testing to provide best possible care to expecting couples for a healthy baby. We offer 1 year fellowship programme and long term observership programme based on eligibility criteria and an entrance examination. More than 15 candidates have completed fellowship and observership from our centre and are providing services in the field of Fetal Medicine in different parts of the country.
Diagnostic Procedures
Therapeutic Interventions
USG Scanning Facilities
Special
High risk Pregnancy Care
Multidisciplinary team management of pregnancies with high risk background maternal conditions
Out-patient department
High-Risk Pregnancy Clinic
High-Risk Pregnancy Clinic
Please take an online appointment for any of the consultants and make an OPD card through the Patient reception Centre for Wednesday or Saturday. Often a genetic consultation is taken before the procedure . Once that is done the procedures are performed on Mondays and Thursdays .
For emergency consultations, kindly send an email on fetalmedicineaiims@gmail.com
“It is possible not just to survive ,but to thrive and live a healthy life again”
It is with this theme that gynae oncologists in the Department of Obstetrics and Gynaecology are relentlessly working and making patients suffered from cancer to make this dream true. Under the leadership of Professor Neerja Bhatla, who herself is an international icon and well-renowned gynae-oncologist, this branch has flourished over the years to provide optimal cancer care.
Gynae oncologists are well-trained specialists to provide cancer screening and treatment services to patients with any type of gynaecological malignancies like cervical cancer, ovarian, uterine, vaginal or vulval cancer etc.
Comprehensive preventive and evidence-based treatment services- Our team of well-trained gynae oncologists is involved in providing comprehensive cancer care with multidisciplinary team-approach involving expert pathologist, radiologist, medical oncologist , radiotherapy and palliative care. We follow stepwise evidence- based approach to evaluate patients, providing appropriate treatment, performing surgeries with expertise, expediting adjuvant treatment , providing life-long follow-up facilities at specialized clinic and overall improving the quality of life of cancer-affected females. Advanced treatment modalities like HIPEC are also available.
Specialized teaching and training- Apart from high-quality patient care, the Department is also running a well-structured MCh programme in gynae oncology with highly-qualified faculty. This comprehensive course is aimed to provide best learning and hand-on-training to next-generation gynae-oncologists. The students who are trained have achieved excellence in this field at national and international level and serving the country by their services.
Research and innovations – As a part of continuing medical education, our centre is also well-known for performing cutting-edge research in gynae-oncology. Ongoing research addresses various issues like basic molecular research in different gynae cancers, innovations in surgical techniques and perioperative care, translational research etc .
Thursday 2 to 5 pm
UNIT I: Prof Reeta Mahey
UNIT-II: Prof. Neena Malhotra
Unit-III: Prof Neeta Singh
Step I- Make an OPD Card under Obst. And Gynecology from Registration Counter located at Rajkumari OPD, Ground Floor, Main Hospital,AIIMS
Step II- After Pre-Investigations and screening for infertility in the morning General OPD Schedule patient will be referred for IVF Facilty-ART Clinic
Step III- Registration for treatment under IVF Facility in ART Clinic on Thursday
| Name | Designation |
| Dr. Neena Malhotra | Professor, Deptt.of Obst. & Gynae |
| Dr. Neeta Singh | Professor, Deptt. Of Obst. & Gynae |
| Dr. Reeta Mahey | Associate professor, Deptt. Of Obst. & Gynae |
Chief embryologist :
Assitant Embryologist :
Lab technician :
Lab Assistant:
OT technician :
Store incharge:
MSSO/Counsellor :
Radiographer :
Nursing Staff:
AIIMS IVF centre is renowned for clinical excellence, technological leadership, process excellence, quality, superior patient care, world class facilities, consistent high success rates and transparency for last 10 years. It is renowned for its expert team, state-of-the-art infrastructure and lab, therapeutic and equipment, continuous research on newer technologies and treatment protocols. Our aim is to serve all sections of the society with equality. We provide the complete evaluation to infertility under one roof, with highest moral and ethical values.
The clinicians at AIIMS IVF facility have been trained at one of the best IVF centres in the world. The team comprises of clinicians, fellows, registrars, embryologists, lab technicians, OT technicians and nursing staff.
We believe in continuously updating ourselves in knowledge and skills by visiting the best centres in the world and inviting experts from best centres of the world for exchange of knowledge and technique.
Our team believes in continuously auditing and evaluating our own results to be able to give the best services and results to our patients. Our centre is engaged in cutting edge research. The centre has published more than 50 international papers. Our IVF facility is unique in that it provides all services under one roof, treatment of fertility to conception to delivery. We have also recently started super-speciality course in Reproductive Medicine since January 2017.
AIIMS IVF centre offers both male and female infertility treatments. The treatment canvas consists of the following:
Making the decision to have a child is momentous. It is to decide forever to have your heart go walking around outside your body. ~Elizabeth Stone
Over the last few years, the department has grown emulating with the ever-increasing advances in the field of medicine. Currently the department has a state of the art set up and expertise with various subspecialities to cater the needs of the population and to continue medical education and research in the best possible way.
The Division of Gynaecological oncology is led by Professor Neerja Bhatla. Apart from providing basic training to the postgraduates and senior residents, the division also provides 3 years MCh course in gynaecological oncology. All cancer patients are managed by Multidisciplinary team with active involvement of Medical oncologists and Radiation oncologists of the institute. The division also provides services for gynaecological cancer patients at NCI Jhajjar.
The division is headed by Professor Vatsla Dadhwal. The division has a close liaison with division of Medical genetics, Pediatric cardiologists and Pediatric surgeons for a comprehensive management and follow up affected pregnancies from intrauterine period to post-natal life. The division provides 1 year fellowship course and long term observership to trainees on management of high-risk mothers and fetuses, fetal ultrasound and invasive procedures.
The division currently led by Professor Garima Kachhawa . It provides 2 years fellowship program for trainees.
The division is renowned for its expert team, state-of-the-art infrastructure and equipment, continuous research on newer technologies and treatment protocols. It is the first Government run IVF center in India. It provides 3 years DM program for trainees.
Experts with enormous experience and expertise run the division. It has a close liaison with the department of urology for training of trainees and comprehensive patient management. The division provides 2 years fellowship course for trainees.
The department offers short term and long term training to qualified individuals from India and abroad. Application forms can be obtained from the office of the Registrar, AIIMS. A prior approval of the head of the department and concerned faculty is required before applications are accepted.
The department regularly conducts workshops in the field of Gynaecology Endoscopy, Gynaecological Oncology, Urogynaecology and Fetal Medicine.
The Department of Obstetrics & Gynaecology is recognized centre mother and child health and offers various courses for the training of undergraduates, postgraduates, senior residents. It offers courses of DM, MCh, fellowships and observerships in various subspecialities of gynaecology.
MD (Obstetrics & Gynaecology): The recruitment occurs twice a year in January and July through an all India entrance examination. It is of 3 years duration.
Senior residents: The selection of senior residents is done twice a year in January and July. It is a two step process consisting of multiple choice questions based theory examination followed by interview/clinical assessment by the department. It is for a maximum duration of 3 years post MD.
Subspecialities: The department offers various other courses in different areas of gynecology including DM in reproductive medicine, MCh in Gynaecological Oncology, fellowships in Maternal Fetal Medicine, Minimally invasive surgery and Urogynaecology. The admission to these courses is conducted twice a year in January and July through a written examination followed by clinical assessment/interview by the department.
Our vision is to be the Center of Excellence for Women’s health providing superlative care with Dignity and Respect
Our mission is to strive towards providing holistic care of women throughout her life through excellence in:
Patient Care: Providing state-of-the art care across subspecialities of obstetrics and gynaecology which is driven by evidence, accessible, equitable and affordable
Education: Educating next generation of professionals in the science (Knowledge), craft (Skill) and art(attitude) in the field while inculcating the values of respect, collaborative learning, and innovation in teaching
Research: Inspiring a culture of intuitive, iterative, and translational research directed at improving the health of women at large
Quality: Ensuring that services are effective; safe; people-centred; timely; equitable; integrated; and efficient.
We are committed to providing:
Enabling environment for personal and collective growth
Patient centered care with involvement of woman and family in decision making
Collaborative learning within the country and across countries
Responsive and supportive management laying down a framework for progress
| NAME | ADDRESS | CONTACT NUMBERS | E-MAIL Ids |
|---|---|---|---|
| A SRINIVASA RAO | 401 SAI JYOTHI PALACE,1-4-879/49 GANDHINAGAR,HYDERABAD-500080 | 040-27643663, 09440966555 | - |
| ABHIJIT DEY | A-1/278 SUSHANT LOK-2 SEC-55,GURGAON-122001,HARYANA | 9811161663 | - |
| ALFZNDDNB KR | OLD HOSPITAL ROAD,CHIMSURRAH HOOGHLY,WB | 0983134704(M) | - |
| ANIL K UAHANTA | 13 RAJGARH ROAD,ANI NAGAR,GUOHATI,ASSAM | 0361-2523816 | - |
| ARVIND JAISWAL | Q-5 MODEL TOWN,DELH-110029 | 011-26196448 | - |
| ASHOK KUMAR | 3221 GROUND FLOOR,PKT B &C SEC-A, VASANT KUNJ,NEW DELHI | 9891650445 | - |
| B S SAHOTA | E 306 GK II NEW DELHI-48 | 9810226675 | - |
| BHAVUK GARG | 63 A DEVPURAM,GANETU COLONY,MUZAFFAR NAGAR,UP-251001 | 0131-2412300, 09899558021 | - |
| C S YADAV | AIIMS | 9868479933 | - |
| D K GHOSE | 415 NAMBARI MALIGAON,GUWAHATO-II | 2571299, 09435108331 | - |
| DEBABRATA BANERJI | BABUBAG,PO-RAJBARI,BURDWAN-7131004 | 094331-24782 | - |
| DHARMESH L KHATRI | RAMDAS PATN,STATION ROAD,AKOLA-444001 | 9899558016, 0724-2441614 | - |
| DILIP GOPALKRISHNAN | 81/1 EAST ANJANEYA TEMPLE ROAD,BASAVANAGRDI,BANGLORE-560004 | 9844007999 | - |
| DIPEN K MENON | WARREH HILL X HOUSE(1st FLOOR) KETTERING GENERAL HOSPITAL,ROTHWELL ROAD,KETTERING NN16 8UZ | 07811312163(M) | - |
| FAROOQUE | RAJGARH ROAD,GUWAHATI-3,ASSAM,GAUHATI MEDICAL COLLEGE | 011-26977815 | - |
| G K AGGARWAL | - | 9810273150 | - |
| GOUTAM SAHE | KOLKOTA,UD-05-0908// 1050/1 SURVEY PARK,KOLKOTA-700016 | 9830047247 | - |
| H A RAJU | P O BOX 3390 SAFA 13034 NEW DAR AL SHIFA HOSPITAL, KWAIT | 00965-5635174, 00965-7202594 | - |
| HANS NAGAR | C 6/7 SDA NEW DELHI-110016 | 9811222359 | - |
| HARSH KUMAR JOHRI | 7 HARDWAN ROAD,DEHRADUN | 0135-2621071, -2621685 | - |
| IBOMCHA THOKCHOM | INPAL MANIPUR | 9436026045 | - |
| J K MANCHANDA | 16/1 2nd FLOOR ASHOK NAGAR,NEW DELHI-110018 | 9810295335, 01125408736(R), 011-65457232(C) | - |
| J P MANOCHA | B-4/218,SAFDARJUNG ENCLAVE,NEW DELHI-1100029 | 011-26108151, 011-26188151, 09811087322 | - |
| JITENDRA MAHESHWARI | F-7 EAST OF KAILASH,KNEE & SHOULDER CLINIC,NEW DELHI-110065 | 011-26286868/69, 9811668866, 9811109833 | - |
| K SUDHIR REDDY | 85 CLAYHILLS DRIVE,DUNDEE DD2 1SG,UNITED KINGDOM | 00447753767502, 08772241519 | - |
| KAMRAM FAROOQUE | 12 G SEC-8,JASOLA VIHAR,NEW DELHI-110029 | 011-26163138, 09811229136 | - |
| KARTHIK SELVARAJ MURUGAPPAN | SNP GARDENS,KURALKUTTAI,PO COIMBATORE DT,TAMIL NADU-642154 | 9968264294, 04252-223674 | - |
| KAUSHIK | - | 9968264294 | - |
| KINTOO DOOMRA | D-23 KALKAJI,NEW DELHI-1100019 | 011-26222277, 09810188582 | - |
| KOOLAM CHANDRA SEKHAR | 410 SARASWATHI RESIDENCY,PADMARAO NAGAR,SECUNDERABAD,A.P. | 09848052245, 09440444474 | - |
| KRISHNA KIRAN E | 17-1-383/N/25 NAGARJUNA COLONY,NEAR CHAMPAPET,HYDERABAD-500079 | 9848074511 | - |
| KULTAR SINGH MALHOTRA | - | 9313361745 | - |
| L L SHAH | TRIBHUWAN UNIVERSITY,TEACHING HOSPITAL,KATHMANDU,NEPAL | 9851073187 | - |
| M F RAHMAN | - | 9810115700 | - |
| M J NAIDU | M V S ACCIDENT HOSPITAL,VIJAY AWADA | 9392935354 | - |
| MAHESH B H | 209 BIJJAWARA,DERANAHALLI TALUA,BANGALORE-562110 | 9341227262 | - |
| MANOJ MIGLANI | F-22/153,SEC-3,ROHINI,NEW DELHI-110085 | 09873337444, 09810381700 | - |
| MUKESH JAIN | MUZAFFAR NAGAR | 9837038437 | - |
| N DEEPAK KACHHAP | 4C/1113 BUKARO STEEL CITY,JHARKHAND-827004 | 06542-233322, 09431739255 | - |
| NARESH KUMAR | 3 STOCKBRIDGE CLOX WIGHTWICK,WOLVERHAMOTON,WVEBBU,UK | 0044-7818434147(M) | - |
| NARESH PRAKASH | SDM HOSPITAL,JAIPUR-302015 | 9829399818 | - |
| PARMESSUR RAMLOLLOO | 3 TRAIT D UNION,VACOAS,TAURITIUS | 6989073 | dr@ramblloog |
| PRAVIN NEPAL | B P KOIRALA INSTITUTE OF HEALTH SCIENCES,GHOPA CAMP,DHAWAN,NEPAL | 9842040503 | - |
| PREM KUMAR V | ABHILASH HOUSE,CHERUMUKKU TEMPLE ROAD,CHEMBOOKAVU,THRISSUR-680020,KERALA | 09447778422, 0487-2330534 | - |
| R K KAPOOR | BLOCK C4C PKT 14 FLAT NO.223 JANAK PURI,NEW DELHI-110058 | 011-25503078, 09810056077 | - |
| R K RASHBIHARI | PURANA RAJBANI,NARGMUBING | 9436025840 | - |
| R NATARAJAN | 22 RIDGEWAY,NORTHAMPTON,NN3 3AN,UK | 441604400028, 447879498814(M) | - |
| RAJIV BAJEKAL | 34KINGWELL ROAD,HADLEYWOOD,BARNET ENGOHY | 7753748061 | - |
| RAVI MITTAL | 2 C ,DDA FLATS,MIG,RAJOURI GARDEN,NEW DELHI | 981017006 | - |
| RAVI MITTAL | 2 C ,DDA FLATS,MIG,RAJOURI GARDEN,NEW DELHI | 981017006 | - |
| RITABH KUMAR | 70 MUNIRKA VIHAR,OPP.JNU.NEW DELHI-110067 | 011-26168164, 9818068073 | - |
| S C SAHU | SAHU HOSPITAL,ST.JOHN's CROSSING,M G ROAD,AGRA(UP) | 9837043377 | - |
| S K DEWAN | SIKKIM HIMALAYAN NURSERY,DEVELOPMENT AREA,GANKTOK,SIKKIM | 9434103698 | - |
| S K KAME | C9/9044 J VASANT KUNJ,NEW DELHI-110070 | 011-2689-4199, -4399 | - |
| S P MANDAL | - | 9312635885, 9810000000 | - |
| SAMEER NARANJE | 618, NEW SUBHEDARLAYOUL,NAGPUR-440024 | 9899419087 | - |
| SANJAY KUMAR SUREEN | 7 MARLECROFT CLOSE,MANCHESIER M23 1DB | 447863161650 | - |
| SANJAY MADAN | - | 9810078483 | - |
| SANJEEV KUMAR BHUYAN | GAUHATI MEDICAL COLLEGE,GAUHATI-781032// NIZARAPAR ROAD,H.NO:26,SILPUKIHIRI,GUWAHATI-781003 | 0361-2664934, 09864063811 | - |
| SANTOSH RATH | F 35/A BJB NAGAR,BHUBANESWAR-751014 | 09437035656, 06742435682 | - |
| SATISH CHOUDHRY | 971/28,JATAL ROAD,PANIPAT | 989689655 | - |
| SATISH KUMAR SHARMA | C-1 SEC-15 PART-1 GURGAON-122001 | 9811047339, 95124-2309240 | - |
| SAURABH SINGH | - | 9911457745 | - |
| SHAH ALAM KHAN | FLAT 704 FTA,A V NAGAR,KHEL GAON ROAD,NEW DELHI-110049 | 011-26266330 | - |
| SHANTANU LAHKAR | ARUNANA TRAUMA & ORTHOPAEDIC HOSPITAL & RESEARCH CENTRE,PALTAN BAZAR,DIBRUGAH-786005,ASSAM | 9435031036 | - |
| SHARAT AGARWAL | G-18 KARAMYOGI ENCLAVE,KAMLA NAGAR,AGRA | 9412456328, 0562-2581700 | - |
| SHISHIR RASTOGI | C-II/13 ANASARI NAGAR,NEW DELHI-110029 | 011-26594533 | - |
| SOURAV SHUKLA | - | 447708436387 | - |
| SUJIT KUMAR NANDI PURKAYA | BELTOLA MEHERPUR,SILCHAR-788015,ASSAM | 03842-240096, 09435174496 | - |
| SURESH RAO | THE OLD CARAGE,BRIGHAM,COCHERMOUTH CUMBOUA,CA13 OXG UK | 1900827335 | - |
| TULSI BHATTACHARYYA | RAJGARH ROAD,GUWAHATI-3,ASSAM,GAUHATI MEDICAL COLLEGE | 03612456409(R), 09864091601(M) | - |
| U C SHARMA | BASHISTHAPUR,BYE LANE 2 WIRELESS,GUWAHATI-781028 | 09435114898, 0361-2223055 | - |
| V K GARG | G-19A, KALKAJI,N.DELHI-110019 | 011-26422934, 011-26226607, 09810431460 | - |
| V K SHARMA | C-263 PLOT NO.2 SCE-11,DWARKA//D-II/113 KIDWARI NAGAR WEST.N.DELHI | 011-26887350, 9810213216 | - |
| VIKAS GUPTA | SEC-26 B21 B NOIDA UP | 9312371941, 9818000000 | - |
The physiotherapy unit is functional from Monday to Saturday. All the patients referred form the OPD are assessed on the same day and called directly for follow-up visits without any registration requirement.
The physiotherapy of indoor patients is also carried out.
Hydrotherapy is an important wing of physiotherapy taking special care of systemic conditions. Modalities available are steam bath, whirlpool bath and tread mill.
| Names | Post |
|---|---|
| Mr. Sunil Kumar Singhal | Supdt. Physiotherapist |
| Mr. Jagdish Pandey | Sr. Tech Officer |
| Mr. Devender F Ramteke | Supdt. Occupational Therapist |
| Mr. Shailesh Kumar Singh | Sr. Physiotherapist |
| Mrs. Neetu Sharma | Physiotherapist |
| Mr. Ajit Kumar | Physiotherapist |
| Ms. Nidhi Bhatia Sachdev | Physiotherapist |
| Ms. Priyanka Aggarwal | Physiotherapist |
| Mr. Amit Kumar | Yoga Instructor |
| Ms. Divya | Jr. Physiotherapist |
| Mr. Abdul Basit | Jr. Physiotherapist |
| year 1962 | ||
| December-62 | Dr. | Kasturi Lal Sawhey |
| Year 1963 | ||
| May-63 | Dr. | Inderjeet Singh Sindhu |
| Dec-63 | Dr. | Brij Mohan Lal Abrol |
| Dec-63 | Dr. | Jiten Kumar Kanjilal |
| Dec-63 | Dr. | Randhir Singh Sangwan |
| Dec-63 | Dr. | Inder Prakash Kohli |
| Year 1964 | ||
| Dec-64 | Dr. | Hari Charan Samant |
| Dec-64 | Dr. | D.N.Mehta |
| Dec-64 | Dr. | Perbodh Chander Sagar |
| Year-1965 | ||
| Dec-65 | Dr. | Krishan Kumar Aggrawal |
| 24077 | Dr. | Sat Prakash |
| Dec-65 | Dr. | Vidya Parkash Sood |
| Dec-65 | Dr. | Udaykant vinodchandra Dave |
| Dec-65 | Dr. | Jagjit Singh |
| Dec-65 | Dr. | Tej Mohan Singh Saluja |
| Year-1966 | ||
| Dec-66 | Dr. | Khagendranath Pramanik |
| Dec-66 | Dr. | Manohar Lal Gulati |
| Dec-66 | Dr. | Surinder Mohan Seth |
| Dec-66 | Dr. | Barin Kumar Roy Chaudhari |
| Dec-66 | Dr. | Bhupindra Krishna |
| Dec-66 | Dr. | Satish Chander Pandhi |
| Year-1967 | ||
| May-67 | Dr. | Promod Lal Bhatia |
| May-67 | Dr. | P.G.Visvanathan |
| May-67 | Dr. | Ravinder Kumar Saxena |
| Year-1968 | ||
| Dec-68 | Dr. | Shankar Das Gupta |
| Year-1969 | ||
| May-69 | Dr. | Lal Mohan Ghosh |
| May-69 | Dr. | Kuldeep Singh Dang |
| May-69 | Dr. | Narender Nath Dutta |
| May-69 | Dr. | Waman Rao Jadhar |
| Year-1970 | ||
| May-70 | Dr. | Gautam Das Gupta |
| May-70 | Dr. | Mahendra Singh Rohatgi |
| May-70 | Dr. | Suraj Prakash Batra |
| May-70 | Dr. | Deo Krishna Chandak |
| May-70 | Dr. | S.Krishnamoorthy |
| May-70 | Dr. | Vishwanath Chaturvedi |
| Year-1971 | ||
| May-71 | Dr. | Parkash Singh Devgan |
| Dec-71 | Dr. | Kali Prasad Saikia |
| Year-1972 | ||
| May-72 | Dr. | Ramaprasad Sen Gupta |
| Dec-72 | Dr. | M.Raveendran |
| Year-1973 | ||
| May-73 | Dr. | P.Shivananda Maiya |
| May-73 | Dr. | N.Balakrishna Pillai |
| Dec-73 | Dr. | Narender Kumar Goyal |
| Dec-73 | Dr. | Rajani Kanta Deka |
| Year-1974 | ||
| May-74 | Dr. | Asit Kumar Chattopadhyay |
| May-74 | Dr. | Gurdip Singh |
| Year-1975 | ||
| Jan-75 | Dr. | M.L.Sharma |
| Jan-75 | Dr. | Ramesh Chandra Deka |
| Jan-75 | Dr. | Sudesh Kumar Ahuja |
| Apr-75 | Dr. | Anil Kumar Vithalrao Saraif |
| Sep-75 | Dr. | P.Y.John |
| Year-1976 | ||
| Feb-76 | Dr. | Akhil Chandra Sarma |
| Nov-76 | Dr. | Brahma Parkash Sharma |
| Dec-76 | Dr. | C.Pushpangada Panicker |
| Dec-76 | Dr. | Gurudas Basak |
| Dec-76 | Dr. | P.R.Natarajan |
| Dec-76 | Dr. | Sanasam Jodha Chandra Singh |
| Dec-76 | Dr. | Yashwant Kumar Maru |
| Year-1977 | ||
| May-77 | Dr. | E.R.Balakrishnan Pillai |
| May-77 | Dr. | S.Sasikumaran Nair |
| Dec-77 | Dr. | Bhagwan Singh Dogra |
| Year-1978 | ||
| May-78 | Dr. | Mohan Thomas Pakalomattom |
| May-78 | Dr. | N.Unnikrishnan Nair |
| Dec-78 | Dr. | Chingtham Chandramani Singh |
| Dec-78 | Dr. | Ravinder Kumar Verma |
| Dec-78 | Dr. | Shambhu Nath Mukherjee |
| Year-1979 | ||
| May-79 | Dr. | Ajit Vikram Daharwal |
| Dec-79 | Dr. | Benjamin D'Souza |
| Dec-79 | Dr. | Samarpal Singh Yadav |
| Year-1980 | ||
| Jul-80 | Dr. | Atul Jain |
| Jul-80 | Dr. | M.A.Gopalakrishna |
| Year-1981 | ||
| May-81 | Dr. | Preet Pal Singh |
| May-81 | Dr. | R.N.Patil |
| Dec-81 | Dr. | Ved Vrat |
| Dec-81 | Dr. | Zohra Embrahim |
| Year-1982 | ||
| May-82 | Dr. | Hidangmayaum H. Sharma |
| Dec-82 | Dr. | Ramesh Kaul |
| Dec-82 | Dr. | Rakesh Prasad |
| Dec-82 | Dr. | Rajesh Bhatia |
| Year-1983 | ||
| May-83 | Dr. | Pradeep Shankar Bhat |
| Dec-83 | Dr. | Dev Ashish Tandon |
| Dec-83 | Dr. | Vinod Rai Gondalia |
| Dec-83 | Dr. | B.Girish Rai |
| Year-1984 | ||
| May-84 | Dr. | Ashok Mohan Shenoy |
| May-84 | Dr. | Ramchhaya Man Amatya |
| Dec-84 | Dr. | Juban Gondalia |
| Dec-84 | Dr. | Subramania Iyer K. |
| Year-1985 | ||
| May-85 | Dr. | Mukhesh Sooknundun |
| Dec-85 | Dr. | Brajendra Baser |
| Dec-85 | Dr. | Subirendra Kumar |
| Dec-85 | Dr. | Rama Krishna T.B. |
| Year-1986 | ||
| May-86 | Dr. | Kedolhouvi Longkumar |
| May-86 | Dr. | Gurpal Singh Bindra |
| Dec-86 | Dr. | Jyothi Ramakrishna (Reddy) |
| Dec-86 | Dr. | Pradeep Kumar Narayan |
| Dec-86 | Dr. | Pradeep Kumar Rathore |
| Year-1987 | ||
| Dec-87 | Dr. | Umang Khetrapal |
| Dec-87 | Dr. | Anil Maheshwari |
| Year-1988 | ||
| Dec-88 | Dr. | Anand Kumar Gairola |
| Dec-88 | Dr. | Yassin Pyarali Ghulam H.M. |
| Year-1989 | ||
| May-89 | Dr. | Sanjay K.Bhendwal |
| Dec-89 | Dr. | Ajit Man Singh |
| Dec-89 | Dr. | Sandeep Samant |
| Year-1990 | ||
| May-90 | Dr. | Abdul Rahim Mohd. Hussain A. |
| May-90 | Dr. | Shantanu Mandal |
| May-90 | Dr. | Tosole Khieya |
| Dec-90 | Dr. | Sundeep Mediratta |
| Dec-90 | Dr. | Alok Thakar |
| Dec-90 | Dr. | H.C.Laldina |
| Year-1991 | ||
| May-91 | Dr. | Sanjay Gupta |
| Dec-91 | Dr. | Amardeep Singh Thind |
| Dec-91 | Dr. | Rajan Bhargava |
| Year-1992 | ||
| May-92 | Dr. | Rakesh Kumar |
| Dec-92 | Dr. | Ashutosh Kacker |
| Dec-92 | Dr. | Vineet Jain |
| Year-1993 | ||
| May-93 | Dr. | Vijay Kumar Goel |
| May-93 | Dr. | Semsey Denzongpa |
| Dec-93 | Dr. | Ongden Gyatso |
| Dec-93 | Dr. | Bibhu Pradhan |
| Year-1994 | ||
| May-94 | Dr. | Parmod Kumar Kalsotra |
| Dec-94 | Dr. | Sameer Nivsarkar |
| Dec-94 | Dr. | Subburaman Nagarajan |
| Year-1995 | ||
| Dec-94 | Dr. | Sangita Ramdev |
| Year-1996 | ||
| May-96 | Dr. | Gyanesh Nandan Lal |
| May-96 | Dr. | K.R.Shashi Prasad |
| May-96 | Dr. | Devanand Jha |
| Dec-96 | Dr. | Jemy Jose |
| Dec-96 | Dr. | Sangeeta Harsha Ben |
| Dec-96 | Dr. | Ciba Annie Paul |
| Year-1997 | ||
| May-97 | Dr. | Asmeeta I.Patel |
| Dec-97 | Dr. | Deepak Sarin |
| Dec-97 | Dr. | Abhinit Kumar |
| Dec-97 | Dr. | Toran Bahadur K.C. |
| Year-1998 | ||
| May-98 | Dr. | Sanjeev Gupta |
| May-98 | Dr. | D.V.S.Phani Bhusan |
| Year-1999 | ||
| May-99 | Dr. | Chava Anjaneyulu |
| May-99 | Dr. | Ramesh A. |
| Dec-99 | Dr. | Paramita Baruah |
| Year-2000 | ||
| May-00 | Dr. | Sanjib Kumar Upadhyay |
| May-00 | Dr. | Tarun Guha |
| May-00 | Dr. | M.Dhiwakar |
| Dec-00 | Dr. | Santanu Roy |
| Dec-00 | Dr. | Gagan Kumar |
| Dec-00 | Dr. | Bubul Chandra Roy |
| Year-2001 | ||
| May-01 | Dr. | Venkatakarthikeyan C. |
| Dec-01 | Dr. | Bikas Kumar Sarkar |
| Dec-01 | Dr. | Manish Prakash |
| Year-2002 | ||
| May-02 | Dr. | Sonia Suprabha Venugopal |
| Dec-02 | Dr. | Rishi Pal Gupta |
| Year-2003 | ||
| May-03 | Dr. | Chandreyi Banerjee |
| May-03 | Dr. | Swapan Kumar Ghosh |
| Dec-03 | Dr. | P. Satish Kumar |
| Dec-03 | Dr. | Prateek Panduranga Nayak |
| Dec-03 | Dr. | Harpreet Singh Koccher |
| Dec-03 | Dr. | Abdullah Rafiei |
| Year-2004 | ||
| Dr. | Sharan C.J. | |
| Dr. | Neizekhotuo Brain Shunyu | |
| Year-2005 | ||
| May-05 | Dr. | Purushottam Chavan |
| May-05 | Dr. | Nishant Saurabh Saxena |
| May-05 | Dr. | S.Shyam Kumar |
| Dec-05 | Dr. | Garima Aggarwal |
| Year-2006 | ||
| May-06 | Dr. | Kapil Sikka |
| Year-2007 | ||
| May-07 | Dr. | Mohnish grover |
| May-07 | Dr. | Parul Sinha |
| May-07 | Dr. | Vikas Gupta |
| Dec-07 | Dr. | Chirom Amit Singh |
| Dec-07 | Dr. | Rohit Verma |
| Year-2008 | ||
| May-08 | Dr. | Rajeev Kumar |
| May-08 | Dr. | Jaspreet Kaur |
| Year-2009 | ||
| May-09 | Dr. | C. Preetam |
| May-09 | Dr. | Gaurav Gupta |
| Dec-09 | Dr. | S. Pookamala |
| Year-2010 | ||
| 2010 | Dr. | Richa Vaish |
| 2010 | Dr. | Om Prakash |
| 2010 | Dr. | Prem Sagar |
| Year-2011 | ||
| 2011 | Dr. | Shuchita Singh |
| 2011 | Dr. | Arvind Kairo |
| 2011 | Dr. | K. Darwin |
| 2011 | Dr. | Vishava Yadav |
| Dr. | Ashutosh Hota | |
| Year-2012 | ||
| Dr | Jaini Lodha | |
| Dr | Dillip K Samal | |
| Dr. | Sandeep P.K. | |
| Dr. | Pol Shashikant Anil | |
| Dr. | Konthoujam Shaphaba Singh | |
| Year-2013 | ||
| Dr. | Laxminarasimman P | |
| Dr. | Madan P Gupta | |
| Dr. | Prachi Jain | |
| Dr. | Dillu R Kandel | |
| Dr. | Diva Shrestha | |
| Dr. | Anup Singh | |
| Dr. | P. Lokesh Kumar | |
| Dr. | Devaraja K | |
| Year-2014 | ||
| Dr. | Smriti Panda | |
| Dr. | Kamlesh K Dubey | |
| Dr. | Dhananjay Kumar | |
| Year-2015 | ||
| Dr. | Bhinyaram | |
| Year-2016 | ||
| Dr | Karan Aggarwal | |
| Dr | Vaisakh K | |
| Dr | Sasi K Kavutarau | |
| Dr | Rishikesh Thakur | |
| Dr | Anil Kumar Saini | |
| Dr | Sumanth Bollu | |
| Year-2017 | ||
| Dr | Ramya Thota | |
| Dr | Prateek Sharma | |
| Dr | Amborish Nath | |
| Dr | Sarath Raveendhan | |
| Dr | Jithin C Shaji | |
| Dr | Rijendra Yogel | |
| Dr | Suresh K | |
| Year-2018 | ||
| Dr | Ashwin Chandran C | |
| Dr | Jarapla Naga Nayak | |
| Dr | N Nageshwara Rao | |
| Dr | Anupam Kanodia | |
| Year-2019 | ||
| Dr | Konkimalla Abhilash | |
| Dr | Arshad Zubair | |
| Dr | Mohammed sherif P | |
| Dr. | Nikita Birua | |
| Dr. | Rachit Pokharel | |
| Dr. | Prankur Verma | |
| Dr. | Subagar A.S. | |
| Dr. | Milind Sagar | |
| Year-2020 | ||
| Dr | Smile Kajal | |
| Dr | Nishes Raj Shrestha | |
| Dr | Prazwal Shrestha | |
| Dr | Debadeep Bagchi | |
| Dr | Geetha P. | |
| Dr | Puja Chatterjee | |
Abstracts Published in Journals :
| S. No. | Author(s) of chapter | Chapter title | Name of editor | Name of the book | Edition | City Of Publication | Publisher | Year of publication | First-Last page |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Subirendra Kumar, Alok Thakar | Foreign bodies | Pramod Kalsotra | ENT Emergencies | 1st | Delhi | Jaypee Brothers | 2023 | 75 |
| 2 | Subirendra Kumar, Alok Thakar | Sudden SNHL | Pramod Kalsotra | ENT Emergencies | 1st | Delhi | Jaypee Brothers | 2023 | 187 |
| 3 | Anup Singh, Kapil Sikka, Alok Thakar | Bilateral Neuropraxic vocal cord palsy after total thyroidectomy | V. Narenderakumar, V. Felix, V. Mariappan | 100 Complications in Otorhinolaryngology and Skull Base Surgery | 1st | Germany | Thieme | 2023 | 287-289 |
| 4 | Sikka K, Tyagi P | Hearing Screening | Ramesh Agarwal, Ashok Deorari, Vinod K Paul, M Jeena Sankar, Anu Sachdeva (eds) | Protocols I Neonatology | 1st | Delhi | CBS Publishers and distributors | 2023 | 394-399 |
| 5 | Sagar P, Thakar A, Samant S | Otorhinolaryngology. | Paul VK, Bagga A | Ghai Essential Pediatrics | 10th Ed | New Delhi | CBS Publishers & Distributors | 2023 | 379-394 |
| 6 | Jaiswal A S, Sagar P | Stridulous child | Thakar A | ClinicalKey Now | 1st | App based | Elsevier | 2023 | |
| 7 | Hitesh Verma | ANATOMY OF EAR AND PHYSIOLOGY OF HEARING | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 3-11 |
| 8 | Hitesh Verma | HEARING EVALUATION | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 12-20 |
| 9 | Hitesh Verma | DISEASES OF EXTERNAL EAR | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 21-29 |
| 10 | Hitesh Verma | EUSTACHAIN TUBE FUNCTION TEST AND OTITIS MEDIA | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 30-36 |
| 11 | Hitesh Verma | TYMPANIC MEMBRANE ANATOMY, DISEASES AND MYRINGOPLASTY | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 37-43 |
| 12 | Hitesh Verma | COMPLICATIONS OF MIDDLE EAR INFECTION | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 44-49 |
| 13 | Hitesh Verma | COM, CHOLESTEATOMA, TYMPANOPLASTY | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 50-57 |
| 14 | Hitesh Verma | MASTOID SURGERIES | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 58-64 |
| 15 | Hitesh Verma | OTOSCLEROSIS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 65-71 |
| 16 | Hitesh Verma | FACIAL NERVE | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 72-82 |
| 17 | Hitesh Verma | SNHL, CAUSES, EVALUATION AND MANAGEMENT | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 83-92 |
| 18 | Hitesh Verma | ANATOMY AND TUMOR OF TEMPORAL BONE | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 93-98 |
| 19 | Hitesh Verma | TINNITUS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 99-102 |
| 20 | Hitesh Verma | DD FOR EAR SYMPTOMS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | ||
| 21 | Hitesh Verma | ANATOMY AND PHYSIOLOGY OF VESTIBULE & VERTIGO | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 109-118 |
| 22 | Hitesh Verma | EXAMINATION OF EAR | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 119-128 |
| 23 | Hitesh Verma | EAR INSTRUMENTS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 129-138 |
| 24 | Hitesh Verma | ANATOMY OF NOSE | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 139-145 |
| 25 | Hitesh Verma | ANATOMY OF NASAL CAVITY PROPER | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 146-152 |
| 26 | Hitesh Verma | PHYSIOLOGY OF NOSE | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 153-158 |
| 27 | Hitesh Verma | ACUTE AND CHRONIC RHINOSINUSITIS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 159-166 |
| 28 | Hitesh Verma | ALLERGIC RHINITIS, VASOMOTOR RHINITIS AND FUNGAL RHINOSINUSITIS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 167-175 |
| 29 | Hitesh Verma | COMPLICATIONS OF SINUSITIS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 176-180 |
| 30 | Hitesh Verma | ANATOMY OF NASAL SEPTUM, SEPTAL SURGERIES AND COMPLICATIONS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 181-186 |
| 31 | Hitesh Verma | EPISTAXIS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 187-193 |
| 32 | Hitesh Verma | FACIAL TRAUMA | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 194-198 |
| 33 | Hitesh Verma | CSF RHINORRHEA, CHOANAL ATRESIA, MUCOCELE AND DACRYOCYSTITIS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 199-205 |
| 34 | Hitesh Verma | ORBIT AND OPTIC NERVE | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 206-210 |
| 35 | Hitesh Verma | GRANULOMATOUS DISEASES OF NOSE | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 211-215 |
| 36 | Hitesh Verma | BENIGN LESIONS OF NOSE AND PNS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 216-222 |
| 37 | Hitesh Verma | MALIGNANT LESION OF NOSE &PNS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 223-228 |
| 38 | Hitesh Verma | COMMON SURGICAL APPROACHES FOR SINONASAL LESIONS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 229-235 |
| 39 | Hitesh Verma | OSA | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 236-240 |
| 40 | Hitesh Verma | EXAMINATION OF NOSE & INSTRUMENTS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 241-252 |
| 41 | Hitesh Verma | ANATOMY OF ORAL CAVITY AND PHARYNX | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 253-259 |
| 42 | Hitesh Verma | SWALLOWING AND DYSPHAGIA | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 260-264 |
| 43 | Hitesh Verma | DISEASES OF ADENOID & TONSILS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 265-274 |
| 44 | Hitesh Verma | BENIGN LESIONS, INFLAMMATORY LESION AND PREMALIGNANT LESION OF THE ORAL CAVITY | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 275-281 |
| 45 | Hitesh Verma | MALIGNAN T LESION OF THE ORAL CAVITY | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 282-290 |
| 46 | Hitesh Verma | MALIGNANT LESION OF OROPHARYNX | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 291-295 |
| 47 | Hitesh Verma | NASOPHARYNGEAL PATHOLOGIES | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 296-300 |
| 48 | Hitesh Verma | EOSPHAGEAL PATHOLOGIES | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 301-308 |
| 49 | Hitesh Verma | SALIVARY GLAND ANATOMY & DISEASES | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 309-320 |
| 50 | Hitesh Verma | ANATOMY AND PHYSIOLOGY OF LARYNX | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 321-329 |
| 51 | Hitesh Verma | SPEECH AND NEUROGENIC DISORDERS OF LARYNX | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 330-337 |
| 52 | Hitesh Verma | ACAUTE AND CHRONIC LARYNGITIS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 338-343 |
| 53 | Hitesh Verma | BENIGN LARYNGEAL LESIONS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 344-350 |
| 54 | Hitesh Verma | LTT AND STENOSIS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 351-357 |
| 55 | Hitesh Verma | AIRWAY OBSTRUCTION STRIDOR AND EXAMINATION OF AIRWAY | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 358-367 |
| 56 | Hitesh Verma | TRACHEOSTOMY | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 368-377 |
| 57 | Hitesh Verma | LARYNGEAL AND HYPOPHARYNGEAL CANCER | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 378-389 |
| 58 | Hitesh Verma | INSTRUMENTS FOR ORAL CAVITY, PHARYNX AND ESOPHAGUS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | |||
| 59 | Hitesh Verma | ANATOMY OF NECK, NECK SPACES AND INFECTIONS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 397-405 |
| 60 | Hitesh Verma | EXAMINATION OF NECK & NECK MASSES | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 406-414 |
| 61 | Hitesh Verma | NECK TRIANGLES, LEVEL OF LYMPHNODES AND NECK DISSECTION | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 415-421 |
| 62 | Hitesh Verma | THYROID GLAND, NODULE AND GOITRE | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 422-432 |
| 63 | Hitesh Verma | FOREIGN BODIES IN ENT | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 433-438 |
| 64 | Hitesh Verma | RADIOLOGY | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 439-448 |
| 65 | Hitesh Verma | KEROSENE INGESTION | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 449-451 |
| 66 | Hitesh Verma | SIMULATOR | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 452-455 |
| 67 | Hitesh Verma | GRAFT AND FLAPS IN ENT | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 456-461 |
| 68 | Hitesh Verma | RECENT ADVANCES | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 462-468 |
| 69 | Hitesh Verma | ENT MENIFESTATIONS OF HIV | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 469-473 |
| 70 | Hitesh Verma | TOPICAL MEDICATIONS IN ENT PRACTICE | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 474-477 |
| 71 | Hitesh Verma | CONSENT & COUNSELLING | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 478-483 |
| 72 | Hitesh Verma | NATIONAL PROGRAMS | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1st | New Delhi | Jaypee | 2024 | 484-490 |
| 73 | CT Yadav Harsha, Verma H | Canal shift and re-entry phenomenon: recurrence or new onset BPPV | Kacker S | Complicated cases in vertigo & dizziness | 3rd | New Delhi | Kontentworx | 2023 | 101-4 |
| 74 | Kajal S, Verma H | Point of care ultrasound in ENT | Khanna P, Bhavana K | Point of care ultrasound a simplified approach | 1st | New Delhi | Jaypee | 2023 | 35-46 |
| S. No. | Author(s) of chapter | Name of the book | Edition | City of publication | Publisher | Year of publication | First-Last page |
|---|---|---|---|---|---|---|---|
| 1 | Hitesh Verma | Textbook Of Ear, Nose & Throat With Head And Neck Surgery For Medical Students | 1 | New Delhi | Jaypee | 2024 | 1-490 |
| Item | 2021-22 | 2022-23 | 2023-24 | Total |
|---|---|---|---|---|
| Journal articles | 128 | 92 | 154 | 374 |
| Abstracts | 107 | 72 | 72 | 251 |
| Chapters in books | 4 | 10 | 7 | 21 |
| Books | 16 | 10 | 74 | 100 |
| Total | 255 | 184 | 307 | 746 |
3rd – Live Surgical Workshop on 2024 TOET International Transoral Endoscopic & Thyroid Course, 2nd – 6th April, 2024, Dr. Ramalingaswami Board Room, AIIMS, New Delhi.
7 prefabricated modular OTs dedicated to the Orthopaedics department, one of its kind in the country with latest technology installed to give highest standard of care to the patients with aesthetic touch to make patient feel calm and comfortable inside the OT complex. This complex also consists of a meeting Room with Live Transmission of surgeries for teaching and demonstration. It also has slim high-end operation theatre lights with 4k camera and 4k recording facility, with a live feed to auditorium, conference hall and consultants' room have been installed.
Bone banks are necessary for providing biological material for a series of orthopaedic procedures. It’s a brainchild and established by Prof Rajesh Malhotra, Head Dept of Orthopaedics and Chief, JPNATC, AIIMS, Delhi. Presently, the dept of Orthopaedics is conducting various training programs to establish bone bank in other parts of the country to cater to the regional population.

Increased life expectancy and joint replacement in ever-younger patients because of expanded indication has in turn increased the numbers of revision procedures over recent decades. In these revision procedures, patients often present with bone losses due to different reasons and replacement of the bone stock will benefit the patients, if this becomes necessary.
Structural bone graft from bone bank also useful in the management of Orthopaedic malignancy, spine surgery and various orthopaedic procedures where bone stock is compromised.
A special modern equipment which allows visualisation of bone, joint and spine in multiple plains thus allowing to perform complex deformity correction of limb and also safe screw fixation in spine surgery especially among children.

First time robotic spine surgeries will be performed in the dept of Orthopaedics, AIIMS, Delhi, a procedure in which robotic arm will allow surgeon to perform spine surgeries in a more precise, faster and minimally invasive manner.

EOS imaging facility installed in the Dept of Orthopaedics, AIIMS, Delhi is first in the country, the EOS Low dose biplanar imaging has been introduced which delivers relatively low dose of radiation (50-80 per cent less than conventional X-rays) that the patient receives while allowing a 3D reconstruction of bones. This is more helpful in understanding the complex association deformities like spinopelvic deformity while performing THA in ankylosed (fused) hips.

It helps in providing additional information about the status of nerve in real time and help to maintain nerve integrity, neural pathways and brain function, thus contributing to clinical risk management and the reduction of neurological impairment during surgical procedures especially during complex spine surgeries.

Gait analysis is used to assess and treat individuals with conditions affecting their ability to walk. Sensor markers placed over patients while they are asked to walk on designated area or treadmill and the motion is captured by the camera system installed in the lab. A model is applied to calculate the movement of the underlying bones. This gives a complete breakdown of the movement of each joint.
Gait analysis is used to analyze the walking ability of humans and can be used for various diagnostic and or prognostic modalities with respect to gait disorders. It has tremendous application for training and rehabilitation of an athlete. It can be also used in the assessment of biomechanics of native joint or after joint replacement procedures to understand and to analyze the gait of the patients.

A new 3D printing technology which can be used inside the human body is offering hope to revision joint replacement, trauma and cancer patients who need bone replacements surgeries. This emerging field aims for the treatment of bone disease. The design and development of the medical implants, tool, instrument and devices are easily possible by using this technology.

Rural Services - The department provides a comprehensive OPD & OT ENT services at the Primary Health Centre at Ballabhgarh, Haryana and once a week services at Centre for speech and hearing disabled at Gurgaon, Haryana
The cochlear implantation (CI) program was started in All India Institute of Medical Sciences in 1996 under the chairmanship of Prof.RC Deka and the first adult patient was successfully operated upon in February 1997. Soon, the department started the Children Program in 1998. Till now (Feb 2020), we have performed more than 1000 cochlear implant surgeries in adults and children. The department has provided support in starting a cochlear implant program in R.R. Hospital, Central Railway Hospital in New Delhi, and also PGIMER in Chandigarh.
A cochlear implant is an electronic device that restores partial hearing to the deaf. It is the only treatment option available for patients with bilateral profound sensorineural hearing loss if there is no benefit with hearing aids.
A cochlear implant is surgically implanted in the ear and activated by a device worn behind the ear. It converts sound to electrical impulses. These impulses are then transmitted via hearing nerve to the brain. The device bypasses damaged parts of the auditory system (hair cells of the cochlea) and directly stimulates the nerve of hearing, allowing individuals who are profoundly hearing-impaired to perceive sound.
Cochlear implants have two parts - a. External (outside) parts that include a microphone, a speech processor, and a transmitter. b. Internal (surgically implanted) parts - a receiver-stimulating system fixed to the skull bone behind the ear and electrodes which are inserted into the cochlea
The microphone picks up sounds and sends them to the speech processor. The speech processor analyzes and digitizes the sound signals and sends them to a transmitter worn on the side of the head just behind the ear. The transmitter sends the coded signals to an implanted receiver. The receiver in turn delivers them to the array of electrodes that stimulate the fibers of the auditory nerve directly. The auditory nerve transmits this information to the brain where it is interpreted as meaningful sound and thus the implanted person starts learning language and speech communication skills.
A cochlear implant is an electronic device that restores partial hearing to the deaf. It is the only treatment option available for patients with bilateral profound sensorineural hearing loss if there is no benefit with hearing aids.
A cochlear implant is surgically implanted in the ear and activated by a device worn behind the ear. It converts sound to electrical impulses. These impulses are then transmitted via hearing nerve to the brain. The device bypasses damaged parts of the auditory system (hair cells of the cochlea) and directly stimulates the nerve of hearing, allowing individuals who are profoundly hearing-impaired to perceive sound.
An implant team consisting of Otolaryngologist, Audiologist, Radiologist, Pediatric Neurologist, Clinical Psychologist and Speech Therapist does the clinical and other laboratory assessment before planning for surgery. Implant surgery is performed under general anesthesia and lasts from two to three hours. The procedure requires a stay in the hospital for 7 to 10 days.
The postoperative rehabilitation will be done by the rehabilitation team consisting of Otolaryngologist, Audiologist and Speech Therapist. Parents’ participation in the training is of paramount importance and one of the parents has to learn the therapy to train the child at home. When the surgical wound is well healed (usually 3 to 4 weeks after surgery) the cochlear implant is activated (switch-on) and a MAP is created using computer based software. The subsequent mapping sessions are individually tailored as per the progress made by the patient. The short and long term goals are set for listening and then language and speech. The therapist teaches the child to listen to the sound that is received from the cochlear implant and helps them in the developing effective spoken communication, leading to development of language and speech.
Cochlear implants do not restore normal hearing, and benefits vary from one individual to another. The implantees are expected to hear and/or recognize sounds/speech and learn language through the auditory input with the help of a cochlear implant. In children, 4-5 years of intensive training is needed.
| S. No. | Title of the project | Name of Principal Investigator | Funded by (Name of funding agency) | Duration (years) | Start year – End year | Total funds sanctioned (Rs) |
|---|---|---|---|---|---|---|
| 1 | Centre for Medical Innovation and Enterpreunership | Alok Thakar | (AIIMS BioNEST) | 4 | 2020 - Ongoing | 4.75 crore |
| 2 | A study on frailty, cognitive dysfunction and associated comorbidities with Hearing loss in Geriatric population | Kapil Sikka | ICMR | 3 | 2024-2027 | 30.9 Lakhs |
| 3 | Intraglandular Botulinum Toxin BoNT Injection for Postoperative Head and Neck Fistula Healing- A Pilot Study | Smriti Panda | Intramural early career grant | 2 | 2024-2026 | 5.85 Lakhs |
| 4 | Prevention of Radiotherapy Induced Xerostomia by intraductal administration of N- Acetyl Cysteine in patients with Oropharyngeal malignancies: A Randomized Clinical Trial | Arvind Kumar Kairo | ICMR | 4 | 2020-2024 | 36 Lakhs |
| 5 | Local application of specific Unani drug for medical management of oral submucosal fibrosis (OSF) a randomized clinical control trial | Arvind Kumar Kairo | CCRUM | 2 | 2023-24 | 35 Lakhs |
| 6 | Phased pilot study to assess the baseline of serum level of Prestin in healthy individuals and in patients of definite Meniere’s Disease as a biomarker of cochlear outer hair cell functional status | Dr Prem Sagar | AIIMS | 5 Lakhs | ||
| 7 | To evaluate nasal eosinophilic miRNAs as potentially diagnostic, prognostic and predictive biomarkers in allergic rhinitis | Dr Shuchita Singh | AIIMS | 2 | 2022-24 | 5 Lakhs |
| 8 | Transorbital approach to infratemporal Fossa - A cadaveric exploratory Study | Dr Anup Singh | AIIMS | 1 year | Jan 2024 | 5 Lakhs |
| 9 | Exome sequencing and molecular characterization in juvenile nasopharyngeal angiofibroma (COLLOBRATIVE PROJECT) | HITESH VERMA/ DR BHUPINDER VERMA | AIIMS | 2 | 2021-23 | 20 Lakhs |
| 10 | Development of single-cell derived clonal spheroids as a tool for drug discovery in cancer research with focus on Head and Neck Cancer | DR R.P.SINGH/ DR HITESH VERMA | DST | 4 | 2019-23 | 3 Crores |
| 11 | Prospective study to evaluate the role of Systemic Bevacizumab therapy in patients with aggressive and complex laryngotracheal and pulmonary recurrent respiratory papillomatosis. | Dr Rajeev Kumar | AIIMS Intramural Collaborative Research Project | 2021-23 | 20 Lakhs | |
| 12 | Study to determine the role of mTOR pathway in the pathogenesis of juvenile nasopharyngeal angiofibroma | Dr Rajeev Kumar | AIIMS Intramural Research Project | 1 | 2021-23 | 5 Lakhs |
| 13 | Phased pilot study to assess baseline serum level of Prestin in healthy individuals and in patients of definite Meniere’s disease and ototoxicity as a biomarker of cochlear outer hair cell functional status | Dr Prem Sagar | AIIMS, New Delhi Intramural project, A-832 | 3 | 2020-23 | 4.5 Lakhs |
| 14 | Device fabrication and clinical validation of a novel mechanical handheld suction device for tracheostomy tube cleaning: a pilot study | Dr Prem Sagar (chief guide), Dr Ritu Dudi (PG thesis candidate) | AIIMS, New Delhi | 2 | 2023-25 | 2 Lakhs |
| 15 | Clinical validation of the effectiveness of automated speech therapy for stuttering delivered by digital means | Shuchita Singh Pachaury | BIRAC | 2 years 3 months | 2020-22 | 10 Lakhs |
| 16 | To determine the efficacy of outpatient antimicrobial therapy (OPAT) with Liposomal amphotericin B in invasive sinonasal mucurmycosis, a randomised controlled trial | Dr. Poonam Sagar | Research section, AIIMS, Delhi | Two years | 2024-2026 | 10 Lakhs |
| S. No. | Title of the project | Name of Principal Investigator | Funded by (Name of funding agency) | Duration (years) | Start year – End year | Total funds sanctioned (Rs) |
|---|---|---|---|---|---|---|
| 1 | Evaluation of factors impacting outcomes of cochlear implants in pediatric population | Kapil Sikka | ICMR | 3.5 Years | 2029-2023 | 35.3 Lakhs |
| 2 | Sound4All: Re-Engineering High end audiometric devices for robust and affordable audiological testing phase II | Kapil Sikka | IGSTC (Indo German Science and Technology Center) | 4 | 2019-2023 | 36 Lakhs |
| 3 | An evaluation of HLA, phagocytic function and trace elements in cases of sinusitis, invasive fungal sinusitis and non-invasive fungal sinusitis | Hitesh Verma | AIIMS | 4 | 2019-23 | 10 Lakhs |
| 4 | ACE-2 receptor expression in sino-nasal mucosa in patients with COVID 19 associated mucormycosis | Hitesh Verma | AIIMS | 2 | 2021-23 | 3.7 Lakhs |
| S. No. | Title of the project |
|---|---|
| 1 | A pilot study to assess the effect of intraductal N acetyl cysteine on swallowing and voice outcomes of patients with oropharyngeal cancer undergoing radiotherapy |
| 2 | To compare different Cochlear Implantation outcome scores with auditory cortical activity seen on functional near infrared spectroscopy in prelingual profound SNHL patients after Cochlear Implantation |
| 3 | Analysis of voice outcomes after radiation or chemo radiation in carcinoma larynx and the effect of N acetyl cysteine on voice parameters |
| 4 | Evaluation of respiratory and voice outcomes in patients with unilateral vocal cord palsy post injection laryngoplasty |
| 5 | Exome sequencing and molecular characterization in juvenile nasopharyngeal angiofibroma |
| 6 | A prospective study to measure the objective, subjective and aesthetic Outcomes in patients undergoing Septorhinoplasty |
| 7 | A comparative study to evaluate functional outcomes following tongue reconstruction with radial artery forearm free flap and infrahyoid myocutaneous flap |
| 8 | A single institutional prospective audit of type-1 tympanoplasty and evaluation of factors affecting the outcome. |
| 9 | to compare post cochlear implant outcome in candidates with and without residual hearing (RH) |
| 10 | Descriptive study of the anatomical variations of the superficial temporal artery and the posterior auricular artery in the patients with unilateral microtia and its implications on the surgical outcomes in auricular reconstruction surgery |
| 11 | To evaluate prospective auditory cortical activity changes on functional near infrared spectroscopy in prelingual profound snhl patients undergoing cochlear implantation |
| 12 | Serum prestin and otolin-1 as markers of cisplatin-induced ototoxicity in cervical cancer patientsThesis |
| 13 | Role of Adjuvant Therapy in Early-Stage Oral Cavity Squamous Cell Carcinoma: An Ambispective Analysis |
| 14 | Ambispective study to assess Universal Newborn Hearing Screening Program |
| 15 | Comparative evaluation of CAD- CAM planning versus traditional free fibula planning in surgical outcomes in mandibular reconstruction-A prospective study |
| 16 | Correlation of Depth Of Invasion with Lymph node Metastasis in Laryngeal and Hypopharyngeal carcinoma |
| 17 | A prospective study to evaluate role of various frailty screening instruments in predicting surgical complications in geriatric head neck cancer patients. |
| 18 | Comparative study evaluating Ex-Vivo US aided deep margin assessment with fresh frozen section analysis in T1-T3 tongue carcinoma: Feasibility study |
| 19 | Ambispective study to assess various primary tumour and ipsilateral nodal factors associated with contralateral nodal metastasis in patients with OCSCC |
| 20 | Study evaluating the effectiveness of Barbed suture versus Vicryl suture for pharyngeal closure after total laryngectomy in PCF reduction |
| 21 | Prospective analysis of predictive factors for tracheal stomal stenosis after total laryngectomy for laryngeal and hypopharyngeal malignancies(2021 -2023, Non funded study) |
| 22 | Role of ultrasound in predicting the depth of tumour invasion and lymph node metastasis in early tongue carcinoma.(2017-till date, Non-Funded Study) |
| 23 | Evaluation of short term and long-term effects of cochlear implantation on vestibular function |
| 24 | A prospective cohort study to evaluate the feasibility and accuracy of fetal vibroacoustic stimulation as a prenatal hearing screening tool |
| 25 | Device fabrication and clinical validation of a novel mechanical handheld suction device for tracheostomy tube cleaning: a pilot study |
| 26 | Short & Long term effects on vestibular apparatus of cochlear implant |
| 27 | A Prospective study to measure the objective, subjective and aesthetic outcomes in patient undergoing Septorhinoplasty |
| 27 | Prospective study to correlate rhinomanometry in DNS patients with endoscopy, NOSE score and NCCT PNS study |
| 28 | A Randomized Control Trial to compare the outcomes of endoscopic and microscopic stapes surgery |
| 29 | Prospective study to evaluate the efficacy of PNN as treatment modality in patient with PAR along with medical management |
| 30 | To evaluate poor prognosis factors in laryngotracheal stenosis: An ambispective study |
| 31 | Impact of NACT on surgical decision and perioperative outcome in patient with very advanced buccal cancer |
| 32 | A randomised control trial on the effectiveness of anti fungal and stetoid nasal douching in allergic fungal rhinosinusitis: a clinical, radiological and biochemical corelation |
| 33 | Descriptive study of the anatomical variations of the superficial temporal artery and the posterior auricular artery in the patients with unilateral microtia and its implications on the surgical outcomes in auricular reconstruction surgery |
| 34 | Prospective audit of tympanoplasty and evaluation of factors affecting the outcome |
| 35 | To assess the outcomes of lateral skull base lesions who have been surgically operated with special reference to quality of life |
| 36 | Prospective assessment of auditory and cognitive performance in children undergoing ear surgeries: A comparative study |
| 37 | Comparative analysis of qPCR, mRNA ISH and p16 IHC for detection of high risk HPV on fine needle aspirates and core needle biopsies in patients with metastatic squamous cell carcinoma in cervical lymph nodes |
| 38 | Role of preoperative nutritional intervention in improving surgical outcome of patients with oral squamous cell carcinoma |
| 39 | Effect of intranasal corticosteroids and antihistaminics v/s omalizumab on adenoid hypertrophy |
| 40 | Effect of Palatal Morphology on Eustachian Tube Function in Children with Adenoid Hypertrophy: an Observation Study |
| 41 | Assessment of pre-cervical (perimarginal and lingual) lymph nodes as first echelon for squamous cell carcinoma of oral cavity |
| 42 | Adversity and QOL Post Treatment of Laryngeal and Hypopharyngeal Cancer and Impact of Novel AIMS-IIT-TEP in its Mitigation. |
| 43 | Evaluating the effectiveness of Barbed suture versus Vicryl for pharyngeal closure after total laryngectomy in PCF reduction: A Randomised controlled study |
| 44 | A Study analysing "Back to Normalcy" in Oral Cavity Cancer Survivors |
| 45 | A prospective study to evaluate the role of various frailty screening instruments in predicting surgical complications in geriatric head neck cancer patients. |
| 46 | Sentinel lymph node detection in oral squamous cell carcinoma with negative neck: comparison between [99mTc] Sulphur colloid AND [99mTc] DTPA ANTICytokeratin- Collagenous Nanoparticle (DC-Col NP) |
| S.No. | Title of the project |
|---|---|
| 1 | A Prospective Study to evaluate the impact of Oral Sub mucous Fibrosis (OSMF) on occult and overt lymph nodal metastases in Gingivo-buccal complex carcinomas (GBCC) (T1-T4a) of Oral cavity |
| 2 | A prospective study to determine early predictive factors of hypocalcemia in patients undergoing total or completion thyroidectomy |
| 3 | Prospective pilot study to assess the effectiveness of novel Forehead Knuckle Tapping method in localisation of better or worse hearing ear as compared to conventional tuning fork testing |
| 4 | A prospective pilot study to evaluate the effect of Supraglottoplasty on Tracheomalacia in pediatric patients with Congenital Laryngotracheomalacia |
| 5 | An ambispective cohort control study to evaluate the incidence of SARS CoV-2 infection in post Adenoidectomy/Adenotonsillectomy patients |
| 6 | Comparison Of Suction Verses Microdissection Method For Harvesting Supporting Cell From Inner Ear |
| 7 | Observational study to correlate site of obstruction in OSA with eustachian tube dysfunction and reflux disorders |
| 8 | Ambispective study to evaluate the utility of Supraclavicular artery island flap [SCAIF] reconstruction in Head and Neck Cancers |
| 9 | A cohort study on determining the effect of preoperative residual hearing on post cochlear implant outcome |
| S. No. | Title of the project | Collaborating department/institution |
|---|---|---|
| 1 | To evaluate the role of Kit-based Loop-Mediated Isothermal Amplification (TB-LAMP) assay in the diagnosis of Extra-pulmonary tuberculosis (EPTB) | Medicine Department |
| 2 | Analysis of circulating DNA for BRAF (T 1799A) mutation as a futuristic non-invasive tool for diagnosis, prognostication, targeted therapy and folloW-up of papillary thyroid cancer | Pathology |
| 3 | Phase IIb/III Study to determine efficacy of curcumin and Metformin to reduce the incidence of Second Primary tumors of Aero-digestive tract in patients with history of head and neck squamous cell carcinoma | National Cancer Grid |
| 4 | Clinical validation of the effectiveness of automated speech therapy for stuttering delivered by digital means | BIRAC |
| 5 | Effect of Cochlear implantation on middle ear and saccular function | Collabrative project with AIISH, Mysuru |
| 6 | Molecular characterization of olfactory neuroblastomas for classification into prognostically and therapeutically relevant subgroups. | Dr. Aanchal Kakkar ( Pathology- PI). |
| 7 | Evaluation of Machine Learning Techniques including Deep Learning for the Identification of Malignancy in Tissue Samples. | AIIMS- IIT Delhi Joint Collaborative Funding 019-2021, Dr. Aanchal Kakkar ( Pathology - PI). |
| 8 | Inter- institutional program for maternal neonatal and infant science : A translational approach- interdisciplinary group for advanced research on birth outcome | DBT India initiative ( GARBH- Ini-Phase II) |
| 9 | A study on the effect of genetic manipulation on mammalian inner ear cells | Dept of Biochemistry |
| 10 | Exome sequencing and molecular characterization in juvenile nasopharyngeal angiofibroma | Biotechnology/ AIIMS |
| 11 | Evaluation of specific molecular alterations and tumor immune microenvironment for detection of clinically actionable targets in high grade salivary gland carcinomas | ICMR Funded, Department of Pathology |
| 12 | The SWOAR trial: A phase III trial evaluating dysphagia-aspiration related structures & submandibular gland sparing Intensity modulated radiotherapy (SWOAR-IMRT) versus standard IMRT in Head and neck squamous cell carcinoma | Department of Radiotherapy |
| 13 | The tumour immune microenvironment of follicular cell -derived thyroid carcinomas across different grades utilizing gene expression and spatial proteomic profiling | Department of Pathology |
| 14 | Role of celecoxib in reducing cognitive impairment in patients receiving definitive chemoradiation for head and neck carcinoma: A phase II randomized placebo controlled trial | Department of Medical Oncology |
| 15 | Potentially malignant lesion atlas project: Validating the efficacy of a novel, Point-of -care diagnostics and developing an integrated multidimensional, prognostic nomogram | ICMR funded, Department of Preventive Oncology, NCI AIIMS |
| 16 | Comparative analysis of qPCR, mRNA ISH and p16 IHC for detection of high risk HPV on fine needle aspirates and core needle biopsies in patients with metastatic squamous cell carcinoma in cervical lymph nodes | Collaborative Intramural, AIIMS |
| 17 | A Phase III , Randomized Controlled Study of Utility of Pectoralis Major Myofascial Flap in Reducing Pharyngocutaneous Fistula Rates After Salvage Total Laryngectomy. | TMH |
| 18 | A randomised, sham controlled, double blind study to evaluate the efficacy of and safety of intra-thecal OAV101 in patients with later onset type-2 spinal muscular atrophy who are ≥ 2 to < 18 years of age, treatment naive, sitting, and never ambulatory. | A phase 3 Clinical trial (STEER) by Novartis Pharmaceuticals.ClinicalTrials.gov Identifier:NCT05089656. |
| 19 | Prevalence and pattern of traumatic dental injury in children and adolescents with severe to profound hearing impairment reporting to a tertiary care centre in North India | Pediatric Dentistry, CDER, AIIMS, New Delhi |
| 20 | Comparison of pulsed radio-frequency versusconventionalradio-frequency in secondary glossopharyngeal neuralgia: a randomised controlled trial | Department of Anaesthesiology, AIIMS, New Delhi |
| 21 | Perioperative anaesthetic management of paediatric congenital laryngomalacia- A retrospective study | Department of Anaesthesiology, AIIMS, New Delhi |
| 22 | A Phase II trial of Pentoxiphylline and alpha tocopherol (PAT) in prevention of radiation induced dysphagia in head and neck squamous cell carcinoma | Radio-therapy |
| 23 | A Phase III prospective randomised trial comparing dysphagia-aspiration related structures & submandibular gland sparing Intensity modulated radiotherapy (SWOAR-IMRT) versus standard IMRT (s-IMRT) paring in locally advanced oropharyngeal and laryngeal carcinomas | Radio-therapy |
| 24 | Ultrasonographic assessment of tonsillar volume in children undergoing tonsillectomy : a predictor of post operative morbidity | Anaesthesiology |
| S. No. | Title of the project | Collaborating department/institution |
|---|---|---|
| 1 | To Understand the Biochemical and Molecular Basis of Mucormycosis in COVID-19 Patients | Dept of Biotechnology |
| 2 | Evaluation of genetic profile of olfactory neuroblastoma | Department of Pathology |
| 3 | Comparison between kit based and in-house preparation of Tc -99m Ubiquicidin | Department of Nuclear Medicine |
| 4 | Utility of 99m Tc- Ubiquicidin scintigraphy in diagnosis of sinonasal mucormycosis | Department of Nuclear Medicine |
| 5 | Utility of Ga - 68 - NOTA- UBI in infectious and non- infectious lesions | Department of Nuclear Medicine |
| 6 | A phase II study of EMF (Erlotinib+ Methotrexate+ Celecoxib) in platinum refractory recurrent /metastatic head neck squamous cell carcinoma | Department of Medical Oncology |
| 7 | Assessment of Oral Microbiome and its significance in upper aerodigestive tract cancers | Department of Medical Oncology |
| 8 | A cohort study to assess the feasibility of WHO ICOPE approach in tertiary health centres | Department of Geriatrics, AIIMS, New Delhi |
| 9 | A longitudinal Survey to assess Patient Satisfaction for Nurse Initiated Follow Up Tele-Consultation among patients discharged from a selected tertiary care hospital | Nursing department |
| 10 | An OMR sheet based feed-back survey on in-patient satisfaction regarding various hospital services in a selected tertiary care hospital | Nursing department |
Department of orthopaedics was created in 1961. Prof. Prakash Chandra was handpicked by Pt. Jawaharlal Nehru and Smt. Rajkumari Amrit Kaur. He was a distinguished and highly accomplished orthopaedic surgeon in U.K. who agreed to return to his country and serve it. He was the first head of the department of orthopaedics under whose leadership the journey started and achieved new hights in each decade.
The Department of orthopaedics in AIIMS has doctors with specializations in the field of arthroscopy and sports medicine, musculoskeletal oncology, paediatric orthopaedics, joint replacement, spine surgery, upper extremity surgery, foot surgery and treatment of complex trauma. All the new and contemporary principles and techniques are being used for the management of these medical problems.
The department has been the leader in the field of orthopaedic education country-wide besides providing best undergraduate and postgraduate training. The regular cadaveric courses, workshops and conferences are most sought-after in the field last year and covered all subspecialties of orthopaedics.
The department witnessed an unparalleled rise in orthopaedics research in last decade and has several research projects with national as well as international funding.
The department is known to perform several complex orthopaedic surgeries and the operation theatres are one of the best equipped, comparable to any advanced centre in the world.
| Monday | Prof Rakesh Kumar, Dr Rajeev Kumar, Dr Arvind Kairo, Dr Poonam Sagar |
| Tuesday | Dr Chirom Amit Singh, Dr Prem Sagar, Dr Shuchita Singh Pachaury |
| Wednesday | Prof Alok Thakar, Dr Kapil Sikka, Dr Hitesh Verma |
| Thursday | Prof Rakesh Kumar, Dr Rajeev Kumar, Dr Arvind Kairo, Dr Poonam Sagar |
| Friday | Dr Chirom Amit Singh, Dr Prem Sagar, Dr Shuchita Singh Pachaury |
| Saturday | Prof Alok Thakar, Dr Kapil Sikka, Dr Hitesh Verma, Dr Anup Singh |
| Clinics | Days | Location |
|---|---|---|
| Vertigo Clinic | Monday (1:30pm onwards) | Room No.C-603, NEWENT OPD |
| Voice Clinic | Monday (1:30pm onwards) | Room No. A-602, ENT OPD |
| H N REHIBILITATION Clinic | Thursday (9:00am onwards) | Room No. A-602, ENT OPD |
| Head & Neck Clinic | Monday, Friday (2:00pm onwards) | IRCH, Room No. 2,3 |
| Audiology & Skull base Clinic | Wednesday (1:30pm onwards) | Room No.C-603, NEWENT OPD |
| Cochlear implant clinic | Wednesday (1:30pm onwards) | Room No.A-634, ENT OPD |
| Rhinology & Facial Plastic Clinic SLEEP SURGERY CLINIC | Friday (1:30pm onwards) Friday (1:30 pm onwards) | Room No.C-603,NEW ENT OPD Room No.C-603,NEW ENT OPD |
| Radiology clinic | Wednesday (1:30pm onwards) | Room number 52 |
| Nuclear Medicine Clinic | 2nd,4th Friday of Month (11am-12pm) | Room number 15 |
| Laboratory | Room No. |
|---|---|
| Audiomery, OAE | 636, B wing rooms |
| ABER, ASSR | 639, 635 |
| Cochlear Implant rehabilitation room | 634 |
| Speech Therapy | 608-611 |
| VNG | 605 |
| Rhinomenometry, allergy testing | 604 |
| Stroboscopy, EMG | 602 |
| Trans-nasal oesophagoscopy | 621 |
| Tinnitus lab | 641 |
| EDUCATION |
The Department has a 3 year residency training program
|
| CONTINUING MEDICAL EDUCATION |
| CME programmes organized |
Year 2019
|
Year 2020
|
The Department has a 3 year residency training program and takes in an average of seven candidates every year. The Department also has 3 years MCh (Head & Neck Oncology) training program and takes in an average of two candidates every year. Candidates are recruited after an entrance examination conducted twice a year. The Department also runs a Skull base fellowship training program in collaboration with the Neurosurgery Department and it takes one candidate every year. Currently, twelve positions of Senior Residents are available for post MS training and are for fixed tenure of three years. Positions are filled in when a vacancy arises and also require entrance examination and interview. The Department runs a schedule of academic activities directed at Post graduate students, MCh students and skull base fellow (seminars, journal clubs, case discussions, and research activity reviews) on every Tuesday (08-00 to 09-00 AM) and & on Thursday (08-00 to 09-00 AM & 15-00 to 17-00 PM). The Department also has a tradition of welcoming ENT Surgeons from other centres for short term and long term training as observers. For details of the same please go to the institute website and write a letter to the Head of the Department.
Bijlani R.L. Understanding Medical Physiology: a textbook for medical students. New Delhi:Jaypee, 3rdedition, 2004.
Bijlani RL. Medical research suggests role for yoga in curing heart disease. Invention Intelligence. 2003, 38(2):63-74.
The Confocal Imaging Facility in the Department of Physiology is equipped with a Leica TCS SP2 AOBS with an inverted microscope DMIRE2 having 6 visible laser lines (458, 476, 496, 514, 546, 633 nm) and 2 UV laser lines (351, 364 nm). It has 4 PMTs to collect emitted light and 1 PMT to collect transmitted light.
Isolated human endometrial epithelial and stromal cells grown on collagen 3-D biomatrix showing evidence of gland formation in vitro. A: Transmitted image; B: Epithelial cell nuclei stained with DAPI; C: Transmitted overlaid image of immunostaining for vascular endothelial growth factor (VEGF); D: Glandular cell immunostaining for VEGF using anti-VEGF Pab & Alexa fluor 633. Leica SP2 AOBS has z-sectioning ability for 200 mm
Serial Z sectioning of human endometrial gland grown in vitro showing localization of intracellular VEGF immunostaining
Colocalization of biomolecules using Leica SP2 AOBS
Isolated human endometrial epithelial and stromal cells grown on 3-D collagen biomatrix expressing progesterone receptor (B) and insulin like growth factor binding protein-2 (C). Cell nuclei visible from DAPI staining (A), PR and IGFBP-2 colocalized in endometrial cells (D). Immunostaining for PR using anti-PR Mab & Alexa Fluor- 488; for IGFBP2 using anti-IGFBP-2 Pab & Alexa Fluor- 633.
Cytoplasmic distribution of viral proteins tagged with enhanced green fluorescent protein
Cytoplasmic expression of Hepatitis E virus fusion protein (A), pORF1EGFP and pORF2EGFP (B) in transfected HepG2 cells. FRET analysis programme is available for further studies.
Contact Details:- Prof. D.Ghosh, Department of Physiology, AIIMS, New Delhi-29. Room No. 2005. Tel No. 26594625.
| Tests available for patients at Central RIA Facility, Room No. 2090 | ||||
| Name of Tests | Sample required | Sample to be sent in | Charges w.e.f. 20/05/2022 | |
| Thyroid | ||||
| 1 | Total T3 | Serum | Plain tube | No charge |
| 2 | Total T4 | Serum | Plain tube | No charge |
| 3 | TSH | Serum | Plain tube | No charge |
| 4 | Free T3 | Serum | Plain tube | No charge |
| 5 | Free T4 | Serum | Plain tube | No charge |
| 6 | Anti TPO | Serum | Plain tube | No charge |
| 7 | Anti Tg | Serum | Plain tube | Rs. 550 |
| Fertility / Pregnancy | ||||
| 8 | Leutinizing Hormone (LH) | Serum | Plain tube | No charge |
| 9 | Follicle Stimulating Hormone (FSH) | Serum | Plain tube | No charge |
| 10 | Prolactin | Serum | Plain tube | No charge |
| 11 | Testosterone | Serum | Plain tube | No charge |
| 12 | Progesterone | Serum | Plain tube | No charge |
| 13 | Estradiol | Serum | Plain tube | No charge |
| 14 | DHEA-S | Serum | Plain tube | No charge |
| 15 | Cortisol | Serum | Plain tube | No charge |
| 16 | 17-hydroxy Progestrone (17-OHP) | Serum | Plain tube | No charge |
| 17 | Anti-Mullerian Hormone (AMH) | Serum | Plain tube | Rs. 650 |
| 18 | Sex Hormone Binding Globulin (SHBG) | Serum | Plain tube | Rs. 900 |
| 19 | Dihydroxy Testosterone (DHT) | Serum | Plain tube | Rs. 350 |
| 20 | Inhibin B | Serum | Plain tube | Rs. 800 |
| 21 | Total-hCG | Serum | Plain tube | No charge |
| TORCH | ||||
| 22 | Cytomegalovirus (CMV) - IgG | Serum | Plain tube | Rs. 400 |
| 23 | Cytomegalovirus (CMV) - IgM | Serum | Plain tube | Rs. 400 |
| 24 | Rubella - IgG | Serum | Plain tube | Rs. 400 |
| 25 | Rubella - IgM | Serum | Plain tube | Rs. 400 |
| 26 | Toxoplasma - IgG | Serum | Plain tube | Rs. 400 |
| 27 | Toxoplasma - IgM | Serum | Plain tube | Rs. 400 |
| Other Hormones | ||||
| 28 | Intact PTH (Parathyroid Hormone) | Serum | Plain tube | No charge |
| 29 | Growth Hormone (GH) | Serum | Plain tube | No charge |
| 30 | Adenocorticotropin Hormone (ACTH) | Serum | Plain tube | No charge |
| Metabolic | ||||
| 31 | Active Vitamin B12 | Serum | Plain tube | No charge |
| 32 | Ferritin | Serum | Plain tube | No charge |
| 33 | Folate | Serum | Plain tube | No charge |
| 34 | 25-hydroxy Vitamin D | Serum | Plain tube | No charge |
| 35 | Insulin | Serum | Plain tube | No charge |
| 36 | C-peptide | Serum | Plain tube | No charge |
| 37 | HbA1c (Glycated Hemoglobin) | Whole blood | EDTA Tube | No charge |
| Cancer Markers | ||||
| 38 | Alpha FetoProtein (AFP) | Serum | Plain tube | No charge |
| 39 | CA-125 | Serum | Plain tube | Rs. 500 |
| 40 | Total PSA (Prostate Specific Antigen) | Serum | Plain tube | No charge |
| 41 | CEA | Serum | Plain tube | No charge |
| 42 | CA 19.9 | Serum | Plain tube | No charge |
| 43 | CA 15.3 | Serum | Plain tube | No charge |
| 44 | HE 4 | Serum | Plain tube | Rs. 1,900 |
| 45 | Free PSA | Serum | Plain tube | Rs. 650 |
| Cardiac Markers | ||||
| 46 | BNP | Plasma | EDTA Tube | Rs 1,250 |
| 47 | STATCKMB | Plasma | EDTA Tube | Rs. 400 |
| 48 | Homocysteine | Plasma | EDTA Tube | Rs. 800 |
| 49 | Troponin I (High Sensitive) | Plasma | EDTA Tube | Rs 850 |
| Immune Marker | ||||
| 50 | Anti-CCP | Serum | Plain tube | Rs. 900 |
| Transplant | ||||
| 51 | Cyclosporine | Whole blood | EDTA Tube | Rs 1,550 |
| 52 | Sirolimus | Whole blood | EDTA Tube | Rs. 2,600 |
| 53 | Tacrolimus | Whole blood | EDTA Tube | Rs. 1,400 |
| Sepsis | ||||
| 54 | Procalcitonin | Serum | Plain tube | Rs. 1,350 |
| Therapeutic Drug Monitoring | ||||
| 55 | Methotrexate | Serum | Plain tube | Rs. 1,800 |
Department of Forensic Medicine and Toxicology, AIIMS, New Delhi organized a Workshop in association with International Committee of Red Cross (ICRC), in Technology Hall, CMET on 17th of March, 2018. The Workshop focused on concept of Dignified Management of Dead, providing comfort to grieved relatives, relevant forensic issues affecting the living etc. The aim of the Workshop was to increase awareness, knowledge, sensitization and responsiveness particularly among Forensic Medicine experts working in Delhi.
The event started with registration of delegates and the welcome address was delivered by Head of the Department, Dr Sudhir K Gupta followed by the National Anthem. In the Inauguration ceremony, the following dignitaries were on the dais and also addressed the delegates:
Dr. Uwom O. Eze (Regional Forensic Coordinator, ICRC) discussed about “ICRC Humanitarian Forensic Action”. Dr Bipin B. Chaudhary, DCP, Homeguards, deliberated about “Police Perspective” towards Humanitarian Forensic Action. This was followed by High Tea, after which the Delegates were assembled into different workgroups to deliberate and discuss the Humanitarian aspects of Forensic Medicine practice for future guidelines, operational aspects and capacity building. The following were the Working Groups:
This was followed by 10 min Presentation by each of the Working Groups and Compilation of recommendations by rapporteurs. The Workshop was concluded by Closing Remarks, delivered by Head of the Department, Dr Sudhir K Gupta. The event was co-ordinated by Dr Adarsh Kumar (Prof), Dr Kulbhushan Prasad (Asst Prof), Dr Abhishek Yadav (Asst Professor), Dr Antara Deb Barma (Senior resident), Dr Arijit Dey (Senior Resident) along with the support of other resident doctors and staff of the Department. Dr Prashanth Bhagvath coordinated the event from ICRC side. The Workshop was followed by Lunch for all delegates. Altogether, about 80 delegates attended the workshop and participated actively with their inputs.
















The role of Forensic Medicine experts is not limited only to complete postmortem examination and routine medicolegal duties. The concept of humanitarian approach such as Dignified Management of Dead, providing comfort to grieved relatives, relevant forensic issues affecting the living etc are very relevant considering socio-cultural realities of the society but are often neglected in the day to day duties of a Forensic expert. Keeping this relevant but neglected aspect in mind, an initial step was envisaged by Dr Sudhir K Gupta, Professor and Head and Dr Uwom Eze, Forensic Coordinator, ICRC.
A Symposium was held on 29/08/2018 to increase awareness, knowledge, sensitization and responsiveness particularly among young Forensic Medicine experts who are the future of this country. This symposium was a joint venture of AIIMS & International Committee of Red Cross (India) with vision and aim to discuss the Humanitarian aspects of Forensic Medicine practice for future guidelines and a roadmap, and also discussing the operational aspects and capacity building, with your active collaboration as a stakeholder.
The event started with registration of delegates. The event was formally inaugurated by Dr Sudhir K Gupta, Professor & Head of the Department. The following speakers addressed the delegates:
This was followed by an interactive session with all the participants, where all deliberated and discussed about the Humanitarian aspects of Forensic Medicine practice for future guidelines, operational aspects and capacity building. The vote of thanks was given by Dr Abhishek Yadav (Asst Professor).
The event was co-ordinated by Dr Kulbhushan Prasad (Asst Prof), Dr Abhishek Yadav (Asst Professor), Dr Antara Deb Barma (Senior resident), Dr Swati Tyagi (Senior Resident) along with the support of other resident doctors and staff of the Department. Dr Prashanth Bhagvath coordinated the event from ICRC side. The Workshop was followed by Lunch for all delegates. Altogether, about 90 delegates attended the symposium and participated actively with their inputs.










A trainee will be continuously assessed. This assessment is based on a written 2-hour evaluation once in 6 months and the continuous evaluation of the clinical work that the trainee is assigned to do. If he or she does not come up to minimum standard, the faculty may ask him or her to leave at any time during the course of the training programme. He or she will have to maintain a log book which will be the primary mode of assessment during the trainees stay in the department. We expect the candidate to be hard working because of the lengthy and busy periods of duty. Honesty is the quality that the department cherishes. By the end of the training, we expect the candidate to be:
Department of Forensic Medicine and Toxicology, AIIMS, New Delhi organized an interactive academic meet jointly in association with Indian Association of Friendships with Foreign Countries (IAFFC) and Embassy of Hungary, New Delhi, in the Board room of the Department on 7th of December, 2018 at 11:30 AM.
The interactive lecture was given by Dr Viktor Soma Poor, Assistant Professor, University of Pecs, Hungary and the topics of lecture were:
The session was chaired by the respected Head of the Department, Dr Sudhir K Gupta and Dr Hilda Farkas, Counselor, Science and Technology, Embassy of Hungary. Dr J S Nischal, Secretary, IAFFC was also present. The event was coordinated by Dr Kulbhushan Prasad, Asst Prof and Dr Abhishek Yadav, Asst Professor with Dr Antara Debbarma, Senior resident of the Department.
The event started with the welcome address followed by the National Anthem. The topic was presented by Dr Viktor Soma Poor, Assistant Professor, Department of Forensic Medicine ,University of Pecs. The first session was a walk through the life of Ignac Semmelweis, the Hungarian physician whose work resulted in drastically reducing the number of women dying after child birth by mere introduction of handwashing, but was put in a mental asylum where he tragically passed away. Even today his work has not yet received the due acknowledgment by the medical fraternity. He also advised the young budding researchers in the department to “To see what everybody else has seen, and to think what nobody else has thought”. The second session was presented by him regarding the diagnosis of drowning, which included DNA based identification of diatom and algae. Following these two sessions, the faculties and residents came up with their queries regarding the topics discussed and the practical difficulties faced in diagnosing a case of drowning by the doctors of Forensic Medicine in the India. The event ended with the vote of thanks and felicitation of Dr Viktor Soma Poor by Dr Sudhir K Gupta.










All the programmes include experience in clinical management, surgical procedures, ICU care and research.
This includes working up patients, examining patients in the outpatient department, performing operations and doing on-call duties. Irrespective of the duration or type of training programme the candidate is accepted for, he or she will be required to work initially as a first on call resident, the duties of which are similar in nature to that of a house officer's. If he or she is a long term trainee then at a later date the candidate is assigned second on call duties which are equivalent to a surgical registrar's responsibilities.
Each trainee is required to complete a research project which may consist of analysis of retrospective clinical data, prospective clinical investigation or experimental research.
This includes presenting and evaluating research publications at journal clubs, reviewing and summarizing the literature on a current topic, presenting cases in the combined and grand rounds of the Institute, paper or poster presentations at local, national or international conferences.
Operations which a trainee or resident will assist and learn may include the following:
Portal hypertension
Liver
Biliary tract
Pancreas
Oesophagus
Stomach and duodenum
Colon and rectum
Department of Forensic Medicine and Toxicology, AIIMS, New Delhi organized a symposium jointly in association with Ogilvy India on the ‘Role of Forensic DNA Technology in Expediting Justice and Fighting Crime’, held at India International Centre on 17th of July, 2019.
The event started with the welcome address followed by the National Anthem. The Opening remarks were given by Ms Arneeta Vasudeva, (Sr VP & Capability Head, PR) Ogilvy India. The keynote speech was delivered by Dr Sudhir K Gupta Head of the Department. The speech highlighted the need for educating and training first-line responders on proper collection & handling of DNA samples while at the same time creating dedicated infrastructure to attend to rape survivors. Dr Gupta explained the importance establishment of National one-stop sexual assault examination, care, and research centre enabled with state-of-the-art DNA collection and testing facilities. Dr BB Choudhary (DCP Delhi Police) talked about the role of investigating officers in collection and preservation of crime scene evidence. Dr Vivek Sehajpal (Additional Director, Himachal Pradesh FSL) gave an interactive presentation on how to collect & preserve DNA samples of different types, along with a practical demo of the DNA collection kits.
The second was a panel discussion led by the Dr Sudhir K Gupta, Professor & Head, Department of Forensic Medicine, All India Institute of Medical Sciences (AIIMS), New Delhi. The session was co-chaired by Dr Vivek Sehajpal, Dr Deepa Verma (Director, Delhi FSL), Dr Harish Pathak (Professor, KEM Mumbai), and Tim Schellberg (Founder & President, Gordon Thomas Honeywell).
The topics of discussion were:
Expert Panel emphasized on the rise in demand for DNA testing and increasing our capacity for Justice to survivors of Sexual Assault. Panel recommended the plan for specialised trained crime scene examination teams to ensure quick retrieval of Forensic evidence while ensuring proper collection and preservation. Dr Harish Pathak shared his experience from his centre where One stop crisis centre is established and is functional. Mr. Tim Schellberg while quoting Nirbhaya Gangrape trial showed the need and the power of DNA sample in helping the prosecution build an airtight case based on the DNA of the accused found at the crime scene. It was followed by the discussion session where audience came up with their queries regarding the topics discussed and the practical difficulties faced by the doctors of Forensic Medicine in the India. The event ended with the vote of thanks and felicitation of the chairpersons.
The event was coordinated by Dr Kulbhushan Prasad, Asst Professor and Dr Abhishek Yadav, Asst Professor along with Resident doctors of the Department.








Department of Forensic Medicine and Toxicology, AIIMS, New Delhi organized an Interactive academic knowledge exchange programme with following International Faculties on 10th of September, 2019 at 11:30 AM.
The event was coordinated by Dr Abhishek Yadav, Asst Professor, Dr Kulbhushan Prasad, Asst Prof and Dr Abilash S, Senior resident.
The event started with the round of the department Facilities including Mortuary, Forensic Histopathology Lab, Forensic radiology, DNA Lab and toxicology Lab. The guest faculty members gave their inputs, suggestions and advise regarding the betterment of the infrastructure and working protocol. They addressed the queries of the technicians, scientists, resident doctors and Faculty members regarding their respective working areas.
It was followed by interactive lecture by Dr Stephen Cordner. The topic was presented by Professor Stephen M Cordner, Ex-Director, University of Monash, Victorian Institute of Forensic Medicine, Australia. He gave a brief overview of the establishment of Digital Autopsy under his leadership at the Victorian Institute of Forensic Medicine, Australia. He also shared his experience as a Forensic Pathologist working at the institute along with some practical tips and guidance regarding possible pit falls in the Forensic practice which can be avoided. He appreciated the Departments’ effort in establishing the DNA lab and Toxicology lab and its functional status. The Department of Forensic Medicine is starting the Digital Autopsy Services shortly and Professor Stephen M Cordner congratulated the Head of the Department on the achievement and also shared pros and cons of implementing Digital autopsy. He also advised the young residents and researchers of the department to use the powerful tool of CT scan for better learning and also for taking the subject to better heights. Following the lecture, the faculties and residents came up with their queries regarding the topic discussed and the possible use of Digital Autopsy techniques in Forensic Medicine practice in Indian setup.
The event ended with the vote of thanks and felicitation of Professor Stephen M Cordner by Dr Sudhir K Gupta, Prof & Head.











Organizing Chairman: Dr. Sudhir K Gupta, Prof & Head, Dept. of Forensic Medicine AIIMS, New Delhi.
Organizing coordinators: Dr. Abhishek Yadav & Dr. Kulbhushan Prasad
Organizing Team: Dr. AK Jaiswal, Dr. Varun Chandran A, Dr. Swati Tyagi, Dr. Hemant Kumar Kanwar, Dr. Abilash S, Dr. Abhishek Varun, Dr. Zahid Ali C H, Dr. Aravindan V, Dr. Balaji D, Dr. Raveena.
Department of Forensic Medicine & Toxicology, AIIMS New Delhi organized the 2nd Annual AIIMS Forensic Guild Conclave 2021, over two days from 19th to 20th March. The event was open to faculties of Forensic Medicine and Toxicology from all the other AIIMS in the country.
The inaugural ceremony began with formal procedure of lamp lighting to seek the blessings of goddess Saraswati. The lamp was lighted by the chief guest Dr. BB Choudhary (DCP, Delhi Police) along with Dr. Sudhir K Gupta in the presence of Dr. Binay K Bastia and Dr. D N Bhardwaj. The Chief Guest then delivered a brief lecture highlighting the importance of training of Police and other non-medical staff, in medicolegal work as well as emphasized regarding good communication and interaction by the doctors.
The session was delivered by Prof & Head, Dr. Sudhir K Gupta, Forensic Medicine & Toxicology Department, AIIMS New Delhi, who gave a deep insight into the topic, “2nd or 3rd opinion in cases of CBI & referred from court”.
He discussed the highlights of the cases encountered by him and highlighted the need for evaluating the circumstantial evidences in every case and also gave a holistic definition for Forensic Medicine. The delegates were given the opportunity to have hands on the actual case files of the CBI cases and discuss the same with the Board members of the cases. Each case was discussed with photographs along with explanations and basis for giving a particular opinion.





Chief guest: Dr. Balram Bhragava, Director General, ICMR
Centre for advanced Research and Excellence in Virtual Autopsy has been established as a joint collaboration
The inaugural function began with national anthem followed by the welcoming of the chief guest by Dr. Sudhir Kumar Gupta, Prof & Head Dept. of Forensic Medicine AIIMS, New Delhi, followed by Lamp lighting ceremony commenced.
Formal inauguration of the first of its kind, the “Centre for advanced research and excellence in Virtual Autopsy Centre “was done by unveiling a plaque to mark the inauguration by Dr. Balram Bhargava and Dr. Sudhir Kumar Gupta. The event was graced by the presence of faculties of different AIIMS of the country who were taking part in the historic 2nd Annual AIIMS Forensic Guild Conclave, 2021. This was followed by traditional ribbon cutting and inauguration of the CT Scan complex. Dr. Balram Bhargava gave an inspiring and thought-provoking talk by emphasizing the need for innovations in forensic medicine as well as good working environment with all facilities. He presented the importance of death and also quoted the lines from the song, “Gambler” by Kenny Rogers where the gambler gives important tips for life to a young man. He also mentioned about death in sleep as the best death which was explained by the Chief Guest with opinions taken from the delegates, regarding the same.
Dr Balram Bhargava was then given a tour of the Centre for Advanced research and Excellence in Virtual Autopsy and adjoining renovated odouless Autopsy Mortuary Suite




Department of Forensic Medicine and Toxicology, All India Institute of Medical Sciences, New Delhi organized a workshop on 12th and 13th June 2023 in Centre for Advanced Research and Excellence in Virtual Autopsy as a joint venture of AIIMS & International committee of Red Cross (ICRC), India on Virtual Autopsy and Forensic Anthropology. This workshop included lectures and practical exercises over two days on the topics related to Virtual Autopsy, basic elements of establishing a biological profile (sex, age, ancestry, stature) from the skeleton and assessing hard tissue injuries and other characteristics that might contribute to a positive identification. The principal course resource faculty were:
The workshop was attended by delegates from all over India including JIPMER, PGI Chandigarh, AIIMS Bhopal, IIT Gandhi Nagar, AIIMS Rishikesh, RMl Lucknow as well as international delegates from Nepal, Bhutan and Maldives.
The event was coordinated by Dr Abhishek Yadav (Addl Prof), Dr Kulbhushan Prasad (Addl Prof), Dr Abilash S (Asst Prof) and Dr Swati Tyagi (Asst Prof).






Department of Forensic Medicine and Toxicology, All India Institute of Medical Sciences, New Delhi organized a workshop on 09th October 2023 in Centre for Advanced Research and Excellence in Virtual Autopsy as a with International committee of Red Cross (ICRC), India to sensitize the need for enhancing forensic human identification capacity in mass fatality incidents for forensic practitioners dealing with Management of Dead for better understanding of their role and responsibilities. The workshop was attended by delegates from different Medical colleges and Hospitals of Delhi
The principal course resource faculty were:




The workshop titled "Innovation, Knowledge, and Awareness in Virtual Autopsy" was a landmark event held at the prestigious Centre for Advanced Research and Excellence in Virtual Autopsy, AIIMS New Delhi, on February 23, 2024. Co-organized by the Department of Forensic Medicine and Toxicology, AIIMS New Delhi, and the ICMR Headquarters New Delhi, it brought together a diverse cohort of medical professionals. Participants included faculty members from various AIIMS branches, residents, staff from AIIMS New Delhi, and personnel from ICMR-New Delhi.
The esteemed presence of Chief Guest Shri Subramanian Swamy added to the significance of the occasion. Shri Subramanian Swamy not only attended the event but also honored principal Investigator Dr Sudhir kumar Gupta, Professor & Head, who played pivotal role in pioneering the establishment of Centre for Advanced Research and Excellence in Virtual Autopsy. The workshop offered a comprehensive insight into the journey of establishing CARE in virtual autopsy at AIIMS New Delhi. A significant milestone was achieved with the release of the first-of-its-kind Standard Operating Procedure (SOP) for virtual autopsy by the Department of Forensic Medicine, AIIMS. It celebrated the collective contributions of individuals and teams in pioneering this innovative field.
Various sessions during the workshop covered essential topics such as Postmortem CT (PMCT) fundamentals, advancements in dental estimation for age determination, and understanding decomposition changes and artifacts. Practical applications of virtual autopsy in diagnosing sudden unexplained deaths and road traffic accidents were also explored.Hands-on training sessions provided attendees with valuable experience in operating PMCT and digital X-ray equipment. The workshop further enriched participants with detailed case studies, including those on hemopericardium and asphyxia deaths.
The principal course resource faculty were:






| Year | Name | Course |
|---|---|---|
| 1985 | Peush Sahni | PhD |
| GK Pande | PhD | |
| 1986 | VS Rana | Army, long term trainee |
| 1987 | S Shenoy | PhD |
| 1988 | Mihir K Mohapatra | Odisha state, long term trainee |
| K Sudhakar Reddy | Senior Resident | |
| 1989 | PK Patnaik | Army, long term trainee |
| 1990 | HK Rangan | Army, long term trainee |
| VP Bhalla | Army, long term trainee | |
| RP Choubey | Army, long term trainee | |
| Subash Gupta | Senior Resident | |
| 1991 | Vivek Kohli | Senior Resident |
| 1992 | Deepak Govil | PhD |
| V Baskaran | PhD | |
| 1993 | Rajan Chaudhary | Army, long term trainee |
| AK Pujahari | Army, long term trainee | |
| P Radhakrishna | Senior Resident | |
| DN Dwivedi | MCh | |
| 1994 | PK Mishra | PhD |
| Vivek Tandon | MCh | |
| AK Sharma | Army, long term trainee | |
| C Srinath | MCh | |
| 1995 | JK Banerjee | Army, long term trainee |
| Sujoy Pal | MCh | |
| 1996 | SR Ghosh | Army, long term trainee |
| Anupam Saha | Army, long term trainee | |
| 1997 | Kunal Ghosh | MCh |
| C. Sudeep Naidu | MCh | |
| Ravi Shankar Bhat | MCh | |
| Y Govardhan Rao | MCh | |
| 1998 | Premal R Desai | MCh |
| V Suresh | MCh | |
| Alok R Sinha | Army, long term trainee | |
| 1999 | Vinay Kumaran | MCh |
| Vipon Kumar | Army, long term trainee | |
| BB Das | MCh | |
| 2000 | CK Jakhmola | Army, long term trainee |
| Rajneesh K Singh | MCh | |
| K Ramachandra Naidu | MCh | |
| SS Chauhan | Army, long term trainee | |
| 2001 | Sorabh Kapoor | MCh |
| DVL Narayan Rao | MCh | |
| Victor Vinod Babu | MCh | |
| MS Ray | Army, long term trainee | |
| 2002 | C Srinivas Prabhu | MCh |
| P Pankaj Rao | Army, long term trainee | |
| 2003 | Sundeep S Saluja | MCh |
| Aribam D Sharma | MCh | |
| 2004 | Sukanta Ray | MCh |
| Lakshman S Khiria | MCh | |
| Sarat C Jayasingh | Odisha, Long term trainee | |
| Supriyo Ghatak | MCh | |
| C Madhusudhan | MCh | |
| 2005 | MN Pawan Kumar | MCh |
| Vijay Ramachandran | MCh | |
| 2006 | Utpal Anand | MCh |
| Rajesh Gangavatikar | MCh | |
| 2007 | Amit Javed | MCh |
| Vishnu Prasad NR | MCh | |
| Mukund P Kulkarni | MCh | |
| 2008 | Vivek Mangla | MCh |
| Sumit Sanyal | MCh | |
| Gaurav N Chaubal | MCh | |
| 2009 | Sumesh Kaistha | MCh |
| Nikhil Agarwal | MCh | |
| 2010 | Elan Kumaran | MCh |
| Joseph George | MCh | |
| SP Samantaray | MCh | |
| 2011 | Senthil G | MCh |
| Ameet Kumar | MCh | |
| Rajesh Panwar | MCh | |
| Vishnu Prasad Ravella | MCh | |
| Arif Ali Khan | MCh | |
| 2012 | P Pattanaik | MCh |
| V Arun Kumar | MCh | |
| Anand Narayan Singh | MCh | |
| Vipin IS | MCh | |
| Bhabani Prasad Bordoloi | MCh | |
| 2013 | Ragini Kilambi | MCh |
| M Adil Afsan | MCh | |
| Sujeet Kumar Saha | MCh | |
| Hemant A Jain | MCh | |
| Srinivasan Ramachandran | MCh | |
| 2014 | Karthik Raichurkar | MCh |
| Vedavyas Mohapatra | MCh | |
| Ashish George | MCh | |
| Sri Aurobindo Prasad Das | MCh | |
| 2015 | Dhruv Jain | MCh |
| Pradeep Krishna RV | MCh | |
| Shruthi HS | MCh | |
| Abhishek Aggarwal | MCh | |
| Soumen Roy | MCh | |
| Tuhin Subhra Mandal | MCh | |
| 2016 | Amruth Raj C | MCh |
| Inbaraj B | MCh | |
| Ravi Shankar Biswas | MCh | |
| Gursagar Singh Sahota | MCh | |
| Pradeep Jeyakumar S | MCh | |
| 2017 | Ashish Shrivastava | MCh |
| Bhoopkishor Pathak | MCh | |
| Tanmay Datta | MCh | |
| Basant Narayan Singh | MCh | |
| 2018 | Jayapal R | MCh |
| Balakrishnan S | MCh | |
| Pradeep Kumar S | MCh | |
| Manpreet Uppal | MCh | |
| Vikash Moond | MCh |
| S No | Name of the Student | Role |
|---|---|---|
| 1 | Anand BA | Intern |
| 2 | Anil Kumar Sanwal | JR (Non-Academic) |
| 3 | Arun Goel | JR |
| 4 | Arvind Kohli | Short term trainee |
| 5 | Arvinder Soin | JR |
| 6 | Barua D | Short term trainee |
| 7 | Das NN | Short term trainee |
| 8 | Deepak Mitra | JR (Non-academic) |
| 9 | Deepak Mittal | JR |
| 10 | Gauri Bedi | Intern |
| 11 | Malini Venkatraman | Intern |
| 12 | Joshi CS | Army, Short term trainee |
| 13 | Kushal Mittal | JR (Non-academic) |
| 14 | Manu Arora | Army, Short term trainee |
| 15 | Mishra SK | JR (Non-academic) |
| 16 | Mohan Reddy V | JR |
| 17 | Narad | Short term trainee |
| 18 | Pankaj Rastogi | JR (Non-academic) |
| 19 | Panna Lal | JR (Non-academic) |
| 20 | Patnaik AM | JR (Non-academic) |
| 21 | Prasad AS | JR (Non-academic) |
| 22 | Rana Patir | SR |
| 23 | Rashmi Punj Sinha | JR (Non-academic) |
| 24 | Reddy PP | JR |
| 25 | Salilbindu Chakraborty | JR (Non-academic) |
| 26 | Sandeep Agarwala | Intern |
| 27 | Sanjay Chugh | JR (Non-academic) |
| 28 | Sanjeev Haribhakti | Short term trainee |
| 29 | ShitriBona Lotha | JR |
| 30 | Simhachalam G | Short term trainee |
| 31 | Singh SK | JR (Non-academic) |
| 32 | Srinivas Deshpande | Short term trainee |
| 33 | Subodh Adhikari | Short term trainee |
| 34 | Sudhanshu | Short term trainee |
| 35 | Sumeet Shah | Short term trainee |
| 36 | Suneet Sood | SR |
| 37 | Tariq Azad | Short term trainee |
| 38 | Vetrivel S | Short term trainee |
The department is very keen on developing Indian solutions to Indian problems. Most of the research conducted in the department is aimed at this goal. A weekly research meeting is used as a means to assess the progress in this area.
The ongoing research projects include:
We have started a programme to try and set up a clinical liver transplantation facility at the AIIMS. Regular liver transplantation journal clubs are held every week and experimental as well as clinical liver transplants are carried out as and when it is feasible or the donor is available
Journal Publication The department faculty are actively involved in the publication of The National Medical Journal of India', Tropical Gastroenterology' both of which are indexed journals and "GI Surgery Annual' which is in its twelfth year of publication.
Patients admitted for certain investigations and invasive radiological interventions are provided day-care facilities
Emergency referrals from other hospitals with the following conditions:
Gastrointestinal bleeding: variceal and non-variceal
The department has a 8-bedded ICU in D6 ward which is fully staffed with nursing, physiotherapy and paraclinical staff. It is equipped to provide invasive/non-invasive ventilatory support, critical care and hemodynamic monitoring and care for the comatose patient. Apart from the nursing staff, the ICU is manned by two Senior Residents on 24- hour duty, supported by another Senior Resident on cover duty. Supervision of ICU functioning is done on a daily basis by the Faculty on call. Patients undergoing elective/emergency surgery are managed postoperatively in the ICU for initial 48-72 hours before being moved to the general ward depending upon the clinical recovery and magnitude of the surgery.
The Department was instrumental in getting the Transplantation of Human Organs Act passed in 1994. The first orthotopic liver transplantation was done in January 1996. Since then we have developed a clinical liver transplantation facility at the AIIMS. Currently the focus is on performing deceased donor liver transplantation. Joint Multi-disciplinary Meetings (GI Surgery, Gastroenterology, Anaesthesiology, Paediatric surgery, Psychiatry) are held on a regular basis for listing prospective recipients (1st and 3rd Friday of every month). Within the department we have designated Donor and Recipient teams. Transplantation journal clubs are held every week and clinical deceased-donor orthotopic liver transplants are carried out as and when deceased donors become available. Once transplantation is done the patient is managed in Special Isolation HDU in D6 ward with dedicated nursing and 24-hr Resident support.
Our department is running regular OPD on Monday, Wednesday, Thursday, Friday & Saturday. A stoma care clinic as well as a dietician clinic is also run on the same days.
Schedule:
| Day | Consultant | Consultant | Consultant |
|---|---|---|---|
| Monday | Dr. Sujoy Pal | Dr. Nihar Ranjan Dash | Dr. Rajesh Panwar |
| Wednesday | Dr. Nihar Ranjan Dash | Dr. Anand Narayan Singh | Dr. Saurabh Galodha |
| Thursday | Dr. Nihar Ranjan Dash | Dr. Saurabh Galodha | Dr. Kailash Chand Kurida |
| Friday | Dr. Sujoy Pal | Dr. Rajesh Panwar | Dr. Anand Narayan Singh |
| Saturday | Dr. Sujoy Pal | Dr. Kailash Chand Kurida |
A specific referral to the department of GI Surgery is required to get an OPD appointment.
Appointments for OPD may be obtained either online at https://ors.gov.in/orsportal/ or offline from the patient registration counter in the new RAK OPD from 8:30 am to 10:30 am on OPD days. More details regarding offline appointment are available at https://www.aiims.edu/aiims/hosp-serv/citizen-charter/opd-services.htm
The department of gastrointestinal surgery has been actively involved in education of M.Ch. residents, MS residents and M.B.B.S. students.
The academic activities for the M.Ch. residents include a weekly audit, presentations of abstracts of recently published papers, a seminar, journal club, clinical case based discussions and presentation on research and dissertation projects. These sessions are moderated by the institute faculty as well as experts from all over the country. Besides these, a combined round with Gastroenterology and a GI Radiology conference are held once in a week, and a GE-GI Surgery histopathology conference once in two weeks.
MS (surgery) residents are posted in the department of gastrointestinal surgery for a period of 6 weeks on rotation basis. During this period they are involved in the patient care as well as the academic activities of the department.
The department is actively involved in the teaching of undergraduate students as well. The department faculty as well as senior residents teach relevant topics to 6th and 8th semester students during their surgery rotation. Besides this, the department faculty is also involved in various integrated seminars and case-based studies for the undergraduates.
The Department offers training for varying periods. Candidates who have passed MS in General Surgery from a recognized Medical College or University and have an interest in GI surgery are eligible to apply. Trainees may be sponsored by the State Governments, the Defence Services or other government organizations. Initially the candidate should contact the Head of the Department to ascertain whether there is a suitable place in the training programme and, if possible, visit the Department. If one wishes to apply for long term training (non-MCh), he or she should inform us of the duration of the intended stay (1-2 years) in the department. Once the application has been provisionally accepted by the department another application to this effect should then be sent to the Dean, AIIMS. Details of the application format and regulations governing such training are available on the AIIMS web site (http://www.aiims.edu/aiims/academic/guideline_ST_LT.htm). The various training programmes that one could apply for include:
Long term training (1 to 2 years): The candidate would be a part of the 'core' patient care team directly involved in patient care and will be expected to do first on call duties for 6 to 9 months and second on call
duties thereafter. He or she will assist in all major operations and will probably learn to perform some of them independently.
Training leading to the award of M Ch degree (3 years): For this programme candidates are selected through a two-step competitive examination held at the national level. The Department has a total of 12 positions currently; 9 for general candidates and 3 for candidates sponsored by various organizations, central and state governments, Defence Services etc. The examination includes a written test comprising of multiple choice questions. Candidates are shortlisted and called for a practical and viva-voce examination in the department. The practical examination may include case discussions, interpretation of imaging investigations and clinical problems. The dates for these examinations are announced in the national newspapers. The entrance examinations are held in May/June or November/December of any given year.The academic sessions start in January and July. Candidates are requested to refer to the prospectus issued by the Dean, AIIMS for further details.
The following number of patients was seen in outpatient: Routine OPD and special clinics during the year 2021-22.
New cases : 17790 Old cases : 35622
| Name of the clinic | New cases | Old cases |
|---|---|---|
| Liver Clinic | 901 | 6182 |
| Pancreas clinic | 664 | 2251 |
| IBD & ITB Clinic | 512 | 4121 |
| Interventional Clinic | 156 | 206 |
| Celiac Clinic | 67 | 493 |
Endoscopy services:
List of procedures being performed:
|
G.I. Motility:
High resolution esophageal manometry
High resolution anorectal manometry
Biofeedback therapy
24 hr. ambulatory PH monitoring
| Dr. Soumya Mahapatra | 2018-19 |
| Dr. Ashish Aggarwal | 2019-2020 |
| Dr. Atul Rana | 2020 Jan - Dec |
| Dr. PabitraSahu | 2020 Jan - Dec |
| Dr. Sudheer K.Vuyyuru | 2020-21 Jul - June |
| Dr. Abhinav Anand | 2020-21 Jul - June |
| Dr. Rahul Sethia | 2020-21 Jul - June |
| Dr. Gedella. V.Teja | 2021-22 Jan - Dec. |
| Dr. Srikant Gopi | 2021-22 Jan - Dec. |
| Dr. K. Bhaskar | 2021- 22 Jan - Dec. |
| Dr. Peeyush Kumar | 2021-22 Jul – June |
| Dr. Peddapulla Chandan | 2021-22 Jul – June |
| Dr. David Mathew Thomas | 2021-22 Jul – June |
| Dr. Piyush Pathak | 2021-22 Jul – June |
| Dr. Samagra Aggarwal | 2022-23 Jan – Dec |
DM Resident Alumni List:
Lists of PhD alumni:
| S.No | Name | Batch (year of passing) |
|---|---|---|
| Dr. Rakesh Kumar Tondon | 1981 | |
| Dr. Dinesh Kumar Bhargva | 1982 | |
| Dr. Nilima Raina | 1982 | |
| Dr. Yogendra Kumar Joshi | 1983 | |
| Dr. L.N. Balaji | 1989 | |
| Dr. Deepika Nayar | 1999 | |
| Dr. Geetanjali Goindi | 1999 | |
| Dr. Nandani Saxena | 2002 | |
| Dr. Priyali Pathak | 2004 | |
| Dr. Preeti Singh | 2005 | |
| Dr. Payal Bhardwaj | 2007 | |
| Dr. Shalu Midha | 2010 | |
| Dr. Jaya Joy Benjamin | 2010 | |
| Dr. Supreet Kaur | 2010 | |
| Dr. Kajal Jain | 2012 | |
| Dr. Nidhi Singh | 2012 | |
| Dr. Veena Mishra | 2013 | |
| Dr. Asha Mishra | 2015 | |
| Dr. Pooja Goswami | 2012 | |
| Dr. Namrata Singh | 2016 | |
| Dr. Sumaira Rashid | 2017 | |
| Dr. Alka Kumari | 2018 | |
| Dr. Ritika Rampal | 2018 | |
| Dr. Gajendra Kumar | 2018 | |
| Dr. Safoora Rashid | 2020 | |
| Dr. Neeti Nadda | 2020 |
Governing Council member, World Gastroenterology Organization (2021-23); Chair, Clinical Research Committee, World Gastroenterology Organization (2021-23); Council member, Asian Pacific Association of Gastroenterology (2017-23, two terms); Member of the Climate Committee and Planetary Health, World Gastroenterology Organization; Secretary general of Indian Society of Gastroenterology (2016-2022); Society Member, National Agriculture and Biotechnology Institution, Chandigarh; Society Member, Center of Innovative and Applied Bioprocessing; Editorial Advisory Board Member, Clinical and Translational Gastroenterology (American College of Gastroenterology); Member of Biosafety Committee, School of Life Sciences, JNU; Institutional Ethics Review Board (IERB), JNU, (2020 onwards); Member of the Special Committee of the Special Centre for Systems Medicine, Member; Member, ICMR Committee on the International travel grant; Member, ICMR Project Review Committee; Member, Project review and monitoring Committee, BIRAC, DBT; Member, Academic Committee, Translational Health Sciences and Technology Institute; Coordinator of the Department of Biotechnology Consortium on Celiac Disease; Group leader, Asian Pacific Working Group on Celiac disease; Coordinator of Indian Society of Gastroenterology Task Force on Inflammatory Bowel Disease; Coordinator of Young Clinician Program, Indian Society of Gastroenterology and Train the Trainer Program
Recipient of Third prize in Presidential poster category during ISGCON 2021 (Indian Gastroenterological Society, Oral paper appreciation award in the Virocon2021 (Indian Virological Society) AIIMS, Bibi Nagar, Research Associate Fellowship, ICMR (Dr. Neeti Nadda/ Dr. Nayak Mentor), Research Associate Fellowship, ICMR; Reviewer and expert committee member for Innovation & Translation Research (ITR), ICMR, Reviewer for ICMR RA and SRF, and ICMR Project review committee member for (diarrheal diseases); Reviewer to extramural funding of DST SERB, AYUSH/CCRH, ICMR STS expert group, ICMR ITR (innovation translation research)group and DBT nominee for Institute Biosafety committee (IBSC).
| Authors | Chapter Title | Name of editors | Book | Publisher | Year | pages |
|---|---|---|---|---|---|---|
| Makharia GK | Abdominal tuberculosis | Sharma SK, Mohan Alladi | Textbook of Tuberculosis and Non-tuberculous Mycobacterial diseases | Jaypee Brothers Medical Publishers | 2020 | 208-221 |
| Singh Prashant, Makharia GK | Food allergy and food hypersensitivity | Rao SSC, Young Yeh Lee, Ghoshal UC | Clinical and Basic Neurogastroenterology and Motility | Elsevier, Academic Press | 2020 | 387-395 |
| Anand Abhinav, Agarwal Ashish, Makharia GK | Non-celiac gluten sensitivity | Ajay Kumar | Gastroenterology Annual | 2019 |
| SNo | Author of Chapter | Chapter Title | Name of editor | Name of the book | Edn. | City of publication | Publisher | Year of pub. | First last page |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Alka Singh, Pooja, Govind K Makharia | Citrulline as a marker of villous abnormality and implications for diet and nutrition | Victor Preedy | Biomarkers in Disease: Methods, Discoveries and Applica | London | Springer Nature | 2022 | Under Printing |
Dr. Umesh Kapil
Completed
Advanced Centre for Liver Disease (different projects in liver diseases)
Principal Investigator : Dr. S.K. Acharya
Funding Agency : ICMR – Advanced Centre for Liver Disease
Total : Rs. 2 crore
Duration : 2004-10
Is chronic pancreatitis a pre-malignant disease?
A pilot study to estimate community prevalence of Celiac Disease.
Efficacy and Safety of Mesalamine Delayed-Release Tablets (1.2g), Par Pharmaceutical (Test Drug) in the treatment of active mild to moderate ulcerative colitis: A Double Blinded, Double Dummy, Multicentre Randomized Phase III, Comparison with Placebo and Lialda (1.2g) Mesalamine Delayed-Release Tablets, Shire US Inc (Reference Drug) – 292-07.
A multicentre (Country wide) prospective data collection of patients with Inflammatory Bowel Disease under Indian Society of Gastroenterology task force on Inflammatory Bowel Disease.
Natural Course of Immunotolent Patients with chronic HBV infectioin
Health Related quality of life in patient with chronic liver disease and effect of probiotics in the treatment of MHE and health related quality of life
Efficacy of daily iron folic acid supplementation in correction of iron deficiency anemia in children aged 3-5 years.
Resolution of Bitot’s Sports after Administration of Mega-dose of Vitamin A in a cohort of children in 1-5 years of age with Bitot’s sport
“Validity of Spot Testing Kits in the Assessment of Iodine Content of Salt-A Multicentric Study”
A Study of Mutational and Histopathological risk factors for Gallbladder Cancer in Patients with Gallstones.
“Role of TNF-α in the pathogenesis of experimental acute pancreatitis and the effect of anti-TNF-α therapy in attenuating the severity of pancreatitis and in the subsequent regeneration of the pancreas”
A multi-centric study on treatment of abdominal tuberculosis (intestinal or peritoneal): A randomized controlled trial to compare the 6 months of Cat-I treatment with 9 months of Cat-I treatment (extension for 3 months) in abdominal tuberculosis under the Revised National Tuberculosis Control Program.
Detection of Mycobacterial pathogens in patients with Crohn’s Disease.
Characterization of tight Junction proteins in patients with Crohn’s Disease and Celiac Disease.
Pathophysiology of paracellular permeability and tight junctions in the first degree relatives of patients with celiac disease.
Small intestinal and whole gut metagenome in patients with celiac disease, their first degree relatives and controls.
"Zoonotic potential of Mycobacterium avium paratuberculosis (MAP) in human Ulcero-constrictive Ileocaecal Disease"
Phase 3, Randomised, Placebo-Controlled, Blinded, Multicentre Study of the Induction and Maintenance of Clinical Response and Remission by MLN0002 in Patients with Moderate to Severe Ulcerative Colitis.
Phase 3, Randomized, Placebo Controlled, Blinded, Multicenter, Multiple Dose Study to Determine the Efficacy and Safety of MLN0002 for the Induction & Maintenance of Clinical Response and Remission in Patients with Active Crohn’s Disease.
Completed:
Ongoing:
Completed
Ongoing
The following number of patients was seen in outpatient: Routine OPD and special clinics during the year 2017-18.
Special clinics
A. Routine Gastroenterology Clinic (Monday to Friday)
New cases : 26531
Old cases : 47572
B. Special clinics:
| Name of the clinic | New cases | Old cases |
|---|---|---|
| Liver Clinic | 1463 | 13250 |
| Pancreas clinic | 707 | 991 |
| IBD &ITB Clinic | 475 | 6833 |
| Interventional Clinic | 272 | 323 |
| Celiac Clinic | 108 | 699 |
C.Endoscopy services:
List of procedures
Diagnostic and therapeutic endoscopies : 32235
Diagnostic and therapeutic colonoscopies : 4865
Diagnostic sigmoidoscopies : 4723
Sideviewing endoscopies : 1230
Endoscopic retrograde cholangiopancreatography (ERCP) : 4260
Endoscopic ultrasound (Diagnostic and therapeutic) : 930
Fibroscan 8502
G.I.Motility 191
In-Patient Services The inpatient beds and intensive care unit of the Department of Gastroenterology are located on the second floor in the main building – AB2 ward. AB2 ward has 28 beds . Intensive Care Unit The ICU is located in AB 2 ward and has 6 beds in the intensive wing and 1 bed as step down care bed. The ICU has state of the art facilities including the most sophisticated equipment including monitors, ventilators, and arterial blood gas analyzer. A Senior resident is on duty around the clock in the ICU . The nurse patient ratio is 1:1.5 |
The Department offers training for varying periods.
Training leading to the award of DM degree (3 years): Candidates who have passed MD in Internal Medicine from a recognized Medical College or University and have an interest in Gastroenterology are eligible to apply. For this programme candidates are selected through a two-step competitive examination held at the national level. The examination includes a written test followed by practical and viva-voce examination for shortlisted candidates in the written examination. The practical examination may include case discussions, radiology films and clinical problems. The dates for these examinations are announced in the national newspapers and AIIMS examination section website (https://www.aiimsexams.org/). The sessions start biannually in January and July. The entrance examinations are held in May and December for the corresponding session. Candidates are requested to refer to the prospectus issued by the Dean AIIMS for further details as well as number of seats during each session.
During this super specialization training, fellows have clinical training getting exposed to diverse patient population presenting with a broad range of GI disorders and handle all kinds of GI emergencies during this period. They are also trained in various procedures such as liver biopsy, diagnostic and therapeutic endoscopic procedures including upper GI endoscopy, colonoscopy and ERCP. They are also exposed to advanced endoscopic procedures/newer techniques such as fibroscan, portal hemodynamics, endoscopic ultrasonography and enteroscopy. They have combined clinical rounds and discussions with departments of GI surgery, radiology and pathology. They should complete one thesis/dissertation during this periods working on clinically relevant and endemic problems.
Advanced GI fellowship training (1 year): Candidates who completed their DM degree are eligible for this course; which consists of written examination and viva-voice. The sessions start biannually in January and July. Advanced GI fellowships are being conducted in following divisions: inflammatory bowel disease, hepatology, pancreas and advanced endoscopy.
Short term training programme (Observer status): This may last for 1 to 6 months. As an observer, the candidate will not be given responsibilities in patient care but will be expected to attend the clinical rounds, observe operations and participate in the academic meetings.
Training leading to award of PhD Degree: Entrance examination which consists of a multiple choice based theory examination and a viva-voce is held twice a year to select candidates for admission to PhD course.
| Name | Passing Year | Current Designation | Email ID |
|---|---|---|---|
| Dr. Swapnil Jathar | 2014 | Consultant & Physician, Elderly and Acute Medicine, Northampton General Hospital | jatharswapnil@gmail.com |
| Dr. Akash Kumar Ambastha | 2014 | Consultant, Healthworld Hospital, Durgapur, West Bengal | akash.rgkmch@gmail.com |
| Dr. Vijay Kumar | 2015 | Sr. Consultant & Head, Department of Geriatric Medicine, Primus Super Speciality Hospital, Chankyapuri, New Delhi | vjg737@gmail.com |
| Dr. Ramesh Kandel | 2015 | Consultant-Geriatrician Arogin Health Care & Research Centre, Kathmandu (Nepal), Consultant - WHO (Nepal) | drameshkandel@gmail.com |
| Dr. Gaurav R Desai | 2015 | Specialty Registrar, Oxford University Hospitals, UK | gaufed@gmail.com |
| Dr. Harjit Singh Bhatti | 2015 | Consultant, Geriatrician, Sitaram Bhartia Institute of Science & Research | harjitbhatti4@gmail.com |
| Dr. Sriniwas Thakur | 2016 | Consultant Geriatrician, Spectrum Clinic, Thane (Mumbai), Jupiter Hospital, Thane (Mumbai), Bethany Hospital, Thane (Mumbai) | yourgeriatrician@hotmail.com |
| Dr. Venugopalan G | 2016 | Associate Professor, Department of Geriatric Medicine, JIPMER Puducherry | drvenu88@gmail.com |
| Dr. Nidhi Soni | 2016 | Assistant professor, Geriatric medicine, AIIMS, New Delhi | nidhisoni1962@gmail.com |
| Dr. Hrishikesh Indani | 2016 | Consultant Geriatrcian, Shraddha Clinic, Sangamner, Maharashtra | hrishi.in2989@gmail.com |
| Dr. Rishav Bansal | 2016 | Consultant & HOD, Geriatric Medicine, Santokba Durlabhji Memorial (SDMH) Hospital, Jaipur | rishavbansal.aiims@gmail.com |
| Dr. Saroj Yadav | 2016 | Associate Consultant, Geriatric Medicine, Aakash Healthcare Dwarka, New Delhi | drsarojkr17@gmail.com |
| Dr. Kamal Bandhu | 2017 | Independent Practice, Patna, Bihar | kbandhu1@gmail.com |
| Dr. Ramesh Sah | 2017 | Senior Resident, Neurology, Nayati Medicity, Mathura | sahramesh7@gmail.com |
| Dr. Ayantika Haldar | 2017 | Registrar in Geriatrics, The Queen Elizabeth Hospital, Adelaide, Australia | ayantikahaldar@gmail.com |
| Dr. Manicka Saravanan | 2017 | Consultant Geriatric Medicine, Department of Geriatric Medicine, MGM Malar Hospital | manickasaravanan252@gmail.com |
| Dr. Pramod Kumar | 2017 | Assistant Professor, Geriatric medicine, AIIMS, New Delhi | pramodataiims.001@gmail.com |
| Dr. Shailendra Bhadouria | 2018 | Senior Resident, GR Medical College, Gwalior, M.P. | bhadouria.shailendra@yahoo.com |
| Dr. Sunny Singhal | 2018 | Assistant Professor, Department of Geriatric Medicine, SMS Medical College & Hospital, Jaipur, Rajasthan | docsunnysinghal@gmail.com |
| Dr. Sumitabh Singh | 2018 | Post hoc, Deptt. of Medicine, Division of Cardiology, University of Texas Southwestern, Dallas, Texas, USA | sumitabh1712@gmail.com |
| Dr. Mamta Saini | 2019 | Assistant Consultant, Geriatric Medicine, Mahavir Jaipuriya Rajasthan Hospital Limited, Jaipur | mamtaangel90@gmail.com |
| Dr. Abhijith R Rao | 2019 | Assistant Professor, Geriatric Medicine, AIIMS, New Delhi | abhijith.rrao@gmail.com |
| Dr. Meenal Thakral | 2019 | Classified Specialist, Artemis Hospitals, Gurgaon | drmeenal.thakral30@gmail.com |
| Dr. Gudeti Baburao | 2019 | Sr. Resident, ESIC Hospital, Hyderabad | baburaogudeti@gmail.com |
| Dr. Bhrigu Jain | 2019 | Consultant Geriatrics, Department of Internal Medicine and Geriatrics, Medanta the Medcity, Gurugram | bhrigujainaiims@gmail.com |
| Dr. Gevesh C. Dewangan | 2019 | Specialist Medicine, ESIC Hospital, Raipur. Director Vriddhacare Clinic, Raipur | gvsaiims@gmail.com |
| Dr. Ravi Sah | 2019 | Consultant Physician, Shivam Hospital, Jal Vayu Vihar, Gurgaon | ravisah76@gmail.com |
| Dr. Ananta Aryal | 2020 | Consultant Geriatrician, Nepal Korea Friendship Municipality Hospital, Bhaktpur, Nepal | rtranantaracdg@gmail.com |
| Dr. Mujtaba Waris | 2020 | Respiratory trainee (ST4), University Hospitals Sussex | mujtabawaris@gmail.com |
| Dr. Ambica Singh | 2020 | Assistant Professor, Geriatric Medicine, AIIMS, New Delhi | dr.ambicasingh.aiims@gmail.com |
| Dr. Karishma De | 2020 | Associate Consultant, Aster Malabar Institute of Medical Sciences, Kannur, Kerala | karishma.de@gmail.com |
| Dr. Sreerag P Rajan | 2020 | Consultant Geriatric Medicine, Coorporative Hospital, Payannur, Kerala | callmesrg@gmail.com |
| Dr. Akash Jaiswal | 2020 | Attending Consultant Geriatric Medicine, Fortis Memorial Research Institute, Gurugram | akash.jai123@gmail.com |
| Dr. Bhawana Painkra | 2020 | Consultant Geriatric Medicine, Rajagiri Hospital, Aluva, Ernakulam | bhawanapainkra@gmail.com |
| Dr. Yamini Ajmera | 2021 | Consultant Geriatrician, Sama Hospital, New Delhi. Founder, Vayodha Senior Care | yaminiajnera8@gmail.com |
| Dr. Bharti Kumari | 2021 | Senior Resident, Department of Geriatric Medicine, AIIMS, New Delhi | dr.lovelybharti@gmail.com |
| Dr. Akshata Rao | 2021 | Senior Resident, Department of Geriatric Medicine, AIIMS, New Delhi | akshatarao2012@gmail.com |
| Dr. Sunil Jyani | 2021 | Assistant Professor, Department of Geriatric Medicine, Mahatma Gandhi Medical College and Hospital, Jaipur | drsuniljyani@gmail.com |
| Dr. Anushree | 2021 | Senior Resident, Amrita Institute of Medical Sciences, Kochi | anushreeas45@gmail.com |
| Dr. Athul Vyas | 2021 | Specialist & Associate Coordinator, Department of Geriatrics, KIMS Health, Trivandrum | athul.vyas@gmail.com |
| Dr. Sudeep George | Sr. Resident, Deptt of Geriatric Medicine, AIIMS, New Delhi | doc.sidts@gmail.com | |
| Dr. Suman Maity | Senior Resident, Department of Geriatric Medicine, Medical College, Kolkata | maitymission01@gmail.com | |
| Dr. Subramonian Ashwin | CTF Medicine, Medway Maritime Hospital | ashwinmonian@gmail.com | |
| Dr. Monica D. Sharma | Sr. Resident, Deptt. of Geriatric Medicine, AIIMS | drmonikasharma2808@gmail.com | |
| Dr. Sakthi Kiruthika K | Sr. Resident, Deptt of Geriatric Medicine, AIIMS, New Delhi | sakthikiruthika17@gmail.com | |
| Dr. Gaurav Sharma | Consultant Geriatric Medicine, AIG Hospitals, Hyderabad, Telangana | gsonline.ktm@gmail.com | |
| Dr. Parul Bhitani | Sr. Resident, Geriatric Medicine, AIIMS, Rishikesh | ||
| Dr. Rajkr. Tata | Sr. Resident, Deptt of Geriatric Medicine, AIIMS, New Delhi | ||
| Dr. Vedula N.Mihir | Sr. Resident, Deptt of Geriatric Medicine, AIIMS, New Delhi | ||
| Dr. Saumparup Pal | Sr. Resident (Academic), Deptt. of Hosp. Medicine & Critical Care, AIIMS, Rishikesh | ||
| Dr. Swarup Dasq | Sr. Resident, Deptt of Geriatric Medicine, AIIMS, New Delhi | ||
| Dr. Yogesh Poonia | Sr. Resident, Deptt of Geriatric Medicine, AIIMS, New Delhi | ||
| Dr. Afeef A. | Asst. Geriatrician (on deputation), District Hospital, Palakkad | ||
| Dr. Arundhati S.Wariar | Trust grade Registrar, Department of Medicine for Older People, Kettering General Hospital | ||
| Dr. Shreya Biswal | Senior Resident, Geriatric Medicine, AIIMS, New Delhi | ||
| Dr. Vasu | Senior Resident, Geriatric Medicine, AIIMS, New Delhi | ||
| Dr. Richa Mallick | Senior Resident, Geriatric Medicine, AIIMS, New Delhi | ||
| Dr. Bhabhor k.Narsinhbhai | Senior Resident, Geriatric Medicine, AIIMS, New Delhi | ||
| Dr. Diparani Tekhelmayum | Fellowship in Geriatric Rheumatology, Department of Geriatric Medicine, BHU | ||
| Dr. Tejas S.R. | Senior Resident, Geriatric Medicine, AIIMS, New Delhi | ||
| Dr. Venugopal Mantry | Senior Resident, Geriatric Medicine, AIIMS, New Delhi |
| Name | Year of Training | Current Designation | Email id |
|---|---|---|---|
| Lt. Col (Dr.) Pradeep Behal | 2013-2014 | Classified Specialist Medicine and Geriatric Medicine, Officer in Charge Palliative care centre Base Hospital, Delhi Cantonment | majorbehl@gmail.com |
| Lt. Col (Dr.) Dheeraj Nauhwaar | 2016-2017 | Classified Specialist Medicine and Geriatric Medicine, currently in Democratic Republic of Congo UN Mission | dheerunauhwaar@gmail.com |
| Dr. Sumit Bhaskar | 2019-21 | NA | sumitbhasker@gmail.com |
| Name | Guide |
|---|---|
| Major (Dr.) Joyita Banerjee | Dr. A B Dey |
| Dr. Rashmita Pradhan | Dr. A B Dey |
| Dr. Masroor Anwar | Dr. A B Dey |
| Sr No | Title | Source of Funding | Year |
|---|---|---|---|
| 1 | GIS Based Surveillance of People with Dementia and Its Risk Factors among People Residing in South Delhi by Multi-Disciplinary Collaborative Approach- A Pilot Cross Sectional Study for Customized Care Plan and Policy Planning | DHR | 2022-2024 |
| 2 | Health Awareness Amongst Elderly and Family Member of India through Series of Audio Visual and Print Media, Leveraging Existing Old Age Solution Portal of the Department of Geriatric Medicine-AIIMS | Central Warehousing Corporation (CWC) | 2023-2024 |
| 3 | Development and validation of an android based application app to assess cognitive status of older people through speech, emotion and visuo-spatial pattern recognition. | DST | 2023-2025 |
| 4 | Validating Biomarker Panel in Five Different Cohorts to Define and Predict Biological Ageing, Disease Burden and Mortality in Human Subjects- A Pilot Prospective Cohort Study. | ICMR | 2023-2026 |
| 5 | Efficacy of adjunct probiotics in combination with standard of care as compared to standard of care alone in elderly patients with moderate unipolar depression: A randomized double-blind parallel-group placebo-controlled multi-center pilot trial (Site PI at AIIMS, ND) | ICMR | 2023-2025 |
| 6 | Determination of anti-aging and antioxidant potential of a Unani formulation | CCRUM, Ministry of AYUSH, Government of India | 2021-2024 |
| 7 | Blood plasma derived exosomal profiling of cytokines and chemokines in frail elderly and assessment of impact of Nordic walking intervention on exosomes | ICMR | 2023-2026 |
| 8 | Association between the Dual-Task gait performance and cognitive frailty among older adults | Intramural | 2024-2026 |
| 9 | Impact of Geriatric assessment-based intervention on Health-Related Quality of life of older patients with cancer | Intramural | 2024-2026 |
| Sr No | Title | Source of Funding | Year |
|---|---|---|---|
| 1 | Effect of Smart Nordic Walking Training on Mobility Independence in Community Elderly - A pilot Study | ICMR | 2019-22 |
| 2 | Characteristics of Indian Super Agers- A pilot prospective cohort study with a potential future predictive model | ICMR | 2019-22 |
| 3 | Harmonized Diagnostic Assessment of Dementia (DAD) for Longitudinal Aging Study of India (LASI) Genomic Study | NIH | 2019-2024 |
| 4 | www.oldagesoulutions.org- a web portal for older people and their care givers | DST | 2019-22 |
| 5 | Harmonized Diagnostic Assessment of Dementia (DAD) for Longitudinal Aging Study of India (LASI) | National Institute of Health, USA (R01) | 2015-2020 |
| 6 | Development of platform and technical guidelines for application of mobile telephony in old age care (mAging program) | M/o Health & Family Welfare | 2016-2017 |
| 7 | Longitudinal Aging Study of India (LASI) | M/o Health & Family Welfare | 2015-2019 |
| 8 | Effect Of Multimodal Intervention (Diet, Exercise, And Computer Based Cognitive Training) Amongst Elderly Subject With Subjective Cognitive Impairment (SCI) From Delhi & NCR-A Randomised Control Trial | Department of Science and Technology | 2017-2020 |
| 9 | www.oldagesoulutions.org-a web portal for older people and their care givers | Department of Science and Technology | 2018-2020 |
| 10 | Predicting frailty in Indian hospital setting; comparison of three indicators. | AIIMS Intramural Grant | 2016-2017 |
| 11 | Study of Sarcopenia: Establishment of norms for diagnosis, prevalence and risk factors in ageing North Indian population and development of preventive strategies. | Indian Council of Medical Research (ICMR) Extramural grant | 2019 - 2022 |
| 12 | National Study of Knowledge, Attitude, Perception &Medical Awareness towards a Model of – Intergenerational Engagement & Science, for Sanitation, Hygiene & Health | DST | 2019-2020 |
| 13 | Clinical Frailty Scale as a predictor of mortality in older adults with SARI- A Prospective observation study | None | 2020-21 |
| 14 | Clinical characteristics of Critically ill older adults with COVID-19: A retrospective study | None | 2020-21 |
| 15 | Metabolic syndrome and its association in outcome of covid-19 in older adults – prospective cross sectional study | None | 2020-21 |
| 16 | Performance in 6-min walk test in prediction of Covid-19 complication – A prospective observation study | None | 2020-21 |
| 17 | Collaborative Multi-centric Clinical Trial to study the effect of Ayush Rasayana (A & B) on ageing in apparently healthy elderly subjects | Central Council for Research in Ayurvedic Sciences | 2014-2017 |
| 18 | www.oldagesoulutions.org- a web portal for older people and their care givers | Department of Science and Technology | 2014-2017 |
| 19 | Predicting frailty in Indian hospital setting; comparison of three indicators. | AIIMS Intramural Grant | |
| 20 | A randomized clinical trial on the effect of Laser Therapy treatment on diabetic peripheral neuropathic pain in older adults | Lab India Healthcare Limited | 2016-2017 |
| 21 | Urinary incontinence among older Indians: Assessment of management strategies and impact on quality of life | Svenska Cellulosa Aktiebolaget SCA, India | 2015-2016 |
| 22 | Dementia care: utility and implementation of a novel non-pharmacological intervention | Ministry of Health and Family Welfare | 2014-2016 |
| 23 | Impact of age and age related functional decline on cancer care | Ministry of Health and Family Welfare | 2012-2015 |
| 24 | A study of health and functionality of the oldest old in a tertiary health care setting | Ministry of Health and Family Welfare | 2012-2015 |
| 25 | Impact of nutritional supplementation and rehabilitation in pre-frail older patients in Geriatric Department of a Tertiary care hospital in India | Ministry of Health and Family Welfare | 2012-2015 |
| 26 | Impact of regulatory T-cells on host immunity among older pulmonary | Indian Council of Medical Research | 2012-2014 |
| 27 | Development of a web-portal directed at welfare of older people | Department of Science and Technology | 2008-2013 |
| 28 | Health emergencies in older people: predictors of hospital revisit | Indian Council of Medical Research | 2008-2012 |
2D Echocardiography
Physiotherapy
Dietician
Gait and Balance Assessment
Gait and Balance Training
Vaccination
Laser Therapy for Diabetic Peripheral Neuropath
Geriatric Medicine Location : National Cener for Agenig (NCA)
General Ward Beds – 32
ICU Beds – 10
Short Admission – 10
Private Ward Beds – 12
Geriatric Medicine- Ground Floor, National Center for Ageing ( NCA)
Days and Timing: Daily (Monday to Saturday)
Registration timing: 8:30am-11:00am
If you are a new patient Click here
If you are a new patient Click here
If you are a new patient Click here
| Days | Faculty members in OPD | Clinic |
|---|---|---|
| Time: 9.00 A.M. to 1. 00P.M | Time : 2.00 P.M. - 5.00 P.M | |
| Monday | Dr. Pramod Kumar & Dr. Ambica Singh | |
| Tuesday | Dr. Prashun Chatterjee, Dr. Nidhi Soni & Dr. Abhijith R. Rao | |
| Wednesday | Dr. Avinash Chakrawarthy, Dr. Pramod Kumar & Dr. Ambica Singh | Memory Clinic |
| Thursday | Dr. Nidhi Soni & Dr. Abhijith R. Rao | Geriatric Oncology Clinic |
| Friday | Dr. Prashun Chatterjee & Dr. Pramod Kumar & Dr. Ambica Singh | |
| Saturday | Dr. Avinash Chakravarty, Dr. Nidhi Soni & Dr. Abhijith R. Rao |
Older Indians carry a large burden of disease and disability and pose a tremendous challenge for the health sector as well as also social and economic infrastructure. Several initiatives of Government of India namely: National Policy on Older Persons, National Health Policy, National Population Policy, Maintenance and Welfare of Parents and Senior Citizens Act, 2007 and the National Program for Health Care of the Elderly launched in the financial year 2010-11, have emphasized the need for provision of quality and specialist health care of the older population. Specialized training in the field of gerontology and Geriatric medicine has become the need of the hour to realize the state initiatives in old age care.
The goals of this curriculum are to create a cadre of health professionals in the care of the older people; who would:
After completion of post graduation in Geriatric Medicine, the physician should be able to fulfill the following objectives:
Anatomy, Physiology, Biochemistry, Pharmacology, Microbiology, Pathology, Forensic and toxicology
Introduction to Clinical Medicine: Headache, chest pain, abdomen pain, joint pain, chills and fever, lassitude and asthenia, dyspnea, cough, hemoptysis, cyanosis, edema, palpitations, nausea and vomiting, dysphagia, gastrointestinal bleeding, jaundice, ascites, weakness, sexual dysfunction, tremor, chorea, athetosis, syncope, dizziness and vertigo, disorders of sensation and motor weakness,delirium, memory loss, sleep disorders, convulsions, anemia, carcinoma of unknown primary.
Immunological Factors in Disease: Components of immune system, mechanism of the immune response, immune deficiency and lympho-proliferative disorders, types of immune reaction and their relation to disease, suppression of immune reactions and its effects, Sjogren’s syndrome, systemic lupus erythematosus, vasculitis and sarcoidosis.
Infection and Diseases: Nature of microorganisms, epidemiology and spread of infections, defense of human host, diagnosis of infections, pyrexia of unknown origin, streptococcal infections, staphylococcal infections, typhoid, tetanus, brucellosis, sexually transmitted infections, hospital acquired infections, gram negative bacterial infections, anaerobic infections, fungal infections, parasitic infections, tuberculosis and HIV.
Chemotherapy of Infections: Antibiotics and other antibacterial agents, anti-virals, anti-fungals, anti-retroviral, anti-parasitic therapy and antimicrobial stewardship.
Disturbances in Electrolyte and Water Metabolism: Hyper- and hyponatremia, hyper- and hypokalemia, calcium and magnesium metabolism, disturbances in h+ ion concentration.
Diseases of the Cardiovascular System: Cardiac arrhythmias, heart failure, valvular heart disease. ischemic heart disease, pericardial diseases, cardiomyopathies, myocarditis, atherosclerosis, hypertension, diseases of the aorta, peripheral vascular disease, deep venous thrombosis.
Diseases of the Respiratory System: Disease of the upper respiratory tract, bronchial asthma, chronic obstructive pulmonary disorder (COPD), cor-pulmonale, bronchiectasis, interstitial lung disease (ILD), occupational and environmental lung disease, sleep apnea, acute and chronic respiratory failure, neoplasm of lung, diseases of pleura, mediastinum and diaphragm.
Diseases of the Gastrointestinal System: Diseases of the esophagus, gastro-esophageal reflux disorder (GERD), peptic ulcer, gastritis and other diseases of the stomach, inflammatory diseases of small and large intestine, diverticulosis, malignancy of stomach, colon; mal-absorption syndrome, diseases of the peritoneum.
Diseases of the Liver and Biliary Tract: diagnostic procedures in liver disorders, derangement of hepatic/ biliary metabolism, acute hepatitis, chronic active hepatitis, cirrhosis of liver, tumors of liver, suppurative diseases of liver, infiltrative and metabolic diseases of liver, disorders of gall bladder and bile duct.
Diseases of the Pancreas: Diagnosis of pancreatic diseases, acute and chronic pancreatitis, Tumors of pancreas.
Diseases of the Kidney and Urinary System: Acute renal failure, chronic kidney disease, dialysis, glomerulonephritis, nephrotic syndrome, vascular diseases of the kidney, infections of the urinary tract, obstructive uropathy, urinary incontinence, nephrolithiasis.
Diseases of the Endocrine System: Hypothalamus and pituitary gland, hyper- and hypothyroidism; hyper- and hypoparathyroidism; diabetes mellitus, hyperinsulinism / glucagon and its effects; diseases of the adrenal cortex and medulla; diseases of the testes and ovaries, disorders of bone and mineral metabolism, osteoporosis and metabolic syndrome.
Diseases of Blood and Blood Forming Organs: Blood formation and destruction, 2, bone marrow failure, blood groups and blood transfusion; abnormal hemoglobins, myeloproliferative disorders, leukemia, lymphomas, amyloidosis, plasma cell disorders, diseases of spleen and reticulo-endothelial system, febrile neutropenia, disorders of platelets, hemorrhagic disorders, coagulation disorders, antiplatelet, anticoagulant and fibrinolytics, chemotherapy and it side-effects.
Diseases of Connective Tissue, Joints and Bones: Osteoarthritis, Rheumatoid arthritis, including late onset rheumatoid arthritis (LORA), spondyloarthritides, polymyalgia rheumatica, fibromyalgia, gout and pseudo-gout, tumor of bone.
Diseases of the Nervous System: Diagnostic methods in neurology, coma, headache, epilepsy, sleep disorders, dementia, diseases of cranial nerves, cerebro-vascular diseases, diseases of the spinal cord, diseases of the peripheral nervous system and muscles, diseases of the autonomic nervous system, Parkinson’s disease and other movement disorders, pyogenic infections of the CNS, viral infections, multiple sclerosis and other demyelinating diseases; metabolic and nutritional diseases of brain; degenerative diseases.
Diseases of the Skin: Skin lesions of general medical significance, generalized pruritus, pigmentation of the skin, disorders of melanin metabolism, photosensitivity and other reactions to light; hirsutism and alopecia; cutaneous manifestations of internal malignancy, Psoriasis, Scabies, Fungal infections of skin.
Psycho-Geriatrics: Epidemiology of mental disorders in the elderly, definition and classification of psychiatric disorders, delirium /acute confusional state, depression in old age, bipolar disorder, functional psychiatric disorders in old age, personality and behavioral disorders, psycho-geriatric service - principles of treatment.
Critical care Medicine: Sepsis and septic shock, shock and cardiac arrest, cardiopulmonary resuscitation, neurological critical care, oncological emergencies, mechanical ventilation, nutrition in critically ill, respiratory critical care, analgesia and sedation in ICU, fever in ICU, fluid and inotrope management.
Management of Psychiatric Illness: Alcoholism and other substance abuse, care-giver problems, depression and other mood disorders, acute psychosis and other psychotic disorders, anxiety disorders, somatoform and somatization disorders.
General: Demography, world trends, Trends in India and developing countries, the aged and society – past and present, evolution of geriatric medicine.
Gerontology: Normal and abnormal ageing, theories of ageing, metabolic and structural aspects of ageing, biochemical changes in the normal ageing brain, ageing in tissues and cells, atherosclerosis and ageing, ecology of human senses, the milieu interior and ageing.
Geriatric Medicine: How are older patients different; common patterns of disease in old age, frailty, alteration in pain and temperature responses, missing symptoms, complications of illness, non-specific presentations, masking by known disease, history taking in the elderly, physical examination of the old patient, comprehensive geriatric assessment.
Investigations in the elderly: Policy and interpretation; Radiological, hematological and biochemical investigations; ECG, Urinalysis, Radio isotope tests; Bone Scan; Imaging – ultrasound, CT Scan, MRI and PET Scan; How much to investigate; Concept of normal range.
Immunology: Genetic aspects of immunity and immunological diseases; mutation, alternative theories of ageing, cancer, immunological surveillance.
Nutrition: Nutritional requirement; changes in total body mass and body composition; nutritional assessment, nutritional deficiency in old age, vitamin D, iron, trace elements, vitamins, recommended intake of nutrients, prevention of nutritional deficiency.
Cardiovascular System: Physiology and pathology of cardiovascular system in old age; investigation of heart diseases in old age, cardiac arrhythmias, coronary artery disease and acute myocardial infarction; hypertension and hypertensive heart disease; postural hypotension, valvular heart disease, chronic congestive heart failure, aortic aneurysm, infective endocarditis, peripheral vascular disease, deep venous thrombosis and pulmonary embolism.
Endocrine and Metabolic Disorders: Changes with ageing, diabetes mellitus, diseases of the pituitary, parathyroid, and thyroid; obesity, sexual dysfunction, disorders of sodium, potassium, calcium, magnesium and zinc; disturbances of fluid metabolism, hyperpyrexia / heat stroke.
Central Nervous System: The ageing brain, vascular lesions of the central nervous system, dementia, degenerative disorders including Parkinsonism, head trauma, infections of the nervous system, epilepsy, peripheral neuropathy, disorders of spinal cord and nerve roots; neoplasia.
Genitourinary System: Structural changes with ageing, acute and chronic renal failure; infections of the genitourinary tract, diseases of the bladder and prostate; urinary incontinence, ageing changes in the genital tract, post-menopausal bleeding, gynecological disorders in the elderly.
Disorders of the Special Senses: Disorders of the eye, Hearing disturbances, Disturbance of taste and smell; Dental problems.
Infections in the Elderly: Host defenses – natural barriers; white cell response, immune mechanism; diagnosis of fevers, urinary tract infection -diagnosis and treatment; pneumonias -cause, diagnosis and treatment; septicemia, bacterial endocarditis, antibiotic treatment, rational use of antibiotics, vaccination of elderly.
Gastro-intestinal System: Changes with age, investigations of the gastro-intestinal tract, disorders of the mouth, GERD, hiatus hernia, acid peptic disease, disease of the pancreas, diseases of the small intestine, diseases of the large intestine, fecal incontinence, gi malignancy, disease of the liver and biliary system; constipation – prevention and management.
Respiratory System: Changes with age, infections of the respiratory system, chronic obstructive airway disease, bronchial asthma, cor pulmonale, bronchogenic carcinoma, respiratory abnormalities in extra-pulmonary conditions, respiratory failure.
Musculoskeletal System: The ageing joints, gait and balance impairment, degenerative joint disease, gout and pseudo-gout; rheumatoid arthritis, infective arthritis, myopathy, myositis, polymyalgia rheumatic, temporal arteritis, osteoporosis, osteomalacia.
Hematopoietic System: Changes with ageing, anemia in the elderly, the leukemia and lymphomas; paraproteinaemia, myelodysplastic syndromes, disorders of hemostasis.
Dermatology: The ageing skin, pruritus, cancers/benign lesions, pemphigus and pemphigoid; senile purpura, herpes zoster, intertrigo, leg ulcer.
Malignancy in old age: Incidence, clinical significance, Presentation, investigation and management; counseling.
Pharmacological Aspects of Ageing: Pharmacokinetics in the elderly, pharmacodynamics, drug selection and dosage; drug interactions, adverse drug reactions, drug compliance, drug misuse.
Surgery in the Elderly: Pre-operative assessment, priorities for surgery, surgical emergencies, fractures, gangrene –amputation, elective surgery, post-operative problems and management; anesthesia in old age.
Special Problems: Pressure sore, care of the chronically ill, care of patients with terminal illness; religion and illness; falls; nursing home placement, ortho-geriatric care.
Preventive Geriatrics:
Rehabilitation:
Advances in Geriatric Medicine: Alzheimer’s disease, Parkinsonism, osteoporosis, urinary incontinence, falls / prevention of fractures, parenteral nutrition, stroke clinic and memory clinic; anti-ageing research
Duration: 3 years
1st year: First 6 months Geriatric Medicine and Rotation in periphery
2nd year: Rotation in peripheryand Geriatric Medicine
3rd year: Rotation in periphery and Geriatric Medicine
Rotations include: Geriatric Medicine: 18 months; Emergency Medicine (2months), Pulmonary Medicine (1 months), Intensive Care Unit (3months), Cardiology (2 month), Neurology (2 months), Hematology (15 days ), Physiotherapy (15 days), Rheumatology (15 days), Psychiatry (15 days), Gastroenterology (1 month), Endocrinology (1 month), Nephrology (1 month), Medical Oncology (1 month), Palliative Medicine (15days) and Day Care and Special Clinics (45days)
Procedures’ skills performed: IV line insertion, arterial line insertion, central line insertion, endo-tracheal intubation, bone marrow biopsy, thoracocentesis, peritoneocentesis, lumbar puncture, ICD insertion, peritoneal catheter insertion, foley’s catheter insertion, point of care ultrasound,synovial fluid aspiration, intraarticular injection,skin biopsy,nerve biopsy, muscle biopsy etc.
Procedures’ skills observed: Angiography, 2 D-echocardiography, Endoscopy, Colonoscopy, Fibroscan, Bronchoscopy, Dialysis, Renal biopsy, Plasmapheresis, NCV/ EMG etc.
Educational strategies: It should be problem oriented as well as integrated with other disciplines. Apart from that the curriculum should be both hospital and community oriented.
Teaching method: Teaching methods should include the following:
Internal Assessment is mandatory in postgraduate curriculum in AIIMS. It should be valid, objective and reliable; it should cover cognitive, psychomotor and affective domains. The Internal Assessment should be conducted in theory and clinical examination. The thesis is assessed separately.
Feedback from the internal assessment should be given to the students, and contribute towards final evaluation.
Assessment
| Academic Activities | Assessment |
|---|---|
| Journal Club/Seminar | Assessment after each session |
| Theory Assessment | End of every semester (80) |
| Practical Assessment | End of every semester (80) |
End Assessment: At the end of the training programme
Thesis
Thesis will be submitted by each candidate at least six months before the theoretical and practical examination. The thesis shall be examined by a minimum of three examiners; one internal and two external examiners, who shall not be the examiners for theory and practical; on the acceptance of the thesis by two examiners, the candidate shall appear for the final examination.
Theory:Theory consists of four papers:
| Paper I | Applied Basic Sciences |
| Paper II | General Medicine and Psycho-Geriatrics |
| Paper III | Geriatric Medicine |
| Paper IV | Social and Preventive Geriatrics including rehabilitation, and advances in geriatrics |
Theory Examination:
| Paper | Title | Duration | Max. Marks |
|---|---|---|---|
| Internal Assessment | 80 | ||
| 1 | Applied Basic Sciences | 3 hours | 80 |
| 2 | General Medicine & Psycho-Geriatrics | 3 hours | 80 |
| 3 | Geriatric Medicine | 3 hours | 80 |
| 4 | Social & Preventive Geriatrics including, Rehabilitation & Advances in Geriatrics | 3 hours | 80 |
Clinical:
Clinical examination will comprise of 4 cases with different problems and will carry 80 marks each and the candidate will be provided 45 minutes to complete the evaluation. The candidate will be assessed for his/her ability to complete total assessment and management of medical and social problem with stress on multiple pathologies. The communication skills and case sheet writing skill shall also be evaluated. Score out of 80 marks from internal assessment will be added to the final tally.
Practical:
X-ray, ultrasound, CT, MRI, ECG, biochemical report, psychiatric assessment, retinal assessment via Ophthalmoscope
Oral and Practical
Books
Journals
With one of the best residency programmes, the department of geriatric medicine boasts of training its residents extensively in various aspects of health care of elderly. The goal is to create a cadre of health professionals in the care of the older people who would:
The MD students (Junior Residents) are posted within the ward of the department for 18 months. During this period they are also posted in High Dependency Unit (HDU) where they manage critically ill patients including those requiring mechanical ventilation following a well-defined protocol (acute care for elderly). Besides the in-patient management, the residents also attend to the patients in OPD and other clinics (memory clinic and fragility fracture clinic). They also learn and perform various short procedures such as thoracocentesis, lumbar puncture, paracentesis, bone marrow biopsy, central line placement etc. during this period.
For the remaining 18 months they are rotated through various medical specialties including 3 months in Intensive Care Unit and 2 months in Emergency Medicine/Medical Casualty. Rotation in other clinical departments includes Cardiology, Neurology, Pulmonary Medicine and Sleep Disorders, Nephrology, Hematology, Medical Oncology, Gastroenterology, Rheumatology, Endocrinology, Psychiatry and Palliative Medicine. During these rotations, the junior residents attend OPD of the respective department along with their various clinics and additionally take part in ward duties, clinical rounds and patient management. Additionally, they are also posted in Geriatric Day care where they are trained in other aspects of geriatrics including orthogeriatrics, nutrition and physiotherapy.
During the 3 years of residency, the junior residents are also supposed to present various academic presentations including seminars, journal clubs, short clinical lectures and weekly audit. They are also required to submit an original thesis as a partial requirement for MD degree. Additionally, they are encouraged to participate and present in various national and international conferences.
Since its establishment the Department has trained 19 doctors and awarded them MD Geriatric Medicine degree.
The department also provides scope for registration for PhD in Geriatric Medicine and Gerontology. Two scholar have been awarded Ph D since inception of the department on 2012.
In addition to postgraduate and PhD training in Geriatric Medicine, the department is also involved in following programs:
| Name of the course | Details of admission |
|---|---|
| MD (Geriatric Medicine) | Session- January and July |
| Ph. D | Session- January and July |
तच्चक्षुर्देवहितंपुरस्ताच्छुक्रमुच्चरत् |
पश्येमशरद: शतंजीवेमशरद: शत |
श्रुणुयामशरद: शतंप्रब्रवामशरद: शतमदीन: स्यामशरद: शतम् |
भूयश्चशरद: शतात् ||
यजु. 36/24
O Benefactor of Devotees, I concentrate on Thy pure energy. Give me perfect health. May my eyes, ears, tongue and the other organs function in a proper and healthy way for a hundred years! May I not become helpless and dependant!
The Institute gets grants under the Heads Salaries, General & Capital Creation from the Government of India, Ministry of Health and Family Welfare. In addition, grants are received for National Drug Dependence Treatment.. Besides, extramural grants are also received from various external funding agencies such as ICMR, DST, CSIR, WHO, UNICEF, DBT, etc. for various research projects. Grant received from the Government of India under these three heads and other agencies are further allocated to various Centres/Departments/Research Projects as per their projections/requirements.
Finance Division of the Institute monitors/controls the expenditure against the above funds/budget by obtaining monthly expenditure from the respective centers/units/departments and also administers day to day financial matters, payment of salaries to faculty and staff, payment of personal claims, pension and GPF in respect of the employees of the institute. At the time of making the payment, all the checks as prescribed by the Government of India are being exercised by the respective DDOs cum Accounts Officers.
Budget-related: FD’s Budget wing is responsible for calling for annual requirements from various Centres / Departments / Divisions to formulate projections for next year. The Budget Estimates/Revised Estimates are sent to Ministry of Health & Family Welfare for allocation of Budget in the above three heads.
Project Formulation & Appraisal: Institute is growing in terms of load of patient-care, medical education & research. There are several ongoing projects of very high value and critical to carry out the mandate of AIIMS. The FD assist the Director, Standing Finance Committee & Governing Body of AIIMS and MoHFW/Government in ensuring compliance, prioritization and concurrence of projects.
Financial Concurrence: There are proposals on account of procurement of Machinery & Equipment, Rate Contract for chemicals, medicines, consumables, contract for works & services etc. received in FD for financial concurrence / advice. The scrutiny by FD is critical to ensure best value for money to public exchequer.
Scrutiny of bills for payment: Bills on account of personal claims, procurement of good & services through GeM, tendering etc. are processed and paid. While making payments, all prescribed checks are exercised by the FD. The FD caters to more than 15,000 employees & pensioners and over 2500 students & Residents.
Internal Audit: With increased activities and expansion of AIIMS, the number of units required to be audited annually has gone up substantially. The Internal Audit of the Institute is a continuous & mandatory process as the Ministry as well as the Office of the DGACE has emphasized upon the need to strengthen the internal audit of the Institute so that the procedural faults, if any, can be brought to the notice of the concerned authorities at initial level and rectified there only.
Accounts & Audit: AIIMS, being Central Autonomous Body, has to compile the Annual Accounts by 30th June each year and present the same for audit by C&AG’s team. The Audited Utilization Certificates (UCs), of previous year’s Grant-in-Aid releases to Institute, are required to be sent to the Ministry for further continued budgetary support. The Annual Accounts, along with Separate Audit Report & Audit Certificate, is received by 31st October and tabled by MoHFW in the Parliament by 31st December.
All the above works are executed by the Financial Advisor, Finance and Chief Accounts Officers (F&CAOs)/Account Officer under the overall control of Senior Financial Advisor.
The Clarification/orders have been issued by M/o Finance & DOPT for TA/LTC.
| S.No. | Name | Month | Year of Passing |
|---|---|---|---|
| 1. | Dr. Tirath Das Dogra | Dec. | 1976 |
| 2. | Dr. Purna Chandra Dikshit | Dec. | 1977 |
| 3. | Dr. Surinder Ticku | Dec. | 1977 |
| 4. | Dr. Damyanti Thakur | Dec. | 1978 |
| 5. | Dr. Ravindra Kumar Gehlot | Dec. | 1978 |
| 6. | Dr. Sunil Kumar Khanna | Dec. | 1981 |
| 7. | Dr. Lallukhum Fimate | Dec. | 1981 |
| 8. | Dr. Anil Aggarwal | May | 1982 |
| 9. | Dr. Banwari Lal Meel | May | 1982 |
| 10. | Dr. Sudhanshu Raj Sharma | Dec. | 1983 |
| 11. | Dr. Balbir Kaur | May | 1984 |
| 12. | Dr. Anil Kumar Tripathy | Dec. | 1984 |
| 13. | Dr. Gopal Krishna Chaubey | May | 1985 |
| 14. | Dr. Rohitashwa | May | 1985 |
| 15. | Dr. D. V. Saharan | Dec. | 1985 |
| 16. | Dr. Ramesh Kumar Sharma | Dec. | 1985 |
| 17. | Dr. Pankaj Vats | May | 1986 |
| 18. | Dr. Satish Kr. Verma | Dec. | 1986 |
| 19. | Dr. Somadutta Sharma | Dec. | 1986 |
| 20 | Dr. Daya Nand Bhardwaj | May | 1987 |
| 21 | Dr. Mahender Singh Sagar | Dec. | 1988 |
| 22 | Dr. Subhash Chander Mehta | Dec. | 1988 |
| 23 | Dr. Ginya Bomjen | Dec. | 1993 |
| 24 | Dr. Bharat Lal Meena | May | 1994 |
| 25 | Dr. Bishwanath Yadav | May | 1996 |
| 26 | Dr. Lal Rozama | May | 1997 |
| 27 | Dr. Prabir Kumar Deb | May | 1998 |
| 28 | Dr. Ranjit Kumar Das | Dec. | 1998 |
| 29 | Dr. Millo Tabin | Dec. | 1999 |
| 30 | Dr. Prashant Kulshrestha | May | 2001 |
| 31 | Dr. G. A. Sunil Kr. Sharma | May | 2001 |
| 32 | Dr. Farida Noor | May | 2001 |
| 33 | Dr. Sanjeev Lalwani | May | 2002 |
| 34 | Dr. Amarantha Donna Ropmay | Dec. | 2002 |
| 35 | Dr. Varun Dixit | May | 2003 |
| 36 | Dr. Shyamal Chandra Sarkar | May | 2003 |
| 37 | Dr. Shalini Girdhar | Dec. | 2003 |
| 38 | Dr. Abhijit Rudra | May | 2004 |
| 39 | Dr. Ravi Raut Ji | May | 2004 |
| 40. | Dr. Chittaranjan Behera | May | 2004 |
| 41. | Dr. M. G. Jayan | May | 2004 |
| 42. | Dr. Parthasarathi Pramanik | Dec. | 2005 |
| 43. | Dr. Arvind Kumar | Dec. | 2006 |
| 44. | Dr. Siva Prasad Yellasiri | May | 2007 |
| 45. | Dr. Raghvendra Kumar Vidua | Dec. | 2007 |
| 46. | Dr. Sunay Mahesh | Dec. | 2008 |
| 47. | Dr. Sudipta Ranjan Singh | Dec. | 2008 |
| 48. | Dr. Akhilesh Raj Jhamad | May | 2010 |
| 49. | Dr. Ashish Jain | May | 2010 |
| 50 | Dr. Manish Goyal | May | 2010 |
| 51 | Dr. Shashank Pooniya | May | 2012 |
| 52 | Dr. Hari Prasad | May | 2012 |
| 53 | Dr. Asit Kumar Sikary | Dec | 2012 |
| 54 | Dr. Karthik Krishna | May | 2013 |
| 55 | Dr. Munish Sharma | May | 2013 |
| 56 | Dr. Rajanikanta Swain | May | 2013 |
| 57 | Dr. Hansraj Singh | May | 2014 |
| 58 | Dr. Rajesh Kumar | May | 2014 |
| 59 | Dr. Deepak Prakash | May | 2014 |
| 60 | Dr. Piyush Sharma | May | 2015 |
| 61 | Dr. Manjul Bijarnia | Dec. | 2015 |
| 62 | Dr. Mantaran Singh Bakshi | May | 2016 |
| 63 | Dr. Mohan Singh Meena | May | 2017 |
| 64 | Dr. Krishna Kumar Singh | May | 2017 |
| 65 | Dr. Shyam Kishore | May | 2017 |
| 66 | Dr. Shivani Dhaka | Dec | 2017 |
| 67 | Dr. Jay Narayan Pandit | Dec | 2019 |
| 68 | Dr. Vanika | June | 2020 |
| 69 | Dr. Ruchi Kumari | June | 2020 |
| 70 | Dr. Ramesh Babu | June | 2020 |
| 71 | Dr. Zahid Ali CH | Dec. | 2020 |
| 72 | Dr. Naresh Jeengar | Dec. | 2020 |
| 73 | Dr. Aravindan V | June | 2021 |
| 74 | Dr. Reisha Rejal | Dec | 2021 |
| 75 | Dr. Balaji D | Dec | 2021 |
| 76 | Dr. Alex Eldo Simon | June | 2022 |
| 77 | Dr. Raveena Divya | Dec | 2022 |
| 78 | Dr. Aditya Kumar Chauhan | June | 2023 |
| 79 | Dr. Gokul G | Dec. | 2023 |
| 80 | Dr. Manivel | Dec. | 2023 |
| 81 | Dr. Ajay Kumar | Dec. | 2023 |
| 82 | Dr. Pawan Kumar | May | 2024 |
| 83 | Dr. Pooja Gupta | May | 2024 |
| S.No. | Name | Month | Year of Passing |
|---|---|---|---|
| 1. | Dr. Hema | Mar. | 1983 |
| 2. | Dr. Satya Prakash Saxena | Jan. | 1986 |
| 3. | Dr. Anupuma Raina | Jan. | 1997 |
| 4. | Dr. Yukti Sharma | Sept. | 2005 |
| 5. | Dr. Somia Bashir | Sept. | 2005 |
| 6. | Dr. Bhuvnesh Yadav | Sept. | 2009 |
| 7. | Dr. Jaya Raj | Oct. | 2014 |
| 8. | Dr. Mohineesh | Oct. | 2014 |
| 9. | Ms. Anita Yadav | Aug. | 2018 |
Evaluation of vitreous humour as a bio matrix for the quantification of drugs and chemicals in postmortem forensic investigation.
We are providing service for disputed paternity test referred by Police and Court only.
Department of Forensic Medicine and Toxicology is having well established Toxicology laboratory for doing analysis of following tests.
Toxicology laboratory is equipped with the following major sophisticated analytical equipments for day today work.
Toxicology laboratory regularly provides short term and long term training to the students from India and abroad. Laboratory also supports research work for M.D. and Ph.D.students

A state of the art digital radiological unit, first of its kind in the country has been established at the AIIMS mortuary. It is the first step of the Department towards the goal of Virtual Autopsy, the technique in which the cause of death is decided without the dissection of the body with the help of radiological investigations. Virtual autopsy (virtopsy) is a new concept and involves a full-body computed tomography and magnetic resonance imaging examination to obtain two-dimensional and three-dimensional documentation. It has been proposed as an alternative to conventional autopsy in cases when the next of kin oppose or do not want the body to be dissected and as a complementary tool for better visualization of postmortem findings.
The digital X-ray unit is being used in the department as a powerful tool in the postmortem examination. It can detect even the minute fractures invisible to the naked eye. The cutting edge technology is less time consuming and promises to be a boon for interpreting findings from imaging studies to aid in Medicolegal Investigations. Radiological studies are instrumental in autopsy cases involving the location of foreign bodies within the body (i.e., bullets, gas emboli) and other mechanical injuries.
Age estimation in both living and dead is being conducted by the digital X-rays. Age estimation of the living as well as of cadavers relies heavily on data regarding growth and developmental stages of the individual as obtained from dental and skeletal radiographs. Identification is one of the usefulness of the digital X-ray which is worth mentioning. Antemortem and postmortem radiographic comparison is a routinely adopted procedure in the identification of unknown human remains. The use of radiographs in routine and mass disaster identification has long been in effect.
The digital X-ray unit is maintained by a Radiographer under a Faculty Incharge. The facility has computerized record keeping which expedites the retrieval of individual x-ray films. The radiographs can be sent in the soft copy for further consultation.

DIGITAL X-RAY UNIT
CONSOLE ROOM WITH
CONTROLLING STATION
The Forensic Histopathology Laboratory primarily deal in processing the samples of medico legal cases which comes under the jurisdiction of AIIMS i.e. south and southeast district of Delhi. Besides these, Academic samples of thesis of M.D. Doctors and Ph D students are also processed in the laboratory.


The department is providing embalming services in medicolegal cases required for transportation of dead body to faraway places in India and abroad. It is also done to preserve bodies for future dissection/teaching purpose. In rare occasions the embalming is done on the dead body of important personality for public view.
A charge of INR 8000/- in cash only, is to be deposited in the Hospital Cash Counter. If the cash counter is unable to receive the payment due to any technical problem then the charges are collected by the staff in charge of mortuary before the embalming procedure. A receipt of cash payment is handed over to the relatives. The staff shall deposit the amount on the next working day at Accounts section and obtain the original receipt.
Round the clock supervision of Casualty is maintained for imparting Expert Opinion (medicolegal services) in requisite cases belonging to jurisdiction of South and South East Delhi. These include cases of injury, sexual offences, poisoning and other complicated medico-legal cases. The department is attending all the calls pertaining to medical examination in police & judicial custody.
The Department of Forensic Medicine conducts the Medicolegal Examination of accused of sexual assault. The Jurisdiction of the cases dealt in the department is the same as that of the Postmortem Cases i.e. South and Southeast District of Delhi.
AIIMS caters to the jurisdiction of all police stations under south and south-east districts of Delhi which include magistrate inquest cases, board cases and exhumation cases. There are two mortuaries – one at main hospital and other at Trauma centre.
The Department provides medico-legal postmortem services on all days of the week during normal working hours i.e. Monday to Friday: 9AM to 5PM and on Saturdays: 9AM to 1PM. The services are also provided on Sunday from 9AM to 1PM.
The Department of Forensic Medicine provides the Mortuary services and preserves dead bodies under the following situations:


The department is actively engaged in undergraduate and postgraduate teaching activities. Currently eight postgraduate students and five PhD students are enrolled in the department. The department is also imparting short-term/Long-term training in Toxicology & DNA Fingerprinting to B.Sc./M.Sc students of other universities from all over the country. The departmental faculty also imparts education by giving guest lectures to allied personnel’s like Doctors, Judges, Police Officials, Forensic Scientists through various agencies like NICFS, NIHFW, CDTS, CBI, NIA.
| Days | Faculty and Room No | Clinics |
|---|---|---|
| Monday | Dr. Rajesh Khadgawat (C-318) Dr. Yashdeep Gupta (C-319) Dr. Rahul Gupta (C-316) | Pediatric & Adolescent Endocrinology Clinic (PAEC), Time 2-5 PM Dr. Rajesh Khadgawat Dr. Viveka P Jyotsna |
| Tuesday | Dr. Nikhil Tandon (C-318) Dr. Ravinder Goswami (C-319) Dr. Viveka P Jyotsna (C-317) | |
| Wednesday | Dr. Yashdeep Gupta (C-319) Dr. Alpesh (C-317) Dr. Rahul Gupta (C-316) | |
| Thursday | Dr. Nikhil Tandon (C-318) Dr. Ravinder Goswami (C-319) Dr. Viveka P Jyotsna (C-317) | |
| Friday | Dr. Rajesh Khadgawat (C-318) Dr. Alpesh (C-317) Dr. Rahul Gupta (C-316) | Gestational Diabetes Mellitus Clinic (C-319) Time: 9 AM - 1 PM |
| Saturday | No Endocrine Clinic | Diabetes of Young Clinic (DOY) Time: 9 AM - 1 PM Dr. Nikhil Tandon Dr. Ravinder Goswami Dr. Alpesh Goyal |
| Endo New Patient | Endo Old Patient | Endo Follow-up Tele-consultation | PAE Clinic | DOY Clinic | GDM Clinic | Total |
|---|---|---|---|---|---|---|
| 8364 | 20438 | 3027 | 504 | 1137 | 125 | 33595 |
| S.No | Name | Month & Year of Passing |
|---|---|---|
| 1. 2. | Dr. Ambrish Mithal Dr. K. M. Prasanna Kumar | June 1987 |
| 3. | Dr. Gumpeny Ramachandra Sridhar | June 1988 |
| 4. 5. | Dr. B. Jaya Kumar Dr. P. G. Sundaraman | Dec 1988 |
| 6. 7. | Dr. Arun Kumar Dr. Pankaj Shah | June 1990 June 1990 |
| 8. | Dr. Ajay Sood | Dec 1990 |
| 9. 10. 11. | Dr. Dr. C. V. Harinarayana Dr. Surender Kumar Dr. S. Sridhar | Dec 1991 |
| 12. 13 | Dr. T. K. Jagadhish Dr. Vipin Mishra | June 1992 |
| 14. | Dr. Ramchandra G. Naik | June 1993 |
| 15. 16 | Dr. Sarita Bajaj Dr. Ravinder Goswami | Dec 1993 |
| 17. 18 | Dr. Sudhir Tripathy Dr. Dinesh Chandra Sharma | June 1994 |
| 19. | Dr. S. K. Jain | Dec 1994 |
| 20. | Dr. Sandeep Kumar Mathur | Dec 1995 |
| 21. 22 | Dr. Uma Kaimal Dr. Mahendra K. Garg | June 1996 |
| 23. 24. 25. | Dr. C. S. Dwarkanath Dr. Devjit Tripathy Dr. Rajesh Kumar Garg | Dec 1996 |
| 26. | Dr. Sri Venkata Madhu | June 1997 |
| 27. 28 | Dr. Krishna Biswas Dr. Rajendra Kumar Sharma | Dec 1998 |
| 29. 30 | Dr. Mala Dharmalingam Dr. Abhay Inderjit Ahluwalia | June 1999 |
| 31. 32. | Dr. Sanjay Kalra Dr. Ramesh Omprakash Goyal | Dec 1999 |
| 33. | Dr. Rangel Neil De Jesus Stephen | June 2002 |
| 34. | Dr. Dinesh Kumar Dhanwal | Dec 2002 |
| 35. 36. 37. | Dr. Mohd. Ashraf Ganie Dr. Bindu Kulshreshtha Dr. Manas Patim Baruah | June 2003 |
| 38. | Dr. Rajeev Khanna | June 2004 |
| 39. 40. | Dr. T. Satish Chandra Dr. Bashir Ahmad Laway | Dec 2005 |
| 41. 42. | Dr. Yashpal Singh Dr. Madhav Rao Vupputuri | June 2006 |
| 43. 44. | Dr. D. Hari Kishore Reddy Dr. Jim Philip | Dec 2006 |
| 45. 46. 47. | Dr. Ankush Desai Dr. Gagan Priya Dr. Sunil Kumar | June 2007 |
| 48. | Dr. Abhay Kumar Sahoo | Dec 2007 |
| 49. | Dr. Sandeep Kansara | June 2008 |
| 50. 51. 52. | Dr. J. Kanakamani Dr. Salam Ranbir Dr. Ajay Gupta | Dec 2008 |
| 53. 54. | Dr. Ksh Achouba Singh Dr. Emmy Grewal | Dec 2009 |
| 55. 56. | Dr. Jaya Prakash Sahoo Dr. C. ShivaPrasad | June 2010 |
| 57. 58. 59. 60. | Dr. Naseer Ali Dr. Rajat Gupta Dr. Saptarishi Bhattacharya Dr. Thushanth Thomas | Dec 2010 |
| 61. 62. | Dr. Ansumali Joshi Dr. Parjeet Kaur | Dec 2011 |
| 63. | Dr. Deepak Khandelwal | June 2012 |
| 64. 65. 66. | Dr. Yashdeep Gupta Dr. Sameer Aggarwal Dr. Sachin Chittwar | Dec. 2012 |
| 67. 68. 69. | Dr. Gunjan Dr. Sivaprakash Dr. Rajiv Singla | June 2013 |
| 70. 71. | Dr. Sagar Modi Dr. Ram Kumar | Dec. 2013 |
| 72. | Dr. Vineet Kumar Surana | June 2014 |
| 73. | Dr. Shyam Kishore | June 2015 |
| 74. 75. 76. | Dr. Atul Dhingra Dr. Neelam Pandey Dr. Abilash Nair | Dec. 2015 |
| 77. 78. | Dr. Nishant Raizada Dr. Kumar Abhisheka | June 2016 |
| 79. 80. 81. 82. | Dr. Semanti Chakraborty Dr. Sweety Agrawal Dr. Himika Chawla Dr. Arun Kumar Chandresh Singh | Dec. 2016 |
| 83. | Dr. Hammadur Rahaman | June 2017 |
| 84. | Dr. Sreejith M. | Dec. 2017 |
| 85. | Dr. Alpesh Goyal | June 2018 |
| 86. | Dr. Rakhi Malhotra | Dec. 2018 |
| 87. 88. 89. 90. | Dr. Pramila Dharmshaktu Dr. Aishwarya Krishnamurthy Dr. Uttio Gupta Dr. Charandeep Singh | June 2019 June 2019 June 2019 June 2019 |
| 91. | Dr. Saurav Khtiwada | Dec. 2019 |
| 92. | Dr. Hiya Boro | Dec. 2020 |
| 93. 94. | Dr. Sarah Alam Dr. Suraj S. Kubihal | June 2020 June 2020 |
| 95. | Dr. Vinay Dogra | Dec. 2020 |
| 96. | Dr. Velmurugan M. | June 2021 |
| 97. | Dr. Kiran Deep Kamal | Dec. 2021 |
| 98. 99. 100. | Dr. Tejaswi V Dr. Uthara Elsa Mathew Dr. Kiran Kumar Golla | June 2022 June 2022 June 2022 |
| S.No | Description |
|---|---|
| 1 | Androgen Excess Disorders during infancy & adolescence https://www.aiims.edu/aiims/departments/endocrino/CME.pdf |
| 2 | ISBMR Meeting |
| Investigation | Platform | Quality Assessment |
|---|---|---|
| Thyroid hormones (T4, free T4, TSH) | Roche Cobas e411 | UK NEQAS Birmingham Thyroid Hormones |
| Thyroid hormones (T3, free T3) | Roche Cobas e411 | Calibrators and Quality Control samples |
| Steroid hormones (Cortisol, DHEAS, testosterone in males) | Roche Cobas e411 | UK NEQAS Birmingham Steroid Hormones |
| Steroid hormones (Estradiol) | Roche Cobas e411 | Calibrators and Quality Control samples |
| Steroid hormones (Aldosterone) | Diasorin Liaison XL | UK NEQAS Birmingham Steroid Hormones |
| Steroid hormones (Testosterone in females, 17-OH progesterone) | SCIEX QTRAP 6500+ LC-MS/MS system | UK NEQAS Birmingham Steroid Hormones |
| Steroid hormones (Panel 1 and Panel 2 steroid analytes) | SCIEX QTRAP 6500+ LC-MS/MS system | Calibrators, Internal Standards, and Quality Control samples |
| Peptide hormones (LH, FSH, Prolactin, Macroprolactin, ACTH, PTH) | Roche Cobas e411 | UK NEQAS Edinburgh Peptide Hormones |
| Peptide hormones (Insulin, C-peptide) | Roche Cobas e411 | UK NEQAS Guildford Peptide Hormones |
| Peptide hormones (GH) | Diasorin Liaison XL | UK NEQAS Edinburgh Peptide Hormones |
| Peptide hormones (Direct Renin Concentration, FGF-23, Calcitonin, IGF-1) | Diasorin Liaison XL | Calibrators and Quality Control samples |
| Vitamin D (25-hydroxy-vitamin D) | Diasorin Liaison XL | Vitamin D External Quality Assessment Scheme (DEQAS) |
| Autoantibody (TPO antibody, GAD antibody) | Roche Cobas e411, RSR ELISA kit | Calibrators and Quality Control samples |
| INVESTIGATION | PLATFORM | QUALITY ASSESSMENT |
|---|---|---|
| HbA1c | G8 Toshiba | BIO-RAD External Quality Assurance Services |
| Lipid Profile Total Cholesterol, HDL-Direct, LDL-Direct, Triglycerides, VLDL | Cobas Integra 400 PLUS ROCHE | BIO-RAD External Quality Assurance Services |
| Plasma Glucose (Fasting, post-prandial, 75gm GTT) | Cobas Integra 400 PLUS ROCHE | BIO-RAD External Quality Assurance Services |
| Serum and Urine Osmolality | Advanced Instrument | - Calibrator and Reference solution - BIO-RAD External Quality Assurance Services for serum osmolality |
| Urine pH | Microprocessor pH meter Widsons Scientific | pH reference solution and buffer solution |
| IgA Ttg | Euroimmun ELISA Kits | Graphs, blank and control wells |
| Serum Total Calcium, Phosphorus, Alkaline Phosphatase, Serum Album | Cobas Integra 400 PLUS ROCHE | BIO-RAD External Quality Assurance Services |
Ongoing
Ongoing
Ongoing
| S.No | OPD Days/ Timing | Name of Faculty Member(s) | Clinic Days/ Timing | Name of Faculty Member(s) | |
|---|---|---|---|---|---|
| 1. | Monday (Morning) | Dr. Rajesh Khadgawat and Dr. Yashdeep Gupta | Monday (Afternoon) - Paediatric and Adolescent Endocrine Clinic (PAEC) | Dr. Rajesh Khadgawat and Dr. Viveka P Jyotsna | |
| 2. | Tuesday (Morning) | Dr. Nikhil Tandon, Dr. Ravinder Goswami, and Dr. Viveka P Jyotsna | No Clinic | -- | |
| 3. | Wednesday (Morning) | Dr. Yashdeep Gupta | No Clinic | -- | |
| 4. | Thursday (Morning) | Dr. Nikhil Tandon, Dr. Ravinder Goswami, and Dr. Viveka P Jyotsna | No Clinic | -- | |
| 5. | Friday (Morning) | Dr. Rajesh Khadgawat | Friday (Morning) - Gestational Diabetes Mellitus (GDM) Clinic | Dr. Yashdeep Gupta | |
| 6. | No OPD | -- | Saturday (Morning) - Diabetes of Young (DOY) Clinic | Dr. Nikhil Tandon, Dr. Ravinder Goswami |
| Name of the Training | Details for Admission |
|---|---|
| Short term and long term training. | Clinical Endocrinology and Metabolism, Diabetes Mellitus. |
| Name of the Course | Details for Admission |
|---|---|
| D. M. (Endocrinology) Ph.D. | Students are admitted during January and July |
Nursing services forms an integral part of any health care facility. These \services aim at high quality nursing care to the patients and community. The professional nurses work in an environment that encourages professionalism and expertise in providing holistic patient care with the members of allied disciplines in the hospital. The nurses at AIIMS conduct themselves within the boundary of ethical and legal framework.
Indeed, on any given day, nursing professionals handle a wide array of responsibilities ranging from patient care, ward management, humanre sources management, facilities management, as well as attendant’s management.
When working in healthcare, nurses often handle fast-paced situations that require quick decisions and specific skills, so having a value system in place is fundamental. Not only do they provide a frame work of behavior and help to influence important decision, they;
Chief Nursing Officer - Nursing Superintendent - Dy. Nursing Superintendent - Asstt. Nursing Superintendent - Senior Nursing Officer - Nursing Officer
One of the major challenges in nursing administration is staffing nursing units. Staffing in AIIMS, New Delhi is based on SIU Norms which are as follows;
One of the major challenges in nursing administration is staffing nursing units. Staffing in AIIMS, New Delhi is based on SIU Norms which are as follows :
The Department of Obstetrics and Gynaecology, at All India Institute of Medical Sciences, New Delhi was established in the year 1958 and is committed to provide highest quality of care in the field of women’s health, strengthening research and innovations in teaching.
Over the years the department has grown keeping pace with the ever-increasing advances in the field of medicine. Here we are committed to provide respectful maternity care. Various Quality Improvement initiatives have been taken to improve patient care services and experience. Currently the department has a state of the art set up and expertise in the fields of Gynaecological Oncology, In Vitro Fertilization & Reproductive Medicine, Fetal medicine, High risk Obstetrics and Gynaecological endoscopy.
In addition to providing the latest in patient care, the department under a dynamic leadership, strives to maintain a high standard of research and also train the young doctors to become experts in the field.
Admission to post graduate courses is quite coveted and students from all over the country compete in an All India entrance examination. Postgraduate course (MD) is of three years duration and includes a thesis. Selection of junior residents for postgraduate course is made twice a year i.e. in January and July. The department run an orientation program of one week for these newly joined junior residents to make them familiar with the working protocols.
The department also offers sub-specialty courses like D.M. (Reproductive Medicine), M.C.H. (Gynecologic Oncology), Fellowship in Fetal Medicine, Fellowship in Minimally Invasive Surgery and Fellowship in Uro-gynecology.
Apart from the Post graduate and subspeciality courses the department offers training to the senior residents who obtain an overall comprehensive experience in all the sub specialties of Obstetrics and Gynecology. Online and hybrid teaching mode was adopted during Covid. Students are initially imparted with various skills through the hands on simulation based learning in SET facility. Several skill based modules have been prepared and taught in undergraduate teaching.
Department also offers short term and long term observerships in Gynecological endoscopy, IVF and Fetal medicine. In keeping with the spirit of the AIIMS mandate of teaching and research along with patient care, the department regularly organizes conferences and workshops in various subspecialties.
As a part of commitment towards the National Family Planning program, the department has an active family planning unit, which offers all the modalities of reversible and permanent methods of contraception. The Department also has an active role in the management of the Comprehensive Rural Health Centre at Ballabhgarh and the out reach OPD and operation facilities for gynecologic cancer patients at National Cancer Institute, Jhajjar.
In the Covid time the department extended its Covid care services at the Jai Prakash Narayan Apex Trauma Center, Delhi and collaborated with WHO SEARO and MOHFW to develop Obstetric Modules for training of doctors, paramedical and frontline workers.
Currently there are more than 130 projects in the department ongoing which are funded/ nonfunded including thesis and dissertations, 24 departmental projects including thesis and dissertations are completed this year. Department is conducting 36 projects in collaboration with other departments and 5 projects have been completed this year
Excellence in patient care, research, and education is the overall goal of the Department of Orthopaedics at AIIMS.The Department of Orthopaedics Surgery provides a comprehensive and integrated Orthopaedics program for patients, students, residents, and fellows.In addition to general Orthopaedics, the department has a faculty which specializes in the field of joint replacement, sports medicine ,hand surgery, musculoskeletal oncology, pediatric Orthopaedics ,spine surgery and treatment of complex trauma. The recent innovations in Orthopaedic surgery such as minimally invasive joint replacement, surface replacement arthroplasty, revision hip and knee replacements, minimally invasive spine surgery , vascular grafting for non unions, limb re-implantations, arthroscopic PCL and shoulder surgery are all being practiced with excellent results.There is also a bone bank facility in the department where both live donor bone and cadaveric bone are preserved and used as and when required.ICMR and CSIR funded research projects in the field of Orthopaedics are also being carried out.The Institute also has modern Physiotherapy Unit which works is close co-ordination with the Orthopaedic Department for comprehensive care of patients.
Research
The department witnessed an unparalleled rise in orthopaedic research in last decade and has several research projects with national as well as international funding.
Operation Theatres : There are 7 modular Operation Theatres dedicated to the Orthopaedics department with latest technology installed to provide quality care to the patients and make them feel calm and comfortable inside the OT complex.
The following advanced facilities are also available in the Department of Orthopaedics:
The Department of Otorhinolaryngology-Head & Neck Surgery is a leading Department in the country with expertise in all of the current subspecialties in Otorhinolaryngology. It provides OPD services to assess hearing and vertigo (Audiometry, ABR, OAE, Impedance, ASSR, hearing aid trial, VNg, VEMP etc.), nasal disease, sleep pathology assessment (Nasal endoscopies, Rhinomenometry, Apneography, Skin prick test, etc) laryngology (EMG, speech assessment, FOl, Stroboscopy, etc), head- neck cancer & skull-base lesion (TNE,FOL,NBI, etc). The Department also runs Specialized Clinics (head and neck cancer, rhinology and facial plastic, otology and skullbase, cochlear impant , vertigo, voice and rehabilitation).
The Department is performing office based procedures in the field of otology (examination under microscope, scarless myringoplasty, otoendoscopic examination of middle ear, intratympanic injection therapy, post-operative care), rhinology (diagnostic nasal endoscopy, NBI, post-operative cavity cleaning), laryngology (Botox injection for strained voices {spasmodic dysphonia, vocal cord palsy}NBI, ), head and neck cancer (biopsy, NBI, TNE).
The Department is equipped with advanced instruments required for the handling of diseases in the Otorhinolaryngology (CO2 and diode laser, Navigation system, Transoral Endoscopic Ultrasonic Surgery (TOUSS), Microdebrider, Nerve monitor, Coblator, RFA, Robotic Surgery, Microscopes, Endoscopes, CUSA, etc).
The Department also providing all kind of surgical services related to ear (Cochlear Implant, Stapes Surgeries, Ossiculoplasty , Mastoid Surgeries , Surgeries related to benign & malignant lesion of ear, etc) Nose & Para-nasal sinuses (FESS, Septoplasty, Rhinoplasty, Adenoidectomy, DCR, CSF rhinorrhoea, Optic nerve decompression, surgeries for benign & malignant lesion), Skull-Base (glomus tumour, Angiofibroma, Endoscopic & Open Skull Base Surgeries for anterior & lateral skullbase) sleep surgeries (modified UPPP, expansion pharyngoplasty, tonsillectomy, epiglottoplasty, etc), laryngology & airway (Endoscopic & Open Airway Surgery, Tracheal Resection anastomosis, glottis surgery, laser surgery, etc), cancer related surgery in all part of otorhinolaryngology ( maxillectomy, laryngectomy, neck dissection, glossectomy, thyroidectomies, mandibulectomy, etc with robot, laser, touss, bone cutting saw) & reconstructive surgeries (pinnaplasty, rhinoplasty, skin cancer care, scar revision, facial palsy rehabilitation, free flaps etc).
The Department has also been playing a prominent role in the academic and research activities. MS (ENT), McH (Head and Neck Cancer Surgery) and Skull-Base Fellowship are the degree courses run in the Department. We are getting trainees from various parts of the Country and various Countries on a regular basis. The teaching courses in the subspecialties of the Otorhinolaryngology are being conducted regularly.
Nuclear Medicine is a branch of medical science where radionuclides are used for diagnosis and treatment of human diseases. The discovery of artificial radioactivity and the development of nuclear reactors and particle accelerators have played a significant role in radiotracer technology. Organ/tissue-specific compounds, known as radiopharmaceuticals, are administered to the patient for diagnostic and therapeutic procedures. Nuclear medicine imaging and non-imaging procedures provide important information about the functional status of the body organs. Radiotracer technology made it possible to define disease in terms of physiology and biochemistry rather than anatomy or histopathology. Radioactive tracers of glucose, fatty acids, amino acids, etc. make it possible to examine the physiological and pathological aspects of the organs of the body, the regeneration and repair when injured, and the response to drugs. Advances in molecular biology have made a dramatic impact on the practice of medicine. This has led to the birth of “Molecular Nuclear Medicine”. Studies with receptor-based radiopharmaceuticals provide insight into the biochemical processes of proteins as they carry out instructions from genetic coding. The advent of hybrid imaging techniques such as single photon emission tomography-computed tomography (SPECT/CT) and positron emission tomography-computed tomography (PET/CT) permits 3D reconstruction of imaging data with high accuracy and anatomical localization of abnormal lesions in the body. We have three SPECT/CT Scanners and three dedicated Gamma Cameras, two PET/CT systems, and one 11 MeV Cyclotron in the department.
Radionuclides are also used for the therapy of malignant and non-malignant conditions. A lot of progress has taken place over the past few years in therapeutic nuclear medicine. With the use of suitable radiopharmaceuticals, targeted therapy is also possible. The department routinely performs several radionuclide therapies (both outpatient and inpatient) related to thyroid disorders, joint disorders, various cancers, etc.
Department of nephrology started in 1969 initially as a unit of department of medicine. Dr. Awasthi working in the department of medicine set-up dialysis unit around 1970 and first hemodialysis was done on 5th Aug 1971. However, the renal clinic already existed since 27th Oct 1969. Professor KK Malhotra was first faculty looking after the nephrology unit of the department of medicine after returning from USA. Thereafter, Prof. Ramesh Kumar joined in 1973. Before that in April 1972, first renal transplant was already done in the department. Subsequently, faculty in the unit of nephrology was Prof. SC Dash, who joined the nephrology on 25th March 1977 followed by Prof. SC Tiwari in September 1980.
In early days, nephrology was in a building called ‘old operation theatre’ block, where ward was on first floor (without a lift) and dialysis unit was on ground floor. Department shifted in main hospital block just before Dipawali in 1987 on 4th floor when neurosurgery shifted from 4th floor to ‘CN Center’. Recently department was renovated to match with a private set-up hospital with a teaching hospital expertise. Initially there were two types of resident in nephrology, one who were coming from medicine and other who were joining nephrology directly. In the earlier period resident joining nephrology directly were doing Diplomate Board of Nephrology through National Board of Examination.
In 1989 department of nephrology was created with two faculty and D.M. in nephrology was started in 1992. In 1989 Prof. SK Agarwal joined the separated department as adhoc faculty and then continued as regular faculty since 1991. Subsequently four more faculty members, Dr. Sanjeev Saxena, Dr. Sanjay Gupta, Dr. D Bhowmik and Dr. S Mahajan joined the department, while Prof. KK Malhotra, Prof. Ramesh Kumar, Prof. SC Dash and Prof. SC Tiwari and Prof.SK. Agarwal left the department following retirement (Voluntary or otherwise) or resignation. Dr Soumita Bagchi, Dr RK Yadav and Dr Arunkumar S joined the department as faculty members during the next few years. Currently, department has five faculty and thirteen senior resident strength. It has nine regular hemodialysis stations, four isolation hemodialysis stations, and two acute intermittent peritoneal dialysis beds. It provides one of best nephrology care for it’s all aspect, to patients of all socioeconomic background in a public sector hospital set-up including plasmapheresis, CRRT, SLED etc on a much subsidized cost. Currently department is doing nearly 140 renal transplant per year; majority being living related and also cadaver renal transplant.
Department of Microbiology was established in the year 1957 with Prof. S.L. Kalra, Prof. Ghosh Ray and Prof. L.N. Mohapatra as founder members. Prof. S. Balaya founded Virology; Prof. S. Mittal, Parasitology; Prof. Usha Gupta, Anaerobic Bacteriology; Prof. R.A. Bhujwala, Bacteriology & STD and Prof. Ishwari Nair, Entomology.
| Sr. No. | Name | From | To |
|---|---|---|---|
| 1 | PROF. S.L. KALRA | 1957 | 1968 |
| 2 | PROF. L.N. MOHAPATRA | Jan. 1971 | Jan. 1985 |
| 3 | PROF. SHRINIWAS | Feb. 1985 | Sept. 1990 |
| 4 | PROF. RAMESH KUMAR | Oct. 1990 | Sept. 1996 |
| 5 | PROF. PRADEEP SETH | Oct. 1996 | Apr. 2005 |
| 6 | PROF. J.C. SAMANTARAY | May 2005 | May 2015 |
| 7 | PROF. GITA SATPATHY | June 2015 | Nov. 2019 |
| 8 | PROF. RAMA CHAUDHRY | Dec. 2019 | Jan. 2023 |
| 9 | PROF. Lalit Dar | Feb. 2023 | - |
Vision of the department is to provide up-to-date and holistic theoretical & practical training for MBBS, MD (Microbiology), DM (Infectious Diseases), and PhDs; to carry out frontline research in all disciplines of Microbiology and to train good academicians, teachers and researchers in the discipline.
"Department of Microbiology is a multidisciplinary unit consisting of Bacteriology, Anaerobic bacteriology, Special Bacterial Pathogen Laboratory, Virology , Mycology, Serology, Immunology, HIV Laboratory, Parasitology, Mycobacteriology, CBNAAT, Mycoplasma laboratory, STD laboratory and Hospital Infection Control laboratory"
The laboratory facilities include state of the art automated blood culture system, MALDI–TOF (Matrix Assisted Laser Desorption/Ionization – Time of Flight), Automated identification and antimicrobial susceptibility testing system, Gene Xpert, Flow Cytometry System, Conventional PCR, Real time PCR, Testing for SARS-CoV-2along with the conventional microbiological tools for diagnostic services.
The Department of Microbiology has been at the forefront in fighting the COVID-19 pandemic, be it the diagnostic support including RT-PCR and CBNAAT as well as infection control activities.
The Department of Microbiology, AIIMS, New Delhi has been NABL accredited from 15th November, 2019 as per ISO:15189. One of the first Department of Microbiology in public health sector for getting NABL Accreditation. All the routine tests of the department including molecular tests are included in NABL Scope.
The NABL Certification No. is MC-3267 (125.54 KB) and SCOPE is attached.
The Department of Medicine has been at the forefront of achieving the “Trinity of Mission” at AIIMS. It provides holistic patient care services, strives for innovation in medical education, and conducts translational and clinical research.
The department has launched quality improvement initiatives to enhance various aspects of patient care services. The Department continues to strengthen the existing services continuously to provide quality care to ever increasing number of patients coming to AIIMS.
The Department is continuously updating and improving the digital platform (https://www.aiimsmedicine.org)used for teaching, training, and assessment. Online assessment of our students is now a regular feature in addition to the traditional assessment system. Emphasis is placed on the practical skill development of undergraduates through workplace-based assessments and feedback. Additionally, mentorship and wellness programs are being prioritized for residents.
The faculties of the department are at the forefront of contributing to national guidelines across a vast spectrum of clinical conditions. During the COVID-19 pandemic, the Department of Medicine took the lead at the national level to tackle COVID-19 by preparing management guidelines and algorithms that were subsequently adapted as National Guidelines for the management of COVID-19. With the vision of ending the TB strategy by 2025, all faculty and resident doctors have worked hard to draft an extensive training module on extrapulmonary tuberculosis, which was launched by the Honourable Prime Minister of India on March 24, 2023.
(Additional Professor & Head)
The Department of Laboratory Medicine was created as a new department in 1988 with an aim to centralize patients’ investigations conducted at various places in All India Institute of Medical Sciences, New Delhi. Simultaneous with creation of single-spot laboratory facilities, it was also aimed to improve the area of investigative medicine with advancement of technologies used and expansion of test profiles to meet patients’ requirement.
Recruitment of faculty from various diagnostic specialties in early 90s was a step in the direction for development of an integrated, holistic approach towards diagnostics. Like any other department at AIIMS, the faculty tried to develop all essential activities including patient-care services, teaching and training of residents and basic and translational research related to diagnostics. With time, this department started a unique postgraduate teaching program with three-year residency leading to award of MD (Laboratory Medicine). The department also successfully runs a PhD program in Laboratory Medicine. The research endeavors have also brought intra and extra mural research-grants from various national and international bodies.
The department has state-of-the-art SMART Lab which is an end-to-end, integrated laboratory with total lab automation for clinical biochemistry, hematology, coagulation and serology testing providing high quality results with minimum Turn Around Time. Besides, it houses a fully automated Dry Clinical Chemistry platform, and fully automated hematology cell counters with automated slide maker and Stainer.
At present the patient care services are offered from two premises: Main Department (main hospital building, adjacent to Old RAK OPD block) and SMART Lab (new RAK OPD block).The department caters to the Main Hospital (IPD and Emergency), CN Centre, OPD block, Surgical block, Maternal & Child Health block and other centres. The department run 24x7 services for clinical chemistry, hematology, clinical pathology and clinical microbiology services from both the premises. The department manages two centralized blood collection centres in the Old and New RAK OPDs with a footfall of more than 1000 patients everyday. The OPD collection timings are from 8AM to 6:30PM.
This department has about 180 staff members that include faculty, senior residents, junior residents (academic), junior residents (non-academic), scientists and PhD scholars. On an average, the department of Laboratory Medicine conducts about 1lakh tests on a daily basis with utmost care on pre-analytical and analytical procedures and constant monitoring of quality through internal and external quality control programs. The reports are available online through appropriate access control.
Faculty/Scientists and resident doctors remain engaged in UG/PG teaching, tutorials, case discussions, Journal clubs, inter disciplinary discussion and research in various areas related to investigative medicine. This department also arranges laboratory training to postgraduate students from Department of Pathology, Department of Biochemistry and Department of Transfusion Medicine at AIIMS. It is also involved in teaching of B.Sc. (Nursing) students and training to PG/PhD scholars coming from various other institutions/universities. The faculty and researchers also conduct international and national workshops, CME and conferences on various topics of current importance periodically.
Welcome to the future of Diagnostics…..!!!
The Department of Hospital Administration, AIIMS, is the pioneering department in India which started the post graduate Master’s Degree in Hospital Administration, popularly known as MHA. It is the oldest Department providing teaching and training to the country’s Hospital managers in the “science and art” of Hospital Administration and Management. The department introduced the specialty of Hospital Administration in the country in the year 1962, and has since evolved into a “center of excellence” for teaching, training and research in the field of Hospital Administration and Management in the country. Alumni from the Department have held high positions in various Institutions of repute in both public and private sector Hospitals/Colleges and Defence organizations.
In the year 1961, Dr. J.R. Mc Gibony, Consultant to the World Health Organisation (WHO) for the field of Hospital Administration, recommended the introduction of Hospital Administration as a separate specialty like any other broad specialty of medical sciences. With this initiative in 1961-62, a comprehensive programme and syllabus for Post Graduate course in Hospital Administration was drafted. One Post Graduate student, an Indian doctor from the University of New South Wales, Australia was admitted to serve his Administrative Residency at AIIMS. The Australian student completed his thesis and MD in Hospital Administration in 1962-63. The course in Hospital Administration was formally approved in 1963-64 and a full fledged Department of Hospital Administration was started in 1966 under the pioneership of Brig (Dr.) Gaind, the then Medical Superintendent, for the first time in India. The erstwhile MHA (Master in Hospital Administration) course was officially started in February, 1966 and was recognized as a distinct post-graduate discipline by the Medical Council of India, in consonance with the AIIMS Act 1956. It is the precursor to MD (Hospital Administration) course in the country which started in late 1970’s.
The Department of Hospital Administration occupies pride of place in managing Hospital operations in the Main Hospital and Centers of AIIMS, which has resulted in the “Kayakalp” award for tertiary care institutions being won by AIIMS, New Delhi every time, since it’s inception in 2015. Faculty members of the department are handling independent charge of hospital administration at the Medical Superintendent/Additional Medical Superintendent level in various ‘centers’ of the Institute. They are responsible for management of various ancillary and support services, medical records, human resource management, procurement and supply chain management, and handling legal and ethical issues at respective centers and main hospital. They are also co-ordinating new projects at AIIMS including the AIIMS Re-development Project, and looking after administrative areas of the Institute. The department also regularly organizes training programme for all categories of Hospital staff on various aspects of hospital administration and managerial development for better functioning. In addition, the department runs 24 hours Administrative Control Rooms at Main Hospital, J.P.N.A.T.C and NCI, Jhajjar, a unique concept which functions as an extension of the Medical Superintendent’s office after office hours.
The department is actively involved and strongly committed to capacity building and human resources development in hospital administration at national and international stages. Being the pioneer in starting a post-graduate teaching program in the speciality of Hospital Administration in the 1960s, the unique concepts started here have become the standard norm/template for setting up such Departments in Medical Colleges. The concept of “Administrative Control Room” has also been adopted by erstwhile Medical Council of India as a mandatory requirement for starting MD Hospital Administration courses in other Medical Colleges in India.
The Department also provides guidelines for developing courses and curricula for starting organization specific training courses in the field of hospital administration to various public sector and private institutions in the country. WHO fellows and Senior Doctors from various neighboring countries are imparted short and long term trainings on hospital management in the department. A series of Healthcare Executive Management Development Programs have been conducted by the department for senior hospital administrators and top level hospital management personnel from India and abroad during last 2 decades. The Department has organized more than 50 workshops, Seminars/Conferences during last few decades.
The department provides consultancy on diverse areas like Newer Healthcare Facility Planning & Management, Healthcare Registries Planning and Innovation, Healthcare Human Resources Management, Disaster Management, Hospital Equipment Planning and Management and Healthcare Financing and Insurance Product Development as and when requested by Public sector organisations, State Governments, Ministries of Central Govt. It is also involved in the development of standards for different categories of hospitals along with BIS, NQAS, NABH and acting as a Think-Tank for the preparation of National Healthcare Policy Guidelines.
The department runs a 3 years post graduate (MD) course in hospital administration from Jan-2016 leading to award of degree of MD(HA) for both “sponsored” and “open” category candidates. Resident Administrators are posted in various areas of the Hospital and centers for a period of 3-4 months to observe and understand the functioning of the ward/service area. They are also posted in the Control Room “round the clock” as Duty Officers, and coordinate various hospital activities. They also assist the faculty in “hands-on” management of various hospital activities, and, in turn, gain valuable experience of hospital management. They have to complete one research study (thesis) on suitable topic related to hospital administration, after approval of Institutional Ethics Committee (IEC), and four dissertations, at least one of which has to be published in a “peer reviewed” and indexed journal during this tenure. The MD program has formative and summative assessments for holistic assessment of candidates undertaking the course. The term end (final) Examination comprises of 4 Theory papers, and Practical Exams, usually held in the months of May and December respectively. Our alumni have held top administrative positions in various organizations of national and international importance. Many of them are also serving as independent consultants in Hospital Administration in the corporate sector.
Admission to the MD(HA) programme is through a competitive exam (INI-SS) conducted twice a year by Exam Section, AIIMS. An advertisement is placed in national dailies in the month of August and January for sessions beginning December and July respectively. Potential candidates are expected to have up to date knowledge of Medico-legal issues, Public Health, National Health Programs, and general awareness about issues pertaining to hospital and health sector. For details of admission procedure, form etc.
Various long and short term trainings are provided to Faculty members/Medical Officers from other Govt Medical Colleges/ Military and Paramilitary services/ State Govt Health services who are handling administrative responsibilities under following categories
1. Short Term Trainings upto period of six months
2. Long Term Trainings : 6 months to 2 years
3. Training to Foreign Nationals and WHO fellows
4. Continuing Medical Education Programmes (Conference/Workshops/Seminars etc.)
Trainees are expected to attend lectures, interact/observe faculty members and Residents while working, taking area rounds, and carry out “under-study” duties in the Control Room. They are also sensitized about the functioning of the various centers at AIIMS for better understanding.
Details of the training, fee, schedule etc. can be obtained from the academic section of the Institute or from the institute website .
Unique and dynamic blends of experiential and didactic learning methods are utilized to impart, share, promote and preserve knowledge and skills. The concept of Integrated Learning Methodology comprising Lectures, case analysis, simulation exercises, syndicates, group discussions and practical project work are used to develop conceptual, analytical and decision-making skills. Residents are encouraged to participate actively in the “operational decision making processes” of various activities of the Institute. They are also made Member secretary of various Medical Boards constituted on the orders of Courts, to gain insight into medico-legal issues. It prepares them for handling independently the real life management of hospitals and healthcare facilities. Resident’s performance is continuously assessed through direct observations and faculty feedback system during bi-monthly assessments during which all Faculty members of the Department are present.
Continuous Quality improvement in training, teaching and research in the field of Hospital Administration through Thesis/Protocol presentations, Journal Clubs, Seminars etc are also carried out.
In the pursuit of excellence in the teaching and training of Hospital Administration, the department has started several initiatives to develop model syllabi, to meet the changing demands and skill set requirements in this field. Efforts are underway to bring quality standards.
As a pioneering step in this direction the department has become the first of its kind in the country to have documented its teaching, training, research and patient care management process through ISO-9001:2000 Quality Management Systems Certification in 2011. Further, efforts are underway to provide inspiration and leadership in improving healthcare processes and imparting Hospital Administration Education for the nation as well as the South East Asia Region. The Faculty members from the Department have been actively involved in development of National Standards, Guidelines and policy making in the field of Hospital Administration.
The department is located adjacent to the Medical Superintendent’ office on the ground floor of the Old Private ward block at AIIMS. It houses a Departmental library, a well equipped and state of art Conference-cum-Board room and provision for Tele-Education and Tele-Linkage, Senior and Junior Residents Rooms. Latest IT facilities are provided to all faculty and residents to facilitate teaching and learning. The New Private ward-III and newer Blocks in Masjid Moth Campus also have some rooms/areas for Department faculty and residents posted there. These facilities are in addition to the central training infrastructure of AIIMS including central Boardrooms, 24 hours Library, Lecture theatres, Central IT and Computer facility and Centre for Medical Education and Technology.

The department of Hematology is a composite department provides both Clinical Hematology and Hemato-Pathology services to the Institute. Clinical Hematology service provides comprehensive management for patients with benign and malignant hematological illnesses. The department runs specialized outpatient clinics for patients with these illnesses. The department has been performing autologous and allogeneic Hematopoetic Stem Cell Transplantation (HCT), including haploidentical donor HCT, for various benign and hematological illnesses like aplastic anemia, thalassemia, myeloma, lymphomas, leukemias, and myelodysplastic syndromes. Hemato-Pathology provides state-of-the-art evaluation of blood and bone marrow diseases. Expert hematopathology services offered by the department include: Bone marrow examination including immunohistochemistry and cytochemistry; Flowcytometry; molecular diagnostics; specialized hemolytic and coagulation tests.
Information on latest developments in education and research :
Book 1
Book 2
A proposal was made in 1980 to establish a Department of Gastrointestinal (GI) Surgery at the All India Institute of Medical Sciences. This department would perform only complicated GI operations which were not usually done elsewhere in the country, train surgeons from other parts of the country and do research into Indian GI surgical problems. The department was created as a unit of the Department of Surgery in May 1985. In September 1989 it was given full departmental status. The department is now established and has trained a large number of surgeons to set up GI surgical departments in India and abroad. In pursuance of the objectives of the department an MCh course was started in 1994 and in 1997 the first batch completed their course. The main fields of specialization of the department are portal hypertension, hepato-pancreato-biliary diseases, hepatic venous outflow obstruction, ulcerative colitis, gastrointestinal haemorrhage and oesophageal diseases and liver transplantation. Its main thrust is on providing a high quality of patient care, training of residents, good record keeping, research publications and research into Indian diseases. The department has its own 8 bed intensive care unit (ICU) with ventilators, cardiac monitors; blood gas and electrolyte management facility. All patient records are computerized. The department faculty are actively involved in the publication of 'The National Medical Journal of India', ‘Tropical Gastroenterology' both of which are indexed journals and the ‘GI Surgery Annual' which is in its 26th year of publication.
In 1990 it was felt that the field of liver transplantation should be developed by the department. This required the law on brain death to be amended. The Department took a lead in this field and in 1994 The Transplantation of Human Organs Act was passed by the Indian Parliament. Following this attempts are in progress to establish a liver transplant program in India.
Apart from other activities, the department has developed indigenous medical equipment. An anorectal manometric system to evaluate anorectal function has been successfully developed and is being commercially marketed. Oesophageal manometry and continuous pH monitoring systems to diagnose gastro-oesophageal reflux disease have been developed and technology transfer of this equipment is in progress. The department has also developed a rapid blood and fluid infusion system and is currently working on a cheap low flow infusion system. A peritoneovenous shunt, has been successfully devised and marketed.
So far more than 100 surgeons have received either short or long term training in the department. The department has pioneered the establishment of a new surgical superspeciality in India the need for which is being realized nationwide in both the private and public sectors. We strive hard to ensure that the department continues to serve as a role model in this field.
The Department of Gastroenterology at All India Institute of Medical Sciences was started in the year 1971 with an aim to create qualified gastroenterologists for the country. Prof BN Tandon was instrumental in creating the department of Gastroenterology at All India Institute of Medical Sciences. He was the first head of this department and continued to lead it until his retirement on 31st Aug 1991. Thereafter, Dr. Rakesh Tandon was Prof. & Head of Gastroenterology from 1991 to 31st Dec 2002, Dr. MP Sharma was the Prof. & Head of Gastroenterology from 1st Jan 2003 to 30th April 2004, Dr. SK Acharya from 1st May 2004 to 31st Oct 2016, Prof Umesh Kapil from 01 Nov 2016 to Feb 10, 2017 and Prof. Anoop Saraya from Feb 11, 2017 to 31st Dec 2023. Currently, Prof Pramod Garg is heading the department from 01 Jan 2024.
By now, the department has produced 121 DM students in Gastroenterology. At present, the chiefs of Gastroenterology in major institutions of the country are alumni of the department of Gastroenterology at AIIMS. Since, the inception of this department it has provided state of the art services and provided training to many physicians in specific areas like luminal gastroenterology, liver diseases and endoscopy.
The department has been consistently ranked as the Best Department of Gastroenterology in India for many years in surveys conducted by leading News Weeklies. In Dec 2011 department was awarded as the Best Department of Gastroenterology in India at the CNBC TV18 India Healthcare Awards.
Content Provider: Dr. Deepak Gunjan
Globally, life expectancy has increased by 25 years since 1950. Healthy older individuals contribute positively to society in many ways, and the World Health Organization (WHO) emphasizes enabling them to continue doing what they enjoy for as long as possible.
India is undergoing a rapid demographic shift, with a rising number of senior citizens. Life expectancy in India has increased significantly, from 32 years at the time of independence in 1947 to over 70 years today. This phenomenon of population aging has profound implications for society, particularly the healthcare system. Older adults require financial security, emotional and social support, and—most critically—regular access to effective and affordable healthcare.
Recognizing these challenges, the All India Institute of Medical Sciences (AIIMS) took an early initiative by establishing a weekly geriatric clinic in 1993, which was later upgraded to a daily service in August 2010. This marked the foundation for the development of a dedicated Department of Geriatric Medicine. Under the visionary leadership of Prof. (Dr.) A B Dey, a separate academic department was established in January 2012. The department admitted its first batch of MD students in the same year and opened a dedicated Geriatric Medicine ward in July 2012. Over time, the department expanded its clinical services to provide holistic care, integrating physiotherapy, counseling, dietary services, and a specialized Memory Clinic for dementia patients.
The department has also been at the forefront of research and innovation in aging-related fields. It has established a dedicated departmental research laboratory and has contributed to multiple national and international research projects. Key areas of research include dementia, sarcopenia, longevity, superagers, centenarians, and assistive devices for older adults.
The Department of Geriatric Medicine at AIIMS is a WHO Collaborating Centre (CC) for Healthy Ageing in India, playing a crucial role in developing strategies and policies to promote healthy aging across the country. This recognition underscores the department’s leadership in geriatric healthcare, education, and research at both national and global levels.
Today, the Department of Geriatric Medicine operates from the National Centre for Ageing (NCA) at AIIMS, New Delhi, offering comprehensive outpatient, inpatient, and ICU services for older adults. The NCA serves as a hub for geriatric clinical care, medical education, and research, training undergraduate, postgraduate, and doctoral students while conducting cutting-edge studies in geriatrics and gerontology.
Looking ahead, the department remains committed to advancing the field of geriatric medicine, fostering innovation, and strengthening India's healthcare system to meet the evolving needs of its aging population.
| Senior Financial Advisor | |
| Smt. Divya Yanamadala | |
| Financial Advisor | |
| F & CAOs | - |
| Shri Vijay Pal Singh | - |
| Shri Padam Singh | - |
| Ms. Rakesh Kumari | - |
| Accounts Officers | ||
|---|---|---|
| Sh. Trilok Chand | Sh. Prem Pal | Smt. Meenakshi Dabral |
| Sh. Prakash Kumar Giri | Sh. Bharat Bhushan | Sh. Joginder Singh |
| Sh. Anil Kumar | Shri Satish Kumar Yadav | Sh. Upendra Kumar |
| Sh. Yogesh Kumar | Sh. Shivanand Thakur | Smt. Snehlata |
| Shri Rajesh Kr. Bairwa | - | - |
| Asstt. Accounts Officers | ||
|---|---|---|
| Smt. Meena Gupta | Shri Braham Singh | Smt.. Rashu Kabtiyal |
| Smt. S. Tanveer | Smt. Sushil Kumari | Sh. Satya Dev Sharma |
| Sh. Nagender | Sh. Arvind Kumar | Ms. Veena Gaba |
| Ms. Urmila | - | - |
| Jr. Account Officers Vacant |
CENTRE FOR ADVANCED RESERACH AND EXCELLENCE IN VIRTUAL AUTOPSY
STANDARD GUIDELINES FOR DIGNIFIED AUTOPSY IN COVID-19 DEATHS




The Department of Forensic Medicine and Toxicology started functioning in year 1957. Later Prof. Jagdish Chandra joined as Lecturer and was designated as Head of Department. Medicolegal postmortem work was started from year 1968. At present, apart from routine medico-legal works, department is engaged in multifarious activities of teaching, training and research. It is involved in medico-legal postmortems, Clinical Forensic medicine Services & court related works. Department is providing expert opinions in referred cases from courts, National Human Rights Commission, CBI, Crime Branch, Delhi Police and Investigating agencies from other states. The department is running various laboratory services like Forensic histopathology laboratory, Toxicology laboratory and DNA laboratory.
Dr Sudhir K Gupta has taken the charge of Professor and Head of Department since August 2013 and has introduced new innovative developments like Embalming facility in public interest. His long term plan is to develop Cadaveric Training Centre, Cadaver organ/tissue retrieval and processing Centre, Odourless Autopsy suite, Virtual Dissection-less autopsy, Forensic Molecular Biology unit, One stop crisis center for survivors of Sexual assault and Therapeutic transplantation Centre from brain dead in future. Clinical toxicology and antidote banking for treatment of poisoning cases is also being envisaged.
Forensic Anthropology laboratory, first of its kind in the country, is being developed in the department. It will be well-equipped as per international standards and will act as quality training centre and provide mentor facility for whole country.
The Department is planning to set up a facility which could manage approximately 1000 dead bodies simultaneously and will have all the necessary infrastructural, manpower, resources, residential and transportation facilities related to Forensic Human Identification related to any disaster and Dignified Management of the Dead. At present there is no such single centre nationwide which could handle the management of dead efficiently as a unified centre in case of a mass disaster. The High-throughput design will encompass all aspects of the management of the dead, starting from recovery of the bodies to final burial rites, including support to the affected families and communities. The setting up of such facility will require a significant amount of time, until which additional facility for handling of 100 bodies in a case of disaster will be established along with the present mortuary set-up.
Endocrinology started at AIIMS in 1964 under the leadership of Prof. MMS Ahuja as a subspecialty of internal medicine. It acquired the status of a department in 1986. The department has excellent facilities for patient care education and research. It has done pioneering work in the field of Diabetes, thyroid, metabolic bone disease, pediatric and adolescent endocrinology.
| Sr. No. | Name of Residents |
|---|---|
| 1 | Dr. Bharathi Arunan |
| 2 | Dr. J Kirtana |
| 3 | Dr. Anuj A |
| 4 | Dr. S Bharadhan |
| 5 | Dr. S Jayasree |
| 6 | Dr. Mohit |
| 7 | Dr. Sayan Maharatna |
| 8 | Dr. Souradeep Chowdhury |
| 9 | Dr. Sunit Sikdar |
| 10 | Dr. Baidhnath Kumar Gupta |
| 11 | Dr. Indra Shekhar |
| 12 | Dr. Karthick Kumar V |
| 13 | Dr. Akansha Didwania |
| 14 | Dr. Ashwin Varadarajan |
| 15 | Dr. Megha Priyadarshi |
| 16 | Dr. Ayan Mandal |
| 17 | Dr. Aranya Kumar Das |
| 18 | Dr. Madhav Mohta |
| 19 | Dr. Shah Harshil Chandreshkumar |
| 20 | Dr. Ravi Bhushan |
| 21 | Dr. Chandana Acharya |
| 22 | Dr. MD Tariq Maula |
| 23 | Dr. Sandeep Rao Kordcal |
| 24 | Dr. Sanjana Pant |
| Sr. No. | Name of Residents |
|---|---|
| 1 | Dr. Charu Rajori |
| 2 | Dr. Sarthak Gupta |
| 3 | Dr. Madhav Bansal |
| 4 | Dr. Maneet Kaur |
| 5 | Dr. Elen Susan Tide |
| 6 | Dr. Anamika Seth |
| 7 | Dr. Himani Gupta |
| 8 | Dr. Vivek M S |
| 9 | Dr. Vidushi V |
| 10 | Dr. Vishal K |
| 11 | Dr. Kaushalya D |
| 12 | Dr. Althaf Majeed |
| Sr. No. | Enrollment No. | Name | D.O.J |
|---|---|---|---|
| 1 | P-2022/16979 | Ms. Kavita | 24.09.2022 |
| 2 | P-2022/16980 | Ms. Mahek Farhan | 24.09.2022 |
| 3 | P-2022/16981 | Ms. Nisha Kumari | 24.09.2022 |
| 4 | P-2022/16982 | Mr. Anish Kumar Chauhan | 24.09.2022 |
| 5 | P-2022/16983 | Ms. Isha Rathore | 24.09.2022 |
| 6 | P-2022/16984 | Ms. Shikha Roy | 03.10.2022 |
| 7 | P-2023/17085 | Ms. Neeti Bharadwaj | 12.08.2023 |
| 8 | P-2023/17086 | Ms. Dakshita Joshi | 12.08.2023 |
| 9 | P-2023/17087 | Ms. Bindiya | 12.08.2023 |
| 10 | P-2023/17088 | Ms. Nishu | 12.08.2023 |
| 11 | P-2023/17089 | Mr. Ankit Kumar | 14.09.2023 |
| 12 | P-2023/17090 | Ms. Daina Sapam | 14.09.2023 |
| 13 | P-2023/17091 | Ms. Aisha Farhat | 12.08.2023 |
| S.No. | ENROLMENT NUMBER | TITLE | NAME | DATE OF JOINING | SESSION | CHIEF SUPERVISOR | DESIGNATION |
|---|---|---|---|---|---|---|---|
| 1 | P-2019/14812 | MS. | MRIDULA SHARMA | 22.07.2019 | JAN&JUL'2019 | DR. SUBRATA SINHA | PROFESSOR |
| 2 | P-2019/14814 | MS. | ALISHA ARORA | 01.08.2019 | JAN&JUL'2019 | DR. ARCHANA SINGH | ADDITIONAL PROFESSOR |
| 3 | P-2019/14815 | MR. | SAGAR TYAGI | 01.08.2019 | JAN&JUL'2019 | DR. SUDIP SEN | PROFESSOR |
| 4 | P-2019/14817 | MS. | ANTARA MALIK | 31.07.2019 | JAN&JUL'2019 | DR. KALPANA LUTHRA | PROFESSOR |
| 5 | P-2019/14818 | MS. | RASHMI GUPTA | 26.08.2019 | JAN&JUL'2019 | DR. ASHOK SHARMA | ADDITIONAL PROFESSOR |
| 6 | P-2019/14819 | MS. | MAHAIWON SHADANG | 01.08.2019 | JAN&JUL'2019 | DR. RIYAZ AHMAD MIR | ASSOCIATE PROFESSOR |
| 7 | P-2020/14861 | MS. | SHAIFALI SHARMA | 14.02.2020 | JAN'2020 | DR. KALPANA LUTHRA | PROFESSOR |
| 8 | P-2020/14898 | MR. | BLESSED RAJ | 04.11.2020 | JUL'2020 | DR. RAKHEE YADAV | ASSOCIATE PROFESSOR |
| 9 | P-2020/14899 | MS. | RUPINDER KAUR | 04.11.2020 | JUL'2020 | DR. PRMAOD KUMAR GAUTAM | ASSOCIATE PROFESSOR |
| 10 | P-2020/14900 | MS. | MANVI ARORA | 06.11.2020 | JUL'2020 | DR. KUNZANG CHOSDOL | PROFESSOR |
| 11 | P-2020/14901 | MR. | DEEPAK | 17.10.2020 | JUL'2020 | DR. ARCHANA SINGH | ADDITIONAL PROFESSOR |
| 12 | P-01-2021/14952 | DR. | VADANYA SHRIVASTAVA | 10.04.2021 | JAN'2021 | DR. SUDIP SEN | PROFESSOR |
| 13 | P-01-2021/14953 | DR. | SANKET KATPARA | 07.04.2021 | JAN'2021 | DR. KALPANA LUTHRA | PROFESSOR |
| 14 | P-01-2021/14955 | MR. | MOHAMMAD SABIQUE BEG | 12.04.2021 | JAN'2021 | DR. PARTHAPRASAD CHATTOPADHYAY | PROFESSOR |
| 15 | P-01-2021/14956 | MR. | SANTOSH KUMAR | 12.04.2021 | JAN'2021 | DR. ASHOK SHARMA | ADDITIONAL PROFESSOR |
| 16 | P-01-2021/14956 (A) | MS. | ISHU | 29.05.2021 | JAN'2021 | DR JAYANTH KUMAR | ADDITIONAL PROFESSOR |
| 17 | P-01-2021/14956 (B) | MR. | NEHA KASHYAP | 24.06.2021 | JAN'2021 | DR SUBHRADIP KARMAKAR | ADDITIONAL PROFESSOR |
| 18 | P-07-2021/14988 | MR. | HARSH BHAKHRI | 04.12.2021 | JUL'2021 | DR. KALPANA LUTHRA | PROFESSOR |
| 19 | P-07-2021/14989 | MS. | HEMA YADAV | 04.12.2021 | JUL'2021 | DR. RIYAZ AHMAD MIR | ASSOCIATE PROFESSOR |
| 20 | P-01-2022/15016 | MS. | RITIKA SINGH | 12.04.2022 | JAN'2022 | DR. PARTHAPRASAD CHATTOPADHYAY | PROFESSOR |
| 21 | P-07-2022/15046 | MS. | AYESHA RAHMAN | 26.09.2022 | JAN'2022 | DR. RIYAZ AHMAD MIR | ASSOCIATE PROFESSOR |
| 22 | P-01-2023/15077 | MS. | TANU BANSAL | 26.09.2023 | JAN'2023 | DR JAYANTH KUMAR | ADDITIONAL PROFESSOR |
| 23 | P-01-2023/15078 | MS. | MANI KAPOOR | 26.09.2023 | JAN'2023 | DR. KUNZANG CHOSDOL | PROFESSOR |
| 24 | P-01-2023/15079 | MS. | ANAMTA GUL | 26.09.2023 | JAN'2023 | DR SUBHRADIP KARMAKAR | ADDITIONAL PROFESSOR |
| 25 | P-01-2023/15080 | MS. | RUCHI | 26.09.2023 | JAN'2023 | DR JAYANTH KUMAR | ADDITIONAL PROFESSOR |
| 26 | P-01-2023/15081 | MS. | ALISHER BEHERA | 26.09.2023 | JAN'2023 | DR. ASHOK SHARMA | ADDITIONAL PROFESSOR |
| 27 | P-01-2023/15083 | MS. | GEETA RANI | 26.09.2023 | JAN'2023 | DR. ARCHANA SINGH | ADDITIONAL PROFESSOR |
| 28 | P-01-2023/15084 | MS. | SONALI CHAKRABORTY | 26.09.2023 | JAN'2023 | DR. PRAGYAN ACHARYA | ADDITIONAL PROFESSOR |
| 29 | P-01-2024/15148 | DR. | MADHUTI CHAKRABORTY | 26.03.2024 | JAN'2024 | DR. KALPANA LUTHRA | PROFESSOR |
| 30 | P-01-2024/15149 | DR. | SHRUTI GUPTA | 23.03.2024 | JAN'2024 | DR. KUNZANG CHOSDOL | PROFESSOR |
| 31 | P-01-2024/15150 | MR. | GURPREET SINGH | 26.03.2024 | JAN'2024 | DR SUBHRADIP KARMAKAR | ADDITIONAL PROFESSOR |
| 32 | P-01-2024/15151 | MR. | SOVIK ROY | 23.03.2024 | JAN'2024 | DR. ARCHNA SINGH | PROFESSOR |
| Specialty | 2014-16 | 2015-17 |
|---|---|---|
| Pediatric Nursing | Ms. Ananya Susan Joy Ms. Merine Therese Jose Ms. Babita Yadav Mr. Sunil Kumar Poonia Ms. Punam Ms. Sonali Surya | Mr. Rohitashw Kumar Ms. Nisha Varghese Ms. Ashitha M. Varghese Ms. Osheen K Joy |
| Psychiatric Nursing | Ms. Linu Thomas Mr. Dhawal Dwivedi Mr. Nithish Thomas Ms. C. Lalengkimi | Ms. Laxmi Kumari Mr. Manphool Singh |
| Cardio logical/ CTVS Nursing | Ms. Nitta Das Mr. Harpreet Singh Mr. Mohmmed Toseef Ms. Anne Lorate Ms. Rashmi Vijaya Ms. Rakhangmi Donna Thangal | Ms. P. Usha Ms. Mamata Rai Ms. Archana JoseT Ms. Jyotishana |
| Neuro Science Nursing | Ms. Antonita Jeena Mohan Ms. Divya Sojan Mr. Rohit Kumar | Ms. Megha Sharma Ms. Sreevidya V.S Ms. Tenzin Nyidol |
| Onco logical Nursing | Ms. Jitha Titus Mr. Mukesh Kumar Ms. Shashi Bala Ms. Subina Manandhar | Ms. Akanglemla Imichen Ms. Maggie Renjith Ms. Anu Jose |
| Critical Care Nursing | - | Ms. Sonu Yadav Ms. Sonia Devi Ms. Reena Joji |
| Nephro logical Nursing | - | Ms. Jiya Mariya Thomas Ms. Teena Mary James Ms. Savita Gahalain |
(a.)Faculty
Dr.(Prof.) L.R. Murmu (Superannuated in November, 2021)
Dr. Praveen Aggarwal (superannuated on 31.10.2023)
(b.)Post-graduate residents
Research output from the department has been high-quality and there were around 84 publications from the department in peer-reviewed, indexed journals in the last three years.
Journal Articles
2019-2020
2020-2021
2021-2022
Journal Articles
2022-2023
Publications: 2023-24
Journal Articles
Editors of Books
Aggarwal P, Nayer J, Ekka M, Kumar A, Mishra PR. Washington Manual of Emergency Medicine (South Asian Edition), 2023.
Editors of Books
Chapters in Books
Department of Emergency Medicine provides emergency care round-the-clock to patients with a variety of emergencies. It is manned by faculty, senior residents and junior residents to provide efficient emergency care. The number of patients attending the Emergency Department has been increasing over the past few years. In the year 2023-24, nearly 1,23,962 patients attended the emergency department.
The department has two operation theatres for immediate surgical interventions. Nearly 212 minor OT procedures were done during 2023-24 which included tracheostomies and others. The department has high-end facilities to manage and monitor critically ill patients. It has all types of equipment required for emergency care. These include defibrillators, ventilators, cardiac monitors, infusion pumps, NIVs, HFNCs, nebulizers and others.
The department has a high quality Point of Care Testing Laboratory (POCT) running throughout 24 hours. Nearly 2,38,001 tests were done in the lab. during the year 2021-22. These tests included, complete blood count, quantitative Troponin I, ABG and VBG, NT-pro BNP, D-dimer, Urine tox. screen, PT/INR, and urine osmolality.
Department of Emergency Medicine provides emergency care round-the-clock to patients with a variety of emergencies. It is manned by faculty, senior residents and junior residents to provide efficient emergency care. The number of patients attending the Emergency Department has been increasing over the past few years. In the year 2023-24, nearly 1,23,962 patients attended the emergency department.
The department has two operation theatres for immediate surgical interventions. Nearly 212 minor OT procedures were done during 2023-24 which included tracheostomies and others. The department has high-end facilities to manage and monitor critically ill patients. It has all types of equipment required for emergency care. These include defibrillators, ventilators, cardiac monitors, infusion pumps, NIVs, HFNCs, nebulizers and others.
The department has organized various life support courses for undergraduates, postgraduates and nurses posted in the department. These courses have also benefitted residents from other disciplines of the institute. It has conducted AIIMS Emergency ECG and rapid sequence intubation courses for postgraduates of the institute as well as other colleges. The department runs a schedule of academic activities for the residents of Emergency Medicine (seminars, journal clubs, case discussions, panel discussions) twice a week for around nine hours. Education and skill are imparted to residents on the use of ultrasound in emergency care of patients. Simulation-based teaching (both table-top and on high-fidelity simulator) is imparted to the residents. Live workshops, cadaver-based training and hands-on skill session in first week of every month has provided confidence to residents in managing the patients. The faculty from the department have been a part of development of ‘e-modules’ for SET facility in the institute which helps in dissemination of medical knowledge to students in a standardized and practical format. In addition, the department faculty was involved in didactic teaching of undergraduates, postgraduates and nursing students through lectures and seminars, online as well as offline.
Various skill-based courses like Emergency ECG course, Emergency ultrasound course, Difficult airway course, Simulation based training course, bedside procedural skill development courses have been conceptualized, designed, developed and are being conducted regularly and successfully for postgraduate students. The departmental faculty is also involved in teaching and training of postgraduates from other departments (including Medicine, Surgery, Geriatric Medicine, Anaesthesia and Critical Care Medicine, Dermatology, Psychiatry and several others), undergraduate students, nursing students and paramedics in the field of Emergency medicine, including life support courses. The department is also involved in training the existing and future faculty from other colleges and hospitals in the specialty of Emergency Medicine.
The Department runs postgraduation course leading to the award of MD degree in Emergency Medicine. Selection is done through Institute of National Importance Combined Entrance Test(INI-CET). The sessions start biannually in January and July. There were 46 post-graduate residents in the department during the year 2021-22, including one foreign national/ sponsored candidate.
During three-years of training, residents are exposed to diverse emergencies, both pediatric and adult. They are rotated through other departments/centres to get further exposure in managing emergencies. The rotational postings include Trauma Centre, and other clinical departments. They are also trained in various emergency procedures such as cardiopulmonary resuscitation, ventilation, hemodynamic monitoring, central line insertions, fracture management, sonography as diagnostic and therapeutic modality, and others. The department runs a schedule of academic activities for the residents of Emergency Medicine (seminars, journal clubs, case discussions, panel discussions) twice a week for around nine hours. Education and skill are imparted to residents on the use of ultrasound in emergency care of patients. Simulation-based teaching (both table-top and on high-fidelity simulator) is imparted to the residents. Live workshops, cadaver-based training and hands-on skill session have provided confidence to residents in managing the patients.
Department of Emergency Medicine was established in 2011. It was created with the vision of providing holistic and quality emergency medical care to all those who seek it. The academic programme of the department started in July 2012 with three seats of postgraduates per year. The missions of the department are:
63rd AIIMS Foundation Day, 25th-30th Sep 2018
Symposium on 'Plant Based Nutrition for prevention and Treatment of Chronic Diseases'organized by Dept of Dietetics in collaboration with Physicians Committee for Responsible Medicine, USA on 30th July 2018
Symposium on 'Plant Based Nutrition for prevention and Treatment of Chronic Diseases'organized by Dept of Dietetics in collaboration with Physicians Committee for Responsible Medicine, USA on 30th July 2018
Symposium on 'Plant Based Nutrition for prevention and Treatment of Chronic Diseases'organized by Dept of Dietetics in collaboration with Physicians Committee for Responsible Medicine, USA on 3>0th July 2018
Enteral Nutrition Booklet release by Prof. Rajesh Malhotra, Chief Trauma Centre, on 5th September 2018
Swachta award 2018
Panel Discussion on 'Plant Based Nutrition for prevention and Treatment of Chronic Diseases
National Nutrition Month celeberation,Theme-Traditional Healthy & Nutritious Indian food for Pregnant and Lactating women on 7th- 8th Sep 2018 at 3rd floor, Amrit kaur OPD, Dept of Obs & Gynae, Organized by Dept. of Dietetics.
National Nutrition Month celeberation,Theme-Traditional Healthy & Nutritious Indian food for Pregnant and Lactating women on 7th- 8th Sep 2018 at 3rd floor, Amrit kaur OPD, Dept of Obs & Gynae, Organized by Dept of Dietetics
DR.PARMEET KAUR
CHIEF DIETICIAN
AIIMS
| Year’s | Name |
|---|---|
| 2023 | Dr. Narayanan B |
| 2022 | Dr. Rhea Ahuja |
| 2022 | Dr. Ananya Sharma |
| 2021 | Dr. Nikhil Mehta |
| 2021 | Dr. Nayaranan A |
| 2019 | Dr. Snehal Agarwal |
| 2019 | Dr. Pratik Mohta |
| 2018 | Dr. Suman Patra |
| 2018 | Dr. Neha Taneja |
| 2016 | Dr. Prateek Sondhi |
| 2016 | Dr. Deepika Yadav |
| 2015 | Dr. Sanjay Singh |
| 2014 | Dr. Riti Bhatia |
| 2014 | Dr. Minu Jose |
| 2013 | Dr. Neetu Bhari |
| 2013 | Dr. Vishal Gupta |
| 2011 | Dr. Divya Seshadri |
| 2009 | Dr. Jyoti Dhawan |
| 2007 | Dr. Sushrata Dash |
| 2007 | Dr. Komal Agarwal |
| 2005 | Dr. Radhakrishna Bhat |
| 2005 | Dr. Jasleen Kaur |
| S.N. | NAMES | YEAR OF PASSING | |
|---|---|---|---|
| 1 | Dr.Ameer Bharat Mani A.D. | DECEMBER | 1962 |
| 2 | Dr.Gurmohan Singh Khurana | DECEMBER | 1962 |
| 3 | Dr.B.V.Satyanarayana | DECEMBER | 1962 |
| 4 | Dr.C.Sobhanadri | MAY | 1963 |
| 5 | Dr.Brij Mohan Singh Bedi | MAY | 1963 |
| 6 | Dr.Lalit Kumar Bhutani | DECEMBER | 1963 |
| 7 | Dr.Harish Chandra Mohanty | DECEMBER | 1963 |
| 8 | Dr.Tarun Chandra Saikia | MAY | 1964 |
| 9 | Dr.K.M.Rama Rao | MAY | 1964 |
| 10 | Dr.M.I.Joy | MAY | 1964 |
| 11 | Dr.Jagjit Singh Pasricha | MAY | 1964 |
| 12 | Dr.Pasumarty Nagabhushanam | DECEMBER | 1964 |
| 13 | Dr.Vinod Kumar Sood | DECEMBER | 1964 |
| 14 | Dr.Virendra Nath Sehgal | DECEMBER | 1964 |
| 15 | Dr.T.Gopinathan | MAY | 1965 |
| 16 | Dr.Chandra Rajaratnam | MAY | 1965 |
| 17 | Dr.Jaidev Singh Mehta | DECEMBER | 1965 |
| 18 | Dr.Iyokomiyake(Matsumoto) | DECEMBER | 1965 |
| 19 | Dr.Kariyappala Siddapa | DECEMBER | 1965 |
| 20 | Dr.Harsha Kumar Sud | DECEMBER | 1965 |
| 21 | Dr.Dharam Pal | MAY | 1966 |
| 22 | Dr.Urmil Sabharwal(Khurana) | MAY | 1966 |
| 23 | Dr.Amar Kishore Sharma | MAY | 1967 |
| 24 | Dr.K.M.Prakash | MAY | 1967 |
| 25 | Dr.Mohammad Abdul Wali | MAY | 1967 |
| 26 | Dr.Rattan Singh | MAY | 1967 |
| 27 | Dr.Raghunath Patnaik | DECEMBER | 1967 |
| 28 | Dr.Ravinder Kumar Pandhi | DECEMBER | 1967 |
| 29 | Dr.Yashwant Kumar Malhotra | DECEMBER | 1967 |
| 30 | Dr.Vijay Kumari Gupta | MAY | 1968 |
| 31 | Dr.Mohammed Shati | DECEMBER | 1968 |
| 32 | Dr.Navnit Kumar Sharma | DECEMBER | 1968 |
| 33 | Dr.Amar Singh Sohi | MAY | 1969 |
| 34 | Dr.Ghulam Hassan Hajini | MAY | 1969 |
| 35 | Dr.Harbhajan Singh Girgia | MAY | 1969 |
| 36 | Dr.Kurvi Anandam | MAY | 1969 |
| 37 | Dr.P.A.Sarojini | MAY | 1969 |
| 38 | Dr.P.Sugathan | MAY | 1969 |
| 39 | Dr.Cynthia Joan Phyllis Papali | MAY | 1970 |
| 40 | Dr.Narender Kumar Mathur | DECEMBER | 1970 |
| 41 | Dr.Om Prakash Singh | DECEMBER | 1970 |
| 42 | Dr.Yogesh Chandra Minocha | DECEMBER | 1970 |
| 43 | Dr.Jogesh Das | DECEMBER | 1971 |
| 44 | Dr.Ramesh Chandra Sharma | DECEMBER | 1971 |
| 45 | Dr.Virender Kumar Khurana | DECEMBER | 1971 |
| 46 | Dr.Ashok Kumar Bajaj | DECEMBER | 1972 |
| 47 | Dr.Ram Dhan Mukhija | DECEMBER | 1972 |
| 48 | Dr.Shridhar Gopal Deshpande | DECEMBER | 1972 |
| 49 | Dr.Tilak Raj Bedi | DECEMBER | 1972 |
| 50 | Dr.Muthalampet Parameswaran | MAY | 1973 |
| 51 | Dr.Krishan Chander Nayyar | MAY | 1973 |
| 52 | Dr.Girdhar Gopaldhir | MAY | 1973 |
| 53 | Dr.Vikram Datt | DECEMBER | 1973 |
| 54 | Dr.A.Abraham | DECEMBER | 1973 |
| 55 | Dr.Bhawneshwar Kumar Girdhar | JAN. | 1975 |
| 56 | Dr.Dhanyamraju Seshagiri Rao | JAN. | 1975 |
| 57 | Dr.Kanwar Amrinder Jit | JAN. | 1975 |
| 58 | Dr.Syamalendra Mohan Sinha | JAN. | 1975 |
| 59 | Dr.Kolumum Ramachandran Ramak. | MAY | 1975 |
| 60 | Dr.Madhawa Anand Tutakne | MAY | 1975 |
| 61 | Dr.Raj Kumar Dutta | MAY | 1975 |
| 62 | Dr.Susheela Abraham | DECEMBER | 1975 |
| 63 | Dr.Mary George | MAY | 1976 |
| 64 | Dr.Mohan Zachariah Mani | MAY | 1976 |
| 65 | Dr.Malkit Singh | DECEMBER | 1976 |
| 66 | Dr.Monica Mohindra | DECEMBER | 1976 |
| 67 | Dr.Muidul Huda | DECEMBER | 1976 |
| 68 | Dr.Laxmi V.Nair | MAY | 1977 |
| 69 | Dr.Jyoti Borah | MAY | 1977 |
| 70 | Dr.Dinesh Chandra Govil | MAY | 1977 |
| 71 | Dr.Shashank M.Bhate | DECEMBER | 1977 |
| 72 | Dr.Alur Sainath Kumar | MAY | 1978 |
| 73 | Dr.Ramesh Chandra Dinkar Rao B | MAY | 1978 |
| 74 | Dr.Shailja Ratan Shukla | MAY | 1978 |
| 75 | Dr.Velampalayam Rajagopala K. | MAY | 1978 |
| 76 | Dr.Bhagwath Bachonee | DECEMBER | 1978 |
| 77 | Dr.Subhash Chander Bharija | MAY | 1979 |
| 78 | Dr.Cyriac Malayil Jacob | MAY | 1979 |
| 79 | Dr.Mahesh Chandra Mathur | MAY | 1979 |
| 80 | Dr.Sanjiv Kandhari | DECEMBER | 1979 |
| 81 | Dr.Ramji Gupta | DECEMBER | 1980 |
| 82 | Dr.Chandrakant Laxman Kotkar | DECEMBER | 1981 |
| 83 | Dr.Jose Thomas | DECEMBER | 1981 |
| 84 | Dr.Elizabeth George | MAY | 1982 |
| 85 | Dr.Vinod Kumar Sharma | MAY | 1982 |
| 86 | Dr.G.Zamzachin | MAY | 1983 |
| 87 | Dr.K.Lokendro Singh | MAY | 1983 |
| 88 | Dr.D.A.Satish | DECEMBER | 1983 |
| 89 | Dr.Rukma Lal Sharma | DECEMBER | 1983 |
| 90 | Dr.Shrinath Singh | DECEMBER | 1983 |
| 91 | Dr.Neena Vaswani | MAY | 1984 |
| 92 | Dr.Maya Jacob | MAY | 1984 |
| 93 | Dr.Vijay Ram Battu | DECEMBER | 1984 |
| 94 | Dr.Abhay Yeshwantrao Bhalme | MAY | 1985 |
| 95 | Dr.Narendra Kumar Singh | MAY | 1985 |
| 96 | Dr.Dileep Kumar Jayant | MAY | 1987 |
| 97 | Dr.Kolalapudi Seetharamanjan. | MAY | 1987 |
| 98 | Dr.M.Ramam | DECEMBER | 1987 |
| 99 | Dr.Kaushal Kishore Verma | DECEMBER | 1988 |
| 100 | Dr.Bindu Dewan | DECEMBER | 1988 |
| 101 | Dr.Omar Jabr Ismail Obar | MAY | 1989 |
| 102 | Dr.James Thanzama | MAY | 1989 |
| 103 | Dr.Uttam Kumar Khan | MAY | 1989 |
| 104 | Dr.Ajay K. Hindocha | MAY | 1990 |
| 105 | Dr.Urmi Mala Das | DECEMBER | 1990 |
| 106 | Dr.Siddartha Sankar Das | DECEMBER | 1991 |
| 107 | Dr.Binod Kumar Khaitan | DECEMBER | 1991 |
| 108 | Dr.Lalit Kumar Gupta | MAY | 1992 |
| 109 | Dr.Thokchom Nandakishore | DECEMBER | 1992 |
| 110 | Dr.Vizolie Z.Suokhrie | DECEMBER | 1992 |
| 111 | Dr.Vikas Khera | DECEMBER | 1992 |
| 112 | Dr.Vinay Shanker Gupta | MAY | 1993 |
| 113 | Dr.Lalthilengliani | MAY | 1993 |
| 114 | Dr.Atul Taneja | DECEMBER | 1993 |
| 115 | Dr.Neeraj Bajaj | DECEMBER | 1993 |
| 116 | Dr.Devraj Dogra | DECEMBER | 1994 |
| 117 | Dr.Paschal Vivek D'souza | MAY | 1995 |
| 118 | Dr.Vijay Gandhi | DECEMBER | 1995 |
| 119 | Dr.Naina Kala Sharma | DECEMBER | 1995 |
| 120 | Dr.Aziza Rustom | MAY | 1996 |
| 121 | Dr.Arun Joshi | MAY | 1996 |
| 122 | Dr.Leishiwon Kumrah | MAY | 1996 |
| 123 | Dr.Sanjay Kumar Rathi | MAY | 1996 |
| 124 | Dr.E.Mhabemo Ovung | MAY | 1997 |
| 125 | Dr.Apra Sood | MAY | 1997 |
| 126 | Dr.Shyamal Kanti Chakrabarti | DECEMBER | 1998 |
| 127 | Dr.Yashpal Manchanda | DECEMBER | 1999 |
| 128 | Dr.Rajesh Kumar | DECEMBER | 1999 |
| 129 | Dr.Arun Achar | DECEMBER | 1999 |
| 130 | Dr.Yumnam Lokendra Singh | DECEMBER | 1999 |
| 131 | Dr.Taru Garg | DECEMBER | 1999 |
| 132 | Dr.Sandeep Sharma | DECEMBER | 2000 |
| 133 | Dr.Krishna Deb Barman | MAY | 2001 |
| 134 | Dr.Prasad H.R.Y. | MAY | 2001 |
| 135 | Dr.Arpana Rijal | DECEMBER | 2001 |
| 136 | Dr.Sudip Das | DECEMBER | 2001 |
| 137 | Dr.Trilokraj Tejasvi | MAY | 2002 |
| 138 | Dr.Radhakrishna Bhat | DECEMBER | 2002 |
| 139 | Dr.Suchibrata Das | DECEMBER | 2002 |
| 140 | Dr.Pakhi P.S.Pandarwani | DECEMBER | 2003 |
| 141 | Dr.Saurabh Agarwal | DECEMBER | 2003 |
| 142 | Dr.Anil Kumar Vijai Minz | MAY | 2004 |
| 143 | Dr.Krishna Sumanthm | DECEMBER | 2004 |
| 144 | Dr.Amit Kumar Malhotra | MAY | 2005 |
| 145 | Dr.Jasleen Kaur | DECEMBER | 2005 |
| 146 | Dr.Amit Kumar Malhotra | MAY | 2005 |
| 147 | Dr.Jasleen Kaur | DEC | 2005 |
| 148 | Dr.Chandra Mohan Kudligi | DECEMBER | 2006 |
| 149 | Dr.Arika Bansal | DECEMBER | 2006 |
| 152 | Dr.Dinesh P Asati | MAY | 2007 |
| 153 | Dr.Komal Aggarwal | DECEMBER | 2007 |
| 154 | Dr.Sushruta Shefali Dash | DECEMBER | 2007 |
| 155 | Dr.Pooja Sehdev | MAY | 2008 |
| 156 | Dr.Pradeep Kumar Sethy | MAY | 2008 |
| 157 | Dr.Nidhi Shah | MAY | 2008 |
| 158 | Dr.Chandanmal Suthar | DEC | 2008 |
| 159 | Dr.Pooja Khetan | MAY | 2009 |
| 160 | Dr.Pankajchaturvedi | DECEMBER | 2009 |
| 161 | Dr.Dilip Kumar Meena | DECEMBER | 2009 |
| 162 | Dr.Parul Verma | MAY | 2010 |
| 163 | Dr.Sah Gaurang Krishna | DECEMBER | 2010 |
| 164 | Dr.Saurabh Singh | DECEMBER | 2010 |
| 165 | Dr.Amrendra Kumar | MAY | 2011 |
| 166 | Dr.Divya Seshadri | MAY | 2011 |
| 167 | Dr.Ashok Roopchand Wadhwani | MAY | 2011 |
| 168 | Dr.Kavish Chouhan | MAY | 2011 |
| 169 | Dr.Ashwin Rao | DECEMBER | 2011 |
| 170 | Dr.K.Maharaja | MAY | 2012 |
| 171 | Dr.Aditi Jha | MAY | 2012 |
| 172 | Dr.Mahendra E Sonune | DECEMBER | 2012 |
| 173 | Dr.Neetu Bhari | MAY | 2013 |
| 174 | Dr.Sunil Kumar Kothiwala | MAY | 2013 |
| 175 | Dr.Binamra Basnet | MAY | 2013 |
| 176 | Dr.Vishal Gupta | DECEMBER | 2013 |
| 177 | Dr. Priyanka | MAY | 2014 |
| 178 | Dr. Aanchal Panth | MAY | 2014 |
| 179 | Dr. Riti Bhatia | MAY | 2014 |
| 180 | Dr. Prashant Gupta | MAY | 2014 |
| 181 | Dr. Minu Jose Chiramel | DECEMBER | 2014 |
| 182 | Dr. Shreyans Mutha | DECEMBER | 2014 |
| 183 | Dr. Pawan Kumar | DECEMBER | 2014 |
| 184 | Dr. Pramod Agrawal | DECEMBER | 2014 |
| 185 | Dr. Mankul Goyal | DECEMBER | 2014 |
| 186 | Dr. Suman Patra | MAY | 2015 |
| 187 | Dr. Ajay Kumar Rai | MAY | 2015 |
| 188 | Dr. Prakash Kumar Khute | MAY | 2016 |
| 189 | Dr. Piyush Pahadiya Khatik | MAY | 2016 |
| 190 | Dr. Kanya Rani Vashisht | MAY | 2016 |
| 191 | Dr. Sanjay Singh | MAY | 2016 |
| 192 | Dr. Sweta Subhadarshani | DECEMBER | 2016 |
| 193 | Dr. Geetika Srivastava | DECEMBER | 2016 |
| 194 | Dr. Deepika Yadav | MAY | 2017 |
| 195 | Dr. Alok Kumar Sahoo | MAY | 2017 |
| 196 | Dr. Tanvi Dev | MAY | 2017 |
| 197 | Dr. Setu Mittal | MAY | 2017 |
| 198 | Dr. Neha Taneja | DECEMBER | 2017 |
| 199 | Dr. Mamta Rai | DECEMBER | 2017 |
| 200 | Dr. Nimitha .P | DECEMBER | 2017 |
| 201 | Dr. Saurabh Bhatia | MAY | 2018 |
| 202 | Dr. Himabindu S | MAY | 2018 |
| 203 | Dr. Sarojpoudel | DECEMBER | 2018 |
| 204 | Dr. Priyesh | DECEMBER | 2018 |
| 205 | Dr. Maninder Kaur | DECEMBER | 2018 |
| 206 | Dr. Gridharan Senthilnathan | MAY | 2019 |
| 207 | Dr. Abhishek G N | MAY | 2019 |
| 208 | Dr. Snehal Agrawal | MAY | 2019 |
| 209 | Dr. Mohta Pratik Rajendra | DECEMBER | 2019 |
| 210 | Dr. Gunaabalaji D.R. | DECEMBER | 2019 |
| 211 | Dr. Nikhil Mehta | JUNE | 2020 |
| 212 | Dr. Sandesh Shah | JUNE | 2020 |
| 213 | Dr. Karthik L | JUNE | 2020 |
| 214 | Dr. Narayanana | JUNE | 2020 |
| 215 | Dr. Prashant Bharti | JUNE | 2020 |
| 216 | Dr. Jitender | DECEMBER | 2020 |
| 217 | Dr. Utpal Patel | DECEMBER | 2020 |
| 218 | Dr. Pankhuri Dudani | DECEMBER | 2020 |
| 219 | Dr. Ananya Sharma | JUNE | 2021 |
| 220 | Dr. Parth K Radhani | JUNE | 2021 |
| 221 | Dr. Akash | JUNE | 2021 |
| 222 | Dr. Suvesh Singh | JUNE | 2021 |
| 223 | Dr. Nil Mani Priyadarshi | DECEMBER | 2021 |
| 224 | Dr. Rhea Ahuja | DECEMBER | 2021 |
| 225 | Dr. Sachin Gupta | DECEMBER | 2021 |
To gain more information regarding eligibility and procedure for applying for above fellowships and training kindly contact Room No 4070, Teaching Block, AIIMS, Ansari Nagar, New Delhi (Phone-91-11-26583217) or write a mail to office.dermatology@gmail.com
Our indoor patient department has a day care facility for administering pulsed steroids and biologics.
Patients requiring day care and admission to the hospital are admitted to the 30-bed D-I Ward located on the first floor of the Ward Block in the main Hospital. Patients are admitted after evaluation in the OPD or emergency department.
The department caters to the needs of outdoor patients daily (Monday to Friday) from 9:00 AM.
The following facilities are available for patients:
| Morning OPD | Afternoon Clinics | Dermato Surgery | Laser | Ward Round | DPR | |
|---|---|---|---|---|---|---|
| Monday | Dr.M. Ramam Dr.Sujay Khandpur Dr.Neetu Bhari STD Clinic Dr. Neetu Bhari | Leprosy Dr. Vishal Gupta Photodermatology Dr. Sujay Khandpur Dr. Neetu Bhari | Hair Removal Laser Dr Neetu Bhari | Dr. Kaushal K. Verma Dr. Somesh Gupta | Dr.M Ramam | |
| Tuesday | Dr. Kaushal K Verma Dr. Somesh Gupta Dr. Kanika Sahni Dr. Neha Taneja STD Clinic Dr. Somesh Gupta | Dr Vishal Gupta | Dr G Sethuraman | Dr.Vishal Gupta | ||
| Wednesday | Dr G Sethuraman Dr. Neetu Bhari Dr. Vishal Gupta STD Clinic Dr. Vishal Gupta | Dermatosurgery Dr.Kaushal K. Verma Dr. Somesh Gupta Dr Kanika Sahni STD Follow up Dr Kaushal K Verma Dr Somesh Gupta | Dr. Somesh Gupta | Carbon Dioxide Laser Dr. Kaushal K. Verma Dr. G Sethuraman Dr. Vishal Gupta | Dr. Sujay Khandpur | Dr. Sujay Khandpur |
| Thursday | Dr. M. Ramam Dr.Sujay Khandpur Dr. Kanika Sahni Dr. Neha Taneja STD Clinic Dr Kanika Sahni | Psoriasis Dr. Sujay Khandpur Dr. Kanika Sahni Pigmentation Dr. Kanika Sahni Dr. Vishal Gupta | Vitiligo Surgery Dr. Somesh Gupta | Nd-Yag Laser Dr. Kanika Sahni Dr G sethuraman | Dr. Vishal Gupta | Dr. Neetu Bhari |
| Friday | Dr. Kaushal K. Verma Dr. Somesh Gupta Dr. Vishal Gupta STD Clinic Dr. Kaushal K. Verma | Allergy Dr. Kaushal K Verma Dr. Neetu Bhari Dr. Vishal Gupta Paediatric Dermatology Dr G Sethuraman Dr. Neetu Bhari Dr. Vishal Gupta | Dr. Kanika Sahni | PDL Dr. Sujay Khandpur | Dr. M. Ramam Dr. Neetu Bhari | Dr. M Ramam |
| Saturday | Case Conference All Faculty | Dermatopathology Conference 12-1.00 PM Dr M Ramam Dr. Sujay Khandpur Dr. Neetu Bhari Dr. Vishal Gupta | Dr. Kanika Sahni | By rotation: Dr. M Ramam Dr. Sujay Khandpur Dr. Neetu Bhari Dr. Vishal Gupta |
The department was set up by the late Prof K C Kandhari (HoD,1960-1970) and subsequently headed by late Prof L K Bhutani (1974-1996), Prof J S Pasricha (1996-1998), Prof R K Pandhi (1998-2001), Prof Vinod K Sharma (2001-2020), and Prof Neena Khanna (2020-2022). Prof Kaushal K Verma is heading the department since July 2022.
The department is widely recognised for the quality and innovativeness of its teaching programme for both undergraduate and postgraduates and its contributions to patient care and research. The latter include advances in the diagnosis and treatment of pemphigus, vitiligo (using both medical and surgical techniques and phototherapy), air-borne contact dermatitis, mycetoma, drug reactions, epidermolysis bullosa, ichthyosis-associated rickets and dermatopathology, among others. Faculty members have authored several popular undergraduate and postgraduate textbooks that are used in centres around the world.
Members of the faculty have served in leadership positions in national and international professional organisations, provided consultations to governmental and non-governmental agencies, organised workshops and conferences, served on the faculty of meetings worldwide and as visiting professors at universities in other countries.
The Department provides training to MBBS, MD and PhD students. These students are chosen through a centralised selection test conducted by AIIMS.
Additionally, short term observerships are offered to both national and international trainees in various aspects of the specialty (see https://www.aiims.edu/en/academic_section_training.html for requirements and application details).
Outpatient services
The Skin OPD is located on the third floor of the new Rajkumari Amrit Kaur OPD and caters to outdoor patients from Monday to Friday from 9:00 AM.
An Appointment is required to visit the department.
Our department provides care for adults and children with diseases of the skin, hair and nail, leprosy and sexually transmitted infections. We provide medical, surgical, phototherapy, laser and aesthetic services, as appropriate.
The department also runs specialty clinics in the afternoon for leprosy, photodermatoses, dermato-surgery and aesthetics, pediatric dermatology, vitiligo and other pigmentary diseases, psoriasis and allergic diseases of the skin including urticaria, contact dermatitis and drug allergies. Patients are referred to the afternoon clinics after initial evaluation in the morning OPDs.
Patients requiring day care and admission to the hospital are admitted to the 30-bed D-I Ward located on the first floor of the Ward Block in the main Hospital. Patients are admitted after evaluation in the OPD or emergency department.
Faculty members of the department are involved in conducting several funded and non-funded research projects on various aspects of skin diseases, leprosy and sexually transmitted infections. The department has a well-equipped research laboratory.
| S.No. | List | Link |
|---|---|---|
| 1 | M.Sc (N) Cardilogical/CTVS Nursing Students (2006-2024) | Link |
| 2 | M.Sc (N) Critical Care Nursing Students (2006-2024) | Link |
| 3 | M.Sc (N) Nephrological Nursing Students (2006-2024) | Link |
| 4 | M.Sc (N) Neurosciences Nursing Students (2006-2024) | Link |
| 5 | M.Sc (N) Oncological Nursing Students (2006-2024) | Link |
| 6 | M.Sc (N) Paediatrics Nursing Students (2006-2024) | Link |
| 7 | M.Sc (N) Psychiatric Nursing Students (2006-2024) | Link |
| 8 | Ph.D Nursing Students from 2015 to 2024 | Link |
| 9 | B.Sc (PB) Nursing Students (2023-2025) Batch | Link |
| 10 | B.Sc (H) Nursing Students (2021-2025) Batch | Link |
| S. No. | Programs Offered | Duration | No. of Seats |
|---|---|---|---|
| 1. | B. Sc. (Hons.) Nursing | 4 years | 77 |
| 2. | B. Sc. (Post-Basic) Nursing | 2 years | 25 |
| 3. | M. Sc. Nursing Pediatric Nursing Psychiatric Nursing Cardio logical /CTVS Nursing Neurological Nursing Oncological Nursing Critical Care Nursing Nephrological Nursing | 2 years | 22 |
The department organized “64th Annual National Conference of Indian Public Health Association (IPHA)” at AIIMS, New Delhi from February 28 to March 2, 2020 that was attended by more than 1100 national and international public health delegates.
Plantation drive was conducted in SDH, Ballabgarh and both the PHCs on June 5, 2022, as a part of the world environment day.

National collaborations for research, training and health programs

International collaborations
In the year 2021-2022, a total of 96 articles has been published with the faculties and/or residents of the department being one of the authors. Following are the list of those published articles.

SDH, Ballabgarh has operation theatre complex (OT) with one minor and two major operation theatres. The OT are equipped with latest technology including ventilators, anesthesia services for general, spinal and local anesthesia. Major services conducted here include cholecystectomy, total abdominal hysterectomy, vaginal hysterectomy, lower section caesarean section (LSCS) and hernia repair. The OT has an operating microscope for ophthalmic surgeries, using which cataract surgery with intra ocular lens (IOL) implantation and other ocular surgeries are performed.
A branch library is located in the campus of Ballabgarh with recent edition medical books. The library also has computer facilities for searching various medicine databases including Medline, Cochrane, Google Scholar etc.
Health talk on various health topic is provided at regular intervals by resident doctors, undergraduate students and nursing students, in both urban and rural field areas.


Urban Health Centre also provides basic laboratory services which include hemoglobin estimation, blood sugar measurement, and blood grouping.
The laboratory is equipped with auto analyzers for blood biochemistry, hematology, cytology, and microscopic facility. It also provides X-ray and ultrasound services. All the investigations are free of cost and available as per hospital hours, while urgent and emergency investigations are available round the clock.
Basic laboratory investigations including hemoglobin estimation, blood glucose measurement, blood grouping, peripheral smear for malaria, and sputum smear microscopy are provided free of cost in both the PHCs.
No inpatient services are available at UHC, Dakshinpuri.

Sub district hospital, Ballabgarh has a 50 bedded ward, a well-equipped labour room and neonatal unit. Doctor on duty, nursing staff and other auxillary staff remains available in ward for 24 hours. Specialist doctor in obstetrics & gynecology and pediatrics are available in the campus, remain on call.


Each PHC has 6 inpatient beds. Patients with conditions which can be managed at PHCs are admitted to wards. Delivery hut along with newborn care corner is available for delivery services of ANC. ANC patients are admitted for delivery and are discharged 48 hours after the delivery. All admissions are for shorter duration and no patients with chronic morbidity are admitted in the wards.
Outpatient services are provided at the Urban Health Clinic (UHC) in Dakshinpuri resettlement colony, Dr. Ambedkar Nagar on 5 days a week. The clinic is run by residents of the department. Also, immunization services are provided through immunization clinics held twice in a week
Comprehensive Rural Health Services Project (CRHSP), Ballabgarh comprises a sub district hospital (SDH), and two Primary Health Centres (PHCs) at Dayalpur, and at Chhainsa. Outpatient services at Sub district hospital (SDH), Ballabgarh includes the following:
| Daily | Once weekly |
|---|---|
| General Medicine | Non-Communicable Disease Clinic |
| General Surgery | Physical Medicine and Rehabilitation (PMR) |
| Paediatrics | Paediatric Surgery |
| Obstetrics and Gynaecology | Nutrition OPD |
| Ophthalmology | |
| Psychiatry | Thrice weekly |
| Dental | Ante-natal clinic |
| AYUSH (Homeopathy) | |
| AYUSH (Ayurveda) | Twice weekly |
| Orthopaedics | Dermatology |
| Ear, Nose, and Throat |
PHCs provide the following outpatient services:

Both PHC Dayalpur and PHC Chhainsa provide outpatient services daily in the forenoon. Patients are seen by residents of Community Medicine and interns. Patients who can be managed at PHC are provided treatment during the clinic; patients requiring more specialized care are referred to SDH, Ballabgarh. AYUSH OPD service is available at PHC Dayalpur.
Extension Health Clinics (EHC) provide outpatient services at subcentre. Each of the six subcentres is visited once a week by residents and interns as per the schedule. Drugs are provided to the patients for a week depending on the availability. Outreach Antenatal Camps are conducted in the villages regularly so as to provide quality antenatal care at village level.
Outreach Specialty clinics (ORSO) are held at both the PHCs, once a week on Tuesdays. Senior residents of obstetrics, paediatric, ophthalmology, psychiatry visit the PHC for providing consultation.
The postgraduate students of Community Medicine are posted in the urban health programme for 18 months, which is divided into postings at the urban health centre, academic activities, field assignments, and other special activities. The posting at CRHSP, Ballabgarh, is for 18 months and is residential. Out of the total duration, they spend 5 months and 10 days each at the sub-district hospital (SDH) and both primary health centres (PHCs) on a rotational basis. This gives them adequate opportunities to gain the necessary skills and experience at both SDH and PHCs.The regular teaching programme includes seminars, family and clinical case presentations, operational research, and problem-solving exercises based on the Health Management Information System and field data. Residents also participate in various activities conducted at PHCs and in villages under different National Health Programmes.
The interns are posted for a total duration of three months at CRHSP Ballabgarh. This period is divided into six weeks at SDH and three weeks at each of the PHCs located in Dayalpur and Chhainsa. The entire posting is residential.At SDH, interns are posted in OPDs and wards, helping them learn basic clinical skills and inpatient management, including conducting normal deliveries. In OPDs, they are rotated through all available clinical disciplines under the supervision of respective Senior Residents (SRs).During their PHC posting, interns participate in healthcare delivery at PHC clinics, sub-centres, and antenatal clinics. They are also posted at the delivery huts under the overall supervision of SRs in Community Medicine. They gain experience in supervising health workers, following up on tuberculosis treatment defaulters, supervising sub-centres, conducting outreach activities, immunization, and other ongoing PHC activities.At the end of their CRHSP posting, interns submit their logbook, duly signed by respective SRs, for an end-posting assessment.
MBBS students in their 4th-5th semesters are posted in the urban health programme for five weeks, where they conduct epidemiological exercises, health talks, and family studies. During these semesters, they also participate in the Family Health Advisory Services (FHAS), where they follow up with assigned families over nine months and implement interventions to improve their health. Recently, FHAS was remodeled to focus on chronic diseases, children, and adolescents.MBBS students of the 7th semester from AIIMS, New Delhi, are posted at CRHSP Ballabgarh in four batches for six weeks each. During this posting, they are taught concepts of epidemiology and given an orientation to community health, including social determinants of health, community aspects of child and mental health, health systems at various levels, and health programmes.The students also undertake a brief qualitative research project under the module Orientation of Undergraduates to Community Health (OUCH). Each six-week posting concludes with an internal assessment.
B.Sc. nursing students and post certificate nursing students are posted for one and half months at CRHSP Ballabgarh. This posting is residential in nature. They spend one month at SDH and two weeks in either of the two PHCs. They are provided training in antenatal care, management of ward, and immunization. They are posted both in OPD and in ward. They provide health talks, and IEC in OPD, and ward. Training of nursing students is supervised by a Faculty Member from the College of Nursing, AIIMS, New Delhi
Regional training of Network Institutions to deliver People-centred integrated NCD care: 4-8 Oct 2021 – online
Training programme on the use of “Larvicide and Insecticides for the Prevention and Control of Vector Borne Diseases” was organized for staff of DPORC on 07.05.2021 at CCM, AIIMS
Training of State Nodal Officer under National Programme of Climate Change and Human Health (NPCCHH) – August 2021
Training of trainers of development of Skill module for SET facility AIIMS
7th International Course on Public Health Approaches to Non-communicable diseases
Workshop on “Future Primary Health Care Systems”
Periodic in-service trainings are conducted for different cadres of staff working at the CRHSP Ballabgarh.
A three-year postgraduate course in Community Medicine (MD) is offered by the department. Selection of the junior residents for the course is based on the Institute of National Importance - Combined Entrance Examination (INI-CET), held twice a year. Please refer to the education section for course details.
Candidates are selected through the Common Entrance Test (CET), held twice a year. The seats are made available according to the availability of vacancies with respective faculty. The final selection of candidates for the course is through a departmental interview. Following are the thesis/dissertations of past PhD candidates in the department:
| S.No | Title | Author | Guide | Date |
|---|---|---|---|---|
| 1 | Health beliefs in relation to coronary heart disease | Usha Srivastav | L. M. Nath | 1995 |
| 2 | Impact of Vitamin A supplementation in infancy on immune response to oral polio and measles vaccines | Rajeev Bahl | L. M. Nath / Shashi Kant | 1997 |
| 3 | Epidemiology of Typhoid fever: Descriptive information from a longitudinal study | Anju Sinha | V.P. Reddaiah | 2002 |
| 4 | Health status of the aged in a rural community | Anil Goswami | V.P. Reddaiah | 2002 |
| 5 | A study of hygiene behavior of water treatment practices of residents of slums in North India in the context of an ongoing behavior change intervention | Ritvik | Anand Krishnan | 2010 |
| 6 | Implementation and evaluation of health settings approved for prevention of non-communicable diseases in children of middle schools of rural Ballabhgarh (block), district Faridabad, Haryana, India | Deepika Singh Saraf | Anand Krishnan | 2013 |
| 7 | Economic evaluation of influenza immunization of under 5 children in India | Debjani Ram Purakayastha | Anand Krishnan | 2016 |
| 8 | Estimation of mortality burden in India due to respiratory viruses: Influenza and respiratory syncytial virus | Venkatesh Vinayak Narayan | Anand Krishnan | 2019 |

The All India Institute of Medical Sciences (AIIMS) was established by the Parliament of India in 1956 as an Institute of national importance with the object “to develop patterns of teaching in undergraduate and postgraduate medical education in all its branches so as to demonstrate a high standard of medical education to all medical colleges and other allied institutions in India”. Since the inception of the institute, the Centre for Community Medicine (CCM) has been a key department at AIIMS. The Centre aims to produce high quality public health professionals and community physicians. The Centre is consistently working towards discovery of new knowledge in domain of public health, advocacy for application of new ideas in health care of populations. The main focus area of the Centre has been on evolution of a replicable model of comprehensive health services and providing consultancy to strengthen capacity of health organizations at national and international level.
To establish and maintain rural and urban health organizations which will form centres for the field training of the medical, dental, and nursing students of the Institute as well as for the research into community health problems. This is in consonance with the stated function of AIIMS, Section 14, f(v) of AIIMS Act, 1956
To respond to the evolving national public health needs in keeping with global standards of teaching, research, and service by creating a professional workforce to translate knowledge to action and thereby contribute towards HEALTH FOR ALL
The Urban health program of the Centre provides community based health services to marginalised population of an urban resettlement colony in Dakshinpuri Extension, Ambedkar Nagar, New Delhi. Preventive, promotive and curative health services along with basic laboratory services are provided to the population covered by the Urban health program.
The details of the urban health program of the Centre are available in following link
The Rural health program of the Centre is also known as the Comprehensive Rural Health Services Project (CRHSP), Ballabgarh. The rural field practice area was started in 1961 with aid of Rockefeller Foundation. In year 1965 the CRHS Project was formally established in Ballabgarh Block, Faridabad District of Haryana as a collaborative project between Haryana State Government and AIIMS. The project comprises of:
The details of the rural health program of the Centre are available in following link
| S. No | Year | Name | Surname | Email ID |
|---|---|---|---|---|
| 1 | 1973 | Dr. Saroj | Chooramani | sarojchooramani@gmail.com |
| 2 | 1975 | Dr. Dilip Kumar | Mitra | dkmitra2002@yahoo.com |
| 3 | 1975 | Dr. Hira Lal | Goswami | dr_hlgoswami@rediffmail.com |
| 4 | 1975 | Dr. Madhuri | Nigam | |
| 5 | 1977 | Dr. R.K. | Tandon | raghavtandon30@gmail.com |
| 6 | 1977 | Dr. Y. Nayudamma | Nayudamma | drnayudamma@gmail.com |
| 7 | 1978 | Dr. Mohd. Ashraf | Mufti | |
| 8 | 1978 | Dr. Rajiv | Kulshrestha | krajeev48@yahoo.com |
| 9 | 1979 | Dr. N.C.K. | Reddy | nck_suka@yahoo.co.in |
| 10 | 1980 | Dr. A.B. | Mathur | azadmathur@hotmail.com |
| 11 | 1980 | Dr. Om Prakash | Tucker | omptucker@hotmail.com |
| 12 | 1982 | Dr. D.K. | Gupta | profdkgupta@gmail.com |
| 13 | 1983 | Dr. M.A. | Hussainy | USA |
| 14 | 1983 | Dr. Satyanarayana | Gorthi | sngorthi@hotmail.com |
| 15 | 1983 | Dr. Veereshwar | Bhatnagar | veereshwarb@hotmail.com |
| 16 | 1984 | Dr. Prashant | Upadhyaya | praline.new@gmail.com |
| 17 | 1984 | Dr. Ajay | Kumar | ajayaruna112@rediffmail.com |
| 18 | 1984 | Dr. Jayanta Kumar | Iyengar | deceased |
| 19 | 1984 | Dr. Kapil Kumar | Vidyarthi | kvidyarthi@dataone.in |
| 20 | 1986 | Dr. Anurag | Krishna | anurag_krishna@hotmail.com |
| 21 | 1986 | Dr. Vivek Gharpure | Vishwanath | ivekvgharpure@gmail.com |
| 22 | 1986 | Dr. Meera Luthra | Khazanchi | meera55@yahoo.com |
| 23 | 1987 | Dr. M. | Bajpai | bajpai2@hotmail.com |
| 24 | 1987 | Dr. N.K. | Jetley | nkjetly@hotmail.com |
| 25 | 1988 | Dr. Mohd Yusuf | Wani | doc.dm431@yahoo.com |
| 26 | 1988 | Dr. Sudhir | Chandna | sudhirchandna@gmail.com |
| 27 | 1988 | Dr. P.C. | Das | pcdas@yahoo.com |
| 28 | 1988 | Dr. S.N. | Kureel | snkkgmu@rediffmail.com |
| 29 | 1989 | Dr. Rajiv | Chadha | rajiv_chadha_01@yahoo.com |
| 30 | 1989 | Dr. P. Subba | Rao | polasubbarao@hotmail.com |
| 31 | 1990 | Dr. R.V. Shivarama | Prasad | rvsp@vsnl.com |
| 32 | 1991 | Dr. Devesh | Misra | dmisra@doctors.org.uk, dmisra@ntlworld.com |
| 33 | 1991 | Dr. Sandeep | Agarwala | sandpagr@hotmail.com |
| 34 | 1991 | Dr. Amita | Sen | amitasen1959@yahoo.com |
| 35 | 1992 | Dr. Satish Kumar | Agarwal | dr_satish_aggarwal@yahoo.com |
| 36 | 1992 | Dr. John | Rattan | drjohnsimmi@yahoo.com |
| 37 | 1992 | Dr. R | Ramaswamy | |
| 38 | 1994 | Dr. Simmi | Rattan | drjohnsimmi@yahoo.com |
| 39 | 1994 | Dr. P.K. | Jenna | pradeepjena@msn.com |
| 40 | 1994 | Dr. Raman | Kataria | jss_ganiyari@rediffmail.com |
| 41 | 1994 | Lt.Col. Ravi | Kale | drravikale@yahoo.com |
| 42 | 1995 | Dr. Sanjay | Gupta | |
| 43 | 1995 | Dr. Ashish | Minocha | ashish.minocha@nnuh.nhs.uk |
| 44 | 1995 | Dr. Rakesh | Handa | drrakeshhanda@gmail.com |
| 45 | 1996 | Dr. Richa | Lal | richalal@sgpgi.ac.in |
| 46 | 1996 | Dr. Anindya | Chattopadhya | achattopadhyay@yahoo.com |
| 47 | 1996 | Dr. Jyanto | Goswami | drjayanta@hotmail.com |
| 48 | 1997 | Dr. Thichen | Lama | thichen@hotmail.com, thichenlama@yahoo.co.uk |
| 49 | 1997 | Dr. M. | Srinivas | srinivasem@hotmail.com |
| 50 | 1997 | Dr. Anand | Alladi | alladianand@gmail.com |
| 51 | 1997 | Dr. Kanishka | Das | kanishkadas@hotmail.com |
| 52 | 1998 | Dr. Sumit | Dave | sdave_dr@yahoo.com |
| 53 | 1998 | Dr. Anupam | Lal | anupamlall@doctors.org.uk |
| 54 | 1998 | Dr. Hemonta Kumar | Dutta | drhemontad@rediffmail.com |
| 55 | 1999 | Dr. Manu | Arora | dr_manu_arora@hotmail.com, drmanuarora@gmail.com |
| 56 | 1999 | Dr. V.V.S.S. Chandra | Sekhram | vvsssekharam@yahoo.co.in |
| 57 | 1999 | Dr. Lakshmi | Nambirajan | lnambirajan@hotmail.com |
| 58 | 2001 | Dr. Sai | Prasad T.R | trsai@rediffmail.com |
| 59 | 2001 | Dr. Archana | Puri | puriarchana@hotmail.com |
| 60 | 2001 | Dr. Akshay Pratap Singh | Chauhan | akshaypratap2000@gmail.com |
| 61 | 2001 | Dr. Nisar Ahmed | bhat | nisarabuhade@yahoo.com |
| 62 | 2001 | Dr. Antony Robert | Charles | robertantony@hotmail.com |
| 63 | 2003 | Dr. Kamlesh | Pal | kamlesh_pal@yahoo.com |
| 64 | 2003 | Dr. Samir Kant | Acharya | drsamir293@gmail.com |
| 65 | 2003 | Dr. Manoj Kumar | Mohanty | manoj65us@yahoo.com |
| 66 | 2003 | Dr. Rajiv | Barua | dr_rajibraybaruah@yahoo.co.in |
| 67 | 2003 | Dr. Arbinder Kumar | Singal | arbinders@yahoo.com |
| 68 | 2004 | Dr. Balamourougane | P | bala_sowba@rediffmail.com |
| 69 | 2004 | Dr. Arun | Kumr | krishnarun@yahoo.com |
| 70 | 2005 | Dr. Lalit | Parida | drlalitparida@yahoo.co.in |
| 71 | 2006 | Dr. Gautam Shanker | Agarwal | gautamdoc@gmail.com |
| 72 | 2006 | Dr. Bibekananda | Jindal | drvivekjindal@rediffmail.com |
| 73 | 2007 | Dr. Manish | Pathak | mp3pathak@yahoo.co.in |
| 74 | 2007 | Dr. M | Raghvan | dr_ragavan_2001@rediffmail.com |
| 75 | 2007 | Dr. Devendra | Yadav | drdevyadav@gmail.com, drdevendra@hotmail.com |
| 76 | 2008 | Dr. Vishesh | Jain | visheshu@gmail.com |
| 77 | 2008 | Dr. Aejaz | Baba | draejaz@yahoo.com |
| 78 | 2009 | Dr. Suhasini | Gazula | suhasinigazula@gmail.com, suhasinigazula@rediffmail.com |
| 79 | 2009 | Dr. G | Moorthy | drmoorty@gmail.com |
| 80 | 2009 | Dr. Lucky | Gupta | drguptalucky@yahoo.com |
| 81 | 2009 | Dr. Kishorjit Irom | Singh | driksingh@yahoo.co.in |
| 82 | 2010 | Dr. Pramod | Sharma | drsharmapramod@yahoo.co.in |
| 83 | 2010 | Dr. Prabudh | Goel | drprabudhgoel@gmail.com |
| 84 | 2010 | Dr. Anand | Sinha | dranandsinha@hotmail.com |
| 85 | 2011 | Dr. Shasanka | Panda | drshasanka_aiims@yahoo.co.in |
| 86 | 2012 | Dr. Nidhi | Sugandhi | drnidhisugandhi@gmail.com |
| 87 | 2012 | Dr. V.Shankar | Raman | shankyafmc@yahoo.com |
| 88 | 2012 | Dr. Gayatri | Munghate | drgayatrism@gmail.com |
| 89 | 2012 | Dr. Shailesh | Solank | drshaileshsolanki82@rediffmail.com |
| 90 | 2012 | Dr. Ankur | Mandelia | ramblingreflections@yahoo.com |
| 91 | 2013 | Dr. Ajay | Verma | talk2ajayverma@rediffmail.com |
| 92 | 2013 | Dr. Nitin | Sharma | nitinsharma4you@gmail.com |
| 93 | 2013 | Dr. Rajan | Garg | rajangarg1985@yahoo.com |
| 94 | 2013 | Dr. Dibyarup Datta | Pramanik | dibyarupdatta@gmail.com |
| 95 | 2014 | Dr. Amit | Singh | amitps2011@gmail.com |
| 96 | 2014 | Dr. Karunesh | Chand | karuneshshahi@gmail.com |
| 97 | 2014 | Dr. S.K. | Dey | santodey@gmail.com |
| 98 | 2015 | Dr. Vikram | Khanna | vikramaiims@gmail.com |
| 99 | 2015 | Dr. Deepak | Mittal | doc.dm431@yahoo.com |
| 100 | 2015 | Dr. Divya | Bhadoo | drdbhadoo@gmail.com |
| 101 | 2015 | Dr. Anuj | Bhatia | abcbhatiaraghu@gmail.com |
| 102 | 2015 | Dr. Narinder | Techchandani | narinder_tek@yahoo.com |
| 103 | 2015 | Dr. Aparajita | Mitra | aparajita270@gmail.com |
| 104 | 2016 | Dr. Kashish | Kumar | kashmodern@gmail.com |
| 105 | 2016 | Dr. Alisha | Gupta | alisha.aiims@gmail.com |
| 106 | 2017 | Dr. Rafey Abdul Rahman | Tasneem Ahmed | rafey123@gmail.com |
| 107 | 2016 | Dr. Abhishek | Ranjan | anujsingh1505@gmail.com |
| 108 | 2017 | Dr. Devendra Soni | Soni | devedbrasibu83@gmail.com |
| 109 | 2017 | Dr. Sreekar | Gundapaneni | mrgsreekar@gmail.com |
| 110 | 2018 | Dr. Abhimanyu | Varshney | drabhimanuu1989@gmail.com |
| 111 | 2017 | Dr. Ravi | Patcharu | ravipatcharu@gmail.com |
| 112 | 2018 | Dr. Abhishek | Gupta | shanky26@gmail.com |
| 113 | 2019 | Dr. Kanika | Sharma | kanika_medico@yahoo.com |
| 114 | 2019 | Dr. Murli | Krishna | krishna.aiims@gmail.com |
| 115 | 2018 | Dr. Divya | Murali | divya.m57@gmail.com |
| 116 | 2019 | Dr. Vivek K Singh | Singh | singhvivec@yahoo.co.in |
| 117 | 2019 | Dr. Varun Kumar | M | drvarunkumar999@gmail.com |
| 119 | 2019 | Dr. Pritesh | Maheshwari | priteshmah@gmail.com |
| 120 | 2019 | Dr. Siddarth | Tyagi | drcsidharth@gmail.com |
| 122 | 2020 | Dr. Sachit | Anand | ravi.sachit@gmail.com |
| 123 | 2020 | Dr. Ruchira | Nandan | ruchira.nandan@gmail.com |
| 124 | 2020 | Dr. Hari | Krishna | krishna.aiims@gmail.com |
| 125 | 2021 | Dr. Teg Rabab Singh | Singh | rabab.aiims@gmail.com |
| 126 | 2020 | Dr. Suramya | Anand | suramya.anand@gmail.com |
| 127 | 2020 | Dr. Saket | Davera | docsak.iaf@gmail.com |
| 128 | 2021 | Dr. Tanvi | Goel | tanvigoel@gmail.com |
| 129 | 2021 | Dr. Shreya | Tomar | shreya305@gmail.com |
| 130 | 2022 | Dr. Ankur | Bhardwaj | ankur.sprout@gmail.com |
| 131 | 2022 | Dr. Dhruv | Mahajan | 280691dhruv@gmail.com |
| 132 | 2022 | Dr. Mehak Sehgal | Sehgal | mehak.sehgal91@gmail.com |
| 133 | 2022 | Dr. Vimalendu | Jha | docvjha@gmail.com |
| 134 | 2022 | Dr. Jadhav | Shishir | Jadhavshishir03@gmail.com |
| 135 | 2023 | Dr. Apoorva | Singh |
20th CONGRESS OF ASIAN ASSOCIATION OF PEDIATRIC SURGEONS with WOFAPS Executive Meeting, Venue: Hotel Taj Palace and Convention center, New Delhi. Website: www.aaps2006.com.
Workshop on Anorectal Malformation (by Prof A. Pena), Venue: AIIMS, New Delhi. Website: www.aaps2006.com.
Pediatric Intensive care (for Nurses), Conference Hall, AIIMS, New Delhi. Venue: AIIMS, New Delhi. Website: www.aaps2006.com.
Workshop on Pediatric Urology (VUR, Intersex and Hypospadias) (Prof Prem Puri, Prof W. Snodgrass, Mr A.Bracka, Prof. John Hutson, Prof Asopa) Venue: AIIMS, New Delhi. Website: www.aaps2006.com.
3rd World Congress of Pediatric surgery, under the auspices of World Federation of Associations of Pediatric Surgeons, New Delhi with Post Congress Live Operative Workshops on Hypospadias & DSD Venue: Hotel Taj Palace, New Delhi. Website: www.pedsurgery.in.
| 1 | Comparative study of smooth muscle cell characteristics and myofibroblasts in processes vaginalis of pediatric hernia, hydrocele and hypospadias |
| 2 | Patient specific three-dimensional printed models of aberrant anatomy for surgical planning of anorectal malformation |
| 3 | Differences in the Microvessel Density and Growth Factors between the inner and outer preputial skin in Distal Hypospadias |
| 4 | Cross-sectional Study to establish a normal reference range (nomogram) for Testosterone and Dihydro-testosterone in boys of age group 0-14 year. |
| 1 | Comparative study of smooth muscle cell characteristics and myofibroblasts in processes vaginalis of pediatric hernia, hydrocele and hypospadias |
| 2 | Patient specific three-dimensional printed models of aberrant anatomy for surgical planning of anorectal malformation |
| 3 | Differences in the Microvessel Density and Growth Factors between the inner and outer preputial skin in Distal Hypospadias |
| 4 | Cross-sectional Study to establish a normal reference range (nomogram) for Testosterone and Dihydro-testosterone in boys of age group 0-14 year. |
| 1 | Comparative study of smooth muscle cell characteristics and myofibroblasts in processes vaginalis of pediatric hernia, hydrocele and hypospadias |
| 2 | Patient specific three-dimensional printed models of aberrant anatomy for surgical planning of anorectal malformation |
| 3 | Differences in the Microvessel Density and Growth Factors between the inner and outer preputial skin in Distal Hypospadias |
| 4 | Cross-sectional Study to establish a normal reference range (nomogram) for Testosterone and Dihydro-testosterone in boys of age group 0-14 year. |
| 5 | Biochemical and enzymatic analysis of bile in choledochal cyst and correlation with histopathological features & expression of immune modulators. |
| 6 | Study of clinical significance of genetic alterations and feasibility of adopting Children Oncology Group (COG) risk stratification of Wilms tumor in Indian Children |
| 7 | Patient specific three-dimensional printed models of aberrant anatomy for surgical planning of anorectal malformation |
| 8 | Cross-sectional Study to establish a normal reference range (nomogram) for Testosterone and Dihydro-testosterone in boys of age group 0-14 year |
| 9 | To Evolve Evidence-Based Hypospadias Repair Guidelines for Hypospadias Repair (Urological Condition) in Indian Context |
| 9 | Development of Technology based Doctor-Patient Interface to Facilitate Patient Care and Health Research in Paediatric Urology |
| 10 | Development of a portable rapidly adjustable camera holding device to minimize image tremor and fatigue of the camera holding assistant during minimally invasive surgery in children |
| 11 | Incidence and severity of psychosocial and somatic disorders in survivors of childhood solid malignant tumors |
| 12 | Role of Urinary Prohibition and other urinary biomarkers levels at diagnosis in children with favorable histology Wilms’s Tumor in predicting tumor response and risk of recurrence |
| 13 | To study the temporal relationship between urinary molecular markers (TFF3, NGAL and Microalbumin) and conventional markers of renal injury to elucidate elicit their relative value as a ‘Point of care’ test during follow-up of patients of bladder exstrophy epispadias complex. |
| 14 | Long term outcomes in BEEC |
| 15 | Normative values of renal length, parenchymal thickness and renal elastography in Indian Pediatric population |
| 16 | H19 long non-coding RNA (lncRNA) and its association with the clinical outcomes in Indian pediatric patients of Wilms tumor |
| 17 | Assessment of Ureteric Jets as a Supportive Diagnostic Modality in Unilateral PUJO and it’s Utility of Follow-up |
| 18 | A comparative study of smooth muscle characteristics and myofibroblasts in Processus vaginalis of pediatric inguinal hernia, hydrocele and undescended testis. |
| 19 | Correlation between hand digit length ratio and severity of hypospadias in pre-pubertal boys in Indian population |
| 20 | Pediatric surgical point of view on achalasia cardia-an observational study. |
| 21 | Compliance to the provisional date of elective surgery allotted to pediatric surgery out-patients of a tertiary-care, public-funded teaching hospital of North India |
| 22 | Differences in the Microvessel Density and Growth Factors between the inner and outer preputial skin in Distal Hypospadias |
| 23 | Long term effects in BEEC |
Clinical services are available in general pediatric surgery with thrust areas in the field of gastro-intestinal surgery, urology, thoracic surgery, plastic surgery, endocrine surgery, neonatal surgery, neurosurgery and oncology.
Facilities for therapeutic and diagnostic endoscopic procedures of the oesophagus, tracheo-bronchial tree and genito-urinary tract are also available.
The department has the following laboratory facilities :
The department has admitting facilities for 35 children in the 6B Ward Pediatric Surgery in Mother and Child Block, 8 neonatal surgical cases in the neonatal surgical ICU (AB-5 ICU) and 4 Emergency beds in Paediatric Surgery (AB-5 Ward). The neonatal surgical ICU is fully equipped with vital signs monitors, conventional neonatal ventilators, high frequency ventilator and other necessary equipment for neonatal care. One senior resident and a junior resident are available round the clock in the ward and one senior resident in the neonatal ICU for patient care and emergency services.
The facilities for routine pre-operative and post-operative care of surgical patients, ventilatory care, parenteral nutrition and chemotherapy are provided by the resident staff. Due to the shortage of staff and the indoor beds, most of the time, only the serious and indexed cases find admissions in the ward. The waiting list is long and may run for years.
The department conducts 2 OTs per day in main Operating Theatre (2 nd Floor – Mother and Child Block). In addition, conducts operations at the extension center in Ballabgarh on Wednesdays.
The department is a training center for pediatric surgery towards the degree of M.Ch.(Pediatric Surgery) which is recognized by the Medical Council of India (MCI). Surgical training is conducted in the fields of pediatric gastro-intestinal surgery, urology, thoracic surgery, plastic surgery, endocrine surgery, neonatal surgery, neurosurgery, minimal access surgery, oncology, therapeutic and diagnostic endoscopic procedures of the oesophagus, tracheo-bronchial tree and genito-urinary tract.
There are two kinds of training programmes being conducted in the department. A 3-year course and a 6-year course. During both these courses the candidate has to work on and submit two dissertations (one clinical and one experimental) towards partial fulfillment for the degree of M.Ch.
For the 3-year course a candidate has to have a MS in General Surgery (MCI recognized) and the enrollment is vacancy based through a competitive examination conducted by AIIMS for DM/MCh courses. Selected candidates for the 3-year course are treated as academic senior residents during their tenure and they are eligible to take the M.Ch. examination at the end of three years.
For the 6-year comprehensive course the candidate has to have an M.B.B.S degree (MCI recognized) and two candidates are enrolled every year in January and July through the AIIMS PG entrance examination. In the 6-year course, for the first three years the candidate is a junior resident while in the remaining 3 years he/she is an academic senior resident. In this course the candidate is eligible to take the M.Ch. examination at the end of five years but the sixth year is compulsory and is treated as senior residency. During the three years of junior residency of the 6-year course the candidate has to successfully complete 6 months in pediatric surgery and 1-year rotation in allied specialties (9 months general surgery, 2 months orthopedic surgery and 1 month neurosurgery) before he/she is allowed to continue with the course. In addition in both the courses the candidates have to successfully complete 2 months of rotation posting in pediatrics.
In addition to the above seats, the department has provision to admit three sponsored candidates - those sponsored by state health services, armed forces etc. At any given time the department has a maximum strength of 9 senior residents and three junior residents. Further, the department also trains junior residents on rotation from M.S. general surgery and M.Ch. neurosurgery courses and senior residents from the D.M. neonatology course. Observers and trainees from other pediatric surgical departments from India and abroad also visit the department for varying periods after obtaining the due permission from the academic section, AIIMS.
The faculty of the department takes regular instructional lectures for M.B.B.S. and B.Sc. (Nursing) students and participates in guest lectures, CME’s and symposia conducted by other scientific organizations and institutions in India and abroad. From time to time the department organizes guest lectures, symposia, seminars and live operative workshops, as a part of ongoing CME programmes.
The Department of Paediatric Surgery was created as an independent Department in 1969 with Dr. P.upadhyaya as the first Head of Department. Thereafter the department was headed by Prof. M. Rohatgi (1987-1993) and then Prof. D.K.Mitra (1993-2004). The current Head of the Department, Prof. M. Bajpai took charge in 2018. Under his leadership, Dr. Vishesh Jain, Dr. Prapudh Goel, Dr. Anjan Dhua and Dr. Devendra Kumar Yadav have joined the Department as Assistant Professors in 2014 and are currently working in the capacity of Additional Professors. Dr. Ajay Verma in 2020, Dr. Sachit Anand and Dr. Divya Gali in 2023 are the youngest to join the ranks of faculty and are holding the post of Assistant Professor.
It is first time in the history of AIIMS, New Delhi that the top most positions occupied by the faculty members of the Department of Paediatric Surgery i.e. Director of AIIMS, New Delhi is Prof. M. Srinivas and Dean (Academic) is Prof. M. Bajpai.
Under the leadership and guidance of Prof. M. Bajpai, the Department of Paediatric Surgery has been shifted to the Mother and Child Block during 2022 and started functioning. The Paediatric Surgery OPD is located on the Ground Floor, the Operation Theatres are located on the 2nd Floor, Wards are located on 6th Floor B Wing and Department’s administrative offices are located on “7th Floor of the Mother and Child Block.
The department has been on the forefront and is rated as one of the finest departments not only in the country but at the international level for its quality patient care, teaching, training and research. The Department established a state-of-the-art neonatal intensive care unit exclusively for the surgical newborns, for the first time in the country. The department has contributed significantly in promoting the development of paediatric surgery at the national and international level and is regularly represented in the national and international associations and various societies, projecting the current status and the contribution in the field of paediatric surgery from this major teaching institution.
It is a pleasant task to recall the history of the department and take pride in its achievements. However as in everyday life, difficult moments did creep in and in overcoming these, we believe we have emerged stronger after each such episode.
It was in 1968, that Dr.P.Upadhyaya, then Associate Professor of Surgery, returned after availing a WHO fellowship in Paediatric Surgery and took charge of the Paediatric Surgery unit within the department of General Surgery at AIIMS.
It was on 29th March 1971, that the umbilical cord was finally severed and the Department of Paediatric Surgery came on its own with Dr.Upadhyaya as its first head. It was a humble beginning with 24 beds earmarked within the surgical ward and two registrars - Dr.L.K.Sharma and Dr.R.K.Kashyap. Dr.M.Rohatgi joined the department in May 1970 as Assistant Professor, the faculty strength of the department has gradually increased to six with the joining of Dr.D.K.Mitra (1976), Dr.D.K.Gupta (1985), Dr.V.Bhatnagar (1986), Dr.M.Bajpai (1988), Dr.S.Agarwala (1994), Dr.M.Srinivas (1999), Dr Shilpa Sharma (2012). Dr V Jain (2014), Dr P Goel (2014), Dr A Dhua (2014) and Dr D K Yadav (2014). Thereafter, three more new faculty members namely Dr. A Verma (2020), Dr. Sachit Anand and Dr. Divya Gali in 2023 in the capacity of Assistant professor, the department strength stands at 11 faculty members. The Department of Paediatric Surgery has been shifted to Mother and Child Block.
Dr.P.Upadhyaya became the first professor in 1976 and was the head of the department till his retirement in 1987. From this time onwards Dr. M.Rohatgi was the head till her untimely demise in January 1993 in a train accident. Prof. D.K.Mitra, took over as the Head of the Department in 1993 and superannuated in December 2004. Prof. D. K. Gupta and Prof. V. Bhatnagar held the post as the head in 2018. Prof. M. Bajpai took over the reigns as the Head of the Department from December 2018.
The first M.Ch. trainee, Dr. S.Chooramani was selected in July 1972 and has been bestowed with the honourable Padamshree award in 2011. Since then,107 M.Ch. trainees and 1 PhD student have been groomed into holding responsible teaching positions in the country and abroad. Due to ever increasing clinical and research workload, the strength of the senior residents was increased from two to four in 1979, to six in 1982 and again to nine in 1994. Currently our department has an intake capacity of 15 Senior Residents.The six years' integrated M.Ch. course in Pediatric Surgery (after MBBS) was launched in the Department in July 1979 and it continues till date. In addition, the department also trains post-graduates in general surgery, paediatrics and neurosurgery for 2-12 weeks making them aware of the common paediatric surgical problems and their management. The Department frequently receives postgraduate students in Pediatric surgery from different centres in the country for 4-12 weeks to obtain exposure in neonatal surgical techniques and post-operative care.
Experimental work including animal experiments forms an integral part of the M.Ch. training, besides the routine clinical project. Original experimental work has been carried out in the field of splenic conservation, CSF shunts, embryo-toxic factors in congenital malformations, duplication cysts, metabolic responses to surgery, biliary atresia,intersex disorders, paediatric urological problems, intestinal atresia, oesophageal atresia, to name a few. The Department has two laparoscopic Endo trainers. Many innovations made in the department are being utilized in day-to-day practice for the benefit of the patients.
In April 1993 the department received a jolt when a fire consumed the department’s offices and laboratory destroying precious records and equipment. What we see today is the department rebuilt after such a colossal loss.
The paediatric surgical ward was trans-located to its present position on 5th floor (AB-5 wing) in the year 1969, and has now strength of 40 beds. The neonatal surgical intensive care unit (NSICU) was upgraded in 2000 to accommodate 8 neonates and in 2009 to accommodate 10 neonates and a separate feeding area for the mothers. The NSICU is equipped with state-of-the-art life support systems for each new-born (ventilator, monitors, infusion pumps, humidifier, photo-therapy machine, blood gas analyser and others).
The department has been receiving support from the associate departments like anaesthesiology, nuclear medicine, radiology, pathology, oncology and neonatology at odd hours. The department has also been extending the specialized services and running the afternoon clinics in the field of hydrocephalus, paediatric urology, oncology, intersex disorders and antenatal diagnosis and management. A follow-up clinic has also been started to manage the surgical newborns with antenatally detected malformations efficiently.
Blood gas analyser and four channel recorders were installed in the ward way back in 1972, and now have been upgraded. The Urodynamic machine serves both the clinical as well as the research purposes. Micro-analyser and multi-channel monitoring system have been added recently. The ward now has a special care area equipped with the latest monitoring equipment, ventilators, intra-cranial pressure monitoring device, and facility for uroflowmetry and ano-rectal manometry. Oesophageal pH and manometry have also been recently added. The Department has also acquired a Doppler ultrasound machine to meet the requirements of the neonates and children with various types of disorders.
In 1975, the first neonatal surgical ICU, in India, was established at the AIIMS. This was initially located in separate cubicles at one end of the children’s surgical ward. However, its limitations were realized and in 1979 it was shifted to a separate area with its own air-conditioning, air filtration plant, and temperature and humidity control, with a capacity of 7 neonates and this was partially equipped under the Colombo plan by the British Government. Due to the ever-increasing workload at this institute, the neonatal surgical ICU has now been expanded to accommodate ten newborns. It has been completely renovated and freshly equipped with state of art incubators, open infant care systems, portable incubators, neonatal ventilators, multi-function monitors, electronic weighing scale for the newborns, humidifiers, syringe pumps and slow suction machines.
From its inception the department has tried to take care of all surgical needs of children. The Upadhyaya shunt was the first of its kind in India, manufactured using an indigenously developed valve in the department. The department has acquired fame and status as a centre of excellence in the field of neonatal surgery, paediatric neurosurgery, thoracic surgery, plastic surgery, gastro-intestinal surgery, hepatobiliary surgery, urologic surgery, onco-surgery and endoscopic surgery. However, the Department of Pediatric Surgery is only a part of this premier major institution and hence we face the limitation of the number of available beds and the operating time to us, forcing patients to be on the waiting list for months for routine and reconstructive surgery.
At the national level, the department of paediatric surgery at this institute has made significant contributions to the development of Pediatric Surgery. The first ever national gathering of the country’s Pediatric Surgeons took place in 1976 during the 1st WHO/NAMS sponsored National Seminar on Pediatric Surgery at AIIMS. The recommendations of the seminar formed the blue print for the evolution of paediatric surgery. A follow-up on this was made during the 2nd WHO/NAMS National Seminar on Pediatric Surgery in 1982 at AIIMS.
The department hosted the first International Workshop on Neonatal Surgery in 1980. Since then, the department has been holding various workshops, symposia, conferences and other teaching courses each year. Over 50 such conferences have already been organized by the department in the field of paediatric thoracic surgery, pancreatic and hepatobiliary surgery, vascular malformations, oesophageal surgery, paediatric urology and intersex disorders, inviting each time distinguished faculty members from India and abroad. The department also hosted workshops and seminars for the training of nurses in neonatal intensive care, knot tying, staplers, suture practicum and neonatal resuscitation. International Workshop on Hypospadias and Intersex Disorders in 1999, International Workshop on Neonatal Surgery in the year 2000 and recently the International Workshop on Neurogenic bladder and the Hypospadias in 2001 have been very well attended by delegates not only from various parts of India but overseas also. All these have proved to be very educative and informative. The 3rd World Congress on Pediatric Oesophagus including Prevention and Treatment of Caustic Oesophageal Burns & Live Operative Workshop on Oesophageal Surgery (February 1-3, 2002) organized by the Department is another feather in its cap in the field of education. The Biennial Asian Association of Pediatric Surgeons was organized in August 2006 and had about 660 delegates from 80 countries. The 3rd World Congress of Pediatric Surgery along with the 36th Annual National Conference of Indian Association of Pediatric Surgeons, 21-24 October, 2010 was organized by the department as a landmark congress in the speciality including delegates from 93 countries. This was associated with 3 major workshops, the Pre congress course on Minimally Invasive surgery, 21 October 2010, Pre congress course on Anorectal Malformations, 21 October 2010 and Live Operative Workshop on Hypospadias and DSD, 25-26 October 2010.
This was shortly followed by the Symposium on Pediatric Uro-oncology in association with the Indian Society of Pediatric Urology, from December 3-4, 2010. An International workshop cum Symposium on Pediatric Urology and Annual Conference of Delhi Chapter of IAPS and Pediatric Urology Chapter of IAPS was organized from 29-31 August, 2013. A Public Awareness Program on Hernia in Children was organized on 7th September 2013 AIIMS, New Delhi.
The Department regularly holds meetings of the of the Delhi chapter of IAPS, New Delhi, Past and present members of the Department have received many prestigious awards and honours. The faculty members have served not only the National Association with flying colours but have also been nominated uncontested to the Asian Association and the World federation of Association of Pediatric Surgeons. The faculty members are constantly updating their knowledge by participating in the national and the international conferences. They have also visited centres of excellence in Pediatric Surgery the world over through various fellowships and scholarships.
The Department has also been conducting biennial meets under the Aegis of Indian Society of Paediatric Urology and Asian Society of Paediatric Urology. These meetings are focused group discussions and symposiums on the current and updated topics of paediatric urology with involvement of internationally acclaimed faculties.
1. To offer the best possible care to the surgical neonate and child
2. To train the students and nurses in the field of Pediatric Surgery
3. To establish guidelines on how a particular problem should be solved in the Indian setting
4. To carry out research in the specialty under ethical and scientific guidelines
5. To serve as a role model for ideal paediatric surgical practice
The Department of Pediatric Surgery at AIIMS offers State-of-the-art patient care, not only in General Pediatric Surgery, but also in the field of Neonatal surgery, Pediatric Urology including Disorders of Sexual Differentiation, Thoracic surgery, Oncology, Gastrointestinal Surgery, Laparoscopy, Endoscopy (Bronchoscopy, Esophagoscopy and Cystoscopy) and Neurosurgery in children up to 14 years of age.
The Department has several follow-up clinics including antenatal counselling for congenital malformations and follow-up of the cases till they reach adolescence and even after adulthood in some selected cases where meticulous surgery is required. The Department has daily outpatient services and follow up clinics in the mornings and afternoons.
Currently (July 2022), there are seventeen trainees (3-year M.Ch. students and 6-yr M.Ch.) including 13 senior and 4 junior residents in the Department. Apart from these, there are regular student on rotations from General Surgery, Neonatology and Neurosurgery to learn the basics of the speciality. There is a stringent academic training program with regular morning classes from 8-9 am daily before the routine clinical work starts.
Many alumni of the Department are presently holding key faculty positions (Principal of the Medical College, Heads of the Departments in India and Consultant Pediatric surgeons) in various paediatric surgical centres in India and abroad and making us proud.
The Department has made remarkable strides in the past and continues to work hard for excellence in patient care, clinical and experimental research, and post-doctoral teaching and training the residents. We remain committed to continue this tradition to the best of our ability and dedication, and hopefully prove up to the expectations of the public at large.
With the new Mother and Child Block coming up, the department is all set to expand the horizon in terms of the care provided and research conducted.
Willis Potts - one of the pioneers of paediatric surgery in North America, highlighting these very principles from the preface of his book "Surgeon and the Child" published in 1959 - dedicating it to the new born baby who has the great misfortune of being born with a serious deformity saying that "if this baby could speak, it would beg imploringly of the Surgeon, please exercise the greatest gentleness with my miniature tissues and try to correct the deformity at the first operation. Give me blood and the proper amount of fluid and electrolytes; and plenty of oxygen to the anaesthesia and I will show that I can tolerate terrific amount of surgery. You will be surprised at the speed of my recovery and I shall be always grateful to you."
The paediatric surgical patient requires tender care with delicate skills and diligent follow up as the new-born, baby or toddler grows through adolescence into a mature adult. As paediatric surgeons we learn from the little kids daily and are grateful to them for giving us the opportunity to serve them.
| NAME | MONTH AND YEAR OF JOINING | MONTH AND YEAR OF PASSING | CHIEF GUIDE |
|---|---|---|---|
| Dr. Madhav Gajanan Deo | January 1958 | May 1960 | Prof.V.Ramalingaswami |
| Dr. Amrit Lal Aurora | January 1959 | May 1961 | Prof.V.Ramalingaswami |
| Dr. T.V.Madhavan | July 1959 | December 1961 | Prof.V.Ramalingaswami |
| Dr. S.K.Sood | July 1959 | May 1962 | Prof.V.Ramalingaswami |
| Dr. Hardhan Roy | July 1959 | May 1962 | Prof.V.Ramalingaswami |
| Dr. Subimal Roy | July 1959 | December 1962 | Prof.V.Ramalingaswami |
| Dr. Muneshwar S.Ahluwalia | July 1960 | December 1962 | Prof. H.D. Tandon |
| Dr. Nirmala Krishnan | July 1959 | May 1963 | Prof.V.Ramalingaswami |
| Dr. Kulwant Duggal (Jolly) | July 1959 | December 1963 | Prof. H.D. Tandon |
| Dr. Meera Ahuja (Dhawan) | January 1963 | December 1964 | |
| Dr. Sushila Chauhan | July 1962 | May 1965 | Prof.V.Ramalingaswami |
| Dr. C.A. Lakshmi Narayan | July 1962 | May 1965 | |
| Dr. K.Janardan Reddy | July 1963 | May 1965 | Prof. H.D. Tandon |
| Dr. Gurdip Singh Sidhu | July 1962 | May 1965 | |
| Dr. Luna Banerji | January 1963 | December 1965 | Prof.V.Ramalingaswami |
| Dr. Prabodh Kumar Gupta | July 1962 | December 1965 | Prof. H.D. Tandon |
| Dr. Banarasi Dass Sabbarwal | July 1962 | December 1965 | Prof.V.Ramalingaswami |
| Dr. U.N.Bhuyan | July 1963 | May 1966 | Prof.V.Ramalingaswami |
| Dr. Puja Kapoor (Kala) | July 1963 | May 1966 | Prof. H.D. Tandon |
| Dr. A.J. Veliath | January 1964 | December 1966 | Prof.V.Ramalingaswami |
| Dr. Meera Mathur | January 1964 | May 1966 | Prof.V.Ramalingaswami |
| Dr. Dinyar Bhathena | July 1965 | May 1967 | Prof. N.C. Nayak |
| Dr. Yogeshwar Dayal | July 1964 | December 1967 | Prof. M.G. Deo |
| Dr. Jaya Kasturi | January 1966 | May 1969 | Prof. H.D. Tandon |
| Dr. Atul Kumar Bhan | January 1967 | December 1969 | Prof. M.G. Deo |
| Dr. Ina Dhanda | January 1967 | December 1969 | Prof.V.Ramalingaswami |
| Dr. Indira Nath | January 1967 | December 1969 | Prof. N.C. Nayak |
| Dr. Kusum Verma (Anand) | January 1967 | December 1969 | Prof.V.Ramalingaswami |
| Dr. Prem Chopra | January 1968 | December 1970 | Prof. N.C. Nayak |
| Dr. T.S. Shylaja | January 1968 | May 1971 | Prof. H.D. Tandon |
| Dr. Ranendra Nath Basu | July 1968 | December 1971 | Prof. S.K.Sood |
| Dr. Vinay Kumar | January 1969 | December 1971 | Prof. M.G. Deo |
| Dr. Kamaraju Suguna Ratnakar | July 1969 | May 1972 | Prof. M.G. Deo |
| Dr. Jag Bhawan | January 1970 | December 1972 | Prof. Subimal Roy |
| Dr. Uma Sethi | July 1969 | December 1972 | Prof. H.D. Tandon |
| Dr. Prasanta Kumar Das | July 1970 | May 1973 | Prof. N.C. Nayak |
| Dr. Jag Pal Singh Suri | July 1970 | May 1973 | Prof. M.Mathur |
| Dr. Sarla Rani Agarwal | January 1971 | January 1975 | Prof. S.K. Sood |
| Dr. S.K.Shankar | July 1971 | January 1975 | Prof. M.G. Deo |
| Dr. Aruna Sud | July 1972 | May 1975 | Prof. H. D. Tandon |
| Dr. R.N.Visveswara | July 1972 | May 1975 | Prof. H.D. Tandon |
| Dr. Veena Singhal | July 1972 | May 1975 | Prof. S.K. Sood |
| Dr. Indra Mital | January 1973 | December 1975 | Prof. N.C. Nayak |
| Dr. Kusum Joshi | January 1973 | December 1975 | Prof. M.G. Deo |
| Dr. Arati Bhatia | July 1974 | May 1976 | No Thesis |
| Dr. C.D. Sasi Kumar (Major) | July 1974 | May 1976 | --do— |
| Dr. K.P.P.Rao | July 1973 | December 1976 | --do— |
| Dr. Asha Dhar | July 1973 | December 1976 | Prof. N.C. Nayak |
| Dr. Goculdas Rajaram Bhangui | February 1975 | December 1976 | No thesis |
| Dr. H.G. Shrestha | March 1975 | May 1977 | --do— |
| Dr. Ramesh Chopra | July 1973 | May 1977 | Dr.K.Verma |
| Dr. Shakti Ghai | July 1973 | May 1977 | Dr.K.Verma |
| Dr. Bharat Bhushan Sharma | July 1975 | May 1977 | No Thesis |
| Dr. M.Baqui Rostaiy | July 1975 | December 1977 | --do— |
| Dr. Najibullah Fraidon | July 1975 | May 1977 | --do— |
| Dr. Ashok Mukherjee | July 1975 | May 1977 | --do— |
| Dr. Paramjit Singh Bhatia | June 1975 | December 1977 | --do— |
| Dr. Sant Lal Jain | July 1975 | December 1977 | --do— |
| Dr. Kasturi Narasimham | January 1976 | December 1977 | --do— |
| Dr. Asha Chug | July 1976 | May 1978 | --do— |
| Dr. Pramod Kumar Rath | July 1976 | May 1978 | --do— |
| Dr. Kusum Angrish | January 1977 | December 1978 | --do— |
| Dr. Malini Vijayaraghavan | January 1977 | December 1978 | --do— |
| Dr. S.Sandhyamani | January 1977 | December 1978 | --do— |
| Dr. Subhash Chander Sharma | July 1977 | May 1979 | --do— |
| Dr. Geeta Ashok Raj (Mohan) | July 1977 | May 1979 | No thesis |
| Dr. C.Chandrasekharan Kartha | July 1977 | May 1979 | --do— |
| Dr. Mridula Gami (Thakur) | July 1977 | May 1979 | --do— |
| Dr. Mira Mohanty | January 1978 | December 1979 | --do— |
| Dr. Priti Kapoor | January 1978 | December 1979 | --do— |
| Dr. Nalini Lal Ahluwalia | July 1978 | December 1979 | --do— |
| Dr. Mrinalini Honavar | July 1978 | July 1980 | --do— |
| Dr. Neelam Marwaha (Bhanot) | January 1978 | December 1980 | Prof. N.C. Nayak |
| Dr. Surender Kumar Juneja | January 1978 | December 1980 | Prof. H.D. Tandon |
| Dr. Rajeev Kumar | July 1978 | May 1981 | Prof. U.N. Bhuyan |
| Dr. Chitra Chowdhury | July 1978 | May 1981 | Prof. Subimal Roy |
| Dr. S.K. Panda | January 1979 | December 1981 | Prof. N.C. Nayak |
| Dr. Ashok Kumar Mukhopadhya | January 1979 | December 1981 | Prof. Subimal Roy |
| Dr. Manoj Kumar Singh | July 1979 | May 1982 | Prof. U.N. Bhuyan |
| Dr. Hari Prasad Pati | July 1979 | May 1982 | Prof. K.Verma |
| Dr. Renu Saxena | January 1980 | December 1982 | Prof. Meera Mathur |
| Dr. K.P. Arvindan | January 1980 | December 1982 | Prof. U.N. Bhuyan |
| Dr. S.Iralu | Prof. A.K. Saraya | ||
| Dr. Paramajit Singh Randhawa | July 1980 | May 1983 | Prof. H.D. Tandon |
| Dr. Ashish Kumar Mandal | July 1980 | December 1983 | Prof. A.K. Saraya |
| Dr. Siddhartha Datta Gupta | January 1981 | December 1983 | Prof. N.C. Nayak |
| Dr. Vinita Agarwal | January 1981 | December 1983 | Prof. H.D. Tandon |
| Dr. Lalita Murthy | July 1981 | June 1984 | Prof. K.Verma |
| Dr. Asis Kumar Karak | July 1981 | May 1984 | Prof. Meera Mathur |
| Dr. Susheila Maiya Dali | July 1981 | June 1984 | Dr.N.C. Nayak |
| Dr. Neelam Dhingra | January 1982 | December 1984 | Prof. K.Verma |
| Dr. Krishna Govind Badami | July 1982 | May 1985 | Prof. A.K.Saraya |
| Dr. Mala Gupta | August 1982 | December 1985 | Prof. P.Chopra |
| Dr. Satish Kumar Tickoo | January 1983 | December 1985 | Dr.M.Bhargava |
| Dr. Neeta Kumar | July 1983 | June 1986 | |
| Dr. Amit Kumar Dinda | July 1983 | June 1986 | Prof. A.K. Saraya |
| Dr. Shikha Bose | July 1983 | May 1986 | Prof. N.C. Nayak |
| Dr. Maheswar Sahoo | July 1983 | May 1986 | Dr.K.Kapila |
| Dr. Anil Kumar Khemani | January 1984 | May 1987 | Prof.K.Verma |
| Dr. Harminder Singh | January 1984 | May 1987 | |
| Dr. Shobha Sharma | January 1985 | December 1987 | |
| Dr. A.Raja Sekhar | July 1985 | May 1988 | Prof. K.Verma |
| Dr. Sunita | January 1986 | December 1988 | |
| Dr. Yashwant Singh | January 1986 | December 1988 | Prof.S.Roy |
| Dr. Rajiv Dhir | July 1986 | May 1989 | Prof. K.Verma |
| Dr. Yogesh Verma | July 1986 | May 1989 | |
| Dr. Samir Ranjan Bhowmik | July 1986 | December 1989 | Dr.U.N. Bhuyan |
| Dr. Angeli Misra | July 1986 | December 1989 | Prof. P.Chopra |
| Dr. Arakeri Vani Rao | January 1988 | December 1990 | Prof. K.Verma |
| Dr. R.Leelavathi | July 1988 | May 1991 | Prof. P.Chopra |
| Dr. Uttara Bagchi | July 1988 | May 1991 | |
| Dr. Suash Sharma | July 1989 | May 1992 | Dr.C.Sarkar |
| Dr. Baljit Singh | July 1989 | May 1992 | |
| Dr. Makarla Bharani Prakash | July 1989 | May 1992 | Prof. K.Kapila |
| Dr. Dibesh Pal | January 1989 | May 1992 | Prof. Meera Mathur |
| Dr. Nidhi Jindal | January 1990 | December 1992 | Prof. P.Chopra |
| Dr. Jobina Wanniang | January 1990 | May 1993 | Prof. P.Chopra |
| Dr. Prakash Kumar Pradhan | July 1990 | May 1993 | Dr.M.K.Singh |
| Dr. Subhash Chander | January 1990 | May 1993 | Prof. P.Chopra |
| Dr. Rohini Sridhar | July 1990 | May 1993 | Prof. K.Verma |
| Dr. Eric Zomawea Colbert | July 1990 | December 1993 | Prof. M.Mathur |
| Dr. Vikram Deshpande | July 1991 | May 1994 | Prof. K.Verma |
| Dr. Anita Deshpande (Gambhir) | July 1991 | December 1994 | Prof. P.Chopra |
| Dr. K.Venkateswaran | January 1992 | December 1994 | Prof. R.Dawar |
| Dr. Sumeet Gujral | January 1992 | May 1995 | Dr.M.K.Singh |
| Dr. Seema G.Kashyap | July 1992 | May 1995 | Prof. K.Verma |
| Dr. Neena Verma | July 1992 | May 1995 | Dr.S.Datta Gupta |
| Dr. Selina Bhattarai | July 1992 | May 1995 | Prof. R.Dawar |
| Dr. Chetna Taneja | January 1993 | December 1995 | Prof. R.Dawar |
| Dr. Manju Nair | January 1993 | December 1995 | Dr.M.K. Singh |
| Dr. Amarnath Thakur | January 1993 | December 1995 | Dr.M.Vijayaraghavan |
| Dr. Sunati Sahoo | July 1993 | May 1996 | Prof.M.Mathur |
| Dr. Chanda Sharma | July 1993 | May 1996 | Dr.A.K.Dinda |
| Dr. Dilip Kumar | July 1993 | December 1996 | Dr.M.Vijayaraghavan |
| Dr. Shatrughan Prasad Sah | July 1993 | December 1996 | Dr.R.Dawar |
| Dr. Akhilesh Singh Karan | January 1994 | December 1996 | Dr.S.Datta Gupta |
| Dr. Minal B.Kanase | January 1994 | May 1997 | Prof.P.Chopra |
| Dr. Partha Manas Das | July 1994 | December 1997 | Dr.S.Datta Gupta |
| Dr. Puneet Taneja | January 1995 | December 1997 | Dr.S.Datta Gupta |
| Dr. Saroj Goel | Sept. 1995 | May 1998 | Dr.R.Dawar |
| Dr. Nandita Majumdar | July 1995 | May 1998 | Prof.P.Chopra |
| Dr. Rendemo Shitiri | March 1996 | May 1999 | Dr.A.K.Dinda |
| Dr. Arvind Kumar Sinha | November 1996 | December 1999 | Dr.M.K.Singh |
| Dr. Abhijit Datta | September 1996 | December 1999 | Dr.A.K.Dinda |
| Dr. Gautam Bandyopadhyay | October 1996 | December 1999 | Dr.S.Datta Gupta |
| Dr. Pulakesh Pramanik | February 1997 | December 1999 | Dr.C.Sarkar |
| Dr. Nimisha Gupta | March 1997 | December 1999 | Dr.A.K.Karak |
| Dr. I.Satish Rao | July 1997 | May 2000 | Dr.M.K.Singh |
| Dr. AASR Mannan | January 1998 | December 2000 | Dr.M.K.Singh |
| Dr. N.Gopendro Singh | January 1998 | May 2001 | Dr.A.K.Dinda |
| Dr. Angela Mercy Ralte | May 1998 | May 2001 | Dr.C.Sarkar |
| Dr. Anurag Dhakar | July 1998 | June 1999 | |
| Dr. Sanjay Mukhopadhyay | January 1999 | December 2001 | Dr.S.Datta Gupta |
| Dr. Anupma Nayak | January1999 | December 2001 | Dr.C.Sarkar |
| Dr. Surinder Kumar Attri | July 1999 | December 2002 | Dr.C.Sarkar |
| Dr. Bal Chander | July 1999 | May 2002 | Dr.A.K.Dinda |
| Dr. Anup Kumar Das | January 2000 | December 2002 | Dr.Kusum Verma |
| Dr. Epari Sridhar | January 2000 | December 2002 | Dr.Ruma Ray |
| Dr. Anuradha De | July 2000 | Dr A K Dinda | |
| Dr. Niharendu Ghara | July 2000 | May 2003 | Dr.M.C.Sharma |
| Dr. Amrish Kamboj | July 2000 | May 2003 | Dr.A.K.Dinda |
| Dr. Shupriyo Chaudhary | July 2000 | Dr A K Karak | |
| Dr. Aruna K Minz | January 2001 | December 2003 | Dr Manoj K Singh |
| Dr. Manu Kukreja | January 2001 | December 2003 | Dr M C Sharma |
| Dr. Asit Ranjan Mridha | July 2001 | May 204 | Dr A K Dinda |
| Dr. Payal Srivastava | January 2002 | Dr A K Karak | |
| Dr. S.S. Bhatti | January 2002 | Dr R Dawar | |
| Dr. Nidhi Aggarwal | July 2002 | Dr M K Singh | |
| Dr. Arvind Rishi | July 2002 | Dr M C Sharma | |
| Dr. Shree Gopal Sharma | July 2002 | Dr A K Dinda | |
| Dr. Kamlesh Kumar | January 2003 | Dr Kusum Verma | |
| Dr. Kamaljet Singh | July 2003 | Dr A K Dinda | |
| Dr. Anand Rajan | July 2003 | Dr S K Panda | |
| Dr. Shipra Aggarwal | January 2004 | Dr V K Iyer | |
| Dr. Anita Chopra | July 2004 | Dr V K Iyer | |
| Dr. Ayushi Jain | July 2004 | Dr M C Sharma | |
| Dr. Nadeem Tanveer | January 2005 | Dr M C Sharma | |
| Dr. R. Kanchana | July 2005 | Dr Manju Aron | |
| Dr. R. Ashok Kumar | July 2005 | Dr A K Dinda | |
| Dr. Kalyani Kulkarni | July 2005 | Dr S K Panda | |
| Dr. Santosh Kumar | January 2006 | Dr M K Singh | |
| Dr. Kishore Gopal Banerjee | July 2006 | Dr A K Dinda | |
| Dr. Charu Chandra Saxena | July 2006 | Dr Rajni Safaya | |
| Dr. Bhaskar Shukla | July 2006 | Dr C Sarkar | |
| Dr. Elanthendral | July 2006 | Dr V K Iyer | |
| Dr. Priti | July 2006 | Dr Sandeep Mathur | |
| Dr. Kiran CS | January 2007 | December 2009 | Dr C Sarkar |
| Dr. Ranajoy Ghosh | January 2007 | December 2009 | Dr A K Dinda |
| Dr. Prashant Durgapal | July 2007 | June 2010 | Dr Sandeep Mathur |
| Dr. Sanjeev Chitragar | July 2007 | June 2010 | Dr V K Iyer |
| Dr. Aanchal Kakkar | January 2008 | December 2010 | Dr V Suri |
| Dr. Saumya Mallick | January 2008 | December 2010 | Dr M K Singh |
| Dr. A Satish Selva Kumar | January 2008 | December 2010 | Dr Ruma Ray |
| Dr. Savit B Prabhu | January 2008 | December 2010 | Dr S K Panda |
| Dr. Monika Breta | July 2008 | June 2011 | Dr M K Singh |
| Dr. Lavleen Singh | July 2008 | June 2011 | Dr A K Dinda |
| Dr. Maneesh Kumar Vijay | July 2008 | June 2011 | Dr Sandeep Mathur |
| Dr. Prashant Pranesh Joshi | January 2009 | December 2011 | Dr M C Sharma |
| Dr. Ashok Singh | July 2009 | May 2012 | Dr M C Sharma |
| Dr. Shwetha Kamath | July 2009 | May 2012 | Dr A K Karak |
| Dr. Suvendu Purkait | July 2009 | May 2012 | Dr C Sarkar |
| Dr. Reena Mittal | July 2009 | May 2012 | Dr S Datta Gupta |
| Dr. Binny Khandakar | July 2009 | May 2012 | Dr Sandeep Mathur |
| Dr. Shubhra Jain | January 2010 | Dec. 2012 | Dr M K Singh |
| Dr. Taher H Chharchoodawala | January 2010 | Dec. 2012 | Dr M C Sharma |
| Dr. Abhijit Das | July 2010 | May 2013 | Dr Sandeep Mathur |
| Dr. Rakesh Kumar Deepak | July 2010 | May 2013 | Dr Rajni Safaya |
| Dr. Sawan Kumar | July 2010 | May 2013 | Dr V Suri |
| Dr. Rakesh Kumar Gupta | July 2010 | May 2013 | Dr M C Sharma |
| Dr. Partheeban Balasundaram | July 2010 | May 2013 | Dr M K Singh |
| Dr. Sawan Kumar | July 2010 | May 2013 | Dr Vaishali Suri |
| Dr. Ramtake Prashant P. Singh | Jan 2011 | Dec. 2013 | Dr Sandeep Mathur |
| Dr. Archana George Vallonthaiel | Jan 2011 | Dec. 2013 | Dr Manoj Kumar Singh |
| Dr. Immanuel Pradeep J.N. | Jan 2011 | Dec. 2013 | Dr AK Dinda |
| Dr. Aruna Nambirajan | Jan 2011 | Dec. 2013 | Dr Mehar Chand Sharma |
| Dr. Kavneet Kaur | July 2011 | May 2014 | Dr Chitra Sarkar |
| Dr. Kalpana Kumari | July 2011 | May 2014 | Dr Mehar Chand Sharma |
| Dr. Maikal Kuijur | July 2011 | May 2014 | Dr Venkat K Iyer |
| Dr. Ranjit Kumar | Jan. 2012 | Dec. 2014 | Dr AK Dinda |
| Dr. Bhavna Sharma | July 2012 | May 2015 | Dr Manoj Kumar Singh |
| Dr. Parul Jain | July 2012 | May 2015 | |
| Dr. Brijnandan Gupta | July 2012 | May 2015 | Dr Siddharth Dutta Gupta |
| Dr. Manish Singh | July 2012 | May 2015 | |
| Dr. Tripti Nakra | July 2012 | May 2015 | Dr Sandeep Mathur |
| Dr. Madhu Rajeshwari S. | July 2012 | May 2015 | Dr Mehar Chand Sharma |
| Dr. Nishtha Khera | July 2013 | May 2016 | |
| Dr. Shouriyo Ghosh | July 2013 | May 2016 | |
| Dr. Battu Sudha Nagavalli | Jan 2014 | Dec 2016 | |
| Dr. Libin Babu Cherian | Jan 2014 | Dec 2016 | |
| Dr. Ekta Rahul | July 2014 | May 2017 | |
| Dr. Kirti | July 2014 | May 2017 | Dr. Deepali Jain |
| Dr. Balamurugan | July 2014 | May 2017 | |
| Dr. Hemanth Kumar R. | Jan 2015 | Dec. 2017 | Dr. Geetika Singh |
| Dr. Khushbu Khetan | Jan 2015 | Dec. 2017 | |
| Dr. Nisha | July 2015 | May 2018 | |
| Dr. Jayati | July 2015 | May 2018 | Dr. Prasenjit Das |
| Dr. Neetika Gurang | July 2015 | May 2018 | Dr. M.C. Sharma |
| Dr. Anubhav | July 2015 | May 2018 | Dr. Seema Khausal |
| Dr. Sulaiman | July 2015 | May 2018 | Dr. Prasenjit Das |
| Dr. Jahnvi | July 2015 | May 2018 | |
| Dr. Rimlee Dutta | July 2015 | May 2018 | Dr. Prasenjit Das |
| Dr. Anil Sharma | July 2015 | May 2018 | |
| Dr. Anju G.S. | Jan 2016 | Dec 2018 | Dr. M.C. Sharma |
| Dr. Swaroopa Gadela | Jan 2016 | Dec 2018 | Dr. Sudheer Arava |
| Dr. Sajida Batool | Jan 2016 | Dec 2018 | Dr. Rajini Yadav |
| Dr. Mohammed Jassim | July 2016 | May 2019 | Dr. Geetika Singh |
| Dr. Abhishek Satapathy | July 2016 | May 2019 | Dr. AK Dinda |
| Dr. Arun Kumar Panda | July 2016 | May 2019 | Dr. Saumyaranjan Mallick |
| Dr. Nadeem | July 2016 | May 2019 | Dr. Shipra Aggarwal |
| Dr. Vijay Mariadas Antony | July 2016 | May 2019 | Dr. Deepali Jain |
| Dr. Hemlata Jangir | July 2016 | May 2019 | Dr. Seema Kaushal |
| Dr. Sanjay Sriram | Jan 2017 | Dec 2019 | Dr. Vaishali Suri |
| Dr. Mimna Murali | Jan 2017 | Dec 2019 | Dr. Asit Ranjan Mridha |
| Dr. Anjana Johnson | Jan 2017 | Dec 2019 | Dr. Sandeep Mathur |
| Dr. Supraja K.S. | Jan 2017 | Dec 2019 | |
| Dr. Priyadarsani. S. | July 2017 | May 2020 | Dr. AK Dinda |
| Dr. Shraddhanjali Satapathy | July 2017 | May 2020 | Dr. Deepali Jain |
| Dr. Christabella Thomas | July 2017 | May 2020 | Dr. Sudheer Arava |
| Dr. Shalini Kardam | July 2017 | May 2020 | Dr. Shipra Aggarwal |
| Dr. Nivetha Ambalavanan | July 2017 | May 2020 | Dr. M.C. Sharma |
| Dr. Rahul Raj | July 2017 | May 2020 | Dr. Geetika Singh |
| Dr. Balachander. S. | Jan 2018 | Dec 2020 | Dr. Rajini Yadav |
| Dr. Hena Khandakar | Jan 2018 | Dec 2020 | Dr. Seema Kaushal |
| Dr. Surabhi Jain | July 2018 | May 2021 | Dr. Saumyaranjan Mallick |
| Dr. Priyanka Mani | July 2018 | May 2021 | Dr. Prasenjit Das |
| Dr. Sivakumar | July 2018 | May 2021 | Dr. Sandeep Mathur |
| Dr. Mohammed Shafeeq | July 2018 | Dec 2021 | Dr. Vaishali Suri |
| Dr. Isha Shrestha | July 2018 | May 2021 | Dr. Asit Ranjan Mridha |
| Dr. Anuma Sharma | July 2018 | May 2021 | Dr. Sudheer Arava |
| Dr. Disha Kakkar | July 2018 | May 2021 | |
| Dr. Diya Roy | July 2018 | May 2021 | Dr. Aanchal Kakkar |
| Dr. Rajeshwari Sabapathy | Jan 2019 | Dec 2021 | Dr. Geetika Singh |
| Dr. Deepa. S. | July 2019 | May 2022 | Dr. M.C. Sharma |
| Dr. Salma Ferosh Usman Khan | July 2019 | May 2022 | Dr. Rajini Yadav |
| Dr. Sunil Kumar | July 2019 | May 2022 | |
| Dr. Pranitha Gaddam | July 2019 | May 2022 | Dr. Shipra Aggarwal |
| Dr. Shivangi Daggar | July 2019 | May 2022 | Dr. Seema Kaushal |
| Dr. Trisha Mondal | July 2019 | May 2022 | Dr. Saumyaranjan Mallick |
| Dr. Syed Saad Salman | Jan 2020 | Dec 2022 | Dr. Asit Ranjan Mridha |
| Dr. Sachita Pandey | Jan 2020 | Dec 2022 | Dr. Prasenjit Das |
| Dr. Shalini Suman | Jan 2020 | Dec 2022 | Dr. Vaishali Suri |
| Dr. Shweta Meena | Jan 2020 | Dec 2022 |
The list of ongoing funded research projects with the departmental faculty as principal investigators (PI)/ Co-PI are given below:
Immunohistochemistry
Electron microscopy
Flow cytometry
| Name | Place | Contact No. |
|---|---|---|
| Surgical Pathology Specimen receiving room | 1079 | 118 |
| Grossing laboratory | 1078 | 118 |
| Histopathology Laboratory | 1066 | 113, 114 |
| Cytopathology specimen receiving room | 1069 | 115 |
| Cytopathology Laboratory | 1069 | 115 |
| Renal Pathology and Transplant Immunology Laboratory | 1059 | - |
| Thoracic Pathology laboratory | 3006, Convergence Block | - |
| Gastrointestinal Pathology laboratory | 1084A | 119 |
| Cardiac Pathology laboratory | 1083A | - |
| Dermatological Pathology laboratory | 3006, Convergence Block | - |
| Lymphoma laboratory | 1073A | 116 |
| Report dispatch and enquiry | 1085A | 120 |
Rapid on-site assessment for adequacy of minimally invasive procedures such as ultrasound guided aspiration/ biopsy and endoscopy guided procedures are routinely provided.
FNAC clinic - Fine needle aspiration of superficial lumps is performed in Room No. 5054, OPD block, between 9 AM and 12 noon everyday including Saturdays.
The Department of Pathology at A.I.I.M.S, New Delhi, founded in 1957, has been a pioneer in the field of pathology since its inception. The Department is a leading innovator in research, service, and education. The department offers state of the art histopathology and cytopathology patient care services incorporating advanced diagnostic methods that include immunohistochemistry, electron microscopy, immunofluorescence, immunoblot, and molecular techniques such as in-situ hybridization and polymerase chain reaction.
The Department is currently headed by Professor. Venkateswaran K. Iyer (2021 onwards).
In the year 2021-2022, Department of Pathology has been able to maintain high-level academics and efficient clinical services, despite the waves and troughs of COVID-19 pandemic. The department is engaged in routine diagnostic reporting of Surgical Pathology and Cytopathology, and teaching of undergraduate and postgraduate students in addition to performing high quality research in various areas of pathology. The department provided services to large number of patients by processing approximately 40,000 surgical pathology and 17,000 cytopathology specimens.
New facilities have been added in the department for routine patient care services related to molecular pathology and cytogenetic work-up, which include in-situ hybridization, flow cytometry, tissue microarray, capillary electrophoresis, real-time PCR etc. The diagnostic and predictive immunohistochemical panel has been expanded and a total of 50,558 slides have been stained and studied during this period.
The Department is regularly providing reports for molecular tests in all pathology sub-specialities. A few examples include EGFR gene mutations, ALK and ROS-1 rearrangements in lung cancer, Her-2/neu amplification in breast cancers, TCR clonality assay in lymphomas, multiple gene fusions and other molecular alterations in salivary gland tumors as well as soft tissue sarcomas, and has started providing MYCN amplification in pediatric neuroblastomas, and FOXO1 fusions in rhabdomyosarcomas. Liquid biopsy testing using patients’ blood plasma has been standardized and included in patient-care program. We have been doing resistant mutation analysis in therapy-progressed EGFR-positive lung cancer patients by liquid biopsy and reports are released in clinics.
We are moving towards Digital Pathology sphere for implementation of next generation pathology in future. In that context, department has organized national cytology conference ‘CYTOCON 2021’ entirely in virtual mode with overwhelming participation from all over the country. Many virtual workshops were organized including a one on digital pathology where whole slide images were used for teaching purposes.
In addition, during this year also, AIIMS Pathology monthly Webinar Series (Department of Pathology YouTube channel) was as successful as earlier years in which lectures from many international alumni including the eminent Dr. Vinay Kumar, editor of Robbins and Cotran basis of disease, Dr.Rifat Mannan, Dr. Sonika Dahiya, Dr. Kamaljeet Singh, Dr. Kalyani Patel from USA, were streamed on YouTube.
The undergraduate and postgraduate teaching programs are being constantly updated and refreshed to meet the knowledge and skills sets currently required of trainees in the era of evidence based medical practice.
The Department faculty have received funding for approximately 30 extramural and 21 intramural projects related to pathology and molecular features of wide spectrum of neoplastic and non-neoplastic diseases. The faculty of the department has presented their research work at various virtual national and international conferences and received awards individually or to their residents. More than 200 papers have been published in peer reviewed national and international journals during the year 2021 alone.
Notably, Dr. Sandeep R. Mathur has been awarded the prestigious Earnest Fernandez slide seminar by Indian Academy of Cytologists in Annual Conference held in Nov 2021. Dr. Deepali Jain was the first Indian to receive the prestigious Mary J. Matthews Pathology/ Translational Research Award, International Association for the Study of Lung Cancer (IASLC), Sep 2021, and was listed in most cited work of top 10 doctors of AIIMS New Delhi which was prepared from Stanford University California list of world’s top 2% of scientists.
We have many faculty members contributing to World Health Organization (WHO) blue books for classification of tumors of various systems edited by International Agency for Research on Cancer (IARC), Lyon, France.
Publications are given in the respective profile
The focus of research has been in following areas:
Dr. KH Reeta
Dr. Pooja Gupta
Dr. HN Yadav
Dr. Sudhir Chandra Sarangi
Dr. KH Reeta
Dr. Pooja Gupta
Dr. H N Yadav
Dr. Sudhir Chandra Sarangi
National Poisons Information Centre (NPIC) in Department of Pharmacology, AIIMS, New Delhi initiated an outreach project with a theme BE CAUTIOUS, BE POISON SAFE. This theme aims to increase awareness towards poisons and poisoning among general public including Children, Parents and Occupational Workers. It also intends to increase knowledge regarding poisons and poisonous substances and disseminate knowledge of poison prevention measures that can be practiced to reduce the risk of accidental poisonings. It also advocates to adopt safe practices and enforce effective poison control measures.
Awareness activities organized in the past by National Poisons Information Centre (NPIC), AIIMS, New Delhi
| Name: Dr. Madhuri Gupta Designation: Scientist Qualification: M.Sc., Ph.D. Area of Interest: Analytical chemistry & pesticides Phone: 011-26593677, 26589391 Email: madhurijaswal71@ymail.com |
| Name: Dr. Sunder S. Samuel Designation: Scientist Qualification: M.Sc., Ph.D. Area of Interest: Cardio & neurotoxicology Phone: 011-26593677, 26589391 Email: sunder_sam@yahoo.co.uk |
| Name: Dr. Swati Sharma Designation: Scientist Qualification: M.Sc., Ph.D. Area of Interest: Pharmacogenomics & bioinformatics Phone: 011-26593677, 26589391 Email: mail_swati84@yahoo.co.in / drswati2107@gmail.com |
| Name: Dr. Devendra Singh Designation: Scientist Qualification: M.Phamr, Ph.D. Area of Interest: Neuropharmacology, Ischemic Stroke, Alzheimer’s Disease, Preclinical research Phone: 011-26593677, 26589391 Email: dvndr.singh@gmail.com |
| Name: Dr. Ajay Godwin Potnuri Designation: Scientist Qualification: M.S (Pharm), Ph.D. Area of Interest: Cardiovascular Pharmacology and toxicology with a special emphasis on hypertensive heart disease and vascular biology Email: dr.ajaygodwin.p@gmail.com |
| Name: Dr. Jyoti Designation: Scientist Qualification: M.Sc., Ph.D. Area of Interest: Endocrinology, Neurosciences Email: jyotiswarup11@gmail.com |
ABOUT NPIC | |
The National Poisons Information Centre (NPIC) was established in February 1995 in the Department of Pharmacology, All India Institute of Medical Sciences (AIIMS), New Delhi. The Centre provides round-the-clock information on management of poisonings to Health Care Professionals and the general public. Toll Free No. - 1800 116 117 Tel No. - 011-2658 9391, 011-2659 3677 E-mail: npicaiims2010@gmail.com |
The Faculty of the Department of Pharmacology is significantly contributing to undergraduate and postgraduate teaching and research. The research activities of the department focus mainly in the area of molecular pharmacology, inflammation research, neuropharmacology and cardiovascular pharmacology. The department is also providing hospital services and running the National Poisons Information Centre that provides round-the-clock information on various aspect of poisoning and its management.
Prof. B.K. Anand (1917-2007)
After completing his pioneering research in the USA on the role of Hypothalamus in the feeding behavior of rat in 1952, he came back to India to establish and lead the Department of Physiology from 1956 till 1974. He was awarded Shanti Swarup Bhatnagar Prize for Science and Technology in 1963 and Padma Shri in 1969 for his meritorious contributions.
Prof. Baldev Singh (1904-1998)
He is often referred to as the ‘Grand-father Neuron’ by the scientific community. He joined as Emeritus Professor of Physiology in AIIMS. He was interested in research on lateral hypothalamus, highaltitude, yoga, sleep, consciousness and hyperpyrexia.Under his leadership, the department became an international center of neurophysiological research.
Professor GS Chhina (1926–2011)
He joined department of Physiology at AIIMS and worked with Dr BK Anand and Dr Baldev Singh on food intake, reproduction and yoga. Even after retirement in 1986, he continued working as Emeritus Professor and contributed to the field of Physiology.

Surender Kumar Manchanda (1931-1998)
He joined the Department of Physiology as a Demonstrator under Prof. B.K.Anand in 1957.He took over as the Head and Professor of Physiology 1974 and led the Department till November 1991. He made major scientific contributions in the field of Neurosciences and Reproduction.
Anasuya B, Deepak KK, Jaryal A. The cardiovascular variability during transient 6° head down tilt and slow breathing in yoga experienced healthy individuals. Int J Yoga. 2021;14:188-97.
Anil AK, Vanidassane I, Netam R, Pushpam D, Bakhshi S, Deepak KK. Autonomic dysfunction in postoperative primitive neuroectodermal tumor of heart. Ann Clin Neurophysiol. 2021;23(2):126-129.
Shankhwar V, Singh D, Deepak KK. Effect of countermeasure bodygear on cardiac-vascular-respiratory coupling during 6-degree head-down tilt: An earth-based microgravity study. Life Sci Space Res (Amst). 2022;32:45-53.
Tamuli D, Kaur M, Jaryal AK, Srivastava A, Kumaran SS, Deepak KK. Structural atrophy of central autonomic network correlates with the functional attributes of autonomic nervous system in spinocerebellar ataxia patients. Journal of Clinical Neuroscience, J Clin Neurosci. 2021;93:274-28.
Shankhwar V, Singh D, Deepak KK. Effect of Novel Designed Bodygear on Gastrocnemius and Soleus Muscles during Stepping in Human Body. Microgravity Sci. Technol. 2021;33(2):29.
Shankhwar V, Singh D, Deepak KK. Characterization of Electromyographical Signals from Quadricep and Hamstring muscles to Evaluate the performance of Squats Coupled with Gravity Modulating Bodygear. Microgravity Sci. Technol. 2021;33(4):39.
Anasuya B, Deepak KK, Jaryal A. Yoga Practitioners Exhibit Higher Parasympathetic Activity and Baroreflex Sensitivity and Better Adaptability to 40 mm Hg Lower-Body Negative Pressure. Int J Yoga Therap. 2021;31(1):2.
Chandran DS, Kaur S, Deepak KK. Student perceptions on synchronous virtual versus face-to-face teaching for leader-centered and participant-centered postgraduate activities during COVID-19. Adv Physiol Educ. 2021;45(3):554-562.
Goswami N, Singh A, KK Deepak. Developing a “dry lab” activity using lower body negative pressure to teach physiology. Adv Physiol Educ. 2021;45(3):445-453.
Khan WF, Krishna A, Roy A, Prakash O, Jaryal AK, Deepak KK, et al. Effect of structured training in improving the ergonomic stress in laparoscopic surgery among general surgery residents. Surg Endosc. 2021;35(8):4825-4833.
Singh A, Srivastav S, Yadav K, Chandran DS, Jaryal A, Deepak KK. Neurohormonal responses to oscillatory lower body negative pressure in healthy subjects. Acta Astronautica. 2021;186:396-402.
Kulshreshtha P, Deepak KK, Yadav RK, Mukherjee D. Cardiac autonomic neuropathy in fibromyalgia: Revisited. J Back Musculoskelet Rehabil. 2022;35(1):111-117.
Deepak KK, Rao MM. Yoga and Meditation as an Adjunct Interventional Strategy for COVID-19 Management. Ann Natl Acad Med Sci (India). 2021;57(02):065-067.
Shankhwar V, Singh D, Deepak KK. Cardiac-vascular-respiratory coupling analysis during 6-degree head-down tilt microgravity analogue. Biomed Signal Process Control. 2022;72(49):103358.
Samanchi R, Muthukrishnan SP, Dada T, Sihota R, Kaur S, Sharma R. Altered spontaneous cortical activity in mild glaucoma: A quantitative EEG study. Neurosci Lett. 2021;759:136036.
Gurja JPK, Muthukrishnan SP, Tripathi M, Sharma R. Reduced Resting State Cortical Alpha Connectivity Reflects Distinct Functional Brain Dysconnectivity in Alzheimer’s Disease and Mild Cognitive Impairment. Brain Connect. 2022;12(2):134-145
Chandran DS, Muthukrishnan SP, Barman SM, M. Peltonen L, Ghosh S, Sharma R, et al. Operations perspective to competency-based medical education: Experiences of IUPS-ICMR Physiology Education Workshop series (2018-2019) conducted in India. Indian J Med Res. 2021;154(4):553–7.
Sambhav R, Jena S, Chatterjee A, Bhasin S, Santapuri S, Kumar L, et al. An Integrated Dynamic Closed Loop Simulation Platform for Elbow Flexion Augmentation Using an Upper Limb Exosuit Model. Front Robot AI. 2022;9:768841.
Sadananda S, Dastidar SG, Chitturi V, Singh Balhara YP, Sharma R, Kaur S. Electroencephalography-based cortical sources of working memory in the subjects with opioid addiction: A pilot study. Indian J Med Res. 2021;154(4):583-591./p>
Kumar S, Pal A, Jain S, Velpandian T, Mathur R. Electromagnetic field stimulation attenuates phasic nociception after complete spinal cord injury in rats. Brain Sci. 2021;11:1431.
Sharma S, Sunil, Kochhar KP, Jain S. A review on cognitive impairments in Parkinson's disease. Acta Scientific Veterinary Sci. 2021;3(12):27-32.
Sharma S, Kochhar KP, Jain S, Jayasunder R, Divya MR. Therapeutic potential of Indian traditional medicines in Parkinson’s disease. Adv Phytomed. 2021;10(2):252-263.
Sharma S, Singh D, Kochhar KP, Jain S, Gupta RK. A brief review on altered gut microbiota and metabolites in Parkinson's disease. Academia letters 2022.
Chaudhary S, Kumari S, Kumaran SS, Goyal V, Jain S, Kaloiya GS. In vitro and in vivo NMR based metabolomics in Parkinson's disease. J Magn Reson Open. 2022;10(11):100050.
Jha VK, Bhowmik D, Agarwal SK, Kaur M, Jaryal A. Improvement in Pulse Wave Velocity and Baroreflex Sensitivity Three-and Six-Month Postrenal Transplantation. Saudi J Kidney Dis Transpl. 2021;32(3):657-670.
Jha VK, Bhowmik D, Agarwal SK, Kaur M, Jaryal A. Renal Transplantation Significantly Improves Autonomic Function with Normalization of Baroreflex Sensitivity as Early as Three-Month Post-transplantation. Saudi J Kidney Dis Transpl. 2021;32(3):645-656.
Bir M, Gupta U, Jaryal AK, Singh A, Netam R, Kale SS, et al. Predictive value of intraoperative D-wave and m-MEP neurophysiological monitoring in patients with preoperative motor deficits in immediate and late postoperative period. J Craniovertebr Junction Spine. 2021;12(1):26-32.
Badhwar S, Chandran DS, Jaryal AK, Narang R, Patel C, Deepak KK. Brachial Artery "Low-Flow Mediated Constriction" Is Associated with Myocardial Perfusion Defect Severity and Mediated by an Altered Flow Pattern during Occlusion. Pulse (Basel). 2021;9(3-4):99-108
Vishwakarma LC, Sharma B, Singh V, Jaryal AK, Mallick HN. Acute sleep deprivation elevates brain and body temperature in rats. J Sleep Res. 2021;30(2):e13030.
Gagnani SP, Yadav P, Roychoudhury A, Bhutia O, Jaryal AK. Longitudinal electromyographic changes in masseter and anterior temporalis muscle before and after temporomandibular joint arthroplasty in ankylosis patients. J Stomatol Oral Maxillofac Surg. 2021;122(6):573-577.
Nongrem G, Surve A, Venkatesh P, Sagar R, Yadav RK, Chawla R, et al. Effect of short-term meditation training in central serous chorioretinopathy. Indian J Ophthalmol. 2021;69:3559-63.
Dada T, Lahri B, Mahalingam K, Shakrawal J, Kumar A, Sihota R, et al. Beneficial effect of mindfulness based stress reduction on optic disc perfusion in primary open angle glaucoma: A randomized control trial. J Tradit Complement Med. 2021;11(6):581–586.
Yadav R, Yadav RK, Pandey RM, Upadhyay AD. Predictors of Health-Related Quality of Life in Indians with Metabolic Syndrome Undergoing Randomized Controlled Trial of Yoga-Based Lifestyle Intervention vs Dietary Intervention. Behav Med. 2021;47(2):151-160.
Magan D, Yadav RK. Right Broca's area is hyperactive in right-handed subjects during meditation: Possible clinical implications? Med Hypotheses. 2021;150:110556.
Sankalp, Dada T, Yadav RK, Sharma HB, Netam RK, Kochhar KP. Effect of Tratak (yogic ocular exercises) on intraocular pressure in glaucoma: An RCT. Int J Yoga 2022;15:59-69.
Dada T, Mondal S, Midha N, Mahalingam K, Sihota R, Gupta S, Angmo D, Yadav RK. Effect of Mindfulness-Based Stress Reduction on Intraocular Pressure in Patients With Ocular Hypertension: A Randomized Control Trial. Am J Ophthalmol. 2022;239:66-73.
Yadav B, Bade G, Guleria R, Talwar A. Exhaled Breath Temperature and Systemic Biomarkers for Assessment of Airway Inflammation in Asthmatics. J Assoc Physicians India. 2021;69(7):11-12.
Bade G, Akhtar N, Trivedi A, Madan K, Guleria R, Talwar A. Impulse oscillometry as a measure of airway dysfunction in Sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2021;38(3):e2021037.
Shanmugasundaram K, Talwar A, Madan K, Bade G. Pulmonary Functions and Inflammatory Biomarkers in Post-Pulmonary Tuberculosis Sequelae. Tuberc Respir Dis (Seoul). 2022;85(2):175-184.
Trivedi A, Bade G, Madan K, Ahmed Bhat M, Guleria R, Talwar A. Effect of Smoking and Its Cessation on the Transcript Profile of Peripheral Monocytes in COPD Patients. Int J Chron Obstruct Pulmon Dis. 2022;17:65-77.
Nanda S, Arya S, Bhatia R. Do Nociceptive flexion reflex and subjective pain coincide? Neurol India. 2021;69(6):1853-4.
Singh A, Roy Choudhary A, Bhutia O, Yadav R, Bhatia R, Yadav P. Longitudinal changes in electromyographic activity of masseter and anterior temporalis muscle before and after alloplastic total join replacement in patients with temporomandibular ankylosis: A prospective study. Br J Oral Maxillofac Surg. 2022;S0266-4356(22)00041-9.
Nabeel PM, Chandran DS, Kaur P, Thanikachalam S, Sivaprakasam M, Joseph J. Association of incremental pulse wave velocity with cardiometabolic risk factors. Sci Rep. 2021;11(1):15413.
Tarik M, Ramakrishnan L, Bhatia N, Goswami R, Kandasamy D, Roy A, et al. The effect of Bacillus coagulans Unique IS-2 supplementation on plasma amino acid levels and muscle strength in resistance trained males consuming whey protein: a double-blind, placebo-controlled study. Eur J Nutr. 2022.
Raj KV, Nabeel PM, Chandran D, Sivaprakasam M, Joseph J. High-frame-rate A- mode ultrasound for calibration-free cuffless carotid pressure: feasibility study using lower body negative pressure intervention. Blood Press. 2022;31(1):19-30.
Akhtar N, Srivastava RK, Shrivastava D. How Losing Sleep Following Vaccination May Weaken the Response to SARS-CoV Vaccines. Sleep Vigil. 2022: 1–3.
Bhat SY, Akhtar N, Sengupta T, Netam R, Kumar VM, Mallick HN. Electroencephalographic and electromyographic events during spontaneous and final arousal from sleep: a study of the sequence of appearance and significance. Sleep Vigil. 2021.
Somanath S, Sharma B, Puskar P, Roy A, Akhtar N, Mallick HN. The Wake Promoting Role of the Mediodorsal Thalamic Nuclei in Rat. Sleep Vigil. 2021.
Aggarwal K, Akhtar N, Mallick HN. Sleep quality mediates the relationship between risk of obstructive sleep apnea and acute stress in young adults. J Physiol Pharmacol. 2021;72(1).
Puskar P, Sengupta T, Sharma B, Nath SS, Mallick HN, Akhtar N. Changes in sleepwake cycle after microinjection of agonist and antagonist of endocannabinoid receptors at the medial septum of rats. Physiol Behav. 2021;237:113448.
Sharma B, Sengupta T, Chandra Vishwakarma L, Akhtar N, Mallick HN. Muscle temperature is least altered during total sleep deprivation in rats. J Therm Biol. 2021;98:102910.
Badhwar S, Chandran DS, Jaryal AK, Narang R, Deepak KK. Regional arterial stiffness in central and peripheral arteries is differentially related to endothelial dysfunction assessed by brachial flow-mediated dilation in metabolic syndrome. Diab Vasc Dis Res. 2017:1479164117748840.
Mary H, Singh D, Deepak KK. Identifying deep breath effect on cardiovascular signals using conditional entropy: an information domain approach. Biomed Eng. 2018;30(02):1850012.
Mary H, Singh D, Deepak KK. Harmonic Analysis of Arterial Blood Pressure Signal Using Fourier Decomposition for Autonomic Health Assessment. Current Trend Sig Process. 2017;7(3):7-14.
Choudhary N, Deepak KK, Chandra PS, Bhatia S, Sagar R, Jaryal AK, et al. Comparison of Autonomic Function before and after Surgical Intervention in Patients with Temporal Lobe Epilepsy. J Epilepsy Res. 2017;7(2):89.
Lal C, Kaur M, Jaryal AK, Deepak KK, Bhowmik D, Agarwal SK. Reduced baroreflex sensitivity, decreased heart rate variability with increased arterial stiffness in predialysis. Indian J Nephrol. 2017;27(6):446.
Bhagat OL, Kharya C, Jaryal A, Deepak KK. Acute effects on cardiovascular oscillations during controlled slow yogic breathing. Indian J Med Res. 2017;145(4):503.
Bhaskar L, Kharya C, Deepak KK, Kochupillai V. Assessment of Cardiac Autonomic Tone Following Long Sudarshan Kriya Yoga in Art of Living Practitioners. J Altern Complement Med. 2017;23(9):705-12.
Yadav K, Singh A, Badhwar S, Jaryal AK, Coshic P, Deepak KK, et al. Decreased Spontaneous Baroreflex Sensitivity as an Early Marker for Progression of Haemorrhage. Eur J Prev Cardiol. 2017;24(3):275-81.
Singh A, Kumar MS, Jaryal AK, Ranjan P, Deepak KK, Sharma S, et al. Diabetic status and grade of nonalcoholic fatty liver disease are associated with lower baroreceptor sensitivity in patients with nonalcoholic fatty liver disease. J Gastroenterol Hepatol. 2017;29(8):956-61.
Kumar A, Jaryal AK, Gulati S, Chakrabarty B, Singh A, Deepak KK et al. Cardiovascular autonomic dysfunction in children and adolescents with Rett Syndrome. Pediatr Neurol. 2017;70:61-6.
Choudhury MI, Singh P, Juneja R, Tuli S, Deepak KK, Prasad A, et al. A Novel Modular Tonometry-Based Device to Measure Pulse Pressure Waveforms in Radial Artery. J Med Device. 2018;12(1):011011.
Deepak KK. Editorial: Innovations in Physiology: Way to Make Rapid Advances in Research. Indian J Physiol Pharmacol. 2017;61(4):322.
Tamuli D, Godiyal AK, Kaur M, Jaryal AK, Srivastava AK, Deepak KK. Autonomic Function Based Classification of Spinocerebellar Ataxia Type 1 and 2 Using Machine Learning Classifiers. Indian J Physiol Pharmacol. 2017;61(4):323-32.
Deepak KK. Editorial: Promoting Research in Medical Sciences. Indian J Physiol Pharmacol. 2017; 61(3):208.
Yadav R, Jaryal AK, Mallick HN. Participation of preoptic area TRPV4 ion channel in regulation of body temperature. J Therm Biol. 2017;66:81-6.
Datta K, Tripathi M, Mallick HN. Yoga Nidra: An innovative approach for management of chronic insomnia-A case report. Sleep Sci Prac. 2017;1(1):7.
Trivedi A, Ghosh D, Guleria R, Mehta N, Talwar A. CD14 Positive Selection Displays an Edge in the Isolation of Macrophages from Induced Sputum of COPD Patients Using Immunobead Technology. Indian J Physiol Pharmacol. 2018;62(1):32-40.
Sharma S, Kaur S, Tripathi M, Talwar A, Sharma R. Differential Deficits in Attention, Working and Semantic Memory Discriminates Between Mild Cognitive Impairment and Alzheimer’s Disease. Indian J Physiol Pharmacol. 2017;61(4):348-56.
Srivastava A, Goyal V, Sood SK, Sharma R. Reduced saccadic velocity and pupillary width in young onset Parkinson’s disease. Neurol Psychiatry Brain Res. 2018;27:17-20.
Dey S, Bose S, Kumar S, Rathore R, Mathur R, Jain S. Extremely low frequency magnetic field protects injured spinal cord from the microglia-and iron-induced tissue damage. Electromagn Biol Med. 2017;36(4):330-40.
Khan R, Sharma A, Jain S, Mohanty S, Prasad K. Intra‐arterial transplantation of human bone marrow mesenchymal stem cells (hBMMSCs) improves behavioral deficits and alters gene expression in rodent stroke model. J Neurochem. 2017 Dec 1;143(6):722-35.
Yadav K, Singh A, Jaryal AK, Coshic P, Deepak KK, et al. Modulation of cardiac autonomic tone in non-hypotensive hypovolemia during blood donation. J Clin Monitor Comput. 2017;31(4):739-46.
Garg P, Badhwar S, Jaryal AK, Kachhawa G, Deepak KK, Kriplani A. The temporal trend of vascular function in women with gestational diabetes. Vasc Med. 2017;22(2):96-102.
Yadav R, Yadav RK, Sarvottam K, Netam R. Framingham Risk Score and Estimated 10-Year Cardiovascular Disease Risk Reduction by a Short-Term Yoga-Based Lifestyle Intervention. J Alt Comp Med. 2017;23(9):730-7.
Bhardwaj P, Sinha S, Yadav RK. Medical and scientific writing: Time to go lean and mean. Perspect Clin Res. 2017;8(3):113.
Kochhar KP, Oberoi AK, Hazra S, Lal PR. The role of traditional diet and yoga for infertility: a blend and balance of traditional knowledge and modern medicine. Indian J Trad Know. 2017;16(S):69-74.
Tanwar S, Mattoo M, Jain S, Kumar U, Gupta N, Bhatia R et al. Role of Hypothalamic–Pituitary–Gonadal Axis Hormones in Patients with Fibromyalgia Syndrome. Adv Biores. 2017;8(6):176-181.
The Integral Health Clinic provides yoga-based intervention for prevention and management of chronic diseases.
*The Autonomic Function Lab is involved in providing patient care services to many of the clinical disciplines since 1989. Till date the lab is credited to have tested over 6,000 patients from Neurology, Gastroenterology, Endocrinology, Medicine, Orthopaedics, IRCH, Paediatrics and others. Autonomic Function Tests provide an important investigative tool for the diagnosis, prognosis and management of many diseases. The lab routinely tests 3-4 patients daily and also offers services for both basic and clinical research. Currently this lab is fully equipped with sophisticated instruments to conduct vascular function tests. This lab is also conducting clinical research on various diseases and treatment modalities.
Patients are generally referred for Autonomic Function Tests from the OPDs or Clinical wards. They are required to get a date for the tests from the lab and they are also given proper instructions.
Tests that are performed for the benefit of the patients
Routine
Under standardization
Pain Neurophysiology Laboratory provides diagnostic facility for the referred patients of early Alzheimer’s disease. It also provides auxiliary services to the pain clinic, AIIMS in the choice of intervention and its evaluation for chronic headache and neuralgia patients
R. No. 2035, 2nd floor, PC Block/ Teaching Block, Dept of Physiology
Ph. 011-26593370/ Int 3370
IHC Vision Statement : To deliver the benefits of Mind, Medicine and Meditation integration for health & wellness, and generate scientific evidences
The IHC (Integral Health Clinic) is a facility that puts health promotion at the forefront, with the “human being” at the center. It was established by Prof RL Bijlani in Feb 2000, and after successfully completing 21 years, a new and contemporary version of the same was launched, and renamed as “Integral Health & Wellness Clinic” in Feb 2021.
The manifesto of this outpatient facility is beyond the therapeutic gains and embraces the mindset of health consciousness. The facility is a unique one, and caters to the destressing needs of the AIIMS employees including faculty, students, residents, and staff, and their families.
With years standing in its past as a testimony, it has catered to the people from all the walks of life with an array of health and wellness needs. During the recent COVID pandemic, we remained committed to increased health and wellness needs at physical, mental and emotional levels and continued online and offline services as much as possible in-line with the COVID guidelines.
The IHC principally deploys yoga-based lifestyle intervention to the participants. The regular participants would include patients referred from collaborating departments within AIIMS, e.g., Psychiatry, Surgical Disciplines, Endocrinology & Metabolism, Obstetrics & Gynecology, Pediatrics, RPC (glaucoma, dry eye syndrome etc.), Medicine, Rheumatology, Orthopaedics, PMR etc. Participants might have a need to manage a chronic disease (hypertension, coronary heart diseases, obesity etc.) or they might be just looking for general health and wellness needs that gives them a better and balanced lifestyle.
An optimized and structured program as per requirements is available and is customizable enough to fit one’s needs. The usual duration of this yoga-based lifestyle intervention is 2 weeks (60 to 90 min/day) at IHC. Participants are always welcome to return for a refresher course. The entire touch-time is highly engaging and provides a strong moral support to prevent fall-out.
Practically anyone, including but not limited to the referred patients from the collaborating departments, AIIMS, New Delhi and otherwise apparently healthy people are all welcome. Specific populations like patients with chronic diseases (obesity, diabetes type 2, hypertension, bronchial asthma, premenstrual syndrome, depression etc.) and healthy persons to uphold their health & wellness may enroll here.
Early morning sessions (before 9 am) OR late evening sessions (after 5 pm) may be organized as per the need and/ or, demands of patients/ participants.
The Department has provision for short-term training in its various laboratories. Interested candidates should apply to the Dean, AIIMS, New Delhi 110 029.
The Department admits students to Ph.D., M.D. and M.Sc courses.
Ph.D. is research oriented course centered around the project of advanced research.
M.D. and M.Sc are courses in which the emphasis on breadth rather than depth. They equipped the students for a teaching career in physiology.
For details of eligibility, procedure of admission and schedule of entrance examinations, please refer to the website of the Examination Section of the All India Institute of Medical Sciences.
Department of Physiology was established and developed by eminent neurophysiologist Prof. Bal Krishan Anand in 1956. The first batch of MBBS students were admitted in 1956. First MD students(1959) were Dr Pritam Kaur Gill and Dr Sushil Dua while first PhD student(1965) was Dr. R.Vijayan Pillai. During the golden period of department (1956-1975), department attracted many national and international researchers and students which included Dr SK Dua, Dr GS Chhina, Dr KN
Sharma, Dr SK Manchanda, Dr T Desiraju, Dr Usha Nayar, Dr Utaka Oomura to name few. First scientific investigation in the world on yoga and meditation was started by Dr Anand and Dr Chhina in the department in 1961.
Courses available
Clinical Investigations and Interventions
Department of Physical Medicine and Rehabilitation,AIIMS,New Delhi 110608,India
Please prefix the following codes prior to the phone numbers, depending on the country you are calling from:-
When dialing from outside India: +91 11
When dialing from within India: 011
| Name | Designation | Contact No. | Email address |
|---|---|---|---|
| Dr Sanjay Wadhwa | Prof and Head | 26594916 | dr_wadhwa@rediffmail.com |
| Dr SL Yadav | Professor | 26594374 | yadav60@hotmail.com |
| Dr Gita Handa | Professor | 26593337 | gitahanda@hotmail.com |
| Dr Srikumar V | Addl. Professor | 26593232 | vsri21@yahoo.co.in |
| Dr Asem Rangita Chanu | Assoc. Professor | 26593232 | angita8@gmail.com |
| Office | 26594916 | ||
| P&O Workshop | 26594570 | ||
| OPD | 26593759 | ||
| Physiotherapy | 6708 | ||
| Occupational Therapy | 6587 | ||
| Mrs Ila Bhasin | MSSO | 6627 | |
| Nursing Station | 4055 | ||
| Stores | 3702 |
FAX: 26588663, 26588641
Content Provided by : Dr. Asem Rangita Chanu
Format: Name, Designation, Present affiliation (where known).
Format: Name, Designation, Present affiliation (where known).
| S.No. | Name | Course | Deptt. | Passing Month | Year |
|---|---|---|---|---|---|
| 1 | DR. MANOMOHAN BISWAS | M.D. | PM&R | DECEMBER | 1996 |
| 2 | DR. GITA HANDA | M.D. | PM&R | MAY | 1997 |
| 3 | DR. AKOIJAM JOY SINGH | M.D. | PM&R | MAY | 1997 |
| 4 | DR. ASIM KUMAR PALIT | M.D. | PM&R | DECEMBER | 1997 |
| 5 | DR. NILO Z. KIBA | M.D. | PM&R | MAY | 1998 |
| 6 | DR. MAHESWARAPPA B.M. | M.D. | PM&R | MAY | 1999 |
| 7 | DR. GANESH ARUN JOSHI | M.D. | PM&R | DECEMBER | 1999 |
| 8 | DR. JAYANTA ROY | M.D. | PM&R | MAY | 2000 |
| 9 | DR. ASHESHRAY CHAUDHURY | M.D. | PM&R | MAY | 2000 |
| 10 | DR. MANNEMELA SUPRAJA | M.D. | PM&R | MAY | 2000 |
| 11 | DR. SATYABRATA NATH | M.D. | PM&R | DECEMBER | 2000 |
| 12 | DR. SINDHUV. | M.D. | PM&R | MAY | 2001 |
| 13 | DR. MALLIKARJUNA NALLEGOWDA | M.D. | PM&R | MAY | 2002 |
| 14 | DR. SURESH R. | M.D. | PM&R | MAY | 2003 |
| 15 | DR. PALLAB DAS | M.D. | PM&R | MAY | 2003 |
| 16 | DR. DIGANTA BORAH | M.D. | PM&R | DECEMBER | 2003 |
| 17 | DR. MOHAMMED MOHIUDDIN ARAF | M.D. | PM&R | MAY | 2004 |
| 18 | DR. NAOREM AJIT SINGH | M.D. | PM&R | MAY | 2004 |
| 19 | DR. ANIL KUMAR GUPTA | M.D. | PM&R | MAY | 2006 |
| 20 | DR. MEEKA KHANNA | M.D. | PM&R | MAY | 2006 |
| 21 | DR. SRIKUMAR V | M.D. | PM&R | DECEMBER | 2006 |
| 22 | DR. NAVEEN MATHEW JOSE | M.D. | PM&R | DECEMBER | 2006 |
| 23 | DR. AMBIKA DAMODARAN | M.D. | PM&R | MAY | 2007 |
| 24 | DR. NAMAN GOEL | M.D. | PM&R | MAY | 2007 |
| 25 | DR. OM PRAKASH | M.D. | PM&R | MAY | 2009 |
| 26 | DR. DHEERAJ A | M.D. | PM&R | DECEMBER | 2009 |
| 27 | DR. SUSHIL SINGH LOITONGBAM | M.D. | PM&R | MAY | 2010 |
| 28 | DR. SUMAN BADHAL | M.D. | PM&R | DECEMBER | 2010 |
| 29 | DR. SUMANT KUMAR SINGH | M.D. | PM&R | MAY | 2011 |
| 30 | DR. RAJ KUMAR | M.D. | PM&R | DECEMBER | 2011 |
| 31 | DR. PRAJNARANJANI M | M.D. | PM&R | MAY | 2012 |
| 32 | DR. SUMALATHA K B | M.D. | PM&R | MAY | 2012 |
| 33 | DR. HARLEEN UPPAL | M.D. | PM&R | MAY | 2013 |
| 34 | DR. RAMITA SARDANA | M.D. | PM&R | MAY | 2013 |
| 35 | DR. SOUMYA SAXENA | M.D. | PM&R | MAY | 2013 |
| 36 | DR. SANJEEV KUMAR SHARMA | M.D. | PM&R | DECEMBER | 2013 |
| 37 | DR. VIPUL AGRAWAL | M.D. | PM&R | MAY | 2014 |
| 38 | DR. NITIN JOSHI | M.D. | PM&R | DECEMBER | 2014 |
| 39 | DR. RATNESH KUMAR | M.D. | PM&R | MAY | 2015 |
| 40 | DR. VASUNDHARA SAHA | M.D. | PM&R | DECEMBER | 2016 |
| 41 | DR. SHALINI MISHRA | M.D. | PM&R | MAY | 2017 |
| 42 | DR. SIVARUBAN | M.D. | PM&R | MAY | 2017 |
| 43 | DR. ARUN KUMAR CHOUDHARY | M.D. | PM&R | MAY | 2017 |
| 44 | DR. DAVINDER KUMAR VERMA | M.D. | PM&R | MAY | 2017 |
| 45 | DR. HAFIS RAHMAN M.C | M.D. | PM&R | DECEMBER | 2017 |
| 46 | DR. KANHU CHARAN MALLIK | M.D. | PM&R | DECEMBER | 2017 |
| 47 | DR. NOUFAL ALI | M.D. | PM&R | DECEMBER | 2017 |
| 48 | DR. SANDIPAN HAZRA | M.D. | PM&R | MAY | 2018 |
| 49 | DR. LUKRAM SUMILA | M.D. | PM&R | MAY | 2019 |
| 50 | DR. RENI BENNY | M.D. | PM&R | DECEMBER | 2019 |
| 51 | DR. RITIKA PARIHAR | M.D. | PM&R | DECEMBER | 2019 |
| 52 | DR. KRISHNA B | M.D. | PM&R | JUNE | 2020 |
| 53 | DR. FATHIMA HANEENA P | M.D. | PM&R | JUNE | 2020 |
| 54 | DR. SAMANTAK SAHU | M.D. | PM&R | JUNE | 2020 |
| 55 | DR. RAKTIM SWARNAKAR | M.D. | PM&R | JUNE | 2020 |
| 56 | DR. ARJUN S | M.D. | PM&R | DECEMBER | 2020 |
| 57 | DR. ANSARUL HAQ MIYAN | M.D. | PM&R | DECEMBER | 2020 |
| 58 | DR. POOJA VASHISTHA | M.D. | PM&R | DECEMBER | 2020 |
| 59 | DR. ARAVIND PR | M.D. | PM&R | JUNE | 2021 |
| 60 | DR. VINEET KASHYAP | M.D. | PM&R | DECEMBER | 2021 |
| 61 | DR. SANGEETH A P | M.D. | PM&R | December | 2022 |
| 62 | DR. SUKHSHARAN KAUR DHILLON | M.D. | PM&R | December | 2022 |
| 63 | DR. AAKHIL NABUHANA | M.D. | PM&R | MAY | 2023 |
| 64 | DR. JISHNU P | M.D. | PM&R | MAY | 2023 |
| 65 | DR. VELUGULETI UJWAL | M.D. | PM&R | MAY | 2018 |
| 66 | DR. SANDIPAN NASKAR | M.D. | PM&R | MAY | 2023 |
| 67 | DR. ALHAT VINEET PETER | M.D. | PM&R | DECEMBER | 2023 |
| 68 | DR. SHOIBAM JENIFA DEVI | M.D. | PM&R | DECEMBER | 2023 |
Details of awards and honours won are available in the annual report of the AIIMS, available elsewhere on the Website of AIIMS.
IJPMR: Indian Journal of Physical Medicine and Rehabilitation (an official journal of Indian Association of Physical Medicine and Rehabilitation) is published from the department from October 1993 until April 2010. It can be accessed online by clicking here.
Please check on the profile of individual faculty members for salient research publications done by the individual faculty members.
Details of publications done are compiled in the Annual Reports of the AIIMS, which is available elsewhere on the website of AIIMS.
Invented by Dr SK Varma and Mr SH Mulla.
A majority of the activities of daily living in India are performed in squatting or Cross – legged sitting positions, e.g. eating, preparing food, home making, working in the farms, sitting in meetings of religious gatherings, attending school etc. It is so much merged in the routine life style that when someone loses the leg above the knee (amputation), wearing above knee prosthesis (artificial leg) of presently available designs means a total change in life style from floor level to chair level living. That means, the activities the person used to perform sitting on the ground, would have to be done sitting on a chair or stool. This change applies more to rural amputees. The conventional above knee prosthesis does not permit the user to squat or sit cross-legged on the ground which is an essential part of the activities of daily living for the people living in India and most of Afro-Asian Countries. This inability to squat or to sit Cross-legged occurs in a conventional above knee prosthesis because the knee flexion in such a prosthesis is not allowed beyond 100 degrees.
At AIIMS a new above knee prosthesis has been designed which permits squatting as well as cross-legged sitting. This is world's first design. For more details, please click here.
Invented by Dr U Singh and Mr SS Wason.
Patients using this type of joint fitted in a HKAFO (above knee caliper with hip joint and pelvic belt) can also sit cross-legged and squat, which was not possible with conventional orthoses (calipers). This was also world’s first design of the kind. For more details, please click here.
Invented by the team under of Dr SK Varma.
This replaces the heavy and metallic orthoses with light weight orthosis that can be fitted with any type of shoe or even canvas or sports shoe.
Invented by Mr JB Joshi and Mr SS Wason
This was an innovative design of a goniometer based on pendulum to detect even minor motions of the neck and head in any direction. This was applauded during the international scientific meets.
Invented by the Team under Dr SK Varma.
Collection of soil from ileostomy was a costly affair for Indians. This indigenous bag was a boon for the Indian colostomy patients.
Invented by a team from IIT Delhi (Dr Sneh Anand and others) and AIIMS: Dr U Singh.
It was a collaborative work with IIT Delhi. Prototype developed under the PhD thesis project of Dr Deepak Joshi. Patent filed and accepted. For more details please click here.
EMG
Balance Assessment
Equipment
Gym
Traction
Tilt table
Steps
Held on Thursdays at 9.30 AM.
Comprehensive Rural Health Services Project is run by AIIMS in collaboration with the Haryana Governments' Health Services. PMR OPD and minor procedures are done in CRHS Ballabgarh, the out-reach service of AIIMS.
The department is equipped with many state of the art equipments some of which are as follows:
Various aids and appliances are fabricated:
Held on Mondays at 2 PM.
Patients having foot deformities or other foot related problems are evaluated by the doctors and where necessary, foot pressure analysis is done. If orthotic devices are indicated, shoe inserts are machine molded as per the requirement. A team of doctors along with the Prosthetist and Orthotists are available in the clinic. Patients for the clinic are seen only by prior appointments. One needs to be seen in the PMR OPD, the doctors in PMR decide if the patient needs to be seen in the foot clinic.
Held on Thursdays at 2 PM.
Patients are prescribed Prosthetic and Orthotic (PO) appliances like belts, collars, calipers, artificial limbs, splints etc. in the OPDs/ Wards etc. Such appliances are fabricated in our PO workshop. Prior to these being delivered to the patient, final check out is done by the doctors. Appointments are given to the patients whose jobs are pending in the PO workshop.
Held on Mondays at 2 PM.
Most persons with disability require disability certificate. Standards were laid down in expert group meetings held by our department and were later suggested to the Government of India. These have been incorporated in the Gazette of India. Please check the Government’s guidelines for issuance of Disability Certificates. Patients desirous of getting certificates of disability are advised to check the notification issued by the respective state governments from time to time. As per the latest guidelines, the certificates of disability shall be issued to the patients by the notified hospitals catering to the respective geographical area only.
Railway concession certificates for the persons with disability are issued to the needy.
Held on Fridays at 2 PM.
Problems of the patients requiring comprehensive rehabilitation are discussed by a team of doctors. Appointments for the same are given during OPD hours by the treating doctors. Decision to discuss the case is taken by the tre
Hospital indoor facilities are provided to those patients who can benefit with intensive rehabilitation program under supervision.
Limited facilities in both general and private wards are available.
Charges for the indoor patients in the general ward as well as the private ward are as per the AIIMS policy. Details are available elsewhere on the AIIMS website.
A wide spectrum of activities are undertaken by the Rehabilitation Team and thus catering to a variety of patients. To give few examples, patients with neck or back pain, knee pain, various joint disorders, developmental disorders like cerebral palsy, neurological conditions like stroke, spinal cord injuries etc. It is not an overstatement to say that any person might benefit with a Rehabilitation intervention. Patients are initially seen by the specialist doctors who are responsible for the accurate diagnosis and treatment planning.
General OPD is conducted by the Resident Doctors along with the Faculty Members. Days of availability of most doctors during the week are fixed.
Monday to Saturday.
Sundays and
Gazetted Holidays as notified by Government of India (Central) for Delhi Region.
Monday through Friday: 8.30AM to 11.00 AM
Saturdays: 8.30 AM to 10.30 AM
Monday, Wednesday, Friday
Dr Sanjay Wadhwa
Dr SL Yadav
Dr Asem Rangita Chanu
Tuesday, Thursday, Saturday
Dr Gita Handa
Dr Srikumar V
Degree Awarded: MD (PMR)
Duration: Three Years.
Type: Full Term Post-Graduate Residency Program.
Entry Qualification: MBBS
How to apply: AIIMS PG Entrance Examination conducted by AIIMS twice a year.
Details: Watch the AIIMS Website and AIIMS Examinations Website.
Degree Awarded: None.
Duration: From a few days to Two Year.
What is it: Tailored to the needs of the trainees sponsored by government institutions from India and abroad.
How to apply: Please visit the website of "Academic Section" - "Courses and Trainings" offered. Duly filled application form available on the website, duly forwarded by the head of the institution.


The Department of Physical Medicine and Rehabilitation is actively engaged in providing high quality clinical care, education and research in the field of Physical Medicine and Rehabilitation and is dedicated to improving quality of life of persons with physically disabling conditions.
The PMR Specialist doctor is called "Physiatrist" who treats the patient as a whole with the goal to help patients understand their condition and provide the tools and resources to manage a successful healing process with the ultimate aim at improving the functioning of the patient. The continuity of care offers a variety of treatment methods to reduce or eliminate challenges and address recurrence. The services offered are related to musculoskeletal problems, brain injury, stroke, spinal cord injury, acute and chronic pain management, amputation, work injuries, orthopedic injuries, sports medicine, pediatricneuromusculo-skeletal problems and the developmental delays.
With the addition of quality to the lives of patients through comprehensive diagnosis and treatment and focused team approach, the patients are able to fully optimize their physical health.
| OPD Reception | 011-2673-9469 |
| Burns Emergency Counter | 011-2673-9543 |
| HOD Office | 011-2673-9607 |
| Duty Officer | 011-2673-9488 |
| BPS 3 Ward | 011-2673-9534 |
| BPS 4 Ward | 011-2673-9631/9632 |
Location:
Click here to locate Burns and Plastic Surgery Block on Google Maps

You can also reach us via google maps by scanning the following code from your smartphone:

Kindly send your feedback at-
plastichod@gmail.com
| Burns & Plastic Surgery OPD (Morn. Hours) | ||||||
|---|---|---|---|---|---|---|
| Room No | Monday | Tuesday | Wednesday | Thursday | Friday | Saturday |
| 19 | Prof. Maneesh Singhal /Senior Resident | Senior Resident / Faculty | Prof. Maneesh Singhal / Senior Resident | Senior Resident | Senior Resident | Senior Resident |
| 18 | Senior Resident | Dr. Shivangi Saha | Dr. Suvashis Dash | Dr. Aparna Sinha | Dr. Shivangi Saha | Dr. Suvashis Dash |
| 17 | Dr. Raja Tiwari | Dr. Shashank Chauhan | Dr. Raj Kumar Manas | Dr. Shashank Chauhan | Dr. Raja Tiwari | Dr. Raj Kumar Manas |
The department faculty is actively involved in teaching of
MCh Plastic and Reconstructive Surgery ( 3 years)
Cadaveric flap dissection course (Six Monthly)
Brachial plexus surgery cadaveric workshop (Annsually)
Ear reconstruction operative workshop and hands on Cartilage carving workshop (Annually)
Plastic, Reconstructive & Burns Surgery - For a better life!

The Department of Plastic, Reconstructive & Burns Surgery was formally established at AIIMS, in 2015. Before that, Plastic Surgery care was integral to the discipline of General Surgery, including ENT, Surgical Oncology, and Paediatric Surgery.
Professor Upadhyaya, Head of Paediatric Surgery and Professor IK Dhawan founded state of the art cleft surgery at the AIIMS in the early eighties. It was also around that time, Dr Rakesh Khazanchi joined the faculty. Having been trained in advanced microsurgery from Melbourne, Australia, he focused on limb and hand replantation with micro-vascular tissue transfers, and interdisciplinary cleft care in collaboration with the Department of Orthodontics.
Dr Maneesh Singhal joined the Institute as faculty in 2005 in the Department of Surgical Disciplines and enhanced the legacy by harnessing various Plastic & Reconstructive procedures and collaborations. In 2015, the Department came into formal existence and the concept for state-of-the-art dedicated Burn and Plastic surgery block was envisaged. The block became a reality and was inaugurated on 18th January 2021. Although in its nascent stage, it is already making its presence known, not just nationally but in the international arena also. The endeavour of this young and enthusiastic team of surgeons is to reduce the morbidity and provide functionality by reconstructive and microsurgical procedures thereby providing an improved quality of life to the patients. This centre will cater to one thousand burn patients annually with facilities that are unavailable anywhere else in the country.
With a facility for 100 indoor beds, dedicated burns emergency and ICU, equipped with modern state of the art care facilities and managed by highly trained faculty, dedicated residents, and health care staff, AIIMS Burn and Plastic Surgery Block is expected to become the standalone facility to the cause of care of burns and multitude of reconstruction care in coming times. The block has an easy access to trauma centre by a connecting bridge which will enhance interdisciplinary collaborative care. The department continues to works in collaboration with various other specialities such as Neurosurgery, Cardiac surgery, Orthopaedic surgery etc and independently it caters to almost all emergency hand injuries, microvascular reconstruction for complex limb trauma, post burn reconstruction, maxillofacial trauma, oncoplastic reconstruction, aesthetic breast surgery, Breast reconstruction and other congenital anomalies like Cleft lip & palate, Syndactyly, Polydactyly, Camptodactyly, Hypoplastic thumb deformity, etc. The team works in collaboration with Orthopaedic surgery to run the Hand Clinic, with the department of Orthodontics to run the Cleft Clinic, with the department of Dermatology to run the Aesthetic clinic, with the department of Neurosurgery to run the Brachial Plexus Injury clinic and the Amputation clinic along with PMR. There is a dedicated team of physiotherapists and occupational therapists that play a key role in the rehabilitation of post traumatic as well as post operative cases.
The team caters to reconstructive needs of patients at JPN Apex Trauma Centre, Dr. R. P. Centre for Ophthalmic Sciences, Centre for Dental Education and Research, Dr. BRAIRCH, CN Centre and Main AIIMS hospital.
Besides formal training of MCh. residents, the Department has taken a lead in capacity building for the nation, enhance & share the experience through various collaborations. To enhance skills and improve outcomes, the Department also focuses on paramedical health care training such as nursing officers, specialized wound care personnel.
With the launch of this dedicated block housing patient care, teaching and research care facilities, the Department is set to become a centre of excellence offering the most up-to-date patient treatment, fostering high standards of research and innovation and training future doctors to become experts in the field of Plastic surgery under the guidance of a dynamic leadership.
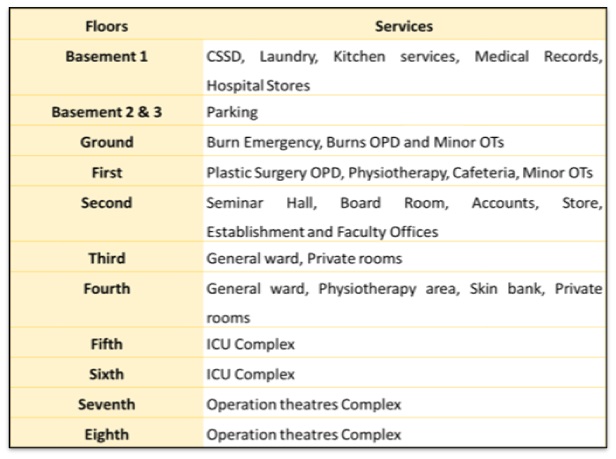

Block Emergency Exterior

Block OPD Exterior
Group Photo (Jan 2021)
PULMONARY MEDICINE OPD
Dr. Shubham Agarwal
.Dr. Benin Rajesh
Dr. Naren Chandra Dr. Sujay H.S.
Dr. Ayush Goel Dr. Muniza Bai Dr. Pranay C.S.
Dr. Jagbir Singh
Dr. Akshay Kawedia
Dr. Abhishek Chauhan
Dr. Soumya S. Dash
Dr. Pratyakcha Rai
Dr. Anchal Jain
Dr. Harsh Arora
Dr. Avishek Layak
Special Clinics
| Name of the clinic | Total number of cases in last year |
| Lung cancer clinic | |
| Sleep clinic |
Procedure done
Flexible bronchoscopies:
EBUS
Thoracoscopies
PFTs
Sleep studies
The department provides indoor care for various respiratory diseases such as COPD, Asthma, Pulmonary infections (Bacterial, fungal and viral), Interstitial lung disease, Lung cancer, Pleural diseases, and others. Our central inpatient ward is on the third floor in the New Private Ward wing.
We have a dedicated respiratory ICU with eight beds on the same floor attached to the ward. The ICU has advanced monitoring facilities, critical care ventilators, and various equipment required to care for critically ill patients. The ICU is manned around the clock by senior residents.
We also have a “Daycare” facility of 9 beds where patients are admitted for routine daycare procedures such as bronchial artery embolization(BAE) and other radiological techniques such as USG and CT-guided lung biopsies.
Department also caters to facilities for lung cancer patients, such as chemotherapy, and newer modalities of lung cancer treatment, such as monoclonal antibodies and other biologicals.
Department provides laboratory services such as skin prick tests (SPT), workup of various allergic disorders, including asthma, ABPA, and CPA (chronic pulmonary aspergillosis), and testing of ADA (adenosine deaminase) in various body fluids.
Department caters to general OPD services and special clinics. [Lung cancer clinic (Wednesday) and ILD, Pulmonary hypertension and sleep clinic (Friday)]
OPD days
Monday (9 am)
Thursday (9 am)
Special clinics (2 pm)
Wednesday (Lung cancer clinic)
Friday (ILD, Pulmonary hypertension, and Sleep clinic)
As part of outpatient management, the following services are provided
Interventional Pulmonology services
The Department offers various interventional pulmonology services, which include:
Interventional Bronchoscopy:
Flexible bronchoscopy and EBUS
Rigid bronchoscopy
Thoracoscopy
ICU: Percutaneous dilatational tracheostomy
Pulmonary function lab
Sleep lab
Lung cancer
Lung transplantation
Tuberculosis (DOTS clinic)
Pulmonary rehabilitation
international conference on Pulmonary, Critical Care & Sleep Medicine, the PULMOCRIT, has been successfully conducted by the Department since 2012, involving leading international and national faculties. Delegates from across the Indian subcontinent attended the conference. During the COVID-19 pandemic, the meeting was conducted in virtual mode. The Department has conducted online CME lecture series for Pulmonologists on topics like Endobronchial ultrasonography, Asthma, and Interstitial Lung Disease. The Department has been disseminating information about the COVID-19 pandemic to healthcare providers across the country through the AIIMS National COVID-19 grand rounds.
The Department has trained over 30 resident doctors via its 3-year DM program in Pulmonary, Critical Care & Sleep Medicine since its inception in 2012.
Besides the DM and Ph.D. courses, the Department provides training to residents from other specialties who are posted on a rotation basis. This includes:
The Department has been conducting an annual international conference, the PULMOCRIT, since 2012. As part of this, a 2-day workshop has been held on various practical aspects of Pulmonology, including the following over previous years:
This course is a 3-year pulmonary, Critical Care and Sleep Medicine fellowship program with an annual intake of 5 Academic Senior Residents. Candidates who have completed an MD degree in Internal Medicine or Respiratory Medicine are eligible to join this course. The selection is made via a competitive national-level entrance exam comprising two steps: a written exam followed by an interview.
During this training program, the fellows rotate in Pulmonary Ward, Intensive Care Unit (ICU), Bronchoscopy Suite, Sleep Lab, and Pulmonary Function Lab. They attend the general pulmonary out-patient department (OPD), Lung Cancer Clinic, Sleep Disorders Clinic, Interstitial Lung Disease Clinic, DOTS (TB) clinic, and Lung Transplant Clinic. They encounter a wide variety of challenging pulmonary cases referred from across the country. By the end of the program, the fellows will be competent in flexible bronchoscopy, endobronchial ultrasonography (EBUS), chest drain placement, percutaneous tracheostomy, and various ICU procedures. They acquire diverse skills, including critical care ultrasonography, mechanical ventilation, extracorporeal membrane oxygenation (ECMO), polysomnography, and pulmonary function testing.
The fellows are expected to present academic seminars, journal clubs, and physiology rounds as part of the program. They perform original research work for their DM dissertation. They also regularly attend multidisciplinary meetings with radiologists, pathologists, surgeons, radiation oncologists, anaesthesiologists, and palliative care physicians as part of the patient care routine.
The Department has a running Ph.D. program with an intake every six months via a competitive examination. Students who have a master's degree in the life sciences are eligible. This program allows the student to carry out cutting-edge research in basic and clinical Pulmonary Medicine.
The Department of Pulmonary, Critical Care and Sleep Medicine was initially established as the Department of Pulmonary Medicine and Sleep Disorders, a separate super specialty department at AIIMS, New Delhi, in May 2011. The institute later changed the name to its current name, keeping the department's mandate in terms of training and services.
Prof. Randeep Guleria was the founder and First Head of the department and laid the foundation for establishing the facilities and services the department currently provides. As of date, the department has seven faculty members. The department has an ongoing DM (Pulmonary, Critical Care, and Sleep Medicine) training program and a Ph.D. program. Currently, there are 15 positions for DM students and six seats for Non-Academic Senior Residents in the Department.
The department has a nine-bed Pulmonary Medicine ward and an eight-bed Pulmonary Medicine Intensive Care Unit. We also have a large daycare unit providing support for Chemotherapy for lung cancer patients and various diagnostic and therapeutic procedures. Care is offered to patients suffering from various respiratory ailments. The ICU caters to patients suffering from acute respiratory issues. It has advanced facilities, including Point-of-care Ultrasound (POCUS), Neurally adjusted ventilator assist (NAVA) ventilators, and Extracorporeal membrane oxygenation (ECMO).
Laboratory facilities include a Pulmonary function testing laboratory (PFT), allergy testing laboratory, biochemistry laboratory (Serum ACE level and body fluid ADA levels), Sleep Laboratory, and Bronchoscopy laboratory.
Advanced Interventional Pulmonology facilities are being provided, including Endobronchial Ultrasound-Guided Transbronchial needle aspiration (EBUS-TBNA and EUS-B-FNA), Medical thoracoscopy, therapeutic rigid bronchoscopic airway procedures, Airway Stenting, Endobronchial Electrocautery, and Cryotherapy. The department also provides facilities for navigational bronchoscopy and bronchial thermoplasty for severe asthma. Regarding flexible diagnostic bronchoscopy, procedures like transbronchial needle aspiration (TBNA), Bronchoscopic Lung Biopsy, Endobronchial Biopsy, and bronchoalveolar lavage (BAL) are being routinely performed. More than 2500 bronchoscopic procedures are performed in the department every year. The department also provides simulator-based training in flexible bronchoscopy, EBUS-TBNA, and rigid bronchoscopy.
The department has well-equipped sleep laboratories which provide comprehensive Polysomnography services. This includes full-night polysomnography, split-night polysomnography, PAP titration, actigraphy, and multiple sleep latency test (MSLT).
The pulmonary function testing laboratory (PFT) has facilities for spirometry, diffusion capacity testing, and lung volume assessment using body plethysmography. More than 10000 procedures are being done yearly in the lung function laboratory. Advanced lung function testing facilities such as fractional exhaled nitric oxide (FENO), Impulse Oscillometry for airway disease, and cardiopulmonary exercise testing (CPET) are also available. Pulmonary rehabilitation services are routinely provided to indoor and outdoor patients with a dedicated pulmonary rehabilitation service for patients with chronic respiratory diseases. Magnetic phrenic nerve stimulation studies are also being done for patients with suspected diaphragmatic dysfunction.
In allergy medicine, the department provides facilities for total serum IgE, Aspergillus-specific IgE, IgG testing, and skin prick testing. This helps evaluate patients with bronchial asthma, allergic bronchopulmonary aspergillosis, and chronic pulmonary aspergillosis.
We are in the process of compiling our alumni data. All our ex-faculty members, students and senior residents please contact Dr. Ashu Seith at : ashubhalla1@yahoo.com for details.
| S. No. | Investigation | To Contact Room No. |
|---|---|---|
| 1 | X-Ray | 39 |
| 2 | Ultrasound | 39 |
| 3 | Color Doppler | 39 |
| 4 | Mammography | 39 |
| 5 | CT Scan | 39 |
| 6 | MRI | 18 |
| 7 | DSA | 80 |
| 8 | Ultrasound guided procedures | 60 |
| 9 | CT guided procedures | 8 |
Approximately 3,50,000 exams are performed each year with busy, surgical, oncologic, medical, pediatric, obstetrical and trauma services.
This refers to plain radiographs such as Chest X-rays, spine x-rays, KUB, Abdomen, extremities, joints.
Patient Information:
Plain radiography, or X-ray, is the most common diagnostic procedure in imaging. It uses X Rays which after passing through the body part under consideration produces a ‘shadow’ or ‘image’ on a receptor which can be documented on a X Ray film.
Preparation and Procedure
For most X-ray examinations (except X Ray of the abdomen), no special preparation is required. As with most other imaging procedures, jewellery and other metallic articles should be removed because they may interfere with the exam.
The patient is positioned - standing, Sitting on a stool or lying on radiographic table depending on the body part radiographed.. Typically two or more x-rays are taken from different angles to give the radiologist multiple views of the region being studied for a better understanding of the pathology.
Fluoroscopy is a live, real time radiology technique using X Rays that enables the radiologist to visualize the organ or organ system being studied, either with or without the aid of a contrast agent,. The contrast agent is needed to enhance the visibility of soft tissues which normally are not visible on x-ray alone. During fluoroscopy the image is viewed on a television monitor by the radiologist. The contrast agents (or "contrast media" as they are also known) used are administered through intravenous injection, oral ingestion, as an enema or retrogradely through a fissure/sinus or an external opening visible on the surface.
Fluoroscopic procedures that are performed in our department include:
Barium studies are used to examine the Gastro-Intestinal system, including the oesophagus, stomach, small bowel and large bowel. A ready made barium sulphate suspension (powder in water) is used to coat the inside of the area being investigated. Air or other gas is often used along with barium to expand and coat (double contrast) the area under investigation to allow for more complete and better delineation of the normal and pathological regions. A Radiologist (specialist doctor) and a Technologist will perform the examinations, sometimes assisted by a Registered Nurse.
IT IS IMPORTANT THAT PATIENT BRINGS ALL PREVIOUS X-RAYS, SCANS OR ANY OTHER BIOCHEMICAL REPORTS WITH THEM ON THEIR DATE OF APPOINTMENT.
Refers to X Ray mammography (digital mammography with 3D Tomosynthesis) available in our department:
Patient Information:
Mammography is also a type of x-ray examination used to identify early cancers in breast tissue. Women should schedule a mammogram at a time when their breasts are likely not to be tender, such as the week before their menstrual period. The breast is compressed in a cassette for better visualization and both a top-to-bottom and a side view of each breast will be taken. Occasionally, additional views or an ultrasound exam may be requested by the radiologist for more information.
Other procedures also performed under mammographic guidance include ductography (imaging of the ducts of the breasts), Stereotactic facility (which enables needle biopsy procedures using computerized aid) and hook-wire localization.
Ultrasound imaging, also called ultrasound scanning or sonography, involves using high-frequency sound waves (Ultrasound) in diagnostic range to produce images of the inside of the body. Ultrasound exams do not use ionizing radiation (as used in x-rays or CT scan). Because ultrasound images are captured in real-time, they can show both the structure and movement of the body's internal organs, as well as blood flowing through blood vessels.
Ultrasound imaging is a noninvasive medical test that helps radiologist to diagnose diseases. Also since it does not use ionizing radiation, it is safe to use in children and in pregnant women.
Ultrasound tests that are performed in our department include:
Patient Information:
Patient lies on a couch and an operator places an ultrasound probe (transducer) on the skin over the part of the body to be examined. The probe is a bit like a very thick blunt pen. Lubricating jelly is put on patient’s skin so that the probe makes good contact with the body and ultrasound beam can traverse into the body part. The probe is connected by a wire to the ultrasound machine and monitor. Pulses of ultrasound are sent from the probe through the skin into your body. The ultrasound waves then bounce back from the various structures within the body.These echoes are detected by the same probe and are transormed into images by the computer within the ultrasound machine which are then displayed on the monitor of the machine. The picture is constantly updated so the scan (real time) can show both movements as well as structure. For example, the valves of a heart opening and closing during a scan of the heart. The operator moves the probe around over the skin surface to get views from different angles.
The ultrasound scan is a painless procedure and takes about 5-45 minutes, depending on the indication. A record of the results of the test can be made as still pictures or as a video recording.
Some special preparations are needed for specific studies which are communicated to patient in the appointment document e.g full urinary bladder for prostate or pelvis examination in women. Patient should continue to take their usual medication.
Also called a computed axial tomography (CAT) scan, CT is a method of body imaging in which a thin X-ray beam rotates all around the patients body part. Small detectors measure the amount of X-rays that make it through the patient or particular area of interest. A computer analyzes the data to construct a cross-sectional image.
CT scans may be done with or without contrast. "Contrast" refers to a substance taken by mouth (oral contrast) or injected into an intravenous (IV contrast) line that causes the particular organ or tissue under study to be seen more clearly. Contrast examinations require special preparation.
Patient will be asked to lie on a narrow table that slides into the center of the scanner gantry. Depending on the study being performed, one may need to lie on their stomach, on the back, or on the side. If intravenous contrast needs to be administered then an intravenous line will be placed in a small vein of the back of a hand or arm.
A CT scan is done to examine any part of the body : head and neck including brain, chest, abdomen, extremity and spine. CT is used not only as a diagnostic tool but is also used to guide interventional procedures such as biopsies and placement of drainage tubes.
CT scans may be performed to help diagnose tumors, evaluate blood vessels, evaluate infective and inflammatory conditions, determine calcium "scores" of the coronary arteries or check for other internal diseases, injuries (trauma) or damage.
CT scan uses ionizing radiation and therefore needs to be performed very carefully in selected patients after proper advice and recommendation from your treating physician.
Following CT investigations are performed in our department :
Patient Information:
Preparing for CT exam
Some patients are at high risk of allergic reaction or kidney failure when given Iodine-based intravenous contrast.
If you have any of the following occurrences in your medical history please inform the staff while you are scheduling your appointment:
All patients undergoing contrast enhanced CT scans must have BUN and Creatinine blood test results within 30 days prior to their CT exam.
Please do not eat within 4 hours of your exam, but drink plenty of water before if you will have IV contrast for your study.
Diabetic patients will need to stop Glucophage or Metformin the night before the examination. This decision is best taken in consultation with your treating doctor.
Do not re-start medication until BUN and Creatinine are back to normal results. This decision is best taken in consultation with your treating doctor.
Also called Magnetic Resonance Imaging or nuclear magnetic resonance (NMR) imaging, an MRI is a non-invasive procedure that uses powerful magnets and radiofrequency waves to construct images of the body.
The patient will be asked to lie still on a table that slides into a long tunnel-like tube within the scanner. . In this environment, some patients may feel claustrophobic. If contrast is to be administered then a canula will be placed, usually in a small vein of the hand or forearm. A technologist will operate the machine and observe you during the entire study from an adjacent room while taking several sets of images.
Following MR procedures are performed :
Patient Information:
Preparation for MRI
Most MRI exams require no special preparation. However for some types of scans you may be asked not to eat or drink for 4 hours prior to your test.
Most MR examinations do not usually require any special patient preparations. Whenever required, the contrast medium is administered immediately prior to the examination. It is safe and and is usually well tolerated by most patients. Caution needs to be taken in some patients with chronic kidney disease. Patients with cardiac pacemaker and cochlear implants cannot undergo MRI. However patients with metallic clip and hip or knee prosthesis may undergo MRI subject to the nature of prosthesis.
If you have had recent exams to diagnose this same or a similar problem at another facility, it would be helpful for the radiologist to see those exams. If available, please bring prior studies with you.
The duration of study may vary in different patients. Most examinations would finish in an hour.
Interventional Radiology (abbreviated IR or sometimes VIR for vascular and interventional radiology) is a subspecialty of radiology in which minimally invasive procedures are performed using image guidance. Some of these procedures are done for purely diagnostic purposes (e.g., angiogram), while others are done for treatment purposes (e.g., angioplasty, embolization) or taking biopsies / FNAC samples. Pictures (images) are used to direct these procedures, which are usually done with needles or other tiny instruments like small tubes called catheters. The images provide road maps that allow the Interventional Radiologist to guide these instruments through the body to the areas of interest
The procedures that we perform fall into three broad categories:
The teaching is elaborate and consists of both theoretical and applied/ hand on training. It is based on the prescribed curriculum of the Institute.
AIIMS Radiology courses held at a regular interval at a institute, on selected topics. Details available at www.aiimsradiologycourses.com
The Department of Radiodiagnosis at the All India Institute of Medical Sciences was started in the year 1956 under the leadership of Dr N.G. Gadedkar.
Following eminent professors have headed the department so far
22/09/1956 to 31/12/1966

01/01/1967 to 11/03/1970

12/03/1970 to 02/03/1985
03/03/1985 to 29/08/1987

30/08/1987 to 30/04/2001

01/05/2001 to 31/10/2005

01/11/2005 to 29/02/2008

-
Currently, Dr. Deep Narayan Srivastava is the Head of the department
The Department of Radiodiagnosis has state of art diagnostic, interventional and research facilities. These facilities are available at the Department of Radiodiagnosis in the Main hospital and at Radiodiagnosis sections at the Dr B.R Ambedkar Institute Rotary Cancer hospital, Dr Rajendra Prasad Centre for ophthalmology, and at Jai Prakash Narayan Apex trauma Centre. The department runs three year post-graduate program (MD); three Fellowship courses (in GI radiology, Thoracic radiology & Pediatric radiology) of one year each and a three year B.Sc (Hons.) MTR (Medical Technology in Radiography) course in radiography.
The department has the following strength of staff
| Main | Dr B.R Ambedkar Institute Rotary Cancer hospital | Dr Rajendra Prasad Centre for ophthalmology | Jai Prakash Narayan Apex trauma Centre | |
|---|---|---|---|---|
| Faculty | 13 | 4 | 1 | 2 |
| Scientist | 1 | - | - | - |
| Senior residents | 31 Main + 3 NMR + 8 Surgical block + 1 Plastic & Burn | 5 BRIRCH+ 4 for NCI Jhajjar | 1 | 20 |
| Junior residents | 25 | - | - | - |
| Radiographers | 64 | 16 | 2 | 30 |
| B.Sc. MTR students | 29 | - | - | - |






Computed Tomography (CT): Multi Slice CT : Three
One 256 slice dual source Dual Energy Scanner, one 128 slice CT scanner, one 256 slice single
source dual energy CT is in the process of installation
Magnetic Resonance Imaging (MRI) : One 1.5 T MR Scanner
Beside these there are two 3T scanners and one 1.5 T MR Scanner in the Department of NMR which are also accessible to Department of Radiodiagnosis on a sharing basis
Diagnostic Radiography : Nine flat panel Digital Radiography units
Mammography : One flat panel high end 3D Digital mammography with Tomosynthesis
One prone table breast biopsy unit
Ultrasound : Twenty high end ultrasound colour Doppler machines (with few having capability for shear wave elastography and Contrast Enhanced Ultrasound)
Fluoroscopy units : Four units -
Two digital flat panel radiography cum fluoroscopy units, one flat panel over couch fluoroscopy unit and one under couch fluoroscopy unit under installation
C arm fluoroscopy : oneflat panel unit
Digital Subtraction Angiography : Two high end Flat panel Digital Subtraction Angiography units
Radiofrequency Ablation (Bipolar) unit : one
Laser Ablation unit : one
Portable Radiography units : 14 (of which 8 are flat panel digital radiography units, 2 are digital with in-built CR system and 4 are conventional portable radiography units.
The department is equipped with PACS and RIS which networks all the imaging modalities for a smooth workflow. Two film digitizers are installed in the department.
| Sr. No. | Equipment | Main Department | BRA, IRCH | JPN Trauma Centre | RPC |
|---|---|---|---|---|---|
| 1 | X-Ray Machines | 9 | 1 | 2 | 1 |
| 2 | Mammography | 1 | 1 | - | - |
| 3 | Fluoroscopy | 4 | 1 | 1 | - |
| 4 | C arm digital flat panel unit | 1 | - | - | - |
| 5 | Ultrasound | 20 | 2 | 3 | 1 |
| 6 | CT Scan | 2+1(under installation) | 1 | 2 | 1 |
| 7 | MRI | 1 (+ 2 at NMR) =3 | - | 1 | - |
| 8 | DSA | 2 | - | 1 | - |
| 9 | RFA | 1 | - | - | - |
| 10 | Portable X-Ray | 14 | 4 | 7 | - |
| 11 | Portable Ultrasound | 4 | 2 | 1 | - |
| S.No. | |
|---|---|
| 1 | Mr. Ankit Roy Choudhary, 2018 |
| 2 | Ms. Isha Rishi, 2018 |
| 3 | Ms. Kanika, 2018 [Currently: PhD student, Dept of Reproductive Biology, AIIMS, New Delhi] |
| 4 | Ms. Priyanka Nagar, 2018 [Currently: PhD student, Jawaharlal Nehru University, New Delhi] |
| 5 | Mr. Abhishek Singh Yadav, 2019 |
| 6 | Mr. Aiyush Sharma, 2019 |
| 7 | Mr. Jitendar Kumar, 2019 |
| 8 | Ms. Ranjana Rana, 2019 [Currently: PhD student, Dept of Reproductive Biology, AIIMS, New Delhi] |
| 9 | Ms. Shaleena Minz, 2019 |
| 10 | Mr. A. Muninagesh, 2020 [Currently: PhD student, Dept of Reproductive Biology, AIIMS, New Delhi] |
| 11 | Mr. J. Moses Azaraiah, 2020 [Currently: PhD student, Dept of Reproductive Biology, AIIMS, New Delhi] |
| 12 | Mr. Joginder, 2020 |
| 13 | Ms. Nivita Gugnani, 2020 |
| 14 | Ms. Aaluri Chandini, 2021 |
| 15 | Ms. Ayushi Goel, 2021 |
| 16 | Ms. Surbhi Jain, 2021 |
| 17 | Ms. Kajal Sihag, 2021 [Currently: PhD student, Dept of Reproductive Biology, AIIMS, New Delhi] |
| 18 | Ms. Afsa Junaid, 2021 |
| 19 | Ms. Yashaswi Sharma, 2021 |
Publications in journals - 10
Chapters in books and monographs - 01
Polycystic ovarian disease
Premature ovarian failure
Hyperprolactinemia
Gonadal Failure (hyper, hypo and eu-gonadotropic)
Male & female infertility
Genomics & Epigenomics of infertility and how to predict as well as prevent
Recurrent in-vitro fertilization failure
Role of thyroid hormone on Leydig cell function
Sertoli cell only syndrome
Testicular Maturation Arrest
Biology of Placenta-related pregnancy complications
Insulin Signaling in Reproductive Aging
HDACi in Aging
Oxidative stress & RNA binding Proteins in early embryo development
Biology of skewed sex ratio
Sexual dysfunction
Phenotypic heterogeneity in congenital malformation
Microdeletion syndrome
Herbal extracts on prostate cancer
Flavonoids on prostate epithelial cells
Prostate cancer & BPH
For details vide web pages of individual faculty and scientists of department
Refer to webpage of individual faculty & scientists of the department
Blood tests for hormones, cancer markers etc.
Semen analysis
Molecular Cytogenetic analysis
| Sample Collection : | Room No. 2090, Teaching Block Cross Wing |
| Timing : | Monday – Friday: 8.30 – 11.00 AM (for Hormones) 8.30 AM – 7.00 PM (for Cancer markers & other tests) Saturday: 8.30 – 11.00 AM (for Hormones) 8.30 A.M. - 3.30 P.M. (for Cancer markers & other tests) |
| Sample Collection : | New RAK OPD (Basement) |
| Timing : | Monday – Friday: 8.00 – 11.00 AM (for Hormones) 8.00 AM – 7.00 PM (for Cancer markers & other tests) Saturday: 8.00 – 11.00 AM (for Hormones) 8.00 A.M. - 3.30 P.M. (for Cancer markers & other tests) |
| Payment : | Payment receipt should accompany the test requisition form at the time of submitting the blood sample. Money should be deposited at: Rajkumari Amrit Kaur OPD, Ground Floor OR Central Admission Counter (near Railway reservation counter at AIIMS Gate No.1) |
| EHS Patients : | Should bring OPD Card and EHS Book |
| Reports : | 1. Can be collected from respective OPD 2. Can be printed from ORS patient portal (https://ors.gov.in) under Lab Reports 3. In case of any difficulty, duplicate report can be collected from Room no. 5010, 5th Floor, Teaching Block |
| For any other clarifications or details contact : 011-26594338 / 4276 |
| OR contact : |
| Dr. Pradeep K. Chaturvedi |
| 26594363, 26593304 |
| E-mail: pkchat@gmail.com |
Andrology Lab
Complete Semen Analysis (count, motility, vitality, morphology), Fructose qualitative assessment
| Sample Collection : | Room No. 2090-C, 2nd Floor, Teaching Block |
| Timing : | All days (with appointment) 9.30 – 11.00 AM |
| Payment : | No charges |
| Reports : | Reports can be collected from lab after 3-5 days |
| For any other clarifications or details contact : |
| Dr. Mona Sharma |
| 26594166 |
| E-mail: dr.mona18sharma@gmail.com |
Molecular Cytogenetics Lab
Fluorescent In-Situ Hybridization (FISH) and STR/microsatellite PCR
| Test | Sample requirement | Approximate turnaround time | Cost (Rs.) |
Fluorescent In-Situ Hybridization (FISH) Microdeletion FISH
Sex Chromosome FISH Post bone marrow transplantation (sex mismatched): engraftment status XX or XY disorder of sex development (Intersex) SRY gene FISH Intersex
Aneuploidy FISH (preimplantation, prenatal, postnatal & oncologic application) Chromosome 1, 2, 3, 4, 6, 7, 8, 9, 10, 11, 12, 14/22, 15, 16, 17, 18, 20, 22, X, Y
Oncological FISH RB1, cMYC, HER2, ABL, BCR, BCL2, IGH, PML1, RARA, ETO, AML1, MYH11, etc |
1 ml Heparinized & 1 ml EDTA blood in sterile condition
|
Within one month |
2000 2000 2000 2000 3000 2000 2000 2000 2000
2000 |
| STR/microsatellite PCR | All microdeletions All aneuploidies | 1-2 days | Free |
| Sample Collection : | Room No. 2100, 2nd Floor, Teaching Block |
| Sample requirement, Storage & Transportation : | For FISH 1 ml Heparinized & 1 ml EDTA blood in sterile condition Transport to laboratory within 24 hours Storage temperature & transportation temperature (if more than 6 hours) preferably between 5-10*C Semen/mouth wash/urine samples are preferred to be collected on site (laboratory) For STR/microsatellite PCR 2 ml EDTA blood (patient along with parents) |
| Timing : | Monday – Saturday |
| Payment : | Charges as given above |
| Reports : | As given above |
| For any other clarifications or details contact : |
| Dr. Ashutosh Halder/ Dr. Manish Jain |
| 011-26594211 / 26594386 |
| E-mail: ashutoshhalder@gmail.com |
1. PhD
2. Postgraduate:
M.Sc. (Reproductive Biology & Clinical Embryology)
Part of Developmental Biology module for MSc Biotechnology students
Rotation for MD Lab Medicine students
Rotation for MD Biochemistry students
Andrology lab trainings to DM Reproductive Medicine students
3. Continuing Medical Education:
Organize National Workshop on Molecular Cytogenetics
1. PhD in Reproductive Biology
Twice yearly: Session starts January and July
2. MSc in Reproductive Biology and Clinical Embryology
Once Yearly: Session starts August
3. Short & Long term Training
Short Term
Short-term (one to three month/s) training
on Molecular Cytogenetics,
Radioimmunoassay/other hormone assay,
Cell culture system based biochemical or
molecular study, etc
The department has a fully functional clinical immunology laboratory catering to the entire AIIMS, New Delhi. Several immunological investigations e.g. RF, ANA (IIF), ENA Profile, C3, C4, ANCA (IIF), ASMA, Anti-LKM, Immunoglobulins, Anti-cardiolipin antibodies, Crystal Studies etc.) are routinely done. Lab is currently equipped with following techniques :- ELISA, IIF, LIA, LATEX agglutination, Nail Fold Capillaroscopy and Polarised Microscopy.
Department is also contributing to human resource in rheumatology by training physicians for various hospitals in India. Also, medical doctors from various countries have been provided training in rheumatology.
The faculty and the residents see nearly 100-120 monthly consultations and referrals from different departments of AIIMS, New Delhi.
The department has a fully functional six bedded day care centre which provides facilities for procedures like infusions of biologics and other affects like cyclophosphamide, intra-articular injections and aspirations and other diagnostic procedures like minor salivary gland biopsy, nerve biopsy, skin biopsy and muscle biopsy. Department also run a musculoskeletal ultrasound service and have been performing 150 to 200 scans and ultrasound guided procedures per month. Rheumatology day care is the best example of providing state of art patient care services in an economical way under resource constraint setting.
The department currently does not have a separate ward and provides inpatient services in collaboration with unit 3 of Department of Medicine.
Outpatient services are delivered in Rheumatology OPD every Tuesday/Friday. In addition, a Rheumatology Clinic is being run every Thursday (2pm onwards).
The department currently has a three years non-academic course for senior residents six months non-academic course for junior residents. It soon plans to start three years academic course ‘DM’ in rheumatology once indoor beds are made available to the department.
The knowledge about rheumatological diseases is scarce in the general public and majority of the patients are not able to recognize its signs and symptoms until the disease is advanced leading to significant morbidity. In an effort to increase general public awareness, the department organizes various public health lectures, distributes bilingual pocket booklets on various rheumatological diseases explaining the general population its signs and symptoms and steps for better management. The faculty frequently participates in programmes on radio/television about the above-mentioned aspects of diseases.
The Department of Rheumatology, earlier functional as a Clinical Immunology & Rheumatology division under Department of Medicine was established as a separate super speciality department on 7 August 2015. Prof. (Dr.) Uma Kumar is the founder Head of this department. Currently, department has five faculty members including Prof. Uma Kumar, six senior residents, two junior residents (non-academic). The department is providing outpatient services, state of the art Rheumatology Day Care facility for intravenous infusions (biological agent, chemotherapeutic drugs & steroid pulse etc), interventions (joint injections, various biopsies) and musculoskeletal ultrasound. The department has a fully functional Clinical Immunology laboratory where investigations for immunological and rheumatological diseases are done. Approximately 50000 lab tests are performed each year.
The department has made significant progress since its inception. The department has provided high quality outpatient services to nearly 40000 patients in last one year. Patients with wide array of diseases ranging from various forms of inflammatory arthritis like rheumatoid arthritis, systemic lupus erythematosus, scleroderma, vasculitis, inflammatory myositis etc. attend outpatient clinic.
The department is actively involved in creation of public awareness about the rheumatological diseases. Various public health lectures, and audio/video programmes are conducted every year explaining to the patients about the diseases and its management. In addition, department frequently organizes CMEs, and Updates for physicians. Several awareness booklets on rheumatic disorders are also distributed to public and patients time to time.
OPD workflow
Out Patient Services
The Surgery OPD is located on the ground floor of the Surgery Block, Majid Moth Campus, AIIMS New Delhi.
The registration for morning OPD is done between 8.00 a.m. to 11.00 a.m. daily.
| Name of Consultant | OPD Days |
|---|---|
| Unit I | |
| Prof. Sunil Chumber Dr. Piyush Ranjan Dr. Yashwant Rathore Dr. Ankita Singh Dr. Devender Singh | Every Monday |
| Unit II | |
| Prof. Sandeep Aggarwal Dr. Manjunath Maruti Pol Dr. Aditya Kumar Dr. Washim Firoz Khan Dr. Aditya Baksi | Every Tuesday |
| Unit III | |
| Prof. Rajinder Parshad Prof. Hemanga K. Bhattacharjee Dr. Mohit Joshi Dr. Suhani | Every Wednesday |
| Unit IV | |
| Prof. V. Seenu Dr. Asuri Krishna Dr. Brijesh Kumar Singh Dr. Sushant Soren | Every Thursday |
| Unit V | |
| Prof. V. K. Bansal Dr. Om Prakash Dr. Sanjeet Kumar Rai Dr. Geeta Prasad Dr. Arun Anand | Every Friday |
| Unit VI | |
| Prof. Anita Dhar Dr. Kamal Kataria Dr. Nelson T Dr. Uttam Kumar Thakur | Every Saturday |
The afternoon clinics are located on the ground floor of the Surgery Block, Majid Moth Campus, AIIMS New Delhi.
The registration for afternoon clinics is done between 1:30 p.m to 2:30 p.m.
| Days | Clinics | Name of Faculty | Clinic Room No. |
|---|---|---|---|
| Surgery Unit - I | |||
| Every Wednesday Afternoon | Male Health Clinic | Dr. Sunil Chumber | Room No: 18 |
| Endocrine Surgery Clinic | Dr. Piyush Ranjan | Room No: 3, 4 | |
| GI, GB, Haematology & Hernia Clinic | Dr. Yashwant Rathore | Room No: 1, 2 | |
| Stoma, Hernia & Coloproctology Clinic | Dr. Devender Singh | Room No: 17 | |
| Benign Breast Disease | Dr. Ankita Singh | Room No: 15 | |
| Breast Cancer Clinic | Room No: 16 | ||
| Surgery Unit-II | |||
| Every Thursday Afternoon | Bariatric Clinic | Prof. Sandeep Aggarwal Dr. Manjunath Maruti Pol Dr. Aditya Kumar Dr. Washim Firoz Khan Dr. Aditya Baksi | Room No: 16 |
| Follow Up Clinic | Room No: 17 | ||
| Surgery Unit-III | |||
| Every Monday Afternoon | Endocrine Surgery Clinic | Dr. Suhani | Room No: 15 |
| Every Friday Afternoon | Breast Cancer Clinic | Prof. Rajinder Parshad Dr. Suhani Dr. Mohit Joshi | Room No: 15, 16, 17 |
| Follow-Up Clinic | Prof. Rajinder Parshad Prof. Hemanga K. Bhattacharjee Dr. Mohit Joshi Dr. Suhani | Room No: 3, 18 | |
| Pectus and Chest Wall Clinic | Dr. Rajinder Parshad Dr. Mohit Joshi Prof. Hemanga K. Bhattacharjee | Room No: 1 | |
| Cancer Genetic Clinic | Dr. Rajinder Parshad Dr. Suhani | Room No: 2 | |
| Surgery Unit-IV | |||
| Every Thursday Afternoon | Breast Cancer Clinic | Prof. V. Seenu Dr. Asuri Krishna Dr. Brijesh Kumar Singh Dr. Sushant Soren | Room No: 1, 2 |
| Follow Up Clinic | Room No: 4 | ||
| Surgery Unit-V | |||
| Every Monday Afternoon | Breast Clinic | Room No: 17, 18 | |
| HPB Clinic and Follow-up Clinic | Prof. V. K. Bansal Dr. Om Prakash Dr. Sanjeet Kumar Rai Dr. Geeta Prasad Dr. Arun Anand | Room No: 3, 4 | |
| Renal Transplant Surgery Clinic and Vascular Access Clinic | Room No: 1, 2 | ||
| Surgery Unit-VI | |||
| Every Tuesday Afternoon | Breast Cancer Clinic | Dr. Kamal Kataria | Room No: 3 |
| Benign Breast Disease | |||
| Endocrine Clinic | Dr. Kamal Kataria | Room No: 4 | |
| Vascular Clinic | Dr. Anita Dhar Dr. Uttam Kumar Thakur | Room No: 15 | |
| Hepatopancreatic Biliary (HPB) Clinic | Dr. Uttam Kumar Thakur | Room No: 16 | |
| Proctology Clinic | Dr. Nelson T. | Room No: 17 | |
| Hernia Clinic | Room No: 18 | ||
| Every Thursday Afternoon | Breast Cancer Clinic | Dr. Anita Dhar | Room No: 15 |
| Follow Up Clinic | Room No: 3 | ||
Year – 1961
Year – 1962
Year – 1963
Year - 1964
Year – 1965
Year – 1966
Year – 1967
Year – 1968
Year – 1969
Year – 1970
Year – 1971
Year – 1972
Year – 1973
Year – 1974
Year – 1975
Year - 1976
Year – 1977
Year – 1978
Year – 1979
Year - 1980
Year – 1981
Year – 1982
Year – 1983
Year - 1984
Year - 1985
Year – 1986
Year - 1987
Year – 1988
Year – 1989
Year – 1990
Year – 1991
Year – 1992
Year – 1993
Year – 1994
Year – 1995
Year – 1996
Year – 1997
Year – 1998
Year – 1999
Year – 2000
Year – 2001
Year – 2002
Year – 2003
Year – 2004
Year – 2005
Year – 2006
Year – 2007
Year – 2008
Year – 2009
Year – 2010
Year – 2011
Year – 2012
Year – 2013
Year – 2014
Year – 2015
Year – 2016
Year – 2017
Year – 2018
Year – 2019
Year – 2020
Year – 2021
Year – 2022
Ongoing
| S. No. | Title of the project |
|---|---|
| 1 | Identification of factors predictive for weight loss after Bariatric Surgery: Building a Model for improving outcomes and maintaining weight loss |
| 2 | An observational study to evaluate the role of impaired NAD+ biosynthesis in calf skeletal muscle dysfunction in people with peripheral arterial disease |
| 3 | Study of effectiveness of Maharishi Amrit Kalash on Breast cancer as adjunct therapy along with Neo Adjunct Chemotherapy: An open Randomized controlled clinical trial |
| 4 | VR assisted 3D endoscope for minimal access (laparoscopic) surgery |
| 5 | Study to evaluate the presence of SARS-Cov-2 in different body fluids in SARSCOV-2 positive/suspect patients undergoing laparoscopic, open surgery and endoscopic procedures |
| 6 | Study of Gut Microbiome in patients with gall bladder carcinoma - Intramural Project under AIIMS research grant |
| 7 | RNA-seq based case-control study to identify alternatively spliced events in colorectal adenocarcinoma- Bioinformatics and genomics-based study [2021-12417] |
| 8 | Metabolic resuscitation using early administration of ascorbic acid, thiamine and hydrocortisone in perioperative management of surgical patients with septic shock: A Randomized Controlled trial |
| 9 | Evaluation of adaptability of an indigenously developed low-cost light-weight polycentric polymeric knee joint (PPKJ) and its effect on quality of life and rehabilitation on post-traumatic transfemoral amputees |
| 11 | Development of TIRF based microscopic system with smartphone camera as a detector for autofluorescence dependent intraoperative identification of parathyroid tissue (AIIMS-IIT Collaborative project) |
| 12 | Development of aptamer-based assay for the diagnosis of breast tuberculosis (Breast TB), (AIIMS-THSTI collaborative project) |
| 13 | Study of heavy metals and trace elements (Arsenic, cadmium, chromium, and nickel, selenium, zinc, copper, lead, mercury, cobalt) in gall bladder cancer and cholelithiasis patients. |
| 14 | Study of heavy metals and trace elements (Arsenic, cadmium, chromium, and nickel, selenium, zinc, copper, lead, mercury, cobalt) in Breast cancer and Benign breast disease patients. |
| 15 | Clinical significance of Proteomics in liquid biopsy for Indian breast cancer women: An Exploratory study |
| 16 | To study the role of inflammatory markers in low pressure vs standard pressure laparoscopic cholecystectomy. RCT. |
| 17 | Role of heavy metals in breast cancer |
| 18 | Long Term Outcome of Patients with Walled off Necrosis/Pseudocyst of Pancreas in terms of Recurrence of Acute Pancreatitis, Fluid Collection and Functional Consequences following Internal Drainage by Laparoscopic or Endoscopic method |
| 19 | Prevalence of BRCA1/2 germ line mutation in young Indian Women with triple negative breast cancer |
| 20 | “-Solid Tumor Targeting Using Homing Peptides and Plasmonic Photothermal Technique” |
| 21 | To study the epidemiology of drowning, address the need, developing IEC material and imparting the related training to at-risk school students of schools in the vicinity of the Yamuna River at Delhi- Prospective, non-randomized, interventional study. |
| S. No. | Title of the project |
|---|---|
| 1 | A Label Extension, Single Arm Multicentric Phase III Study To Assess The Efficacy And Safety Of Approved Product Stempeucel® In Patients With Critical Limb Ischemia Due To Buerger’s Disease |
| 2 | Study of effectiveness of Maharishi Amrit Kalash on Breast cancer as adjunct therapy along with Neo Adjunct Chemotherapy: An open Randomized controlled cl |
| 3 | An observational study to evaluate the role of impaired NAD+ biosynthesis in calf skeletal muscle dysfunction in people with peripheral arterial disease |
| 4 | To check the feasibility of aortoplasty balloon catheter for endovascular occlusion of aorta- a cadaveric study |
| 5 | Comparision of wire-guided lumpectomy versus sonographic hematoma guided lumpectomy in management of nonpalpable breast cancers. (Intramural Project) |
| 6 | Development of aptamer-based assay for the diagnosis of breast tuberculosis (Breast TB), (AIIMS-THSTI collaborative project) |
| 7 | “Study of heavy metals and trace elements (Arsenic, cadmium, chromium, and nickel, selenium, zinc, copper, lead, mercury, lead, cobalt) in gall bladder cancer and cholelithiasis patients.” |
| 8 | “Study of heavy metals and trace elements (Arsenic, cadmium, chromium, and nickel, selenium, zinc, copper, lead, mercury, lead, cobalt) in Breast cancer and Benign breast disease patients.” |
| 9 | Clinical significance of Proteomics in liquid biopsy for Indian breast cancer women: An Exploratory study |
| 11 | To study the role of inflammatory markers in low pressure vs standard pressure laparoscopic cholecystectomy. RCT. |
| 12 | Development of aptamer based assay for the diagnosis of breast tuberculosis |
| 13 | Role of heavy metals in breast cancer. |
| 14 | Identification of factors predictive for weight loss after Bariatric Surgery: Building a Model for improving outcomes and maintaining weight loss |
| 15 | Transcendental meditation (TM) to reduce stress and enhance immunity of health care workers during COVID-19 pandemic: a randomized trial (TURMERIC trial) |
| 16 | Study to evaluate the presence of SARS-CoV-2 in different body fluids in SARS-CoV-2 positive/suspect patients undergoing laparoscopic, open surgery, and endoscopic procedures |
| 17 | Study of Gut Microbiome in patients with gall bladder carcinoma |
| 18 | Long-term outcome of patients with Walled off Necrosis/Pseudocyst of Pancreas in terms of recurrence of acute pancreatitis, fluid collection, and functional consequences following internal drainage by laparoscopic or endoscopic method |
| 19 | Prevalence of BRCA1/2 germline mutation in young Indian women with triple-negative breast cancer |
| 20 | RNA-seq based case-control study to identify alternatively spliced events in colorectal adenocarcinoma - Bioinformatics and genomics based study [2021-12417] |
| 21 | Metabolic resuscitation using early administration of ascorbic acid, thiamine, and hydrocortisone in perioperative management of surgical patients with septic shock: A randomized controlled trial. |
| S.N | Title of the project |
|---|---|
| 1 | As Co-investigator "Perioperative blood glucose variability in non-diabetic patients with peritonitis undergoing emergency laparotomy: A propesctive observational study, Dr. Souwik, Deptt of Anesthesia, Institute Research Grants Rs. 5 laksh (Co-Inv, Dr. V.K. Bansal) |
| 2 | An Ambispective study to evaluate the outcomes of living kidney donors left with multiple renal arteries. |
| 3 | Follow-up Study to Evaluate Correlation of Imaging and Operative findings with Clinical and Biochemical Outcome in Patients with Primary Hyperparathyroidism. |
| 4 | Indocyanine Green Fluorescence Imaging for Identifying and Assessing the Perfusion of Parathyroid Glands During Thyroid Surgery - A Pilot Study. |
| 5 | Incidence of postoperative hypocalcemia after Indocyanine Green fluorescence guided vs. Conventional assessment of parathyroid function following total thyroidectomy - A Randomized Controlled Trial. |
| 6 | Comparison of Early outcomes of interrupted double 'x' sutures vs. continuous near far far near method for closure of abdominal wall incisions: A double-blinded randomized control trial. |
| 7 | Incidence of Postoperative and Long-Term Hypocalcemia After Indocyanine Green Fluorescence Guided vs. Conventional Assessment of Parathyroid Function Following Total Thyroidectomy - A Randomized Control Trial. |
| 8 | A study to quantify the burden of insulin resistance in breast cancer women and its relation with other known prognostic and predictive factors of breast cancer. |
| 9 | Long-term outcomes in breast cancer patients in terms of overall disease-free survival and locoregional recurrence (2 decades of surgical audit of breast cancer patients). |
| 10 | Surgical audit of Renal transplantation data of a single surgical unit over the last decade. |
| 11 | Three-Arm Randomized Comparison of Laparoscopic Peritoneal Dialysis Catheter Insertion With or Without Omentectomy Versus Conventional Open Peritoneal Dialysis Catheter Insertion in Chronic Kidney Disease Stage 5 Patients in Terms of Catheter Malfunction and Post-Operative Complications. |
| 12 | The Anatomical basis of the Deep Inferior Epigastric Artery Perforator Flap and the Internal Mammary Perforator Flap: a CT Angiographic and Cadaveric Study. |
| 13 | Affect of preoperative management on perioperative events in patients with neuroendocrine tumors of the adrenal medulla - an ambispective cohort study. |
| 14 | The anatomical basis of Thoracodorsal artery perforator flap, Lateral intercostal artery perforator flap, and Anterior intercostal artery perforator flap: CT angiographic and cadaveric study. |
| 15 | Outcomes of difficult laparoscopic cholecystectomy - a prospective observational study. |
| 16 | Twenty-year audit of breast cancer clinic. |
| 17 | BRCA mutation in young triple-negative breast cancer patients. |
| 18 | A randomized control trial comparing mesh fixation with penetrating fixation device versus fibrin sealant during laparoscopic repair of ventral hernia. |
| 19 | Evaluation of dual dye technique for sentinel lymph node biopsy in breast cancer: two-arm open-label parallel design non-inferiority randomized controlled trial. |
| 20 | To establish an algorithm for the management of axilla in patients with early operable breast cancer having clinically negative axilla. |
| 21 | Neoadjuvant chemotherapy with short-course radiotherapy for locally advanced rectal cancer: a pilot study. |
| 22 | Impact of transcendental meditation™ on acute and chronic stress among surgeons in training: an open-labeled randomized controlled trial. |
| 23 | Functional outcome of patients undergoing thoracic surgery for benign pulmonary and pleural diseases: an ambispective cohort study |
| 24 | A study to explore the role of gamma synuclein as a potential biomarker in breast cancer. |
| 25 | Assessing effectiveness of a video-based intervention administered across a virtual platform on the existing knowledge, attitude, and practices of breast cancer awareness and breast self-examination among literate women in the metropolitan city of Delhi: A quasi-experimental community-based interventional study |
| 26 | Outcomes following abdominal wall closure using MonoMax (poly 4 hydroxy butyrate) suture in emergency midline laparotomy: An ambispective study |
| 27 | Assessment of lateral thermal spread and tissue damage associated with the use of various electrosurgical devices |
| 28 | Assessment of transferability of skills acquired on 3D HD and 4K HD endovision system to 2D HD endovision system: An ex-vivo study |
| 29 | Assessment of workload and musculoskeletal symptoms among minimal access surgeons – A prospective study |
| 30 | Patient-reported outcome measures and objective assessment of achalasia cardia following Laparoscopic Heller’s myotomy and angle of His accentuation |
| 31 | Comparison of Quality of Life, cosmesis, and oncological outcomes of skin-sparing mastectomy with total breast reconstruction using autologous fat grafting versus skin-sparing mastectomy with silicone implant reconstruction versus breast conservative therapy among patients with early breast cancer: A randomized controlled study |
| 32 | A study to validate the accuracy of the AIIMS modification of Paddington score in diagnosing phyllodes tumours, followed by a randomized control trial to evaluate the safety and efficacy of 1CM versus 2CM resection margin in phyllodes tumors |
| 33 | Knowledge and attitudes towards genetic counselling and testing in health care professionals and breast cancer patients |
| 34 | A randomized control trial to evaluate the safety and efficacy of 1cm versus 2cm resection margin in Phyllodes tumours |
| 35 | Comparison of Quality of Life, cosmesis and oncological outcomes of Skin Sparing Mastectomy with total breast reconstruction using autologous fat grafting versus skin sparing mastectomy with silicone implant reconstruction versus Breast Conservative Therapy among patients with Early Breast Cancer: A Randomized controlled trial |
| 36 | Comparison of outcomes in patients with intraductal papilloma undergoing duct excision with 2.5 cm versus 5 cm length: A randomized controlled exploratory study |
| 37 | From RECIST to PERCIST: evolving considerations for PET response criteria in carcinoma breast |
| 38 | Validation of clinical examination with Doppler studies in the management of patients presenting with vascular disease: A Prospective study |
| 39 | Evaluation of role of platelet-rich plasma in healing of chronic diabetic and peripheral arterial disease ulcers as compared to standard medical care: a randomized controlled trial |
| 40 | Comparison of outcomes of Trans-oral vestibular and Axillo-breast approach for endoscopic hemithyroidectomy in patients with benign and indeterminate thyroid lesions- A randomized controlled trial |
| 41 | Role of indocyanine green in predicting limb perfusion in comparison to standard methods in cases of chronic limb-threatening ischemia in correlation with clinical progression |
| 42 | Identification of Sentinel Lymph node in Breast cancer by dual method both by fluorescence and methylene blue. As co PI |
| 43 | Use of fluorescence and hematoma-guided excision of the impalpable breast tumours as Co-PI |
| 44 | Comparison of quality of life between patients undergoing endoscopic thyroidectomy and conventional open thyroid surgery |
| 45 | Development of an aptamer-based assay for the diagnosis of breast tuberculosis (Breast TB) |
| 46 | Study of heavy metals and trace elements (arsenic, cadmium, chromium, nickel, selenium, zinc, copper, lead, mercury, cobalt) in gall bladder cancer and cholelithiasis patients |
| 47 | To record the long-term outcome of patients suffering from benign breast disease: an ambispective study |
| 48 | Impact of Transcendental Meditation (TM) on acute and chronic stress among surgeons in training: An open-labeled randomized controlled trial |
| 49 | Functional outcome of patients undergoing thoracic surgery for benign pulmonary and pleural diseases: An ambispective cohort study |
| 50 | Assessment of transferability of skills acquired on 3D HD and 4K HD endovision systems to 2D HD endovision system: An ex-vivo study |
| 51 | Outcome of abdominal wall closure using poly 4-hydroxy butyrate suture in emergency midline laparotomy: An ambispective study |
| 52 | Assessing the effectiveness of a video-based intervention administered across a virtual platform on the existing knowledge, attitude, and practices of breast cancer awareness and breast self-examination among literate women in the metropolitan city of Delhi: A quasi-experimental community-based interventional study |
| 53 | Assessment of lateral thermal spread and tissue damage associated with the use of various electrosurgical devices |
| 54 | Clinical applicability of whole-body low-dose CT scan for detecting bone metastases in breast cancer patients - a cross-sectional study |
| 55 | Comparison of 3D-CT volumetry and routine spirometry for prediction of postoperative pulmonary function in benign lung diseases |
| 56 | Knowledge and attitude towards genetic counseling and testing in hereditary breast cancer in health care professionals and breast cancer patients |
| 57 | Impact of intraoperative microbreaks on musculoskeletal symptoms and performance of surgical residents during minimal access surgical tasks in a simulated setting |
| 58 | Comparative analysis between different stage cancer patients to discover novel blood-based biomarkers for detection of early-stage breast cancer - A pilot study |
| 59 | A pilot study to compare interstitial multicatheter brachytherapy (IMB) versus volumetric modulated arc therapy (VMAT) for accelerated partial breast irradiation in early breast cancer: An adaptation, toxicity, and cosmesis comparison |
| 60 | Comparison of standard vs. low-pressure laparoscopic cholecystectomy under deep neuromuscular block: A randomized controlled trial |
| 61 | To study the clinical profile, investigations, and outcome of patients undergoing parathyroidectomy: A retrospective and prospective experience |
| 62 | To study the outcomes in patients with cholelithiasis following subtotal cholecystectomy |
| 63 | A RCT to assess the efficacy of using uniform umbilical hygiene preoperatively to reduce incidence of umbilical port site complications in patients undergoing laparoscopic cholecystectomy. |
| 64 | To study etiology, clinical presentation, and outcomes of patients with gastroduodenal perforation. |
| 65 | Correlation of pre and post-operative surgical findings with clinical course in patients undergoing early laparoscopic cholecystectomy for asymptomatic gallstone disease. |
| 66 | To compare inflammatory markers in low-pressure pneumoperitoneum with deep neuromuscular block vs. standard pressure pneumoperitoneum among patients undergoing laparoscopic cholecystectomy for GSD: A RCT. |
| 67 | Use of prophylactic steroid to prevent hypocalcemia in patients undergoing thyroidectomy. |
| 68 | Analysis of patterns of neck trauma and its outcomes at a level 1 trauma center: an ambispective observational study. |
| 69 | Fast-track emergency lap cholecystectomy vs. emergency laparoscopic cholecystectomy in index cases of acute calculus cholecystitis patients presenting to the emergency department – RCT. |
| 70 | To study causes of cancellation among patients scheduled for elective operations. |
| 71 | To assess the functional outcomes in patients undergoing standardized laparoscopic mesh repair in small and medium ventral midline hernias. |
| 72 | To assess the cost-effectiveness of standardized laparoscopic mesh repair in ventral hernia. |
| 73 | To study the complications of laparoscopic inguinal repair |
| 74 | Symptomatic outcomes in patients of asymptomatic gall stones after laparoscopic cholecystectomy |
| 75 | To study the concordance of TIRADS and the Bethesda System for reporting Thyroid Cytopathology with final histopathology in STN |
| 76 | To assess the functional outcomes in patients undergoing standardized mesh repair in small and medium ventral hernias |
| 77 | Telecommunication: An effective tool for early operative follow-up during the COVID-19 pandemic |
| 78 | Illness-Wellness Scale: A new grading system to assess the performance status of COVID or non-COVID patients |
| 79 | To study causes of cancellation among patients scheduled for elective operations |
| 80 | To assess the functional outcomes in patients undergoing standardized laparoscopic mesh repair in small and medium ventral midline hernias |
| 81 | To assess the cost-effectiveness of standardized laparoscopic mesh repair in ventral hernia |
| 82 | To study the complications of laparoscopic inguinal repair |
| 83 | Symptomatic outcomes in patients of asymptomatic gallstones after laparoscopic cholecystectomy |
| 84 | To study the concordance of TIRADS and the Bethesda System for reporting Thyroid Cytopathology with final histopathology in STN |
| 85 | To assess the functional outcomes in patients undergoing standardized mesh repair in small and medium ventral hernias |
| 86 | Telecommunication: An effective tool for early operative follow-up during the COVID pandemic |
| 87 | Illness Wellness Scale: A new grading system to assess the performance status of COVID or non-COVID patients |
| 88 | To study causes of cancellation among patients scheduled for elective operations |
| 89 | Comparison of mesotherapy (nonoperative) with surgery in management of superficial lipomas |
| 90 | Identification of dietary factors predicting weight loss after bariatric surgery |
| 91 | Psychosocial factors affecting post-bariatric surgery weight loss: A prospective observational study |
| 92 | Optimal timing (Early vs Delayed) of laparoscopic cholecystectomy after Endoscopic Retrograde Cholangiopancreatography for choledocholithiasis: A randomized control trial |
| 93 | To Study the Efficacy of Laparoscopically Delivered Transversus Abdominis Plane Block for Postoperative Pain Control in Laparoscopic Ventral Hernia Repair – A Placebo-Controlled Randomized Study |
| 94 | To compare the outcomes of Banded versus Non-Banded Bariatric Procedures - A Prospective Randomized Controlled Trial |
| 95 | To Evaluate and Compare Gastroesophageal Reflux After Antral Preserving and Antral Resecting Laparoscopic Sleeve Gastrectomy for Morbidly Obese Subjects: An Ambispective Study |
| 96 | Omega Loop Gastric Bypass (Mini Gastric Bypass) versus Roux-en-Y Gastric Bypass for the Resolution of Type-II Diabetes Mellitus in Obese Subjects: An Ambispective Study |
| 97 | Impact of Concomitant Hiatal Hernia Repair (HHR) on GERD-Q Score in Patients Undergoing Laparoscopic Sleeve Gastrectomy for Obesity: A Prospective Observational Study |
| 98 | Hem-O-Lok Versus Endoscopic Stapler for Securing Base of Appendix During Laparoscopic Appendectomy: An Exploratory Randomized Controlled Trial |
| 99 | To Compare Inflammatory Markers in Low-Pressure Pneumoperitoneum with Deep Neuromuscular Block Versus Standard Pressure Pneumoperitoneum Among Patients Undergoing Laparoscopic Cholecystectomy for Gallstone Disease: A Randomized Controlled Trial |
| 100 | Outcome of Abdominal Wall Closure Using Poly 4 Hydroxy Butyrate Suture in Emergency Midline Laparotomy: An Ambispective Study |
| 101 | Assessment of Transferability of Skills Acquired on 3D HD and 4K HD Endovision System to 2D HD Endovision System: An Ex-Vivo Study |
| 102 | Impact of Transcendental Meditation (TM) on Acute and Chronic Stress Among Surgeons in Training: An Open-Labeled Randomized Controlled Trial |
| 103 | Mesh fixation with penetrating fixation device versus fibrin sealant during laparoscopic repair of ventral hernia: A double-blind randomized control trial |
| 104 | Neoadjuvant Chemotherapy with Short Course Radiotherapy for Locally Advanced Rectal Cancer: A Pilot Study |
| 105 | Early Versus Delayed Laparoscopic Cholecystectomy in Moderate and Severe Acute Biliary Pancreatitis: A Randomized Controlled Trial (ELCAP Trial) |
| 106 | Questionnaire-Based Survey of Musculoskeletal Dysfunction among General Surgeons and Comparison of Muscle Activity and Fatigue among Expert and Novice Surgeons during Laparoscopic Surgery using Surface Electromyography |
| 107 | Comparison of Early Outcomes of Interrupted Double 'X' Suture vs Continuous Near-Far-Far-Near Method for Closure of Abdominal Wall Incisions: A Double-Blinded Randomized Control Trial |
| 108 | To study the usefulness of pre-operative USG-guided FNAC in avoiding radical surgery in patients with gallbladder wall thickness or polyp associated with gallstone disease |
| 109 | Effect of yoga therapy on quality of life in patients undergoing laparoscopic incisional and ventral hernia repair: A randomized control trial |
| 110 | Short-term and long-term outcomes following laparoscopic and open donor nephrectomy: An ambispective comparative study |
| 111 | Study to Evaluate the Predictors of Outcome in High-Grade Blunt Liver Trauma |
| 112 | To study the correlation between pre-operative pain threshold measured using Quantitative Sensory Testing with post-operative pain scores using Visual Analogue Score in patients with laparoscopic groin hernia repair – A case-control study |
| 123 | A prospective study to evaluate the restoration of abdominal wall dynamics in patients with incisional hernia following laparoscopic IPOM plus repair in comparison to healthy controls using surface EMG |
| 124 | Incidence of postoperative and long-term hypocalcemia after Indocyanine Green fluorescence-guided vs conventional assessment of parathyroid function following total thyroidectomy |
| 125 | Study to develop an objective scoring system to grade the difficulty of laparoscopic cholecystectomy |
| 126 | Long-term outcomes in breast cancer patients in terms of overall disease-free survival and locoregional recurrence (2 decades of surgical audit of breast cancer patients) |
| 127 | A study to quantify the burden of insulin resistance in breast cancer women and its relation with other known prognostic and predictive factors of breast cancer |
| 128 | Surgical audit of renal transplantation data of a single surgical unit over the last decade |
| 129 | Assessment of Amphiregulin and CRISPLD1 as visceral adipose tissue-derived modulators of cardiovascular health in obesity |
| 130 | Optimal timing (early vs delayed) of laparoscopic cholecystectomy after Endoscopic Retrograde Cholangiopancreatography (ERCP) for choledocholithiasis: A randomized controlled trial |
| 131 | To study the effectiveness of laparoscopically delivered transversus abdominis plane block for postoperative pain control in laparoscopic ventral hernia repair - a placebo-controlled randomized study |
| 132 | To determine the best non-invasive marker or a combination of them that correlates the most with liver biopsy in the extent of fibrosis in morbidly obese patients with non-alcoholic fatty liver disease undergoing bariatric surgery |
| 133 | A randomized controlled study to assess the efficacy of using uniform umbilical hygiene preoperatively to reduce the incidence of umbilical port site complications in patients undergoing laparoscopic cholecystectomy |
| 134 | Impact of Concomitant Hiatal Hernia Repair on GERD-Q Score in Patients Undergoing Laparoscopic Sleeve Gastrectomy for Obesity: A Prospective Observational Study. |
| 135 | Omega loop gastric bypass (mini gastric bypass) versus Roux-en-Y gastric bypass for resolution of type-II diabetes mellitus in obese subjects: A Prospective Randomized Controlled Trial. |
| 136 | Investigation of the involvement of plasma membrane ATP binding transporter A1 (ABCA1) mediated insulin resistance. |
| 137 | Molecular characterization of transfer RNA-derived RNA fragments and expression of mitochondrial fusion proteins in Non-Alcoholic Fatty Liver Disease. |
| 138 | Stapled versus concurrent stapled and hand-sewn anastomosis in small intestine surgery: An exploratory randomized controlled trial. |
| 139 | End-to-side versus side-to-side anastomosis with ligation of vein distal to anastomosis for proximal arteriovenous fistula surgery: An exploratory randomized controlled trial. |
| 140 | Polymeric clip versus endoscopic stapler for securing the base of the appendix during laparoscopic appendectomy: An exploratory randomized controlled trial. |
| SURGERY BLOCK, Beds Distribution | |
| Wards | No. Of Beds |
| A1 (Private ward) | 10 |
| A8 (Private Ward) | 10 |
| B1 | 39 |
| A2B2 | 55 |
| A3B3 | 55 |
| ICU | 12 |
| HDU | 12 |
| TICU | 10 |
| Isolation Ward | 6 |
| Total Beds | 209 |
Every Tuesday , 1st and 3rd Saturday - 9.00 a.m. onwards
Surgery Block , Room No. 1, Ground Floor.
Every Thursday, 2.00 pm Onwards
Room No. 17, Surgery Surgery Block , Ground Floor.
For Queries Contact: Ph. No: 011-26551795
Mobile: 8929638529, 9810834840 (Kindly call between 11.00 a.m. to 4.00 p.m. only)
Email: aiimsbariatric@gmail.com
Professor-In charge : Dr. Sandeep Aggarwal
Professor, Department of Surgical Disciplines
Fellows: Dr. Vitish Singla
Dietitian: Ms Richa Jaiswal
Coordinator: Mrs Rachna Chaudhary
Obesity is a major public health problem in India which is already known for the high prevalence of diabetes. Thus Diabesity (Obesity + Diabetes) requires concerted efforts for treatment. Besides diabetes, patients with severe obesity commonly have other related diseases like high blood pressure, deranged lipid profile, PCOD, Fatty liver (NAFLD), osteoarthritis, gastro-oesophageal reflux, obstructive sleep apnea and poor quality of life. Bariatric surgery is the most effective treatment for such patients that provides long term weight loss and resolution/improvement of these obesity related diseases.
A specialised bariatric surgery program has been in operation at AIIMS since 2008 with the objective to provide high quality, safe and affordable surgical treatment for weight loss to patients with severe obesity. Prof. Aggarwal is considered as one of the pioneers of bariatric surgery in India and is vastly experienced in this field. More than 1000 surgeries have been conducted at AIIMS with excellent results. AIIMS, New Delhi is also one of the few centres in the country where high quality research in bariatric surgery is conducted.
http://www.ncbi.nlm.nih.gov/sites/myncbi/1bu6cqctzJLkT/bibliography/42715046/public/?sort=date&direction=descending
The decision of undergoing bariatric surgery is often a difficult one for patients and their relatives. In the Bariatric Surgery Clinic, a specialised team of doctors and dietician offer detailed explanation of the various treatment options for weight loss including bariatric surgery procedures and their pros and cons. This specialty clinic provides an opportunity for the patients to clarify all their doubts and reach an informed decision An experienced Program Coordinator is also present to facilitate further evaluation and consultations with other departments. The clinic also provides a unique opportunity to newly registered patients to interact with the ones who have already experienced bariatric surgery and find out more about the quality of life after such surgery. All attempts are made to make the procedure patient friendly.
Bariatric surgery requires lifelong follow up. The operated patients are actively followed and reminders are sent to them to attend the clinic The team has a specialist dietician to address the dietary issues of patients before and after surgery, which are as important as the surgery itself.
The Bariatric Surgery Clinic of AIIMS operates every Thursday at 2 pm in Room no.17, Ground floor Surgery Block.
Instagram Link
https://instagram.com/aiims_bariatric?igshid=MzNlNGNkZWQ4Mg==
Facebook Link
Log in to Facebook
https://www.facebook.com/groups/896967914895011/?mibextid=NSMWBT
OUTPATIENT SERVICES
Morning OPD Services :
The Surgery OPD is located on the ground floor of the Surgery Block, Majid Moth Campus, AIIMS New Delhi.
The registration for morning OPD is done between 8.00 a.m. to 11.00 a.m. daily.
| Name of Consultant | OPD Days |
|---|---|
| Unit I | |
| Prof. Sunil Chumber Dr. Piyush Ranjan Dr. Yashwant Rathore Dr. Ankita Singh Dr. Devender Singh | Every Monday |
| Unit II | |
| Prof. Sandeep Aggarwal Dr. Manjunath Maruti Pol Dr. Washim Firoz Khan Dr. Aditya Baksi | Every Tuesday |
| Unit III | |
| Prof. Rajinder Parshad Dr. Mohit Joshi Dr. Suhani Dr. Aditya Kumar | Every Wednesday |
| Unit IV | |
| Dr. Asuri Krishna Dr. Brijesh Kumar Singh Dr. Sushant Soren | Every Thursday |
| Unit V | |
| Prof. V. K. Bansal Dr. Om Prakash Dr. Sanjeet Kumar Rai Dr. Geeta Prasad Dr. Arun Anand | Every Friday |
| Unit VI | |
| Prof. Anita Dhar Dr. Kamal Kataria Dr. Nelson T Dr. Uttam Kumar Thakur | Every Saturday |
Afternoon specialty clinics:
The afternoon clinics are located on the ground floor of the Surgery Block, Majid Moth Campus, AIIMS New Delhi.
The registration for afternoon clinics is done between 1:30 p.m to 2:30 p.m.
| Days | Clinics | Name of Faculty | Clinic Room No. |
|---|---|---|---|
| Surgery Unit - I | |||
| Every Wednesday Afternoon | Male Health Clinic | Dr. Sunil Chumber | Room No: 18 |
| Endocrine Surgery Clinic | Dr. Piyush Ranjan | Room No: 3, 4 | |
| GI, GB, Haematology & Hernia Clinic | Dr. Yashwant Rathore | Room No: 1, 2 | |
| Stoma, Hernia & Coloproctology Clinic | Dr. Devender Singh | Room No: 17 | |
| Benign Breast Disease | Dr. Ankita Singh | Room No: 15 | |
| Breast Cancer Clinic | Room No: 16 | ||
| Surgery Unit-II | |||
| Every Thursday Afternoon | Bariatric Clinic | Prof. Sandeep Aggarwal Dr. Manjunath Maruti Pol Dr. Aditya Kumar Dr. Washim Firoz Khan Dr. Aditya Baksi | Room No: 16 |
| Follow Up Clinic | Room No: 17 | ||
| Surgery Unit-III | |||
| Every Monday Afternoon | Endocrine Surgery Clinic | Dr. Suhani | Room No: 15 |
| Every Friday Afternoon | Breast Cancer Clinic | Prof. Rajinder Parshad Dr. Suhani Dr. Mohit Joshi | Room No: 15, 16, 17 |
| Follow-Up Clinic | Prof. Rajinder Parshad Prof. Hemanga K. Bhattacharjee Dr. Mohit Joshi Dr. Suhani | Room No: 3, 18 | |
| Pectus and Chest Wall Clinic | Dr. Rajinder Parshad Dr. Mohit Joshi Prof. Hemanga K. Bhattacharjee | Room No: 1 | |
| Cancer Genetic Clinic | Dr. Rajinder Parshad Dr. Suhani | Room No: 2 | |
| Surgery Unit-IV | |||
| Every Thursday Afternoon | Breast Cancer Clinic | Prof. V. Seenu Dr. Asuri Krishna Dr. Brijesh Kumar Singh Dr. Sushant Soren | Room No: 1, 2 |
| Follow Up Clinic | Room No: 4 | ||
| Surgery Unit-V | |||
| Every Monday Afternoon | Breast Clinic | Room No: 17, 18 | |
| HPB Clinic and Follow-up Clinic | Prof. V. K. Bansal Dr. Om Prakash Dr. Sanjeet Kumar Rai Dr. Geeta Prasad Dr. Arun Anand | Room No: 3, 4 | |
| Renal Transplant Surgery Clinic and Vascular Access Clinic | Room No: 1, 2 | ||
| Surgery Unit-VI | |||
| Every Tuesday Afternoon | Breast Cancer Clinic | Dr. Kamal Kataria | Room No: 3 |
| Benign Breast Disease | |||
| Endocrine Clinic | Dr. Kamal Kataria | Room No: 4 | |
| Vascular Clinic | Dr. Anita Dhar Dr. Uttam Kumar Thakur | Room No: 15 | |
| Hepatopancreatic Biliary (HPB) Clinic | Dr. Uttam Kumar Thakur | Room No: 16 | |
| Proctology Clinic | Dr. Nelson T. | Room No: 17 | |
| Hernia Clinic | Room No: 18 | ||
| Every Thursday Afternoon | Breast Cancer Clinic | Dr. Anita Dhar | Room No: 15 |
| Follow Up Clinic | Room No: 3 | ||
Clinical classes & lectures are conducted for undergraduate students pursuing MBBS, B.SC Nursing & B.Sc OTT
Postgraduate and M. Ch Teaching Schedule:
Departmental seminar:
Multidisciplinary meets:
Other academics: The following programs are conducted every six months for newly inducted academic MS & M. Ch programs
Minimally invasive surgery training center
The “State of art” Minimally Invasive Surgery Training Centre provides courses in Operative Laparoscopy- Basic and Advanced, laparoscopic suturing skills and laparoscopic colorectal surgery. Training modules in Gynecology and Urology are being developed.
Postgraduates Residency Program
Junior Residents – 3 year Postgraduate training program leading on to degree of MS General Surgery
From General Surgery to Surgical Disciplines: A really short history!
The department of Surgical disciplines is located at the Surgery Block in the Masjd Moth campus of AIIMS, New Delhi. It has got outpatient services including minor operation theatre for day care procedures; inpatient services with 209 beds including general wards, private rooms, Intensive care unit, high dependency unit and transplant ICU; and twelve operation theatres. The department runs numerous sub-speciality clinics in the afternoon, that includes the breast cancer, benign breast diseases, endocrine surgery, renal transplant, hepato-pancreato-biliary surgery, hematology surgery, hernia, colo-proctology, pectus and chest wall clinic, cancer genetic clinic, vascular access clinic and stoma services. Each unit also runs a follow up clinic to provide dedicated care to post-operative patients.
The department has kept abreast with newer procedures and technologies in all its areas of expertise including breast, endocrine, colorectal, vascular, abdominal wall reconstruction, thoracic, bariatric surgery and minimal access surgery. The department has witnessed many firsts including renal transplant in the youngest patient in our country and has collaborated with the departments of CTVS, pulmonary medicine, cardiac-anesthesia for initiating lung transplant services. The faculty from the department have mentored initiation of various programs such as the sentinel lymph node biopsy (breast cancer), renal transplant and bariatric surgery programs in other premier medical institutions of the country.
The department is a research hub to various clinical trials, most of which get published in various peer reviewed journals of national and international importance. The faculty and residents regularly present their research work in all major national and international conferences, receiving awards for many of these. The residents of our department regularly receive travel grants and fellowships from various international scientific bodies to present their research work.
The department contributes to the teaching and training of MBBS graduates and interns, BSc nursing and OT technician students at our institute. The department conducts the MS General surgery, MCh in breast endocrine and general surgery, MCh minimal access and general surgery, Fellowships in bariatric surgery and renal transplant surgery. Regular conferences and training programs are initiated by the department to train surgeons from across the country and neighboring SAARC nations. Initiatives aimed at knowledge exchange with various international institutions of repute are undertaken by the department in the form of inviting faculty for lectures and inhouse training; as well as sending own faculty for short term fellowship/observership. The department faculty and residents have taken a lead to promote simulation-based training of various basic and advances surgical procedures. Medical graduates from various countries like Germany, France and surgeons from various countries like Bangladesh attend the department from time to time as observers.
The department has a large alumni base located across the globe. Many of their achievements have been commendable, adding to the pride and glory of our department.
PUBLICATIONS
Awards And Honours
Prof. N.K. Mehra received the chief of the Army Staff Award in February 2003. He was elected ‘International Councillor for the prestigeous International Histocompatibility Workshops. He continues to be the 'council member' of the International union of Immunological Societies (IUIS), Vice President of the Federation of Immunological Societies of Asia-Oceania (FIMSA) and as international councillor for the Australasian and South East Asian Tissue Typing Association (ASEATTA). He serves as the 'Honorary Consultant' to the Armed Forces Medical Services (AFMS), a trustee of the Immunology Foundation India, member of the DBT Task Force on Human Resource Development, and Human Genetics and Genome analysis, member of the Scientific Advisory Committee of JALMA Institute for Leprosy, Agra and Institute of Cytology and Preventive Oncology (ICPO), New Delhi, member of the Advisory Board of the Special Centre for Molecular Medicine, Jawaharlal Nehru University, New Delhi. member of the Board of Studies in Human Genetics of the Guru Nanak Dev University (GNDU), Amritsar, member of the ICMR Task Force on Immunology and of Project review committees of the ICMR, member of BHU Advisory Board for Molecular Genetics.
Prof. N.K. Mehra is on the Editorial Board of several prestigeous international journals: Microbes and Infection (Pasteur Institute, Paris), Tissue Antigens (Australia), Modern Rheumatology (Japan), International journal of Human Genetics (India), Journal of Clinical Immunology (USA). He was invited Guest speaker at the inaugural scientific meeting of the Allergy and Immunology Society of Srilanka (ALSSL) and at the Braunschweig Streptococcal colloquium, Branschweig, Germany. Professor Mehra is a member of the ethical, legal and social implications (ELSI) Committee of the Type 1 Diabetes Genetics consortium (T1DGC) of the NIH, Washington, USA. He was elected as Vice President of the Indian Society of Organ Transplantation (ISOT).
Dr. Uma Kanga (Scientist II) serves as the ‘Councillor’ for the Australasian and South East Asian Tissue Typing Association (ASEATTA).
Visiting Scientists
Dr Beverly Smith Keiling (USA), Dr Andreas D Keling (USA), Prof John Fahey (USA), Dr Jaspal Kaeda (UK), Dr Nikolai Petrovasky (Australia). Dr. Sudhir Gupta (USA), Dr Sophie Caillat Zucman (France).
Significant Events
The department has established several new technologies including ELISA-PRA and Flow-PRA, for assessment of graft dysfunction following renal and bone marrow transplantation. Chimerism analysis following BMT is also performed to assess the engraftment status of the recipient. These tests are very informative for post transplant monitoring. The services are offered for patient care purposes on routine basis.
Completed Projects
| Project Title | PI | Funding Agency | Total Funding | Duration |
|---|---|---|---|---|
| Advanced Program in Histocompatibility & Transplant Immunology (APHTI) | Prof N.K Mehra | DBT | 68.17 lacs | 2000-02 |
Ongoing Projects
| Project Title | Principal Investigator(s) | Funding Agency | Total Funding | Duration |
|---|---|---|---|---|
| Advanced Programming Histocompatibility & Transplantation Immunology (APHTI)- Contd for another 2 years | Prof N.k Mehra | DBT | 17.0 lacs | 2003-05 |
| Heterogenetiy of HLA-B27 gene in the Indian Population | Dr Uma Kanga & Prof. N.K Mehra | DBT | 16.01 lacs | 2000-03 |
| Human Genome Diversity: HLA studies | Prof . N.K Mehra | DBT | 30.56 lacs | 2001-04 |
| Immunogenetics of mycobacterial diseases : A 13th IHWC international study | Prof. N.K Mehra | ICMR | 18.35 lacs | 2001-04 |
| Evaluation of virus specific response in HIV-I subtype C infected individuals in North India (HLA Component) | Prof N.K Mehra | DBT | 15.5 lacs | 2002-04 |
| Molecular analysis of Cytokine gene polymorphism in leprosy | Prof. N.K Mehra | ICMR | 26.48 lacs | 2002-05 |
| Immunogenetic and Humoral Profile of Type 1 Diabetes in Indian Population | Prof . N.K Mehra | ICMR | 24 lacs | 2003-06 |
| Evaluation of immunological and cytopathological characteristics of first-degree relatives of patients of Juvenile autoimmune thyroiditis | Prof. N.K Mehra | INMAS | 3 lacs | 2003-05 |
Collaborative Research Projects
| Project Title | Name of collaborative department |
|---|---|
| Evaluation of virus specific response in HIV-I subtype C infected individuals in North India (HLA Component) | Dept. Of Microbiology,AIIMS |
| Immunogenetics and Humoral Profile of Type I Diabetes in Indian Population | Dept of Endocrinology AIIMS , Laboratoire d' Immunologie, INSERM ,Paris |
| Molecular Analysis of Cytokine gene polymorphism in leprosy | Centre JALMA Institute for Leprosy (JALMA) ,Agra |
| Evaluation of immunological and cytopathological characterstics of first degree relatives of patients of Juvenile sutoimmune throiditis' | Institute of Nuclear Medicine and Allied Sciences (INMAS) , New Delhi |
| An Evaluation of Immunological Predictors of Graft dysfunction following renal transplantation | Department of Nephrology and General Surgery, AIIMS |
HLA Matching
| Recipents | Donors | Total | |
|---|---|---|---|
| Renal Transplant Patients | 200 | 225 | 425 |
Bone Marrow Transplant Patients
| Leukimas | 62 | 260 | 322 |
| Aplastic Anemia | 20 | 65 | 85 |
| Thalassemias | 22 | 55 | 77 |
| Others | 23 | 60 | 83 |
| HLA-DNA Matching | 125 | 175 | 300 |
Cadaver Dover Organ Transplantation
| Cadaver Donor | 5 |
| Kidney Recipients | 30 |
| Heart Recipients | 5 |
Cross Match Tests
| Serology | 267 |
| Flowcytometry | 30 |
| Panel Reactive antibody (PRA) | 300 |
DIAGNOSTICS
| Spondyloarthropathies | 356 |
| Other disease | 85 |
New Technologies for Patient Services
| Flow PRA | 70 | ||
| ELISA PRA | 70 | ||
| Chimerism Studies in BMT | 85 | 90 | 175 |
Unrelated Donor Search for BMT
During the year, a total of 260 requests for search of unrelated HLA matched Donor from the 'Asian Indian Donor Marrow Registery ' for bone marrow transplantation(BMT) were received. These include 120 from USA , 65 from Europe , 27 from various Asian Countries and 48 from India.
The Department Provides short term training to junior residents of Pathology and Laboratory medicine and Senior Residents (DM Students ) of the Department of Hematology . Two Graduate and two postgraduate students from the various other departments of AIIMS received short term training . Four students from various universities , three doctors from other hospitals in Delhi and one doctor from Dhaka, Bangladesh attended 4-6 months training in the Laboratory techniques of HLA testing . During the year, three students completed their Ph.D and were awarded.
The Faculty of the department participated in and delivered 40 lectures in Continuing education programs , symposia, national and international conferences during the year. A quality control exercise for DNA typing of HLA genes has been started at the national level. The department provides a course on basic and clinical immunogenetics for M.Sc students of University of Delhi (South Campus) and Banaras Hindu University
Professor & Head
salilmitra2[at]gmail[dot]com
Addl. Professor
umakanga24[at]gmail[dot]com
Assoc. Professor
rakeshdeepak2008[at]gmail[dot]com
Scientist-II
sabkamalikek09[at]hotmail[dot]com
Scientist-II
latahp[at]gmail[dot]com
Scientist-I
goswamisanjeev[at]yahoo[dot]com
Scientist-I
raiprabin79[at]gmail[dot]com
For organizing blood donation camps and enquiry regarding blood donation:
Phone: 011-26593726
Email: aiimsbloodbank@gmail.com
For other enquires:
Phone: 011-26594438
International Voluntary Blood donor day 2019

National Voluntary Blood Donation Day 2019

Mega Blood Donation Camp 2020

Voluntary Convalescent plasma donation camp 2020




International Women's Day Celebration 2021

Mega Camp 2021

Platelet serology.
Use of RFID technology for better traceability of blood components.
Emphasis on evidence based blood usage using various point of care tests.
" There are future plans to provide Rheopheresis and Extracorporeal Photopheresis for the benefit of the patients"
A Voluntary Blood Donation Camp was held on 1st Feb.,2018 at "Rashtrapati Bhavan"
A Mega Blood Donation Camp `1.0' was held on 27.02.20 at JLN Auditorium, AIIMS participation from AIIMS Family & Armed Forces



A Voluntary Convalescent Plasma Donation Camp held on 19.07.20 in association with Delhi Police and this occasion was graced by Dr. Harsh Vardhan (Union Minister for Health & Family Welfare)



A Mega Bood Donation Camp2.0 was held on 03.02.21 at JLN Auditorium, AIIMS with participation from AIIMS Family and Armed Forces


International Women's Day celebrated on 08.03.21 by organizing a Voluntary Blood Donation Camp with participation NDRF, CRPF, RAK, College of nursing & AIIMS Family



74th Independence Day was celebrated undr the aegis of 'Azadi ka Amrit Mahotsav' voluntary blood donation camps organized in association with Central Industrial Security Force ( CISF) from 9th to 15 Aug.,2021



In continuation of 'Azadi ka Marit Mahotsav' a Mega Blood Donation Camp 3.0 was held 25.02.22 at Community Centre, AIIMS, with AIIMS Family & armed forces


Journal articles:
| SN | Authors | Title of presentation | Name of the conference | Date | City/Country |
|---|---|---|---|---|---|
| 1 | Chippy CS, Pandey HC, Seth T, Coshic P, Thapliyal RM, Sharma V | High dose IVIG & steroid for incompatible transfusion in a case with multiple alloantibody | HEAMATOCON 2019 60th Annual conference of Indian Society of Hematology and Blood Transfusion | November 7-10 2019 | New Delhi |
| 2. | Chippy CS, Pandey HC, Thapliyal RM, Sharma V | Pan reactivity in antibody screen and identification: is it justified to transfuse least incompatible red cells? | TRANSMEDCON 2019 - 8th Annual Conference of Indian Society of Transfusion Medicine | January 9 – 11, 2020 | Mumbai |
| 3. | Jain R, Kumar R, Coshic P, Pandey HC | Audit of Blood Transfusion Requisitions and role of implementation of blood bank software clinician module with resident training in improving transfusion practice at a tertiary care hospital | TRANSMEDCON 2019 - 8th Annual Conference of Indian Society of Transfusion Medicine | January 9 – 11, 2020 | Mumbai |
| 4. | Kumar R, pandey HC, Jain R, Coshic P | Retrospective comparison between non-treponemal and treponemal tests for screening of blood donors for syphilis and their correlation with donor history at tertiary care hospital. | TRANSMEDCON 2019 - 8th Annual Conference of Indian Society of Transfusion Medicine | January 9 – 11, 2020 | Mumbai |
| 5. | Meena SK, pandey HC, Thapliyal RM, Sharma V | Use of adsorption studies to detect underlying alloantibodies in AIHA Patients – experience of a referral center | TRANSMEDCON 2019 - 8th Annual Conference of Indian Society of Transfusion Medicine | January 9 – 11, 2020 | Mumbai |
| 6. | Pandey HC | Retrospective analysis of differences in red cell usage across different age groups and specialties in a tertiary care hospital | TRANSMEDCON 2019 - 8th Annual Conference of Indian Society of Transfusion Medicine | January 9 – 11, 2020 | Mumbai |
| 7. | C Chippy, H Pandey, M Mahapatra, R Chaurasia, G Patidar, P Coshic, R Thapliyal, V Sharma | Prospective observational study to find the prevalence & to serologically characterize autoimmune hemolytic anemia (AIHA) patients in a tertiary care teaching center | 36th International congress of ISBT | 12-16 DEC 2020 | Virtual Congress |
| 8. | H C Pandey, M Varghese, A Rana, R Kumar, P Kumar | Estimation of Incidence Rates & Residual Risks of HIV, HBV and HCV in Indian Settings Using NAT Window Period Yield Cases | 36th International congress of ISBT | 12-16 DEC 2020 | Virtual Congress |
| 9. | H C Pandey, P Coshic, R Kumar, N Jamshed, R Subramaniam | Evaluation of radio frequency identification technology for inventory management and patient identification before transfusion | 36th International congress of ISBT | 12-16 DEC 2020 | Virtual Congress |
| 11. | Mona Vijayaran, Mukul Aggarwal, Stitha P. Gudala, Jasmita Dass, Hem C. Pandey, Tulika Seth, Manoranjan Mahapatra | CMV infection in an infant presenting as steroid refractory AIHA | HEMATOCON2020 VIRTUAL | 21-22 NOV 2020 | Virtual Conference |
| SN | Title of talk | Name of the CME/conference | Date | City/Country (only if outside India) |
|---|---|---|---|---|
| 1. | Inventory Management During COVID-19 Pandemic | 45th Annual Conference, ISBTI, TRANSCON 2020 | 27th Feb 2021 | Chennai (Virtual event) |
| 2. | Pre-transfusion testing and compatibility issues | NHM “Training of Trainers for Strengthening of Blood Services and e-Rakt Kosh” for blood bank officials of Haryana | 18th March 2021 | Noida (Virtual event) |
| 3. | Advancing transfusion safety: evidence-based practices | Workshop on - Medication safety: Going beyond the “Rights” | 18th March 2021 | Noida (Virtual event) |
| 4. | Panel discussion on “False positivity, donor notification, donor re-entry and donor deferral & its impact” | CME on "Blood Safety and Quality: Infectious Diseases" | 5th April 2019 | New Delhi |
| 5. | Pre-transfusion testing and compatibility issues | NHM “Training of Trainers for Strengthening of Blood Services and e-Rakt Kosh” for blood bank officials of Madhya Pradesh | 13th June 2019 | Noida |
| 6. | Pre-transfusion testing and compatibility issues | NHM “Training of Trainers for Strengthening of Blood Services and e-Rakt Kosh” for blood bank officials of Telangana | 31st July 2019 | Noida |
| 7. | Pre-transfusion testing and compatibility issues | NHM “Training of Trainers for Strengthening of Blood Services and e-Rakt Kosh” for blood bank officials of Uttarakhand | 28th August 2019 | Noida |
| 8. | Significance of DAT in neonatal hyperbilirubinemia – interpretation and management | CME on “Advancements & New Horizons in Pediatric Transfusion Practices” | 31st August 2019 | New Delhi |
| 9. | Panel discussion on “Perinatal and neonatal transfusion practices” | CME on “Advancements & New Horizons in Pediatric Transfusion Practices” | 31st August 2019 | New Delhi |
| 10. | Panel Discussion on “National Blood and Plasma policy-Towards strengthening Transfusion services in India” | CME on ‘Introducing PBM- Transition from Product to Patient Centric Approach’ | 29-30th November 2019 | Jaipur |
| 11. | Pre-transfusion testing and compatibility issues | NHM “Training of Trainers for Strengthening of Blood Services and e-Rakt Kosh” for blood for blood bank officials of Telangana | 19th December 2019 | Noida |
| 12. | Pre-transfusion testing and compatibility issues | NHM “Training of Trainers for Strengthening of Blood Services and e-Rakt Kosh” for blood for blood bank officials of Maharashtra | 23rd January 2020 | Noida |
| 13. | Pre-transfusion testing and compatibility issues | NHM “Training of Trainers for Strengthening of Blood Services and e-Rakt Kosh” for blood for blood bank officials of Chhattisgarh | 4th February 2020 | Noida |
| 14. | Pre-transfusion testing and compatibility issues | NHM “Training of Trainers for Strengthening of Blood Services and e-Rakt Kosh” for blood for blood bank officials of Chhattisgarh | 3rd March 2020 | Noida |
| 15. | ABO blood group discrepancies and their resolution | Advanced Immunohematology Wet Workshop’ | 01.02.19 | New Delhi |
| 16. | Application of immunohematology tests in neonatology and pediatrics | “Hands-on Workshop” on “Basics in Immunohematology” | 02.02.19 | Noida |
| 17. | Problem Solving: Hemolytic disease of newborn (HDN) | “Hands-on Workshop” on “Basics in Immunohematology” | 02.02.19 | Noida |
| 18. | Weak D-Clinical Significance & Approach to Identification | CME cum workshop on “Advanced Immuno-hematology in Transfusion Medicine” | 15.02.19 | New Delhi |
Departmental projects:
Collaborative research projects with other departments
a. Ongoing:
b. Completed:
We also provide autologous PRP (platelet rich plasma) for orthopedic ailments such as arthritis, non-union of fracture and rotator cuff injury.
14th June 2018 – World Blood Donor Day Celebration
It is a well-known fact that blood cannot be manufactured. It is a living tissue with limited shelf life and availability and it can only be obtained through one's blood donation. To maintain the supply of safe blood, recruiting and retaining of voluntary non-remunerated blood donors is essential. For this purpose, Blood centre, Main Hospital of AIIMS New Delhi was always at the forefront in organizing voluntary blood donation camps. Events like "Nukkad Nakat, Cyclothon, Walkathon, Marathon, Flash Mob' were also organized to promote and propagate the message of Voluntary Blood Donation.
Our blood bank, is divided into various sections:
Committed to motivation, recruitment and retention of regular voluntary blood donors. Blood donations are taken both In-House (At Blood Centre) and at camps organized across NCR Region in association with various Government, Defence and Non-Government Organizations.
| Donor Services | ||
| Year | Total No of Units Collected | Total No of Camps Organized |
| 2018 | 33266 | 105 |
| 2019 | 51470 | 115 |
| 2020 | 38021 | 73 |
| 2021 | 36078 | 44 |
Timings for blood donation at Main Blood Bank :
| Monday to Friday | 9.00am to 5.30pm |
| Saturday | 9.00am-4.30pm |
Apheresis is separation of whole blood into components. It is done by a specialized equipment celled 'Cell Separators'. It has both blood donor and therapeutic applications.
Donor Applications:
Collection of Single Donor Apheresis Platelets (SDAP) which are used for transfusion in patients with thrombocytopenia and Source Plasma, which was used extensively in COVID-19 pandemic as Convalescent Plasma when collected from those recovered after SARS CoV-2 infection.
Therapeutic Applications:
Used for Therapeutic plasma Exchange (TPE) in various conditions, Lipid or LDL Aphereis in patients with pathological triglyceride levels, hematopoietic stem cell harvest for bone marrow transplant, red cell exchange and others.
Same therapeutic principle in used, often in addition with Glycosorb to bring down the level of ABO antibodies in patients due to receive ABO incompatible renal graft.


Blood collected from healthy donors is screened for infectious markers of Hepatitis B, Hepatitis C, HIV and Syphilis using Chemiluminiscence technique and Malariausing rapid antigen testing. These tests ensure high sensitivity and specificity and are as per the national mandatory guidelines. The donors testing reactive for any such viral markers are informed about the test results, counseled and referred for treatment.

We were one of the first institutes to start screening of all the collected blood units by nucleic acid testing using ID-NAT, which was inaugurated in 2008. During all these years, we have been upgrading the lab with newer technologies as and when they were available. This lab is fully automated with versatility, user-friendly software while minimizing lab space and minimizing operator interaction.


DrAmbikaNanu started component preparation in the 1970s. We are one of the transfusion services who are processing almost 100% of the collected blood into components. The following components are available round the clock:
Following modifications are also available on request of clinician:
Quality control of all blood products is done regularly as per the regulatory guidelines.



CrCross match and issue section deals with request for different blood components from clinicians. Packed red blood cells are issued after screening of irregular antibodies and a full cross match. Platelets and plasma components are issued as per patient requirement.The turn around time varies from less than 15 minutes for emergency transfusion to 4-5 hours for routine cases.

The department started performing antibody screening from the year of 1988. Currently, the laboratory is equipped with fully automated immunohematological analyzer for blood grouping and antibody screening which is based on Erythrocyte Magnetization technology, which is done for all the patients.The laboratory also performs various tests such as DCT, ICT, resolution of various blood group discrepancies, antibody identification, work up of transfusion reactions, saliva secretor status, adsorption, elution studies and immunohematological support in various clinical conditions such as AIHA patients, multi transfused patients and various solid organ and bone marrow patients.


| 1 | Blood Grouping |
| 2 | Direct Anti-Globulin Test (DAT) |
| 3 | Screening for red cell antibodies |
| 4 | Antenatal screening and titres for red cell antibodies |
| 5 | Identification of red cell allo-antibodies |
| 6 | Phenotyping for red cell antigens |
| 7 | Screening and titres for cold antibodies |
| 8 | ABO antibody titres |
| S.No | Name of Senior Resident | Joining Session |
|---|---|---|
| 1 | Dr Lubna Naseer | Jun-19 |
| 2 | Dr Aparna Krishna | Dec-19 |
| 3 | Dr Sapna Chopra | Jun-20 |
| 4 | Dr P Suganya | Jun-20 |
| 5 | Dr Vidushi Gupta | Jun-20 |
| 6 | Dr Kamini Gupta | Feb-21 |
| 7 | Dr Eswara P. Chennamsetty | Feb-21 |
| 8 | Dr Seema Kumari Meena | Feb-21 |
| 9 | Dr Ritesh | Feb-21 |
| 10 | Dr Chippy C S | Dec-22 |
| 11 | Dr Ritika Basnotra | Dec-22 |
The department of Transfusion Medicine (Blood bank), AIIMS, was established in the year 1996 under the able guidance of Dr Ambika Nanu, Dr. Usha Gupta, Dr Kabita Chatterjee. Dr Poonam Coshic is the CMO In Charge currently.





| 1 | Main blood bank | All the patients other than that in cardio, neuro science centre and trauma centre. | 2147 beds |
| 2 | Cardio and neuroscience centre blood bank | Cardio and neuro science centre. CLICK HERE | 222 beds |
| 3 | Trauma centre blood bank | Trauma centre. CLICK HERE | 215 beds |
Our motto is to provide adequate and timely supply of safe and quality blood and blood components, duly tested and free from transfusion-transmitted infections, in a timely manner to the right patient (RIGHT BLOOD, RIGHT TIME, RIGHT PATIENT).
We are gradually phasing out replacement donors and moving towards voluntary non-remunerated blood donation. We have striven hard to bring world class technologies to our institute for the operation of our blood transfusion services and ensured its functioning in an updated manner. Universal precautions are strictly adhered to, and the guidelines of Good Manufacturing Practices are followed in all the sections of blood banking
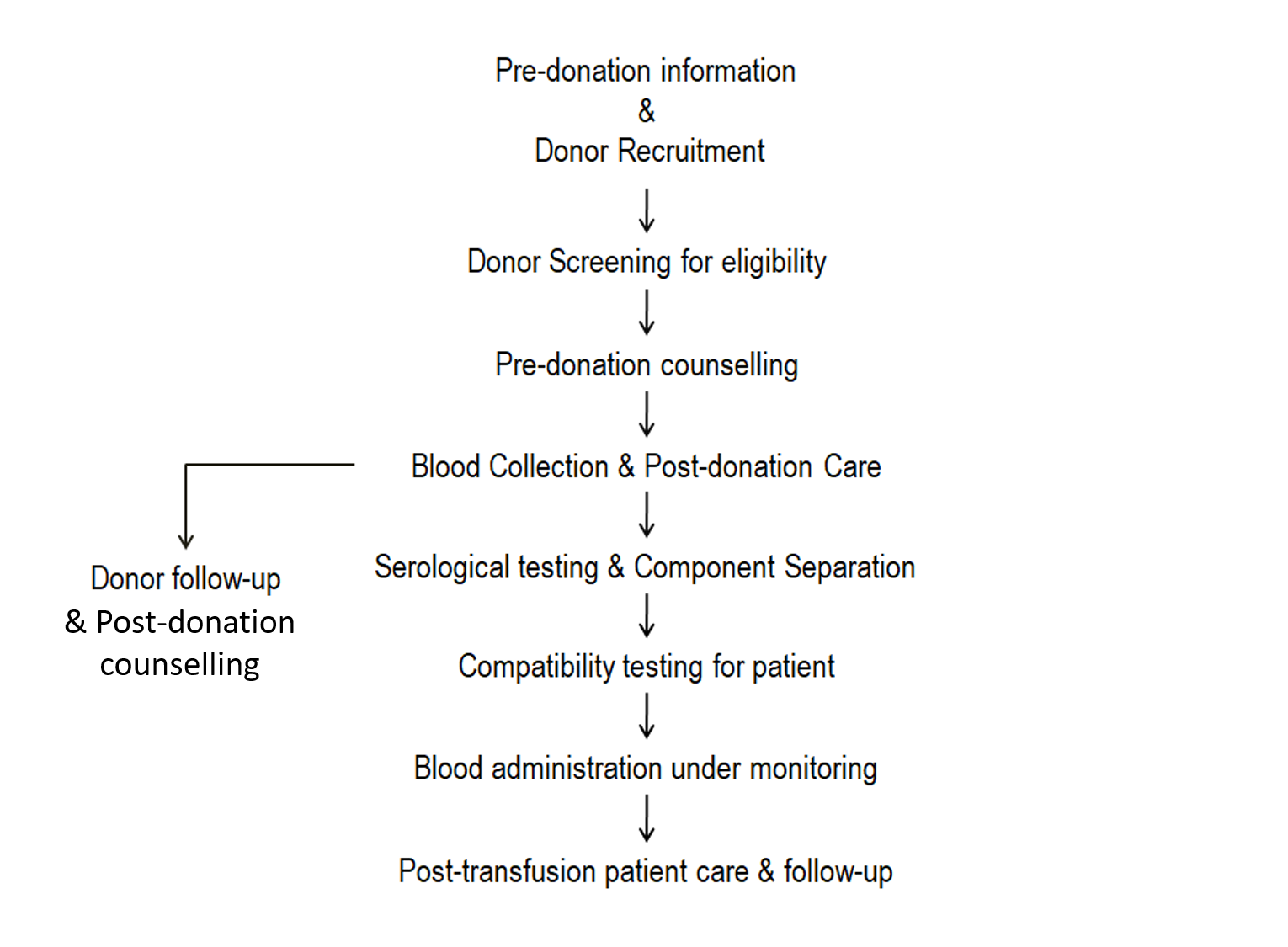
| 1 | Datta, Nand Sarup | 2 | Chally, Roy | 3 | Ghei, Ram Nath |
| 4 | Reddy, AVS | 5 | Chakravarty, Anil Kumar | 6 | Rao, DVN |
| 7 | Wadhwa, Surender Nath | 8 | Sharma, SK | 9 | Rama Raju, BV |
| 10 | Singh, Trilochan | 11 | Raghavaiah, Nimmagadda Veera | 12 | Chhabra, Jagjit Singh |
| 13 | Tandon, Jugal Kishore | 14 | Nair, G.R.Bahulayan | 15 | Patnaik, Biswa Bihari |
| 16 | Sahu, Laxmi Kanta | 17 | Belokar, Wasant Keshao | 18 | Virdi, Jaspal Singh |
| 19 | Mufti, Ghulam Rasool | 20 | Gupta, Narmada Prasad | 21 | Kankalia, Sharad Kumar P |
| 22 | Sharma, Rohtas Kumar | 23 | Mathur, Brijbans | 24 | Chattopadhyay, P Kumar |
| 25 | Roychoudhary, Tapan Kumar | 26 | Yusuf, Rafeek | 27 | Trehan, Pradeep Kumar |
| 28 | Yadav, Rajinder | 29 | Javali, Dilip | 30 | Kumar, Sunil |
| 31 | Umraiya, Matadeen | 32 | Mahanta, Rajendra Kumar | 33 | Krishna Murthy, Chanduru |
| 34 | Kochhar, Gurinder Singh | 35 | Singh, Sinam Sekharjit | 36 | Reddy, Parvathareddy |
| 37 | Rajagopal, V | 38 | Kotwal, Subhash Vinayak | 39 | Deka, Phanindra Mohan |
| 40 | Mohanty, Nayan Kumar | 41 | Fazal, Ali Reza | 42 | Bhatyal, Hardev |
| 43 | Ahlawat, Rajesh Kumar | 44 | Bhatia, Vipan | 45 | Ravi, R |
| 46 | Gill, Inderbir Singh | 47 | Gupta, Sunil | 48 | Khan, Muneer |
| 49 | Ramesh, Ottra | 50 | Baruah, Sumar | 51 | Murali, Tanjore Rangaswami |
| 52 | Joshi, Dhananjay Parashuram | 53 | Mehta, Vipin Kumar | 54 | Shenoy, Sunil P |
| 55 | Rao, S.V.S. | 56 | Luthra, Ashok Kumar | 57 | Padmakar, N.P. |
| 58 | Batura, Deepak | 59 | Yadav, Satya Prakash | 60 | Jadeja, Narendrasingh A |
| 61 | Chakraborty, Sudip Charan | 62 | Seth, Amlesh | 63 | Singh, Barinder Pal |
| 64 | Sood, Rajeev | 65 | Songra, Mool Chand | 66 | Taneja, Rajesh |
| 67 | Singh, Pritpal | 68 | Chahal, Rohit | 69 | Goswami, Atul Kumar |
| 70 | Kayashta, Anil | 71 | Jain, Devendra Kumar | 72 | Dorairajan, Lalgudi |
| 73 | Sood, Rajeev | 74 | Aron, Monish | 75 | Talwar, Manoj Kumar |
| 76 | Srinath, N | 77 | Sood, Swapan | 78 | Kumar, Manal |
| 79 | Ghose, Sujit | 80 | Agrawal, Anjani Kumar | 81 | Singh, Dharam Vir |
| 82 | Pawar, Ratnesh Singh | 83 | Rajeev, Thekumpadam P.Veetil | 84 | Ansari, Mohd.S. |
| 85 | Goel, Apul | 86 | Mandal, Subhasis | 87 | Kumar, Rajeev |
| 88 | Nabi, Ghulam | 89 | Khaitan, Anurag | 90 | Singh, Iqbal |
| 91 | Doddamani, Daresh | 92 | Kumar, Pawan | 93 | Goel, Rajiv |
| 94 | Dash, Sarat C | 95 | Mundada, Omprakash | 96 | Tandon, Sanjeev |
| 97 | Sivaramakrishna, Bodapati | 98 | Jindal, Lokesh | 99 | Gautam, Gagan |
| 100 | Yadav, Rajiv | 101 | Kumar, Atul | 102 | Kolla, Surendra Babu |
| 103 | Kumar, Anup | 104 | Singh, A.Kaku | 105 | Nayyar, Rishi |
| 106 | Singh, Ashutosh | 107 | Misra, Saurabh | 108 | Sharma, Sachit |
| 109 | Sharma, Nitin | 110 | Panda, S. | 111 | Mukerjee, SD |
| 112 | Ram, Ishwar | 113 | Singh, Prabhjot | 114 | Anand, Ajay |
| 115 | Saini, Ashish | 116 | Sahay, Shailesh | 117 | Saxena, Vaibhav |
| 118 | Nayak, B | 119 | Javali, Tarun | 120 | Abrol, Nitin |
| 121 | Mahapatra, Sanjay | 122 | Rai, Pramod Kumar | 123 | Swaroop, Laxman |
| 124 | Bora, Girdhar Singh | 125 | Regmi, Subodh | 126 | Choudhary, Lok Prakash |
| 127 | Singh, Animesh | 128 | Rao, Niren | 129 | Gupta, Rajan |
| 130 | Agarwal, Tapan | 131 | Desai, Pragnesh | 132 | Kumar, Ashish |
| 133 | Shrivastava, Nitin | 134 | Yadav, Siddharth | 135 | Tiwari, Devi Prasad |
| 136 | Srivastava, Prashant | 137 | Shukla, Abhishek | 138 | Kaushal, Rohit |
| 139 | Khan, Naveed | 140 | Prakash, Pradeep | 141 | Saini, Sumit |
| 142 | Kumar, Prashant | 143 | Bansal, Devanshu | 144 | Dadhwal, Rohit |
| 145 | Gurnani, Nishant | 146 | P, Sridhar | 147 | Garg, Harshit |
| 148 | Sharma, Kulbhushan | 149 | Pethe, Kiran Sahil | 150 | Singh, Prashant |
| 151 | Kumar, Naveen | 152 | Goel, Ritesh | 153 | Maheshwari, Parteek |
| 154 | Khattar, Manish |
Publications
Indexed Articles Abstracts Books & Monographs
Urology Minor OT/ Urodynamics/ Uroflowmetry/ Stone analysis:
SWL (Lithotripsy):
The department provides inpatient services through general wards, emergency wards and private wards. For elective surgery, patients are given a ‘date for admission’ based on their disease and availability of operating slots. There is significant waiting period for most elective surgeries. Emergencies are attended to round the clock and admissions for these are made through the casualty on the ground floor.
The department performs all modern urologic surgeries including (but not limited to):
| Urology OPD | ||
| New RAK OPD, A Block, 4th Floor, 9.30 AM | ||
| Faculty | Day | Room |
| Prof Amlesh Seth | Wed | A-427 |
| Prof Rajeev Kumar | Tue | A-421 |
| Fri | A-401 | |
| Dr B Nayak | Tue/Fri | A-422 |
| Dr Rishi Nayyar | Mon/Wed | A-421 |
| Dr Sanjay Kumar | Mon/Wed | A-428 |
| Dr Sidharth Jain | Mon/Wed | A-423 |
| Dr Manoj Kumar | Tue/Fri | A-429 |
| Dr Sridhar P | Tue | A-427 |
| Wed | NCI | |
| Dr. Prashant Singh | Mon | A-429 |
| Fri | NCI | |
| Andrology & Infertility Clinic | ||
| New RAK OPD, A Block, 4th Floor, Room No. 401 | ||
| Friday: 9.30 AM | ||
| Uro-malignancy Clinic | ||
| BRAIRCH, Ground Floor, Room No. 6, | ||
| Thursday: 10 AM | ||
| Uro-oncology OPD (NCI-Jhajjar) | ||
| Wednesday, Friday | ||
The department is a recognized training center for a post graduate degree in Urology. This involves a three-year training programme followed by an examination. Admission to this programme is based on an admission test conducted by the AIIMS. The department is also a recognized center for the Endourology fellowship of the Endourology Society.
The faculty of the department participates in and delivers lectures in continuing medical education programmes, symposia, national and International conferences. The department imparts lectures for the undergraduates and nursing students.
The department is regularly visited by post-graduate students, fellows and faculty from India and abroad on various training and observership programs. The focus of a number of these visits is to learn laparoscopy, robotics and upper tract endourology
The faculty of the department continues to be examiners for NBE and M.Ch. Urology in various universities and Inspector for the Medical Council of India and National Board for recognition of standard of examination and facilities for M.Ch. postgraduate courses.
Short Term and Long Term training
The department offers short term and long term training to qualified individuals from India and abroad. Training is provided in all aspects of Urology and a prior approval of the department faculty is required before applications are accepted. Application forms can be obtained from the office of the Registrar, AIIMS. (http://aiims.edu/aiims/academic/guideline_ST_LT.htm).
The department is a recognized training centre for award of the MCh degree in Urology. 11 post graduate students are enrolled for the three-year MCh program. This includes 8 students admitted through open competitive exam and 3 students who are sponsored for training by Government organizations. Recruitment takes place twice every year in the months of January and July. Details of the recruitment and eligibility criteria are available from the Academic Section of AIIMS Update this link: https://www.aiims.edu/en/academic_section_courses.html
Urology as a distinct specialty was initiated at AIIMS with the creation of a Urology Clinic in the Department of Surgery in the year 1958. In 1963, a separate department of Urology was created with Dr. Sarinder Man Singh’s appointment as Associate Professor and Head of Urology and Dr. B.C. Bapna’s appointment as Assistant Professor.
The Department is dedicated to the teaching and training of Urology of the highest standard. The M.Ch. training program was started in the year 1966 and, since then, over 100 postgraduates have been trained and they now occupy various important chairs in India and abroad. The post-graduate training program of the department has 11 positions, 8 posts of regular senior residents and 3 posts for sponsored candidates from the armed forces as well as Governmental and autonomous bodies from all over India. The MCh training program lasts for 3 years with periodic assessment before the final MCh examination. Admission is based on a competitive entrance examination.
The Department is fully equipped with the latest technology such as Endourological surgery (TUR, PCNL and URS (1989), ESWL (1987), Urodynamics, Ultrasound, Lasers, Microsurgery, Laparoscopic surgery (1992) and Robotic surgery (March 2005). State of the art medical care is provided for a variety of urological ailments and it serves as a referral center for complicated problems for patients in North India, Bihar, Orissa, Assam and neighboring countries like Nepal, Afghanistan, Bhutan etc. The out-patients clinic is attended by over 35000 patients annually including close to 12000 new cases. The department conducts over 2000 major surgeries annually
The All India Institute of Medical Sciences (AIIMS) was established by the Parliament of India in 1956 as an Institute of national importance with the object “to develop patterns of teaching in undergraduate and postgraduate medical education in all its branches so as to demonstrate a high standard of medical education to all medical colleges and other allied institutions in India”. Since the inception of the institute, the Centre for Community Medicine (CCM) has been a key department at AIIMS. The Centre aims to produce high quality public health professionals and community physicians. The Centre is consistently working towards discovery of new knowledge in domain of public health, advocacy for application of new ideas in health care of populations. The main focus area of the Centre has been on evolution of a replicable model of comprehensive health services and providing consultancy to strengthen capacity of health organizations at national and international level.
To establish and maintain rural and urban health organizations which will form centres for the field training of the medical, dental, and nursing students of the Institute as well as for the research into community health problems. This is in consonance with the stated function of AIIMS, Section 14, f(v) of AIIMS Act, 1956
To respond to the evolving national public health needs in keeping with global standards of teaching, research, and service by creating a professional workforce to translate knowledge to action and thereby contribute towards HEALTH FOR ALL
The Urban health program of the Centre provides community based health services to marginalised population of an urban resettlement colony in Dakshinpuri Extension, Ambedkar Nagar, New Delhi. Preventive, promotive and curative health services along with basic laboratory services are provided to the population covered by the Urban health program.
The details of the urban health program of the Centre are available in following link
The Rural health program of the Centre is also known as the Comprehensive Rural Health Services Project (CRHSP), Ballabgarh. The rural field practice area was started in 1961 with aid of Rockefeller Foundation. In year 1965 the CRHS Project was formally established in Ballabgarh Block, Faridabad District of Haryana as a collaborative project between Haryana State Government and AIIMS. The project comprises of:
The details of the rural health program of the Centre are available in following link
Testing TODAT
asdasdas
The department of Neuroimaging & Interventional Neuroradiology at All India institute of Medical Sciences is dedicated to the highest quality patient care, education, research, and community service. The department provides imaging and interpretation services to Neurosciences Centre.
The objectives of the Neuroimaging & Interventional Neuroradiology Department are:
The department is currently equipped with two Digital Subtraction Angiography systems (the biplane ‘Siemens ARTZEE’ & Philips FD 20/20 with facilities for rotational angiography & 3-D reconstruction. One 1.5T MR system (GE 450w), one CT scanner (Siemens Definition Edge 128-slice CT scanner and one color Doppler unit (HP ‘Sonos 4500’) serves as mainstays of diagnostic studies. These units cater to the requirements of the Neurosciences centre.
Welcome to the Computer Facility at the All India Institute of Medical Sciences (AIIMS), New Delhi. As a pioneering institution in healthcare and medical education, AIIMS is committed to leveraging cutting-edge technology to advance research, education, and patient care. Starting its humble journey in 1978 as a unit in the Department of Biophysics, it became a Specialty Centre in Jan'1989. All these years, our Computer Facility has stood as a testament to this commitment, providing state-of-the-art infrastructure and support services to meet the evolving needs of our esteemed faculty, researchers, students, and healthcare professionals.
In today's digital age, information technology plays a vital role in every aspect of healthcare, from research and education to clinical practice and administration. The Computer Facility at AIIMS New Delhi serves as the technological backbone, facilitating the seamless integration of IT solutions into various facets of our institution.
Services Offered: Our Computer Facility offers a comprehensive range of services tailored to meet the diverse needs of our stakeholders :
The Computer Facility, is dedicated to providing technological support and resources to facilitate excellence in education, research, and patient care. By harnessing the power of technology, we aim to drive innovation, foster collaboration, and empower the AIIMS community to address the most pressing challenges in healthcare.
| Senior Financial Advisor | |
|---|---|
| Smt. Divya Yanamadala |
| Financial Advisor |
|---|
| - |
| F & CAOs |
|---|
| Shri Vijay Pal Singh |
| Shri Padam Singh |
| Ms. Rakesh Kumari |
| Accounts Officers | ||
|---|---|---|
| Sh. Trilok Chand | Sh. Prem Pal | Smt. Meenakshi Dabral |
| Sh. Prakash Kumar Giri | Sh. Bharat Bhushan | Sh. Joginder Singh |
| Sh. Anil Kumar | Shri Satish Kumar Yadav | Sh. Upendra Kumar |
| Sh. Yogesh Kumar | Sh. Shivanand Thakur | Smt. Snehlata |
| Shri Rajesh Kr. Bairwa | - | - |
| Asstt. Accounts Officers | ||
|---|---|---|
| Smt. Meena Gupta | Shri Braham Singh | Smt.. Rashu Kabtiyal |
| Smt. S. Tanveer | Smt. Sushil Kumari | Sh. Satya Dev Sharma |
| Sh. Nagender | Sh. Arvind Kumar | Ms. Veena Gaba |
| Ms. Urmila | - | - |
| Jr. Account Officers |
|---|
| Vacant |
Coming Soon
Coming Soon
Coming Soon
Coming Soon
Coming Soon
Coming Soon
Coming Soon
Coming Soon
Coming Soon
Professor & Head
Contact number: 11-26593660
anatomy[at]aiims[dot]edu
Additional Professor
Contact number: 11-26593517
rimadadaaiims20[at]gmail[dot]com
Professor
Contact number: 11-26593489
arundhatis[at]aiims[dot]edu
Professor
Contact number: 11-26594702
renudhingraaiims[at]gmail[dot]com
Professor
Contact number: 11-26593568 , 9654215492
tapas_nag[at]aiims[dot]edu
Professor
Contact number: 11-26593225
sehgalritu[at]hotmail[dot]com
Professor
Contact number: 11-26593922
sarojkaler[at]gmail[dot]com
Additional Professor
Contact number: 11-26594986
tonygeorgejacob[at]gmail[dot]com
Additional Professor
Contact number: 11-26598058
seemahkg[at]gmail[dot]com
Additional Professor
Contact number: 11-26596624
sirohi.neerja[at]gmail[dot]com
Additional Professor
Contact number: 11-26598048
subhashmbu[at]gmail[dot]com
Assistant Professor
Contact number: 11-26598032
prabhakar.emf[at]gmail[dot]com
Assistant Professor
Contact number: 11-26593660
arthiganapathy08[at]gmail[dot]com
Asstt. Prof.(Contract basis)
parulkushal7[at]gmail[dot]com
Scientist
Contact number: 011-26593517
prabhakp[at]gmail[dot]com
Scientist
Contact number: 9711887047
mkaiims[at]gmail[dot]com
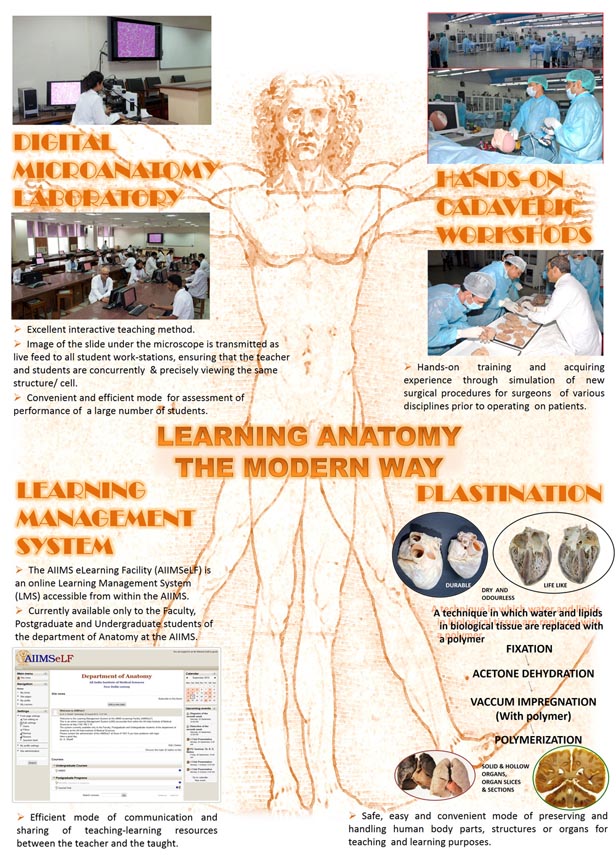
The department of Anatomy, one of the first departments to be set up, has contributed to the development of Anatomy curriculum which is implemented throughout the country by the Medical Council of India. Research and publications from this department have often been quoted in the bible of Anatomy- i.e, Gray’s Textbook of Anatomy.
The department is involved in medical teaching and training at the undergraduate, postgraduate and doctoral levels and also provides services that include diagnostics in genetic disorders and fluorosis. It runs a National Centre for Electron microscopy that regularly provides training for technicians and investigators. The department is a WHO-recognized Centre for training in Human Genetics. The department is also an active collaborator and organizer of various cadaveric workshops for post-graduate training and skills training in surgical and allied disciplines.
The main thrust areas of research in the department are neurobiology, male and female infertility, auditory and visual pathways, ageing-related disorders, pain biology, addiction genetics, pre-ecclampsia, enteric nervous system, pancreatitic pathogenesis, morphometry using state-of-the-art design-based stereology, autophagy and cell death, rare and common genetic disorders, ecotoxicology, breast cancer, nanobiology and drug-delivery systems, plastination and cancer biology including rare endocrine tumours.
The department provides training opportunities and support in the fields of Anatomical sciences, Genetics and Electron Microscopy to all Indians and nationals of SAARC countries.
Coming Soon
| Department | Name | AIIMS Email-Id | Alternate Email-Id |
|---|---|---|---|
| Director | Dr M. Srinivas | director[at]aiims[dot]gov[dot]in | - |
| Dean (Academic) | Dr. Kaushal kr. Verma | dean.acad[at]aiims[dot]gov[dot]in | - |
| Medical Superintendent | Dr. Nirupam Madaan | ms.main[at]aiims[dot]gov[dot]in | - |
| Additional Director (Administration) | Sh. Karan Singh | dd[at]aiims[dot]gov[dot]in | - |
| Dean (Research) | Dr. Nikhil Tandon | dean.research[at]aiims[dot]gov[dot]in | - |
| Prof. In Charge (Computer Facility) | Dr. Pooja Gupta | piccf[at]aiims[dot]gov[dot]in | - |
| Dean (Examinations) | Dr. | dean.exam[at]aiim[dot]gov[dot]in | - |
| Associate Dean (Academics) | Dr. Rakesh Lodha | associatedeanacad[at]aiims[dot]edu | - |
| Associate Dean (Research) | Dr. Vineet Ahuja | assodeanres[at]aiims[dot]gov[dot]in | researchsectionaiims[at]gmail[dot]com |
| Associate Dean (Examinations) | Dr. Naval K Vikram | assodean.exam[at]aiims[dot]gov[dot]in | - |
| Registrar | Dr. Girija Pd. Rath | registrar[at]aiims[dot]gov[dot]in | aiims.reg[at]gmail[dot]com |
| Asstt. Controller of Examinations | Sh. Manoj Kr. Singh | - | - |
Address : Ansari Nagar, New Delhi - 110029
Board Number : +91-11-26588500 / 26588700
Fax : +91-11-26588663 / 26588641
Important E-mail Addresses at AIIMS
AIIMS Hospital Ghaziabad
TEsttt
| YEAR - 1963 | |||
| 1. | DR. SURESH CHANDRA PANT | MAY | 1963 |
| YEAR – 1965 | |||
| 2. | DR. DAVINDER MOHAN | MAY | 1965 |
| 3. | DR. K. SUDHAKAR SHETTY | DEC | 1965 |
| YEAR – 1966 | |||
| 4. | DR. P. RAGHURAM REDDY | MAY | 1966 |
| 5. | DR. SHUBHA TRIVEDI | MAY | 1966 |
| 6. | DR. SATISH CHANDER MALIK | MSY | 1966 |
| 7. | DR. ADARSH SINGH MAHAL | DEC | 1966 |
| 8. | DR. BHUJANGRA RAO K. | DEC | 1966 |
| 9. | DR. VIRAT KRISHAN | DEC | 1966 |
| YEAR – 1967 | |||
| 10. | DR. JAGDISH SINGH TEJA | MAY | 1967 |
| 11. | DR. SUDARSHAN CHAWLA | MAY | 1967 |
| 12. | DR. RAMESH CHAND SETH | DEC | 1967 |
| YEAR – 1968 | |||
| 13. | DR. SURESH CHANDRA PANT | MAY | 1968 |
| 14. | DR. ANIL KUMAR AGARWAL | DEC | 1968 |
| 15. | DR. DIGVIJAY SINGH ROEL | DEC | 1968 |
| YEAR – 1969 | |||
| 16. | DR. BALWANT RAIAGNIHOTRI | MAY | 1969 |
| 17. | DR. EARNEST ROMESH CHANDER | MAY | 1969 |
| 18. | DR. LAL MOHAN GHOSH | MAY | 1968 |
| 19. | DR. PRAKASH BULAKIDAS BANTHIA | MAY | 1969 |
| 20. | DR. THUMULURY SIVA SUBRAHAMANYAN | MAY | 1969 |
| 21. | DR. GUL B. ADVANI | DEC. | 1969 |
| YEAR – 1970 | |||
| 22. | DR. DILEEP SINGH RASTOGI | MAY | 1970 |
| 23. | DR. MANJIT SINGH DHILLON | MAY | 1970 |
| 24. | DR. PREM LATA NANDA | DEC. | 1970 |
| YEAR – 1971 | |||
| 25. | DR. BENOYENDRA NATH MAJUMDAR | MAY | 1971 |
| 26. | DR. RANVIR KUMAR SOOD | DEC. | 1971 |
| YEAR – 1972 | |||
| 27. | DR. SWARN KANTA KHERA | MAY | 1972 |
| 28. | DR. BACHITTAR SINGH | DEC. | 1972 |
| 29. | DR. KANWAL KRISHAN BINDAL | DEC. | 1972 |
| 30. | DR. NEENA MAHAJAN | DEC. | 1972 |
| YEAR – 1973 | |||
| 31. | DR. HARINDER MOHAN CHAWLA | MAY | 1973 |
| 32. | DR. VELAGAPUDI BAPUJI RAO | MAY | 1973 |
| 33. | DR. SHYAM LAL KHANNA | MAY | 1973 |
| 34. | DR. S. RAJKUMAR | DEC. | 1973 |
| YEAR – 1974 | |||
| 35. | DR. RABINDRA NATH NANDI | MAY | 1974 |
| YEAR – 1975 | |||
| 36. | DR. V. M. DAMODARAN NAMBOODIRI | MAR. | 1975 |
| 37. | DR. VIRINDER KUMAR | MAY | 1975 |
| YEAR – 1976 | |||
| 38. | DR. M. G. THOMAS | FEB. | 1976 |
| 39. | DR. DAVINDER SINGH KOCHHAR | APR. | 1976 |
| 40. | DR. VENUGOPALAN RAGHAVAKURUP | MAY | 1976 |
| 41. | DR. ADARSH KUMAR VOHRA | DEC. | 1976 |
| YEAR – 1977 | |||
| 42. | DR. PRANIT KUMAR CHAUDHURY | JAN. | 1977 |
| 43. | DR. RAJAT RAY | FEB. | 1977 |
| 44. | DR. SUMAN AGARWAL | MAY | 1977 |
| 45. | DR. BIMAL CHOWDHARY | MAY | 1977 |
| 46. | DR. RATNA BILWANI | MAY | 1977 |
| 47. | DR. ANANDI LAL | DEC. | 1977 |
| YEAR – 1978 | |||
| 48. | DR. K. NAGARAJA RAO | MAY | 1978 |
| 49. | DR. P. N. RAMANI | MAY | 1978 |
| 50. | DR. HARINDER SINGH SETHI | DEC. | 1978 |
| 51. | DR. KULWANT SINGH BAGHIANA | DEC. | 1978 |
| 52. | DR. VINAY KAPOOR | DEC. | 1978 |
| YEAR – 1979 | |||
| 53. | DR. JACOB K. JOHN | MAY | 1979 |
| 54. | DR. SHOBHA PILLAI | JUNE | 1979 |
| 55. | DR. MOHAN DAS. E. | DEC. | 1979 |
| YEAR – 1980 | |||
| 56. | DR. SANDI SYLEM | JULY | 1980 |
| 57. | DR. MINAKSHI MUKHOPADHYAYA | JULY | 1980 |
| 58. | DR. PREVESH KUMAR RUSTAGI | DEC. | 1980 |
| YEAR – 1981 | |||
| 59. | DR. PERMINDER SINGH SACHDEV | DEC. | 1981 |
| 60. | DR. SHEKAR SAXENA | DEC. | 1981 |
| 61. | DR. DHRUBA MAN SHRESTHA | DEC. | 1981 |
| YEAR – 1982 | |||
| 62. | DR. GEEANESWAR GAYA | MAY | 1982 |
| 63. | DR. SURENDRA KUMAR JAYASWAL | DEC. | 1982 |
| 64. | DR. PADMA RAJU VARREY | DEC. | 1982 |
| YEAR – 1983 | |||
| 65. | DR. ADITYAN JEE | DEC. | 1983 |
| 66. | DR. ALOK SARIN | DEC. | 1983 |
| YEAR – 1984 | |||
| 67. | DR. ASHOK SHARMA | DEC. | 1984 |
| 68. | DR. SMITA LAXMIKANT NIMGAONKAR | DEC. | 1984 |
| YEAR – 1985 | |||
| 69. | DR. MOPIDEVI VIJAYA GOPAL | MAY | 1985 |
| 70. | DR. NIRAKAR MAN SHRESTHA | MAY | 1985 |
| 71. | DR. MAHENDRA KUMAR NEPAL | DEC. | 1985 |
| 72. | DR. K. B. BALA RAJU | DEC. | 1985 |
| YEAR – 1986 | |||
| 73. | DR. G. S. P. RAJU | MAY | 1986 |
| 74. | DR. K. PRAVEEN LAL | DEC | 1986 |
| YEAR – 1987 | |||
| 75. | DR. PARTMA SARATHI DAS | MAY | 1987 |
| 76. | DR. AJIT KUMAR DAS | DEC | 1987 |
| YEAR – 1988 | |||
| 77. | DR. KHONDAKAR ABUYL HASANAT | DEC | 1968 |
| 78. | DR. RATAKONDA SANTHISAGAR | DEC | 1988 |
| YEAR - 1989 | |||
| 79. | DR. P. MALLIKARJUNA | DEC. | 1969 |
| 80. | DR. VEMIREDDY SREE NIVASULU | DEC | 1969 |
| YEAR - 1990 | |||
| 81. | DR. J. PRAVEEN | MAY | 1990 |
| 82. | DR. PRATAP SHARAN | DEC. | 1990 |
| YEAR – 1991 | |||
| 83. | DR. SHIVANANDA JENA | MAY | 1991 |
| 84. | DR. ANIL KUMAR NIGAM | MAY | 1991 |
| 85. | DR. SORAM MANIKANTA SINGH | DEC. | 1991 |
| YEAR - 1992 | |||
| 86. | DR. SANJEEV KUMAR | MAY | 1992 |
| 87. | DR. KAVURU BUSH | DEC. | 1992 |
| 88. | DR. EAMON KALYAN DUTTA | DEC. | 1992 |
| 89. | DR. SUNIL KUMAR | DEC. | 1992 |
| YEAR - 1993 | |||
| 90. | DR. VIVEK KATOCH | MAY | 1993 |
| 91. | DR. K. NEGI REDDY | MAY | 1993 |
| 92. | DR. MADHURI V. KAMBLE | MAY | 1993 |
| 93. | DR. ANJU DHAWAN | DEC. | 1993 |
| 94. | DR. CHANDNI SINGH | DEC. | 1993 |
| YEAR - 1994 | |||
| 95. | DR. GEETA CHAUDHARY | DEC. | 1994 |
| 96. | DR. DHANESH KUMAR | DEC. | 1994 |
| YEAR - 1995 | |||
| 97. | DR. PRITHWIS BHAUMIK | MAY | 1995 |
| 98. | DR. PRASANT KUMAR SAMANTARAY | MAY | 1995 |
| 99. | DR. RAHUL TOMAR | DEC. | 1995 |
| 100. | DR. NIRUJ KUMAR AGRAWAL | DEC. | 1995 |
| 101. | DR. SIMRAT SINGH SETHI | DEC. | 1995 |
| 102. | DR. KOIJAM SHANTIBALA DEVI | DEC. | 1995 |
YEAR - 1996
| |||
| 103. | DR. KIRTANA BALLAKOOR | MAY | 1996 |
| 104. | DR. PRAVIR SHANKAR PRASAD | DEC. | 1996 |
| YEAR - 1997 | |||
| 105. | DR. SABAASIAM (BALJEET KAUR) | MAY | 1997 |
| 106. | DR DR. KHURSHID AHMAD KHURSHID | DEC. | 1997 |
| YEAR - 1998 | |||
| 101. | DR.DR. A. TEMSUYANGER A. O. | MAY | 1998 |
| 108. | DR DR. RAMESH KUMAR | MAY | 1998 |
| 10S. | DR.DR. AMIYA BANERJEE | MAY | 1998 |
| 110. | DR. PRAMOD MOHAN SHYANGWA | MAY | 1998 |
| 111. | DR. SUJIT KUMAR NAIK | DEC. | 1998 |
| 112. | DR. RAJKUMAR LENIN SINGH | DEC. | 1998 |
| YEAR – 1999 | |||
| 113. | DR. EDWIN K. SIMON | MAY | 1999 |
| 114. | DR. NEERAJ BERRY | MAY | 1999 |
| 115. | DR. JFSU NATH | DEC. | 1999 |
| 116. | DR. NAND KUMAR | DEC. | 1999 |
| 117. | DR. PALLAB KUMAR MAULIK | DEC. | 1999 |
| 118. | DR. ATUL AMBEKAR | DEC. | 1999 |
| YEAR – 2000 | |||
| 119. | DR. SAJAL KUMAR GUPTA | MAY | 2000 |
| 120. | DR. AJAY KUMAR BHATT | MAY | 2000 |
| 121. | DR AMULYA BHARAT | MAY | 2000 |
| 122. | DR. AMITABHA SAHA | DEC. | 2000 |
| 123. | DR. EDDIE OSMOND MUKHIM | DEC. | 2000 |
| YEAR – 2001 | |||
| 124. | DR. MONALARINDAM B. | MAY | 2001 |
| 125. | DR. MANOJ KUMAR M. N. | MAY | 2001 |
| 126. | DR. SANJAY KR. PATANAYAK | MAY | 2001 |
| 127. | DR. RAJESH KUMAR | MAY | 2001 |
| 128. | DR. FARZANA KADER LINDA | MAY | 2001 |
| 129. | DR. SUBHAS SOREN | DEC. | 2001 |
| 130. | DR. SHANTANU DE | DEC. | 2001 |
| YEAR – 2002 | |||
| 131. | DR. VIJENDER SINGH | DEC. | 2002 |
| 132. | DR. PRIYANKA BHATIA | DEC. | 2002 |
| YEAR – 2003 | |||
| 133. | DR. RABI SHAKYA | MAY | 2003 |
| 134. | DR. AVINASH HOSANAGAR | MAY | 2003 |
| 135.. | DR. ANKUSH SINGHAL | DEC. | 2003 |
| 136. | DR. NILOTPAL DAS | DEC. | 2003 |
| 137. | DR. SHASHI BHUSHAN KUMAR | DEC. | 2003 |
| 138. | DR. DEEPAK GARG | DEC. | 2003 |
| 139. | DR. SRINIVAS T. R. | DEC. | 2003 |
| 140. | DR. AMARDEEP KUMAR | DEC | 2003 |
| YEAR – 2004 | |||
| 141. | DR. MITALI BHUYAN | MAY | 2004 |
| 142. | DR. RAVINDRA V. RAO | MAY | 2004 |
| 143. | DR. KUMAR RANJAN MAJI | MAY | 2004 |
| 144. | DR. TINA LAL | MAY | 2004 |
| 145. | DR. AMBICA PRASAD JHA | MAY | 2004 |
| 146. | DR. RAJA SADHU | DEC. | 2004 |
| YEAR – 2005 | |||
| 147. | DR. RAMAN GARG | MAY | 2005 |
| 148. | DR. SHIVANAND KATTIMANI | MAY | 2005 |
| 149. | DR. RAMAN DEEP | MAY | 2005 |
| 150. | DR. SABISH BALAN | DEC. | 2005 |
| YEAR – 2006 | |||
| 151. | DR. RAJIV KUMAR SHARMA | MAY | 2006 |
| 152. | DR. YATAN PAL SINGH BALHARA | MAY | 2006 |
| 153. | DR. ALOK AGRAWAL | DEC. | 2006 |
| 154. | DR. MRIDULA KAYAL | DEC. | 2006 |
| 155. | DR. A. SHYAM SUNDAR | DEC. | 2006 |
| 156. | DR. JATINDER MOHAN CHAWLA | DEC. | 2006 |
| 157. | DR. SUNNY T. VARGHESE | DEC. | 2006 |
| YEAR – 2007 | |||
| 158. | DR. NAND KISHORE | MAY | 2007 |
| 159. | DR. ROZATKARABHIJIT RAMDAS | MAY | 2007 |
| 160. | DR. PREETI SINHA | MAY | 2007 |
| 161. | DR. PRASHANT GOYAL | MAY | 2007 |
| 162. | DR. SHIVA PRAKASH | MAY | 2007 |
| 163. | DR. KUSHAL D. JAIN | MAY | 2007 |
| YEAR – 2008 | |||
| 164. | DR. KOUSHIK SINHA DEB | MAY | 2008 |
| 165. | DR. AMIT KUMAR GUPTA | DEC. | 2008 |
| 166. | DR. BISWADIP CHATTERJEE | DEC. | 2008 |
| 167. | DR. VIJETA KUSHWAHA | DEC. | 2008 |
| 168. | DR. ROHIT VERMA | DEC. | 2008 |
| YEAR – 2009 | |||
| 169. | DR. SURESH CHAND | MAY | 2009 |
| 170. | DR. LITON MALLICK | MAY | 2009 |
| 171. | DR. ABHISHEK PALLAVA | DEC. | 2009 |
| 172. | DR. PRADIPTA MAJUMDAR | DEC. | 2009 |
| 173. | DR. ANISH P. K. | DEC. | 2009 |
| 174. | DR. SANTOSH I. RAMDURG | DEC. | 2009 |
| YEAR – 2010 | |||
| 175. | DR. SIVARAMAN SUBHRAMANIAN | MAY | 2010 |
| 176. | DR. PRASHANTH SWAMINATHAN | MAY | 2010 |
| 177. | DR. ASHISH MITTAL | MAY | 2010 |
| 178. | DR. BICHITRA NANDA PATRA | MAY | 2010 |
| 179. | DR. SHRIGOPAL GOYAL | MAY | 2010 |
| YEAR – 2011 | |||
| 180. | DR. SIDDHARTH SARKAR | MAY | 2011 |
| 181. | DR. RAJEEV RANAJAN | MAY | 2011 |
| 182. | DR. ADITYA PAWAR | MAY | 2011 |
| 183. | DR. SAGAR BERA | MAY | 2011 |
| 184. | DR. PIYALI MANDAL | MAY | 2011 |
| 185. | DR. RISHAB GUPTA | DEC | 2011 |
| 186. | DR. VIJAY KRISHNAN | DEC | 2011 |
| YEAR – 2012 | |||
| 187. | DR. ANIRUDDHA BASU | MAY | 2012 |
| 188. | DR. TULESHWAR SINGH | MAY | 2012 |
| 189. | DR. ROSHAN BHAD | MAY | 2012 |
| 190. | DR. NANDITA HAZARI | DEC | 2012 |
| 191. | DR. SUNDAR GNANAVEL | DEC | 2012 |
| YEAR – 2013 | |||
| 192. | DR. MRINMAY DAS | MAY | 2013 |
| 193. | DR. ASHOK CHAUDHARY | MAY | 2013 |
| 194. | DR. MADHURIMA GHOSH | MAY | 2013 |
| 195. | DR. SATHYAPRAKASH | MAY | 2013 |
| 196. | DR. SHAILESH JHA | MAY | 2013 |
| 197. | DR. SHAMBHU PRASAD | MAY | 2013 |
| 198. | DR. RAJU BHATTARAI | MAY | 2013 |
| 199. | DR. DEEKSHA ELWADHI | MAY | 2013 |
| 200. | DR ARUMUGANATHAN ANMUGAVINAYAGAM | DEC | 2013 |
| 201. | DR. MOHIT VARSHNEY | DEC | 2013 |
| YEAR - 2014 | |||
| 202. | DR. NRIPENDRA KUMAR | MAY | 2014 |
| 203. | DR. ANIL YADAV | MAY | 2014 |
| 204. | DR. NISHANTH KN | MAY | 2014 |
| 205. | DR. SAURABH KUMAR | MAY | 2014 |
| 206. | DR. ROHIT ALOK | DEC | 2014 |
| 207. | DR. PARVESH BATRA | DEC | 2014 |
| 208. | DR. ANANYA MAHAPATRA | DEC | 2014 |
| 209. | DR. ANKIT GUPTA | DEC | 2014 |
| 210. | DR. VAIBHAV PATIL | DEC | 2014 |
| YEAR – 2015 | |||
| 211. | DR. SHOBHIT JAIN | MAY | 2015 |
| 212. | DR. PAWAN SHARMA | MAY | 2015 |
| 213. | DR. ARGHYA PAL | MAY | 2015 |
| 214. | DR. ARPIT PARMAR | MAY | 2015 |
| 215. | DR. DARA SINGH POONIA | MAY | 2015 |
| 216. | DR. PRASHANT GUPTA | MAY | 2015 |
| 217. | DR. SHYAMANAND ROY | DEC | 2015 |
| 218. | DR. ASHISH PAKHRE | DEC | 2015 |
| YEAR – 2016 | |||
| 219. | DR. POOJA PATTNAIK | MAY | 2016 |
| 220. | DR. SNEHIL GUPTA | MAY | 2016 |
| 221. | DR. SURESH THAPALIYA | MAY | 2016 |
| 222. | DR. SACHIN KUMAR | MAY | 2016 |
| 223. | DR. ABHINAV PANDEY | MAY | 2016 |
| 224. | DR. NAJEF MOIDEEN | DEC | 2016 |
| 225. | DR. SARTAJ DEEPAK | DEC | 2016 |
| 226. | DR. RISHI GUPTA | DEC | 2016 |
| 227. | DR DEEPAK CHARAN | DEC | 2016 |
| YEAR - 1963 | |||
| 1. | DR. SURESH CHANDRA PANT | MAY | 1963 |
| YEAR – 1965 | |||
| 2. | DR. DAVINDER MOHAN | MAY | 1965 |
| 3. | DR. K. SUDHAKAR SHETTY | DEC | 1965 |
| YEAR – 1966 | |||
| 4. | DR. P. RAGHURAM REDDY | MAY | 1966 |
| 5. | DR. SHUBHA TRIVEDI | MAY | 1966 |
| 6. | DR. SATISH CHANDER MALIK | MSY | 1966 |
| 7. | DR. ADARSH SINGH MAHAL | DEC | 1966 |
| 8. | DR. BHUJANGRA RAO K. | DEC | 1966 |
| 9. | DR. VIRAT KRISHAN | DEC | 1966 |
| YEAR – 1967 | |||
| 10. | DR. JAGDISH SINGH TEJA | MAY | 1967 |
| 11. | DR. SUDARSHAN CHAWLA | MAY | 1967 |
| 12. | DR. RAMESH CHAND SETH | DEC | 1967 |
| YEAR – 1968 | |||
| 13. | DR. SURESH CHANDRA PANT | MAY | 1968 |
| 14. | DR. ANIL KUMAR AGARWAL | DEC | 1968 |
| 15. | DR. DIGVIJAY SINGH ROEL | DEC | 1968 |
| YEAR – 1969 | |||
| 16. | DR. BALWANT RAIAGNIHOTRI | MAY | 1969 |
| 17. | DR. EARNEST ROMESH CHANDER | MAY | 1969 |
| 18. | DR. LAL MOHAN GHOSH | MAY | 1968 |
| 19. | DR. PRAKASH BULAKIDAS BANTHIA | MAY | 1969 |
| 20. | DR. THUMULURY SIVA SUBRAHAMANYAN | MAY | 1969 |
| 21. | DR. GUL B. ADVANI | DEC. | 1969 |
| YEAR – 1970 | |||
| 22. | DR. DILEEP SINGH RASTOGI | MAY | 1970 |
| 23. | DR. MANJIT SINGH DHILLON | MAY | 1970 |
| 24. | DR. PREM LATA NANDA | DEC. | 1970 |
| YEAR – 1971 | |||
| 25. | DR. BENOYENDRA NATH MAJUMDAR | MAY | 1971 |
| 26. | DR. RANVIR KUMAR SOOD | DEC. | 1971 |
| YEAR – 1972 | |||
| 27. | DR. SWARN KANTA KHERA | MAY | 1972 |
| 28. | DR. BACHITTAR SINGH | DEC. | 1972 |
| 29. | DR. KANWAL KRISHAN BINDAL | DEC. | 1972 |
| 30. | DR. NEENA MAHAJAN | DEC. | 1972 |
| YEAR – 1973 | |||
| 31. | DR. HARINDER MOHAN CHAWLA | MAY | 1973 |
| 32. | DR. VELAGAPUDI BAPUJI RAO | MAY | 1973 |
| 33. | DR. SHYAM LAL KHANNA | MAY | 1973 |
| 34. | DR. S. RAJKUMAR | DEC. | 1973 |
| YEAR – 1974 | |||
| 35. | DR. RABINDRA NATH NANDI | MAY | 1974 |
| YEAR – 1975 | |||
| 36. | DR. V. M. DAMODARAN NAMBOODIRI | MAR. | 1975 |
| 37. | DR. VIRINDER KUMAR | MAY | 1975 |
| YEAR – 1976 | |||
| 38. | DR. M. G. THOMAS | FEB. | 1976 |
| 39. | DR. DAVINDER SINGH KOCHHAR | APR. | 1976 |
| 40. | DR. VENUGOPALAN RAGHAVAKURUP | MAY | 1976 |
| 41. | DR. ADARSH KUMAR VOHRA | DEC. | 1976 |
| YEAR – 1977 | |||
| 42. | DR. PRANIT KUMAR CHAUDHURY | JAN. | 1977 |
| 43. | DR. RAJAT RAY | FEB. | 1977 |
| 44. | DR. SUMAN AGARWAL | MAY | 1977 |
| 45. | DR. BIMAL CHOWDHARY | MAY | 1977 |
| 46. | DR. RATNA BILWANI | MAY | 1977 |
| 47. | DR. ANANDI LAL | DEC. | 1977 |
| YEAR – 1978 | |||
| 48. | DR. K. NAGARAJA RAO | MAY | 1978 |
| 49. | DR. P. N. RAMANI | MAY | 1978 |
| 50. | DR. HARINDER SINGH SETHI | DEC. | 1978 |
| 51. | DR. KULWANT SINGH BAGHIANA | DEC. | 1978 |
| 52. | DR. VINAY KAPOOR | DEC. | 1978 |
| YEAR – 1979 | |||
| 53. | DR. JACOB K. JOHN | MAY | 1979 |
| 54. | DR. SHOBHA PILLAI | JUNE | 1979 |
| 55. | DR. MOHAN DAS. E. | DEC. | 1979 |
| YEAR – 1980 | |||
| 56. | DR. SANDI SYLEM | JULY | 1980 |
| 57. | DR. MINAKSHI MUKHOPADHYAYA | JULY | 1980 |
| 58. | DR. PREVESH KUMAR RUSTAGI | DEC. | 1980 |
| YEAR – 1981 | |||
| 59. | DR. PERMINDER SINGH SACHDEV | DEC. | 1981 |
| 60. | DR. SHEKAR SAXENA | DEC. | 1981 |
| 61. | DR. DHRUBA MAN SHRESTHA | DEC. | 1981 |
| YEAR – 1982 | |||
| 62. | DR. GEEANESWAR GAYA | MAY | 1982 |
| 63. | DR. SURENDRA KUMAR JAYASWAL | DEC. | 1982 |
| 64. | DR. PADMA RAJU VARREY | DEC. | 1982 |
| YEAR – 1983 | |||
| 65. | DR. ADITYAN JEE | DEC. | 1983 |
| 66. | DR. ALOK SARIN | DEC. | 1983 |
| YEAR – 1984 | |||
| 67. | DR. ASHOK SHARMA | DEC. | 1984 |
| 68. | DR. SMITA LAXMIKANT NIMGAONKAR | DEC. | 1984 |
| YEAR – 1985 | |||
| 69. | DR. MOPIDEVI VIJAYA GOPAL | MAY | 1985 |
| 70. | DR. NIRAKAR MAN SHRESTHA | MAY | 1985 |
| 71. | DR. MAHENDRA KUMAR NEPAL | DEC. | 1985 |
| 72. | DR. K. B. BALA RAJU | DEC. | 1985 |
| YEAR – 1986 | |||
| 73. | DR. G. S. P. RAJU | MAY | 1986 |
| 74. | DR. K. PRAVEEN LAL | DEC | 1986 |
| YEAR – 1987 | |||
| 75. | DR. PARTMA SARATHI DAS | MAY | 1987 |
| 76. | DR. AJIT KUMAR DAS | DEC | 1987 |
| YEAR – 1988 | |||
| 77. | DR. KHONDAKAR ABUYL HASANAT | DEC | 1968 |
| 78. | DR. RATAKONDA SANTHISAGAR | DEC | 1988 |
| YEAR - 1989 | |||
| 79. | DR. P. MALLIKARJUNA | DEC. | 1969 |
| 80. | DR. VEMIREDDY SREE NIVASULU | DEC | 1969 |
| YEAR - 1990 | |||
| 81. | DR. J. PRAVEEN | MAY | 1990 |
| 82. | DR. PRATAP SHARAN | DEC. | 1990 |
| YEAR – 1991 | |||
| 83. | DR. SHIVANANDA JENA | MAY | 1991 |
| 84. | DR. ANIL KUMAR NIGAM | MAY | 1991 |
| 85. | DR. SORAM MANIKANTA SINGH | DEC. | 1991 |
| YEAR - 1992 | |||
| 86. | DR. SANJEEV KUMAR | MAY | 1992 |
| 87. | DR. KAVURU BUSH | DEC. | 1992 |
| 88. | DR. EAMON KALYAN DUTTA | DEC. | 1992 |
| 89. | DR. SUNIL KUMAR | DEC. | 1992 |
| YEAR - 1993 | |||
| 90. | DR. VIVEK KATOCH | MAY | 1993 |
| 91. | DR. K. NEGI REDDY | MAY | 1993 |
| 92. | DR. MADHURI V. KAMBLE | MAY | 1993 |
| 93. | DR. ANJU DHAWAN | DEC. | 1993 |
| 94. | DR. CHANDNI SINGH | DEC. | 1993 |
| YEAR - 1994 | |||
| 95. | DR. GEETA CHAUDHARY | DEC. | 1994 |
| 96. | DR. DHANESH KUMAR | DEC. | 1994 |
| YEAR - 1995 | |||
| 97. | DR. PRITHWIS BHAUMIK | MAY | 1995 |
| 98. | DR. PRASANT KUMAR SAMANTARAY | MAY | 1995 |
| 99. | DR. RAHUL TOMAR | DEC. | 1995 |
| 100. | DR. NIRUJ KUMAR AGRAWAL | DEC. | 1995 |
| 101. | DR. SIMRAT SINGH SETHI | DEC. | 1995 |
| 102. | DR. KOIJAM SHANTIBALA DEVI | DEC. | 1995 |
YEAR - 1996
| |||
| 103. | DR. KIRTANA BALLAKOOR | MAY | 1996 |
| 104. | DR. PRAVIR SHANKAR PRASAD | DEC. | 1996 |
| YEAR - 1997 | |||
| 105. | DR. SABAASIAM (BALJEET KAUR) | MAY | 1997 |
| 106. | DR DR. KHURSHID AHMAD KHURSHID | DEC. | 1997 |
| YEAR - 1998 | |||
| 101. | DR.DR. A. TEMSUYANGER A. O. | MAY | 1998 |
| 108. | DR DR. RAMESH KUMAR | MAY | 1998 |
| 10S. | DR.DR. AMIYA BANERJEE | MAY | 1998 |
| 110. | DR. PRAMOD MOHAN SHYANGWA | MAY | 1998 |
| 111. | DR. SUJIT KUMAR NAIK | DEC. | 1998 |
| 112. | DR. RAJKUMAR LENIN SINGH | DEC. | 1998 |
| YEAR – 1999 | |||
| 113. | DR. EDWIN K. SIMON | MAY | 1999 |
| 114. | DR. NEERAJ BERRY | MAY | 1999 |
| 115. | DR. JFSU NATH | DEC. | 1999 |
| 116. | DR. NAND KUMAR | DEC. | 1999 |
| 117. | DR. PALLAB KUMAR MAULIK | DEC. | 1999 |
| 118. | DR. ATUL AMBEKAR | DEC. | 1999 |
| YEAR – 2000 | |||
| 119. | DR. SAJAL KUMAR GUPTA | MAY | 2000 |
| 120. | DR. AJAY KUMAR BHATT | MAY | 2000 |
| 121. | DR AMULYA BHARAT | MAY | 2000 |
| 122. | DR. AMITABHA SAHA | DEC. | 2000 |
| 123. | DR. EDDIE OSMOND MUKHIM | DEC. | 2000 |
| YEAR – 2001 | |||
| 124. | DR. MONALARINDAM B. | MAY | 2001 |
| 125. | DR. MANOJ KUMAR M. N. | MAY | 2001 |
| 126. | DR. SANJAY KR. PATANAYAK | MAY | 2001 |
| 127. | DR. RAJESH KUMAR | MAY | 2001 |
| 128. | DR. FARZANA KADER LINDA | MAY | 2001 |
| 129. | DR. SUBHAS SOREN | DEC. | 2001 |
| 130. | DR. SHANTANU DE | DEC. | 2001 |
| YEAR – 2002 | |||
| 131. | DR. VIJENDER SINGH | DEC. | 2002 |
| 132. | DR. PRIYANKA BHATIA | DEC. | 2002 |
| YEAR – 2003 | |||
| 133. | DR. RABI SHAKYA | MAY | 2003 |
| 134. | DR. AVINASH HOSANAGAR | MAY | 2003 |
| 135.. | DR. ANKUSH SINGHAL | DEC. | 2003 |
| 136. | DR. NILOTPAL DAS | DEC. | 2003 |
| 137. | DR. SHASHI BHUSHAN KUMAR | DEC. | 2003 |
| 138. | DR. DEEPAK GARG | DEC. | 2003 |
| 139. | DR. SRINIVAS T. R. | DEC. | 2003 |
| 140. | DR. AMARDEEP KUMAR | DEC | 2003 |
| YEAR – 2004 | |||
| 141. | DR. MITALI BHUYAN | MAY | 2004 |
| 142. | DR. RAVINDRA V. RAO | MAY | 2004 |
| 143. | DR. KUMAR RANJAN MAJI | MAY | 2004 |
| 144. | DR. TINA LAL | MAY | 2004 |
| 145. | DR. AMBICA PRASAD JHA | MAY | 2004 |
| 146. | DR. RAJA SADHU | DEC. | 2004 |
| YEAR – 2005 | |||
| 147. | DR. RAMAN GARG | MAY | 2005 |
| 148. | DR. SHIVANAND KATTIMANI | MAY | 2005 |
| 149. | DR. RAMAN DEEP | MAY | 2005 |
| 150. | DR. SABISH BALAN | DEC. | 2005 |
| YEAR – 2006 | |||
| 151. | DR. RAJIV KUMAR SHARMA | MAY | 2006 |
| 152. | DR. YATAN PAL SINGH BALHARA | MAY | 2006 |
| 153. | DR. ALOK AGRAWAL | DEC. | 2006 |
| 154. | DR. MRIDULA KAYAL | DEC. | 2006 |
| 155. | DR. A. SHYAM SUNDAR | DEC. | 2006 |
| 156. | DR. JATINDER MOHAN CHAWLA | DEC. | 2006 |
| 157. | DR. SUNNY T. VARGHESE | DEC. | 2006 |
| YEAR – 2007 | |||
| 158. | DR. NAND KISHORE | MAY | 2007 |
| 159. | DR. ROZATKARABHIJIT RAMDAS | MAY | 2007 |
| 160. | DR. PREETI SINHA | MAY | 2007 |
| 161. | DR. PRASHANT GOYAL | MAY | 2007 |
| 162. | DR. SHIVA PRAKASH | MAY | 2007 |
| 163. | DR. KUSHAL D. JAIN | MAY | 2007 |
| YEAR – 2008 | |||
| 164. | DR. KOUSHIK SINHA DEB | MAY | 2008 |
| 165. | DR. AMIT KUMAR GUPTA | DEC. | 2008 |
| 166. | DR. BISWADIP CHATTERJEE | DEC. | 2008 |
| 167. | DR. VIJETA KUSHWAHA | DEC. | 2008 |
| 168. | DR. ROHIT VERMA | DEC. | 2008 |
| YEAR – 2009 | |||
| 169. | DR. SURESH CHAND | MAY | 2009 |
| 170. | DR. LITON MALLICK | MAY | 2009 |
| 171. | DR. ABHISHEK PALLAVA | DEC. | 2009 |
| 172. | DR. PRADIPTA MAJUMDAR | DEC. | 2009 |
| 173. | DR. ANISH P. K. | DEC. | 2009 |
| 174. | DR. SANTOSH I. RAMDURG | DEC. | 2009 |
| YEAR – 2010 | |||
| 175. | DR. SIVARAMAN SUBHRAMANIAN | MAY | 2010 |
| 176. | DR. PRASHANTH SWAMINATHAN | MAY | 2010 |
| 177. | DR. ASHISH MITTAL | MAY | 2010 |
| 178. | DR. BICHITRA NANDA PATRA | MAY | 2010 |
| 179. | DR. SHRIGOPAL GOYAL | MAY | 2010 |
| YEAR – 2011 | |||
| 180. | DR. SIDDHARTH SARKAR | MAY | 2011 |
| 181. | DR. RAJEEV RANAJAN | MAY | 2011 |
| 182. | DR. ADITYA PAWAR | MAY | 2011 |
| 183. | DR. SAGAR BERA | MAY | 2011 |
| 184. | DR. PIYALI MANDAL | MAY | 2011 |
| 185. | DR. RISHAB GUPTA | DEC | 2011 |
| 186. | DR. VIJAY KRISHNAN | DEC | 2011 |
| YEAR – 2012 | |||
| 187. | DR. ANIRUDDHA BASU | MAY | 2012 |
| 188. | DR. TULESHWAR SINGH | MAY | 2012 |
| 189. | DR. ROSHAN BHAD | MAY | 2012 |
| 190. | DR. NANDITA HAZARI | DEC | 2012 |
| 191. | DR. SUNDAR GNANAVEL | DEC | 2012 |
| YEAR – 2013 | |||
| 192. | DR. MRINMAY DAS | MAY | 2013 |
| 193. | DR. ASHOK CHAUDHARY | MAY | 2013 |
| 194. | DR. MADHURIMA GHOSH | MAY | 2013 |
| 195. | DR. SATHYAPRAKASH | MAY | 2013 |
| 196. | DR. SHAILESH JHA | MAY | 2013 |
| 197. | DR. SHAMBHU PRASAD | MAY | 2013 |
| 198. | DR. RAJU BHATTARAI | MAY | 2013 |
| 199. | DR. DEEKSHA ELWADHI | MAY | 2013 |
| 200. | DR ARUMUGANATHAN ANMUGAVINAYAGAM | DEC | 2013 |
| 201. | DR. MOHIT VARSHNEY | DEC | 2013 |
| YEAR - 2014 | |||
| 202. | DR. NRIPENDRA KUMAR | MAY | 2014 |
| 203. | DR. ANIL YADAV | MAY | 2014 |
| 204. | DR. NISHANTH KN | MAY | 2014 |
| 205. | DR. SAURABH KUMAR | MAY | 2014 |
| 206. | DR. ROHIT ALOK | DEC | 2014 |
| 207. | DR. PARVESH BATRA | DEC | 2014 |
| 208. | DR. ANANYA MAHAPATRA | DEC | 2014 |
| 209. | DR. ANKIT GUPTA | DEC | 2014 |
| 210. | DR. VAIBHAV PATIL | DEC | 2014 |
| YEAR – 2015 | |||
| 211. | DR. SHOBHIT JAIN | MAY | 2015 |
| 212. | DR. PAWAN SHARMA | MAY | 2015 |
| 213. | DR. ARGHYA PAL | MAY | 2015 |
| 214. | DR. ARPIT PARMAR | MAY | 2015 |
| 215. | DR. DARA SINGH POONIA | MAY | 2015 |
| 216. | DR. PRASHANT GUPTA | MAY | 2015 |
| 217. | DR. SHYAMANAND ROY | DEC | 2015 |
| 218. | DR. ASHISH PAKHRE | DEC | 2015 |
| YEAR – 2016 | |||
| 219. | DR. POOJA PATTNAIK | MAY | 2016 |
| 220. | DR. SNEHIL GUPTA | MAY | 2016 |
| 221. | DR. SURESH THAPALIYA | MAY | 2016 |
| 222. | DR. SACHIN KUMAR | MAY | 2016 |
| 223. | DR. ABHINAV PANDEY | MAY | 2016 |
| 224. | DR. NAJEF MOIDEEN | DEC | 2016 |
| 225. | DR. SARTAJ DEEPAK | DEC | 2016 |
| 226. | DR. RISHI GUPTA | DEC | 2016 |
| 227. | DR DEEPAK CHARAN | DEC | 2016 |
Centre for Advanced Research and Excellence in Neuromodulation ( CARE )
Centre for Advanced Research and Excellence in Neuromodulation ( CARE )
Patient Education
| Serum lithium estimation | |
| Timings for sample collection | 9.30 am to 12.30 p.m. (Monday to Saturday) |
| Timings for Report: | Approximately one hour |
| ECT (Modified) | Monday & Friday |
| Repetitive Transcranial Magnetic Stimulation (rTMS) | Monday to Friday |
On the basis of recent research we all know that there is neurobiological process involved in our emotion, memory and behavior. Transcranial Magnetic brain stimulation (TMS) is a technique for gently modulating the brain cells. It utilizes a specialized electromagnet that generates brief magnetic pulses, roughly up to the strength of an MRI scanner’s magnetic field but much more focused. The magnetic pulses pass easily through the skull just like the MRI scanner but because they are short pulses and not a static field, they can modulate the underlying cerebral cortex. It has also been shown that these changes may last for long period of time after stimulation is stopped leading to therapeutic effect.
TMS is currently a potential treatment for patients with Depression, patients who experience hallucinatory "voices" and a variety of other Psychiatric and Neurological disorders. For patients with Depression, many research studies have shown clinical improvement following rTMS.
For patients reporting auditory hallucinations (voices), research has not been as extensive but initial results have been promising and suggest that low frequency TMS administered to parts of the brain underlying speech perception may reduce these voices.
The Food and Drug Administration (USA) has approved rTMS for Depressive disorder just 3 months back. TMS has been approved in Canada and Israel as a treatment of Depression for patients who have not responded to medications.
rTMS is an outpatient procedure and does not require anesthesia or sedation. Few patients may experience discomfort at the site of stimulation for short time. Generally rTMS produces a slight tapping sensation on the scalp. When administered at selected stimulation sites it can cause little contraction of the muscles of the scalp. Mild headache and transient lightheadedness may sometimes result from rTMS. These symptoms usually resolve by themselves shortly after the treatment is over.
It depends on the treatment/research protocol, but generally each session takes about 20 minutes. Treatment protocols vary in duration, but most require at approximately 10-15 sessions given five times per week.
The brain is directly stimulated by rTMS. However studies reported so far, no loss of memory, impaired concentration and other cognitive impairment. This is in contrast to the well known cognitive side effects associated with Electroconvulsive therapy (ECT)
The main risk of rTMS is rare induction of seizure. However with proper safety guidelines chances of seizures are negligible. For stimulation at low frequency no seizures have been reported.
Patient Education
| Serum lithium estimation | |
| Timings for sample collection | 9.30 am to 12.30 p.m. (Monday to Saturday) |
| Timings for Report: | Approximately one hour |
| ECT (Modified) | Monday & Friday |
| Repetitive Transcranial Magnetic Stimulation (rTMS) | Monday to Friday |
On the basis of recent research we all know that there is neurobiological process involved in our emotion, memory and behavior. Transcranial Magnetic brain stimulation (TMS) is a technique for gently modulating the brain cells. It utilizes a specialized electromagnet that generates brief magnetic pulses, roughly up to the strength of an MRI scanner’s magnetic field but much more focused. The magnetic pulses pass easily through the skull just like the MRI scanner but because they are short pulses and not a static field, they can modulate the underlying cerebral cortex. It has also been shown that these changes may last for long period of time after stimulation is stopped leading to therapeutic effect.
TMS is currently a potential treatment for patients with Depression, patients who experience hallucinatory "voices" and a variety of other Psychiatric and Neurological disorders. For patients with Depression, many research studies have shown clinical improvement following rTMS.
For patients reporting auditory hallucinations (voices), research has not been as extensive but initial results have been promising and suggest that low frequency TMS administered to parts of the brain underlying speech perception may reduce these voices.
The Food and Drug Administration (USA) has approved rTMS for Depressive disorder just 3 months back. TMS has been approved in Canada and Israel as a treatment of Depression for patients who have not responded to medications.
rTMS is an outpatient procedure and does not require anesthesia or sedation. Few patients may experience discomfort at the site of stimulation for short time. Generally rTMS produces a slight tapping sensation on the scalp. When administered at selected stimulation sites it can cause little contraction of the muscles of the scalp. Mild headache and transient lightheadedness may sometimes result from rTMS. These symptoms usually resolve by themselves shortly after the treatment is over.
It depends on the treatment/research protocol, but generally each session takes about 20 minutes. Treatment protocols vary in duration, but most require at approximately 10-15 sessions given five times per week.
The brain is directly stimulated by rTMS. However studies reported so far, no loss of memory, impaired concentration and other cognitive impairment. This is in contrast to the well known cognitive side effects associated with Electroconvulsive therapy (ECT)
The main risk of rTMS is rare induction of seizure. However with proper safety guidelines chances of seizures are negligible. For stimulation at low frequency no seizures have been reported.
Clinical Statistics (2005 - 06)
No. of beds available-30
Patient Care
| New | Old | Total | |
| General OPD | 1429 | - | 1429 |
Specialty clinic
| New | Old | Total | ||
| a) | Child Guidance | 458 | 272 | 730 |
| b) | Walk-in-clinic | 14116 | 23947 | 38063 |
| c) | De-addiction | 172 | 989 | 1161 |
| Total | 16175 | 25208 | 41383 | |
| Grand Total | 23886 | 72386 | 96272 |
Admission 435
Discharge 431
Clinical Statistics (2005 - 06)
No. of beds available-30
Patient Care
| New | Old | Total | |
| General OPD | 1429 | - | 1429 |
Specialty clinic
| New | Old | Total | ||
| a) | Child Guidance | 458 | 272 | 730 |
| b) | Walk-in-clinic | 14116 | 23947 | 38063 |
| c) | De-addiction | 172 | 989 | 1161 |
| Total | 16175 | 25208 | 41383 | |
| Grand Total | 23886 | 72386 | 96272 |
Admission 435
Discharge 431
| Name of Faculty | Designation | Designated OPD Days in Psychiatry OPD |
|---|---|---|
डॉ प्रताप शरण | Professor and HOD प्राध्यापक और विभागाध्यक्ष | Tuesday,Friday मंगलवार, शुक्रवार |
डॉ राजेश सागर | Professor प्राध्यापक | Wednesday, Saturday बुधवार, शनिवार |
डॉ नंद कुमार | Professor प्राध्यापक | Monday,Thursday सोमवार, गुरुवार |
डॉ ममता सूद | Professor प्राध्यापक | Tuesday,Friday मंगलवार, शुक्रवार |
डॉ रमनदीप | Professor प्राध्यापक | Wednesday, Saturday बुधवार, शनिवार |
डॉ सुजाता सतपथी | Professor प्राध्यापक | Monday,Wednesday, Thursday सोमवार, बुधवार, गुरुवार |
डॉ कौशिक सिन्हा देब | Additional Professor अतिरिक्त प्राध्यापक | Monday,Thursday सोमवार, गुरुवार |
डॉ रोहित वर्मा | Additional Professor अतिरिक्त प्राध्यापक | Monday,Thursday सोमवार, गुरुवार |
डॉ बिचित्रा नंदा पात्रा | Additional Professor अतिरिक्त प्राध्यापक | Wednesday, Saturday बुधवार, शनिवार |
डॉ गगन हंस | Additional Professor अतिरिक्त प्राध्यापक | Tuesday,Friday मंगलवार, शुक्रवार |
DrVaibhav Patil डॉ वैभव पाटिल | Assistant Professor सहायक प्राध्यापक | Friday शुक्रवार |
डॉ विजय प्रसाद बर्रे | Assistant Professor सहायक प्राध्यापक | Tuesday,Friday, Saturday मंगलवार, शुक्रवार, शनिवार |
डॉ निष्ठा चावला | Assistant Professor सहायक प्राध्यापक | Monday,Thursday सोमवार, गुरुवार |
डॉ प्रीति क | Assistant Professor सहायक प्राध्यापक | Tuesday, Wednesday, Saturday मंगलवार, बुधवार, शनिवार |
डॉ. स्वाति केडिया गुप्ता | Assistant Professor सहायक प्राध्यापक | Monday, Tuesday, Thursday सोमवार, मंगलवार, गुरुवार |
| Name of Faculty | Designation | Designated OPD Days in Psychiatry OPD |
|---|---|---|
डॉ प्रताप शरण | Professor and HOD प्राध्यापक और विभागाध्यक्ष | Tuesday,Friday मंगलवार, शुक्रवार |
डॉ राजेश सागर | Professor प्राध्यापक | Wednesday, Saturday बुधवार, शनिवार |
डॉ नंद कुमार | Professor प्राध्यापक | Monday,Thursday सोमवार, गुरुवार |
डॉ ममता सूद | Professor प्राध्यापक | Tuesday,Friday मंगलवार, शुक्रवार |
डॉ रमनदीप | Professor प्राध्यापक | Wednesday, Saturday बुधवार, शनिवार |
डॉ सुजाता सतपथी | Professor प्राध्यापक | Monday,Wednesday, Thursday सोमवार, बुधवार, गुरुवार |
डॉ कौशिक सिन्हा देब | Additional Professor अतिरिक्त प्राध्यापक | Monday,Thursday सोमवार, गुरुवार |
डॉ रोहित वर्मा | Additional Professor अतिरिक्त प्राध्यापक | Monday,Thursday सोमवार, गुरुवार |
डॉ बिचित्रा नंदा पात्रा | Additional Professor अतिरिक्त प्राध्यापक | Wednesday, Saturday बुधवार, शनिवार |
डॉ गगन हंस | Additional Professor अतिरिक्त प्राध्यापक | Tuesday,Friday मंगलवार, शुक्रवार |
DrVaibhav Patil डॉ वैभव पाटिल | Assistant Professor सहायक प्राध्यापक | Friday शुक्रवार |
डॉ विजय प्रसाद बर्रे | Assistant Professor सहायक प्राध्यापक | Tuesday,Friday, Saturday मंगलवार, शुक्रवार, शनिवार |
डॉ निष्ठा चावला | Assistant Professor सहायक प्राध्यापक | Monday,Thursday सोमवार, गुरुवार |
डॉ प्रीति क | Assistant Professor सहायक प्राध्यापक | Tuesday, Wednesday, Saturday मंगलवार, बुधवार, शनिवार |
डॉ. स्वाति केडिया गुप्ता | Assistant Professor सहायक प्राध्यापक | Monday, Tuesday, Thursday सोमवार, मंगलवार, गुरुवार |
Submitted to
Indian Psychiatric Society (IPS)
Department of Psychiatry,
All India Institute of Medical Sciences, New Delhi
Report Citation:
This report should be cited as:
Department of Psychiatry, AIIMS (2008). ICD-11: Draft Proposal for Changes in the Classification of Mental and Behavioural Disorders
Editor:
Pratap Sharan,
Professor,
Department of Psychiatry,
AIIMS, New Delhi
Rajat Ray,
Professor,
Chief, National Drug Dependence Treatment Centre and Head, Department of Psychiatry,
AIIMS, New Delhi
Dr Pratap Sharan had full access to all of the materials in this report and takes responsibilityfor the integrity and accuracy of its summarization.
Contents
| S. No. | Chapter | Pages |
|---|---|---|
| 1 | Introduction | 1 |
| 2 | Classification of Psychiatric Disorders: General Issues | 2-12 |
| 3 | Organic, including Symptomatic, Mental Disorders | 13-18 |
| 4 | Mental and Behavioural Disorders due to Psychoactive Substance Use | 19-24 |
| 5 | Schizophrenia, Schizotypal and Delusional Disorders | 25-34 |
| 6 | Mood Disorders | 35-46 |
| 7 | Neurotic, Stress Related and Somatoform Disorders | 47-50 |
| 8 | Behavioural Syndromes associated with Physiological Disturbances and Physical Factors | 51-59 |
| 9 | Personality Disorders | 60-70 |
| 10 | Categories ‘F70 – F98’ | 71-76 |
The draft proposal for changes in the classification of mental and behavioural disorders towards ICD 11 was prepared under the aegis of the Department of Psychiatry, All India Institute of Medical Sciences for consideration in an Indian Psychiatric Society (IPS) Committee, which will send its recommendations to the World Psychiatric Association (WPA). The draft proposal is also available on the Departmental website.
Each chapter was prepared by faculty members, who were assisted by residents of the department. In preparing their suggestions the authors often referred to the Robins and Guze criteria to evaluate the validity of various categories and specifiers. The initial suggestions made by the authors were discussed in a series of departmental meetings comprising of the entire professional staff of the department and thus the final draft proposal has received inputs from more than 30 trained professional staff from various disciplines (Psychiatry, Clinical Psychology, and Biochemistry) and another 20 professionals in training.
Each chapter of the draft proposal ha the following structure:
CLASSIFICATION OF PSYCHIATRIC DISORDERS: GENERAL ISSUES
Pratap Sharan, MD, PhD, Shiv Prakash, MD
Recommendations
Supporting evidence for proposed changes
The clinician is focused on treatment and rehabilitation of individuals or groups while the public health expert seeks to employ a broader range of health interventions which include promotion, preventive, curative or rehabilitative strategies aimed at populations and groups at risk. Thus, the clinicians have a relatively greater interest in the current condition of the patient, and diagnostic categories that are narrow and which predict treatment response; while the public mental health expert is relatively more interested in risk/ causative/ developmental factors toward pathology, service delivery to the population, diagnostic categories that vary in breadth (broad for communicating with non-experts and narrow for some specific interventions) and are predictive of response to the entire range of preventive efforts. Public health experts also look at the broader spectrum of health and their determinants (Mezzich 2002a, 2002b).
Classificatory systems have public mental health implications, e.g. concept of diagnosis is crucial to epidemiology and surveillance of population health (Mezzich 2002a). However, since public health is not the explicit focus of the classificatory exercises, many issues that are relevant to public health, have not been addressed. For example, diagnoses like mixed anxiety depression and age-related cognitive decline are disputed because they are below an ‘appropriate’ threshold, but they contribute significantly to disorder burden. Within the spectrum of mental health intervention, prevention and promotion have become realistic and evidence-based alternatives. These bring new challenges to classification system - the challenge of defining boundaries of disorders, risk categories and normality (Mrazek and Hagerty 1994; Mrazek and Hosman 2002).
Public health also has much to contribute to classification. In an effort to move from descriptive criteria based approach to an etiology based approach, epidemiology serves as the bridge between proposed aetiologies or disease mechanisms and potential manifestations (Caine 2003).
Mental health has been conceptualized in two broad ways: ‘positive’ mental health (Jahoda, 1958; Maslow 1968; Tudor 1996) and ‘functional’ metal health (Hosman 1997). The former considers mental health in terms of qualities such as self-confidence, identity, ability to love, happiness, etc. that are seen as worthwhile to promote because they represent a fundamental human values in themselves. The ‘functional model’ considers mental health more in terms of psychological resources and abilities, that people need to have for a satisfying and productive life e.g. in the domains of health, relationships, work, ability to cope with stress, etc.. For this last part, the functional model of mental health coincides with the concept of protective factors.
A growing body of cross-cultural evidence indicates that various psychological, social and behavioural factors such as secure attachment, an optimistic outlook on life with a sense of purpose and direction, effective strategies for coping with challenge, emotionally rewarding social relationships, etc. are protective of health and supportive to positive mental health (Cacioppo et al 2000; Ryff and Singer 2003). Such protection facilitates resistance (resilience) to disease (disorder), minimizes and delays the emergence of disabilities and promotes more rapid recovery from illness (WHO 2002). Good mental health may also be facilitated by religious/ spiritual feelings, experience, orientation and world view (Bhugra and Osbourne, 2004). Thus, it has to be borne in mind that definition of mental health may be at least partially culture-bound with both commonalities and differences between cultures.
The recognition of positive mental health features in psychiatric patients would also substantially reduce the stigma associated with mental illness. A similar reorientation with reference of classification was achieved in the transformation of International Classification of Impairments, Disabilities and Handicaps (WHO 1980) to International Classification of Functioning (WHO 2001b).
In many situations prevention enhances options for managing disorders e.g. it may be possible to prevent many cases of conduct disorders, while it may be fairly difficult to treat them (Reid 1993). Prevention may also be significant for many individuals, who do not have access to treatment or those who receive inappropriate services. A growing number of randomized controlled prevention trials and community trials have offered evidence for significant changes on a wide variety of targeted outcome indicators, including indicators for risk and protective factors, mental and behavioural disorders and improvements in mental health (Mrazek and Haggerty 1994; Clarke et al 1995; Hosman and Llopis 1999).
Risks do not occur in isolation; in fact many risks cannot be disentangled in order to be considered in isolation as they act at different levels which vary over time. Clearly, one outcome can be caused by many risk factors (equifinality – multiple pathways to the same disorder), but similarly one risk factor can lead to many outcomes (multifinality – overlapping pathways to different disorders). Further, there is a non-linear relationship between risk factors and outcomes. Although one or two risk factors may show little prediction to poor outcome, there are rapidly increasing rates of disorders with additional risk factors (Rutter 1979; Greenberg et al 2001). Another point that needs to be borne in mind about risks is that some of the distal risks cannot appropriately be defined at the individual level (e.g. social disintegration).
Addition of an axis for risk and protective factors in the classificatory system could serve as the link between etiological understanding of disorders and promotive, preventive, curative and rehabilitative interventions. Risk factors may help in identifying subtypes that may aid in the exploration of pathophysiology and etiology (Andreasen and Carpenter, 1993). The axis on risk factors could be used as a matrix with Axis I (clinical diagnosis), to eliminate the need for some specifiers. For example, postpartum depression could be labelled as depression on Axis I and the specifier 'postpartum' would appear on the axis for risk factors. This axis could replace the Axis III and IV of DSM IV and Axis III of ICD-10 as it is broader in scope. It will end the artificial mind-body divide in relation to etiological factors. In addition, it will emphasize distal social and developmental causes of disorders which are not emphasized in the present classification systems and can be major foci of public mental health policies.
A substantial volume of literature suggests that subthreshold conditions have considerable public health importance. Subthreshold depressions (e.g. mixed anxiety depression, recurrent brief depression, minor depression, etc.) are reported to occur in up to 24% of the general adult (Horwath et al 1992) and 52% of the elderly (Pincus et al 1999) populations. Further, it is difficult to differentiate subthreshold depression and major depressive disorder on the basis of demographic and clinical characteristics; medical and psychiatric comorbidity; dysfunction (subtheshold depression cause five-times more disability days than major depressive disorders and dysthymia combined); follow up studies; outcome (in terms of chronicity and suicide), and a family vulnerability for major depression (Broadhead et al 1990; Johnson et al 1992; Judd et al 1998).
However, since less than one-fourth of subjects with minor depression develop major depression (Broadhead et al 1990; Wells et al 1992) in most cases subthreshold depression should be considered as an indicator of risk for developing threshold depression - a focus for indicated prevention (a subcategory of primary prevention). Subthreshold depressive categories should therefore be included in the classification under the rubric of prevention relevant categories.
Regier et al (2002) suggest that the diagnostic thresholds in current classificatory systems reflect an emphasis on treatment over prevention. Altering the threshold for caseness will change the latitude for prevention and treatment within the public mental health spectrum. Assignment of boundaries between normal states, high risk states and disorders can be made on the basis of empirical studies of risk (Vasan et al 2002). Definition of prevention relevant categories would encourage studies aimed at understanding their causation (Pincus et al 1999; 2003) and early intervention for those at risk for future morbidity, comorbidity and mortality rather than limiting intervention to after significant morbidity has occurred.
The preoccupation with over-refined categories and subcategories has led to complex diagnostic systems that are difficult to use in the community setting. Moreover, the evergrowing list of types/subtypes contains many conditions that are rarely diagnosed (Bertelsen 2002).
Definition of broad categories would be useful from the promotion and prevention perspective. Over the last 3 decades, the majority of evidence-based promotive and preventive trials have focused on common or generic protective and risk factors, e.g. interventions for increasing self-esteem, emotional resilience, problem-solving and coping skills (Mrazek and Haggerty 1994; Hosman & Llopis, 1999); and prevention of broad categories such as depression (Rutz et al 1992a; 1992b), anxiety symptoms and disorders (Dadds et al 1999), externalising problems and substance abuse (Wolchik et al 2000), or suicidal behavior (Zenere and Lazarus, 1997). When varying clinical presentation have major risk factors in common, subtyping is less relevant from the preventive perspective.
The increase in number of disorders has added to the problems of comorbidity – nearly one-third of cases in the general population have comorbid psychiatric problems (Wittchen 1996). At least some of these would be artefacts, a function of the number of available categories. Data suggest that much comorbidity in the mental health field is due to shared antecedents (genetic and environmental, e.g. childhood adversity) (Kendler et al 1992; Brown et al 1996; Livesley et al 1998; Mineka et al 1998), a fact that goes against the possibility of independence and chance co-occurrence of disorders. Thus, Krueger et al (1998) found support for a 2-factor model for explaining comorbidity – a latent internalizing factor (depression and anxiety) and a latent externalizing factor (conduct disorder, marijuana and alcohol dependence). The lack of independence between diagnoses could explain the absence of diagnostic specificity of treatment response (Regier et al 2002).
The argument for definition of broad categories is not against the existence of narrower categories. When subtypes have major subtype–specific and malleable determinants, fine divisions of categories could be relevant for prevention, treatment and rehabilitation, wherein strategies are targeted to reduction in number of episodes, duration, severity and dysfunction associated with illnesses and secondary morbidity (McGorry 1992). Hence, close attention should be paid to the number, hierarchy and specificity of categories during revision of classifications.
A life-course approach to study of health and illness has come to dominate public health following the recognition of the fact that risks as well as symptomatic expression of disorders vary across developmental spans (Ingram and Price, 2001) and that exposure to disadvantageous experiences and environments accumulate throughout life to increase the risk of illnesses (WHO 2002).
The need for a developmentally informed diagnostic system is most acute for definition of psychopathology in children and adolescents because most of the current diagnostic systems are based solely on models of adult psychopathology. Ryan et al (1987) and Kashani et al (1997) found that children especially pre-schoolers with depressive disorders presented with somatic complaints and aggressive behaviour and most showed psychomotor agitation. The diagnosis may be overlooked because of the presence of these associated symptoms that are suggestive of an externalising disorder. These findings combined with the observation of Kovacs (1986) that younger children may not be capable of experiencing or reporting the symptoms thought to be representative of major depression, emphasize the need to have developmentally relevant criteria for diagnosis.
Other studies have emphasized the need for greater attention to the life course approach to mental disorders. The results of several prospective longitudinal studies of population based samples of children and adolescents show that retrospective adult studies may seriously overestimate the age at onset of many disorders (Costello et al 1999, Lewinsohn et al 2000). In addition, some disorders e.g. ADHD and major psychoses may show early prodromes (Pine et al 2002). An episode of depression or anxiety is a risk factor for further episodes of same general type of disorder, e.g. major depression and suicide (Kovacs and Devlin 1998; Mineka et al 1998), and attention deficit hyperactivity disorders is a predictor of conduct disorder/antisocial personality disorder, substance use disorder and bipolar disorder (Biederman e al 1998; Faraone et al 1998). Some heterotypic associations are also apparent. High levels of anxiety in children predicted increase in depression over time, however high levels of reported depression in children did not predict increase in anxiety (Kolvin and Trowell 2002). Tic disorder shows longitudinal association with obsessive compulsive disorder with tic decreasing and obsessive symptoms increasing over time (Pine et al 2002). Interplay of biological and environmental risk factors could influence courses both singly and across related disorders, e.g. childhood sexual abuse for externalizing disorders (Brown et al 1996) and kindling for schizophrenia, bipolar and other disorders (Frances and Egger, 1999). Failure to take a life course approach makes the occurrence of such comorbidity perplexing.
Current data show that 85% of the variation in DNA sequence is common to ethnic groups. Such observations suggest that the risk of common illnesses including mental illnesses largely derive from alleles shared across all group of humans, supporting the possibility of having universal syndromes. But variations at the genetic level across ethnic groups (15%) and environmental risk factors provide for the possibility of substantial phenotypic variations across cultures and across time spans (Hyman 2002).
ICD 10 and DSM-IV do not adequately consider the possibility that context affects prototypical manifestations of an illness. It would be desirable to develop a system of classification that is flexible for local and cultural adaptations. For example, in some cultures people may not volunteer sadness as a symptom because a conceptually equivalent term may not exist in the language, or because of stigma attached to it, or because it is not recognized as an illness (Patel 2001). In such circumstances it would be better to use local concepts, e.g. 'Kufungisisa' (thinking too much) in Shona language of Zimbabwe or 'Neurasthenia' in China (Kleinman and Kleinman 1985; Patel 2001). Application of a universally defined criteria set in such cultures in an inflexible way, would lead to gross underestimation of prevalence of somatic symptoms related to depression and also of the prevalence of depression in the population studied (Alarcón et al 2002).
Avoidance of the concept of cultural variations in common psychiatric disorders leads to paradoxical situations. ICD-10 emphasizes adverse medical and psychological consequences in dependence and harmful use categories to ease application across different cultures and countries (Rounsaville 2002). However, development of social consequences more often predates physical and psychological problems in the natural history of pathological substance use disorders. As a consequence, rates as well as test-retest reliability of ICD-10 harmful use were lower than that of DSM-IV abuse (Chatterji et al 1997; Rounsaville 2002). On the other hand, acute and transient psychosis, a culturally informed diagnosis has been shown to have some genetic (Das et al 1999), epidemiological and prognostic validity (Susser et al 1996).
A simple system of psychiatric classification that can readily be translated into indigenous categories of illness is highly desirable. Attempts at crosswalks between ICD-10 and indigenous categories can be seen in Chinese Classification for Mental Disorders-3rd Edition (CCMD-3) (Chen 2002), Latin American Guide for Psychiatric Diagnosis (GLDF) (Berganza et al 2002) and Third Cuban Glossary of Psychiatry (GC-3) (Otero-Ojeda 2002).
The relative validity of these categorical and dimensional approaches rests on a number of empirical considerations (Widiger & Samuel, 2005). An especially important issue concerns the nature of the underlying distributions. Taxometric studies suggest that both latent categories and dimensions are widely distributed. Dimensional models receive extensive support in the broad neurotic spectrum, predominating among the mood and anxiety disorders, e.g. chronic worry and posttraumatic stress (Ruscio et al, 2001). Analyses of depression have yielded mixed results but generally have found evidence of continuity rather than discontinuity (Haslam & Beck, 1994; Ruscio & Ruscio, 2002). However, melancholic depression appears to be better understood as a latent category and there are indications of latent categories in the domain of social anxiety and inhibition. Also, categorical models enjoy more support in the domain of personality disorders than might not have been anticipated.
Dimensional systems allow one to model the severity of dysfunction, not simply its presence versus absence (Clark et al, 1995). A large body of evidence also indicates that the artificial dichotomization of continuous measures leads to substantial losses in reliability, stability and validity (Widiger, 1992). Dimensional approach may also help in preparing for the future inclusion of genetic, imaging, and biochemical elements to psychiatric diagnoses.
Multiaxial evaluation provides a vehicle for describing different aspects of a patient’s condition in order to improve our understanding of the condition and thereby to improve its management. Many multiaxial systems have been proposed and there is much variance among them regarding specific axes (Mezzich et al 1987). However, only a limited number of axes can be included in a system that is manageable in regular work internationally. Economizing arrangements could be considered to accommodate information within the multiaxial system, e.g. Mezzich et al (1987) found two broad and pervasive themes in their review of multiaxial systems: phenomenology and etiological/ associated factors. The latter could accommodate sub themes like biological, psychological, cultural, and spiritual aspects. Axes which cannot be accommodated within a given list could be considered as special - for use with particular populations or situations.
Axis I (categorical diagnoses related to health/ illhealth) would comprise of:
Axis II (dimensions related to health/ illhealth) would comprise of consensually agreed upon dimensions. Some dimensions that can be considered are:
The axis could also accomodate endophenotypes, cognitive structures, defence mechanisms, etc. for which consensus can be obtained.
Axis III (risk, protective and contextual factors) would include consensually agreed upon risk/protective, formative, precipitating and perpetuating factors. The axis would be subdivided into the following dimensions:
DSM-IV and ICD-10 were not particularly well suited for use in non-speciality settings. It is noteworthy that in the 'Beyond Blue' Project, an Australian initiative to combat depression, 'depression' and 'anxiety disorders' were the two major categories used in the skill focused training provided to general practitioners and in media advocacy work (Beyond Blue 2001). Neither ICD-10 nor DSM-IV was adopted.
Primary Care: The ICD-10 has two primary care versions - a concise version (containing 25 conditions) for those with medical training and prescription responsibility and a brief version (containing 6 conditions) for other primary care workers with limited medical training (WHO 1996). Similarly, a primary care version exists for the DSM-IV (APA 1996). The problem with ICD-10 PHC versions is that the categories in the two versions do not match each other and the detailed version of the ICD-10; however, they provide a simple way of classifying mental disorders. The DSM-IV primary care version on the other hand maintains its ties with the detailed DSM-IV but it does not simplify the classification per se, focusing instead on simplifying the process of reaching the DSM-IV classification by following a workbook style, wherein symptoms branch out into diagnostic algorithms (Pingitore and Sansone 1998).
The best solution would be to have three versions of increasing complexity, in which the categories of the more complex version are nested in the broader categories of the less complex system.
General Medical Health System: Trimble (2002) has suggested that ICD/DSM should have links to other classificatory systems, e.g. the international classification of epileptic seizures, movement disorders, lobar atrophies, dementia and sleep disorders (ASDA 1990; Mckeith et al 1996; McKhann et al 1984; Neary et al 1998). This could be achieved in many different ways. One could be to reproduce those classificatory systems/diagnostic criteria within the published ICD/DSM volumes. Another could be providing crosswalks between categories in one system with those in the other system. There is also the case for the provision of similar crosswalk to the classification used by nurses, e.g. Contemprory Nursing Diagnosis Manual of North American Nursing Diagnosis Association (NANDA 1994). Guidance is also needed for linking individual diagnosis to the International Classification of Functioning (ICF) as suggested by Kopelman and Fleminger (2002) and Jenkins et al (2002).
Address for Correspondence: Professor Pratap Sharan, Department of Psychiatry, All India Institute of Medical Sciences, Ansari Nagar, New Delhi – 110029, INDIA. Email: pratapsharan[at]gmail[dot]com
Prof. S. K. Khandelwal, MD, MRCPsych, Dr. Kumar R. Maji, MD
Recommendations
1. Changing the name of the F00-F09 category from – ‘organic, including symptomatic, mental disorders’ to ‘neuropsychiatric disorders including symptomatic, mental disorders’.
2. To place tic disorder under F00-F09 from its current place under F95 (F90 - F98: behavioural and emotional disorders with onset usually occurring in childhood and adolescence).
3. To exclude organic dissociative disorder
The essence of classification system is to arrange something in an ordered fashion instead of placing it haphazardly. From ancient to recent times, various efforts have been made to classify mental disorders, with gradual refinement of the concept of mental disorders and their classifications. ICD-10 (International Classification of Disease - 10th edition) and DSM-IV (Diagnostic and Statistical Manual of Mental Disorders - 4th edition) are the two widely accepted classificatory systems for mental disorders, though certain others country specific classificatory systems do exist.
Mental disorders classificatory system is not only used by psychiatrist, it is also used by other physicians, psychologists, social workers, nurses, occupational and rehabilitation therapists, counselors and other health and mental health professionals. Efforts should be made to make the ICD-11 more clinically useful and acceptable to those who apply it, should have few differences with DSM-V and at the same time, it should keep the layout of existing coding system intact.
Great strides have been made over the past few decades in the field of clinical neuroscience, including functional and structural brain imaging, electrophysiology and electro-diagnosis, cellular and molecular biology, genetics and neuropsychopharmacology. Despite these developments in the field of neuroscience, the understanding of the pathophysiology of mental disorders is still in a nascent state. Therefore, the seminal article by Robins and Guze (1970) is still relevant to the process of revision of classification of mental disorders.
This rubric in ICD-10 covers a range of mental disorders with a common theme of demonstrable etiology in cerebral disease, brain injury, or other insult leading to cerebral dysfunction which may be primary (where the causative factors affect the brain directly) or secondary (where systemic diseases involve brain like other multiple organs). The term ‘organic’ used here means that disorders or syndrome in this category can be attributed to an independently diagnosable cerebral or systemic disease or disorder and the term ‘symptomatic’ is used where the cerebral involvement is secondary to systemic illness (ICD-10, Clinical Descriptions and Diagnostic Guidelines).
The use of the term ‘organcity’ in psychiatric classification is attended with controversy. DSM-II (1968), categorized organic mental disorders as organic brain syndrome (OBS), caused by diffuse brain dysfunction that lead to deficits in orientation and intellectual functioning (e.g. memory, judgement, comprehension) and to changes in affective modulation (lability or shallowness). Subsequently, OBS was replaced by the term organic mental disorders (OMD) in DSM-III (1980), which further made a fundamental distinction between OBS and OMD with reference to absence or presence of etiological factors. In DSM-III-R (1987), all these disorder were placed under the section of ‘Organic Mental Syndromes and Disorders’ which was eventually deleted in the DSM-IV (1994).
In ICD-8 (1969) all organic psychotic conditions were placed along with functional psychoses under the rubric of ‘psychosis’ (290-299). Code 290 to 294 in ICD-8 (290: senile and pre-senile dementia, 291: alcoholic psychosis, 292: psychosis associated with intracranial infection, 293: psychosis associated with other cerebral condition, 294: psychosis associated with other physical condition) underwent mild modifications and were included in ICD-9 under a new term: ‘organic psychotic conditions (290-294). The latest revision ICD-10 (1992) retained the term ‘organic’ for this group of disorders.
Discussion
The term organic is very difficult to define and moreover, it incorrectly implies non-biological basis for non-organic (functional) psychiatric illnesses. In addition, merely placing ‘organic’ in front of a variety of symptom or syndromes (hallucinosis, catatonic disorder, delusional disorder, mood disorder, anxiety disorder, dissociative disorder, emotionally labile disorder), does not advance classification keeping in view the future development in neurosciences (Kopelman et al 2002). The term ‘neuropsychiatric disorder’ is probably the appropriate substitute for organic mental disorder, owing to its broad spectrum coverage. For example, head-injury, within neuropsychiatric disorders, would include (besides dementia due to head trauma and post-concussional syndrome) confusional states, memory disorders, executive and personality changes, head-injury related mood changes, etc. Epilepsy is another disorder where a number of specific neuropsychiatric syndromes could be incorporated.
Code F06 in ICD-10, uses the term ‘other mental disorders due to brain damage and dysfunction and to physical disease,’ while DSM-IV uses the term ‘mental disorders due to general medical condition.’ In the ICD-10 code, the word ‘organic’ has been placed before psychiatric disorders which often manifest in certain medical conditions. More clarity and specificity is required in describing these conditions or subtypes to avoid confusion among other health professionals who often witness such conditions, which is probably not possible by mere presence of the term ‘organic’ before such entity. Example of more appropriate description would be – catatonic disorder in Vit-B12 deficiency, delusional (schizophrenia – like) disorder in epilepsy etc. (Kopelman et al 2002). However, this type of description is reminiscent of ‘combination categories’ of ICD-8. Therefore, more accurate and appropriate description of these conditions requires utilization of separate independent axes.
Tic disorders comprise a group of disorders, such as, transient tic disorder, chronic motor or vocal tic disorder, combined vocal and multiple motor tic disorder (de la Tourette’s syndrome), other tic disorder and tic disorder unspecified. Currently, ‘tic disorder’ has been placed in the category of ‘behavioural and emotional disorders with onset usually occurring in childhood and adolescence’ (F90-F98; F95) of ICD-10. Tic disorder has also found a place under G-25 [diseases of nervous system, other extrapyramidal and movement disorders] of ICD-10, as an inclusion term. Though the onset predominantly occurs during childhood and adolescence, onset has been reported in adult age group also (Burd et al, 1986a, b).
Discussion
Tic disorders have a substantial genetic basis; with first degree relatives having up to ten fold increased risk (Tourette Syndrome Association International Consortium for Genetics 1999). It also has high concordance rate in monozygotic twin (53%) in comparison to dizygotic twins (8%) (Leckman et al 1995b). Compelling indirect evidence from pharmacological studies indicates involvement of basal ganglia (Leckman et al 1995b). Electrical stimulation of the amygdala produces motor and vocal responses resembling tics (Jadresic 1992). Though the definite pathophysiology of tic disorders is not known but internationally a research consensus has been reached which suggest that the basal ganglia and the related thalamo-cortical circuitry is involved.
We proposes that tic disorder should be placed under ‘Neuropsychiatric disorder’ currently ‘F00-F09’, instead of its placement under ‘F90-F98’ as in ICD-10. Further information about the onset of illness could well be coded using a fifth character code.
The term ‘dissociative’ has replaced the older term ‘hysteria’ in current ICD-10. The basic theme in dissociative disorder is disruption (partial or complete) in the usually integrated function of consciousness, memory, identity, perception and motor control, in the absence of any physical disorder that might explain the symptoms. The evidence for psychological causation has been presumed in the form of clear or unclear (if patient denies) stressful events or problems or disturbed relationship with onset. ICD-10 has given preference of plausible mechanism for causation by using the term ‘dissociation’ instead of older term ‘psychogenic’ for this condition to avoid etiological assumptions.
‘Organic dissociative disorder’ has been placed in category of F06 (other mental disorders due to brain damage and dysfunction and to physical disease) of current ICD-10 whereas in DSM–IV, no such entity exists.
Discussion
The term ‘organic dissociative disorder’ is paradoxical. The mere presence of organic lesion somewhere in the brain of an individual, which is unrelated with dissociative symptoms can’t make him/her a patient with organic dissociative disorder. If the lesion is related with the symptoms then the diagnosis cannot remain dissociative, and in that situation diagnoses like organic amnestic syndrome would be a more appropriate as per the current ICD-10 classificatory system. Moreover, there is dearth of literature on this issue, raising questions about its diagnostic validity.
We propose that such a paradoxical term should be excluded from ICD-11.
As per the coding conventions of ICD-10, each of the categories has a code composed of four characters. The first character is a letter which designates the chapter – a group of diseases of particular specificity. The second character – a digit describes a subgroup of disorders, e.g. organic, including symptomatic, mental disorder. The third character, also a digit, describes the disease or disorder and the fourth character – a digit, details the condition more elaborately e.g. describing its course and other characteristics. A further fifth, sixth and seventh character could be used as a specifier to have more accurate descriptions.
The ICD-10 chapter F categorizes dementia utilizing four different codes (F00 -dementia in Alzheimer’s disease, F01 - vascular dementia, F02 – dementia in other diseases classified elsewhere, F03 - unspecified dementia), whereas DSM-IV places different types of etiologically based dementias under a single section (dementia), because dementias share common symptoms and presentation.
Discussion
Placement of dementia in ICD-10, utilizing four different codes invites criticism regarding the diagnostic validity and reliability of each code for dementia. Dementia, characterized by the development of multiple cognitive deficits (including memory impairment) that are due to the multiple etiologies (e.g. Alzheimer’s disease, cerebrovascular disease or combination of both), or due to direct physiological effects of general medical conditions or to the persisting effects of substance, is a clinical diagnosis (Boise et al 1999). Having four different codes for dementia in ICD-10 is anomalous with respect to the basic coding convention of ICD-10, as all of these apparently separate disorders have common symptomatology. Placing dementia as a single code (as is the case with DSM-IV) would likely improve its diagnostic stability and probably would improve its applicability and usefulness in clinical practice and research.
Therefore, we propose that dementia should have a single code with further sub typing, based on probable etiological factor (fourth character). Further specification could be achieved with fifth and sixth characters. An example is given below:
F - Mental health chapter
0 - Neuropsychiatric disorder
0 - Dementia
0 - Alzheimer’s disease
0 - Early onset
However, some members of the Department suggested caution with this recommendation based on the argument that classification was not only meant to code disorders but also to assist in research related to aetiology, outcome and prognosis; and also that such a change would require shifting of conditions from their current places, e.g. alcohol and other substance induced dementia.
In clinical practice of psychiatry, we often notice psychotropic induced psychiatric conditions which would require urgent attention and proper management, e.g. lithium toxicity, valproate toxicity, neuroleptic malignant syndrome (NMS), acute dystonia, tardive dyskinesia, serotonin syndrome etc.
Currently these conditions are placed in ICD-10 either in the chapter of nervous system disease [G21 (secondary Parkinsonism), G24 (dystonia), G25 (other extrapyramidal and movement disorder)] or in the chapter of Y40-Y59 (Drugs, medicaments and biological substances causing adverse effects in therapeutic use).
DSM-IV placed these conditions under the rubric of ‘other conditions that may be a focus of clinical attention’.
Discussion
In the coming years, more developments are expected in the field of neuropsycho-pharmacology with newer pharmacological molecules to treat psychiatric disorder. In clinical psychiatric practice, medication induced problems are very common and some of the conditions have poor prognosis which often require clinical attention. Proper management of these conditions would require an understanding and adequate knowledge about these conditions. These conditions fulfil features of ‘organicity’ with temporal association, clear and consistent clinical descriptions, possible explainable pathophysiology and good diagnostic reliability and validity; hence, they deserve a place in F00-F09.
The house, however, felt that their placement within codes for physical disorders was adequate if they did not cause specific mental syndromes.
The characteristic feature of this disorder is a decline in cognitive performance (memory, learning, or concentration) to an extent that is insufficient to make a diagnosis of dementia, delirium or organic amnestic disorder. However, the objective tests indicate deficits and the individual experiences distress or difficulty in carrying out usual activities. The disorder has been placed under the code F06 (other mental disorder due to brain damage and dysfunction and to physical disease). DSM-IV does not have such a diagnostic entity. However, DSM-IV includes mild neurocognitive disorder in the category of cognitive disorder not otherwise specified.
Discussion
The ICD-10 (Clinical Descriptions and Diagnostic Guidelines) mentions that the boundaries of this category (mild cognitive disorder) are still to be firmly confirmed. Mild cognitive disorder as a diagnostic entity fails to differentiate between age related cognitive change, old age specific cognitive problems, and the presence of psychopathology (depression, anxiety) with genuine mild cognitive deficiency. Various outcome studies have failed to demonstrate its diagnostic stability or utility as a predictor of dementia (Christensen et al. 1995, Christensen et al. 1997, Schroder et al. 1998, Ritchie et al. 2001, Larrieu et al. 2002, Kumar et al. 2005). Therefore, it was proposed that this entity should not be included as a separate category in ICD-11. If included, it should be kept in the unspecified category of mental disorders.
However, the house wished to retain this category because it was felt that it is a common condition and more studies are required before it is excluded.
Address for Correspondence: Dr. S. K. Khandelwal, Professor, Department of Psychiatry and National Drug Dependence Treatment Centre, All India Institute of Medical Sciences, New Delhi-110029, India. Fax: +91 11 26588663. E-mail:
ICD-11: DRAFT PROPOSAL FOR CHANGES IN THE ‘MENTAL AND EHAVIOURAL DISORDERS DUE TO PSYCHOACTIVE SUBSTANCE USE’ SECTION
Tripathi BM, MD, MRCPsy; Jhanjee S, MD, DNB; Kattimani S, MD
Suggestion: removal from diagnostic system
Currently, this diagnosis is applicable to alcohol use only and the clinical utility and diagnostic validity of this category has not been established. Hence, this category needs to be removed from the classificatory system.
Caffeine is a commonly used psychoactive substance and its use is socially sanctioned across cultures. Current categorization of caffeine with stimulants suggests that caffeine is a drug of potentially abuse. This has treatment and policy implications, hence, caffeine should be removed from this category. However, since coding inappropriate use of caffeine has some clinical utility, it may be coded in the Z category.
Suggestion: Replacement of the term ‘harmful use’ by the term ‘misuse’ and proposal for new diagnostic criteria.
Proposed diagnostic criteria for ‘misuse of psychoactive substance’ are as under:
This diagnosis requires that at least one of the criteria mentioned below is met, but the criteria for dependence syndrome are not fulfilled.
Suggestion: The current subcategories, F1x.21, F1x.22, and F1x.23 should be subsumed under a single subcategory named ‘F1x.21 supported abstinence’.
In order to simplify and make room for growing evidence in favour of non-pharmacological interventions in maintaining abstinence, the currently existing subcategories like F1x.21-currently abstinent but in a protected environment, F1x.22-currently abstinent on a clinically supervised maintenance or replacement regime and F1x.23- currently abstinent but receiving treatment with aversive or blocking drugs, should be subsumed under a single subcategory of ‘supported abstinence’.
In view of their clinical utility these two subcategories should be incorporated in the classificatory system.
Suggestion: Injecting drug use should be included in the classification either as a specifier or in the Z Category.
In view of clinical and public health implications of using drugs via parenteral route, this needs to be documented either as a specifier in this chapter or needs to be placed under the Z category.
Supporting evidence for proposed changes
I. F1x.07-Pathological intoxication
There is no Indian or International literature supporting the clinical utility and validity of this diagnostic category. The inter-rater reliability of this condition is poor and other factors may be responsible for such a presentation, e.g. personality traits, metabolic changes and the social context under which alcohol is consumed. An example of the pragmatic difficulties associated with its use is the forensic situation, where it may be difficult to defend the diagnosis due to lack of scientific evidence, and lack of expert consensus (Winckler 1999). Hence, it would be better to remove from this category from the classificatory system.
II. F15-Mental and behavioral disorders due to use of other stimulants, including caffeine
Caffeine has been placed in F15 along with other stimulants. The ‘other stimulants’ are psychoactive substances with known abuse liability and potential to produce dependence. Current categorization suggests that caffeine is a potentially abusive drug. This implies that a large population consuming caffeine has a psychiatric problem (with potential for stigmatization) and is in need of treatment intervention. Placing it along with other stimulants in this category does not do justice to such a widely used substance. Hence, caffeine should be removed from this category. Since, the presence of this category may still retain some clinical utility as a condition meriting health attention in specific situations, inappropriate use of caffeine may be coded in the Z category.
III. F1x.1 Harmful use: Change in title and criteria for diagnosis
Current diagnostic criteria for ‘harmful use of psychoactive substance’ require that actual damage should have been caused to the mental or physical health of the user. The diagnosis is arrived at by assessment of retrospective damage done to the subject and it does not consider the potential harm by use of the psychoactive substance in the future. This makes the diagnosis ‘harmful use’ very restrictive, as it cannot be applied to many individuals who may benefit from clinical intervention. Further, many studies have documented poor inter-rater reliability for this diagnostic category (Pull et al, 1997) and the concordance between ‘abuse’ in DSM-IV and ‘harmful use’ in ICD-10 is low (Hasin 2003). To obviate these shortcomings a change in current diagnostic criteria are proposed, as above.
The term ‘harmful use’ may be replaced by the term ‘misuse of psychoactive substance.’ Other terms like ‘abuse’ of psychoactive substance was not considered because of the derogatory connotation attached with the word while the term ‘hazardous use of psychoactive substance’ may highlight the dangerousness involved in the substance use, which may not be universal for all psychoactive substances. The term ‘dysfunctional use’ was considered but the house felt that ‘misuse’ had greater acceptability in current scientific discourse.
IV. Consolidation of subcategories F1x.21, F1x.22, F1x.23 under a single subcategory named ‘F1x.21 supported abstinence’
The current subcategories, F1x.21, F1x.22, and F1x.23 are:
These subcategories can be brought together under a single subcategory F1x.21- ‘supported abstinence’, to make the coding system more uniform and simple, in light of the fact that abstinence states may be supported by methods other than those mentioned in the existing subcategories such as by involvement in self-help groups like Alcoholic Anonymous(AA), cognitive behavior therapy and other non-pharmacological interventions.
V. Creation of new subcategories F1x.8x Sleep disorders due to psychoactive substance use’ and F1x.8x Sexual dysfunction due to psychoactive substance use
Patients using psychoactive substance commonly report sleep disorders and sexual dysfunction. These conditions act as risk factors for relapse if they are not addressed properly. Kumar and Muthulagan (2004) have documented the presence of sleep disorders in patients abstaining from alcohol and many studies have reported that sexual dysfunctions are common in various disorders related to psychoactive substance use (Kumar et al, 1997; Gupta and Jiloha 1998; Singh 1998).
VI. Inclusion of specifier or new subcategory: injectible drug use (IDU)
In addition to the obvious health risks associated with injection drug use, experts opine that this form of drug use gives rise to a severe form of dependence. Results from the National Household Survey, India (NHS, India), show that 0.1% of the sample reported ‘ever’ -injecting drug use (Ray 2004). Common reasons for shifting to injecting route cited by the sample were - better high, and peer pressure due to association with other IDU users. About 97% reported having shared syringes and 74.2% reported having shared needles (Ray, 2004). Needle sharing and unsafe sexual practices as part of drug use subculture can lead to HIV infection and AIDS in this population of drug users. The rate of HIV seroconversion seems to be significantly more rapid in India than that observed in Western countries (Agarwal et al, 1998; Birla Singh and Sharma 1998). Due to the obvious public health and clinical implications of injection drug use, it merits an inclusion as a specifier in the psychoactive substance use section or a placement in the Z category.
VII. Creation of a new category: Mental and behavioral disorders due to psychoactive substance use of mixed properties
Current classificatory systems categorize psychoactive substances based on their psychoactive properties, viz. hallucinogens, sedatives or stimulants while at the same time some psychoactive substances have been placed under the their respective generic drug classes like opioids, cannabinoids, nicotine, cocaine, etc. There should be uniformity in categorizing psychoactive substances either based on the class of substances they belong to or based on their main psychoactive property. There are psychoactive substances having both stimulant and hallucinogenic properties like MDMA. There may be difficulty in categorizing such substances, and to overcome this, a suggestion to introduce a separate category named ‘mental and behavioral disorders due to psychoactive substance use of mixed properties’ was made. This did not find consensus in the group discussion and hence was dropped from the final proposal.
VIII. To include psychoactive substances like antidepressants and antihistamines with known abuse and dependence producing capability under the category of substance use disorders
There was a suggestion to include other psychoactive substances with proven dependence and withdrawal producing capability like
antidepressants, monoamine oxidase inhibitors (Ananath et al, 1995) and antihistamines (Pal et al, 2005), under the ‘mental and behavioural disorders due to psychoactive substance use’ category, moving them from the existing category of F55.0 (abuse of non-dependence producing substances) in ICD-10. The house felt that in the absence of strong evidence, it would be inappropriate to consider these drugs as psychoactive substances with abuse liability. Hence the suggestion was dropped from the final draft.
IX. To change the title from ‘Psychoactive substance induced psychotic disorders’ to ‘Behavioral and psychological manifestations due to psychoactive substance use’ for better representation of wide array of specific behavioral and psychiatric manifestations due to psychoactive substance use
Subcategories under ‘Psychoactive substance induced psychotic disorders’ may be changed to include a broad array of behavioral and psychological symptoms and syndromes like depressive disorder, panic attacks, obsessive-compulsive disorder, agoraphobia etc. Hence it was proposed to change psychotic disorders to ‘Psychiatric and behavioral changes due to psychoactive substance use’ or ‘Behavioral and psychological manifestations due to psychoactive substance use’. Since any change in the title was likely to replicate the main title ‘Mental and behavioral disorders due to psychoactive substance use’ of this chapter, this suggestion was withheld.
X. Creation of separate category of ‘cannabis induced psychosis’
Cannabis induced psychosis has been extensively described in Indian literature. It was argued that cannabis induced psychosis be considered as a separate independent category under F12.5. It differs from other psychiatric disorders in terms of psychopathology that consists of both psychotic (paranoid delusions) and affective symptoms, and is characterized by rapid changes in symptomatology. Such a presentation cannot be easily categorized into either affective or psychotic disorder (Sarkar et al, 2003; Mallik et al, 2004) and has course and treatment implications. A specific rubric will also draw increased research attention to this condition. The house felt that sufficient literature had not yet accrued to support a separate category of cannabis induced psychosis, so this suggestion was dropped from the final draft.
XI. Sub typing alcohol use disorders
A descriptive study showed that patients with primary alcoholism differ from patients with secondary alcoholism on severity of dependence, presence of interpersonal problems, in their compliance to treatment and in maintaining abstinence in the follow-up period (Ramesh et al, 1996).Some authors have tried to study drinking pattern using multivariate techniques. Based on factor analysis of their data, one group of authors proposed that alcohol use was of 3 types - alcohol abuse, alcohol dependence and social drinking (Mathrubootham et al, 1997). Alcohol dependence could be further classified into low and moderate dependence.Such studies support the exclusion of social drinking from diagnostic categorization, and can help in reduction of false positives for alcohol abuse or dependence. However some authors have used the term ‘problems drinkers’ to identify those who do not fulfilling criteria for alcohol dependence but still require some form of intervention for their alcohol use (Satesh and Sengupta 1997). The house agreed with the onclusions reached by Gupta and Basu (1999) that alcohol subtyping would merit further study before inclusion in the classificatory system.
XII. Sub typing of opioid dependence into early onset and late onset opioid dependence
Some authors have suggested the differentiation between opioid dependence of early onset defined as age less than 20 years at the initiation of opioids and late onset defined as age more than 20 years at the initiation of opioids. There appears to be significant difference between the two groups regarding substance use pattern and presence of psychopathology, which might need to be considered in treatment planning (De et al, 1998).However, the house felt that the evidence for the use of this specifier was not compelling as yet.
XIII. Inclusion of protracted withdrawal as specifier
There was suggestion to consider ‘protracted withdrawal state’ as a specifier besides the existing F1x.3 withdrawal state, which is an acute physiological state due to sudden cessation or decrease in the quantity of psychoactive substance on which an individual is dependent. It has been well established that protracted withdrawal is one of the risk factor for relapse in cases of psychoactive substance use disorders (Satel et al, 1993).However, the house felt that there was not enough evidence to support the separation of acute and protracted withdrawal states.
Concluding comments:
ICD revision process should also consider the identification of risk factors for relapse and factors that alter prognosis and intervention strategies. The multiaxial system similar to that suggested by WPA workgroup in 1994 may be used with some alteration (Kastrup 2002). It needs to be established whether diagnostic criteria needs to be changed in order to make its applicable in special populations like women (Selvaraj et al, 1997; Prasad et al, 2000; Irpati et al, 2005), elderly (Grover et al, 2005), and adolescents (Tripathi and Lal 1999). While revising existing classification, available research evidence should be considered carefully, and proposed changes should be evaluated for their utility in treatment decisions and in prognostication, for forensic purposes, for potential benefits to special groups like children. Also, issues related to third parties like reimbursement providers, public opinion and implication for government policies should be carefully considered during the revision process.
References:
Address for Correspondence:Dr. B. M. Tripathi, Professor, Department of Psychiatry and National Drug Dependence Treatment Centre, All India Institute of Medical Sciences, New Delhi-110029, India. Fax: +91 11 26588663. E-mail: bmt_54[at]yahoo[dot]com
Rakesh Lal, MD, Mamta Sood, MD, DPM, Amardeep Kumar, MD
Recommendations
Schizophrenia (F 20)
Thus, we propose the draft for this section should read as follows:
F 20.x.a.b.c.d
Type of schizophrenia – x
Course – a
Age at onset – b
Catatonic symptoms – c
Depressive symptoms - d
Delusional disorders (F22)
Acute and transient psychotic disorders (F23)
x – subtype
a – course which may be: 0 - single episode, 1- recurrent, current episode
Schizoaffective disorders (F25)
x – subtype
a – course which may be: 0 - concurrent, 1- sequential
Supportive Evidence for Proposed Changes
Introduction
Schizophrenia, schizotypal and delusional disorders (F20-F29) section in ICD10 include non-affective psychiatric disorders conceptualized to be broadly related to each other. The classification of these disorders in ICD-10 has achieved fairly good reliability, ensuring the international comparability of research, clinical work and education. While, these categories have not achieved expected nosological validity based on criteria given by Robin and Guze (1970), the past decade has witnessed research into specific areas that has elucidated and questioned many already existing issues and has thrown up several new issues for consideration.
F20: Schizophrenia
I. Higher weight should be given to negative symptoms of schizophrenia
There is an emphasis on positive symptoms for diagnosing schizophrenia in ICD10. Presence of only one SFRS is enough to make the diagnosis whereas two of the negative, catatonic, formal thought disorder or persistent hallucinations with accompanying delusions/overvalued ideas are required to make the diagnosis of schizophrenia. Inclusion of Schneider’s first rank symptoms (SFRS)/positive symptoms in the diagnostic guidelines has increased reliability of diagnosis of schizophrenia in ICD10. However, it is now well established that SFRS are present in other psychiatric conditions as well (Taylor et al, 1973; Brockington et al, 1980). Also, current research recognizes that negative symptoms are defining features of schizophrenia.
Negative symptoms have been reported frequently in patients with schizophrenia.
Patients of schizophrenia with affected relatives are reportedto have a high magnitude of negative symptoms that are relativelytreatment resistant. Twin studies and other data show that relativesof probands with greater negative symptoms have higher morbid risks for illness than the relatives of probands who have greaterpositive symptoms. Negative symptoms are also presentin some nonschizophrenic relatives of patients with schizophrenia,as in those with schizotypal personality disorders (Malaspina et al, 2000).
Typical antipsychotics cause relatively more improvement in positive symptoms as compared to negative symptoms. Moreover, typical antipsychotics cause extra pyramidal side effects which may mimic some of the negative symptoms. Atypical antipsychotics have been proven in placebo-controlled trials to be effective in treating negative symptoms of acute schizophrenic episodes (Moller et al, 2003). Negative symptoms are widely suspected to reflect frontal lobe dysfunction and are associated with poor outcome (Potkin et al, 2002).
Discussion: The literature suggests that negative symptoms are increasingly recognized as defining features of schizophrenia but it is not clear how they can be used in differentiating schizophrenia from other conditions. Some studies report that negative feature like apathy may be useful in this regard. Studies are needed to identify pattern and type of primary negative symptoms in schizophrenia. Increasing the weight age of negative symptoms in making diagnosis of schizophrenia can be achieved by adding another criteria that records negative symptoms not currently included under (h) like avolition, loss of drive, aimless behaviour, empty speech.
II. Addition of early onset (onset before 18 years of age) as age of onset specifier
Awareness about early onset schizophrenia is increasing. Premorbid developmental impairments, including language, motor and social deficits; insidious onset in at least 75% of children; elementary auditory hallucinations; less complex delusions related to childhood themes; and negative symptoms namely flat or inappropriate affect; are more frequent and pronounced in earlier, than in later-onset schizophrenia.. A marked deterioration from the previous level of functioning is also present in these children, and an impaired outcome is reported in approximately 50-60% of cases.
The frequency of childhood schizophrenia is less than 1 in 10,000 children, but there is a remarkable increase in frequency between 13 and 18 years of age (Remschmidt et al, 2005).
There is strong evidence for the importance of genetic factors in schizophrenia in children and adolescents (Remschmidt et al, 2005).
Early onset schizophrenia has greater neuropsychological deficits than adult onset schizophrenia (Biswas et al, 2006; White et al, 2006). Early onset schizophrenia is also more severe and is frequently treatment-resistant (Shaw et al, 2006). The long-term course of childhood- and adolescent-onset schizophrenia is worse than in adult-onset schizophrenia, and the patients with manifestation of the disorder below the age of 14 have a very poor prognosis (Remschmidt et al, 2005).
Discussion: Early onset schizophrenia (onset before 18 years) has good internal and external validity. Thus, the group proposed its (age of onset) inclusion as a specifier ‘b’.
III. Pattern of course needs to be simplified
The review of literature did not support the complex pattern included under the current course specifier in ICD-10. It is tedious for use in clinical practice as well as research, hence it is rarely used. Provision of a simpler pattern of course specifier would increase its clinical utility without compromising on its validity. The group proposed the following pattern for course specifier:
IV. Removal of catatonic schizophrenia F20.2 as a subgroup of schizophrenia and placing it as clinical course specifier of schizophrenia
Kraepelin recognized catatonia as a form of dementia praecox and Bleuler included it within his wide group of schizophrenias. Catatonia as a subtype of schizophrenia has been included in all classificatory systems. Recent research shows that catatonia is a syndrome which is characterized by association with neurological and general medical conditions, mood disorders; use of effective therapeutics and development of reliable instruments.
Catatonic presentations are common in acute in-patient psychiatric settings (Banerjee et al, 1995; Chalasani et al, 2005). The prevalence of catatonia among psychiatricpatients is reported to range from 7.6% to 38 % (Taylor et al, 2003).
Catatonic presentation is more common in mood disorder than in schizophrenia. It is also found in many other conditions (Taylor et al, 2003).
Catatonia responds to specific treatments like lorazepam and ECT irrespective of the disorder (Taylor et al 2003).
Discussion: Customary clinical practice continues to overvalue the idea that presence of catatonia is diagnostic of schizophrenia. The reliability of catatonic features is good; however the internal and external validity of catatonic schizophrenia is questionable. This type of presentation appears in the course of schizophrenia at various stages with limited stability. Further, it is recommended that at the time of presentation, if catatonic features are present, these are treated symptomatically with lorazepam or ECT; final management, course and prognosis are decided by the underlying condition that is uncovered after patient recovers from catatonia. So, catatonia can be conceptualized mainly as a clinical specifier. Thus, the group proposes its placement as a clinical course specifier ‘c’.
V. Removal of post-schizophrenic depression as a subtype; depressive symptoms to be included as a phase specifier.
Depression occurs frequently in schizophrenia. Occurrence of depression in schizophrenia has often been associated with worse outcome , impaired functioning, personal suffering , higher rates of relapse or rehospitalization and suicide. In ICD 10, depressive features are included under schizophrenia as ‘mild degree of depression’ preceding psychotic symptoms and as ‘post psychotic depression subtype’. In the former situation, it is a symptom and in the latter situation, a syndrome. A depressive episode present concurrently with schizophrenia is diagnosed as a schizoaffective disorder. The confusion attending the term depression in schizophrenia is attributable to three questions viz., whether it is the symptom or syndrome of depression that is being considered; the phase of schizophrenia in which it is occurring; and its causation (whether it is integral part of schizophrenic process, a de-novo phenomenon or a reaction to stress).
Depressive symptoms in schizophrenia are often severe but are poorly recognized by psychiatrists (Bressan et al, 2003). The prevalence varies from 7%-75% according to the approach used for their identification (Micallef et al, 2006). Depressive symptoms of substantial severity are often found in 50% of newly diagnosed cases of schizophrenia and 33% of cases of chronic schizophrenia that have relapsed (Whitehead et al, 2002).
A Cochrane systematic data review found no convincing evidence to support or refute the use of antidepressants in treating depression in people with schizophrenia (Whitehead et al, 2002). However, a study done by Birchwood et al (2000) found that depression accompanying acute psychotic phase remits with psychosis.
Discussion: Post-schizophrenic depression as a subtype of schizophrenia has questionable reliability and validity. Depression in schizophrenia is common and it occurs during prodrome, active psychotic phase, within first year and thereafter. The efficacy of antidepressants is equivocal. The boundary problem exists with schizoaffective disorder (depressive type) and depressive episode (F32.-). Thus, the group proposes removal of post-schizophrenic depression as a subtype; depressive symptoms should be included as a course specifier‘d’. Depressive symptoms fulfilling diagnostic criteria for depressive episode (F32.-) occurring could be diagnosed independently as a co morbid condition.
VI. Dimensions of schizophrenia to be introduced
Over the last decade many studies have highlighted the dimensions of schizophrenia. In eighties, the negative–positive distinction was extensively studied. Van der Does et al (1995) investigated the stability of an earlier reported four-dimensional symptom model (positive symptoms, negative symptoms, disorganization, and depression) and found a stable four-dimensional structure that closely resembled the factor structure of their first assessment. The symptom dimensions were uncorrelated, except for disorganization and depression. The results of a cluster analysis suggest the existence of at least four subtypes of schizophrenia: positive, negative, mixed, and disorganized. A fifth subtype included patients with few symptoms and suggested the occurrence of simple schizophrenia (Dollfus et al, 1996; Lykouras et al, 2001). Klingberg et al (2006) reported the occurrence of five factors viz., negative, impulsive, positive, disorganization, and depression.
Discussion: While the search of literature suggests the occurrence of many dimensions underlying schizophrenia, the evidence for reliability and validity of different dimensions is variable. Issues pertaining to dimensional classification will be covered under the general section.
VII. Introduction of schizo-obsessive subtype of schizophrenia under ‘Conditions meriting further study’
Co-occurrence of obsessive compulsive (OC) symptoms and psychotic illness was first recognized over a century ago. Interest in this area has been revived recently because of increased recognition of higher-than-expected co morbidity rates. There is growing evidence that patients with schizophrenia and obsessive compulsive disorder, termed schizo-obsessive may represent a special category of schizophrenia population.
Recent studies have revealed much higher co-morbidity rates for OCD in the schizophrenia than previously recognized. Investigators have reported prevalence rates of clinically significant OC symptoms in schizophrenia population to be 10%-52% and of OCD in schizophrenia population to be 7.8%-26% (Berman et al, 1995; Kruger et al, 2000; Tibbo et al, 2000; Craig et al, 2002; Thomas et al 2005). Comparisons of current co-morbidity figures with individual lifetime prevalence rates for each disorder (2%-3% for OCD and 1% for schizophrenia) suggests that there exists greater than chance rate of co-occurrence between the two conditions (Bottas et al, 2005).
Schizophrenia with OC symptoms possess a distinct clinical and neuropsychological profile that differs from that of schizophrenia without OC symptoms. This profile includes a worse clinical course with poor treatment response, lower functioning levels, and greater impairment of functions primarily subserved by the frontal lobes. In addition, the former patients showed a higher level of negative symptoms and worse overall psychopathology (Hwang, 2000).
There is significant overlap in the proposed circuits of OCD and schizophrenia, which may lead to co-expression of symptoms. Although there is overlap in neurotransmitter dysfunction, the interactions are complex, especially in regard to the serotonin and dopamine systems (Tibbo et al 1999, Gross-Isseroff et al 2003).
Discussion: at present the epidemiological and biological evidence suggests that schizo-obsessive disorder as a subtype of schizophrenia deserves attention as it may be sufficiently distinct in terms of aetiology, treatment and outcome. The group proposes that schizo-obsessive subtype of schizophrenia should be introduced as a conditions meriting further study.
F22: Persistent delusional disorder
VIII. Deletion of the term ‘persistent’
ICD-10 mentions the word ‘persistent’ to mean that these disorders are ‘usually persistent and sometimes lifelong’. The global outcome of delusional disorders is shown to be better than that for schizophrenia. Kendler and Walsh (1995) reported the duration of illness for delusional disorders (38±26 months) to be shorter than that for schizophrenia (159±134 months). It is argued that to bring this category closer to that of DSM-IV the term ‘persistent’ should be dropped.
IX. Shifting of F24 (induced delusional disorder) under F22
The underlying assumption behind placing F24 as a separate diagnostic category in ICD-10 appears to be presence of a definite cause and spontaneous resolution of symptoms after removal of the cause. Literature review suggests that this category has not been adequately validated. The occurrence of its four subtypes viz., folie imposee, folie simultanee, folie communiqué and folie induite is largely based on the resistance offered and time of appearance of psychotic symptoms in the secondary cases. Except for folie imposee, these disorders in secondary cases do not have a clear onset and offset with the primary case (Wehmeier et al, 2003). Management of these patients requires multiple treatments including removal of etiologic agent, antipsychotics, individual and group psychotherapy, and family therapy (Kumar et al, 2005). As these conditions are phenomenologically similar to cases with delusional disorders, the group proposes that this category can be shifted under F22 as F22.1 for better understanding of etiology and long term course and outcome.
F23: Acute and transient psychotic disorders
X. Introduction of course specifier for acute and transient psychotic disorders
Acute and transient psychotic disorders get re-diagnosed as other non-organic psychotic disorder if they recur. Studies have suggested that these cases recur and recurrent acute remitting psychotic states are 10 times more common in developing than in industrialized countries; are two times more common in females than males; exhibit long term benign course and have lesser negative symptoms (Susser et al,1995; Sajith et al, 2002). Better delineation of non-affective acute remitting psychosis in current diagnostic systems could lead to better understanding of this condition and improve the applicability of diagnostic systems in developing countries, where these conditions are more common than in industrialized countries. To better understand the course and outcome of acute and transient psychotic disorders, the group proposed the introduction of a course specifier for this group of disorders. A fifth character may be used to classify the course e.g. F23.x.a
x – subtype
a – course which may be 0 - single episode, and 1 - recurrent, current episode
F25: Schizoaffective disorders
XI. Introduction of concurrent and sequential subtypes as course specifier
In ICD-10, the schizoaffective disorder is defined as the concurrent occurrence of schizophrenic symptoms with a major affective disorder. Longitudinal aspects of course are npt reflected well in the current classification. There is little evidence to support a chronological distinction regarding the co-existence of schizophrenic and affective symptomatology. Thus two types of schizoaffective disorder must be distinguished: the 'concurrent' and the 'sequential' type (Marneros 2003). The first includes conditions with coincident schizophrenic and affective symptoms and the latter is defined as the schizoaffective disorder under a longitudinal aspect subsuming disorders with a symptom change between different episodes. The group felt that this change will improve the reliability and validity of schizoaffective disorders. A fifth character may be used to classify course e.g. F25.x.a
x – subtype
a – course which may be 0 – concurrent, and 1 - sequential
Conclusions
In the coming decades, efforts to explore simpler clues like endo-phenotypes to genetic underpinnings of disorders covered under this section will continue. It is being conceptualized that both genes and brain circuits they regulate may underlie symptom complexes across many diagnostic categories. The dimensional approach to psychiatric diagnosis will probably help in better segregating these symptom complexes. Also, there is issue of sub-threshold symptoms seen in primary care. Besides reliability and validity, issues of clinical utility are important. The changes proposed in the present classification of these disorders need to synthesize these issues.
References
Address for Correspondence:Dr Mamta Sood, Assisant Professor, Department of Psychiatry, All India Institute of Medical Sciences (AIIMS), New Delhi. Email: soodmamta[at]gmail[dot]com
Atul Ambekar, MD, Raman Deep MD, Rajat Ray, MD
Recommendations
Introduction
We began by conducting a comprehensive search (comprising both electronic and manual search) of the studies on mood disorders published in the Indian psychiatric/mental health journals. Attempt was also made to include the psychiatric research published in Indian medical/social journals (i.e. journals not dedicated to psychiatry/mental health alone). This review of the available Indian literature was conducted focusing on studies published between years 1992 (i.e. when ICD-10 was published) till date. We could locate 190 articles on mood disorders of which 161 had been published in Indian journals and 29 in International journals.
All the research articles were color-coded and divided into five broad categories for diagnostic validity as per Robins and Guze criteria (i.e. clinical description, family studies, laboratory studies, follow-up studies, and delimitation from other disorders: Table 1).
TABLE 1: Number of publications according to categories for diagnostic validity
| ICD-10 sub category | Clinical Description* | Family Studies* | Lab studies* | Follow-up studies* | Delimitation from other disorders* | Total |
|---|---|---|---|---|---|---|
| Manic episode | 23 | 4 | 4 | 10 | 1 | 42 |
| Bipolar affective disorder | 25 | 9 | 14 | 21 | 6 | 75 |
| Depressive episode | 56 | 2 | 25 | 21 | 5 | 109 |
| Recurrent depressive disorder | 2 | 1 | 2 | 5 | 0 | 10 |
Persistent mood disorder -Cyclothymia -Dysthymia |
0 1 |
0 0 |
0 1 |
0 1 |
0 0 |
0 3 |
| Total# | 107 | 16 | 46 | 58 | 12 | 239 |
Publications include: Original research articles/reviews/case reports/letter to editors/posters
*As per Robin and Guze Criteria (loosely applied) - ‘’Best fit’’
#Total is more than 100 % (i.e. 190 articles) as some articles could be classified in more than 1 category
The evidence was weighed for and against the diagnostic validity of a particular entity in mood disorders category and discussed among the members of team. We conducted a more diligent search in Indian and international literature for the following areas: (1) data inadequately represented in the Indian literature; (2) entities that were controversial in terms of their nosological status; (3) new categories/criteria/specifiers which could be potential candidate for inclusion: and (4) of interest as reflected in recent literature. References to publications from other countries have been made in the following situations: (1) as a primary reference where Indian studies were non-existent; (2) as supplement to the available Indian studies; and (3) to provide for an international perspective on controversial/debatable areas.
Chronic mania: Clinical description of chronic mania dates back to the 19th century when Kraepelin routinely described such cases in his presentations. More recently, chronic mania has been defined as presence of symptoms in excess of 2 years (Perugi et al, 1998). Prolonged continuation of manic episode has been reported from India as well, mainly in the form of case-reports. A manic episode lasting approximately five decades has been reported (Mendhekar et al, 2004). In the international literature, the prevalence of chronic mania is estimated to be around 6-13%, due to the variable criteria sets chosen to describe the condition(Perugi et al,1998; Malhi et al, 2001). Chronic mania differs partially in its psychopathological presentation from acute mania. While, disturbances in the biological functions such as sleep and appetite are hallmark of an acute episode, chronic mania is devoid of the psychomotor and vegetative symptoms seen in the acute episode. Though, schizophrenia is a potential differential diagnosis in such cases, the absence of the flattening of affect and gross thought abnormality differentiates chronic mania from schizophrenia. At times, it becomes very difficult to diagnose a case of mania because of “personality style of the patient superimposed on a cyclothymic or hyperthymic temperament” (Mendhekar et al, 2004). Though not many follow-up studies are available, experts suggest that chronic mania is a poor responder to the conventional treatment for the mood disorders namely the mood stabilizers and neuroleptics.
Chronic depression: Studies examining depressive disorders have reported a relatively high frequency of cases with a chronic course. This is especially true for elderly patients, females, and those with comorbid illnesses (medical/psychiatric/substance use) (McIntyre and O'Donovan, 2004).
Mania in partial remission: Generally a manic episode is short lasting and its mean duration is reported to be three months. However, a few case reports from India suggest that some episode do not remit completely. For instance, Chawla and colleagues (2006) reported the case with five episodes over past 22 years with persistent mood congruent delusion in the inter-episodic period. Characterization of the ‘inter-episodic’ period in such cases by the specifier “in partial remission” would benefit communication between professionals as well as management of the case.
Depression in partial remission: Incomplete remission from depression is quite common, with approximately one third of patients continuing to have residual depression (Burt, 2004). The presence of residual symptomatology after an episode of depression is associated with an increased risk of short-term relapse and a chronic course; a higher risk of suicide attempts; poor social functioning; higher comorbidity and poor outcome of comorbid illnesses; and increased social and economic costs (Kennedy and Paykel, 2004).
The Satra Bruk classification workshop held in Sweden in 1999 proposed the introduction of a specifier for post partum onset (defined as onset within three months of delivery) (Elliott, 2000).
Depression with post-partum onset: An average general populationprevalence figure of 13% has been reported for postpartum depression (O’Hara and Swain,1996).In the Indian context, Patel et al (2002) reported prevalence of postpartum depression in 23% of mothers at 6-8 weeks of childbirth; 78% of these patientshad had clinically substantial psychological morbidity duringthe antenatal period. More than one-half of the patients remainedill at 6 months after delivery. Incidence has been found to be 16% and 10% in early and late post-partum period, respectively, in another study (Sood and Sood, 2003). Economic deprivation and poor marital relationships were important risk factors for occurrence and chronicity of depression. The gender of child was also found to be a determinant of postnatal depression, a reflection of the cultural preference for a male child over a female one (Patel et al, 2002). In developedcountries, the risk factors for postnatal depression are pasthistory of psychological disorder, psychological disorder duringpregnancy, low socioeconomic status, complicated delivery, andpoor marital relationship. Additionally, post-partum depression has been found to have a substantial risk of recurrence in subsequent post-partum periods (30%-50%). Women in developing countries whosepopulations have low incomes face considerable inequalities,ranging from fewer opportunities in education and employmentto less control over personal decisions, such as the use ofcontraception to plan pregnancies. Thus women in developing countries have all the risk-factors for post-natal depression in abundance, making the specification of ‘onset during postpartum period’ even more important in such contexts.
Post-partum mania: Despite diverse presentations, there is strong evidence fromclinical, outcome, and genetic studies for a close relationship between puerperal psychosis and bipolar disorder (Dorothy et al, 2006). Women who have suffered an episode of puerperal psychosis remainat high risk of developing further affective episodes (Davidson and Robertson,1985),and puerperal episodes of illness follow 20% to 30% of birthsto women with a history of bipolar disorder or affective psychosis(Kendell,1987). Family studies of puerperal psychosis consistently demonstratefamilial aggregation of psychiatric (predominantly affective)disorder, with morbidity risks for first-degree relatives inthe range of 10% to 50% (Platz and Kendell, 1988; Dean, 1989). The findingof higher rates of affective disorder in relatives of puerperalprobands suggests a major overlap in the familial factors predisposingto puerperal psychosis and bipolar disorder.
A number of attempts have been made by various researchers to define a "biological symptomatic profile" of depression by means of genetic, biological and therapeutic studies (Staner, 1988; Rush and Weissenburger, 1994; Schotte, 1997; Parker, 2000; Hill and Gorzalka, 2005). Psychomotor and appetite disturbances, early awakening, anhedonia and psychotic symptoms seem more likely to reflect this biological dysfunction in depression (Staner, 1988). Studies have supported the construct validity of the DSM-III melancholic subtype of major depression. Schotte (1997) has proposed the integrated threshold model:
Melancholic symptom features are predictive of a positive response to ECT and to tricyclic antidepressants in the severely ill. Key features include psychomotor retardation, unreactive mood, pervasive anhedonia, and distinct quality of mood. Melancholic features are associated with shorter REM latency and/or nonsuppression of cortisol during the dexamethasone suppression test. Depressive episodes that are not melancholic may take on melancholic features with repetition and passage of time in some individuals. Once melancholic features are present, it is unclear whether they repeat across subsequent episodes. Melancholic features are not uniquely associated with a positive family history of depression per se, but they may be especially associated with a family history of severe depression (Rush and Weissenburger, 1994). Bipolar depression appears to be more likely to be 'melancholic' in type, thus providing an indirect strategy for the clinical definition of melancholia (Parker, 2000)
A recent study has pointed towards some similarities between melancholic depression and an endocannabinoid deficiency state. Interestingly, endocannabinoid activity is down-regulated by chronic stress and possibly increased by some antidepressant regimens. It has been proposed that an endocannabinoid deficiency may underlie some of the symptoms of melancholic depression, and that enhancement of this system may ultimately be a novel form of pharmacotherapy for treatment-resistant depression (Hill and Gorzalka, 2005).
While, the validity of the specification of melancholic symptoms in a depressive episode has been largely established (Rush and Weissenburger, 1994), we are raising a semantic issue here. In the current system (ICD-10) the symptoms historically regarded as ‘melancholic’ are called ‘somatic’. We propose that the term ‘melancholic' should be preferred as it is specific to depression, while the term ‘somatic’ leads to confusion with ‘somatoform symptoms / disorders.’
Approximately 8-14% of patients with psychiatric illness have catatonia as a presenting feature (Pommepuy and Januel, 2002).
Depression with catatonia: Depressed patients with catatonia have been found to be older, to have a significantly higher frequency of major depression, to have more severe cognitive impairments and more severe deficits in activities of daily living than depressed non-catatonic patients (Starksteinet al, 1996).
Mania with catatonia: Manic patients with catatonia are reported to have more mixed episodes, more severe manic symptoms, more general psychopathology, higher co-morbidity, longer hospitalization, and lower Global Assessment of Functioning (GAF) scores than the noncatatonic patients. Thus, the presence of catatonic symptoms in mania is regarded as a marker of a worse course and outcome (Braunig et al, 1998).
An increasing amount of research has challenged the traditional view that juvenile-onset bipolar disorder is a rare condition. The cumulative incidence of bipolar disorder in childhood and adolescence may equal the 1% rate in adults (Lewinsohn et al, 1995). Available Western studies suggest that childhood/ adolescent onset bipolar disorder have a greater prevalence of chronicity, psychosis, mixed and atypical features, high incidence of rapid cycling, and poor response to mood stabilizers (Geller et al, 2004; Wozniak, 2005). However, studies from India report a high rate of recovery and low chronicity (Rajeev et al, 2003; Jairam, 2004).
We support the continued inclusion of mood disorders within ‘general psychiatric’ disorder categories rather than among F90-F98 (…disorders with onset usually occurring in childhood and adolescence). However, we recommend that onset in childhood and adolescence be specified to ensure required clinical and research attention towards these conditions.
Traditionally, bipolar disorder has been considered as an episodic disorder with good inter-episode recovery. More recent studies have shown that in some cases complete recovery may not be achieved and subsyndromal symptoms persist in the inter-episodic period. The notion of complete interepisodic recovery is challenged further by studies documenting that certain patients demonstrate social, marital, occupational and cognitive dysfunction, even when euthymic (Watson and Young, 2001).
In line with our earlier recommendation for a specifier for complete/ incomplete remission of single ‘episode,’ we suggest that a provision should be made to specify whether the lifetime course of a recurrent disorder is characterised by complete/incomplete interepisodic recovery.
There are a few studies on seasonal pattern of mood disorders from India. The available evidence suggests that:
A significant proportion (22%) of bipolar affective disorder patients has been found to have seasonal pattern (Avasthi et al, 1996). Further, patients with seasonal pattern have been reported to have episodes mostly in summer and winter, longer episode duration and more psychotic features as compared to patients with no seasonal pattern. There also appears to be a genetic propensity present to mood variations in relation to environmental temperature (Fernandes et al, 1996).
The studies on seasonal pattern of mood disorders from India have been mainly limited to one group of authors. If, indeed, the concept of seasonal pattern (more so, the reverse seasonal pattern) of mood disorders is to be validated, there is a need to replicate these findings in other centres of India. A provision in the classificatory system for separately coding the specifier of seasonal pattern will stimulate further research in this area.
Rapid cycling among patients with bipolar affective disorders is important because of its implications for long-term prognosis and for the use of antidepressants. Indian literature about rapid cycling is mainly restricted to case-reports (Garg et al, 1998). International literature (Bauer et al, 1994) suggests that about 15-20% of bipolar disorders have a course which could be characterised as ‘rapid cycling’ (defined as four or more mood episodes in a year). Rapid cycling is associated with female gender, substantial depressive morbidity, high risk for serious suicide attempts, poor response to lithium and fair response to calcium channel blockers (Frye and Altshuler, 1997; Coryell et al, 2003). Some studies suggest that rapid cycling (spontaneous or induced) once established, becomes for many years a stable rhythm in a substantial proportion of patients (Koukopoulos A, et al, 2003). However, other studies examining data related to phenomenology, family history, and long-term outcome do not support rapid cycling as a separate entity but as a temporary complicated clinical state (Kilzieh and Akiskal, 1999)
We propose that patients with a course characterized by four or more episodes in a year for at least two consecutive years should be specified as having ‘rapid cycling.’ The duration criterion (two years) is in line with that currently employed for other chronic disorders such as dysthymia and cyclothymia as suggested by certain authors (Koukopoulos et al, 2003).
As discussed in the recommendation number 1.4, the term ‘somatic syndrome’ does not include somatic (i.e. physical) symptoms of depression. The symptoms described are more commonly referred to as melancholic symptoms in the existing literature. In order to avoid confusion with somatic symptoms and in line with the available research, we recommend the change of terminology from ‘somatic’ to ‘melancholic’.
The ICD prefers the use of the term mood over affective as mood represents a more enduring emotional state in contrast to affect which represents a feeling tone in response to present events. The F30-39 category has been named mood disorders in ICD-10. Following the same rationale, the term bipolar affective disorder can be replaced by bipolar mood disorder.
Somatic (i.e. physical or somatoform) symptoms of depression are common in manycountries, but their frequency varies depending on how somatizationis defined. In part, this variation may also reflect characteristics of physiciansand health care systems, as well as cultural differences amongpatients.
In some Western as well as Indian studies, a majority of patients with depression present with somatic (i.e. physical or somatoform) symptoms but acknowledgepsychological symptoms (such as depressed mood or guilt) when they were specifically asked about them (Goldberg & Bridges, 1988; Raguram et al, 2001). Even more importantly, the largest study to examine the relation between somatic symptoms and depression (which utilized data from World Health Organization's studyof psychological problems in general health care - 25, 916 patients from 15 primarycare centres in 14 countries in 5 continents) found that somatic symptoms are often the only or predominant presenting complaints in some patients with depressive illnesses (Simon et al, 1999). In this study, of the 5447patients who underwent a structured assessment for depressive and somatoform disorders, 1146 met the criteria for major depression. Among them, 69% reported only somatic symptoms (Simon et al, 1999).
The personal significance and meaning of the symptoms are shaped by cultural notions concerning the human body in health and in sickness. Although both depressive and somatic symptoms were distressing to Indian patients, qualitative analysis showed that depressive symptoms, unlike somatic symptoms, were construed as socially disadvantageous (Raguram et al, 2001).
Anger attacks have been proposed as a specific form of anger in depression. They are characterized by a rapid onset of intense anger and a crescendo of autonomic arousal occurring in response to trivial provocations. They resemble panic attacks but lack the predominant affects of fear and anxiety associated with panic attacks. They typically occur in situations in which an individual feels emotionally trapped and experiences outbursts of anger that are later described by the patient as being uncharacteristic and inappropriate to the situation at hand. The prevalence of anger attacks in depressed patients is approximately 30% to 40 % (Fava and Rosenbaum, 1999). Though the presence or absence of hostility, anger and aggression in depression has been a matter of controversy, anger attacks have been found to occur more often in depressed patients in comparison to healthy controls. Some studies have reported that depressed patients with anger attacks differ from those without such attacks in terms of clinical profile, comorbid personality disorders and certain biological variables. Serotonergic dysfunction may characterize this distinct subtype of depression - depression with anger attacks (Painuly et al, 2005). Fraquas et al (2006) reported that serum levels of homocysteine were positively correlated with length of current major depressive episode in patients with anger attacks but not in those without anger attacks. The attacks have been found to disappear in 53% to 71% of depressed patients treated with fluoxetine, sertraline, or imipramine (Fava and Rosenbaum, 1999). Significance of aggression as a gender-specific diagnostic criterion for depression has been proposed as ‘male depressive syndrome’ (Winkler, 2005).
In the current edition of ICD, recurrent mania finds mention as an inclusion term under other bipolar affective disorders (31.8). The previous edition, ICD-9, had a separate category called recurrent mania. However, there has been persistent debate about the same. Avasthi et al (1996) reported that recurrent mania was by no means uncommon in India (6.5%). A recent review examining the nosological status and validity of recurrent unipolar mania (Harish et al 2005) also concluded that unipolar or recurrent mania occurs in sizeable number of patients (5%-25%). Unipolar mania exhibit consistent differences from bipolar mania in clinical, course and outcome, laboratory and family studies.
We recommend that, recurrent mania should be coded separately under the broad category of bipolar affective disorders rather than as an inclusion term with ‘other bipolar disorders’.
There are few Indian data on depressive episode(s) with hypomania. Klerman (1989) and Akiskal (1999) labelled recurrent depression with hypomania as Bipolar affective disorder (BPAD)-II in their classifications of bipolar spectrum disorders. Bipolar II disorder is also recognized as adistinct subtype in the DSM-IV (1994) classification. The life-time prevalence rates of both bipolar I and bipolarII disorders have been estimated at 0.6%, giving a combinedfigure of 1.2% (Weissman and Myers, 1978). A number of recent studies have helped in establishing bipolar-II disorder as a separate entity from BPAD-I disorder as well as recurrent depressive disorder. The summary of these studies is presented below:
Clinical description:Goodwin and Jamison (1990) have suggested that sub-syndromal bipolarity appears at a meanage of 14 years, while the initial episode of bipolar I disorder occurs at a median age of 18 years and bipolar II disorderat a median age of 21 years. Majority of available studies conclude that bipolar II disorder has an intermediate age of onset as compared to bipolar I or unipolar disorder.
The gender ratio of bipolar II patients tended to favour women having this disorder as compared to bipolar I patients where the gender ratio was fairly equal (Dunner, 1993). Clinical differences have been found in some studies comparing females and males suffering from BPAD-II. Females, as opposed to males, had significantly lower age at onset, more axis I co-morbidity, atypical depressions, intra–depression hypomanic symptoms (i.e., mixed depression), and family history of suicidal behavior. Females had more sadness, loss of energy, loss of interest, and suicidal ideas (Benazzi, 2005). Differences were found mainly on the depressive pole of the disorder and not of great magnitude but the authors concluded that these findings merit further attention.
When compared with Bipolar-I and unipolar disorders, researchhas found certain distinct differences in rates of recovery, clinical features and number of episodes. Rapid cycling was noted among bipolar I and bipolar II (but not unipolar) patients. Patients with seasonal affective disorder were more likely to be bipolar II than unipolar. Clinically depressed bipolar I patients evidenced psychomotor retardation; whereas, depressed bipolar II and unipolar patients either had psychomotor agitation or psychomotor retardation. One clinical feature that has consistently appeared to differentiate patients with bipolar II disorder from those with bipolar Idisorder or unipolar depression is the risk of suicide, whichappears to be elevated in this group (Bourgeois 1997). A history of suicide attempt was highest among bipolar II as compared to bipolar I and unipolar depressed patients (Dunner 1993). This may be related to the fact that the diagnosisis often missed, and consequently patients are ineffectivelytreated (MacQueen and Young, 2001). Also, high rates of comorbid disorders have been reported among patientswith bipolar II disorder (Savino et al, 1993; Pini et al, 1997), including substance abuseor dependence, anxiety disorders, and personality disorders.
Family studies: distinct familial inheritancefor bipolar II disorder has been suggested (Cassano et al, 1999). A tendencytowards a mild expression of mania may run in families (Kato et al, 2000). A summation of the large-scale studies where relatives of bipolar I, bipolar II, and unipolar patients were interviewed to determine their diagnosis revealed an elevated morbid risk for mania (bipolar I disorder) in relatives of bipolar I patients and bipolar II patients, as compared to relatives of unipolar patients and an elevated morbid risk for bipolar II disorder in relatives of bipolar II probands. These latter data suggested that bipolar II might "breed true." The family study data supported the notion that bipolar II was more similar to bipolar I than unipolar disorder but that bipolar II may be (on a familial basis) somewhat distinct from both bipolar I and unipolar disorder.
Laboratory studies: Preliminary imaging (Altshuler et al, 1995) and biochemical(Kato et al, 2000) studies that have separately examined subjects with bipolarI and bipolar II disorders have found differences in these groupsthat further support the view of bipolar II disorder as a discretediagnostic entity. Periventricular hyperintensities were found to be more common in bipolar I patients (62%) than in bipolar II patients (38%) and normal comparison subjects (30%; Altshuler et al, 1995). The rate of 5178C genotype was significantly higher in patients with bipolar disorder (64.8%, P < 0.05) compared with controls (53.2%) when paternally transmitted cases were excluded. This effect was more prominent in patients with bipolar II disorder (75.6%, P < 0.02 to controls). Bipolar II patients with 5178A genotype without family history had significantly later age at onset (56.0 ±14.7 years, P < 0.05) than other bipolar patients (Kato et al 2000). The major difficulty in assessing the review of the biological studies was the fact that no biological study consistently predicted discrimination of bipolar from unipolar patients, and many of the studies suffered from small sample size and lack of replication.
Some studies have found differences betweenbipolar I and bipolar II disorders on magnetic resonance imaging (MRI)and on the presence of vascular abnormalities, includingRaynaud's phenomenon, migraine and ‘migraine equivalents’(Altshuler et al, 1995).
Delimitation from other disorders: t he conceptof a trichotomy of mood disorders—bipolar I, bipolar II,and unipolar major depression—has been supported by studies that found distinct patterns of symptoms (as discussed above) and distinct familial inheritancefor bipolar II disorder (Cassano et al, 1999). Researchhas found distinct differences in rates of recovery,clinical features, and number of episodes. Preliminary imaging (Altshuler et al, 1995) and biochemical (Kato, 2000) studies that have separately examined subjects with bipolarI and bipolar II disorders have found differences in these groupsthat further support the view of bipolar II disorder as a discretediagnostic entity. The results of some studies support the notion that bipolarII disorder is intermediate between unipolar depression andbipolar I disorder with respect to illness course.
Follow-up studies: b ipolar II disorder appears to be diagnostically stable (Angst, 1986; Coryell, 1996).A variety of studies suggest that the probability of patients with bipolar II disorderdeveloping a manic episode was about 4% to 17% over up to 40 years of follow-up, with many of the studies supporting low rates of diagnostic conversion from bipolar II to bipolar I (Dunner and Tay, 1993; Coryell et al, 1995). Studies suggest that the number of episodes of depression maybe a stronger predictor of psychosocial outcome than mania in Bipolar II disorder (MacQueen et al, 2000). Preliminary studies suggest that the newer anticonvulsants maybe of benefit for this group.
There seems to be overwhelming evidence for existence of a valid diagnostic entity, characterised by depressive episode(s) with hypomania, which has been labelled “Bipolar-II disorder” in research studies as well as in DSM-IV. The ICD-10 at present mentions it as an inclusion term under ‘other bipolar disorders’ (F31.8). Over past one-and-half decades since the current version of ICD came into being, even more research evidence has been generated pointing towards diagnostic validity of this entity. Hence, in our opinion it is now time that this entity be accorded a distinct status of its own.
CONCLUSIONS
For the purpose of proposing modifications to the classification of mood disorders in the ICD-11, we have restricted ourselves to only those recommendations, (a) which have some evidence of validity in the existing literature, and (b) which have potential utility for the clinicians and researchers if incorporated. While the strength of the evidence-base varies from one recommendation to another, in terms of utility, we believe all of them to be quite useful. For many of our recommendations, we have deliberately not gone into details of definition / criteria. We believe that these definitions and criteria could only be refined, once the system provides for coding them. Till this consensus about definitions is achieved, we suggest that drafters for ICD-11 incorporate these recommendations with the most likely acceptable and/or flexible criteria, leaving some room for clinicians and researchers.
References
Address for Correspondence: Dr. Atul Ambekar M.D., Assistant Professor, National Drug Dependence Treatment Centre, All India Institute of Medical Sciences.
R K Chadda, MD, Nand Kumar, MD
Recommendations
Introduction
We were assigned with the task of possible modifications in the classification and categorisation of the Neurotic, Stress related and Somatoform disorders grouped under the codes F 40 to F 49 in the ICD-10 (International Classification of Diseases, 10th revision) for proposed ICD 11. Our recommendations were formulated on the basis of a comprehensive search (both electronic and manual search) of Indian and international literature pertaining to anxiety, somatoform and stress related disorder. The literature search of Indian studies was focused on studies published since 1990 onwards. The collected evidence was presented to an expert-panel comprising of Faculty of Department of Psychiatry, All India Institute of Medical Sciences, New Delhi for thorough discussion. This final draft of the recommendations has been prepared based on the consensus of the expert panel. We have made an attempt to examine the validity of our recommendations in the light of Robins and Guze (1970) criteria viz. clinical description, family studies, follow-up studies, laboratory studies and delimitation from other disorders.
In ICD 10, the essential feature of generalized anxiety disorder(GAD) is anxiety that is generalized and persistent and not restricted to any particular environmental circumstances. In addition the sufferer must have primary symptoms of anxiety on most days for at least several weeks at a time and usually for several months. The ICD 10 does not mention the exact duration of clinical features to diagnose the anxiety disorder.
The current diagnostic threshold for GAD raises questions about diagnostic requirements, such as whether 6-month duration and other psycho-physiological symptoms are needed for optimal identification of individuals who suffer from a clinically significant condition. Flint (2005) highlighted that in the community, period-prevalence of co morbidity of GAD with another psychiatric disorder is 4%, while the prevalence of pure GAD is only 1%. Early recognition of GAD is of paramount importance considering the co morbidity between GAD and other (especially depressive) disorders (Kessler 2001). Temporally primary GAD significantly predicts the subsequent onset of depression and other secondary disorders highlighting the importance of early intervention and treatment of primary GAD to prevent the subsequent onset of secondary anxiety and depression. Unfortunately, little is known about this possibility because, few people with pure GAD seek treatment. Specification of a duration criterion (preferably for 3 months) could help in early identification of the disorder (before the onset of co morbidity) and paving the way for collection of epidemiological data on pure GAD and also to develop outreach strategies that may correct this situation of low help-seeking in such cases.
Recent data from the US National Co morbidity Survey Replication (NCS-R), carried out during 2001-2003 also focused on the duration requirement for diagnosis of GAD using WHO Composite International Diagnostic Interview as assessment tool (Kessler 2005, Ruscio et al 2007). The report suggests that a large number of people suffer from a GAD-like syndrome with less than six months duration. The study also pointed out that cases of GAD with episodes of 1-5 months did not differ greatly from those with episodes of six or more months in onset, persistence, impairment, co-morbidity, parental GAD, or sociodemographic correlates.
The past decade has seen tremendous strides in the knowledge about the cause, epidemiology, and treatment of obsessive compulsive disorder. Research on clinical characteristics of the disorder have focused on several areas, including identification of subtypes, the role of insight, and patterns of co morbidity (Aigner et al 2005, Bellino et al 2005).
Poor insight identifies a group of OCD patients with distinct clinical characteristics. InOCD with poor insight, patients generally fail to recognize that the obsessions or compulsions are excessive or unreasonable. In a study from India, Ravi Kishore et al (2004) evaluated 100 subjects with OCD (DSM-IV), who had received adequate drug treatment. They observed that 25% of the subjects had poor insight. Poor insight was associated with poor response to drug treatment, earlier age-at-onset, longer duration of illness, a greater number of obsessive-compulsive symptoms, more severe illness and higher co morbidity rate, particularly with major depression. In a study conducted in Bangalore (India), it was observed that poor insight was an important clinical predictor of poor response to treatment with SSRI (seen in 40% to 60% of the sample); (Shetti et al 2005). Similarly, Erzegovesi (2001) evaluated clinical variables that might influence the antiobsessional response to proserotonergic drugs in a sample of 159 patients with obsessive-compulsive disorder (OCD). It was observed that non responders (43.4%) had an earlier onset and a higher frequency of "poor insight" subtype and somatic obsessions in comparison to treatment responders.
Several studies have shown significant brain abnormalities in OCD patients (Aigner et al, 2005). A recent MRI study has shown that there are significantly more features suggestive of structural brain abnormalities in OCD patients with poor insight in comparison to OCD patients with good insight (Aigner et al 2005).
Literature on clinical and psychobiological distinctiveness of hoarding behaviour in OCD (Bellino 2005; Lochner at al 2005) also supports the need for a specifier related to insight in OCD. In OCD, hoarding is associated with poor insight, lack of resistance to the compulsion to hoard, poor treatment motivation, poor response to SSRIs in comparison to other OCD symptom dimensions. Further, at the level of biological and psychosocial determinants, pathological hoarding could be associated with schizophrenia, OCD, and tic disorders, possibly through dopaminergic mechanisms (Damecour & Charron 1998).
Co morbidity between OCD and schizophrenia is an area of emerging interest. Evidence shows that obsessions and compulsions are more common in patients with schizophrenia than was previously thought (Matsunaga et al 2000). Matsunaga et al (2000) further observed that OCD patients are less likely to have poor insight (PI), compared to patients with OCD and schizophrenia; however, OCD patients with poor insight showed a similar degree of functional impairment to that observed in patients with OCD and schizophrenia, pointing towards different outcomes in the two subgroups of OCD. The authors compared 78 OCD patients (primary interest [PI] group: 36% of the sample based on insight question of the Yale-Brown Obsessive-Compulsive Scale) with 20 schizophrenics with OCD (OCD+S). After a 6-month combination of clomipramine and cognitive-behavioral treatment, 14 of 25 OCD PI patients no longer fell in the PI category, which was associated with reduced OCD severity and depressive status. Schizotypal personality disorder (SPD) was more common in patients whose insight remained poor even after the treatment. Co morbid SPD in PI patients may be associated with worse prognosis.
The current classification systems ICD–10 (World Health Organization, 1992) does not give clear operational guidelines for the diagnosis of Dhat syndrome, possibly because it is considered a culture-bound syndrome. Once we label a clinical entity as culture bound, it runs the risk of exclusion from mainstream psychiatric classification with resultant lack of research and understanding (Chadda & Ahuja 1990; Bhatia & Malik 1991; Sumathipala et al 2004).
Dhat syndrome, originally described in India based on cultural beliefs of people, has been found to be highly prevalent in countries neighboring India such as Pakistan, Nepal, Myanmar, Sri Lanka and others (Sumathipala 2004). The patients of Dhat syndrome present with multiple somatic and psychological symptoms in the background of perceived loss of semen. This causal belief is not culture bound - male preoccupation with semen loss is universal and has been frequently associated with depression and anxiety. Similarly, in patients presenting with ‘Dhat syndrome,’ it is not uncommon on clinical exploration to find underlying neurotic and depressive disorders. Several authors have commented that Dhat syndrome should be considered as a culturally determined symptom of (or syndrome within) common disorders like depression, anxiety and somatisation rather than as a culture bound syndrome (Wig 1994). Various experts have questioned the validity of Dhat syndrome being viewed as a single neurotic disorder in ICD–10, where it is included under ‘other specific neurotic disorders’ (F48.8). Indeed, it is difficult to classify a high proportion of these cases as ‘pure’ Dhat (Chadda & Ahuja 1990; Chadda 1995; Bhatia & Malik 1991). Several Indian studies have recommended that Dhat syndrome should be integrated into existing rubrics of psychiatric classification in appropriate places (Chadda & Ahuja 1990; Bhatia & Malik 1991; Wig 1994). This might help to formulate the management of Dhat syndrome comprehensively on a biopsychosocial model depending upon its clinical presentation.
Fatigue is a common symptom in Dhat syndrome. Disorders with fatigue as the main symptom are often grouped together as functional somatic syndromes (Bhatia & Malik 1991; Barsky & Borus 1999). The basic cognitive formulation offered to explain these disorders is based on somatosensory amplification, misattribution and abnormal illness behaviour. These mechanisms seem to operate in patients with Dhat syndrome, who frequently make their first contact with departments other than psychiatry, for example urology, dermatology and general medicine, and are then referred to psychiatry. Also, partly as a result of arbitrary diagnostic guidelines, but also due to their own expectations and characteristics, patients are often dissatisfied with their treatment or causal explanations offered (Chadda & Ahuja 1990). These features suggest that patients without anxiety and depression should be placed within somatoform disorders.
References:
Address for Correspondence: Professor R K Chadda, Department of Psychiatry, All India Institute of Medical Sciences, New Delhi – 110029. Email: drrakeshchadda[at]hotmail[dot]com
Anju Dhawan, MD, Tina Lal, MD
Recommendations
Proposals for the Category F50: Eating Disorders
Proposals for the Category F53: Mental and Behavioral Disorders associated with Perinatal Period
Introduction
Measuring the validity of psychiatric diagnoses is still anunsolved problem. Yet, revisions of the Diagnostic and StatisticalManual of Mental Disorders and of chapter V of the InternationalClassification of Diseases are now under way, with the hopeof improving the validity of the current systems. In this article we present few proposals for changes in the section F50-59 of the ICD 10, on the basis of available Indian data, Western data and clinical experience with due emphasis on criteria laid down by Robins and Guze and Kendell.
Evidence for the Proposed Changes
F50: EATING DISORDERS
Recent years have seen increasing dissatisfaction with the criteria for eating disorders as they currently stand, which combined with good evidence that a large number of patients of all ages presenting for treatment fall into the ‘not otherwise specified’ or ‘atypical’ category, has resulted in lively debate and suggestions for improvement.
Anorexia nervosa (AN) and bulimia nervosa (BN) are currently considered as disorders confined to the Western culture. Although many influences have been noted as formative in the development of eating disorders, slimness has received most attention in recent years. The recent identification of eating disorders in non-Western societies and different subcultures within the Western world has led to suggestions that Western cultural ideals of slimness and beauty have infiltrated these societies (Nasser, 1994; Shroff & Thompson, 2004). The biomedical definition of anorexia nervosa and bulimia nervosa emphasizes fat phobia in the presentation of these disorders. However, evidence exists that suggests anorexia nervosa and bulimia nervosa can exist without the Western fear of fatness and that this culturally biased view may obscure health care professionals’ understanding of a patient’s own cultural reasons for self-starvation, and even hinder their recovery Khandelwal et al, 1995).
Anorexia nervosa was earlier believed to be limited to the white Caucasian population in the West. But, in the last two decades it has been identified with increasing frequency in non western societies (including Hong Kong, Taiwan, China, Malaysia, India, Pakistan and Singapore) as well as ethnic groups in the West.
Current diagnostic criteria for anorexia nervosa are largely influenced by western cultural concept of dread of fat and drive for thinness. The diagnostic criteria for anorexia nervosa as outlined by the ICD 10 include: ‘A body image distortion in the form of specific psychopathology whereby a dread of fatness persists as an intrusive overvalued idea and the patient imposes a low weight threshold on himself or herself’. The contemporary diagnostic criteria therefore de-emphasize ‘emaciation’ and emphasize ‘fat-phobia’. Nasser (1994) attributed the transculturality of anorexia nervosa to a globalization of ‘fat-phobia’ because of the emergence of a culturally shrunken world due to mass communication technology. Thus, Western researchers presume that incidences of anorexia nervosa in non-Western societies are replicas of the West. As a result, fat-phobia still remains the ‘core’ psychopathology underlying anorexia nervosa despite its presence in non-Western societies. Indeed, in the current diagnostic systems cases that do not meet the criterion of fat-phobia are labeled as atypical (eating disorder not otherwise specified (EDNOS) in DSM IV or atypical in ICD 10).
Dread of fatness as the core psychopathology does not explain all cases of anorexia nervosa especially in the non western societies. Several cases of anorexia nervosa without accompanying fat-phobia have been reported in different societies and cultures (China: Lee 1995, Lee 2001; India: Khandelwal and Saxena 1990, Khandelwal et al, 1995). Lee et al (2001) evaluated 48 consecutive patients with broadly defined anorexia nervosa with a self-report rationale for food refusal questionnaire. Two-thirds (32) of the patients expressed fat-phobia but one third (16) did not. Sensation of abdominal bloating and low appetite were among the other rationales given by patients for refusal to eat. Based on a qualitative analysis of 70 Chinese anorexia nervosa patients (who had all been examined by an experienced psychiatrist over a period of 12 years), Lee (1995) reported that 59% of patients did not express any fat-phobia throughout their illness. They differed from their fat-phobic counterparts only in that they were premorbidly slimmer and demonstrated no signs of bulimia, often considered a sign of fat phobia.
Khandelwal & Saxena (1990) and Khandelwal et al (1995) asserted that the presentation of eating disorders in India varied from the typical description of anorexia nervosa. Their female anorexic patients typically showed decreased appetite, excessive weight loss and amenorrhea but no fat-phobia or body image disturbance. Though finally diagnosed and treated as cases of eating disorder, they presented considerable difficulty in diagnosis according to current classification systems. They suggested that this variation was due to sociocultural factors, as Indian culture does not dictate slimness as a beauty ideal, and that there was not as much concern with body image as in the West.
Banks (1992) studied the case of two anorectic women from the Minneapolis–St Paul area of Minnesota. Both women were from conservative religious fundamentalist backgrounds and expressed their desire to reduce food intake through religious understanding about food, the body and sexuality, provided by their religious culture.
The western version of fat phobic anorexia nervosa has neglected the full metaphorical significance of self-starvation and, when applied in a cross-cultural context, may constitute a category fallacy. Most non-Western patients will fall into the atypical group by not fulfilling criteria of dread of fat. Lee (1995) suggested the use of more culturally sensitive diagnostic criteria. One of the diagnostic criterions suggested by Lee (1995) states that, ‘the patients use complaints (such as abdominal bloating or pain, loss of appetite, no hunger, distaste for food, fear of fatness, and/or “don’t know”) to resist attempts to make them increase food intake.’ Due to its seeming ubiquity in Western anorexics and the relative lack of cross-cultural studies on anorexia nervosa it may be too early to shed the concept of fat phobia entirely. Hence, fat phobia should be retained as a specifier of anorexia nervosa, rather than as an essential criterion.
The criterion of amenorrhea was not required for the diagnosis of AN or BN by DSM-III although it was typically associated with anorexia nervosa. Amenorrhea was initially introduced as a criterion for several reasons (Garfinkel et al, 1996; Falk & Halmi, 1982). It was mentioned in historical reports of cases of anorexia nervosa in females. Also, it was hypothesized in more recent decades that anorexia was due to a primary impairment of hypothalamic functioning. Since then, however, it has been observed that amenorrhea generally follows loss of body weight and body fat. While, amenorrhea can occur is a minority of women before substantial weight loss (Theander, 1970), women with all the behavioral and psychopathological symptoms characteristics of anorexia nervosa including weight below the current diagnostic criterion may continue to menstruate. Also, there is no parallel criterion for males (Watson & Andersen, 2003). In a large community epidemiological survey, amenorrhoea did not discriminate between women with anorexia nervosa and women with all the features except amenorrhoea, across a number of relevant variables (Garfinkel et al, 1996).
ICD-10 differs from DSM-IV in being less stringent about the duration of amenorrhea and including some reference to change in male reproductive hormone function. There are some inherent limitations however in both of these diagnostic systems, as they impose a historically appreciated but perhaps overly specific medical criterion of amenorrhea. Current ICD-10 and DSM-IV anorexia nervosa category excludes substantial numbers of individuals who do not fulfill the monotheitic diagnostic criteria, because of the absence of amenorrhea, or because their final weight does not reach the required threshold, despite having clinically significant psychopathologies gravitating around preoccupation with body weight, food, and eating (Mitrany, 1992; Williamson et al 1992; Thaw et al, 2001). A diagnosis of eating disorder not otherwise specified (EDNOS), which is typically regarded as residual, is often misinterpreted as indicating problems of lesser clinical significance (Mitchell, 2005). Levels of distress, behavioral abnormalities, and cognitions similar to those associated with a full syndrome eating disorder often accompany EDNOS (Herzog et al, 1993; Thaw et al, 2001). In an effort to develop homogenous diagnostic groups that can have implications for treatment and course, care must be taken not to exclude people because of small variability in the symptom picture (Dancyger & Garfinkel, 1995).
It is therefore suggested that amenorrhea may be retained as a specifier of anorexia nervosa rather than as an essential criteria. Anorexia Nervosa may be identified on the basis of substantial self induced starvation to the extent of producing significant medical morbidity, which may include amenorrhea.
The weight criterion for anorexia nervosa has also varied over the years. Regardless of the degree of actual weight loss, patients with anorexia nervosa - like symptoms appear to experience a high degree of physiological and psychological distress similar to full anorexia nervosa. For example, a patient may begin dieting at a healthy personal weight of 115% (of ideal) and loses to 90% of this weight, with significant functional medical consequences, but never reach the 85% criterion. In fact partial-syndrome anorexia appears to be more common than anorexia nervosa (King, 1989; Walters & Kendler, 1995). About 1.5% of young women have an eating disorder in full form (Dancyger & Garfinkel, 1995; Ghaderi & Scott, 2001) and another 7%–10% have some, but not all of the features of an eating disorder (Dancyger & Garfinkel, 1995). There is controversy as to whether eating disorders are qualitatively distinct or whether they exist along a continuum of dieting and weight concerns. Herzog et al (1993) followed up a group of 33 women with partial syndrome AN, BN, or both for an average of 41 months. At follow-up, 45% of the subjects had gone on to develop a full-criteria eating disorder, and as many as 82% had met full criteria for an eating disorder at least once during the course of their illness. Similarly, King (1989) observed a spectrum of eating disorder severities with some movement between diagnostic groupings over the 12–18 month follow-up in his study of women in a general practice. These findings suggest that a continuum of pathology may exist in which partial syndromes may reflect an earlier phase in the disorder and thus an artifact of the particular timing of the intake interview or assessment.
The primary weight criterion for a diagnosis of anorexia nervosa is a weight less than 85% of what is considered normal for that person’s age and height (DSM-IV). A body mass index (BMI) less than or equal to 17.5 kg/m2, which originated from the ICD-10 diagnostic criteria for research is not adjusted for age and sex. It should be realized that a body mass index of 17.5 is a strict weight cutoff only for individuals over age 20. For children, and to a lesser extent for adolescents, the body mass index cutoff is less strict than the primary DSM-IV weight criterion.
In keeping with the categorical approach to diagnosis, a cutoff may be specified on the dimension of body size/weight. If ICD persists with BMI, at the minimum, it would require a better specification with regard to age and sex.
F53: Mental and Behavioral Disorders associated with Puerperium Not Elsewhere Classified
Recently delivered mothers are vulnerable to the whole spectrum of general psychiatric disorders, as well as those resulting from the physical and psychological changes of childbirth. Nearly 30% of women have adjustment problems and 15%-20% have minor to major depression. Maternal suicide and infanticide are rare but the more common and yet less recognized risks are those of maternal illness – beginning in utero – on the infant. Considering the high risk of maternal and infant morbidity and mortality (Appleby, 1991; Patel et al, 2003; Anoop et al, 2004; Buist, 2006) associated with post partum disorders it is essential to fabricate a diagnostic system with adequate sensitivity for identification of these disorders.
The rubric of postpartum disorders may be particularly important for developing countries. Indian studies have found high rates of post partum depression (16% to 23%) and have highlighted the importance of social factors, specifically poverty and female gender of the infant as risk factors for the same (Patel et al 2002; Chandran et al 2002).
Current status of postpartum disorder in ICD 10: The ICD-10, permits the classification of mental and behavioural disorders associated with the puerperium (F53) only if they have an onset within six weeks of delivery and if they cannot be classified elsewhere in the ICD 10 either because insufficient information is available or because it is considered that special additional clinical features are present that make classification elsewhere inappropriate. It will usually be possible to classify mental disorders associated with puerperium by using two other codes: the first is elsewhere in chapter V (F) and indicates the specific type of mental disorder (usually affective F30-F39), and the second is O99.3 (mental diseases and diseases of the nervous system complicating the puerperium) of ICD 10. The DSM-IV, with an even shorter onset specifier of four weeks, is restricted to four diagnoses only, and likewise is rarely used. In the light of available evidence that post partum disorders can occur for periods up to 1 year post delivery and that symptoms may have onset during the last trimester of pregnancy the current “6 weeks post partum onset” diagnostic criteria in ICD 10 is too restrictive.
Specific features of postnatal mood disorder are acknowledged in the text of DSM IV (e.g., fluctuating course and mood lability, delusions including the baby, risk of infanticide, disinterest in the infant, guilt because of dissonance between the mother's mood and society's expectation of happiness, and less than optimum development of a mother/infant relationship). These features are not described in the ICD 10.
Recent literature shows a growing focus on the entire perinatal period for mental health of the mother as this period significantly influences the healthy development of the fetus and the newborn. The perinatal mental health period spans conception to two years after childbirth according to some experts (Kowalenko et al 2000; Currid, 2004). It is the time when women are most likely to be admitted to a psychiatric hospital (Dean and Kendell, 1981), are at increased risk of experiencing an affective mental illness, and those with a pre-existing mental illness are more prone to relapse or recurrence of the condition (R C Psych 2000; Pritchard & Harris, 1996). A meta-analysis of 59 studies (including 12,810 women, mainly from developed countries) found an average prevalence rate of non-psychotic postnatal depression (PND) of 13% (95% CI - 12.3%-13.4%) (O' Hara et al, 1996). Most cases develop within the first 3 months, with a peak incidence at 4-6 weeks. Although one study showed that most cases last around 3 months and resolve spontaneously without treatment, another study showed that 50% of cases lasted over 6 months and some persisted at 4 years. Two prospective studies from Goa and Tamil Nadu detected depressive disorder in 23% and 16% respectively, with depression persisting six months after child birth in 11%-14% of women (Chandran et al 2002; Patel et al 2002). Depression and anxiety often begin in pregnancy, particularly in the third trimester, and so ‘perinatal’ rather than postnatal depression might be a better term.
However, the evidence for familial aggregationwas significant for narrowly defined postpartum depression (onsetwithin 4-8 weeks of delivery) but not for a broader definition(onset within 6 months of delivery) that is perhaps more typicalof the way the diagnosis is used as a lay term and applied inclinical practice (Forty et al, 2006). Based on such evidence, the Satra Bruk classification workshop held in Sweden in 1999, proposed to add a postnatal onset specifier of 3 months (Elliot, 2000).
Balancing available scientific evidence with common clinical usage a proposal for ICD 11 is to replace the duration of onset in the puerperium by onset from conception to 3 months post delivery i.e., the perinatal period.
Recently delivered mothers are vulnerable to the entire spectrum of general psychiatric disorders, as well as those resulting from the physical and psychological changes of childbirth. The postpartum “blues” can be part of the normative postpartum adjustment and affect up to 80% of women (Robin, 1962; Pitt, 1968). The mild symptoms of the blues differ qualitatively and quantitatively from postpartum major depression and do not interfere with maternal role functioning (Miller, 1999).
The prevalence of major or minor depression in pregnant women ranges from 7% to 26% (Chandran et al 2002; Patel et al 2002; Moses-Kolko & Roth, 2004). Depression during pregnancy is a strong predictor of postpartum depression and is associated with adverse effects on fetal development (Graff et al, 1991; Chandran et al 2002; Patel et al 2002). The reported rate of recurrence of postnatal depression (PND) after a subsequent childbirth is 30% and the rate is higher for women in whom the first episode of PND is the first-ever depressive episode, compared with the rate in women who have had previous non-puerperal depression (41% vs. 18%) (Cooper & Murray, 1995).
Most cases of post-partum psychosis are manic-depressive in form, and there is much evidence for a close connection between puerperal and bipolar disorders. Nearly half of women with bipolar disorder experience childbearing-related episodes (Blehar et al, 1998), predominantly depression. Another literature links post-partum and 'cycloid' (acute polymorphic) psychoses.
Post-partum anxiety disorders are underemphasized and may be more common than depression (Matthey et al, 2003). A review of eight studies of 'panic disorder' showed that 44% anxious women had an exacerbation and 10% a new onset, in the puerperium (Hertzberg, 1999). The focus of anxiety is also important, because it may indicate specific psychological treatment. Since the pioneering study of Bydlowski and Raoul-Duval (1978), over 40 papers have appeared on PTSD resulting from stressful parturition. There have been eight quantitative studies, showing rates up to 5.6% (Creedy et al, 2000). Obsessions of infanticide were among the first post-partum disorders to be described (Chapman, 1959; Button, 1972). Other morbid phenomena can also become a problem for some mothers. A disorder akin to dysmorphophobia, based on the bodily changes resulting from pregnancy and childbirth, is common.
The available evidence regarding etiology, familiality and course of postpartum mental illness especially postpartum depression and postpartum psychosis, the two most studied disorders do not support post partum disorders as a distinct diagnostic entity. Though the exact etiology is unknown, childbirth seems to act as a specific trigger for many mental disorders in line with the stress diathesis model. As nearly the entire spectrum of mood disorders, psychotic disorders and anxiety and stress related conditions are seen in the perinatal period we propose that the specifier ‘onset within perinatal period’ should be added to all diagnoses in mood disorder, psychosis and adjustment disorder sections (ICD-10 F20-29, F30-39, F43 ).
Psychiatric disorders occurring in the postpartum period have many unique features. Chandran et al (2002) assessed 50 Indian women admitted to a psychiatric hospital for severe mental illness occurring in the postpartum period. Nearly half (43%) of the mothers reported infanticidal ideas, 36% reported infanticidal behavior, and 34% reported both infanticidal ideas and behavior. Logistic regression analyses indicated that presence of depression and psychotic ideas predicted infanticidal ideas, whereas presence of psychotic ideas toward the infant predicted infanticidal behavior.
Many mothers are excessively anxious about the health and safety of their children or they may fear the awesome responsibility of infant care. Most mothers are shielded from this by family support, but it can be a problem in isolated nuclear families. A mother with infant-focused anxiety may develop a phobia for the infant (Sved-Williams, 1992). Fear of cot death can reach pathological proportions (Weightman et al, 1999). Its main manifestation is nocturnal vigilance – the mother lying awake listening to the infant's breathing, with frequent checks that lead to exhausting sleep deprivation. As mentioned earlier, obsessions of infanticide were among the first post-partum disorders to be described (Chapman, 1959; Button, 1972) and a disorder akin to dysmorphophobia, based on the bodily changes resulting from pregnancy and childbirth is common.
Specific features of postnatal mood disorder are not acknowledged in the ICD 10 though they appear in the text of DSM IV (e.g., fluctuating course and mood lability, etc.). It is recommended that the text description of various disorders should highlight features specific to the perinatal period.
Developing a relationship with the newborn is the central and most important psychological process of the puerperium. A disturbed mother infant relationship is phenomenon distinct from depression. On one hand, mothers’ aversion to her infant is often disproportionate to depression and can occur without it; on the other hand, only a minority of depressed mothers has a relationship problem with their infants. This has led to proposals for a distinct ‘disorder of impaired mother-infant interaction’ (Brockington, 2004). Disorders of the mother-infant relationship are prominent in 10-25% of mothers referred to psychiatrists after childbirth. The etiology is probably different from post-partum depression, with more emphasis on unwanted pregnancy and challenging infant behaviour.
The main reason for the neglect of these disorders is their absence from ICD-10 and DSM-IV. In ICD-10, attachment disorders of childhood (reactive 94.1 and disinhibited 94.2) and 'Z codes' that include hostility towards the child, and scapegoating, address issues related only to the child's psychiatric state. One of the challenges for ICD-11 and DSM-V is to find a place for these disorders, so that they can be recognized by practitioners, and referred for expert treatment (Ainsworth et al, 1972; Salariya et al,1984; Hipwell & Kumar, 1996; Nagata et al, 2000; Brockington et al, 2001).
Though research in this area is lacking, the identification of this concept will sharpen the focus of studies aimed at preventing child abuse and neglect. Disorders of mother infant interaction may be included in the category F 53.
References
Address for Correspondence: Dr. Anju Dhawan, Associate Professor, Department of Psychiatry, AIIMS, New Delhi. Email address-anjudh[at]hotmail[dot]com
Pratap Sharan, MD, PhD, Nanaji Kaw, MD, Sabish Balan, MD, Kushal Jain, MD
Recommendations
Many South Asian psychiatrists would question the relevance of diagnosing and studying personality disorders. A major reason for the lack of interest in these conditions is their apparent rarity. A meta-analysis of general population studies carried out in India puts the prevalence figure for personality disorders at 0.6 per 1000 (Reddy and Chandrashekhar 1998). Very low rates have also been reported from Sri Lanka (Wijesinghe et al 1978). However, there are several shortcomings in the surveys conducted in developing countries (de Girolamo and Reich 1993).
Since the publication of the Diagnostic and Statistical Manual (DSM-III) in 1980 and its creation of a separate diagnostic axis (i.e. Axis II) for personality disorders, interest in the description and classification of personality disorders has expanded dramatically in the West. Between 20% and 40% of outpatients and more than 50% of inpatients in the western psychiatric set-up are reported to have comorbid personality disorders (Tyrer et al 1991). Comorbidity studies in India also suggest that personality disorders are common. In recent Indian studies, rates as high as 37.5% in patients with bipolar disorder, 40.8% in those with major depressive disorder (Naidu et al 1998) and 25.6% in those with substance use disorder (Kishore et al 1994) have been reported.
If personality disorders were a common but benign condition, there would still be no pragmatic reason to study them. However, they lead to a disturbance in functioning as great as that in most major mental disorders (Nakao et al 1992). Personality disorders are associated with high rates of separation and divorce; unemployment and inefficiency; and poor quality of life for the individual and his/her family. Patients with personality' disorders have an increased risk of mortality through suicide, homicide and accidents. Also, when a personality disorder is present, treatment of other coexisting psychiatric or medical conditions is frequently more complicated, lengthier, or less successful; a pattern that may at times be due to lack of recognition of the personality disorder (Oldham 1994).
The ICD-10 and DSM-IV are different but overlapping classification systems. Both have adopted polythetic diagnosis criterion a polythetic approach as against a monothetic approach. There are some differences in the nomenclatures such as anankastic in ICD-10 is obsessive-compulsive in DSM-IV, anxious in ICD-10 is avoidant in DSM-IV, and dissocial in ICD-10 is antisocial in DSM-IV. In ICD-10, borderline and impulsive personality disorders are viewed as subtypes of emotionally unstable personality disorder. In ICD-10, schizotypal disorder is considered to be an attenuated manifestation of schizophrenia and is categorized with the psychotic disorders; narcissistic, depressive and passive aggressive personality disorders do not find a mention.
There are also several marked differences in the criteria of the two systems and some minor variation in wording. The ICD-10 form of paranoid personality disorder includes excessive self-importance and self-reference as criteria, while in DSM-IV excessive self-importance forms a central part of narcissistic personality disorders. DSM-IV's schizoid personality disorder omits preoccupation with fantasy and introspection as criteria, though these are required in ICD-10.On the other hand, DSM-IV's antisocial personality disorder requires features of childhood conduct disorder, and emphasizes on law-breaking and criminal acts, while ICD-10's dissocial personality disorder does not mention childhood conduct symptoms in its set of criteria and is more concerned with generic concepts such as lack of empathy, inability to profit from experience and inability to maintain enduring relationships. In general, ICD-10 maintains a division between personality and mental state less clearly; for example, allowing the inclusion of persistent feelings of anxiety as a criterion in anxious personality disorder, and of obsessions in anankastic personality disorder.
ICD-10 requires the presence of three of the seven criteria to make a diagnosis (except for emotionally unstable personality disorder), while DSM-IV requires four or five from a list that varies from seven to nine (with the exception of antisocial personality disorder) (Sara et al 1996).
Current classification systems employ a categorical model for classifying personality disorders. However, there is considerable overlap among personality disorders. The dimensional model of classification has been proposed as a means to overcome these problems, as it can provide flexible, comprehensive and reliable information on subjects. However, much of the external validity research that is available currently has been conducted using categorical concepts, even though data on dimensional conceptualization of personality disorders is fast accumulating. Data support sometimes categorical, sometimes dimensional and sometimes both types of concepts.
Epidemiology: The prevalence of personality disorders defined in categorical terms range from 10.3% to 13.5% in community samples when assessment instruments specific to these disorders are used. The rate varied with age, with some decrease in older age groups. Urban populations and lower socioeconomic groups showed higher rates. The sex ratio was different for specific types of personality disorders, though the overall rate of prevalence was roughly equal for the two sexes (Reich and de Girolamo 1997). Prevalence rates of personality disorders may be lower in developing countries but methodological shortcomings in surveys done in these countries preclude direct comparisons. In the International Pilot Study of Personality Disorders (IPSPD), the following personality disorders were frequently diagnosed in a clinical sample at Bangalore (India): schizotypal (19.1 %) and borderline (14.7%) according to the DSM-III-R system; and emotionally unstable (8.6%) according to the ICD-I0 system (Loranger et al1997).
Reliability: The overlap between personality disorders defined in categorical terms is a reason forthe modest reliability seen in diagnosis, when different categorical conceptualizations of the same personality disorder (Hirshfield and Holzer 1994), different diagnostic systems (Sara et al 1996), or even different instruments operationalizing the same diagnostic system (Zimmerman 1994) are used.
Face validity: The face validity of the criteria sets for categorical definitions is low forboth the DSM-IIIR (Blashfield and Breen 1989) and ICD10 (Blashfield 1990) personality disorders.
Biological studies: There is some genetic support to categorical conceptualization of cluster A personality disorders, which are seen as existing in a genetic spectrum with psychotic disorders (Siever 1994, Siever, 2005). Antisocial personality disorder also appears to be heritable (Cadoret et al1995), but the specificity of a familial/genetic relationship of other personality disorders is suspect (Reich 1989; Torgersen 1994). On the other hand, Livesley and coworkers (Livesley et al 1992; Livesley 2005) demonstrated that 15 of the 18 personality disorder dimensions thought to underlie the DSM-III-R personality disorders had heritability in the range of 30%-60%. The results were similar to those reported for normal personalities and suggested a continuity between the normal and disordered personality.
Neuroimaging studies have provided some evidence for categorically defined personality disorders, e.g. increased ventricular-to-brain ratio and inefficient prefrontal cerebral processing in schizotypal subjects (Siever 1994). Positron emission tomography (PET) studies have also demonstrated some abnormalities in patients with antisocial personality disorder and metabolite borderline personality disorder (Doaln 1994; De la Fuente et al 1998; Pidimore et al 2005; Schmahl and Bremner 2006).
Neurochemical studies on the other hand have mainly provided evidence for dimensional conceptualization of personality features. E.g. schizotypal patients who display features of the deficit dimension have low cerebrospinal fluid (CSF) levels of the dopamine metabolite homovanillic acid (HVA) and those who have features of psychotic dimension have high CSF HVA levels (Siever 1994). In patients with duster B personality disorders (antisocial and borderline), 5-hydroxyindole acetic acid (5-HIAA) (a metabolite of serotonin) levels in the CSF and parameters of 5-HT (serotonin) functioning have been found to be inversely related to dimensions of impulsive aggression and negative affect. Also, platelet monoamine oxidase (MAO) levels are inversely related to dimensions of sensation-seeking and impulsivity (Dolan 1994; Coccarro et al 1997; Lara and Akiskal 2006, Lyons-Ruth et al, 2007).
Electrophysiological studies provide some evidence for categorically defined concepts. Abnormalities in relation to eye-movement and information processing have been reported to occur in patients with schizotypal personality disorder (Cadenhead et al 1993; Siever 1994; Evans et al 2007). Patients with borderline personality disorder have a decreased latency and increased density of rapid eye movements (REM) during sleep EEG recording. Some studies have also reported eye movement dysfunction and auditory evoked potential abnormalities in these patients (Lahmeyer et al1989; De la Fuente et al 1998; Boutros et al 2003; Howard and McCullagh, 2007). Evoked potential studies done under distraction conditions in patients with antisocial personality disorder reveal abnormalities in the P300 wave, suggesting deficits in information processing.
Treatment Studies: These studies have largely supported dimensional concepts. In general, pharmacotherapy aims at the correction of target symptoms such as aggression and behavioural dyscontrol, anxiety and mood dysregulation, and psychotic symptoms (including cognitive distortions) (Stein 1992; Cloninger et al 1997; Mohan 2002; Lara and Akiskal 2006). The limited data available on analytic psychotherapy (Bateman and Fonagy 1999) also do not support a diagnosis-based approach However, some data on other forms of psychotherapy have shown promise for specific categories of personality disorders, e.g. cognitive-behavioural therapy in avoidant personality disorder (Alden 1989) and dialectical behaviour therapy for borderline personality disorder (Linehan et al 1991).
Course and outcome: The literature regarding the long-term outcome of personality disorders is sparse (Skodol et al 2007). Most attention has been paid to formerly institutionalized patients with borderline, antisocial and schizotypal personality disorders. Borderline patients at 10-25 years follow up have a wide range of outcomes, from clinical recovery (50%-60%) to suicide (3%-9%). Suicide is particularly common in patients who have co-morbid depression or a history of substance abuse. If psychopathic traits are prominent, the long-term outcome in antisocial persons is bleak, though a substantial proportion of persons who exhibit a pattern of antisocial behaviour alone, recovers by the fourthdecade of life (Stone 1993). Schizotypal patients tend to remain isolated and lead marginal lives.
Boundary problems: within categorically defined personality disorders: Even though moderate internal consistency may exist forDSM-IIIR criteria sets of individual personality disorders, the correlation with other personality disorders is fairly high (Nunberger et al 1994; Widiger 2003). Consequently, there is a high rate of comorbidity (1.3 to 6.0) between personality disorders (Dolan et al 1995). Studies using multivariate statistical techniques have found that dimensions derived empirically bear a resemblance to some DSM-IIIR diagnoses but the correspondence between them is not close. In general, these studies have partially supported the cluster concept of the DSM system, with usually four superordinate factors corresponding to clusters I, II, III and obsessive-compulsive personality disorder emerging across many but not all studies (Hyler and Lyons 1988; Schroeder and Livesley 1991; Mulder and Joyce 1997; Skodol et al, 2007). The current classification systems have been criticized for either making over-refined descriptive distinctions, or forwrongly conceptualizing personality disorders as categories when they might be more properly described as trait dimensions.
Boundary problems: between personality disorders (Axis II) and symptom (state) disorders (Axis I): Although the distinction between Axes I and II disorders is valuable from the clinical point of view, the differentiation between the two sets of disorders is often problematic and at times even illusory. Particular problems exist in relation to differentiation between schizotypal personality disorder and schizophrenia spectrum disorders; borderline personality disorder and mood disorders; antisocial personality disorder and substance use disorders; and avoidant personality disorder and social phobia (Widiger and Shea 1991).
Boundary problems: between normal personality and personality disorder: Supporters of dimensional approach view personality disorders as extremes of temperamental traits found in the normal population (Schroeder and Livesley 1991; Costa and Widiger 1994; Paris 1997). The main reservations against this approach have been that (i) it has not been shown whether the three to five major dimensions found to describe normal personality (Digman 1990) also continuously underlie personality disorders; and (ii) some of the symptoms of personality disorders e.g. suicidal behaviour, self-mutilation do not have normative personality counterparts (Lenzwenger and Clarkin 1996). However, Livesley et al. (1992) showed that trait dimensions of personality disorders underlying DSM-III-R personality disorders in patient and general population samples are continuously distributed. They also demonstrated considerable similarity between the second-order factors (four) of personality pathology traits and four of the 'big five' factors of normal personality (Schroeder and Livesley 1991).
Authors who have used dimensional scaling techniques (Widiger et al 1987; Schroeder and Livesley 1991; Livesley et al 1992) and some who have carried out biological investigations in the area of personality disorders (Livesley et al 1993; Coccarro et al 1997) feel that the dimensional model fits the data on personality pathology in a better way. However, there are problems with this approach. It is not clear how personality pathology is actually organized at the latent level. The limited empirical evidence available suggests that schizotypy (Lenzwenger and Korfine 1992), borderline pathology (Trull et al 1990) and psychopathy (Harris et al 1994) may be organized as categories at the latent level. Further, biologists such as Kagan et al. (1987) and Magnusson (1986) noted that at least some personality traits may be dealt with in terms of physiobehavioural composites that are qualitatively distinct (categorical) rather than continuous (dimensional). In defence of the dimensional model, it may be said that the categorical criteria sets of schizotypal, borderline and antisocial personality disorders have been criticized for being saturated with items conveying the presence of symptomatic acts rather than personality traits (Stone 1993). Thus, they may have been more liable to show discreteness. The matter has not been adequately explored up to now for exclusive reliance on one or the other type of concepts.
Apart from the categories of personality disorders, ICD 11 should provide for agreed upon dimensions of personality and personality disorders. Evidence based candidates may be:
Dimensional models of personality:
Dimensional models of PDs:
Livesley and Jackson (1992) suggest ways to improve the classification of personality disorders by changing the way the classification is developed, evaluated, and modified so that it successively approximates a valid system. They argue that the first step in developing a classification is to ensure the content validity of diagnostic concepts because this is a prerequisite for other components of validity. Using trait and behavioural exemplars together in personality disorder criterion is a way to improve the content validity of personality disorders as it helps in tying the criterion to the concept and structure of the personality disorder, and in clarifying the nature of diagnostic items and the model for organizing diagnostic decisions. An example of using trait and behavioural exemplars together is given below:
Gross and persistent attitude of irresponsibility and disregard for social norms, rules and obligations, e.g. leaving a child less than 3 years of age alone at home for an hour to go and buy alcohol, dring at high speed around a blind corner, takes bribes, etc.
Specification of trait and behaviour exemplars would reduce the discrepancy between DSM-IV's antisocial personality disorder, which emphasizes law-breaking and criminal acts; and ICD-10's dissocial personality disorder, which is more concerned with generic concepts such as lack of empathy, inability to profit from experience and inability to maintain enduring relationships.
Defining the trait underlying the behaviour will also clarify the differentiation between Axis I and Axis II disorders. The differentiation between Axes I and II disorders parallels to some extent the distinction between personality traits and emotional states. Neuroticism, for example, involves the disposition to experience negative affects (McCrae and Costa 1990), and a correlation with mood states supports rather than questions its validity (Watson and Clark 1984). States and traits may best be conceptualized under prototypal concepts that provide meaningful distinction, but merge into each other at the boundaries (coaxial syndrome). It is useful to retain the differentiation because it has been shown that states affect personality domains differently, with relatively large parts of personality and behaviour (e.g. novelty-seeking, reward dependence) remaining unaffected by current states such as anxiety or depression (Svrakic et al 1992). Efforts to increase the distinction between state and trait disorders by adding or deleting existing criteria might change the meaning of the construct under study, e.g. borderline personality disorder would not remain the same if affective instability were to be removed from its description (Widiger and Shea 1991). On the other hand, defining the trait features consistently will improve reliability without compromising on validity.
The International Pilot Study for Personality Disorders (IPSPD) (Loranger et al 1997) demonstrated that personality disorders, as presently defined, could be identified at all sites (multinational, multilingual, multicultural). Similarly, cross-national studies suggest that the Three Factor Model of Eysenck (Eysenck 1982) and Five Factor Model (Costa and Widiger 1994) were invariant across cultures. However, these studies do not confirm the cross-cultural validity or usefulness of western diagnostic categories or personality dimensions, as they may have identified ethnic artefacts rather then culturally meaningful configurations (Lewis-Fernandez and Kleinman 1994). The five factors that emerged on the use of a lexicon of Chinese trait descriptors were different from the factors extracted from the Chinese translation of English words from an established five-factor questionnaire (Yang and Bond 1990). It has been hypothesized that culture can influence: the genetic selection of specific temperamental characteristics in highly inbred groups, learning inside and outside the family, the threshold when personality vulnerability cannot be compensated by the person, and the social threshold when such decompensations are labeled pathological (Neki 1970; Paris 1997).
From a cultural constructionist perspective, personality disorders are based on Anglo-American concepts of personhood and codes of appropriate bahaviour and owe their existence to the medicalization of disvalued social behaviour. Anxious (avoidant) and dependent personality disorders were excluded from the Chinese classificatory system because of the apparent rarity of these disorders and because it was felt that some of the defining features (e.g. subordination of one’s own needs to those of others on whom one is dependent) were normative in the Chinese culture which defines personhood not by autonomy and assertiveness but by intergenerational interdependence and self-effacement (Mezzich et al 2000).
In a similar way histrionic and dependent personality disorder may not be very useful in the Indian context. An observation of 290 cases (two thirds randomly selected and one third selected because of evidence of personality pathology) in a North-Western Indian clinical sample drawn from a general hospital setting (Sharan 2001) revealed only two case of histrionic personality disorder (0.7%) and 1 case of dependent personality disorder (0.3%). These disorders were not reported in the Bangalore centre (sample drawn from mental hospital setting) of the IPSPD also (Loranger et al1997). Histrionic behaviour may not be reported (histrionic personality disorder dimension had a moderately negative correlation with the lie/social desirability scale) or may be suppressed due to social disapproval, while dependent behaviour may be culturally normative. Specific problems with the criteria sets found in the Indian context were:
Dependent PD (DPD)
Histrionic PD (HPD)
ICD-10 requires the presence of three of the seven criteria to make a diagnosis (except for emotionally unstable personality disorder), while DSM-IV requires four or five from a list that varies from seven to nine (with the exception of antisocial personality disorder) (Sara et al1996). Livesley et al (1987) developed reliable scales to assess more than 50 traits thought to underlie each of the DSM III personality disorders.
The larger number of traits for each personality disorder would improve content coverage for personality disorders ensuring that they are not too narrowly defined. This expansion would also make it possible to include more culture-specific traits in the criterion set without reducing the possibility of making the diagnosis cross-culturally - with the help of other (less culture-specific) criteria.
ICD-10 requires the presence of three of the seven criteria to make a diagnosis for all personality disorders, except for emotionally unstable PD – impulsive type, in which only 2 of 5 criteria suffice. Three criteria of this disorder have overlapping behavioural referrants, hence the diagnosis can be made very easily. This is reflected in Indian studies. Emotionally unstable PD – impulsive type was the commonest diagnosis in an enriched clinical sample (two thirds randomly selected, one third selected for personality pathology) from Chandiagrh (4.1% definite diagnosis, 6.6% probable diagnosis) (Sharan, 2001); and also in the Bangalore sample of the IPSPD (4.3%) (Loranger et al 1997). However, clinicians rarely use the diagnosis owing perhaps to the unfamiliarity of the concept or because they think that it is only a part syndrome (Sharan, 2001).
Specification of mixed PD does not mention the number criteria required and the number of types of PD from which these criteria should be selected. Further, the mixed category may have no added advantage in a situation where all personality disorders have a lot of overlap and comorbid diagnosis is the norm.
No substantial empirical data have accrued to substantiate the validity of the following entities:
Hence, giving them a status above better established entities like narcissistic personality disorder appears anomalous.
Sharan (2001) found unexpectedly large (>0.4) correlation between the dimensional scores of ICD 10 paranoid and dissocial and emotionally unstable personality disorders. This is reflected in clinical experience (Sharan, paper submitted for publication) where a constellation of traits which can be tentatively termed as controlling/dominating personality disorder, present often for treatment. They seem to share features of emotionally unstable, paranoid (with narcissistic elements) and anankastic personality disorders. Studies of normal personality dimensions carried out in eastern cultures have noted rotational differences in structure, e.g. rotation of extraversion and agreeableness axes towards dominance and affiliation (Kagitbak et al 1996). Kagitbak et al (1996) feel that cultural nuances like an emphasis on smooth interpersonal relationships in Asia may be responsible for this shift of axes. It is understandable that conflicted dominance may show up (be labelled as) a personality disorder in cultures that emphasize subservience to hierarchy. In a similar way, while anxious (avoidant) personality was excluded from the Chinese classificatory system, Shinkeisitsu and Tajin Kyoufu (avoiding/rejecting due to interpersonal sensitivity) personality were described in Japan (Ono et al 1996). Shinkeisitsu and Tajin Kyoufu may reflect conflicts along the dimension of affiliation.
Controlling/dominating personality disorder and Tajin Kyoufu have parallels in the Structural Analysis of Social Behaviour (SASB) model (Benjamin 1996) where interpersonal behaviours as conceptualized as constituted by inputs from two primary dimensions - interdependence (dominance/submission versus independence) and affiliation (aggression versus sexuality).
Kernberg (1996) regards affects to be instinctive components of human behavior that emerge in the earliest stages of development and are gradually organized as part of early object relations into gratifying, rewarding, pleasurable affects or libido as an overarching drive, and into painful, aversive, negative affects which are organized into aggression as an overarching drive. Rage represents the basic affect of aggression as a drive, and its vicissitudes explain the origins of hatred and envy, as well as of anger and irritability as moods. He suggests that the earliest function of rage is the effort to eliminate a source of irritation or pain. A second function of rage is to eliminate an obstacle or barrier toward gratification. The third, developmentally a higher level function of rage is the elimination of a bad object that is intra psychically perceived as a willful source of frustration standing between the self and the gratification of a need. At a more advanced level, the wish is no longer to destroy the bad object, but to make it suffer. At a further level of development, the wish to make the bad object suffer shifts into the wish to dominate and control the bad object in order to avoid fears of persecution from it; as obsessive mechanisms attempt to regulate the suppression or repression of aggression. Finally, the original self-affirmative implications of rage may be seen in sublimatory aspects of the aggressive response in the search for autonomy and self-affirmation, and for freedom from external control. We feel that the controlling/dominating personality disorder person probably operates at the level where the wish to make the bad object suffer shifts into the wish to dominate and control the bad object as obsessive mechanisms attempt to regulate the suppression or repression of aggression but often fail to do so.
Proposed criteria for controlling/dominating PD
Zuckerman M, Kuhlman DM, Joireman J, et al. A comparison of three structural models of personality: the big three, the big five and the alternate five. J Pers Soc Psychol 1993; 65:757-768.
Address for Correspondence: Professor Pratap Sharan, Department of Psychiatry, All India Institute of Medical Sciences, Ansari Nagar, New Delhi – 110029.
Manju Mehta, PhD; Rajesh Sagar, MD; Ravindra Rao, MD.
The diagnostic criteria for Attention Deficit Hyperactivity Disorder (ADHD) followed by the Diagnostic and Statistical Manual (DSM – IV) should be incorporated as it is in the ICD 11 edition. Thus, the criteria should be as follows:
I. Either A or B:
A.Six or more of the following symptoms of inattention have been present for at least 6 months to a point that is disruptive and inappropriate for the developmental level:
Often does not follow instructions and fails to finish schoolwork, chores, or duties in the workplace (not due to oppositional behavior or failure to understand instructions).
Often avoids, dislikes, or doesn't want to do things that take a lot of mental effort for a long period of time (such as schoolwork or homework).
Often loses things needed for tasks and activities (e.g. toys, school assignments, pencils, books, or tools).
B.Six or more of the following symptoms of hyperactivity-impulsivity have been present for at least 6 months to an extent that is disruptive and inappropriate for developmental level:
The following categories for hyperkinetic disorder should be used in ICD 11.
Suggested criteria:
Evidence for the Proposed Changes
The current diagnostic criteria for hyperkinetic disorder in the ICD 10 differ from the diagnostic criteria incorporated in DSM IV in the following ways:
§ ICD 10 has divided the symptoms of hyperkinetic disorder into 3 main clusters – inattention, hyperactivity and impulsivity; DSM IV, on the other hand, has combined the hyperactivity and impulsivity clusters.
§ ICD 10 requires that the child should meet the criteria in more than one situation, whereas DSM IV requires the child has impairment in more than one situation (rather than meeting the entire criteria in more than one situation).
For ADHD/ hyperkinetic disorder, DSM IV criteria are better researched, while ICD 10 descriptions are used more often in clinics. Consequently, much of the published articles work relate to DSM IV criteria of ADHD.
Epidemiological studies: Malhi and Singhi (2000) reported that 8.1% of a consecutive sample of 245 children referred for evaluation to the Psychology outpatient services of the Department of Pediatrics of a tertiary care teaching hospital had ADHD. In a similar study, Mukhopadhyay et al (2003) found that 15.5% of children presenting to a child guidance clinic in a pediatric hospital over a one year period had ADHD. These studies demonstrated the utility of the ADHD diagnosis and the ease of applicability of DSM IV criteria in the Indian pediatric population.
Phenomenology: A factor analysis of symptoms of the disorder showed that a two-factor model had the best fit to the data – inattention and hyperactivity/ impulsivity (Hudziak et al, 1998). This supports the DSM IV proposal of two subtypes of ADHD rather than the three subtypes proposed by ICD 10. Studies have shown that while ADHD is a broad, heterogeneous category, the subgroup of children diagnosed as hyperkinetic disorder (the subtype in ICD 10) fit in the severe ADHD combined subtype of DSM IV criteria (El-Sayed et al, 2003).
Course and prognosis: A study that compared the predictive validity of ADHD according to ICD 10 and DSM IV criteria (Lahey et al. 2006) concluded that while both ICD-10 hyperkinetic disorder and DSM-IV ADHD exhibit predictive validity over 6 years, ICD-10 hyperkinetic disorder appears to under-identify children with persistent ADHD symptoms and related impairment. Children who met criteria for DSM-IV ADHD but not hyperkinetic disorder exhibited at least as much functional impairment over time as hyperkinetic children. A review by El-Sayed et al (2003) concluded that children showing symptoms above the threshold for a diagnosis of ADHD according to DSM IV are at risk of developing co morbid conditions and increasing stress in both parents and teachers. Theses reports suggest that children with features of ADHD, who cannot be diagnosed by ICD 10, but receive such a diagnosis according to DSM IV criteria need to be identified and managed appropriately.
The hyperkinetic disorder (ADHD) in ICD 10 and DSM IV is currently sub classified as follows (Table 1):
| ICD 10 | DSM IV |
|---|---|
| F90.0 Disturbance of activity and attention | 314.01 ADHD, combined type (ADHD-C) 314.02 ADHD, predominantly inattention type (ADHD-I) 314.03 ADHD, predominantly hyperactive-impulsive type (ADHD-HI) |
| F98.8 Inclusion term in other specified behavioral and emotional disorders | |
| --- | |
| F90.1 Hyperkinetic conduct disorder | --- |
| F90.8 Other hyperkinetic disorder | --- |
| F90.9 Hyperkinetic disorder, unspecified | ADHD NOS |
ICD: International Classification of Disease; DSM: Diagnostic and Statistical Manual
ADHD: Attention Deficit Hyperactivity Disorder
The authors propose the following categories to be used for hyperkinetic disorder/ADHD in ICD 11:
Epidemiological studies: Studies using the DSM IV criteria show that ADHD – inattentive subtype is the most common one followed by ADHD – combined subtype (2nd most common) and ADHD – hyperactive impulsive subtype (Graetz et al, 2001; Ford et al, 2003). The study by Malhi and Singhi (2000) confirmed that all the 3 subtypes of ADHD (according to DSM IV criteria) were common in India – 50% of the children had hyperactive-impulsive subtype, 35% had the inattentive subtype and 15% had the combined subtype.
Sociodemographic profile: Studies have shown that ADHD-hyperactive impulsive subtype is more frequent in the younger age group as compared to the ADHD-inattention subtype (Nolan et al. 1999, Malhi and Singhi, 2000). It also has been seen that ADHD-inattention subtype is more common among females than males (Biederman et al. 2002).
Comorbidity: Studies have shown differences in the comorbidity between the three subtypes of ADHD. Thus, higher rates of anxiety and depression were seen in those with ADHD-combined subtype and ADHD-inattention subtype compared to those with ADHD-hyperactive impulsive subtype (MTA Cooperative Group, 1999). One study has found higher rates of bipolar disorder and tic disorder in those with ADHD-combined subtype (Faraone et al, 1998). Oppositional defiant and conduct disorders are most commonly seen in children with ADHD-combined subtype, followed by ADHD-hyperactive impulsive and ADHD-inattention subtypes (Morgan et al, 1996). An Indian study (Malhi and Singhi, 2000) found differences between the 3 subtypes with respect to intelligence, academic difficulties, relationship with peers and behavioral problems.
Family studies: Though some studies have shown increased rates of a particular subtype in the relatives of the affected children (Faraone et al. 2000), other studies have not found such increased rates (Smalley et al, 2000). Thus the family studies have been inconclusive.
Treatment response: Studies on differential stimulant treatment response among various subtypes of hyperkinetic disorder/ADHD are not available as most of the trials have only recruited children with combined ADHD (MTA Cooperative Group, 1999). Studies that have employed other subtypes, have not reported treatment response separately (Kratochvil et al, 2002).
Course and prognosis: The degree and type of impairment have been shown to be different among different subtypes of ADHD. Lahey et al (2006) have shown that ADHD-combined and ADHD-hyperactive impulsive subtypes have greater impairment than ADHD-inattention subtype. It is also seen that ADHD-inattention subtype is associated with more academic problems, whereas ADHD-hyperactive impulsive subtype is associated with more social and behavioral problems (Gadow et al, 2000; Graetz et al, 2001).
Thus, studies have shown that there are several differences between the subtypes of ADHD, thereby making it important to recognize these subtypes.
Co-occurrence: While most children who meet the criteria for conduct disorder also meet the criteria for ADHD; only about one third of adolescents with conduct disorder meet the criteria for ADHD (Reeves et al, 1987; Szatmari et al, 1989).
Impairment: In terms of academic achievement, children with combined ADHD/conduct disorder have higher rates of reading disorders than ADHD and controls (McGee et al, 1984). Children with combined ADHD/conduct disorder were found to be more impaired in verbal skill, visual motor integration and visuospatial skills as compared to children with ADHD and controls (Moffitt and Silva, 1988). An Indian study (Malhotra et al, 1999) compared hyperkinetic conduct disorder (HCD) with conduct disorder and found that the HCD children had lower intelligence, more perinatal complications and delayed milestones.
Family history: Biederman et al (1992) examined the rates of psychiatric diagnosis among relatives of a large sample of ADHD and ADHD/conduct disorder. While the rates of ADHD was the same in both group of relatives, conduct disorder was more common among relatives of combined ADHD/conduct disorder than among ADHD disorder alone. Furthermore, relatives with conduct disorder also tended to have ADHD. This means that the two disorders co-segregated, indicating that ADHD/conduct disorder is a distinct familial subtype.
Course and prognosis: Studies have shown differences in the long term outcomes of both subgroups of children. The ADHD/conduct disorder subgroup showed more antisocial and defiant behaviors (August et al, 1983). Also this group showed a higher rate of substance use. Studies have also concluded that while ADHD itself conveys some risk for adult antisocial behavior, the combined ADHD/conduct disorder group had sharp rise in the risk of adult antisocial personality and criminal conviction (Mannuzza et al, 1989). The Indian study (Malhotra et al, 1999) that compared hyperkinetic conduct disorder (HCD) with conduct disorder also found that the HCD group had an younger age of onset, more gradual development of conduct symptoms and a longer duration of conduct symptoms.
Treatment response: Studies do not show any difference in the response to stimulant treatment between the ADHD/conduct disorder and ADHD group alone (Klonman et al, 1989).
Available evidence suggests that there is a need to have a separate diagnostic subgroup of hyperkinetic disorder.
The group of F70 – F79 consists of mental retardation, which includes the mild, moderate and severe types. Most of the intelligence tests used have a separate category for borderline intelligence. The DSM IV, too, places borderline intelligence in the group of ‘additional conditions that may be a focus of clinical attention’.
Borderline intellectual functioning, has received little attention to date. However, some studies on prevalence of this condition show that it is present in up to 7%–18% of the population (Hassiotis et al, 1999; Ninivaggi, 2001).
In a study by Chen et al (2006), it was seen that children with subaverage cognitive abilities were more likely to develop mental health problems than their counterparts with IQs above 80 in later life. Another study by Hassiotis et al (1999) which have also shown that those with comorbid borderline intelligence and psychotic illness had greater disability and were more likely to suffer extrapyramidal side-effects and show evidence of negative symptoms than those with psychotic illness with normal intelligence. This may lead to difficulties in other domains of adaptive functioning. Thus, studies have shown that individuals with borderline intelligence may require a separate category.
Hence, borderline intelligence should be included in the ‘Z’ category to provide recognition to this condition in the international classificatory system.
Author for correspondence: Dr. Rajesh Sagar, Associate Professor, Department of Psychiatry, All India Institute of Medical Sciences, New Delhi – 110029. E-mail: rsagar_29[at]yahoo[dot]com
| YEAR - 1963 | |||
| 1. | DR. SURESH CHANDRA PANT | MAY | 1963 |
| YEAR – 1965 | |||
| 2. | DR. DAVINDER MOHAN | MAY | 1965 |
| 3. | DR. K. SUDHAKAR SHETTY | DEC | 1965 |
| YEAR – 1966 | |||
| 4. | DR. P. RAGHURAM REDDY | MAY | 1966 |
| 5. | DR. SHUBHA TRIVEDI | MAY | 1966 |
| 6. | DR. SATISH CHANDER MALIK | MSY | 1966 |
| 7. | DR. ADARSH SINGH MAHAL | DEC | 1966 |
| 8. | DR. BHUJANGRA RAO K. | DEC | 1966 |
| 9. | DR. VIRAT KRISHAN | DEC | 1966 |
| YEAR – 1967 | |||
| 10. | DR. JAGDISH SINGH TEJA | MAY | 1967 |
| 11. | DR. SUDARSHAN CHAWLA | MAY | 1967 |
| 12. | DR. RAMESH CHAND SETH | DEC | 1967 |
| YEAR – 1968 | |||
| 13. | DR. SURESH CHANDRA PANT | MAY | 1968 |
| 14. | DR. ANIL KUMAR AGARWAL | DEC | 1968 |
| 15. | DR. DIGVIJAY SINGH ROEL | DEC | 1968 |
| YEAR – 1969 | |||
| 16. | DR. BALWANT RAIAGNIHOTRI | MAY | 1969 |
| 17. | DR. EARNEST ROMESH CHANDER | MAY | 1969 |
| 18. | DR. LAL MOHAN GHOSH | MAY | 1968 |
| 19. | DR. PRAKASH BULAKIDAS BANTHIA | MAY | 1969 |
| 20. | DR. THUMULURY SIVA SUBRAHAMANYAN | MAY | 1969 |
| 21. | DR. GUL B. ADVANI | DEC. | 1969 |
| YEAR – 1970 | |||
| 22. | DR. DILEEP SINGH RASTOGI | MAY | 1970 |
| 23. | DR. MANJIT SINGH DHILLON | MAY | 1970 |
| 24. | DR. PREM LATA NANDA | DEC. | 1970 |
| YEAR – 1971 | |||
| 25. | DR. BENOYENDRA NATH MAJUMDAR | MAY | 1971 |
| 26. | DR. RANVIR KUMAR SOOD | DEC. | 1971 |
| YEAR – 1972 | |||
| 27. | DR. SWARN KANTA KHERA | MAY | 1972 |
| 28. | DR. BACHITTAR SINGH | DEC. | 1972 |
| 29. | DR. KANWAL KRISHAN BINDAL | DEC. | 1972 |
| 30. | DR. NEENA MAHAJAN | DEC. | 1972 |
| YEAR – 1973 | |||
| 31. | DR. HARINDER MOHAN CHAWLA | MAY | 1973 |
| 32. | DR. VELAGAPUDI BAPUJI RAO | MAY | 1973 |
| 33. | DR. SHYAM LAL KHANNA | MAY | 1973 |
| 34. | DR. S. RAJKUMAR | DEC. | 1973 |
| YEAR – 1974 | |||
| 35. | DR. RABINDRA NATH NANDI | MAY | 1974 |
| YEAR – 1975 | |||
| 36. | DR. V. M. DAMODARAN NAMBOODIRI | MAR. | 1975 |
| 37. | DR. VIRINDER KUMAR | MAY | 1975 |
| YEAR – 1976 | |||
| 38. | DR. M. G. THOMAS | FEB. | 1976 |
| 39. | DR. DAVINDER SINGH KOCHHAR | APR. | 1976 |
| 40. | DR. VENUGOPALAN RAGHAVAKURUP | MAY | 1976 |
| 41. | DR. ADARSH KUMAR VOHRA | DEC. | 1976 |
| YEAR – 1977 | |||
| 42. | DR. PRANIT KUMAR CHAUDHURY | JAN. | 1977 |
| 43. | DR. RAJAT RAY | FEB. | 1977 |
| 44. | DR. SUMAN AGARWAL | MAY | 1977 |
| 45. | DR. BIMAL CHOWDHARY | MAY | 1977 |
| 46. | DR. RATNA BILWANI | MAY | 1977 |
| 47. | DR. ANANDI LAL | DEC. | 1977 |
| YEAR – 1978 | |||
| 48. | DR. K. NAGARAJA RAO | MAY | 1978 |
| 49. | DR. P. N. RAMANI | MAY | 1978 |
| 50. | DR. HARINDER SINGH SETHI | DEC. | 1978 |
| 51. | DR. KULWANT SINGH BAGHIANA | DEC. | 1978 |
| 52. | DR. VINAY KAPOOR | DEC. | 1978 |
| YEAR – 1979 | |||
| 53. | DR. JACOB K. JOHN | MAY | 1979 |
| 54. | DR. SHOBHA PILLAI | JUNE | 1979 |
| 55. | DR. MOHAN DAS. E. | DEC. | 1979 |
| YEAR – 1980 | |||
| 56. | DR. SANDI SYLEM | JULY | 1980 |
| 57. | DR. MINAKSHI MUKHOPADHYAYA | JULY | 1980 |
| 58. | DR. PREVESH KUMAR RUSTAGI | DEC. | 1980 |
| YEAR – 1981 | |||
| 59. | DR. PERMINDER SINGH SACHDEV | DEC. | 1981 |
| 60. | DR. SHEKAR SAXENA | DEC. | 1981 |
| 61. | DR. DHRUBA MAN SHRESTHA | DEC. | 1981 |
| YEAR – 1982 | |||
| 62. | DR. GEEANESWAR GAYA | MAY | 1982 |
| 63. | DR. SURENDRA KUMAR JAYASWAL | DEC. | 1982 |
| 64. | DR. PADMA RAJU VARREY | DEC. | 1982 |
| YEAR – 1983 | |||
| 65. | DR. ADITYAN JEE | DEC. | 1983 |
| 66. | DR. ALOK SARIN | DEC. | 1983 |
| YEAR – 1984 | |||
| 67. | DR. ASHOK SHARMA | DEC. | 1984 |
| 68. | DR. SMITA LAXMIKANT NIMGAONKAR | DEC. | 1984 |
| YEAR – 1985 | |||
| 69. | DR. MOPIDEVI VIJAYA GOPAL | MAY | 1985 |
| 70. | DR. NIRAKAR MAN SHRESTHA | MAY | 1985 |
| 71. | DR. MAHENDRA KUMAR NEPAL | DEC. | 1985 |
| 72. | DR. K. B. BALA RAJU | DEC. | 1985 |
| YEAR – 1986 | |||
| 73. | DR. G. S. P. RAJU | MAY | 1986 |
| 74. | DR. K. PRAVEEN LAL | DEC | 1986 |
| YEAR – 1987 | |||
| 75. | DR. PARTMA SARATHI DAS | MAY | 1987 |
| 76. | DR. AJIT KUMAR DAS | DEC | 1987 |
| YEAR – 1988 | |||
| 77. | DR. KHONDAKAR ABUYL HASANAT | DEC | 1968 |
| 78. | DR. RATAKONDA SANTHISAGAR | DEC | 1988 |
| YEAR - 1989 | |||
| 79. | DR. P. MALLIKARJUNA | DEC. | 1969 |
| 80. | DR. VEMIREDDY SREE NIVASULU | DEC | 1969 |
| YEAR - 1990 | |||
| 81. | DR. J. PRAVEEN | MAY | 1990 |
| 82. | DR. PRATAP SHARAN | DEC. | 1990 |
| YEAR – 1991 | |||
| 83. | DR. SHIVANANDA JENA | MAY | 1991 |
| 84. | DR. ANIL KUMAR NIGAM | MAY | 1991 |
| 85. | DR. SORAM MANIKANTA SINGH | DEC. | 1991 |
| YEAR - 1992 | |||
| 86. | DR. SANJEEV KUMAR | MAY | 1992 |
| 87. | DR. KAVURU BUSH | DEC. | 1992 |
| 88. | DR. EAMON KALYAN DUTTA | DEC. | 1992 |
| 89. | DR. SUNIL KUMAR | DEC. | 1992 |
| YEAR - 1993 | |||
| 90. | DR. VIVEK KATOCH | MAY | 1993 |
| 91. | DR. K. NEGI REDDY | MAY | 1993 |
| 92. | DR. MADHURI V. KAMBLE | MAY | 1993 |
| 93. | DR. ANJU DHAWAN | DEC. | 1993 |
| 94. | DR. CHANDNI SINGH | DEC. | 1993 |
| YEAR - 1994 | |||
| 95. | DR. GEETA CHAUDHARY | DEC. | 1994 |
| 96. | DR. DHANESH KUMAR | DEC. | 1994 |
| YEAR - 1995 | |||
| 97. | DR. PRITHWIS BHAUMIK | MAY | 1995 |
| 98. | DR. PRASANT KUMAR SAMANTARAY | MAY | 1995 |
| 99. | DR. RAHUL TOMAR | DEC. | 1995 |
| 100. | DR. NIRUJ KUMAR AGRAWAL | DEC. | 1995 |
| 101. | DR. SIMRAT SINGH SETHI | DEC. | 1995 |
| 102. | DR. KOIJAM SHANTIBALA DEVI | DEC. | 1995 |
YEAR - 1996
| |||
| 103. | DR. KIRTANA BALLAKOOR | MAY | 1996 |
| 104. | DR. PRAVIR SHANKAR PRASAD | DEC. | 1996 |
| YEAR - 1997 | |||
| 105. | DR. SABAASIAM (BALJEET KAUR) | MAY | 1997 |
| 106. | DR DR. KHURSHID AHMAD KHURSHID | DEC. | 1997 |
| YEAR - 1998 | |||
| 101. | DR.DR. A. TEMSUYANGER A. O. | MAY | 1998 |
| 108. | DR DR. RAMESH KUMAR | MAY | 1998 |
| 10S. | DR.DR. AMIYA BANERJEE | MAY | 1998 |
| 110. | DR. PRAMOD MOHAN SHYANGWA | MAY | 1998 |
| 111. | DR. SUJIT KUMAR NAIK | DEC. | 1998 |
| 112. | DR. RAJKUMAR LENIN SINGH | DEC. | 1998 |
| YEAR – 1999 | |||
| 113. | DR. EDWIN K. SIMON | MAY | 1999 |
| 114. | DR. NEERAJ BERRY | MAY | 1999 |
| 115. | DR. JFSU NATH | DEC. | 1999 |
| 116. | DR. NAND KUMAR | DEC. | 1999 |
| 117. | DR. PALLAB KUMAR MAULIK | DEC. | 1999 |
| 118. | DR. ATUL AMBEKAR | DEC. | 1999 |
| YEAR – 2000 | |||
| 119. | DR. SAJAL KUMAR GUPTA | MAY | 2000 |
| 120. | DR. AJAY KUMAR BHATT | MAY | 2000 |
| 121. | DR AMULYA BHARAT | MAY | 2000 |
| 122. | DR. AMITABHA SAHA | DEC. | 2000 |
| 123. | DR. EDDIE OSMOND MUKHIM | DEC. | 2000 |
| YEAR – 2001 | |||
| 124. | DR. MONALARINDAM B. | MAY | 2001 |
| 125. | DR. MANOJ KUMAR M. N. | MAY | 2001 |
| 126. | DR. SANJAY KR. PATANAYAK | MAY | 2001 |
| 127. | DR. RAJESH KUMAR | MAY | 2001 |
| 128. | DR. FARZANA KADER LINDA | MAY | 2001 |
| 129. | DR. SUBHAS SOREN | DEC. | 2001 |
| 130. | DR. SHANTANU DE | DEC. | 2001 |
| YEAR – 2002 | |||
| 131. | DR. VIJENDER SINGH | DEC. | 2002 |
| 132. | DR. PRIYANKA BHATIA | DEC. | 2002 |
| YEAR – 2003 | |||
| 133. | DR. RABI SHAKYA | MAY | 2003 |
| 134. | DR. AVINASH HOSANAGAR | MAY | 2003 |
| 135.. | DR. ANKUSH SINGHAL | DEC. | 2003 |
| 136. | DR. NILOTPAL DAS | DEC. | 2003 |
| 137. | DR. SHASHI BHUSHAN KUMAR | DEC. | 2003 |
| 138. | DR. DEEPAK GARG | DEC. | 2003 |
| 139. | DR. SRINIVAS T. R. | DEC. | 2003 |
| 140. | DR. AMARDEEP KUMAR | DEC | 2003 |
| YEAR – 2004 | |||
| 141. | DR. MITALI BHUYAN | MAY | 2004 |
| 142. | DR. RAVINDRA V. RAO | MAY | 2004 |
| 143. | DR. KUMAR RANJAN MAJI | MAY | 2004 |
| 144. | DR. TINA LAL | MAY | 2004 |
| 145. | DR. AMBICA PRASAD JHA | MAY | 2004 |
| 146. | DR. RAJA SADHU | DEC. | 2004 |
| YEAR – 2005 | |||
| 147. | DR. RAMAN GARG | MAY | 2005 |
| 148. | DR. SHIVANAND KATTIMANI | MAY | 2005 |
| 149. | DR. RAMAN DEEP | MAY | 2005 |
| 150. | DR. SABISH BALAN | DEC. | 2005 |
| YEAR – 2006 | |||
| 151. | DR. RAJIV KUMAR SHARMA | MAY | 2006 |
| 152. | DR. YATAN PAL SINGH BALHARA | MAY | 2006 |
| 153. | DR. ALOK AGRAWAL | DEC. | 2006 |
| 154. | DR. MRIDULA KAYAL | DEC. | 2006 |
| 155. | DR. A. SHYAM SUNDAR | DEC. | 2006 |
| 156. | DR. JATINDER MOHAN CHAWLA | DEC. | 2006 |
| 157. | DR. SUNNY T. VARGHESE | DEC. | 2006 |
| YEAR – 2007 | |||
| 158. | DR. NAND KISHORE | MAY | 2007 |
| 159. | DR. ROZATKARABHIJIT RAMDAS | MAY | 2007 |
| 160. | DR. PREETI SINHA | MAY | 2007 |
| 161. | DR. PRASHANT GOYAL | MAY | 2007 |
| 162. | DR. SHIVA PRAKASH | MAY | 2007 |
| 163. | DR. KUSHAL D. JAIN | MAY | 2007 |
| YEAR – 2008 | |||
| 164. | DR. KOUSHIK SINHA DEB | MAY | 2008 |
| 165. | DR. AMIT KUMAR GUPTA | DEC. | 2008 |
| 166. | DR. BISWADIP CHATTERJEE | DEC. | 2008 |
| 167. | DR. VIJETA KUSHWAHA | DEC. | 2008 |
| 168. | DR. ROHIT VERMA | DEC. | 2008 |
| YEAR – 2009 | |||
| 169. | DR. SURESH CHAND | MAY | 2009 |
| 170. | DR. LITON MALLICK | MAY | 2009 |
| 171. | DR. ABHISHEK PALLAVA | DEC. | 2009 |
| 172. | DR. PRADIPTA MAJUMDAR | DEC. | 2009 |
| 173. | DR. ANISH P. K. | DEC. | 2009 |
| 174. | DR. SANTOSH I. RAMDURG | DEC. | 2009 |
| YEAR – 2010 | |||
| 175. | DR. SIVARAMAN SUBHRAMANIAN | MAY | 2010 |
| 176. | DR. PRASHANTH SWAMINATHAN | MAY | 2010 |
| 177. | DR. ASHISH MITTAL | MAY | 2010 |
| 178. | DR. BICHITRA NANDA PATRA | MAY | 2010 |
| 179. | DR. SHRIGOPAL GOYAL | MAY | 2010 |
| YEAR – 2011 | |||
| 180. | DR. SIDDHARTH SARKAR | MAY | 2011 |
| 181. | DR. RAJEEV RANAJAN | MAY | 2011 |
| 182. | DR. ADITYA PAWAR | MAY | 2011 |
| 183. | DR. SAGAR BERA | MAY | 2011 |
| 184. | DR. PIYALI MANDAL | MAY | 2011 |
| 185. | DR. RISHAB GUPTA | DEC | 2011 |
| 186. | DR. VIJAY KRISHNAN | DEC | 2011 |
| YEAR – 2012 | |||
| 187. | DR. ANIRUDDHA BASU | MAY | 2012 |
| 188. | DR. TULESHWAR SINGH | MAY | 2012 |
| 189. | DR. ROSHAN BHAD | MAY | 2012 |
| 190. | DR. NANDITA HAZARI | DEC | 2012 |
| 191. | DR. SUNDAR GNANAVEL | DEC | 2012 |
| YEAR – 2013 | |||
| 192. | DR. MRINMAY DAS | MAY | 2013 |
| 193. | DR. ASHOK CHAUDHARY | MAY | 2013 |
| 194. | DR. MADHURIMA GHOSH | MAY | 2013 |
| 195. | DR. SATHYAPRAKASH | MAY | 2013 |
| 196. | DR. SHAILESH JHA | MAY | 2013 |
| 197. | DR. SHAMBHU PRASAD | MAY | 2013 |
| 198. | DR. RAJU BHATTARAI | MAY | 2013 |
| 199. | DR. DEEKSHA ELWADHI | MAY | 2013 |
| 200. | DR ARUMUGANATHAN ANMUGAVINAYAGAM | DEC | 2013 |
| 201. | DR. MOHIT VARSHNEY | DEC | 2013 |
| YEAR - 2014 | |||
| 202. | DR. NRIPENDRA KUMAR | MAY | 2014 |
| 203. | DR. ANIL YADAV | MAY | 2014 |
| 204. | DR. NISHANTH KN | MAY | 2014 |
| 205. | DR. SAURABH KUMAR | MAY | 2014 |
| 206. | DR. ROHIT ALOK | DEC | 2014 |
| 207. | DR. PARVESH BATRA | DEC | 2014 |
| 208. | DR. ANANYA MAHAPATRA | DEC | 2014 |
| 209. | DR. ANKIT GUPTA | DEC | 2014 |
| 210. | DR. VAIBHAV PATIL | DEC | 2014 |
| YEAR – 2015 | |||
| 211. | DR. SHOBHIT JAIN | MAY | 2015 |
| 212. | DR. PAWAN SHARMA | MAY | 2015 |
| 213. | DR. ARGHYA PAL | MAY | 2015 |
| 214. | DR. ARPIT PARMAR | MAY | 2015 |
| 215. | DR. DARA SINGH POONIA | MAY | 2015 |
| 216. | DR. PRASHANT GUPTA | MAY | 2015 |
| 217. | DR. SHYAMANAND ROY | DEC | 2015 |
| 218. | DR. ASHISH PAKHRE | DEC | 2015 |
| YEAR – 2016 | |||
| 219. | DR. POOJA PATTNAIK | MAY | 2016 |
| 220. | DR. SNEHIL GUPTA | MAY | 2016 |
| 221. | DR. SURESH THAPALIYA | MAY | 2016 |
| 222. | DR. SACHIN KUMAR | MAY | 2016 |
| 223. | DR. ABHINAV PANDEY | MAY | 2016 |
| 224. | DR. NAJEF MOIDEEN | DEC | 2016 |
| 225. | DR. SARTAJ DEEPAK | DEC | 2016 |
| 226. | DR. RISHI GUPTA | DEC | 2016 |
| 227. | DR DEEPAK CHARAN | DEC | 2016 |
Submitted to
Indian Psychiatric Society (IPS)
Department of Psychiatry,
All India Institute of Medical Sciences, New Delhi
Report Citation:
This report should be cited as:
Department of Psychiatry, AIIMS (2008). ICD-11: Draft Proposal for Changes in the Classification of Mental and Behavioural Disorders
Editor:
Pratap Sharan,
Professor,
Department of Psychiatry,
AIIMS, New Delhi
Rajat Ray,
Professor,
Chief, National Drug Dependence Treatment Centre and Head, Department of Psychiatry,
AIIMS, New Delhi
Dr Pratap Sharan had full access to all of the materials in this report and takes responsibilityfor the integrity and accuracy of its summarization.
Contents
| S. No. | Chapter | Pages |
|---|---|---|
| 1 | Introduction | 1 |
| 2 | Classification of Psychiatric Disorders: General Issues | 2-12 |
| 3 | Organic, including Symptomatic, Mental Disorders | 13-18 |
| 4 | Mental and Behavioural Disorders due to Psychoactive Substance Use | 19-24 |
| 5 | Schizophrenia, Schizotypal and Delusional Disorders | 25-34 |
| 6 | Mood Disorders | 35-46 |
| 7 | Neurotic, Stress Related and Somatoform Disorders | 47-50 |
| 8 | Behavioural Syndromes associated with Physiological Disturbances and Physical Factors | 51-59 |
| 9 | Personality Disorders | 60-70 |
| 10 | Categories ‘F70 – F98’ | 71-76 |
The draft proposal for changes in the classification of mental and behavioural disorders towards ICD 11 was prepared under the aegis of the Department of Psychiatry, All India Institute of Medical Sciences for consideration in an Indian Psychiatric Society (IPS) Committee, which will send its recommendations to the World Psychiatric Association (WPA). The draft proposal is also available on the Departmental website.
Each chapter was prepared by faculty members, who were assisted by residents of the department. In preparing their suggestions the authors often referred to the Robins and Guze criteria to evaluate the validity of various categories and specifiers. The initial suggestions made by the authors were discussed in a series of departmental meetings comprising of the entire professional staff of the department and thus the final draft proposal has received inputs from more than 30 trained professional staff from various disciplines (Psychiatry, Clinical Psychology, and Biochemistry) and another 20 professionals in training.
Each chapter of the draft proposal ha the following structure:
CLASSIFICATION OF PSYCHIATRIC DISORDERS: GENERAL ISSUES
Pratap Sharan, MD, PhD, Shiv Prakash, MD
Recommendations
Supporting evidence for proposed changes
The clinician is focused on treatment and rehabilitation of individuals or groups while the public health expert seeks to employ a broader range of health interventions which include promotion, preventive, curative or rehabilitative strategies aimed at populations and groups at risk. Thus, the clinicians have a relatively greater interest in the current condition of the patient, and diagnostic categories that are narrow and which predict treatment response; while the public mental health expert is relatively more interested in risk/ causative/ developmental factors toward pathology, service delivery to the population, diagnostic categories that vary in breadth (broad for communicating with non-experts and narrow for some specific interventions) and are predictive of response to the entire range of preventive efforts. Public health experts also look at the broader spectrum of health and their determinants (Mezzich 2002a, 2002b).
Classificatory systems have public mental health implications, e.g. concept of diagnosis is crucial to epidemiology and surveillance of population health (Mezzich 2002a). However, since public health is not the explicit focus of the classificatory exercises, many issues that are relevant to public health, have not been addressed. For example, diagnoses like mixed anxiety depression and age-related cognitive decline are disputed because they are below an ‘appropriate’ threshold, but they contribute significantly to disorder burden. Within the spectrum of mental health intervention, prevention and promotion have become realistic and evidence-based alternatives. These bring new challenges to classification system - the challenge of defining boundaries of disorders, risk categories and normality (Mrazek and Hagerty 1994; Mrazek and Hosman 2002).
Public health also has much to contribute to classification. In an effort to move from descriptive criteria based approach to an etiology based approach, epidemiology serves as the bridge between proposed aetiologies or disease mechanisms and potential manifestations (Caine 2003).
Mental health has been conceptualized in two broad ways: ‘positive’ mental health (Jahoda, 1958; Maslow 1968; Tudor 1996) and ‘functional’ metal health (Hosman 1997). The former considers mental health in terms of qualities such as self-confidence, identity, ability to love, happiness, etc. that are seen as worthwhile to promote because they represent a fundamental human values in themselves. The ‘functional model’ considers mental health more in terms of psychological resources and abilities, that people need to have for a satisfying and productive life e.g. in the domains of health, relationships, work, ability to cope with stress, etc.. For this last part, the functional model of mental health coincides with the concept of protective factors.
A growing body of cross-cultural evidence indicates that various psychological, social and behavioural factors such as secure attachment, an optimistic outlook on life with a sense of purpose and direction, effective strategies for coping with challenge, emotionally rewarding social relationships, etc. are protective of health and supportive to positive mental health (Cacioppo et al 2000; Ryff and Singer 2003). Such protection facilitates resistance (resilience) to disease (disorder), minimizes and delays the emergence of disabilities and promotes more rapid recovery from illness (WHO 2002). Good mental health may also be facilitated by religious/ spiritual feelings, experience, orientation and world view (Bhugra and Osbourne, 2004). Thus, it has to be borne in mind that definition of mental health may be at least partially culture-bound with both commonalities and differences between cultures.
The recognition of positive mental health features in psychiatric patients would also substantially reduce the stigma associated with mental illness. A similar reorientation with reference of classification was achieved in the transformation of International Classification of Impairments, Disabilities and Handicaps (WHO 1980) to International Classification of Functioning (WHO 2001b).
In many situations prevention enhances options for managing disorders e.g. it may be possible to prevent many cases of conduct disorders, while it may be fairly difficult to treat them (Reid 1993). Prevention may also be significant for many individuals, who do not have access to treatment or those who receive inappropriate services. A growing number of randomized controlled prevention trials and community trials have offered evidence for significant changes on a wide variety of targeted outcome indicators, including indicators for risk and protective factors, mental and behavioural disorders and improvements in mental health (Mrazek and Haggerty 1994; Clarke et al 1995; Hosman and Llopis 1999).
Risks do not occur in isolation; in fact many risks cannot be disentangled in order to be considered in isolation as they act at different levels which vary over time. Clearly, one outcome can be caused by many risk factors (equifinality – multiple pathways to the same disorder), but similarly one risk factor can lead to many outcomes (multifinality – overlapping pathways to different disorders). Further, there is a non-linear relationship between risk factors and outcomes. Although one or two risk factors may show little prediction to poor outcome, there are rapidly increasing rates of disorders with additional risk factors (Rutter 1979; Greenberg et al 2001). Another point that needs to be borne in mind about risks is that some of the distal risks cannot appropriately be defined at the individual level (e.g. social disintegration).
Addition of an axis for risk and protective factors in the classificatory system could serve as the link between etiological understanding of disorders and promotive, preventive, curative and rehabilitative interventions. Risk factors may help in identifying subtypes that may aid in the exploration of pathophysiology and etiology (Andreasen and Carpenter, 1993). The axis on risk factors could be used as a matrix with Axis I (clinical diagnosis), to eliminate the need for some specifiers. For example, postpartum depression could be labelled as depression on Axis I and the specifier 'postpartum' would appear on the axis for risk factors. This axis could replace the Axis III and IV of DSM IV and Axis III of ICD-10 as it is broader in scope. It will end the artificial mind-body divide in relation to etiological factors. In addition, it will emphasize distal social and developmental causes of disorders which are not emphasized in the present classification systems and can be major foci of public mental health policies.
A substantial volume of literature suggests that subthreshold conditions have considerable public health importance. Subthreshold depressions (e.g. mixed anxiety depression, recurrent brief depression, minor depression, etc.) are reported to occur in up to 24% of the general adult (Horwath et al 1992) and 52% of the elderly (Pincus et al 1999) populations. Further, it is difficult to differentiate subthreshold depression and major depressive disorder on the basis of demographic and clinical characteristics; medical and psychiatric comorbidity; dysfunction (subtheshold depression cause five-times more disability days than major depressive disorders and dysthymia combined); follow up studies; outcome (in terms of chronicity and suicide), and a family vulnerability for major depression (Broadhead et al 1990; Johnson et al 1992; Judd et al 1998).
However, since less than one-fourth of subjects with minor depression develop major depression (Broadhead et al 1990; Wells et al 1992) in most cases subthreshold depression should be considered as an indicator of risk for developing threshold depression - a focus for indicated prevention (a subcategory of primary prevention). Subthreshold depressive categories should therefore be included in the classification under the rubric of prevention relevant categories.
Regier et al (2002) suggest that the diagnostic thresholds in current classificatory systems reflect an emphasis on treatment over prevention. Altering the threshold for caseness will change the latitude for prevention and treatment within the public mental health spectrum. Assignment of boundaries between normal states, high risk states and disorders can be made on the basis of empirical studies of risk (Vasan et al 2002). Definition of prevention relevant categories would encourage studies aimed at understanding their causation (Pincus et al 1999; 2003) and early intervention for those at risk for future morbidity, comorbidity and mortality rather than limiting intervention to after significant morbidity has occurred.
The preoccupation with over-refined categories and subcategories has led to complex diagnostic systems that are difficult to use in the community setting. Moreover, the evergrowing list of types/subtypes contains many conditions that are rarely diagnosed (Bertelsen 2002).
Definition of broad categories would be useful from the promotion and prevention perspective. Over the last 3 decades, the majority of evidence-based promotive and preventive trials have focused on common or generic protective and risk factors, e.g. interventions for increasing self-esteem, emotional resilience, problem-solving and coping skills (Mrazek and Haggerty 1994; Hosman & Llopis, 1999); and prevention of broad categories such as depression (Rutz et al 1992a; 1992b), anxiety symptoms and disorders (Dadds et al 1999), externalising problems and substance abuse (Wolchik et al 2000), or suicidal behavior (Zenere and Lazarus, 1997). When varying clinical presentation have major risk factors in common, subtyping is less relevant from the preventive perspective.
The increase in number of disorders has added to the problems of comorbidity – nearly one-third of cases in the general population have comorbid psychiatric problems (Wittchen 1996). At least some of these would be artefacts, a function of the number of available categories. Data suggest that much comorbidity in the mental health field is due to shared antecedents (genetic and environmental, e.g. childhood adversity) (Kendler et al 1992; Brown et al 1996; Livesley et al 1998; Mineka et al 1998), a fact that goes against the possibility of independence and chance co-occurrence of disorders. Thus, Krueger et al (1998) found support for a 2-factor model for explaining comorbidity – a latent internalizing factor (depression and anxiety) and a latent externalizing factor (conduct disorder, marijuana and alcohol dependence). The lack of independence between diagnoses could explain the absence of diagnostic specificity of treatment response (Regier et al 2002).
The argument for definition of broad categories is not against the existence of narrower categories. When subtypes have major subtype–specific and malleable determinants, fine divisions of categories could be relevant for prevention, treatment and rehabilitation, wherein strategies are targeted to reduction in number of episodes, duration, severity and dysfunction associated with illnesses and secondary morbidity (McGorry 1992). Hence, close attention should be paid to the number, hierarchy and specificity of categories during revision of classifications.
A life-course approach to study of health and illness has come to dominate public health following the recognition of the fact that risks as well as symptomatic expression of disorders vary across developmental spans (Ingram and Price, 2001) and that exposure to disadvantageous experiences and environments accumulate throughout life to increase the risk of illnesses (WHO 2002).
The need for a developmentally informed diagnostic system is most acute for definition of psychopathology in children and adolescents because most of the current diagnostic systems are based solely on models of adult psychopathology. Ryan et al (1987) and Kashani et al (1997) found that children especially pre-schoolers with depressive disorders presented with somatic complaints and aggressive behaviour and most showed psychomotor agitation. The diagnosis may be overlooked because of the presence of these associated symptoms that are suggestive of an externalising disorder. These findings combined with the observation of Kovacs (1986) that younger children may not be capable of experiencing or reporting the symptoms thought to be representative of major depression, emphasize the need to have developmentally relevant criteria for diagnosis.
Other studies have emphasized the need for greater attention to the life course approach to mental disorders. The results of several prospective longitudinal studies of population based samples of children and adolescents show that retrospective adult studies may seriously overestimate the age at onset of many disorders (Costello et al 1999, Lewinsohn et al 2000). In addition, some disorders e.g. ADHD and major psychoses may show early prodromes (Pine et al 2002). An episode of depression or anxiety is a risk factor for further episodes of same general type of disorder, e.g. major depression and suicide (Kovacs and Devlin 1998; Mineka et al 1998), and attention deficit hyperactivity disorders is a predictor of conduct disorder/antisocial personality disorder, substance use disorder and bipolar disorder (Biederman e al 1998; Faraone et al 1998). Some heterotypic associations are also apparent. High levels of anxiety in children predicted increase in depression over time, however high levels of reported depression in children did not predict increase in anxiety (Kolvin and Trowell 2002). Tic disorder shows longitudinal association with obsessive compulsive disorder with tic decreasing and obsessive symptoms increasing over time (Pine et al 2002). Interplay of biological and environmental risk factors could influence courses both singly and across related disorders, e.g. childhood sexual abuse for externalizing disorders (Brown et al 1996) and kindling for schizophrenia, bipolar and other disorders (Frances and Egger, 1999). Failure to take a life course approach makes the occurrence of such comorbidity perplexing.
Current data show that 85% of the variation in DNA sequence is common to ethnic groups. Such observations suggest that the risk of common illnesses including mental illnesses largely derive from alleles shared across all group of humans, supporting the possibility of having universal syndromes. But variations at the genetic level across ethnic groups (15%) and environmental risk factors provide for the possibility of substantial phenotypic variations across cultures and across time spans (Hyman 2002).
ICD 10 and DSM-IV do not adequately consider the possibility that context affects prototypical manifestations of an illness. It would be desirable to develop a system of classification that is flexible for local and cultural adaptations. For example, in some cultures people may not volunteer sadness as a symptom because a conceptually equivalent term may not exist in the language, or because of stigma attached to it, or because it is not recognized as an illness (Patel 2001). In such circumstances it would be better to use local concepts, e.g. 'Kufungisisa' (thinking too much) in Shona language of Zimbabwe or 'Neurasthenia' in China (Kleinman and Kleinman 1985; Patel 2001). Application of a universally defined criteria set in such cultures in an inflexible way, would lead to gross underestimation of prevalence of somatic symptoms related to depression and also of the prevalence of depression in the population studied (Alarcón et al 2002).
Avoidance of the concept of cultural variations in common psychiatric disorders leads to paradoxical situations. ICD-10 emphasizes adverse medical and psychological consequences in dependence and harmful use categories to ease application across different cultures and countries (Rounsaville 2002). However, development of social consequences more often predates physical and psychological problems in the natural history of pathological substance use disorders. As a consequence, rates as well as test-retest reliability of ICD-10 harmful use were lower than that of DSM-IV abuse (Chatterji et al 1997; Rounsaville 2002). On the other hand, acute and transient psychosis, a culturally informed diagnosis has been shown to have some genetic (Das et al 1999), epidemiological and prognostic validity (Susser et al 1996).
A simple system of psychiatric classification that can readily be translated into indigenous categories of illness is highly desirable. Attempts at crosswalks between ICD-10 and indigenous categories can be seen in Chinese Classification for Mental Disorders-3rd Edition (CCMD-3) (Chen 2002), Latin American Guide for Psychiatric Diagnosis (GLDF) (Berganza et al 2002) and Third Cuban Glossary of Psychiatry (GC-3) (Otero-Ojeda 2002).
The relative validity of these categorical and dimensional approaches rests on a number of empirical considerations (Widiger & Samuel, 2005). An especially important issue concerns the nature of the underlying distributions. Taxometric studies suggest that both latent categories and dimensions are widely distributed. Dimensional models receive extensive support in the broad neurotic spectrum, predominating among the mood and anxiety disorders, e.g. chronic worry and posttraumatic stress (Ruscio et al, 2001). Analyses of depression have yielded mixed results but generally have found evidence of continuity rather than discontinuity (Haslam & Beck, 1994; Ruscio & Ruscio, 2002). However, melancholic depression appears to be better understood as a latent category and there are indications of latent categories in the domain of social anxiety and inhibition. Also, categorical models enjoy more support in the domain of personality disorders than might not have been anticipated.
Dimensional systems allow one to model the severity of dysfunction, not simply its presence versus absence (Clark et al, 1995). A large body of evidence also indicates that the artificial dichotomization of continuous measures leads to substantial losses in reliability, stability and validity (Widiger, 1992). Dimensional approach may also help in preparing for the future inclusion of genetic, imaging, and biochemical elements to psychiatric diagnoses.
Multiaxial evaluation provides a vehicle for describing different aspects of a patient’s condition in order to improve our understanding of the condition and thereby to improve its management. Many multiaxial systems have been proposed and there is much variance among them regarding specific axes (Mezzich et al 1987). However, only a limited number of axes can be included in a system that is manageable in regular work internationally. Economizing arrangements could be considered to accommodate information within the multiaxial system, e.g. Mezzich et al (1987) found two broad and pervasive themes in their review of multiaxial systems: phenomenology and etiological/ associated factors. The latter could accommodate sub themes like biological, psychological, cultural, and spiritual aspects. Axes which cannot be accommodated within a given list could be considered as special - for use with particular populations or situations.
Axis I (categorical diagnoses related to health/ illhealth) would comprise of:
Axis II (dimensions related to health/ illhealth) would comprise of consensually agreed upon dimensions. Some dimensions that can be considered are:
The axis could also accomodate endophenotypes, cognitive structures, defence mechanisms, etc. for which consensus can be obtained.
Axis III (risk, protective and contextual factors) would include consensually agreed upon risk/protective, formative, precipitating and perpetuating factors. The axis would be subdivided into the following dimensions:
DSM-IV and ICD-10 were not particularly well suited for use in non-speciality settings. It is noteworthy that in the 'Beyond Blue' Project, an Australian initiative to combat depression, 'depression' and 'anxiety disorders' were the two major categories used in the skill focused training provided to general practitioners and in media advocacy work (Beyond Blue 2001). Neither ICD-10 nor DSM-IV was adopted.
Primary Care: The ICD-10 has two primary care versions - a concise version (containing 25 conditions) for those with medical training and prescription responsibility and a brief version (containing 6 conditions) for other primary care workers with limited medical training (WHO 1996). Similarly, a primary care version exists for the DSM-IV (APA 1996). The problem with ICD-10 PHC versions is that the categories in the two versions do not match each other and the detailed version of the ICD-10; however, they provide a simple way of classifying mental disorders. The DSM-IV primary care version on the other hand maintains its ties with the detailed DSM-IV but it does not simplify the classification per se, focusing instead on simplifying the process of reaching the DSM-IV classification by following a workbook style, wherein symptoms branch out into diagnostic algorithms (Pingitore and Sansone 1998).
The best solution would be to have three versions of increasing complexity, in which the categories of the more complex version are nested in the broader categories of the less complex system.
General Medical Health System: Trimble (2002) has suggested that ICD/DSM should have links to other classificatory systems, e.g. the international classification of epileptic seizures, movement disorders, lobar atrophies, dementia and sleep disorders (ASDA 1990; Mckeith et al 1996; McKhann et al 1984; Neary et al 1998). This could be achieved in many different ways. One could be to reproduce those classificatory systems/diagnostic criteria within the published ICD/DSM volumes. Another could be providing crosswalks between categories in one system with those in the other system. There is also the case for the provision of similar crosswalk to the classification used by nurses, e.g. Contemprory Nursing Diagnosis Manual of North American Nursing Diagnosis Association (NANDA 1994). Guidance is also needed for linking individual diagnosis to the International Classification of Functioning (ICF) as suggested by Kopelman and Fleminger (2002) and Jenkins et al (2002).
Address for Correspondence: Professor Pratap Sharan, Department of Psychiatry, All India Institute of Medical Sciences, Ansari Nagar, New Delhi – 110029, INDIA. Email: pratapsharan[at]gmail[dot]com
Prof. S. K. Khandelwal, MD, MRCPsych, Dr. Kumar R. Maji, MD
Recommendations
1. Changing the name of the F00-F09 category from – ‘organic, including symptomatic, mental disorders’ to ‘neuropsychiatric disorders including symptomatic, mental disorders’.
2. To place tic disorder under F00-F09 from its current place under F95 (F90 - F98: behavioural and emotional disorders with onset usually occurring in childhood and adolescence).
3. To exclude organic dissociative disorder
The essence of classification system is to arrange something in an ordered fashion instead of placing it haphazardly. From ancient to recent times, various efforts have been made to classify mental disorders, with gradual refinement of the concept of mental disorders and their classifications. ICD-10 (International Classification of Disease - 10th edition) and DSM-IV (Diagnostic and Statistical Manual of Mental Disorders - 4th edition) are the two widely accepted classificatory systems for mental disorders, though certain others country specific classificatory systems do exist.
Mental disorders classificatory system is not only used by psychiatrist, it is also used by other physicians, psychologists, social workers, nurses, occupational and rehabilitation therapists, counselors and other health and mental health professionals. Efforts should be made to make the ICD-11 more clinically useful and acceptable to those who apply it, should have few differences with DSM-V and at the same time, it should keep the layout of existing coding system intact.
Great strides have been made over the past few decades in the field of clinical neuroscience, including functional and structural brain imaging, electrophysiology and electro-diagnosis, cellular and molecular biology, genetics and neuropsychopharmacology. Despite these developments in the field of neuroscience, the understanding of the pathophysiology of mental disorders is still in a nascent state. Therefore, the seminal article by Robins and Guze (1970) is still relevant to the process of revision of classification of mental disorders.
This rubric in ICD-10 covers a range of mental disorders with a common theme of demonstrable etiology in cerebral disease, brain injury, or other insult leading to cerebral dysfunction which may be primary (where the causative factors affect the brain directly) or secondary (where systemic diseases involve brain like other multiple organs). The term ‘organic’ used here means that disorders or syndrome in this category can be attributed to an independently diagnosable cerebral or systemic disease or disorder and the term ‘symptomatic’ is used where the cerebral involvement is secondary to systemic illness (ICD-10, Clinical Descriptions and Diagnostic Guidelines).
The use of the term ‘organcity’ in psychiatric classification is attended with controversy. DSM-II (1968), categorized organic mental disorders as organic brain syndrome (OBS), caused by diffuse brain dysfunction that lead to deficits in orientation and intellectual functioning (e.g. memory, judgement, comprehension) and to changes in affective modulation (lability or shallowness). Subsequently, OBS was replaced by the term organic mental disorders (OMD) in DSM-III (1980), which further made a fundamental distinction between OBS and OMD with reference to absence or presence of etiological factors. In DSM-III-R (1987), all these disorder were placed under the section of ‘Organic Mental Syndromes and Disorders’ which was eventually deleted in the DSM-IV (1994).
In ICD-8 (1969) all organic psychotic conditions were placed along with functional psychoses under the rubric of ‘psychosis’ (290-299). Code 290 to 294 in ICD-8 (290: senile and pre-senile dementia, 291: alcoholic psychosis, 292: psychosis associated with intracranial infection, 293: psychosis associated with other cerebral condition, 294: psychosis associated with other physical condition) underwent mild modifications and were included in ICD-9 under a new term: ‘organic psychotic conditions (290-294). The latest revision ICD-10 (1992) retained the term ‘organic’ for this group of disorders.
Discussion
The term organic is very difficult to define and moreover, it incorrectly implies non-biological basis for non-organic (functional) psychiatric illnesses. In addition, merely placing ‘organic’ in front of a variety of symptom or syndromes (hallucinosis, catatonic disorder, delusional disorder, mood disorder, anxiety disorder, dissociative disorder, emotionally labile disorder), does not advance classification keeping in view the future development in neurosciences (Kopelman et al 2002). The term ‘neuropsychiatric disorder’ is probably the appropriate substitute for organic mental disorder, owing to its broad spectrum coverage. For example, head-injury, within neuropsychiatric disorders, would include (besides dementia due to head trauma and post-concussional syndrome) confusional states, memory disorders, executive and personality changes, head-injury related mood changes, etc. Epilepsy is another disorder where a number of specific neuropsychiatric syndromes could be incorporated.
Code F06 in ICD-10, uses the term ‘other mental disorders due to brain damage and dysfunction and to physical disease,’ while DSM-IV uses the term ‘mental disorders due to general medical condition.’ In the ICD-10 code, the word ‘organic’ has been placed before psychiatric disorders which often manifest in certain medical conditions. More clarity and specificity is required in describing these conditions or subtypes to avoid confusion among other health professionals who often witness such conditions, which is probably not possible by mere presence of the term ‘organic’ before such entity. Example of more appropriate description would be – catatonic disorder in Vit-B12 deficiency, delusional (schizophrenia – like) disorder in epilepsy etc. (Kopelman et al 2002). However, this type of description is reminiscent of ‘combination categories’ of ICD-8. Therefore, more accurate and appropriate description of these conditions requires utilization of separate independent axes.
Tic disorders comprise a group of disorders, such as, transient tic disorder, chronic motor or vocal tic disorder, combined vocal and multiple motor tic disorder (de la Tourette’s syndrome), other tic disorder and tic disorder unspecified. Currently, ‘tic disorder’ has been placed in the category of ‘behavioural and emotional disorders with onset usually occurring in childhood and adolescence’ (F90-F98; F95) of ICD-10. Tic disorder has also found a place under G-25 [diseases of nervous system, other extrapyramidal and movement disorders] of ICD-10, as an inclusion term. Though the onset predominantly occurs during childhood and adolescence, onset has been reported in adult age group also (Burd et al, 1986a, b).
Discussion
Tic disorders have a substantial genetic basis; with first degree relatives having up to ten fold increased risk (Tourette Syndrome Association International Consortium for Genetics 1999). It also has high concordance rate in monozygotic twin (53%) in comparison to dizygotic twins (8%) (Leckman et al 1995b). Compelling indirect evidence from pharmacological studies indicates involvement of basal ganglia (Leckman et al 1995b). Electrical stimulation of the amygdala produces motor and vocal responses resembling tics (Jadresic 1992). Though the definite pathophysiology of tic disorders is not known but internationally a research consensus has been reached which suggest that the basal ganglia and the related thalamo-cortical circuitry is involved.
We proposes that tic disorder should be placed under ‘Neuropsychiatric disorder’ currently ‘F00-F09’, instead of its placement under ‘F90-F98’ as in ICD-10. Further information about the onset of illness could well be coded using a fifth character code.
The term ‘dissociative’ has replaced the older term ‘hysteria’ in current ICD-10. The basic theme in dissociative disorder is disruption (partial or complete) in the usually integrated function of consciousness, memory, identity, perception and motor control, in the absence of any physical disorder that might explain the symptoms. The evidence for psychological causation has been presumed in the form of clear or unclear (if patient denies) stressful events or problems or disturbed relationship with onset. ICD-10 has given preference of plausible mechanism for causation by using the term ‘dissociation’ instead of older term ‘psychogenic’ for this condition to avoid etiological assumptions.
‘Organic dissociative disorder’ has been placed in category of F06 (other mental disorders due to brain damage and dysfunction and to physical disease) of current ICD-10 whereas in DSM–IV, no such entity exists.
Discussion
The term ‘organic dissociative disorder’ is paradoxical. The mere presence of organic lesion somewhere in the brain of an individual, which is unrelated with dissociative symptoms can’t make him/her a patient with organic dissociative disorder. If the lesion is related with the symptoms then the diagnosis cannot remain dissociative, and in that situation diagnoses like organic amnestic syndrome would be a more appropriate as per the current ICD-10 classificatory system. Moreover, there is dearth of literature on this issue, raising questions about its diagnostic validity.
We propose that such a paradoxical term should be excluded from ICD-11.
As per the coding conventions of ICD-10, each of the categories has a code composed of four characters. The first character is a letter which designates the chapter – a group of diseases of particular specificity. The second character – a digit describes a subgroup of disorders, e.g. organic, including symptomatic, mental disorder. The third character, also a digit, describes the disease or disorder and the fourth character – a digit, details the condition more elaborately e.g. describing its course and other characteristics. A further fifth, sixth and seventh character could be used as a specifier to have more accurate descriptions.
The ICD-10 chapter F categorizes dementia utilizing four different codes (F00 -dementia in Alzheimer’s disease, F01 - vascular dementia, F02 – dementia in other diseases classified elsewhere, F03 - unspecified dementia), whereas DSM-IV places different types of etiologically based dementias under a single section (dementia), because dementias share common symptoms and presentation.
Discussion
Placement of dementia in ICD-10, utilizing four different codes invites criticism regarding the diagnostic validity and reliability of each code for dementia. Dementia, characterized by the development of multiple cognitive deficits (including memory impairment) that are due to the multiple etiologies (e.g. Alzheimer’s disease, cerebrovascular disease or combination of both), or due to direct physiological effects of general medical conditions or to the persisting effects of substance, is a clinical diagnosis (Boise et al 1999). Having four different codes for dementia in ICD-10 is anomalous with respect to the basic coding convention of ICD-10, as all of these apparently separate disorders have common symptomatology. Placing dementia as a single code (as is the case with DSM-IV) would likely improve its diagnostic stability and probably would improve its applicability and usefulness in clinical practice and research.
Therefore, we propose that dementia should have a single code with further sub typing, based on probable etiological factor (fourth character). Further specification could be achieved with fifth and sixth characters. An example is given below:
F - Mental health chapter
0 - Neuropsychiatric disorder
0 - Dementia
0 - Alzheimer’s disease
0 - Early onset
However, some members of the Department suggested caution with this recommendation based on the argument that classification was not only meant to code disorders but also to assist in research related to aetiology, outcome and prognosis; and also that such a change would require shifting of conditions from their current places, e.g. alcohol and other substance induced dementia.
In clinical practice of psychiatry, we often notice psychotropic induced psychiatric conditions which would require urgent attention and proper management, e.g. lithium toxicity, valproate toxicity, neuroleptic malignant syndrome (NMS), acute dystonia, tardive dyskinesia, serotonin syndrome etc.
Currently these conditions are placed in ICD-10 either in the chapter of nervous system disease [G21 (secondary Parkinsonism), G24 (dystonia), G25 (other extrapyramidal and movement disorder)] or in the chapter of Y40-Y59 (Drugs, medicaments and biological substances causing adverse effects in therapeutic use).
DSM-IV placed these conditions under the rubric of ‘other conditions that may be a focus of clinical attention’.
Discussion
In the coming years, more developments are expected in the field of neuropsycho-pharmacology with newer pharmacological molecules to treat psychiatric disorder. In clinical psychiatric practice, medication induced problems are very common and some of the conditions have poor prognosis which often require clinical attention. Proper management of these conditions would require an understanding and adequate knowledge about these conditions. These conditions fulfil features of ‘organicity’ with temporal association, clear and consistent clinical descriptions, possible explainable pathophysiology and good diagnostic reliability and validity; hence, they deserve a place in F00-F09.
The house, however, felt that their placement within codes for physical disorders was adequate if they did not cause specific mental syndromes.
The characteristic feature of this disorder is a decline in cognitive performance (memory, learning, or concentration) to an extent that is insufficient to make a diagnosis of dementia, delirium or organic amnestic disorder. However, the objective tests indicate deficits and the individual experiences distress or difficulty in carrying out usual activities. The disorder has been placed under the code F06 (other mental disorder due to brain damage and dysfunction and to physical disease). DSM-IV does not have such a diagnostic entity. However, DSM-IV includes mild neurocognitive disorder in the category of cognitive disorder not otherwise specified.
Discussion
The ICD-10 (Clinical Descriptions and Diagnostic Guidelines) mentions that the boundaries of this category (mild cognitive disorder) are still to be firmly confirmed. Mild cognitive disorder as a diagnostic entity fails to differentiate between age related cognitive change, old age specific cognitive problems, and the presence of psychopathology (depression, anxiety) with genuine mild cognitive deficiency. Various outcome studies have failed to demonstrate its diagnostic stability or utility as a predictor of dementia (Christensen et al. 1995, Christensen et al. 1997, Schroder et al. 1998, Ritchie et al. 2001, Larrieu et al. 2002, Kumar et al. 2005). Therefore, it was proposed that this entity should not be included as a separate category in ICD-11. If included, it should be kept in the unspecified category of mental disorders.
However, the house wished to retain this category because it was felt that it is a common condition and more studies are required before it is excluded.
Address for Correspondence: Dr. S. K. Khandelwal, Professor, Department of Psychiatry and National Drug Dependence Treatment Centre, All India Institute of Medical Sciences, New Delhi-110029, India. Fax: +91 11 26588663. E-mail:
ICD-11: DRAFT PROPOSAL FOR CHANGES IN THE ‘MENTAL AND EHAVIOURAL DISORDERS DUE TO PSYCHOACTIVE SUBSTANCE USE’ SECTION
Tripathi BM, MD, MRCPsy; Jhanjee S, MD, DNB; Kattimani S, MD
Suggestion: removal from diagnostic system
Currently, this diagnosis is applicable to alcohol use only and the clinical utility and diagnostic validity of this category has not been established. Hence, this category needs to be removed from the classificatory system.
Caffeine is a commonly used psychoactive substance and its use is socially sanctioned across cultures. Current categorization of caffeine with stimulants suggests that caffeine is a drug of potentially abuse. This has treatment and policy implications, hence, caffeine should be removed from this category. However, since coding inappropriate use of caffeine has some clinical utility, it may be coded in the Z category.
Suggestion: Replacement of the term ‘harmful use’ by the term ‘misuse’ and proposal for new diagnostic criteria.
Proposed diagnostic criteria for ‘misuse of psychoactive substance’ are as under:
This diagnosis requires that at least one of the criteria mentioned below is met, but the criteria for dependence syndrome are not fulfilled.
Suggestion: The current subcategories, F1x.21, F1x.22, and F1x.23 should be subsumed under a single subcategory named ‘F1x.21 supported abstinence’.
In order to simplify and make room for growing evidence in favour of non-pharmacological interventions in maintaining abstinence, the currently existing subcategories like F1x.21-currently abstinent but in a protected environment, F1x.22-currently abstinent on a clinically supervised maintenance or replacement regime and F1x.23- currently abstinent but receiving treatment with aversive or blocking drugs, should be subsumed under a single subcategory of ‘supported abstinence’.
In view of their clinical utility these two subcategories should be incorporated in the classificatory system.
Suggestion: Injecting drug use should be included in the classification either as a specifier or in the Z Category.
In view of clinical and public health implications of using drugs via parenteral route, this needs to be documented either as a specifier in this chapter or needs to be placed under the Z category.
Supporting evidence for proposed changes
I. F1x.07-Pathological intoxication
There is no Indian or International literature supporting the clinical utility and validity of this diagnostic category. The inter-rater reliability of this condition is poor and other factors may be responsible for such a presentation, e.g. personality traits, metabolic changes and the social context under which alcohol is consumed. An example of the pragmatic difficulties associated with its use is the forensic situation, where it may be difficult to defend the diagnosis due to lack of scientific evidence, and lack of expert consensus (Winckler 1999). Hence, it would be better to remove from this category from the classificatory system.
II. F15-Mental and behavioral disorders due to use of other stimulants, including caffeine
Caffeine has been placed in F15 along with other stimulants. The ‘other stimulants’ are psychoactive substances with known abuse liability and potential to produce dependence. Current categorization suggests that caffeine is a potentially abusive drug. This implies that a large population consuming caffeine has a psychiatric problem (with potential for stigmatization) and is in need of treatment intervention. Placing it along with other stimulants in this category does not do justice to such a widely used substance. Hence, caffeine should be removed from this category. Since, the presence of this category may still retain some clinical utility as a condition meriting health attention in specific situations, inappropriate use of caffeine may be coded in the Z category.
III. F1x.1 Harmful use: Change in title and criteria for diagnosis
Current diagnostic criteria for ‘harmful use of psychoactive substance’ require that actual damage should have been caused to the mental or physical health of the user. The diagnosis is arrived at by assessment of retrospective damage done to the subject and it does not consider the potential harm by use of the psychoactive substance in the future. This makes the diagnosis ‘harmful use’ very restrictive, as it cannot be applied to many individuals who may benefit from clinical intervention. Further, many studies have documented poor inter-rater reliability for this diagnostic category (Pull et al, 1997) and the concordance between ‘abuse’ in DSM-IV and ‘harmful use’ in ICD-10 is low (Hasin 2003). To obviate these shortcomings a change in current diagnostic criteria are proposed, as above.
The term ‘harmful use’ may be replaced by the term ‘misuse of psychoactive substance.’ Other terms like ‘abuse’ of psychoactive substance was not considered because of the derogatory connotation attached with the word while the term ‘hazardous use of psychoactive substance’ may highlight the dangerousness involved in the substance use, which may not be universal for all psychoactive substances. The term ‘dysfunctional use’ was considered but the house felt that ‘misuse’ had greater acceptability in current scientific discourse.
IV. Consolidation of subcategories F1x.21, F1x.22, F1x.23 under a single subcategory named ‘F1x.21 supported abstinence’
The current subcategories, F1x.21, F1x.22, and F1x.23 are:
These subcategories can be brought together under a single subcategory F1x.21- ‘supported abstinence’, to make the coding system more uniform and simple, in light of the fact that abstinence states may be supported by methods other than those mentioned in the existing subcategories such as by involvement in self-help groups like Alcoholic Anonymous(AA), cognitive behavior therapy and other non-pharmacological interventions.
V. Creation of new subcategories F1x.8x Sleep disorders due to psychoactive substance use’ and F1x.8x Sexual dysfunction due to psychoactive substance use
Patients using psychoactive substance commonly report sleep disorders and sexual dysfunction. These conditions act as risk factors for relapse if they are not addressed properly. Kumar and Muthulagan (2004) have documented the presence of sleep disorders in patients abstaining from alcohol and many studies have reported that sexual dysfunctions are common in various disorders related to psychoactive substance use (Kumar et al, 1997; Gupta and Jiloha 1998; Singh 1998).
VI. Inclusion of specifier or new subcategory: injectible drug use (IDU)
In addition to the obvious health risks associated with injection drug use, experts opine that this form of drug use gives rise to a severe form of dependence. Results from the National Household Survey, India (NHS, India), show that 0.1% of the sample reported ‘ever’ -injecting drug use (Ray 2004). Common reasons for shifting to injecting route cited by the sample were - better high, and peer pressure due to association with other IDU users. About 97% reported having shared syringes and 74.2% reported having shared needles (Ray, 2004). Needle sharing and unsafe sexual practices as part of drug use subculture can lead to HIV infection and AIDS in this population of drug users. The rate of HIV seroconversion seems to be significantly more rapid in India than that observed in Western countries (Agarwal et al, 1998; Birla Singh and Sharma 1998). Due to the obvious public health and clinical implications of injection drug use, it merits an inclusion as a specifier in the psychoactive substance use section or a placement in the Z category.
VII. Creation of a new category: Mental and behavioral disorders due to psychoactive substance use of mixed properties
Current classificatory systems categorize psychoactive substances based on their psychoactive properties, viz. hallucinogens, sedatives or stimulants while at the same time some psychoactive substances have been placed under the their respective generic drug classes like opioids, cannabinoids, nicotine, cocaine, etc. There should be uniformity in categorizing psychoactive substances either based on the class of substances they belong to or based on their main psychoactive property. There are psychoactive substances having both stimulant and hallucinogenic properties like MDMA. There may be difficulty in categorizing such substances, and to overcome this, a suggestion to introduce a separate category named ‘mental and behavioral disorders due to psychoactive substance use of mixed properties’ was made. This did not find consensus in the group discussion and hence was dropped from the final proposal.
VIII. To include psychoactive substances like antidepressants and antihistamines with known abuse and dependence producing capability under the category of substance use disorders
There was a suggestion to include other psychoactive substances with proven dependence and withdrawal producing capability like
antidepressants, monoamine oxidase inhibitors (Ananath et al, 1995) and antihistamines (Pal et al, 2005), under the ‘mental and behavioural disorders due to psychoactive substance use’ category, moving them from the existing category of F55.0 (abuse of non-dependence producing substances) in ICD-10. The house felt that in the absence of strong evidence, it would be inappropriate to consider these drugs as psychoactive substances with abuse liability. Hence the suggestion was dropped from the final draft.
IX. To change the title from ‘Psychoactive substance induced psychotic disorders’ to ‘Behavioral and psychological manifestations due to psychoactive substance use’ for better representation of wide array of specific behavioral and psychiatric manifestations due to psychoactive substance use
Subcategories under ‘Psychoactive substance induced psychotic disorders’ may be changed to include a broad array of behavioral and psychological symptoms and syndromes like depressive disorder, panic attacks, obsessive-compulsive disorder, agoraphobia etc. Hence it was proposed to change psychotic disorders to ‘Psychiatric and behavioral changes due to psychoactive substance use’ or ‘Behavioral and psychological manifestations due to psychoactive substance use’. Since any change in the title was likely to replicate the main title ‘Mental and behavioral disorders due to psychoactive substance use’ of this chapter, this suggestion was withheld.
X. Creation of separate category of ‘cannabis induced psychosis’
Cannabis induced psychosis has been extensively described in Indian literature. It was argued that cannabis induced psychosis be considered as a separate independent category under F12.5. It differs from other psychiatric disorders in terms of psychopathology that consists of both psychotic (paranoid delusions) and affective symptoms, and is characterized by rapid changes in symptomatology. Such a presentation cannot be easily categorized into either affective or psychotic disorder (Sarkar et al, 2003; Mallik et al, 2004) and has course and treatment implications. A specific rubric will also draw increased research attention to this condition. The house felt that sufficient literature had not yet accrued to support a separate category of cannabis induced psychosis, so this suggestion was dropped from the final draft.
XI. Sub typing alcohol use disorders
A descriptive study showed that patients with primary alcoholism differ from patients with secondary alcoholism on severity of dependence, presence of interpersonal problems, in their compliance to treatment and in maintaining abstinence in the follow-up period (Ramesh et al, 1996).Some authors have tried to study drinking pattern using multivariate techniques. Based on factor analysis of their data, one group of authors proposed that alcohol use was of 3 types - alcohol abuse, alcohol dependence and social drinking (Mathrubootham et al, 1997). Alcohol dependence could be further classified into low and moderate dependence.Such studies support the exclusion of social drinking from diagnostic categorization, and can help in reduction of false positives for alcohol abuse or dependence. However some authors have used the term ‘problems drinkers’ to identify those who do not fulfilling criteria for alcohol dependence but still require some form of intervention for their alcohol use (Satesh and Sengupta 1997). The house agreed with the onclusions reached by Gupta and Basu (1999) that alcohol subtyping would merit further study before inclusion in the classificatory system.
XII. Sub typing of opioid dependence into early onset and late onset opioid dependence
Some authors have suggested the differentiation between opioid dependence of early onset defined as age less than 20 years at the initiation of opioids and late onset defined as age more than 20 years at the initiation of opioids. There appears to be significant difference between the two groups regarding substance use pattern and presence of psychopathology, which might need to be considered in treatment planning (De et al, 1998).However, the house felt that the evidence for the use of this specifier was not compelling as yet.
XIII. Inclusion of protracted withdrawal as specifier
There was suggestion to consider ‘protracted withdrawal state’ as a specifier besides the existing F1x.3 withdrawal state, which is an acute physiological state due to sudden cessation or decrease in the quantity of psychoactive substance on which an individual is dependent. It has been well established that protracted withdrawal is one of the risk factor for relapse in cases of psychoactive substance use disorders (Satel et al, 1993).However, the house felt that there was not enough evidence to support the separation of acute and protracted withdrawal states.
Concluding comments:
ICD revision process should also consider the identification of risk factors for relapse and factors that alter prognosis and intervention strategies. The multiaxial system similar to that suggested by WPA workgroup in 1994 may be used with some alteration (Kastrup 2002). It needs to be established whether diagnostic criteria needs to be changed in order to make its applicable in special populations like women (Selvaraj et al, 1997; Prasad et al, 2000; Irpati et al, 2005), elderly (Grover et al, 2005), and adolescents (Tripathi and Lal 1999). While revising existing classification, available research evidence should be considered carefully, and proposed changes should be evaluated for their utility in treatment decisions and in prognostication, for forensic purposes, for potential benefits to special groups like children. Also, issues related to third parties like reimbursement providers, public opinion and implication for government policies should be carefully considered during the revision process.
References:
Address for Correspondence:Dr. B. M. Tripathi, Professor, Department of Psychiatry and National Drug Dependence Treatment Centre, All India Institute of Medical Sciences, New Delhi-110029, India. Fax: +91 11 26588663. E-mail: bmt_54[at]yahoo[dot]com
Rakesh Lal, MD, Mamta Sood, MD, DPM, Amardeep Kumar, MD
Recommendations
Schizophrenia (F 20)
Thus, we propose the draft for this section should read as follows:
F 20.x.a.b.c.d
Type of schizophrenia – x
Course – a
Age at onset – b
Catatonic symptoms – c
Depressive symptoms - d
Delusional disorders (F22)
Acute and transient psychotic disorders (F23)
x – subtype
a – course which may be: 0 - single episode, 1- recurrent, current episode
Schizoaffective disorders (F25)
x – subtype
a – course which may be: 0 - concurrent, 1- sequential
Supportive Evidence for Proposed Changes
Introduction
Schizophrenia, schizotypal and delusional disorders (F20-F29) section in ICD10 include non-affective psychiatric disorders conceptualized to be broadly related to each other. The classification of these disorders in ICD-10 has achieved fairly good reliability, ensuring the international comparability of research, clinical work and education. While, these categories have not achieved expected nosological validity based on criteria given by Robin and Guze (1970), the past decade has witnessed research into specific areas that has elucidated and questioned many already existing issues and has thrown up several new issues for consideration.
F20: Schizophrenia
I. Higher weight should be given to negative symptoms of schizophrenia
There is an emphasis on positive symptoms for diagnosing schizophrenia in ICD10. Presence of only one SFRS is enough to make the diagnosis whereas two of the negative, catatonic, formal thought disorder or persistent hallucinations with accompanying delusions/overvalued ideas are required to make the diagnosis of schizophrenia. Inclusion of Schneider’s first rank symptoms (SFRS)/positive symptoms in the diagnostic guidelines has increased reliability of diagnosis of schizophrenia in ICD10. However, it is now well established that SFRS are present in other psychiatric conditions as well (Taylor et al, 1973; Brockington et al, 1980). Also, current research recognizes that negative symptoms are defining features of schizophrenia.
Negative symptoms have been reported frequently in patients with schizophrenia.
Patients of schizophrenia with affected relatives are reportedto have a high magnitude of negative symptoms that are relativelytreatment resistant. Twin studies and other data show that relativesof probands with greater negative symptoms have higher morbid risks for illness than the relatives of probands who have greaterpositive symptoms. Negative symptoms are also presentin some nonschizophrenic relatives of patients with schizophrenia,as in those with schizotypal personality disorders (Malaspina et al, 2000).
Typical antipsychotics cause relatively more improvement in positive symptoms as compared to negative symptoms. Moreover, typical antipsychotics cause extra pyramidal side effects which may mimic some of the negative symptoms. Atypical antipsychotics have been proven in placebo-controlled trials to be effective in treating negative symptoms of acute schizophrenic episodes (Moller et al, 2003). Negative symptoms are widely suspected to reflect frontal lobe dysfunction and are associated with poor outcome (Potkin et al, 2002).
Discussion: The literature suggests that negative symptoms are increasingly recognized as defining features of schizophrenia but it is not clear how they can be used in differentiating schizophrenia from other conditions. Some studies report that negative feature like apathy may be useful in this regard. Studies are needed to identify pattern and type of primary negative symptoms in schizophrenia. Increasing the weight age of negative symptoms in making diagnosis of schizophrenia can be achieved by adding another criteria that records negative symptoms not currently included under (h) like avolition, loss of drive, aimless behaviour, empty speech.
II. Addition of early onset (onset before 18 years of age) as age of onset specifier
Awareness about early onset schizophrenia is increasing. Premorbid developmental impairments, including language, motor and social deficits; insidious onset in at least 75% of children; elementary auditory hallucinations; less complex delusions related to childhood themes; and negative symptoms namely flat or inappropriate affect; are more frequent and pronounced in earlier, than in later-onset schizophrenia.. A marked deterioration from the previous level of functioning is also present in these children, and an impaired outcome is reported in approximately 50-60% of cases.
The frequency of childhood schizophrenia is less than 1 in 10,000 children, but there is a remarkable increase in frequency between 13 and 18 years of age (Remschmidt et al, 2005).
There is strong evidence for the importance of genetic factors in schizophrenia in children and adolescents (Remschmidt et al, 2005).
Early onset schizophrenia has greater neuropsychological deficits than adult onset schizophrenia (Biswas et al, 2006; White et al, 2006). Early onset schizophrenia is also more severe and is frequently treatment-resistant (Shaw et al, 2006). The long-term course of childhood- and adolescent-onset schizophrenia is worse than in adult-onset schizophrenia, and the patients with manifestation of the disorder below the age of 14 have a very poor prognosis (Remschmidt et al, 2005).
Discussion: Early onset schizophrenia (onset before 18 years) has good internal and external validity. Thus, the group proposed its (age of onset) inclusion as a specifier ‘b’.
III. Pattern of course needs to be simplified
The review of literature did not support the complex pattern included under the current course specifier in ICD-10. It is tedious for use in clinical practice as well as research, hence it is rarely used. Provision of a simpler pattern of course specifier would increase its clinical utility without compromising on its validity. The group proposed the following pattern for course specifier:
IV. Removal of catatonic schizophrenia F20.2 as a subgroup of schizophrenia and placing it as clinical course specifier of schizophrenia
Kraepelin recognized catatonia as a form of dementia praecox and Bleuler included it within his wide group of schizophrenias. Catatonia as a subtype of schizophrenia has been included in all classificatory systems. Recent research shows that catatonia is a syndrome which is characterized by association with neurological and general medical conditions, mood disorders; use of effective therapeutics and development of reliable instruments.
Catatonic presentations are common in acute in-patient psychiatric settings (Banerjee et al, 1995; Chalasani et al, 2005). The prevalence of catatonia among psychiatricpatients is reported to range from 7.6% to 38 % (Taylor et al, 2003).
Catatonic presentation is more common in mood disorder than in schizophrenia. It is also found in many other conditions (Taylor et al, 2003).
Catatonia responds to specific treatments like lorazepam and ECT irrespective of the disorder (Taylor et al 2003).
Discussion: Customary clinical practice continues to overvalue the idea that presence of catatonia is diagnostic of schizophrenia. The reliability of catatonic features is good; however the internal and external validity of catatonic schizophrenia is questionable. This type of presentation appears in the course of schizophrenia at various stages with limited stability. Further, it is recommended that at the time of presentation, if catatonic features are present, these are treated symptomatically with lorazepam or ECT; final management, course and prognosis are decided by the underlying condition that is uncovered after patient recovers from catatonia. So, catatonia can be conceptualized mainly as a clinical specifier. Thus, the group proposes its placement as a clinical course specifier ‘c’.
V. Removal of post-schizophrenic depression as a subtype; depressive symptoms to be included as a phase specifier.
Depression occurs frequently in schizophrenia. Occurrence of depression in schizophrenia has often been associated with worse outcome , impaired functioning, personal suffering , higher rates of relapse or rehospitalization and suicide. In ICD 10, depressive features are included under schizophrenia as ‘mild degree of depression’ preceding psychotic symptoms and as ‘post psychotic depression subtype’. In the former situation, it is a symptom and in the latter situation, a syndrome. A depressive episode present concurrently with schizophrenia is diagnosed as a schizoaffective disorder. The confusion attending the term depression in schizophrenia is attributable to three questions viz., whether it is the symptom or syndrome of depression that is being considered; the phase of schizophrenia in which it is occurring; and its causation (whether it is integral part of schizophrenic process, a de-novo phenomenon or a reaction to stress).
Depressive symptoms in schizophrenia are often severe but are poorly recognized by psychiatrists (Bressan et al, 2003). The prevalence varies from 7%-75% according to the approach used for their identification (Micallef et al, 2006). Depressive symptoms of substantial severity are often found in 50% of newly diagnosed cases of schizophrenia and 33% of cases of chronic schizophrenia that have relapsed (Whitehead et al, 2002).
A Cochrane systematic data review found no convincing evidence to support or refute the use of antidepressants in treating depression in people with schizophrenia (Whitehead et al, 2002). However, a study done by Birchwood et al (2000) found that depression accompanying acute psychotic phase remits with psychosis.
Discussion: Post-schizophrenic depression as a subtype of schizophrenia has questionable reliability and validity. Depression in schizophrenia is common and it occurs during prodrome, active psychotic phase, within first year and thereafter. The efficacy of antidepressants is equivocal. The boundary problem exists with schizoaffective disorder (depressive type) and depressive episode (F32.-). Thus, the group proposes removal of post-schizophrenic depression as a subtype; depressive symptoms should be included as a course specifier‘d’. Depressive symptoms fulfilling diagnostic criteria for depressive episode (F32.-) occurring could be diagnosed independently as a co morbid condition.
VI. Dimensions of schizophrenia to be introduced
Over the last decade many studies have highlighted the dimensions of schizophrenia. In eighties, the negative–positive distinction was extensively studied. Van der Does et al (1995) investigated the stability of an earlier reported four-dimensional symptom model (positive symptoms, negative symptoms, disorganization, and depression) and found a stable four-dimensional structure that closely resembled the factor structure of their first assessment. The symptom dimensions were uncorrelated, except for disorganization and depression. The results of a cluster analysis suggest the existence of at least four subtypes of schizophrenia: positive, negative, mixed, and disorganized. A fifth subtype included patients with few symptoms and suggested the occurrence of simple schizophrenia (Dollfus et al, 1996; Lykouras et al, 2001). Klingberg et al (2006) reported the occurrence of five factors viz., negative, impulsive, positive, disorganization, and depression.
Discussion: While the search of literature suggests the occurrence of many dimensions underlying schizophrenia, the evidence for reliability and validity of different dimensions is variable. Issues pertaining to dimensional classification will be covered under the general section.
VII. Introduction of schizo-obsessive subtype of schizophrenia under ‘Conditions meriting further study’
Co-occurrence of obsessive compulsive (OC) symptoms and psychotic illness was first recognized over a century ago. Interest in this area has been revived recently because of increased recognition of higher-than-expected co morbidity rates. There is growing evidence that patients with schizophrenia and obsessive compulsive disorder, termed schizo-obsessive may represent a special category of schizophrenia population.
Recent studies have revealed much higher co-morbidity rates for OCD in the schizophrenia than previously recognized. Investigators have reported prevalence rates of clinically significant OC symptoms in schizophrenia population to be 10%-52% and of OCD in schizophrenia population to be 7.8%-26% (Berman et al, 1995; Kruger et al, 2000; Tibbo et al, 2000; Craig et al, 2002; Thomas et al 2005). Comparisons of current co-morbidity figures with individual lifetime prevalence rates for each disorder (2%-3% for OCD and 1% for schizophrenia) suggests that there exists greater than chance rate of co-occurrence between the two conditions (Bottas et al, 2005).
Schizophrenia with OC symptoms possess a distinct clinical and neuropsychological profile that differs from that of schizophrenia without OC symptoms. This profile includes a worse clinical course with poor treatment response, lower functioning levels, and greater impairment of functions primarily subserved by the frontal lobes. In addition, the former patients showed a higher level of negative symptoms and worse overall psychopathology (Hwang, 2000).
There is significant overlap in the proposed circuits of OCD and schizophrenia, which may lead to co-expression of symptoms. Although there is overlap in neurotransmitter dysfunction, the interactions are complex, especially in regard to the serotonin and dopamine systems (Tibbo et al 1999, Gross-Isseroff et al 2003).
Discussion: at present the epidemiological and biological evidence suggests that schizo-obsessive disorder as a subtype of schizophrenia deserves attention as it may be sufficiently distinct in terms of aetiology, treatment and outcome. The group proposes that schizo-obsessive subtype of schizophrenia should be introduced as a conditions meriting further study.
F22: Persistent delusional disorder
VIII. Deletion of the term ‘persistent’
ICD-10 mentions the word ‘persistent’ to mean that these disorders are ‘usually persistent and sometimes lifelong’. The global outcome of delusional disorders is shown to be better than that for schizophrenia. Kendler and Walsh (1995) reported the duration of illness for delusional disorders (38±26 months) to be shorter than that for schizophrenia (159±134 months). It is argued that to bring this category closer to that of DSM-IV the term ‘persistent’ should be dropped.
IX. Shifting of F24 (induced delusional disorder) under F22
The underlying assumption behind placing F24 as a separate diagnostic category in ICD-10 appears to be presence of a definite cause and spontaneous resolution of symptoms after removal of the cause. Literature review suggests that this category has not been adequately validated. The occurrence of its four subtypes viz., folie imposee, folie simultanee, folie communiqué and folie induite is largely based on the resistance offered and time of appearance of psychotic symptoms in the secondary cases. Except for folie imposee, these disorders in secondary cases do not have a clear onset and offset with the primary case (Wehmeier et al, 2003). Management of these patients requires multiple treatments including removal of etiologic agent, antipsychotics, individual and group psychotherapy, and family therapy (Kumar et al, 2005). As these conditions are phenomenologically similar to cases with delusional disorders, the group proposes that this category can be shifted under F22 as F22.1 for better understanding of etiology and long term course and outcome.
F23: Acute and transient psychotic disorders
X. Introduction of course specifier for acute and transient psychotic disorders
Acute and transient psychotic disorders get re-diagnosed as other non-organic psychotic disorder if they recur. Studies have suggested that these cases recur and recurrent acute remitting psychotic states are 10 times more common in developing than in industrialized countries; are two times more common in females than males; exhibit long term benign course and have lesser negative symptoms (Susser et al,1995; Sajith et al, 2002). Better delineation of non-affective acute remitting psychosis in current diagnostic systems could lead to better understanding of this condition and improve the applicability of diagnostic systems in developing countries, where these conditions are more common than in industrialized countries. To better understand the course and outcome of acute and transient psychotic disorders, the group proposed the introduction of a course specifier for this group of disorders. A fifth character may be used to classify the course e.g. F23.x.a
x – subtype
a – course which may be 0 - single episode, and 1 - recurrent, current episode
F25: Schizoaffective disorders
XI. Introduction of concurrent and sequential subtypes as course specifier
In ICD-10, the schizoaffective disorder is defined as the concurrent occurrence of schizophrenic symptoms with a major affective disorder. Longitudinal aspects of course are npt reflected well in the current classification. There is little evidence to support a chronological distinction regarding the co-existence of schizophrenic and affective symptomatology. Thus two types of schizoaffective disorder must be distinguished: the 'concurrent' and the 'sequential' type (Marneros 2003). The first includes conditions with coincident schizophrenic and affective symptoms and the latter is defined as the schizoaffective disorder under a longitudinal aspect subsuming disorders with a symptom change between different episodes. The group felt that this change will improve the reliability and validity of schizoaffective disorders. A fifth character may be used to classify course e.g. F25.x.a
x – subtype
a – course which may be 0 – concurrent, and 1 - sequential
Conclusions
In the coming decades, efforts to explore simpler clues like endo-phenotypes to genetic underpinnings of disorders covered under this section will continue. It is being conceptualized that both genes and brain circuits they regulate may underlie symptom complexes across many diagnostic categories. The dimensional approach to psychiatric diagnosis will probably help in better segregating these symptom complexes. Also, there is issue of sub-threshold symptoms seen in primary care. Besides reliability and validity, issues of clinical utility are important. The changes proposed in the present classification of these disorders need to synthesize these issues.
References
Address for Correspondence:Dr Mamta Sood, Assisant Professor, Department of Psychiatry, All India Institute of Medical Sciences (AIIMS), New Delhi. Email: soodmamta[at]gmail[dot]com
Atul Ambekar, MD, Raman Deep MD, Rajat Ray, MD
Recommendations
Introduction
We began by conducting a comprehensive search (comprising both electronic and manual search) of the studies on mood disorders published in the Indian psychiatric/mental health journals. Attempt was also made to include the psychiatric research published in Indian medical/social journals (i.e. journals not dedicated to psychiatry/mental health alone). This review of the available Indian literature was conducted focusing on studies published between years 1992 (i.e. when ICD-10 was published) till date. We could locate 190 articles on mood disorders of which 161 had been published in Indian journals and 29 in International journals.
All the research articles were color-coded and divided into five broad categories for diagnostic validity as per Robins and Guze criteria (i.e. clinical description, family studies, laboratory studies, follow-up studies, and delimitation from other disorders: Table 1).
TABLE 1: Number of publications according to categories for diagnostic validity
| ICD-10 sub category | Clinical Description* | Family Studies* | Lab studies* | Follow-up studies* | Delimitation from other disorders* | Total |
|---|---|---|---|---|---|---|
| Manic episode | 23 | 4 | 4 | 10 | 1 | 42 |
| Bipolar affective disorder | 25 | 9 | 14 | 21 | 6 | 75 |
| Depressive episode | 56 | 2 | 25 | 21 | 5 | 109 |
| Recurrent depressive disorder | 2 | 1 | 2 | 5 | 0 | 10 |
Persistent mood disorder -Cyclothymia -Dysthymia |
0 1 |
0 0 |
0 1 |
0 1 |
0 0 |
0 3 |
| Total# | 107 | 16 | 46 | 58 | 12 | 239 |
Publications include: Original research articles/reviews/case reports/letter to editors/posters
*As per Robin and Guze Criteria (loosely applied) - ‘’Best fit’’
#Total is more than 100 % (i.e. 190 articles) as some articles could be classified in more than 1 category
The evidence was weighed for and against the diagnostic validity of a particular entity in mood disorders category and discussed among the members of team. We conducted a more diligent search in Indian and international literature for the following areas: (1) data inadequately represented in the Indian literature; (2) entities that were controversial in terms of their nosological status; (3) new categories/criteria/specifiers which could be potential candidate for inclusion: and (4) of interest as reflected in recent literature. References to publications from other countries have been made in the following situations: (1) as a primary reference where Indian studies were non-existent; (2) as supplement to the available Indian studies; and (3) to provide for an international perspective on controversial/debatable areas.
Chronic mania: Clinical description of chronic mania dates back to the 19th century when Kraepelin routinely described such cases in his presentations. More recently, chronic mania has been defined as presence of symptoms in excess of 2 years (Perugi et al, 1998). Prolonged continuation of manic episode has been reported from India as well, mainly in the form of case-reports. A manic episode lasting approximately five decades has been reported (Mendhekar et al, 2004). In the international literature, the prevalence of chronic mania is estimated to be around 6-13%, due to the variable criteria sets chosen to describe the condition(Perugi et al,1998; Malhi et al, 2001). Chronic mania differs partially in its psychopathological presentation from acute mania. While, disturbances in the biological functions such as sleep and appetite are hallmark of an acute episode, chronic mania is devoid of the psychomotor and vegetative symptoms seen in the acute episode. Though, schizophrenia is a potential differential diagnosis in such cases, the absence of the flattening of affect and gross thought abnormality differentiates chronic mania from schizophrenia. At times, it becomes very difficult to diagnose a case of mania because of “personality style of the patient superimposed on a cyclothymic or hyperthymic temperament” (Mendhekar et al, 2004). Though not many follow-up studies are available, experts suggest that chronic mania is a poor responder to the conventional treatment for the mood disorders namely the mood stabilizers and neuroleptics.
Chronic depression: Studies examining depressive disorders have reported a relatively high frequency of cases with a chronic course. This is especially true for elderly patients, females, and those with comorbid illnesses (medical/psychiatric/substance use) (McIntyre and O'Donovan, 2004).
Mania in partial remission: Generally a manic episode is short lasting and its mean duration is reported to be three months. However, a few case reports from India suggest that some episode do not remit completely. For instance, Chawla and colleagues (2006) reported the case with five episodes over past 22 years with persistent mood congruent delusion in the inter-episodic period. Characterization of the ‘inter-episodic’ period in such cases by the specifier “in partial remission” would benefit communication between professionals as well as management of the case.
Depression in partial remission: Incomplete remission from depression is quite common, with approximately one third of patients continuing to have residual depression (Burt, 2004). The presence of residual symptomatology after an episode of depression is associated with an increased risk of short-term relapse and a chronic course; a higher risk of suicide attempts; poor social functioning; higher comorbidity and poor outcome of comorbid illnesses; and increased social and economic costs (Kennedy and Paykel, 2004).
The Satra Bruk classification workshop held in Sweden in 1999 proposed the introduction of a specifier for post partum onset (defined as onset within three months of delivery) (Elliott, 2000).
Depression with post-partum onset: An average general populationprevalence figure of 13% has been reported for postpartum depression (O’Hara and Swain,1996).In the Indian context, Patel et al (2002) reported prevalence of postpartum depression in 23% of mothers at 6-8 weeks of childbirth; 78% of these patientshad had clinically substantial psychological morbidity duringthe antenatal period. More than one-half of the patients remainedill at 6 months after delivery. Incidence has been found to be 16% and 10% in early and late post-partum period, respectively, in another study (Sood and Sood, 2003). Economic deprivation and poor marital relationships were important risk factors for occurrence and chronicity of depression. The gender of child was also found to be a determinant of postnatal depression, a reflection of the cultural preference for a male child over a female one (Patel et al, 2002). In developedcountries, the risk factors for postnatal depression are pasthistory of psychological disorder, psychological disorder duringpregnancy, low socioeconomic status, complicated delivery, andpoor marital relationship. Additionally, post-partum depression has been found to have a substantial risk of recurrence in subsequent post-partum periods (30%-50%). Women in developing countries whosepopulations have low incomes face considerable inequalities,ranging from fewer opportunities in education and employmentto less control over personal decisions, such as the use ofcontraception to plan pregnancies. Thus women in developing countries have all the risk-factors for post-natal depression in abundance, making the specification of ‘onset during postpartum period’ even more important in such contexts.
Post-partum mania: Despite diverse presentations, there is strong evidence fromclinical, outcome, and genetic studies for a close relationship between puerperal psychosis and bipolar disorder (Dorothy et al, 2006). Women who have suffered an episode of puerperal psychosis remainat high risk of developing further affective episodes (Davidson and Robertson,1985),and puerperal episodes of illness follow 20% to 30% of birthsto women with a history of bipolar disorder or affective psychosis(Kendell,1987). Family studies of puerperal psychosis consistently demonstratefamilial aggregation of psychiatric (predominantly affective)disorder, with morbidity risks for first-degree relatives inthe range of 10% to 50% (Platz and Kendell, 1988; Dean, 1989). The findingof higher rates of affective disorder in relatives of puerperalprobands suggests a major overlap in the familial factors predisposingto puerperal psychosis and bipolar disorder.
A number of attempts have been made by various researchers to define a "biological symptomatic profile" of depression by means of genetic, biological and therapeutic studies (Staner, 1988; Rush and Weissenburger, 1994; Schotte, 1997; Parker, 2000; Hill and Gorzalka, 2005). Psychomotor and appetite disturbances, early awakening, anhedonia and psychotic symptoms seem more likely to reflect this biological dysfunction in depression (Staner, 1988). Studies have supported the construct validity of the DSM-III melancholic subtype of major depression. Schotte (1997) has proposed the integrated threshold model:
Melancholic symptom features are predictive of a positive response to ECT and to tricyclic antidepressants in the severely ill. Key features include psychomotor retardation, unreactive mood, pervasive anhedonia, and distinct quality of mood. Melancholic features are associated with shorter REM latency and/or nonsuppression of cortisol during the dexamethasone suppression test. Depressive episodes that are not melancholic may take on melancholic features with repetition and passage of time in some individuals. Once melancholic features are present, it is unclear whether they repeat across subsequent episodes. Melancholic features are not uniquely associated with a positive family history of depression per se, but they may be especially associated with a family history of severe depression (Rush and Weissenburger, 1994). Bipolar depression appears to be more likely to be 'melancholic' in type, thus providing an indirect strategy for the clinical definition of melancholia (Parker, 2000)
A recent study has pointed towards some similarities between melancholic depression and an endocannabinoid deficiency state. Interestingly, endocannabinoid activity is down-regulated by chronic stress and possibly increased by some antidepressant regimens. It has been proposed that an endocannabinoid deficiency may underlie some of the symptoms of melancholic depression, and that enhancement of this system may ultimately be a novel form of pharmacotherapy for treatment-resistant depression (Hill and Gorzalka, 2005).
While, the validity of the specification of melancholic symptoms in a depressive episode has been largely established (Rush and Weissenburger, 1994), we are raising a semantic issue here. In the current system (ICD-10) the symptoms historically regarded as ‘melancholic’ are called ‘somatic’. We propose that the term ‘melancholic' should be preferred as it is specific to depression, while the term ‘somatic’ leads to confusion with ‘somatoform symptoms / disorders.’
Approximately 8-14% of patients with psychiatric illness have catatonia as a presenting feature (Pommepuy and Januel, 2002).
Depression with catatonia: Depressed patients with catatonia have been found to be older, to have a significantly higher frequency of major depression, to have more severe cognitive impairments and more severe deficits in activities of daily living than depressed non-catatonic patients (Starksteinet al, 1996).
Mania with catatonia: Manic patients with catatonia are reported to have more mixed episodes, more severe manic symptoms, more general psychopathology, higher co-morbidity, longer hospitalization, and lower Global Assessment of Functioning (GAF) scores than the noncatatonic patients. Thus, the presence of catatonic symptoms in mania is regarded as a marker of a worse course and outcome (Braunig et al, 1998).
An increasing amount of research has challenged the traditional view that juvenile-onset bipolar disorder is a rare condition. The cumulative incidence of bipolar disorder in childhood and adolescence may equal the 1% rate in adults (Lewinsohn et al, 1995). Available Western studies suggest that childhood/ adolescent onset bipolar disorder have a greater prevalence of chronicity, psychosis, mixed and atypical features, high incidence of rapid cycling, and poor response to mood stabilizers (Geller et al, 2004; Wozniak, 2005). However, studies from India report a high rate of recovery and low chronicity (Rajeev et al, 2003; Jairam, 2004).
We support the continued inclusion of mood disorders within ‘general psychiatric’ disorder categories rather than among F90-F98 (…disorders with onset usually occurring in childhood and adolescence). However, we recommend that onset in childhood and adolescence be specified to ensure required clinical and research attention towards these conditions.
Traditionally, bipolar disorder has been considered as an episodic disorder with good inter-episode recovery. More recent studies have shown that in some cases complete recovery may not be achieved and subsyndromal symptoms persist in the inter-episodic period. The notion of complete interepisodic recovery is challenged further by studies documenting that certain patients demonstrate social, marital, occupational and cognitive dysfunction, even when euthymic (Watson and Young, 2001).
In line with our earlier recommendation for a specifier for complete/ incomplete remission of single ‘episode,’ we suggest that a provision should be made to specify whether the lifetime course of a recurrent disorder is characterised by complete/incomplete interepisodic recovery.
There are a few studies on seasonal pattern of mood disorders from India. The available evidence suggests that:
A significant proportion (22%) of bipolar affective disorder patients has been found to have seasonal pattern (Avasthi et al, 1996). Further, patients with seasonal pattern have been reported to have episodes mostly in summer and winter, longer episode duration and more psychotic features as compared to patients with no seasonal pattern. There also appears to be a genetic propensity present to mood variations in relation to environmental temperature (Fernandes et al, 1996).
The studies on seasonal pattern of mood disorders from India have been mainly limited to one group of authors. If, indeed, the concept of seasonal pattern (more so, the reverse seasonal pattern) of mood disorders is to be validated, there is a need to replicate these findings in other centres of India. A provision in the classificatory system for separately coding the specifier of seasonal pattern will stimulate further research in this area.
Rapid cycling among patients with bipolar affective disorders is important because of its implications for long-term prognosis and for the use of antidepressants. Indian literature about rapid cycling is mainly restricted to case-reports (Garg et al, 1998). International literature (Bauer et al, 1994) suggests that about 15-20% of bipolar disorders have a course which could be characterised as ‘rapid cycling’ (defined as four or more mood episodes in a year). Rapid cycling is associated with female gender, substantial depressive morbidity, high risk for serious suicide attempts, poor response to lithium and fair response to calcium channel blockers (Frye and Altshuler, 1997; Coryell et al, 2003). Some studies suggest that rapid cycling (spontaneous or induced) once established, becomes for many years a stable rhythm in a substantial proportion of patients (Koukopoulos A, et al, 2003). However, other studies examining data related to phenomenology, family history, and long-term outcome do not support rapid cycling as a separate entity but as a temporary complicated clinical state (Kilzieh and Akiskal, 1999)
We propose that patients with a course characterized by four or more episodes in a year for at least two consecutive years should be specified as having ‘rapid cycling.’ The duration criterion (two years) is in line with that currently employed for other chronic disorders such as dysthymia and cyclothymia as suggested by certain authors (Koukopoulos et al, 2003).
As discussed in the recommendation number 1.4, the term ‘somatic syndrome’ does not include somatic (i.e. physical) symptoms of depression. The symptoms described are more commonly referred to as melancholic symptoms in the existing literature. In order to avoid confusion with somatic symptoms and in line with the available research, we recommend the change of terminology from ‘somatic’ to ‘melancholic’.
The ICD prefers the use of the term mood over affective as mood represents a more enduring emotional state in contrast to affect which represents a feeling tone in response to present events. The F30-39 category has been named mood disorders in ICD-10. Following the same rationale, the term bipolar affective disorder can be replaced by bipolar mood disorder.
Somatic (i.e. physical or somatoform) symptoms of depression are common in manycountries, but their frequency varies depending on how somatizationis defined. In part, this variation may also reflect characteristics of physiciansand health care systems, as well as cultural differences amongpatients.
In some Western as well as Indian studies, a majority of patients with depression present with somatic (i.e. physical or somatoform) symptoms but acknowledgepsychological symptoms (such as depressed mood or guilt) when they were specifically asked about them (Goldberg & Bridges, 1988; Raguram et al, 2001). Even more importantly, the largest study to examine the relation between somatic symptoms and depression (which utilized data from World Health Organization's studyof psychological problems in general health care - 25, 916 patients from 15 primarycare centres in 14 countries in 5 continents) found that somatic symptoms are often the only or predominant presenting complaints in some patients with depressive illnesses (Simon et al, 1999). In this study, of the 5447patients who underwent a structured assessment for depressive and somatoform disorders, 1146 met the criteria for major depression. Among them, 69% reported only somatic symptoms (Simon et al, 1999).
The personal significance and meaning of the symptoms are shaped by cultural notions concerning the human body in health and in sickness. Although both depressive and somatic symptoms were distressing to Indian patients, qualitative analysis showed that depressive symptoms, unlike somatic symptoms, were construed as socially disadvantageous (Raguram et al, 2001).
Anger attacks have been proposed as a specific form of anger in depression. They are characterized by a rapid onset of intense anger and a crescendo of autonomic arousal occurring in response to trivial provocations. They resemble panic attacks but lack the predominant affects of fear and anxiety associated with panic attacks. They typically occur in situations in which an individual feels emotionally trapped and experiences outbursts of anger that are later described by the patient as being uncharacteristic and inappropriate to the situation at hand. The prevalence of anger attacks in depressed patients is approximately 30% to 40 % (Fava and Rosenbaum, 1999). Though the presence or absence of hostility, anger and aggression in depression has been a matter of controversy, anger attacks have been found to occur more often in depressed patients in comparison to healthy controls. Some studies have reported that depressed patients with anger attacks differ from those without such attacks in terms of clinical profile, comorbid personality disorders and certain biological variables. Serotonergic dysfunction may characterize this distinct subtype of depression - depression with anger attacks (Painuly et al, 2005). Fraquas et al (2006) reported that serum levels of homocysteine were positively correlated with length of current major depressive episode in patients with anger attacks but not in those without anger attacks. The attacks have been found to disappear in 53% to 71% of depressed patients treated with fluoxetine, sertraline, or imipramine (Fava and Rosenbaum, 1999). Significance of aggression as a gender-specific diagnostic criterion for depression has been proposed as ‘male depressive syndrome’ (Winkler, 2005).
In the current edition of ICD, recurrent mania finds mention as an inclusion term under other bipolar affective disorders (31.8). The previous edition, ICD-9, had a separate category called recurrent mania. However, there has been persistent debate about the same. Avasthi et al (1996) reported that recurrent mania was by no means uncommon in India (6.5%). A recent review examining the nosological status and validity of recurrent unipolar mania (Harish et al 2005) also concluded that unipolar or recurrent mania occurs in sizeable number of patients (5%-25%). Unipolar mania exhibit consistent differences from bipolar mania in clinical, course and outcome, laboratory and family studies.
We recommend that, recurrent mania should be coded separately under the broad category of bipolar affective disorders rather than as an inclusion term with ‘other bipolar disorders’.
There are few Indian data on depressive episode(s) with hypomania. Klerman (1989) and Akiskal (1999) labelled recurrent depression with hypomania as Bipolar affective disorder (BPAD)-II in their classifications of bipolar spectrum disorders. Bipolar II disorder is also recognized as adistinct subtype in the DSM-IV (1994) classification. The life-time prevalence rates of both bipolar I and bipolarII disorders have been estimated at 0.6%, giving a combinedfigure of 1.2% (Weissman and Myers, 1978). A number of recent studies have helped in establishing bipolar-II disorder as a separate entity from BPAD-I disorder as well as recurrent depressive disorder. The summary of these studies is presented below:
Clinical description:Goodwin and Jamison (1990) have suggested that sub-syndromal bipolarity appears at a meanage of 14 years, while the initial episode of bipolar I disorder occurs at a median age of 18 years and bipolar II disorderat a median age of 21 years. Majority of available studies conclude that bipolar II disorder has an intermediate age of onset as compared to bipolar I or unipolar disorder.
The gender ratio of bipolar II patients tended to favour women having this disorder as compared to bipolar I patients where the gender ratio was fairly equal (Dunner, 1993). Clinical differences have been found in some studies comparing females and males suffering from BPAD-II. Females, as opposed to males, had significantly lower age at onset, more axis I co-morbidity, atypical depressions, intra–depression hypomanic symptoms (i.e., mixed depression), and family history of suicidal behavior. Females had more sadness, loss of energy, loss of interest, and suicidal ideas (Benazzi, 2005). Differences were found mainly on the depressive pole of the disorder and not of great magnitude but the authors concluded that these findings merit further attention.
When compared with Bipolar-I and unipolar disorders, researchhas found certain distinct differences in rates of recovery, clinical features and number of episodes. Rapid cycling was noted among bipolar I and bipolar II (but not unipolar) patients. Patients with seasonal affective disorder were more likely to be bipolar II than unipolar. Clinically depressed bipolar I patients evidenced psychomotor retardation; whereas, depressed bipolar II and unipolar patients either had psychomotor agitation or psychomotor retardation. One clinical feature that has consistently appeared to differentiate patients with bipolar II disorder from those with bipolar Idisorder or unipolar depression is the risk of suicide, whichappears to be elevated in this group (Bourgeois 1997). A history of suicide attempt was highest among bipolar II as compared to bipolar I and unipolar depressed patients (Dunner 1993). This may be related to the fact that the diagnosisis often missed, and consequently patients are ineffectivelytreated (MacQueen and Young, 2001). Also, high rates of comorbid disorders have been reported among patientswith bipolar II disorder (Savino et al, 1993; Pini et al, 1997), including substance abuseor dependence, anxiety disorders, and personality disorders.
Family studies: distinct familial inheritancefor bipolar II disorder has been suggested (Cassano et al, 1999). A tendencytowards a mild expression of mania may run in families (Kato et al, 2000). A summation of the large-scale studies where relatives of bipolar I, bipolar II, and unipolar patients were interviewed to determine their diagnosis revealed an elevated morbid risk for mania (bipolar I disorder) in relatives of bipolar I patients and bipolar II patients, as compared to relatives of unipolar patients and an elevated morbid risk for bipolar II disorder in relatives of bipolar II probands. These latter data suggested that bipolar II might "breed true." The family study data supported the notion that bipolar II was more similar to bipolar I than unipolar disorder but that bipolar II may be (on a familial basis) somewhat distinct from both bipolar I and unipolar disorder.
Laboratory studies: Preliminary imaging (Altshuler et al, 1995) and biochemical(Kato et al, 2000) studies that have separately examined subjects with bipolarI and bipolar II disorders have found differences in these groupsthat further support the view of bipolar II disorder as a discretediagnostic entity. Periventricular hyperintensities were found to be more common in bipolar I patients (62%) than in bipolar II patients (38%) and normal comparison subjects (30%; Altshuler et al, 1995). The rate of 5178C genotype was significantly higher in patients with bipolar disorder (64.8%, P < 0.05) compared with controls (53.2%) when paternally transmitted cases were excluded. This effect was more prominent in patients with bipolar II disorder (75.6%, P < 0.02 to controls). Bipolar II patients with 5178A genotype without family history had significantly later age at onset (56.0 ±14.7 years, P < 0.05) than other bipolar patients (Kato et al 2000). The major difficulty in assessing the review of the biological studies was the fact that no biological study consistently predicted discrimination of bipolar from unipolar patients, and many of the studies suffered from small sample size and lack of replication.
Some studies have found differences betweenbipolar I and bipolar II disorders on magnetic resonance imaging (MRI)and on the presence of vascular abnormalities, includingRaynaud's phenomenon, migraine and ‘migraine equivalents’(Altshuler et al, 1995).
Delimitation from other disorders: t he conceptof a trichotomy of mood disorders—bipolar I, bipolar II,and unipolar major depression—has been supported by studies that found distinct patterns of symptoms (as discussed above) and distinct familial inheritancefor bipolar II disorder (Cassano et al, 1999). Researchhas found distinct differences in rates of recovery,clinical features, and number of episodes. Preliminary imaging (Altshuler et al, 1995) and biochemical (Kato, 2000) studies that have separately examined subjects with bipolarI and bipolar II disorders have found differences in these groupsthat further support the view of bipolar II disorder as a discretediagnostic entity. The results of some studies support the notion that bipolarII disorder is intermediate between unipolar depression andbipolar I disorder with respect to illness course.
Follow-up studies: b ipolar II disorder appears to be diagnostically stable (Angst, 1986; Coryell, 1996).A variety of studies suggest that the probability of patients with bipolar II disorderdeveloping a manic episode was about 4% to 17% over up to 40 years of follow-up, with many of the studies supporting low rates of diagnostic conversion from bipolar II to bipolar I (Dunner and Tay, 1993; Coryell et al, 1995). Studies suggest that the number of episodes of depression maybe a stronger predictor of psychosocial outcome than mania in Bipolar II disorder (MacQueen et al, 2000). Preliminary studies suggest that the newer anticonvulsants maybe of benefit for this group.
There seems to be overwhelming evidence for existence of a valid diagnostic entity, characterised by depressive episode(s) with hypomania, which has been labelled “Bipolar-II disorder” in research studies as well as in DSM-IV. The ICD-10 at present mentions it as an inclusion term under ‘other bipolar disorders’ (F31.8). Over past one-and-half decades since the current version of ICD came into being, even more research evidence has been generated pointing towards diagnostic validity of this entity. Hence, in our opinion it is now time that this entity be accorded a distinct status of its own.
CONCLUSIONS
For the purpose of proposing modifications to the classification of mood disorders in the ICD-11, we have restricted ourselves to only those recommendations, (a) which have some evidence of validity in the existing literature, and (b) which have potential utility for the clinicians and researchers if incorporated. While the strength of the evidence-base varies from one recommendation to another, in terms of utility, we believe all of them to be quite useful. For many of our recommendations, we have deliberately not gone into details of definition / criteria. We believe that these definitions and criteria could only be refined, once the system provides for coding them. Till this consensus about definitions is achieved, we suggest that drafters for ICD-11 incorporate these recommendations with the most likely acceptable and/or flexible criteria, leaving some room for clinicians and researchers.
References
Address for Correspondence: Dr. Atul Ambekar M.D., Assistant Professor, National Drug Dependence Treatment Centre, All India Institute of Medical Sciences.
R K Chadda, MD, Nand Kumar, MD
Recommendations
Introduction
We were assigned with the task of possible modifications in the classification and categorisation of the Neurotic, Stress related and Somatoform disorders grouped under the codes F 40 to F 49 in the ICD-10 (International Classification of Diseases, 10th revision) for proposed ICD 11. Our recommendations were formulated on the basis of a comprehensive search (both electronic and manual search) of Indian and international literature pertaining to anxiety, somatoform and stress related disorder. The literature search of Indian studies was focused on studies published since 1990 onwards. The collected evidence was presented to an expert-panel comprising of Faculty of Department of Psychiatry, All India Institute of Medical Sciences, New Delhi for thorough discussion. This final draft of the recommendations has been prepared based on the consensus of the expert panel. We have made an attempt to examine the validity of our recommendations in the light of Robins and Guze (1970) criteria viz. clinical description, family studies, follow-up studies, laboratory studies and delimitation from other disorders.
In ICD 10, the essential feature of generalized anxiety disorder(GAD) is anxiety that is generalized and persistent and not restricted to any particular environmental circumstances. In addition the sufferer must have primary symptoms of anxiety on most days for at least several weeks at a time and usually for several months. The ICD 10 does not mention the exact duration of clinical features to diagnose the anxiety disorder.
The current diagnostic threshold for GAD raises questions about diagnostic requirements, such as whether 6-month duration and other psycho-physiological symptoms are needed for optimal identification of individuals who suffer from a clinically significant condition. Flint (2005) highlighted that in the community, period-prevalence of co morbidity of GAD with another psychiatric disorder is 4%, while the prevalence of pure GAD is only 1%. Early recognition of GAD is of paramount importance considering the co morbidity between GAD and other (especially depressive) disorders (Kessler 2001). Temporally primary GAD significantly predicts the subsequent onset of depression and other secondary disorders highlighting the importance of early intervention and treatment of primary GAD to prevent the subsequent onset of secondary anxiety and depression. Unfortunately, little is known about this possibility because, few people with pure GAD seek treatment. Specification of a duration criterion (preferably for 3 months) could help in early identification of the disorder (before the onset of co morbidity) and paving the way for collection of epidemiological data on pure GAD and also to develop outreach strategies that may correct this situation of low help-seeking in such cases.
Recent data from the US National Co morbidity Survey Replication (NCS-R), carried out during 2001-2003 also focused on the duration requirement for diagnosis of GAD using WHO Composite International Diagnostic Interview as assessment tool (Kessler 2005, Ruscio et al 2007). The report suggests that a large number of people suffer from a GAD-like syndrome with less than six months duration. The study also pointed out that cases of GAD with episodes of 1-5 months did not differ greatly from those with episodes of six or more months in onset, persistence, impairment, co-morbidity, parental GAD, or sociodemographic correlates.
The past decade has seen tremendous strides in the knowledge about the cause, epidemiology, and treatment of obsessive compulsive disorder. Research on clinical characteristics of the disorder have focused on several areas, including identification of subtypes, the role of insight, and patterns of co morbidity (Aigner et al 2005, Bellino et al 2005).
Poor insight identifies a group of OCD patients with distinct clinical characteristics. InOCD with poor insight, patients generally fail to recognize that the obsessions or compulsions are excessive or unreasonable. In a study from India, Ravi Kishore et al (2004) evaluated 100 subjects with OCD (DSM-IV), who had received adequate drug treatment. They observed that 25% of the subjects had poor insight. Poor insight was associated with poor response to drug treatment, earlier age-at-onset, longer duration of illness, a greater number of obsessive-compulsive symptoms, more severe illness and higher co morbidity rate, particularly with major depression. In a study conducted in Bangalore (India), it was observed that poor insight was an important clinical predictor of poor response to treatment with SSRI (seen in 40% to 60% of the sample); (Shetti et al 2005). Similarly, Erzegovesi (2001) evaluated clinical variables that might influence the antiobsessional response to proserotonergic drugs in a sample of 159 patients with obsessive-compulsive disorder (OCD). It was observed that non responders (43.4%) had an earlier onset and a higher frequency of "poor insight" subtype and somatic obsessions in comparison to treatment responders.
Several studies have shown significant brain abnormalities in OCD patients (Aigner et al, 2005). A recent MRI study has shown that there are significantly more features suggestive of structural brain abnormalities in OCD patients with poor insight in comparison to OCD patients with good insight (Aigner et al 2005).
Literature on clinical and psychobiological distinctiveness of hoarding behaviour in OCD (Bellino 2005; Lochner at al 2005) also supports the need for a specifier related to insight in OCD. In OCD, hoarding is associated with poor insight, lack of resistance to the compulsion to hoard, poor treatment motivation, poor response to SSRIs in comparison to other OCD symptom dimensions. Further, at the level of biological and psychosocial determinants, pathological hoarding could be associated with schizophrenia, OCD, and tic disorders, possibly through dopaminergic mechanisms (Damecour & Charron 1998).
Co morbidity between OCD and schizophrenia is an area of emerging interest. Evidence shows that obsessions and compulsions are more common in patients with schizophrenia than was previously thought (Matsunaga et al 2000). Matsunaga et al (2000) further observed that OCD patients are less likely to have poor insight (PI), compared to patients with OCD and schizophrenia; however, OCD patients with poor insight showed a similar degree of functional impairment to that observed in patients with OCD and schizophrenia, pointing towards different outcomes in the two subgroups of OCD. The authors compared 78 OCD patients (primary interest [PI] group: 36% of the sample based on insight question of the Yale-Brown Obsessive-Compulsive Scale) with 20 schizophrenics with OCD (OCD+S). After a 6-month combination of clomipramine and cognitive-behavioral treatment, 14 of 25 OCD PI patients no longer fell in the PI category, which was associated with reduced OCD severity and depressive status. Schizotypal personality disorder (SPD) was more common in patients whose insight remained poor even after the treatment. Co morbid SPD in PI patients may be associated with worse prognosis.
The current classification systems ICD–10 (World Health Organization, 1992) does not give clear operational guidelines for the diagnosis of Dhat syndrome, possibly because it is considered a culture-bound syndrome. Once we label a clinical entity as culture bound, it runs the risk of exclusion from mainstream psychiatric classification with resultant lack of research and understanding (Chadda & Ahuja 1990; Bhatia & Malik 1991; Sumathipala et al 2004).
Dhat syndrome, originally described in India based on cultural beliefs of people, has been found to be highly prevalent in countries neighboring India such as Pakistan, Nepal, Myanmar, Sri Lanka and others (Sumathipala 2004). The patients of Dhat syndrome present with multiple somatic and psychological symptoms in the background of perceived loss of semen. This causal belief is not culture bound - male preoccupation with semen loss is universal and has been frequently associated with depression and anxiety. Similarly, in patients presenting with ‘Dhat syndrome,’ it is not uncommon on clinical exploration to find underlying neurotic and depressive disorders. Several authors have commented that Dhat syndrome should be considered as a culturally determined symptom of (or syndrome within) common disorders like depression, anxiety and somatisation rather than as a culture bound syndrome (Wig 1994). Various experts have questioned the validity of Dhat syndrome being viewed as a single neurotic disorder in ICD–10, where it is included under ‘other specific neurotic disorders’ (F48.8). Indeed, it is difficult to classify a high proportion of these cases as ‘pure’ Dhat (Chadda & Ahuja 1990; Chadda 1995; Bhatia & Malik 1991). Several Indian studies have recommended that Dhat syndrome should be integrated into existing rubrics of psychiatric classification in appropriate places (Chadda & Ahuja 1990; Bhatia & Malik 1991; Wig 1994). This might help to formulate the management of Dhat syndrome comprehensively on a biopsychosocial model depending upon its clinical presentation.
Fatigue is a common symptom in Dhat syndrome. Disorders with fatigue as the main symptom are often grouped together as functional somatic syndromes (Bhatia & Malik 1991; Barsky & Borus 1999). The basic cognitive formulation offered to explain these disorders is based on somatosensory amplification, misattribution and abnormal illness behaviour. These mechanisms seem to operate in patients with Dhat syndrome, who frequently make their first contact with departments other than psychiatry, for example urology, dermatology and general medicine, and are then referred to psychiatry. Also, partly as a result of arbitrary diagnostic guidelines, but also due to their own expectations and characteristics, patients are often dissatisfied with their treatment or causal explanations offered (Chadda & Ahuja 1990). These features suggest that patients without anxiety and depression should be placed within somatoform disorders.
References:
Address for Correspondence: Professor R K Chadda, Department of Psychiatry, All India Institute of Medical Sciences, New Delhi – 110029. Email: drrakeshchadda[at]hotmail[dot]com
Anju Dhawan, MD, Tina Lal, MD
Recommendations
Proposals for the Category F50: Eating Disorders
Proposals for the Category F53: Mental and Behavioral Disorders associated with Perinatal Period
Introduction
Measuring the validity of psychiatric diagnoses is still anunsolved problem. Yet, revisions of the Diagnostic and StatisticalManual of Mental Disorders and of chapter V of the InternationalClassification of Diseases are now under way, with the hopeof improving the validity of the current systems. In this article we present few proposals for changes in the section F50-59 of the ICD 10, on the basis of available Indian data, Western data and clinical experience with due emphasis on criteria laid down by Robins and Guze and Kendell.
Evidence for the Proposed Changes
F50: EATING DISORDERS
Recent years have seen increasing dissatisfaction with the criteria for eating disorders as they currently stand, which combined with good evidence that a large number of patients of all ages presenting for treatment fall into the ‘not otherwise specified’ or ‘atypical’ category, has resulted in lively debate and suggestions for improvement.
Anorexia nervosa (AN) and bulimia nervosa (BN) are currently considered as disorders confined to the Western culture. Although many influences have been noted as formative in the development of eating disorders, slimness has received most attention in recent years. The recent identification of eating disorders in non-Western societies and different subcultures within the Western world has led to suggestions that Western cultural ideals of slimness and beauty have infiltrated these societies (Nasser, 1994; Shroff & Thompson, 2004). The biomedical definition of anorexia nervosa and bulimia nervosa emphasizes fat phobia in the presentation of these disorders. However, evidence exists that suggests anorexia nervosa and bulimia nervosa can exist without the Western fear of fatness and that this culturally biased view may obscure health care professionals’ understanding of a patient’s own cultural reasons for self-starvation, and even hinder their recovery Khandelwal et al, 1995).
Anorexia nervosa was earlier believed to be limited to the white Caucasian population in the West. But, in the last two decades it has been identified with increasing frequency in non western societies (including Hong Kong, Taiwan, China, Malaysia, India, Pakistan and Singapore) as well as ethnic groups in the West.
Current diagnostic criteria for anorexia nervosa are largely influenced by western cultural concept of dread of fat and drive for thinness. The diagnostic criteria for anorexia nervosa as outlined by the ICD 10 include: ‘A body image distortion in the form of specific psychopathology whereby a dread of fatness persists as an intrusive overvalued idea and the patient imposes a low weight threshold on himself or herself’. The contemporary diagnostic criteria therefore de-emphasize ‘emaciation’ and emphasize ‘fat-phobia’. Nasser (1994) attributed the transculturality of anorexia nervosa to a globalization of ‘fat-phobia’ because of the emergence of a culturally shrunken world due to mass communication technology. Thus, Western researchers presume that incidences of anorexia nervosa in non-Western societies are replicas of the West. As a result, fat-phobia still remains the ‘core’ psychopathology underlying anorexia nervosa despite its presence in non-Western societies. Indeed, in the current diagnostic systems cases that do not meet the criterion of fat-phobia are labeled as atypical (eating disorder not otherwise specified (EDNOS) in DSM IV or atypical in ICD 10).
Dread of fatness as the core psychopathology does not explain all cases of anorexia nervosa especially in the non western societies. Several cases of anorexia nervosa without accompanying fat-phobia have been reported in different societies and cultures (China: Lee 1995, Lee 2001; India: Khandelwal and Saxena 1990, Khandelwal et al, 1995). Lee et al (2001) evaluated 48 consecutive patients with broadly defined anorexia nervosa with a self-report rationale for food refusal questionnaire. Two-thirds (32) of the patients expressed fat-phobia but one third (16) did not. Sensation of abdominal bloating and low appetite were among the other rationales given by patients for refusal to eat. Based on a qualitative analysis of 70 Chinese anorexia nervosa patients (who had all been examined by an experienced psychiatrist over a period of 12 years), Lee (1995) reported that 59% of patients did not express any fat-phobia throughout their illness. They differed from their fat-phobic counterparts only in that they were premorbidly slimmer and demonstrated no signs of bulimia, often considered a sign of fat phobia.
Khandelwal & Saxena (1990) and Khandelwal et al (1995) asserted that the presentation of eating disorders in India varied from the typical description of anorexia nervosa. Their female anorexic patients typically showed decreased appetite, excessive weight loss and amenorrhea but no fat-phobia or body image disturbance. Though finally diagnosed and treated as cases of eating disorder, they presented considerable difficulty in diagnosis according to current classification systems. They suggested that this variation was due to sociocultural factors, as Indian culture does not dictate slimness as a beauty ideal, and that there was not as much concern with body image as in the West.
Banks (1992) studied the case of two anorectic women from the Minneapolis–St Paul area of Minnesota. Both women were from conservative religious fundamentalist backgrounds and expressed their desire to reduce food intake through religious understanding about food, the body and sexuality, provided by their religious culture.
The western version of fat phobic anorexia nervosa has neglected the full metaphorical significance of self-starvation and, when applied in a cross-cultural context, may constitute a category fallacy. Most non-Western patients will fall into the atypical group by not fulfilling criteria of dread of fat. Lee (1995) suggested the use of more culturally sensitive diagnostic criteria. One of the diagnostic criterions suggested by Lee (1995) states that, ‘the patients use complaints (such as abdominal bloating or pain, loss of appetite, no hunger, distaste for food, fear of fatness, and/or “don’t know”) to resist attempts to make them increase food intake.’ Due to its seeming ubiquity in Western anorexics and the relative lack of cross-cultural studies on anorexia nervosa it may be too early to shed the concept of fat phobia entirely. Hence, fat phobia should be retained as a specifier of anorexia nervosa, rather than as an essential criterion.
The criterion of amenorrhea was not required for the diagnosis of AN or BN by DSM-III although it was typically associated with anorexia nervosa. Amenorrhea was initially introduced as a criterion for several reasons (Garfinkel et al, 1996; Falk & Halmi, 1982). It was mentioned in historical reports of cases of anorexia nervosa in females. Also, it was hypothesized in more recent decades that anorexia was due to a primary impairment of hypothalamic functioning. Since then, however, it has been observed that amenorrhea generally follows loss of body weight and body fat. While, amenorrhea can occur is a minority of women before substantial weight loss (Theander, 1970), women with all the behavioral and psychopathological symptoms characteristics of anorexia nervosa including weight below the current diagnostic criterion may continue to menstruate. Also, there is no parallel criterion for males (Watson & Andersen, 2003). In a large community epidemiological survey, amenorrhoea did not discriminate between women with anorexia nervosa and women with all the features except amenorrhoea, across a number of relevant variables (Garfinkel et al, 1996).
ICD-10 differs from DSM-IV in being less stringent about the duration of amenorrhea and including some reference to change in male reproductive hormone function. There are some inherent limitations however in both of these diagnostic systems, as they impose a historically appreciated but perhaps overly specific medical criterion of amenorrhea. Current ICD-10 and DSM-IV anorexia nervosa category excludes substantial numbers of individuals who do not fulfill the monotheitic diagnostic criteria, because of the absence of amenorrhea, or because their final weight does not reach the required threshold, despite having clinically significant psychopathologies gravitating around preoccupation with body weight, food, and eating (Mitrany, 1992; Williamson et al 1992; Thaw et al, 2001). A diagnosis of eating disorder not otherwise specified (EDNOS), which is typically regarded as residual, is often misinterpreted as indicating problems of lesser clinical significance (Mitchell, 2005). Levels of distress, behavioral abnormalities, and cognitions similar to those associated with a full syndrome eating disorder often accompany EDNOS (Herzog et al, 1993; Thaw et al, 2001). In an effort to develop homogenous diagnostic groups that can have implications for treatment and course, care must be taken not to exclude people because of small variability in the symptom picture (Dancyger & Garfinkel, 1995).
It is therefore suggested that amenorrhea may be retained as a specifier of anorexia nervosa rather than as an essential criteria. Anorexia Nervosa may be identified on the basis of substantial self induced starvation to the extent of producing significant medical morbidity, which may include amenorrhea.
The weight criterion for anorexia nervosa has also varied over the years. Regardless of the degree of actual weight loss, patients with anorexia nervosa - like symptoms appear to experience a high degree of physiological and psychological distress similar to full anorexia nervosa. For example, a patient may begin dieting at a healthy personal weight of 115% (of ideal) and loses to 90% of this weight, with significant functional medical consequences, but never reach the 85% criterion. In fact partial-syndrome anorexia appears to be more common than anorexia nervosa (King, 1989; Walters & Kendler, 1995). About 1.5% of young women have an eating disorder in full form (Dancyger & Garfinkel, 1995; Ghaderi & Scott, 2001) and another 7%–10% have some, but not all of the features of an eating disorder (Dancyger & Garfinkel, 1995). There is controversy as to whether eating disorders are qualitatively distinct or whether they exist along a continuum of dieting and weight concerns. Herzog et al (1993) followed up a group of 33 women with partial syndrome AN, BN, or both for an average of 41 months. At follow-up, 45% of the subjects had gone on to develop a full-criteria eating disorder, and as many as 82% had met full criteria for an eating disorder at least once during the course of their illness. Similarly, King (1989) observed a spectrum of eating disorder severities with some movement between diagnostic groupings over the 12–18 month follow-up in his study of women in a general practice. These findings suggest that a continuum of pathology may exist in which partial syndromes may reflect an earlier phase in the disorder and thus an artifact of the particular timing of the intake interview or assessment.
The primary weight criterion for a diagnosis of anorexia nervosa is a weight less than 85% of what is considered normal for that person’s age and height (DSM-IV). A body mass index (BMI) less than or equal to 17.5 kg/m2, which originated from the ICD-10 diagnostic criteria for research is not adjusted for age and sex. It should be realized that a body mass index of 17.5 is a strict weight cutoff only for individuals over age 20. For children, and to a lesser extent for adolescents, the body mass index cutoff is less strict than the primary DSM-IV weight criterion.
In keeping with the categorical approach to diagnosis, a cutoff may be specified on the dimension of body size/weight. If ICD persists with BMI, at the minimum, it would require a better specification with regard to age and sex.
F53: Mental and Behavioral Disorders associated with Puerperium Not Elsewhere Classified
Recently delivered mothers are vulnerable to the whole spectrum of general psychiatric disorders, as well as those resulting from the physical and psychological changes of childbirth. Nearly 30% of women have adjustment problems and 15%-20% have minor to major depression. Maternal suicide and infanticide are rare but the more common and yet less recognized risks are those of maternal illness – beginning in utero – on the infant. Considering the high risk of maternal and infant morbidity and mortality (Appleby, 1991; Patel et al, 2003; Anoop et al, 2004; Buist, 2006) associated with post partum disorders it is essential to fabricate a diagnostic system with adequate sensitivity for identification of these disorders.
The rubric of postpartum disorders may be particularly important for developing countries. Indian studies have found high rates of post partum depression (16% to 23%) and have highlighted the importance of social factors, specifically poverty and female gender of the infant as risk factors for the same (Patel et al 2002; Chandran et al 2002).
Current status of postpartum disorder in ICD 10: The ICD-10, permits the classification of mental and behavioural disorders associated with the puerperium (F53) only if they have an onset within six weeks of delivery and if they cannot be classified elsewhere in the ICD 10 either because insufficient information is available or because it is considered that special additional clinical features are present that make classification elsewhere inappropriate. It will usually be possible to classify mental disorders associated with puerperium by using two other codes: the first is elsewhere in chapter V (F) and indicates the specific type of mental disorder (usually affective F30-F39), and the second is O99.3 (mental diseases and diseases of the nervous system complicating the puerperium) of ICD 10. The DSM-IV, with an even shorter onset specifier of four weeks, is restricted to four diagnoses only, and likewise is rarely used. In the light of available evidence that post partum disorders can occur for periods up to 1 year post delivery and that symptoms may have onset during the last trimester of pregnancy the current “6 weeks post partum onset” diagnostic criteria in ICD 10 is too restrictive.
Specific features of postnatal mood disorder are acknowledged in the text of DSM IV (e.g., fluctuating course and mood lability, delusions including the baby, risk of infanticide, disinterest in the infant, guilt because of dissonance between the mother's mood and society's expectation of happiness, and less than optimum development of a mother/infant relationship). These features are not described in the ICD 10.
Recent literature shows a growing focus on the entire perinatal period for mental health of the mother as this period significantly influences the healthy development of the fetus and the newborn. The perinatal mental health period spans conception to two years after childbirth according to some experts (Kowalenko et al 2000; Currid, 2004). It is the time when women are most likely to be admitted to a psychiatric hospital (Dean and Kendell, 1981), are at increased risk of experiencing an affective mental illness, and those with a pre-existing mental illness are more prone to relapse or recurrence of the condition (R C Psych 2000; Pritchard & Harris, 1996). A meta-analysis of 59 studies (including 12,810 women, mainly from developed countries) found an average prevalence rate of non-psychotic postnatal depression (PND) of 13% (95% CI - 12.3%-13.4%) (O' Hara et al, 1996). Most cases develop within the first 3 months, with a peak incidence at 4-6 weeks. Although one study showed that most cases last around 3 months and resolve spontaneously without treatment, another study showed that 50% of cases lasted over 6 months and some persisted at 4 years. Two prospective studies from Goa and Tamil Nadu detected depressive disorder in 23% and 16% respectively, with depression persisting six months after child birth in 11%-14% of women (Chandran et al 2002; Patel et al 2002). Depression and anxiety often begin in pregnancy, particularly in the third trimester, and so ‘perinatal’ rather than postnatal depression might be a better term.
However, the evidence for familial aggregationwas significant for narrowly defined postpartum depression (onsetwithin 4-8 weeks of delivery) but not for a broader definition(onset within 6 months of delivery) that is perhaps more typicalof the way the diagnosis is used as a lay term and applied inclinical practice (Forty et al, 2006). Based on such evidence, the Satra Bruk classification workshop held in Sweden in 1999, proposed to add a postnatal onset specifier of 3 months (Elliot, 2000).
Balancing available scientific evidence with common clinical usage a proposal for ICD 11 is to replace the duration of onset in the puerperium by onset from conception to 3 months post delivery i.e., the perinatal period.
Recently delivered mothers are vulnerable to the entire spectrum of general psychiatric disorders, as well as those resulting from the physical and psychological changes of childbirth. The postpartum “blues” can be part of the normative postpartum adjustment and affect up to 80% of women (Robin, 1962; Pitt, 1968). The mild symptoms of the blues differ qualitatively and quantitatively from postpartum major depression and do not interfere with maternal role functioning (Miller, 1999).
The prevalence of major or minor depression in pregnant women ranges from 7% to 26% (Chandran et al 2002; Patel et al 2002; Moses-Kolko & Roth, 2004). Depression during pregnancy is a strong predictor of postpartum depression and is associated with adverse effects on fetal development (Graff et al, 1991; Chandran et al 2002; Patel et al 2002). The reported rate of recurrence of postnatal depression (PND) after a subsequent childbirth is 30% and the rate is higher for women in whom the first episode of PND is the first-ever depressive episode, compared with the rate in women who have had previous non-puerperal depression (41% vs. 18%) (Cooper & Murray, 1995).
Most cases of post-partum psychosis are manic-depressive in form, and there is much evidence for a close connection between puerperal and bipolar disorders. Nearly half of women with bipolar disorder experience childbearing-related episodes (Blehar et al, 1998), predominantly depression. Another literature links post-partum and 'cycloid' (acute polymorphic) psychoses.
Post-partum anxiety disorders are underemphasized and may be more common than depression (Matthey et al, 2003). A review of eight studies of 'panic disorder' showed that 44% anxious women had an exacerbation and 10% a new onset, in the puerperium (Hertzberg, 1999). The focus of anxiety is also important, because it may indicate specific psychological treatment. Since the pioneering study of Bydlowski and Raoul-Duval (1978), over 40 papers have appeared on PTSD resulting from stressful parturition. There have been eight quantitative studies, showing rates up to 5.6% (Creedy et al, 2000). Obsessions of infanticide were among the first post-partum disorders to be described (Chapman, 1959; Button, 1972). Other morbid phenomena can also become a problem for some mothers. A disorder akin to dysmorphophobia, based on the bodily changes resulting from pregnancy and childbirth, is common.
The available evidence regarding etiology, familiality and course of postpartum mental illness especially postpartum depression and postpartum psychosis, the two most studied disorders do not support post partum disorders as a distinct diagnostic entity. Though the exact etiology is unknown, childbirth seems to act as a specific trigger for many mental disorders in line with the stress diathesis model. As nearly the entire spectrum of mood disorders, psychotic disorders and anxiety and stress related conditions are seen in the perinatal period we propose that the specifier ‘onset within perinatal period’ should be added to all diagnoses in mood disorder, psychosis and adjustment disorder sections (ICD-10 F20-29, F30-39, F43 ).
Psychiatric disorders occurring in the postpartum period have many unique features. Chandran et al (2002) assessed 50 Indian women admitted to a psychiatric hospital for severe mental illness occurring in the postpartum period. Nearly half (43%) of the mothers reported infanticidal ideas, 36% reported infanticidal behavior, and 34% reported both infanticidal ideas and behavior. Logistic regression analyses indicated that presence of depression and psychotic ideas predicted infanticidal ideas, whereas presence of psychotic ideas toward the infant predicted infanticidal behavior.
Many mothers are excessively anxious about the health and safety of their children or they may fear the awesome responsibility of infant care. Most mothers are shielded from this by family support, but it can be a problem in isolated nuclear families. A mother with infant-focused anxiety may develop a phobia for the infant (Sved-Williams, 1992). Fear of cot death can reach pathological proportions (Weightman et al, 1999). Its main manifestation is nocturnal vigilance – the mother lying awake listening to the infant's breathing, with frequent checks that lead to exhausting sleep deprivation. As mentioned earlier, obsessions of infanticide were among the first post-partum disorders to be described (Chapman, 1959; Button, 1972) and a disorder akin to dysmorphophobia, based on the bodily changes resulting from pregnancy and childbirth is common.
Specific features of postnatal mood disorder are not acknowledged in the ICD 10 though they appear in the text of DSM IV (e.g., fluctuating course and mood lability, etc.). It is recommended that the text description of various disorders should highlight features specific to the perinatal period.
Developing a relationship with the newborn is the central and most important psychological process of the puerperium. A disturbed mother infant relationship is phenomenon distinct from depression. On one hand, mothers’ aversion to her infant is often disproportionate to depression and can occur without it; on the other hand, only a minority of depressed mothers has a relationship problem with their infants. This has led to proposals for a distinct ‘disorder of impaired mother-infant interaction’ (Brockington, 2004). Disorders of the mother-infant relationship are prominent in 10-25% of mothers referred to psychiatrists after childbirth. The etiology is probably different from post-partum depression, with more emphasis on unwanted pregnancy and challenging infant behaviour.
The main reason for the neglect of these disorders is their absence from ICD-10 and DSM-IV. In ICD-10, attachment disorders of childhood (reactive 94.1 and disinhibited 94.2) and 'Z codes' that include hostility towards the child, and scapegoating, address issues related only to the child's psychiatric state. One of the challenges for ICD-11 and DSM-V is to find a place for these disorders, so that they can be recognized by practitioners, and referred for expert treatment (Ainsworth et al, 1972; Salariya et al,1984; Hipwell & Kumar, 1996; Nagata et al, 2000; Brockington et al, 2001).
Though research in this area is lacking, the identification of this concept will sharpen the focus of studies aimed at preventing child abuse and neglect. Disorders of mother infant interaction may be included in the category F 53.
References
Address for Correspondence: Dr. Anju Dhawan, Associate Professor, Department of Psychiatry, AIIMS, New Delhi. Email address-anjudh[at]hotmail[dot]com
Pratap Sharan, MD, PhD, Nanaji Kaw, MD, Sabish Balan, MD, Kushal Jain, MD
Recommendations
Many South Asian psychiatrists would question the relevance of diagnosing and studying personality disorders. A major reason for the lack of interest in these conditions is their apparent rarity. A meta-analysis of general population studies carried out in India puts the prevalence figure for personality disorders at 0.6 per 1000 (Reddy and Chandrashekhar 1998). Very low rates have also been reported from Sri Lanka (Wijesinghe et al 1978). However, there are several shortcomings in the surveys conducted in developing countries (de Girolamo and Reich 1993).
Since the publication of the Diagnostic and Statistical Manual (DSM-III) in 1980 and its creation of a separate diagnostic axis (i.e. Axis II) for personality disorders, interest in the description and classification of personality disorders has expanded dramatically in the West. Between 20% and 40% of outpatients and more than 50% of inpatients in the western psychiatric set-up are reported to have comorbid personality disorders (Tyrer et al 1991). Comorbidity studies in India also suggest that personality disorders are common. In recent Indian studies, rates as high as 37.5% in patients with bipolar disorder, 40.8% in those with major depressive disorder (Naidu et al 1998) and 25.6% in those with substance use disorder (Kishore et al 1994) have been reported.
If personality disorders were a common but benign condition, there would still be no pragmatic reason to study them. However, they lead to a disturbance in functioning as great as that in most major mental disorders (Nakao et al 1992). Personality disorders are associated with high rates of separation and divorce; unemployment and inefficiency; and poor quality of life for the individual and his/her family. Patients with personality' disorders have an increased risk of mortality through suicide, homicide and accidents. Also, when a personality disorder is present, treatment of other coexisting psychiatric or medical conditions is frequently more complicated, lengthier, or less successful; a pattern that may at times be due to lack of recognition of the personality disorder (Oldham 1994).
The ICD-10 and DSM-IV are different but overlapping classification systems. Both have adopted polythetic diagnosis criterion a polythetic approach as against a monothetic approach. There are some differences in the nomenclatures such as anankastic in ICD-10 is obsessive-compulsive in DSM-IV, anxious in ICD-10 is avoidant in DSM-IV, and dissocial in ICD-10 is antisocial in DSM-IV. In ICD-10, borderline and impulsive personality disorders are viewed as subtypes of emotionally unstable personality disorder. In ICD-10, schizotypal disorder is considered to be an attenuated manifestation of schizophrenia and is categorized with the psychotic disorders; narcissistic, depressive and passive aggressive personality disorders do not find a mention.
There are also several marked differences in the criteria of the two systems and some minor variation in wording. The ICD-10 form of paranoid personality disorder includes excessive self-importance and self-reference as criteria, while in DSM-IV excessive self-importance forms a central part of narcissistic personality disorders. DSM-IV's schizoid personality disorder omits preoccupation with fantasy and introspection as criteria, though these are required in ICD-10.On the other hand, DSM-IV's antisocial personality disorder requires features of childhood conduct disorder, and emphasizes on law-breaking and criminal acts, while ICD-10's dissocial personality disorder does not mention childhood conduct symptoms in its set of criteria and is more concerned with generic concepts such as lack of empathy, inability to profit from experience and inability to maintain enduring relationships. In general, ICD-10 maintains a division between personality and mental state less clearly; for example, allowing the inclusion of persistent feelings of anxiety as a criterion in anxious personality disorder, and of obsessions in anankastic personality disorder.
ICD-10 requires the presence of three of the seven criteria to make a diagnosis (except for emotionally unstable personality disorder), while DSM-IV requires four or five from a list that varies from seven to nine (with the exception of antisocial personality disorder) (Sara et al 1996).
Current classification systems employ a categorical model for classifying personality disorders. However, there is considerable overlap among personality disorders. The dimensional model of classification has been proposed as a means to overcome these problems, as it can provide flexible, comprehensive and reliable information on subjects. However, much of the external validity research that is available currently has been conducted using categorical concepts, even though data on dimensional conceptualization of personality disorders is fast accumulating. Data support sometimes categorical, sometimes dimensional and sometimes both types of concepts.
Epidemiology: The prevalence of personality disorders defined in categorical terms range from 10.3% to 13.5% in community samples when assessment instruments specific to these disorders are used. The rate varied with age, with some decrease in older age groups. Urban populations and lower socioeconomic groups showed higher rates. The sex ratio was different for specific types of personality disorders, though the overall rate of prevalence was roughly equal for the two sexes (Reich and de Girolamo 1997). Prevalence rates of personality disorders may be lower in developing countries but methodological shortcomings in surveys done in these countries preclude direct comparisons. In the International Pilot Study of Personality Disorders (IPSPD), the following personality disorders were frequently diagnosed in a clinical sample at Bangalore (India): schizotypal (19.1 %) and borderline (14.7%) according to the DSM-III-R system; and emotionally unstable (8.6%) according to the ICD-I0 system (Loranger et al1997).
Reliability: The overlap between personality disorders defined in categorical terms is a reason forthe modest reliability seen in diagnosis, when different categorical conceptualizations of the same personality disorder (Hirshfield and Holzer 1994), different diagnostic systems (Sara et al 1996), or even different instruments operationalizing the same diagnostic system (Zimmerman 1994) are used.
Face validity: The face validity of the criteria sets for categorical definitions is low forboth the DSM-IIIR (Blashfield and Breen 1989) and ICD10 (Blashfield 1990) personality disorders.
Biological studies: There is some genetic support to categorical conceptualization of cluster A personality disorders, which are seen as existing in a genetic spectrum with psychotic disorders (Siever 1994, Siever, 2005). Antisocial personality disorder also appears to be heritable (Cadoret et al1995), but the specificity of a familial/genetic relationship of other personality disorders is suspect (Reich 1989; Torgersen 1994). On the other hand, Livesley and coworkers (Livesley et al 1992; Livesley 2005) demonstrated that 15 of the 18 personality disorder dimensions thought to underlie the DSM-III-R personality disorders had heritability in the range of 30%-60%. The results were similar to those reported for normal personalities and suggested a continuity between the normal and disordered personality.
Neuroimaging studies have provided some evidence for categorically defined personality disorders, e.g. increased ventricular-to-brain ratio and inefficient prefrontal cerebral processing in schizotypal subjects (Siever 1994). Positron emission tomography (PET) studies have also demonstrated some abnormalities in patients with antisocial personality disorder and metabolite borderline personality disorder (Doaln 1994; De la Fuente et al 1998; Pidimore et al 2005; Schmahl and Bremner 2006).
Neurochemical studies on the other hand have mainly provided evidence for dimensional conceptualization of personality features. E.g. schizotypal patients who display features of the deficit dimension have low cerebrospinal fluid (CSF) levels of the dopamine metabolite homovanillic acid (HVA) and those who have features of psychotic dimension have high CSF HVA levels (Siever 1994). In patients with duster B personality disorders (antisocial and borderline), 5-hydroxyindole acetic acid (5-HIAA) (a metabolite of serotonin) levels in the CSF and parameters of 5-HT (serotonin) functioning have been found to be inversely related to dimensions of impulsive aggression and negative affect. Also, platelet monoamine oxidase (MAO) levels are inversely related to dimensions of sensation-seeking and impulsivity (Dolan 1994; Coccarro et al 1997; Lara and Akiskal 2006, Lyons-Ruth et al, 2007).
Electrophysiological studies provide some evidence for categorically defined concepts. Abnormalities in relation to eye-movement and information processing have been reported to occur in patients with schizotypal personality disorder (Cadenhead et al 1993; Siever 1994; Evans et al 2007). Patients with borderline personality disorder have a decreased latency and increased density of rapid eye movements (REM) during sleep EEG recording. Some studies have also reported eye movement dysfunction and auditory evoked potential abnormalities in these patients (Lahmeyer et al1989; De la Fuente et al 1998; Boutros et al 2003; Howard and McCullagh, 2007). Evoked potential studies done under distraction conditions in patients with antisocial personality disorder reveal abnormalities in the P300 wave, suggesting deficits in information processing.
Treatment Studies: These studies have largely supported dimensional concepts. In general, pharmacotherapy aims at the correction of target symptoms such as aggression and behavioural dyscontrol, anxiety and mood dysregulation, and psychotic symptoms (including cognitive distortions) (Stein 1992; Cloninger et al 1997; Mohan 2002; Lara and Akiskal 2006). The limited data available on analytic psychotherapy (Bateman and Fonagy 1999) also do not support a diagnosis-based approach However, some data on other forms of psychotherapy have shown promise for specific categories of personality disorders, e.g. cognitive-behavioural therapy in avoidant personality disorder (Alden 1989) and dialectical behaviour therapy for borderline personality disorder (Linehan et al 1991).
Course and outcome: The literature regarding the long-term outcome of personality disorders is sparse (Skodol et al 2007). Most attention has been paid to formerly institutionalized patients with borderline, antisocial and schizotypal personality disorders. Borderline patients at 10-25 years follow up have a wide range of outcomes, from clinical recovery (50%-60%) to suicide (3%-9%). Suicide is particularly common in patients who have co-morbid depression or a history of substance abuse. If psychopathic traits are prominent, the long-term outcome in antisocial persons is bleak, though a substantial proportion of persons who exhibit a pattern of antisocial behaviour alone, recovers by the fourthdecade of life (Stone 1993). Schizotypal patients tend to remain isolated and lead marginal lives.
Boundary problems: within categorically defined personality disorders: Even though moderate internal consistency may exist forDSM-IIIR criteria sets of individual personality disorders, the correlation with other personality disorders is fairly high (Nunberger et al 1994; Widiger 2003). Consequently, there is a high rate of comorbidity (1.3 to 6.0) between personality disorders (Dolan et al 1995). Studies using multivariate statistical techniques have found that dimensions derived empirically bear a resemblance to some DSM-IIIR diagnoses but the correspondence between them is not close. In general, these studies have partially supported the cluster concept of the DSM system, with usually four superordinate factors corresponding to clusters I, II, III and obsessive-compulsive personality disorder emerging across many but not all studies (Hyler and Lyons 1988; Schroeder and Livesley 1991; Mulder and Joyce 1997; Skodol et al, 2007). The current classification systems have been criticized for either making over-refined descriptive distinctions, or forwrongly conceptualizing personality disorders as categories when they might be more properly described as trait dimensions.
Boundary problems: between personality disorders (Axis II) and symptom (state) disorders (Axis I): Although the distinction between Axes I and II disorders is valuable from the clinical point of view, the differentiation between the two sets of disorders is often problematic and at times even illusory. Particular problems exist in relation to differentiation between schizotypal personality disorder and schizophrenia spectrum disorders; borderline personality disorder and mood disorders; antisocial personality disorder and substance use disorders; and avoidant personality disorder and social phobia (Widiger and Shea 1991).
Boundary problems: between normal personality and personality disorder: Supporters of dimensional approach view personality disorders as extremes of temperamental traits found in the normal population (Schroeder and Livesley 1991; Costa and Widiger 1994; Paris 1997). The main reservations against this approach have been that (i) it has not been shown whether the three to five major dimensions found to describe normal personality (Digman 1990) also continuously underlie personality disorders; and (ii) some of the symptoms of personality disorders e.g. suicidal behaviour, self-mutilation do not have normative personality counterparts (Lenzwenger and Clarkin 1996). However, Livesley et al. (1992) showed that trait dimensions of personality disorders underlying DSM-III-R personality disorders in patient and general population samples are continuously distributed. They also demonstrated considerable similarity between the second-order factors (four) of personality pathology traits and four of the 'big five' factors of normal personality (Schroeder and Livesley 1991).
Authors who have used dimensional scaling techniques (Widiger et al 1987; Schroeder and Livesley 1991; Livesley et al 1992) and some who have carried out biological investigations in the area of personality disorders (Livesley et al 1993; Coccarro et al 1997) feel that the dimensional model fits the data on personality pathology in a better way. However, there are problems with this approach. It is not clear how personality pathology is actually organized at the latent level. The limited empirical evidence available suggests that schizotypy (Lenzwenger and Korfine 1992), borderline pathology (Trull et al 1990) and psychopathy (Harris et al 1994) may be organized as categories at the latent level. Further, biologists such as Kagan et al. (1987) and Magnusson (1986) noted that at least some personality traits may be dealt with in terms of physiobehavioural composites that are qualitatively distinct (categorical) rather than continuous (dimensional). In defence of the dimensional model, it may be said that the categorical criteria sets of schizotypal, borderline and antisocial personality disorders have been criticized for being saturated with items conveying the presence of symptomatic acts rather than personality traits (Stone 1993). Thus, they may have been more liable to show discreteness. The matter has not been adequately explored up to now for exclusive reliance on one or the other type of concepts.
Apart from the categories of personality disorders, ICD 11 should provide for agreed upon dimensions of personality and personality disorders. Evidence based candidates may be:
Dimensional models of personality:
Dimensional models of PDs:
Livesley and Jackson (1992) suggest ways to improve the classification of personality disorders by changing the way the classification is developed, evaluated, and modified so that it successively approximates a valid system. They argue that the first step in developing a classification is to ensure the content validity of diagnostic concepts because this is a prerequisite for other components of validity. Using trait and behavioural exemplars together in personality disorder criterion is a way to improve the content validity of personality disorders as it helps in tying the criterion to the concept and structure of the personality disorder, and in clarifying the nature of diagnostic items and the model for organizing diagnostic decisions. An example of using trait and behavioural exemplars together is given below:
Gross and persistent attitude of irresponsibility and disregard for social norms, rules and obligations, e.g. leaving a child less than 3 years of age alone at home for an hour to go and buy alcohol, dring at high speed around a blind corner, takes bribes, etc.
Specification of trait and behaviour exemplars would reduce the discrepancy between DSM-IV's antisocial personality disorder, which emphasizes law-breaking and criminal acts; and ICD-10's dissocial personality disorder, which is more concerned with generic concepts such as lack of empathy, inability to profit from experience and inability to maintain enduring relationships.
Defining the trait underlying the behaviour will also clarify the differentiation between Axis I and Axis II disorders. The differentiation between Axes I and II disorders parallels to some extent the distinction between personality traits and emotional states. Neuroticism, for example, involves the disposition to experience negative affects (McCrae and Costa 1990), and a correlation with mood states supports rather than questions its validity (Watson and Clark 1984). States and traits may best be conceptualized under prototypal concepts that provide meaningful distinction, but merge into each other at the boundaries (coaxial syndrome). It is useful to retain the differentiation because it has been shown that states affect personality domains differently, with relatively large parts of personality and behaviour (e.g. novelty-seeking, reward dependence) remaining unaffected by current states such as anxiety or depression (Svrakic et al 1992). Efforts to increase the distinction between state and trait disorders by adding or deleting existing criteria might change the meaning of the construct under study, e.g. borderline personality disorder would not remain the same if affective instability were to be removed from its description (Widiger and Shea 1991). On the other hand, defining the trait features consistently will improve reliability without compromising on validity.
The International Pilot Study for Personality Disorders (IPSPD) (Loranger et al 1997) demonstrated that personality disorders, as presently defined, could be identified at all sites (multinational, multilingual, multicultural). Similarly, cross-national studies suggest that the Three Factor Model of Eysenck (Eysenck 1982) and Five Factor Model (Costa and Widiger 1994) were invariant across cultures. However, these studies do not confirm the cross-cultural validity or usefulness of western diagnostic categories or personality dimensions, as they may have identified ethnic artefacts rather then culturally meaningful configurations (Lewis-Fernandez and Kleinman 1994). The five factors that emerged on the use of a lexicon of Chinese trait descriptors were different from the factors extracted from the Chinese translation of English words from an established five-factor questionnaire (Yang and Bond 1990). It has been hypothesized that culture can influence: the genetic selection of specific temperamental characteristics in highly inbred groups, learning inside and outside the family, the threshold when personality vulnerability cannot be compensated by the person, and the social threshold when such decompensations are labeled pathological (Neki 1970; Paris 1997).
From a cultural constructionist perspective, personality disorders are based on Anglo-American concepts of personhood and codes of appropriate bahaviour and owe their existence to the medicalization of disvalued social behaviour. Anxious (avoidant) and dependent personality disorders were excluded from the Chinese classificatory system because of the apparent rarity of these disorders and because it was felt that some of the defining features (e.g. subordination of one’s own needs to those of others on whom one is dependent) were normative in the Chinese culture which defines personhood not by autonomy and assertiveness but by intergenerational interdependence and self-effacement (Mezzich et al 2000).
In a similar way histrionic and dependent personality disorder may not be very useful in the Indian context. An observation of 290 cases (two thirds randomly selected and one third selected because of evidence of personality pathology) in a North-Western Indian clinical sample drawn from a general hospital setting (Sharan 2001) revealed only two case of histrionic personality disorder (0.7%) and 1 case of dependent personality disorder (0.3%). These disorders were not reported in the Bangalore centre (sample drawn from mental hospital setting) of the IPSPD also (Loranger et al1997). Histrionic behaviour may not be reported (histrionic personality disorder dimension had a moderately negative correlation with the lie/social desirability scale) or may be suppressed due to social disapproval, while dependent behaviour may be culturally normative. Specific problems with the criteria sets found in the Indian context were:
Dependent PD (DPD)
Histrionic PD (HPD)
ICD-10 requires the presence of three of the seven criteria to make a diagnosis (except for emotionally unstable personality disorder), while DSM-IV requires four or five from a list that varies from seven to nine (with the exception of antisocial personality disorder) (Sara et al1996). Livesley et al (1987) developed reliable scales to assess more than 50 traits thought to underlie each of the DSM III personality disorders.
The larger number of traits for each personality disorder would improve content coverage for personality disorders ensuring that they are not too narrowly defined. This expansion would also make it possible to include more culture-specific traits in the criterion set without reducing the possibility of making the diagnosis cross-culturally - with the help of other (less culture-specific) criteria.
ICD-10 requires the presence of three of the seven criteria to make a diagnosis for all personality disorders, except for emotionally unstable PD – impulsive type, in which only 2 of 5 criteria suffice. Three criteria of this disorder have overlapping behavioural referrants, hence the diagnosis can be made very easily. This is reflected in Indian studies. Emotionally unstable PD – impulsive type was the commonest diagnosis in an enriched clinical sample (two thirds randomly selected, one third selected for personality pathology) from Chandiagrh (4.1% definite diagnosis, 6.6% probable diagnosis) (Sharan, 2001); and also in the Bangalore sample of the IPSPD (4.3%) (Loranger et al 1997). However, clinicians rarely use the diagnosis owing perhaps to the unfamiliarity of the concept or because they think that it is only a part syndrome (Sharan, 2001).
Specification of mixed PD does not mention the number criteria required and the number of types of PD from which these criteria should be selected. Further, the mixed category may have no added advantage in a situation where all personality disorders have a lot of overlap and comorbid diagnosis is the norm.
No substantial empirical data have accrued to substantiate the validity of the following entities:
Hence, giving them a status above better established entities like narcissistic personality disorder appears anomalous.
Sharan (2001) found unexpectedly large (>0.4) correlation between the dimensional scores of ICD 10 paranoid and dissocial and emotionally unstable personality disorders. This is reflected in clinical experience (Sharan, paper submitted for publication) where a constellation of traits which can be tentatively termed as controlling/dominating personality disorder, present often for treatment. They seem to share features of emotionally unstable, paranoid (with narcissistic elements) and anankastic personality disorders. Studies of normal personality dimensions carried out in eastern cultures have noted rotational differences in structure, e.g. rotation of extraversion and agreeableness axes towards dominance and affiliation (Kagitbak et al 1996). Kagitbak et al (1996) feel that cultural nuances like an emphasis on smooth interpersonal relationships in Asia may be responsible for this shift of axes. It is understandable that conflicted dominance may show up (be labelled as) a personality disorder in cultures that emphasize subservience to hierarchy. In a similar way, while anxious (avoidant) personality was excluded from the Chinese classificatory system, Shinkeisitsu and Tajin Kyoufu (avoiding/rejecting due to interpersonal sensitivity) personality were described in Japan (Ono et al 1996). Shinkeisitsu and Tajin Kyoufu may reflect conflicts along the dimension of affiliation.
Controlling/dominating personality disorder and Tajin Kyoufu have parallels in the Structural Analysis of Social Behaviour (SASB) model (Benjamin 1996) where interpersonal behaviours as conceptualized as constituted by inputs from two primary dimensions - interdependence (dominance/submission versus independence) and affiliation (aggression versus sexuality).
Kernberg (1996) regards affects to be instinctive components of human behavior that emerge in the earliest stages of development and are gradually organized as part of early object relations into gratifying, rewarding, pleasurable affects or libido as an overarching drive, and into painful, aversive, negative affects which are organized into aggression as an overarching drive. Rage represents the basic affect of aggression as a drive, and its vicissitudes explain the origins of hatred and envy, as well as of anger and irritability as moods. He suggests that the earliest function of rage is the effort to eliminate a source of irritation or pain. A second function of rage is to eliminate an obstacle or barrier toward gratification. The third, developmentally a higher level function of rage is the elimination of a bad object that is intra psychically perceived as a willful source of frustration standing between the self and the gratification of a need. At a more advanced level, the wish is no longer to destroy the bad object, but to make it suffer. At a further level of development, the wish to make the bad object suffer shifts into the wish to dominate and control the bad object in order to avoid fears of persecution from it; as obsessive mechanisms attempt to regulate the suppression or repression of aggression. Finally, the original self-affirmative implications of rage may be seen in sublimatory aspects of the aggressive response in the search for autonomy and self-affirmation, and for freedom from external control. We feel that the controlling/dominating personality disorder person probably operates at the level where the wish to make the bad object suffer shifts into the wish to dominate and control the bad object as obsessive mechanisms attempt to regulate the suppression or repression of aggression but often fail to do so.
Proposed criteria for controlling/dominating PD
Zuckerman M, Kuhlman DM, Joireman J, et al. A comparison of three structural models of personality: the big three, the big five and the alternate five. J Pers Soc Psychol 1993; 65:757-768.
Address for Correspondence: Professor Pratap Sharan, Department of Psychiatry, All India Institute of Medical Sciences, Ansari Nagar, New Delhi – 110029.
Manju Mehta, PhD; Rajesh Sagar, MD; Ravindra Rao, MD.
The diagnostic criteria for Attention Deficit Hyperactivity Disorder (ADHD) followed by the Diagnostic and Statistical Manual (DSM – IV) should be incorporated as it is in the ICD 11 edition. Thus, the criteria should be as follows:
I. Either A or B:
A.Six or more of the following symptoms of inattention have been present for at least 6 months to a point that is disruptive and inappropriate for the developmental level:
Often does not follow instructions and fails to finish schoolwork, chores, or duties in the workplace (not due to oppositional behavior or failure to understand instructions).
Often avoids, dislikes, or doesn't want to do things that take a lot of mental effort for a long period of time (such as schoolwork or homework).
Often loses things needed for tasks and activities (e.g. toys, school assignments, pencils, books, or tools).
B.Six or more of the following symptoms of hyperactivity-impulsivity have been present for at least 6 months to an extent that is disruptive and inappropriate for developmental level:
The following categories for hyperkinetic disorder should be used in ICD 11.
Suggested criteria:
Evidence for the Proposed Changes
The current diagnostic criteria for hyperkinetic disorder in the ICD 10 differ from the diagnostic criteria incorporated in DSM IV in the following ways:
§ ICD 10 has divided the symptoms of hyperkinetic disorder into 3 main clusters – inattention, hyperactivity and impulsivity; DSM IV, on the other hand, has combined the hyperactivity and impulsivity clusters.
§ ICD 10 requires that the child should meet the criteria in more than one situation, whereas DSM IV requires the child has impairment in more than one situation (rather than meeting the entire criteria in more than one situation).
For ADHD/ hyperkinetic disorder, DSM IV criteria are better researched, while ICD 10 descriptions are used more often in clinics. Consequently, much of the published articles work relate to DSM IV criteria of ADHD.
Epidemiological studies: Malhi and Singhi (2000) reported that 8.1% of a consecutive sample of 245 children referred for evaluation to the Psychology outpatient services of the Department of Pediatrics of a tertiary care teaching hospital had ADHD. In a similar study, Mukhopadhyay et al (2003) found that 15.5% of children presenting to a child guidance clinic in a pediatric hospital over a one year period had ADHD. These studies demonstrated the utility of the ADHD diagnosis and the ease of applicability of DSM IV criteria in the Indian pediatric population.
Phenomenology: A factor analysis of symptoms of the disorder showed that a two-factor model had the best fit to the data – inattention and hyperactivity/ impulsivity (Hudziak et al, 1998). This supports the DSM IV proposal of two subtypes of ADHD rather than the three subtypes proposed by ICD 10. Studies have shown that while ADHD is a broad, heterogeneous category, the subgroup of children diagnosed as hyperkinetic disorder (the subtype in ICD 10) fit in the severe ADHD combined subtype of DSM IV criteria (El-Sayed et al, 2003).
Course and prognosis: A study that compared the predictive validity of ADHD according to ICD 10 and DSM IV criteria (Lahey et al. 2006) concluded that while both ICD-10 hyperkinetic disorder and DSM-IV ADHD exhibit predictive validity over 6 years, ICD-10 hyperkinetic disorder appears to under-identify children with persistent ADHD symptoms and related impairment. Children who met criteria for DSM-IV ADHD but not hyperkinetic disorder exhibited at least as much functional impairment over time as hyperkinetic children. A review by El-Sayed et al (2003) concluded that children showing symptoms above the threshold for a diagnosis of ADHD according to DSM IV are at risk of developing co morbid conditions and increasing stress in both parents and teachers. Theses reports suggest that children with features of ADHD, who cannot be diagnosed by ICD 10, but receive such a diagnosis according to DSM IV criteria need to be identified and managed appropriately.
The hyperkinetic disorder (ADHD) in ICD 10 and DSM IV is currently sub classified as follows (Table 1):
| ICD 10 | DSM IV |
|---|---|
| F90.0 Disturbance of activity and attention | 314.01 ADHD, combined type (ADHD-C) 314.02 ADHD, predominantly inattention type (ADHD-I) 314.03 ADHD, predominantly hyperactive-impulsive type (ADHD-HI) |
| F98.8 Inclusion term in other specified behavioral and emotional disorders | |
| --- | |
| F90.1 Hyperkinetic conduct disorder | --- |
| F90.8 Other hyperkinetic disorder | --- |
| F90.9 Hyperkinetic disorder, unspecified | ADHD NOS |
ICD: International Classification of Disease; DSM: Diagnostic and Statistical Manual
ADHD: Attention Deficit Hyperactivity Disorder
The authors propose the following categories to be used for hyperkinetic disorder/ADHD in ICD 11:
Epidemiological studies: Studies using the DSM IV criteria show that ADHD – inattentive subtype is the most common one followed by ADHD – combined subtype (2nd most common) and ADHD – hyperactive impulsive subtype (Graetz et al, 2001; Ford et al, 2003). The study by Malhi and Singhi (2000) confirmed that all the 3 subtypes of ADHD (according to DSM IV criteria) were common in India – 50% of the children had hyperactive-impulsive subtype, 35% had the inattentive subtype and 15% had the combined subtype.
Sociodemographic profile: Studies have shown that ADHD-hyperactive impulsive subtype is more frequent in the younger age group as compared to the ADHD-inattention subtype (Nolan et al. 1999, Malhi and Singhi, 2000). It also has been seen that ADHD-inattention subtype is more common among females than males (Biederman et al. 2002).
Comorbidity: Studies have shown differences in the comorbidity between the three subtypes of ADHD. Thus, higher rates of anxiety and depression were seen in those with ADHD-combined subtype and ADHD-inattention subtype compared to those with ADHD-hyperactive impulsive subtype (MTA Cooperative Group, 1999). One study has found higher rates of bipolar disorder and tic disorder in those with ADHD-combined subtype (Faraone et al, 1998). Oppositional defiant and conduct disorders are most commonly seen in children with ADHD-combined subtype, followed by ADHD-hyperactive impulsive and ADHD-inattention subtypes (Morgan et al, 1996). An Indian study (Malhi and Singhi, 2000) found differences between the 3 subtypes with respect to intelligence, academic difficulties, relationship with peers and behavioral problems.
Family studies: Though some studies have shown increased rates of a particular subtype in the relatives of the affected children (Faraone et al. 2000), other studies have not found such increased rates (Smalley et al, 2000). Thus the family studies have been inconclusive.
Treatment response: Studies on differential stimulant treatment response among various subtypes of hyperkinetic disorder/ADHD are not available as most of the trials have only recruited children with combined ADHD (MTA Cooperative Group, 1999). Studies that have employed other subtypes, have not reported treatment response separately (Kratochvil et al, 2002).
Course and prognosis: The degree and type of impairment have been shown to be different among different subtypes of ADHD. Lahey et al (2006) have shown that ADHD-combined and ADHD-hyperactive impulsive subtypes have greater impairment than ADHD-inattention subtype. It is also seen that ADHD-inattention subtype is associated with more academic problems, whereas ADHD-hyperactive impulsive subtype is associated with more social and behavioral problems (Gadow et al, 2000; Graetz et al, 2001).
Thus, studies have shown that there are several differences between the subtypes of ADHD, thereby making it important to recognize these subtypes.
Co-occurrence: While most children who meet the criteria for conduct disorder also meet the criteria for ADHD; only about one third of adolescents with conduct disorder meet the criteria for ADHD (Reeves et al, 1987; Szatmari et al, 1989).
Impairment: In terms of academic achievement, children with combined ADHD/conduct disorder have higher rates of reading disorders than ADHD and controls (McGee et al, 1984). Children with combined ADHD/conduct disorder were found to be more impaired in verbal skill, visual motor integration and visuospatial skills as compared to children with ADHD and controls (Moffitt and Silva, 1988). An Indian study (Malhotra et al, 1999) compared hyperkinetic conduct disorder (HCD) with conduct disorder and found that the HCD children had lower intelligence, more perinatal complications and delayed milestones.
Family history: Biederman et al (1992) examined the rates of psychiatric diagnosis among relatives of a large sample of ADHD and ADHD/conduct disorder. While the rates of ADHD was the same in both group of relatives, conduct disorder was more common among relatives of combined ADHD/conduct disorder than among ADHD disorder alone. Furthermore, relatives with conduct disorder also tended to have ADHD. This means that the two disorders co-segregated, indicating that ADHD/conduct disorder is a distinct familial subtype.
Course and prognosis: Studies have shown differences in the long term outcomes of both subgroups of children. The ADHD/conduct disorder subgroup showed more antisocial and defiant behaviors (August et al, 1983). Also this group showed a higher rate of substance use. Studies have also concluded that while ADHD itself conveys some risk for adult antisocial behavior, the combined ADHD/conduct disorder group had sharp rise in the risk of adult antisocial personality and criminal conviction (Mannuzza et al, 1989). The Indian study (Malhotra et al, 1999) that compared hyperkinetic conduct disorder (HCD) with conduct disorder also found that the HCD group had an younger age of onset, more gradual development of conduct symptoms and a longer duration of conduct symptoms.
Treatment response: Studies do not show any difference in the response to stimulant treatment between the ADHD/conduct disorder and ADHD group alone (Klonman et al, 1989).
Available evidence suggests that there is a need to have a separate diagnostic subgroup of hyperkinetic disorder.
The group of F70 – F79 consists of mental retardation, which includes the mild, moderate and severe types. Most of the intelligence tests used have a separate category for borderline intelligence. The DSM IV, too, places borderline intelligence in the group of ‘additional conditions that may be a focus of clinical attention’.
Borderline intellectual functioning, has received little attention to date. However, some studies on prevalence of this condition show that it is present in up to 7%–18% of the population (Hassiotis et al, 1999; Ninivaggi, 2001).
In a study by Chen et al (2006), it was seen that children with subaverage cognitive abilities were more likely to develop mental health problems than their counterparts with IQs above 80 in later life. Another study by Hassiotis et al (1999) which have also shown that those with comorbid borderline intelligence and psychotic illness had greater disability and were more likely to suffer extrapyramidal side-effects and show evidence of negative symptoms than those with psychotic illness with normal intelligence. This may lead to difficulties in other domains of adaptive functioning. Thus, studies have shown that individuals with borderline intelligence may require a separate category.
Hence, borderline intelligence should be included in the ‘Z’ category to provide recognition to this condition in the international classificatory system.
Author for correspondence: Dr. Rajesh Sagar, Associate Professor, Department of Psychiatry, All India Institute of Medical Sciences, New Delhi – 110029. E-mail: rsagar_29[at]yahoo[dot]com
Centre for Advanced Research and Excellence in Neuromodulation (CARE)
Public Health Awareness book on Mental Health ('Mansik Rog') in Hindi.
| Serum lithium estimation | |
| Timings for sample collection | 9.30 am to 12.30 p.m. (Monday to Saturday) |
| Timings for Report: | Approximately one hour |
| ECT (Modified) | Monday & Friday |
| Repetitive Transcranial Magnetic Stimulation (rTMS) | Monday to Friday |
What is rTMS?
On the basis of recent research we all know that there is neurobiological process involved in our emotion, memory and behavior. Transcranial Magnetic brain stimulation (TMS) is a technique for gently modulating the brain cells. It utilizes a specialized electromagnet that generates brief magnetic pulses, roughly up to the strength of an MRI scanner’s magnetic field but much more focused. The magnetic pulses pass easily through the skull just like the MRI scanner but because they are short pulses and not a static field, they can modulate the underlying cerebral cortex. It has also been shown that these changes may last for long period of time after stimulation is stopped leading to therapeutic effect.
What disorders has rTMS been shown to be useful for?
TMS is currently a potential treatment for patients with Depression, patients who experience hallucinatory "voices" and a variety of other Psychiatric and Neurological disorders. For patients with Depression, many research studies have shown clinical improvement following rTMS.
For patients reporting auditory hallucinations (voices), research has not been as extensive but initial results have been promising and suggest that low frequency TMS administered to parts of the brain underlying speech perception may reduce these voices.
The Food and Drug Administration (USA) has approved rTMS for Depressive disorder just 3 months back. TMS has been approved in Canada and Israel as a treatment of Depression for patients who have not responded to medications.
What happens in rTMS treatment?
rTMS is an outpatient procedure and does not require anesthesia or sedation. Few patients may experience discomfort at the site of stimulation for short time. Generally rTMS produces a slight tapping sensation on the scalp. When administered at selected stimulation sites it can cause little contraction of the muscles of the scalp. Mild headache and transient lightheadedness may sometimes result from rTMS. These symptoms usually resolve by themselves shortly after the treatment is over.
rTMS Treatment Lab in AIIMS
How long treatment session/course last?
It depends on the treatment/research protocol, but generally each session takes about 20 minutes. Treatment protocols vary in duration, but most require at approximately 10-15 sessions given five times per week.
Are there any risks associated with rTMS?
The brain is directly stimulated by rTMS. However studies reported so far, no loss of memory, impaired concentration and other cognitive impairment. This is in contrast to the well known cognitive side effects associated with Electroconvulsive therapy (ECT)
The main risk of rTMS is rare induction of seizure. However with proper safety guidelines chances of seizures are negligible. For stimulation at low frequency no seizures have been reported.
Why there is interest in rTMS?
No. of beds available-30
| New | Old | Total | |
|---|---|---|---|
| General OPD | 1429 | - | 1429 |
| New | Old | Total | ||
|---|---|---|---|---|
| a) | Child Guidance | 458 | 272 | 730 |
| b) | Walk-in-clinic | 14116 | 23947 | 38063 |
| c) | De-addiction | 172 | 989 | 1161 |
| Total | 16175 | 25208 | 41383 | |
| Grand Total | 23886 | 72386 | 96272 |
Admission - 435
Discharge - 431
| (A)Under Graduate Teaching | |
| 24 hrs | 3rd Semester |
| 14 hrs | 6th Semester |
| 6 hrs | 8th Semester |
| Clinical Posting | |
| 20 days | 4-5th Semester |
| 40 days | 6-8th Semester |
| (B) B SC Nursing | |
| 38 hrs in both the Semester | |
| (C) M.D.(Psychiatry) | |
| Post Graduate Teaching Program | |
| Journal Club | |
| Seminar | |
| Case Conference | |
| Faculty/Staff Seminar | |
| Frequency-once every week besides CCR & CGR in every semester | |
| (D) PhD (clinical Psychology) | |
Workshop on Psychological Approaches to Pain Management (January 21st, 2006)
A one day workshop was organized by Department of Psychiatry, All India Institute of Medical Sciences (AIIMS) on 21.01.06 in collaboration with the Indian Society for Pain Research and Therapy (ISPRAT).
The objective of the workshop was to sensitize clinicians about the psychological aspects of pain and to illustrate assessment and management of pain behaviour.
The workshop was inaugurated by Prof. A. Bhattacharya Ex HOD of Anaesthesia, GTB Hospital and currently Pain Consultant at Samvedna Hospital, NOIDA. In his keynote address he introduced the theme of the workshop by highlighting the need for adopting a psychosocial approach to the understanding of pain.
In summary, the workshop outlined a comprehensive approach towards pain management with an emphasis on psychological aspects of treatment which improve quality of life, foster coping skills and enhance the patients’ sense of empowerment and control.
The workshop was attended by more than a hundred and fifty participants from various fields and was appreciated 2006
Centre for Advanced Research and Excellence in Neuromodulation (CARE)
| (A)Under Graduate Teaching | |
| 24 hrs | 3rd Semester |
| 14 hrs | 6th Semester |
| 6 hrs | 8th Semester |
| Clinical Posting | |
| 20 days | 4-5th Semester |
| 40 days | 6-8th Semester |
| (B) B SC Nursing | |
| 38 hrs in both the Semester | |
| (C) M.D.(Psychiatry) | |
| Post Graduate Teaching Program | |
| Journal Club | |
| Seminar | |
| Case Conference | |
| Faculty/Staff Seminar | |
| Frequency-once every week besides CCR & CGR in every semester | |
| (D) PhD (clinical Psychology) | |
Workshop on Psychological Approaches to Pain Management (January 21st, 2006)
A one day workshop was organized by Department of Psychiatry, All India Institute of Medical Sciences (AIIMS) on 21.01.06 in collaboration with the Indian Society for Pain Research and Therapy (ISPRAT).
The objective of the workshop was to sensitize clinicians about the psychological aspects of pain and to illustrate assessment and management of pain behaviour.
The workshop was inaugurated by Prof. A. Bhattacharya Ex HOD of Anaesthesia, GTB Hospital and currently Pain Consultant at Samvedna Hospital, NOIDA. In his keynote address he introduced the theme of the workshop by highlighting the need for adopting a psychosocial approach to the understanding of pain.
In summary, the workshop outlined a comprehensive approach towards pain management with an emphasis on psychological aspects of treatment which improve quality of life, foster coping skills and enhance the patients’ sense of empowerment and control.
The workshop was attended by more than a hundred and fifty participants from various fields and was appreciated
2006
| (A)Under Graduate Teaching | |
| 24 hrs | 3rd Semester |
| 14 hrs | 6th Semester |
| 6 hrs | 8th Semester |
| Clinical Posting | |
| 20 days | 4-5th Semester |
| 40 days | 6-8th Semester |
| (B) B SC Nursing | |
| 38 hrs in both the Semester | |
| (C) M.D.(Psychiatry) | |
| Post Graduate Teaching Program | |
| Journal Club | |
| Seminar | |
| Case Conference | |
| Faculty/Staff Seminar | |
| Frequency-once every week besides CCR & CGR in every semester | |
| (D) PhD (clinical Psychology) | |
Workshop on Psychological Approaches to Pain Management (January 21st, 2006)
A one day workshop was organized by Department of Psychiatry, All India Institute of Medical Sciences (AIIMS) on 21.01.06 in collaboration with the Indian Society for Pain Research and Therapy (ISPRAT).
The objective of the workshop was to sensitize clinicians about the psychological aspects of pain and to illustrate assessment and management of pain behaviour.
The workshop was inaugurated by Prof. A. Bhattacharya Ex HOD of Anaesthesia, GTB Hospital and currently Pain Consultant at Samvedna Hospital, NOIDA. In his keynote address he introduced the theme of the workshop by highlighting the need for adopting a psychosocial approach to the understanding of pain.
In summary, the workshop outlined a comprehensive approach towards pain management with an emphasis on psychological aspects of treatment which improve quality of life, foster coping skills and enhance the patients’ sense of empowerment and control.
The workshop was attended by more than a hundred and fifty participants from various fields and was appreciated
2006
Centre for Advanced Research and Excellence in Neuromodulation ( CARE )
Centre for Advanced Research and Excellence in Neuromodulation ( CARE )
The Department of Psychiatry has been a pioneer in providing mental health services in a General Hospital Setting. The department runs regular out-patient walk-in and follow-up clinics in addition to weekly specialty clinics for child and adolescent psychiatric disorders, psychosomatic disorders, common mental disorders, severe mental disorders, dual diagnosis disorders and brain stimulationtherapies. Consultation liaison services are provided for the patients admitted in other wards of the hospital andemergency psychiatric services are provided on a round-the-clock. The department also provides community outreach services 6 days a week at the CRHSP, Ballabgarh, including one day each at the Primary Health Centre at Dayalpur and Chhainsa. Besides pharmacotherapeutic interventions, psychological treatments, modified electro convulsive therapy (MECT) and advanced treatments like rTMS, tDCS and biofeedback are routinely provided. During the year 2017-18, the department provided out-patient consultation services to a total of 17, 204 new cases and 66, 333 follow up cases and in-patient management to 282 patients.
The department is at the forefront of medical education with courses for MBBS, B.Sc/M.Sc nursing, MD (Psychiatry) and PhD (Clinical Psychology) scholars. The departmentalso conducts short term training courses of residents posted from other departments (Medicine, Geriatric Medicine, Emergency Medicine, Palliative Medicine, and DM Neurology). For MBBS students, teaching includes theory lectures of 20 hours (6th semester) and clinical training of 7 hours (3rd semester), 25 days (4th-5th semester) and 40 days (in 6th/8th semester).The department undertakes regular collaborative research with national and international agencies like World Health Organization (WHO), University of California, National Institute of Health Research (UK), ICMR, and is one of the leading partners for research regarding the development of psychiatric classificatory system (ICD-11) by WHO. The department organizes year round public educational events for public dissemination of research knowledge and to promote awareness of mental health issues.
Currently primary mandate of the department is to develop highly trained manpower, and formulate curriculum and techniques for undergraduate and postgraduate medical education. Exploration of general mental health morbidity, culturally appropriate treatment of mental disordersand epidemiology of substance abuse remains the main research focus of the department.
History of the Department:
The Department of Psychiatry had informal beginning in 1958, when DrLuvia Taylor Gregg, Honorary Consultant in Psychiatry, began formal teaching in psychiatry for the first batch of MBBS students. Dr Gregg planned to introduce 100 hours of teaching in psychiatry in MBBS curriculum. Prof KL Wig, the then Head, Department of Medicine (later Director, AIIMS) was instrumental in integrating teaching of psychiatry throughout the clinical posting in medicine, so that the exposure to psychiatry was spread to all the 3 years on weekly basis. Since there was no inpatient unit in psychiatry, MBBS students were sent to the Mental Hospital, Agra for exposure to inpatients in psychiatry. DrVimlaVirmani, who later headed the Department of Neurology, had worked as clinical tutor in the initial years of the Department history.Dr SC Malik, one of the earliest post graduate pass out from AIIMS, wrote in one of his memoirs, “we had about 80-100 hours' exposure in psychiatry at the under-graduate level. Psychiatry at that time was (mostly) ‘Dynamic Psychiatry’ with highly laden emphasis on psycho-analysis and analytically oriented psychotherapy. For the undergraduates it was a very thrilling experience and many of us approached Mrs. Gregg to know about ourselves - our hidden complexes etc. Our exposure to psychiatry was spread to all the 3 years on a weekly basis”
Dr AS Mahal joined as Assistant Professor in 1962 and Dr D Satyanand as Professor and Head in Aug 1963. DrSatyanand started regular MD Psychiatry programme in psychiatry, the first in the country. Post graduate psychiatry in general hospital setting provided the groundworks for de-stigmatizing psychiatry and in moving mental disorders outside the custodial boundaries of mental asylums, within the community. The MD course also fostered integration as medical residents could now opt for Psychiatry as their specialization in general hospital settings.
Anothermilestone contribution of the department was the development of rural mental health services, through the Indian council of Medical research funded mental health project at the Comprehensive Rural Health Services Project (CRHSP), Ballabhgarh during 1964, under the leadership of DrD Satyanand. The integration of Psychiatry training in rural undergraduate medical curriculum is a continuing legacy of this project. The department continues to provide regular care at its rural centres to fulfill its obligation towards development of rural and community psychiatry.
Another first achieved by the department of psychiatry, under leadership of DrSatyanand, was the beginning of Child Guidance Clinic in Delhi in 1964. From seeing only cases of mental retardation and hyperkinetic disorders initially, this clinic, now caters to a wide variety of psychiatric disorders and behavioral issues of children.
The first batch of successful psychiatrists completed their training at AIIMS in 1964 and DrSatyanand retired in late 1966. During 1967-1968, Dr Erna Hoch, a Swiss psychiatrist, who had migrated to India, headed the Department as Honorary Professor and Head for about one and half year.From 1969-1980, she was medical director and professor of psychiatry in the only psychiatric hospital in the province of Cashmere (Kashmir). In 1988, Erna Hoch returned to Switzerland to live in the Tessin. Her famous book “Sources and Resources” represents a collections of articles written while in India propounding on the cultural influence of mental ailments and their treatment.
Prof JS Neki, who joined the department in September 1968 as Professor and Head, introduced the concept of ‘Guru-Chela’ paradigm in the practice of psychotherapy with due consideration to Indian culture and context. He was also instrumental in opening doors for Psychiatry in other departments. Due to his efforts, posts for psychologists were created in the department of Pediatrics and Neurosciences.
Prof N N Wig (Picture courtesy: Shubh Singhvia Flikr) and Prof Rajat Ray
In 1980, Prof NN Wig joined the department. He was part of the expert group formed for preparing draft of National Mental Health Programme (NMHP), which was completed in 1982. Prof Wig also strengthened the relationship of psychiatry with neurosciences in 1984, by holding the first faculty position in Neuropsychiatry at AIIMS.
The de-addiction services started in AIIMS outpatient department in 1976.Prof D Mohan, then Head of the Department, and an AIIMS alumnus, persistently endeavored to minimize the gross imbalancebetween the resources required to meet the increasing needs for de-addiction services and those available. Thus was formed the De-Addiction Centre (DAC), initially functional from premises of DeenDayalUpadhyay Hospital. The DAC subsequently evolved to become National Drug Dependence Treatment Centre (NDDTC), a national centre and a WHO collaborating centreand became fully operational from its new premises in Ghaziabad from April 2003.
Prof R Ray, who became head of the department after the retirement of Prof D Mohan, was pioneer in carrying out the first national survey on substance use disorders under Ministry of Social Justice and Empowerment, Government of India, carried out from March 2000 to November 2001.
Prof SK Khandelwal, who became the head in 2013, developed the department further with multiple liaison services and creation of specialty clinics at AIIMS. His position as faculty of neuropsychiatryfurther strengthened the relation of psychiatry with neurosciences. DrKhandelwal is also credited with opening ofone of the first lithium clinic in India where free testing could be carried out for patient suffering from Bipolar Disorder. Under his leadership, various National CMEs and public lectures have been organized. In 2016 the department hosted the World Congress of Social Psychiatry under the leadership of Prof Khandelwal and Prof R K Chadda, who succeeded Prof Khandelwal as the Head of the Department and Chief of the National Drug Dependence Treatment Centre upon his retirement.
The Department of Psychiatry has been a pioneer in providing mental health services in a General Hospital Setting. The department runs regular out-patient walk-in and follow-up clinics in addition to weekly specialty clinics for child and adolescent psychiatric disorders, psychosomatic disorders, common mental disorders, severe mental disorders, dual diagnosis disorders and brain stimulationtherapies. Consultation liaison services are provided for the patients admitted in other wards of the hospital andemergency psychiatric services are provided on a round-the-clock. The department also provides community outreach services 6 days a week at the CRHSP, Ballabgarh, including one day each at the Primary Health Centre at Dayalpur and Chhainsa. Besides pharmacotherapeutic interventions, psychological treatments, modified electro convulsive therapy (MECT) and advanced treatments like rTMS, tDCS and biofeedback are routinely provided. During the year 2017-18, the department provided out-patient consultation services to a total of 17, 204 new cases and 66, 333 follow up cases and in-patient management to 282 patients.
The department is at the forefront of medical education with courses for MBBS, B.Sc/M.Sc nursing, MD (Psychiatry) and PhD (Clinical Psychology) scholars. The departmentalso conducts short term training courses of residents posted from other departments (Medicine, Geriatric Medicine, Emergency Medicine, Palliative Medicine, and DM Neurology). For MBBS students, teaching includes theory lectures of 20 hours (6th semester) and clinical training of 7 hours (3rd semester), 25 days (4th-5th semester) and 40 days (in 6th/8th semester).The department undertakes regular collaborative research with national and international agencies like World Health Organization (WHO), University of California, National Institute of Health Research (UK), ICMR, and is one of the leading partners for research regarding the development of psychiatric classificatory system (ICD-11) by WHO. The department organizes year round public educational events for public dissemination of research knowledge and to promote awareness of mental health issues.
Currently primary mandate of the department is to develop highly trained manpower, and formulate curriculum and techniques for undergraduate and postgraduate medical education. Exploration of general mental health morbidity, culturally appropriate treatment of mental disordersand epidemiology of substance abuse remains the main research focus of the department.
History of the Department:
The Department of Psychiatry had informal beginning in 1958, when DrLuvia Taylor Gregg, Honorary Consultant in Psychiatry, began formal teaching in psychiatry for the first batch of MBBS students. Dr Gregg planned to introduce 100 hours of teaching in psychiatry in MBBS curriculum. Prof KL Wig, the then Head, Department of Medicine (later Director, AIIMS) was instrumental in integrating teaching of psychiatry throughout the clinical posting in medicine, so that the exposure to psychiatry was spread to all the 3 years on weekly basis. Since there was no inpatient unit in psychiatry, MBBS students were sent to the Mental Hospital, Agra for exposure to inpatients in psychiatry. DrVimlaVirmani, who later headed the Department of Neurology, had worked as clinical tutor in the initial years of the Department history.Dr SC Malik, one of the earliest post graduate pass out from AIIMS, wrote in one of his memoirs, “we had about 80-100 hours' exposure in psychiatry at the under-graduate level. Psychiatry at that time was (mostly) ‘Dynamic Psychiatry’ with highly laden emphasis on psycho-analysis and analytically oriented psychotherapy. For the undergraduates it was a very thrilling experience and many of us approached Mrs. Gregg to know about ourselves - our hidden complexes etc. Our exposure to psychiatry was spread to all the 3 years on a weekly basis”
Dr AS Mahal joined as Assistant Professor in 1962 and Dr D Satyanand as Professor and Head in Aug 1963. DrSatyanand started regular MD Psychiatry programme in psychiatry, the first in the country. Post graduate psychiatry in general hospital setting provided the groundworks for de-stigmatizing psychiatry and in moving mental disorders outside the custodial boundaries of mental asylums, within the community. The MD course also fostered integration as medical residents could now opt for Psychiatry as their specialization in general hospital settings.
Anothermilestone contribution of the department was the development of rural mental health services, through the Indian council of Medical research funded mental health project at the Comprehensive Rural Health Services Project (CRHSP), Ballabhgarh during 1964, under the leadership of DrD Satyanand. The integration of Psychiatry training in rural undergraduate medical curriculum is a continuing legacy of this project. The department continues to provide regular care at its rural centres to fulfill its obligation towards development of rural and community psychiatry.
Another first achieved by the department of psychiatry, under leadership of DrSatyanand, was the beginning of Child Guidance Clinic in Delhi in 1964. From seeing only cases of mental retardation and hyperkinetic disorders initially, this clinic, now caters to a wide variety of psychiatric disorders and behavioral issues of children.
The first batch of successful psychiatrists completed their training at AIIMS in 1964 and DrSatyanand retired in late 1966. During 1967-1968, Dr Erna Hoch, a Swiss psychiatrist, who had migrated to India, headed the Department as Honorary Professor and Head for about one and half year.From 1969-1980, she was medical director and professor of psychiatry in the only psychiatric hospital in the province of Cashmere (Kashmir). In 1988, Erna Hoch returned to Switzerland to live in the Tessin. Her famous book “Sources and Resources” represents a collections of articles written while in India propounding on the cultural influence of mental ailments and their treatment.
Prof JS Neki, who joined the department in September 1968 as Professor and Head, introduced the concept of ‘Guru-Chela’ paradigm in the practice of psychotherapy with due consideration to Indian culture and context. He was also instrumental in opening doors for Psychiatry in other departments. Due to his efforts, posts for psychologists were created in the department of Pediatrics and Neurosciences.
Prof N N Wig (Picture courtesy: Shubh Singhvia Flikr) and Prof Rajat Ray
In 1980, Prof NN Wig joined the department. He was part of the expert group formed for preparing draft of National Mental Health Programme (NMHP), which was completed in 1982. Prof Wig also strengthened the relationship of psychiatry with neurosciences in 1984, by holding the first faculty position in Neuropsychiatry at AIIMS.
The de-addiction services started in AIIMS outpatient department in 1976.Prof D Mohan, then Head of the Department, and an AIIMS alumnus, persistently endeavored to minimize the gross imbalancebetween the resources required to meet the increasing needs for de-addiction services and those available. Thus was formed the De-Addiction Centre (DAC), initially functional from premises of DeenDayalUpadhyay Hospital. The DAC subsequently evolved to become National Drug Dependence Treatment Centre (NDDTC), a national centre and a WHO collaborating centreand became fully operational from its new premises in Ghaziabad from April 2003.
Prof R Ray, who became head of the department after the retirement of Prof D Mohan, was pioneer in carrying out the first national survey on substance use disorders under Ministry of Social Justice and Empowerment, Government of India, carried out from March 2000 to November 2001.
Prof SK Khandelwal, who became the head in 2013, developed the department further with multiple liaison services and creation of specialty clinics at AIIMS. His position as faculty of neuropsychiatryfurther strengthened the relation of psychiatry with neurosciences. DrKhandelwal is also credited with opening ofone of the first lithium clinic in India where free testing could be carried out for patient suffering from Bipolar Disorder. Under his leadership, various National CMEs and public lectures have been organized. In 2016 the department hosted the World Congress of Social Psychiatry under the leadership of Prof Khandelwal and Prof R K Chadda, who succeeded Prof Khandelwal as the Head of the Department and Chief of the National Drug Dependence Treatment Centre upon his retirement.
Professor & Head
Contact number: 11-26593660
anatomy[at]aiims[dot]edu
Additional Professor
Contact number: 11-26593517
rimadadaaiims20[at]gmail[dot]com
Professor
Contact number: 11-26593489
arundhatis[at]aiims[dot]edu
Professor
Contact number: 11-26594702
renudhingraaiims[at]gmail[dot]com
Professor
Contact number: 11-26593568 , 9654215492
tapas_nag[at]aiims[dot]edu
Professor
Contact number: 11-26593225
sehgalritu[at]hotmail[dot]com
Professor
Contact number: 11-26593922
sarojkaler[at]gmail[dot]com
Additional Professor
Contact number: 11-26594986
tonygeorgejacob[at]gmail[dot]com
Additional Professor
Contact number: 11-26598058
seemahkg[at]gmail[dot]com
Additional Professor
Contact number: 11-26596624
sirohi.neerja[at]gmail[dot]com
Additional Professor
Contact number: 11-26598048
subhashmbu[at]gmail[dot]com
Assistant Professor
Contact number: 11-26598032
prabhakar.emf[at]gmail[dot]com
Assistant Professor
Contact number: 11-26593660
arthiganapathy08[at]gmail[dot]com
Asstt. Prof.(Contract basis)
parulkushal7[at]gmail[dot]com
Scientist
Contact number: 011-26593517
prabhakp[at]gmail[dot]com
Scientist
Contact number: 9711887047
mkaiims[at]gmail[dot]com
The department of Anatomy, one of the first departments to be set up, has contributed to the development of Anatomy curriculum which is implemented throughout the country by the Medical Council of India. Research and publications from this department have often been quoted in the bible of Anatomy- i.e, Gray’s Textbook of Anatomy.
The department is involved in medical teaching and training at the undergraduate, postgraduate and doctoral levels and also provides services that include diagnostics in genetic disorders and fluorosis. It runs a National Centre for Electron microscopy that regularly provides training for technicians and investigators. The department is a WHO-recognized Centre for training in Human Genetics. The department is also an active collaborator and organizer of various cadaveric workshops for post-graduate training and skills training in surgical and allied disciplines.
The main thrust areas of research in the department are neurobiology, male and female infertility, auditory and visual pathways, ageing-related disorders, pain biology, addiction genetics, pre-ecclampsia, enteric nervous system, pancreatitic pathogenesis, morphometry using state-of-the-art design-based stereology, autophagy and cell death, rare and common genetic disorders, ecotoxicology, breast cancer, nanobiology and drug-delivery systems, plastination and cancer biology including rare endocrine tumours.
The department provides training opportunities and support in the fields of Anatomical sciences, Genetics and Electron Microscopy to all Indians and nationals of SAARC countries.
In view of the increasing incidents of ragging in colleges and elsewhere that reached proportions unbecoming of a civilised society the Hon’ble Supreme court admitted and heard the SLP No (s) 24295 of 2006 University of Kerala Vs Council, Principals’, Colleges, Kerala & Ors (with SLP(C) No.24296-99/2004 & W.P. (Crl) No. 173/2006 and SLP(C) No.14356/2005).
Pursuant to an order of Hon’ble Supreme Court of India dated November 27, 2006, the Ministry of Human Resource Development has constituted a Committee under the Chairmanship of Shri R.K. Raghavan (former Director, CBI) to look into the issue of ragging and suggest means of prevention of ragging in educational institutions.
The Committee primarily examined the following broad aspects of ragging:
The Committee had carried out a very detailed study with the help of voluntary organizations including CURE (Coalition for Uprooting Ragging from Education) and SPACE (Society for Peoples Action Change and Enforcement) and collected voluminous public opinion on the various factors contributing for ragging. Noted psychologists and educationists assisted the committee. The National Informatics Centre at the Ministry of Human Resources hosted a guest book in their website. Nearly eleven press releases were made during this period of evaluation and committee visited several cities in the country. A subcommittee of the Medical Council of India was also constituted for this purpose. A questionnaire was prepared that elicited over 12500 responses. In short a wide cross-section of the society provided the necessary background information, data and suggestions on tackling ragging in the country for consideration by the esteemed committee.
Subsequently the committee submitted a detailed report with suitable recommendations and measures required to effectively curb the menace. The recommendations of the Committee were duly accepted and the following directives have been issued to all the educational institutions for necessary implementation by the Hon’ble Supreme Court on 16 May 2007.
The All India Institute of Medical Sciences requests all students, parents and guardians to go through these directives and co-operate in the implementation of the directives of the Honourable Supreme Court of India. It is hoped that this will signal an end to the menace of ragging. Strict action shall be taken in accordance with the directives in case any student is found to indulge in ragging.
This web page is for the patients undergoing Coronary Artery Bypass Grafting (CABG). This web page attempts to explain the cause of the disease, the risk factors, the effects of disease and possible treatment options. It tells about the surgery, preoperative preparation and postoperative care in hospital and at home. Lastly, an effort has been made to spread preventive awareness about the coronary artery disease. For better understanding, at the cost of technical perfection, language has been made as simple as possible.
This web page is for the patient who has a heart valve problem and who seeks treatment for the same. The web page describes in various chapters some of the fundamentals of blood circulation through the heart and the function of the valves and the effects of the disease. The web page also tells about the symptoms, tests that are used for diagnosis and after care. It tells about the surgery and postoperative care while the patient is in hospital. Finally it explains the aftercare when the patient is at home. For the purpose of better understanding, language has been made as simple as possible and efforts have been made to explain the facts in common language.
The content and character of the discipline of Biostatistics has undergone a radical change during the last few decades. From being a passive and descriptive discipline, Biostatistics has emerged as a vigorous, dynamic and constructive instrument of decision making in the area of health and medical care. Powerful and sophisticated statistical techniques of planning and analysis of biological experiments and investigations, development of probabilistic models in epidemiology and application of operations research techniques in health care delivery have opened up new dimensions and capabilities in medical and health research. In this context, a medical persons’ training, particularly that of a medical researcher, would be considered incomplete today without a reasonable acquaintance with the potentialities of applications of bio-statistical techniques to enable him/her to plan his/her research studies with scientifically and statistically valid designs and to arrive at valid and meaningful conclusions applying appropriate statistical methods.
At the All India Institute of Medical Sciences (AIIMS), Biostatistics was a part of the then Department of Preventive and Social Medicine till 1973. In October 1973, an independent Biostatistics Unit was carved out from the Department of Preventive and Social Medicine. In 1986, the “Biostatistics Unit” was renamed as the “Department of Biostatistics” fulfilling a long felt need for such a department. As an independent department, it caters to the needs of all the faculty, scientific staff and students in the Institute in teaching and research.
The biophysics department was one of the first to be formed in a medical setup in India and continues to be at the top of India's academics and research. The academic curriculum of the department includes doctoral (Ph.D.) and postgraduate (M.Sc., M.D.) courses. The department receives extramural research funding from various government agencies like DST, DBT, ICMR, DHR, CSIR, etc. as well as intramural funding.
The department focuses on several key research areas: Protein structure and drug designing, Biomarker discovery, pathophysiology, and novel diagnostics & therapeutics of different diseases.
Protein structure-function relationships to gain detailed insights into their biological roles and use the relevant protein structures as targets for designing new drug molecules using a rational structure-based approach. The understanding of molecular and biophysical mechanisms of various pathologies utilizing cutting-edge technologies. The roles of p53 and alike key molecular pathways; electrophysiological studies in drug-resistant epilepsy; understanding the roles of exosomes in the pathogenesis of neurodegenerative diseases and cancers; and infertility and recurrent pregnancy loss are some of the key areas where the department emphasizes understanding underlying pathophysiology. The research emphasis is on finding novel diagnostics and therapeutics approaches for various pathologies e.g., Cancer, Neurological and Heart diseases, Infectious diseases, Infertility, etc. In finding novel diagnostics strategies, research work in the department focuses on Biomarker Discovery by Comparative Proteomics analysis including Multi-Omics Analyses, and Exosomes based early detection of various diseases. Also, in search of new therapeutics, foremost is Drug Discovery and Designing including specific and potent small molecules and Aptamer inhibitory molecules, Antibody-like inhibitors (Nanobodies)
The department has a state-of-the-art X-ray crystallography facility with other scientific instrumentations like SPR-based technologies for protein-protein interactions, Peptide Synthesizer, Robotic Nano Dispenser for Crystallization, AKTA Pure Chromatography System, CD Spectroscopy, Fourier transform Infrared Spectroscope with Microscope, Cellular electrophysiology facility, etc.
Department of Anaesthesiology, Pain Medicine Critical Care
Room No-5011, 5 th floor
Teaching Block, AIIMS,
Ansari Nagar, New Delhi-110029
Contact No- 91-11-26593212
| Name | Year |
|---|---|
| Dr. L. Narhari Rao | 1961 |
| Dr. Martin Issac | 1962 |
| Dr. Nalini R Kalle | 1962 |
| Dr. S. C. Khatariar | 1962 |
| Dr. K. V. Prasada Rao | 1963 |
| Dr. J. M. Mandappa | 1963 |
| Dr. Thimmaiah M. Nagarajan | 1964 |
| Dr. Thoppilaabraham Koshy | 1964 |
| Dr. B. Rama Mohan Rao | 1964 |
| Dr. Mary Thomas | 1964 |
| Dr. Sushila Dhawan | 1965 |
| Dr. Vasudev S. Hatandgi | 1965 |
| Dr. K. Sheela | 1965 |
| Dr. Anand Ramchander Gudi | 1965 |
| Dr. Sudhakar V. Mayadeo | 1965 |
| Dr. Bani Kumar Sharma | 1966 |
| Dr. S. Vaidyanath | 1966 |
| Dr. Shantanu K. Goel | 1966 |
| Dr. T.S. Ganapathy | 1966 |
| Dr. Vijay Kumar | 1966 |
| Dr. M. Sriram | 1966 |
| Dr. W. Sridhar Rao | 1966 |
| Dr. N. R. Satyanarayan | 1967 |
| Dr. Punnoose V. A | 1967 |
| Dr. Biman Chandra Ray | 1967 |
| Dr. R. Rajgopalan | 1968 |
| Dr. Shreniwas Ramchandra | 1969 |
| Dr. Sushma Khanna | 1969 |
| Dr. Nita Saxena | 1970 |
| Dr. Rejamd. Abdul Muiz Bora | 1970 |
| Dr. B.D. Sujatha | 1970 |
| Dr. Cherian Abraham | 1970 |
| Dr. Hira Lal Kaul | 1970 |
| Dr. Sudhendu Das Gupta | 1970 |
| Dr. Nirode Baran Moulick | 1970 |
| Dr. Anantapur B. Ramamurthy | 1971 |
| Dr. Attibele Ramchandra | 1971 |
| Dr. Nalini Raja | 1971 |
| Dr. Nirupama Das | 1971 |
| Dr. Surath Manimala | 1972 |
| Dr. Surindar Singh Saini | 1972 |
| Dr. Gorla Satyamurthy | 1972 |
| Dr. Urmila Devi Passi | 1972 |
| Dr. V. Mahadevan | 1973 |
| Dr. Nirupama R Katre | 1973 |
| Dr. Gita | 1973 |
| Dr. Leela Kriplani | 1974 |
| Dr. T.S. Jayalakshmi | 1974 |
| Dr. Neelofer Bano | 1974 |
| Dr. Sanatan Das | 1974 |
| Dr. Avilavarapu Veeraju | 1975 |
| Dr. Deen Dayal Tantla | 1976 |
| Dr. Gour Mohan Bhar | 1976 |
| Dr. Koka Sri Hari | 1976 |
| Dr. Kiran Bhasin | 1976 |
| Dr. Meera Krishnan | 1976 |
| Dr. M. R. Rajgopal | 1976 |
| Dr. Rashmi Madan | 1976 |
| Dr. T. Madhavi Kutty | 1976 |
| Dr. Vimla Verma | 1976 |
| Dr. Gur Baksh Kohli | 1976 |
| Dr. Gopi Nath Kalla | 1976 |
| Dr. Vidya Murthy | 1976 |
| Dr. Krishna Panigrahi | 1976 |
| Dr. Bikram Rajkumar Ahuja | 1976 |
| Dr. Hemant Yashwant Sane | 1976 |
| Dr. M. Sujata Prasad | 1976 |
| Dr. S. Q. Shah Sayeed | 1976 |
| Dr. Ashok Vasantro Sumant | 1977 |
| Dr. Banambar Ray | 1977 |
| Dr. Hari Har Dash | 1977 |
| Dr. Shailaja C. Kale | 1977 |
| Dr. S. Sathiavathy | 1977 |
| Dr. Anil Karlekar | 1978 |
| Dr. Iftikar Ahmed | 1978 |
| Dr. Jyotsana Basu | 1978 |
| Dr. Roshan Lal Garg | 1978 |
| Dr. Raj Kumar Achoubisana | 1978 |
| Dr. Sharmila Sen Gupta | 1978 |
| Dr. Tej Kishan Kaul | 1978 |
| Dr. Aruna Ramesh Patil | 1978 |
| Dr. Bharati Belani | 1978 |
| Dr. E. Vijay Kumar | 1978 |
| Dr. Mahesh Kumar Arora | 1978 |
| Dr. Pran Nath | 1978 |
| Dr. Rajeshwar K Talwar | 1978 |
| Dr. Surjeet Kaur | 1978 |
| Dr. Vijay Ticku | 1978 |
| Dr. G. Parmeshwara | 1979 |
| Dr. A. Subramaniam Annapurna | 1979 |
| Dr. Sushila Chandrasekharan | 1979 |
| Dr. Rajiv Singla | 1979 |
| Dr. S. Vijayraghavan | 1979 |
| Dr. Jaspal Kaur Khurana | 1979 |
| Dr. Sunil D. Shittoot | 1980 |
| Dr. K. Bhaskaran | 1980 |
| Dr. Milan Kanti Chowdhary | 1980 |
| Dr. Jyoti Bhushan Pandya | 1980 |
| Dr. Yatin Mehta | 1980 |
| Dr. Ravinder Kumar Batra | 1980 |
| Dr. Abraham Fenn Cheriyan | 1981 |
| Dr. Selvarajan N | 1981 |
| Dr. Shachi Nandan Rattan | 1981 |
| Dr. Swaran Prabha | 1981 |
| Dr. Parmod Kumar Bithal | 1981 |
| Dr. Anil Kumar Jain | 1981 |
| Dr. Chander Mohan Bhagat | 1981 |
| Dr. Suman Dhingra | 1981 |
| Dr. Amar Pal Bhalla | 1982 |
| Dr. Sunil Kumar | 1982 |
| Dr. Yankidonka Shimpo | 1982 |
| Dr. Abha Saxena | 1982 |
| Dr. Dinesh Kumar Chaudhary | 1982 |
| Dr. Bupesh Kaul | 1982 |
| Dr. Tarun Kumar Danda | 1982 |
| Dr. Ridaplinwar | 1982 |
| Dr. Navneet Kaur | 1982 |
| Dr. Bandana Chatterjee | 1983 |
| Dr. P. Issac Muthiah | 1983 |
| Dr. Sushil Kumar Sonar | 1983 |
| Dr. Praveen Kumar Khilnani | 1983 |
| Dr. Usha Goel | 1983 |
| Dr. Mary Abraham | 1983 |
| Dr. Praveen Kumar Kalia | 1984 |
| Dr. Subrata Nag | 1984 |
| Dr. Gajender Singh | 1984 |
| Dr. Jagdish M Shahani | 1984 |
| Dr. Maya | 1984 |
| Dr. Nongthombam Tomcha Singh | 1984 |
| Dr. Ravi Saksena | 1984 |
| Dr. R. Rajeshwari | 1984 |
| Dr. Purnima Raina | 1985 |
| Dr. Kongbrailatpam N. Devi | 1985 |
| Dr. Brahma Deo Jha | 1985 |
| Dr. Chandra Bahadur Karky | 1985 |
| Dr. Shashi Bhushan Bhatt | 1985 |
| Dr. Arvind Kr. Gupta | 1985 |
| Dr. Ashutosh Wali | 1985 |
| Dr. Rajiv Chawla | 1986 |
| Dr. A. Durga Prasad | 1986 |
| Dr. Ashutosh Gupta | 1986 |
| Dr. Shubhangi S. Muley | 1986 |
| Dr. Vivek Vardhan Veturi | 1986 |
| Dr. Niraj Vishnoi | 1986 |
| Dr. Panchanan Mandal | 1986 |
| Dr. Muntimadugu Mastan | 1986 |
| Dr. Mantha Srinivas | 1987 |
| Dr. Tiakala Longkumar | 1987 |
| Dr. V. Latha | 1987 |
| Dr. Shailendra Joshi | 1987 |
| Dr. Sandhya | 1988 |
| Dr. Lokesh Kashyap | 1988 |
| Dr. Sushma Ahlawat | 1988 |
| Dr. Sunil Kr. Gupta | 1988 |
| Dr. M. Krishna Mohan | 1989 |
| Dr. Y. Lakshminarayan | 1989 |
| Dr. Udaya Lakshmi Rao | 1989 |
| Dr. Dharamavaran S.R. | 1989 |
| Dr. Abhiram Mallick | 1989 |
| Dr. Allu Satyanarayana | 1989 |
| Dr. Radha Mohan Issursing | 1989 |
| Dr. Vijaya Narasimha Raju G. | 1989 |
| Dr. Veena Hatta | 1989 |
| Dr. Arvind Kumar. Singh | 1990 |
| Dr. Neilavinuo Khimiao | 1990 |
| Dr. Anshuman | 1990 |
| Dr. Virginia Reade Khyriem | 1990 |
| Dr. Rajendra Prasad | 1991 |
| Dr. Anju Romina Bhalora | 1991 |
| Dr. Bindu Pandit | 1991 |
| Dr. Mary Muanpuii Ralte | 1991 |
| Dr. Rashmi Bodra | 1992 |
| Dr. Sujata Chaudhary | 1992 |
| Dr. Manisha Mehta | 1992 |
| Dr. Anand Kulkarni | 1992 |
| Dr. Nanda Gopal Mandal | 1992 |
| Dr. Navin Prakash | 1992 |
| Dr. Manjula | 1992 |
| Dr. Mona Sachdeva | 1992 |
| Dr. Sunita | 1993 |
| Dr. Dinesh Thakur | 1993 |
| Dr. Pradeep Kumar Rai | 1993 |
| Dr. Tika Nath Sharma | 1993 |
| Dr. Manabendra Haldar | 1993 |
| Dr. Balagurumurthy | 1993 |
| Dr. Lakshmi Ganesan | 1994 |
| Dr. Kuchi B. Sridevi | 1994 |
| Dr. Shiv Kumar Singh | 1994 |
| Dr. Peyyety Janaki Subhadra | 1994 |
| Dr. Gagan Deep Singh | 1994 |
| Dr. Sanjay Kumar | 1995 |
| Dr. Kundan Das | 1995 |
| Dr. Chandra Mogera | 1995 |
| Dr. Anupam Krishna Das | 1995 |
| Dr. Balachundhar Subramaniam | 1995 |
| Dr. Kathirvel Subramaniam | 1995 |
| Dr. Abhijit Kanti Dam | 1995 |
| Dr. Ajay Patekar | 1995 |
| Dr. Sivakumar Nagaraju | 1995 |
| Dr. Ashikho Savio | 1995 |
| Dr. Meenakshi | 1996 |
| Dr. Linette Judith Morris | 1996 |
| Dr. Nagesha S.K. | 1996 |
| Dr. Sri.Sri Palanivel | 1996 |
| Dr. Nilmani Upadhyay | 1996 |
| Dr. Senthil Kumar S. | 1996 |
| Dr. Mylapore Latha | 1996 |
| Dr. Prabhakara B. | 1996 |
| Dr. Khalid Hussain Abu | 1997 |
| Dr. Tamil Selvan Perumal | 1997 |
| Dr .Ilavajady S. | 1997 |
| Dr. Shivakumar S. | 1997 |
| Dr. Ajay Kumar | 1998 |
| Dr. B. Sennaraj | 1998 |
| Dr. Balakrishna Bhattarai | 1998 |
| Dr. Sampath Shenoy | 1999 |
| Dr. Piyush N. Mallick | 1999 |
| Dr. Vanlalnghaka Darlong | 1999 |
| Dr. Puneet Maheswari | 1999 |
| Dr. Anuj Bhatia | 1999 |
| Dr. Birendra P. Sah | 1999 |
| Dr. Sukham Thoibahenba Singh | 1999 |
| Dr. Pratap Rudra Mahanty | 1999 |
| Dr. Amar Singh Bodh | 1999 |
| Dr. Kallol Deb | 2000 |
| Dr. Subramanyam M.S. | 2000 |
| Dr. Hemant Kumar | 2000 |
| Dr. Anindya S. Mondal | 2000 |
| Dr. Sailesh K. Mishra | 2001 |
| Dr. Amit Sudan | 2001 |
| Dr. Ashit K. Naik | 2001 |
| Dr. Sumesh Arora | 2001 |
| Dr. Nalin Sharma | 2001 |
| Dr. Jagan D. | 2001 |
| Dr. T.Senthil Kumar | 2002 |
| Dr. Lalit Sehgal | 2002 |
| Dr. Bhupendra Singh | 2002 |
| Dr. Sajith Chakithandy | 2002 |
| Dr. Anirvan Karmakar | 2002 |
| Dr. Rahul Seewal | 2002 |
| Dr. Anand H.Kulkarni | 2002 |
| Dr. Sudesh Prakash | 2002 |
| Dr. Ajit Bhat | 2002 |
| Dr. Umesh G. | 2002 |
| Dr. Jaydeb Ray | 2002 |
| Dr. Saju Sharafudeen | 2003 |
| Dr. Arvind Palanisamy | 2003 |
| Dr. Chaitali Sen | 2003 |
| Dr. Sundar Krishnan | 2003 |
| Dr. Madan Kumar N. | 2003 |
| Dr. Ashwini Kumar Sharma | 2003 |
| Dr. Nagendra Prasad C. | 2003 |
| Dr. Prashanth S.M. | 2004 |
| Dr. Tanaji Sambhaji | 2004 |
| Dr. Arun Kumar Jala Venkataraju | 2004 |
| Dr. Sajay D. | 2004 |
| Dr. Rengarajan J. | 2004 |
| Dr. Dhamodaran P. | 2004 |
| Dr. Sameer Desai | 2004 |
| Dr. Subramanian H.A. | 2004 |
| Dr. Sudarshan T. Lakhe | 2004 |
| Dr. Rabi Kumar Panigrahi | 2005 |
| Dr. R. Manikandan | 2005 |
| Dr. Soumya Swarup Ray | 2005 |
| Dr. Gururaj N. | 2005 |
| Dr. Lenin Banu E. | 2005 |
| Dr. R. Vijay Kumar | 2006 |
| Dr. Kunal Karamchandani | 2006 |
| Dr. Sunil Kumar Nanda | 2006 |
| Dr. Umakanth R.K. | 2006 |
| Dr. Senthikumar M. | 2006 |
| Dr. Gokul Toshniwal | 2006 |
| Dr. Mahesh Kumar Agrawal | 2006 |
| Dr. P. Sakthi Rajan | 2006 |
| Dr. Chaitra M. | 2007 |
| Dr. Mritunjay Kumar | 2007 |
| Dr. Bala Chandran S. | 2007 |
| Dr. Somnath Bose | 2007 |
| Dr. Anil Agarwal | 2007 |
| Dr. T. Chitra Rajeswari | 2007 |
| Dr. M.S. Kalaiselvan | 2008 |
| Dr. Dalim Kumar Baidya | 2008 |
| Dr. Abhijit Laha | 2008 |
| Dr. Shalini Kalyanaraman | 2008 |
| Dr. Priyanka Jain | 2008 |
| Dr. Abraham Sonny | 2008 |
| Dr. Praveen Talawar | 2008 |
| Dr. Prabhu R. | 2008 |
| Dr. Dipal Shah | 2009 |
| Dr. Puneet Khanna | 2009 |
| Dr. Chandrashish Chakravarty | 2009 |
| Dr. Avneep Aggarwal | 2009 |
| Dr. Priya Rudingwa | 2009 |
| Dr. Krithika Krishnan | 2009 |
| Dr. Rahul Kumar Anand | 2009 |
| Dr. Bikash Ranjan Ray | 2009 |
| Dr. Shiv Kumar S. | 2010 |
| Dr. N.V.G. Hariprasad | 2010 |
| Dr. Preet Mohinder Singh | 2010 |
| Dr. Khaja Mohideen S. | 2010 |
| Dr. Sujatha M. | 2010 |
| Dr. Gautham G. | 2010 |
| Dr. Nishad P. K. | 2010 |
| Dr. Thilaka Muthiah | 2010 |
| Dr. Ravi Raj | 2011 |
| Dr. Deepak Mathew Gregory | 2011 |
| Dr. N. Suryakumar | 2011 |
| Dr. Valluvan R | 2011 |
| Dr. Pradipta Kumar Barik | 2011 |
| Dr. S. Gnanasekarna | 2011 |
| Dr. Mohanaselvi S | 2011 |
| Dr. Pallavi Mishra | 2011 |
| Dr. Varadharajan N | 2011 |
| Dr. Sree Kumar E.J. | 2012 |
| Dr. Anuradha Purushottam Borle | 2012 |
| Dr. Ankur Sharma | 2012 |
| Dr. Hashir. A | 2012 |
| Dr. Sanjeev Kumar. S | 2012 |
| Dr. S. Sivanesan | 2012 |
| Dr. Shwetha. S | 2012 |
| Dr. Kanil Ranjith Kumar. P. | 2012 |
| Dr. Ajisha Aravindan | 2012 |
| Dr. Ravindran C | 2013 |
| Dr. Anil Kumar Malik | 2013 |
| Dr. Mona Sharma | 2013 |
| Dr. Suhas. P | 2013 |
| Dr. Shiv Akshat | 2013 |
| Dr. Srivivasa Raghavan G. | 2013 |
| Dr. Prerna Varma | 2013 |
| Dr. Riddhi Kundu | 2013 |
| Dr. Rajaganesh R. | 2013 |
| Dr. Rajkumar S. | 2013 |
| Dr. Arijit Sardar | 2013 |
| Dr. Shubhangi | 2013 |
| Dr Gurkirat Kaur | 2014 |
| Dr Kaushal Kumar | 2014 |
| Dr Tailang Bumer | 2014 |
| Dr Deepak Singhal | 2014 |
| Dr Kavu Devi S | 2014 |
| Dr Farris Hussain KN | 2014 |
| Dr Bright Jebaraj Selvaraj | 2014 |
| Dr P Hemkumar | 2014 |
| Dr Rinoy Chandran | 2014 |
| Dr Rahul Kumar Gupta | 2014 |
| Dr Sumit Bansal | 2014 |
| Dr Priyankar Kumar Dutta | 2015 |
| Dr King Jee Dhar | 2015 |
| Dr Girijapathi | 2015 |
| Dr Neiseville Nisa | 2015 |
| Dr Senthil Packiasabapathy | 2015 |
| Dr Velmurugan | 2015 |
| Dr Sumit Gupta | 2015 |
| Dr Gnana Sagar | 2015 |
| Dr Ejas P. Bava | 2015 |
| Dr Sahir Aftab | 2015 |
| Dr. Gopikrishnan A | 2016 |
| Dr. Bharathram V | 2016 |
| Dr. Purabi Acharya | 2016 |
| Dr. Ankita Mishra | 2016 |
| Dr. Keerthi P. Nandakumar | 2016 |
| Dr. Sathianarayanan S | 2016 |
| Dr. Rupali Patnaik | 2016 |
| Dr. Varsha Mathews | 2017 |
| Dr. Purnima N | 2017 |
| Dr. Mohammed Rizwan | 2017 |
| Dr. Ramkumar | 2017 |
| Dr. Tanvi M Meshram | 2017 |
| Dr. Sayan Nath | 2017 |
| Dr. Dhruv Jain | 2017 |
| Dr. Shivangi Mishra | 2017 |
| Dr. Abhishek Singh | 2017 |
| Dr. Apala R Chowdhury | 2017 |
| Dr. Neethu M | 2017 |
| Dr. Tarun Arun Sahu | 2017 |
| Dr. Sathish Raja Selvam P | 2017 |
| Dr. Neha Agrawal | 2017 |
| Dr. Deepak Poudel | 2017 |
| Dr. Rohit Kumar Chaudhary | 2017 |
The department provides anesthesia/day care services in the following centres and surgical disciplines
The Intensive care unit in the 8th floor (AB 8) adjacent to Main operation theatres provides intensive care services to post-surgical patients and medical patients on referral basis, The ICU has state of the art ventilators, Multi-parameter monitors and has a laboratory of its own
Department has a best teaching program for DM (Critical Care Medicine) students, Post graduates and Senior Residents which consists of seminars, journal clubs, case discussion, tutorials, Guest lectures etc (4 days a week), All residents take part in the teaching activities regularly. This is in addition to daily teaching activity based on the cases conducted in the operation theatres Intensive Care Unit.
Six monthly semester examination
The Department has got the latest “Human Simulator” for teaching and hands on training of anesthesia, vascular access, central neuraxial blockade, peripheral nerve blockade and emergency scenarios including CPR. The simulator is also used for teaching and training and assessing Non-Technical Skills (NTS).
Faculty members moderate the teaching activity in classrooms and simulators. The newly junior residents have an additional basic teaching and orientation program by Senior Residents.
Department also participates in regular and Continuing Medical Education for student nurses, In-service Nurses and paramedical staff.
DM (Critical Care Medicine) is of three years duration course. Selection of the candidates will be done twice a year i.e. in January and July with intake of five students (four regular & one sponsored) based on computer based screening test followed by Departmental Clinical/practical Assessment test.
Postgraduate course (MD) is of three years duration, selection of junior residents for post-graduates course is made twice a year i.e. in January and July. No diploma course is available for this speciality. Apart from regular seats sponsored candidates from different states/countries are also allowed to join the course as per the rules of the institute. The selection is based on an All-India entrance examination.
Short-term courses are available as per the rules of the AIIMS in the following areas
This Department/Centre was established in 1971 as a Joint venture of Indian Institute of Technology Delhi and All India Institute of Medical Sciences, Delhi. The Centre has applied engineering principles to address medical and biological problems. It has faculty drawn from IIT Delhi as well as AIIMS New Delhi. In addition, the centre has collaborative projects with major institutes and hospitals in India. Over the years the Centre has become premier centre in the country.
The growth rate of CBME IITD is comparable to the global R&D. Centre has provided interdisciplinary base to develop health care technologies. Over the last two decades the focus has shifted to include biological medicine, behaviour or molecular health and develop innovative biological materials, implants, devices, and informatics approaches for the prevention, diagnosis, treatment, rehabilitation and injury mechanics. Innovations in instrumentation, drug delivery, tissue engineering and biosensors have been internationally recognized.
Research forms an integral part of the activities of our faculty members. Please click on the individual faculty member’s name to know more about their research activities and important publications
The department conducts free of charge ELISA based tests for four tumor markers (CA-19.9, CEA, PSA and AFP) in serum samples for patients of the Institute. On an average 40 -50 tests are reported every week.
NOTE :
| 1. | Name designation of the Officer | : | |
| 2. |
| : : | |
| 3. | Country to be visited | : | |
| 4. | Purpose of visit | : | |
| 5. | Actual date of Conference/Meeting (Documentary evidence may kindly be submitted) | : | |
| 6. | Proposed date of departure from India | : | |
| 7. | : | ||
| 8. | Whether he/she is actively engaged in Research in the subject matter of the Conference/symposium/seminar alongwith the brief description of the research in which he/she is engaged and the subject Matter of the Conference /seminar/ symposium. | : | |
| 9. | His/her specific contribution in the research as mentioned in Col. (7) above. | : | |
| 10. | How will his/her participation in the Conference/symposium/seminar in Question make a valuable contribution at the conferences/symposium/seminar Projecting the image of the Institute abroad. | : | |
| 11. | How will his/her participation in Conference/symposium/seminar in Question help in his/her work at this Institute. | : | |
| 12. | The specific details of travel costs, Registration fee and maintenance etc. (separately) travel by shortest route to be arranged directly with Air India Corporation is permissible. | : | - Air-fare by Air India Rs. ________________ - Regn. Fee (if any) Rs. ________________ - Maintenance Rs. ________________ = TOTAL Rs. ________________ |
| 13. | Indicate whether he/she has applied for financial assistance to any other Governmental agencies for the purpose. | : | |
| 14. | Indicate the month and year when he availed financial assistance from the institute last. | : | |
| 15. | Evidence of invitation letter and acceptance of his/her paper in the above conference etc. (Original of Photostat copy should be (enclosed). In case no invitation letter or acceptance of paper has so far been received, please indicate the date by which the same is likely to receive. | : | |
| 16. | Require to submit a copy of the abstract of paper accepted for presentation at the scientific meetings / congress etc. |
Certified that the particulars furnished above by me are correct to the best of my knowledge and nothing has been concealed.
Signature of applicant Date :
Remarks of the forwarding Officer
S I G N A T U R E
D A T E :
(Academic Section)
(on roll list till 12.08.2022)
| S. No. | Name OF PhD | Department | Session of Joining |
|---|---|---|---|
| 1 | KUMARI PRIYAM | ANATOMY | JAN'2016 |
| 2 | SHRISTY RAMAN | ANATOMY | JAN'2018 |
| 3 | DEVYANI SHARMA | ANATOMY | JAN'2020 |
| 4 | PRIYA KUMARI GORAI | ANATOMY | JAN'2020 |
| 5 | SANIA YASMIN | ANATOMY | JAN'2020 |
| 6 | SHIVANI | ANATOMY | JAN'2020 |
| 7 | ARTI JOSHI | ANATOMY | JAN'2020 |
| 8 | ANJALI YADAV | ANATOMY | JUL'2020 |
| 9 | ANJALI MAURYA | ANATOMY | JAN'2021 |
| 10 | AKANKSHA MISHRA | ANATOMY | JAN'2021 |
| 11 | AMIT KUMAR | ANATOMY | JAN'2021 |
| 12 | DEEPIKA KUMARI | ANATOMY | JUL'2021 |
| 13 | BHASKAR SHARMA | ANATOMY | JAN'2022 |
| 14 | ANURAG KUMAR | BIOCHEMISTRY | JUL'2017 |
| 15 | VIKAS KUMAR | BIOCHEMISTRY | JUL'2017 |
| 16 | VINNYFRED VINCENT | BIOCHEMISTRY | JUL'2017 |
| 17 | MOHIT ARORA | BIOCHEMISTRY | JUL'2017 |
| 18 | SUMEDHA SALUJA | BIOCHEMISTRY | JAN'2018 |
| 19 | ROHINI SAHA | BIOCHEMISTRY | JAN'2018 |
| 20 | TRYAMBAK PRATAP SRIVASTAVA | BIOCHEMISTRY | JAN'2018 |
| 21 | SAKSHI SHUKLA | BIOCHEMISTRY | JAN'2018 |
| 22 | SAJIB KUMAR SARKAR | BIOCHEMISTRY | JUL'2018 |
| 23 | VANDANA YADAV | BIOCHEMISTRY | JUL'2018 |
| 24 | NEHA SINGH | BIOCHEMISTRY | JUL'2018 |
| 25 | ASHU | BIOCHEMISTRY | JUL'2018 |
| 26 | SUBHADIP KUNDU | BIOCHEMISTRY | JUL'2018 |
| 27 | SWARANDEEP SINGH | BIOCHEMISTRY | JUL'2018 |
| 28 | SUNIL SINGH | BIOCHEMISTRY | JUL'2018 |
| 29 | ANITA | BIOCHEMISTRY | JUL'2018 |
| 30 | NISHA MANAV | BIOCHEMISTRY | JUL'2018 |
| 31 | KHUSHWANT SINGH | BIOCHEMISTRY | JUL'2018 |
| 32 | SANJEEV GOSWAMI | BIOCHEMISTRY | JUL'2018 |
| 33 | K DAVID RAJA | BIOCHEMISTRY | JAN&JUL'2019 |
| 34 | SIMRAN LAKHINA | BIOCHEMISTRY | JAN&JUL'2019 |
| 35 | MRIDULA SHARMA | BIOCHEMISTRY | JAN&JUL'2019 |
| 36 | VISHAKHA HOODA | BIOCHEMISTRY | JAN&JUL'2019 |
| 37 | ALISHA ARORA | BIOCHEMISTRY | JAN&JUL'2019 |
| 38 | SAGAR TYAGI | BIOCHEMISTRY | JAN&JUL'2019 |
| 39 | ANTARA MALIK | BIOCHEMISTRY | JAN&JUL'2019 |
| 40 | RASHMI GUPTA | BIOCHEMISTRY | JAN&JUL'2019 |
| 41 | MAHAIWON SHADANG | BIOCHEMISTRY | JAN&JUL'2019 |
| 42 | SHAIFALI SHARMA | BIOCHEMISTRY | JAN'2020 |
| 43 | AISHWARYA SINGH | BIOCHEMISTRY | JAN'2020 |
| 44 | DEEPIKA VERMA | BIOCHEMISTRY | JAN'2020 |
| 45 | BLESSED RAJ | BIOCHEMISTRY | JUL'2020 |
| 46 | RUPINDER KAUR | BIOCHEMISTRY | JUL'2020 |
| 47 | MANVI ARORA | BIOCHEMISTRY | JUL'2020 |
| 48 | DEEPAK | BIOCHEMISTRY | JUL'2020 |
| 49 | VADANYA SHRIVASTAVA | BIOCHEMISTRY | JAN'2021 |
| 50 | SANKET KATPARA | BIOCHEMISTRY | JAN'2021 |
| 51 | KOMAL SAGAR | BIOCHEMISTRY | JAN'2021 |
| 52 | MOHAMMAD SABIQUE BEG | BIOCHEMISTRY | JAN'2021 |
| 53 | SANTOSH KUMAR | BIOCHEMISTRY | JAN'2021 |
| 54 | ISHU | BIOCHEMISTRY | JAN'2021 |
| 55 | NEHA KASHYAP | BIOCHEMISTRY | JAN'2021 |
| 56 | HARSH BHAKHRI | BIOCHEMISTRY | JUL'2021 |
| 57 | HEMA YADAV | BIOCHEMISTRY | JUL'2021 |
| 58 | SUMAN SAHA | BIOCHEMISTRY | JAN'2022 |
| 59 | RITIKA SINGH | BIOCHEMISTRY | JAN'2022 |
| 60 | FARAH NAZ | BIOPHYSICS | JAN'2018 |
| 61 | ABHINAY KUMAR SINGH | BIOPHYSICS | JUL'2018 |
| 62 | YUDHISHTHIR YADAV | BIOPHYSICS | JUL'2018 |
| 63 | RAJKUMAR K | BIOPHYSICS | JUL'2018 |
| 64 | VIVEK DUBEY | BIOPHYSICS | JUL'2018 |
| 65 | ABHINAV SAINI | BIOPHYSICS | JUL'2018 |
| 66 | VIKAS KUMAR | BIOPHYSICS | JUL'2018 |
| 67 | PAWAN KUMAR TIWARI | BIOPHYSICS | JUL'2018 |
| 68 | YOGESH AGGARWAL | BIOPHYSICS | JAN&JUL'2019 |
| 69 | VIPRA | BIOPHYSICS | JAN&JUL'2019 |
| 70 | LAKSHAY MALHOTRA | BIOPHYSICS | JAN&JUL'2019 |
| 71 | AYUSHI THAPLIYAL | BIOPHYSICS | JAN'2020 |
| 72 | ANKIT MAURYA | BIOPHYSICS | JAN'2020 |
| 73 | TUSHAR | BIOPHYSICS | JUL'2020 |
| 74 | KM RENU | BIOPHYSICS | JUL'2020 |
| 75 | NEELAM | BIOPHYSICS | JUL'2020 |
| 76 | DEEPA | BIOPHYSICS | JUL'2020 |
| 77 | NABEEL AHMAD | BIOPHYSICS | JUL'2020 |
| 78 | MOHD SALMAN | BIOPHYSICS | JUL'2020 |
| 79 | POORVI VISHWAKARMA | BIOPHYSICS | JUL'2020 |
| 80 | KAMAL | BIOPHYSICS | JUL'2020 |
| 81 | DIPIKA SHARMA | BIOPHYSICS | JAN'2021 |
| 82 | RISHABH SINGH | BIOPHYSICS | JAN'2021 |
| 83 | NIVEDITA VATS | BIOPHYSICS | JUL'2021 |
| 84 | ALANKRITA SINGH | BIOPHYSICS | JUL'2021 |
| 85 | AMIT KUMAR YADAV | BIOPHYSICS | JUL'2021 |
| 86 | ABHAY MISHRA | BIOPHYSICS | JUL'2021 |
| 87 | SAKSHI KUMARI | BIOPHYSICS | JAN'2022 |
| 88 | TIRTHANKAR KOLEY | BIOPHYSICS | JAN'2022 |
| 89 | SANSKRITI RAI | BIOPHYSICS | JAN'2022 |
| 90 | LEENA SAPRA | BIOTECHNOLOGY | JUL'2018 |
| 91 | ASHA BHARDWAJ | BIOTECHNOLOGY | JAN&JUL'2019 |
| 92 | SHEETAL NEGI | BIOTECHNOLOGY | JAN&JUL'2019 |
| 93 | DEEKSHA MADHRY | BIOTECHNOLOGY | JAN&JUL'2019 |
| 94 | MANISH TRIPATHI | BIOTECHNOLOGY | JUL'2020 |
| 95 | SEEMA JANGIR | BIOTECHNOLOGY | JUL'2020 |
| 96 | ANJALI SINGH | BIOTECHNOLOGY | JUL'2020 |
| 97 | VAISHALI THUKRAL | BIOTECHNOLOGY | JAN'2021 |
| 98 | KANCHAN SAINI | BIOTECHNOLOGY | JAN'2021 |
| 99 | SUMEDHA YADAV | BIOTECHNOLOGY | JAN'2021 |
| 100 | DEEPAK POKHREAL | BIOTECHNOLOGY | JUL'2021 |
| 101 | DEEKSHA SACHDEVA | BIOTECHNOLOGY | JAN'2022 |
| 102 | TAHSEEN KHAN | BIOTECHNOLOGY | JAN'2022 |
| 103 | MAQSOOD ALI | BIOTECHNOLOGY | JAN'2022 |
| 104 | VISHAL BASU | BIOTECHNOLOGY | JAN'2022 |
| 105 | AMIT KHATRI | BIOTECHNOLOGY | JAN'2022 |
| 106 | AKHIL KUMAR | BIOTECHNOLOGY | JAN'2022 |
| 107 | APRAJITA TRIPATHI | BIOTECHNOLOGY | JAN'2022 |
| 108 | NEHA SINGH | C.C.M. | JUL'2020 |
| 109 | ASHUTOSH BANSAL | CARDIAC BIOCHEMISTRY (CNC) | JUL'2020 |
| 110 | SHIPRA | CARDIAC BIOCHEMISTRY (CNC) | JUL'2020 |
| 111 | PRIYANKA SOLANKI | CARDIAC BIOCHEMISTRY (CNC) | JAN'2022 |
| 112 | SANTOSHI KUMARI | CARDIOLOGY | JAN'2022 |
| 113 | AYON GUPTA | CENTRE FOR COMMUNITY MEDICINE (CCM) | JUL'2018 |
| 114 | SHRUTI VASHISHT | CENTRE FOR COMMUNITY MEDICINE (CCM) | JAN'2020 |
| 115 | AMAN DUA | CENTRE FOR COMMUNITY MEDICINE (CCM) | JAN'2020 |
| 116 | MAHASWETA DUBEY | CENTRE FOR COMMUNITY MEDICINE (CCM) | JUL'2021 |
| 117 | NISHAKAR THAKUR | CENTRE FOR COMMUNITY MEDICINE (CCM) | JUL'2021 |
| 118 | SRILOY MOHANTY | CIMR | JUL'2017 |
| 119 | SHIVANI SHARMA | CLINICAL NEURO PSYCHOLOGY | JUL'2017 |
| 120 | PAYAL KAHOL | COLLEGE OF NURSING | JAN'2021 |
| 121 | SOUVIK MANNA | COMMUNITY OPHTHALMOLOGY | JAN&JUL'2019 |
| 122 | SUMIT GROVER | COMMUNITY OPHTHALMOLOGY (RPC) | JUL'2021 |
| 123 | PREETI SHARMA | DERMATOLOGY & VENEREOLOGY | JUL'2017 |
| 124 | APOORVA | DERMATOLOGY & VENEREOLOGY | JUL'2017 |
| 125 | LAVINA RAJPUT | DERMATOLOGY & VENEREOLOGY | JAN'2021 |
| 126 | MEENAKSHI SHARMA | DIVISION OF FORENSIC PATHOLOGY & MOLECULAR DNA (JPNATC) | JUL'2017 |
| 127 | SAMRINA MAHTAB | ENDOCRINOLOGY AND METABOLISM | JUL'2015 |
| 128 | RUCHIKA KAUSHIK | FORENSIC MEDICINE & TOXICOLOGY | JUL'2017 |
| 129 | NEHA AFARIA | FORENSIC MEDICINE & TOXICOLOGY | JAN'2021 |
| 130 | KANGANA AGGARWAL | FORENSIC MEDICINE & TOXICOLOGY | JAN'2021 |
| 131 | SONU KUMAR | GASTROENTEROLOGY & HNU | JUL'2017 |
| 132 | ADITYA BAJAJ | GASTROENTEROLOGY & HNU | JAN'2018 |
| 133 | MANASVINI MARKANDEY | GASTROENTEROLOGY & HNU | JAN'2018 |
| 134 | SUMAIRA QAMAR | GASTROENTEROLOGY & HNU | JAN&JUL'2019 |
| 135 | DEEPAK RATHI | GASTROENTEROLOGY & HNU | JUL'2020 |
| 136 | SAMBUDDHA KUMAR | GASTROENTEROLOGY & HNU | JAN'2021 |
| 137 | RUTUMBARA DASH | GASTROENTEROLOGY & HNU | JUL'2021 |
| 138 | BIPIN TIWARI | GASTROENTEROLOGY & HNU | JAN'2022 |
| 139 | ANAND KUMAR | LAB MEDICINE | JUL'2016 |
| 140 | AKANKSHA PRIYA | LAB MEDICINE | JUL'2020 |
| 141 | RAM AASAREY | LAB MEDICINE | JAN'2022 |
| 142 | MEDHAVI PANDEY | LAB. ONCOLOGY (BRAIRCH) | JAN'2016 |
| 143 | MEETU DAHIYA | LAB. ONCOLOGY (BRAIRCH) | JUL'2016 |
| 144 | JAY SINGH | LAB. ONCOLOGY (BRAIRCH) | JAN'2017 |
| 145 | RAHUL KUMAR | LAB. ONCOLOGY (BRAIRCH) | JUL'2018 |
| 146 | ATUL BASNAL | LAB. ONCOLOGY (BRAIRCH) | JUL'2018 |
| 147 | HARSHITA DUBEY | LAB. ONCOLOGY (BRAIRCH) | JAN'2020 |
| 148 | NEETU RAWAL | LAB. ONCOLOGY (BRAIRCH) | JAN'2020 |
| 149 | HARSH GOEL | LAB. ONCOLOGY (BRAIRCH) | JAN'2020 |
| 150 | SUPRIYA AWASTHI | LAB. ONCOLOGY (BRAIRCH) | JAN'2020 |
| 151 | AAFREEN KHAN | LAB. ONCOLOGY (BRAIRCH) | JUL'2020 |
| 152 | PREITY SHARMA | LAB. ONCOLOGY (BRAIRCH) | JUL'2020 |
| 153 | MERCILENA BENJAMIN | LAB. ONCOLOGY (BRAIRCH) | JAN'2021 |
| 154 | AVANISH KUMAR PANDEY | LAB. ONCOLOGY (BRAIRCH) | JAN'2021 |
| 155 | GADHA K LEONS | LAB. ONCOLOGY (BRAIRCH) | JAN'2022 |
| 156 | SHEIKH MOHAMMAD UMAR | MEDICAL ONCOLOGY | JAN'2020 |
| 157 | CHRISTINE MARIANNE WILSON | MEDICAL ONCOLOGY | JAN'2020 |
| 158 | RAVI CHAUHAN | MEDICAL ONCOLOGY | JAN'2020 |
| 159 | MOHINI MENDIRATTA | MEDICAL ONCOLOGY | JAN'2020 |
| 160 | ABHIRUP MUKHOPADHYAY | MEDICAL ONCOLOGY | JUL'2020 |
| 161 | DEEPAK GULWANI | MEDICAL ONCOLOGY | JUL'2020 |
| 162 | ASHNA GUPTA | MEDICAL ONCOLOGY | JUL'2020 |
| 163 | RIDHIMA GOEL | MEDICAL ONCOLOGY | JUL'2020 |
| 164 | ARUNDHATHI DEV J R | MEDICAL ONCOLOGY | JUL'2020 |
| 165 | AKANKSHA KASHYAP | MEDICAL ONCOLOGY | JUL'2021 |
| 166 | HARSHUL KAPOOR | MEDICAL ONCOLOGY | JAN'2022 |
| 167 | SAHIL | MEDICAL PHYSICS (IRCH) | JAN'2018 |
| 168 | ASHISH BINJOLA | MEDICAL PHYSICS (IRCH) | JAN&JUL'2019 |
| 169 | V DHARUMAN | MEDICAL PHYSICS (IRCH) | JAN'2021 |
| 170 | AKANSHA PURI | MICROBIOLOGY | JAN&JUL'2019 |
| 171 | DEEPAK KOCHER | MICROBIOLOGY | JAN'2021 |
| 172 | SONAKSHI GUPTA | MICROBIOLOGY | JAN'2021 |
| 173 | LATA KUMARI | MICROBIOLOGY | JAN'2022 |
| 174 | INDU KAPOOR | NEUROANESTHESIOLOGY & CRITICAL CARE, NEUROSCIENCES CENTRE | JAN&JUL'2019 |
| 175 | PRERNA BALI | NEUROLOGY | JAN'2016 |
| 176 | JYOTI SHARMA | NEUROLOGY | JAN&JUL'2019 |
| 177 | ANANDAPADMANABHAN R | NEUROLOGY | JAN&JUL'2019 |
| 178 | ARTI SAINI | NEUROLOGY | JAN&JUL'2019 |
| 179 | CHHAVI SHARMA | NEUROLOGY | JUL'2020 |
| 180 | SHWETA SAHNI | NEUROLOGY | JUL'2021 |
| 181 | APHRODITE CHAKRABORTY | NEUROLOGY | JUL'2021 |
| 182 | ALISHA REYAZ | NEUROLOGY | JAN'2022 |
| 183 | JYOTSNA SINGH | NEUROPATHOLOGY LABORATORY (NSC) | JAN'2020 |
| 184 | BANDANA JASSAL | NEUROPATHOLOGY LABORATORY (NSC) | JAN'2020 |
| 185 | IMAN DANDAPATH | NEUROPATHOLOGY LABORATORY (NSC) | JAN'2020 |
| 186 | AGRIMA SHARMA | NEUROPATHOLOGY LABORATORY (NSC) | JAN'2020 |
| 187 | RITUPARNA CHAKRABORTY | NEUROPATHOLOGY LABORATORY (NSC) | JAN'2022 |
| 188 | RAFAT MALIK | NEUROPATHOLOGY LABORATORY (NSC) | JAN'2022 |
| 189 | PRIYA SHARMA | NEURO-PSYCHOLOGY | JUL'2020 |
| 190 | KAVERI SHARMA | NEURO-SURGERY | JAN'2020 |
| 191 | RAJESH KUMAR MISHRA | NUCLEAR MAGNETIC RESONANCE (NMR) | JUL'2016 |
| 192 | ANKITA SINGH | NUCLEAR MAGNETIC RESONANCE (NMR) | JUL'2017 |
| 193 | PANKAJ | NUCLEAR MAGNETIC RESONANCE (NMR) | JAN'2020 |
| 194 | CHETNA BANGA | NUCLEAR MAGNETIC RESONANCE (NMR) | JAN'2020 |
| 195 | HIMANSHU SINGH | NUCLEAR MAGNETIC RESONANCE (NMR) | JUL'2020 |
| 196 | VISHWA | NUCLEAR MAGNETIC RESONANCE (NMR) | JUL'2020 |
| 197 | NISHA CHAUHAN | NUCLEAR MAGNETIC RESONANCE (NMR) | JUL'2021 |
| 198 | NARESH KUMAR | NUCLEAR MEDICINE | JUL'2020 |
| 199 | SONA DHARMENDRA | OBST. & GYNAECOLOGY | JUL'2018 |
| 200 | SPONDITA BANERJEE | OBSTETRICS & GYNAECOLOGY | JAN'2022 |
| 201 | SANA NAFEES | OCULAR BIOCHEMISTRY (RPC) | JAN'2021 |
| 202 | POOJA | OCULAR BIOCHEMISTRY (RPC) | JUL'2021 |
| 203 | JAYANTI JHA | OCULAR PATHOLOGY (RPC) | JUL'2018 |
| 204 | NIKHIL KUMAR | OCULAR PATHOLOGY (RPC) | JAN'2021 |
| 205 | ANANNYA TULI | OCULAR PHARMACOLOGY | JUL'2020 |
| 206 | TAPAS KUMAR ROY | OCULAR PHARMACOLOGY | JUL'2020 |
| 207 | NIHAL SINGH | OCULAR PHARMACOLOGY (RPC) | JAN'2022 |
| 208 | NANDYALA SUSHMA | OPHTHALMOLOGY (RPC) | JUL'2020 |
| 209 | SRIDEVI NAIR | OPHTHALMOLOGY (RPC) | JAN'2021 |
| 210 | SHIVAM SHARMA | OPHTHALMOLOGY (RPC) | JUL'2021 |
| 211 | VINAY GUPTA | OPHTHALMOLOGY (RPC) | JUL'2021 |
| 212 | ABHISHEK YADAV | OPHTHALMOLOGY (RPC) | JUL'2021 |
| 213 | KASHISH | PAEDIATRIC SURGERY | JUL'2020 |
| 214 | PRABUDH GOEL | PAEDIATRIC SURGERY | JUL'2020 |
| 215 | KANA RAM JAT | PAEDIATRICS | JAN'2020 |
| 216 | AKHILA SANKAR | PAEDIATRICS | JUL'2020 |
| 217 | ARNAB NANDY | PAEDIATRICS | JAN'2021 |
| 218 | HARSHITA MAKKAR | PAEDIATRICS | JAN'2022 |
| 219 | SHRUTI KAHOL | PATHOLOGY | JUL'2018 |
| 220 | MONIKONGKONA BORUAH | PATHOLOGY | JAN'2020 |
| 221 | LALITA MEHRA | PATHOLOGY | JAN'2020 |
| 222 | TRISHLA JADON | PATHOLOGY | JAN'2020 |
| 223 | POOJA YADAV | PATHOLOGY | JUL'2020 |
| 224 | AMBER RATHOR | PATHOLOGY | JUL'2020 |
| 225 | ANSH GOSWAMI | PATHOLOGY | JUL'2020 |
| 226 | MUZAMIL AHMAD MIR | PATHOLOGY | JUL'2020 |
| 227 | WARISA KHATOON | PATHOLOGY | JAN'2021 |
| 228 | SURABHI JAIN | PATHOLOGY | JAN'2022 |
| 229 | HIMANSHU | PATHOLOGY | JAN'2022 |
| 230 | NITIKA LANGEH | PEDIATRICS | JUL'2017 |
| 231 | BRIJESH KUMAR | PEDIATRICS | JUL'2018 |
| 232 | SHALINI RAWAL | PHARMACOLOGY | JUL'2017 |
| 233 | POORVA BHARGAVA | PHARMACOLOGY | JAN'2018 |
| 234 | SADIA SHAH | PHARMACOLOGY | JAN'2018 |
| 235 | PAMILA DUA | PHARMACOLOGY | JUL'2018 |
| 236 | JATIN SHARMA | PHARMACOLOGY | JAN&JUL'2019 |
| 237 | SOUMYA SUCHARITA PATTNAIK | PHARMACOLOGY | JAN&JUL'2019 |
| 238 | ANIL KUMAR SAHU | PHARMACOLOGY | JAN&JUL'2019 |
| 239 | HIMANSHU SHARMA | PHARMACOLOGY | JAN&JUL'2019 |
| 240 | DIKSHA | PHARMACOLOGY | JUL'2020 |
| 241 | DEEKSHA SHARMA | PHARMACOLOGY | JUL'2020 |
| 242 | VANI VISWANATHAN | PHARMACOLOGY | JAN'2021 |
| 243 | ARTI | PHARMACOLOGY | JUL'2021 |
| 244 | R.PRATHIBAN | PHYSIOLOGY | JAN'2015 |
| 245 | MEGHA SHREE SAMPATH | PHYSIOLOGY | JUL'2016 |
| 246 | NABA SAMI | PHYSIOLOGY | JUL'2018 |
| 247 | CHAITHANYA LEON | PHYSIOLOGY | JUL'2018 |
| 248 | SAKSHI | PHYSIOLOGY | JUL'2018 |
| 249 | ANKIT | PHYSIOLOGY | JAN&JUL'2019 |
| 250 | SUNIL | PHYSIOLOGY | JAN&JUL'2019 |
| 251 | PRITIKA DUTTA | PHYSIOLOGY | JAN&JUL'2019 |
| 252 | JEEVITHA POORASAMY | PHYSIOLOGY | JAN'2020 |
| 253 | SWARNABHA SARKAR | PHYSIOLOGY | JAN'2020 |
| 254 | SAMREEN FATIMA | PHYSIOLOGY | JAN'2020 |
| 255 | SHWETA | PHYSIOLOGY | JUL'2020 |
| 256 | GUNJAN SHARMA | PHYSIOLOGY | JUL'2020 |
| 257 | AASHEESH KUMAR | PHYSIOLOGY | JAN'2021 |
| 258 | GARIMA SHARMA | PHYSIOLOGY | JAN'2021 |
| 259 | GAURAV SAINI | PHYSIOLOGY | JUL'2021 |
| 260 | DEEKSHA PATEL | PHYSIOLOGY | JUL'2021 |
| 261 | MOHAMMAD SHADAB ALI | PMSD (PULMONARY MEDICINE AND SLEEP DISORDERS) | JAN'2020 |
| 262 | DIVYANJALI RAI | PMSD (PULMONARY MEDICINE AND SLEEP DISORDERS) | JAN'2021 |
| 263 | JAYA TAK | PMSD (PULMONARY MEDICINE AND SLEEP DISORDERS) | JAN'2022 |
| 264 | SANIMAR KOCHHAR | PSYCHIATRY | JAN'2017 |
| 265 | SALONI DANG | PSYCHIATRY | JUL'2018 |
| 266 | NIKITA BHATI | PSYCHIATRY (CLINICAL PSYCHIATRY) | JAN'2016 |
| 267 | DEBABANI BHATTACHARYA | PSYCHIATRY (CLINICAL PSYCHOLOGY) | JAN'2015 |
| 268 | CHANDAN J. DAS | RADIODIAGNOSIS | JAN'2018 |
| 269 | JAGANMOY CHOUDHURY | REPRODUCTIVE BIOLOGY | JAN'2017 |
| 270 | PALAK SINGH | REPRODUCTIVE BIOLOGY | JUL'2017 |
| 271 | NEHA KAUSHIK | REPRODUCTIVE BIOLOGY | JUL'2018 |
| 272 | RANJANA RANA | REPRODUCTIVE BIOLOGY | JAN&JUL'2019 |
| 273 | KANIKA | REPRODUCTIVE BIOLOGY | JAN&JUL'2019 |
| 274 | SOUMYA RASTOGI | REPRODUCTIVE BIOLOGY | JAN&JUL'2019 |
| 275 | PRIYAL SHARMA | REPRODUCTIVE BIOLOGY | JAN&JUL'2019 |
| 276 | NITESH KUMAR | REPRODUCTIVE BIOLOGY | JAN&JUL'2019 |
| 277 | PRAMILA | REPRODUCTIVE BIOLOGY | JAN&JUL'2019 |
| 278 | JALA MOSES AZARAIAH | REPRODUCTIVE BIOLOGY | JUL'2020 |
| 279 | A MUNI NAGESH | REPRODUCTIVE BIOLOGY | JAN'2021 |
| 280 | NISHA SHARMA | REPRODUCTIVE BIOLOGY | JAN'2021 |
| 281 | KAJAL SIHAG | REPRODUCTIVE BIOLOGY | JUL'2021 |
| 282 | AAYUSHI TANEJA | REPRODUCTIVE BIOLOGY | JAN'2022 |
| 283 | YASHVI SHARMA | STEM CELL | JAN'2020 |
| 284 | E PRANSHU RAO | STEM CELL | JUL'2020 |
| 285 | MEENAKSHI MENDIRATTA | STEM CELL | JUL'2021 |
| 286 | NIDA MIR | SURGERY (JPNATC) | JAN'2022 |
| 287 | GOPIKA GUPTA | TII (TRANSPLANT IMMUNOLOGY & IMMUNOGENETICS) | JAN'2016 |
| 288 | PAWANDEEP KAUR | TII (TRANSPLANT IMMUNOLOGY & IMMUNOGENETICS) | JUL'2017 |
| 289 | AKANKSHA SHARMA | TII (TRANSPLANT IMMUNOLOGY & IMMUNOGENETICS) | JUL'2017 |
| 290 | CHAVAN NITIN LAXMAN | TII (TRANSPLANT IMMUNOLOGY & IMMUNOGENETICS) | JAN'2018 |
| 291 | MICHAEL JOHN KANIAMPARAMPIL | TII (TRANSPLANT IMMUNOLOGY & IMMUNOGENETICS) | JAN&JUL'2019 |
| 292 | GIRIJA MEHTA | TII (TRANSPLANT IMMUNOLOGY & IMMUNOGENETICS) | JAN&JUL'2019 |
| 293 | PARIKSHIT SANYAL | TII (TRANSPLANT IMMUNOLOGY & IMMUNOGENETICS) | JAN'2020 |
The Academic Section develops policy, plans and executes academic activities in pursuance of the objective of the Institute as enshrined in AIIMS Act, 1956.The objective of the Institute is to develop patterns of teaching in the Undergraduate and Postgraduate medical education in all its branches so as to demonstrate a high standard of medical education to all other medical colleges and other allied institution in India, to bring together in one place educational facilities. These activities encompass the undergraduate, postgraduate and doctoral programmes for medical, nursing and paramedical courses. These activities are conducted by the undergraduate, postgraduate and paramedical cells of Academic Section.
The Department functions under the Administrative Control of Dean (Academic) supported by Associate Dean (Academic) and Registrar.
(Rules as per record maintained in Academic Section shall prevail in case of any discrepancy)
The department of Anatomy, one of the first departments to be set up, has contributed to the development of Anatomy curriculum which is implemented throughout the country by the Medical Council of India. Research and publications from this department have often been quoted in the bible of Anatomy- i.e, Gray’s Textbook of Anatomy.
The department is involved in medical teaching and training at the undergraduate, postgraduate and doctoral levels and also provides services that include diagnostics in genetic disorders and fluorosis. It runs a National Centre for Electron microscopy that regularly provides training for technicians and investigators. The department is a WHO-recognized Centre for training in Human Genetics. The department is also an active collaborator and organizer of various cadaveric workshops for post-graduate training and skills training in surgical and allied disciplines.
The main thrust areas of research in the department are neurobiology, male and female infertility, auditory and visual pathways, ageing-related disorders, pain biology, addiction genetics, pre-ecclampsia, enteric nervous system, pancreatitic pathogenesis, morphometry using state-of-the-art design-based stereology, autophagy and cell death, rare and common genetic disorders, ecotoxicology, breast cancer, nanobiology and drug-delivery systems, plastination and cancer biology including rare endocrine tumours.
The department provides training opportunities and support in the fields of Anatomical sciences, Genetics and Electron Microscopy to all Indians and nationals of SAARC countries.





“We care-when you are unaware”
All-India Institute of Medical Sciences, New Delhi, was founded by an act of Parliament by Government of India in 1956, with the objective to develop patterns of training in undergraduate and postgraduate medical education in all its branches so as to demonstrate a high standard of medical education to all medical colleges and other allied institutions in India; to bring together in one place educational facilities of the highest order for the training of personnel in all important branches of health activity; and to attain self-sufficiency in postgraduate medical education. Anaesthesiology was one of the main Clinical Departments to achieve the objectives and mandate of the Institute.
The Department of Anaesthesiology started in 1956, with two operation theatres and ICU in an “Old Operation Theatre” block under the leadership of Col. G.C.Tandon (1958-1970).
In 1958, Professor (Lt. Col.) G.C. Tandon was deputed to All India Institute of Medical Sciences and he was the Founder Professor and first Head of the Department of Anaesthesiology and also as a Medical Superintendent of AIIMS Hospital. Prof. Tandon was responsible for recognition of Anaesthesiology as a broad specialty related to Medicine and start for the first time M.D. (Anaesthesiology) training programme in 1959. This pattern has been nationally accepted. His efforts led to recognition of Anaesthesiology as an independent speciality related to Medicine by Medical Council of India in 1959, leading to creation of independent Departments and Professorships in most Medical Colleges. Prof. Tandon was the First President of Delhi Society of Anaesthesia in 1961, which was the forerunner of the present ISA Delhi branch. In 1964, Prof. Tandon was elected as the President of Indian Society of Anaesthetists at the last joint conference with Association of Surgeons in Bombay. He was the Editor of Indian Journal of Anaesthesia for a number of years.
In 1964, the Department’s administrative offices were shifted to “Teaching block”, 5th floor East wing, and the operation theatres were shifted to C & D blocks of 8th floor (12 operation theatres) in 1969.
The Department was subsequently headed by Prof. G.R. Gode (1970-1988). Prof. G.R. Gode joined the AIIMS Faculty in 1966 and rose to the post of Associate Professor and took over as Head of the Department in 1970 from Col. G.C. Tandon. He was elevated to the post of Professor in Anaesthesiology in 1975. He took active interest in the clinical trials in the management of human rabies. Due to him in 1979, the Australasian International Conference was held in A.I.I.M.S, New Delhi. He was honored as an Emeritus Scientist by the ICMR. Professor G.R. Gode retired on 31st March, 1988 after 34 years of an illustrious career as one of the pioneer Anaesthesiologist of the country.
Although Dr. V. A. Punnoose didn’t head the department, but his contribution in developing the department are tremendous. He did MD (Anaesthesia) at AIIMS in May 1967 and subsequently joined as faculty. Dr. Punnoose was a rare example of dedicated teacher. He was above all, a very honest, sincere and good human being. Dr. Punnoose was very accessible, friendly and always available for help without any hesitations or preconditions. He used to be seen in operation theatre complex almost 24 hours a day including holidays and weekends. His contribution to the teaching was phenomenal. His contribution to the research for the department was unforgettable. Dr Punnoose devoted his full time attention to setting up anaesthetic services in the cardiac center. He was one of the pioneer in this field and established standards of practice which was followed by a number of departments which came up later in both government and private sector. He resigned the faculty position at AIIMS in 1983. His popularity among the students was so great that even after retirement from the institute; he was mobbed by them whenever or wherever they got a chance to meet him.
Till 1984, services to all subspecialties of Anaesthesiology (Cardiothoracic-vascular, Neuro-anaesthesiology and Institute Rotary Cancer Hospital) were supported by the staff of the main Department in addition to their own staff till they established themselves.
Prof. H. L. Kaul (1988-2004), took over as HOD from Professor G.R.Gode. He is the first postgraduate student of the Department who became Head of the Department in1988. He post-graduated from AIIMS. in 1970 and joined as a Faculty in September, 1971. He is the founder member of the Research Society of Anaesthesiology and Allied Sciences (RSAAS) and Research Society of Anaesthesiology and Clinical Pharmacology. The Journal of Anaesthesiology and Clinical Pharmacology was started by him. He was the Chief Editor of the Journal till December1999. He was one of the founder member of the South Asian Confederation of Anaesthesiologists (SACA) and Asian and Oceanic Society of Regional Anaesthesia (1999-2001) and was holding important portfolios of other societies. He had conducted several National and International Workshops, Conferences and Congresses.
Prof. Chandralekha (2004-2006 and 2007-2015), took over from Prof. Kaul in April 2004. She was instrumental in upgrading the AB8 ICU and AB8 Recovery Area. She also started state of the art Human Anaesthesia Simulator training courses. She conducted successful three ‘ “International Conferences on Recent advances in Anaesthesia and Analgesia (INCRAA)”.
Prof. Ravi Saksena (2006-2007) headed the department for a very brief period, but during this period he started Anaesthesia Services in JPNA Trauma center. He was the Chairperson for Emergency Response Centre and also started Course on “Life Saving AnaesthesiaSkills” training (Ministry of Health & Family Welfare) for the doctors posted in peripheral areas.
Prof. M. K. Arora, retired on the 31st of October 2017, he had taken over as Head of Department in March 2015. During his tenure as HOD, the Department was renamed as Department of Anaesthesiology, Pain Medicine and Critical Care and the DM Critical care programme was started. Anaesthesia services were expanded to support operations in the Centre for Dental Education and Research (CDER), in the GE Endoscopy area and Dr Rajendra Prasad Centre for Ophthalmic Sciences Casualty OT (for EUAs in children). Training sessions for OT Technicians were started. The Department strength increased to 39 faculty members.
The Department was headed by Prof Ravinder Batra till August 31st 2018. From 1st August 2018, Dr Rajeshwari Subramaniam has taken over the charge of the Department and headed the department till February 2022. Prof. Lokesh Kashyap took the charge of head of the department on 1st March 2022 and he is present leading the department.
The Department organized the annual IAPA conference, Ultrasound conference, Post Graduate Assembly, Critical Care update on Mechanical ventilation from Nov 2018 up to mid-2019. The Department was heavily damaged by fire in August 2019, which forced the Faculty to abandon their offices. The porta cabin rooms in the PAC clinic area were equipped with internet and appropriate office furniture and the Department operated from there till May 2020. At the peak of COVID epidemic the Department was cleaned by staff themselves, and by August 2020 the Department could shift back to the original office. Meanwhile, Prof. Maya superannuated on May 2021.
The Department was given additional charge of managing the COVID-suspect patients , and ultimately hundreds of critically ill COVID- 19 patients in C6, D6 and AB6 which was accomplished in a smooth and efficient manner.
At present, the Department provides protocolled anaesthesia and ICU services to General Surgery, Obstetric and Gynaecology, IVF, ENT, Orthopaedics, Urology, Paediatric Surgery, GI surgery, RP Centre of Ophthalmic theatres, CDER (Oral and Maxillofacial surgery) and JPNA Trauma centre; it also provides peripheral anesthesia services to interventional radiology, MRI, CT scan, ECT, acute and chronic pain services, resuscitation and obstetric analgesia services. Anaesthesia & intensive care services were extended to the newly functional Burn & Plastic Surgery block and Surgical block.
Over the years, along with the development of Medical Sciences, the Department has set up its own high standards in patient care, education and research. All operation theatres are equipped with state of the art anaesthesia machines, facilities for invasive blood pressure and CVP monitoring, Entropy and BIS monitoring and coagulation monitoring and rapid fluid infuser for major surgery and ultrasonography for regional anesthesia blocks and for vascular access.
Intensive Care Unit (AB 8 ICU) at 8th floor, adjoining operation theatre is equipped with modern ventilators, multiparameter monitors, ultrasonography, and echocardiography machine and, a dedicated laboratory. The ICU caters to post surgical and medical patients. The department has also purchased and installed the latest version of ECMO machine. The first ECMO was carried out in last week of February.
The AB8 post anesthesia recovery room (PACU) is the one of the state of the art recovery room and is equipped with multi-parameter monitors, patient controlled analgesia (PCA)/opioid infusion pumps, anaesthesia machine and defibrillator machine for emergency requirement.
Pre-Anaesthesia Check-up (PAC) Clinic: Referred patients scheduled for surgical/investigative procedures are screened in the PAC Clinic which is located in room no 4 / 5, 4th floor Porta Cabin OPD block from 2pm to 5pm on every Monday, Wednesday and Friday with prior appointment. From 15th January, 2018, onwards, PAC Clinic will be functional from 9am to 12 noon five days a week i.e., Monday to Friday.
Pain Clinic: Patients suffering from Acute and Chronic pain are referred in this Clinic for treatment. This Clinic is situated AB 7 ward (7th Floor) “Pre Anaesthesia Room” (PAR) area, from 2pm to 5pm on every Monday, Wednesday and Friday. In the pain clinic, facilities for various modalities of pain therapy viz., radio-frequency ablation, neurolytic block, TENS, Acupuncture, Acupulsor, etc. are available. Image guided interventional pain management procedures are carried out once a week (Thursday) in the operation theatre.
Research Society of Anaesthesiology and Allied Sciences (RSAAS): The mandate of this society is to promote research and academics among the faculty and residents of the department.
The Department started “Research Society of Anaesthesiology & Clinical Pharmacology’in 1982 under the leadership of Prof. H.L. Kaul. Subsequently, “Journal of Anaesthesiology and Clinical Pharmacology” was started with Prof. H. L. Kaul as a Chief Editor, this was being published and edited for many years from the Department of Anaesthesiology.
Department regularly conducts National & International conferences, workshops and Continuous Medical Education programs.
Postgraduate course (MD) is of three years duration and includes a thesis. The selection of Junior Residents for post-graduates course is made twice a year i.e. in January and July. Diploma course in anesthesia is not available for this speciality. Apart from regular seats sponsored candidates from different states and countries are also allowed to join the course as per the rules of the institute. The selection is based on an All-India entrance examination.
All postgraduate students are rotated in all surgical specialties, Intensive Care, Pre Anesthesia clinics and Pain clinics. The Department has fixed guidelines for anaesthetic procedures to be undertaken and the curriculum planning for the junior residents. Thesis writing is mandatory for partial fulfilment for the final MD examination. AIIMS post graduate teaching is one of the best teaching programme which consists of seminars, journal clubs, case discussion, tutorials and Guest lectures (4 days a week), All Junior and Senior Residents take part in the didactic teaching activities regularly under the faculty moderation. This is in addition to daily teaching activity based on the cases conducted in the operation theatres & Intensive Care Unit.
Department runs a DM (Critical Care Medicine) residency program and its curriculum includes clinical rotation in the various intensive care units of the institute and a thrice weekly academic schedule.
The Department has got the latest “Human Simulator” and skill development lab for teaching and hands on training of anesthesia, vascular access, central neuraxial blockade, peripheral nerve blockade and emergency scenarios including CPR. The simulator is also used for teaching and assessing Non-Technical Skills (NTS).
The tenure of Senior Residency is of three-year duration, during which, Residents are rotated in all subspecialties and Intensive Care Unit for imparting excellent training in this specialty.
Prof. Rath has been instrumental in advancing cancer care, emphasizing the importance of research, education, and collaboration in tackling the challenges of cancer. His work often focuses on improving patient outcomes and integrating innovative approaches into clinical practice. He is recognized for his leadership in establishing cancer treatment protocols and promoting awareness about cancer prevention and early detection.
His contributions extend beyond clinical practice, involving active participation in academic and professional organizations dedicated to oncology. Through his efforts, he has helped shape the landscape of cancer treatment and research in India.

Professor Lalit Kumar is a distinguished oncologist and a leading expert in the field of cancer research and treatment in India. He is known for his work in medical oncology, particularly in the areas of hematologic malignancies and solid tumors. Under his leadership, the institute has focused on advancing cancer care through innovative research, patient-centric treatment protocols, and the integration of advanced technologies in oncology. His dedication to improving patient outcomes and his advocacy for cancer awareness make him a key figure in the oncology community.

Professor Sushma Bhatnagar is a renowned figure in the field of oncology, particularly known for her expertise in palliative care and pain management for cancer patients. She has been instrumental in advancing the practice of supportive and palliative care in India, focusing on improving the quality of life for patients facing serious illnesses.
Her advocacy for comprehensive cancer care and her commitment to training healthcare providers have significantly impacted the field, ensuring that patients receive holistic support throughout their treatment journey.




















Dr. Tushar Agarwal completed his graduation (M.B.B.S.) in 1998 from theUniversity College of Medical Sciences, Delhi University and PostGraduation in Ophthalmology (M.D.) from RP Centre, AIIMS in 2002.Hehas been on the faculty of the Dr. R.P. Centre for OphthalmicSciences, since September 2005, where he is currently working asAdditional Professor of Ophthalmology.
He completed his Senior Residency in 2005. His areas of specialization include Cataract, Cornea and Refractive Surgery. He has contributedseveral chapters to national and international books on ophthalmologyand published over 50 papers in international peer reviewed journals.His currently pursuing research in the areas of pediatric cataractsurgery, iris repair and reconstruction techniques ,Pterygiumand new techniquesof lamellar corneal surgery.
Currently he serves on the Editorial Board of the World Journal ofOphthalmology. He is/ has been a reviewer for the American Journal ofOphthalmology, British Journal of Ophthalmology, Ophthalmology,Journal of Cataract and Refractive Surgery and African Journal ofMicrobiology Research.He has been awarded the Indian National Sciences Academy (INSA) YoungScientist Medal for the Year 2004. He is the recipient of theAchievement Award and “Best of Show” Award by the American Academy ofOphthalmology. He was also awarded the ESCRS/Alcon video Prize forScientific Video by the European Society of Cataract and RefractiveSurgeons.
He can be reached at tusharagarwal[at]gmail[dot]com
Dr. Tushar Agarwal completed his graduation (M.B.B.S.) in 1998 from theUniversity College of Medical Sciences, Delhi University and PostGraduation in Ophthalmology (M.D.) from RP Centre, AIIMS in 2002.Hehas been on the faculty of the Dr. R.P. Centre for OphthalmicSciences, since September 2005, where he is currently working asAdditional Professor of Ophthalmology.
He completed his Senior Residency in 2005. His areas of specialization include Cataract, Cornea and Refractive Surgery. He has contributedseveral chapters to national and international books on ophthalmologyand published over 50 papers in international peer reviewed journals.His currently pursuing research in the areas of pediatric cataractsurgery, iris repair and reconstruction techniques ,Pterygiumand new techniquesof lamellar corneal surgery.
Currently he serves on the Editorial Board of the World Journal ofOphthalmology. He is/ has been a reviewer for the American Journal ofOphthalmology, British Journal of Ophthalmology, Ophthalmology,Journal of Cataract and Refractive Surgery and African Journal ofMicrobiology Research.He has been awarded the Indian National Sciences Academy (INSA) YoungScientist Medal for the Year 2004. He is the recipient of theAchievement Award and “Best of Show” Award by the American Academy ofOphthalmology. He was also awarded the ESCRS/Alcon video Prize forScientific Video by the European Society of Cataract and RefractiveSurgeons.
He can be reached at tusharagarwal[at]gmail[dot]com

Dr. Parijat Chandra completed his M.B.B.S. from the University College of Medical Sciences (UCMS), Delhi. He was awarded the Sridharan Gold medal in Anatomy, Sridharan Gold medal with distinction in Pharmacology; silver medals with distinction in Physiology, Biochemistry; and silver medal in Preventive & Social medicine. He was awarded silver medals for overall ranking in first and final MBBS.
He completed his M.D. (Ophthalmology) from the prestigious R.P. Centre, AIIMS in the year 2000. He was also awarded degree of D.N.B. (Ophthalmology) by National Board of Examinations. He completed his senior residency training in vitreoretinal surgery from R.P. Centre, AIIMS. Thereafter he joined the faculty in Dr. R.P. Centre, AIIMS and is currently working as Professor of Ophthalmology.
His key area of work is in research, management and surgery of paediatric vitreoretinal diseases, especially Retinopathy of Prematurity (ROP). He is a regular speaker at national and international conferences, and has 150+ peer-reviewed Pubmed indexed publications. He has been engaged in screening and management of ROP including ROP Surgery in AIIMS since last 24 years.
He has conducted nationwide ROP training workshops. He was Co-PI of the Sightsaver’s National ROP Project (2013-2016). He was organizing secretary of the 2nd World ROP Congress in New Delhi (2009) and Chief Scientific Program Coordinator of the 3rd World ROP Congress in Shanghai, China (2012). He organized the National ROP Summit supported by QEDJT (2013). He was awarded the prestigious Michael Trese Oration from the Indian ROP Society (2023) and ACOIN Felicitation Award (2016). He has been member of committees from NNF, WHO, RBSK Govt of India for formulation ROP related guidelines. He is member of the National ROP Task Force under the Ministry of Health and Family Welfare, Government of India.
He has been a coinvestigator in many multicentric international clinical trials like DEGAS, MONET, IMROP, MONET, SHIELD, RAINBOW. He mentors quality improvement teams in AIIMS and is AIIMS chapter leader at Institute of Healthcare Improvement USA at IHI.org.
Email: parijatchandra[at]gmail[dot]com

Chief
Dr. Rajendra Prasad Centre for Ophthalmic Sciences
All India Institute of Medical Sciences, New Delhi
Patents: Two
Diseases of the Retina, Vitreous and Uvea
Contact: 011- 26593188
26593094
Diseases of the Retina, Vitreous and Uvea
Contact: 011- 26593188
26593094


















































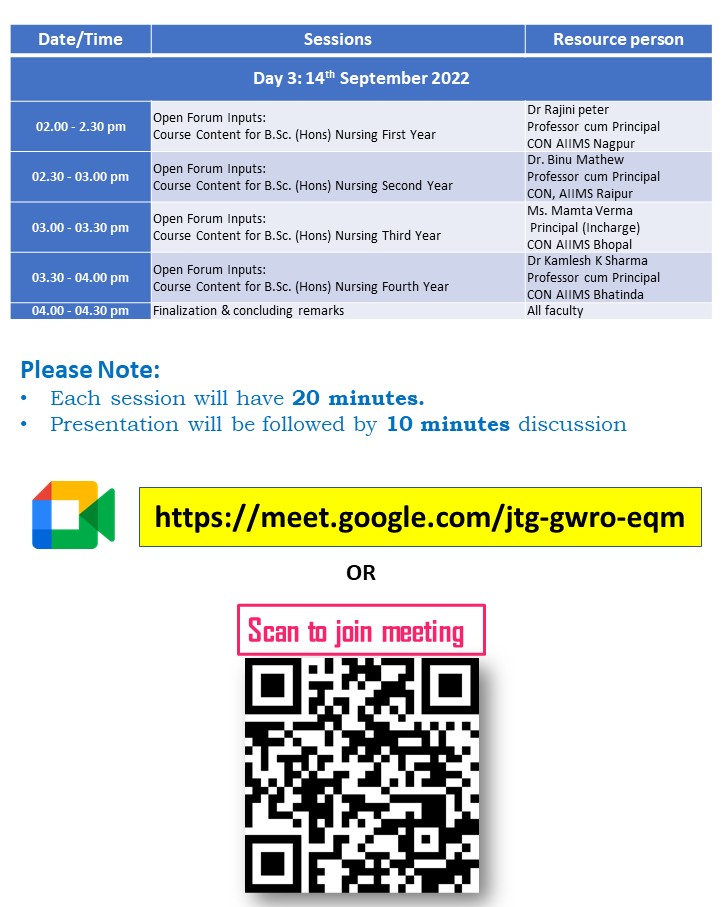
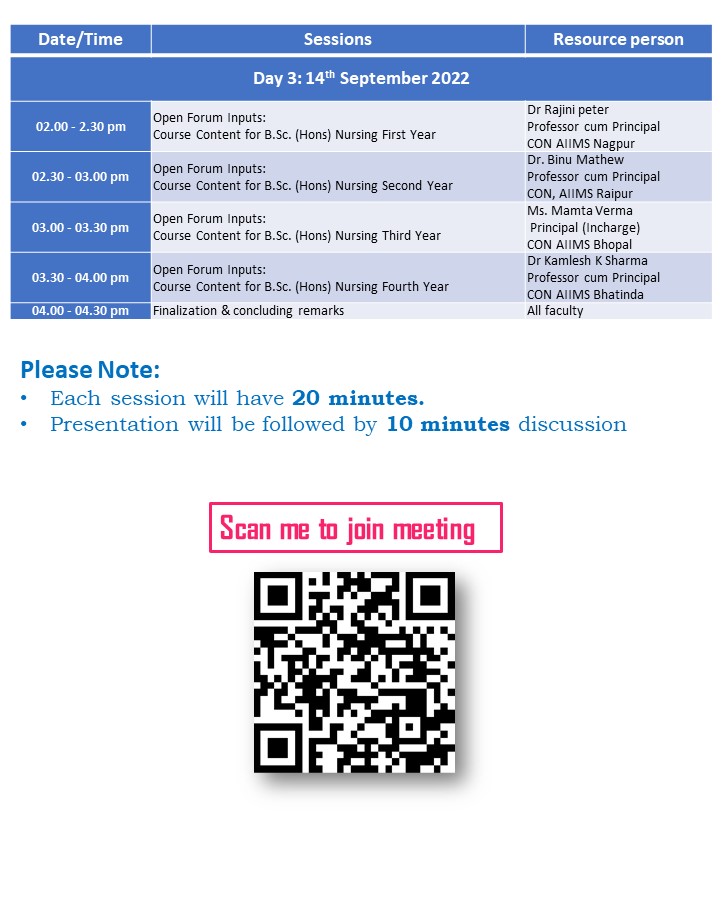
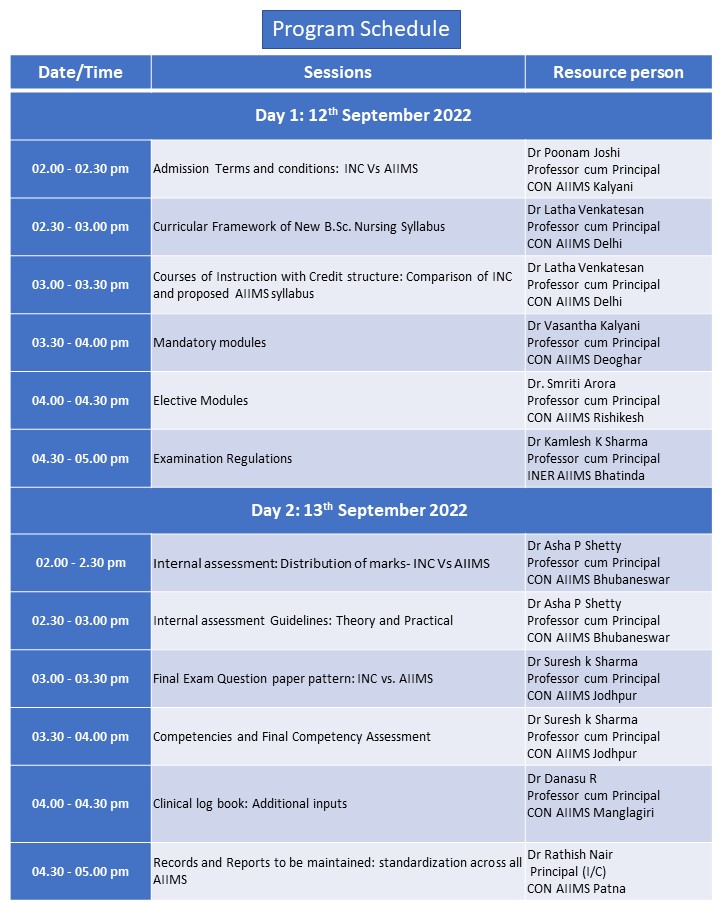
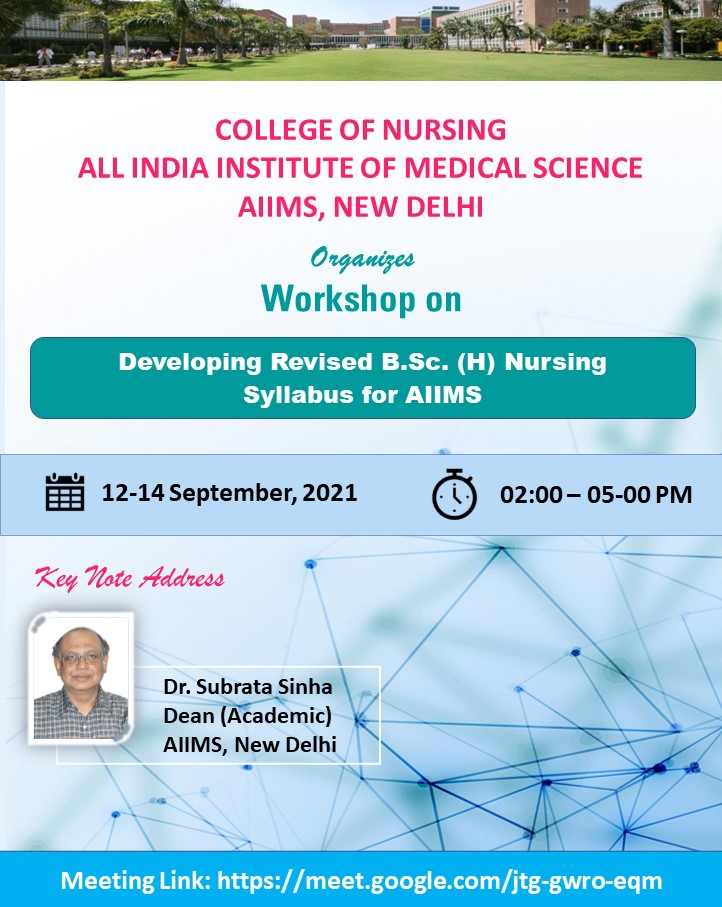






































DR. Rajendra Prasad Centre for Ophthalmic Sciences is the apex institute in India for ophthalmic care. Glaucoma facility is one of the main pillars of R P Centre. It has been providing the best and most advanced ophthalmic care to the patients for 45 years. Glaucoma being a silent thief of sight is a disease and our centre has taken equal effort and commitment of the ophthalmologist in educating the public about the disease and its consequences .
Our Glaucoma facility has a unique infrastructure and is able to provide a lifelong care and follow up to patients since they are enrolled in our glaucoma clinic. We have 3 eminent faculty members in charge of the glaucoma services, with 3 glaucoma clinics a week and a glaucoma facility lab which runs all week days. Our specialty glaucoma clinic on an average provides services to 2500 new patients and 6300 old patients. Residents assist the faculty members in providing necessary care to the glaucoma patients. The glaucoma lab has 3 optometrists trained in ophthalmic investigations, especially pertaining to glaucoma .
The faculty in new glaucoma clinic confirms the diagnosis of glaucoma and initiates the treatment for the patients who were screened and referred from outpatient department. These patients are then followed up in the old glaucoma clinic as required. The glaucoma lab has all the advanced diagnostic modalities namely HRT. GDx,HVF,GVF,OCT,ASOCT, UBM, tonometer,keratometer, pachymeter.
The eye health education unit of department is pro-actively engaged in developing IEC materials of common eye problem. Various IEC materials like small booklets, pamphlets, posters, Audio-visual movie pertaining to eye care have been developed. Community leaders, parents and guardians, school teachers are main target for eye health education. Community ophthalmology has initiated health education activities for patients utilizing out-patient and inpatient services at the institute. This is in addition to the already ongoing health education activities at the primary eye care clinics. The topics for health education are wide ranging such as general eye care, care of spectacles, refractive error, care after cataract surgery, glaucoma, retinoblastoma, retinopathy of prematurity etc. These are undertaken in conjunction with faculty and residents from respective sub-specialties, optometrists, nurses and medical social workers of RP Centre. Faculty from the department were involved in the NPCB program on sensitization of Doctors/Paramedics about the eye donation and its importance as well as the vital information related to eye donation and delivered talks on the same during the Eye Donation Fortnight 2020.
Cataract, Refractive Error, Presbyopia, General Eye Care, Conjunctivitis, Vitamin 'A', Eye Donation
Magnitude of Trachoma NPCB Survey (2014-2015)
Recent Contributions in Community Eye Health Research
RPC Model of Low Vision & Rehabilitation Services
Excellence in Primary Eye Care
Vision Delhi- A Primary Eye Cate Initiative (1st April to 31st March)
Health education booklet on PEC (http://www.aiims.edu/images/depart/RPC/Books/Booklet%20RPC-28%20June%202014%20Output.pdf)
The department is currently involved in The National Survey on Human Resources & Infrastructure for Paediatric Eye Care Services in India. As on 15th October 2020, there are nearly 10303 eye institutes in the entire country, out of which 8125 (78.9%) institutes have been contacted telephonically for participation in the HR survey. Out of them, completed responses have been received from 7200 institutes (Response Rate 88.6%) & about 2000 institutes were found to have paediatric oriented services (defined as paediatric OT facilities under general anaesthesia).
National Blindness Survey was completed in 30 districts and National Trachoma Survey in 24 districts in the country with support from National Programme for Control Blindness (NPCB), Government of India. Under the NBS and in each district, a sample of 3000 participants aged 50 years and above were enumerated and at-least 90% of them were examined across 50 clusters spread throughout the district. A GIS based map of each cluster covered was also being prepared. It was for the first time that an assessment of diabetic status and evaluation of patients (either newly diagnosed or previously diagnosed) for presence of Diabetic Retinopathy was also being done in a nation-wide manner. Each survey was facilitated and closely monitored by faculty from RP Centre at initiation, interim and towards the end of the survey which required 10-18 days of continuous field work. Emphasis was given for involvement of local medical colleges or renowned non-profit centres of Ophthalmology when doing the survey in a district. Over 93,000 participants were enrolled in the National Blindness Survey and over 25,00 children and 55,000 adults in the National Trachoma Survey.
Historically, the Community Ophthalmology department has been engaged in various national level blindness surveys, INDEYE and INDGEN studies on age related eye diseases and its genetic component in collaboration with LSH&TM, manpower and management training with Lions Club International Foundation, operational research studies with ORBIS, situational assessment of eye care infrastructure, Corneal Opacity Rural Epidemiological (CORE) study, North India Myopia Study (NIMS), training programs in primary eye care. Innovative tools such as the IND-VFQ, a National Surveillance Unit to assess the cataract surgical outcomes in country, IEC material on primary eye care were also developed and put into practice by the department. National agencies like ICMR, DST have been collaborated with in community based research work. Close collaborations have been developed with international agencies like World Health Organization, London School of Hygiene and Tropical Medicine UK, Wellcome trust, ORBIS, Sightsavers, Operation Eyesight Universal, CBM, Lions Clubs International Foundation etc.

Substance Use Prevention: Resource Material for Parents and Adolescents
The Drug Dependence Treatment Centre, AIIMS was established in the year 1988 and was functional from the premises of the Deen Dayal Upadhyay Hospital, New Delhi. In 2003 it was upgraded as the National Centre (National Drug Dependence Treatment Centre) and is fully operational from its new premises in Ghaziabad, Delhi-NCR since April 2003.
The National Drug Treatment Centre, Ghaziabad (NDDTC), AIIMS has been established as the apex centre for treatment of drugs and substance abuse disorders in the country. It provides a state of art model for de‐addiction treatments. This centre has full range of specialists & facilities. The NDDTC is situated on 10 acre beautiful campus near CGO Complex at Ghaziabad, Delhi-NCR. It is presently having 50 bedded treatment facilities with expansion plan for the future.
The centre has well qualified multi-disciplinary faculty and staff (medical doctors, pre-clinical scientists, social scientists, research staff, nursing staff, laboratory personnel and administrative staff) to render various modalities of care. Clinical care is provided through outpatient, inpatient settings and community clinics. Help is available for the treatment of disorders related to use of all the substances i.e. Alcohol, Opioids, Cannabis, Tobacco etc. and behavioral addictions. Treatment modalities include both pharmacological (i.e. with medications) and non-pharmacological (i.e. psychological / social) treatments. Both medically assisted and drug-free treatment related to drug use, and long-term supervised medications (Buprenorphine/Methadone/Naltrexone maintenance therapy) are provided. The centre carries out the relevant hematological, biochemical laboratory tests to monitor health damage. Further, several drugs of abuse are screened simultaneously through analysis of patients’ urine sample.
The centre has been involved in:
The centre provides clinical care to about 4000 new patients and about 35000 old patients every year. It also provides clinical care to about 33000 patients in its community clinic. In addition, every year about 600 patients are seen in Tobacco use cessation clinic, about 40 patients in adolescent clinic and about 300 patients in dual diagnosis clinic.
The years 1999-2012 saw much growth and many achievements for the centre. The centre has developed curricula, training schedules, modalities and resource materials for training of trainers, Medical Doctors (GDMOs), nurses and laboratory personnel. Between January 1989 and October 2007, about 40 courses for doctors have been organized. Various manuals for doctors are available. The training programmes have been reviewed and modified through workshops of resource persons.
Besides clinical care, NDDTC has been involved in a multitude of other areas. Right from its inception, NDDTC has played a leadership role in the country and has worked on development of various replicable models of care, training of post-graduate psychiatry students and health professionals, development of resource materials, research and policy planning.
Following is a brief overview of recent contributions:
Faculty members from NDDTC are members of various expert committees and technical groups at regional and international level, and contributing to policy development. The Ex-Chief of the Centre was a member of the International Narcotics Control Board (INCB), the monitoring body for the implementation of the United Nations international drug control conventions.
Project Number Research Section AIIMS: I-1391
IEC, AIIMS: Ethical Approval No. IEC-260/04.03.2022,RP-36/2022
The COVID-19 pandemic continues to inflict a heavy toll on the lives of the Indian population. The number of people infected as well as recovered from COVID-19 is unprecedented to date. There are non-specific reports of persisting symptoms in persons who have recovered from COVID-19 either short or long-term. The long-term consequence of COVID-19 is unknown and the information on late sequelae of COVID-19 is limited as of today. The current study is a community-based door-to-door study that will explore the pre-existing health impairments, including hypertension and diabetes before the pandemic, and post-covid 19 symptoms among participants living in the rural predominant districts. Furthermore, the study also aims to know the prevalence of COVID-19 disease, the death rate, and COVID-19 vaccination coverage in the country’s rural population. The second part of the study is to assess the post-COVID-19 symptoms, health problems and mortality following infection, and vaccination status among patients with a history of the disease.
Project Number Research Section AIIMS: I-1391
IEC, AIIMS: Ethical Approval No. IEC-260/04.03.2022,RP-36/2022
The COVID-19 pandemic continues to inflict a heavy toll on the lives of the Indian population. The number of people infected as well as recovered from COVID-19 is unprecedented to date. There are non-specific reports of persisting symptoms in persons who have recovered from COVID-19 either short or long-term. The long-term consequence of COVID-19 is unknown and the information on late sequelae of COVID-19 is limited as of today. The current study is a community-based door-to-door study that will explore the pre-existing health impairments, including hypertension and diabetes before the pandemic, and post-covid 19 symptoms among participants living in the rural predominant districts. Furthermore, the study also aims to know the prevalence of COVID-19 disease, the death rate, and COVID-19 vaccination coverage in the country’s rural population. The second part of the study is to assess the post-COVID-19 symptoms, health problems and mortality following infection, and vaccination status among patients with a history of the disease.
| Title | Download |
|---|---|
| In charge | Dr.T.Velpandian, Prof. of Ocul Pharmacology |
| Faculty | Dr. Nabanita Halder, Prof. of Ocul Pharmacology |
HPBAF - High Precision Bio-analytical Lab (DST-FIST grant)
MolDyne – Molecular Dynamics Lab
OcuCel- Cell culture facility for invitro drug screening
NODDL – Novel Ocular Drug Development Lab
ADD-FOND – Adv.DrugDelv. Fac. For Ocu. Neovascular Dis.
GLP-Disp - Pharmacy (IV-Parentral dispensing Facility)
| Student’s Name | Research topics |
|---|---|
| MadhuNath | Evaluation of the Role of Retinal Renin Angiotensin System (RAS) in the Animal Model of Retinopathy of Prematurity (ROP) |
| Hanuman Sharma | Functional Importance of Nucleoside Transporters in the Ocular Disposition of their Substrates |
| AnkitaKotnala | Evaluation of A2E Biological Functions Relevant to the Pathology of Age Related Macular Degeneration |
| Moksha Laxmi | Understanding the Drug Transporter Functions in Blood Ocular Barriers during ocular inflammation in the Experimental Models of Uveitis |
| Ujjwalkumar Das | Developing and validating QSPR model to define enhanced drug penetration across blood ocular barriers |
State-of-the-Art Facilities Available at Ocular Pharmacology and Pharmacy

Department of Ocular Pharmacology Research Contributions

Malachite Green Toxicity
First reported the Ocular toxicity of Malachite green in Holi color (Hindustan times March 2006)- J Hazard Mater. 2007
Ocular drug disposition studies in progress
Indian Solar Ultraviolet Radiation Assessment Project- ISUVRA under WHO-INTERSUN Project
Corneal angiogenesis model for screening antiangiogenis compounds
Ocular drug disposition studies using concentric microdialysis probe
CADD experiments with Androgen receptors
CADD experiment to design ocular specific FQ

HPBAF
Neo-vascular research

NODDL-Sterile facility

MOLDYN
Professor and In-charge of Ocular Pharmacology & Pharmacy

Dr. Thirumurthy Velpandian
Professor and In-charge of Ocular Pharmacology & Pharmacy
He has completed graduation in Pharmaceutical Sciences from Tamil Nadu Dr.MGR Medical University with a Distinction in Pharmacology. He pursued his post graduation in Drug Assay in Pharmacology and subsequently pursed PhD from All India Institute of Medical Sciences (AIIMS), New Delhi. He was awarded PhD in 1999 for his studies on liposome drug delivery to eye and its corneal interactions in which he has done a part of his study from the InstitutfürAnatomie und Zellbiologie - UniversitätWürzburg, Germany. After serving as a Senior Demonstrator and DST Young Scientist Project investigator at AIIMS in the Department of Pharmacology, he has joined as Assistant Professor of Ocular Pharmacology at Dr.RPCentre for Ophthalmic Sciences of AIIMS in 2003 at present he is the Professor and In-Charge of Ocular Pharmacology and Pharmacy Division.
He has been working on ocular pharmacokinetics with the special reference to the contribution of xenobiotic transporters in blood ocular barriers. He has been involved in developing animal models, drugs, their formulations and their delivery systems for ocular angiogenesis, infections, cataract and dry eye. His laboratory is also involved in studying ocular toxicity drugs, tear lipidomics, pharmacogenomics and ocular QSPR studies using molecular dynamics. His team was involved in addressing several environmental issues contributing towards ocular toxicity of chemical agents.
So far his research has been funded by extramural projects from DST, DBT, ICMR, MHFW, DRDO, AIIMS (intramural), Pharmaceutical companies in India and agencies from abroad. His laboratory has received Level I grant under DST-FIST program for High Precision Bioanalytical Facility (HPBAF) with tandem mass spectroscopy (LC-MS/MS).
He has had the honour of being invited to serve at various places in diverse capacities of speaker, moderator, Session Chairman, Academic Committee member, Technical expert, as well examiner in Biological and Pharmaceutical sciences. He has also been included as advisor and member in various committees of Govt.of India for making decision in drug & research related affairs time to time.
E-Mail:-: tvelpandian[at]hotmail[dot]com
Publications from our laboratory in PubMed (Ctrl + Click)
2014- Dr.Vinod Kumar Bhargava Award for Clinical Pharmacology and Drug Discovery by NAMS
2014- Editor (Pharmacology) , Indian Journal of Physiology and Pharmacology
2014- AIIMS Excellence Research Award – Commendation Certificate
2012- Visiting Professor – MIT- Harvard (Health Sciences and Technology)
2011- Visiting Faculty - BPKIHS, Nepal (Clinical Pharmacology)
2010- Nominated Member of the PG-Curriculum Review Committee of Sikkim University
CSIR ‘Senior Research Fellowship’,
ISER – Pharmacia International Travel Fellowship,
Servior Young Investigators Award,
| Total Publications | 107 |
| Publications in indexed journals | 101 |
| First and Corresponding Author | 38 |
| Un-indexed or in other database | 04 |
| Review articles | 02 |
| Chapters in book | 12 |
| Patents (published) | 05 |
| Patents under commercialization | 02 |
| Patent filed | 02 |
He has completed graduation in Pharmaceutical Sciences from Tamil Nadu Dr.MGR Medical University with a Distinction in Pharmacology. He pursued his post graduation in Drug Assay in Pharmacology and subsequently pursed PhD from All India Institute of Medical Sciences (AIIMS), New Delhi. He was awarded PhD in 1999 for his studies on liposome drug delivery to eye and its corneal interactions in which he has done a part of his study from the InstitutfürAnatomie und Zellbiologie - UniversitätWürzburg, Germany. After serving as a Senior Demonstrator and DST Young Scientist Project investigator at AIIMS in the Department of Pharmacology, he has joined as Assistant Professor of Ocular Pharmacology at Dr.RPCentre for Ophthalmic Sciences of AIIMS in 2003 at present he is the Professor and In-Charge of Ocular Pharmacology and Pharmacy Division.
He has been working on ocular pharmacokinetics with the special reference to the contribution of xenobiotic transporters in blood ocular barriers. He has been involved in developing animal models, drugs, their formulations and their delivery systems for ocular angiogenesis, infections, cataract and dry eye. His laboratory is also involved in studying ocular toxicity drugs, tear lipidomics, pharmacogenomics and ocular QSPR studies using molecular dynamics. His team was involved in addressing several environmental issues contributing towards ocular toxicity of chemical agents.
So far his research has been funded by extramural projects from DST, DBT, ICMR, MHFW, DRDO, AIIMS (intramural), Pharmaceutical companies in India and agencies from abroad. His laboratory has received Level I grant under DST-FIST program for High Precision Bioanalytical Facility (HPBAF) with tandem mass spectroscopy (LC-MS/MS).
He has had the honour of being invited to serve at various places in diverse capacities of speaker, moderator, Session Chairman, Academic Committee member, Technical expert, as well examiner in Biological and Pharmaceutical sciences. He has also been included as advisor and member in various committees of Govt.of India for making decision in drug & research related affairs time to time.
E-Mail: tvelpandian[at]hotmail[dot]com
Publications from our laboratory in PubMed (Ctrl + Click)
http://www.ncbi.nlm.nih.gov/pubmed/?term=velpandian+T+or+pandian+TV
2014- Dr.Vinod Kumar Bhargava Award for Clinical Pharmacology and Drug Discovery by NAMS
2014- Editor (Pharmacology) , Indian Journal of Physiology and Pharmacology
2014- AIIMS Excellence Research Award – Commendation Certificate
2012- Visiting Professor – MIT- Harvard (Health Sciences and Technology)
2011- Visiting Faculty - BPKIHS, Nepal (Clinical Pharmacology)
2010- Nominated Member of the PG-Curriculum Review Committee of Sikkim University
CSIR ‘Senior Research Fellowship’,
ISER – Pharmacia International Travel Fellowship,
Servior Young Investigators Award,
| Title | Download |
|---|---|
| Total Publications | 107 |
| Publications in indexed journals | 101 |
| First and Corresponding Author | 38 |
| Un-indexed or in other database | 04 |
| Review articles | 02 |
| Chapters in book | 12 |
| Patents (published) | 05 |
| Patents under commercialization | 02 |
| Patent filed | 02 |
No. F.35-1/90-Estt.II
13 OCT 2005
Sub:- Constitution of Central Grievance Committee at AIIMS
As per the directions issued by the Hon'ble High Court vide order number LPA-19156/2005 dated 22.09.2005 the Director AIIMS is pleased to constitute a Central Grievance Committee with the following faculty officers to attend to public grievances complaints about the functioning of AIIMS.
| 1. | Dean AIIMS | Chairman |
| 2. | Dr. R. Guleria. Prof. of Medicine | Member |
| 3. | Dr. M.C. Mishra Prof of Surgery | Member |
| 4. | Dr. N.R. Jagannathan Prof & HOD of NMR | Member |
| 5. | Prof. A.K. Mahapatra Prof of Neurosurgery | Member |
| 6. | Dr. D.K. Sharma Medical Superintendent | Member |
| 7. | Dr. R.B. Vajpayee Prof. of Opthalmology. Dr. R.P. Centre | Member |
| 8. | Dr. G.K. Rath Prof & Head of Radiotherapy, Dr. BR IRCH | Member |
| 9. | Administrative Officer (H) | Member Secretary |
The Central Grievance Committee will meet periodically to discuss the grievance complaints received form public and submit its Action Taken Report to the Director, AIIMS (ATTAR SINGH)
CHIEF ADMINISTRATIVE OFFICER
An act of Parliament in 1956 established a the All India Institute of Medical Sciences (AIIMS) as an autonomous Institution of national importance and defined its objectives and functions. By virtue of this Act, the Institute awards its own medical degrees and other academic distinctions. The degrees awarded by the Institute under this Act are recognised medical qualifications for the purpose of the Indian Medical Council Act and, notwithstanding anything contained therein, are deemed to be included in the first schedule of that Act, entitling the holders to the same privileges as those attached to the equivalent awards from other Universities of India.
Tentative Schedule of Entrance Examination for the Year 2013
The basic information regarding the programme details for admission to different programmes by the Institute are given in a tabular form. The same indicates the name, duration of the course, tentative month of the examination and its Admission Notice. The same are also published in leading Newspapers and AIIMS websites i.e. www.aiims.edu and www.aiims.ac.in
| S.No. | Name of Course | Eligibility | Duration | Month of Exam | Admission Notice |
|---|---|---|---|---|---|
| 1. | B.Sc. (Hons). Paramedical Course
| 10+2 or equivalent with 50% marks (45% for SC/ST) in English, Physics Chemistry Bio. or Maths | 3 Yrs. | June | March |
| 2. | B.Sc. (Hons). Nursing | 10+2 or equivalent with 50% marks (45% for SC/ST) in English, Physics Chemistry Bio. Age 17Yrs. above (for female candidates only) | 4Yrs. | June | March |
| 3. | B.Sc. (Hons). (Post Certificate) | 10+2 or equivalent Certificate in Gen. Nsg. Midwifery and be an 'A' Grade Nurse, registered with State Nurses Registration council. Minimum 3yrs. experience as a staff Nurse in a recognised hospital or as a public health nurse. | 2 Yrs. | June | March |
| 4.(i) | M.Sc. / M. Biotech (Anatomy, Biochemistry, Physiology, Pharmacology) | B.Sc. (Minimum 3 years duration in any subjects) B.V. Sc./B. Pharma with 60% marks (55% for SC/ST) OR MBBS/BDS with atleast 55% marks (50% for SC/ST) | 2 Yrs. | July | March |
| 4.(ii) | M.Sc. (Perfusion Technology) | B.Sc. with Biology or B.Sc. In Perfusion Technology from a recognised University. | 2 Yrs. | July | March |
| 4.(iii) | M.Sc. (Nuclear Medicine Technology) | B.Sc. In Nuclear Medicine from a recog. University OR B.Sc. with Physics/ Chemistry / Maths from a recognised University. OR B.Sc. in allied/related subject i.e. Radio Diagnosis (MRT) Radiotherapy from a recog. University. OR B.Sc. in Life Sc. with Physics as a subject from recognised University. | 2 Yrs. | July | March |
| 4.(iv) | M.Sc. (Urology Technology) | B.Sc. with Science (Biology Compulsory at 10+2 level) OR B.Sc. Theatre Technique. | 2 Yrs. | July | March |
| 4.(v) |
| B.Sc. (Hons.) Nursing, B.Sc. Nursing (PC)/ Post Basic from any recognised University with 60% marks (55% marks for SC/ST) | 2 Yrs. | July | March |
| 5. | MBBS | 10+2 or equivalent with 60% marks (50% for SC/ST) in English, Physics Chemistry Bio. Age: 17yrs.. as on 31st of December of the year of admission above | 5½ Yrs. | 1st. June | December |
| 6. | AIPGMEE MD/MS/MDS/ P.G. Diploma | MBBS/BDS OR Foreign Medical degree from a college recognised by MCI/DCI. Date of completion of internship (12 months) on or before 31st March or earlier. | 3 Yrs. from the date of admission | January | September |
| 7. | AIIMS-PG (MD/MS/MDS) | MBBS/BDS with 55% marks (50% for SC/ST) and must have completed 12 months compulsory internship in a recognised hospital. | 3 Yrs. | May November | March August |
| 8. | DM | MD in required speciality Age limit 35 yrs (5 yrs. relaxable for SC/ST) upper age limit is not applicable for sponsored candidates. | 3 Yrs. | June December | March August |
| 9.(i) | M.Ch. | MS in General Surgery of AIIMS OR any other University recognised by MCI Age limit: 35 yrs. relaxable for SC/ST) upper age limit is not applicable for sponsored candidates. | 3 Yrs. | June / December | March August |
| 9.(ii) | M.Ch. (6 yrs. course) | MBBS degree one year compulsory Internship with 55% marks in aggregate in all MBBS professional exams. The eligibility criteria are the same as specified for MD/MS (3 year course) | 6 Yrs. | June / December | March August |
| 10. | MHA | Medical Graduate: MBBS with 55% marks minimum 3 yrs. exp. in a recognised hospital OR 5 yrs. experience as Gen. Practitioner. Non Med. Graduates: Eligible for sponsored seat only Bachelor's degree in Arts or Science Nursing OR Business Admn. OR Commerce OR Engineering OR any Technical subject with atleast 60% marks. Experience of 7 yrs. in responsible Administrative position. | 2 Yrs. for Medical Graduates 3 Yrs. for non-Medical Graduates | June/ December June/ December | March August March August |
| 11. | Ph.D Admission to Ph.D. is subject to availability of research/ funds/fellowship/grant from recognised funding agencies. | M.Sc. OR Master Degree in any subject allied to Bio-Medical Sciences OR Master degree in Nursing with 60% marks. OR Master of Surgery OR Doctor of Medicine OR MBBS with a minimum of 55% marks. in the professional examinations OR an equivalent Degree OR Diplomat of the NBE. | 3-5 Yrs. | January / July | March August |
For enquiries, please contact:
Examination Section
All India Institute of Medical Sciences
Ansari Nagar, New Delhi - 11002
Tel: 2658 8500, 2658 8700, 2658 9900
Fax: 2658 8789
Email: kanil[dot]aiims[at]gmail[dot]com

M.B.,B.S.,- Madras Medical College ,Chennai.
M.D., - All India Institute of Medical Sciences, New Delhi.
D.N.B., - National Board of Examinations, New Delhi.
Pediatric Anesthesia.
Regional Anesthesia and Acute pain management.

Ophthalmic Anaesthesia, Pediatric Anaesthesia, Difficult Airway, Bariatric Anaesthesia, Obstetric Anaesthesia, Regional anaesthesia, Transplant Anaesthesia
| Total publications | 105 |
| Index publications | 90 |
| Chapter in books | 10 |
| Invited speakers in conferences | 50 |
Email :dilipshende[at]yahoo[dot]com
Mobile: 9868397820

Paediatric, Ophthalmic Anaesthesia, Orthopaedic and Regional anaesthesia, Thoracic anaesthesia, ENT and Major Head & Neck, General Surgery including Renal Transplant/Minimally invasive surgery, Gynaecology, Obstetrics, Intensive Care.
One year fellowship in the field of Obstetric Anaesthesia (1996)in United Kingdom.
I am having full GMC UK Registration and I am on Specialist Register UK.
Worked as Consultant anaesthetist (2011 Jan-2012Dec) with NHS UK.
I am interested in clinical research and have around 40 publications in various journals including British Journal of Anaesthesia, Anesthesiology,Anaesthesia ,Paediatric Anaesthesia. Presented research papers in many international conferences and delivered talks/Chaired sessions in many National conferences
E-mail: vgupta[at]aiims[dot]edu, drguptavivek[at]yahoo[dot]com
Phone: +91(11) 26594097, +91 9899410420

Ongoing Projects
| Sr | Title | Role | Period | Funding Agency |
|---|---|---|---|---|
| 1. | Epidemiological Study of Avoidable Blindness in India | Co-Investigator | 2015-2018 | MoHFW, Govt. of India |
| 2. | Retrospective and prospective audits of the phenotype, causes and correlates of Trichiasis-WHO Trachoma Collaborative Study | Co-Investigator | 2015-2018 | WHO |
| 3. | Patterns and pathways of care seeking for cataract and common ocular morbidities and impact of local volunteers on the pathways among urban vulnerable population settings of West Delhi | Principal Investigator | 2017-2019 | SSMI |
| 4. | Diabetic Retinopathy: An Epidemiological Study of its Risk Factors and Biological Markers in Delhi | Co-Investigator | 2017-2019 | MoHFW, Government of India |
| 5. | Multi-centric study of the impact of exposure to Ultra Violet Radiation (UVR), and aerosols exposure on ocular health in India | Co-Investigator | 2018-2023 | ICMR, Government of India |
| 6. | Health-Related Quality of Life and Costing of cataract surgery for treatment of age-related cataract in India | Co-Investigator | 2017-2018 | DHR, Government of India |
| 7. | To evaluate the effect of increased outdoor activity on the incidence and progression of myopia in school children | Co-Investigator | 2016-2018 | Department of Science and Technology |
| 8. | Development of a culturally appropriate health literacy instrument and assessing its validity in Hindi speaking patients receiving general and primary eye care services in New Delhi | Principal Investigator | 2016-17 | AIIMS Intramural |
| 9. | Operational research project on strengthening integrated primary eye care in urban vulnerable populations of Delhi | Co-Investigator | 2016-2018 | Sightsavers International |
| 10. | SNOMED-CT: NRCeS – Development of National Drug Repository database | Co-Investigator | 2017-2018 | MoHFW C-DAC Pune |
| 11. | Establishing a Technical Support Unit (TSU) for Verbal Autopsy based Cause of Death Ascertainment in the Sample Registration System, Registrar General of India - MINErVA - N1715 | Co-Investigator | 2017-2022 | Registrar General of India |
| 12. | Epidemiological study of Childhood Blindness in Delhi | PhD Thesis Co-Guide | 2016-2019 | PhD Thesis |
| 13. | Community based Operational Research Study on involvement of Accredited Social Health Activist (ASHAs) in Strengthening Primary Eye Care Services for Urban Vulnerable Population of Delhi | PhD Thesis Co-Guide | 2015-2019 | PhD Thesis |
| 14. | A Population based study to assess the prevalence of glaucoma in Delhi | PhD Thesis Co-Guide | 2017-2020 | PhD Thesis |
| 15. | Tools to Diagnose – Eye- Development and assessment of image analysis tool for identification of glaucoma | Principal Investigator | 2017- | PhD Collaborative IIT-Delhi |
| 16. | Tools to Diagnose – Eye- Development and assessment of image analysis tool for identification of DR | Co- Investigator | 2017- | PhD Collaborative IIT-Delhi |
| 17. | Comprehensive primary eye care services in rural areas of Delhi | Co- Investigator | 2017-2020 | DJJS |
| 18. | Vision Screening and Eyeglasses Dispensing Program for Students in Delhi Schools | Co- Investigator | 2017-2018 | VisionSpring |
| 19. | Community Ophthalmology Programme in South Delhi | Co- Investigator | 2017-2018 | Deepalaya |
| 20. | A Sustainable Model for Comprehensive Outreach Eye Care Service in NCR | Co- Investigator | 2017-2018 | Deepalaya |
| 21. | A Sustainable Model for Comprehensive Outreach Eye Care Service for underserved population in Delhi Slums and resettlement colonies | Co- Investigator | 2017-2018 | Deepalaya |
| 22. | A Sustainable Model for Comprehensive Outreach Eye Care Service in NCR | Co- Investigator | 2017-2018 | Hero Motocorp |
| 23. | A Sustainable Model for Comprehensive Outreach Eye Care Service for underserved population | Co- Investigator | 2017-2018 | Sparsh |
| 24. | A Community based Assessment of Disability among Adult Population in Delhi using WHO-ICF framework | Ph.D Thesis Co-Guide | 2019 | Ph.D Thesis |
PROGRAM
ABSTRACTS
Place: Department of Physiology, All India Institute of Medical Sciences
Time: November 3 to 7 2009

Dr. Suraj is a Professor working in Community Ophthalmology, at Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi. He has done his post-graduation in Community Medicine from PGIMER, Chandigarh, and completed a master’s degree in Public Health for Eye Care from the London School of Hygiene Tropical Medicine (LSHTM), London. He has extensively worked in assistive technology in collaboration with national and international organizations, including WHO. He is one of the expert members of the technical working of WHO, Geneva for redesigning the Rapid Assistive Technology Assessment (rATA) study tool. He has led the rATA study in India, supported by the WHO. He served as a technical expert and led the national monitoring unit of rATA India under ICMR, New Delhi Ministry of Health. He was also an expert observer in developing the National Assistive Products Priority List of India as well as finalizing the technical draft on India making a Global Hub for Assistive Technology of the Ministry of Health. He is serving as one of the key members of NCAHT (National Centre for Assistive Health Technology), AIIMS New Delhi funded by ICMR, New Delhi. He was also nominated as one of the members by AIIMS to visit Japan under the JICA-AIIMS medical devices program. He is an expert member of site inspection of those START-UP funded by DBT, Govt. of India. He has established the Vision Rehabilitation Training Centre in Dr. R.P.Centre and led a twinning Low Vision Rehabilitation program in Southeast Asia with support from the WHO Southeast Asia Regional Office. He also received the best government assistive initiative in the government sector organized by jointly AssiTech Foundation and IIT Madras. He is one of the key investigators for the National Blindness Survey supported by the Ministry of Health. He has received various awards, including oration at national and international conferences. He has published more than 100 research papers in national and international peer-reviewed indexed journals, 29 chapters, and 20 books, including various vision rehabilitation guides, and is a reviewer of regular of the Lancet Global Health. He served as Guest Academic Editor of Frontier in Public Health and PLoS One. He also chaired many national and international scientific conferences, including the Asia Pacific Academy of OPhthalmolgogy(APAO).
Senjam SS, Manna S, Bascaran C. Smartphones-Based Assistive Technology: Accessibility Features and Apps for People with Visual Impairment, and its Usage, Challenges, and Usability Testing. Clin Optom (Auckl). 2021;13:311-322
https://doi.org/10.2147/OPTO.S336361
Senjam S S, Balhara YPS, Kumar P. Assessment of Post COVID-19 Health Problems and Its Determinants in North India: A Descriptive Cross-Sectional Study. Available at SSRN: https://ssrn.com/abstract=3937558 or http://dx.doi.org/10.2139/ssrn.3937558
Senjam S.S. Smartphones as assistive technology for visual impairment. Eye (2021). https://doi.org/10.1038/s41433-021-01499-w
Senjam SS. Smartphones for Vision Rehabilitation. Accessible features and Apps, Opportunity, Challenges, and Usability Evaluation. IntechOpen: 200AD. DOI: http://dx.doi.org/10.5772/intechopen.97703 .
Email: praveenvashist[at]yahoo[dot]com

As Officer In-Charge of Community Ophthalmology at the apex ophthalmic institute of the country, I have been instrumental in developing models for community outreach services and strengthening epidemiological research and training in the field of community eye care. I have been Principal Investigator of 42 research and community eye care projects implemented in RP Centre in partnership with international, national organizations including WHO, NPCBVI, ICMR, DST, SightSavers, Operation Eyesight Universal, VisionSpring, ORBIS, LCIF and CBM. I have more than 80 publications in international and national peer-reviewed journals. I have delivered more than 300 lectures as resource person/faculty in conferences and CMEs organized at international and national level. I routinely provide technical assistance to NPCBVI and was appointed as Principal Investigator for the National Blindness Survey 2015-19 and National Trachoma Surveys 2014-17. As an outcome of this National Trachoma Survey, Government of India declared elimination of active trachoma among children in India. I have also been appointed by WHO as member of dossier review committee for elimination of Trachoma in Nepal and Myanmar. I have been involved in blindness control and rehabilitation activities with WHO SEARO and coordinating the activities of WHO-Collaborative Centre for Prevention of Blindness at RP Centre, AIIMS. I am also Vice President and key resource person for Vision 2020-Right to Sight, India.
| Year | Title of Award | Awarding Body |
|---|---|---|
| 2010 | Commonwealth scholarship for the MSc Community Eye Health Course at London school of Hygiene Tropical Medicine, London, UK | Commonwealth UK |
| 2014 | AIIMS Excellence Research Award | AIIMS, New Delhi |
| 2014 | Exemplary individual contribution in the field of Community Eye Care Services | COSI |
| 2014 | GOLD MEDAL" for services in community eye care and trachoma surveys | ACOIN |
| 2016 | AIIMS Excellence Award for Certificate of Commendation under clinical research | AIIMS, New Delhi |
| 2019 | Awarded by MoH FW, Nirman Bhawan for taking “Initiatives for eye care awareness for MOHFW. | DGHS, Govt of India |
| 2019 | Awarded Ophthalmic Ratna award | Manthan EHC foundation, Haryana |
| Sr. No | Project Title | Source of Funding | Year |
|---|---|---|---|
| 1 | Regional pilot model to integrate Low Vision and Vision Rehabilitation Services at various levels of Health care delivery system through a Person- Centered Approach involving Assistive Technology | WHO | 2020 |
| 2 | Mapping of Human Resource Infrastructure for Pediatric eye care services in India | Orbis | 2020 |
| 3 | Correlation between outdoor activity as measured by UV radiation exposure and myopic refractive error in school going children in New Delhi (C0-PI) | Orbis | 2019-20 |
| 4 | Prospective audits of the phenotype, causes and correlates of Trichiasis: A WHO Trachoma Collaborative Study (Co-PI) | WHO | 2019-2020 |
| 5 | To evaluate the effect of increased outdoor activity on the incidence and progression of myopia in school children (Co-PI) | DST | 2017-2019 |
| 6 | Vision Screening and Eyeglasses Dispensing Program for Students in Delhi Schools | Visionspring | 2017-2019 |
| 7 | Multi-centric study of impact of exposure to Ultra Violet Radiation (UVR) aerosol exposure on ocular health in India Phase 2 (Co-PI) | ICMR | 2018-2023 |
| 8 | A Sustainable Model for Comprehensive Outreach Eye Care Service for underserved population in Delhi Slums and resettlement colonies | Deepalaya | 2017-2022 |
| 9 | A Sustainable Model for Comprehensive Outreach Eye Care Service for underserved population in Delhi and NCR | Sparsh | 2017-2022 |
| 10 | A Sustainable Model for Comprehensive Outreach Eye Care Service in NCR- Dharuhera | Heromotors | 2017-20 |
| 11 | A Sustainable Model for Comprehensive Outreach Eye Care Service in NCR- Tauru | Deepalaya | 2017-2022 |
| 12 | Community Ophthalmology Programme in South Delhi | Deepalaya | 2017-18 |
| 13 | An Operational Research on Developing Disability Inclusive Eye Health Program in India (Co-PI) | CBM | 2016-2020 |
| 14 | Operational Research project on strengthening integrated primary eye care in urban vulnerable populations of Delhi” | Sightsavers | 2016-19 |
| 15 | National Blindness Survey- Rapid Assessment of Avoidable Blindness and diabetic retinopathy in India: Epidemiological Study of avoidable blindness in India | NPCB, Govt of India | 2015-19 |
Professor,Ocular Pathology

Dr Seema Kashyap completed her graduation from TNMC Bombay and joined AIIMS as a post graduate in 1992. After completing her MD (AIIMS) in Pathology in 1995, she worked as a Senior Resident at the AIIMS Pathology department till 1998. She joined as an Assistant Professor at Dr. R. P. Centre, Ocular Pathology section in 1999.
Email : dr_skashyap[at]hotmail[dot]com
Area of interest
Research work
1 HMG proteins in childhood malignant intraocular tumours
2. Molecular sudy of mitochondrial genes in Retinoblastoma
3. Evaluation of of P- Glycoprotein (P-gp) , Cell Division Cycle (Cdc25) and Plk Proteins in Retinoblastoma”
4.Gene expression profile of human uveal melanoma
5.Tumour angiogenesis (VEGF) in locally advanced Retinoblastoma
6. Sirtuin 1 and FOXO 3 in intraocular and orbital retinoblastoma
7.Molecular Characterization of NFκB pathway in Uveal Melanoma.
Professor of Ocular Pathology

| Professor of Ocular Pathology | |
MBBS, MD Pathology (PGIMER, Chandigarh) Fellow, Doheny Eye institute, Los Angeles, California Email: drseemasen[at]gmail[dot]com | |
Main Interests o Ophthalmic histopathology and cytopathology o Ocular Oncology o Corneal Pathology o Glaucoma Academic and Research Contributions
|
Email: drnishathussain[at]aiims[dot]edu

Dr. Nishat Hussain Ahmed aims at working on a holistic approach for management, prevention and control of infectious diseases. She is dedicated for continuous quality improvement, and has been instrumental in inconstant betterment of patient care and infection control activities at the centre. Herself a Gold medallist from Mumbai University for her exceptional performance in MD Microbiology, she is a passionate teacher and exults in teaching and mentoring undergraduate, postgraduate and super specialty medical students. She is serving as Officer In-Charge of Ocular Microbiology section since December 2019 and Nodal Officer for COVID-19 HIC for R P Centre since March 2020
Her research interests revolve around clinical research in infectious diseases, which is of immediate benefit to the patients. Notable are, her award-winning works on novel subspecies of Staphylococcus hominis in blood stream infections of patients with underlying malignancy; development of a molecular test to simultaneously detect five ocular viral pathogens; and on Rhodotorula species- an emerging yeast as a pathogen in ocular infections. She has more than fifty publications in indexed medical journals and has presented papers and delivered talks in various national and international conferences.
Dr Seema Kashyap completed her graduation from TNMC Bombay and joined AIIMS as a post graduate in 1992. After completing her MD (AIIMS) in Pathology in 1995, she worked as a Senior Resident at the AIIMS Pathology department till 1998. She joined as an Assistant Professor at Dr. R. P. Centre, Ocular Pathology section in 1999.
Email : dr_skashyap[at]hotmail[dot]com
Dr Seema Kashyap completed her graduation from TNMC Bombay and joined AIIMS as a post graduate in 1992. After completing her MD (AIIMS) in Pathology in 1995, she worked as a Senior Resident at the AIIMS Pathology department till 1998. She joined as an Assistant Professor at Dr. R. P. Centre, Ocular Pathology section in 1999.
Email : dr_skashyap[at]hotmail[dot]com

She is a Human Biology graduate from All India Institute of Medical Sciences (AIIMS), New Delhi. She has pursued her post graduation in Pharmacology and subsequently completed her PhD in Ocular Pharmacology from AIIMS, New Delhi in 2004. Subsequently she has joined as a lecturer in PharmacologyDeptt.at Delhi Institute of Pharmaceutical Science &Research (DIPSAR), New Delhi and in 2005 she has been appointed as a Scientist-I in the Deptt. Of Pharmacology, AIIMS. In 2012, she has joined as an Assistant Professor in Ocular Pharmacology & Pharmacy at Dr.RPCentre for Ophthalmic Sciences, AIIMS, New Delhi.
She has been working on in-vitro screening of drugs in cells and organ culture. She is also into developing drugs for dry eye with special reference to postmenopausal dry eye syndrome. Her fields of interests also include exploration of mechanisms involved in diabetic retinopathy and ocular inflammation.
She has been funded by extramural project from DST.

MBBS, MD Pathology (PGIMER, Chandigarh)
Fellow, Doheny Eye institute,
Los Angeles, California
Email:-drseemasen[at]gmail[dot]com
Fellow, Doheny Eye institute,
Los Angeles, California
Email: drseemasen[at]gmail[dot]com
Professor and In-charge of Ocular Pharmacology Pharmacy
Dr. Thirumurthy Velpandian
Professor and In-charge of Ocular Pharmacology Pharmacy
He has completed graduation in Pharmaceutical Sciences from Tamil Nadu Dr.MGR Medical University with a Distinction in Pharmacology. He pursued his post graduation in Drug Assay in Pharmacology and subsequently pursed PhD from All India Institute of Medical Sciences (AIIMS), New Delhi. He was awarded PhD in 1999 for his studies on liposome drug delivery to eye and its corneal interactions in which he has done a part of his study from the InstitutfürAnatomie und Zellbiologie - UniversitätWürzburg, Germany. After serving as a Senior Demonstrator and DST Young Scientist Project investigator at AIIMS in the Department of Pharmacology, he has joined as Assistant Professor of Ocular Pharmacology at Dr.RPCentre for Ophthalmic Sciences of AIIMS in 2003 at present he is the Professor and In-Charge of Ocular Pharmacology and Pharmacy Division.
He has been working on ocular pharmacokinetics with the special reference to the contribution of xenobiotic transporters in blood ocular barriers. He has been involved in developing animal models, drugs, their formulations and their delivery systems for ocular angiogenesis, infections, cataract and dry eye. His laboratory is also involved in studying ocular toxicity drugs, tear lipidomics, pharmacogenomics and ocular QSPR studies using molecular dynamics. His team was involved in addressing several environmental issues contributing towards ocular toxicity of chemical agents.
So far his research has been funded by extramural projects from DST, DBT, ICMR, MHFW, DRDO, AIIMS (intramural), Pharmaceutical companies in India and agencies from abroad. His laboratory has received Level I grant under DST-FIST program for High Precision Bioanalytical Facility (HPBAF) with tandem mass spectroscopy (LC-MS/MS).
He has had the honour of being invited to serve at various places in diverse capacities of speaker, moderator, Session Chairman, Academic Committee member, Technical expert, as well examiner in Biological and Pharmaceutical sciences. He has also been included as advisor and member in various committees of Govt.of India for making decision in drug research related affairs time to time. /p>
E-Mail:- tvelpandian[at]hotmail[dot]com
Publications from our laboratory in PubMed (Ctrl + Click)
http://www.ncbi.nlm.nih.gov/pubmed/?term=velpandian+T+or+pandian+TV
Awards, Honours Recognitions/p>
2014- Dr.Vinod Kumar Bhargava Award for Clinical Pharmacology and Drug Discovery by NAMS
2014- Editor (Pharmacology) , Indian Journal of Physiology and Pharmacology
2014- AIIMS Excellence Research Award – Commendation Certificate
2012- Visiting Professor – MIT- Harvard (Health Sciences and Technology)
2011- Visiting Faculty - BPKIHS, Nepal (Clinical Pharmacology)
2010- Nominated Member of the PG-Curriculum Review Committee of Sikkim University
CSIR ‘Senior Research Fellowship’,
ISER – Pharmacia International Travel Fellowship,
Servior Young Investigators Award,/p>
Publications and Patents/p>
| Total Publications | 107 |
| Publications in indexed journals | 101 |
| First and Corresponding Author | 38 |
| Un-indexed or in other database | 04 |
| Review articles | 02 |
| Chapters in book | 12 |
| Patents (published) | 05 |
| Patents under commercialization | 02 |
| Patent filed | 02 |
Dr. Rajendra Prasad Centre for Ophthalmic Sciences has been recognized as the Apex Organisation by the Government of India under the National Programme for the Control of Blindness.
This programme was launched in 1976 to combat blindness problem in India with the objectives of:
The Centre also assists the Ministry of Health in short term and long term planning and evaluation of the programme. It undertakes and plans epidemiological investigations and provides technical leadership to the entire nation.
The Centre is actively collaborating with various National and International agencies like ICMR, WHO and others in various fields of clinical, applied and basic research. It has also been designated as a WHO Collaborating Centre.

Genetics of Ocular diseases
Tissue and Cell culture, Stem Cell culture
Multidrug resistance
Angiogenesis in ARMD and glaucoma
Email: kaurjasbir[at]rediffmail[dot]com
OPDs: Room no. 33. Wed/Sat 9am-1pm.
Email: neiwete[at]aiims[dot]edu

Dr. Neiwete Lomi is currently Associate Professor at Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences (AIIMS), New Delhi. Dr. Lomi has done MBBS from SKMCH, Muzaffarpur, Bihar and completed post-graduation in Ophthalmology from AIIMS, New Delhi. Subsequently, he obtained super specialty training in Cornea, Refractive Surgery and Glaucoma from PGIMER Chandigarh. His current field of interest is in ocular oncology, specially retinoblastoma and uveal melanoma. Besides ocular oncology works, he is also a compassionate and dedicated ophthalmic surgeon working actively in clinical and research activity in the speciality of cornea, cataract and refractive surgery. Dr. Lomi is one of the first ophthalmic surgeon from north India to perform plaque brachytherapy on ocular tumors since 2017 and also initiated Gamma knife stereotactic radiosurgery for treating large choroidal melanoma in collaboration with Gamma knife unit at AIIMS. Currently he is working in institutional project on melanogenesis in ocular melanoma, Radiomics and Radiogenomics profiling in retinoblastoma and improvised plaque brachytherapy for various ocular tumours.
Cornea, Cataract Refractive Surgery Services
Email: noopurgupta[at]hotmail[dot]com
Noopur Gupta is a Cornea faculty at Dr. R P Centre, AIIMS, New Delhi. With more than 14 years of teaching and research experience behind her, she has made significant scientific deliberations as chairperson, instructor, judge and faculty at various regional, national and international conferences including World Ophthalmology Congress, Asia Pacific Academy of Ophthalmology and ASIA ARVO.
She was awarded the first prize and Excellence in Ophthalmic Research at 63rd AIOS, 2005. She received the ORBIS International Medal for best paper contributing to prevention of blindness in developing world at ESCRS, 2009 for her work on keratomalacia. Her extensive work on dry eye has been lauded at the Annual Conference of All India Ophthalmological Society (Best Paper, 2003) and published as Cover Story in Ocular Surgery News, APAO edition 2012 for being invited as the Dry eye expert faculty in Asia Pacific Region.
With more than 100 publications to her credit, she is a reviewer and editor of many national and international journals including IOVS. She has been instrumental in planning and implementation of population-based studies on trachoma, corneal blindness, diabetic retinopathy, RAAB, RAVI, and impact of global warming on ocular health. She is credited for conducting the first population-based study on corneal diseases in India, as part of her doctoral research at the prestigious All India Institute of Medical Sciences, New Delhi. As a key ophthalmologist and Expert Advisor, she has led trachoma surveys in Andaman Nicobar islands and helped in advocacy to reduce the burden of trachoma in these islands.
Lead Guest Editor of Journal of Ophthalmology
Reviewer of many international and national indexed journals (IOVS, IJO , Scientific World Journal, International Ophthalmology, International Journal of Occupational and Environmental Health, Asian Cardiovascular and Thoracic Annals, Journal of Clinical Experimental Ophthalmology, Saudi Journal of Ophthalmology and Journal of Ophthalmology)
Dry Eye Expert in Asia Pacific region-Cover story in Ocular Surgery News (Jul-Aug 2012)
Invited faculty, instructor, chairperson, judge- ASIA ARVO, APAO, MP State Action Plan by Vision 2020 and NPCB, National Meet for Strategic Planning For Glaucoma Management, AIOS, Annual Mid term DOS.

"Fellowship Award in Ocular Oncology at Wills Eye Institute, Philadelphia, USA " instead of "Transfer Technology fellowship award in Ocular Oncology at Wills Eye Institute, Philadelphia, 2011"
| S. No. | Topic | Month | Organizer(S) |
|---|---|---|---|
| 1. | Stem Cell Transplantation | 26-27 Nov., 2005 | Dr. Lalit Kumar IRCH Dr. Balram Airan, CTVS |
| 2. | Pediatric Malignancies | 29-31 Dec., 2005 | Dr. D.K. Gupta Paed Surgery |
| 3. | Tuberculosis & HIV | 13-15 Jan., 2006 | Dr. R. Guleria, Medicine |
| 4. | Lifestyle Disorders | 16-18 Feb., 2006 | Dr. K.S. Reddy |
| 5. | Minimal Access Surgery | 10-12 March, 2006 | Dr. M.C. Mishra |
| 6. | Cutting edge technology in reproductive health | 8-9 April, 2006 | Dr. S. Mittal |
| 7. | Comprehensive Rural health care-the way forward | 26-28 May, 2006 | Dr. C.S Pandav, CCM |
| 8. | Recent Advances in Ophthalmic Surgery | 22-23 July, 2006 | Dr. R.B. Vajpayee, RPC |
| 9. | Hepatitis | 1-3 Aug., 2006 | Dr. S.K. Acharya, Gastro |
| 10. | Comprehensive cancer care-preventive, curative & palliative | 26-27, Aug., 2006 | Dr. V. Kochupillai, IRCH |
| 11. | Adolescent health | 2-3 Sept., 2006 | Dr. Veena Kalra |
Cornea, Cataract & Refractive Surgery Services, Section VI – R P Centre
OPD: Room no 41, Wednesday / Saturday – R P Centre OPD

Dr.MurugesanVanathi completed her medical undergraduation MBBS from the prestigious Madras Medical College of Madras University, Chennai, Tamil Nadu and joined her postgraduation, M.D. (Ophthalmology) from Dr Rajendra Prasad Centre of Ophthalmic Sciences, All India Institute of Medical Sciences (AIIMS), New Delhi in 1995. She completed her senior residency training in Cornea & ocular surface, Cataract & Refractive Surgery from Dr Rajendra Prasad Centre of Ophthalmic Sciences, All India Institute of Medical Sciences (AIIMS), New Delhi. She has also worked as Senior Research Associate in Dr Rajendra Prasad Centre of Ophthalmic Sciences, All India Institute of Medical Sciences (AIIMS), New Delhi and Cornea Consultant, Aravind Eye Hospital and Postgraduate Institute, Pondicherry. She has been a faculty member in Dr Rajendra Prasad Centre of Ophthalmic Sciences, All India Institute of Medical Sciences (AIIMS), New Delhi since September 2005 and is currently working as Professor of Ophthalmology – Cornea & Ocular Surface, Cataract & Refractive Services of Section VI of the centre. She is also the Co-Office In-charge for National Eye Bank Services of Section VI of Dr Rajendra Prasad Centre of Ophthalmic Sciences, All India Institute of Medical Sciences (AIIMS), New Delhi.
She has also completed an international clinical fellowship in Cornea, from the renowned Singapore National Eye Institute, Singapore in advanced lamellar transplants of the cornea. She had extensive work experience in the field of cornea and ocular surface (medical and surgical), cataract & refractive surgery, limbal stem cell transplantation, and the various types of basic and advanced corneal transplantationprocedures.
She has to her credit over 80 indexed international publications including landmark review articles in the prestigious journals of Survey of Ophthalmology, and others such as Cornea, British Journal of Ophthalmology, Ophthalmic Research, Ocular Surface and several others. She has contributed chapters for several international sub-specialty books in her field of expertise. She has also co-edited and written several sections of the popular current ophthalmic text book “POSTGRADUATE OPHTHALMOLOGY” and “UNDERGRADUATE OPHTHALMOLOGY”.
She is a compassionate and dedicated ophthalmic surgeon currently working actively in clinical, surgical and research and management diseases of the cornea, ocular surface and eye banking with in depth clinical expertise and special interest in advanced lamellar corneal transplants, limbal stem cell transplantation, ocular surface diseases, pediatric keratoplasty, besides routine clinical work.
She is an active member of several ophthalmic professional bodies including American Society of Cataract and Refractive Society, Cornea Society, Asia Cornea Society, All India Ophthalmic Society, Ocular Surface Society, Indian Intraocular implant and refractive surgery and several state societies including the Delhi Ophthalmic Society. She has served as executive member of Delhi Ophthalmological Society (2011 – 2013) and as Editor of Delhi Ophthalmological Society (2013 – 2015) and is the current General Secretary of Delhi Ophtlamological Society (2015 – 2017). She has been awarded the gold medal for excellence in ophthalmology by the Indian Intraocular implant and refractive surgery society. She is also on the editorial board and is a reviewer of several national and international scientific journals of her field of expertise. She is also the North Zone Chairperson of Eye Bank Association of India and the executive council member of Indian Cornea &Keratorefractive Surgeons Society. She has presented her original clinical and research work as scientific papers and has participated as faculty in several national and international conferences of her specialty. She is also actively involved in teaching undergraduates, ophthalmic paramedical personnel, clinical and surgical teaching of postgraduate and senior residents besides active participation in thesis work of several students.
Venue: J.L. Auditorium
Date /Time: Friday, 6 PM
Duration: Lecture 25-30' Panel Discussion 45'
| Sr. No. | Topic | Date | Speaker | Panel Discussion |
|---|---|---|---|---|
| 1 | Kidney Transplantation | 28-10-05 | Dr. S. Guleria | Prof. S.C. Dash (M)h Prof. N.K. Mehrah Dr. A. Bagga |
| 2. | Arthritis : Myths and realities | 11-11-05 | Dr. R.Handa | Prof. Ashok Kumar (M) Dr. Uma Kumar Dr. Rajiv Gupta |
| 3. | Diabetes : Prevention and Control | 16-12-05 | Dr. N Tandon | Prof. A.C. Amini (M) Mrs Rekha Sharma Dr. S. RamaMurthy Dr. Sanjay Agarwal Dr. Atul Kumar |
| 4. | HIV infection and AIDS | 13-01-06 | Dr. Bir Singh Dr. N. Wig | Prof. S.K. Sharma (M) Dr. Bir Singh Dr. M. Vajpayee Prof. K.K. Verma |
| 5. | Diet, Exercise and Healthy heart | 24-02-06 | Dr. D.Prabhakaran | Prof. K.S. Reddy (M) Ms. Alka Khosla Dr. K.K. Deepak |
| 6. | Stroke | 17-03-06 | Dr. Rohit Bhatia | Prof. K. Prasad (M) Dr. Sumit Singh Dr. Vinay Goel Dr. Achal Srivastava |
| 7. | Brittle Bones (Osteoporosis) | 21-04-06 | Dr. Rajesh Malhotra | Prof. S. Bhan (M) Dr. S. Khadgawat Dr. Renu Mishra |
| 8. | Coping with Cancer | 12-05-06 | Dr. Lalit Kumar | Prof. G.K. Rath (M) Dr. P.K. Julka Dr. N.K. Shukla Dr. S. Bhatnagar |
| 9. | Prevention of unintended Pregnancy | 11-08-06 | Dr. N. Bhatla | Prof. S. Mittal Dr. Sunil Chumber Dr. Vatsala Dadhwal |
| 10. | Surviving a Heart Attack | 14-07-06 | Dr. B. Bhargava | Prof. V.K. Bahl (M) Dr. A.K. Bisoi Dr. G. Karthikayen |
| 11. | Ageing - Adding life to years and Years of life. | 28-07-06 | Prof. A.B. Dey (M) | |
| 12. | Right to Sight | 18-08-06 | Dr. G.V.S. Murthy | Prof. R.V. Azad (M) Dr. Ramanjit Sihota Dr. Radhika Tandon |
| 13. | Epilepsy | 08-09-06 | Dr. M.V. Padma | Prof. M. Behari (M) Prof. V. Kalra Dr. Manjari Tripathi Dr. Garima Shukla Dr. Mamta Bhushan |
Email: radhika_tan[at]yahoo[dot]com; radhikatandon[at]aiims[dot]edu

Faculty In Charge Unit 6
Chairperson National Eye Bank, AIIMS
Chairperson Low Vision Servics, RPC
Immediate Past President Eye Bank Association of India
| Degree | Year | Institute | Field of Study |
|---|---|---|---|
| MBBS | 1986 | AIIMS | Graduate Degree in Medicine |
| MD | 1989 | AIIMS | Ophthalmology |
| DNB | 1990 | National Board of Examinations | Ophthalmology |
| FRC Ophth | 1992 | Royal College of Ophthalmologists, London, UK | Ophthalmology |
| FRCS Ed | 1992 | Royal College of Surgeons, Edinburgh, UK | Ophthalmology |
| Sl. No. | Institution/Place | Designation | From Date | To Date |
|---|---|---|---|---|
| 1 | Dr Rajendra Prasad Centre for Ophthalmic Sciences (AIIMS) | Professor of Ophthalmology | Sep 2005 | Currently ongoing |
| 2 | Dr Rajendra Prasad Centre for Ophthalmic Sciences (AIIMS) | Additional Professor of Ophthalmology | Jul 2002 | Aug 2005 |
| 3 | Dr Rajendra Prasad Centre for Ophthalmic Sciences (AIIMS) | Associate Professor of Ophthalmology | Jul 1998 | Jun 2002 |
| 4 | Dr Rajendra Prasad Centre for Ophthalmic Sciences (AIIMS) | Assistant Professor of Ophthalmology | Sep 1993 | Jun 1998 |
| 5 | Royal Hallamshire Hospital, Sheffield, UK | Senior House Officer | Jun 1992 | Aug 1993 |
| 6 | District General Hospital, Barnsley, UK | Senior House Officer | Feb 1992 | May 1992 |
| 7 | West Suffolk Hospital, Bury St Edmunds, UK | Senior House Officer | Feb 1991 | Jan 1992 |
| 8 | Dr Rajendra Prasad Centre for Ophthalmic Sciences (AIIMS) | Senior Resident in Ophthalmology | Jan 1990 | Jan 1991 |
| 9 | Dr R P Centre for Ophthalmic Sciences, AIIMS, New Delhi. | Resident in Ophthalmology | 1987 | 1989 |
| 10 | All India Institute of Medical Sciences (AIIMS), New Delhi, India | Intern | 1985 | 1986 |
Pursuit of excellence; to reach the pinnacle of success; best possible ophthalmic healthcare, education and research; sincerity, dedication, integrity, striving for perfection, compassion, professional attitude, courtesy, etiquette, community service, high quality and meticulous work.
Skills: Cataract, Femtosecond Laser, Phacoemulsification, Pediatric Lens Surgery, Cornea: Transplants, Eye Banking, Stem Cell Therapy, Keratoprosthesis, Refractive: Femtosecond Laser, ICL, Premium Toric IOL
| S.No. | Name of Award | Awarding Agency | Year |
|---|---|---|---|
| 1. | Silver Medal awardee for securing highest rank in female medical graduates. | President of India, Government of India. | 1985 |
| 2 | Gold medal awardee | Royal College of Surgeons, Edinburgh | 1993 |
| 3. | Best Presentation | Delhi Ophthalmological Society | 1998 |
| 4. | Appointed In Charge | National Eye Bank at R P Centre, AIIMS | 2001 |
| 5. | Elected as member | National Academy of Sciences, India | 2001 |
| 6 | Elected member executive committee | Eye Bank Association of India (EBAI) | 2002 |
| 7. | Commonwealth Fellowship | - | - |
| 8. | Team leader for ORBIS sponsored project for setting up Pediatric Ophthalmology units | RPC, AIIMS and RIOs in India | - |
| 9. | Elected Chairperson-North Zone | Eye Bank Association of India. (EBAI) | 2006 |
| 10. | Appointed Chairperson ICMR Task Force on Global Climate Change and Eye Health | ICMR | 2006 |
| 11. | Invited as Reviewer for Journals | Eye, British Journal of Ophthalmology, Ophthalmology, IJO and NMJI | 2007 |
| 12. | Gold Medal Awardee for Ophthalmology | Intraocular Implant and Refractive Society | 2008 |
| 13. | Reviewer for journals | American Journal of Ophthalmology, Archives of Ophthalmology, British Journal of Ophthalmology and Eye | 2008 |
| 14. | Elected Secretary | Eye Bank Association of India (EBAI) | 2009 |
| 15. | Appointed on panel of experts for accreditation of eye banks in India | Eye Bank Association of India (EBAI) | 2009 |
| 16. | Appointed member of panel of experts for inspections under the Transplantation of Human Organs Act 1994 | 2009 | |
| 17. | Invited reviewer for cornea section of Asia ARVO | Cornea | 2009 |
| 18. | Appointed member of Task Force on Stem Cell Research | Department of Biotechnology | 2010 |
| 19. | Appointed member | DBT, GOI-NEI, NIH Joint Working Group for Indo-US Vision Research | 2010 |
| 20. | External Examiner for final MMed (Ophthalmology) | National University of Singapore | 2010 |
| 21. | External Examiner for exit examination in Ophthalmology by the Joint Commission for Specialist Training in Ophthalmology, | National University of Singapore | 2010 |
| 22. | Reviewer | Cornea, AJO, BJO, Eye, IJO and NMJI | 2010 |
| 23. | American Academy of Ophthalmology Achievement Award External Examiner Ophthalmology MMed and Exit Exam for Specialist Training. | National University of Singapore | 2011 |
| 24. | Member of ICMR High Powered committee on Impact of Global Warming on Health Expert for curriculum and requirements for training in Ophthalmology, MCI | ICMR MCI | 2012 |
| 25. | Member Expert Committee | National Organ and Tissue Transplant Organization (NOTTO) | 2013 |
| 26. | Vice President | Eye Bank Association of India | 2014 |
| 27. | Appointed Expert for Cornea Blindness Backlog free Punjab | Govt. of Punjab and NPCB | 2015 |
| 28. | President | Eye Bank Association of India | 2016 |
| 29. | Member Advisory Committee | National Program for Control of Blindness and Vision Impairment | 2017 |
| 30. | Chairman Vision Disability Sub Committee | Ministry of Social Justice and Empowerment | 2017 |
| 31. | Member MCI Expert Group on Vision | MCI | 2017 |
| 32. | Chairman NPCBVI sub-committee on Elimination of Corneal Blindness | NPCB | 2018 |
| 33. | Chairman Committee for developing Standard Treatment Workflows in Ophthalmology | ICMR and DHR, Government of India | 2019 |
| 34. | Fellowship | National Academy of Medical Sciences | 2021 |
More than 300 publications in International and National journal.
All Citation: 8522, h-index: 45.
For more information regarding detail publications please visit:
ORCID Id: https://orcid.org/0000-0001-9554-9933
Datta S, Biswas NR, Saxena R, Deepak KK, Menon V, Garg SP, Tandon R. Ocular and cardiovascular autonomic function in diabetic patients with varying severity of retinopathy. Indian J PhysiolPharmacol. 2005; 49(2):171-8.
Ocular and cardiovascular autonomic function in diabetic patients with varying severity
Tamhane A, Vajpayee RB, Biswas NR, Pandey RM, Sharma N, Titiyal JS, Tandon R. Evaluation of amniotic membrane transplantation as an adjunct to medical therapy as compared with medical therapy alone in acute ocular burns.Ophthalmology. 2005; 112(11):1963-9.
Evaluation of amniotic membrane transplantation as an adjunct to medical therapy as
Sethi HS, Menon V, Sharma P, Khokhar S, Tandon R. Visual outcome after intravenous dexamethasone therapy for idiopathic optic neuritis in an Indian population: a clinical case series. Indian J Ophthalmol. 2006; 54(3):177-83
Visual outcome after intravenous dexamethasone therapy for idiopathic optic neuritis in
Pal N, Titiyal JS, Tandon R, Vajpayee RB, Gupta S, Murthy GV. Need for optical and low vision services for children in schools for the blind in North India. Indian J Ophthalmol. 2006 ; 54(3):189-93.
Need for optical and low vision services for children in schools for the blind in North
Sinha R, Chhabra MS, Vajpayee RB, Kashyap S, Tandon R. Recurrent Salzmann's nodular degeneration: report of two cases and review of literature. Indian J Ophthalmol. 2006; 54(3):201-2.
Recurrent Salzmann's nodular degeneration: report of two cases and review of
Vajpayee RB, Vasudendra N, Titiyal JS, Tandon R, Sharma N, Sinha R. Automated lamellar therapeutic keratoplasty (ALTK) in the treatment of anterior to mid stromal corneal pathologies. Acta Ophthalmol Scand. 2006; 84(6):771-3.
Automated lamellar therapeutic keratoplasty (ALTK) in the treatment of anterior to mid
Vajpayee RB, Sharma N, Jhanji V, Titiyal JS, Tandon R. One donor cornea for 3 recipients: a new concept for corneal transplantation surgery. Arch Ophthalmol. 2007; 125(4):552-4.
One donor cornea for 3 recipients: a new concept for corneal transplantation
Agarwal T, Jhanji V, Dutta P, Tandon R, Sharma N, Titiyal JS, Vajpayee RB. Automated vitrector assisted optical iridectomy: customized iridectomy. J Cataract Refract Surg. 2007; 33(6):959-61.
Gharai S, Venkatesh P, Tandon R, Garg S. Peripheral ulcerative keratitis and central retinal vein occlusion as the initial manifestation of HIV infection.OculImmunolInflamm. 2007; 15(5):407-9.
Peripheral ulcerative keratitis and central retinal vein occlusion as the initial
Sharma N, Prakash G, Sinha R, Tandon R, Titiyal JS, Vajpayee RB. Indications and outcomes of phototherapeutic keratectomy in the developing world. Cornea. 2008; 27(1):44-9.
Indications and outcomes of phototherapeutic keratectomy in the developing
Tandon R, Mehta M, Satpathy G, Titiyal JS, Sharma N, Vajpayee RB. Microbiological profile of donor corneas: a retrospective study from an eye bank in north India. Cornea.2008; 27(1):80-7.
Microbiological profile of donor corneas: a retrospective study from an eye bank in north India.
Tandon R, Chawla B, Verma K, Sharma N, Titiyal JS. Outcome of treatment of mooren ulcer with topical cyclosporine a 2%. Cornea. 2008; 27(8):859-61.
Outcome of treatment of mooren ulcer with topical cyclosporine a 2%.
Jhanji V, Tandon R, Sharma N, Titiyal JS, Satpathy G, Vajpayee RB. Whole globe enucleation versus in situ excision for donor corneal retrieval-a prospective comparative study. Cornea. 2008; 27(10):1103-8.
Whole globe enucleation versus in situ excision for donor corneal retrieval-a prospective
Chawla B, Agarwal P, Tandon R,Titiyal JS. Peripheral ulcerative keratitis with bilateral optic nerve involvement as an initial presentation of acute lymphocytic leukemia in an adult. IntOphthalmol. 2009; 29(1):53-5.
Peripheral ulcerative keratitis with bilateral optic nerve involvement as an initial
Kaushal S, Prakash G, Sen S, Tandon R. Documentation of capsular opacification and incomplete cell migration barrier formation by ThinOptX IOL using Miyake-Apple view. Cont Lens Anterior Eye. 2009; 32(4):181-3.
Sharma R, Titiyal JS, Prakash G, Sharma N, TandonR, Vajpayee RB. Clinical profile and risk factors for keratoplasty and development of hydrops in north Indian patients with keratoconus. Cornea. 2009; 28(4):367-70.
Clinical profile and risk factors for keratoplasty and development of hydrops in north
Halder N, Joshi S, Nag TC, Tandon R, Gupta SK. Ocimum sanctum extracts attenuate hydrogen peroxide induced cytotoxic ultrastructural changes in human lens epithelial cells.Phytother Res. 2009; 23(12):1734-7.
Ocimum sanctum extracts attenuate hydrogen peroxide induced cytotoxic ultrastructural
Paliwal P, Gupta J, Tandon R, Sharma A, Vajpayee RB. Clinical and genetic profile of Avellino corneal dystrophy in 2 families from north India. ArchOphthalmol. 2009; 127(10):1373-6.
Clinical and genetic profile of Avellino corneal dystrophy in 2 families from north India.
Khanduja S, Jhanji V, Sharma N, Vashist P, Murthy GV, Gupta S, Satpathy G, Tandon R, Titiyal JS, Vajpayee RB. Rapid assessment of trachomaamong children living in rural northern India. Ophthalmic Epidemiol. 2009; 16(4):206-11.
Rapid assessment of trachomaamong children living in rural northern India.
Chawla B, Agarwal P, Tandon R, Titiyal JS, Sharma N, Agarwal T, Navak N, SatpathyG. In vitro susceptibility of bacterial keratitis isolates to fourt h-generation fluoroquinolones.Eur J Ophthalmol. 2010; 20(2):300-5.
Prakash G, Sharma N, Tandon R, Titiyal JS. Iatrogenic conjunctival entrapment of cilium and scleral ulceration after subtenon steroid injection. Eye Contact Lens. 2010; 36(2):137-8.
Iatrogenic conjunctival entrapment of cilium and scleral ulceration after subtenon steroid
Tandon R, Sinha R, Moulick P, Agarwal P, Titiyal JS, Vajpayee RB. Pattern of bilateral blinding corneal disease in patients waiting for keratoplasty in a tertiary eye care centre in northern India. Cornea. 2010; 29(3):269-71.
Tandon R, Padmanabhan P, Gujar P. Intraepithelial flap creation during epi-LASIK. J Cataract Refract Surg. 2010; 36(4):702-3.
Satpathy G, Patnayak D, Titiyal JS, Nayak N, Tandon R, Sharma N, Vajpayee RB. Post-operative endophthalmitis: Antibiogram genetic relatedness betweenPseudomonas aeruginosa isolates from patients phacoemulsifiers. Indian J Med Res. 2010; 131:571-7.
Paliwal P, Gupta J, Tandon R, Sharma N, Titiyal JS, Kashyap S, Sen S, Kaur P, Dube D, Sharma A, Vajpayee RB. Identification and characterization of a novel TACSTD2 mutation in gelatinous drop-like corneal dystrophy. Mol Vis. 2010; 16:729-39.
Identification and characterization of a novel TACSTD2 mutation in gelatinous drop-like
Shah VM, Tandon R, Satpathy G, Nayak N, Chawla B, Agarwal T, Sharma N, Titiyal JS, Vajpayee RB. Randomized clinical study for comparative evaluation of fourt h-generation fluoroquinolones with the combination of fortified antibiotics in the treatment of bacterial corneal ulcers.Cornea. 2010; 29(7):751-7
Chawla B, Sharma N, Tandon R, Kalaivani M, Titiyal JS, Vajpayee RB. Comparative evaluation of phototherapeutic keratectomy and amniotic membrane transplantation for management of symptomatic chronic bullous keratopathy. Cornea. 2010; 29 (9): 976- 9.
Comparative evaluation of phototherapeutic keratectomy and amniotic membrane
Paliwal P, Sharma A, Tandon R, Sharma N, Titiyal JS, Sen S, Nag TC, Vajpayee RB. Congenital hereditary endothelial dystrophy - mutation analysis of SLC4A11 and genotype- phenotype correlation in a North Indian patient cohort. Mol Vis. 2010; 16:2955- 63.
Congenital hereditary endothelial dystrophy - mutation analysis of SLC4A11 and genotype-
Khurana S, Sharma N, Agarwal T, Chawla B, Velpandian T, Tandon R, Titiyal JS. Comparison of olopatadine and fluorometholone in contact lens-induced papillary conjunctivitis. Eye Contact Lens. 2010; 36(4):210-4.
Comparison of olopatadine and fluorometholone in contact lens-induced papillary
Paliwal P, Sharma A, Tandon R, Sharma N, Titiyal JS, Sen S, Kaur P, Dube D, Vajpayee RB. TGFBI mutation screening and genotype-phenotype correlation in north Indian patients with corneal dystrophies.Mol Vis. 2010; 16:1429-38.
TGFBI mutation screening and genotype-phenotype correlation in north Indian patients
Sharma N, Goel M, Velpandian T, Titiyal JS, Tandon R, Vajpayee RB. Evaluation of umbilical cord serum therapy in acute ocular chemical burns. Invest Ophthalmol Vis Sci. 2011; 52(2):1087-92.
Evaluation of umbilical cord serum therapy in acute ocular chemical burns.
Tandon R, Gupta N, Kalaivani M, Sharma N, Titiyal JS, Vajpayee RB. Amniotic membrane transplantation as an adjunct to medical therapy in acute ocular burns. Br J Ophthalmol. 2011; 95(2):199-204.
Amniotic membrane transplantation as an adjunct to medical therapy in acute ocular burns.
Gupta N, Kalaivani M, Tandon R. Comparison of prognostic value of Roper Hall and Dua classification systems in acute ocular burns. Br J Ophthalmol. 2011; 95(2):194-8.
Comparison of prognostic value of Roper Hall and Dua classification systems in acute
Satpathy G, Mishra AK, Tandon R, Sharma MK, Sharma A, Nayak N, Titiyal JS, Sharma N. Evaluation of tear samples for Herpes Simplex Virus 1 (HSV) detection in suspected cases of viral keratitis using PCR assay and conventional laboratory diagnostic tools. Br J Ophthalmol. 2011; 95(3):415-8.
Bakhshi S, Nongpiur ME, Sen S, Tandon R. Recurrence of unifocal limbal Langerhans cell histiocytosis with partial response to chemotherapy and prolonged remission.Pediatr Blood Cancer. 2011; 56(4):687-8.
Recurrence of unifocal limbal Langerhans cell histiocytosis with partial response to
Paliwal P, Tandon R, Dube D, Kaur P, Sharma A. Familial segregation of a VSX1 mutation adds a new dimension to its role in the causation of keratoconus.Mol Vis. 2011; 17: 481-5.
Familial segregation of a VSX1 mutation adds a new dimension to its role in the
Gupta N, Sachdev R, Tandon R. Ocular surface squamous neoplasia in xerodermapigmentosum: clinical spectrum and outcome. Graefes Arch ClinExpOphthalmol. 2011; 249(8):1217-21.
Ocular surface squamous neoplasia in xerodermapigmentosum: clinical spectrum and
Sharma S, Tandon R, Mohanty S, Sharma N, M V, Sen S, Kashyap S, Singh N. Culture of corneal limbal epithelial stem cells: experience from benchtop to bedside in a tertiary care hospital in India. Cornea. 2011; 30(11):1223-32.
Culture of corneal limbal epithelial stem cells: experience from benchtop to bedside in a
Sen S, Sharma S, Gupta A, Gupta N, Singh H, Roychoudhury A, Mohanty S, Sen S, Nag TC, Tandon R. Molecular characterization of explant cultured human oral mucosal epithelial cells. Invest Ophthalmol Vis Sci. 2011;52(13):9548-54.
Molecular characterization of explant cultured human oral mucosal epithelial cells.
Sharma S, Mohanty S, Gupta D, Jassal M, Agrawal AK, Tandon R. Cellular response of limbal epithelial cells on electrospun poly-ε-caprolactone nanofibrous scaffolds for ocular surface bioengineering: a preliminary in vitro study.Mol Vis. 2011; 17:2898- 910.
Chauhan S, Sen S, Sharma A, Dar L, Kashyap S, Kumar P, Bajaj MS, Tandon R. Human papillomavirus: a predictor ofbetter survival in ocular surface squamous neoplasia patients. Br J Ophthalmol. 2012 Dec; 96(12):1517-21. doi: 10.1136/bjophthalmol-2012-301907. Epub 2012 Aug 31.
Human papillomavirus: a predictor ofbetter survival in ocular surface squamous neoplasia patients.
Sharma N, Samal A, Sharma R, Tandon R, Titiyal JS, Satpathy G, Sen S, Vajpayee RB. Evaluation of 0.3% gatifloxacin hydrochloride in decontamination of donor corneas. Eye Contact Lens. 2012 Sep; 38(5):295-9.
Evaluation of 0.3% gatifloxacin hydrochloride in decontamination of donor corneas.
Khanduja S, Jhanji V, Sharma N, Vashist P, Murthy GV, Gupta SK, Satpathy G, Tandon R, Titiyal JS, Vajpayee RB. Trachoma prevalence in women living in rural northern India: rapid assessment findings. Ophthalmic Epidemiol. 2012 Aug; 19(4):216-20.
Trachoma prevalence in women living in rural northern India: rapid assessment findings.
Titiyal JS, Sachdev R, Sinha R, Tandon R, Sharma N. Modified surgical technique for improving donor adherence in DSAEK in the aphakicvitrectomized eye. Cornea. 2012; 31(4):462-4.
Modified surgical technique for improving donor adherence in DSAEK in the
124. Sinha R, Shekhar H, Sharma N, Tandon R, Titiyal JS, Vajpayee RB. Intrascleral fibrin glue intraocular lens fixation combined with Descemet-stripping automated endothelial keratoplasty or penetrating keratoplasty. J Cataract Refract Surg. 2012 Jul; 38(7):1240-5.
Paliwal P, Sharma A, Tandon R, Sharma N, Titiyal JS, Sen S, Vajpayee RB. Molecular genetic analysis of macular corneal dystrophy patients from North India.Ophthalmic Res. 2012; 48(1):28-32.
Molecular genetic analysis of macular corneal dystrophy patients from North
Sharma N, Sachdev R, Titiyal JS, Tandon R, Vajpayee RB. Penetrating autokeratoplasty for unilateral corneal opacification. Eye Contact Lens.2012; 38(2):112- 5.
Penetrating autokeratoplasty for unilateral corneal opacification.
Gupta N, Tandon R. Sociodemographic features and risk factor profile of keratomalacia in early infancy.Cornea. 2012; 31(8):864-6.
Sociodemographic features and risk factor profile of keratomalacia in early
Kumar A, Kumar A, Bali SJ, Tandon R. Performance analysis of efforts towards promotion of corneal donation at a tertiary care trauma center in India.Cornea. 2012; 31(7):828-31.
Performance analysis of efforts towards promotion of corneal donation at a tertiary care
Aldave AJ, Sangwan VS, Basu S, Basak SK, Hovakimyan A, Gevorgyan O, Kharashi SA, Jindan MA, Tandon R, Mascarenhas J, Malyugin B, Padilla MD, Maskati Q, Agarwala N, Hutauruk J, Sharma M, International results with the Boston type I Keratoprosthesis. Yu F.Ophthalmology. 2012 119(8):1530-8.
International results with the Boston type I Keratoprosthesis.
Agarwal T, Jhanji V, Satpathy G, Nayak N, Chawla B, Tandon R, Titiyal JS. Moxifloxacin resistance: intrinsic to antibiotic or related to mutation?Optom Vis Sci. 2012;89(12):1721-4.
Sharma S, Tandon R, Mohanty S, Kashyap S, Vanathi M. Phenotypic evaluation of severely damaged ocular surface after reconstruction by cultured limbal epithelial cell transplantation.Ophthalmic Res. 2013;50(1):59-64.
Phenotypic evaluation of severely damaged ocular surface after reconstruction by
Sharma N, Chacko J, Velpandian T, Titiyal JS, Sinha R, Satpathy G, Tandon R, Vajpayee RB. Comparative evaluation of topical versus intrastromalvoriconazole as an adjunct to natamycin in recalcitrant fungal keratitis. Ophthalmology. 2013; 120(4):677-81.
Vanathi M, Kashyap S, Khan R, Seth T, Mishra P, Mahapatra M, Tandon R. Ocular surface evaluation in allogenic hematopoietic stem cell transplantation patients. Eur J Ophthalmol. 2014 Mar 7:0. [Epub ahead of print]
Ocular surface evaluation in allogenic hematopoietic stem cell transplantation patients.
Sharma N, Roy S, Maharana PK, Sehra SV, Sinha R, Tandon R,Titiyal JS, Vajpayee RB. Outcomes of corneal collagen crosslinking in pseudophakic bullous keratopathy. Cornea. 2014 Mar;33(3):243-6.
Outcomes of corneal collagen crosslinking in pseudophakic bullous keratopathy.
Sehra SV, Titiyal JS, Sharma N, Tandon R, Sinha R. Change in corneal microstructure with rigid gas permeable contact lens use following collagen cross-linking: an in vivo confocal microscopy study. Br J Ophthalmol. 2014 Apr;98(4):442-7. Epub 2013 Dec 24
Gogia V, Gupta S, Titiyal JS, Panda A, Pandey RM, Tandon R.A preliminary descriptive analysis of Corneal Transplant Registry of National Eye Bank in India. Cont Lens Anterior Eye. 2014; 37(2):111-5
A preliminary descriptive analysis of Corneal Transplant Registry of National Eye Bank in India.
Sehra SV, Titiyal JS, Sharma N, Tandon R, Sinha R. Change in corneal microstructure with rigid gas permeable contact lens use following collagen cross-linking: an in vivo confocal microscopy study. Br J Ophthalmol. 2014; 98(4):442-7.
Tandon R, Singh A, Gupta N, Vanathi M, Gupta V. .Upgradation and modernization of eye banking services: Integrating tradition with innovative policies and current best practices. Indian J Ophthalmol. 2017; 65: 109-115.
Chauhan S, Sen S, Sharma A, Kashyap S, Tandon R, Bajaj MS, Pushker N, Vanathi M, Chauhan SS. p16INK4aoverexpression as a predictor of survival in ocular surface squamous neoplasia.
p16INK4aoverexpression as a predictor of survival in ocular surface squamous neoplasia.
Satpathy G, Behera HS, Sharma A, Mishra AK, Mishra D, Sharma N, Tandon R, Agarwal T, Titiyal JS. A 20-year experience of ocular herpes virus detection using immunofluorescence and polymerase chain reaction. Clin Exp Optom. 2018 Mar 6. doi: 10.1111/cxo.12669. [Epub ahead of print]
Chauhan S, Sen S, Sharma A, Kashyap S, Tandon R, Pushker N, Vanathi M, Chauhan SS. Loss of pRB in Conjunctival Squamous Cell Carcinoma: A Predictor of Poor Prognosis. Appl Immunohistochem Mol Morphol. 2018 Feb 27. doi:10.1097/PAI.0000000000000592. [Epub ahead of print]
Loss of pRB in Conjunctival Squamous Cell Carcinoma: A Predictor of Poor Prognosis.
Selvan H, Yadav S, Tandon R. Big double bubble trouble: in vivo real time demonstration of 'mixed-type bubble' and its consequent effects during deep anterior lamellar keratoplasty. Eye (Lond). 2018 Feb 16. doi: 10.1038/s41433-018-0038-y. [Epub ahead of print] No abstract available.
Selvan H, Singh A, Tandon R. Deep blue dot corneal degeneration: confocal characteristics. Int Ophthalmol. 2018 Feb 8. doi: 10.1007/s10792-018-0849-7. [Epub ahead of print]
Deep blue dot corneal degeneration: confocal characteristics.
Saxena R, Vashist P, Tandon R, Pandey RM, Bhardawaj A, Gupta V, Menon V. Incidence and progression of myopia and associated factors in urban school children in Delhi: The North India Myopia Study (NIM Study). PLoS One. 2017 Dec 18;12(12):e0189774. doi: 10.1371/journal.pone.0189774. eCollection 2017.
Singh A, Gupta N, Ganger A, Vashist P, Tandon R. Awareness Regarding Eye Donation in an Urban Slum Population: A Community-Based Survey. Exp Clin Transplant. 2017 Dec 18. doi: 10.6002/ect.2017.0077. [Epub ahead of print]
Awareness Regarding Eye Donation in an Urban Slum Population: A Community-Based Survey.
Dar L, Tandon R.How safe is safe, and where are we in the journey toward safest of safe? Indian J Ophthalmol. 2017 Nov;65(11):1075-1076. doi: 10.4103/ijo.IJO_1054_17. No abstract available.
How safe is safe, and where are we in the journey toward safest of safe?
Selvan H, Patil M, Yadav S, Tandon R. Triple chamber: a clinical rarity after deep anterior lamellar keratoplasty and role of optical coherence tomography in management. Int Ophthalmol. 2017 Oct 30. doi: 10.1007/s10792-017-0755-4. [Epub ahead of print]
Meel R, Dhiman R, Vanathi M, Pushker N, Tandon R, Devi S. Clinicodemographic profile and treatment outcome in patients of ocular surface squamous neoplasia. Indian J Ophthalmol. 2017 Oct;65(10):936-941. doi: 10.4103/ijo.IJO_251_17.
Clinicodemographic profile and treatment outcome in patients of ocular surface squamous neoplasia.
Dhiman R, Devi S, Duraipandi K, Chandra P, Vanathi M, Tandon R, Sen S. Cysticercosis of the eye. Int J Ophthalmol. 2017 Aug 18;10(8):1319-1324. doi: 10.18240/ijo.2017.08.21. eCollection 2017. Review.
Gupta N, Vashist P, Tandon R, Gupta SK, Kalaivani M, Dwivedi SN. Use of traditional eye medicine and self-medication in rural India: A population-based study. PLoS One. 2017 Aug 22;12(8):e0183461. doi: 10.1371/journal.pone.0183461. eCollection 2017.
Use of traditional eye medicine and self-medication in rural India: A population-based study.
Patel D, Tandon R, Ganger A, Vij A, Lalwani S, Kumar.Study of death to preservation time and its impact on utilisation of donor corneas. A.TropDoct. 2017 Oct;47(4):365-370. doi: 10.1177/0049475517713406. Epub 2017 Jun 13.
Study of death to preservation time and its impact on utilisation of donor corneas.
Yadav S, Singh A, Tandon R.Folds in Descemet Membrane Associated With Forceps-Induced Injury. JAMA Ophthalmol. 2017 Jun 8;135(6):e170669. doi: 10.1001/jamaophthalmol.2017.0669. Epub 2017 Jun 8. No abstract available.
Folds in Descemet Membrane Associated With Forceps-Induced Injury.
Singh A, Sen S, Vanathi M, Tandon R. Corneal keloid with cystoid cicatrix:post-small-incision cataract surgery. Can J Ophthalmol. 2017 Jun;52(3):e93-e95. doi: 10.1016/j.jcjo.2016.11.013. Epub 2017 Jan 12. No abstract available.
Corneal keloid with cystoid cicatrix:post-small-incision cataract surgery.
Ganger A, Devi S, Gupta N, Vanathi M, Tandon R.Ocular surface squamous neoplasia masquerading as peripheral ulcerative keratitis. Trop Doct. 2017 Jul;47(3):233-236. doi: 10.1177/0049475516682133. Epub 2016 Dec 5. No abstract available.
Ocular surface squamous neoplasia masquerading as peripheral ulcerative keratitis.
Saha S, Gantyala SP, Aggarwal S, Sreenivas V, Tandon R, Goswami R. Long-term outcome of cataract surgery in patients with idiopathic hypoparathyroidism and its relationship with their calcemic status. J Bone Miner Metab. 2017 Jul;35(4):405-411. doi: 10.1007/s00774-016-0767-6. Epub 2016 Jul 27.
Sinha R, Bansal M, Sharma N, Dada T, Tandon R, Titiyal JS. Transscleral Suture-Fixated Versus Intrascleral Haptic-Fixated Intraocular Lens: A Comparative Study. Eye Contact Lens. 2017 Nov;43(6):389-393. doi: 10.1097/ICL.0000000000000287.
Satpathy G, Ahmed NH, Nayak N , Tandon R , Sharma N , Agarwal T , Vanathi M, Titiyal JS , Spectrum of mycotic keratitis in north India: Sixteen years study from a tertiary care ophthalmic centre.J Infect Public Health.2018 Dec 29. pii: S1876-0341(18)30322-8. doi: 10.1016/j.jiph.2018.12.005. [Epub ahead of print]
Roy S, Yadav S, Dasgupta T, Chawla S, Tandon R, Ghosh S.Interplay between hereditary and environmental factors to establish an in vitro disease model of keratoconus. Drug Discov Today. 2018 Nov5. pii: S1359-6446(18)30146-6. doi: 10.1016/j.drudis.2018.10.017.
Mukhija R, Gupta N, Ganger A, Kashyap S, Hussain N, Vanathi M, Tandon R. Isolated Primary Corneal Acremonium Eumycetoma: Case Report and Literature Review. Cornea. 2018 Dec;37(12):1590-1592. doi: 10.1097/ICO.0000000000001750.
Isolated Primary Corneal Acremonium Eumycetoma: Case Report and Literature Review.
Nair S, Vanathi M, Mahapatra M, Seth T, Kaur J, Velpandian T, Ravi A, Titiyal JS, Tandon R. Tear inflammatory mediators and protein in eyes of post allogenic hematopoeitic stem cell transplant patients. Ocul Surf. 2018 Jul;16(3):352-367. doi: 10.1016/j.jtos.2018.04.007. Epub 2018 May
Noopur G, Praveen V, Radhika T, Sanjeev K G, Mani K, Deepak K. Attitudes and Perception Towards Eye Donation in Patients with Corneal Disease: A Case-controlled Population-based Study. Curr Eye Res. 2018 Jun;43(6):734-739. doi: 10.1080/02713683.2018.1449221. Epub 2018 Apr 13.
Ahmed NH, Sharma A, Satpathy G, Titiyal JS, Tandon R, Agarwal T, Vanathi M, Sharma N. Chlamydia trachomatisAntigen Positivity in Patients with Different Ocular Manifestations over 8 Years. J Glob Infect Dis. 2018 Jan-Mar;10(1):16-18. doi: 10.4103/jgid.jgid_100_17.
Singh D, Ganger A, Gupta N, Vanathi M, Khadgawat R, Tandon R.Primary Bullous Keratopathy in a Patient With Werner Syndrome Treated With Corneal Transplant. Exp Clin Transplant. 2018 Mar 9. doi: 10.6002/ect.2017.0163. [Epub ahead of print]
Primary Bullous Keratopathy in a Patient With Werner Syndrome Treated With Corneal Transplant.
Chauhan S, Sen S, Sharma A, Kashyap S, Tandon R, Bajaj MS, Pushker N, Vanathi M, Chauhan SS.p16INK4aoverexpression as a predictor of survival in ocular surface squamous neoplasia. Br J Ophthalmol. 2018 Jun;102(6):840-847. doi: 10.1136/bjophthalmol-2017-311276. Epub 2018 Mar 6.
p16INK4aoverexpression as a predictor of survival in ocular surface squamous neoplasia.
Satpathy G, Behera HS, Sharma A, Mishra AK, Mishra D, Sharma N, Tandon R, Agarwal T, Titiyal JS.A 20-year experience of ocular herpes virus detection using immunofluorescence and polymerase chain reaction. Clin Exp Optom. 2018 Sep;101(5):648-651. doi: 10.1111/cxo.12669. Epub 2018 Mar 6.
Chauhan S, Sen S, Sharma A, Kashyap S, Tandon R, Pushker N, Vanathi M, Chauhan SS.Loss of pRB in Conjunctival Squamous Cell Carcinoma: A Predictor of Poor Prognosis. Appl Immunohistochem Mol Morphol. 2018 Jul;26(6):e70-e76. doi: 10.1097/PAI.0000000000000592.
Loss of pRB in Conjunctival Squamous Cell Carcinoma: A Predictor of Poor Prognosis.
Selvan H, Yadav S, Tandon R.Eye (Lond). Big double bubble trouble: in vivo real time demonstration of 'mixed-type bubble' and its consequent effects during deep anterior lamellar keratoplasty. 2018 Jul;32(7):1282-1283. doi: 10.1038/s41433-018-0038-y. Epub 2018 Feb 16
Selvan H, Singh A, Tandon R. Deep blue dot corneal degeneration: confocal characteristics. Int Ophthalmol. 2018 Feb 8. doi: 10.1007/s10792-018-0849-7. [Epub ahead of print]
Deep blue dot corneal degeneration: confocal characteristics.
Saxena R, Vashist P, Tandon R, Pandey RM, Bhardawaj A, Gupta V, Menon V. Incidence and progression of myopia and associated factors in urban school children in Delhi: The North India Myopia Study (NIM Study). PLoS One. 2017 Dec 18;12(12):e0189774. doi: 10.1371/journal.pone.0189774. eCollection 2017.
Singh A, Gupta N, Ganger A, Vashist P, Tandon R. Awareness Regarding Eye Donation in an Urban Slum Population: A Community-Based Survey. Exp Clin Transplant. 2018 Dec;16(6):730-735. doi: 10.6002/ect.2017.0077. Epub 2017 Dec 18.
Awareness Regarding Eye Donation in an Urban Slum Population: A Community-Based Survey.
Selvan H, Patil M, Yadav S, Tandon R.Triple chamber: a clinical rarity after deep anterior lamellar keratoplasty and role of optical coherence tomography in management. Int Ophthalmol. 2018 Dec;38(6):2683-2687. doi: 10.1007/s10792-017-0755-4. Epub 2017 Oct 30.
Ganger A, Gupta N, Tomar AS, Vanathi M, Tandon R.Infective keratitis in Indian patients with corneal dystrophies. Trop Doct. 2018 Jul;48(3):199-206. doi: 10.1177/0049475517736709. Epub 2017 Oct 17.
Infective keratitis in Indian patients with corneal dystrophies.
Gupta N, Ganger A, Bhartiya S, Verma M, Tandon R.In Vivo Confocal Microscopic Characteristics of Crystalline Keratopathy in Patients with Sclerokeratitis. Ocul Immunol Inflamm. 2018;26(5):700-705. doi: 10.1080/09273948.2017.1281422. Epub 2017 Feb 22.
AntonitaJ.MohanaSandhya Gupta bRadhika Tandon c A comparative study of knowledge and attitude regarding tissues and organ donation, between general population and relatives of transplant patients. Current Medicine Research and Practice. Volume 8, Issue 5 ,September–October 2018, Pages 159-164
Singh A, Gupta N, Ganger A, Singh D, Kashyap S, Tandon R.Sutureless Customized Lamellar Corneal Transplant in a Patient with Gelatinous Drop-Like Corneal Dystrophy. Exp Clin Transplant. 2019 Jul 19. doi: 10.6002/ect.2019.0043.
Abulhamael AM, Tandon R, Alzamzami ZT, Alsofi L, Roges RA, Rotstein I.Treatment Decision-making of Cracked Teeth: Survey of American Endodontists. J Contemp Dent Pract. 2019 May 1;20(5):543-547.
Treatment Decision-making of Cracked Teeth: Survey of American Endodontists.
Singh A, Vanathi M, Kishore A, Gupta N, Tandon R.Evaluation of strip meniscometry, tear meniscusdepth in the diagnosis of dry eye disease in asian Indian eyes. Ocul Surf. 2019 Jul 2. pii: S1542-0124(18)30402-6. doi: 10.1016/j.jtos.2019.07.002.
Gupta N, Vashist P, Ganger A, Tandon R, Gupta SK.Eye donation and eye banking in India. Natl Med J India. 2018 Sep-Oct;31(5):283-286. doi: 10.4103/0970-258X.261189.
Gunasekaran S, Dhiman R, Vanathi M, Mohanty S, Satpathy G, Tandon R. Ocular Surface Microbial Flora in Patients with Chronic Limbal Stem Cell Deficiency Undergoing Cultivated Oral Mucosal Epithelial Transplantation. Middle East Afr J Ophthalmol. 2019 Jan-Mar;26(1):23-26. doi: 10.4103/meajo.MEAJO_172_16.
Daggumilli S, Vanathi M, Ganger A, Goyal V, Tandon R. Corneal Evaluation in Patients With Parkinsonism on Long-Term Amantadine Therapy. Cornea. 2019 Apr 9. doi: 10.1097/ICO.0000000000001951.
Corneal Evaluation in Patients With Parkinsonism on Long-Term Amantadine Therapy.
Gupta V, Saxena R, Vashist P, Bhardwaj A, Pandey RM, Tandon R, Menon V. Spectacle Coverage among Urban Schoolchildren with Refractive Error Provided Subsidized Spectacles in North India. Optom Vis Sci. 2019 Apr;96(4):301-308. doi: 10.1097/OPX.0000000000001356.
264. Meenakshi Wadhwani, Praveen Vashist, Suraj Singh Senjam, Vivek Gupta, Rohit Saxena, Radhika Tandon. A population-based study on the prevalence and causes of childhood blindness andvisual impairment in North India.Indian J Ophthalmol. 2021 Jun;69(6):1381-1387. doi:10.4103/ijo.IJO_2408_20
Noopur Gupta, Saumya Yadav, Anthony W Solomon, Shubhi Jain, Seema Kashyap, Murugesan Vanathi, Radhika Tandon. Atypical Corneal Phenotype in Patients With Trachoma and Secondary Amyloidosis.Cornea. 2021 Jun 29. doi:10.1097/ICO.0000000000002791
Anita Ganger, Archita Singh, M Kalaivani, Noopur Gupta, Murugesan Vanathi, Sujata Mohanty, Radhika Tandon. Outcomes of surgical interventions for the treatment of limbal stem cell deficiency.Indian J Med Res 2021 Jul;154(1):51-61. doi:10.4103/ijmr.IJMR_1139_18.
Sangeetha Vijayam S Pai, Alisha Kishore, Seema Sen, Namrata Sharma, Radhika Tandon. Conjunctival Autofluorescence and Cytological Changes in Pterygium.Cornea 2021 Aug 30. doi: 10.1097/ICO.0000000000002820.
Raghav D Ravani, Saumya Yadav,Brijesh Takkar , Seema Sen, Seema Kashyap, Deepika Gupta, Manjeet Jassal,Ashwini Agrawal, Sujata Mohanty,Radhika Tandon. Experimental evaluation of safety and efficacy of plasma-treated poly-ε-caprolactone membrane as a substitute for human amniotic membrane in treating corneal epithelial defects in rabbit eyes.Indian J Ophthalmol. 2021 Sep; 69 (9):2412-2416. doi: 10.4103/ijo.IJO_2986_20.
Sharon D’Souza, Rohit Shetty, Gairik Kundu, Namrata Sharma, Radhika Tandon, Himanshu Matalia,Bhavya Gorimanipalli, Chaitra Jayadev. COVID-19 positivity rate in corneal tissue donors – A cause for concern! Indian J Ophthalmol. 2021 Oct; 69(10): 2808–2811. doi:10.4103/ijo.IJO_1163_21
COVID-19 positivity rate in corneal tissue donors – A cause for concern!.
Nimmy Raj, Murugesan Vanathi, Nishat Hussain Ahmed, Noopur Gupta, Neiwete Lomi, Radhika Tandon . Recent Perspectives in the Management of Fungal Keratitis.J Fungi (Basel) 2021 Oct 26;7(11):907. doi: 10.3390/jof7110907.
Sheetal Chauhan, Neelam Pushker, Radhika Tandon, Seema Kashyap, Murugesan Vanathi, Mandeep S Bajaj. Clinical Significance of Cyclin Expression Profiling in Ocular Surface Squamous Neoplasia. Appl Immuno histochem Mol Morphol2021 Oct 18. doi: 10.1097/PAI.0000000000000981.
Raj N, Gupta N, Kumar D, Vashist, Tandon R. Population-based study on the prevalence, clinical characteristics and vision-related quality of life in patients with corneal opacity resulting frominfectious keratitis: results from the Corneal Opacity Rural Epidemiological study. Br J Ophthalmol. 2021 Nov 12:bjophthalmol-2021-320077. doi:10.1136/bjophthalmol-2021-320077.
Yogita Gupta, Alisha Kishore, Pooja Kumari, Neelima Balakrishnan, Neiwete Lomi, Noopur Gupta, M Vanathi, Radhika Tandon . Peripheral ulcerative keratitis.Surv Ophthalmol Nov-Dec 2021;66(6):977-998. doi:10.1016/j.survophthal.2021.02.013.
TanveerAlam Khan, Navneet Sidhu, Livia Khan, Seema Sen, Nishat Hussain, RadhikaTandon,Noopur Gupta.Bilateral Immune-Mediated Keratolysis After Immunization With SARS- CoV-2 Recombinant Viral Vector Vaccine.Cornea 2021 Dec 1;40(12):1629-1632.doi: 10.1097/ICO.0000000000002844.
Sheetal Chauhan, Seema Sen, Shyam S Chauhan, Neelam Pushker, Radhika Tandon, Seema Kashyap, Murugesan Vanathi, Mandeep S Bajaj.Stratifin in ocular surface squamous neoplasia and its association with p53. Acta Ophthalmol.2021 Dec;99(8):e1483-e1491. doi: 10.1111/aos.14844. Epub 2021 Mar26
Sneha Aggarwal, Murugesan Vanathi, Viney Gupta, Radhika Tandon. Our experience with rose k2 contact lens for visual rehabilitation in keratoconic corneas following collagen cross linking. Contact Lens and Anterior Eye. 2019; 42 (6); S1 E25 Dec 2019. DOI:https://doi.org/10.1016/j.clae2019.10.084
Book Name: (Corneal infection and inflammation: A colour atlas) Edited by Noopur Gupta, Ritika Mukhija, Radhika Tandon (2021). Corneal Infection and Inflammation: A Colour Atlas. Doi:10.1201/9781003024897
Evaluation of Barrett universal II formula for intraocular lens power calculation in Asian Indian population. Kuthirummal N, Vanathi M, Mukhija R, Gupta N, Meel R, Saxena R, Tandon R.Indian J Ophthalmol 2020;68(1):59‐64. doi:10.4103/ijo.IJO_600_19
AIIMS Golden Jubilee Celebrations - CME Continuing Medical Education
Specialisation: Srtabismus and Neuro-Ophthalmology
Email: drmsswati[at]rediffmail[dot]com

MBBS : Pt. Jawahar Lal Nehru Memorial Medical College Raipur (C.G)
MD: Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi
1. Assist Professor (Ophthalmology)- 22/05/14- till date
Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi
2. Assist Professor (Ophthalmology)- 11/07/11- 21/05/14
Post Graduate Institute of Medical Education & Research, Chandigarh
3. Senior Research Associate- 23/09/09- 10/07/11
Neuro-Ophthalmology and Strabismus services,
Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi
4. Research Officer (Ophthalmology)- 7/01/2009-22/09/09
INDEYE Study of Cataract and Age-related Macular Degeneration India-INDGEN,
Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi
5. Senior Resident 07/01/2006 – 06/01/2009
Neuro-Ophthalmology & Strabismus and Glaucoma Services,
Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India
Email: rohitsaxena80[at]yahoo[dot]com

Prof. Rohit Saxena completed his graduation from the All India Institute of Medical Sciences (AIIMS) in 1996 and joined Dr Rajendra Prasad Centre for Ophthalmic Sciences (AIIMS) as a postgraduate student in 1996. After completing his MD course in Ophthalmology in 1999, he was a Senior Resident at the centre till 2002. He joined the faculty as Assistant Professor at the centre in 2003. He has completed his PhD in Ophthalmology in 2016.
Dec 2014: Completed course on Good Clinical Practices by NIDA Clinical Trials Network.
Sept 2007: Professional Diploma in Clinical Research (PGDR), Catalyst Clinical Services, New Delhi
July 2006: Post-Graduate Certificate course in Hospital Management, National Institute of Health and Family Welfare, New Delhi.
March 1999: Basic Sciences Assessment in Ophthalmology, International Council of Ophthalmology.
Two weeks Observer ship and Training Programme at the New England Eye Centre, Boston, Massachusetts, U.S.A. from 16th to 30th Nov. 2001.
Delhi Ophthalmology Society
All India Ophthalmological Society
Strabismological & Pediatric Ophthalmology Society of India
International Strabismological Association
Address: 493, 4th Floor, Dr R P Centre for Ophthalmic Sciences, AIIMS, New Delhi – 110029
Phone no: 011 26593020
Email: pushkern[at]hotmail[dot]com

Dr. Neelam Pushker completed her undergraduate and postgraduate training from All India Institute of Medical Sciences (AIIMS), New Delhi. She also completed her Senior Residency training from Dr R P Centre, AIIMS. She joined as Faculty in Oculoplasty, Orbit and Tumor Services of Dr R P Centre, AIIMS, in 2000. She is currently working as Professor of Ophthalmology. She is surgically skilled in performing highly specialized orbital, lacrimal, socket and eyelid surgeries. Reconstructive procedures of eyelid, socket, congenital anomalies etc using grafts such as mucous membrane, skin, amniotic membrane, sclera and synthetic implants are routinely performed by her. She has vast experience in cosmetic and corrective surgeries such as blepharoplasty, ptosis, lid retraction, socket expansion, trauma etc. Treatment of benign and malignant orbital, ocular surface and eyelid tumors is a major part of her surgical and clinical experience. She has published more than 135 papers in peer reviewed indexed international journals and also some chapters in books. Amongst some recent awards, she has received Best Paper Award (OPAI), 2012; AIIMS Excellence Research Award, 2014 and Asia-Pacific Academy of Ophthalmology-Achievement Award, 2015. She is member of various scientific societies and reviewed papers for national and international journals. She has chaired sessions, performed live surgery, presented videos and delivered guest lectures in several national and international conferences and meetings.
Some of her pioneer and innovative work are in the field of eyelid reconstructive surgery, sentinel lymph node biopsy in eyelid tumors, orbital infection, ptosis, contracted socket, congenital periorbital anomalies and lacrimal problems. She has officiated as Chief Guide in about 20 MD thesis, also as a co-supervisor in M.D, PhD and D.M thesis. She has collaborated in basic sciences services research work on molecular and genetic aspects of tumors and congenital anomalies. Some of these researches have been published in high index journal viz. Ophthalmology, American Journal of Ophthalmology and British Journal of Ophthalmology.
In developing countries like India, where there is a shortage of both basic doctors and specialists, medical education stands at cross roads. It seems inescapable that our medical education policy has to be oriented towards production of a basic doctor, a specialist and superspecialist. Recognising the dearth of ophthalmologists, training of paramedical personnel to help them is very essential. The teaching programme of the Centre is aimed as follows:
Post Graduate Teaching
Post Graduates are given intensive training for a period of 3 years as resident doctors. Admission to postgraduation course is done every 6 months and in all 24 students admitted per year. The teaching programme includes lectures, case conferences, symposia, journal clubs and demonstrations. Post-graduate teaching is updated from time to time. The teaching schedule includes the recent developments and newer trends in various fields of ophthalmology. Both the basic sciences and clinical courses are spread over three years. The post graduates are attached with consultants so that they can be given personal attention. They are given training in general ophthalmology and in various subspecialities including microsurgery. They are taught to do all types of surgery and are also given experience in community ophthalmology especially during eye camps. Emphasis is given on proper understanding of their role in the National Programme for Control of Blindness. The residents at the completion of their training have a very strong theoretical as well as practical background to provide all types of ophthalmic services. They are also capable of undertaking independent research work and teaching of undergraduate students. The passed out students are holding responsible teaching and non-teaching positions not only in India but also abroad. Some sponsored candidates from other countries had post-graduate training at this Centre.
Undergraduate Teaching
The undergraduate students are taught ophthalmic examination along with investigations, diagnosis and management of common eye disorders. They are made familiar with prevalence of blindness, preventive and rehabilitative measures available and their role in the National Programme for Control of Blindness. The teaching programme includes lectures, seminars, clinical work, field work and tutorials with the following objectives:
B.Sc. (Hons) Ophthalmic Technique
This course is of 3 years duration.The objectives of the course are (i) to achieve general understanding of human biology and basic medical sciences related to ophthalmology, (ii) to enable candidates to work under the supervision of an ophthalmologist in hospitals, clinics and community, in order to help in the execution of integrated approach of promotive, preventive, diagnostic, curative and rehabilitative aspects of ophthalmic care, (iv) to be able to carry out refraction work including contact lenses, (v) to be able to assess disorders of ocular motility and visual functions, give orthoptic and pleoptic exercises. The teaching exercises include lectures, seminars, demonstrations and postings in operation theatres mobile eye camps and various investigative labs. Admission to this course is done yearly and about 24 students are admitted.
Post Doctoral Workshops
This Centre has so far held 101 workshops in which specialists from all over the country have participated. Various specialities in which workshops were held include eye bank and corneal grafting, ophthalmo-plastic surgery, glaucoma, contact lens, neuro ophthalmology, retina, ocular motility and amblyopia (squint), ocular pathology, lens uvea, ocular trauma, paediatric ophthalmology, medical ophthalmology and phacoemulsification.
A large number of National level workshops and seminars under the auspices of W.H.O., I.C.M.R. and Ministry of Health have been conducted.
Post-doctoral short and long term trainees
A large number of ophthalmologists from India and abroad have been trained under this programme. During 2000, 22 short term trainees visited the Centre.
Email: msbajaj32[at]hotmail[dot]com
Phone (Off ): 91-11-26593072

Dr. M. S. Bajaj, is Professor of Ophthalmology at Rajendra Prasad Center for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India, which is a tertiary care referral and teaching hospital
He is involved in clinical, teaching and research work in Ophthalmology at this apex institute of national importance. He specializes in the fields of Oculoplasty, Orbital Diseases, Lacrimal Disorders and Ocular tumors.
His research work focuses on these superspecialties and includes evolving newer and more innovative surgical techniques. His work has been published in various international journals of repute, in addition to being presented at numerous prestigious superspecialty meetings and conferences.
Cornea, Cataract & Refractive Surgery Services, Section VI – R P Centre
Email: drpraful13[at]gmail[dot]com, drprafulla[at]aiims[dot]edu
Twitter: praful@276

Dr. Prafulla Kumar Maharana completed his graduation (M.B.B.S.) in 2006 from the MKCG Medical College, Berhampur, Orissa and PostGraduation in Ophthalmology (M.D.) from Dr. R.P. Centre, AIIMS, New Delhi in 2010. He has completed his senior residency in the field of cornea, cataract and refractive services from Dr. R.P. Centre, AIIMS, NewDelhi.
Hehas joined as faculty of the Dr. R.P. Centre for OphthalmicSciences in 2016and currently working as Assistant Professor of Ophthalmology in Unit-3.Previously, He has worked as Assistant Professor of Ophthalmology at AIIMS, Bhopal & AIIMS, Bhubaneswar. His areas of specialization include Cataract, Cornea and Refractive Surgery. His field of interest includes Keratoconus, Corneal infections and Keratoplasty.
He has contributedseveral chapters (19) to National and International books on ophthalmology and published 27research papers in international peer reviewed PubMed indexed journals. In addition, he has published several non-index papers.
He has been awarded Gold medal by India Academy of Pediatrics in the year 2005. He is the recipient of (as co-author) the “Best Surgical Video” by FRANZCO, Australiatwice (2002 2015) in his career.
Dr. Dewang Angmo
MD,DNB,FAICO(Glaucoma),FRCS(Glasg),FICO(UK),MNAMS
Assistant Professor of Ophthalmology
Glaucoma, Strabismology and Neuro-ophthalmology Services
Section IV – Dr R P Centre
OPD: Room no 36A, Monday/ Thursday – R P Centre OPD
Dr Dewang Angmocompleted herundergraduate training MBBS from the prestigious Maulana Azad Medical College (MAMC), Delhi University and joined her postgraduation MD (Ophthalmology) training from Dr Rajendra Prasad Centre for Ophthalmic Sciences (RPC), All India Institute of MedicalSciences (AIIMS), New Delhi. She then completed her Senior Residency in Glaucoma, Cornea, Cataract and Refractive Surgery services from RPC, AIIMSfollowed by DNB, FRCS(Glasg), FICO(UK) and MNAMS degrees. She also did a short term fellowship in glaucoma from Singapore national eye centre. Thereafter, she joined as Senior Research associate in RPC, AIIMS.She has also worked as Assistant Professor in Chacha Nehru Bal Chikitsalaya, New Delhi affiliated to MAMC, Delhi University. She is currently working as Assistant Professor at Dr RPC, AIIMS, New Delhi since November 2016.
Dr. Angmo has co-authored over 30 peer reviewed research papers in Ophthalmology. She has authored/ edited 2 text books in Glaucoma and has over 20 chapters in various national and international textbooks. Her research areas include the specialities of glaucoma, strabismus and neuro-ophthalmology.
She has received research awards and Young Investigator awards by various international and national societies like the World Glaucoma Congress (2015; HongKong), Asia ARVO (2015; Japan), and the Delhi Ophthalmological Society (2015). She has presented her original clinical and research work as scientific papers and has participated as faculty in several national and international conferences of her specialty.
She can be reached at dewang45[at]gmail[dot]com; drdewang[at]aiims[dot]edu
Dr Tanuj Dada is currently Professor of Ophthalmology and Head of Glaucoma Services at RP Centre for Ophthalmic Sciences, AIIMS-New Delhi. He is a graduate of AIIMS, New Delhi and was awarded the gold medals for best undergraduate and postgraduate in ophthalmology and best clinical research under the age of 35 years at AIIMS. He has over 300 research publications in peer reviewed indexed journals and has authored 5 textbooks on glaucoma.
He is editor of the All India Ophthalmological Society Guidelines for diagnosis and management of Primary Angle Closure Disease, Primary Open Angle Glaucoma and Glaucoma Surgery.
He serves on the Board of Directors of the Asia Pacific Glaucoma Society, as Secretary of the International Society Glaucoma Surgery and on the education consensus committees of the World glaucoma Association. He is Chief Editor of theJournal of Current Glaucoma Practice, Associate editor of the journal of glaucoma and on the editorial board of American journal of ophthalmology.
He has served on the International Council of Ophthalmology (ICO) committee for formulation of residency and glaucoma fellowship curricula, ICO glaucoma task force which published ICO global guidelines for Glaucoma eye care and as an expert WHO Development Group for the package of glaucoma interventions.
Current leadership positions include appointment as vice chair of the programme planning committee for World Glaucoma Congress (WGC 2023, international co-ordinator for glaucoma scientific programme at Asia Pacific Academy of Ophthalmology (APAO 2023) and chairman of scientific committee of Asia Pacific Glaucoma Society Congress (APGC 2022).
He has innovated several new techniques of Glaucoma surgery and pioneered the research on meditation and glaucoma.

In-charge, Unit-IV, Cornea, Cataract and Refractive Surgery Services
Dr. Rajendra Prasad Centre for Ophthalmic Sciences
All India Institute of Medical Sciences
New Delhi -110029, India
Dr. Namrata Sharma did her post-graduation from Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi.
She did her fellowship from Moorfields Eye Hospital in London, UK.
She is the Regional Secretary, Asia-Pacific Academy of Ophthalmology (APAO).
She is the Honorary General Secretary of All India Ophthalmological Society (AIOS).
Her clinical work includes phacoemulsification surgeries and foldable intraocular lens implantation and excimer laser refractive procedures such as Laser in situ keratomileusis (LASIK), Photorefractive Keratectomy (PRK) Small incision Lenticule Extraction (SMILE) and phakic intraocular lenses.
Her keen areas of interest are corneal transplantation including lamellar surgeries such as Deep anterior lamellar keratoplasty (DALK), Descemet’s Stripping Automated Endothelial Keratoplasty (DSAEK) and Descemet Membrane Endothelial Keratoplasty (DMEK), anterior segment reconstructive procedures, ocular surface surgeries and keratoprosthesis. Her areas of research include all aspects of corneal diseases (including Keratoconus, Fuchs dystrophy, Chemical Injuries, Corneal Ulcers and Steven Johnson Syndrome) cataract and refractive surgeries as well as laboratorybased stem cell based therapies.
Email: manpreet[dot]aiims[at]gmail[dot]com

| Title | Download |
|---|---|
| Invited Speaker in Conferences (International National) | 40 |
| Total Publications (International National) | 131 |
| Indexed Publications (Published / Accepted) | 62 |
| International Journals | 56 |
| National Journals | 06 |
Email: tusharagarwal[at]gmail[dot]com

Dr. Tushar Agarwal completed his graduation (M.B.B.S.) in 1998 from theUniversity College of Medical Sciences, Delhi University and PostGraduation in Ophthalmology (M.D.) from RP Centre, AIIMS in 2002. Hehas been on the faculty of the Dr. R.P. Centre for OphthalmicSciences, since September 2005, where he is currently working asAdditional Professor of Ophthalmology.
He completed his Senior Residency in 2005. His areas of specialization include Cataract, Cornea and Refractive Surgery. He has contributedseveral chapters to national and international books on ophthalmologyand published over 50 papers in international peer reviewed journals.His currently pursuing research in the areas of pediatric cataractsurgery, iris repair and reconstruction techniques ,Pterygiumand new techniquesof lamellar corneal surgery.
Currently he serves on the Editorial Board of the World Journal ofOphthalmology. He is/ has been a reviewer for the American Journal ofOphthalmology, British Journal of Ophthalmology, Ophthalmology,Journal of Cataract and Refractive Surgery and African Journal ofMicrobiology Research.He has been awarded the Indian National Sciences Academy (INSA) YoungScientist Medal for the Year 2004. He is the recipient of theAchievement Award and “Best of Show” Award by the American Academy ofOphthalmology. He was also awarded the ESCRS/Alcon video Prize forScientific Video by the European Society of Cataract and RefractiveSurgeons.
Dr. Shikha Gupta, M.D. works as Assistant Professor, at Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences (AIIMS), New Delhi since 2016. Dr. Gupta graduated in Medicine and completed post graduation in Ophthalmology from AIIMS. Subsequently, she obtained super specialty training in Cornea, Refractive Surgery, Pediatric Cataract and Glaucoma from the same institution. Dr. Gupta has co-authored over 70 peer reviewed research papers in Ophthalmology. She is the editor ' Textbook of Pterygium Management. 2016. Jaypee Medical Publishers'. Besides she has written many chapters for books on glaucoma. She is currently conducting research on newer therapies for neuroprotection.
Dr. Gupta has received research awards and Young Investigator awards by various international and national societies like the American Academy of Ophthalmology (2010), Asia ARVO (2011), All India Ophthalmological Society (2012, 2016), Glaucoma Society of India (2016) and the Delhi Ophthalmological Society (2012, 2014) on multiple occasions. Her surgical video on repair of post traumatic cyclodialysis has been recognized as amongst the best by the World Glaucoma Congress (2015). She was also awarded Prof. H. K. Tiwari Trophy (2011), Prof L.P. Aggarwal Trophy (2009) and Satyanand Gold Medal (2007) at AIIMS.
Email: drvinod_agg[at]yahoo[dot]com

Additional Professor,Vitreo-retina services at Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi 110029.
Email: dr[dot]rohanrpc[at]gmail[dot]com

Vitreo-Retina Uveitis
Medical School: Maulana Azad Medical College, New Delhi
Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi
3 years training in Vitreo-Retina
Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi
Fellow of the Royal College of Surgeons of Glasgow
Distinction in Ophthalmology in MBBS
Lt. Governer’s All Rounder Trophy in MBBS
More than 250 PUBMED indexed publications
Edited textbook on Ocular Tuberculosis
Reviewer of articles of International journals such as Ophthalmic surgery, Lasers and Imaging and American Journal of Ophthalmology and Indian Journal of Ophthalmology
Currently performing advanced vitreo-retinal surgery, treating medical retinal disorders and disorders pertaining to uveitis.
Email: parijatchandra[at]gmail[dot]com
Dr. Parijat Chandra completed his M.B.B.S. from the University College of Medical Sciences (UCMS), Delhi. He was awarded the Sridharan Gold medal in Anatomy, Sridharan Gold medal with distinction in Pharmacology; silver medals with distinction in Physiology, Biochemistry; and silver medal in Preventive & Social medicine. He was awarded silver medals for overall ranking in first and final MBBS.
He completed his M.D. (Ophthalmology) from the prestigious R.P. Centre, AIIMS in the year 2000. He was also awarded degree of D.N.B. (Ophthalmology) by National Board of Examinations. He completed his senior residency training in vitreoretinal surgery from R.P. Centre, AIIMS. Thereafter he joined the faculty in Dr. R.P. Centre, AIIMS and is currently working as Professor of Ophthalmology.
His key area of work is in research, management and surgery of paediatric vitreoretinal diseases, especially Retinopathy of Prematurity (ROP). He is a regular speaker at national and international conferences, and has 150+ peer-reviewed Pubmed indexed publications. He has been engaged in screening and management of ROP including ROP Surgery in AIIMS since last 24 years.
He has conducted nationwide ROP training workshops. He was Co-PI of the Sightsaver’s National ROP Project (2013-2016). He was organizing secretary of the 2nd World ROP Congress in New Delhi (2009) and Chief Scientific Program Coordinator of the 3rd World ROP Congress in Shanghai, China (2012). He organized the National ROP Summit supported by QEDJT (2013). He was awarded the prestigious Michael Trese Oration from the Indian ROP Society (2023) and ACOIN Felicitation Award (2016). He has been member of committees from NNF, WHO, RBSK Govt of India for formulation ROP related guidelines. He is member of the National ROP Task Force under the Ministry of Health and Family Welfare, Government of India.
He has been a coinvestigator in many multicentric international clinical trials like DEGAS, MONET, IMROP, MONET, SHIELD, RAINBOW. He mentors quality improvement teams in AIIMS and is AIIMS chapter leader at Institute of Healthcare Improvement USA at IHI.org.
Prof. Viney Gupta is Professor of Ophthalmology, Glaucoma Services of Dr Rajendra Prasad Centre for Ophthalmic Sciences ,All India Institute of Medical Sciences, New Delhi.
Member secy of the Academic committee of Dr Rajendra Prasad Centre for Ophthalmic Sciences
Has been Treasurer Glaucoma Society of India (2011-2013) .
Joint Organising Secretary, Annual Conference of Delhi Ophthlamological Society (2004).
Started the Indian Pediatric glaucoma Society and is the President and founding member of the Society.

Email: skhokhar38[at]yahoo[dot]com | skhokhar38[at]gmail[dot]com

Professor in charge Lens Clinic at RPC which deals with all forms of Pediatric cataracts including Congenital, traumatic and syndromic cataracts.
He has been invited to Sydney in 2011 to demonstrate and teach his techniques in Pediatric cataracts.
He was invited to take lecture for the Registrars in Ophthalmology at Hobart Sydney in 2013
Invited to take a class on Pediatric cataracts for FRCS Students at Royal Free hospital London in Sept 2014
The lens clinic has about 10 to 15 cases new cases every week ,thus being the largest center in world for pediatric cataract cases
He is teaching and performing cataract in Difficult situations for last 15 years .The cases of Subluxatedlenses,Irido Fundal colobomas,Traumaticcataracts,Non –Dilating pupils,Hard and supra hard cataracts ,Glaucoma patients etc
He is the pioneer in Phakic IOLs at the Centre ,started 9 years back and done more than 1000 eyes Corneal Ablative procedures are also been performed in unit IV under his guidance
He has travelled around the globe to present his pioneer work in Pediatric cataract in the European and Asia Pacific meets
Designed special cannula –Khokhar’s Capsular painting cannula for Phacoemulsification in white cataracts
Patents: Two
R.P Center
PUBLIC LECTURE : Children with disabilities -lets make their lives better(11/12/2014)
PUBLIC LECTURE : Recurrent Cough, cold and Wheezing in children: Is it ASTHMA ( 25/11/2014)
PUBLIC LECTURE IN GLAUCOMA- Improvements in Care ( 11/03/2015 )
PUBLIC LECTURE : BREAST & CERVICAL CANCER; Prevention and Managment ( 28/01/2015 )
PUBLIC LECTURE ON QUIT TOBACCO, CHOOSE HEALTH ( 30/05/2015 )
PUBLIC LECTURE ON HEALTHY BODY THROUGH HEALTHY MOUTH ( 20/03/2015)
PUBLIC LECTURE ON AUTISM AWARENESS : Bringing them into the Mainstream ( 30/014/2015 )
PUBLIC LECTURE ON HEAD & NECK CANCER: An Increasing Problem & Its Solutions ( 24/07/2015)
Public Lecture on HEPATITIS: Causes,Treatment and Preventions ( 28/07/2015 )
Ultrasound examination is a very important tool for investigation in retinal disorders, orbital diseases and other ocular pathologies. The lab has the latest equipment to perform A and B ultrasonography of the eye as well as orbit. It caters to a large number of patients from the outpatient department and wards. Provides useful information for diagnosis and management of several eye disorders
Research in various advances in cardiac Anaesthesia is in process. Every
year 20 Research papers are presented in various national & international
conferences. The faculty is being enlisted for guest lectures
1. Funded research projects completed-
* Professor Usha Kiran- one DST project
* Dr Neeti Makhija- two AIIMS projects
* Dr Poonam Malhotra Kapoor- 4 ICMR & AIIMS projects
* Dr Minati Choudhury- five
* Dr Sambhunath Das- one AIIMS project
2. PhD programme started with 3 students
3. Departmental clinical projects- till now approx 40 in number
Other facilities- ECMO services, transesophageal Echocardiography, Emergency cardiac care.
प्र.1:कोरोनरी धमनी रोग (सीएडी)किसे कहते हैं?
क: कोरोनरी धमनी रोग अत्यंत आम किस्म का ह्दयरोग है। यह रोग ह्दय की मांसपेशियों में रक्त की आपूर्ति करने वाली धमनियां (कोरोनरी धमनियां) के सख्त और संकरी होने पर होता है। यह भीतरी दीवारों पर कोलोस्ट्रोल तथा प्लेक नामक अन्य सामग्री जमने पर ऐसा होता है। इसे एथेरोस्क्लेरोसिस कहते है। इससे छाती में दर्द (एन्जायना) हो सकता है या दिल का दौरा पड़ सकता है। अधिकतर दिल के दौरे तब पड़ते हैं जब रक्त के थक्के अचानक ह्दय की रक्त आपूर्ति बंद कर देते हैं, जिससे ह्दय की स्थायी हानि होती हैं। समय के साथ-साथ, सीएडी ह्दय की मांसपेशियां कमज़ोर कर देती हैं और इससे ह्दयपात और एरिथमियां हो सकते हैं।
प्र.2: सीएडी की शिनाख्त़ प्रक्रियाएं क्या हैं?
क: सीएडी की शिनाख्त़ करने के लिए ईसीजी, इकोकार्डियोग्राफी, कोरोनरी सीटी एंजियोग्राफी तथा कार्डिएक सिंगल फोटोन एमिशन द्वारा परिकलित टोमोग्राफी (एसपीइसीटी), और कोरोनरी एंजियोग्राफी जैसी पद्धतियां अपनाई जाती हैं।
प्र.3: सीएडी का उपचार कैसे किया जाता है?
क: (i) चिकित्सीय प्रबंधन (ii)परक्युटेनियस कोरोनरी हस्तक्षेप-एंजियोप्लास्टी/स्टेंटिंग (iii)सीएबीजी(बायपास सर्जरी) (LV) कोरोनरी धमनियों की क्षति की तीव्रता और बायें वेंट्रिक्युलर (एलवी) कार्य की व्याप्ति के आधार पर चिकित्सक चिकित्सीय प्रबंधन थवा एंजियोप्लास्टी अथवा सीएबीजी का मशविरा देते हैं।
प्र.4: परक्युटेनियस कोरोनरी हस्तक्षेपके विभिन्न प्रकार क्या हैं?
क: (i) बलुनिंग (पीओबीए) (ii) बेयर मेटल स्टेंट (बीएमएस) आरोपण (iii) ड्रग एल्युटिंग स्टेंट (डीइएस) आरोपण आजकल, लगभग सभी एंजियोप्लास्टी में डीईएस आरोपण किया जाता है।
प्र.5: कोरोनरी एंजियोग्राम क्या होता है?
क: सीएडी की व्याप्ति एवं तीव्रता जानने हेतु सीएडी के निश्चित निदान और उसके सही उपचार के लिए कार्डिएक कैथ लैब में कोरोनरी धमनियों की इमेजिंग की जाती है। इसे कोरोनरी एंजियोग्राफी कहते हैं।
प्र.6: एंजियोप्लास्टी किसे कहते हैं?
क: एंजियोप्लास्टी वह प्रक्रिया है जिसमें कोरोनरी धमनियों के अवरोधित क्षेत्र खोलने के लिए गुब्बारे का इस्तेमाल किया जाता है। सीएडी के कुछ लक्षणों को कम करने के उद्देश्य से ऐसा किया जाता है। दिल का दौरा पड़ने पर हृदय को होनेवाली क्षति से बचाने के लिए भी ऐसा किया जाता है (प्राथमिक एंजियोप्लास्टी/स्टेंटिंग).
प्र.7: स्टेंट क्यों इस्तेमाल किया जाता है?
क: कोरोनरी धमनियों का अवरोध हटाने के लिए स्टेंट इस्तेमाल किए जाते है। स्टेंट एक छोटा-सा मेटल-मेश ट्यूब होता है जिसे कोरोनरी धमनी का अवरोधित क्षेत्र खुला रखने के लिए किया जाता है। इसके अलावा, ड्रग एल्युटिंग स्टेंट, धमनियें में दवाई डालते हैं। स्टेंटिंग प्रक्रिया के बाद धमनी में से गुब्बारा निकाल दिया जाता है, लेकिन कोरोनरी धमनी में स्टेंट रखा रहता है।
प्र.8: स्टेंट के विभिन्न घटक कौन-से हैं?
क: ड्रग एल्युटिंग स्टेंट निम्न से बनते हैं i) स्टेंट प्लॅटफॉर्म (स्टेनलेस स्टील, कोबाल्ट क्रोमियम, प्लॅटिनम क्रोमियम, इत्यादि) और बलून एक्सपांडेबल डिलीवरी प्रणाली ii) औषधीय एजेंट (एवरोलिमस, सिरोलिमस, इत्यादि) iii) दवा वाहक (उदाहरण पॉलिमर- नॉनबायोडिग्रेडेबल/बायोडिग्रेडेबल)विभिन्न व्यास एवं लम्बाई के स्टेंट उपलब्ध होते हैं। हमारे अस्पताल में,अनेक उत्पादकों के स्टेंट उपलब्ध हैं। एंजियोप्लास्टी के समय, उपचारकर्ता डॉक्टर, मरीज़ को उसकी बीमारी के अनुसार, कौन-सा स्टेंट उपयुक्त होगा, इसकी जानकारी देते हैं। हमारे वेबसाईट पर, विभिन्न प्रकार के स्टेंट और उनकी कीमत की जानकारी उपलब्ध कराई गई है।
प्र.9: प्राथमिक एंजियोप्लास्टी/स्टेंटिंग और उसकी लागत बताएँ।
क:दिल का दौरा पड़ने पर प्राथमिक एंजियोप्लास्टी/स्टेंटिंग की जाती है जो एक आपातकालीन प्रक्रिया है। हमारे अस्पताल में यह प्रक्रिया नि:शुल्क किया जाता है।
प्र.10: मैं स्टेंटिंगा की तैयारी कैसे करूं?
क: आपके डॉक्टर आपकी सम्पूर्ण चिकित्सा जांच करेंगे और आपको विस्तृत निर्देश देंगे। अस्पताल में आने पर अनेक प्रकार के रूटीन परीक्षण किए जाएंगे जैसे कि एक्स-रे, इलेक्ट्रोकार्डियोग्राम (इकेजी), इकोकार्डियोग्राफी अथवा रक्त जांच इत्यादि।
प्र.11: मुझे सरकार से लाभ कैसे प्राप्त होगा?
क: निर्धारित दिशा-निर्देशों के अनुसार आप प्रधानमंत्री जन आरोग्य योजना के अंतर्गत लाभान्वित हो सकते हैं।
प्र.12: मुझे कब तक स्टेंट रखना होगा?
क: कोरोनरी धमनी को दीर्घकालीन साबुत रखने के लिए उसमें स्टेंट लगाए जाते हैं।
प्र.13: क्या मुझे स्टेंट की अनुभूति होगी?
क: नहीं, आपको स्टेंट की अनुभूति नहीं होगी।
प्र.14: क्या स्टेंट हिल सकता है?
क: स्टेंट खोलकर कोरोनरी धमनी की भीतरी दीवार पर लगाने के पश्चात वो वहां स्थायी तौर पर रहेगा। it will remain in place permanently..
प्र.15: कोरोनरी स्टेंट कैसे काम करते हैं?
क:कोरोनरी स्टेंट छोटे, वायर मेश ट्यूब होते हैं जो अवरोधित धमनियों को चौड़ा करने और ह्दय में पर्याप्त रक्त प्रवाह पुन:स्थापित करने में सहायता करते हैं।
प्र.16: मैं कितने समय में कार्य पर लौट सकता हूँ?
क:अधिकतर लोग सफल प्रक्रिया के कुछ ही दिनों बाद काम पर लौटते हैं।
प्र.17:मैं अपनी नियमित गतिविधियां पुन: कब शुरू कर सकता/ती हूँ?
क:आपके डॉक्टर आपको बताएंगे कि नियमित गतिविधियां पुन: शुरू करना कब सही होगा। अधिकतर मरीज़, सफल एंजियोप्लास्टी के एक सप्ताह बाद अपना सामान्य रूटीन शुरू कर पाते हैं।
प्र.18: क्या मैं स्टेंट लगवाने के बाद खेल सकता हूँ?
क:आपके डॉक्टर आपको बताएंगे कि आपके लिए कौन-सी शारीरिक गतिविधियां सही हैं और आप कब खेल सकते हैं।
प्र.19: क्या मेरे स्टेंट से मेटल डिटेक्टर ट्रिगर होंगे?
क:नहीं, आपके कोरोनरी स्टेंट मेटल डिटेक्टर अलार्म ट्रिगर नहीं करेंगे और आप सुरक्षित तौर पर उनसे निकल सकते हैं।
प्र.20: एंजियोप्लास्टी/स्टेंटिंग के पश्चात मुझे कितने समय तक दवाईयां लेनी होंगी?
क: स्टेंट थ्राम्बोसिस (स्टेंट आरोपण के स्थान पर कोरोनरी धमनी में खून का थक्का) का जोखिम कम करने के लिए यह अत्यंत महत्त्वपूर्ण है कि आप अपने डॉक्टर द्वारा बताई गई दवाएं लें। यदि आप स्वस्थ महसूस कर रहे हैं, तो भी आप ये दवाईयां, विशेषकर ब्लड थिनर लेना तब बंद न करें जब तक कि आपके ह्दयरोगविशेषज्ञ नहीं कहते। यदि आपके ह्दय में ड्रग-इल्युटिंग स्टेंट लगाया गया है, तो आपको संभवत: एक वर्ष या उससे अधिक समय तक दवाईयां लेनी होंगी। अपने डॉक्टर के निर्देशों का अक्षरश: पालन करें।
प्र.21: क्या मुझे छाती में दर्द जैसे कोरोनरी धमनी रोग के लक्षणों का पुन: अनुभव होगा?
क: संभव है कि आपको पुन: इन लक्षणों का अनुभव होगा, जिसका कारण उपचारित कोरोनरी धमनी में नया ब्लॉकेज या अन्य स्थान पर नया ब्लॉकेज हो सकता है। यदि आपको ऐसा लगे, तो अपने डॉक्टर को तुरंत सूचित करें।
प्र.22: मुझे कैसे पता चलेगा कि मेरी धमनी पुन: संकरी हो गई है?
क: हालांकि रेस्टेनोसिस घटाने के लिए स्टेंट इस्तेमाल किए जाते हैं, फिर भी यह संभव है कि आपकी धमनी पुन:संकरी हो जाएँ। यदि ऐसा होता है, तो आपको वही लक्षण दुबारा अनुभव होंगे जो स्टेंट प्रक्रिया के पहले आपको महसूस हुए थे। ये लक्षण छाती में दर्द अथवा सांस लेने में कठिनाई जैसे हो सकते हैं, विशेषत: शारीरिक गतिविधि के दौरान। यदि आपको दर्द हो रहा है, तो तुरंत डॉक्टर को सूचित करें।
प्र.23: मैं लक्षणों की पुनरावृत्ति कैसे रोक सकता हूँ?
क: हालांकि लक्षणों की पुनरावृत्ति रोकने का कोई तरीका नहीं है, फिर भी आप व्यायाम, धूम्रपान न करके और स्वस्थ पोषण द्वारा इसका खतरा कम कर सकते हैं। अपने डॉक्टर से पूछें कि आपको अपनी जीवनशैली में कौन-से बदलाव लाने होंगे।
प्र.24: यदि मुझे फिर भी दर्द हुआ तो?
क:यदि आपको दर्द हो रहा है, तो तुरंत हमारे अस्पताल के आपात कक्ष में आएँ।
Patient education- perioperative psychological relaxation by RajYoga meditation.
CURRICULUM VITAE

Full Name: Dr (Prof) P Sarat Chandra,
Address: Professor, Head Unit I,
Dept of Neurosurgery, AIIMS,
New Delhi, 110029; Room 7, 6th floor, CN Center,
AIIMS. Phone (landline) 011-26546477;
Mobile- 9013605782;
Email:
saratpchandra3@gmail.com
saratpchandra@aiims.edu
Dr P Sarat Chandra is currently a senior Professor, Dept of Neurosurgery at the reputed All India Institute of Medical Sciences (AIIMS), New Delhi for 22 years.
Initial Education: Dr Chandra has graduated his MBBS with honors and distinction in Physiology and Surgery and was the best outgoing student of his batch (Pfizer gold medalist). He completed his neurosurgical training from NIMHANS, Bangalore and then joined AIIMS as a faculty in 1998.
Publications: Dr Chandra over his course of 22 years operated over 25000 cases, 2000 epilepsy surgeries and published 492 papers (https://scholar.google.com/citations?user=C_fTZQsAAAAJ&hl=en), was awarded 14 extra mural major research grants and 9 patents.
Research and contributions: He has 3 major research projects (funded by Dept of Biotechnology, Ministry of Science and Technology and Principle Scientific Advisor’s Office to the Prime Minister), completed 14 extra-mural research projects,
He has trained over 35 residents and PhD’s. Also 9 fellows in epilepsy & epilepsy surgery from several parts of India and other countries (Indonesia, Nepal, Kenya). All fellows have successfully established their own epilepsy surgery programs in their respective centres.
He established the Centre of Excellence for Epilepsy and MEG resource facility, the first of its kind of facility in India with [1.]Advanced epilepsy surgery centre [2.]Advanced brain mapping and electrophysiological centre [3.]Advanced molecular/intra-cellular electrophysiology. The centre has its own research faculty, PhD students, technicians and fellows (again for first time in India) for seamless integration of clinical/ research work to study causes of drug-resistant epilepsy. Till date > 10 PhD’s passed out are in full-time research careers in epilepsy. His centre helped in raising awareness towards epilepsy research in India.The YouTube link shows a short summary movie about the COE and MEG resource facility and its achievements. https://youtu.be/EiXyk1HdA4E
Dr Chandra is also the lead Principle investigator for a prestigious project “Advanced research for epilepsy”, a multi institutional first of its kind of project funded by Office of Principle Scientific Advisor (PSA) to Govt. of India (Role of dysfunctional benzodiazepine binding site on GABAA receptor in benzodiazepine-resistance; mass spectrometric lipid profiles in FCD’s and molecular modelling/identification of novel drug targets).
He has 9 patents, including 1 patent with USA and PCT (Paris Convention Treaty) International patent. He has developed new surgical techniques for the first time which have been validated and published. These include 1.] Endoscopic Hemispherotomy for epilepsy: a minimally invasive procedure, 2.] Robotic thermocoagulative hemispherotomy: a bloodless surgery 3.] Endoscopic corpus callosotomy for epilepsy: a minimally invasive procedure to treat severe drug resistant epilepsy 4.] Radiofrequency ablation disconnection of hypothalamic hamartoma using Robotic and O-arm guidance: a minimally invasive technique for these challenging lesions. 5.] Distraction, Compression, Extension and Reduction (DCER) for severe AAD and Basilar invagination in a single stage surgery.6.] Expandable tubular retractor for endoscopic pituitary surgery. 7.] Portable video EEG system with link to a mobile app and AI (along with IIT-D), called EPISAVES-see below.
His key areas of research include: Study of various bio-markers/receptors in abnormal epileptogenic areas (histone deacetylases alterations, altered kynurenine pathway metabolism, IDH-R132H-FAT1-ROS-HIF-1alfa signalling pathways, mTOR pathway in FCD’s, genome-wide DNA methylation and RNAseq analysis, GABA receptor mediated epileptogenicity, epigenetic regulations, endogenous activity of NMDA receptors, dual networks)
Some specific contributions for epilepsy:
Dr Chandra has organized several International meetings/teaching programs to enhance Epilepsy Surgery outreach along with several invited International faculty. Some include [1.] Annual COE EEG & epilepsy surgery Master Classes organized in various parts of India, 2012-2020 (8 years, AIIMS Rishikesh, AIIMS Raipur, BHU Varanasi, AIIMS Bhubaneswar, AIIMS Patna, & AIIMS Delhi) [2.] Epilepsy Schools at AIIMS Jodhpur (2019) [3.] Asian Epilepsy Surgery Congress, Udaipur, 2015 [4.] Organizer and faculty for Epilepsy Conclaves 2016-2018 [5.] Current trends in Epilepsy with host of International faculty 2006 [6.] ILAE & ASEPA workshop on epilepsy surgery, 2009 [7.] 1st Indo-German Neurosurgical meeting of Neurological Society of India Annual Congress (>4000 delegates).
He delivered Invited lectures (>100) in several International congresses. Some include ILAE (IEC, Vienna, 2018, AOEC (2016, 2007) , AESC (2020, Taiwan, online; 2019 Japan; 2018 Shanghai; 2016 Korea; 2015 Udaipur; 2012-2020) and ESTM (Gothenburg 2014, Prague 2016, Vienna 2018 and online in 2020), Japanese epilepsy society (2018,2017, 2016, 2008), CNS(Houston, 2018; Boston 2017); Annual Congress of Japanese Neurological surgeons (2017). His talks focus on developing strategies to make epilepsy surgery affordable and effective in developing countries especially based on this own experience of >2000 cases. He also advocates the need to amalgamate research with clinical work and the need to enhance epilepsy surgery outreach. He has described new techniques on epilepsy surgery: Endoscopic hemispherotomy/corpus callosotomy and Robotic thermo-coagulative hemispherotomy (ROTCH). The latter is a “bloodless” technique of hemispherotomy using thermo coagulation disconnection (https://www.youtube.com/watch?v=qRUfiPp5csU&t=3604s), now published in JNS Pediatrics.
He has performed demonstration surgeries in India and internationally, teaching epilepsy surgeries along with minimally invasive techniques (Mumbai, Surat, various AIIMS, Delhi, Jabalpur) and also in various countries (Kula Lumpur, Malaysia 2016, Indonesia 2013, 2015, 2017, 2018; Morocco 2015,2016, 2017, 2018; Kathmandu 2015, 2017, 2018). Most demonstrations also include endoscopic hemispherotomy and corpus callosotomy which has reduced morbidity and duration of hospital stay significantly.
He is on executive board of several International bodies [1.] Member, Epilepsy Surgery Task Force, ILAE (https://www.ilae.org/p-sarat-chandra) [2.] Member, Epilepsy Surgery, Developing World, ILAE (https://www.ilae.org/p-sarat-chandra) [3.] Co-Chair, Epilepsy Surgery section, AOEC, ILAE [4.] President Elect, Indian Epilepsy Society (IES), local chapter affiliated to ILAE [5.] Faculty 1000, ILAE [6.] Ex member, Paediatric Epilepsy Surgery Sub-commission, ILAE [7.] Ex-President, Asian Epilepsy Surgery Congress [8.] Ex board member of Indian Epilepsy Society [8.] Ex-Board member for Society for Brain mapping and therapeutics (SBMT).He has been on board the paediatric sub-commission to create the guidelines for paediatric epilepsy surgery. He has contributed towards Guidelines for epilepsy management in India (GEMIND), which is now online.
As a Co-Chair of Epilepsy Surgery of AOEC, he is conducting epilepsy-surgery sensitization classes for Nepal and Bhutan. He is developing an mobile app for collecting epilepsy surgery database from developing countries in Asia. The app is so designed to be intuitive, easy to use to allow easy entry of data. This would be the first of its kind for Asia and AOEC.
He was the main contributor for surgery for surgical arm for the first ever RCT for paediatric epilepsy surgery [Diwedi R et al; N Engl J Med 2017 Oct 26;377(17): 1639-1647; https://pubmed.ncbi.nlm.nih.gov/29069568/; Chandra PS et al; N Engl J Med 2018 Jan 25;378(4):399; https://pubmed.ncbi.nlm.nih.gov/29365299/]. The study demonstrated a 10 fold improvement of good outcome for surgery in Children vs medical treatment (77% vs 7%). It also demonstrated better cognitive outcomes for surgery in Children with drug resistant epilepsy as compared to medical therapy demonstrating the need for early surgery.
He contributed for HOPS (Hemispherectomy-Outcome-Prediction-Scale study, LANCET, https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3514748). The study analysed 1237 hemispheric surgeries in paediatric patients, 31 centres, 12 countries to identify predictors of seizure freedom after surgery.
Epilepsy Self-help social groups: Co-founder of Ekatwam. This group is involved in providing free medicines and helping poor patients with the cost of epilepsy surgery. This group has now helped > 10,000 patients. (https://www.facebook.com/pages/category/Non-Governmental-Organization--NGO-/Ekatwam-Epilepsy-Delhi-243645915696765/).
Specific contributions for Spine: Dr Chandra has been a pioneer from developing new techniques for cranio-vertebral junction especially for congenital
Others: He has been part of National program for development of a National program for epilepsy surgery collaborating with the Ministry of Health Government of India (Chandra PS et al. Epilepsy surgery: recommendations for India. Ann Indian Acad Neurol. 2010; https://pubmed.ncbi.nlm.nih.gov/20814490/).
Summarizing his primary area of focus has been Epilepsy, Epilepsy surgery and epilepsy networks where he has contributed significantly providing new surgical techniques, understanding mechanisms of epileptogenesis and epilepsy networks and also provided and created research and training facilities to take this further. He has also contributed in spine (cranio-vertebral junction and Vertebral body haemangiomas) by creating new surgical techniques, patenting new instruments and implants which have made the surgery easier, safer, and with less morbidity. He also has had significant experience in minimally invasive skull base surgery, robotic neurosurgery and cerebrovascular surgery. He also occupies leadership positions in several scientific societies and bodies.
Dr P Sarat Chandra is currently working as Professor and Head of Unit I at the Dept of Neurosurgery, AIIMS, Delhi. He is the Team Leader for Centre of Excellence for Epilepsy (COE) and the faculty in charge for the Epilepsy Surgery and Functional Neurosurgery Fellowship Program in AIIMS.
| 1.] A compact-portable ambulatory video electroencephalography (VEEG) unit for seizure monitoring and comprehensive care for epilepsy patients (In Process)- Figure 6 | Dr P Sarat Chandra Dr Manjari Tripathi Kirandeep Kaur Amol Bhardwaj Anmol Gupta Dhananjay Goel | Indian Paten 201811033960 | 10.09.2018 |
| 2.] Implant system to enhance the cervico-occitial (cranio-vertebral junction) stabilization- commercialized with Medsolutions via FITT, IIT, Delhi- Figure 7- lower part | Dr P Sarat Chandra P Prarthana Chandra | Indian Patent 201911002700 | 22.01.19 |
| 3.] A disposable nasal retractor for endoscopic trans-sphenoidal pituitary gland surgery- commercialized with Walnut Medicals- Figure 9 | Dr P Sarat Chandra Kirandeep Kaur | Indian Patent 201911005181 | 09.02.19 |
| 4.] Disposable multi-port system for cranial endoscopic surgeries- In process for commercialization with Walnut Medicals | Dr P Sarat Chandra P Prarthana Chandra | 201911012505 | 23.03.19 |
| 5.] Novel techniques for reduction of basilar invagination and atlanto axial dislocation and surgical instruments thereof. The technique is in process with Medtronic (Mempis) for Commercialization of a universal spine reducer using this his, USA) as a industry-institute collaborative project- | Dr P Sarat Chandra AIIMS, Delhi | S20160128736A1 United States/ PCT patent US14/897,156 https://patents.google.com/patent/US20160128736 | 2014 |
Occipto-C1 and C2 spacer (Indian Patent Application No. 201611023116 dated July 5, 2016)
commercialized with Medtronics via AIIMS, Delhi- Figure 7- upper part | Dr P Sarat Chandra AIIMS, Delhi | Patent 201611023116 | July 5, 2016) |
| 6.] Designed a “disposable endoscopic carpal tunnel release set”- commercialized with AVM surgical via NRDC, Delhi | Dr P Sarat Chandra Dr Manjari Tripathi AIIMS, Delhi | Patent application no. 306/Del/ 2009 | 17.02.2009 |
| 7.] Designed a “special monopolar cautery”- Commercialized- AVM Surgicals | Dr P Sarat Chandra Nirmal Thakur AIIMS, Delhi | ||
| 8.] Multielectrode point radio frequency ablation device for performing bloodless epilepsy surgery | Dr P Sarat Chandra |
| Project No. | Grant | Research proposed | Research outcome |
|---|---|---|---|
| 1. | Principal Scientific Advisor, (PSA), Govt of India | Development and demonstration of a portable device for rapid detection of epileptiform discharges | Portable device development for rapid detection of epileptiform discharges in low cost clinical settings |
| b) Investigating the role of dysfunctional benzodiazepine binding site on GABA A receptor in benzodiazepine resistance associated with drug resistant epilepsy | Benzodiazepine resistance is caused by alterations in expression levels of GABA A receptor subunits in DRE | ||
| c)Investigating the role of mass spectrometric lipid profiles of brain tissues resected from patients with focal cortical dysplasia in defining the epileptogenic zone | Epileptogenic zone of Graded tissue of FCD is being demarcated by using the expression of lipids in those regions as biomarkers. | ||
| d) epilepsy research i)molecular modelling to understand resistance to anti epileptic drug ii)identification of novel drug targets using tools of data science | Development of resistance in DRE by molecular modelling of drug targets using bioinformatics tools | ||
| 2. | COE Phase II, DBT, Govt of India | a) Eloquent cortex mapping in chronic intractable epilepsy using Nex-Stim Navigated brain stimulation system (NBS), functional MRI and MEG: A comparative study. | Accurate localisation of epileptogenic zone by various imaging techniques leads to better management of seizures |
| b) Investigating the role of metabolites and neurotransmitters in abnormal synaptic transmission associated with mesial temporal lobe epilepsy (MTLE) and focal cortical dysplasia (FCD): Possible biomarkers for localization of epileptogenic foci. | Alterations in the frequency and amplitude of EPSPs after kyunurenic acid application Alterations in levels of glutamate and GABA neurotransmitters in DRE leading to hyper excitability | ||
| c) Validation of the potential candidate genes identified in both MTLE and FCD patients for their possible role as prognostic/diagnostic biomarkers. | Various genes like FN1, TGFbeta, SMAD3, MMP9 are found to be altered in DRE patients and can be used as potential diagosnitic biomarkers | ||
| 3. | SERB, DST, Govt. Of India | Deciphering the role of casein kinase 2 in mesial temporal lobe epilepsy | Alterations in CK2 levels in MTLE contribute to hyperexcitability associated with MTLE |
| 4. | DBT, Govt of India | Role of kynurenic acid, a glutamate receptor inhibitor, in hyper excitability associated with mesial temporal lobe epilepsy | Reduced kynurenic acid relates to alterations in hyperexcitability in mesial temporal lobe epilepsy |
Figure 1: Shows various photographs in their respective timelines showing the establishment of MEG centre at National Brain Research Centre (NBRC). This centre has been established as a part of Centre of Excellence for Epilepsy as a collaborative project between AIIMS (New Delhi) and NBRC. Till date, more than 1700 MEG’s have been performed from all over the country and also from neighbouring countries like Bangladesh, UAE, and Nepal. All MEG’s are done completely free of cost.

Figure 2: The following figure collage shows the major achievements of Phase I COE under the leadership of Nominee, Dr P Sarat Chandra
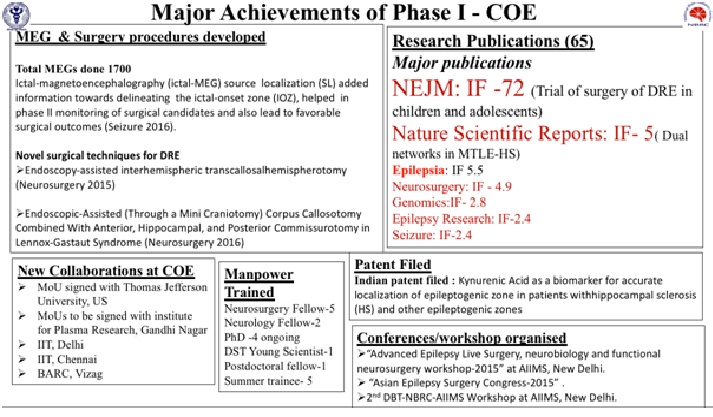
Figure 2: The following figure given below shows the capability of COE in creating advanced algorithms to localize epileptogenic networks. The networks are localized first by using MEG (using CURRY and S-Loretta software), followed by coherence studies which provides connectivity patterns in the brain. Coherence basically indicates identifying networks of neurons in the brain which fire at same frequency. There are reasons to believes based on Nominee’s studies that coherent neurons are connected with each other in patients with epilepsy. Such findings provide valuable insights to identify networks in persons with drug resistant epilepsy.
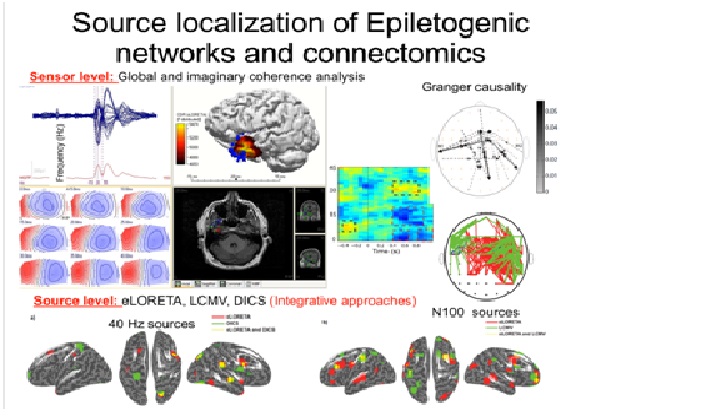
Figure 3: : The following figure shows the main components of the COE for which the Nominee is the PI and Team Leader. These include [1.] The Epilepsy surgery division [2.] Clinical Electrophysiology [3.] The MEG and Brain mapping centre located in the National Brain Research Centre [4.] Intra-cellular electrophysiology and molecular division. Such a multi-team and multi-speciality centre is the first of its kind for the country, and even for the whole South East Asia.
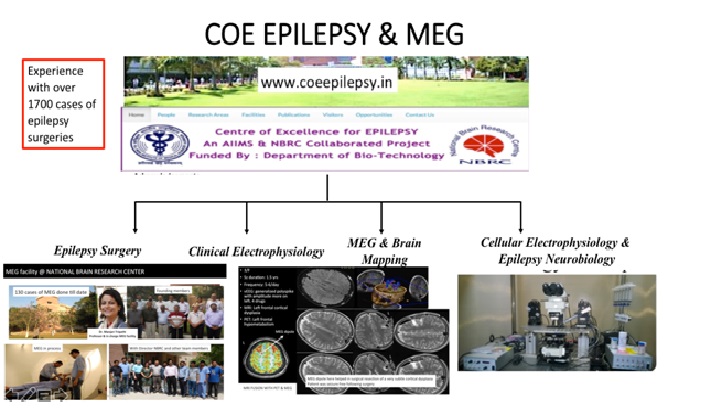
Figure 4: The following figure collage given below shows the capability of Cellular electrophysiology and Epilepsy Neurobiology lab (located in the convergence centre, AIIMS, named after Prof PN Tandon). This division has the capability of recording EPSC’s from live neurons provided from surgically resected brain samples which are carried to this lab within 10 minutes of surgical resection. This provides again valuable insights into connectivity patterns at the cellular and molecular level. The following figure collage given below is an excerpt from the publication in Scientific reports (Nature) which demonstrated for the first time, 2 separate networks, one from hippocampus and the other from the anterior temporal lobe. Such a finding provided immense translational value providing evidence at cellular level to perform an anterior temporal lobectomy + amygdalo-hippocampectomy as opposed to performing selective amygdalo-hippocampectomy. Such an evidence was earlier favoured by well known the meta-analysis performed by Josephson (Neurology, Impact factor 8.03). However, our study was the first of its kind to demonstrate this at the cellular level.
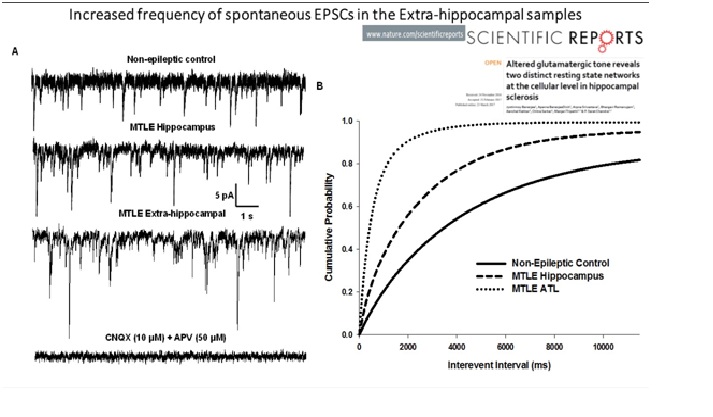
Figure 5: Interview of the candidate Prof Chandra published in the reputed Japanese medical magazine Practical Neurosurgery currently on the new technique developed by him on Epilepsy Surgery
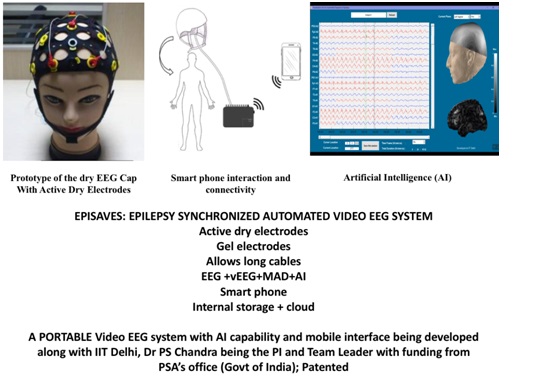
Figure 6:
Figure 7: The technique of DCER for severe AAD and basilar invagination is patented, validated (>200 papers) and published. It is an established procedure which reduces operative time, morbidity, and hospital stay by> 50%. The nominee is also developing new implants and instrument in collaboration with DBT and Medtronics.
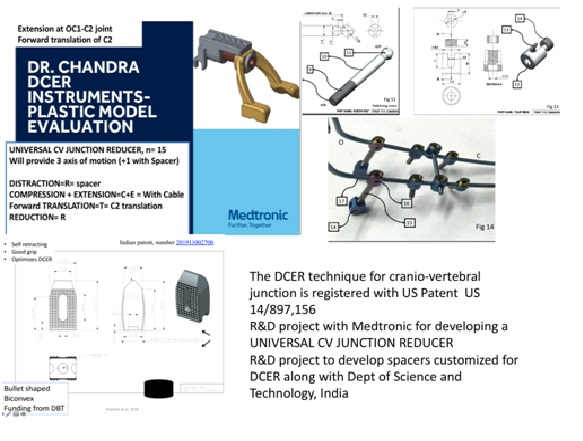
Figure 8: The technique of absolute alcohol embolization for vertebral hemangioma was published in several newspapers after it cured a young pregnant lady, wife of a reporter who came completely paraplegic during pregnancy. Following treatment, she became completely normal and delivered a normal healthy boy.
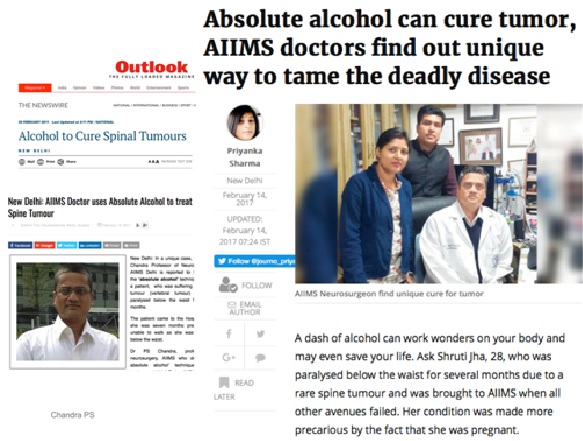
Figure 9:
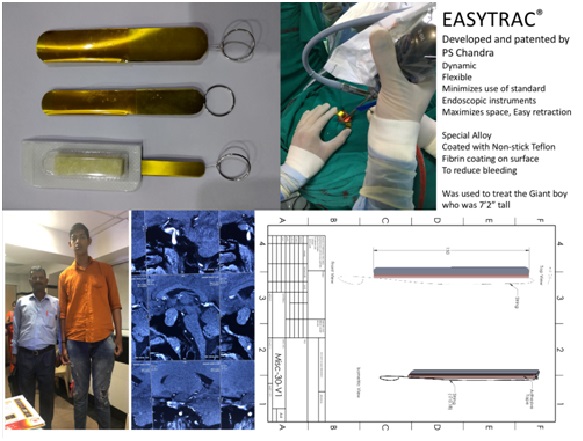
*Chapters as shown in list above and also as a screen shot are the techniques developed by the author for the first time in literature and now accepted worldwide and also standard chapters in textbooks. The above 2 textbooks are highly reputed textbooks in this field.
Please SEE complete references (Total 392) at the end1-173174-392
| S. No. | Conference Title/Agenda | Year | Venue |
|---|---|---|---|
| Conferances, Guest Lectures & Visiting Professor: | |||
| 1 | Indian Epilepsy School 2019 – Faculty Presented 2 lectures of 1.] Disconnective Epilepsy Surgery 2.] Resective Epilepsy Surgery | 22nd to 25th Aug 2019 | Jodhpur |
| 2 | Korean Cervical Spine Research Society-13th Annual Meeting of the Korean Cervical Spine Research Society Presented Key note Oration Reducing severe AAD and BI using the DCER principle | 8th June 2019 | Korea |
| 3 | 3rd International Conference on Clinical Spine & Orthopedic BIOMECHANICS Presented on the biomechanics of Cranio vertebral junction | 26th to 28th April 2019 | New Delhi |
| 4 | American Association of Neurological Surgeons Presented Invited lecture symposium on “ Endoscopic Hemispherotomy: From Concepts to Practice” | 13th to 17th April 2019 | San Diego |
| 5 | 11th Annual Conference CME Credit Hours 2 – MPMC/CME-08/2019/505 | 4th April 2019 | Bhopal |
| 6 | NEURO ENDOCON 2019 Invited faculty: gave lecture on Endoscopic management of Large Intra ventricular tumors | 29th to 31st March 2019 | Madurai, Tamil Nadu |
| 7 | CAWNPORE NEUROLOGICAL SOCIETY 2019, Kanpur Guest Faculty in UP-UK-NEURON 2019 | 2nd & 3rd February 2019 | Kanpur |
| 8 | ASSICON 2019-32nd Annual Conference of Association of Spine Surgeons of India Invited Faculty | 24th to 27th January 2019 | Ahmedabad |
| 9 | 15th Instructional & 9th Foundation Course participated as Faculty organized by Neurological Society of India | 12th & 13th January 2019 | Cuttack, Orissa |
| 10/td> | 4th ASSICON, International Congress on Minimal Invasive Neurosurgery Faculty | Jan, 19-21, 2018 | Chennai, India |
| 11 | AIIMS Microneurosurgery Workshop Faculty, Gave live surgical demonstration | Feb 15-17, 2018 | AIIMS, New Delhi |
| 12 | NESON, Nepal Faculty and lecturer | Mar 5-7, 2018 | Nepal |
| 13 | NEUROCON, Nagpur Faculty, presented multiple lecutures | Apr, 1-5, 2018 | UP, India |
| 14 | Annual Congress on Skull Base Surgery(SBSSI) Faculty | Apr, 4-6, 2018 | Chennai, India |
| 15 | 2nd ASSI (Association of Spinal surgeons of India) Conference, Faculty | May, 8-9, 2018 | New Delhi, India |
| 16 | Indian Epilepsy Society Conference Faculty | May, 18-19, 2018 | New Delhi, India |
| 17 | ISC (Instructional Spine Course) Faculty | July, 9-10, 2018 | Amritsar, Punjab, India |
| 18 | Neurotrauma Conference Faculty | Aug, 16-19, 2018 | AIIMS, New Delhi, India |
| 19 | 13th European Congress on Epileptology Presented paper on “Endoscopic hemispherotomy” Faculty | Aug, 26-30, 2018 | Vienna, Austria |
| 20 | Neurovision Faculty | Oct, 9-10, 2018 | Bhubaneswar, Orissa |
| 21 | Congress of Neurological Surgeons, Annual Meeting Faculty | Oct, 5-9, 2018 | Houston, Texas |
| 22 | 52nd Congress of Japanese Epilepsy Society Faculty Invited Oration: Optimizing Surgical Strategies to make Epilepsy Surgery affordable in Developing Countries. | Oct, 23-24, 2018 | Yokohama, Japan |
| 23 | 12th Asian Epilepsy Surgery Conference Faculty | Oct, 26-27, 2018 | Bali, Indonesia |
| 24 | 15th EEG workshop and Masterclass in Epilepsy -Organiser, presented multiple lectures on Epilepsy Surgery and EEG | Nov, 22-24 | Varanasi, UP |
| 25 | 67th Annual Conference of the Neurologocal Society of India Faculty | Dec, 13-16, 2018 | Jaipur Rajasthan |
| 26 | Neurological Society of India annual congress -Chaired session on cranio-vertebral junction anomalies -Spoke on Endoscopic hemispherotomy | 30th Nov-2nd December, 2017 | Nagpur, India |
| 27 | Asian Epilepsy surgery congress - Participated as board member - Gave lecture on the following topics - Robotic radiofrquency ablation of hypothalamic hamartomas - Endoscopic hemispherotomy - First Radomized trail for Pediatric epilepsy surgery published in NEJM | 17-19th, November, 2017 | Shanghai, China |
| 28 | Annual Skull Base Surgery congress -Participated as secretary general -Lecture on Trans-septal endoscopic robotic approach to supra sellar lesions and tumors | 27-29th October, 2017 | Cochin, India |
| 29 | 76th Annual congress of neurological surgeons of Japan - Gave luncheon seminar on “Epilepsy surgery” - Spoke on “Endoscopic hemispherotomy” | 13th October, 2017 | Nagoya, Japan |
| 30 | CNS-Boston- Faculty, Participated in the following events - Moderated the symposium on minimally invasive epilepsy surgery and spoke on endoscopic hemispherotomy - Talk on Utilizing the DCER priniciple to reduce severe basilar invagination and atlanto axial dislocation | 8-11th October, 2017 | Boston, USA |
| 31 | NEUROVASCON: Faculty: Clipping techniques of complex posterior aneurysms | 15-17th Septermber, 2017 | Delhi, India |
| 32 | Epilepsy Surgery Update: Participated in this congress as the Chief faculty, provided several lectures and performed live surgery | 23rd July, 2017 | Surabaya, Indonesia |
| 33 | Asian Congress of Neuro Surgeon Congress (ACNS) Participated as faculty and presented paper on- Eyebrow keyhole mini-fronto orbital craniotomy approach to anterior circulation aneurysms | 19-22nd July, 2017 | Indonesia |
| 34 | INI International Neurosurgical Congress, Hannover. Participated as faculty and presented paper on “Endoscopic hemispherotomy and corpus callosotomy” | 16-19th June, 2017 | Hannover, Germany |
| 35 | SPINE Update: Participated as faculty and presented on the DCER principle for CV junction anomalies | 30th April, 2017 | Vadodara, Gujrat |
| 36 | Neurosurgery Update: Participated as faculty and presented on endoscopic hemispherotomy | 15-16th April, 2017 | Agra, India |
| 37 | Neuroendocon annual congress, Participated as faculty and presented on -Endoscopic hemispherotomy -Robotic guided trans-septal approach to pituitary tumors | 7-8TH April, 2017 | Jaipur, India |
| 38 | Ginde oration: Mumbai Delivered guest lecture and operated a live surgery on endoscopic hemispherotomy as part of the CME operative workshop | 22n-23rd March, 2017 | Mumbai, India |
| 39 | CTRF: AIIMS, Delhi, Participated as faculty and gave hands on demonstration on DCER technique for CV Junction | 19th March, 2017 | AIIMS, New Delhi |
| 40 | NESON: Nepalese neurosurgical society annual meeting; Participated as faculty and presented a paper on “Strategies to localize epileptogenic networks” | 10th March, 2017 | Kathmandu, Nepal |
| 41 | Clinical Spine Biomechanics: Participated as faculty and presented “Biomechanics of CV Junction | 4th March, 2017 | ISIC, Delhi |
| 42 | Faculty and gave a lecture at the Epilepsy Congress on : Epilepsy networks for planning surgical strategies | 17-19th February, 2017 | Patna, India |
| 43 | Visiting Professor, Univerisity hospital, Kuala Lumpur, Malaysia. Performed a live operative case of endoscopic hemispherotomy | 1st-3rd, December, 2016 | Kula Lumpur, Malaysia |
| 44 | Indian Epilepsy School. Participated as faculty and presented the following topic: Advances in surgical strategies to localize epileptogenic networks | 25-27th, November, 2016 | Ludhiana, India |
| 45 | 24th Annual congress of Indian Academy of Neurology. Participated as faculty and presented the following lecture 1.) Neuromodulation techniques to manage drug refractory epilepsy | 11th November, 2016 | Kolkotta, India |
| 46 | Neurovision, a CME on neurosciences. Participated as guest faculty and spoke on following topics 1.) Strategies to localize epileptogenic networks 2.) Management of low grade gliomas in eloquent cortical regions | 10th, November, 2016 | Bhubanesar, Odisha |
| 47 | Epilepsy Surgery Symposium, participated as faculty and presented the following topics 1.) The utility of MEG for localization of epileptogenic networks 2.) Use of robotic SEEG to localize epileptogenic networks following a robust hypothesis following video EEG, SPECT, PET, and MEG 3.) Endoscopic hemispherotomy | 7-8th November, 2016 | Bangalore, India |
| 48 | Asian Epilepsy Surgery Congress, participated as President and presented the following lectures 1.) Endoscopic disconnection techniques 2.) Development of Epilepsy surgery in India | 4-5th, November, 2016 | Incheon, Korea |
| 49 | Visiting Professor, University hospital Rabat, Morocco: Operated 2 cases of hemispherotomies and presented several papers on epilepsy surgery and pre-surgical localization techniques. This was the first time that hemispherotomy was performed in Morocco | 23rd-28th, October, 2016 | Rabat, Morocco |
| 50 | International Spine and spinal injuries congress, participated as faculty and presented the following paper “Reduction of old C2 fractures using DCER principle” | 6-8th October, 2016 | Kathmandu, Nepal |
| 51 | 27th Annual INDSPN conference & ISPN CME, participated as faculty and presented “Newer strategies for pediatric epilepsy surgery” | 1-4th October, 2016 | AIIMS, New Delhi |
| 52 | Asia Spine Congress, Participated ad faculty, presented the following paper “Reducing severe cranio-vertebral junction deformity using DCER principle” | 22-24th September, 2016 | Seoul, Korea |
| 53 | Epilepsy Surgery Techniques, conducted by International League against epilepsy Presented the following paper as faculty “Endoscopic hemispherotomy” | 17th September, 2016 | Prague, Czeh Republic |
| 54 | SKULL BASE CON 2016, Participated as the general secretary of SBSSI and also presented the following lecture “Reduction of severe deformity, decompression of the spinal canal and stabilization of severe AAD and basilar invagination using the DCER principle” | 8-11th September, 2016 | Jaipur, India |
| 55 | CME on Endoscopic techniques for epilepsy surgery- Participated as the only Chief faculty and demonstrated a live operative case of endoscopic hemispherotomy | 23-28th August, 2016 | Kulala Lumpur, Malaysia |
| 56 | Advanced spine workshop- Participated as faculty, gave lecture on “Reduction of severe AAD and basilar invagination using the DCER principle”. Demonstrated live operative cases of severe basilar invagination | 13-14th August, 2016 | AIIMS, Delhi |
| 57 | CME on Epilepsy update- Participated as faculty presented lectures on epilepsy surgery and operated 2 cases of mesial temporal sclerosis as live surgical demonstration | 6-7th August, 2016 | Surat, India |
| 58 | ASRAM neurocon-2016- Participated as faculty, presented various surgeries and performed live operative cases of endoscopic CSF repair and acoustic schwanomma | 29-31st July, 2016 | Eluru,India |
| 59 | CME on craniovertebral junction anomalies. Faculty- presented various lectures and demonstrated a live operative case | 22-23rd July, 2016 | Jabalpur, India |
| 60 | 3rd Walter Dandy Educational course- Faculy, Presented the following lectures -Vascular bypass techniques - Micro surgical clipping of Acom aneurysms | 14-16th July, 2016 | Udaipur, India |
| 61 | 7th India-Japan Neurosurgical conference- Presented the following topic- Endoscopic disconnective techniques for epilepsy surgery | 18-20th June, 2016 | Osaka, Japan |
| 62 | 6th International Neurosurgery update and educational initiative of the Asian Australian Sociaty of Neurological Surgeons. Participated as faculty, gave the following lecture- Surgical strategies to manage gliomas located in eloquent regions | 4-5th June, 2016 | Mumbai, India |
| 63 | Participated as faculty and conducted the following activities -Chairperson for plenary session -Lecture given “Determinants for epilepsy surgery outcomes” | 28-29th May, 2016 | EPILEPSY CONCLAVES, Pune, India |
| 64 | Participated as faculty, gave the following plenary lecture - Endoscopic applications of Epilepsy surgery - Co-author for paper “The role of MEG propogation to localize the epileptogenic networks” | 15th, May, 2016 | Asiano-Oceanic Epilepsy Comission Congress, ILAE, Hong Kong AOEC is the largest congress of this region for Epilepsy. |
| 65 | Participated as faculty -Operated live surgery of a case with severe basilar invagination and atlanto axial dislocation -Gave a lecture on “The technique of DCER for correcting BI, AAD and deformity” | 6-8th, April, 2016 | AIIMS, New Delhi |
| 66 | Conducted a cadaveric workshop and delivered 2 guest lectures on a workshop for Cranio-vertebral junction anomalies -Trans laminar screw fixation and occipito-cervical fixation -The technique of DCER for cranio-vertebral junction anomalies surgery | 23-24th, April, 2016 | PGIMER, Chandigarh |
| 67 | Delivered the following plenary lectures -Endoscopic applications in Epilepsy Surgery -Localizing epileptogenic networks for planning surgical strategy | 17-19th April, 2016 | 5th Symposium of World Federation of Neurosurgical Societies (WFNS) and MASSIN interim meeting, Tehran, Iran |
| 68 | Participated as faculty, delivered the following lectures - Endoscopic applications for epilepsy surgery - Endoscopic excision of intraventricular tumors | 15-16th April, 2016 | 3rd Neuroendoscopic conference, AIIMS, New Delhi |
| 69 | Delivered the following guest lectures -Basilar invagination, incidence and management -Complication avoidance in cranio-vertebral junction surgery with case vignettes | March, 2016 | Spine Summit (Joint congress of CNS, NASA) Orlando, US |
| 70 | Delivered the following guest lectures -A new technique to reduce basilar invagination and atlanto axial dislocation -Plenary session: Overcoming barriers of epilepsy surgery in resource poor countries | March, 2016 | 11th Asian Congress of Neurosurgeons Society (ACNS), Surabaya, Indonesia |
| 71 | Demonstrated Live Surgery of DCER in congenital basilar invagination and atlanto axial dislocation | March, 2016 | Live Annual Microneurosurgery workshop, AIIMS, New Delhi |
| 72 | Dr AD Sehgal Oration; Annual Epilepsy Congress (Indian Epilepsy Society): Creating Cost effective and efficacious strategies for Epilepsy Surgery for Inida | February, 2016 | Annual Epilepsy Congress (Indian Epilepsy Society): Vishakapatnam |
| 73 | Guest Lecture: Endoscopic Epilepsy Surgery | December 2015 | Annual Congress of Neurological Society of India, Hyderabad |
| 74 | Guest lecture: Complication avoidance in craniovertebral junction surgery | December, 2015 | Annual Congress of Spinal Surgeons of India, Goa |
| 75 | Guest lecture: The technique of DCER to reduce basilar invagination and atlanto axial dislocation through a posterior only approach | 16-18th November, 2015 | Annual Skull Base Congress, Bangalore |
| 76 | Guest lecture: Applying the law of levers to reduce basilar invagination and atlanto axial dislocation. | 05/2015 | ANEICON, ORISSA; |
| 77 | Guest lectureApplying the law of levers to reduce basilar invagination and atlanto-axial dislocation: Description of a new technique. | 04/2015 | Asian Australasian Congress of Neurological Surgeons, Juju Island, Korea; |
| 78 | Organized the "Advanced Epilepsy Surgery, Epilepsy Neurobiology and functional workshop". Advanced Epilepsy Surgery, Epilepsy Neurobiology and functional workshop, | 04/2015 | AIIMS, New Delhi, |
| 79 | Organised the advanced Epilepsy Surgery, functional and pain workshop-9-11th April, 2015. Organised the advanced Epilepsy Surgery, functional and pain workshop- | 9-11th April, 2015; 04/2015 | AIIMS, New Delhi, |
| 80 | Disconnective epilepsy surgery: paper presented as invited faculty at the EPILEPSY CONCLAVE. | 04/2015 | Hyderabad; |
| 81 | Pondicherry neurosciences club, presented an oration on “Creating a successful epilepsy surgery program | 4th January, 2015 | Pondicherry |
| 82 | Chief faculty at the JIPMER cranio vertebral junction anomalies cadaveric workshop, presented 2 lectures as a faculty | 2-4th January, 2015 | Pondicherry |
| 83 | Giant MCA aneurysm-How I do it?, Applying the law of levers for reduction of basilar invagitation and AAD, Faculty and EC member of NSI CON 2014 | 10-14TH December, 2014 | Coimbatore |
| 84 | Posterior cervical spine solutions: Partcipated as faculty in this hands on spine workshop | 28-29th, September, 2014 | Bangalore |
| 85 | Indo-American Spinal Alliance (IASA) hands on spine workshop for cervical spine: Partcipated as a faculty presented the lecture: Surgical concepts of C1-C2 fixation | 26-27th September, 2014 | Bangalore |
| 86 | Annual congress of neurospinal surgeons society congress. Ahmedabad, presented the papers - Management of intra medullary spinal tumors in AO spine symposium - Evolving paradigms in management of basilar invagination and atlanto-axial dislocation | 21st September, 2014 | Ahmedabad |
| 87 | VHS annual microneurosurgery workshop. Participated as a Chief faculty in this live operative workshop. Received felicitation from His Excellency, Abdul Kalam, former President of India for the same | 18-20th, September, 2014 | Chennei |
| 88 | 9th Asian Epilepsy Surgery Congress. Presented the following paper “Endoscopic hemispherotomy: From concepts to practice”. Participated as faculty | 3rd-7th October, 2014 | Tokyo, Japan |
| 89 | Annual congress for Instructional course in spine. Presented the paper “Osteoarthritis of CV Junction” | August, 2014 | Udaipur |
| 90 | 10th AOEC, Singapore: Presented the following paper in ASEPA teaching course “Multimodal imaging and epileptogenic networks” and participated as a faculty | 7-9th August, 2014 | Singapore |
| 91 | Epilepsy Conclave 2014 | 12-13th Jul, 2014 | Goa, India |
| 92 | Post Pediatric Epilepsy Meeting | 4-5th Jul, 2014 | Gothenburg, Sweden |
| 93 | European Congress on Epileplogy (ECE) | 29th Jun to 3rd Jul, 2014 | Stockholm, Europe |
| 94 | Complex Spine Trauma, JPNA Trauma Centre. Faculty, gave didactic lectures and demonstrated live surgeries | 11th & 12th May 2014 | AIIMS, New Delhi |
| 95 | NSI Conference Curriculum Course: Conducted this course with senior members of NSI at AIIMS and created an uniform guidelines for neurosurgical curriculum | 15th March 2014 | AIIMS, New Delhi |
| 96 | NSI Teaching Program | Feb, 2014 | Kolkatta |
| 97 | AIIMS Microneurosurgery Workshop | 21st to 23rd Feb 2014 | JPNA Trauma Centre, New Delhi. |
| 98 | Rammiah, Banglore: Faculty for cervical spine hands on cadaveric course at MSR advanced facility for cadaveric training | Feb 2014 | Banglore |
| 99 | -Invited faculty: Presented the following talk: “Epileptogenic networks and the Epilepsy Surgeon” | 24-27th October | 7th Asian Epilepsy Surgery Congress, Beijing |
| 100 | Techniques of Epilepsy surgery- Invited lecture Chief faculty for 3D cadaveric workshop for epilepsy Invited faculty for “1st National Functional congress and cadaveric workshop” | September, 2013 | 1st National Stereotactic and Functional cadaveric workshop, Surabaya, Indonesia |
| 101 | “Distraction, compression extension and reduction” Deription of a new novel technique for reduction of BI and AAD “Developing customized treatment paradigms for pharmacoresistant epilepsy in developing countries” Presented the above papers as a invited faculty at WFNS, Seoul, Kore | September, 2013 | WFNS, Seoul, Korea, |
| 102 | “Long term outcome in persons with drug refractory epilepsy after resection in unilateral mesial temporal sclerosis” Poster presented. | June 23-27th, 2013 | Montreal International Epilepsy Congress, Canada |
| 103 | Presidential Symposium “Epilepsy Focus: Is It a Zone or a Network? | June 13-15th, 2013 | Korean Epilespy Congress, Korea |
| 104 | Presented Paper “Distraction, compression, extension and reduction for basilar invagination and atlanto-axial dislocation- a new novel technique” | April 4-6th, 2013 | Global Spine Congress, Hong Kong |
| 105 | Chairman of the operative workshop conducted at the Calicut govt college on cranio-vertebral junctions-“The juncture” delivered a lecture on newer techniques on management of craniovertebral junction anomalies. | Feb 28th, 2013 | Calicut govt medical college |
| 106 | Recent advances in molecular mechanisms of neurological disorders, Faculty and invited speaker: “Epileptogenic networks and epileptogenic focus: Role of multimodal imaging”. | Feb 22nd, 2013 | AIIMS, New Delhi |
| 107 | 1st Indo-German meeting for NEUROBIONICS: Faculty, presented guest lecture on “Role of electrical stimulation for bladder and bowel disorders”. Moderated the session on “Role of VNS and other electrical stimulation modalities for epilepsy” | Feb 16th, 2013 | JIPMER, Pondicherry |
| 108 | Joint Neurosurgical Convention, 6th International Mt Bandai symposium for Neurosciences, The 7th Pan Pacific Neurosurgery congress Was an invited guest faculty and presented at the main penary session “Distraction, Compression, Extension and reduction of Basilar invagination and atlanto axial dislocation: Description of a new nove technique“. | Jan 29th-Feb 4th, 2013 | Hawai, USA |
| 109 | Advanced workshop on epilepsy surgery Faculty, gave a lecture on “Pediatric Temporal Epilepsy surgery” and participated as a faculty | 5-6th, January, 2012 | Kochi, Kerela |
| 110 | 61st Annual National Congress of Neurological Society of India, Delhi NCR Organizing secretary Conducted the CV Junction symposium and gave a lecture on intra operative manupilations to reduce basilar invagination and AAD Gave a lecture on posterior circulation aneurysms Moderated the “meet the expert” symposium and presented a case on “Status epilepticus in a neonate” | 17th-22nd December, 2012 | Delhi, NCR |
| 111 | 6th Asian Epilepsy Surgery Congress, Busan Korea. Participated as a faculty, and Board member of AESC. Presented the paper “Pediatric epilepsy surgery from India- Investigations, Outcome and QOL” | 8-10th, November, 2012 | Busan, Korea |
| 112 | ISPN Annual congress: held at AIIMS; Vice Chairman for scientific committee; gave two lectures: 1) Role of spacers and jammers in CVJ anomalies 2)Hemispherotomy for epilepsy surgery | 31-2nd Nov, 2012 | AIIMS |
| 113 | First instructional course on CV Junctions anomalies: GB Pant Medical college, New Delhi, 12-13th, October, 2012. Participated as a faculty and spoke on “Spacer distraction and extension to reduce AAD and BI” | 12-13th October, 2012 | GB Pant Medical college, New Delhi |
| 114 | International Spine and Spinal injuries conferences (ISICON), 12-14TH October, 2012. Participated as faculty; Panelist on workshops on “Metastatic spinal tumors” and “Cervical myelopathy” | 12-14th October, 2012 | Indian Spinal injuries center, New Delhi |
| 115 | Fundamentals of spine surgery: Hands on spine workshop on basics of spine surgery. Conducted this workshop and gave lectures on management of CVjunction, spondylolisthesis, and anterior cervical approach. Also provided hands on workshop training for spine instrumentation. Course conducted by Academia for spine education, Medtronic. | 29-30th Sept, 2012 | New Delhi, Hotel Claridges |
| 116 | ICVS: Annual congress of cerebraovascular society Participated as faculty, Chaired and participated as a panelist in the CME on 21st and presented a paper on 23rd on “mini-orbito-fronatal craniotomy for anterior cirucaltion aneurysms” | September, 21-23rd, September, 2012 | Mumbai |
| 117 | Spine 2012, Annual congress of Neurospinal surgeons society of India (NSSA) Was faculty and National coordinator for this congress Chaired and participated as a panelist on the session for bio-informatics for spine surgery, spoke on the following topics (1) Distractive compressive extensive reduction for basilar invagination and atlanto axial dislocation- a new novel technique (2) Cervical vertebral tumors | September, 13-15th, 2012 | Chennei |
| 118 | ICS-2012, Official congress of the ASSICON Was National Faculty- presented 2 papers 1) Video on cervical spacer jamming 2) Panel discussion of a difficult case of cervical tumor | August 13-16th, 2012 | Srinagar |
| 119 | Total cervical spine solution: Conducted this workshop on cervical spine with hands on models and gave 3 lecture: cervical arthroplasty, cervical trauma, cervical spine stabilization | July, 14-15th, 2012 | New Delhi |
| 120 | Chief faculty, Video spine symposium, Ahmedabad orthopedic association, Ahemedabad Delivered 2 video lectures: Cervical arthroplasty, and TLIF for lumbar spine fusion | July, 9th, 2012 | Ahmedabad |
| 121 | Guest faculty: Cleveland Clinic Kokilaben Epilepsy symposium, | May 2012 | Mumbai. |
| 122 | Guest faculty: Presented a lecture on "Management of cervical spine tumors", | March 2012 | ASSICON, New Delhi. |
| 123 | Guest faculty:, presented a lecture "Epilepsy surgery" in the Epilepsy surgery symposium | March 2012 | NSSI conference, Pune. |
| 124 | Guest lecture: research paradigms for epilepsy surgery. | April; 2012 | Bombay Neurological Association |
| 125 | Presented the following papers in the NSI annual congress held in Bangalore: (1) Key hole approach to aneurysms (2) Basilar top aneurysms: how I do it video session (3)Best paper for CeibaGiegi Epilepsy award paper | 2011; December | NSI annual congress held in Bangalore |
| 126 | Pediatric epilepsy surgery with QOL: Experience with 130 cases; | 2011; October | ISPN, Goa |
| 127 | In hospital management of epilepsy: Lecture for nursing symposium | 2011; October | ISPN, Goa |
| 128 | Participated and presented cases as a faculty in the Epilepsy surgery symposium | 2011; October | ISPN, Gos |
| 129 | Challenges in pediatric epilepsy surgery | 2011 | ILAE |
| 130 | Faculty, Consensus for providing guidelines for pediatric epilepsy surgery | 2011 | ILAE, Rome 2011 |
| 131 | Challenges in pediatric epilepsy surgery, experience with 150 cases. | 2011 | ILAE congress, Rome, 2012 |
| 132 | Faculty and Secretary General, Asian Epilepsy Surgery Society. | 2010 September | Annual International congress, Taipei |
| 133 | Guest faculty, King Fahad Hospital, Saudi Arabia; International Medical Symposium sponsored by the Ministry of Health and His Royal Highness King Mohammad Bin Saud: Gave 2 lectures: “Keyhole Cranio orbital approach to aneurysms” & “Surgery for Intractable Epilepsy”. | 2010 | King Fahad Hospital, Saudi Arabia; International Medical Symposium |
| 134 | ISSICON; International Spine and Spine Injuries: Invited Faculty; delivered guest lecture; Management of Vertebral body haemangiomas. | 2009 | ISSICON |
| 135 | Presented paper on “Intraoperative absolute alcohol embolization for vertebral body haemangiomas. | 2009 September | WFNS, Boston |
| 136 | Faculty, National, AO Spine, AO Spine Principles Course. | Jul-09 | New Delhi |
| 137 | Faculty and speaker at the San SevoloAlumini meeting (ILAE). | 2009 | PECS, Budapest (ILAE world congress 2009) |
| 138 | Keynote speaker at the 3rd Asian Epilepsy Surgery Congress (AESC). | Jun-09 | Osaka, Japan. |
| 139 | Attended and participated as a faculty and board of Director at the world congress of International brain mapping society. | November, 2008 | www.IBMISPS.org, held in UCLA. |
| 140 | “Trend of epilepsy surgery in India” Guest lecture presented at the World congress AESC, Beijing China, | 2008 | World congress AESC, Beijing China. |
| 141 | “Epilepsy surgery in India” Guest lecture delivered at the Japanese Epilepsy society. | 2008 | Tokyo, Japan. |
| 142 | Attending International faculty and presented paper: Epilepsy surgery for post infectious pathologies; experience from AIIMS. | 2007 | Asiano-Oceanic congress, Xiamen, China, 2007 |
| 143 | North America skull base meeting: Phoenix, Arizona, USA, attended the meeting. | 2006 | Phoenix, Arizona, USA |
| 144 | Advanced Neuroendoscopy workshop at UCLA: under Prof Frazee. | Feb 2006. | UCLA. |
| 145 | “Role of MRI-SPECT coregistration and diffusion weighted images in localizing the epileptogienic tuber in tuberous sclerosis” Poster presented at the American Epilepsy association (AES). | December 2005. | Washington DC |
| 146 | 2004; “Cognitive outcome comparison between right and left temporal surgeries for intractable epilepsy” Poster presented at “15th Cleveland-Bethel advanced symposium on epilepsy management with workshop in techniques in epilepsy surgery”. | July 15-18th, 2004 | Cleveland Clinic, US. |
| 147 | 2003; “Neuropsychological assessment of patients undergoing epilepsy surgery using a customised Hindi battery” Poster presented at International epilepsy congress held at Lisbon in October 2003 Chandra PS, Sanyal S, Gupta S, Singh VP, Bhatia M, Gaikwad S, Tripathi M, Mehta VS. Neuropsychological assessment and outcome following surgery for intractable epilepsy using specially developed battery for Indian patients. Epilepsia, 25 th IEC proceedings. Epilepsia, vol 44, supp 8, 103, 2003. | Oct-03 | Lisbon |
| 148 | 2002; Attended the Annual STICH investigators meeting as one of the STICH investigators. | June 29th, 2002 | Newcastleupontyne, U.K. |
| 149 | “Traumatic CV junction anomalies: Experience of 125 cases over 10 years”. | 26th to 29th, June, 2002. | EMN congress held at Newcastle. |
| 150 | “Management of CV junction anomalies with special reference to posterior circulation strokes: Experience of 456 cases over 10 years”: CME guest lecture given. | 14th Feb, 2002. | National Neuroscience Institute, Singapore. |
| 151 | 2002; “Management of bony CV junction anomalies: Experience of 456 cases over 10 years” Paper presented. | 16th-19th Feb, 2002 | 13th Annual Meeting of North American Skull Base Society |
| 152 | “Management of bony CV junction anomalies: Experience of 456 cases over 10 years from a tertiary centre in a developing country”: Guest lecture delivered. | 7th March, 2002. | Neurosurgical grand rounds at UCSF, San Francisco. |
| 153 | "Endoscopic management of colloid cyst of third ventricle- series of 23 cases" paper presented. | November, 2002. | Asian Congress of Neurological Surgeons, Hong Kong, |
| 154 | “Role of mild hypothermia in aneurysmal surgery” Paper presented. at the International update of Clinical Neuropharmacology. | 2001 | Maldives. |
| 155 | “Craniovertebral Junction Anomalies with posterior circulation territory infarcts:A short series” :RamDas GV, Chandra PS, Kale SS- Paper presented. | 2001 | 12th World Congress of Neurosurgery, Sydney. |
| 156 | “A decade of Trans-oral surgery- Analysis of 385 patients of CV Junction anomalies: Kale SS, Chhabra RS, Chandra PS, Patir R. Paper read at | 2001 | 12th World Congress of Neurosurgery, Sydney. |
| 157 | “Cerebral meningiomatosis presenting with intractable seizures” Poster presented. | November 11-13th, 2000. | 3rd Congress of Asian Epilepsy Organisation (AOEO), New Delhi, |
| 158 | “Foramen magnum tumours: AIIMS experience”- Paper presented at the 5th Asian-oceanian International congress on skull base surgery. | Nov 12-15th 1999 | Mumbai. |
| 159 | Faculty and guest lecture: Symposium on Paediatric epilepsy surgery organized in Hyderabad by the local epilepsy society. Gave talks on [1] Invasive monitoring for epilepsy [2] Hypothalamic hamartoma | 2011; November 5-6th | Hyderabad. |
| 160 | NEUROVASCON, 2011: [1] Key hole approach to aeurysems [2] Basilar top aneurysm | 2011; October. | |
| 161 | Faculty and Guest lecture: Circumferential fusion for dorsal instability | 2011; September. | Neurospinal Surgeons association annual congress, Bangalore |
| 162 | Guest Invited lecture: Keyhole approach to aneurysms: presented. | 2010; September | NEUROVASCON 2010, Bhubneswar |
| 163 | Guest lecture at the Indian Institute of Science: Developing lab models to create better surgical paradigms for epilepsy surgery | 2010; July. | |
| 164 | Symposium on Epilepsy; Patna. Organized by Bihar Chapter of Indian Epilepsy Society; Guest faculty, gave lecture on “ Surgery for Intractable Epilepsy”. | 2010 | Bihar, India |
| 165 | Faculty UPNEUROCON; lecture on “Hemispherotomy for intractable epilepsy” | 2010; April | Fortis Noida. |
| 166 | Attended as an expert in the committee to develop “Guidelines to develop Epilepsy Education In India”; by the Indian Epilepsy Association” | 2010; April | - |
| 167 | Attended as an expert in the committee to develop MEG in India. | 2010; March | Atomic Research Commission, Kalpakam, Tamil Nadu |
| 168 | Faculty; Neurotropicon; JIPMER, Pondicherry; Gave a lecture: “Craniovertebral junction anomalies in India” | 2010; March | India |
| 169 | Faculty and Co Chairman for Symposium on Minimally invasive spine surgery and total disc replacement. | 2010; January 18th | New Delhi |
| 170 | Chairman of the course, SKELETAL, AO spine, on advanced managed for spinal trauma with hands of workshop. | 21-22nd November, 2009 | Gurgaon, New Delhi |
| 171 | Guest lecture, Trauma 2009: 360 degrees fusion for dorsal column instability. | 12-15th November, 2009 | JPN Apex trauma center, AIIMS. |
| 172 | Guest lecture as faculty: ILAE/ASEPA International workshop on Epilepsy surgery, Hemispherotomy for epilepsy surgery. | 7-8th November, 2009: | - |
| 173 | Guest lecture as faculty: ILAE/ASEPA International workshop on Epilepsy surgery, AIIMS: Future directions for epilepsy surgery in India. | 7-8th November, 2009 | AIIMS |
| 174 | Guest lecture as faculty: ILAE/ASEPA International workshop on Epilepsy surgery,: Conducted the round table discussion with IES on development of guidelines for epilepsy surgery in India. | 7-8th November, 2009 | AIIMS |
| 175 | 2009; Guest lecturer; AO Spine Principles Course, New Delhi, [1] Approach to Anterior cervical Spine [2] Outcome of Surgery for degenerative lumbar spine disease [3] Spinal Implant complications [4] Intraspinal tumors | Jul-09 | New Delhi. |
| 176 | “Pediatric Epilepsy Surgery”. CME guest lecture given on the occasion of “Pediatric neurosurgery CME”. | 30thMay, 2009. | CMC Ludhiana. |
| 177 | 2009; “Epilepsy Surgery”. CME guest lecture given on the “Epilepsy Update”. | 10th May 2009. | IES, Patna. |
| 178 | “Role of Electrocorticography in epilepsy surgery” CME guest lecture given. | 2008 | Annual conference of Neurological society of India, Pune. |
| 179 | Facutly, Instructional Course in Spine, August 7, Shila, delivered 4 lectures on CV junction, circumferential fusion. | 2008, August 7 | - |
| 180 | Faculty and speaker and panel participant; Indo-US, DBT-NIH workshop. | 2008 | Dept of Biotechnology; Ministry of Science and Technology, India, Hyderabad. |
| 181 | Faculty and panel discussant, Trauma 2008; International Conference cum Live Workshop, Indian Society of Trauma. | November 2008. | JPN Apex Trauma Center, AIIMS, New Delhi. |
| 182 | GEMIND: Guidelines for epilepsy management laid down by Indian Epilepsy Society; Committee meetings; attended as expert core committed for laying down National guidelines, | Aug-08 | - |
| 183 | Chairman, Workshop on Minimally invasive Spine Surgery. | March 2008. | Manipal Hospital, Bangalore. |
| 184 | “Neurosurgical perspectives of traumatic brain injury” Guest lecture given at the annual Indraprasthaphysiotherapatist’s conference. | 2008 | Indraprasthaphysiotherapatist’s conference |
| 185 | “Role of neurosurgeon in ICU infection” guest lecture given at the 2007 annual armed forces [R & R hospital] neurosciences update. | 2007 | R&R hospital |
| 186 | 2006; Post operative ICU infections: Invited Talk given in May 2006 at the R&R hospital annual conference | May-06 | R&R hospital |
| 187 | 2006; Invited guest lecture: “Epilepsy surgery in adults” at Current Trends in Epilepsy: an international symposium. | Nov 3-5th, 2006. | AIIMS. |
| 188 | “Endoscopic excision of colloid cysts” guest lecture given at Brain and spine endoscopic workshop held at Jaipur on 21-22nd February, 2004 and participated as a National faculty [workshop conducted by Prof M Gaab, Neurosurgery clinic, Hanover, Germany] | 2004 | Jaipur. |
| 189 | “CV junction anomalies: lessons learnt from 632 cases: guest lecture given at the National skull base conference. | December 2004. | Mumbai. |
| 190 | Attended and participated in the live AO SPINE SYMPOSIUM. | 4-6TH July, 2003. | Cochin |
| 191 | “Surgery for pediatric intractable epilepsy” Invited guest lecture given at PEDINEUROCON 2003 [National convention on Pediatric Neurology: Indian academy of Pediatrics] | November 22nd, 2003 | PEDINEUROCON 2003 |
| 192 | “Neuroendoscopy” Invited guest lecture given at the CME section of the Neurological Society of India, PGI Chandigarh in “How I do it?” | 12thDecemebr, 2003. | Neurological Society of India, PGI Chandigarh. |
| 193 | “Neuroendoscopy” guest lecture given on the CME: How I do It? Of the Neurological Society of India annual conference held in PGI, Chadigarh, | Decemebr 2003. | PGI, Chadigarh. |
| 194 | “Epilepsy surgery for pediatric patients: AIIMS experience” guest lecture given at Pedineurocon 2203. | 22ndNovemeber 2003. | Jaipur. |
| 195 | “Trans oral surgery for CV junction anomalies & Odontoid screw fixation for type II dens fracture: How I do it?” Video sessions of personally operated cases shown as an invited guest speaker at SPINE 2002. | 18th-21st July, 2002. | Kanyakumari. |
| 196 | “CV junction anomalies: Experience of single stage surgery from 516 cases”. Talk given as an invited guest speaker at SPINE 2002. | 18th-21st July 2002. | Kanyakumari. |
| 197 | 2002; "Management of head injuries" Invited lecture given for CME on 'Management of a trauma patient'. | December 22, 2002. | Association of surgeons of India- ASICON CME education foundation, New Delhi. |
| 198 | “Head injuries- Recent trends in Management”- Talk given on the inaugural function of the 2nd Nursing update held in the Nursing College All India Institute of Medical sciences. | 2001 | AIIMS. |
| 199 | 2001; Participitated as a panellist on one-day symposium on “Modern day concepts in disinfection &sterilisation practices”. | 17th February 2001. | AIIMS. |
| 200 | 2001; Gave a talk on “Aseptic practices in clinical practice” as an invited speaker on the occasion of National conference on infection control in India hospitals, was the chairperson of one of the groups in the workshop for setting the “National policy for guidelines on aseptic practices, disinfection and sterilization procedures”. | OCT 17-19, 2001. | AIIMS. |
| 201 | Endoscopic management of colloid cysts: Series of 18 cases:Ramdas GV, Suri A, Chandra PS; Paper read at NEUROCON 2001. | 2001 | Neurological Society of India, Mumbai. |
| 202 | ; “Posterior circulation strokes associated with cranio-vertebral junction anomalies: Series of 9 cases”: Paper presented at NEUROCON 2001. | 2001 | Neurological Society of India, Mumbai. |
| 203 | ; “Endoscopic management of the cystic lesions of brain” Talk given as one of the guest speakers at the Minimal access neurological surgery workshop,chaired by Prof Pernezky 2001. | Feb 23-24th, 2001. | Sir Ganga Ram hospital. |
| 204 | “Endoscopic evacuation of spontaneous intracerebral hematomas”: Guest lecture presented on the occasion of 3rd Annual meeting of Delhi Neurological Association, 2001. | 2001 | Annual meeting of Delhi Neurological Association, 2001. |
| 205 | 2001; “Craniovertebral junction anomalies: A retrospective study of 385 cases- lessons learnt”- Paper presented at the National conference of Spine. | July 2001. | Kodaikanal. |
| 206 | “Craniovertebral junction anomalies : Lessons learnt in 10 years”: Paper read at 3rd National skull base conference, Madras, 2001. | 2001 | National skull base conference, Madras. |
| 207 | “Trigeminal neurinomas: A series of 25 cases” paper presented at SGPGI, skull base conference. | 2000 | Post graduate Institute, Lucknow. |
| 208 | “Trigeminal neurinomas: A series of 25 cases” paper presented at SGPGI, skull base conference. | 2000 | Post graduate Institute, Lucknow. |
| 209 | Attended and actively participated the Midas Rex hands on workshop. | Mar-99 | AIIMS. |
| 210 | “Post traumatic epilepsy” Talk given on the occasion of the inaugural function of Delhi Neurological Association held at Sir Ganga Ram Hospital in April’ 99 and participated as one of the members in the panel discussion. | Apr-99 | Sir Ganga Ram Hospital |
| 211 | 1999; “Hands on workshop on Neuroendoscopy” Participated this workshop.(conducted by A Pernezky, T Kanno, Y,. Kato, AK Banerjii). | Nov 10-12th, 1999. | VIMHANS |
| 212 | 1999; “Hands on workshop on neuroendoscopy and Neuronavigation” Participated this workshop (conducted by M. Gaab, A Grotenhuis, Hechl P) | Sept 9th, 1999. | CMC Vellore |
| 213 | “Paediatric nosocomial infections in neurosurgery” Paper presented at the International Paediatric CME held at Calcutta, | Dec 1998. | International Paediatric CME held at Calcutta, |
| 214 | “Cavernous sinus neurofibromas arising from ocular cranial nerves” Paper presented at the First National skull base conference. | Nov, 1998. | New Delhi. |
| 215 | “Hands on workshop on spinal surgery” Participated this workshop. | June 21-22nd, 1997. | MS Ramaiah Medical college. |
| 216 | “Neuroendoscopic management of unilateral hydrocephalus” Poster presented at NSI Calcutta-96. | 1996 | NSI Calcutta-96. |
| 217 | 1994;“CME on Pediatric Neurosurgery” attended this CME held at Mumbai (conducted by Marion L Walker and SN Bhagawati). | March 12-16th, 1994. | Mumbai. |
| 218 | “Morbidity and Mortality in surgery for pituitary adenomas” Paper presented at Neurological society of India, Madras 1993. | 1993 | Madras. |
30 publications still pending to be udated
All the information mentioned above is correct to the best of my information
P Sarat Chandra
Lab Services- anaesthesia care in cardiac cath Lab, ECHO Lab, MRI and CT scan room
Inpatient- anaesthesia care in operation theatre (OT), intensive care unit (ICU), coronary care unit (CCU)

Name: Dr. Harshal Ramesh Salve, MBBS, MD, MIPHA, MIAPSM
Designation: Additional Professor, Centre for Community Medicine, AIIMS, New Delhi
Email: harshalsalve@ymail.com, harshalsalve@aiims.edu
Office - #40, Centre for Community Medicine, Old OT Block , AIIMS, New Delhi
Phone - – 11-26593366
Experience: 13 Years of experience of Physician, Teacher and Community based Researcher at AIIMS New Delhi. Dr. Salve worked with Ministry of Health, GoI at national level, State Governments and International agencies such as World Health Organization on expert committees, research projects and technical reports. His major area of work are Non-Communicable Diseases, Climate Change, Air Pollution, Mental Health and Health System Research. Dr. Salve is member of WHO collaborating centre and MINErVA at AIIMS. Dr. Salve was part of inter-ministerial Central team for assessing response for COVID 19 pandemic in the State of Maharashtra and Rajasthan. Dr Salve contributed in generating awareness regarding Covid 19 among general public on print and TV media. Currently Dr Salve working at Comprehensive Rural Health Services Project (CRHSP), Ballabgarh
Awards/ Fellowship/ Significant Contribution: Dr. Salve has an experience of working in 15 funded community based research projects. Dr Salve is Co-Ordinator for Co-ordinator - Collaborative on Air Pollution and Health Effects Research in India (CAPHER-India) funded by Health Effect Institute, Boston
Publications/ Books: He has 50 publications on his credit in national and international peer reviewed journals. Dr. Salve written Chapter on “Mental Health” in IAPSM textbook of Community Medicine
1.Financial support received (Research projects)
| Title | Source of Funding | Year | Total Amount (INR) |
|---|---|---|---|
| Chief Investigator (11) | |||
| CAPHER-Collaborative on Air Pollution and Health Effects Research, India (Pending for HMSE clearance, got ethical clearance) | Health Effects Institute, Boston USA | 2021-22 | 48,81,800 |
| Preparing NCD Health Emergency Framework and documenting best practices adopted by States/UT for continuing NCD services during COVID 19 Pandemic | WHO – India office | 2021 | 27,72,000 |
| Community practices in COVID-19 outbreak in rural Ballabgarh, Haryana: A mixed method study | AIIMS Intramural Project | 2020 - 2021 | 2,75,000/- |
| Delhi Cluster – Delhi Research Implementation and Innovation (DRIIV):Tackling air pollution in Delhi NCR | Office of Scientific Advisor, GoI | 2020 - 22 | 8,00,000/- |
| Priorities for Advancing Research on Health Effects of Air Pollution in India | Health Effects Institute, Boston USA | 2019 | 19,93,670/- |
| Pilot study on implementation of screening and management protocol for COPD/Asthma under NPCDS in rural North India | NCDC | 2019 (Six Months) | 40,750 |
| Development of tool for intervention at School level using WHO advocated Health promoting School for addressing NCD Risk factors | WHO - SEARO | 2019 (Six Months) | 6,28,650 |
| Mortality burden of ambient PM2.5 exposure in Rural Ballabgarh, Haryana, North India. | AIIMS – IIT Joint Collaborative Project Grant | 2018 - 2020 | 8,90,584 |
| Developing Community level Climate based Early Warning System (CCEWS) for Vector Borne Diseases in National Capital Region, India | DST, Climate Change Program (SPLICE Division) | 2017-2020 | 55,62,628 |
| Association of Common Mental Disorders with Diabetes –A Community Based Case-Control Study | AIIMS Intramural Grant | 2016-18 | 9,89,000 |
| Organizing Diabetes Screening Station on World Health Day -2016 | WHO-SEARO | 2016 | 1,03,418 |
| Co-Investigator (12) | |||
| Innovation Learning Centre for supporting implementation of Comprehensive Primary Health Care in a selected district of Haryana | National Health Systems Resource Centre (NHSRC), Ministry of Health and Family Welfare | 2018-2021 | 41,45,000 |
| Emerging drug resistance in community-acquired urinary tract infection and molecular insights into dynamics of resistance traits in Indian isolates- A multi-centriccross-sectionalstudy | ICMR | 2019-22 | 65,00,000 |
| ICMR Task Force Centre on Rational use of drugs | ICMR | 2019-22 | 30,25,679 |
IMPLEMENTATION PLAN Title Feasibility tesng and esmaon of cardiovascular disease risk status in a rural populaon in Ballabgarh, Haryana using updated WHO CVD risk charts. IMPLEMENTATION PLAN Title Feasibility tesng and esmaon of cardiovascular disease risk status in a rural populaon in Ballabgarh, Haryana using updated WHO CVD risk charts. Feasibility testing and estimation of cardiovascular disease risk status in a rural population in Ballabgarh, Haryana using updated WHO CVD risk charts. | WHO HQ (Geneva) | 2020 | 8,03,190 |
| Strengthening implementation of National Program for Prevention and Control of Cancer, Diabetes, Cardiovascular diseases and Stroke (NPCDCS) in states: Capacity Building of Program Managers/ Coordinators by Developing Training Manual | WHO-Country Office for India | 2016 | 19,19,000 |
| Piloting of the National Survey for Monitoring National Non-communicable Diseases Targets and Preparation of Operational Manual: Phase-1 (This is for Operational Manual and Training of field staff pioloting) | WHO-Country Office for India | 2016-17 | 13,56,000 |
| Piloting of the National Survey for Monitoring the NCDs Targets 2016 and Validation of urinary sodium levels in India | WHO-Country Office for India | 2016-17 | 15,60, 206 |
| Indexing health for monitoring progress towards Sustainable Developmental Goals (SDGs) – Collaborative Project with Government of Andhra Pradesh | Government of Andhra Pradesh | 2016-17 | 15,00,000 |
| Survey for Monitoring the National Non Communicable (NCD) Targets (I-966) | ICMR | 2017-18 | 1,30,00,000 |
| Establishing a Technical Support Unit (TSU) for Verbal Autopsy based Cause of Death Ascertainment in the Sample Registration System, Vital Statistics Division, Office of Registrar General of India | Office of Registrar General of India, Government of India | 2017-25 | 2,89,06,205 (Per annum) |
| Development of training course for NCD programme managers and directors for enhancing managerial and leadership skills for NCD multi-sectoral governance andcoordination | WHO – India Office | 2018 | 7,00,000 |
| Review of National Programme for Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) | WHO – India Office | 2019 | 13,50,500 |
Dr. Salve presented research papers and gave talks in various international and national conferences.
Q.1: What is coronary artery disease (CAD)?
A: Coronary artery disease is the most common type of heart disease. It happens when the arteries that supply blood to heart muscle(coronary arteries) become hardened and narrowed. This is due to build up of cholesterol and other material called plaque, on their inner walls. This build up is called atherosclerosis. This can lead to chest pain (angina) or a heart attack. Most heart attacks happen when a blood clot suddenly cuts off the hearts blood supply, causing permanent heart damage. Over time, CAD can also weaken the heart muscle and contribute to heart failure and arrhythmias.
Q.2: What are the diagnostic modalities for CAD?
A: Various diagnostic modalities are increasingly used in the diagnosis of CAD which includes ECG, Echocardiography, coronary CT angiography, and cardiac single photon emission computed tomography (SPECT), and coronary angiography.
Q.3: What are the treatment modalities for CAD?
A: (i) Medical Management (ii)Percutaneous Coronary Intervention- Angioplasty/Stenting (iii)CABG(By pass surgery)Depending on the extent and severity of involvement of coronary arteries and left ventricular (LV) function, clinician advises medical management or angioplasty or CABG.
Q.4: What are different types of percutaneous coronary intervention?
A: (i) Balloning(POBA) (ii) Bare metal stent(BMS)implantation (iii) Drug eluting stent(DES)implantationNowdays, almost all angioplasties are being performed using DES impantation.
Q.5: What is a coronary angiogram?
A:&For definitive diagnosis of CAD to find out extent and severity of CAD and for its proper treatment,imaging of coronary arteries is done in cardiac cath lab.This is called as coronary angiography.
Q.6: What is angioplasty?
A: Angioplasty is a procedure that uses a balloon to open up blocked areas of your coronary arteries. It is performed to relieve some of the symptoms associated with CAD. It is also performed during a heart attack to prevent damage to the heart(Primary Angioplasty/stenting).
Q.7: What is the stent used for?
A: Stents are used for relieving obstruction in coronary arteries. The stent is a small metal-mesh tube that is implanted in the area of your coronary artery to help keep it open. Drug eluting stents in addition are designed to deliver medication to the artery. After the stenting procedure, the balloon is removed from your artery, but the stent will remain in your coronary artery.
Q.8: What are the different components of stents?
A:Drug eluting stent is made up of i) Stent platform (Stainless steel, Cobalt chromium, Platinum chromium, etc.) and Balloon expandable delivery system ii) Pharmacological agent (Everolimus, Sirolimus, etc.) iii) Drug Carrier (eg. Polymer- Nonbiodegradable/Biodegradable)These stents are available in various diameters and lengths . Stents from different manufacturers are available at our hospital. At the time of angioplasty, treating doctor discusses and informs the patient regarding the suitability of the stent according to his/her disease. The information about various kinds of stents along with their costs is available at our website.
Q.9: What is Primary angioplasty/stenting and its cost?
A: Primary angioplasty/stenting is an emergency procedure done during the time of ongoing heart attack.At our hospital,it is being done free of cost.
Q.10: How do I prepare for stenting?
A:Your doctor will give you a complete medical exam and provide you with detailed instructions. When you arrive at the hospital, you can expect to have a series of routine tests, such as an x-ray, electrocardiogram (EKG),echocardiography or blood tests etc.Q.11: How can I get benefit from Government?A: One can avail benefits under the Pradhan Mantri Jan Arogya Yojana as per the laid guidelines.
Q.12: How long will I have the stent?
A: Stents are designed to remain within your coronary artery permanently to provide lasting support.
Q.13: Will I feel the stent?
A: No. You will not feel the stent inside of you.
Q.14: Can the stent move?
A: Once the stent is opened and deployed at the inside wall of your coronary artery, it will remain in place permanently.
Q.15: How do coronary stents work?
A: Coronary stents are small, wire mesh tubes that help widen clogged arteries and restore adequate blood flow to the heart.
Q.16: How soon can I go back to work?
A: The majority of people return to work within a few days following a successful procedure.
Q.17: When can I resume my regular activities?
A: Your doctor will advise you on when it’s safe to resume your regular activities. Many patients can follow their normal routine with in a week after their successful angioplasty.
Q.18: Can I exercise and play sports with a stent?
A: Your doctor will tell you what physical activities are right for you and when you can safely resume them.
Q.19: Will my stent set off metal detectors?
A: No, your coronary stent will not trigger metal detector alarms and you can walk through them safely.
Q.20: How long should I take my medications after angioplasty/stenting?
A: The most important thing that you can do to minimize the risk of stent thrombosis(clot in coronary artery at the site of stent implantation) is to take the medications prescribed by your doctor prescribes. Do not stop taking these medicines specially blood thinners(Antiplatelets) until your cardiologist tells you to, even if you are feeling better.If you have a drug-eluting stent, you may need to take your medication for an extended period of time, perhaps a year or longer. Follow your doctor’s instructions exactly.
Q.21: Will I experience the symptoms of coronary artery disease again, such as chest pain?
A: It is possible that you will experience symptoms again, either because of a new blockage in the treated coronary artery or a new blockage in a different place. If you experience these symptoms, notify your doctor immediately.
Q.22: How will I know if my artery re-narrows?
A: Although the stents are intended to reduce restenosis, it is still possible for your artery to re-narrow. If this happens, you may experience symptoms similar to those experienced when you first noticed before your stent procedure. These symptoms may include chest pain or shortness of breath, especially during physical activity. If you experience pain, inform your doctor immediately.
Q.23: How can I help prevent a recurrence of symptoms?
A: While there is no sure way to prevent a recurrence of symptoms, you can reduce the risk through exercise, not smoking and eating a healthy diet. Ask your doctor about lifestyle changes you can make.
Q.24: What if I still have pain?
A: If you experience pain, immediately visit the emergency at our hospital .
Training is important to Junior & Senior Residents from AIIMS, Other Hospitals & Army
Faculty and Students from other Hospitals for Specialized training in Cardiac Anaesthesia.
3 years course with senior resident training programme for 6 open and 3 sponsored candidates is being conducted in department. During their training programme they do research on two topics for their degree. The resident doctors are trained in department of cardiology, Cath Lab, ECHO and postoperative cardiac intensive care.
| Incharge | Dr.Seema Sen | Professor |
| Faculty | Dr.Seema Kashyap | Professor |
This section provides diagnostic services to the Centre which include Post graduate students of ophthalmology are exposed to Ocular pathology, Histopathology and Cytopathology. It performs on an average 80,000 investigations per year. In addition, teaching and training programmes in ocular pathology are also conducted for other medical colleges and hospitals in India.
Research work on orbital, intraocular tumors & eyelid tumors, glaucoma and corneal pathologies is being done. The department organized Ocular Pathology workshop under the Indian Association of Ocular Pathologist on 25th March, 2006.
Diagnostic histopathology of ocular specimens is undertaken. In addition frozen section guided excision of lid tumors and frozen section for various histochemical stains is also done.
a) Blood investigations are done with the help of Auto analyzer.
b)Urine analysis – Routine examination including urine for-
c)Sample collection of RPC ward and OPD patients for all investigations at various Dr. R. P. Centre laboratories.
Diagnostic and research purposes-Aids in differential diagnosis of tumours and as cancer biomarkers
Ocular Pathology Museum was started by Prof. Ratnakar in 1976. Interesting cases of lid, orbital lesion, intra ocular tumor are still being preserved for teaching purposes.
(a) Funded Research: Provide only the titles of the ongoing and completed research projects indicating the name of Investigator(s), Funding agency, total funding and duration (from-to) of the project. Please provide the information under Ongoing and Completed projects.
b) Departmental Research: only the titles of ongoing and completed research project.

Cryostat machine for rapid per operative diagnosis and fat stain
Well differentiated Retinoblastoma (Haematoxylin & Eosin Stain)

PAS Stain (Goblet cells)
Sebaceous gland Carcinoma (Papanicolaou stain)
Metastatic adenocarcinoma (MGG stain)

Autoanalyser
Vimentin For Mesenchymal lesions
p53 tumor suppressor gene in Rb.



| Name | Designation |
|---|---|
| Mr. Deepak Panjnani | Steno |
| Mr. Kailash Kumar | H/A |
| एम.डी. (जैवभौतिकी) | एम.एससी.(जैवभौतिकी) | पीएच.डी.(जैवभौतिकी) | |
|---|---|---|---|
| अवधि | 3 वर्ष | 2 वर्ष | 3-5वर्ष |
| प्रवेश परीक्षा के (महीने) | मई और नवंबर | जुलाई | जनवरी और जुलाई |
| पाठ्यक्रम (सिलेबस) | एमडी (बायोफिजिक्स) सिलेबस | एम.एससी. (बायोफिजिक्स) सिलेबस | - |
जैवभौतिकी विभाग विभिन्न संस्थानों और विश्वविद्यालयों के एम.एससी और एम.टेक विद्यार्थियों को दीर्घकालिक और अल्पकालिक प्रशिक्षण प्रदान करता है।
| S.No | Date | Particulars of Assets | Name &address of supplier | Bill No. & date | Location of the Assets | Remarks |
|---|---|---|---|---|---|---|
| 1 | 04/03/03 | 3M Steri-Vac (1) | 3M (I) Ltd. | 996/CNC/CARD/02-03 | Cath Lab, CNC 01no. | P-317/4 |
| 2 | 15/03/04 | Anaesthesia Machine Excel-210E Astopad Plus Control (1) | Rohanika Electronics | 100-79/CNC/CARD/02-03 | Cath Lab, CNC 01no. | P-331/4 |
| 3 | 31/05/05 | Defibrillator LP-20 (1) | Intstromedix | 100-34/CNC/CARD/04-05 | .CT2 CCU CNC 01No. | P-16/5 |
| 4 | 07/07/05 | Programmable Stimulator BARD (1) | Advanced Micronic Device | 100-31/CNC/CARD/04-05 | Cath Lab. CNC 01No. | P-19/5 |
| 5 | 29/03/05 | Dual Chamber Pacemaker (2) | Saturn Med. System | 1211/CNC/CARD/04-05. | Cath Lab, CNC 02nos. | P-30/5 |
| 6 | 29/03/05 | Single Chamber Pacemaker (10) | Saturn Med. System | 1210/CNC/CARD/04-05 | CT3 CNC 01no Cath Lab, CNC 02nos CT2 CCU CNC 02nos. CT6 CNC 02nos. | P-31/5 |
| 7 | 27/05/06 | Multiweigh (3-in-1) (Zeal) | Globe Medical System | 1472/CNC/CARD/05-06 | Cath Lab. CNC 02nos. (41) | P-34/5 |
| 8 | 30/08/06 | Transfusion Syringe Pumps (9) | J.Mitra & Bros. | 100-48/CNC/CARD/05-06 | Cath Lab, CNC 03nos CT2 CCU CNC 05nos. CT6 CNC 01nos | P-36/5 |
| 9 | 28/10/06 | Latest Advanced Tech. Ventilator (Servo) (1) | Maquet Medical India (P) Ltd. | 100-51/CNC/CARD/05-06 | CT2 CCU CNC 01no. CT6 CNC 01no | P-39/5 |
| 11 | 17/10/06 | IE33 Echocardiog-raphy System 01No. S.N.02RBWD | Philips Electronics (I) Ltd. | 100-52/CNC/CARD/05-06 | ECHO Lab. CNC 01no. | P-40/5 |
| 12 | 09/10/06 | TMT System (GE Model 2100) | Wipro GE Medical System Ltd. | 100-74/CNC/CARD/05-06 | TMT Lab. CNC 01no. | P-41/5 |
| 13 | 12/04/07 | Transport Monitor (M9000). | Advanced Micronic Devices Ltd. | 1381/CNC/CARD/06-07 | CT6 CNC 01no. 81 condemned | P-43/5 |
| 14 | 29/05/07 | External Defibrillator Med Aid 05Nos. | Advanced Micronic Devices | 1380/CNC/CARD/06-07 | CT3 CNC 01nos. CT6 CNC 01no. 3 condemned | P-46/5 |
| 15 | 05/07/07 | ACT200 Plus TM Automated Coagulation Timer 03Nos. | J.Mitra & Bros. | 1379/CNC/CARD/06-07 | Cath Lab, CNC 01no. CT2 CCU. CNC 01no CT3 CNC 01no. | P-48/5 Through CTVS Department CNC |
| 16 | 09/08/07 | Air Supply Unit for Horus Extend Unit 02Nos. | Electrocare System & Services (P) Ltd. | 1476/CNC/CARD/06-07 | CT2 CCU CNC 02nos. | P-49/5 |
| 17 | 10/08/07 | Ventilator 02Nos. | Electrocare System & Services (P) Ltd. | 100-83/CNC/CARD/06-07 | CT2 CCU CNC 02nos. | P-50/5 |
| 18 | 16/07/07 | Hemodynamic Recorder for Cath Lab I & II 02Nos. | Wipro GE Healthcare | 100-61/CNC/CARD/06-07 | Cath Lab CNC 02nos.(26, 27) | P-51/5 |
| 19 | 26/09/07 | Infusion Pumps 20Nos. | J.Mitra & Bros. | 100-56/CNC/CARD/06-07 | CT3 CNC 05nos Cath Lab CNC 05nos. CT2 CCU CNC 08nos. | P-53/5 |
| 20 | 05/10/07 | RF Generator & Infusion Pump 01No. | Johnson & Johnson Ltd. | 100- 57/CNC/CARD/06-07 | Cath Lab. CNC 01no. | P-56/5 |
| 21 | 19/03/08 | Intra Cardio Echo Catheter 01No. | Siemens Ltd | 100-30/CARD/CNC/06-07 | Echo Lab. CNC 01no. | P-61/5 |
| 22 | 15/04/08 | ECG Machine AT1 (Schiller) 02Nos. | Schiller Healthcare (I) Pvt. Ltd. | 1114/CARD/CNC/07-08 | ECG Lab CT6 CNC 2nos. (6, 7) | P-63/5 |
| 23 | 04/09/2008 | Bi Plane Cardiovascular Catheterisation Lab (Siemens) Lab I 01No. | Siemens Ltd., 127, Henkestrasse, D-91052, Erlangen, Germany/Local-4A Ring Road, I.P. Estate, New Delhi-02 | 100-47/CNC/CARD/07-08 | Cath Lab CNC 01No. HANDED OVER TO CARDIAC-RADIOLOGY | P-65-66/5 |
| 24 | 04/09/2008 | Local Accessories For Cath Lab S.O.100-47/CNC/CARD/07-08 | Siemens,4A Ring Road, I.P. Estate, New Delhi-02 | 1196/CNC/CARD/07-08 | Cath Lab CNC 01No LOCAL ACCESSRIES Lead glass 01no Servo stablizer150KVA 01no On-Line UPS 10KVA 01no. Personal Computer 03nos. Lead Aprons 10nos | P-67/5 |
| 25 | 17/12/08 | IVUS ILAB 240CART | Boston Scientific International B.V. | 836/CARD/CNC/08-09 | Cath Lab CNC 01No. | P-69/5 |
| 26 | 29/12/08 | VIVID 7 Dimension- Leadership 4D Cardiovascular Ultrasound System S.N. 11211V7L | Wipro GE Heath Care (P) Ltd. | 100-9/CARD/CNC/08-09 | Echo Lab CNC 01No. (4) | P-70/5 |
| 27 | 30/03/09 | TILT Table (Electric Operated) | India Medico Instruments. | 1280/CNC/CARD/08-09 | Tilt Lab . CNC(41) | P-71/5 |
| 28 | 13/04/09 | Anaesthesia Machine Prima SP 102 System | Indian Surgical Equipment Co. (P) | 100-5/CARD/CNC/08-09 | Cath Lab,CNC (33) | P72/5 |
| 29 | 25/8/09 | Blood Gas & Electrolyte Analyzer | Rohit Surgical (P) Ltd. | 502/CNC/CARD/09-10 | CT2CCU 02Nos Cath Lab 02Nos CT6 01No | P-75/5 |
| 30 | 16/10/09 | iE33 Intelligent Echocardiog-raphy Ultrasound System 01No. S.N. 034K85 | Philips Electronics (I) Ltd. | 100-44/CNC/CARD/08-09 | ECHO Lab. CNC 01no.(2) | P-76/5 |
| 31 | 25/03/10 | E.P.LAB | St Jude Medical (I) Pvt.Ltd. | 1485/CNC/CARD/09-10 | Cath Lab CNC 01No. (42) | P-77/5 |
| 32 | 26/03/10 | IABP(ARROW) | Ace Medical | 1486/CNC/CARD/09-10 | Cath Lab CNC 02 Nso.(7, 8) | P-78/5 |
| 33 | 26/03/10 | ECG Machine CP-200 | BPLNoble Biomedicals Allen Welsch | 1400/CNC/CARD/09-10 | ECG Lab OPD CNC 02Nos. (3,10) | P-79/5 |
| 34 | 27/03/10 | Basic Digital Copier (Size A-3) | VSM Agencies Pvt. Ltd | 1490/CNC/CARD/09-10 | Deptt. of CARD, CNC 01No. | P-80/5 |
| 35 | 03/6/10 | LP-15 Defib. Monitor with External Pacer | Medtronic Trading NL BV / Rohanika Electronics & Med | 100-60/CNC/CARD/09-10 | Cath Lab CNC 01No.(15) Tilt Lab. CNC 01No.(42) 1 condemned ? | P-81/5 |
| 36 | 06/10/10 | Cardiac Monitors | Philips Electronics | 100-61/CNC/CARD/09-10 | CT-6 Paed. CNC 16Nos. | P-82/5 |
| 37 | 06/10/10 | Ei33 2D Echocardiography Color Doppler System S.N. 03B4T9 | Philips Electronics | 100-59/CNC/CARD/09-10 | ECHO Lab. CNC 01No.(5) | P83/5 |
| 38 | 20/01/11 | FFR (Fractional Flow Reserve) | Kox Med &Lab (P) Ltd. | 1010/CNC/CARD/10-11 | Cath Lab CNC 01No. (25) | P-84/5 |
| 39 | 10/03/11 | ACT Plus (ACT-200) (Medtronic) | J.Mitra & Bros | 1246/CNC/CARD/10-11 | Cath Lab CNC 01No. | P-85/5 |
| 40 | 25/05/10 | Single Plane Cardiovascular Catheterisation with Digital Substraction Angiography (Wipro GE) Lab-III | Wipro GE Healthcare (P) Ltd. | 100-40/CNC/CARD/09-10 | Cath Lab CNC 01No HANDED OVER TO CARDIAC-RADIOLOGY | P-86/5 |
| 41 | 25/05/10 | Local Accessories For S.O.100-40/CNC/CARD/09-10 | Wipro GE Healthcare (P) Ltd. | 1510/CNC/CARD/09-10 | Cath Lab CNC LOCAL ACCESSORIES Pressure Injector_Model Mark V Pro Vis Feom Medrad 01no 120 KVA UPS with 30 minutes backup 01no 150KVA Stablizer 01no. 10 Nos Lead Aprons with hanger 01no. Two way communication between Cathlab and control room 01no | P-87/5 |
| 42 | 25/04/11 | Portable 2D (CX50) Echocardiography Color Doppler System S.N. PHI42-02294 HW Rev.B.1 | Philips Electronics (I) Ltd | 100-23/CNC/CARD/10-11 | ECHO Lab. 1No(7) | P-88/5 |
| 43 | 25/04/11 | Ei33 2D ECHO Cardiography Color Doppler System S.N. B00PXJ HW Rev. G.1 | Philips Electronics (I) Ltd | 100-24/CNC/CARD/10-11 | ECHO Lab. 1No(3) (Buy Back P143/4 HDI (ATL 9HDI 100-34/CNC/CARD/98-99 | P-89/5 |
| 44 | 17/06/11 | External Pacer with Defib. BeneHeart D6 | Shenzhen Mindray Bio-Medical Electronics Co. Ltd. | 100-47/CNC/CARD/10-11 | Cath Lab CNC 02Nos. CT2 CCU, CNC 02Nos CT3 CNC 02 Nos. | P-90/5 |
| 45 | 12/07/11 | Infant Warmer & Nursing Station | Phoenix Medical Systems (P) Ltd. | 244/CNC/CARD/ 11-12 | CT6 02Nos. | P-91/5 |
| 46 | 16/07/11 | Computerized Stress Test System(TMT Machine)Model: X SCRIBE | Compamedic Instruments (P) Ltd. | 100-38/CNC/CARD/ 10-11 | TMT Lab., CNC 01No. | P-92/5 |
| 47 | 09/08/11 | Transport Incubator | Medix I.C.S.A. | 100-39/ CNC/ CARD /10-11 | CT6 01No. | P-93/5 |
| 48 | 23/08/11 | Hand Held ECHO. Mach. S.N. VH0092903H | Wipro GE Healthcare | 100-40/ CNC/ CARD /10-11 | Echo Lab. CNC, 01No. | P-94/5 |
| 49 | 22/06/11 | Single Plane Cardiovascular Catheterisation with Digital Substraction Angiography Lab. (Philips ) Lab-II | Philips Electroncis (I) Ltd. | 100-25/CNC/CARD/10-11 | Cath Lab CNC 01No HANDED OVER TO CARDIAC-RADIOLOGY | P-95/5 |
| 50 | 22/06/11 | Local Accessories For S.O. 100-25/CNC/CARD/ 10-11 | Philips Electroncis (I) Ltd. | 1293/CNC/CARD/ 10-11 LOCAL ACCESSORIES | Cath Lab CNC LOCAL ACCESSORIES UPS for 120KVA with 30 mins back up 01No. Difib. with External Pacer 01No. Lead Apron 10Nos. ACT Machine 01No. P.C. with CD/DVD combo drive with Printer for CD viewing facility 02Nos. | P-96/5 |
| 51 | 10/02/12 | Cautery Machine (MEGAPOWER) Electro-surgical Generator | Unicore Medical System (P) Ltd. |
1452/CNC/CARD/11-12 | Cath Lab CNC 01No (32) | P-97/5 |
| 52 | 01/03/12 | Holter System | Schiller Healthcare | 1450/CNC/CARD/11-12 | Holter lab. CNC 01No. 10 Nos-25-35 | P-98/5 |
| 53 | 13/04/12 | Terufusion Syringe Pump 220V 50Hz Safety Type | M/s J.Mitra & Bros. | 100-39CNC/CARD/11-12 | Cath Lab CNC 03Nos. CT6 CNC 12Nos. CT3 CNC 12Nos. CT 2 CCU CNC 03Nos. | P-99/5 |
| 54 | 13/08/12 | Cardiac Monitors Intellivue MX 800 | M/s Philips Electronics India Ltd. | 100-37/CNC/CARD/11-12 | CT3 CNC 45Nos Cath Lab 3 Nos (38,39,40) | P-100/5 |
| 55 | 17/11/12 | ECG Machine ( BPL Model) Cardiart 9108 | BPL Noble Biomedical | 1063/CNC/CARD/12-13 | ECG Lab OPD , CNC 02 Nos (1,2) | P-101/5 |
| 56 | 31/08/12 | Shimadzu Motorized Mobile X-Ray Unit | Shimadzu Medical (I) Pvt. Ltd. | 100-56/CNC/CR/11-12 | 01 No CT2 CNC 01 No CT6 CNC HANDED OVER TO CARDIAC-RADIOLOGY | P-102/5 |
| 57 | 21/03/13 | Infusion Pump | Hansraj Nayyar Medical India | 1627/CNC/CARD/12-13 | 04Nos. Cath Lab CNC 02 Nos. CT2 CNC 02 Nos. CT3 CNC 02 Nos. CT6 CNC | P-103/5 |
| 58 | 22/03/13 | Deep Vein Thrombosis Pump (DVT Pump) | Cosmotec Medicaments (P) Ltd. | 1625/CNC/CARD/12-13 | 01 No. CT2 CNC 01 No. CT3 CNC | P-104/5 |
| 59 | 28/03/13 | ECG Machine Pagewriter TC50 | DeAsh Trade-Net (P) Ltd., | 1794/CNC/CARD/12-13 | 01 No. CT3 CNC 01 No. CT6 CNC (11,12) | P-105/5 |
| 60 | 28/03/13 | 3D CARTO ELECTROANATOMICAL EP AND MAPPING SYSTEM | Johnson & Johnson Ltd., | 1871/CNC/CARD/12 -13 | 01No. Cath Lab CNC (44) | P-106/5 |
| 61 | 28/03/13 | Optical Coherence Tomography (OCT) C7-XR System | St Jude Medical India (P) Ltd. | 1875/CNC/CARD/12-13 | 01No. Cath Lab CNC (22) | P-107/5 |
| 62 | 30/03/13 | Dual Chamber Temporary Pacemaker PACE T20 | J. Mitra & Bros., | 1777/CNC/CARD/12-13 | 05Nos. Cath Lab CNC | P-108/5 |
| 63 | 30/03/13 | Single Chamber Temporary Pacemaker Pace T10 | J. Mitra & Bros., | 1782/CNC/CARD/12-13 | 05Nos. Cath Lab CNC | P-109/5 |
| 64 | 30/03/13 | Portable C-Arm DSA | Philips Electronics (I) Ltd., | 1774/CNC/CARD/12-13 | 01 No. CT2 CNC HANDED OVER TO CARDIAC-RADIOLOGY | P-110/5 |
| 65 | 27/05/13 | 90217-A Untralite Ambulatory Blood Pressure Monitor with 1 Analyzer | M/s Spacelabs Healthcare | 100-14/CNC/CARD/12-13 | 05Nos. Holter Lab. CNC (ABPS 36-40) | P-111/5 |
| 66 | 24/06/13 | Terufusion Syringe Pump 220V ( TE 331NW3S) | M/s J. Mitra & Bros. | 100-27/CNC/CTVS/ CARD/12-13 | 15Nos. CCU CNC 10Nos. CT3 CNC 15Nos CT6 CNC | P-112/5 |
| 67 | 02/07/13 | Advanced Intensive Care Ventilators ICU Model:- GE ENGSTROM CARESTATION | M/s Wipro GE Healthcare (P) Ltd | 100-38/CNC/CARD/12-13 | 02Nos. CCU CNC 02Nos CT6 CNC | P-113/5 |
| 68 | 09/07/13 | INTRA AORTIC BALLOON PUMP ( IABP- CS100) | M/s Datascope Corpn. Local:- J Mitra & Bros | 100-25/CNC/CARD/12-13 | 02Nos. Cath Lab CNC (6, 9) | P-114/5 |
| 69 | 16/07/13 | Portable CX50 Compact Extreem Ultrasound System S.N. US 31302098 | Philips Electronics (I) Ltd., | 100-16/CNC/CARD/12-13 | 01No CT6 CNC (8) | P-115/5 |
| 70 | 19/07/13 | Hemodynamic Recorder Model:- GE MAC Lab. | M/s Wipro GE Healthcare (P) Ltd | 100-52/CNC/CARD/12-13 | 02Nos. Cath Lab CNC (27, 29) | P-116/5 |
| 71 | 31/03/14 | Forced Air Warmer Unit Mistral –Air ® Plus | M/s Hansraj Healthcare (P) Ltd. | 1647/CNC/CARD/13-14 | 03Nos. CT-6 CNC 01No. Cath Lab ?2 Nos | P-117/5 |
| 72 | 17/06/14 | Syringe Infusion Pump Model WIT-301A | Surya Dev Healthcare | 262/CNC/CARD/14-15 | 10Nos. CCU CNC 05Nos. CT3 CNC 05Nos CT6 CNC | P-118/5 |
| 73 | 14/07/14 | Philips IntelliVue MX 800 Patient Monitor | M/s Philips Healthcare | 100-15/CNC/CARD/ 12-13 | 21Nos. CCU CNC ( 01No. Holter/TMT Lab CNC) 14Nos. CT6 CNC | P-119/5 |
| 74 | 11/02/15 | External Defibrillator, Monitor with Transcutaneous Pacer Phillips | DeAsh Trade-Net (P) Ltd. | 474/CNC/CARD/14-15 | 02Nos. CT2 CCU, CNC | P-120/5 |
| 75 | 11/02/15 | Philips ECG Machine PAGEWRITER TC50 | DeAsh Trade-Net (P) Ltd. | 844/CNC/14-15 | 01No. CT2 CCU, CNC | P-121/5 |
| 76 | 11/05/15 | Infant Warmer Make Phoenix Model:- CIC101 | Phoenix Medical Systems (P) Ltd. | 1338/CNC/14-15 | 04Nos. CT6 CNC | P-122/5 |
| 77 | 10/07/15 23/07/15 | Portable 2D Echocardiography Color Doppler System Model:- GE VIVID Q S.N. 055659 Portable Card 01No. Storage Device (3TB HDD) 01No. | Wipro GE Wipro GE | 100-31/CNC/CARD/14-15 1599/CNC/14-15 | 01No. CT2 CCU CT2 CCU | P-123/5 P-123/5 |
| 78 | 21/07/15 17/07/15 | Fabian HFO Ventilator Essential Accessories for Fabian HFO Ventilator | Acutronics Medical Systems Phoenix Medical Systems | 100-10/ CNC/CARD/14-15 1598/CNC/CARD/14-15 | 01No. CT6 CNC CT6 CNC | P-124/5 P-124/5 |
| 79 | 26/08/15 28/08/15 | Cath Lab Model:-INFX 8000V/G1 Make: Toshiba-Main Unit Accessories | Erbis Engineering Co. Ltd. Erbis Engineering Co. Ltd | 100-26/CNC/CARD/14-15 1419/CNC/CARD/14-15 | Cath Lab, CNC HANDED OVER TO CARDIAC-RADIOLOGY Cath Lab, CNC | P-125/5 P-125/5 |
| 80 | 04/01/16 | Portable 2D Echocardiography Color Doppler System With Intracardiac Echo Facility CX50 Compact Xtreme Ultrasound System S.N. SG 91500055 | Philips Medical Systems | 100-04/CNC/CARD/14-15/ST | 01No.ECHO lab, CNC | P-126/5 |
| 81 | 03/03/16 | BFW Head Light | Asia Pacipic Export/J. Mitra & Bros. | 100-13/CNC/CARD/14-15/ST | 01No. Cath Lab , CNC | P-127/5 |
| 82 | 04/07/16 | EPIQ CV Ultrasound System S.N. US316B0387 | Philips Medical System | 100-28/CNC/CARD/14-15/AT | 01No.ECHO lab, CNC | P-128/5 |
| 83 | 27/07/16 | Syringe Pump M- AP-12-DL Make SSMED | S.S. Medical Systems (I) Pvt. Ltd. | 188/CNC/CARD/16-17/ST | 04Nos. CT2 CCU, CNC 03Nos. CT3, CNC 03Nos. CT6, CNC 03Nos. Cath Lab. CNC | P-129/5 |
| 84 | 03/10/16 | New Holter Recorder for Holter Lab. | Schiller Healthcare | 858/CNC/CARD/16-17 | 10Nos. Holter Lab, CNC | P-130/5 |
| 85 | 02/12/16 | Portable ECG Machine Model-3312B | Taurus Healthcare (P) Ltd. | 1047/CNC/CARD/16-17 | 02Nos. ECG Lab CT-6 02Nos. ECG Lab OPD | P-131/5 |
| 86 | 31/3/17 | External Defibrillator, with Transcutaneous Pacer | Medina 2500 | 1393/CNC/CARD/ 16-17 | 01Nos. CT2 01Nos. CT3 01Nos. CT6 01Nos. TMT 01Nos. Cath Lab | P-132/5 |
| S.No | Date | Particulars of Assets | Name &address of supplier | Bill No. & date | Location of the Assets | Remarks |
|---|---|---|---|---|---|---|
| 1 | 04/03/03 | 3M Steri-Vac (1) | 3M (I) Ltd. | 996/CNC/CARD/02-03 | Cath Lab, CNC 01no. | P-317/4 |
| 2 | 15/03/04 | Anaesthesia Machine Excel-210E Astopad Plus Control (1) | Rohanika Electronics | 100-79/CNC/CARD/02-03 | Cath Lab, CNC 01no. | P-331/4 |
| 3 | 31/05/05 | Defibrillator LP-20 (1) | Intstromedix | 100-34/CNC/CARD/04-05 | .CT2 CCU CNC 01No. | P-16/5 |
| 4 | 07/07/05 | Programmable Stimulator BARD (1) | Advanced Micronic Device | 100-31/CNC/CARD/04-05 | Cath Lab. CNC 01No. | P-19/5 |
| 5 | 29/03/05 | Dual Chamber Pacemaker (2) | Saturn Med. System | 1211/CNC/CARD/04-05. | Cath Lab, CNC 02nos. | P-30/5 |
| 6 | 29/03/05 | Single Chamber Pacemaker (10) | Saturn Med. System | 1210/CNC/CARD/04-05 | CT3 CNC 01no Cath Lab, CNC 02nos CT2 CCU CNC 02nos. CT6 CNC 02nos. | P-31/5 |
| 7 | 27/05/06 | Multiweigh (3-in-1) (Zeal) | Globe Medical System | 1472/CNC/CARD/05-06 | Cath Lab. CNC 02nos. (41) | P-34/5 |
| 8 | 30/08/06 | Transfusion Syringe Pumps (9) | J.Mitra & Bros. | 100-48/CNC/CARD/05-06 | Cath Lab, CNC 03nos CT2 CCU CNC 05nos. CT6 CNC 01nos | P-36/5 |
| 9 | 28/10/06 | Latest Advanced Tech. Ventilator (Servo) (1) | Maquet Medical India (P) Ltd. | 100-51/CNC/CARD/05-06 | CT2 CCU CNC 01no. CT6 CNC 01no | P-39/5 |
| 11 | 17/10/06 | IE33 Echocardiog-raphy System 01No. S.N.02RBWD | Philips Electronics (I) Ltd. | 100-52/CNC/CARD/05-06 | ECHO Lab. CNC 01no. | P-40/5 |
| 12 | 09/10/06 | TMT System (GE Model 2100) | Wipro GE Medical System Ltd. | 100-74/CNC/CARD/05-06 | TMT Lab. CNC 01no. | P-41/5 |
| 13 | 12/04/07 | Transport Monitor (M9000). | Advanced Micronic Devices Ltd. | 1381/CNC/CARD/06-07 | CT6 CNC 01no. 81 condemned | P-43/5 |
| 14 | 29/05/07 | External Defibrillator Med Aid 05Nos. | Advanced Micronic Devices | 1380/CNC/CARD/06-07 | CT3 CNC 01nos. CT6 CNC 01no. 3 condemned | P-46/5 |
| 15 | 05/07/07 | ACT200 Plus TM Automated Coagulation Timer 03Nos. | J.Mitra & Bros. | 1379/CNC/CARD/06-07 | Cath Lab, CNC 01no. CT2 CCU. CNC 01no CT3 CNC 01no. | P-48/5 Through CTVS Department CNC |
| 16 | 09/08/07 | Air Supply Unit for Horus Extend Unit 02Nos. | Electrocare System & Services (P) Ltd. | 1476/CNC/CARD/06-07 | CT2 CCU CNC 02nos. | P-49/5 |
| 17 | 10/08/07 | Ventilator 02Nos. | Electrocare System & Services (P) Ltd. | 100-83/CNC/CARD/06-07 | CT2 CCU CNC 02nos. | P-50/5 |
| 18 | 16/07/07 | Hemodynamic Recorder for Cath Lab I & II 02Nos. | Wipro GE Healthcare | 100-61/CNC/CARD/06-07 | Cath Lab CNC 02nos.(26, 27) | P-51/5 |
| 19 | 26/09/07 | Infusion Pumps 20Nos. | J.Mitra & Bros. | 100-56/CNC/CARD/06-07 | CT3 CNC 05nos Cath Lab CNC 05nos. CT2 CCU CNC 08nos. | P-53/5 |
| 20 | 05/10/07 | RF Generator & Infusion Pump 01No. | Johnson & Johnson Ltd. | 100- 57/CNC/CARD/06-07 | Cath Lab. CNC 01no. | P-56/5 |
| 21 | 19/03/08 | Intra Cardio Echo Catheter 01No. | Siemens Ltd | 100-30/CARD/CNC/06-07 | Echo Lab. CNC 01no. | P-61/5 |
| 22 | 15/04/08 | ECG Machine AT1 (Schiller) 02Nos. | Schiller Healthcare (I) Pvt. Ltd. | 1114/CARD/CNC/07-08 | ECG Lab CT6 CNC 2nos. (6, 7) | P-63/5 |
| 23 | 04/09/2008 | Bi Plane Cardiovascular Catheterisation Lab (Siemens) Lab I 01No. | Siemens Ltd., 127, Henkestrasse, D-91052, Erlangen, Germany/Local-4A Ring Road, I.P. Estate, New Delhi-02 | 100-47/CNC/CARD/07-08 | Cath Lab CNC 01No. HANDED OVER TO CARDIAC-RADIOLOGY | P-65-66/5 |
| 24 | 04/09/2008 | Local Accessories For Cath Lab S.O.100-47/CNC/CARD/07-08 | Siemens,4A Ring Road, I.P. Estate, New Delhi-02 | 1196/CNC/CARD/07-08 | Cath Lab CNC 01No LOCAL ACCESSRIES Lead glass 01no Servo stablizer150KVA 01no On-Line UPS 10KVA 01no. Personal Computer 03nos. Lead Aprons 10nos | P-67/5 |
| 25 | 17/12/08 | IVUS ILAB 240CART | Boston Scientific International B.V. | 836/CARD/CNC/08-09 | Cath Lab CNC 01No. | P-69/5 |
| 26 | 29/12/08 | VIVID 7 Dimension- Leadership 4D Cardiovascular Ultrasound System S.N. 11211V7L | Wipro GE Heath Care (P) Ltd. | 100-9/CARD/CNC/08-09 | Echo Lab CNC 01No. (4) | P-70/5 |
| 27 | 30/03/09 | TILT Table (Electric Operated) | India Medico Instruments. | 1280/CNC/CARD/08-09 | Tilt Lab . CNC(41) | P-71/5 |
| 28 | 13/04/09 | Anaesthesia Machine Prima SP 102 System | Indian Surgical Equipment Co. (P) | 100-5/CARD/CNC/08-09 | Cath Lab,CNC (33) | P72/5 |
| 29 | 25/8/09 | Blood Gas & Electrolyte Analyzer | Rohit Surgical (P) Ltd. | 502/CNC/CARD/09-10 | CT2CCU 02Nos Cath Lab 02Nos CT6 01No | P-75/5 |
| 30 | 16/10/09 | iE33 Intelligent Echocardiog-raphy Ultrasound System 01No. S.N. 034K85 | Philips Electronics (I) Ltd. | 100-44/CNC/CARD/08-09 | ECHO Lab. CNC 01no.(2) | P-76/5 |
| 31 | 25/03/10 | E.P.LAB | St Jude Medical (I) Pvt.Ltd. | 1485/CNC/CARD/09-10 | Cath Lab CNC 01No. (42) | P-77/5 |
| 32 | 26/03/10 | IABP(ARROW) | Ace Medical | 1486/CNC/CARD/09-10 | Cath Lab CNC 02 Nso.(7, 8) | P-78/5 |
| 33 | 26/03/10 | ECG Machine CP-200 | BPLNoble Biomedicals Allen Welsch | 1400/CNC/CARD/09-10 | ECG Lab OPD CNC 02Nos. (3,10) | P-79/5 |
| 34 | 27/03/10 | Basic Digital Copier (Size A-3) | VSM Agencies Pvt. Ltd | 1490/CNC/CARD/09-10 | Deptt. of CARD, CNC 01No. | P-80/5 |
| 35 | 03/6/10 | LP-15 Defib. Monitor with External Pacer | Medtronic Trading NL BV / Rohanika Electronics & Med | 100-60/CNC/CARD/09-10 | Cath Lab CNC 01No.(15) Tilt Lab. CNC 01No.(42) 1 condemned ? | P-81/5 |
| 36 | 06/10/10 | Cardiac Monitors | Philips Electronics | 100-61/CNC/CARD/09-10 | CT-6 Paed. CNC 16Nos. | P-82/5 |
| 37 | 06/10/10 | Ei33 2D Echocardiography Color Doppler System S.N. 03B4T9 | Philips Electronics | 100-59/CNC/CARD/09-10 | ECHO Lab. CNC 01No.(5) | P83/5 |
| 38 | 20/01/11 | FFR (Fractional Flow Reserve) | Kox Med &Lab (P) Ltd. | 1010/CNC/CARD/10-11 | Cath Lab CNC 01No. (25) | P-84/5 |
| 39 | 10/03/11 | ACT Plus (ACT-200) (Medtronic) | J.Mitra & Bros | 1246/CNC/CARD/10-11 | Cath Lab CNC 01No. | P-85/5 |
| 40 | 25/05/10 | Single Plane Cardiovascular Catheterisation with Digital Substraction Angiography (Wipro GE) Lab-III | Wipro GE Healthcare (P) Ltd. | 100-40/CNC/CARD/09-10 | Cath Lab CNC 01No HANDED OVER TO CARDIAC-RADIOLOGY | P-86/5 |
| 41 | 25/05/10 | Local Accessories For S.O.100-40/CNC/CARD/09-10 | Wipro GE Healthcare (P) Ltd. | 1510/CNC/CARD/09-10 | Cath Lab CNC LOCAL ACCESSORIES Pressure Injector_Model Mark V Pro Vis Feom Medrad 01no 120 KVA UPS with 30 minutes backup 01no 150KVA Stablizer 01no. 10 Nos Lead Aprons with hanger 01no. Two way communication between Cathlab and control room 01no | P-87/5 |
| 42 | 25/04/11 | Portable 2D (CX50) Echocardiography Color Doppler System S.N. PHI42-02294 HW Rev.B.1 | Philips Electronics (I) Ltd | 100-23/CNC/CARD/10-11 | ECHO Lab. 1No(7) | P-88/5 |
| 43 | 25/04/11 | Ei33 2D ECHO Cardiography Color Doppler System S.N. B00PXJ HW Rev. G.1 | Philips Electronics (I) Ltd | 100-24/CNC/CARD/10-11 | ECHO Lab. 1No(3) (Buy Back P143/4 HDI (ATL 9HDI 100-34/CNC/CARD/98-99 | P-89/5 |
| 44 | 17/06/11 | External Pacer with Defib. BeneHeart D6 | Shenzhen Mindray Bio-Medical Electronics Co. Ltd. | 100-47/CNC/CARD/10-11 | Cath Lab CNC 02Nos. CT2 CCU, CNC 02Nos CT3 CNC 02 Nos. | P-90/5 |
| 45 | 12/07/11 | Infant Warmer & Nursing Station | Phoenix Medical Systems (P) Ltd. | 244/CNC/CARD/ 11-12 | CT6 02Nos. | P-91/5 |
| 46 | 16/07/11 | Computerized Stress Test System(TMT Machine)Model: X SCRIBE | Compamedic Instruments (P) Ltd. | 100-38/CNC/CARD/ 10-11 | TMT Lab., CNC 01No. | P-92/5 |
| 47 | 09/08/11 | Transport Incubator | Medix I.C.S.A. | 100-39/ CNC/ CARD /10-11 | CT6 01No. | P-93/5 |
| 48 | 23/08/11 | Hand Held ECHO. Mach. S.N. VH0092903H | Wipro GE Healthcare | 100-40/ CNC/ CARD /10-11 | Echo Lab. CNC, 01No. | P-94/5 |
| 49 | 22/06/11 | Single Plane Cardiovascular Catheterisation with Digital Substraction Angiography Lab. (Philips ) Lab-II | Philips Electroncis (I) Ltd. | 100-25/CNC/CARD/10-11 | Cath Lab CNC 01No HANDED OVER TO CARDIAC-RADIOLOGY | P-95/5 |
| 50 | 22/06/11 | Local Accessories For S.O. 100-25/CNC/CARD/ 10-11 | Philips Electroncis (I) Ltd. | 1293/CNC/CARD/ 10-11 LOCAL ACCESSORIES | Cath Lab CNC LOCAL ACCESSORIES UPS for 120KVA with 30 mins back up 01No. Difib. with External Pacer 01No. Lead Apron 10Nos. ACT Machine 01No. P.C. with CD/DVD combo drive with Printer for CD viewing facility 02Nos. | P-96/5 |
| 51 | 10/02/12 | Cautery Machine (MEGAPOWER) Electro-surgical Generator | Unicore Medical System (P) Ltd. |
1452/CNC/CARD/11-12 | Cath Lab CNC 01No (32) | P-97/5 |
| 52 | 01/03/12 | Holter System | Schiller Healthcare | 1450/CNC/CARD/11-12 | Holter lab. CNC 01No. 10 Nos-25-35 | P-98/5 |
| 53 | 13/04/12 | Terufusion Syringe Pump 220V 50Hz Safety Type | M/s J.Mitra & Bros. | 100-39CNC/CARD/11-12 | Cath Lab CNC 03Nos. CT6 CNC 12Nos. CT3 CNC 12Nos. CT 2 CCU CNC 03Nos. | P-99/5 |
| 54 | 13/08/12 | Cardiac Monitors Intellivue MX 800 | M/s Philips Electronics India Ltd. | 100-37/CNC/CARD/11-12 | CT3 CNC 45Nos Cath Lab 3 Nos (38,39,40) | P-100/5 |
| 55 | 17/11/12 | ECG Machine ( BPL Model) Cardiart 9108 | BPL Noble Biomedical | 1063/CNC/CARD/12-13 | ECG Lab OPD , CNC 02 Nos (1,2) | P-101/5 |
| 56 | 31/08/12 | Shimadzu Motorized Mobile X-Ray Unit | Shimadzu Medical (I) Pvt. Ltd. | 100-56/CNC/CR/11-12 | 01 No CT2 CNC 01 No CT6 CNC HANDED OVER TO CARDIAC-RADIOLOGY | P-102/5 |
| 57 | 21/03/13 | Infusion Pump | Hansraj Nayyar Medical India | 1627/CNC/CARD/12-13 | 04Nos. Cath Lab CNC 02 Nos. CT2 CNC 02 Nos. CT3 CNC 02 Nos. CT6 CNC | P-103/5 |
| 58 | 22/03/13 | Deep Vein Thrombosis Pump (DVT Pump) | Cosmotec Medicaments (P) Ltd. | 1625/CNC/CARD/12-13 | 01 No. CT2 CNC 01 No. CT3 CNC | P-104/5 |
| 59 | 28/03/13 | ECG Machine Pagewriter TC50 | DeAsh Trade-Net (P) Ltd., | 1794/CNC/CARD/12-13 | 01 No. CT3 CNC 01 No. CT6 CNC (11,12) | P-105/5 |
| 60 | 28/03/13 | 3D CARTO ELECTROANATOMICAL EP AND MAPPING SYSTEM | Johnson & Johnson Ltd., | 1871/CNC/CARD/12 -13 | 01No. Cath Lab CNC (44) | P-106/5 |
| 61 | 28/03/13 | Optical Coherence Tomography (OCT) C7-XR System | St Jude Medical India (P) Ltd. | 1875/CNC/CARD/12-13 | 01No. Cath Lab CNC (22) | P-107/5 |
| 62 | 30/03/13 | Dual Chamber Temporary Pacemaker PACE T20 | J. Mitra & Bros., | 1777/CNC/CARD/12-13 | 05Nos. Cath Lab CNC | P-108/5 |
| 63 | 30/03/13 | Single Chamber Temporary Pacemaker Pace T10 | J. Mitra & Bros., | 1782/CNC/CARD/12-13 | 05Nos. Cath Lab CNC | P-109/5 |
| 64 | 30/03/13 | Portable C-Arm DSA | Philips Electronics (I) Ltd., | 1774/CNC/CARD/12-13 | 01 No. CT2 CNC HANDED OVER TO CARDIAC-RADIOLOGY | P-110/5 |
| 65 | 27/05/13 | 90217-A Untralite Ambulatory Blood Pressure Monitor with 1 Analyzer | M/s Spacelabs Healthcare | 100-14/CNC/CARD/12-13 | 05Nos. Holter Lab. CNC (ABPS 36-40) | P-111/5 |
| 66 | 24/06/13 | Terufusion Syringe Pump 220V ( TE 331NW3S) | M/s J. Mitra & Bros. | 100-27/CNC/CTVS/ CARD/12-13 | 15Nos. CCU CNC 10Nos. CT3 CNC 15Nos CT6 CNC | P-112/5 |
| 67 | 02/07/13 | Advanced Intensive Care Ventilators ICU Model:- GE ENGSTROM CARESTATION | M/s Wipro GE Healthcare (P) Ltd | 100-38/CNC/CARD/12-13 | 02Nos. CCU CNC 02Nos CT6 CNC | P-113/5 |
| 68 | 09/07/13 | INTRA AORTIC BALLOON PUMP ( IABP- CS100) | M/s Datascope Corpn. Local:- J Mitra & Bros | 100-25/CNC/CARD/12-13 | 02Nos. Cath Lab CNC (6, 9) | P-114/5 |
| 69 | 16/07/13 | Portable CX50 Compact Extreem Ultrasound System S.N. US 31302098 | Philips Electronics (I) Ltd., | 100-16/CNC/CARD/12-13 | 01No CT6 CNC (8) | P-115/5 |
| 70 | 19/07/13 | Hemodynamic Recorder Model:- GE MAC Lab. | M/s Wipro GE Healthcare (P) Ltd | 100-52/CNC/CARD/12-13 | 02Nos. Cath Lab CNC (27, 29) | P-116/5 |
| 71 | 31/03/14 | Forced Air Warmer Unit Mistral –Air ® Plus | M/s Hansraj Healthcare (P) Ltd. | 1647/CNC/CARD/13-14 | 03Nos. CT-6 CNC 01No. Cath Lab ?2 Nos | P-117/5 |
| 72 | 17/06/14 | Syringe Infusion Pump Model WIT-301A | Surya Dev Healthcare | 262/CNC/CARD/14-15 | 10Nos. CCU CNC 05Nos. CT3 CNC 05Nos CT6 CNC | P-118/5 |
| 73 | 14/07/14 | Philips IntelliVue MX 800 Patient Monitor | M/s Philips Healthcare | 100-15/CNC/CARD/ 12-13 | 21Nos. CCU CNC ( 01No. Holter/TMT Lab CNC) 14Nos. CT6 CNC | P-119/5 |
| 74 | 11/02/15 | External Defibrillator, Monitor with Transcutaneous Pacer Phillips | DeAsh Trade-Net (P) Ltd. | 474/CNC/CARD/14-15 | 02Nos. CT2 CCU, CNC | P-120/5 |
| 75 | 11/02/15 | Philips ECG Machine PAGEWRITER TC50 | DeAsh Trade-Net (P) Ltd. | 844/CNC/14-15 | 01No. CT2 CCU, CNC | P-121/5 |
| 76 | 11/05/15 | Infant Warmer Make Phoenix Model:- CIC101 | Phoenix Medical Systems (P) Ltd. | 1338/CNC/14-15 | 04Nos. CT6 CNC | P-122/5 |
| 77 | 10/07/15 23/07/15 | Portable 2D Echocardiography Color Doppler System Model:- GE VIVID Q S.N. 055659 Portable Card 01No. Storage Device (3TB HDD) 01No. | Wipro GE Wipro GE | 100-31/CNC/CARD/14-15 1599/CNC/14-15 | 01No. CT2 CCU CT2 CCU | P-123/5 P-123/5 |
| 78 | 21/07/15 17/07/15 | Fabian HFO Ventilator Essential Accessories for Fabian HFO Ventilator | Acutronics Medical Systems Phoenix Medical Systems | 100-10/ CNC/CARD/14-15 1598/CNC/CARD/14-15 | 01No. CT6 CNC CT6 CNC | P-124/5 P-124/5 |
| 79 | 26/08/15 28/08/15 | Cath Lab Model:-INFX 8000V/G1 Make: Toshiba-Main Unit Accessories | Erbis Engineering Co. Ltd. Erbis Engineering Co. Ltd | 100-26/CNC/CARD/14-15 1419/CNC/CARD/14-15 | Cath Lab, CNC HANDED OVER TO CARDIAC-RADIOLOGY Cath Lab, CNC | P-125/5 P-125/5 |
| 80 | 04/01/16 | Portable 2D Echocardiography Color Doppler System With Intracardiac Echo Facility CX50 Compact Xtreme Ultrasound System S.N. SG 91500055 | Philips Medical Systems | 100-04/CNC/CARD/14-15/ST | 01No.ECHO lab, CNC | P-126/5 |
| 81 | 03/03/16 | BFW Head Light | Asia Pacipic Export/J. Mitra & Bros. | 100-13/CNC/CARD/14-15/ST | 01No. Cath Lab , CNC | P-127/5 |
| 82 | 04/07/16 | EPIQ CV Ultrasound System S.N. US316B0387 | Philips Medical System | 100-28/CNC/CARD/14-15/AT | 01No.ECHO lab, CNC | P-128/5 |
| 83 | 27/07/16 | Syringe Pump M- AP-12-DL Make SSMED | S.S. Medical Systems (I) Pvt. Ltd. | 188/CNC/CARD/16-17/ST | 04Nos. CT2 CCU, CNC 03Nos. CT3, CNC 03Nos. CT6, CNC 03Nos. Cath Lab. CNC | P-129/5 |
| 84 | 03/10/16 | New Holter Recorder for Holter Lab. | Schiller Healthcare | 858/CNC/CARD/16-17 | 10Nos. Holter Lab, CNC | P-130/5 |
| 85 | 02/12/16 | Portable ECG Machine Model-3312B | Taurus Healthcare (P) Ltd. | 1047/CNC/CARD/16-17 | 02Nos. ECG Lab CT-6 02Nos. ECG Lab OPD | P-131/5 |
| 86 | 31/3/17 | External Defibrillator, with Transcutaneous Pacer | Medina 2500 | 1393/CNC/CARD/ 16-17 | 01Nos. CT2 01Nos. CT3 01Nos. CT6 01Nos. TMT 01Nos. Cath Lab | P-132/5 |
| M.D. (Biophysics) | M.Sc. (Biophysics) | Ph.D. (Biophysics) | |
|---|---|---|---|
| Duration | 3 years | 2 years | 3-5 years |
| Month(s) of Entrance Exam | May and November | July | January and July |
| Course Syllabus | MD (Biophysics) Syllabus | M.Sc. (Biophysics) Syllabus | - |
The Department of Biophysics imparts long- and short-term training to M.Sc and M.Tech students from different institutes and universities.
Cell biology:Organization and structure of prokaryotes and eukaryotes, nucleus, cytoplasm, plasma membrane, mitochondria-structure, function respiratory chain and ATP synthesis, endoplasmic reticulum, golgi apparatus, membranes, ribosomes, peroxisomes, lysozomes, transcription and translation, transport of proteins, cancer and its molecular genetics, oncogenes, tumor suppression gene
Molecular biology: central dogma, genetic code, gene and operon, structure of DNA and RNA, plasmids, selectable markers, agarose gel, PCR, cloning PCR products, expression vectors, cell free translation, c- DNA libraries, genomic libraries, DNA micro arrays, DNA sequencing
Bioinformatics:Introduction, repositories, databases, pairwise sequence based alignment, relationship between sequence and structures, structural bioinformatics, genomics, proteomics, human genome project, software packages
Numerical methods: Introduction to numerical methods, solutions to non-linear algebraic equations by the method of iteration and Newton aphson method, numerical integration by trapezoidal rule and simpson’s rule, numerical solution of ordinary differential equations by picard’s method of successive approximation, Euler’s method and Runge-Kutta method
Dynamics of non-linear processes: Physico-mathematical foundations of the dynamics of non-linear processes, phase plane method, different modes of excitations, nearly sinusoidal oscillations, building up of oscillations, effect of third harmonic distortion, Liapounov criteria of stability, limit cycles
Elementary crystallography: Introduction, symmetry in crystals, lattices and unit cells, crystal systems, Bravais lattices, elements of symmetry- rotation axis, mirror planes and center of inversion, point group symmetry- monoaxial point groups, polyaxial point groups, translational symmetry- screw axis and glide planes, space group, equivalent points, X-ray diffraction and Bragg equation
X-ray diffraction methods: scattering factor, structure factor expression, reciprocal lattice, Ewald’s sphere, electron density equation, phase problem, Patterson function, molecular replacement method, isomorphous replacement, refinement programs and interpretation of results, methods of data collection of crystal containing small molecule and large molecule, factors affecting the measurement of integrated intensities, photographic methods, diffractometers, area detectors and image plates.
Proteins : Purification, structure and function: twenty amino acids: structure and function, the peptide bond, primary structure of a protein: methods of sequence determination, forces determining protein structure, secondary structure of a protein: β strands, β sheets (parallel and anti parallel), β turns, α helix, 3.10 helix and π helix (differences), tertiary structure of a protein: protein folds-all alpha helix motifs (Lone helix, helix-turn-helix, four helix bundle and eight helix bundle), protein folds-all β sheet motifs (β sandwich, β barrel, greek Key topology and β propellars), protein folds- α / β motifs (Tim barrel, Rosman fold, α/β horseshoe), quaternary structure of a protein: macromolecular assemblies, domains and domain swapping, membrane proteins, purification methods, studies of proteins with MALDI-TOF, enzymes and enzyme kinetics, G-proteins and G-protein coupled receptors(GPCRs), proteins as targets for rational structure based drug design
Principles of nucleic acid structure: nucleotide structure and properties: Introduction to DNA, RNA, bases, sugars, phosphates, structure of nucleotide, nucleosides and polynucleotides and their nomenclature scheme. tautomerisation and ionization. genetic code. stereochemistry: nucleoside, torsion angles, sugar confirmation, NMR study, DNA structure: different types of DNA and their structure, DNA motifs, DNA repeats and their significance, function and stability, spectroscpic study of DNA: dye binding, interaction, denaturation, and renaturation of DNA, thermal denaturation and Tm value, RNA: structure and properties, different forms of RNA and their significance, alkaline hydrolysis of RNA, how it differs from DNA, role of 2’OH group, structure of phenylalanine tRNA, enzymes involved in molecular biology: DNA polymerase, RNA polymerase, reverse transcriptase, restriction endonuclease. DNA interaction: protein, dye, drugs and carcinogens, DNA replication: DNA polymerization, mutation, and DNA repair, DNA transcription: RNA synthesis, types of RNA polymerase, DNA polymorphism: repeats of DNA and their significance, single nucleotide polymorphism, c-DNA, cloning and expression and purification
Membrane Biology: Lipid structure and their organization, comparison of different membrane models, diffusion and permeability, different types of transport systems across membranes, liposome and its applications
Peptides-design, synthesis and applications: Introduction to peptides, peptide design, synthesis of peptides (solution phase and solid phase), protection and deprotection of amino and carboxyl group, unnatural amino acids, conformation of peptides, purification and crystallization of peptides, determination of structure of small molecules (briefly), application of peptides
Mathematical methods and their applications in biological systems: Ordinary differential equations of the first degree and first order (variable separable method, linear equation), linear differential equations of the second order with constant coefficients, the Laplace Transform, Inverse Laplace transform, application of Laplace transform to solutions of differential equations, Fourier series and their applications.
Quantum biology and its uses: Classical mechanics, Newton, Lagrange and Hamilton’s equations, Schrodinger’s equation and its complete solution for S.H.O, central force and angular momentum
Quantum chemistry: Atomic orbital models, the wave equation, molecular orbitals, the LCAO method, the overlap method, coulomb and resonance integrals, the hydrogen molecule, charge distributions, approximate methods.
Theoretical modeling of biomolecular systems: Basic principles of modeling, modeling by energy minimization technique, concept of rotation about bonds, energy minimization by basic technique for small molecules, Ramachandran plot, torsional space minimization, energy minimization in cartesian space, molecular mechanics-basic principle, molecular dynamics basic principles
Spectroscopic techniques: Introduction to spectroscopy, basic principles, instrumentation and applications of UV-VIS absorption, infrared, Raman, atomic absorption, fluorescence, circular dichroism, Laser spectroscopy, nuclear magnetic resonance, electron spin resonance, acoustic spectroscopy; solvent perturbation; difference spectroscopy; Fourier transform techniques; applications of Laser; mass spectroscopy.
Cell biology:Organization and structure of prokaryotes and eukaryotes, nucleus, cytoplasm, plasma membrane, mitochondria-structure, function respiratory chain and ATP synthesis, endoplasmic reticulum, golgi apparatus, membranes, ribosomes, peroxisomes, lysozomes, transcription and translation, transport of proteins, cancer and its molecular genetics, oncogenes, tumor suppression gene
Molecular biology: central dogma, genetic code, gene and operon, structure of DNA and RNA, plasmids, selectable markers, agarose gel, PCR, cloning PCR products, expression vectors, cell free translation, c- DNA libraries, genomic libraries, DNA micro arrays, DNA sequencing
Bioinformatics:Introduction, repositories, databases, pairwise sequence based alignment, relationship between sequence and structures, structural bioinformatics, genomics, proteomics, human genome project, software packages
Numerical methods: Introduction to numerical methods, solutions to non-linear algebraic equations by the method of iteration and Newton aphson method, numerical integration by trapezoidal rule and simpson’s rule, numerical solution of ordinary differential equations by picard’s method of successive approximation, Euler’s method and Runge-Kutta method
Dynamics of non-linear processes: Physico-mathematical foundations of the dynamics of non-linear processes, phase plane method, different modes of excitations, nearly sinusoidal oscillations, building up of oscillations, effect of third harmonic distortion, Liapounov criteria of stability, limit cycles
Elementary crystallography: Introduction, symmetry in crystals, lattices and unit cells, crystal systems, Bravais lattices, elements of symmetry- rotation axis, mirror planes and center of inversion, point group symmetry- monoaxial point groups, polyaxial point groups, translational symmetry- screw axis and glide planes, space group, equivalent points, X-ray diffraction and Bragg equation
X-ray diffraction methods: scattering factor, structure factor expression, reciprocal lattice, Ewald’s sphere, electron density equation, phase problem, Patterson function, molecular replacement method, isomorphous replacement, refinement programs and interpretation of results, methods of data collection of crystal containing small molecule and large molecule, factors affecting the measurement of integrated intensities, photographic methods, diffractometers, area detectors and image plates.
Proteins : Purification, structure and function: twenty amino acids: structure and function, the peptide bond, primary structure of a protein: methods of sequence determination, forces determining protein structure, secondary structure of a protein: β strands, β sheets (parallel and anti parallel), β turns, α helix, 3.10 helix and π helix (differences), tertiary structure of a protein: protein folds-all alpha helix motifs (Lone helix, helix-turn-helix, four helix bundle and eight helix bundle), protein folds-all β sheet motifs (β sandwich, β barrel, greek Key topology and β propellars), protein folds- α / β motifs (Tim barrel, Rosman fold, α/β horseshoe), quaternary structure of a protein: macromolecular assemblies, domains and domain swapping, membrane proteins, purification methods, studies of proteins with MALDI-TOF, enzymes and enzyme kinetics, G-proteins and G-protein coupled receptors(GPCRs), proteins as targets for rational structure based drug design
Principles of nucleic acid structure: nucleotide structure and properties: Introduction to DNA, RNA, bases, sugars, phosphates, structure of nucleotide, nucleosides and polynucleotides and their nomenclature scheme. tautomerisation and ionization. genetic code. stereochemistry: nucleoside, torsion angles, sugar confirmation, NMR study, DNA structure: different types of DNA and their structure, DNA motifs, DNA repeats and their significance, function and stability, spectroscpic study of DNA: dye binding, interaction, denaturation, and renaturation of DNA, thermal denaturation and Tm value, RNA: structure and properties, different forms of RNA and their significance, alkaline hydrolysis of RNA, how it differs from DNA, role of 2’OH group, structure of phenylalanine tRNA, enzymes involved in molecular biology: DNA polymerase, RNA polymerase, reverse transcriptase, restriction endonuclease. DNA interaction: protein, dye, drugs and carcinogens, DNA replication: DNA polymerization, mutation, and DNA repair, DNA transcription: RNA synthesis, types of RNA polymerase, DNA polymorphism: repeats of DNA and their significance, single nucleotide polymorphism, c-DNA, cloning and expression and purification
Membrane Biology: Lipid structure and their organization, comparison of different membrane models, diffusion and permeability, different types of transport systems across membranes, liposome and its applications
Peptides-design, synthesis and applications: Introduction to peptides, peptide design, synthesis of peptides (solution phase and solid phase), protection and deprotection of amino and carboxyl group, unnatural amino acids, conformation of peptides, purification and crystallization of peptides, determination of structure of small molecules (briefly), application of peptides
Mathematical methods and their applications in biological systems: Ordinary differential equations of the first degree and first order (variable separable method, linear equation), linear differential equations of the second order with constant coefficients, the Laplace Transform, Inverse Laplace transform, application of Laplace transform to solutions of differential equations, Fourier series and their applications.
Quantum biology and its uses: Classical mechanics, Newton, Lagrange and Hamilton’s equations, Schrodinger’s equation and its complete solution for S.H.O, central force and angular momentum
Quantum chemistry: Atomic orbital models, the wave equation, molecular orbitals, the LCAO method, the overlap method, coulomb and resonance integrals, the hydrogen molecule, charge distributions, approximate methods.
Theoretical modeling of biomolecular systems: Basic principles of modeling, modeling by energy minimization technique, concept of rotation about bonds, energy minimization by basic technique for small molecules, Ramachandran plot, torsional space minimization, energy minimization in cartesian space, molecular mechanics-basic principle, molecular dynamics basic principles
Spectroscopic techniques: Introduction to spectroscopy, basic principles, instrumentation and applications of UV-VIS absorption, infrared, Raman, atomic absorption, fluorescence, circular dichroism, Laser spectroscopy, nuclear magnetic resonance, electron spin resonance, acoustic spectroscopy; solvent perturbation; difference spectroscopy; Fourier transform techniques; applications of Laser; mass spectroscopy.
Designation :Professor
Present Address :Centre for Community Medicine, Old O.T. Block, All India Institute of Medical Sciences, New Delhi-110029
Phone No (office): 011-26593789
E-mail : baridalyne@gmail.com, bari_111@yahoo.com
1. Obtained MBBS degree from Silchar Medical College, Assam in 1993
2. Completed MD in Community Medicine from All India Institute of Medical Sciences, New Delhi in December 1999.
Worked as a faculty since 2003 in Centre for Community Medicine AIIMS
Published 102+papers in various national and international journals. Also involved with numerous research projects on non -communicable diseases, funded by WHO and Indian Council of Medical Research.
Area of work is on health systems, planning, implementation and evaluation of health programs. My interest area is on non-communicable diseases, cancer prevention and control, medical education and primary health care I am actively involved with various activities of the National Program for Prevention and Control of Cancer Diabetes Cardiovascular Disease Stroke (NPCDCS) in India. Supported by WHO India, I have developed a training package for training program managers in NCD programme in various states in India in 2016. I have been a national trainer for NCD program implementation in India and provided training for various states. Developed a training package for supporting WHO PEN implementation for WHO HQ Geneva. Was part of a mission to part of a WHO mission to Eswatini, Africa to provide technical support to adapt the WHO-PEN and train health workers in 2018. Also developed patient education materials and job aids for NCDs for WHO South East Regional Office 2018- 2019. Developed resource materials for management of diabetes for WHO HQ.
Part of the AIIMS Technical Support Unit for mortality surveillance program and development of an online coding platform called MINErVA ( Mortality in INdia Established thRough Verbal Autopsies) which is a collaboration between AIIMS and the office of the Registrar General of India.
Non communicable diseases, cancer prevention and control.
Medical Education – was involved in revising undergraduate and post graduate curriculum by Medical Council of India in 2009.
Urban health
Ocular microbiology Section
Dr R P Centre, AIIMS, New Delhi
Services Provided
Ocular Microbiology section at Dr. RP Centre is involved in diagnosis of ocular infections, infection control at the centre, graduate and post graduate teaching and state of the art research.
The diagnostic facilities at the section are in compliance with international standards, and turnaround time is maintained at all times. On an average, 25000 clinical cases are diagnosed in the section per year. Various modalities of diagnosis and research being used in the section are:
The section is actively involved in hospital infection control in which we take care of
Additionally, The section in-charge is the Nodal Officer of the centre for COVID-19 and member secretary of COVID-19 Committee of the centre. Physical and online training of health care workers, making of educational videos for the monitors of the centre, contact tracing; evaluation of PPE; surveillance of use of PPE and infection control measures; making COVID-19 control SOPs, posters and displays; ensuring disinfection of patient care areas and minimizing transmission in the centre; smooth isolation/quarantine and joining of healthcare workers; commencement and functioning of COVID-19 sample collection kiosk; and channelizing of testing of patients and healthcare workers are amongst the important COVID-19 responsibilities shouldered.
Unit Faculty Names & Designations:
Services Provided (Add photos)
Ocular Infections are diagnosed in minimum turnaround time using international standards

Infection Prevention and Control is integral part of Ocular Microbiology Services

Molecular Pharmacology: definition and determination of important pharmaco-kinetic parameters and pharmaco-dynamic parameters, pharmacokinetic basis of individual difference in response to drugs, pharmacokinetic properties, pharmacopore identification, influence of structural modifications on pharmacokinetic properties, mode of action of drugs, quantitative structure activity relationship, present and future aids to drug design, structure and confirmation of drugs and receptors, drug receptor binding forces, structural aspects of drug-nucleic acid interactions
Peptides-design, synthesis and applications: introduction to peptides, peptide design, synthesis of peptides (solution phase and solid phase), protection and deprotection of amino and carboxyl group, unnatural amino acids, conformation of peptides, purification and crystallization of peptides, determination of structure of small molecules (briefly), application of peptides
Biomechanics: Basic concepts of fluid dynamics, Bernoulli equation and its applications, streamline flow, Reynolds number, viscous flow, effects of gravity and external acceleration on circulation
Biostatistics: mean, median, mode, dispersion, standard deviation, correlation and regression, T-Test, chi-square test, F-test, ANOVA, how to enter data, edit and transform data, descriptive statistics ie. how to calculate mean, SD, range etc., frequency distribution, hypothesis tests for means and proportions, ANOVA, scatter plot, correlation matrix, regression, probability distribution.
Bioinformatics: Introduction, repositories, databases, pairwise sequence based alignment, relationship between sequence and structures, structural bioinformatics, genomics, proteomics, human genome project, software packages
Clinical proteomics
Spectroscopic techniques: Introduction to spectroscopy, basic principles, instrumentation and applications of UV-VIS absorption, infrared, Raman, atomic absorption, fluorescence, Circular dichroism, Laser spectroscopy, nuclear magnetic resonance, electron spin resonance, acoustic spectroscopy; solvent perturbation; difference spectroscopy; Fourier transform techniques; applications of Laser; mass spectroscopy.
Elementary crystallography: Introduction to crystallography, symmetry in crystals, lattices and unit cells, crystal systems, Bravais lattices, elements of symmetry- rotation axis, mirror planes and center of inversion, point group symmetry- monoaxial point groups, polyaxial point groups, translational symmetry- screw axis and glide planes, space group, equivalent points, X-ray diffraction and Bragg’s equation
X-ray diffraction methods: Scattering factor, structure factor expression, reciprocal lattice, Ewald’s sphere, electron density equation, phase problem, Patterson function, molecular replacement method, isomorphous replacement, refinement programs and interpretation of results, methods of data collection of crystal containing small molecule and large molecule, factors affecting the measurement of integrated intensities, photographic methods, diffractometers, area detectors and image plates.
Separation techniques: Basic principles and applications of electrophoresis-types of electrophoresis, estimation of molecular weight of proteins by logirthmic method; basic principles and applications of centrifugation-sedimentation, estimation of sedimentation rate by sedimentation velocity method and equilibrium method; basic principles and applications of chromatography-capacity factor of the gel, Kd value, α value.
Molecular modeling: Basic principle of modeling, modeling by energy minimization technique, concept of rotation about bonds, energy minimization by basic technique for small molecules, Ramachandran plot, torsional space minimization, energy minimization in cartesian space, molecular mechanics-basic principle, molecular dynamics basic principles
Cell biology: Organization and structure of prokaryotes and eukaryotes, nucleus, cytoplasm, plasma membrane, mitochondria-structure, function respiratory chain and ATP synthesis, endoplasmic reticulum, golgi apparatus, membranes, ribosomes, peroxisomes, lysozomes, transcription and translation, transport of proteins, cancer and its molecular genetics, oncogenes, tumor suppression gene
Molecular biology: central dogma, genetic code, gene and operon, structure of DNA and RNA, plasmids, selectable markers, agarose gel, PCR, Cloning PCR products, expression vectors, cell free translation, c- DNA libraries, genomic libraries, DNA micro arrays, DNA sequencing
Proteins, purification, structure and function: twenty amino acids: structure and function, the peptide bond, primary structure of a protein: methods of sequence determination, forces determining protein structure, secondary structure of a protein: β strands, β sheets (parallel and anti parallel), β turns, α helix, 310 helix and π helix (differences), tertiary structure of a protein: protein folds-all α helix motifs (Lone helix, helix-turn-helix, four helix bundle and eight helix bundle), protein folds-all β sheet motifs (β sandwich, β barrel, greek Key topology and β propellars), protein folds- α / β motifs (Tim barrel, Rosman fold, α/β horseshoe), quaternary structure of a protein: macromolecular assemblies, domains and domain swapping, membrane proteins, purification methods, studies of proteins with MALDI-TOF, enzymes and enzyme kinetics, G-proteins and G-protein coupled receptors(GPCRs), proteins as targets for rational structure based drug design
Principles of nucleic acid structure: nucleotide structure and properties: introduction to DNA, RNA, bases, sugars, phosphates, structure of nucleotide, nucleosides and polynucleotides and their nomenclature scheme. tautomerisation and ionization. genetic code. stereochemistry: nucleoside, torsion angles, sugar conformation, NMR study, DNA structure: different types of DNA and their structure, DNA motifs, DNA repeats and their significance, function and stability, spectroscpic study of DNA: dye binding, interaction, denaturation, and renaturation of DNA, thermal denaturation and Tm value, RNA: structure and properties, different forms of RNA and their significance, alkaline hydrolysis of RNA, how it differs from DNA, role of 2’OH group, structure of phenylalanine tRNA, enzymes involved in molecular biology: DNA polymerase, RNA polymerase, reverse transcriptase, restriction endonuclease. DNA interaction: protein, dye, drugs and carcinogens, DNA replication: DNA polymerization, mutation, and DNA repair, DNA transcription: RNA synthesis, types of RNA polymerase, DNA polymorphism: repeats of DNA and their significance, single nucleotide polymorphism, c-DNA, cloning and expression and purification
Membrane biology: Lipid structure and their organization, comparison of different membrane models, diffusions and permeability, different types of transport system across membranes, liposome and its applications
Imaging techniques: Ultrasound, nuclear magnetic resonance, positron emission topography, computer axial tomography, whole body scanner, dose calibrators, gamma scintillation camera, digital imaging techniques, acquisition, analysis and processing of data from gamma camera, enhancement, topographic reconstruction, display and recording of image
Radiation biophysics: production and types of radiations, radiation measurement units, interaction of radiation with matter, detection of radiation by ionization chamber, G.M counter, proportional counter, liquid scintillation counter, radiation protection, molecular effects of radiation on membranes, cytoplasmic organelles, macromolecules, factors modifying effects of radiation, repairs of radiation induced damage
Radio pharmaceuticals: Production of radionuclides by reactors, cyclotrons and particle accelerators, use of radionuclide generators, elements of radiochemistry
Diagnostic use of radionuclides: In vivo imaging and functional studiesof brain, thyroid, heart, biliary tract, liver, kidney, spleen, tumors, bones and abscesses, use of imaging devices and external detectors for organ imaging, time dependent and differential functional studies, use of physiological gating techniques for functional studies, methodology and quality control of competitive binding and radio immunoassay, procedures for the measurement of peptide hormones, drugs and other biological substances, basic principles of radionuclide therapy in thyrotoxicosis and carcinoma thyroid
Bioelectric potentials: Principles and interpretations of electro-encephalogram, electro-cardiogram and electro-retionogram
Dynamics of non-linear Processes: Physico-mathematical foundations of the dynamics of non-linear processes, phase plane method, different modes of excitations, nearly sinusoidal oscillations, building up of oscillations, effect of third harmonic distortion, Liapounov criteria of stability, limit cycles
| Name | Designation | Email ID |
|---|---|---|
| Dr. Neeti Makhija | Professor & HOD | neetimakhija[at]hotmail[dot]com |
| Dr. Sandeep Chauhan, CHIEF, CTC | Professor | sdeep61[at]yahoo[dot]com |
| Dr. Poonam Malhotra Kapoor | Professor | drpoonamaiims[at]gmail[dot]com |
| Dr. Minati Choudhury | Professor | minatichoudhury2002[at]yahoo[dot]co[dot]in |
| Dr. Sambhnath Das | Professor | drsdas.cnc[at]aiims[dot]edu |
| Dr. Parag Gharde | Professor | parag.gharde72[at]rediffmail[dot]com |
| Dr. Suruchi Hasija | Professor | suruchi_hasija[at]hotmail[dot]com |
| Dr. Arindam Choudhury | Professor | archy[at]aiims[dot]edu |
Molecular Pharmacology: definition and determination of important pharmaco-kinetic parameters and pharmaco-dynamic parameters, pharmacokinetic basis of individual difference in response to drugs, pharmacokinetic properties, pharmacopore identification, influence of structural modifications on pharmacokinetic properties, mode of action of drugs, quantitative structure activity relationship, present and future aids to drug design, structure and confirmation of drugs and receptors, drug receptor binding forces, structural aspects of drug-nucleic acid interactions
Peptides-design, synthesis and applications: introduction to peptides, peptide design, synthesis of peptides (solution phase and solid phase), protection and deprotection of amino and carboxyl group, unnatural amino acids, conformation of peptides, purification and crystallization of peptides, determination of structure of small molecules (briefly), application of peptides
Biomechanics: Basic concepts of fluid dynamics, Bernoulli equation and its applications, streamline flow, Reynolds number, viscous flow, effects of gravity and external acceleration on circulation
Biostatistics: mean, median, mode, dispersion, standard deviation, correlation and regression, T-Test, chi-square test, F-test, ANOVA, how to enter data, edit and transform data, descriptive statistics ie. how to calculate mean, SD, range etc., frequency distribution, hypothesis tests for means and proportions, ANOVA, scatter plot, correlation matrix, regression, probability distribution.
Bioinformatics: Introduction, repositories, databases, pairwise sequence based alignment, relationship between sequence and structures, structural bioinformatics, genomics, proteomics, human genome project, software packages
Clinical proteomics
Spectroscopic techniques: Introduction to spectroscopy, basic principles, instrumentation and applications of UV-VIS absorption, infrared, Raman, atomic absorption, fluorescence, Circular dichroism, Laser spectroscopy, nuclear magnetic resonance, electron spin resonance, acoustic spectroscopy; solvent perturbation; difference spectroscopy; Fourier transform techniques; applications of Laser; mass spectroscopy.
Elementary crystallography: Introduction to crystallography, symmetry in crystals, lattices and unit cells, crystal systems, Bravais lattices, elements of symmetry- rotation axis, mirror planes and center of inversion, point group symmetry- monoaxial point groups, polyaxial point groups, translational symmetry- screw axis and glide planes, space group, equivalent points, X-ray diffraction and Bragg’s equation
X-ray diffraction methods: Scattering factor, structure factor expression, reciprocal lattice, Ewald’s sphere, electron density equation, phase problem, Patterson function, molecular replacement method, isomorphous replacement, refinement programs and interpretation of results, methods of data collection of crystal containing small molecule and large molecule, factors affecting the measurement of integrated intensities, photographic methods, diffractometers, area detectors and image plates.
Separation techniques: Basic principles and applications of electrophoresis-types of electrophoresis, estimation of molecular weight of proteins by logirthmic method; basic principles and applications of centrifugation-sedimentation, estimation of sedimentation rate by sedimentation velocity method and equilibrium method; basic principles and applications of chromatography-capacity factor of the gel, Kd value, α value.
Molecular modeling: Basic principle of modeling, modeling by energy minimization technique, concept of rotation about bonds, energy minimization by basic technique for small molecules, Ramachandran plot, torsional space minimization, energy minimization in cartesian space, molecular mechanics-basic principle, molecular dynamics basic principles
Cell biology: Organization and structure of prokaryotes and eukaryotes, nucleus, cytoplasm, plasma membrane, mitochondria-structure, function respiratory chain and ATP synthesis, endoplasmic reticulum, golgi apparatus, membranes, ribosomes, peroxisomes, lysozomes, transcription and translation, transport of proteins, cancer and its molecular genetics, oncogenes, tumor suppression gene
Molecular biology: central dogma, genetic code, gene and operon, structure of DNA and RNA, plasmids, selectable markers, agarose gel, PCR, Cloning PCR products, expression vectors, cell free translation, c- DNA libraries, genomic libraries, DNA micro arrays, DNA sequencing
Proteins, purification, structure and function: twenty amino acids: structure and function, the peptide bond, primary structure of a protein: methods of sequence determination, forces determining protein structure, secondary structure of a protein: β strands, β sheets (parallel and anti parallel), β turns, α helix, 310 helix and π helix (differences), tertiary structure of a protein: protein folds-all α helix motifs (Lone helix, helix-turn-helix, four helix bundle and eight helix bundle), protein folds-all β sheet motifs (β sandwich, β barrel, greek Key topology and β propellars), protein folds- α / β motifs (Tim barrel, Rosman fold, α/β horseshoe), quaternary structure of a protein: macromolecular assemblies, domains and domain swapping, membrane proteins, purification methods, studies of proteins with MALDI-TOF, enzymes and enzyme kinetics, G-proteins and G-protein coupled receptors(GPCRs), proteins as targets for rational structure based drug design
Principles of nucleic acid structure: nucleotide structure and properties: introduction to DNA, RNA, bases, sugars, phosphates, structure of nucleotide, nucleosides and polynucleotides and their nomenclature scheme. tautomerisation and ionization. genetic code. stereochemistry: nucleoside, torsion angles, sugar conformation, NMR study, DNA structure: different types of DNA and their structure, DNA motifs, DNA repeats and their significance, function and stability, spectroscpic study of DNA: dye binding, interaction, denaturation, and renaturation of DNA, thermal denaturation and Tm value, RNA: structure and properties, different forms of RNA and their significance, alkaline hydrolysis of RNA, how it differs from DNA, role of 2’OH group, structure of phenylalanine tRNA, enzymes involved in molecular biology: DNA polymerase, RNA polymerase, reverse transcriptase, restriction endonuclease. DNA interaction: protein, dye, drugs and carcinogens, DNA replication: DNA polymerization, mutation, and DNA repair, DNA transcription: RNA synthesis, types of RNA polymerase, DNA polymorphism: repeats of DNA and their significance, single nucleotide polymorphism, c-DNA, cloning and expression and purification
Membrane biology: Lipid structure and their organization, comparison of different membrane models, diffusions and permeability, different types of transport system across membranes, liposome and its applications
Imaging techniques: Ultrasound, nuclear magnetic resonance, positron emission topography, computer axial tomography, whole body scanner, dose calibrators, gamma scintillation camera, digital imaging techniques, acquisition, analysis and processing of data from gamma camera, enhancement, topographic reconstruction, display and recording of image
Radiation biophysics: production and types of radiations, radiation measurement units, interaction of radiation with matter, detection of radiation by ionization chamber, G.M counter, proportional counter, liquid scintillation counter, radiation protection, molecular effects of radiation on membranes, cytoplasmic organelles, macromolecules, factors modifying effects of radiation, repairs of radiation induced damage
Radio pharmaceuticals: Production of radionuclides by reactors, cyclotrons and particle accelerators, use of radionuclide generators, elements of radiochemistry
Diagnostic use of radionuclides: In vivo imaging and functional studiesof brain, thyroid, heart, biliary tract, liver, kidney, spleen, tumors, bones and abscesses, use of imaging devices and external detectors for organ imaging, time dependent and differential functional studies, use of physiological gating techniques for functional studies, methodology and quality control of competitive binding and radio immunoassay, procedures for the measurement of peptide hormones, drugs and other biological substances, basic principles of radionuclide therapy in thyrotoxicosis and carcinoma thyroid
Bioelectric potentials: Principles and interpretations of electro-encephalogram, electro-cardiogram and electro-retionogram
Dynamics of non-linear Processes: Physico-mathematical foundations of the dynamics of non-linear processes, phase plane method, different modes of excitations, nearly sinusoidal oscillations, building up of oscillations, effect of third harmonic distortion, Liapounov criteria of stability, limit cycles
Additional Professor
Contact Address:
Room No. 33, Old OT Block,
Centre for Community Medicine, AIIMS, New Delhi
E-mail: drsumitaiims2012@gmail.com
Phone No: 011-26594125
Research Gate Link:https://www.researchgate.net/profile/Sumit_Malhotra2
PubMed Link:https://www.ncbi.nlm.nih.gov/pubmed/?term=sumit+malhotra
MBBS, Bangalore Medical College, Bangalore
MD (Community Medicine), AIIMS, New Delhi
DNB (Social and Preventive Medicine)
MSc (Clinical Trials), London School of Hygiene and Tropical Medicine
He served at Comprehensive Rural Health Services Project, Ballabgarh from 2014 to 2019. He has authored a book on Primary Health Care- Indian Scenario with support of World Health Organization- Country Office India and has several publications in National and International indexed peer reviewed journals. He has led health systems based projects evaluating performance of national health initiatives at district and block levels. He is also the nodal person for Innovation and Learning Centre and strengthening implementation of comprehensive primary health care in aspirational district Mewat of Haryana. With keen interest in teaching and training, has conducted and organized several trainings on research methods and monitoring and evaluation. He is currently the nodal person for organizing trainings and workshops on Operational Research as part of Department of Health Research Scheme for Human Resource Development. He has also designed along with team of personnel from World Health Organization, a course on programme management for district and block based programme managers involved in implementation of national health programmes. He is also currently part of AIIMS technical support unit on cause of death ascertainment through verbal autopsy systems and Anaemia Mukht Bharat at Centre for Community Medicine. He has contributed to several national public health programmes. As a faculty, he currently guides MD, PhD and MSc nursing students in public health, epidemiology and operational research projects.
Operational and health systems research, community based interventional trials, adolescent and school health, chronic care including mental health, primary health care, sexual and reproductive health, neonatal health, health literacy.

Designation:Additional Professor
Phone No (Office): 011-26594020
E-mail:drrkaur@aiims.edu
Educational Qualification: MBBS, MD (Community Medicine)
Work Experience
Areas of interest: Maternal and child health, MIYCN, Anemia, Quality Improvement, Medical education, Qualitative Research, Geriatric health
| Name | Designation | Contact Number | |
|---|---|---|---|
| Prof T P Singh | SERB Distinguished Fellow | tpsingh[dot]aiims[at]gmail[dot]com | 26588931 |
| Prof Punit Kaur | Professor & Head of Department | punitkaur1[at]hotmail[dot]com | 26594288, 26593201 |
| Prof Savita Yadav | Professor | savitayadav[at]aiims[dot]edu | 26594608 |
| Prof Sujata Sharma | Professor | sujatasharma[at]aiims[dot]edu | 26594608 |
| Dr Sharmistha Dey | Professor | sharmistha_d[at]hotmail[dot]com | 26593201 |
| Dr Hariprasad G | Professor | g[dot]hariprasad[at]rediffmail[dot]com, dr[dot]hariprasadg[at]gmail[dot]com | 26594240 |
| Dr. Ethayathulla Abdul Samath | Additional Professor | ethayathulla[at]aiims.edu | 26593351 |
| Dr Krishna Kishore Inampudi | Additional Professor | kishorehcu[at]gmail[dot]com, krishna[dot]inampudi[at]aiims[dot]edu | 26584816 |
| Dr. Saroj Kumar | Additional Professor | sarojgupta[dot]k[at]gmail[dot]com | 26594240 |
| Dr. Jyotirmoy Banerjee | Additional Professor | jyotirmoybanerjee1[at]gmail[dot]com, Jyotirmoy[at]aiims[dot]edu | 26549324 |
| Dr Pradeep Sharma | Associate Professor | pradeepbdk[at]gmail[dot]com, pradeep[at]aiims[dot]edu | 26594608 |
| Ms. Asha Bhushan | Scientist-IV | 26594608 | |
| Dr. S. Baskar Singh | Scientist-IV | baskaraiims[at]hotmail[dot]com baskaraiims[at]gmail[dot]com | 26594925 |
| Dr. Manoj Kumar | Scientist-II | manmath[dot]manoj[at]gmail[dot]commkrai[at]aiims[dot]edu | 26594816 |
| Dr. Uddipan Das | Scientist-I | uddipan[dot]das[at]aiims[dot]edu | 26594259 |
| Photograph |  |
| Current Designation & Contact Details | Professor Room No. 11, 5th Floor, Porta Cabin, Teaching Block, AIIMS, New Delhi Email Id: dr.hariprasadg@gmail.com Phone: +91-11-26594029 |
| Recent Employment Details (Past few years) |
|
| Brief Research Area |
|
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.co.in/citations?user=_c0LXmkAAAAJ&hl=en
|
Leishmania donovani PAFAH with D1 Trypanosoma cruzi PAFAH with C1 |
| Photograph | |
| Current Designation & Contact Details | Professor Room No. 11, 5th Floor, Porta Cabin, Teaching Block, AIIMS, New Delhi Email Id: dr.hariprasadg@gmail.com Phone: +91-11-26594029 |
| Recent Employment Details (Past few years) |
|
| Brief Research Area |
|
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.co.in/citations?user=_c0LXmkAAAAJ&hl=en
|
Leishmania donovani PAFAH with D1 Trypanosoma cruzi PAFAH with C1 |
| Name | Designation | Contact Number | |
|---|---|---|---|
| Prof T P Singh | SERB Distinguished Fellow | tpsingh[dot]aiims[at]gmail[dot]com | 26588931 |
| Prof Punit Kaur | Professor & Head of Department | punitkaur1[at]hotmail[dot]com | 26594288, 26593201 |
| Prof Savita Yadav | Professor | savitayadav[at]aiims[dot]edu | 26594608 |
| Prof Sujata Sharma | Professor | sujatasharma[at]aiims[dot]edu | 26594608 |
| Dr Sharmistha Dey | Professor | sharmistha_d[at]hotmail[dot]com | 26593201 |
| Dr Hariprasad G | Professor | g[dot]hariprasad[at]rediffmail[dot]com, dr[dot]hariprasadg[at]gmail[dot]com | 26594240 |
| Dr. Ethayathulla Abdul Samath | Additional Professor | ethayathulla[at]aiims.edu | 26593351 |
| Dr Krishna Kishore Inampudi | Additional Professor | kishorehcu[at]gmail[dot]com, krishna[dot]inampudi[at]aiims[dot]edu | 26584816 |
| Dr. Saroj Kumar | Additional Professor | sarojgupta[dot]k[at]gmail[dot]com | 26594240 |
| Dr. Jyotirmoy Banerjee | Additional Professor | jyotirmoybanerjee1[at]gmail[dot]com, Jyotirmoy[at]aiims[dot]edu | 26549324 |
| Dr Pradeep Sharma | Associate Professor | pradeepbdk[at]gmail[dot]com, pradeep[at]aiims[dot]edu | 26594608 |
| Ms. Asha Bhushan | Scientist-IV | 26594608 | |
| Dr. S. Baskar Singh | Scientist-IV | baskaraiims[at]hotmail[dot]com baskaraiims[at]gmail[dot]com | 26594925 |
| Dr. Manoj Kumar | Scientist-II | manmath[dot]manoj[at]gmail[dot]com, mkrai[at]aiims[dot]edu | 26594816 |
| Dr. Uddipan Das | Scientist-I | uddipan[dot]das[at]aiims[dot]edu | 26594259 |
| Photograph |  |
| Current Designation & Contact Details | Scientist-I Department of Biophysics, Near Lecture Theater-2, PC Block, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110029 Phone (office): +91-11-26594259, Ext: 4259 Email: uddipan.das@aiims.edu |
| Recent Employment Details (Past few years) |
|
| Brief Research Area | Structural biology: We are interested in understanding the intricate structure and function of Membrane proteins and Macromolecular complexes. To accomplish this, we are harnessing the power of Cryo-Electron microscopy and X-ray crystallography along with other biophysical and biochemical methods in order to understand the structure function relationships. |
| Awards & Honours |
|
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?user=_YQkkBcAAAAJ&hl=en
|
| S.No. | Title | From | Upto |
|---|---|---|---|
| 1. | Purchase of Consumable items for patients on Two Year rate contract basis (M/s Boston Scientific India (P) Ltd.) | 26-04-2018 | 25-04-2020 |
| 2 | Purchase of Stent s for patients on Two Year rate contact basis(M/s Boston Scientific India (P) Ltd.) | 16-05-2018 | 15-05-2020 |
| 3. | Purchase of Stents for patients on two years rate contract basis (M/s Kox Med Lab (P) Ltd). | 16-05-2018 | 15-05-2020 |
| 4. | Purchase of Stents for patients on two years rate contract basis (M/s Biotronik Medical Devices (I) (P) Ltd). | 16-05-2018 | 15-05-2020 |
| 5 | Purchase of Stents for patients on Two Year rate ontract basis (M/s Relisys Meditech) | 16-05-2018 | 15-05-2020 |
| 6. | Purchase of Stents for patients on Two Year rate ontract basis ( M/s Shalyaa International) | 16-05-2018 | 15-05-2020 |
| 7 | Purchase of Stents for patients on Two Year rate ontract basis (M/s Sahajanand Laser) | 16-05-2018 | 15-05-2020 |
| 8. | Purchase of Stents for patients on Two Year rate ontract basis (M/s Sahajanand Medical Technologies (P) Ltd.) | 16-05-2018 | 15-05-2020 |
| 9 | Purchase of Stents for patients on Two Year rate ontract basis ( M/s Gauri International) | 16-05-2018 | 15-05-2020 |
| 10 | Purchase of Stents for patients on Two Year rate ontract basis (M/s Boston Scientific India (P) Ltd.) | 16-05-2018 | 15-05-2020 |
| 11. | Purchase of Stents for patients on Two Year rate ontract basis (M/s Integris Health) | 16-05-2020 | 15-05-2020 |
| 12 | Purchase of Stents for patients on Two Year rate ontract basis (M/s Kox Med & Lab (P) Ltd.) | 16-05-2018 | 15-05-2020 |
| 13. | Purchase of Stents for patients on Two Year rate ontract basis (M/s Sahajanand Medical Technologies (P) Ltd.) | 16-05-2018 | 15-05-2020 |
| 14. | Purchase of Stents for patients on Two Year rate ontract basis (M/s Vascular Access solutions) | 16-05-2018 | 15-05-2020 |
| 15 | Purchase of Pacemakers & Devices for patients on two years rate contract basis (M/s Shree Pacetronix Ltd.) | 29-12-2017 | 28-12-2019 |
| 16 | Purchase of pacemakers & Devices for patients on two years contract basis (M/s Boston Scientific (I) Pvt. Ltd). | 29-12-2017 | 28-12-2019 |
| 17 | Purchase of pacemakers & Devices for patients on two years contract basis (Biotronik Medical Devices (I) Pvt. Ltd). | 07-08-2018 | 06-08-2020 |
| 18 | Purchase of Pacemakers & Devices for patients on two years rate contract basis (M/s Grace Mfg. & Trading Co.) | 29-12-2017 | 28-12-2018 |
| 19 | Purchase of Pacemakers & Devices for patients on two years rate contract basis (M/s St. Jude Medical) | 07-08-2018 | 06-08-2020 |
| 20 | Purchase of Pacemakers & Devices for patients on two years rate contract basis (M/s Grace Mfg. & Trading Co.) | 07-08-2018 | 06-08-2020 |
| 21 | Purchase of Consumable items for patients on two years rate contract basis (M/s Ace Cardiopathy Solution(P) Ltd.) | 01-05-2018 | 30-04-2020 |
| 22 | Purchase of Consumable items for patients on two years rate contract basis (M/s Bhagat Jee Sons) | 01-05-2018 | 30-04-2020 |
| 23 | Purchase of Consumable items for patients on two years rate contract basis (M/s Ace Medical) | 01-05-2018 | 30-04-2020 |
| 24 | Purchase of Consumable items for patients on two years rate contract basis (M/s Boston Scientific India Pvt. Ltd.) | 01-05-2018 | 30-04-2020 |
| 25 | Purchase of Consumable items for patients on two years rate contract basis (M/s Emerging Electromedia L.L.P.) | 01-05-2018 | 30-04-2020 |
| 26 | Purchase of Consumable items for patients on two years rate contract basis (M/s Integris Health) | 01-05-2018 | 30-04-2020 |
| 27 | Purchase of Consumable items for patients on two years rate contract basis (M/s J. Mitra & Bros.) | 01-05-2018 | 30-04-2020 |
| 28 | Purchase of Consumable items for patients on two years rate contract basis (M/s Mediserve) | 01-05-2018 | 30-04-2020 |
| 29 | Purchase of Consumable items for patients on two years rate contract basis (M/s J. D. Medicare) | 01-05-2018 | 30-04-2020 |
| 30 | Purchase of Consumable items for patients on two years rate contract basis (M/s Kox Med & Lab (P)Ltd.) | 01-05-2018 | 30-04-2020 |
| 31 | Purchase of Consumable items for patients on two years rate contract basis (M/s Sanyog Enterprises Pvt. Ltd.) | 01-05-2018 | 30-04-2020 |
| 32 | Purchase of Consumable items for patients on two years rate contract basis (M/s Shi Mediware Pvt. Ltd.) | 01-05-2018 | 30-04-2020 |
| 33 | Purchase of Consumable items for patients on two years rate contract basis (M/s Teknoeurg International) | 01-05-2018 | 30-04-2020 |
| 34 | Purchase of Consumable items for patients on two years rate contract basis (M/s Ace Cardiopathy Sol.Pvt. Ltd.) | 15-05-2018 | 14-05-2020 |
| 35 | Purchase of Pacemakers Devices for patients on two years rate contract basis (M/s St. Jude Medical) | 22-03-2018 | 21-03-2020 |
| 36 | Purchase of pacemakers & Devices for patients on two years rate contract basis (M/s Biotronik Medical Devices (I) Pvt. Ltd.) | 29-12-2017 | 28-12-2019 |
| 37 | Purchase of Consumable items for patients on Two Years rate contract basis( M/s Bhagat Jee & Sons) | 15-05-2018 | 14-05-2020 |
| 38 | Purchase of Consumable items for patients on Two Years rate contract basis( M/s Boston Scientific India Pvt.Ltd.) | 15-05-2018 | 14-05-2020 |
| 39 | Purchase of Consumable items for patients on Two Years rate contract basis( M/s Curemed) | 15-05-2018 | 14-05-2020 |
| 40 | Purchase of Consumable items for patients on Two Year rate Contract basis ( M/s Emerging Eletromedia L.L.P.) | 15-05-2018 | 14-05-2020 |
| 41 | Purchase of Consumable items for patients on two year rate contract basis (M/s Gauri International) | 15-05-2018 | 14-05-2018 |
| 42 | Purchase of Consumable items for patients on two year rate Contract basis ( Ms/ Intergris Health) | 15-05-2018 | 14-05-2018 |
| 43 | Purchase of Consumable items for pateints on two year rate Contract basis ( M/s J.D. Medicare) | 15-05-2018 | 14-05-2018 |
| Photograph | |
| Current Designation & Contact Details | Scientist-I Department of Biophysics, Near Lecture Theater-2, PC Block, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110029 Phone (office): +91-11-26594259, Ext: 4259 Email: uddipan[dot]das[at]aiims[dot]edu |
| Recent Employment Details (Past few years) |
|
| Brief Research Area | Structural biology: We are interested in understanding the intricate structure and function of Membrane proteins and Macromolecular complexes. To accomplish this, we are harnessing the power of Cryo-Electron microscopy and X-ray crystallography along with other biophysical and biochemical methods in order to understand the structure function relationships. |
| Awards & Honours |
|
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?user=_YQkkBcAAAAJ&hl=en
|
| Photograph |  |
| Current Designation & Contact Details | Scientist II Room No. 1008, Department of Biophysics, All India Institute of Medical Sciences, New Delhi, India Tel: +91-11-26594816 Email: mkrai[at]aiims[dot]edu; manmath[dot]manoj[at]gmail[dot]com |
| Recent Employment Details (Past few years) |
|
| Brief Research Area | I am working in the area of drug discovery for tuberculosis using rational drug design approach. My goal is to design lead molecules for treatment of drug-resistant tuberculosis. I am also working on design of lead molecules for development of drugs to shorten the treatment duration. |
| Selected Publications/Patents (Last 5 years) | Google Scholar link: https://scholar.google.com/citations?user=wezA8UgAAAAJ&hl=en
|
| Photograph | |
| Current Designation & Contact Details | Scientist II Room No. 1008, Department of Biophysics, All India Institute of Medical Sciences, New Delhi, India Tel: +91-11-26594816 Email: mkrai[at]aiims[dot]edu; manmath[dot]manoj[at]gmail[dot]com |
| Recent Employment Details (Past few years) |
|
| Brief Research Area | I am working in the area of drug discovery for tuberculosis using rational drug design approach. My goal is to design lead molecules for treatment of drug-resistant tuberculosis. I am also working on design of lead molecules for development of drugs to shorten the treatment duration. |
| Selected Publications/Patents (Last 5 years) | Google Scholar link: https://scholar.google.com/citations?user=wezA8UgAAAAJ&hl=en
|
| Photograph |  |
| Current Designation & Contact Details | Scientist-IV Contact: 26594259 (O), 9810492147 (M) Email: baskaraiims[at]hotmail[dot]com, baskaraiims[at]gmail[dot]com |
| Recent Employment Details (Past few years) | Scientist-IV (From July, 2007 to till date) |
| Brief Research Area | At present we are working on Comparative proteomics analysis to identify potent biomarkers during the transformation of premalignant oral conditions to malignant oral squamous cell carcinoma. Besides we are working on cloning, expression of various nucleoside transporters and their role in drug transport in to ocular tissues. (Collaboration with Prof. T. Velpandian, Department of Ocular Pharmacology, Dr. R.P. Centre, AIIMS). |
| Awards & Honours |
|
| Selected Publications/Patents (Last 5 years) |
|
| Photograph | |
| Current Designation & Contact Details | Scientist-IV Contact: 26594259 (O), 9810492147 (M) Email: baskaraiims[at]hotmail[dot]com, baskaraiims[at]gmail[dot]com |
| Recent Employment Details (Past few years) | Scientist-IV (From July, 2007 to till date) |
| Brief Research Area | At present we are working on Comparative proteomics analysis to identify potent biomarkers during the transformation of premalignant oral conditions to malignant oral squamous cell carcinoma. Besides we are working on cloning, expression of various nucleoside transporters and their role in drug transport in to ocular tissues. (Collaboration with Prof. T. Velpandian, Department of Ocular Pharmacology, Dr. R.P. Centre, AIIMS). |
| Awards & Honours |
|
| Selected Publications/Patents (Last 5 years) |
|

| Designation | Scientist-IV |
| agautam[at]aiims[dot]ac[dot]in, ashaykb[at]yahoo[dot]com | |
| Contact Number | +91-11-26594608, +91-11-26593201 |
| Research Interests | Protein Structure Determination ; Data Collection and processing on High intensity X-Ray Beam, Cryocooling: Drug Design |
| Awards | Life Member of Indian Biophysical Society |
| Life Member of Indian Crystallographic Association | |
| Life member of International Union of crystallography | |
| Member of Asian Biophysical Society | |
| Board Member of IJBST and its associated Journals http://ijbst.org | |
| Selected for attending "The XIX IUCr Congress and General Assembly in Geneva” 2002 | |
| The Outstanding scientist of the 21st century award by International Biographical Centre, Cambridge in 2007 | |
| Bursary for the 9th International conference on Biology and Synchrotron radiation from 13-17 August 2007 | |
| Invited by Prof. Kyriacos Petratos for structure determination (BIOXIT) course in crystallography i | |
| Selected for attending the CCP4 study weekend, 2010, East Midland, England. | |
| Honored with “Bharat Jyoti Award” in the seminar “Economic Growth & National Integration” by IIFS society on 26th March 2014 in New Delhi. | |
| Selected as the outstanding scientist of the 21st century award by International Biographical Centre, Cambridge, England.; 2009 | |
Recent Significant Publications
| Singh A, Gautam L, Sinha M, Bhushan A, Kaur P, Sharma S, Singh TP. Crystal structure of peptidyl-tRNA hydrolase from a Gram-positive bacterium, Streptococcus pyogenes at 2.19 Å resolution shows the closed structure of the substrate-binding cleft. FEBS Open Bio. 2014 Oct 22;4:915-22. |
| Singh A, Kumar A, Gautam L, Sharma P, Sinha M, Bhushan A, Kaur P, Sharma S, Arora A, Singh TP. (2014) Structural and binding studies of peptidyl-tRNA hydrolase from Pseudomonas aeruginosa provide a platform for the structure-based inhibitor design against peptidyl-tRNA hydrolase. Biochem J. 463 : 329-37. | |
| Rastogi N, Singh A, Pandey SN, Sinha M, Bhushan A, Kaur P, Sharma S, Singh TP. (2014) Structure of the iron-free true C-terminal half of bovine lactoferrin produced by tryptic digestion and its functional significance in the gut. FEBS J. 281:2871-82. | |
| Kumar S, Singh N, Sinha M, Dube D, Singh SB, Bhushan A, Kaur P, Srinivasan A, Sharma S, Singh TP.(2010): Crystal structure determination and inhibition studies of a novel xylanase and alpha-amylase inhibitor protein (XAIP) from Scadoxus multiflorus. FEBS J.: 277(13):2868-82. | |
| Mir, R., Singh, N., Vikram, G., Sinha, M., Bhushan, A., Kaur, P., Srinivasan, A., Sharma, S. & Singh, T.P. (2010). Structural and binding studies of C-terminal half (C-lobe) of lactoferrin protein with COX-2-specific non-steroidal anti-inflammatory Drugs (NSAIDs). Arch. Biochem. Biophy. 500 , 196 - 202 | |
| Mir R, Kumar RP, Singh N, Vikram GP, Sinha M, Bhushan A, Kaur P, Srinivasan A, Sharma S, Singh TP. (2010). Specific interactions of C-terminal half (C-lobe) of lactoferrin protein with edible sugars: binding and structural studies with implications on diabetes. Int J Biol Macromol.47, 50-9. | |
| Sheikh, I.A., Singh, A.K., Singh, N., Sinha, M., Singh, S.B., Bhushan, A., Kaur, P., Srinivasan, A., Sharma, S. & Singh, T.P. (2009). Structural evidence of substrate specificity in mammalian peroxidases: Structure of the thiocyanate complex with lactoperoxidase and its interactions at 2.4A resolution. J. Biol. Chem. 284, 14849 - 14856. . | |
| Singh, A.K., Kumar, R.P., Pandey, N., Singh, N., Sinha, M., Bhushan, A.,Kaur, P., Sharma, S. & Singh, T.P. (2009). Mode of binding of the tuberculosis prodrug isoniazid to peroxidases: Crystal structure of bovine lactoperoxidase with isoniazid at 2.7A resolution. J. Biol. Chem. 285 , 1569 - 1576 | |
| Mir, R., Singh, N., Vikram, G., Kumar, R.P., Sinha, M., Bhushan, A., Kaur, P., Srinivasan, A., Sharma, S. & Singh, T.P. (2009)). Structural basis of the prevention NSAID-induced damage of the gastrointestinal tract by C-terminal half (C-lobe) of bovine colostrums protein lactoferrin: Binding andstructural studies of the C-lobe complexes with indomethacin, diclofenac, aspirin and ibuprofen. Biophys. J. 97, 3178 – 3186 | |
| Singh, R.K., Ethayathulla, A.S., Jabeen, T., Sharma, S., Kaur, P. & Singh, T.P. (2005) . Aspirin induces its anti-inflammatory effects through its specific binding to phospholipase A2 : Crystal structure of the complex formed between phospholipase A2 and aspirin at 1.9 Å resolution. J. Drug Target. 13 , 113 – 119. |
| Designation | Scientist-IV |
| agautam[at]aiims[dot]ac[dot]in, ashaykb[at]yahoo[dot]com | |
| Contact Number | +91-11-26594608, +91-11-26593201 |
| Research Interests | Protein Structure Determination ; Data Collection and processing on High intensity X-Ray Beam, Cryocooling: Drug Design |
| Awards | Life Member of Indian Biophysical Society |
| Life Member of Indian Crystallographic Association | |
| Life member of International Union of crystallography | |
| Member of Asian Biophysical Society | |
| Board Member of IJBST and its associated Journals http://ijbst.org | |
| Selected for attending "The XIX IUCr Congress and General Assembly in Geneva” 2002 | |
| The Outstanding scientist of the 21st century award by International Biographical Centre, Cambridge in 2007 | |
| Bursary for the 9th International conference on Biology and Synchrotron radiation from 13-17 August 2007 | |
| Invited by Prof. Kyriacos Petratos for structure determination (BIOXIT) course in crystallography i | |
| Selected for attending the CCP4 study weekend, 2010, East Midland, England. | |
| Honored with “Bharat Jyoti Award” in the seminar “Economic Growth & National Integration” by IIFS society on 26th March 2014 in New Delhi. | |
| Selected as the outstanding scientist of the 21st century award by International Biographical Centre, Cambridge, England.; 2009 | |
Recent Significant Publications
| Singh A, Gautam L, Sinha M, Bhushan A, Kaur P, Sharma S, Singh TP. Crystal structure of peptidyl-tRNA hydrolase from a Gram-positive bacterium, Streptococcus pyogenes at 2.19 Å resolution shows the closed structure of the substrate-binding cleft. FEBS Open Bio. 2014 Oct 22;4:915-22. |
| Singh A, Kumar A, Gautam L, Sharma P, Sinha M, Bhushan A, Kaur P, Sharma S, Arora A, Singh TP. (2014) Structural and binding studies of peptidyl-tRNA hydrolase from Pseudomonas aeruginosa provide a platform for the structure-based inhibitor design against peptidyl-tRNA hydrolase. Biochem J. 463 : 329-37. | |
| Rastogi N, Singh A, Pandey SN, Sinha M, Bhushan A, Kaur P, Sharma S, Singh TP. (2014) Structure of the iron-free true C-terminal half of bovine lactoferrin produced by tryptic digestion and its functional significance in the gut. FEBS J. 281:2871-82. | |
| Kumar S, Singh N, Sinha M, Dube D, Singh SB, Bhushan A, Kaur P, Srinivasan A, Sharma S, Singh TP.(2010): Crystal structure determination and inhibition studies of a novel xylanase and alpha-amylase inhibitor protein (XAIP) from Scadoxus multiflorus. FEBS J.: 277(13):2868-82. | |
| Mir, R., Singh, N., Vikram, G., Sinha, M., Bhushan, A., Kaur, P., Srinivasan, A., Sharma, S. & Singh, T.P. (2010). Structural and binding studies of C-terminal half (C-lobe) of lactoferrin protein with COX-2-specific non-steroidal anti-inflammatory Drugs (NSAIDs). Arch. Biochem. Biophy. 500 , 196 - 202 | |
| Mir R, Kumar RP, Singh N, Vikram GP, Sinha M, Bhushan A, Kaur P, Srinivasan A, Sharma S, Singh TP. (2010). Specific interactions of C-terminal half (C-lobe) of lactoferrin protein with edible sugars: binding and structural studies with implications on diabetes. Int J Biol Macromol.47, 50-9. | |
| Sheikh, I.A., Singh, A.K., Singh, N., Sinha, M., Singh, S.B., Bhushan, A., Kaur, P., Srinivasan, A., Sharma, S. & Singh, T.P. (2009). Structural evidence of substrate specificity in mammalian peroxidases: Structure of the thiocyanate complex with lactoperoxidase and its interactions at 2.4A resolution. J. Biol. Chem. 284, 14849 - 14856. . | |
| Singh, A.K., Kumar, R.P., Pandey, N., Singh, N., Sinha, M., Bhushan, A.,Kaur, P., Sharma, S. & Singh, T.P. (2009). Mode of binding of the tuberculosis prodrug isoniazid to peroxidases: Crystal structure of bovine lactoperoxidase with isoniazid at 2.7A resolution. J. Biol. Chem. 285 , 1569 - 1576 | |
| Mir, R., Singh, N., Vikram, G., Kumar, R.P., Sinha, M., Bhushan, A., Kaur, P., Srinivasan, A., Sharma, S. & Singh, T.P. (2009)). Structural basis of the prevention NSAID-induced damage of the gastrointestinal tract by C-terminal half (C-lobe) of bovine colostrums protein lactoferrin: Binding andstructural studies of the C-lobe complexes with indomethacin, diclofenac, aspirin and ibuprofen. Biophys. J. 97, 3178 – 3186 | |
| Singh, R.K., Ethayathulla, A.S., Jabeen, T., Sharma, S., Kaur, P. & Singh, T.P. (2005) . Aspirin induces its anti-inflammatory effects through its specific binding to phospholipase A2 : Crystal structure of the complex formed between phospholipase A2 and aspirin at 1.9 Å resolution. J. Drug Target. 13 , 113 – 119. |
| Photograph |  |
| Current Designation & Contact Details | Assistant Professor Room No. 9, Department of Biophysics, AIIMS, New Delhi pradeepbdk[at]gmail[dot]com & pradeep[at]aiims[dot]edu
Phone: +91-11-26594608 |
| Brief Research Area | Antimicrobial therapeutics, Protein Structure based drug design, Nanomedicine. |
| Awards & Honours |
|
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?hl=en&user=h-T3UPYAAAAJ
|
| Photograph | |
| Current Designation & Contact Details | Assistant Professor Room No. 9, Department of Biophysics, AIIMS, New Delhi pradeepbdk[at]gmail[dot]com & pradeep[at]aiims[dot]edu Phone: +91-11-26594608 |
| Brief Research Area | Antimicrobial therapeutics, Protein Structure based drug design, Nanomedicine. |
| Awards & Honours |
|
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?hl=en&user=h-T3UPYAAAAJ
|
Medical Social Service Officer,
Dr.R.P.Centre for Ophathalmic Sciences,
Room No.114, First Floor, RPCOPD
mssudrrpcaiims[at]gmail[dot]com
| S.No. | Title | Year |
|---|---|---|
| 1 | Monthly Report | June- 2023 |
Dr. Kapil Yadav
Additional Professor
Centre for Community Medicine (CCM)
All India Institute of Medical Sciences (AIIMS), New Delhi
Dr. Kapil Yadav’s Laboratory Team
AIIMS, New Delhi Office Room Number: 37, 38 Center For Community Medicine, Old OT Block, All India Institute of Medical Sciences (AIIMS), Ansari Nagar, New Delhi - 110029, INDIA Phone- 26593848, 26593233 | Ballabhgarh Office Comprehensive Rural Health Services Project (CRHSP)AIIMS, Ballabgarh, Faridabad, Haryana - 121004, INDIA Phone- +91 129 2241362 |
Address for correspondence:
Email: dr_kapilyadav@yahoo.co.in, dr.kapilyadav@gmail.com, drkapilyadavoffice@gmail.com
web- http://www.aiims.edu/en/2014-11-24-12-23-25/faculty.html?id=768
Dr. Kapil Yadav is currently Additional Professor at Centre for Community Medicine, All India Institute of Medical Sciences (AIIMS), New Delhi, India.
He completed his MBBS from University College of Medical Science, New Delhi, and MD (Community Medicine) from All India Institute of Medical Sciences, New Delhi. Before joining AIIMS, he worked at Indian Coalition for Control of Iodine Deficiency Disorders (ICCIDD), New Delhi. Dr. Kapil Yadav joined All India Institute of Medical Sciences (AIIMS) in the year 2003 and have worked at AIIMS ever since, in various capacities.
Dr. Kapil has more than 150 research publications and he contributes regularly to chapters in books, curriculum/course material, and radio and television programs. Dr. Kapil is a technical expert for Anemia Mukt Bharat (AMB) Anemia Control Program and National Iodine Deficiency Disorders control program in India. Dr. Kapil has also been a consultant for the nutrition program in Sri Lanka, Myanmar, Democratic People’s Republic of Korea. He also worked with WHO, UNICEF, WFP, NI, GAIN, BMGF, PATH, FSSAI, and WCD.
Dr. Kapil has been a Principal investigator/ co-investigator of more than 60 research projects. He is the Principal Investigator for National Centre of Excellence and Advanced Research on Anemia Control (NCEAR-A). NCEAR-A is an institutional mechanism envisions to develop and provide technical support to the Ministry of Health and Family Welfare, Government of India, for incorporating scientific, policy and community perspectives in policy and programmatic decisions for control of anemia.
Dr. Kapil’s core area of interest includes Anemia, Iodine Deficiency Disorders, Micronutrient deficiencies, Public Health Nutrition, Food Fortification (salt/ milk), Medical Education, Pedagogy, Urban health, Social Determinants of Health, Health Policy, Epidemiology and Community-based research.
Dr. Kapil is the National Coordinator (India) for Iodine Global Network (IGN) formerly known as ICCIDD. He is a member of several committees constituted by Government of India and state governments in domain of anemia/nutrition, iodine deficiency disorders and public health.
Dr Kapil was awarded the Sri R N Roy award for best original research article by Indian Public Health Association in year 2010 and 2020. He was elected to the prestigious membership of National Academy of Medical Sciences, India in year 2014.
Dr. Kapil is an Editorial Board member, Indian Journal of Public Health, National Service Scheme (NSS), AIIMS, Unit. Dr. Kapil was also an Executive Council member, Indian Association of Preventive and Social Medicine.
Besides public health, Dr. Kapil has keen interest in history and social empowerment movements of marginalised groups. Dr. Kapil is also an avid reader, traveller and a fitness enthusiast.

Additional Professor
Room No. 11, 5th Floor,
Porta Cabin, Teaching Block
Department of Biophysics,
All India Institute of Medical Sciences (AIIMS), New Delhi, India
Tel: 91-11-26549324
e-mail: jyotirmoybanerjee1[at]gmail[dot]com
jyotirmoy[at]aiims[dot]edu
July 2023-Till Date
Additional Professor, Department of Biophysics, All India Institute of Medical Sciences (AIIMS), New Delhi, India.
July 2020-June 2023
Associate Professor, Department of Biophysics, All India Institute of Medical Sciences (AIIMS), New Delhi, India.
May 2017-June 2020
Assistant Professor, Department of Biophysics, All India Institute of Medical Sciences (AIIMS), New Delhi, India.
Cellular electrophysiological studies to understand function of ion channels of central nervous system and investigating regulation of synaptic transmission in drug-resistant epilepsy pathologies at cellular and molecular level.
Google scholar link: https://scholar.google.com/citations?user=81uRX7kAAAAJ&hl=en
1. Dubey V, Roy A, Dixit AB, Tripathi M, Pandey S, Jian S, Chandra PS, Banerjee J*. Dendritic reorganization in the hippocampus, anterior temporal lobe, and frontal neocortex of lithium-pilocarpine induced Status Epilepticus (SE). 2023, Journal of Chemical Neuroanatomy, 133: 102319. doi: 10.1016/j.jchemneu.2023.102329.
2. Kumar K, Dubey V, Zaidi SS, Tripathi M, Siraj F, Sharma MC, Chandra PS, Doddamani R, Dixit AB, Banerjee J*. RNA Sequencing of Intraoperative Peritumoral Tissues Reveals Potential Pathways Involved in Glioma-Related Seizures. 2023, Journal of Molecular Neuroscience, 73:437-447. doi: 10.1007/s12031-023-02125-y.
3. Dubey V, Dixit AB, Banerjee J*. Tempol Suppresses Generalized seizures in animal model of epilepsy. 2023, Neurology India, 71:412-413. doi: 10.4103/0028-3886.375411.
4. Sharma D, Tripathi M, Doddamani R, Sharma MC, Lalwani S, Chandra PS, Dixit AB, Banerjee J*. Correlation of Age at Seizure Onset with GABAA receptor subunit and Chloride Co-transporter configuration in Focal Cortical Dysplasia (FCD). 2023, Neuroscience Letters, 796: 137065. doi: 10.1016/j.neulet.2023.137065. (IF-3.1).
5. Chakraborty A, Dey S, Kumar K, Dixit AB, Tripathi M, Sharma MC, Chandra PS, Banerjee J*. Novel variants in GABAA receptor subunits: A possible association with benzodiazepine resistance in patients with drug-resistant epilepsy. 2023, Epilepsy Research, 189:107056. doi: 10.1016/j.eplepsyres.2022.107056.
6. Kumar K, Banerjee Dixit A, Tripathi M, Dubey V, Siraj F, Sharma MC, Lalwani S, Chandra PS, Banerjee J*. Transcriptomic profiling of nonneoplastic cortical tissues reveals epileptogenic mechanisms in dysembryoplastic neuroepithelial tumors. 2022, Functional & Integrative Genomics; 22:905-917. doi: 10.1007/s10142-022-00869-1.
7. Bera A, Srivastava A, Dubey V, Dixit AB, Tripathi M, Sharma MC, Lalwani S, Chandra PS, Banerjee J*. Altered hippocampal expression and function of cytosolic phospholipase A2 (cPLA2) in temporal lobe epilepsy (TLE). 2022, Neurological Research; 44: 748-753.doi: 10.1080/01616412.2022.2051131.
8. Dubey V, Dey S, Dixit AB, Tripathi M, Chandra PS, Banerjee J*. Differential glutamate receptor expression and function in the hippocampus, anterior temporal lobe and neocortex in a pilocarpine model of temporal lobe epilepsy. 2022, Experimental Neurology;347:113916. doi: 10.1016/j.expneurol.2021.113916.
9. Dey S, Banerjee Dixit A, Tripathi M, Doddamani RS, Sharma MC, Lalwani S, Chandra PS, Banerjee J*. Altered hippocampal kynurenine pathway metabolism contribute to hyperexcitability in human mesial temporal lobe epilepsy-hippocampal sclerosis. 2021, British Journal of Pharmacology; 178:3959-3976.doi: 10.1111/bph.15534.
10. Kumar S, Shanker OR, Kumari N, Tripathi M, Chandra PS, Dixit AB, Banerjee J*. Neuromodulatory effects of SARS-CoV2 infection: Possible therapeutic targets. 2021, Expert Opinion on Therapeutic Targets; 25:509-519.doi: 10.1080/14728222.2021.1953475.
11. Banerjee J, Srivastava A, Sharma D, Dey S, Tripathi M, Sharma MC, et al. Differential regulation of glutamatergic activity in the hippocampus and anterior temporal lobe by cyclin dependent kinase 5 (Cdk5) in mesial temporal lobe epilepsy with hippocampal sclerosis (MTLE-HS). 2021, Neuroscience Letters; 761: 136096. doi: 10.1016/j.neulet.2021.136096.
12. Dey S, Doddamani R, Dixit AB, Tripathi M, Sharma MC, Chandra PS, Banerjee J*. Altered spontaneous glutamatergic and GABAergic activity in the peritumoral cortex of low-grade gliomas presenting with history of seizures. 2021, Frontiers in Neuroscience; 15:689769. doi:10.3389/fnins.2021.689769
13. Sharma D, Dixit AB, Dey S, Tripathi M, Doddamani R, Sharma MC, Lalwani S, Gurjar HK, Chandra PS, Banerjee J*. Increased levels of α4-containing GABAA receptors in focal cortical dysplasia: A possible cause of benzodiazepine resistance. 2021, Neurochemistry International; 148:105084.doi: 10.1016/j.neuint.2021.105084
14.Banerjee J*, Dey S, Dixit AB, Doddamani R, Sharma MC, Garg A, et al. GABAA Receptor-Mediated Epileptogenicity in Focal Cortical Dysplasia (FCD) Depends on Age at Epilepsy Onset. 2020, Front Cell Neurosci; 14:562811.doi: 10.3389/fncel.2020.562811.
15. Banerjee J*, Dey S, Dixit AB, Tripathi M, Doddamani R, Sharma MC, et al. α7 nicotinic receptors contributes to glutamatergic activity in the hippocampus of patients with mesial temporal lobe epilepsy with hippocampal sclerosis (MTLE-HS). 2020, J Neural Transmission; 127:1441-1446.doi: 10.1007/s00702-020-02239-2.
16. Banerjee J, Tripathi M, Chandra PS, Dixit AB. Do SARS-CoV2 viral proteins have neuromodulatory properties? 2020, Neurol India; 68:274-275.doi: 10.4103/0028-3886.283760.
17. Srivastava A, Dixit AB, Paul D, Tripathi M, Sarkar C, Chandra PS, Banerjee J* (2017). Comparative analysis of cytokine/chemokine regulatory networks in patients with hippocampal sclerosis (HS) and focal cortical dysplasia (FCD). Scientific Reports, 7:15904.doi: 10.1038/s41598-017-16041-w.
18. Banerjee J*, Dixit AB, Srivastava A, Ramanujam B, Kakkar A, Sarkar C, Tripathi M & Chandra PS (2017). Altered glutamatergic tone reveals two distinct resting state networks at the cellular level in hippocampal sclerosis. Scientific Reports, 7:319.doi: 10.1038/s41598-017-00358-7.
Additional Professor
Room No. 11, 5th Floor,
Porta Cabin, Teaching Block
Department of Biophysics,
All India Institute of Medical Sciences (AIIMS), New Delhi, India
Tel: 91-11-26549324
e-mail: jyotirmoybanerjee1[at]gmail[dot]com
jyotirmoy[at]aiims[dot]edu
July 2023-Till Date
Additional Professor, Department of Biophysics, All India Institute of Medical Sciences (AIIMS), New Delhi, India.
July 2020-June 2023
Associate Professor, Department of Biophysics, All India Institute of Medical Sciences (AIIMS), New Delhi, India.
May 2017-June 2020
Assistant Professor, Department of Biophysics, All India Institute of Medical Sciences (AIIMS), New Delhi, India.
Cellular electrophysiological studies to understand function of ion channels of central nervous system and investigating regulation of synaptic transmission in drug-resistant epilepsy pathologies at cellular and molecular level.
Google scholar link: https://scholar.google.com/citations?user=81uRX7kAAAAJ&hl=en
In R.P.Centre all Medical Social Services are under one window system. MSSO is coordinating for financial assistance through Ayushman Bharat Pradhan Mantri Jan Arogya Yojana and Janani Shishu Surksha Karyakarm , Rashtriya Arogya Nidhi (RAN/NIAF),Prime Minister's Relief Fund, Health Minister's Discretionary Grant Fund and direct donations , and through requisition Performa for BPL/Poor Indigent patients
| Schemes Type | Schemes Name |
|---|---|
|
|
| |
| |
| |
| Medical Social Service Unit is facilitating for free medicines and Spectacles for poor and indigent outdoor (OPD) patients through Poor Patient's Fund of Centre. |
| If patient isn't eligible under any government scheme and the patient does not have a valid BPL Card/Low Income Certificate/in case of emergency, patient is helped through direct donation . |
| Medical Social Service Unit exempt the hospital charges manually and through e hospital management system based on the Socio-economic assessment. |
| Railway concession certificate is provided to cancer patients and 100% visually impaired patients as per Government norms to ensure the regular follow-up. |
| Year | Number of patients | Amount |
|---|---|---|
| Scheme started on 25th September 2018 | ||
| 2018-2019 | 172 | Rs.19,18,685/- |
| 2019-2020 | 1085 | Rs.1,23,19,350/- |
| 2020-2021 | 304 | Rs.49,08,406/- |
| 2021-2022 | 627 | Rs.68,63,635/- |
| 2022-2023 | 756 | Rs.1,69,88,059/- |
| Total | 2944 | Rs.4,29,98,135/-(Four crore twenty nine lacs ninety eight thousand one hundred thirty five only) |
Government of India has launched Janani Shishu Suraksha Karyakaram (JSSK) on 1st June, 2011 under the flagship of Ministry of health and Family Welfare (MOHFW).The Scheme is implemented in Dr.R.P.Centre in January ,2018 under The Ministry of Health and Family Welfare .In last two years total 1942 patients got benefit under the scheme.
| -- | -- |
|---|---|
| Key features of the Scheme |
|
| Things to remember in the implementation of JSSK |
|
| Year | Number of patients | Amount |
|---|---|---|
| 2018-2019 | 572 | Rs.61,74,205/- |
| 2019-2020 | 1369 | Rs.91,68,100/- |
| 2020-2021 | 667 | Rs.56,47,554 |
| 2021-2022 | 1244 | 6931629 |
| 2022-2023 | 1566 | 7684088 |
| Total | 5418 | Rs3,56,05,576(Three crores fifty six lac five thousand five hundred seventy six only) |
| Year | Number of patients | Amount in Rupees |
|---|---|---|
| 2017-2018 | 20 | Rs.8,68,640 |
| 2018-2019 | 08 | Rs.4,10,600 |
| 2019-2020 | 15 | Rs.18,56,350 |
| 2020-2021 | 11 | Rs.17,41,600 |
| 2021-2022 | Scheme is digitalised and merged under Umbrella Scheme now. | |
| 2022-2023 | 54 | Rs.48,77,190/-(Forty eight lac seventy seven thousand one hundred ninety ) |
| Year | Number of patients | Amount in Rupees |
|---|---|---|
| 2016-2017 | 66 | Rs.1,80,000 |
| 2017-2018 | 186 | Rs.13,39,905 |
| 2018-2019 | 343 | Rs.26,05,050 |
| 2019-2020 | 322 | Rs.22,02,215 |
| 2020-2021 | 96 | Rs.10,12,080 |
| 2021-2022 | 77 | Rs.7,37,433 |
| 2022-2023 | 129 | Rs.31,92,755 |
| Total | 1219 | Rs.1,12,69,438/-(One crore twelve lac sixty nine thousand four hundred thirty eight only) |
Medical Social Service Unit is facilitating for free medicines and Spectacles for poor and indigent outdoor (OPD) patients through Poor Patient's Fund of Centre.Donations for poor & indigent patients undergoing treatment at our centre can be made by Bank Draft/ Cheque drawn in favor of “POOR PATIENTS FUND ACCOUNT / Dr. R.P.Centre for Ophthalmic Sciences”. Donations made under this account are eligible for 100 % tax relief U/S 80G and 35 of the Income Tax Act, 1961vide order no. DIT (E) 2006-2007/A-240/1216 dated 31-08-2006 .
| Year | Number of patients | Amount | Number of patients | Amount in Rupees |
|---|---|---|---|---|
| Medicinal Assistance to OPD patients | Free Spectacles to OPD | |||
| 2016-2017 | 250 | Rs.1,25,900/- | 153 | Rs.71,614/- |
| 2017-2018 | 94 | Rs.45,388/- | 208 | Rs.88,764/- |
| 2018-2019 | 70 | Rs.53,615/- | 250 | Rs.1,22,230/- |
| 2019-2020 | 209 | Rs.1,60,541/- | 269 | Rs.1,40,838/- |
| 2020-2021 | 64 | Rs.53,812/- | 62 | Rs.32,628/- |
| 2021-2022 | 91 | Rs.71,006/- | 128 | Rs.74,961/- |
| 2022-2023 | 101 | Rs.74,598/- | 173 | Rs.1,10,502/- |
| Total | 879 | Rs.10,43,820/- | 1243 | Rs.6,41,537/- |
Medical Social Service Unit exempt the hospital charges manually and through e hospital management system based on the Socio-economic assessment.
| Year | Number of patients | Amount in Rupees |
|---|---|---|
| 2016-2017 | 356 | -- |
| 2017-2018 | 516 | Rs.2,86,063/- |
| 2018-2019 | 663 | Rs.5,25,915/- |
| 2019-2020 | 1380 | Rs.11,26,968/- |
| 2020-2021 | 314 | Rs.2,59,382/- |
| 2021-2022 | 636 | Rs.4,9,2764/- |
| 2022-2023 | 739 | Rs.7,07,117/- |
| 4604 | Rs.33,98,209/-(Thirty three lac ninety eight thousand two hundred and nine only) |
If patient isn't eligible under any government scheme and the patient does not have a valid BPL Card/Low Income Certificate then patient is helped through direct donation.
| Year | Number of patients | Amount in Rupees | |
|---|---|---|---|
| 2016-2017 | 57 | Rs.1,13,372 | |
| 2017-2018 | 49 | Rs.36,759 | |
| 2018-2019 | 30 | Rs.30,590 | |
| 2019-2020 | 22 | Rs.41,821 | |
| 2020-2021 | 03 | Rs.21,200 | |
| 2021-2022 | 18 | Rs.1,36,016 | |
| 2022-2023 | 38 | Rs2,17,082/- | |
| 217 | Rs.5,96,840/-(Five lac ninety six thousand eight hundred forty ) | ||
MSS Unit provides Railway Concession Certificates to the 100% visually disabled patients and Cancer patients for regular treatment follow up(as per government norms).In last 8 years MSS Unit provides railway concession certificates to 3517 patients.
| Year | Number of patients |
|---|---|
| 2016-2017 | 319 |
| 2017-2018 | 649 |
| 2018-2019 | 857 |
| 2019-2020 | 803 |
| 2020-2021 | 164 |
| 2021-2022 | 352 |
| 2022-2023 | 373 |
| Total | 3517 |
| Categories/Sources | Amount Received( in Rupees) |
|---|---|
| Donation received through Donation Boxes | Rs. 1,37,095/- |
| Donation received through various donors | Rs. 13,06,504 |
| Direct/Personal Donations | Rs. 2,17,082/- |
| Total Amount Received | Rs. 16,60,681 /- |
| S.No | Categories | Total Number of Cases | Total Amount |
|---|---|---|---|
| 1 | Free Medicines For Poor and Indigent Outdoor (OPD) Patients Through Poor Patient’s Fund | 101 | Rs.74,598/- |
| 2 | Free Spectacles Provided Through Poor Patients Fund | 173 | Rs.1,10,502/- |
| 3 | Free Surgeries through Consultations | 129 | Rs.3192755/- |
| 4 | Exemptions of Hospital and investigation Charges(IPD&OPD) | 739 | Rs.707117/- |
| 5 | Beneficiaries under Janani Shishu Surkshaa Karyakaram | 1566 | Rs.76,84,088/- |
| 6 | Beneficiaries under Ayushman Bharat-PMJAY | 756 | Rs.1,69,88,059/- |
| 7 | Patients helped through Direct Donations | 38 | Rs.2,17,082/- |
| 8 | RCC(Railway Concession Certificates Issued) | 373 (Permanent-101) (Temporary-272) | - |
| 9 | Counselling/ Ayushmaan Bharat Counselling/ Number of Patients guided and counselled for the benefits of Disability Certificate Issued/ Number of Patients counselled and guided for the benefits of different government schemes | 1628 | - |
| 9 | Total Number of patients helped through Medical Social Service Unit | 5503 | Rs. 2,89,74,201/- (Two Crore eighty Nine Lac seventy four Thousand Two Hundred and one only) |
| 10 | EHS (Coordination for EHS Patients ) | 823 | Rs.2,17,34,888/- |
Heart Valve Surgery (A Guide to Patients)
Prof.J.S.Titiyal

Dr.D.K.Sharma
Ms. Surinder Pal Kaur
Ms. Isha Goswami
“May I Help You Counter”(Part Time Social Guides-7)
| Name | Designation |
|---|---|
| Dr. Chetan D.Patal | Professor & Head |
| Name | Designation |
|---|---|
| Dr. Aarti Vi | Professor |
| Photograph |  |
| Current Designation & Contact Details | Additional Professor Room No: 3011, 3rd Floor, Teaching Block, Department of Biophysics, All India Institute of Medical Sciences, New Delhi - 110029 Phone: +91-11-26594240 (O) Email: sarojgupta[dot]k[at]gmail[dot]com Lab Website: www.skumarlab.com |
| Recent Employment Details (Past few years) |
|
| Brief Research Area | Dr Saroj has established the infrared-based bio-imaging laboratory for bio diagnosis. Initiated to develop the exosome-based diagnostic and therapeutic modalities for neurodegenerative (Parkinson’s and Alzheimer's) and cancer diseases. His laboratory becomes a leading place for exosome-based research. His lab website is: www.skumarlab.com |
| Awards & Honours |
|
| Selected Publications/Patents (Last 5 years) | PATENTS:
PUBLICATIONS: (Last 5 years)Google scholar link: https://scholar.google.co.in/citations?user=kAU_84kAAAAJ&hl=en
|
| Photograph | |
| Current Designation & Contact Details | Additional Professor Room No: 3011, 3rd Floor, Teaching Block, Department of Biophysics, All India Institute of Medical Sciences, New Delhi - 110029 Phone: +91-11-26594240 (O) Email: sarojgupta[dot]k[at]gmail[dot]com Lab Website: www.skumarlab.com |
| Recent Employment Details (Past few years) |
|
| Brief Research Area | Dr Saroj has established the infrared-based bio-imaging laboratory for bio diagnosis. Initiated to develop the exosome-based diagnostic and therapeutic modalities for neurodegenerative (Parkinson’s and Alzheimer's) and cancer diseases. His laboratory becomes a leading place for exosome-based research. His lab website is: www.skumarlab.com |
| Awards & Honours |
|
| Selected Publications/Patents (Last 5 years) | PATENTS:
PUBLICATIONS: (Last 5 years)Google scholar link: https://scholar.google.co.in/citations?user=kAU_84kAAAAJ&hl=en
|
| Name | Designation |
|---|---|
| Dr. Sujata Mohanty | Asstt. Prof. |
| Name | Designation |
|---|---|
| Dr. Aarti Vij | Addl. Prof. |
| S.No. | Name | Designation | |
|---|---|---|---|
| 1 | Dr R.Lakshmy | Professor | lakshmy_ram[at]yahoo[dot]com Area of interest:
|
| Name | Designation |
|---|---|
| Dr. Ruma Ray | Professor |
Dr. Rajendra Prasad, was established on the 10th of March, 1967 as a National centre for ophthalmic science, to provide state of the art patient care, expand human resources for medical education and undertake research to find solutions to eye health problems of national importance.
Dr. R.P.Centre for Ophthalmic Sciences has Medical Social Service Unit to assist, guide and help patients for their treatment. Our unit is serving patients for more than three decades. There are two Medical Social Service Officers to guide and counsel the patient as per the need. The Medical Social Service Officer (MSSO) is an indispensable member of the ‘Multi-professional Health Care Team’ who creates a therapeutic network among the doctor, the patient, the family and the community. The MSSO team works under the supervision of Medical Superintendent of the centre. The Services provided includes Counselling, financial assistance for treatment, psychological and vocational support.
Beside treatment, liaising for various rehabilitation activities including social, economical these everyday more than 400 patients are guided and helped by the part time social guides under supervision of MSSO.
In R.P.Centre all Medical social Services are under one window system. MSSO is coordinating for financial assistance through Ayushman Bharat Pradhan Mantri Jan Arogya Yojana and Janani Shishu Surksha Karyakarm , Rashtriya Arogya Nidhi (RAN/NIAF),Prime Minister's Relief Fund, Health Minister's Discretionary Grant Fund and direct donations , and through requisition Performa for BPL/Poor Indigent patients.
Since 2005, Dr Y S Kusuma has been a faculty member at the AIIMS - Centre for Community Medicine. She graduated from Andhra University with Post-Graduate and Doctoral degrees in Anthropology in 1992 and 1999, respectively. In 1995, she earned a Post-Graduate Diploma in Applied Statistics from the same university.
She started her career as an anthropologist working with various indigenous communities, including particularly vulnerable tribal groups. Her initial interest was understanding the epidemiological transitions due to acculturation and urbanisation. Through her doctoral work, she demonstrated the epidemiological transition in traditional communities and highlighted the need for screening for non-communicable diseases among socioeconomically disadvantaged communities. Additionally, access to primary healthcare in communities of different backgrounds was studied.
Since joining AIIMS, she has concentrated her teaching and research on social determinants of health. She worked with various communities across some Indian states, including rural, urban, and tribal inhabitants and migrants. Since she joined AIIMS, she has completed nine research projects, and three more are now in progress. Her research received grants from the All India Institute of Medical Sciences (AIIMS, New Delhi), the Indian Council of Medical Research (ICMR), the Department of Science and Technology (DST), the Council of Scientific and Industrial Research (CSIR), and the Indian Council of Social Science Research (ICSSR).
In collaboration with State health authorities, she has conducted implementation research with an inclusive partnership strategy to improve healthcare access to socioeconomically disadvantaged migrants. She recently completed implementation research to improve tribal populations’ access to healthcare through health and wellness centres in the context of universal health coverage. Her other research projects include health insurance for the poor, social and behavioural change in the context of vector-borne diseases, maternal and child health care, local governance, and the intersectionality of gender, poverty and social norms on adolescent health.
In addition to a few book chapters, she authored about 100 research papers in national and international journals. Her research interests include socio-behavioural and health systems research and implementation research to improve health and healthcare access for marginalised and vulnerable communities.
Future
Advanced cardiac Monitoring.
DM in cardiac Intensive care.
Courses in Echocardiography certification.
Anaesthesia for surgery for advanced heart failure.
Telemedicine.
Paediatric cardiac Transplant.
Cost Reduction Measures.
Contributions
The faculty of the Department has been participating in Community health camps frequently.
Dr. Usha Kiran participated in 4 Health Awareness campaigns from Kanya Kumari to Delhi, Delhi to Punjab, Kashmir to Chandigarh and 2 Stop Smoking campaigns and organized 2 Headache relief camps.
Dr. Usha Kiran participated in 67 National Health Melas organized by Heart Care Foundation and Medical Wing of Rajasthan Yoga Education and Research Foundation.
Dr. Usha Kiran was invited in Dhaka for introducing spirituality and Yoga in the field of Cardiology and Cardiac Surgery.
Dr. Usha Kiran has delivered Public talks on the topic “Stress Management, raising self esteem, Positive Thinking for patients undergoing heart surgery”.
Dr. Poonam participated in Charitable Health Camps. (Rotary & Lions Club) and gives charitable health services at Ram Memorial Clinic, Madhuban Delhi and participates in school activities of "Bal Kalyan Kendra" at Noida.
Star News Coverage of the Relaxation and Meditation programme for Headache relief and Pain Management which is a part of the research conducted by Dr. Usha Kiran with Neurology Department.
Stress management and Meditation Clinic for Patients and their attendants in the CT5 Ward for last 10 years.

M.B.B.S., M.D., FIPHA
Professor, Centre for Community Medicine
The All India Institute of Medical Sciences, New Delhi, India
drsanjay.aiims@gmail.com, sanjayrai@aiims.edu
AIIMS, New Delhi Office Room Number: 29 Center For Community Medicine AIIMS, New Delhi - 110029, INDIA Phone: +91 11 26592446 | Research and Field area office CRHSP, AIIMS, Ballabgarh, Faridabad, Haryana - 121004, INDIA Phone- +91 129 2241362 |
Dr. Sanjay K Rai is currently Professor at Centre for Community Medicine, All India Institute of Medical Sciences (AIIMS), New Delhi, India. He is also Editor of prestigious WHO-South East Asia Journal of Public Health.
He completed his MBBS from GSVM Medical College, Kanpur and MD (Community Medicine) from the Institute of Medical Sciences, Banaras Hindu University (BHU), Varanasi. Before joining AIIMS, he has worked at Maulana Azad Medical College, New Delhi, and Government Medical College and Hospital, Chandigarh.
Prof. Rai has to his credit over 175 publications and is a regular reviewer of many major national and international journals. He has been involved in more than 40 research projects. Prof. Rai has many awards and honours to his name including “Dr J. E. Park Memorial Oration” of Indian Public Health Association (IPHA), and has also been conferred “Fellowship” of IPHA. He is member of many technical/expert groups constituted by Government of India, Indian Counsil of Medical Research (ICMR), and International Clinical Epidemiology Network (INCLEN) and has contributed in many national health programmes e.g., National AIDS Control Programme, National Health Mission, Revised National Tuberculosis Control Progrmme etc. Prof. Rai is working in the area of HIV / AIDS and has been providing technical support to National AIDS Control Organization (NACO), Ministry of Health & Family Welfare. He is member of many technical resource groups of NACO. Prof. Rai is also focal person for NACO designated National Institute for HIV Surveillance at AIIMS, New Delhi, to monitor and support, HIV Sentinel Surveillance in India.
His other areas of interest are immunization, health system, and communicable diseases including Tuberculosis, Influenza. He was also faculty member for “CME programme for PAN-African e-network project of AIIMS”, a project started by the Hon'ble President of India in 2009 which broadcasts to 35 African countries.
Dr. Rai is National trainer on HIV / AIDS Counselling and Sexually Transmitted Infection (STI) for NACO, Ministry of Health and Family Welfare, Govt. of India, since 1997 and 2008 respectively. He is also National Trainer for “Integrated Management of Neonatal and Child Illnesses (IMNCI)” since 2007.
Dr. Rai has received many travels grant to deliver invited lectures in more than 10 countries.
He was involved in research on human influenza disease burden in India, and also one of the largest influenza vaccine effectiveness trial studies in collaboration with Centre for Disease Control, Atlanta, and University of Alabama, USA.
He is the current (2019-23) National President of Indian Public Health Association (IPHA), and Vice President of the National Medical Organization (NMO) of Delhi State.
Dr. Rai has played a vital role in promoting public health leadership during COVID-19 pandemic.
As President of the Indian Public Health Association, he founded a joint COVID-19 taskforce with eminent public health experts belonging to various public health associations of India e.g., Indian Association of Preventive of Social Medicine (IAPSM), Indian Association of Epidemiologist (IAE) and IPHA. The main objective of the joint taskforce was to advise the Government of India regarding the containment of COVID-19 in India. In this regard, four consecutive statements were produced and sent to the government including the honorable Prime Minister of India. The statements were vital in creating awareness regarding the epidemiology, control measures, use of vaccines, etc. to contain covid-19 in India.He also provided inputs during an interaction with the Prime Minister of India. Awareness generation and educating, both lay people as well as health professionals through print and electronic media was his special forte. In fact, he is one of the most recognizable faces in the digital media. He also played a very important role in development of vaccine against COVID-19 in India. His contribution as Principal Investigator of vaccine safety (phase 1 & 2), and effectiveness (Phase 3) trial at AIIMS, New Delhi, helped timely release of COVAXIN TM vaccine nationally as well as globally.
Positions Held
Dr. Usha Kiran was Executive Council member of Association of Cardiac Anaesthesia from 1996-97.
Dr. Usha Kiran is Vice president of PRAN.
Dr. S.C. Kale was Executive member of IACTA 2001 & 2003.
Dr. Neeta Saxena was president of IACTA in 2002.
Dr. Sandeep Chauhan is Associate Editor of the journal Annals of Cardiac Anaesthesia and Associate Vice President of IACTA.
Dr. Poonam Malhotra Kapoor was the Executive Council Member of IACTA 2003-09 and is now the Treasurer of Indian Association of Cardiac Anaesthesia for the next three years 2009 to 2011 with the Head Office of IACTA at AIIMS. It functions by issuing newsletters of Association activities, recruiting new IACTA members and holding academic, scientific and financial aspects of the Association activities. She is also on the editorial board of the Annals of Cardiac Anaesthesia and Journal of clinical Anaesthesia.
Dr. Minati Choudhury is on the editorial board of journal of clinical Anaesthesia and is the warden of the PG Girls Hostel of AIIMS.
| Photograph | |
| Current Designation & Contact Details | Additional Professor Room No. 3011, Third Floor, Teaching Block, Department of Biophysics, All India Institute of Medical Sciences, New Delhi, India Email: krishna[dot]inampudi[at]aiims[dot]edu & kishorehcu[at]gmail[dot]com Contact No: +91-11-26593834 (O) |
| Recent Employment Details (Past few years) |
|
| Brief Research Area |
|
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?user=7G4HaXEAAAAJ&hl=en
|
| Photograph | |
| Current Designation & Contact Details | Additional Professor Room No. 3011, Third Floor, Teaching Block, Department of Biophysics, All India Institute of Medical Sciences, New Delhi, India Email: krishna[dot]inampudi[at]aiims[dot]edu & kishorehcu[at]gmail[dot]com Contact No: +91-11-26593834 (O) |
| Recent Employment Details (Past few years) |
|
| Brief Research Area |
|
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?user=7G4HaXEAAAAJ&hl=en
|
| 1. | Introduction to AIIMS |
| 2. | Particulars of organization Functions and Duties. |
| 3. | Powers and Duties of Officers and Employees |
| 4. | Rules, Regulations, Instructions, Manual and Records, for Discharging Functions. |
| 5. | Particulars of arrangement that exists for consultation with or representation by the members of the public in relation to the formulation of its policy or implementation thereof |
| 6. | A Statement of the categories of documents that are held by it or under its control. |
| 7. | A Statement of boards, council, committees and other bodies constituted as its part. |
| 8. | The Names, Designation and other particulars of the Public Information Officers. |
| 9. | Procedures followed in Decision Making Process. |
| 10. | Directory of Officers and Employee. |
| 11. | The Monthly Remuneration received by each of the Officers and Employees. |
| 12. | The Budget Allocated to each Agency. (Particulars of all plans, proposed expenditure and reports on disbursement made). |
| 13. | The Manner of Execution of Subsidy Programme. |
| 14. | Particulars of Recipients of Concessions, permits or authorization granted by it. |
| 15. | Norms set by AIIMS for the discharge of its functions. |
| 16. | Information available in an electronic form. |
| 17. | Particulars of the facilities available to citizens for obtaining information. |
| 18. | Other useful information’s: Projects of AIIMS |
| 1. | Introduction to AIIMS |
| 2. | Particulars of organization Functions and Duties. |
| 3. | Powers and Duties of Officers and Employees |
| 4. | Rules, Regulations, Instructions, Manual and Records, for Discharging Functions. |
| 5. | Particulars of arrangement that exists for consultation with or representation by the members of the public in relation to the formulation of its policy or implementation thereof |
| 6. | A Statement of the categories of documents that are held by it or under its control. |
| 7. | A Statement of boards, council, committees and other bodies constituted as its part. |
| 8. | The Names, Designation and other particulars of the Public Information Officers. |
| 9. | Procedures followed in Decision Making Process. |
| 10. | Directory of Officers and Employee. |
| 11. | The Monthly Remuneration received by each of the Officers and Employees. |
| 12. | The Budget Allocated to each Agency. (Particulars of all plans, proposed expenditure and reports on disbursement made). |
| 13. | The Manner of Execution of Subsidy Programme. |
| 14. | Particulars of Recipients of Concessions, permits or authorization granted by it. |
| 15. | Norms set by AIIMS for the discharge of its functions. |
| 16. | Information available in an electronic form. |
| 17. | Particulars of the facilities available to citizens for obtaining information. |
| 18. | Other useful information’s: Projects of AIIMS |
| सूचना का अधिकार अधिनियम 2005 के तहत सी.सी.एम, एम्स नई दिल्ली जठरात्ररोग विज्ञान विभाग एवं एचएनयू एम्स, नई दिल्ली तथा परीक्षा अनुभाग, एम्स नई दिल्ली से संबंधित केन्द्रीय जन सूचना अधिकारी, केंद्रीय सहायक जन सूचना अधिकारी एवं प्रथम अपीलीय प्राधिकारी की नियुक्ति नामांकन के संबंध में/Designation/nomination of Central PUrblic information officer, Central Assttt. Public information officer & First Appellate Authority for relating of CCM, AIIMS, New Delhi Deptt. of Gastroenterology & HNU, AIIMS, New Delhi & Exmination Section, AIIMS, New Delhi, under Right to information Act 2005 - reg. | |
| 1 | Designation/Nomination of Central Public Information officer, Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 2 | Designation/Nomination of Central Public Information officer, Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 3. | Designation/Nomination of Central Public Information officer, Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 4 | Designation/Nomination of Central Public Information officer, Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 5 | Designation/Nomination of Central Public Information officer, Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 6 | Designation/Nomination of Central Public Information officer, Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 7 | Designation/Nomination of Central Public Information officer, Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 8 | Designation/Nomination of Central Public Information officer, Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 9 | Designation/Nomination of Central Public Information officer, Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 10 | Designation/Nomination of Central Public Information officer, Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 11 | Designation/Nomination of Central Public Information officer, Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केन्द्रीय जन सूचना अधिकारी, केन्द्रीय सहायक जन सूचना अधिकारी और प्रथम अपीलीय प्राधिकारी के पदनाम/नामांकन संबंधी। |
| 12 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 13 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 14 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 15 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 16 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 17 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 18 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 19 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 20 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 21 | अ.भा.आ.स , नई दिल्ली में सूचना का अधिकार अधिनियम के अंतर्गत केंन्द्रीय जन-सूचना अधिकारी, केंन्द्रीय सहायक जन-सूचना अधिकारी एवं प्रथम अपीलीय प्राधिकारी को नामित /मनोनीत करनें संबंधी/Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi |
| 22 | Designation/Nomination of Central Public Information officer,Central and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 23 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 24 | Designation/Nomination of Central Public Information officer under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 25 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 26 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi/एम्स, नई दिल्ली में सूचना का अधिकार अधिनियम के तहत केंद्रीय जन-सूचना अधिकारी. केंद्रीय सहायक जन-सूचना अधिकारी और प्रथम अपीली प्राधिकारी को नमोद्षिट नामित करने संबंधी |
| 27 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First Appellate Authority under RTI of AIIMS, New Delhi |
| 28 | Designation/Nomination of Central Public Information officer,Central Assistant Public Information officer and First appellate Authority under RTI of AIIMS, NEw Delhi |
| 29 | Designation/Nomination of Central Public Information officer under Right to Information Act for Deptt. of Forensic Medicine & Toxicology at AIIMS New Delhi |
| 30 | अ.भा.आ.सं. ऩई दिल्ली में सुचना का अधिकार अधिनियम, 2005 के तहत केन्द्रीय जन सूचना सहायक जन सूचना अधिकारियों एव प्रथम अपीलीय अधिकारी के नामाकन संबंधी/ Designation/Nomination of Central Public Information officer, Asstt. Central Public information officer & First Appellate authority under Right to Information Act 2005 at AIIMS, New Delhi |
| 31 | सूचना का अधिकार अधिनियम के अंतर्गत एम्स में एव प्रथम अपीलीय अधिकारी के नामांकन संबंधी/Designation/Nomination of First Appellate Authority under RTI act at AIIMS, Out of Reach OPD, Badsha, Jhajjar (H) |
| 32 | सूचना का अधिकार अधिनियम के अंतर्गत एम्स में प्रथम अपीलीय अधिकारी के नांमाकन संबंधी/Designation/Nomination of First Appellate Authority under RTI Act of AIIMS, New Delhi |
| 33 | अ.भा.आ.सं. ऩई दिल्ली में सुचना का अधिकार अधिनियम, 2005 के तहत केन्द्रीय जन सूचना सहायक जन सूचना अधिकारियों एव प्रथम अपीलीय अधिकारी के नामाकन संबंधी/ Nomination of Central Public Information officer, Asstt. Central Public information officer & First Appellate authority under Right to Information Act 2005 at AIIMS |
| 34 | अ.भा.आ.सं. ऩई दिल्ली में सुचना का अधिकार अधिनियम, 2005 के तहत केन्द्रीय जन सूचना सहायक जन सूचना अधिकारियों एव प्रथम अपीलीय अधिकारी के नामाकन संबंधी/ Nomination of Central Public Information officer, Asstt. Central Public information officer & First Appellate authority under Right to Information Act 2005 at AIIMS |
| 35 | Nomination of Central Public Information Officer, under right to Information Act at AIIMS/सूचना का अधिकार अधिनियम के तहत एम्स में केन्द्रीय जल सूचना अधिकारी के नामांकन संबंधी |
| 36 | सूचना का अधिकार अधिनियम के अंतर्गत एम्स में केन्दीय जन सूचना अधिकार एंव प्रथम अपीलीय प्राधिकारी के नांमाकन संबंधी/ Nomination of Central Public Information Officer & First Appellate Authority under Right to Information Act at AIIMS. |
| 37 | सुचना का अधिकार अधिनियम, 2005 के तहत अ.भा.आ.सं. ऩई दिल्ली में पदमानित-नामांकित अपीलीय प्राधिकारी केन्द्रीय जन सूचना आधिकारियों, केन्द्रीय सहायक जन सूचना अधिकारियों के नाम संबंधी/ Nomination of Central Public Information officer, Asstt. Central Public information officer & First Appellate authority under Right to Information Act at AIIMSसूचना का अधिकार अधिनियम, 2005 के तहत केन्द्रीय लोक सूचना अधिकारी का पदनाम |
| 38 | सूचना का अधिकार अधिनियम के अंतर्गत एम्स में केन्द्रीय जन सुचना अधिकारी, सहायक केन्द्रीय जन सुचना अधिकारी एव प्रथम अपीलीय प्राधिकारी के नामांकन संबंधी ( विभाग नामित है : जे पी एन ए टी सी, प्लास्टिक एण्ट रिकन्सट्रकिटच एण् बर्न सर्जरी, एन,एम,आर, बजट कमपलीशन) Nomination of Central Public Information officer, Asstt. Central Public Information officer & First Appellate Authority under RTI Act at AIIMS (The name of Individual Deptt: JPNATC, Plastic & Reconstructive Burns Surgery, NMR, Budget & Compilation)सूचना का अधिकार अधिनियम, 2005 के तहत केन्द्रीय लोक सूचना अधिकारी का पदनाम |
| 39 | सूचना का अधिकार अधिनियम के अंतर्गत एम्स में केन्द्रीय जन सुचना अधिकारी, सहायक केन्द्रीय जन सुचना अधिकारी एव प्रथम अपीलीय प्राधिकारी के नामांकन संबंधी ( विभाग नामित है :एम्स कैफेटेरिया, एम्स झज्जर, व्यापक ग्रामीण स्वास्थय सेबा परियोजना वल्लभगढ/ Nomination of Central Public Information officer, Asstt. Central Public Information officer & First Appellate Authority under RTI Act at AIIMS (The name of Individual Deptt: AIIMS Cafeteria, NCi Jhajjar, CRHSP, Ballabgarh)सूचना का अधिकार अधिनियम, 2005 के तहत केन्द्रीय लोक सूचना अधिकारी का पदनाम |
| 40 | सूचना का अधिकार अधिनियम के अंतर्गत एम्स में केन्द्रीय जन सुचना अधिकारी, सहायक केन्द्रीय जन सुचना अधिकारी एव प्रथम अपीलीय प्राधिकारी के नामांकन संबंधी ( विभाग नामित है :- प्रसूति एव स्त्री विज्ञान,शैक्षिक अनुभाग, तंत्रिक विज्ञान, अनुसंधान अनुभाग, पेशन प्रकोष्ठ एव एन.पी.एस, बजट, रोकड बही, रोकडिया प्रकोष्ट , नोडल अधिकारी (पो.एफ,एम,एस) रोकड अनुभाग, भाण्डार लेखा, कन्करेंस प्रकोष्ट,वर्क आंडिट, एम.एस.यू, अनुसांधन अनुबाग, एम्स झज्जर/ Nomination of Central Public Information officer, Asstt. Central Public Information officer & First Appellate Authority under RTI Act at AIIMS (The name of Individual Deptt: Obs. & gyne, Academic Sect., NSC, Research Sect, Pension Cell & NPS, Budget & Cash, Cashbook Cashier, Nodal officer (PFMS), Cash Sect., Store A/c Conc. Cell, MSU, GPF, Work Audit, Research Section & AIIMS, Jhajjar)सूचना का अधिकार अधिनियम, 2005 के तहत केन्द्रीय लोक सूचना अधिकारी का पदनाम |
| 41 | सूचना का अधिकार अधिनियम के अंतर्गत एम्स में केन्द्रीय जन सुचना अधिकारी, सहायक केन्द्रीय जन सुचना अधिकारी एव प्रथम अपीलीय प्राधिकारी के नामांकन संबंधी ( विभाग नामित है – नर्सिग माहविधालय, प्रजनन जैव विज्ञान, भेषजगुण विज्ञान, जैव रसायन एवं सुक्ष्म विज्ञान विभाग / Nomination of Central Public Information officer, Asstt. Central Public Information officer & First Appellate Authority under RTI Act at AIIMS ( The name of Individual Deptt. :- College of Nursing, Reproductive Biology, Pharmacology, Biochemistry & Deptt. Of Microbiology)सूचना का अधिकार अधिनियम, 2005 के तहत केन्द्रीय लोक सूचना अधिकारी का पदनाम |
| 42 | सूचना का अधिकार अधिनियम के अंतर्गत एम्स में केन्द्रीय जन सुचना अधिकारी, सहायक केन्द्रीय जन सुचना अधिकारी एव प्रथम अपीलीय प्राधिकारी के नामांकन संबंधी ( विभाग नामित है - हिदी अनुभाग, लेखा परीक्षा अनुभाग, शरीर क्रिया विज्ञान एव डां रा.प्र.केन्द्र/Nomination of Central Public Information officer, Asstt. Central Public Information officer & First Appellate Authority under RTI Act at AIIMS ( The name of Individual Deptt. :- Hindi Section, Audit Section, Physiology, Dr. RPC)सूचना का अधिकार अधिनियम, 2005 के तहत केन्द्रीय लोक सूचना अधिकारी का पदनाम |
| 43 | Nomination of Central Public Information Officer, under right to Information Act of AIIMS/सूचना का अधिकार अधिनियम, 2005 के तहत केन्द्रीय लोक सूचना अधिकारी का पदनाम |
| 44 | सूचना का अधिकार अधिनियम, 2005 के तहत विभिन्न विभागों, एम्स, नई दिल्ली से सबंधित मामलो हेतु पदनामित/नामांकित अपीलीय प्राधिकारी, केन्द्रीय जन सूचना अधिकारी तथा केन्द्रीय सहायक जन सूचना अधिकारी के नाम संबंधी. |
| 45 | Designation/Nomination of Central Public INformation Officer, ACPIO & First Appellate Authority in respect of Deptt. of Pathology, Transport Office & Garage, Estate Sect.,GSLI Stores Section (DO) & CMIR, AIIMs under Right to Information Act. |
| 46 | Designation/Nomination of Central Public Information Officer Deemed CPIO & First Appellate Authority in respect of various Deptt's, AIIMS under Right to Information Act. |
| 47 | Designation/Nomination of First Appellate Authority in respect of Finance Division (Budget Section), Finance Division (Work Audit) AIIMS, New Delhi Under RTI Act. |
| 48 | Designation/Nomination of Central Public Information Officer, & First Appellate Authority in respect of Academic Section, Research Section, Research Section, Store Section (DO), Peadiatric Central Work shop, B.B.Dixit Library, C.M.E.T Central Animal Facility and Pulmonary Medicine & Sleep Disorder, AIIMS, New Delhi, under Right to Information Act. |
| 49 | Designation/Nomination of Central Public Information Officer, and First Appellate Authority in respect of Surekha Vishram Sadan, Sai Vishram Sadan, Rajgarhia Vishram Sadan, and Computer Facililty AIIMS, New Delhi under Right to Information Act |
| 50 | Designation/Nomination of Central public Information officer, Central Assistant public Information Officer & First Appelate authority in respect of Various Deptt.'s AIIMS, New Delhi under Right to Information Act. |
| 51 | Designation/Nomination of Appellate Authority, Central Public Information Officer & Central Assistant Public Information Officer for the matter relating to Computer Facility & Plastic Reconstructive & Burns Surgery, AIIMS, New Delhi under Right to Information Act. |
| 52 | Designation/Nomination of First Appellate Authority in RTI matter relating to Engineering Service Deptt. under right to Information Act |
| 53 | Designation/Nomination of Appellate Authority, Central Public Infromation Officer & Central Assistant Public Information Officer for the matter relating to relating to Deptt. of Rheumatology, AIIMS, New Delhi |
| 54 | Designation/Nomination of Appellate Authority, Central Public Infromation Officer & Central Assistant Public Information Officer for the matter relating to relating to JPNATC, AIIMS and Vigilance Cell, AIIMS, New Delhi, Under RTI-2005 |
| 55 | Designation of Appellate Authority & relating to Finance Division, AIIMS, New Delhi under Right to Information Act, 2005 |
| 56 | Designation of Appellate Authority , Central Public Information Officer & Central Assistant Public Information Officer for matter relating to Department of Psychiatry, AIIMS, New Delhi and National Drug Dependence Treatment Centre(NDDTC), AIIMS, Ghaziabad under Right to Information Act, 2005 |
| 57 | Designation of Appellate Authority , Central Public Information Officer & Central Assistant Public Information Officer for matter relating to Establishment Section-I and Establishment Section-II AIIMS, New Delhi under Right to Information Act, 2005 |
| 58 | Designation of Appellate Authority , Central Public Information Officer & Central Assistant Public Information Officer for matter relating to CDER and Dr. B.R.A.-I.R.C.H AIIMS, New Delhi under Right to Information Act, 2005 |
| 59 | Designation of Appellate Authority , Central Public Information Officer & Central Assistant Public Information Officer for matter relating to Anaethesiology AIIMS, New Delhi under Right to Information Act, 2005 |
| 59 | Designation of Appellate Authority , Central Public Information Officer & Central Assistant Public Information Officer for matter relating to Finance Division, Dr. R.P. Centre for Ophthalmic Sciences and Neuro-Sciences Centre AIIMS, New Delhi under Right to Information Act, 2005 |
| 60 | Designation of Appellate Authority , Central Public Information Officer for matter relating to Vigilance Cell, AIIMS, New Delhi under Right to Information Act, 2005 |
| 61 | Designation of Appellate Authority , Central Public Information Officer & Central Assistant Public Information Officer for matter relating to Department of Obstetrics & Gynaecology, AIIMS under Right to Information Act, 2005 |
| 62 | Designation of Appellate Authority , Central Public Information Officer & Central Assistant Public Information Officer for matter relating to Department of Radio-Diagnosis, Laboratory Medicine and NDDTC, AIIMS under Right to Information Act, 2005 |
| 63 | Designation of Appellate Authority & Central Public Information Officer for matter relating to RTI Cell, AIIMS and Co-ordination Cell, AIIMS, New Delhi under Right to Information Act, 2005 |
| 64 | Designation of Appellate Authority, Central Public Information Officer & Central Assistant Public Information Officer for matter relating to Faculty Cell, Recruitment Cell, Establishment Section-I & II, Legal Cell, Coordination Cell, RTI Cell, ACR Cell, SC/ST Cell, General Section AIIMS, under Right to Information Act,2005 |
| 65 | Designation of Appellate Authority, Central Public Information Officer & Central Assistant Public Information Officer for matter relating to Comprehensive Rural Health Services Project, AIIMS, Ballabgargh under Right to Information Act,2005 |
| 66 | Designation of Appellate Authority, Central Public Information Officer & Central Assistant Public Information Officer for matter relating to K.L.Wig Centre for Medical Education & Technology AIIMS under Right to Information Act,2005 |
| 67 | Designation of Central Public Information Officer & Central Assistant Public Information Officer & Appellate Authority for matter relating to Department of Gastroenterology & HNU, AIIMS under Right to Information Act,2005 |
| 68 | Designation of Central Public Information Officer, Central Assistant Public Information Officer & Appellate Authority for Department of Cardio Thoracic Centreand Neuro Sciences Centre, AIIMS under Right to Information Act,2005 |
| 69 | Designation of Appellate Authority, Central Public Information Officer &Central Assistant Public Information Officer under Right to Information Act, 2005 at the AIIMS. |
| 70 | Designation of Central Public Information Officer, Central Assistant Public Information Officer & Appellate Authority for matter relating to (Sadans) & (Examination) , AIIMS under Right to Information Act, 2005. |
| 71 | Designation of Central Public Information Officer, Central Assistant Public Information Officer & Appellate Authority for matter relating to Department of Computer Facility , AIIMS under Right to Information Act, 2005. |
| 72 | Designation of Central Public Information Officer , Central Assistant Public Information Officer & Appellate Authority for matter relating to Department of Medicine , AIIMS under Right to Information Act, 2005. |
| 73 | Designation of Central Public Information Officer , Central Assistant Public Information Officer & Appellate Authority for matter relating to Stores Section (DO), AIIMS under Right to Information Act, 2005. |
| 74 | Designation of Appellate Authority, Central Public Information Officer & Central Assistant Public Information Officer for matter relating to Department of ENT, Medicine, Obstetrics & Gynaecology, Orthopaedics and Paediatrics, AIIMS under Right to Information Act, 2005. |
| 75 | Designation of Appellate Authority, Central Public Information Officer & Central Assistant Public Information Officer for matter relating to Engineering Service Department, AIIMS under Right to Information Act, 2005. |
| Designation of Appellate Authority, Central Public Information Officer & Central Assistant Public Information Officer for matter relating to Department of Anatomy and Department of Obstetrics & Gynaecology, AIIMS under Right to Information Act, 2005. |
Download the HRIDAY app here. This app is for heart failure patients . It stores the medications lists, helps check the health status and gives health tips about heart failure. You can download and install the app on any android phone. For any help contact the heart failure clinic at AIIMS ,Thursday 2 pm. If you do not have an android phone, you can ask for a paper equivalent of the HRIDAY card which is also available at the clinic.
Focus areas of clinical care and research of the Department.
The department of Cardiac Anaesthesia maintains its records, duly catalogued indexed and computerized (Since Oct 2006) using SPSS software. The headings under which the records are categorized are as under:
These records are registered daily in operation theatre on a medical record sheet and register and also computerized. Annual report of department records is submitted annually.
The normal functioning of the department is according to the rules and regulations laid down by CN Centre, AIIMS. Seven Theatres function everyday with 2 or 3 cases in each theatre daily. One Emergency heart surgery may be taken up anytime in the day/night. One consultant and one or two seniors residents round the clock emergency duty for postoperative care of cardiac patients as well as intensive and ventilatory/resuscitative management in coronary care unit. One consultant on round the clock call for emergency operations. Anaesthesia is given for a total of 14-20 heart operations everyday with postop and coronary ventrilatory care. General anesthesia or monitored anaesthesia care is given in cath. Lab and computerized angiography and MRI in Cardiac patients.Two senior residents are on emergency call-attending calls from CCU, ICU, CTVS wards, Cath. Lab. and Operation Theatres. Bedside pre anaesthetic check up is done daily.
2 academic sessions held per week as part of department’s academic activity – where seminars/Tutorials/Journal Clubs/Examinations are held by faculty & residents. The department has access to the AIIMS Dr. B.B.Dixit Library and National Medical Library at all times. Internet access is available via computer facility in all consultant’s rooms.
Additional Professor R.No.3006, 3rd Floor Teaching Block | |
| Recent employment details | Additional Professor,since July 2020-Till date Associate Professor, since July 2017-June 2020 Assistant Professor,since June 2014-June 2017 |
| Research Interests | The research work is focused on TP53 tumor suppressor gene plays crucial role in suppression of cancer. But the mutation in p53 leads to tumour proliferation sometimes drug resistance cancer cells. The research focused on targeting mutant p53 with structure-based drug design to restore mutant p53 to functional like wild type. We do structure-based drug design by X-ray crystallography and for drug binding and functional studies we various biophysical techniques like ITC, CD, Fluorescence and cell based functional assay in p53 mutant cell lines. The second major project in our lab is antimicrobial drug development against drug resistant bacterial pathogen. We work on bacterial cell division proteins particularly FtsZ and its associate proteins involved forming divisome protein complex assembly. We do structure-based drug design by X-ray crystallography, In silico drug screening and for drug binding studies we various biophysical techniques like ITC, CD, Fluorescence. |
| Any additional information | Associate Professor (2017 - till date): Biophysics, AIIMS, New Delhi, India Assistant Professor (2014 – 2017): Biophysics, AIIMS, New Delhi, India Research Associate (2012-2014): Texas Tech University Health Science center, Texas, USA Post doctoral Fellow (2007 - 2012): University of California San Diego, California, USA. Ph.D. (Biophysics, 2007: AllMS, New Delhi Master of Science (Biophysics, 2002): University of Madras, Chennai Bachelor of Science (Physics -2000): University of Madras, Chennai Google scholar https://scholar.google.com/citations?user=KZJOecsAAAAJ&hl=en Pubmed https://www.ncbi.nlm.nih.gov/pubmed/?term=Ethayathulla+AS%5BAuthor%5D RCSB: |
| Awards and Honors | Senior Research Fellowship awarded by CSIR, New Delhi, India. Senior Research Fellowship in the project from DST, New Delhi, India. Junior Research Fellowship in the project from DST, New Delhi, India. Junior Research Fellowship in the project from DBT, New Delhi, India. |
| Recent Publications |
|
The Department of Cardiology at AIIMS was established under the leadership of Prof. SujoyB. Roy. The department has developed excellent facilities for clinical care and has fully developed facilities for adult and pediatric interventions including coronary interventions, valvuloplasty, device closure of congenital shunts and electrophysiology services (includingradiofrequency ablation, pacemaker, bi-ventricular pacemaker and cardioverter defibrillator implantation). Laboratory testing facilities include treadmill testing, holter recording, echocardiography (including transthoracic, transesophageal, 3-D and fetal echocardiography), Tilt testing for syncope and electrophysiology testing including CARTO system mapping. The department has done pioneering work in the field of rheumatic fever and rheumatic heart disease including juvenile mitral stenosis, coronary artery disease including angioplasties, arrhythmias, cardiomyopathies and congenital heart diseases.
Prof. Sujoy B Roy
Prof. Madan Lal Bhatia
Prof. Rajan Tandon
Prof. Harbans Singh Wasir
Prof. Subhash Chand Manchanda
Prof. Kewal Krishan Talwar
Prof. K. Srinath Reddy
Prof. Vinay Kumar Bahl
Prof. Anita Saxena
Prof. Shyam Sunder Kothari
Prof. Balram Bhargava
Prof. Rajiv Narang (current Head of Department)
The Department is active in training fellows in cardiology and has produced more than 185 DM Cardiologists till date, many of whom are themselves now heading various departments all over India and abroad. Following is the list of alumni of the department:
| S.No. | Name | Month | Year of passing |
|---|---|---|---|
| 1 | DR.J.S.GULERIA | Dec | 1963 |
| 2 | DR.M.L.BHATIA | Dec | 1965 |
| 3 | DR.MAHENDRA PRAKASH GUPTA | May | 1967 |
| 4 | DR.SNEH GADHOKE (KALRA) | May | 1967 |
| 5 | DR.PURUSHOTTAM KR.KHANNA | May | 1968 |
| 6 | DR.HARBANS SINGH WASIR | May | 1969 |
| 7 | DR.MOHAMMAD KHALILULLAH | May | 1969 |
| 8 | DR,SUBHASH CHANDER MANCHANDA | Dec | 1969 |
| 9 | DR.SUDHIR NAIK | Dec | 1970 |
| 10 | DR.D.N.GROVER | May | 1971 |
| 11 | DR.S.SREEDHARAN POTTY | May | 1971 |
| 12 | DR.K.SUGATHAN | Dec | 1971 |
| 13 | DR.SAVITRI SHRIVASTAVA | Dec | 1971 |
| 14 | DR.VIDYA SAGAR KAUSHIK | Dec | 1972 |
| 15 | DR.BARENDRA KANTA DAS | May | 1973 |
| 16 | DR.TONPE DINAKRA RAO | May | 1973 |
| 17 | DR.BHAVANI SANKAR | May | 1973 |
| 18 | DR.HEMLATA TIWARI (JOSHI) | May | 1973 |
| 19 | DR.C.ASHOKAN NAMBIAR | Dec | 1973 |
| 20 | DR.RAJAN JOSEPH MANJURAN | Dec | 1974 |
| 21 | DR.URMILA KUMARI SWAIN | July | 1974 |
| 22 | DR.BIRENDRA PRASAD | May | 1976 |
| 23 | DR.RAJAT KANTI MAHAPATRA | May | 1976 |
| 24 | DR.SUNIEL DALAL | Dec | 1976 |
| 25 | DR.TRIVELLORE ECHAMBAO KASTURI | May | 1977 |
| 26 | DR.P.KRISHNAM RAJU | May | 1978 |
| 27 | DR.ASHA RANI KHANNA | May | 1979 |
| 28 | DR.RAVI RATTAN KASLIWAL | Dec | 1979 |
| 29 | DR.K.SRINATH REDDY | July | 1980 |
| 30 | DR.RAGHAVAN SUBRAMANYAN | July | 1980 |
| 31 | DR.AJAY KUMAR | Dec | 1980 |
| 32 | DR.JALAL-UD-DIN | Dec | 1980 |
| 33 | DR.PRABHAKARAN NARAYANASWAMY.S. | Dec | 1980 |
| 34 | DR.RAJINDER PRASAD BHAT | May | 1981 |
| 35 | DR.RAM BILAS MITTAL | May | 1981 |
| 36 | DR.IPPILIANNAJI VARAPRASADLAL | May | 1981 |
| 37 | DR.GOPISETTI SAI GOPAL | Dec | 1981 |
| 38 | DR.PANCHAPAKESAN RAMACHANDRAN | Dec | 1981 |
| 39 | DR.P.SESHAGIRI RAO | Dec | 1982 |
| 40 | DR.ARUN KUMAR SOOD | Dec | 1982 |
| 41 | DR.MADHOK RAMESH KUMAR | Dec | 1982 |
| 42 | DR.THOMAS TITUS | May | 1983 |
| 43 | DR.KRISHNASWAMY SUBRAMANYAN | May | 1983 |
| 44 | DR.JAGSIH CHANDER MOHAN | May | 1983 |
| 45 | DR.MRITYNJAYA BEHERA | Dec | 1983 |
| 46 | DR.SUMAN BHANDARI | Dec | 1983 |
| 47 | DR.RAVI SHANKAR SHARMA | Dec | 1984 |
| 48 | DR.SATDEV KARLOOPIA | Dec | 1984 |
| 49 | DR.SATISH KUMAR KAUSHIK | Dec | 1984 |
| 50 | DR.CHAKRAPANI SETHU NATH | May | 1985 |
| 51 | DR.GURCHARAN SINGH KALRA | Dec | 1985 |
| 52 | DR.JAGAT PRAKASH SINGH NARULA | Dec | 1985 |
| 53 | DR.SHYAM SUNDER | Dec | 1985 |
| 54 | DR.ANIL KUMAR BHARANI | May | 1986 |
| 55 | DR.S.RADHAKRISHNAN | Dec | 1986 |
| 56 | DR.VISHVA DEV | Dec | 1986 |
| 57 | DR.RAJEEV GUPTA | Dec | 1986 |
| 58 | DR.VISWANATHAN HARIHARAN | Dec | 1986 |
| 59 | DR.SHAYM SUNDER | May | 1987 |
| 60 | DR.RAMESH BABU POTHINENI | Dec | 1987 |
| 61 | DR.DAS GLADWIN SUSEEKAR | Dec | 1987 |
| 62 | DR.RAJIV BAJAJ | May | 1988 |
| 63 | DR.ASHOK GARG | May | 1988 |
| 64 | DR.L.SHYAMKISHORE SINGH | Dec | 1988 |
| 65 | DR.KEWAL CHAND GOSWAMI | Dec | 1988 |
| 66 | DR.BHAVANI DOGRA | May | 1989 |
| 67 | DR.M.VIJAYA KUMAR | May | 1989 |
| 68 | DR.SHIVA NARAAYAN SHARMA | May | 1989 |
| 69 | DR.PRAKASH CHAND NEGI | Dec | 1989 |
| 70 | DR. R.S.VASAN | Dec | 1989 |
| 71 | DR. TARUNKUMAR H. DAVE | May | 1990 |
| 72 | DR. T.KAMALAKAR | May | 1990 |
| 73 | DR. RAJIV NARANG | Dec | 1990 |
| 74 | DR. R.KRISHNA KUMAR | Dec | 1990 |
| 75 | DR. RAJIV AGARWAL | Dec | 1990 |
| 76 | DR. SATISH CHANDRA | Dec | 1990 |
| 77 | DR. Y.VENKATESWARA RAO | May | 1991 |
| 78 | DR. ATUL MATHUR | May | 1991 |
| 79 | DR. PRADEEP JAIN | May | 1991 |
| 80 | DR. GHANASHYAM BASUMATARY | Dec | 1991 |
| 81 | DR. SANJEEV SANGHVI | Dec | 1991 |
| 82 | DR. H.S.SOMANATH | Dec | 1991 |
| 83 | DR. S.RAMAMURTHY | May | 1992 |
| 84 | DR. D.PRABHAKARAN | May | 1992 |
| 85 | DR. SUDHIR | Dec | 1992 |
| 86 | DR. RAJNISH JUNEJA | May | 1993 |
| 87 | DR. SUBHASH CHANDRA | May | 1993 |
| 88 | DR. MANOJ SHARMA | May | 1993 |
| 89 | DR. ANUP KUMAR BORO | May | 1993 |
| 90 | DR. SANGEET SAHAI | Dec | 1993 |
| 91 | DR. DEEPAK THATAI | Dec | 1993 |
| 92 | DR. AJAY BHARGAVA | Dec | 1993 |
| 93 | DR. SHASHI SHEKHAR CHATTERJEE | Dec | 1993 |
| 94 | DR. SANJAY KUMAR CHUGH | May | 1994 |
| 95 | DR. PRASHANT TARAKANT UPASANI | May | 1994 |
| 96 | DR. PUNIT GOEL | May | 1994 |
| 97 | DR. SANJEEV SHARMA | May | 1994 |
| 98 | DR. ANIL KUMAR GOEL | May | 1995 |
| 99 | DR. RAJEEV GUPTA | Dec | 1995 |
| 100 | DR. DHANANJAY KUMAR JHAMB | Dec | 1995 |
| 101 | DR. B. SHARADA | Dec | 1995 |
| 102 | DR. PRAKASH KAMATH K | Dec | 1995 |
| 103 | DR. HANUMANTHU JAGANNAYAKULU | Dec | 1995 |
| 104 | DR. VISHWA VIBHUTI AGARWAL | Dec | 1995 |
| 105 | DR. AJAY MITTAL | May | 1996 |
| 106 | DR. SANDEEP SETH | May | 1996 |
| 107 | DR. DINESH SUDAN | May | 1996 |
| 108 | DR. RAKESH RAI SAPRA | Dec | 1996 |
| 109 | DR. VIKAS CHOPRA | Dec | 1996 |
| 110 | DR. MALIPEDDI BHASKARA RAO | May | 1997 |
| 111 | DR. ARUN KUMAR CHOPRA | May | 1997 |
| 112 | DR. SUNDEEP MISHRA | May | 1997 |
| 113 | DR. SHEKHAR SINGH KASHYA | May | 1997 |
| 114 | DR. RAMDEO YADAVE | Dec | 1997 |
| 115 | DR. N.C.KRISHNA MANI | Dec | 1997 |
| 116 | DR. BISHAV MOHAN | Dec | 1998 |
| 117 | DR. RAKESH YADAV | Dec | 1998 |
| 118 | DR. RAKESH CHAND JINDAL | Dec | 1998 |
| 119 | DR. NITISH NAIK | Dec | 1998 |
| 120 | DR. DHIRAJ GUPTA | May | 1999 |
| 121 | DR. PARTHO PRATIM SENGUPTA | May | 1999 |
| 122 | DR. MRIDUL SHARMA | Dec | 1999 |
| 123 | DR. KAVALIPATI NARASA RAJU | Dec | 1999 |
| 124 | DR. ANIL KUMAR SOOD | Dec | 1999 |
| 125 | DR. RAMRAO MANIKRAO GHODESWAR | Dec | 1999 |
| 126 | DR. HARMINDER SINGH | Dec | 1999 |
| 127 | DR. RAJIV ARORA | May | 2001 |
| 128 | DR. G. KARTHIKEYAN | May | 2001 |
| 129 | DR. ARVIND KOUL | May | 2001 |
| 130 | DR. SARITA GROVER | May | 2001 |
| 131 | DR. PRADEEP KUMAR HASIJA | May | 2002 |
| 132 | DR. YUSUF A | May | 2002 |
| 133 | DR. GAUTAM SHARMA | May | 2002 |
| 134 | DR. PARNEESH ARORA | May | 2002 |
| 135 | DR. SUNIL DWIVEDI | May | 2002 |
| 136 | DR.CHANDRA BHAN MEENA | Dec | 2002 |
| 137 | DR.NEIL BARDOLOI | Dec | 2002 |
| 138 | DR.DHOPESHWARKAR RAJESH ARVIND | Dec | 2002 |
| 139 | DR.KAMMARIPALLE CHANAKYA KISHORE KUMAR | Dec | 2002 |
| 140 | DR.ARUN MOHANTI | Dec | 2002 |
| 141 | DR.S.ANANDARAJA | Dec | 2002 |
| 142 | DR.DEEPAK | May | 2003 |
| 143 | DR.MAMTESH GUPTA | May | 2003 |
| 144 | DR. AMBUJ ROY | May | 2003 |
| 145 | DR.B.RAM PRAKASH | Dec | 2003 |
| 146 | DR. NARESH KUMAR GOYAL | Dec | 2003 |
| 147 | DR.S.RAMAKRISHNAN | May | 2004 |
| 148 | DR.JELAN SINGH | Dec | 2004 |
| 149 | DR.SUMODH KURIEN | Dec | 2004 |
| 150 | DR.HEMANT BEHERA | May | 2005 |
| 151 | DR.SANJEEV KUMAR SHARMA | May | 2005 |
| 152 | DR.RANJIT KR.NATH | May | 2005 |
| 153 | DR.DAVINDER SINGH CHADHA | May | 2005 |
| 154 | DR.MANOHAR SAKHARE | May | 2005 |
| 155 | DR.RAJIV MAHAJAN | Dec | 2005 |
| 156 | DR.AJAY DEEP BHATNAGAR | Dec | 2005 |
| 157 | DR.SANJEEV ASORTA | Dec | 2005 |
| 158 | DR.NAVIN MATHEW | Dec | 2005 |
| 159 | DR.VINEET MALIK | May | 2006 |
| 160 | DR.B.SHANKAR | May | 2006 |
| 161 | DR.AJAY GOPAL | May | 2006 |
| 162 | DR.PRABHAT | Dec | 2006 |
| 163 | DR.KAPIL | Dec | 2006 |
| 164 | DR.S.K.PATRA | Dec | 2006 |
| 165 | DR.RAVI MATH | May | 2007 |
| 166 | DR.NEERAJ | May | 2007 |
| 167 | DR.ANAND AGARWAL | Dec | 2007 |
| 168 | DR.VIVEK CHATURVEDI | Dec | 2007 |
| 169 | DR.NAGESH .C.M. | May | 2008 |
| 170 | DR.AJITH THATCHIL | May | 2008 |
| 171 | DR.RAJENDER THANGJAM | May | 2008 |
| 172 | DR.SHARAD CHANDRA | May | 2008 |
| 173 | DR.AMIT PENDARKAR | May | 2008 |
| 174 | DR.INDRA | Dec | 2008 |
| 175 | DR.PRALOY CHAKRABORTY | Dec | 2008 |
| 176 | DR.SAMEER | May | 2009 |
| 177 | DR.CHIRAYU | May | 2009 |
| 178 | DR.SURESH | May | 2009 |
| 179 | DR.BHARAT BHUSHAN KUKRETI | Dec | 2009 |
| 180 | DR.BHATT KINJAL N | Dec | 2009 |
| 181 | ISHWAR CHANDRA MALAV | Dec | 2009 |
| 182 | DR.NAVREET SINGH | Dec | 2009 |
| 183 | DR.AJAY KUMAR SHARMA | Dec | 2009 |
| 184 | DR.SAROJ KHANAL | May | 2010 |
| 185 | DR.HIMANSHU DABRAL | May | 2010 |
| 186 | DR.SHARATH KUMAR K | Dec | 2010 |
| 187 | DR.JAGDANAND JHA | Dec | 2010 |
| 188 | Dr. Om Murti Anil | May | 2011 |
| 189 | Dr. Pranab Deka | May | 2011 |
| 190 | Dr. Sunil Shivdas | May | 2011 |
| 191 | Dr. Salman Salahuddin | May | 2011 |
| 192 | Dr. Amit Malviya | Dec | 2011 |
| 193 | Dr. Mithun Jacob Varghese | Dec | 2011 |
| 194 | Dr. S. Nagendra Boopathy | Dec | 2011 |
| 195 | Dr. Ramandeep Singh Ahuja | May | 2012 |
| 196 | Dr. Jo Joseph | May | 2012 |
| 197 | Dr. Soumen Devi Dutta | May | 2012 |
| 198 | Dr. Nilkanth C. Patil | Dec | 2012 |
| 199 | Dr. Sudhir S. Shehkar | Dec | 2012 |
| 200 | Dr. Parag W. Barwad | Dec | 2012 |
| 201 | Dr. Naveen Khanna | May | 2013 |
| 202 | Dr. Akhilesh Dubey | May | 2013 |
| 203 | Dr. Doshi Shrenik R. | Dec | 2013 |
| 204 | Dr. Anand Gopal | Dec | 2013 |
| 205 | Dr. R. Ananthakrishnan | Dec | 2013 |
| 206 | Dr. Himanshu Gupta | May | 2014 |
| 207 | Dr. Varun Gupta | May | 2014 |
| 208 | Dr. Jeet Ram | May | 2014 |
| 209 | Dr. Kumar Vaibhav Vikash | May | 2014 |
| 210 | Dr. Cheruparambath Varun | Dec | 2014 |
| 211 | Dr. Vikas Thakran | Dec | 2014 |
| 212 | Dr. Birdevinder Singh | Dec | 2014 |
| 213 | Dr. Prashant Shah | Dec | 2014 |
| 214 | Dr. Abhinit Gupta | May | 2015 |
| 215 | Dr. Binay Kumar | May | 2015 |
| 216 | Dr. Ritesh Kumar Gupta | May | 2015 |
| 217 | Dr. Gajendra Dubey | Dec | 2015 |
| 218 | Dr. Basavaraj Utagi | Dec | 2015 |
| 219 | Dr. Ankit Jain | Dec | 2015 |
| 220 | Dr. Anunay Gupta | May | 2016 |
| 221 | Dr. Rajeev Sharma | May | 2016 |
| 222 | Dr. Deepti | Dec | 2016 |
| 223 | Dr. Suman Karmakar | Dec | 2016 |
| 224 | Dr. Malik Mohammad Azharuddin | May | 2017 |
| 225 | Dr. Danny Kumar | May | 2017 |
| 226 | Dr. Vijay Bohra | May | 2017 |
| 227 | Dr. Anand P. | May | 2017 |
| 228 | Dr. Sridharan. U | May | 2017 |
| 229 | Dr. Abhinav Aggarwal | Dec | 2017 |
| 230 | Dr. Abhishek Gupta | Dec | 2017 |
| 231 | Dr. Raghav Bansal | Dec | 2017 |
| 232 | Dr. Manish Pandey | Dec | 2017 |
| 233 | Dr. Dhara Singh | May | 2018 |
| 234 | Dr. Arvind Dambalkar | May | 2018 |
| 235 | Dr. Vikas Purohit | May | 2018 |
| 236 | Dr. Dinkar Bhasin | Dec | 2018 |
| 237 | Dr. Shanmugam K. | Dec | 2018 |
| 238 | Dr. Shaheer Almed A | Dec | 2018 |
| 239 | Dr. Preetam K | Dec | 2018 |
| 240 | Dr. Nirmal Ghati | Dec | 2018 |
Download the HRIDAY app here. This app is for heart failure patients . It stores the medications lists, helps check the health status and gives health tips about heart failure. You can download and install the app on any android phone. For any help contact the heart failure clinic at AIIMS ,Thursday 2 pm. If you do not have an android phone, you can ask for a paper equivalent of the HRIDAY card which is also available at the clinic.
NATIONAL EYE BANK ulThe National Eye Bank housed in the Dr Rajendra Prasad Centre for Ophthalmic Sciences at the All India Institute of Medical Sciences is celebrating 50 years of its existence and the institute has planned several events to mark it."We received eyes from about 23,000 donors at the Eye Bank, out of which more than 16,000 were used for transplant surgeries. In last one year, we have performed about 1,000 transplantation surgeries.
As part of the National Eye Donation Fortnight--August 25 to September 8-(2016)-the National Eye Bank felicitated about 100 family members of those people, who have donated eyes, as well as NGOs and social workers who have worked in this field.
Different activities conducted in this included programme for Total Health in DD News regarding Eye Donation Promotion Eye Donation Campaign in AIIMS and other Hospitals-- R.M.L.Hospitals, LHMC, S.J.Hospital and awareness session for Asha Workers, Tihar Jail Prisoners and staff.
A walk for eye donation also organised in the institute campus to promote eye donation volunteer ship so as to combat corneal blindness.
Contact phone numbers 011-26593060 /011-26589461

Prof. Nagarur Gopinath who established the dept of Cardiothoracic surgery at the AIIMS in 1964, passed away on Sunday,3rd june, 2007 at Bangalore. He was 84.
He began open heart surgery at the AIIMS in 1964, and began a training program in CTVS, leading to the M.Ch degree in 1966.He has trained a large number of students including half the faculty at the AIIMS. His students are now heading many of the departments in the country.He received the padma Shri from the govt. of India, and the wockhardt lifetime achievement award in 2004,and the lifetime achievement award from the Indian Association of cardiovascular-Thoracic surgeons in 2000.
Following his retirement in 1982 he continued to serve the AIIMS as Emeritus professor and contributed many monographs and papers on preventive aspects of heart disease. He is survived by Mrs. Gopinath, one daughter and two sons. The cardiothoracic centre will certainly feel the void left behind by Prof.Gopinath which will be difficult to fill.
The Department is active in training fellows in cardiology and has produced more than 185 DM Cardiologists till date, many of whom are themselves now heading various departments all over India and abroad. Following is the list of alumni of the department:
| S.No. | Name | Month | Year of passing |
|---|---|---|---|
| 1 | DR.J.S.GULERIA | Dec | 1963 |
| 2 | DR.M.L.BHATIA | Dec | 1965 |
| 3 | DR.MAHENDRA PRAKASH GUPTA | May | 1967 |
| 4 | DR.SNEH GADHOKE (KALRA) | May | 1967 |
| 5 | DR.PURUSHOTTAM KR.KHANNA | May | 1968 |
| 6 | DR.HARBANS SINGH WASIR | May | 1969 |
| 7 | DR.MOHAMMAD KHALILULLAH | May | 1969 |
| 8 | DR,SUBHASH CHANDER MANCHANDA | Dec | 1969 |
| 9 | DR.SUDHIR NAIK | Dec | 1970 |
| 10 | DR.D.N.GROVER | May | 1971 |
| 11 | DR.S.SREEDHARAN POTTY | May | 1971 |
| 12 | DR.K.SUGATHAN | Dec | 1971 |
| 13 | DR.SAVITRI SHRIVASTAVA | Dec | 1971 |
| 14 | DR.VIDYA SAGAR KAUSHIK | Dec | 1972 |
| 15 | DR.BARENDRA KANTA DAS | May | 1973 |
| 16 | DR.TONPE DINAKRA RAO | May | 1973 |
| 17 | DR.BHAVANI SANKAR | May | 1973 |
| 18 | DR.HEMLATA TIWARI (JOSHI) | May | 1973 |
| 19 | DR.C.ASHOKAN NAMBIAR | Dec | 1973 |
| 20 | DR.RAJAN JOSEPH MANJURAN | Dec | 1974 |
| 21 | DR.URMILA KUMARI SWAIN | July | 1974 |
| 22 | DR.BIRENDRA PRASAD | May | 1976 |
| 23 | DR.RAJAT KANTI MAHAPATRA | May | 1976 |
| 24 | DR.SUNIEL DALAL | Dec | 1976 |
| 25 | DR.TRIVELLORE ECHAMBAO KASTURI | May | 1977 |
| 26 | DR.P.KRISHNAM RAJU | May | 1978 |
| 27 | DR.ASHA RANI KHANNA | May | 1979 |
| 28 | DR.RAVI RATTAN KASLIWAL | Dec | 1979 |
| 29 | DR.K.SRINATH REDDY | July | 1980 |
| 30 | DR.RAGHAVAN SUBRAMANYAN | July | 1980 |
| 31 | DR.AJAY KUMAR | Dec | 1980 |
| 32 | DR.JALAL-UD-DIN | Dec | 1980 |
| 33 | DR.PRABHAKARAN NARAYANASWAMY.S. | Dec | 1980 |
| 34 | DR.RAJINDER PRASAD BHAT | May | 1981 |
| 35 | DR.RAM BILAS MITTAL | May | 1981 |
| 36 | DR.IPPILIANNAJI VARAPRASADLAL | May | 1981 |
| 37 | DR.GOPISETTI SAI GOPAL | Dec | 1981 |
| 38 | DR.PANCHAPAKESAN RAMACHANDRAN | Dec | 1981 |
| 39 | DR.P.SESHAGIRI RAO | Dec | 1982 |
| 40 | DR.ARUN KUMAR SOOD | Dec | 1982 |
| 41 | DR.MADHOK RAMESH KUMAR | Dec | 1982 |
| 42 | DR.THOMAS TITUS | May | 1983 |
| 43 | DR.KRISHNASWAMY SUBRAMANYAN | May | 1983 |
| 44 | DR.JAGSIH CHANDER MOHAN | May | 1983 |
| 45 | DR.MRITYNJAYA BEHERA | Dec | 1983 |
| 46 | DR.SUMAN BHANDARI | Dec | 1983 |
| 47 | DR.RAVI SHANKAR SHARMA | Dec | 1984 |
| 48 | DR.SATDEV KARLOOPIA | Dec | 1984 |
| 49 | DR.SATISH KUMAR KAUSHIK | Dec | 1984 |
| 50 | DR.CHAKRAPANI SETHU NATH | May | 1985 |
| 51 | DR.GURCHARAN SINGH KALRA | Dec | 1985 |
| 52 | DR.JAGAT PRAKASH SINGH NARULA | Dec | 1985 |
| 53 | DR.SHYAM SUNDER | Dec | 1985 |
| 54 | DR.ANIL KUMAR BHARANI | May | 1986 |
| 55 | DR.S.RADHAKRISHNAN | Dec | 1986 |
| 56 | DR.VISHVA DEV | Dec | 1986 |
| 57 | DR.RAJEEV GUPTA | Dec | 1986 |
| 58 | DR.VISWANATHAN HARIHARAN | Dec | 1986 |
| 59 | DR.SHAYM SUNDER | May | 1987 |
| 60 | DR.RAMESH BABU POTHINENI | Dec | 1987 |
| 61 | DR.DAS GLADWIN SUSEEKAR | Dec | 1987 |
| 62 | DR.RAJIV BAJAJ | May | 1988 |
| 63 | DR.ASHOK GARG | May | 1988 |
| 64 | DR.L.SHYAMKISHORE SINGH | Dec | 1988 |
| 65 | DR.KEWAL CHAND GOSWAMI | Dec | 1988 |
| 66 | DR.BHAVANI DOGRA | May | 1989 |
| 67 | DR.M.VIJAYA KUMAR | May | 1989 |
| 68 | DR.SHIVA NARAAYAN SHARMA | May | 1989 |
| 69 | DR.PRAKASH CHAND NEGI | Dec | 1989 |
| 70 | DR. R.S.VASAN | Dec | 1989 |
| 71 | DR. TARUNKUMAR H. DAVE | May | 1990 |
| 72 | DR. T.KAMALAKAR | May | 1990 |
| 73 | DR. RAJIV NARANG | Dec | 1990 |
| 74 | DR. R.KRISHNA KUMAR | Dec | 1990 |
| 75 | DR. RAJIV AGARWAL | Dec | 1990 |
| 76 | DR. SATISH CHANDRA | Dec | 1990 |
| 77 | DR. Y.VENKATESWARA RAO | May | 1991 |
| 78 | DR. ATUL MATHUR | May | 1991 |
| 79 | DR. PRADEEP JAIN | May | 1991 |
| 80 | DR. GHANASHYAM BASUMATARY | Dec | 1991 |
| 81 | DR. SANJEEV SANGHVI | Dec | 1991 |
| 82 | DR. H.S.SOMANATH | Dec | 1991 |
| 83 | DR. S.RAMAMURTHY | May | 1992 |
| 84 | DR. D.PRABHAKARAN | May | 1992 |
| 85 | DR. SUDHIR | Dec | 1992 |
| 86 | DR. RAJNISH JUNEJA | May | 1993 |
| 87 | DR. SUBHASH CHANDRA | May | 1993 |
| 88 | DR. MANOJ SHARMA | May | 1993 |
| 89 | DR. ANUP KUMAR BORO | May | 1993 |
| 90 | DR. SANGEET SAHAI | Dec | 1993 |
| 91 | DR. DEEPAK THATAI | Dec | 1993 |
| 92 | DR. AJAY BHARGAVA | Dec | 1993 |
| 93 | DR. SHASHI SHEKHAR CHATTERJEE | Dec | 1993 |
| 94 | DR. SANJAY KUMAR CHUGH | May | 1994 |
| 95 | DR. PRASHANT TARAKANT UPASANI | May | 1994 |
| 96 | DR. PUNIT GOEL | May | 1994 |
| 97 | DR. SANJEEV SHARMA | May | 1994 |
| 98 | DR. ANIL KUMAR GOEL | May | 1995 |
| 99 | DR. RAJEEV GUPTA | Dec | 1995 |
| 100 | DR. DHANANJAY KUMAR JHAMB | Dec | 1995 |
| 101 | DR. B. SHARADA | Dec | 1995 |
| 102 | DR. PRAKASH KAMATH K | Dec | 1995 |
| 103 | DR. HANUMANTHU JAGANNAYAKULU | Dec | 1995 |
| 104 | DR. VISHWA VIBHUTI AGARWAL | Dec | 1995 |
| 105 | DR. AJAY MITTAL | May | 1996 |
| 106 | DR. SANDEEP SETH | May | 1996 |
| 107 | DR. DINESH SUDAN | May | 1996 |
| 108 | DR. RAKESH RAI SAPRA | Dec | 1996 |
| 109 | DR. VIKAS CHOPRA | Dec | 1996 |
| 110 | DR. MALIPEDDI BHASKARA RAO | May | 1997 |
| 111 | DR. ARUN KUMAR CHOPRA | May | 1997 |
| 112 | DR. SUNDEEP MISHRA | May | 1997 |
| 113 | DR. SHEKHAR SINGH KASHYA | May | 1997 |
| 114 | DR. RAMDEO YADAVE | Dec | 1997 |
| 115 | DR. N.C.KRISHNA MANI | Dec | 1997 |
| 116 | DR. BISHAV MOHAN | Dec | 1998 |
| 117 | DR. RAKESH YADAV | Dec | 1998 |
| 118 | DR. RAKESH CHAND JINDAL | Dec | 1998 |
| 119 | DR. NITISH NAIK | Dec | 1998 |
| 120 | DR. DHIRAJ GUPTA | May | 1999 |
| 121 | DR. PARTHO PRATIM SENGUPTA | May | 1999 |
| 122 | DR. MRIDUL SHARMA | Dec | 1999 |
| 123 | DR. KAVALIPATI NARASA RAJU | Dec | 1999 |
| 124 | DR. ANIL KUMAR SOOD | Dec | 1999 |
| 125 | DR. RAMRAO MANIKRAO GHODESWAR | Dec | 1999 |
| 126 | DR. HARMINDER SINGH | Dec | 1999 |
| 127 | DR. RAJIV ARORA | May | 2001 |
| 128 | DR. G. KARTHIKEYAN | May | 2001 |
| 129 | DR. ARVIND KOUL | May | 2001 |
| 130 | DR. SARITA GROVER | May | 2001 |
| 131 | DR. PRADEEP KUMAR HASIJA | May | 2002 |
| 132 | DR. YUSUF A | May | 2002 |
| 133 | DR. GAUTAM SHARMA | May | 2002 |
| 134 | DR. PARNEESH ARORA | May | 2002 |
| 135 | DR. SUNIL DWIVEDI | May | 2002 |
| 136 | DR.CHANDRA BHAN MEENA | Dec | 2002 |
| 137 | DR.NEIL BARDOLOI | Dec | 2002 |
| 138 | DR.DHOPESHWARKAR RAJESH ARVIND | Dec | 2002 |
| 139 | DR.KAMMARIPALLE CHANAKYA KISHORE KUMAR | Dec | 2002 |
| 140 | DR.ARUN MOHANTI | Dec | 2002 |
| 141 | DR.S.ANANDARAJA | Dec | 2002 |
| 142 | DR.DEEPAK | May | 2003 |
| 143 | DR.MAMTESH GUPTA | May | 2003 |
| 144 | DR. AMBUJ ROY | May | 2003 |
| 145 | DR.B.RAM PRAKASH | Dec | 2003 |
| 146 | DR. NARESH KUMAR GOYAL | Dec | 2003 |
| 147 | DR.S.RAMAKRISHNAN | May | 2004 |
| 148 | DR.JELAN SINGH | Dec | 2004 |
| 149 | DR.SUMODH KURIEN | Dec | 2004 |
| 150 | DR.HEMANT BEHERA | May | 2005 |
| 151 | DR.SANJEEV KUMAR SHARMA | May | 2005 |
| 152 | DR.RANJIT KR.NATH | May | 2005 |
| 153 | DR.DAVINDER SINGH CHADHA | May | 2005 |
| 154 | DR.MANOHAR SAKHARE | May | 2005 |
| 155 | DR.RAJIV MAHAJAN | Dec | 2005 |
| 156 | DR.AJAY DEEP BHATNAGAR | Dec | 2005 |
| 157 | DR.SANJEEV ASORTA | Dec | 2005 |
| 158 | DR.NAVIN MATHEW | Dec | 2005 |
| 159 | DR.VINEET MALIK | May | 2006 |
| 160 | DR.B.SHANKAR | May | 2006 |
| 161 | DR.AJAY GOPAL | May | 2006 |
| 162 | DR.PRABHAT | Dec | 2006 |
| 163 | DR.KAPIL | Dec | 2006 |
| 164 | DR.S.K.PATRA | Dec | 2006 |
| 165 | DR.RAVI MATH | May | 2007 |
| 166 | DR.NEERAJ | May | 2007 |
| 167 | DR.ANAND AGARWAL | Dec | 2007 |
| 168 | DR.VIVEK CHATURVEDI | Dec | 2007 |
| 169 | DR.NAGESH .C.M. | May | 2008 |
| 170 | DR.AJITH THATCHIL | May | 2008 |
| 171 | DR.RAJENDER THANGJAM | May | 2008 |
| 172 | DR.SHARAD CHANDRA | May | 2008 |
| 173 | DR.AMIT PENDARKAR | May | 2008 |
| 174 | DR.INDRA | Dec | 2008 |
| 175 | DR.PRALOY CHAKRABORTY | Dec | 2008 |
| 176 | DR.SAMEER | May | 2009 |
| 177 | DR.CHIRAYU | May | 2009 |
| 178 | DR.SURESH | May | 2009 |
| 179 | DR.BHARAT BHUSHAN KUKRETI | Dec | 2009 |
| 180 | DR.BHATT KINJAL N | Dec | 2009 |
| 181 | ISHWAR CHANDRA MALAV | Dec | 2009 |
| 182 | DR.NAVREET SINGH | Dec | 2009 |
| 183 | DR.AJAY KUMAR SHARMA | Dec | 2009 |
| 184 | DR.SAROJ KHANAL | May | 2010 |
| 185 | DR.HIMANSHU DABRAL | May | 2010 |
| 186 | DR.SHARATH KUMAR K | Dec | 2010 |
| 187 | DR.JAGDANAND JHA | Dec | 2010 |
| 188 | Dr. Om Murti Anil | May | 2011 |
| 189 | Dr. Pranab Deka | May | 2011 |
| 190 | Dr. Sunil Shivdas | May | 2011 |
| 191 | Dr. Salman Salahuddin | May | 2011 |
| 192 | Dr. Amit Malviya | Dec | 2011 |
| 193 | Dr. Mithun Jacob Varghese | Dec | 2011 |
| 194 | Dr. S. Nagendra Boopathy | Dec | 2011 |
| 195 | Dr. Ramandeep Singh Ahuja | May | 2012 |
| 196 | Dr. Jo Joseph | May | 2012 |
| 197 | Dr. Soumen Devi Dutta | May | 2012 |
| 198 | Dr. Nilkanth C. Patil | Dec | 2012 |
| 199 | Dr. Sudhir S. Shehkar | Dec | 2012 |
| 200 | Dr. Parag W. Barwad | Dec | 2012 |
| 201 | Dr. Naveen Khanna | May | 2013 |
| 202 | Dr. Akhilesh Dubey | May | 2013 |
| 203 | Dr. Doshi Shrenik R. | Dec | 2013 |
| 204 | Dr. Anand Gopal | Dec | 2013 |
| 205 | Dr. R. Ananthakrishnan | Dec | 2013 |
| 206 | Dr. Himanshu Gupta | May | 2014 |
| 207 | Dr. Varun Gupta | May | 2014 |
| 208 | Dr. Jeet Ram | May | 2014 |
| 209 | Dr. Kumar Vaibhav Vikash | May | 2014 |
| 210 | Dr. Cheruparambath Varun | Dec | 2014 |
| 211 | Dr. Vikas Thakran | Dec | 2014 |
| 212 | Dr. Birdevinder Singh | Dec | 2014 |
| 213 | Dr. Prashant Shah | Dec | 2014 |
| 214 | Dr. Abhinit Gupta | May | 2015 |
| 215 | Dr. Binay Kumar | May | 2015 |
| 216 | Dr. Ritesh Kumar Gupta | May | 2015 |
| 217 | Dr. Gajendra Dubey | Dec | 2015 |
| 218 | Dr. Basavaraj Utagi | Dec | 2015 |
| 219 | Dr. Ankit Jain | Dec | 2015 |
| 220 | Dr. Anunay Gupta | May | 2016 |
| 221 | Dr. Rajeev Sharma | May | 2016 |
| 222 | Dr. Deepti | Dec | 2016 |
| 223 | Dr. Suman Karmakar | Dec | 2016 |
| 224 | Dr. Malik Mohammad Azharuddin | May | 2017 |
| 225 | Dr. Danny Kumar | May | 2017 |
| 226 | Dr. Vijay Bohra | May | 2017 |
| 227 | Dr. Anand P. | May | 2017 |
| 228 | Dr. Sridharan. U | May | 2017 |
| 229 | Dr. Abhinav Aggarwal | Dec | 2017 |
| 230 | Dr. Abhishek Gupta | Dec | 2017 |
| 231 | Dr. Raghav Bansal | Dec | 2017 |
| 232 | Dr. Manish Pandey | Dec | 2017 |
| 233 | Dr. Dhara Singh | May | 2018 |
| 234 | Dr. Arvind Dambalkar | May | 2018 |
| 235 | Dr. Vikas Purohit | May | 2018 |
| 236 | Dr. Dinkar Bhasin | Dec | 2018 |
| 237 | Dr. Shanmugam K. | Dec | 2018 |
| 238 | Dr. Shaheer Almed A | Dec | 2018 |
| 239 | Dr. Preetam K | Dec | 2018 |
| 240 | Dr. Nirmal Ghati | Dec | 2018 |
| Sr.No. | Name | Designation |
|---|---|---|
| 1. | Mr. Ashok Kumar | PS |
| 2. | Ms. Rachna | PA |
Additional Professor R.No.3006, 3rd Floor Teaching Block | |
| Recent employment details | Additional Professor,since July 2020-Till date Associate Professor, since July 2017-June 2020 Assistant Professor,since June 2014-June 2017 |
| Research Interests | The research work is focused on TP53 tumor suppressor gene plays crucial role in suppression of cancer. But the mutation in p53 leads to tumour proliferation sometimes drug resistance cancer cells. The research focused on targeting mutant p53 with structure-based drug design to restore mutant p53 to functional like wild type. We do structure-based drug design by X-ray crystallography and for drug binding and functional studies we various biophysical techniques like ITC, CD, Fluorescence and cell based functional assay in p53 mutant cell lines. The second major project in our lab is antimicrobial drug development against drug resistant bacterial pathogen. We work on bacterial cell division proteins particularly FtsZ and its associate proteins involved forming divisome protein complex assembly. We do structure-based drug design by X-ray crystallography, In silico drug screening and for drug binding studies we various biophysical techniques like ITC, CD, Fluorescence. |
| Any additional information | Associate Professor (2017 - till date): Biophysics, AIIMS, New Delhi, India Assistant Professor (2014 – 2017): Biophysics, AIIMS, New Delhi, India Research Associate (2012-2014): Texas Tech University Health Science center, Texas, USA Post doctoral Fellow (2007 - 2012): University of California San Diego, California, USA. Ph.D. (Biophysics, 2007: AllMS, New Delhi Master of Science (Biophysics, 2002): University of Madras, Chennai Bachelor of Science (Physics -2000): University of Madras, Chennai Google scholar https://scholar.google.com/citations?user=KZJOecsAAAAJ&hl=en Pubmed https://www.ncbi.nlm.nih.gov/pubmed/?term=Ethayathulla+AS%5BAuthor%5D RCSB: |
| Awards and Honors | Senior Research Fellowship awarded by CSIR, New Delhi, India. Senior Research Fellowship in the project from DST, New Delhi, India. Junior Research Fellowship in the project from DST, New Delhi, India. Junior Research Fellowship in the project from DBT, New Delhi, India. |
| Recent Publications |
|
| Photograph |  |
| Current Designation & Contact Details | Professor Department of Biophysics, AIIMS, New Delhi Email: sharmistha_d[at]hotmail[dot]com Phone: +91-11-26546435 |
| Brief Research Area | Blood based biomarker of neurodegenerative diseases and cancers and their therapeutic intervention |
| Awards and Honours |
|
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?user=0OY1WIgAAAAJ&hl=en
|
Sh. OP Saini seen here being felicitated by both Chiefs. Sh. OP Saini worked as Accounts Officer at CN Centre for last 5 years and reverted to his parent department. Sh. NK Bajaj has taken over charge from Sh. OP Saini on 30th April, 2007.
Patients coming to the Cardiothoracic and Cardiology OPDs were benefited from Sh. Piar Singh’s plan to improve patient registration. This has abolished the long queue that were a normal feature for many years. The benefit has been enormous for patients who do not have to suffer by standing for many hours in all weather conditions.
Sh. Piar Singh deserves our applause
A well equipped orthoptic section runs at this centre. This also caters to the training of paramedical personnel (Ophthalmic Technicians). B.Sc. (Hons. in ophthalmology) students, who are given practical as well as theory training. It has all the sophisticated instruments used for diagnosis and therapy of ocular motility disorders (squint) and amblyopia.
The faculty and residents of the department undertake clinical projects assessing utility and advantages of new techniques in
Cardiovascular surgery. These are published as original articles in National and International indexed Journals. To date well over 200 papers in all aspects of Cardiovascular Surgery have been published. More than 350 papers have been presented in National and International Conferences both in India and Abroad.
Electrophysiology is an important tool for investigation in retinal diseases and neuro-ophthalmology. We have the latest equipment to perform visual evoked potential, electro retinography and MFERG. The lab caters to a large number of patients benefit from the OPD, clinics and wards. Provides useful information for diagnosis and management of several eye disorders.
| Photograph | |
| Current Designation & Contact Details | Professor Department of Biophysics, AIIMS, New Delhi Email: sharmistha_d[at]hotmail[dot]com Phone: +91-11-26546435 |
| Brief Research Area | Blood based biomarker of neurodegenerative diseases and cancers and their therapeutic intervention |
| Awards and Honours |
|
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?user=0OY1WIgAAAAJ&hl=en
|
Dr. R.P. Centre became the first Government Institution to initiate excimer laser surgery in the country. A state of the art laboratory for Excimer Laser refractive surgery was started in December, 1998 with the introduction of Chiron Vision (C-LASIK 217) laser machine. This is a sophisticated microsurgery used to alter the focusing power of the cornea using a laser beam and can be used for treatment of myopia, hyperopia and astigmatism. The primary aim of the surgery is to make the subject less dependent or free of spectacles. About 725 eyes of 367 patients have been operated till date with excellent visual results.
This web page is for the patients undergoing Coronary Artery Bypass Grafting (CABG). This web page attempts to explain the cause of the disease, the risk factors, the effects of disease and possible treatment options. It tells about the surgery, preoperative preparation and postoperative care in hospital and at home. Lastly, an effort has been made to spread preventive awareness about the coronary artery disease. For better understanding, at the cost of technical perfection, language has been made as simple as possible.
MD, MPH (USA), PGDHHM, FIPHA, FIAPSM
Room Number: 30
Centre For Community Medicine
Old OT Block
AIIMS, New Delhi - 110029
Phone: +91 (11) 26593773 (Direct)
+91(11) 26593233 (Office)
+91-9868397372 (Cell)
CRHSP-AIIMS,
Civil Hospital
Ballabgarh, Faridabad - 121004
Email:doctormisra@gmail.com
Dr. Puneet Misra is Professor of Community Medicine at the All India Institute of Medical Sciences. He has done his residency in Preventive Medicine. He has over twenty years of experience as Physician, Researcher, Teacher, Epidemiologist and Public Health professional. He has a rich experience of research and academics at various institutions in India and abroad. He has served as a member of the Executive Committee of Indian Association of Preventive and Social Medicine (IAPSM) for many years and was National President of IAPSM for year 2013-14 as the youngest president of organisation ever.
More than 100 peer reviewed and indexed publications, can see at google scholar ID doctormisra and available on the url: https://scholar.google.co.in/citations?hl=en&user=X6LhyWIAAAAJ
Was PI and Co PI in more than 50 studies funded by various organisations including Govt of india, WHO, Unicef, few of recent studies are
| Photograph |  |
| Current Designation & Contact Details | Professor Room No. 9, Department of Biophysics, AIIMS, New Delhi Email: sujatasharma[dot]aiims[at]gmail[dot]com; & sujatasharma[at]aiims[dot]edu Phone: +91-11-26594608 Wikipedia page : https://en.wikipedia.org/wiki/Sujata_Sharma |
| Brief Research Area | Antimicrobial therapeutics, Protein Structure based drug design, Nanomedicine. |
| Awards and Honours |
|
| Selected Publications/Patents (Last 5 years) |
List of Books:
|
This web page is for the patient who has a heart valve problem and who seeks treatment for the same. The web page describes in various chapters some of the fundamentals of blood circulation through the heart and the function of the valves and the effects of the disease.The web page also tells about the symptoms, tests that are used for diagnosis and after care. It tells about the surgery and postoperative care while the patient is in hospital. Finally it explains the aftercare when the patient is at home. For the purpose of better understanding, language has been made as simple as possible and efforts have been made to explain the facts in common language.
| Photograph | |
| Current Designation & Contact Details | Professor Room No. 9, Department of Biophysics, AIIMS, New Delhi Email: sujatasharma[dot]aiims[at]gmail[dot]com; & sujatasharma[at]aiims[dot]edu Phone: +91-11-26594608 Wikipedia page : https://en.wikipedia.org/wiki/Sujata_Sharma |
| Brief Research Area | Antimicrobial therapeutics, Protein Structure based drug design, Nanomedicine. |
| Awards and Honours |
|
| Selected Publications/Patents (Last 5 years) |
List of Books:
|
The faculty of the department perform 65 to 70 open heart surgical procedure per week from Monday through Saturday. In the year 1998 total number of open-heart surgeries performed was 2000 and closed heart surgeries was 600. The department is the only comprehensive facility in the country for all cardiovascular surgical procedures. These include correction of congenital cardiac malformation in newborn, infants and children, including complete correction for total anomalous Pulmonary venous connection, Transposition of Great Arteries, Tricuspid atresia, Univentricular heart, Truncus arteriosis etc. In addition simple congenital heart problems such as Atrial septal defects, Ventricular septal defects, Patent Ductus ateriosus. Coarctation of Aorta etc. are corrected routinely.
In the area of valvular heart surgery. The department offers prosthetic valve replacement, Mitral and Aortic valve repair, replacement of Aortic Valve with homgraft and Pulmonary autograft and repair of Tricuspid valve. The department has the only homograft valve bank with State-of-the-art cryopreservation techniques, and more than 600 homografts have been used so far.
In the area of Coronary artery bypass surgery, the department offers routine coronary artery bypass procedures with the use of saphenous vein, Interal mammary artery, radial artery etc. in addition selected patients undergo surgery without cardiopulmonary bypass and with minimally invasive techniques. Facility for Transmyocardial laser revascularisation is also available.
In the management of end stage heart disease cardiac transplantation, the first successful Orthotopic cardiac transplantation performed in India in this department in 1994. Subsequently several patients have undergone cardiac transplatation ad implantation of Ventricular Assist Devices, such as Thoratec and the Heart-Mate.
In the area of vascular surgery, aneurysms of the Ascending Aorta. Arch, descending and abdominal, aorta and management of vascular injuries are performed routinely.
Newer techniques such as Transesophageal echocardiography, cosmetic surgery, blood conservation are in routine use.
The department has trained over 80 cardiovascular surgeons in India. Postdoctoral course in Cardiovascular Surgery leading to the degree of M.Ch. (CTVS) provides training of Cardiovascular surgeons. The department has 12 senior Residents who are registered for the M.Ch. Course. The department also provides short term training to visiting residents and faculty from several National and International Centres. Comprehensive training in Extra Corporeal Circulation has also been provided to large number of candidates from other Institutions.
| MCH |
| M.Sc. (Perfusion Technology) |
| DM (Cardiac-Anaesthesia) |
| DM (Cardiology) |
Prof. Sandeep Chauhan, Chief, Cardio-Thoracic Sciences Centre
Prof. P. RAJASHEKAR Addl. Medical Superintendent
Obituary of Prof. Nagarur Gopinath, founder & first chief of Cardiothoracic Sciences Center
Cardiothoracic Sciences Centre began functioning in the new building in 1982. The Centre has 200 beds exclusively for Cardiology and Cardiovascular Surgery with all the ancilliary facilities required for comprehensive care for all cardiovascular disorders. In 1986 the Centre became fully independent and functioned entirely from the new 7 floor building. The Cardiothoracic Sciences Centre has the following departments.
Professor N. Gopinath was the founder and first Chief of Cardiothoracic Centre. He was followed by Professor M.L. Bhatia, Professor R. Tandon , Professor P. Venugopal, Professor A. Sampath Kumar, Professor Balram Airan and Professor Vinay Kumar Bahl.
There are eight fully equipped operating rooms with the state-of-art technology to carry out all kinds of complex cardiothoracic and vascular procedures 24X7 through out the year accessible and affordable to everyone. Total bed capacity (136) under CTVS in General ward is distributed in 1st, 4th, 5th and 6thfloors of Cardiothoracic sciences center of which
| Name | E-mail add | DESIGNATION |
|---|---|---|
| Dr. A.K.BISOI | drakbisoi[at]gmail[dot]com | Prof. & HOD (CTVS) |
| Dr. V.DEVAGOUROU | vdeva[at]hotmail[dot]com | Professor (CTVS) |
| Dr. SACHIN TALWAR | sachintalwar[at]hotmail[dot]com, drsachintalwar[at]gmail[dot]com | Professor (CTVS) |
| Dr. P. RAJASHEKAR | praja[at]aiims[dot]edu | Professor (CTVS) |
| Dr. MANOJ SAHU | drmanojsahu[at]gmail[dot]com | Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SARVESH PAL SINGH | sarveshpalsingh[at]gmail[dot]com | Additional Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. P.RAMESH MENON | rpmpgi[at]gmail[dot]com | Additional Professor Pediatrics (Neonatalogy) in CTVS |
| Dr. PRADEEP RAMAKRISHNAN | pradeep[dot]r[dot]reddy85[at]gmail[dot]com | Associate Professor (CTVS) |
| Dr. UMMED SINGH | drusd[at]yahoo[dot]com | Associate Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SUSHAMA GAYATRI B | sushama[dot]gayatri[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. NAVNITA KISKU | navnita[dot]kisku[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. AMITABH SATSANGI | indiactvs[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. MAYANK YADAV | drmayankctvs[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr.BHARATH.V | drbharathv[at]gmail[dot]com | Assistant Professor (CTVS) |
List of Faculty Members in the Department of Cardiology
| Name | Designation | Contact No/Email |
|---|---|---|
| Dr. Neeti Makhija | Professor & HOD | 9868398102 |
| Dr. Sandeep Chauhan | CHIEF, CTC | - |
| Dr. Poonam Malhotra kapoor | Professor | 9868398103 |
| Dr. Minati Choudhury | Professor | 9868398104 |
| Dr.Sambhnath Das | Professor | 9868398105 |
| Dr. Parag Gharde | Professor | 9868398106 |
| Dr. Suruchi Hasija | Professor | 9868398107 |
| Dr. Arindam Choudhury | Professor | 9868398107 |
| Name | Designation |
|---|---|
| Dr. Ruma Ray | Professor |
| Dr. Sudheer Kumar A | Professor |
| Name | Designation | Contact No/Email |
|---|---|---|
| Dr. Priya Jagia | Prof. & HOD | 9868398117 |
| Dr. Sanjeev Kumar | Additional Prof. | - |
| Dr. Niraj N.Pandey | Asstt. Prof. | - |
| Name | Designation |
|---|---|
| Dr. R. Lakshmy | Professor |
| Name | Designation |
|---|---|
| Dr. Sujata Mohanty(Stem Cell) | Professor |
| Name | Designation |
|---|---|
| Dr. Aarti Vij | Professor |
| Dr. Mede Charan Raj | Asstt. Professor |
| Name | Designation |
|---|---|
| Dr. Chetan Patal | Professor |
| Photograph |  |
| Current Designation & Contact Details | Professor Room No. 3004, 3rd Floor, Teaching Block Phone: +91-11-26596445 Email: savitayadav@aiims.edu; & savita11@gmail.com |
| Recent Employment Details (Past few years) |
|
| Brief Research Area | Proteomics, Biomarker discovery and Functional Biophysics:
|
| Award and Honours |
|
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?hl=en&user=Oh3WbL0AAAAJ
|
Professor, Centre for Community Medicine
Tele: 91-11-26594253
Email: kanand[at]aiims[dot]ac[dot]in; kanandiyer[at]yahoo[dot]com, anand[dot]drk[at]gmail[dot]com
Dr, Anand Krishnan has been in AIIMS faculty since 1994 and has spent more than 15 years as faculty in its rural field practice area at Ballabgarh and has been responsible for many initiatives including the use of digital solutions to health care.
| Photograph | |
| Current Designation & Contact Details | Professor Room No. 3004, 3rd Floor, Teaching Block Phone: +91-11-26596445 Email: savitayadav[at]aiims[dot]edu; & savita11[at]gmail[dot]com |
| Recent Employment Details (Past few years) |
|
| Brief Research Area | Proteomics, Biomarker discovery and Functional Biophysics:
|
| Award and Honours |
|
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?hl=en&user=Oh3WbL0AAAAJ
|
The retina lab is well equipped with the latest equipment for the diagnosis and management of several retinal disorders. There are modern equipments for fundus photography, digital angiography, ocular coherence tomography, wide-field imaging and angiography, MFERG, microperimetry, ultrasound biomicroscopy, posterior segment ultrasound, and Retcam examination for ROP.
The retina lab features top-of-the-line equipment for the laser treatment of various pathologies, with not onlyspot laser but also multi-spot laser delivery technology. The lab has advanced equipment which is helpful for retinal exports in diagnosis and management of a large number of retinal diseases.

| Current Designation & Contact Number | Professor & Head of the Department Phone: +91-11-26594288/3201 Email: punitkaur1[at]hotmail[dot]com, punitkaur[at]aiims[dot]edu |
| Brief Research Area | Bioinformatics, Structural Biology, X-ray Crystallography, and Rational Structure Based Drug Design. |
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?hl=en&user=SWeHXa4AAAAJPublications:
Recent Chapter in Book
|
DR. Rajendra Prasad Centre for Ophthalmic Sciences is the apex institute in India for ophthalmic care. Glaucoma facility is one of the main pillars of R P Centre. It has been providing the best and most advanced ophthalmic care to the patients for 45 years. Glaucoma being a silent thief of sight is a disease and our centre has taken equal effort and commitment of the ophthalmologist in educating the public about the disease and its consequences .
Our Glaucoma facility has a unique infrastructure and is able to provide a lifelong care and follow up to patients since they are enrolled in our glaucoma clinic. We have 3 eminent faculty members in charge of the glaucoma services, with 3 glaucoma clinics a week and a glaucoma facility lab which runs all week days. Our specialty glaucoma clinic on an average provides services to 2500 new patients and 6300 old patients. Residents assist the faculty members in providing necessary care to the glaucoma patients. The glaucoma lab has 3 optometrists trained in ophthalmic investigations, especially pertaining to glaucoma .
The faculty in new glaucoma clinic confirms the diagnosis of glaucoma and initiates the treatment for the patients who were screened and referred from outpatient department. These patients are then followed up in the old glaucoma clinic as required. The glaucoma lab has all the advanced diagnostic modalities namely HRT. GDx,HVF,GVF,OCT,ASOCT, UBM, tonometer,keratometer, pachymeter.

A new cornea laboratory has been started this year (2000). It is equipped with the latest state-of-art equipment used for examination of various corneal disorders. These include :
Several Paraclinical Services are provided at RP Centre to augment the clinical services. RPC has dedicated departments of Ocular Biochemistry, Ocular Pathology, Ocular Microbiology, and Ocular Pharmacology.
| Name | E-mail Add | Designation |
|---|---|---|
| Dr. A. K. BISOI | drakbisoi[at]gmail[dot]com | Professor and Head of the Department(CTVS) |
| DR. V.DEVAGOUROU | vdeva[at]hotmail[dot]com | Professor(CTVS) |
| Dr. SACHIN TALWAR | sachintalwar[at]hotmail[dot]com, drsachintalwar[at]gmail[dot]com | Professor(CTVS) |
| Dr. P. RAJASHEKAR | praja[at]aiims[dot]edu | Professor (CTVS) |
| Dr. MANOJ SAHU | drmanojsahu[at]gmail[dot]com | Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SARVESH PAL SINGH | sarveshpalsingh[at]gmail[dot]com | Additional Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr.P.RAMESH MENON | rpmpgi[at]gmail[dot]com | Additional Professor Pediatrics (Neonatalogy) in CTVS |
| Dr. PRADEEP RAMAKRISHNAN | pradeep[dot]r[dot]reddy85[at]gmail[dot]com | Associate Professor (CTVS) |
| Dr. UMMED SINGH | drusd[at]yahoo[dot]com | Associate Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SUSHAMA GAYATRI B | sushama[dot]gayatri[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. NAVNITA KISKU | navnita[dot]kisku[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. AMITABH SATSANGI | indiactvs[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr. MAYANK YADAV | drmayankctvs[at]gmail[dot]com | Assistant Professor (CTVS) |
| Dr.BHARATH.V | drbharathv[at]gmail[dot]com | Assistant Professor (CTVS) |
Holter monitoring is a procedure during which ECG of the patient is continuously recorded over a 24 hour period. For this purpose, leads are placed on the chest and attached to a small unit which patient can keep in his pocket. The patient can then go home and do his/her normal daily activities. The patient has to come back the next day to have the holter unit removed. A diary is also given to the patient where he can make a note of any complaints (giddiness, palpitations, chest pain etc) along with the exact time. The ECG is later analyzed for any abnormalities during this 24 hour period.
After you receive the form for Holter from your consultant in OPD, you can go to room number 48 (9am to 4pm) for an appointment. The patients need to come at 9am on the appointed day. A fees of Rs 300/- needs to be deposited to the cash counter before the procedure. This can be done on any day between 9 am and 8 pm at the cash counter (room number 28-b).
Treadmill test or TMT is done to determine if the heart muscle is getting adequate blood supply during periods of exertion. The patients walk on a treadmill the speed and slope of which increases every 3 minutes. The ECG, blood pressure etc are continuously monitored during the procedure. If the patients feel any discomfort they should tell the doctor and the exercise can be stopped at any time.
After you receive the form for Treadmill test from your consultant in OPD, you can go to room number 48 (9am to 4pm) for an appointment. The patients need to come at 9am on the appointed day. A fees of Rs 300/- needs to be deposited to the cash counter before the procedure. This can be done on any day between 9 am and 8 pm at the cash counter (room number 28-b).
Cardiac cath is a procedure done in cath lab in which thin long tubes are inserted into arteries and veins of upper thigh and advanced to reach the heart. The pressures in different chambers of the heart are recorded and radio-opaque contrast material is injected so as to visualize the heart chambers and blood vessels using X-rays. Using this procedure many heart diseases can be diagnosed and treated. Angioplasty and valve dilatation are extension of the same procedure.
The patients are advised to come to room number 5 or 28 in OPD on one day prior to the procedure at 4pm (called “cath selection”). They should deposit the fees for the procedure before coming at the cash counter (room number 28-b between 9am and 8pm). At the time of cath selection, the patients are given instructions about the procedure. Their ECG, Chest X-ray and blood test may be done at this time. The patients then go back home and come the next day at 8am to the “cath lab”. The patients should be fasting on this day. The morning dose of medicines should be taken with a small amount of water before 7am on the day of cath.
Echocardiography is done to visualize the heart directly, to measure dimensions of important structures, to assess function of different chambers, to assess flow across different valves and for many other parameters. It is a very important investigation for patients with congenital, valvular, coronary and most other heart diseases. For most procedures one can get all information by placing a plastic probe (transducer) on the chest wall (Transthoracic echocardiography). However, sometimes visualization is not sufficient with this and a ‘Transesophageal echocardiography’ is needed.
After you receive the form for Echo test from your consultant in OPD, you can go to room number 48 (9am to 4pm) for an appointment. A fees of Rs 100/- needs to be deposited to the cash counter before the procedure. This can be done on any day between 9 am and 8 pm at the cash counter (room number 28-b). The patients need to come to Echo lab on the appointed day and time. Fasting is needed only for transesophageal echocardiography.
Several Paraclinical Services are provided at RP Centre to augment the clinical services. RPC has dedicated departments of Ocular Biochemistry, Ocular Pathology, Ocular Microbiology, and Ocular Pharmacology.
Professor,
MBBS from LHMC, Delhi (Delhi University) in 1984, MD (Preventive and Social Medicine) from Delhi University in 1988, DNB – MCH (NBE, Delhi), DIM (IGNOU Delhi).
Worked as Lecturer and Reader in Community Medicine at Mahatma Gandhi Institute of Medical Sciences, Sevagram, Wardha, 1991 - 1993.
Worked as Assistant Professor at JIPMER, Pondicherry, 1993.
Faculty, AIIMS since 24/10/93. Worked at CRHSP Ballabgarh and CCM (1997 onwards )
Participated in First National Review of Immunisation Coverage conducted by National Institute of Health and Family Welfare in May 1989as a District Team Member and immunization surveys in Delhi 1987-90.
Member of IPEN, Inclen Resource person for Model Injection Centre Program and India Population Stabilisation Fund.
The Centre has a minor operation theatre for ward patients. The main operation theatres are equipped with all types of specialised instruments for surgery including keratoplasty, retinal detachment, ophthalmoplasty, squint, besides glaucoma, cataract etc. The operation theatre is equipped with operating microscopes and is fitted with a closed circuit T.V. system. Besides other operative appliances, it is also equipped for vitrectomy and lensectomy operations. Phaco emulsification is being used for cataract surgery. As a no stitch/one stitch technique is used, an earlier rehabilitation of patients is generally possible.
There are 300 beds including casualty beds. Of these 4 beds are reserved for E.H.S.beneficiaries, 15 for emergency cases, 3 under Chief's pool and 20 paying ward rooms.
A wing exclusively meant for paediatric patients has been functioning on the 4th floor. The creation of this special paediatric ward emphasises the importance given to the treatment of eye diseases in children.
| Current Designation & Contact Number | Professor & Head of the Department Phone: +91-11-26594288/3201 Email: punitkaur1[at]hotmail[dot]com, punitkaur[at]aiims[dot]edu |
| Brief Research Area | Bioinformatics, Structural Biology, X-ray Crystallography, and Rational Structure Based Drug Design. |
| Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?hl=en&user=SWeHXa4AAAAJPublications:
Recent Chapter in Book
|
 | |
| Designation | SERB Distinguished Fellow |
| tpsingh[dot]aiims[at]gmail[dot]com | |
| Contact Number | +91-11-26588931 |
| Brief Research Area | Structural Biology; Biological Crystallography, Protein Structure Determination and Peptide Design; Rational Structure Based Drug Design |
| Awards and Honors | Fellowships of Academies/Societies:
|
Awards and Honours:
| |
Member of Governing/Research Councils:
| |
Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?hl=en&user=7j3K6wYAAAAJ
|
Fifteen specialty clinics are run in the afternoon which cater to the specific problems of cases requiring investigations and eye care. In these clinics patients are examined, investigated and treated for the specific diseases related to sub-specialties. Here every patient gets the advice of an expert in the field of ophthalmology. After the treatment, patients are referred back to their treating doctor.
| |
| Designation | SERB Distinguished Fellow |
| tpsingh[dot]aiims[at]gmail[dot]com | |
| Contact Number | +91-11-26588931 |
| Brief Research Area | Structural Biology; Biological Crystallography, Protein Structure Determination and Peptide Design; Rational Structure Based Drug Design |
| Awards and Honors | Fellowships of Academies/Societies:
|
Awards and Honours:
| |
Member of Governing/Research Councils:
| |
Selected Publications/Patents (Last 5 years) | Google Scholar Link: https://scholar.google.com/citations?hl=en&user=7j3K6wYAAAAJ
|
Daily forty cabins are run to provide the ophthalmic services in the Out Patient Department. A special cell for refraction has been created to provide prescription for glasses.
The special feature of the O.P.D. is an appointment system. Every patient is given an approximate appointment time for examination and alloted to a doctor for advice and follow up
A new extension OPD with six clinical examination chambers with refraction facility has been added since 2014.
The special features of the Hospital services are :
Round the Clock Emergency Service which includes :
The Centre runs its own Casualty service, where the emergency cases and those patients who come after O.P.D. hours are attended. A junior resident, senior resident and a consultant are available round the clock. There are 15 beds earmarked for Casualty cases. The Casualty wing has an attached operation theatre. Realising the importance of ocular infections as an ocular disaster, an 'Ocular Infection Cell' has been created in the Casualty area which provides immediate investigative support and urgent meticulous treatment in corneal ulcer cases and other cases of ocular infection.
Holter monitoring is a procedure during which ECG of the patient is continuously recorded over a 24 hour period. For this purpose, leads are placed on the chest and attached to a small unit which patient can keep in his pocket. The patient can then go home and do his/her normal daily activities. The patient has to come back the next day to have the holter unit removed. A diary is also given to the patient where he can make a note of any complaints (giddiness, palpitations, chest pain etc) along with the exact time. The ECG is later analyzed for any abnormalities during this 24 hour period.
After you receive the form for Holter from your consultant in OPD, you can go to room number 48 (9am to 4pm) for an appointment. The patients need to come at 9am on the appointed day. A fees of Rs 300/- needs to be deposited to the cash counter before the procedure. This can be done on any day between 9 am and 8 pm at the cash counter (room number 28-b).
Treadmill test or TMT is done to determine if the heart muscle is getting adequate blood supply during periods of exertion. The patients walk on a treadmill the speed and slope of which increases every 3 minutes. The ECG, blood pressure etc are continuously monitored during the procedure. If the patients feel any discomfort they should tell the doctor and the exercise can be stopped at any time.
After you receive the form for Treadmill test from your consultant in OPD, you can go to room number 48 (9am to 4pm) for an appointment. The patients need to come at 9am on the appointed day. A fees of Rs 300/- needs to be deposited to the cash counter before the procedure. This can be done on any day between 9 am and 8 pm at the cash counter (room number 28-b).
Cardiac cath is a procedure done in cath lab in which thin long tubes are inserted into arteries and veins of upper thigh and advanced to reach the heart. The pressures in different chambers of the heart are recorded and radio-opaque contrast material is injected so as to visualize the heart chambers and blood vessels using X-rays. Using this procedure many heart diseases can be diagnosed and treated. Angioplasty and valve dilatation are extension of the same procedure.
The patients are advised to come to room number 5 or 28 in OPD on one day prior to the procedure at 4pm (called “cath selection”). They should deposit the fees for the procedure before coming at the cash counter (room number 28-b between 9am and 8pm). At the time of cath selection, the patients are given instructions about the procedure. Their ECG, Chest X-ray and blood test may be done at this time. The patients then go back home and come the next day at 8am to the “cath lab”. The patients should be fasting on this day. The morning dose of medicines should be taken with a small amount of water before 7am on the day of cath.
Echocardiography is done to visualize the heart directly, to measure dimensions of important structures, to assess function of different chambers, to assess flow across different valves and for many other parameters. It is a very important investigation for patients with congenital, valvular, coronary and most other heart diseases. For most procedures one can get all information by placing a plastic probe (transducer) on the chest wall (Transthoracic echocardiography). However, sometimes visualization is not sufficient with this and a ‘Transesophageal echocardiography’ is needed.
After you receive the form for Echo test from your consultant in OPD, you can go to room number 48 (9am to 4pm) for an appointment. A fees of Rs 100/- needs to be deposited to the cash counter before the procedure. This can be done on any day between 9 am and 8 pm at the cash counter (room number 28-b). The patients need to come to Echo lab on the appointed day and time. Fasting is needed only for transesophageal echocardiography.
| Title | Download | Unit |
|---|---|---|
| Unit I | Unit II | Unit III |
Dr. Sudarshan Khokhar, Prof. of Ophth. Dr. Pradeep Venkatesh,Prof. of Ophth. Dr. Shorya Vardhan Azad, Assoc. Prof. Dr. Amar Pujari, Asstt. Prof. Dr. Saurabh Verma, Asstt. Prof. Dr. Devesh Kumawat, Asstt. Prof. | Dr. Raj Pal, Prof. of Ophth. Dr. Viney Gupta, Prof. of Ophth. Dr. Parijat Chandra, Prof. of Ophth. Dr. Rohan Chawla, Addl. Prof. Dr. Vinod Kr. Agarwal, Addl. Prof. Dr. Shikha Gupta, Assoc. Prof. | Dr. Jeewan.S.Titiyal(Chief) Prof. of Ophth. Dr.Tushar Agarwal, Prof. of Ophth. Dr. Rajesh Sinha, Prof. of Ophth. Dr. Manpreet Kaur, Asstt. Prof. Dr. Sridevi Nair, Asstt. Prof. |
| Unit IV | Unit V | Unit VI |
Dr. Namrata Sharma, Prof. of Ophth. Dr.Tanuj Dada, Prof. of Ophth. Dr. Dewang Angmo, Assoc. Prof. Dr. Prafulla Maharana, Assoc. Prof. Anu Malik, Asstt. Prof. Dr. Karthikeyan M., Asstt. Prof. | Dr. Mandeep S.Bajaj , Prof. of Ophth. Dr. Neelam Pushkar, Prof. of Ophth. Dr.. Rohit Saxena, Prof. of Ophth. Dr. Swati Phuljhele Ashok, Addl. Prof. Dr. Rachna Meel, Addl. Prof. Dr. Rebika, Asstt. Prof. Dr. Sahik Agrawal, Asstt. Prof. | Dr. Radhika Tandon, Prof. of Ophth. Dr. M.Vanathi, Prof. of Ophth. Dr. Bhavna Chawla, Prof. of Ophth. Dr. Noopur Gupta, Addl. Prof. Dr. Neiwete Lomi, Assoc. Prof. |
| Title | Download |
|---|---|
| Ocular Biochemistry | Ocular Pharmacology |
Dr. Jasbir Kaur, Prof. of Ocul. Biochem. Dr. Alok Kumar Ravi, Prof. of Ocul. Biochem. | Dr. T. Velpandian, Prof. of Ocul. Pharmacology Dr. Nabanita Halder, Prof. of Ocul. Pharmacology |
| Ocular Microbiology | Ocular Pathology |
Dr. Nishat Hussain Ahmed, Addl. Prof. of Ocul. Micro. Dr. Karnika Saigal, Asstt. Prof. of Ocul. Micro. | Dr. Seema Sen, Prof. of Ocul. Pathology Dr. Seema Kashyap, Prof. of Ocul. Pathology |
| Community Services | Anaesthesiology |
Dr. Praveen Vashist, Prof. of Comm. Ophth. Dr. Suraj Singh Senjam , Prof. of Comm. Ophth. Dr. Vivek Gupta, Addl. Prof. of Comm. Ophth. | Dr. Dilip Shende, Prof. of Anaesth. Dr. Renu Sinha, Prof. of Anaesth. Dr. Kanil Ranjith Kumar, Asso. Prof. of Anaesth. Dr. Arshad Ayub, Asso. Prof. of Anaesth. |
| Radio-Diagnosis | Medical Superintendent |
| Dr. Sanjay Sharma, Prof. of Radio-Diagno. | Dr. D. K. Sharma, Prof. |
| Ward | Location | Comment |
|---|---|---|
| CT2 ward / CCU (coronary care unit) | Second floor of Cardio-thoracic centre | Patients needing intensive cardiac care are admitted here. |
| CT3 ward / Main cardiology ward | Third floor of Cardio-thoracic centre | Patients aged more than 12 years are admitted here. |
| CT6 ward / Pediatric cardiology ward | Sixth floor of Cardio-thoracic centre | Children aged 12 years or younger are admitted here. |
| Ward | Location | Comment |
|---|---|---|
| CT2 ward / CCU (coronary care unit) | Second floor of Cardio-thoracic centre | Patients needing intensive cardiac care are admitted here. |
| CT3 ward / Main cardiology ward | Third floor of Cardio-thoracic centre | Patients aged more than 12 years are admitted here. |
| CT6 ward / Pediatric cardiology ward | Sixth floor of Cardio-thoracic centre | Children aged 12 years or younger are admitted here. |
REGISTRATION TIME (OLD CASE: - 8:00 AM TO 11:30 AM)
(NEW CASES: - 11:30 AM TO 1:30 PM)
| DOCTOR’S NAME | MONDAY ROOM NO. | WEDNESDAY ROOM NO. | FRIDAY ROOM NO. |
|---|---|---|---|
| Prof. R. Narang | 19 | - | 19 |
| Prof. S. Seth | 8 | - | 8 |
| Prof. R. Yadav | - | 11 | 11 |
| Prof. N. Naik | 12 | 12 | - |
| Prof. S. Singh | 15 | 15 | - |
| Prof. G. Karthikeyan | - | 7 | 7 |
| Prof. Gautam Sharma | - | 19 | 17 |
| Prof. S. Ramakrishnan | 21 | - | 12 |
| Prof. Ambuj Roy | - | 10 | 10 |
| Dr. Saurabh Kumar Gupta | 18 | - | 18 |
| Dr. Deepti Siddharthan | 11 | 13 | - |
| Dr. Satyavir Yadav | 13 | - | 13 |
Senior residents are available in other rooms.
MORNING CLINIC ARRTHYTHMIA CLINIC (WEDNESDAY) REGISTRATION TIME: 9.00AM TO 10.00PM | AFTERNOON CLINIC CORONARY CLINIC (THURSDAY) REGISTRATION TIME: 1.00PM TO 2.00PM | ||
|---|---|---|---|
| CONSULTANTS NAME | ROOM NO | CONSULTANTS NAME | ROOM NO |
| DR. N. NAIK | 21 | DR. R. NARANG | 01 |
| DR. RAKESH YADAV | 20 | ||
| DR. GAUTAM SHARMA | 17 | ||
| DR. DEEPTI SIDHARTHAN | 19 | ||
| CARDIOLOGY CLEARANCE CLINIC (THURSDAY) | |||
| DR. DEEPTI SIDHARTHAN /DR SATYAVIR YADAV | 02 | ||
| HYPERTENSION CLINIC (THURSDAY) | HEART MUSCLE CLINIC (THURSDAY) | ||
| DR. AMBUJ ROY | 15 | DR. S. SETH | 04 |
| DR. SATYAVIR YADAV | 05 | ||
| ADULT CHD CLINIC (THURSDAY) | PROSTHETIC HEART VALVE CLINIC (THURSDAY) | ||
| DR. S. RAMAKRISHNAN | 17 | DR. S. SINGH | 13 |
| DR. G. KATHIKEYAN | 08 | ||
| CARDIOLOGY CLEARANCE CLINIC (THURSDAY) | |||
DR. DEEPTI SIDHARTHAN /
DR SATYAVIR YADAV | 10 |
REGISTRATION TIME (OLD CASE: - 8:00 AM TO 11:30 AM)
(NEW CASES: - 11:30 AM TO 1:30 PM)
| DOCTOR’S NAME | MONDAY ROOM NO. | WEDNESDAY ROOM NO. | FRIDAY ROOM NO. |
|---|---|---|---|
| Prof. R. Narang | 19 | - | 19 |
| Prof. S. Seth | 8 | - | 8 |
| Prof. R. Yadav | - | 11 | 11 |
| Prof. N. Naik | 12 | 12 | - |
| Prof. S. Singh | 15 | 15 | - |
| Prof. G. Karthikeyan | - | 7 | 7 |
| Prof. Gautam Sharma | - | 19 | 17 |
| Prof. S. Ramakrishnan | 21 | - | 12 |
| Prof. Ambuj Roy | - | 10 | 10 |
| Dr. Saurabh Kumar Gupta | 18 | - | 18 |
| Dr. Deepti Siddharthan | 11 | 13 | - |
| Dr. Satyavir Yadav | 13 | - | 13 |
Senior residents are available in other rooms.
MORNING CLINIC ARRTHYTHMIA CLINIC (WEDNESDAY) REGISTRATION TIME: 9.00AM TO 10.00PM | AFTERNOON CLINIC CORONARY CLINIC (THURSDAY) REGISTRATION TIME: 1.00PM TO 2.00PM | ||
|---|---|---|---|
| CONSULTANTS NAME | ROOM NO | CONSULTANTS NAME | ROOM NO |
| DR. N. NAIK | 21 | DR. R. NARANG | 01 |
| DR. RAKESH YADAV | 20 | - | |
| DR. GAUTAM SHARMA | 17 | ||
| DR. DEEPTI SIDHARTHAN | 19 | ||
| - | CARDIOLOGY CLEARANCE CLINIC (THURSDAY) | ||
| - | DR. DEEPTI SIDHARTHAN/ DR SATYAVIR YADAV | 02 | |
| HYPERTENSION CLINIC (THURSDAY) | HEART MUSCLE CLINIC (THURSDAY) | ||
| DR. AMBUJ ROY | 15 | DR. S. SETH | 04 |
| DR. SATYAVIR YADAV | 05 | ||
| ADULT CHD CLINIC (THURSDAY) | PROSTHETIC HEART VALVE CLINIC (THURSDAY) | ||
| DR. S. RAMAKRISHNAN | 17 | DR. S. SINGH | 13 |
| - | DR. G. KATHIKEYAN | 08 | |
| CARDIOLOGY CLEARANCE CLINIC (THURSDAY) | - | ||
| DR. DEEPTI SIDHARTHAN / DR SATYAVIR YADAV | 10 | ||
SENIOR RESIDENTS ARE AVAILABLE IN OTHER ROOMS.

Address: Room no 4007,
4th Floor, Convergence Block,
Department of Biochemistry,
All India Institute of medical Sciences, New Delhi
Phone: +91-11-26549235
Email id: kchosdol[at]gmail[dot]com, kunzangchosdol[at]yahoo[dot]com
Degree
| Subject
| University/ Institution
| Year
|
|---|---|---|---|
PhD
| Biochemistry
| AIIMS, New Delhi
| 2007
|
MD
| Biochemistry
| AIIMS, New Delhi
| 1999
|
MBBS & Internship
| Medicine
| Bundhelkhand University, Jhansi, UP
| 1995
|
Position
| Department
| University/ Institution
| Dates
|
|---|---|---|---|
Professor
| Biochemistry
| All India Institute of Medical Science, New Delhi
| 2014- Till date
|
Additional Professor
| Biochemistry
| All India Institute of Medical Science, New Delhi
| 2010-2014
|
Associate Professor
| Biochemistry
| All India Institute of Medical Science, New Delhi
| 2007-2010
|
Assistant Professor
| Biochemistry
| All India Institute of Medical Science, New Delhi
| 2003-2007
|
Senior Demonstrator
| Biochemistry
| All India Institute of Medical Science, New Delhi
| 2000-2003
|
Presently, we are working to understand the molecular interactions between the oncogene FAT1 and other crucial signalling molecules like p53 and b-catenin in glioma; Understanding the regulation of FAT1 expression; FAT1 regulated miRNA signature in hypoxic glioma and effect of cytotoxic drugs on glioma cells after FAT1 modulation.
1. Madan E, Dikshit B, Gowda SH, Srivastava C, Sarkar C, Chattopadhyay P, Sinha S, Chosdol K (2016) FAT1 is a novel upstream regulator of HIF1α and invasion of high grade glioma. Int J Cancer. 2016 Aug 18. doi: 10.1002/ijc.30386. [Epub ahead of print]
2. Jalota A, Kumar M, Das BC, Yadav AK, Chosdol K, Sinha S (2016) Synergistic increase in efficacy of a combination of 2-deoxy-D-glucose and cisplatin in normoxia and hypoxia: switch from autophagy to apoptosis. Tumour Biol. 2016 Jun 15. [Epub ahead of print]
3. Bhardwaj M, Sen S, Sharma A, Kashyap S, Chosdol K, Pushker N, Bajaj MS, Bakhshi S (2015) ZEB2/SIP1 as novel prognostic indicator in eyelid sebaceous gland carcinoma. Hum Pathol. 2015 Oct;46(10):1437-42
4. Irshad K, Mohapatra SK, Srivastava C,Garg H, Mishra S, Dikshit B, Irshad K, Mohapatra SK, Srivastava C,Garg H, Mishra S, Dikshit B, Sarkar C, Gupta D, Chandra PS, Chattopadhyay P, Sinha S, Chosdol K (2015) A Combined Gene Signature of Hypoxia and Notch Pathway in Human Glioblastoma and Its Prognostic Relevance. PLoS One. 2015 Mar 3;10(3):e0118201.
5. Jayaraj P, Sen S, Sharma A, Chosdol K, Kashyap S, Rai A, Pushker N, Bajaj M. (2015) Eyelid sebaceous carcinoma: a novel mutation in lymphoid enhancer-binding factor 1 (LEF1). Br J Dermatol. 2015 Sep;173(3): 811-4.
6. Chingkheilemba M, Kumar U, Chosdol K, Das N (2014). Lack of role of endothelial nitric oxide synthase gene Glu298Asp polymorphism in rheumatoid arthritis among Asian Indians. IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) 2014; 13( 4): 25-28.
7. Dikshit B, Irshad K, Madan E, Aggarwal N, Sarkar C, Chandra PS, Gupta DK, Chattopadhyay P, Sinha S, Chosdol K (2013). FAT1 acts as an upstream regulator of oncogenic and inflammatory pathways, via PDCD4, in glioma cells. Oncogene. 2013 Aug 15;32(33):3798-808.
8. Agarwal S, Sharma MC, Jha P, Pathak P, Suri V, Sarkar C, Chosdol K, Suri A, Kale SS, Mahapatra AK, Jha P (2013). Comparative study of IDH1 mutations in gliomas by immunohistochemistry and DNA sequencing. Neuro Oncol. 2013 Jun;15(6):718-26.
9. Chosdol K, Misra A, Puri S, Srivastava T, Sarkar C, Mahapatra AK and Sinha S (2009) Frequent LOH and altered expression of tumor supressor FAT identified by RAPD in astrocytic tumors. BMC Cancer 9:5
10. Srivastava T, Chosdol K, Chattopadhyay P, Mahapatra AK, Sarkar C, Sinha S (2007) Frequent loss of heterozygosity encompassing the hMLH1 locus in low grade astrocytic tumors. J Neuro-oncol. Feb;81(3):249-55.
DST; DRDO; DBT; IMRG (AIIMS).

Dr. KhushbooIrshad completed her PhD at the Department of Biochemistry, AIIMS, New Delhi, in 2013 under the supervision of Prof. Kunzang Chosdol, Prof. Subrata Sinha and Prof. P. Chattopadhyay. Her thesis involved the study of correlation between hypoxia and Notch signaling pathway in glioblastoma and identification of a combined gene signature to predict the survival of glioblastoma patients. Her work derived a key prognostic molecular cluster characteristic of the Notch pathway response in hypoxic glioblastoma tumors and gliomasphere cultures (PLoS One (2015); 10(3):e0118201; felicitated with AIIMS Excellence Research Award-2015 that was awarded to Prof. Chosdol). Presently, her research focuses on deciphering the role of FAT1, a novel gene implicated in glioma, in regulating the hallmark features of glioma like stemness and invasiveness, as well as in maintenance of the balance between pro-inflammatory and anti-inflammatory signaling in glioma. She was awarded the DST-SERB Start-Up Research Grant in March 2016, for the project aimed at elucidation of FAT1 function in modulating pro-inflammatory signaling and anti-inflammatory / immunosuppressive signaling pathways in glioma.

Dr. Srinivas H done MBBS from Bangalore Medical college, Rajiv gandhi university of health sciences Karnataka and MD from MAULANA AZAD Medical College, Delhi university, New Delhi. His MD thesis was on procalcitonin, IL 6, TNFalpha and urinary isoprostane in sepsis patients under the guidance of ex HOD and director professor Dr TK Mishra. He has completed one year of senior residency in PGIMER, Chandigarh and two year of senior residency in AIIMS, New Delhi. He has published his work in national and international papers in the various field of sciences and medical education. He is working now on pathway analysis of interaction between FAT1 with p53, HIF 1alpha and beta catenin in glioma as a PhD research scholar under the guidance of Dr KUNZANG CHOSDOL and Dr SUBRATA SINHA. He has done DNB from Diplomate of National Board in biochemistry and certification course in industry program, clinical trials and administration from bioinformatics institute of India. He is a Life member of Association of Medical Biochemistry of India since 2008
Life member of Society for Tissue Engineering and Regenerative Medicine (India),Thiruvananthapuram since 2010 and Indian Association of Cancer Research.

Ms. Chitrangda Srivastava is currently in her final year of PhD. She is working on the characterization of FAT1 gene promoter. In addition, she is analyzing the functional role of FAT1 with EMT and stemness in hypoxic glioma. She completed her M.Sc. from the department of Biochemistry, AIIMS, in 2012. Her M.Sc. thesis involved the study of the role of Notch signalling pathway with EMT and stemness in pathogenesis of glioma under hypoxia. She has won several awards during her PhD tenure, including Best Oral Presentation Award in ACOS-2016, European Young Scientist Travel Award-2015, G.P. Talwar Foundation Travel Award-2015, etc. She is an Associate Member of the American Association of Cancer Research since 2011 and an Associate Member of the European Society of Neuro-Oncology since 2016.

Nargis Malik completed her M.Sc. in toxicology from Meerut University, Currently she is a second year PhD. student working on the “Role of FAT1 gene on the regulation of microRNAs in glioma”
Akankshakanojia has completed her B.Sc.(H) in Biomedical Sciences from Acharya Narendra Dev College, University of Delhi in 2016. She is currently pursuing M.Sc. in Biochemistry from All India Institute of Medical Science, Delhi under the guidance of Dr. Kunzang Chosdol.

Mukesh Kumar is working as a Laboratory Attendant Gr.-II in the Department of Biochemistry since August 2011. He help in the research related work for M.Sc., Ph.D. and M.D. Students in Research Laboratory of Dr. Parthaprasad Chattopadhyay & Dr. Kunzang Chosdol. His nature of duties includes, culture work, DEPC treatment and assistance of UG/PG examination.
DEPARTMENT OF CARDIOLOGYALL INDIA INSTITUTE OF MEDICAL SCIENCESTeaching Program
|
| Name | Affiliation as | Duration | Current Address |
|---|---|---|---|
| K.R. Sundaram | Ph.D. student & Faculty | 1986-1991 | Professor & Head Department of Biostatistics 8thFloor, Medical College Tower Amrita Institute of Medical Sciences & Research Centre Elamakkara P.O. Kochi-682026 Email: krsundaram[at]aims[dot]amrita.edu |
| D.K. Shukla | Ph.D. student | 1991-1996 | Consultant, ICMR, New Delhi- 110029. Email: shukladk[at]hotmail[dot]com |
| V. Sreenivas | Ph.D. student & Faculty | 1992-1996 | No 6-T, Sec-T, Jasola Vihar, Delhi-110025. Email:sreenivas_vishnu[at]yahoo[dot]com |
| Geetha R. Menon | Ph.D. student | 1998-2002 | Scientist-E ICMR-NIMS, New Delhi-110029 Email: grmenon_2000[at]yahoo[dot]com |
| Rajvir Singh | Ph.D. student & (Scientist-I) | 1998-2002 & (1986-2008) | RZF-760A/50-II, Gali No. 3, Raj Nagar-II PalamColony New Delhi-110045 E-mail: rajvir_aiims[at]yshoo[dot]com |
| Prem Chandra | Ph.D. student | 2001-2006 | Ventiv International Pharma Services Pvt. Ltd. GlaxoSmithKline (GSK CHR & D) Sector No. 32, Plot No. 67, Gurgaon, India Email: prem_s77[at]rediffmail[dot]com |
| Shahina Begum | Ph.D. student | 2003-2007 | Scientist-E ICMR-NIRRH, Mumbai. Email: shahina_appe[at]yahoo[dot]com |
| Alok Kumar Dwivedi | Ph.D. student | 2005-2009 | Associate Professor, Texas Tech University Health Sciences Center, El Paso, TX 79905 Email: alok_bhu1[at]yahoo[dot]co[dot]in |
| Dimple Kondal | Ph.D. student | 2005-2009 | Biostatistician Centre for Chronic Disease Control Safdarjung Enclave, New Delhi Email: dimple_guleria1[at]yahoo.co[dot]in |
| Shankar Khanal | Ph.D. student | 2006-2010 | Professor, Central Department of Statistics, Tribhuvan University, Kathmandu, Nepal Email: shankar_cds[at]yahoo[dot]com |
| Kalaivani Mani | Ph.D. student | 2008-2013 | Scientist-I Department of Biostatistics, AIIMS, New Delhi-110029 Email: manikalaivani[at]yahoo[dot]co[dot]in |
| Vineet Kumar Kamal | Ph.D. student | 2010-2016 | Scientist ‘C’ ICMR-NIE, Chennai Email: vineetstats[at]gmail[dot]com |
| Bhaskar Thakur | Ph.D. student | 2011-2017 | Email: bhaskarstatistics[at]gmail[dot]com |
| Mona Pathak | Ph.D. student | 2013-2018 | Assistant Professor Kalinga Institute of Medical Sciences, Bhubaneswar, Odisha, India Email: mona.pathak19[at]gmail[dot]com |
| Ashish Datt Upadhyay | Ph.D. student | 2012-2019 | Jr. Statistician Department of Biostatistics, AIIMS, New Delhi-110029 Email: adu361976[at]rediffmail[dot]com |
| C.P. Yadav | Ph.D. student | 2013-2019 | Scientist ‘B’ ICMR-NIMR, Dwarka, Delhi Email: cpyadav123[at]gmail[dot]com |
| Mr. Vishwajeet Singh | Ph.D. student | 2014-2020 | Email: vishu.bhu1[at]gmail[dot]com |
Teaching Program
| 8 - 8:30 am | 8:30 – 9 am | |
|---|---|---|
| Monday | Research Presentation / Allied department presentation | |
| Tuesday | Cath case discussion | Mortality meeting |
| Wednesday | Cath case discussion | Spotters |
| Thursday | Cath case discussion | Rapid fire questions |
| Friday | Cath case discussion | Short seminar |
| Saturday | 8-9am: Long Seminar 9-10am: Cath case discussion 11-12am: Bedside case discussion | |
Address: Room no 4007,
4th Floor, Convergence Block,
Department of Biochemistry,
All India Institute of medical Sciences, New Delhi
Phone: +91-11-26549235
Email id: kchosdol[at]gmail[dot]com, kunzangchosdol[at]yahoo[dot]com
Degree
| Subject
| University/ Institution
| Year
|
|---|---|---|---|
PhD
| Biochemistry
| AIIMS, New Delhi
| 2007
|
MD
| Biochemistry
| AIIMS, New Delhi
| 1999
|
MBBS & Internship
| Medicine
| Bundhelkhand University, Jhansi, UP
| 1995
|
Position
| Department
| University/ Institution
| Dates
|
|---|---|---|---|
Professor
| Biochemistry
| All India Institute of Medical Science, New Delhi
| 2014- Till date
|
Additional Professor
| Biochemistry
| All India Institute of Medical Science, New Delhi
| 2010-2014
|
Associate Professor
| Biochemistry
| All India Institute of Medical Science, New Delhi
| 2007-2010
|
Assistant Professor
| Biochemistry
| All India Institute of Medical Science, New Delhi
| 2003-2007
|
Senior Demonstrator
| Biochemistry
| All India Institute of Medical Science, New Delhi
| 2000-2003
|
Presently, we are working to understand the molecular interactions between the oncogene FAT1 and other crucial signalling molecules like p53 and b-catenin in glioma; Understanding the regulation of FAT1 expression; FAT1 regulated miRNA signature in hypoxic glioma and effect of cytotoxic drugs on glioma cells after FAT1 modulation.
1. Madan E, Dikshit B, Gowda SH, Srivastava C, Sarkar C, Chattopadhyay P, Sinha S, Chosdol K (2016) FAT1 is a novel upstream regulator of HIF1α and invasion of high grade glioma. Int J Cancer. 2016 Aug 18. doi: 10.1002/ijc.30386. [Epub ahead of print]
2. Jalota A, Kumar M, Das BC, Yadav AK, Chosdol K, Sinha S (2016) Synergistic increase in efficacy of a combination of 2-deoxy-D-glucose and cisplatin in normoxia and hypoxia: switch from autophagy to apoptosis. Tumour Biol. 2016 Jun 15. [Epub ahead of print]
3. Bhardwaj M, Sen S, Sharma A, Kashyap S, Chosdol K, Pushker N, Bajaj MS, Bakhshi S (2015) ZEB2/SIP1 as novel prognostic indicator in eyelid sebaceous gland carcinoma. Hum Pathol. 2015 Oct;46(10):1437-42
4. Irshad K, Mohapatra SK, Srivastava C,Garg H, Mishra S, Dikshit B, Irshad K, Mohapatra SK, Srivastava C,Garg H, Mishra S, Dikshit B, Sarkar C, Gupta D, Chandra PS, Chattopadhyay P, Sinha S, Chosdol K (2015) A Combined Gene Signature of Hypoxia and Notch Pathway in Human Glioblastoma and Its Prognostic Relevance. PLoS One. 2015 Mar 3;10(3):e0118201.
5. Jayaraj P, Sen S, Sharma A, Chosdol K, Kashyap S, Rai A, Pushker N, Bajaj M. (2015) Eyelid sebaceous carcinoma: a novel mutation in lymphoid enhancer-binding factor 1 (LEF1). Br J Dermatol. 2015 Sep;173(3): 811-4.
6. Chingkheilemba M, Kumar U, Chosdol K, Das N (2014). Lack of role of endothelial nitric oxide synthase gene Glu298Asp polymorphism in rheumatoid arthritis among Asian Indians. IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) 2014; 13( 4): 25-28.
7. Dikshit B, Irshad K, Madan E, Aggarwal N, Sarkar C, Chandra PS, Gupta DK, Chattopadhyay P, Sinha S, Chosdol K (2013). FAT1 acts as an upstream regulator of oncogenic and inflammatory pathways, via PDCD4, in glioma cells. Oncogene. 2013 Aug 15;32(33):3798-808.
8. Agarwal S, Sharma MC, Jha P, Pathak P, Suri V, Sarkar C, Chosdol K, Suri A, Kale SS, Mahapatra AK, Jha P (2013). Comparative study of IDH1 mutations in gliomas by immunohistochemistry and DNA sequencing. Neuro Oncol. 2013 Jun;15(6):718-26.
9. Chosdol K, Misra A, Puri S, Srivastava T, Sarkar C, Mahapatra AK and Sinha S (2009) Frequent LOH and altered expression of tumor supressor FAT identified by RAPD in astrocytic tumors. BMC Cancer 9:5
10. Srivastava T, Chosdol K, Chattopadhyay P, Mahapatra AK, Sarkar C, Sinha S (2007) Frequent loss of heterozygosity encompassing the hMLH1 locus in low grade astrocytic tumors. J Neuro-oncol. Feb;81(3):249-55.
DST; DRDO; DBT; IMRG (AIIMS).
Dr. KhushbooIrshad completed her PhD at the Department of Biochemistry, AIIMS, New Delhi, in 2013 under the supervision of Prof. Kunzang Chosdol, Prof. Subrata Sinha and Prof. P. Chattopadhyay. Her thesis involved the study of correlation between hypoxia and Notch signaling pathway in glioblastoma and identification of a combined gene signature to predict the survival of glioblastoma patients. Her work derived a key prognostic molecular cluster characteristic of the Notch pathway response in hypoxic glioblastoma tumors and gliomasphere cultures (PLoS One (2015); 10(3):e0118201; felicitated with AIIMS Excellence Research Award-2015 that was awarded to Prof. Chosdol). Presently, her research focuses on deciphering the role of FAT1, a novel gene implicated in glioma, in regulating the hallmark features of glioma like stemness and invasiveness, as well as in maintenance of the balance between pro-inflammatory and anti-inflammatory signaling in glioma. She was awarded the DST-SERB Start-Up Research Grant in March 2016, for the project aimed at elucidation of FAT1 function in modulating pro-inflammatory signaling and anti-inflammatory / immunosuppressive signaling pathways in glioma.
Dr. Srinivas H done MBBS from Bangalore Medical college, Rajiv gandhi university of health sciences Karnataka and MD from MAULANA AZAD Medical College, Delhi university, New Delhi. His MD thesis was on procalcitonin, IL 6, TNFalpha and urinary isoprostane in sepsis patients under the guidance of ex HOD and director professor Dr TK Mishra. He has completed one year of senior residency in PGIMER, Chandigarh and two year of senior residency in AIIMS, New Delhi. He has published his work in national and international papers in the various field of sciences and medical education. He is working now on pathway analysis of interaction between FAT1 with p53, HIF 1alpha and beta catenin in glioma as a PhD research scholar under the guidance of Dr KUNZANG CHOSDOL and Dr SUBRATA SINHA. He has done DNB from Diplomate of National Board in biochemistry and certification course in industry program, clinical trials and administration from bioinformatics institute of India. He is a Life member of Association of Medical Biochemistry of India since 2008
Life member of Society for Tissue Engineering and Regenerative Medicine (India),Thiruvananthapuram since 2010 and Indian Association of Cancer Research.
Ms. Chitrangda Srivastava is currently in her final year of PhD. She is working on the characterization of FAT1 gene promoter. In addition, she is analyzing the functional role of FAT1 with EMT and stemness in hypoxic glioma. She completed her M.Sc. from the department of Biochemistry, AIIMS, in 2012. Her M.Sc. thesis involved the study of the role of Notch signalling pathway with EMT and stemness in pathogenesis of glioma under hypoxia. She has won several awards during her PhD tenure, including Best Oral Presentation Award in ACOS-2016, European Young Scientist Travel Award-2015, G.P. Talwar Foundation Travel Award-2015, etc. She is an Associate Member of the American Association of Cancer Research since 2011 and an Associate Member of the European Society of Neuro-Oncology since 2016.
Nargis Malik completed her M.Sc. in toxicology from Meerut University, Currently she is a second year PhD. student working on the “Role of FAT1 gene on the regulation of microRNAs in glioma”
Akankshakanojia has completed her B.Sc.(H) in Biomedical Sciences from Acharya Narendra Dev College, University of Delhi in 2016. She is currently pursuing M.Sc. in Biochemistry from All India Institute of Medical Science, Delhi under the guidance of Dr. Kunzang Chosdol.
Mukesh Kumar is working as a Laboratory Attendant Gr.-II in the Department of Biochemistry since August 2011. He help in the research related work for M.Sc., Ph.D. and M.D. Students in Research Laboratory of Dr. Parthaprasad Chattopadhyay & Dr. Kunzang Chosdol. His nature of duties includes, culture work, DEPC treatment and assistance of UG/PG examination.
Cell Regulation & Trafficking Lab

Dr. Parthaprasad Chattopadhyay, Professor
Address : Room No. 4007, Convergence Block, AIIMS, New Delhi.
Phone : 011-26549238
Email : parthoaiims@hotmail.com
MBBS, (1981-1987) R G Kar Medical College, Calcutta University, Kolkata
MD, Biochemistry, (1989-1991) All India Institute of Medical Sciences, New Delhi.
PhD, Biochemistry (1992-1996) All India Institute of Medical Sciences, New Delhi.
Senior Demonstrator (1992-1995) Department of Biochemistry, AIIMS, New Delhi
Assistant Professor (1997-2003) Department of Biochemistry, AIIMS, New Delhi
Associate Professor (2003-2007) Department of Biochemistry, AIIMS, New Delhi
Additional Professor (2007-2011) Department of Biochemistry, AIIMS, New Delhi
Professor (2011- till date) Department of Biochemistry, AIIMS, New Delhi
a) Nanoparticle trafficking within the cell: Tracing the path of nanoparticles within the cell and attempting to modulate their intracellular travel to prolong their stay within the cell for increased unloading of their cargo (drug).
b) Site-directed epigenetic modulation: Using modified CRISPR based techniques to modulate CpG methylation and Histone methylation/acetylation for altering gene expression of tumor suppressor and promoter genes
Department of Biotechnology and Department of Science & Technology, Ministry of Science & Technology, GOI.
Cell Regulation & Trafficking Lab
Dr. Parthaprasad Chattopadhyay, Professor
Address : Room No. 4007, Convergence Block, AIIMS, New Delhi.
Phone : 011-26549238
Email : parthoaiims@hotmail.com
MBBS, (1981-1987) R G Kar Medical College, Calcutta University, Kolkata
MD, Biochemistry, (1989-1991) All India Institute of Medical Sciences, New Delhi.
PhD, Biochemistry (1992-1996) All India Institute of Medical Sciences, New Delhi.
Senior Demonstrator (1992-1995) Department of Biochemistry, AIIMS, New Delhi
Assistant Professor (1997-2003) Department of Biochemistry, AIIMS, New Delhi
Associate Professor (2003-2007) Department of Biochemistry, AIIMS, New Delhi
Additional Professor (2007-2011) Department of Biochemistry, AIIMS, New Delhi
Professor (2011- till date) Department of Biochemistry, AIIMS, New Delhi
a) Nanoparticle trafficking within the cell: Tracing the path of nanoparticles within the cell and attempting to modulate their intracellular travel to prolong their stay within the cell for increased unloading of their cargo (drug).
b) Site-directed epigenetic modulation: Using modified CRISPR based techniques to modulate CpG methylation and Histone methylation/acetylation for altering gene expression of tumor suppressor and promoter genes
Department of Biotechnology and Department of Science & Technology, Ministry of Science & Technology, GOI.

Dr. Kalpana Luthra
Professor & Head
Department of Biochemistry
Room No-4001, 4th Floor,
Convergence Block,
All India Institute of Medical Sciences,
New Delhi-110029
Phone: 011-26549242
Email Id: kalpanaluthra@gmail.com
Dr. Kalpana Luthra is a Professor & Head in the Department of Biochemistry, All India Institute of Medical Sciences (AIIMS), New Delhi, India. She completed her PhD at AIIMS in 1994 and joined as faculty at AIIMS in 1998. She was awarded Shakuntala Amir Chand Prizeby Indian Council of Medical Research (ICMR) for the year 2003 & Fogarty fellowship in 2002 and availed training in HIV-1 antibody related work at New York University. She is a Fellow of The National Academy of Medical Sciences India (NAMS), National Academy of Sciences, India (NASI) & Indian National Science Academy (INSA).
HIV Immunology: Coevolution of virus and antibody responses, generation and characterization of human recombinant anti-HIV-1 monoclonal antibodies
HIV-1 is a complex virus with a remarkable ability to protect itself from our intricate network of immune system. This is achieved by masking itself from the immune recognition by acquiring the host proteins or by escaping the humoral response by virtue of its extraordinary ability to mutate. This leads to generation of diverse strains of HIV-1 virus, making the treatment and prevention a complicated process. More than 90% of the HIV-1 infections in India are caused by clade C viruses. Our lab focuses on studying various aspects of HIV-1 infection which includes:
HIV-1C primary isolates generated in our lab from select infected children showed resistance to neutralization by majority of the known second generation bNAbs (Makhdoomi et al, Virology 2016). We followed up antiretroviral naïve chronically infected children and mapped their plasma for presence of bnAbs (Makhdoomi et al. J Gen Virol. 2017 Jul;98(7):1879-189) and identified a pair of identical twins AIIMS_329 and AIIMS_330. The plasma from both donors showed the evolvement of bnAbs targeting common epitopes in the V2 and V3 regions of the envelope, suggesting bnAb development in these twins may perhaps be determined by specific sequences in the shared virus that can guide development of immunogens aimed at eliciting V2 and V3 bNAbs. Characterization of the neutralization sensitive and resistant viruses coevolving with bNAbs in the contemporaneous AIIMS_330 plasma provides information towards understanding viral alterations that may have contributed to the development of resistance to bnAbs. (Mishra N. J Virol https://doi.org/10.1128/JVI.00654-19).
Our work on circulating HIV-1 in perinatally infected infants defined viral factors associated with early bnAb responses, supportive of polyvalent vaccination approaches capable of inducing bnAbs against HIV-1 (Mishra N. Nat.Commun.,2020) 11:4409 https://doi.org/10.1038/s41467-020-18225-x). As in the case of monozygotic twins, we identified that the antibody response in infants primarily targets the V2 region of HIV-1, making it an attractive target for immunogen design to elicit antibodies.
Using the high throughput technology of HIV-1 specific single B cell sorting, we isolated a bNAb AIIMS-P01 from a pediatric elite neutralizer (Kumar et al, JVI, 2019). This mAb has shown 67% breadth at a potency of 0.5 µg/ml, and shows good neutralizing activity against Indian clade C viruses and needs to be tested in future for in vivo protection against HIV-1 infection.
Recently, we generated and structurally analyzed a heavy chain matured linage antibody 44m of the parental anti-HIV-1 human monoclonal AIIMS P01, that demonstrated improved neutralization potential against globally diverse viruses, as compared to the parent antibody (Kumar S et al. iScience. 2023)
During the COVID-19 pandemic, neutralizing antibodies have been shown to be a critical feature of recovered patients. Given the unique nature of HIV-1 bnAbs and their ability to recognize and/or accommodate viral glycans, we reasoned that the glycan shield of SARS-CoV-2 spike protein can be targeted by HIV-1 specific bnAbs. We showed that HIV-1 specific monoclonal antibodies as well as polyclonal plasma antibodies cross-react and neutralize SARS-CoV-2. (Mishra N. PLoS Pathog 2021. 17(9): e1009958 https://doi.org/10.1371/journal.ppat.1009958.

D r. Swarandeep Singh, is a Research Associate, working on a project entitled "Development of therapeutic broadly neutralizing monoclonal antibodies against circulating HIV-1 clade C in children and adults." He earned his Ph.D. in the HIV-1 Immunology Laboratory at AIIMS New Delhi under the chief guidance of Professor Kalpana Luthra. During his Ph.D., he developed expertise in designing and characterizing HIV-1 vaccines and recombinant monoclonal antibodies. Dr. Singh's primary research interest lies in HIV-1 vaccine design, with a focus on testing designed immunogens in preclinical animal models. Additionally, he actively explores the generation and modification of novel monoclonal antibodies from chronically HIV-1 infected patients for therapeutic purposes. During the COVID-19 pandemic, he has showcased the unique nature of HIV-1 broadly neutralizing antibodies (bnAbs) & polyclonal plasma antibodies cross-reacted and effectively neutralized SARS-CoV-2, showcasing the potential dual application of HIV research insights in combating other viral infections. Through the esteemed HIV-1 Research Trust Fellowship Award (United Kingdom), Dr. Swarandeep Singh has gained advanced skills in the design of self-assembling protein nanoparticles as a platform for HIV vaccines & other innovative vaccine strategies

Ms. Antara Malik is a fifth year PhD student currently working in the lab of Dr. Kalpana Luthra. Primarily, her thesis work is aimed at understanding the status of the immune responses and the role of macrophages and T cells in the immunopathology of Chronic Pancreatitis. The second part of her thesis work involves theelucidation of metabolic alterations associated with the progression of Chronic Pancreatitis.
She completed her Masters in Biotechnology from Jamia Millia Islamia, New Delhi. Her master’s dissertation was conducted in NIPGR (National Institute of Plant Genome Research), New Delhi where her project work involved cloning of Sucrose Transporters and Expression Analysis of Genes in Rice plants. She graduated in Biochemistry (Hons.) from University of Delhi.
Apart from the ongoing research work involving HIV-1, Prof. Kalpana Luthra has also collaborated with Prof. Pramod K. Garg, Department of Gastroenterology and the group recently started working on Chronic Pancreatitis.
Chronic Pancreatitis is an inflammatory disease of the pancreas which results in the slow destruction of pancreatic parenchyma, severe abdominal pain, subsequent fibrosis leading to poor quality of life. The mechanism of inflammation, tissue destruction and fibrosis is not well understood.
Patients commonly experience recurrent exacerbations with painful attacks interspersed by relatively quiescent phases. Also, some patients present with chronic continuous pain. This may be driven by either or both innate and adaptive immune responses on which there are several contradictory studies/lacunae in the existing literature.
Hereby, there arises a need to understand the inflammatory processes in Chronic Pancreatitis with regard to the initiating and effector cells that are involved, and the inflammatory mediators driving the process. The translational significance lies in the possibility of repurposing some of the known anti-inflammatory/immunosuppressive drugs that may be tested in these patients.
Post her Masters, she continued as a JRF in NIPGR, where she was working on the characterization of tissue specific expression pattern of PIF transcription factors in rice and tomato plants in response to high temperature, drought and salt stress via quantitativePCR and generation of PIF regulatory network via transcriptome profiling of over expression and knock out/down lines using RNA Seq librarypreparation.
Further, she joined IARI (Indian Agricultural Research Institute), New Delhi as a JRF where her project was based on the integration of plant and parasite omics to decipher the interactions and identify molecular targets for the management of root knot disease of rice.
Later on, she shifted her research focus to human sciences and joined Dr. B.R. Ambedkar Center for Biomedical Research (ACBR), University of Delhi as a JRF where she was studying the genetic polymorphism of Growth Differentiation Factor15 (GDF15) in patients with Coronary Artery Disease in Asian Indian population followed by the differential expression of GDF15 in these patients at mRNA and protein level.
Life member of Indian Immunology society since January 2023.

Ms. Shaifali Sharma is a Ph.D. Scholar in Prof. Luthra’s Laboratory since February 2020. As a part of her thesis, she is generating HIV-1 envelope immunogen which binds to germline version of known anti-HIV-1 broadly neutralizing antibodies from early HIV-1 infected donors.
She earned her Master’s degree in Medical Biochemistry from AIIMS, New Delhi in 2019. As a part of her M.Sc. thesis dissertation, she studied the HIV-1 envelope glycoprotein by generating pseudoviruses from a chronically infected long term non-progressor, in order to identify envelope features of the virus circulating in patient. After completing her M.Sc., she continued being a part the Lab as a Junior Research Fellow (joined in October 2019) and later registered for Ph.D. in February 2020.
Generation and characterization of HIV-1 subtype-C based trimeric immunogens from infected children. (2019- present)
Life member of Indian Immunology society since April 2018.

Dr. Sanket Katpara is a second year PhD student at the department of biochemistry working under the chief supervision of Professor Kalpana Luthra in the HIV immunology lab. As part of his PhD thesis, he is working on “Generation and Characterization of recombinant anti-HIV-1 human monoclonal antibodies from HIV-1 infected individuals”. He is interested in generation of monoclonal antibodies that can target different epitopes on the HIV-1 envelope which can be used as a combinatorial therapy for the treatment of drug resistant HIV-1 infected individuals.
Earlier he has also completed his M.D. under the supervision of Dr Kalpana Luthra at the Department of Biochemistry, AIIMS. (2017-2020) and worked as a senior resident at the Dept. of Biochemistry, AIIMS, New Delhi (2020-2023)

Mr. Harsh Bhakhri is a PhD scholar (Dec 2021-present) currently in third year, is working on the characterization of the B cell receptor repertoire in HIV-1 subtype C infected individuals and also in generation of human anti-HIV-1 monoclonal antibodies from infected individuals. He has interest in studying the BCR sequences and their association to neutralization response in a cohort of HIV-1 infected individuals. He is also looking into the neutralizing plasma antibody response against various SARS-COV2 variants in different vaccinees for assessment of the protective response of the vaccination drive in Indian population.
He has also completed his M.Sc. in Biochemistry from AIIMS in 2021. His masters dissertation thesis work was to the role of M6A writer METTL3 and readers (IGF2BP1/3) in hematopoietic development and leukemogenesis. He has done his graduation in B.Sc. (Hons) Biochemistry from Sri Venkateswara College, University of Delhi in 2019.
Skills: Generation of pseudo-viruses, Generation of stable cell line, FACS, Neutralization assays, Single B-cell sorting, Single cell PCR, Molecular cloning, Site Directed Mutagenesis, Freestyle mammalian protein expression and purification, Size exclusion chromatography, Genomic data analysis using Galaxy server, R and Python.
Favorite hobbies: Generation of lots of viruses, learning new skills, a little bit of graphic designing, music and badminton.

Dr. Aradhana Sarma is a first year M.D. student at the Department of Biochemistry and is working under the chief supervision of Professor Kalpana Luthra. She is currently working on infectious molecular clones for her M.D. thesis titled “Generation and characterization of infectious molecular clones from HIV-1 viral envelopes derived from infected children”. With the help of this study, she intends to use the lab generated IMCs as potential tools in HIV-1 vaccine and entry inhibitor research.
She has completed her MBBS from Jorhat Medical College and Hospital, Assam.
Anil Kumar (Masalchi/Bearer Gd.II)
Mr. Anil Kumar previously worked as a Lab Attendant in Prof. Luthra’s lab in a research project since May, 2003. He was responsible for smooth functioning and maintenance of the lab, which included packing of tips, autoclaving and sterilization of plastic/glasswares, washing of equipment and cleaning of culture lab. He has completed his 12th standard Delhi in 2013. He is employed as Masalchi/Bearer Gd.II from January 2020.
Mr. Ajeesh T. Gangadharan (Junior Administrative Assistant)
Mr. Ajeesh T. Gangadharan joined Dr.K Luthra’s Lab as a Data Entry Operator in a research project on 1st October, 2005. He completed his B.Com from MG University, Kerala in 2002 & Computer Diploma From NIIT, New Delhi in 2004. After the completion of 15 years of service in various research projects, in September 2021 he joined the same lab as a Junior Administrative Assistant. His nature of work includes entering and systematic maintenance of patient data in Excel sheet, to contact and sent written communications for getting quotations for chemicals, preparing supply orders, processing bills, maintaining Accounts of the project, preparing Utilization certificates & Statement of expenditure, maintaining stock register, compilation of the project reports etc..
Mr. Abdul Wahid Hussain is working as a Lab Technician in Dr. Kalpana Luthra’s lab in a research project since January, 2010. He is an expert phlebotomist. His nature of works are cell culture (mammalian and bacterial) media preparation, Buffers preparation etc., PCR, DNA isolation, Patient sample collection, PBMCs isolation, Protein purification, Biological substance distribution to collaborators, Procurement/ordering of chemicals and lab instruments maintenance. He has completed his M.Sc.MLT from NIMS university Jaipur, Rajasthan in year 2020.
Publications:
Suraj Kumar, Lab Technician
Mr. Suraj Kumar joined Prof. Luthra’s lab in the Chronic Pancreatitis research project as a lab technician in June 2022. He completed his Bachelor of Science (Hons) in Chemistry in the year 2022 through distance learning programme from Indira Gandhi National Open University (IGNOU), New Delhi. Also, he has a Diploma in Medical Lab Technology (2022) from DPMI (Delhi Paramedical Management of Institute) and a Diploma in Information Technology (2019). He is an expert phlebotomist and a quick learner.
His job duties include patient’s sample collection from OPD,Wards, OT’s, ICU (both adults and paediatrics), maintaining records of patient’s clinical data files, sample and reagents/consumable records, patient counselling, PBMC isolation, gel electrophoresis, cell culture media and buffer preparation. He is well versed in the sample processing steps of flow cytometry, macrophage culture, magnetic cell sorting, ELISA and Plasmid isolation (Mini and Midi kits) and is able to carry out flow cytometric data acquisition.
In addition, he is also well trained in the usage of BSL-1 cabinet, Lyophilizer, Multi ELISA reader, Automated cell counter, inverted/ upright microscope, homogenizer, Nanodrop spectrophotometer, cell washer, pH meter, Weighing balance, Autoclave, water bath, hot air oven, centrifuge machines and CO2 Incubator shaker. Currently, he is in the process of learning the data analysis of Flow Cytometry and Mass Spectrometry.
He has previously worked in Sir Ganga Ram Hospital, New Delhi and two other diagnostic centres where he had hands on experience in conducting routine laboratory tests along with RTPCR, ESR,H&E staining, Urine,stool,sputum culture, Leishman, Giemsa,Gram positive and negative staining, Blood group testing, Serology testing (Typhoid, HIV, HCV,HBSAg,Syphilis,Malaria,Dengue IgM/IgG) , BTCT testing and skin test. Apart from this, he gained operational knowledge of instruments like HPLC for HbA1C,ERBA Chem5X(semi-automated),Urinometer (fully automated),Sysmax Coulter, Hemoglobinometer,Fibrometer coagulation and Microtome.
| S. No. | Name of Resident |
|---|---|
| 1. | Dr. Sumit Kumar |
| 2. | Dr. Asharam Panda |
| 3. | Dr. Lamk Kadiyani |
| 4. | Dr. Jeedigunta Mahidhar |
| S. No. | Name of Resident |
|---|---|
| 1. | Dr. Nayani Balbir Singh Makkar |
| 2. | Dr. Sataroopa Mihsra |
| 3. | Dr. Vibhav Sharma |
| 4. | Dr. Pavan Kumar Reddy Velpula |
| S. No. | Name of Resident |
|---|---|
| 1. | Dr. Praveen M. |
| 2. | Dr. Manjit Mahendran |
| 3. | Dr. Mukesh Dhillon |
| 4. | Dr. Devesh Kumar |
| 5. | Dr. Ankur Handa |
| 6. | Dr. Kshitij Prasad |
| S. No. | Name of Resident |
|---|---|
| 1. | Dr. Mohsin Raj |
| 2. | Dr. Sai Durga |
| 3. | Dr. Gorav Sharma |
| 4. | Dr. Pramod |
| 5. | Dr. Charu |
| 6. | Dr. Chandan Sharma |
| 7. | Dr. Shatanik Sarkar |
| S. No. | Name of Resident |
|---|---|
| 1. | Dr. Goutam Kintada |
| 2. | Dr. Aswin K Pius |
| 3. | Dr. Shitij |
| S. No. | Name of Resident |
|---|---|
| 1. | Dr. Nabeel Faisal V. |
| 2. | Dr. Lydia James George |
| 3. | Dr. Abhinav Jain |
| 4. | Dr. Avishkar Agrawal |
| 5. | Dr. Relangi Hitesh Srinavas Krishna |
| 6. | Dr. Souvik Sardar |
| 7. | Dr. Neha Chopra |
| 8. | Dr. Akkineni Krishna Prasad |
| S. No. | Name of Resident |
|---|---|
| 1. | Dr. Sumit Kumar |
| 2. | Dr. Asharam Panda |
| 3. | Dr. Lamk Kadiyani |
| 4. | Dr. Jeedigunta Mahidhar |
| S. No. | Name of Resident |
|---|---|
| 1. | Dr. Nayani Balbir Singh Makkar |
| 2. | Dr. Sataroopa Mihsra |
| 3. | Dr. Vibhav Sharma |
| 4. | Dr. Pavan Kumar Reddy Velpula |
| S. No. | Name of Resident |
|---|---|
| 1. | Dr. Praveen M. |
| 2. | Dr. Manjit Mahendran |
| 3. | Dr. Mukesh Dhillon |
| 4. | Dr. Devesh Kumar |
| 5. | Dr. Ankur Handa |
| 6. | Dr. Kshitij Prasad |
| S. No. | Name of Resident |
|---|---|
| 1. | Dr. Mohsin Raj |
| 2. | Dr. Sai Durga |
| 3. | Dr. Gorav Sharma |
| 4. | Dr. Pramod |
| 5. | Dr. Charu |
| 6. | Dr. Chandan Sharma |
| 7. | Dr. Shatanik Sarkar |
| S. No. | Name of Resident |
|---|---|
| 1. | Dr. Goutam Kintada |
| 2. | Dr. Aswin K Pius |
| 3. | Dr. Shitij |
| S. No. | Name of Resident |
|---|---|
| 1. | Dr. Nabeel Faisal V. |
| 2. | Dr. Lydia James George |
| 3. | Dr. Abhinav Jain |
| 4. | Dr. Avishkar Agrawal |
| 5. | Dr. Relangi Hitesh Srinavas Krishna |
| 6. | Dr. Souvik Sardar |
| 7. | Dr. Neha Chopra |
| 8. | Dr. Akkineni Krishna Prasad |
Dr. Kalpana Luthra
Professor & Head
Department of Biochemistry
Room No-4001, 4th Floor,
Convergence Block,
All India Institute of Medical Sciences,
New Delhi-110029
Phone: 011-26549242
Email Id: kalpanaluthra@gmail.com
Dr. Kalpana Luthra is a Professor & Head in the Department of Biochemistry, All India Institute of Medical Sciences (AIIMS), New Delhi, India. She completed her PhD at AIIMS in 1994 and joined as faculty at AIIMS in 1998. She was awarded Shakuntala Amir Chand Prizeby Indian Council of Medical Research (ICMR) for the year 2003 & Fogarty fellowship in 2002 and availed training in HIV-1 antibody related work at New York University. She is a Fellow of The National Academy of Medical Sciences India (NAMS), National Academy of Sciences, India (NASI) & Indian National Science Academy (INSA).
HIV Immunology: Coevolution of virus and antibody responses, generation and characterization of human recombinant anti-HIV-1 monoclonal antibodies
HIV-1 is a complex virus with a remarkable ability to protect itself from our intricate network of immune system. This is achieved by masking itself from the immune recognition by acquiring the host proteins or by escaping the humoral response by virtue of its extraordinary ability to mutate. This leads to generation of diverse strains of HIV-1 virus, making the treatment and prevention a complicated process. More than 90% of the HIV-1 infections in India are caused by clade C viruses. Our lab focuses on studying various aspects of HIV-1 infection which includes:
HIV-1C primary isolates generated in our lab from select infected children showed resistance to neutralization by majority of the known second generation bNAbs (Makhdoomi et al, Virology 2016). We followed up antiretroviral naïve chronically infected children and mapped their plasma for presence of bnAbs (Makhdoomi et al. J Gen Virol. 2017 Jul;98(7):1879-189) and identified a pair of identical twins AIIMS_329 and AIIMS_330. The plasma from both donors showed the evolvement of bnAbs targeting common epitopes in the V2 and V3 regions of the envelope, suggesting bnAb development in these twins may perhaps be determined by specific sequences in the shared virus that can guide development of immunogens aimed at eliciting V2 and V3 bNAbs. Characterization of the neutralization sensitive and resistant viruses coevolving with bNAbs in the contemporaneous AIIMS_330 plasma provides information towards understanding viral alterations that may have contributed to the development of resistance to bnAbs. (Mishra N. J Virol https://doi.org/10.1128/JVI.00654-19).
Our work on circulating HIV-1 in perinatally infected infants defined viral factors associated with early bnAb responses, supportive of polyvalent vaccination approaches capable of inducing bnAbs against HIV-1 (Mishra N. Nat.Commun.,2020) 11:4409 https://doi.org/10.1038/s41467-020-18225-x). As in the case of monozygotic twins, we identified that the antibody response in infants primarily targets the V2 region of HIV-1, making it an attractive target for immunogen design to elicit antibodies.
Using the high throughput technology of HIV-1 specific single B cell sorting, we isolated a bNAb AIIMS-P01 from a pediatric elite neutralizer (Kumar et al, JVI, 2019). This mAb has shown 67% breadth at a potency of 0.5 µg/ml, and shows good neutralizing activity against Indian clade C viruses and needs to be tested in future for in vivo protection against HIV-1 infection.
Recently, we generated and structurally analyzed a heavy chain matured linage antibody 44m of the parental anti-HIV-1 human monoclonal AIIMS P01, that demonstrated improved neutralization potential against globally diverse viruses, as compared to the parent antibody (Kumar S et al. iScience. 2023)
During the COVID-19 pandemic, neutralizing antibodies have been shown to be a critical feature of recovered patients. Given the unique nature of HIV-1 bnAbs and their ability to recognize and/or accommodate viral glycans, we reasoned that the glycan shield of SARS-CoV-2 spike protein can be targeted by HIV-1 specific bnAbs. We showed that HIV-1 specific monoclonal antibodies as well as polyclonal plasma antibodies cross-react and neutralize SARS-CoV-2. (Mishra N. PLoS Pathog 2021. 17(9): e1009958 https://doi.org/10.1371/journal.ppat.1009958.
D r. Swarandeep Singh, is a Research Associate, working on a project entitled "Development of therapeutic broadly neutralizing monoclonal antibodies against circulating HIV-1 clade C in children and adults." He earned his Ph.D. in the HIV-1 Immunology Laboratory at AIIMS New Delhi under the chief guidance of Professor Kalpana Luthra. During his Ph.D., he developed expertise in designing and characterizing HIV-1 vaccines and recombinant monoclonal antibodies. Dr. Singh's primary research interest lies in HIV-1 vaccine design, with a focus on testing designed immunogens in preclinical animal models. Additionally, he actively explores the generation and modification of novel monoclonal antibodies from chronically HIV-1 infected patients for therapeutic purposes. During the COVID-19 pandemic, he has showcased the unique nature of HIV-1 broadly neutralizing antibodies (bnAbs) & polyclonal plasma antibodies cross-reacted and effectively neutralized SARS-CoV-2, showcasing the potential dual application of HIV research insights in combating other viral infections. Through the esteemed HIV-1 Research Trust Fellowship Award (United Kingdom), Dr. Swarandeep Singh has gained advanced skills in the design of self-assembling protein nanoparticles as a platform for HIV vaccines & other innovative vaccine strategies
Ms. Antara Malik is a fifth year PhD student currently working in the lab of Dr. Kalpana Luthra. Primarily, her thesis work is aimed at understanding the status of the immune responses and the role of macrophages and T cells in the immunopathology of Chronic Pancreatitis. The second part of her thesis work involves theelucidation of metabolic alterations associated with the progression of Chronic Pancreatitis.
She completed her Masters in Biotechnology from Jamia Millia Islamia, New Delhi. Her master’s dissertation was conducted in NIPGR (National Institute of Plant Genome Research), New Delhi where her project work involved cloning of Sucrose Transporters and Expression Analysis of Genes in Rice plants. She graduated in Biochemistry (Hons.) from University of Delhi.
Apart from the ongoing research work involving HIV-1, Prof. Kalpana Luthra has also collaborated with Prof. Pramod K. Garg, Department of Gastroenterology and the group recently started working on Chronic Pancreatitis.
Chronic Pancreatitis is an inflammatory disease of the pancreas which results in the slow destruction of pancreatic parenchyma, severe abdominal pain, subsequent fibrosis leading to poor quality of life. The mechanism of inflammation, tissue destruction and fibrosis is not well understood.
Patients commonly experience recurrent exacerbations with painful attacks interspersed by relatively quiescent phases. Also, some patients present with chronic continuous pain. This may be driven by either or both innate and adaptive immune responses on which there are several contradictory studies/lacunae in the existing literature.
Hereby, there arises a need to understand the inflammatory processes in Chronic Pancreatitis with regard to the initiating and effector cells that are involved, and the inflammatory mediators driving the process. The translational significance lies in the possibility of repurposing some of the known anti-inflammatory/immunosuppressive drugs that may be tested in these patients.
Post her Masters, she continued as a JRF in NIPGR, where she was working on the characterization of tissue specific expression pattern of PIF transcription factors in rice and tomato plants in response to high temperature, drought and salt stress via quantitativePCR and generation of PIF regulatory network via transcriptome profiling of over expression and knock out/down lines using RNA Seq librarypreparation.
Further, she joined IARI (Indian Agricultural Research Institute), New Delhi as a JRF where her project was based on the integration of plant and parasite omics to decipher the interactions and identify molecular targets for the management of root knot disease of rice.
Later on, she shifted her research focus to human sciences and joined Dr. B.R. Ambedkar Center for Biomedical Research (ACBR), University of Delhi as a JRF where she was studying the genetic polymorphism of Growth Differentiation Factor15 (GDF15) in patients with Coronary Artery Disease in Asian Indian population followed by the differential expression of GDF15 in these patients at mRNA and protein level.
Life member of Indian Immunology society since January 2023.
Ms. Shaifali Sharma is a Ph.D. Scholar in Prof. Luthra’s Laboratory since February 2020. As a part of her thesis, she is generating HIV-1 envelope immunogen which binds to germline version of known anti-HIV-1 broadly neutralizing antibodies from early HIV-1 infected donors.
She earned her Master’s degree in Medical Biochemistry from AIIMS, New Delhi in 2019. As a part of her M.Sc. thesis dissertation, she studied the HIV-1 envelope glycoprotein by generating pseudoviruses from a chronically infected long term non-progressor, in order to identify envelope features of the virus circulating in patient. After completing her M.Sc., she continued being a part the Lab as a Junior Research Fellow (joined in October 2019) and later registered for Ph.D. in February 2020.
Generation and characterization of HIV-1 subtype-C based trimeric immunogens from infected children. (2019- present)
Life member of Indian Immunology society since April 2018.
Dr. Sanket Katpara is a second year PhD student at the department of biochemistry working under the chief supervision of Professor Kalpana Luthra in the HIV immunology lab. As part of his PhD thesis, he is working on “Generation and Characterization of recombinant anti-HIV-1 human monoclonal antibodies from HIV-1 infected individuals”. He is interested in generation of monoclonal antibodies that can target different epitopes on the HIV-1 envelope which can be used as a combinatorial therapy for the treatment of drug resistant HIV-1 infected individuals.
Earlier he has also completed his M.D. under the supervision of Dr Kalpana Luthra at the Department of Biochemistry, AIIMS. (2017-2020) and worked as a senior resident at the Dept. of Biochemistry, AIIMS, New Delhi (2020-2023)
Mr. Harsh Bhakhri is a PhD scholar (Dec 2021-present) currently in third year, is working on the characterization of the B cell receptor repertoire in HIV-1 subtype C infected individuals and also in generation of human anti-HIV-1 monoclonal antibodies from infected individuals. He has interest in studying the BCR sequences and their association to neutralization response in a cohort of HIV-1 infected individuals. He is also looking into the neutralizing plasma antibody response against various SARS-COV2 variants in different vaccinees for assessment of the protective response of the vaccination drive in Indian population.
He has also completed his M.Sc. in Biochemistry from AIIMS in 2021. His masters dissertation thesis work was to the role of M6A writer METTL3 and readers (IGF2BP1/3) in hematopoietic development and leukemogenesis. He has done his graduation in B.Sc. (Hons) Biochemistry from Sri Venkateswara College, University of Delhi in 2019.
Skills: Generation of pseudo-viruses, Generation of stable cell line, FACS, Neutralization assays, Single B-cell sorting, Single cell PCR, Molecular cloning, Site Directed Mutagenesis, Freestyle mammalian protein expression and purification, Size exclusion chromatography, Genomic data analysis using Galaxy server, R and Python.
Favorite hobbies: Generation of lots of viruses, learning new skills, a little bit of graphic designing, music and badminton.
Dr. Aradhana Sarma is a first year M.D. student at the Department of Biochemistry and is working under the chief supervision of Professor Kalpana Luthra. She is currently working on infectious molecular clones for her M.D. thesis titled “Generation and characterization of infectious molecular clones from HIV-1 viral envelopes derived from infected children”. With the help of this study, she intends to use the lab generated IMCs as potential tools in HIV-1 vaccine and entry inhibitor research.
She has completed her MBBS from Jorhat Medical College and Hospital, Assam.
Anil Kumar (Masalchi/Bearer Gd.II)
Mr. Anil Kumar previously worked as a Lab Attendant in Prof. Luthra’s lab in a research project since May, 2003. He was responsible for smooth functioning and maintenance of the lab, which included packing of tips, autoclaving and sterilization of plastic/glasswares, washing of equipment and cleaning of culture lab. He has completed his 12th standard Delhi in 2013. He is employed as Masalchi/Bearer Gd.II from January 2020.
Mr. Ajeesh T. Gangadharan (Junior Administrative Assistant)
Mr. Ajeesh T. Gangadharan joined Dr.K Luthra’s Lab as a Data Entry Operator in a research project on 1st October, 2005. He completed his B.Com from MG University, Kerala in 2002 & Computer Diploma From NIIT, New Delhi in 2004. After the completion of 15 years of service in various research projects, in September 2021 he joined the same lab as a Junior Administrative Assistant. His nature of work includes entering and systematic maintenance of patient data in Excel sheet, to contact and sent written communications for getting quotations for chemicals, preparing supply orders, processing bills, maintaining Accounts of the project, preparing Utilization certificates & Statement of expenditure, maintaining stock register, compilation of the project reports etc..
Mr. Abdul Wahid Hussain is working as a Lab Technician in Dr. Kalpana Luthra’s lab in a research project since January, 2010. He is an expert phlebotomist. His nature of works are cell culture (mammalian and bacterial) media preparation, Buffers preparation etc., PCR, DNA isolation, Patient sample collection, PBMCs isolation, Protein purification, Biological substance distribution to collaborators, Procurement/ordering of chemicals and lab instruments maintenance. He has completed his M.Sc.MLT from NIMS university Jaipur, Rajasthan in year 2020.
Publications:
Suraj Kumar, Lab Technician
Mr. Suraj Kumar joined Prof. Luthra’s lab in the Chronic Pancreatitis research project as a lab technician in June 2022. He completed his Bachelor of Science (Hons) in Chemistry in the year 2022 through distance learning programme from Indira Gandhi National Open University (IGNOU), New Delhi. Also, he has a Diploma in Medical Lab Technology (2022) from DPMI (Delhi Paramedical Management of Institute) and a Diploma in Information Technology (2019). He is an expert phlebotomist and a quick learner.
His job duties include patient’s sample collection from OPD,Wards, OT’s, ICU (both adults and paediatrics), maintaining records of patient’s clinical data files, sample and reagents/consumable records, patient counselling, PBMC isolation, gel electrophoresis, cell culture media and buffer preparation. He is well versed in the sample processing steps of flow cytometry, macrophage culture, magnetic cell sorting, ELISA and Plasmid isolation (Mini and Midi kits) and is able to carry out flow cytometric data acquisition.
In addition, he is also well trained in the usage of BSL-1 cabinet, Lyophilizer, Multi ELISA reader, Automated cell counter, inverted/ upright microscope, homogenizer, Nanodrop spectrophotometer, cell washer, pH meter, Weighing balance, Autoclave, water bath, hot air oven, centrifuge machines and CO2 Incubator shaker. Currently, he is in the process of learning the data analysis of Flow Cytometry and Mass Spectrometry.
He has previously worked in Sir Ganga Ram Hospital, New Delhi and two other diagnostic centres where he had hands on experience in conducting routine laboratory tests along with RTPCR, ESR,H&E staining, Urine,stool,sputum culture, Leishman, Giemsa,Gram positive and negative staining, Blood group testing, Serology testing (Typhoid, HIV, HCV,HBSAg,Syphilis,Malaria,Dengue IgM/IgG) , BTCT testing and skin test. Apart from this, he gained operational knowledge of instruments like HPLC for HbA1C,ERBA Chem5X(semi-automated),Urinometer (fully automated),Sysmax Coulter, Hemoglobinometer,Fibrometer coagulation and Microtome.
| S. No. | Name of the Project | Description of the Project |
|---|---|---|
| 1. | Development of longitudinal growth reference and assessment of growth velocity, cardio metabolic measures and its correlation among children in India–A prospective study PI: Dr. M. Kalaivani Source of Funding: Indian Council of Medical Research Amount: Rs. 93.44 Lakhs. Status: On going | The objectives of this longitudinal study is to develop age and sex specific percentiles of anthropometric measures, blood pressure, serum lipids and fasting insulin and plasma glucose levels for children aged 7-17 years. Also, to correlate changes in anthropometric measures with blood pressure, serum lipids, fasting insulin and plasma glucose levels over a period of three years in children aged 11-15 years. Data will be obtained from school going children aged 7-17 years from both the government and private schools in Delhi. |
2. Research (Collaborative Research Projects) The faculty and scientists of the department is involved in almost all the research projects being carried out in the institute either as co-investigator or as consultant. They are also involved in many research projects carried out/ being carried out in other medical colleges and research Institutions as statistical consultant or co-investigator. 3. Research (Collaborative Ph.D/ DM/MCH/MD /MS/MDS/MHA Thesis) The faculty and scientists of the department are involved in almost all the Ph.D./ post-graduate theses being carried out in the institute as Co-guide/ DC member/Consultant. Other technical staff will assist faculty and scientists in analysing thesis/collaborative project data. | ||
3. Research (Collaborative Ph.D/ DM/MCH/MD /MS/MDS/MHA Thesis) The faculty and scientists of the department are involved in almost all the Ph.D./ post-graduate theses being carried out in the institute as Co-guide/ DC member/Consultant. Other technical staff will assist faculty and scientists in analysing thesis/collaborative project data. | ||
| S.NO. | NAME | DESIGNATION |
|---|---|---|
| 1 | MRS. REETA DUTTA | T.O. |
| 2 | MR. SATISH KUMAR | M.R.T |
| 3 | MRS. KIRTI RAO | T.O. |
| 4 | MR. YOKESH PATWAL | M.L.T |
| 5 | MR. DAVINDER JANGRA | M.L.T |
| 6 | MRS. UMA PALI | M.L.T |
| 7 | MR. VIKRAM | M.L.T |
| 8 | MR. GAJENDER SINGH | H/A |
| 9 | MR. SUSHIL KUMAR | H/A |
| 10 | MR. SUDARSHAN | H/A |
| 11 | MR. RAJU | H/A |
| 12 | MR. RAVINDER KUMAR | H/A (SULABH) |
| 13 | MR. DEEPAK KUMAR | H/A (SULABH) |
| 14 | MS. SHIVANI | M.L.T (BECIL) |
| 15 | MS. SAVITA | LAB ATTENDANT (BECIL) |
| 16 | MR. AMIT GUPTA | D.E.O (BECIL) |
| 17 | MR. VIKRAM | H/A (SULABH) |
| 18 | MR. SANDEEP KUMAR | T. O. |
| 19 | MR. AMIT KUMAR | O.T.A |
| 20 | MR. BRIJESH | M.L.T |
| 21 | MR. BHUPENDER | JR. M.L.T |
| 22 | MR. DHARA SINGH | H/A |
| S.NO. | NAME | DESIGNATION |
|---|---|---|
| 1 | MR. BISWAJIT MONDAL | S.T.O |
| 2 | MR. MANGAL SINGH | S.T.O. |
| 3 | MR. MAHAVEER SINGH | T.O. |
| 4 | MR. MANISH MITTAL | T.O. |
| 5 | MR. NANDAN SINGH | M.L.T. |
| 6 | MR. SHRIKESH MEENA | M.L.T. |
| 7 | MR. SAURABH VERMA | M.L.T. |
| 8 | MR. IRSHAD AHMED | M.L.T. |
| 9 | MR. RAHUL SHARMA | M.L.T. |
| 10 | MR. UMESH KUMAR | JR. M.L.T |
| 11 | MR. GAURAV SINGH | M.L.T (BECIL) |
| 12 | MR. GULFAM ALI | M.L.T (BECIL) |
| 13 | MR. BALBIR CHAND | T.O. (OT) |
| 14 | MR. SATISH PAL | O.T.A |
| 15 | MR. RASHID ANWAR | O.T.A |
| 16 | MR. VIKAS KUMAR | O.T.A |
| 17 | MR. ABHILASH VIRAHWAL | O.T.A |
| 18 | MR. ANIL KUMAR | O.T.A |
| 19 | MR. AMARJEET YADAV | O.T.A |
| 20 | MR. SANJEEV KUMAR | H/A |
| 21 | MR. SURESH KUMAR | H/A |
| 22 | MR. KAPIL BAISLA | H/A (SULABH) |
| S.NO. | NAME | DESIGNATION |
|---|---|---|
| 1 | MS. RAJNI | P.S. |
| 2 | MRS. SOBHANA A.S. | P.A. |
| 3 | MRS. ANJNA | P.A. |
| 4 | MR. LEELA RAM | H/A |
| 5 | MR. AYUSH | D.E.O (BECIL) |
The Faculty of the Department is involved in the teaching of biostatistical and epidemiological methods and medical demography for various undergraduate, post-graduate and para-medical courses in the Institute. These courses are run throughout each semester, each year. Some of these courses have full paper in biostatistics. The details of these courses are given below:
| S. No. | Name of the Course | Course Details |
|---|---|---|
| 1. | Undergraduate courses | M.B.B.S In addition, to this, two joint seminars on Fertility and Mortality Measurements and Interpretation of Life Table method and Family Planning Evaluation studies are given in collaboration with the Centre for Community Medicine (CCM) during the clinical phase of the MBBS Programme. Post certificate Course in Nursing and |
| 2. | Post-graduate courses | M.D. (Community Medicine) Biotech, M.Sc. (Reproductive Biology and Clinical Embryology) M.Sc. (Nursing) For students of M. Biotech, M.Sc. (Nursing) and M.Sc. (Reproductive Biology and Clinical Embryology) combined course consisting of 45 hours of lectures and assignment is undertaken during the July session every year. During the course, students are taught basics of biostatistical methods relevant to their discipline. An endline evaluation of the course is done |
| 3. | Continuing Medical Education (CME) | The Faculty of the Department regularly participates and delivers lectures under continuing medical education programmes, seminars, national and international conferences and pre-conference courses workshops held in the Institute and at various parts of the country and abroad. |
| S.NO. | NAME | DESIGNATION |
|---|---|---|
| 1 | MRS. REETA DUTTA | T.O. |
| 2 | MR. SATISH KUMAR | M.R.T |
| 3 | MRS. KIRTI RAO | T.O. |
| 4 | MR. YOKESH PATWAL | M.L.T |
| 5 | MR. DAVINDER JANGRA | M.L.T |
| 6 | MRS. UMA PALI | M.L.T |
| 7 | MR. VIKRAM | M.L.T |
| 8 | MR. GAJENDER SINGH | H/A |
| 9 | MR. SUSHIL KUMAR | H/A |
| 10 | MR. SUDARSHAN | H/A |
| 11 | MR. RAJU | H/A |
| 12 | MR. RAVINDER KUMAR | H/A (SULABH) |
| 13 | MR. DEEPAK KUMAR | H/A (SULABH) |
| 14 | MS. SHIVANI | M.L.T (BECIL) |
| 15 | MS. SAVITA | LAB ATTENDANT (BECIL) |
| 16 | MR. AMIT GUPTA | D.E.O (BECIL) |
| 17 | MR. VIKRAM | H/A (SULABH) |
| 18 | MR. SANDEEP KUMAR | T. O. |
| 19 | MR. AMIT KUMAR | O.T.A |
| 20 | MR. BRIJESH | M.L.T |
| 21 | MR. BHUPENDER | JR. M.L.T |
| 22 | MR. DHARA SINGH | H/A |
| S.NO. | NAME | DESIGNATION |
|---|---|---|
| 1 | MR. BISWAJIT MONDAL | S.T.O |
| 2 | MR. MANGAL SINGH | S.T.O. |
| 3 | MR. MAHAVEER SINGH | T.O. |
| 4 | MR. MANISH MITTAL | T.O. |
| 5 | MR. NANDAN SINGH | M.L.T. |
| 6 | MR. SHRIKESH MEENA | M.L.T. |
| 7 | MR. SAURABH VERMA | M.L.T. |
| 8 | MR. IRSHAD AHMED | M.L.T. |
| 9 | MR. RAHUL SHARMA | M.L.T. |
| 10 | MR. UMESH KUMAR | JR. M.L.T |
| 11 | MR. GAURAV SINGH | M.L.T (BECIL) |
| 12 | MR. GULFAM ALI | M.L.T (BECIL) |
| 13 | MR. BALBIR CHAND | T.O. (OT) |
| 14 | MR. SATISH PAL | O.T.A |
| 15 | MR. RASHID ANWAR | O.T.A |
| 16 | MR. VIKAS KUMAR | O.T.A |
| 17 | MR. ABHILASH VIRAHWAL | O.T.A |
| 18 | MR. ANIL KUMAR | O.T.A |
| 19 | MR. AMARJEET YADAV | O.T.A |
| 20 | MR. SANJEEV KUMAR | H/A |
| 21 | MR. SURESH KUMAR | H/A |
| 22 | MR. KAPIL BAISLA | H/A (SULABH) |
| S.NO. | NAME | DESIGNATION |
|---|---|---|
| 1 | MS. RAJNI | P.S. |
| 2 | MRS. SOBHANA A.S. | P.A. |
| 3 | MRS. ANJNA | P.A. |
| 4 | MR. LEELA RAM | H/A |
| 5 | MR. AYUSH | D.E.O (BECIL) |
| Name | Designation | E-mail ID |
|---|---|---|
| Dr. Rajiv Narang | Professor & Head | r_narang@yahoo.com |
| Dr. Sandeep Seth | Professor | drsandeepseth@hotmail.com |
| Dr. Nitish Naik | Professor | nitishnaik@yahoo.co.in |
| Dr. Rakesh Yadav | Professor | rakeshyadav123@yahoo.com |
| Dr. Sandeep Singh | Professor | drssandeep@hotmail.com |
| Dr. Gautam Sharma | Professor | drsharmagautam@gmail.com |
| Dr. Ambuj Roy | Professor | drambujroy@gmail.com |
| Dr. S. Ramakrsihnan | Professor | ramaaiims@gmail.com |
| Dr Saurabh Kr. Gupta | Professor | drsaurabhmd@gmail.com |
| Dr Deepti Siddharthan | Associate Professor | deeptikailath@gmail.com |
| Dr. Satyavir Yadav | Associate Professor | drsatyaviryadav87@gmail.com |
| Dr. Nirmal Ghati | Assistant Professor | nirmal.cmc@gmail.com |
| Dr. Saurabh Agastam | Assistant Professor | sourabhagstam@gmail.com |
| Dr. Aseem Basha | Assistant Professor | draseemaiims@gmail.com |
| Dr. Sumit Kumar | Assistant Professor | sumitvmmc09@gmail.com |
| Dr. Atit Gawalkar | Assistant Professor | atitgawalkar@gmail.com |
Dr. G. Karthikeyan (Professor, karthik2010) is currently on deputation to Translational Health Science and Technology Institute, Faridabad
Short-Term (Upto 6 months)/Long-Term (Upto 2 years) Observership will be provided to candidates sponsored by Government Institutions/Autonomous Bodies (Government funded)/Defense services only. Applicants must continue to be in training/employment of the sponsoring institution till the end of obsevership at AIIMS, New Delhi.
Fee: Indian Nationals, trainees from SAARC countries and from low income developing countries will be charged obsevership fee of Rs.2000/- per month.
The Ph.D. Programme in the Department was started in January, 1988. Seventeen students have been admitted to this Programme so far, of which sixteen have been awarded the Doctorate Degree.
Rules regarding admission under Ph.D. programme
Master’s degree in Biostatistics/Statistics with at least 60% marks.
This Exam has written test followed by departmental assessment. It is conducted only in Delhi, twice a year, in January and July, subject to availability of seat.
Selection for Ph.D. registration is made through two stage performance evaluation as follows:
The written test carries 80 marks of 90 minutes duration. The question paper consists of Multiple Choice Questions (MCQs) from Statistics/Biostatistics/General knowledge.
Candidates who secure at least 50% marks in the written test (Stage-I), are called for departmental assessment (carrying 20 marks).
Admission to Ph.D. Course is subject to the availability of research funds/fellowship/grant from recognized funding agencies or availability of research projects in the Department of Biostatistics, AIIMS. There is no institute fellowship for Ph.D. course.
3-5 years
National Drug Dependence Treatment Centre
Sector-19, Kamla Nehru Nagar
C.G.O. Complex, Ghaziabad(U.P.)
Tel: 0120-2788974, Fax: 0120-2788979
nddtc[at]aiims[dot]ac[dot]in
National Drug Dependence Treatment Centre
Sector-19, Kamla Nehru Nagar
C.G.O. Complex, Ghaziabad(U.P.)
Tel: 0120-2788974, Fax: 0120-2788979
nddtc[at]aiims[dot]ac[dot]in
| Name | Designation Held | |
|---|---|---|
| Dr. K. Ramachandran | Professor & Founder Head (Oct. 1973 to Jan. 1991) | - |
| Dr. K. R. Sundaram | Professor & Head (Feb. 1991 to Oct. 2005) | krsundaram[at]aims[dot]amrita[dot]edu |
| Dr. R. M. Pandey | Professor & Head (Nov 2005 to Dec 2021) | rmpandey[at]yahoo[dot]com |
| Name | Designation Held | |
|---|---|---|
| Dr. K. Ramachandran | Professor (Oct. 1973 to Jan. 1991) | - |
| Dr. K. R. Sundaram | Professor (Jan. 1976-Oct. 2005) | krsundaram[at]aims[dot]amrita[dot]edu |
| Dr. V. Sreenivas | Professor (Dec. 2001-May 2020) | sreenivas_vishnu[at]yahoo[dot]com |
| Dr. S. N. Dwivedi | Professor (Apr. 1991-Jul. 2021) | Dwivedi7[at]gmail[dot]com |
| Dr. R. M. Pandey | Professor (Nov. 2005 to Dec. 2021) | rmpandey[at]yahoo[dot]com |
| Name | Designation Held | |
|---|---|---|
| Shri. B. S. Parmar | Research Officer | |
| Dr. Rajvir Singh | Scientist - I | rajvir_aiims[at]yahoo[dot]com |
| Shri. R. K. Ahuja | Research Officer (S-I) | rkahuja1951[at]hotmail[dot]com |
| Dr. Guresh Kumar | Scientist-I | chibbegk[at]hotmail[dot]com |
| Dr. M. Kalaivani | Scientist-I | manikalaivani[at]gmail[dot]com |
| Name | Designation Held | |
|---|---|---|
| Shri. Ombir Singh | Statistician | - |
| Shri. Kulwant Singh Kapoor | Statistician | kulwantsinghus[at]yahoo[dot]com |
| Shri. Ashish Datt Upadhayay | Junior Statistician | ashish.upadhayay76[at]gmail[dot]com |
| Mr. Abhay Kumar | Statistical Assistant | - |
| Mr. Pushparaj | Statistical Assistant | shishodiyapushpraj[at]gmail[dot]com |
South Asia's first Mobile Methadone Clinic
"Action Plan for Substance Use Management in Children"
Substance Use Disorders or Addictive Disorders are major public health problems in India. Whileproviding treatment and care to millions of patients affected by the common addiction-relatedproblems always remains a challenge, the average mental health professional is bludgeoned todayby newer issues and challenges which necessitate refreshing and updating the professionalknowledge and skills. In order to address this, a National Continuing Medical Education (CME)program was organized jointly by three reputed bodies: AIIMS, New Delhi; National Academy ofMedical Sciences (NAMS) and Indian Association for Social Psychiatry (IASP), on 22 July 2017at NAMS Auditorium in New Delhi.

Director AIIMS, Padmashree Dr. RandeepGuleria was the Chief Guest,while Shri AK Jha Economic Advisor, Ministry ofHealth and Family Welfare, Government of India wasthe Guest of Honor.The well-rounded and comprehensive programme comprised of a healthy mix of lectures andpresentations by the nationally renowned faculty members, interactive discussions and a PanelDiscussion with leading stakeholders and policy makers. More than 150 delegates (mostly traineesand younger specialists) attended the event in person while close to 80 delegates participatedvirtually from remote locations in AIIMS, Bhubneswar and AIIMS, Jodhpur.
The 14th Annual Day of National Drug Dependence Treatment Centre (NDDTC), All India Institute of Medical Sciences (AIIMS), New Delhi was celebrated at NDDTC, Ghaziabad on 13th April 2017. MsJagjitPavadia, Vice President, International Narcotics Control Board was the Chief Guest on the occasion. MrArun Kumar Jha, Joint Secretary, Ministry of Health and Family Welfare, Government of India was the Guest of Honour. Prof (Dr) Balram Airan, Dean, AIIMS, New Delhi and Prof (Dr) DK Sharma, Medical Superintendent, AIIMS, New Delhi graced the event. Prof (Dr) Rakesh Chadda, Chief NDDTC and Head Department of Psychiatry, AIIMS presented the Annual Report for the year 2016- 2017 highlighting the achievements of the center.

The program was attended by around 200 participants, including faculty from NDDTC and Department of Psychiatry, resident doctors, students, and staff from NDDTC, along with guests from various organizations (including UNODC), NGOs and Ingraham School, Ghaziabad. The theme for symposium for this year’s annual day was ‘Women Substance Use’. The ‘Family Empowerment Clinic’ was also inaugurated on this occasion.
South Asia's first Mobile Methadone Clinic
"Action Plan for Substance Use Management in Children"
Substance Use Disorders or Addictive Disorders are major public health problems in India. Whileproviding treatment and care to millions of patients affected by the common addiction-relatedproblems always remains a challenge, the average mental health professional is bludgeoned todayby newer issues and challenges which necessitate refreshing and updating the professionalknowledge and skills. In order to address this, a National Continuing Medical Education (CME)program was organized jointly by three reputed bodies: AIIMS, New Delhi; National Academy ofMedical Sciences (NAMS) and Indian Association for Social Psychiatry (IASP), on 22 July 2017at NAMS Auditorium in New Delhi.
Director AIIMS, Padmashree Dr. RandeepGuleria was the Chief Guest,while Shri AK Jha Economic Advisor, Ministry ofHealth and Family Welfare, Government of India wasthe Guest of Honor.The well-rounded and comprehensive programme comprised of a healthy mix of lectures andpresentations by the nationally renowned faculty members, interactive discussions and a PanelDiscussion with leading stakeholders and policy makers. More than 150 delegates (mostly traineesand younger specialists) attended the event in person while close to 80 delegates participatedvirtually from remote locations in AIIMS, Bhubneswar and AIIMS, Jodhpur.
The 14th Annual Day of National Drug Dependence Treatment Centre (NDDTC), All India Institute of Medical Sciences (AIIMS), New Delhi was celebrated at NDDTC, Ghaziabad on 13th April 2017. MsJagjitPavadia, Vice President, International Narcotics Control Board was the Chief Guest on the occasion. MrArun Kumar Jha, Joint Secretary, Ministry of Health and Family Welfare, Government of India was the Guest of Honour. Prof (Dr) Balram Airan, Dean, AIIMS, New Delhi and Prof (Dr) DK Sharma, Medical Superintendent, AIIMS, New Delhi graced the event. Prof (Dr) Rakesh Chadda, Chief NDDTC and Head Department of Psychiatry, AIIMS presented the Annual Report for the year 2016- 2017 highlighting the achievements of the center.
The program was attended by around 200 participants, including faculty from NDDTC and Department of Psychiatry, resident doctors, students, and staff from NDDTC, along with guests from various organizations (including UNODC), NGOs and Ingraham School, Ghaziabad. The theme for symposium for this year’s annual day was ‘Women Substance Use’. The ‘Family Empowerment Clinic’ was also inaugurated on this occasion.
The National Drug Dependence Treatment Centre (NDDTC), AIIMS has initiated a new service – delivery of methadone through a mobile van in East Delhi. The new service delivery was inaugurated by the AIIMS Director, Prof. Randeep Guleria on 22 March 2019 in the presence of officers from National AIDS Control Organisation (NACO), United Nations Office on Drugs and Crime (UNODC), and the Director General Health Services, Govt. of Delhi. Representatives from NGOs, and drug user community also attended the inauguration event.
Opioid Addiction is a significant problem in India. The recently released report of National Survey last month estimated that India has about 28 Lakh people affected by addiction to opioids such as heroin, opium and various pharmaceutical products. These people require medicines such as methadone or buprenorphine for treatment of opioid addiction. However, there are very few treatment centres providing these medicines, while the need is very high. It is estimated that less than two percent of the population addicted to opioids in India is receiving this treatment, which is recommended by various UN bodies and the World Health Organization (WHO).
Since methadone is a highly regulated medicine it is only provided as daily observed treatment. This medicine is available in just about a dozen cities in India. “Patients often find it difficult to come to the clinic daily to receive methadone, which leads to patients dropping-out of treatment midway”, informed Dr. Ravindra Rao, in-charge of the methadone clinic. The mobile methadone dispensing unit plans to bridge this gap and improve retention of patients into treatment enabling them to work and lead a healthier life. Currently, such dispensing vans or buses are available in few select developed countries in the world, such as USA, Portugal, Spain, Canada and Netherlands. With the launch of mobile delivery of methadone, India joins this elite club. In fact, India is the first country in the South Asian Region to initiate these services.
The van will be parked at strategic places in East Delhi and adjoining areas for fixed time period in the day, where the patients can come and receive their medicine without having to travel to the main clinic. “In the trial run for last two weeks we already have more than two dozen patients enrolled in the facility and the response is very encouraging” informed Dr. Rao. This number is expected to reach about 100 patients per day, very soon. Based on the success of this initiative, this new approach can be scaled-up in different parts of the country.
For Detail Please Click Here
The National Drug Dependence Treatment Centre (NDDTC), AIIMS has initiated a new service – delivery of methadone through a mobile van in East Delhi. The new service delivery was inaugurated by the AIIMS Director, Prof. Randeep Guleria on 22 March 2019 in the presence of officers from National AIDS Control Organisation (NACO), United Nations Office on Drugs and Crime (UNODC), and the Director General Health Services, Govt. of Delhi. Representatives from NGOs, and drug user community also attended the inauguration event.
Opioid Addiction is a significant problem in India. The recently released report of National Survey last month estimated that India has about 28 Lakh people affected by addiction to opioids such as heroin, opium and various pharmaceutical products. These people require medicines such as methadone or buprenorphine for treatment of opioid addiction. However, there are very few treatment centres providing these medicines, while the need is very high. It is estimated that less than two percent of the population addicted to opioids in India is receiving this treatment, which is recommended by various UN bodies and the World Health Organization (WHO).
Since methadone is a highly regulated medicine it is only provided as daily observed treatment. This medicine is available in just about a dozen cities in India. “Patients often find it difficult to come to the clinic daily to receive methadone, which leads to patients dropping-out of treatment midway”, informed Dr. Ravindra Rao, in-charge of the methadone clinic. The mobile methadone dispensing unit plans to bridge this gap and improve retention of patients into treatment enabling them to work and lead a healthier life. Currently, such dispensing vans or buses are available in few select developed countries in the world, such as USA, Portugal, Spain, Canada and Netherlands. With the launch of mobile delivery of methadone, India joins this elite club. In fact, India is the first country in the South Asian Region to initiate these services.
The van will be parked at strategic places in East Delhi and adjoining areas for fixed time period in the day, where the patients can come and receive their medicine without having to travel to the main clinic. “In the trial run for last two weeks we already have more than two dozen patients enrolled in the facility and the response is very encouraging” informed Dr. Rao. This number is expected to reach about 100 patients per day, very soon. Based on the success of this initiative, this new approach can be scaled-up in different parts of the country.
For Detail Please Click Here
| Name | Designation | E-mail ID |
|---|---|---|
| Dr. Rajiv Narang | Professor & Head | r_narang[at]yahoo[dot]com |
| Dr. Sandeep Seth | Professor | drsandeepseth[at]hotmail[dot]com |
| Dr. Nitish Naik | Professor | nitishnaik[at]yahoo[dot]co[dot]in |
| Dr. Rakesh Yadav | Professor | rakeshyadav123[at]yahoo[dot]com |
| Dr. Sandeep Singh | Professor | drssandeep[at]hotmail[dot]com |
| Dr. Gautam Sharma | Professor | drsharmagautam[at]gmail[dot]com |
| Dr. Ambuj Roy | Professor | drambujroy[at]gmail[dot]com |
| Dr. S. Ramakrsihnan | Professor | ramaaiims[at]gmail[dot]com |
| Dr Saurabh Kr. Gupta | Professor | drsaurabhmd[at]gmail[dot]com |
| Dr Deepti Siddharthan | Associate Professor | deeptikailath[at]gmail[dot]com |
| Dr. Satyavir Yadav | Associate Professor | drsatyaviryadav87[at]gmail[dot]com |
| Dr. Nirmal Ghati | Assistant Professor | nirmal.cmc[at]gmail[dot]com |
| Dr. Saurabh Agastam | Assistant Professor | sourabhagstam[at]gmail[dot]com |
| Dr. Aseem Basha | Assistant Professor | draseemaiims[at]gmail[dot]com |
| Dr. Sumit Kumar | Assistant Professor | sumitvmmc09[at]gmail[dot]com |
| Dr. Atit Gawalkar | Assistant Professor | atitgawalkar[at]gmail[dot]com |
Dr. G. Karthikeyan (Professor, karthik2010) is currently on deputation to Translational Health Science and Technology Institute, Faridabad
| Name | Designation | Contact No. | |
|---|---|---|---|
| Mr. Hem Chandra Sati | Junior Statistician | 26594256 | hem198617[at]yahoo[dot]com |
| Ms. N. Veena | Personal Assistant | 26593240 | vnabaliga[at]gmail[dot]com |
| Mr. Narender Kumar | DEO Gr. ‘A’ | 26593240 | narender_bobby[at]hotmail[dot]com |
| Mr. Vaibhav Saxena | DEO (Contractual) | 26593240 | vaibhavsaxena.08[at]gmail[dot]com |
| Mr. Vinod Kr. Chavan | Animal House Attendant | 26593240 | - |
| Name of Staff | Designation | Contact No. | |
|---|---|---|---|
| Dr. Shivam Pandey | Scientist-I | 26594256 8375981747 | shivam_pandey[at]hotmail[dot]com |
| Ms. Nilima | Scientist-I | 26546773 7676843506 | >nilima3012[at]gmail[dot]com |
| Dr. Sumit Kr. Das | Scientist-I | 26594256 9932756575 | sumitaiimsbiostat[at]gmail[dot]com |

Left to Right: Mr. Manish, Mr. Hari Om, Mr. Kartikeyan, Mrs. Nazmeen, Dr. Archana Singh
1. CEA
2. CA 19.9
3. PSA
4. CA125
5. CA 15.3
6. AFP
7. Testosterone
8. FSH
9. Total T3, Total T4 and TSH
10. Vitamin B12
11. Ferritin
12. Folate
Principle: These tests are being carried out on a chemiluminiscence based immunoassay auto analyser, which is considered as the gold standard for such testing.
Sample collection/sample receiving: Room No. 3049, Department of Biochemistry. Sample collection is done on all working days.
Timings for sample collection: 10:00 AM to 12:30 PM and 2:30 PM to 4:30 PM on all working days (Saturday-10:30 AM to 12:30 PM only).
Test reports: Turnaround time is 24 hours of sample collection. Report will be available in room no. 3049.
Quality control: Our laboratory is carrying out both internal and external quality control assurance programme to deliver quality reports.
Laboratory staff: Mr. Kartikeyan, Mrs. Nazmeen, Mr. Hariom, Mr. Manish
Faculty in-charge: Dr. Archana Singh (II) Phone: Extn. 3467
Note: All outpatients and inpatients including EHS beneficiaries with valid UHID who require any of these tests can contact Room No. 3049 (phoneno:26594267), Department of Biochemistry.

Mr. S. Karthikeyan has completed his D.M.L.T. from Madras Medical College in 1991. He is working as Technical Officer in Biochemistry Department since February 1996. He has 20 years experience in Patient Care Lab. His nature of duties include handling patient blood samples and reporting of all Tumour Markers, Thyroid Profile, Anaemia Profile, Infertility Test through chemiluminiscence based Auto Analyzer and ELISA Reader, maintaining Internal Quality, External Quality, Standardization and Calibration according to NABL. He also maintains the log book of machine maintenance, patient's record, stock reagents and other instruments. He is experienced in handling instruments like FACS Canto Flowcytometer, Confocal Microscope, Inverted Microscope, Nano Drop, and Fluorescence Spectrophotometer.

Mrs. Nazmeen Khan has completed her B.Sc. from Madhya Pradesh Bhoj University, Bhopal, Madhya Pradesh in 1999. She is working as Senior Lab. Technologist in the Dept. Of Biochemistry since December 2004. She has 12 years experience in Research Lab and Patient Care Lab. Her duties include handling patient blood samples and reporting of all Tumour Markers, Thyroid Profile, Anaemia Profile, Infertility Test through chemiluminiscence based Auto Analyzer and ELISA Reader, maintaining Internal Quality, External Quality, Standardization and Calibration according to NABL. She also maintains the log book of machine maintenance, patient's record, stock reagents and other instruments. She is experienced in handling instruments like FACS Canto Flowcytometer, Confocal Microscope, Inverted Microscope, Nano Drop, and Fluorescence Spectrophotometer.

He is working as Medical Lab. Technologist in Biochemistry Department since March 2003. He has 13 years of experience in Research Lab, Culture Lab, UG Lab and Patient Care Lab. His nature of duties include handling patient blood samples and reporting of all Tumour Markers, Thyroid Profile, Anaemia Profile, Infertility Test through chemiluminiscence based Auto Analyzer and ELISA Reader, maintaining Internal Quality, External Quality, Standardization and Calibration according to NABL. He also maintains the log book of machine maintenance, patient's record, stock reagents and other instruments. He is experienced in handling instruments like FACS Canto Flowcytometer, Confocal Microscope, Inverted Microscope, Nano Drop, and Fluorescence Spectrophotometer.
He is working as Junior Medical Lab. Technologist in Biochemistry Department since November 1988. He has 27 years of experience in Research Lab and Patient Care Lab. His nature of duties are like handling patient blood sample of all Tumour Markers, Thyroid Profile, Anemia Profile, Infertility test, maintaining log book, machine maintenance, Stock reagents, processing and keeping records of bills.
The curricula is vibrant with regular opportunities for students to interact with faculty and other members. These include journal club presentations and seminars. Newly enrolled students (M.D., M.Sc.) undergo a departmental rotation with all faculty members. They are then required to join a faculty under whose supervision they will work on a research problem, present their protocol and submit their dissertation. Several new modules have been introduced for the newly enrolled students. These include microteaching (innovative teaching methods, problem-based learning), an introduction to “R”-driven data analytics and soft-skill training. Additionally, the students are examined for their proficiency in general Biochemistry through regular assessments. The Ph.D. program, includes course work which is spread over two semesters. This is composed of didactic classes and includes generalized and specialized Biochemistry, biomedical waste management, ethics, and Biostatistics. Practical training via hands-on laboratory work is practiced. This is aimed at orienting and equipping the scholars with the knowledge and means to undertake full-time research work. The scholars are issued a completion certificate at the end of this.
| Name of Faculty | Designation | Contact No. | |
|---|---|---|---|
| Dr.Maroof Ahmad Khan | Professor & Head | 26593240/26593395/ 9868106928 / 9868397945 | khanmaroofahmad[at]gmail[dot]com |
| Dr. M Kalaivani | Assistant Professor | 26546773/9717319082 | manikalaivani[at]gmail[dot]com |




Left- Mr Fateh Singh, Right- Mr Karan
The curricula is vibrant with regular opportunities for students to interact with faculty and other members. These include journal club presentations and seminars. Newly enrolled students (M.D., M.Sc.) undergo a departmental rotation with all faculty members. They are then required to join a faculty under whose supervision they will work on a research problem, present their protocol and submit their dissertation. Several new modules have been introduced for the newly enrolled students. These include microteaching (innovative teaching methods, problem-based learning), an introduction to “R”-driven data analytics and soft-skill training. Additionally, the students are examined for their proficiency in general Biochemistry through regular assessments. The Ph.D. program, includes course work which is spread over two semesters. This is composed of didactic classes and includes generalized and specialized Biochemistry, biomedical waste management, ethics, and Biostatistics. Practical training via hands-on laboratory work is practiced. This is aimed at orienting and equipping the scholars with the knowledge and means to undertake full-time research work. The scholars are issued a completion certificate at the end of this
The undergraduate laboratory of the department of biochemistry is the hub for teaching the practical aspects of biochemistry to first semester students. The range of practicals covered under the syllabi include simple colorimetry based analyte estimations, such as for glucose proteins to more exhaustive experiments involving lipid analysis, ELISAs, PCRs, enzyme assays and chromatographic analysis.
A faculty in-charge is assigned for overall supervision and the laboratory is permanently staffed by technical support staff that supports the residents in preparing for experiments, manage the chemicals, glassware (or consumables) and instrument inventory, provide necessary logistic support for preparing the laboratory, manage the routine administrative matters, and supervise its cleaning and maintenance.
The laboratory is housed in a spacious, well-ventilated area and has all the necessary infrastructure to support the practical teaching experiments such as colorimeters, incubators, ovens, pH meter etc as a well stocked chemicals repository. Practical experiments are performed by undergraduates supervised by in-house residents.
1. Mr Fateh Singh, Technical Officer
He has done his B.Sc. (MLT) from CCSU, Meerut. He joined AIIMS in the year 1993. He supervises the standardization of all routine UG and PG practicals as well as practical examinations. He is also involved in trouble shooting of practical experiments. He guides fellow colleagues to get trained in biochemistry practical standardization. He also has expertise in blood sampling.
2. Mr Karan Singh, Lab Attendant
He is working from Feb 2014. He helps in arranging instruments and reagents that are used in practical.
Content Provider: Dr. M. Kalaivani
| The content and character of the discipline of Biostatistics has undergone a radical change during the last few decades. From being a passive and descriptive discipline, Biostatistics has emerged as a vigorous, dynamic, and constructive instrument of decision-making in the area of health and medical care. Powerful and sophisticated statistical techniques of planning and analysis of biological experiments and investigations, development of probabilistic models in epidemiology and application of operations research techniques in health care delivery have opened up new dimensions and capabilities in medical and health research. In this context, a medical person’s training, particularly that of a medical researcher, would be considered incomplete today without a reasonable acquaintance with the potentialities of applications of bio-statistical techniques to enable him/her to plan his/her research studies with scientifically and statistically valid designs and to arrive at valid and meaningful conclusions applying appropriate statistical methods. At the All India Institute of Medical Sciences (AIIMS), Biostatistics was a part of the then Department of Preventive and Social Medicine till 1973. In October 1973, an independent Biostatistics Unit was carved out from the Department of Preventive and Social Medicine. In 1986, the “Biostatistics Unit” was renamed as the “Department of Biostatistics” fulfilling a long felt need for such a department. As an independent department, it caters to the needs of all the faculty, scientific staff and students in the Institute in teaching and research. |
The curricula is vibrant with regular opportunities for students to interact with faculty and other members. These include journal club presentations and seminars. Newly enrolled students (M.D., M.Sc.) undergo a departmental rotation with all faculty members. They are then required to join a faculty under whose supervision they will work on a research problem, present their protocol and submit their dissertation. Several new modules have been introduced for the newly enrolled students. These include microteaching (innovative teaching methods, problem-based learning), an introduction to “R”-driven data analytics and soft-skill training. Additionally, the students are examined for their proficiency in general Biochemistry through regular assessments. The Ph.D. program, includes course work which is spread over two semesters. This is composed of didactic classes and includes generalized and specialized Biochemistry, biomedical waste management, ethics, and Biostatistics. Practical training via hands-on laboratory work is practiced. This is aimed at orienting and equipping the scholars with the knowledge and means to undertake full-time research work. The scholars are issued a completion certificate at the end of this.
The Department conducts MSc, MD and PhD courses for graduate and post-graduate students apart from teaching undergraduate medical and nursing students.
Name of Faculty Member: Dr. Alpana Sharma
Designation: Professor
Address: Room No. 3015, 3rd Floor, Department of Biochemistry, AIIMS, New Delhi
Official Phone: +91-11-26546665
Email id: dralpanasharma[at]gmail[dot]com
PhD in Biochemistry in 1987, JN Medical College, Aligarh Muslim University, Aligarh
M.Phil. in Biochemistry in 1982, JN Medical College, Aligarh Muslim University, Aligarh
M.Sc. in Biochemistry in 1980, Aligarh Muslim University, Aligarh
| Position | Department | University/ Institution | Dates |
|---|---|---|---|
| Professor | Biochemistry | AIIMS, New Delhi | 01/07/2014-till date |
| Additional Professor | Biochemistry | AIIMS, New Delhi | 01/07/2010-30/06/2014 |
| Associate Professor | Biochemistry | AIIMS, New Delhi | 01/07/2007-30/06/2010 |
| Assistant Professor | Biochemistry | AIIMS, New Delhi | 01/06/2003- 30/06/2007 |
Fellow of NAMS (FAMS)
Fellow of IABS (FIABS)
Research Focus of the Lab
The primary goal of Dr. Alpana Sharma’s lab is to understand major biological processes at the molecular and immune level with the ultimate aim of alleviating human disease by identification of novel therapeutic agents/targets. To accomplish this, Dr. Sharma’s lab focuses on elucidating the diverse mechanisms of immune escape and exhaustion in solid tumors such as renal cell cancer and bladder cancer wherein the role of memory T cells, regulatory B cells and tumor associated macrophages is being explored. Furthermore, the immune-pathogenesis of autoimmune skin diseases is being studied in order to understand the T-cell biology and crosstalk between macrophages, dendritic cells and NK cells in Pemphigus Vulgaris and Vitiligo. Moreover, the impact of MDSCs and Tregs in atherosclerosis is also another field of interest.
The other field of research is to explore the importance of bone marrow microenvironment in multiple myeloma and cancers of urinary bladder cancer. Her laboratory is interested in identifying biomarkers of diagnostic potential in cancer. In addition, the role of microRNAs in diagnostics and therapeutics of cancer is being studied. Dr. Sharma’s lab is also elucidating anti-cancer potential of natural products. The small molecule based therapeutic drug screening and identification is also an ongoing research work in lab.
Postdoctoral Fellows
Senior Demonstrator
PhD Students
Project Staff
M.Sc. Student
Attendants
Funding Source
List of publications is available on following link:
| Name | Designation | Research theme(s)/Laboratory name | |
|---|---|---|---|
| Dr. Alpana Sharma | Professor | dralpanasharma[at]gmail[dot]com | Immunology and Molecular Biology Laboratory |
| Dr. Shyam S. Chauhan | Professor | s_s_chauhan[at]hotmail[dot]com | Laboratory of Translational and Molecular Oncology |
| Prof. Subrata Sinha | Professor & Head | sub_sinha[at]hotmail[dot]com | Laboratory of Translational Biology |
| Sr. No. | Enrollment No. | Name | D.O.J |
|---|---|---|---|
| 1 | P-2022/16979 | Ms. Kavita | 24.09.2022 |
| 2 | P-2022/16980 | Ms. Mahek Farhan | 24.09.2022 |
| 3 | P-2022/16981 | Ms. Nisha Kumari | 24.09.2022 |
| 4 | P-2022/16982 | Mr. Anish Kumar Chauhan | 24.09.2022 |
| 5 | P-2022/16983 | Ms. Isha Rathore | 24.09.2022 |
| 6 | P-2022/16984 | Ms. Shikha Roy | 03.10.2022 |
| 7 | P-2023/17085 | Ms. Neeti Bharadwaj | 12.08.2023 |
| 8 | P-2023/17086 | Ms. Dakshita Joshi | 12.08.2023 |
| 9 | P-2023/17087 | Ms. Bindiya | 12.08.2023 |
| 10 | P-2023/17088 | Ms. Nishu | 12.08.2023 |
| 11 | P-2023/17089 | Mr. Ankit Kumar | 14.09.2023 |
| 12 | P-2023/17090 | Ms. Daina Sapam | 14.09.2023 |
| 13 | P-2023/17091 | Ms. Aisha Farhat | 12.08.2023 |
Centre for Biomedical Engineering have four core research areas: Biomaterials, Bioinstrumentation, Medical Imaging, and Biomechanics. Centre’s research areas include: Biosensor applications, vascular cell mechanics, molecular markers in diabetes; Lab-on-a-chip; Microfluidics; Capillary Electrophoresis Microchip; Rehabilitation Engineering, Biomedical Transducers and Sensors, Controlled Drug Delivery System, technical validation of Alternate medicine, neuro endoscopy, Integrated Health Care.; Nano medicine, Drug delivery systems ,Soft skin regeneration, Brain and cancer targeting of bioactive molecules; Food Science technology, Chemistry; Orthopaedics, Biomechanics, Recombinant DNA, synthetic biology; Near-infrared optical imaging technology with focus on instrument development, Medical Imaging, MRI CT technique and clinical applications, Quantitative Imaging, Medical Image and signal processing, Analysis and software packaging, bench to bedside research from phantoms to in-vivo in the areas of breast cancer, functional brain translational mapping, and wound care healing.
The average number of Ph.D.’s graduated over the last 5 years per faculty has been 4.4 and the average SCOPUS cited publication per faculty is 8. The amount of research projects per faculty is 70 Lakhs and industrial consultancy is 1.44 Lakhs per faculty per year in past 5 years. Recently major facilities such as confocal laser and Raman spectroscopy have been installed. New labs based on drug delivery, Skin Regeneration, Lab-on-a-chip, laser micromachining and Medical Image Processing have been initiated.
Novel kit for assay of iron in biological fluids; Modulated DC Iontophoretic Device; electrooculogram based Multi-mode Controller; Device for External Counter Pulsation Therapy ; Zig-G, A Wireless ECG system; A Pneumatic Damper Controlled AK Prosthesis; Development of a Biomedical Engineering application Toolkit (BEAT); Contra Lateral Limb Controlled Prosthetic Knee Joint; Wireless ECG patch and system for obtaining High Definition mobile ECG; A Surgical Stapler; Bilayer dressing for wound healing; Point of Care Hb-meter.
Centre for Biomedical Engineering have four core research areas: Biomaterials, Bioinstrumentation, Medical Imaging, and Biomechanics. Centre’s research areas include: Biosensor applications, vascular cell mechanics, molecular markers in diabetes; Lab-on-a-chip; Microfluidics; Capillary Electrophoresis Microchip; Rehabilitation Engineering, Biomedical Transducers and Sensors, Controlled Drug Delivery System, technical validation of Alternate medicine, neuro endoscopy, Integrated Health Care.; Nano medicine, Drug delivery systems ,Soft skin regeneration, Brain and cancer targeting of bioactive molecules; Food Science technology, Chemistry; Orthopaedics, Biomechanics, Recombinant DNA, synthetic biology; Near-infrared optical imaging technology with focus on instrument development, Medical Imaging, MRI CT technique and clinical applications, Quantitative Imaging, Medical Image and signal processing, Analysis and software packaging, bench to bedside research from phantoms to in-vivo in the areas of breast cancer, functional brain translational mapping, and wound care healing.
The average number of Ph.D.’s graduated over the last 5 years per faculty has been 4.4 and the average SCOPUS cited publication per faculty is 8. The amount of research projects per faculty is 70 Lakhs and industrial consultancy is 1.44 Lakhs per faculty per year in past 5 years. Recently major facilities such as confocal laser and Raman spectroscopy have been installed. New labs based on drug delivery, Skin Regeneration, Lab-on-a-chip, laser micromachining and Medical Image Processing have been initiated.
Novel kit for assay of iron in biological fluids; Modulated DC Iontophoretic Device; electrooculogram based Multi-mode Controller; Device for External Counter Pulsation Therapy ; Zig-G, A Wireless ECG system; A Pneumatic Damper Controlled AK Prosthesis; Development of a Biomedical Engineering application Toolkit (BEAT); Contra Lateral Limb Controlled Prosthetic Knee Joint; Wireless ECG patch and system for obtaining High Definition mobile ECG; A Surgical Stapler; Bilayer dressing for wound healing; Point of Care Hb-meter.
| Sr.No. | ENROLMENT NUMBER | TITLE | NAME | DATE OF JOINING | SESSION | CHIEF SUPERVISOR | DESIGNATION |
|---|---|---|---|---|---|---|---|
| 1 | P-2019/14812 | MS. | MRIDULA SHARMA | 22.07.2019 | JAN&JUL'2019 | DR. SUBRATA SINHA | PROFESSOR |
| 2 | P-2019/14814 | MS. | ALISHA ARORA | 01.08.2019 | JAN&JUL'2019 | DR. ARCHANA SINGH | ADDITIONAL PROFESSOR |
| 3 | P-2019/14815 | MR. | SAGAR TYAGI | 01.08.2019 | JAN&JUL'2019 | DR. SUDIP SEN | PROFESSOR |
| 4 | P-2019/14817 | MS. | ANTARA MALIK | 31.07.2019 | JAN&JUL'2019 | DR. KALPANA LUTHRA | PROFESSOR |
| 5 | P-2019/14818 | MS. | RASHMI GUPTA | 26.08.2019 | JAN&JUL'2019 | DR. ASHOK SHARMA | ADDITIONAL PROFESSOR |
| 6 | P-2019/14819 | MS. | MAHAIWON SHADANG | 01.08.2019 | JAN&JUL'2019 | DR. RIYAZ AHMAD MIR | ASSOCIATE PROFESSOR |
| 7 | P-2020/14861 | MS. | SHAIFALI SHARMA | 14.02.2020 | JAN'2020 | DR. KALPANA LUTHRA | PROFESSOR |
| 8 | P-2020/14898 | MR. | BLESSED RAJ | 04.11.2020 | JUL'2020 | DR. RAKHEE YADAV | ASSOCIATE PROFESSOR |
| 9 | P-2020/14899 | MS. | RUPINDER KAUR | 04.11.2020 | JUL'2020 | DR. PRMAOD KUMAR GAUTAM | ASSOCIATE PROFESSOR |
| 10 | P-2020/14900 | MS. | MANVI ARORA | 06.11.2020 | JUL'2020 | DR. KUNZANG CHOSDOL | PROFESSOR |
| 11 | P-2020/14901 | MR. | DEEPAK | 17.10.2020 | JUL'2020 | DR. ARCHANA SINGH | ADDITIONAL PROFESSOR |
| 12 | P-01-2021/14952 | DR. | VADANYA SHRIVASTAVA | 10.04.2021 | JAN'2021 | DR. SUDIP SEN | PROFESSOR |
| 13 | P-01-2021/14953 | DR. | SANKET KATPARA | 07.04.2021 | JAN'2021 | DR. KALPANA LUTHRA | PROFESSOR |
| 14 | P-01-2021/14955 | MR. | MOHAMMAD SABIQUE BEG | 12.04.2021 | JAN'2021 | DR. PARTHAPRASAD CHATTOPADHYAY | PROFESSOR |
| 15 | P-01-2021/14956 | MR. | SANTOSH KUMAR | 12.04.2021 | JAN'2021 | DR. ASHOK SHARMA | ADDITIONAL PROFESSOR |
| 16 | P-01-2021/14956 (A) | MS. | ISHU | 29.05.2021 | JAN'2021 | DR JAYANTH KUMAR | ADDITIONAL PROFESSOR |
| 17 | P-01-2021/14956 (B) | MR. | NEHA KASHYAP | 24.06.2021 | JAN'2021 | DR SUBHRADIP KARMAKAR | ADDITIONAL PROFESSOR |
| 18 | P-07-2021/14988 | MR. | HARSH BHAKHRI | 04.12.2021 | JUL'2021 | DR. KALPANA LUTHRA | PROFESSOR |
| 19 | P-07-2021/14989 | MS. | HEMA YADAV | 04.12.2021 | JUL'2021 | DR. RIYAZ AHMAD MIR | ASSOCIATE PROFESSOR |
| 20 | P-01-2022/15016 | MS. | RITIKA SINGH | 12.04.2022 | JAN'2022 | DR. PARTHAPRASAD CHATTOPADHYAY | PROFESSOR |
| 21 | P-07-2022/15046 | MS. | AYESHA RAHMAN | 26.09.2022 | JAN'2022 | DR. RIYAZ AHMAD MIR | ASSOCIATE PROFESSOR |
| 22 | P-01-2023/15077 | MS. | TANU BANSAL | 26.09.2023 | JAN'2023 | DR JAYANTH KUMAR | ADDITIONAL PROFESSOR |
| 23 | P-01-2023/15078 | MS. | MANI KAPOOR | 26.09.2023 | JAN'2023 | DR. KUNZANG CHOSDOL | PROFESSOR |
| 24 | P-01-2023/15079 | MS. | ANAMTA GUL | 26.09.2023 | JAN'2023 | DR SUBHRADIP KARMAKAR | ADDITIONAL PROFESSOR |
| 25 | P-01-2023/15080 | MS. | RUCHI | 26.09.2023 | JAN'2023 | DR JAYANTH KUMAR | ADDITIONAL PROFESSOR |
| 26 | P-01-2023/15081 | MS. | ALISHER BEHERA | 26.09.2023 | JAN'2023 | DR. ASHOK SHARMA | ADDITIONAL PROFESSOR |
| 27 | P-01-2023/15083 | MS. | GEETA RANI | 26.09.2023 | JAN'2023 | DR. ARCHANA SINGH | ADDITIONAL PROFESSOR |
| 28 | P-01-2023/15084 | MS. | SONALI CHAKRABORTY | 26.09.2023 | JAN'2023 | DR. PRAGYAN ACHARYA | ADDITIONAL PROFESSOR |
| 29 | P-01-2024/15148 | DR. | MADHUTI CHAKRABORTY | 26.03.2024 | JAN'2024 | DR. KALPANA LUTHRA | PROFESSOR |
| 30 | P-01-2024/15149 | DR. | SHRUTI GUPTA | 23.03.2024 | JAN'2024 | DR. KUNZANG CHOSDOL | PROFESSOR |
| 31 | P-01-2024/15150 | MR. | GURPREET SINGH | 26.03.2024 | JAN'2024 | DR SUBHRADIP KARMAKAR | ADDITIONAL PROFESSOR |
| 32 | P-01-2024/15151 | MR. | SOVIK ROY | 23.03.2024 | JAN'2024 | DR. ARCHNA SINGH | PROFESSOR |
| SENIOR RESIDENTS | JUNIOR RESIDENTS | ||||
|---|---|---|---|---|---|
| 1. | Dr. Astha Sachan | 1. | Dr Sachin S Desh | 14. | Dr. K. V. Sreekar |
| 2. | Dr. Suman Saha | 2. | Dr. Shaikh Abdul Mubeen | 15. | Dr. SM. Turab Ul Haq |
| 3. | Dr. Anudeep PP | 3. | Dr. Sona Fazil | 16. | Dr. P.B.N. Vishal |
| 4. | Dr. Vinod | 4. | Dr. Aradhna Sarma | 17. | Dr. Shreya Mohanti |
| 5. | Dr. Harshit Kelkar | 5. | Dr. I. Sanjana | 18. | Dr. Shravya Kethuri |
| 6. | Dr. Shruthi Gupta | 6. | Dr. R. Madhubala | ||
| 7. | Dr. Neha Chaawal | 7. | Dr. Anandam Biswas | ||
| 8. | Dr. Madhuti Chakraborty | 8. | Dr. G. Laxmi Pillai | ||
| 9. | Dr. S. Reddipalli | 9. | Dr. Gitanjali R | ||
| 10. | Dr. Prakash Acharya M.G. | ||||
| 11. | Dr. Spriha Saxena | ||||
| 12. | Dr. A. S. Vaishnavi | ||||
| 13. | Dr. Payal Kumari Goyal | ||||
The Centre has Bioelectronics, Biomechanics, Biomaterials, Biosensor, Preventive Cardiovascular, Animal Experimentation, Medical Imaging, Biosignal Processing, Tissue Engineering, Drug delivery Laboratory, Characterization of nanoparticles, Laser micromachining Lab, Lab-on-a-chip, Biomedical Measurement Systems, Vascular Mechanics laboratories, Artificial Tissue Lab.
For more details and latest updates, visit us at: CBME, IIT-Delhi
Page was last updated on April, 2020. © CBME, 2020
| Sr. No. | Name | Designation |
|---|---|---|
| 1 | Darshna Chandna | P.S. to HOD |
| 2 | Manoj Kumar Sharma | Jr. Administrative Officer |
| 3 | Amrita Sachdeva | Stenographer |
| 4 | Ajeesh T. G. | Jr. Administrative Assistant |
| 5 | Ajay Kumar Parida | Office Attendant Grade I |
| 6 | Danbir Sharma | Office Attendant Grade I |
| 7 | S. Karthikeyan | Senior Technical Officer |
| 8 | Binod Prasad | Senior Technical Officer |
| 9 | Fateh Singh | Senior Technical Officer |
| 10 | Nazmeen Khan | Senior Technical Officer |
| 11 | Purnima Gola | Technical Officer |
| 12 | Jyothi P. | Technical Officer |
| 13 | Meenu Bala | Technical Officer |
| 14 | Anand Saxena | Medical Laboratory Technologist |
| 15 | Ram Kumar | Medical Laboratory Technologist |
| 16 | Soosamma Shaji | Medical Laboratory Technologist |
| 17 | Hari Om Sharma | Medical Laboratory Technologist |
| 18 | Sunil Kumar | Medical Laboratory Technologist |
| 19 | Kamalpreet Kaur | Medical Laboratory Technologist |
| 20 | Pramod Kumar | Junior Medical Laboratory Technologist |
| 21 | Mukesh Kumar | Junior Medical Laboratory Technologist |
| 22 | Jitendra Bihari Lal | Masalchi |
| 23 | Anil Kumar | Masalchi |
Dr. Kalpana Luthra
Professor & Head
Department of Biochemistry
Room No-4001, 4th Floor,
Convergence Block,
All India Institute of Medical Sciences,
New Delhi-110029
Phone: 011-26549242
Email Id: kalpanaluthra[at]gmail[dot]com
Dr. Kalpana Luthra is a Professor & Head in the Department of Biochemistry, All India Institute of Medical Sciences (AIIMS), New Delhi, India. She completed her PhD at AIIMS in 1994 and joined as faculty at AIIMS in 1998. She was awarded Shakuntala Amir Chand Prizeby Indian Council of Medical Research (ICMR) for the year 2003 & Fogarty fellowship in 2002 and availed training in HIV-1 antibody related work at New York University. She is a Fellow of The National Academy of Medical Sciences India (NAMS), National Academy of Sciences, India (NASI) & Indian National Science Academy (INSA).
HIV Immunology: Coevolution of virus and antibody responses, generation and characterization of human recombinant anti-HIV-1 monoclonal antibodies
HIV-1 is a complex virus with a remarkable ability to protect itself from our intricate network of immune system. This is achieved by masking itself from the immune recognition by acquiring the host proteins or by escaping the humoral response by virtue of its extraordinary ability to mutate. This leads to generation of diverse strains of HIV-1 virus, making the treatment and prevention a complicated process. More than 90% of the HIV-1 infections in India are caused by clade C viruses. Our lab focuses on studying various aspects of HIV-1 infection which includes:
The Centre has Bioelectronics, Biomechanics, Biomaterials, Biosensor, Preventive Cardiovascular, Animal Experimentation, Medical Imaging, Biosignal Processing, Tissue Engineering, Drug delivery Laboratory, Characterization of nanoparticles, Laser micromachining Lab, Lab-on-a-chip, Biomedical Measurement Systems, Vascular Mechanics laboratories, Artificial Tissue Lab.
For more details and latest updates, visit us at: CBME, IIT-Delhi
Page was last updated on April, 2020. © CBME, 2020
Dr. Ashish Suri
Professor
Department of Neurosurgery
M.B.B.S., M.Ch., D.N.B., M.N.A.M.S.
| Areas of Interest | Neurosurgerywith special reference to: Skull base surgery and cerebrovascular surgery:
Endoscopic Neurosurgery
Neuro-Oncology
Epilepsy Surgery:
Spine:
Neurosurgery Skills Training Neuro-technology: Virtual Reality Simulation and Neurosurgery Instrumentation | ||||||||||||||||||||||||||||||||
| Qualifications &Additional Training: |
| ||||||||||||||||||||||||||||||||
| Clinical and Surgical Experience: | Served for last 20 years at the All India Institute of Medical Sciences, New Delhi.
| ||||||||||||||||||||||||||||||||
| Innovations in Clinical Neurosurgery: | Neuro-endoscopy:
Skull Base Surgery:
Cerebrovascular Surgery:
Neuro-oncology:
Phrenic nerve stimulation for quadriplegia: first in India | ||||||||||||||||||||||||||||||||
| Awards |
| ||||||||||||||||||||||||||||||||
| Invited Faculty - International |
| ||||||||||||||||||||||||||||||||
| Invited Faculty – National | Various CMEs/ Workshops/ Conferences | ||||||||||||||||||||||||||||||||
| Conference organization: | Organizing Secretary of following conferences:9th Annual Conference of the Skull Base Surgery Society of India and International Skull Base CME and WFNS Microsurgery & Endoscopy Skull Base Cadaver Workshop (Oct. 2007) Annual Conference of Delhi Neurological Association 2009 – DNACON 2009 (Feb. 2009) 11th Annual Conference of the Indian Society of Cerebrovascular Surgery, International CME, 8th, 9thOctober, 2011, Pre- Conference Live Neurosurgery and Neuro-intervention Workshop, 6th, 7thOctober, 2011. Secretary: DBT Indo-German Neurosurgery Skills Training Workshops. Secretary : ICMR funded Neurosurgery Skills Training Workshops Member, Organizing Committee of following conferences
| ||||||||||||||||||||||||||||||||
| Membership of National and International Scientific Societies |
| ||||||||||||||||||||||||||||||||
| Elected offices in Professional Societies |
| ||||||||||||||||||||||||||||||||
| Memberships of editorial boards of journals | Member of the Editorial Board of
Reviewer of articles for various national and international journals:
| ||||||||||||||||||||||||||||||||
| Development of Specialty of Neurosurgery | Neurosurgery Skills Training Facility and Experimental LaboratoryThe Department of Neurosurgery at the All India Institute of Medical Sciences, New Delhi started the “Experimental Microneurosurgery Laboratory” in 1971 through the efforts of Prof. P.N. Tandon and Prof. A.K. Banerji (Emeritus Professors, Department of Neurosurgery). The training laboratory was expanded and renovated into a full fledged training facility named as Neurosurgery Skills Training Facility and Experimental Laboratory with the support of Department of Science and Technology (DST), Ministry of Science and Technology, Govt. of India, Department of Biotechnology (DBT) Indo-German Collaboration, Ministry of Science and Technology, Govt. of India, and Department of Health Research (DHR-ICMR), Ministry of Health and Family Welfare, Govt. of India for hands on skills training of M.Ch and DNB neurosurgery residents and trained /trainee Neurosurgeons from India and abroad. The Neurosurgery Skills Training Facility and Experimental Laboratory is equipped with the state-of-the-art equipment, which simulates a modern Neurosurgery Operation Room environment. The training imparted is aimed at development of Neurosurgical skills and techniques. The training imparted in the form of quarterly workshops, short term training programs and daily skills training sessions is focused on formulation of a new curriculum of neurosurgical skills development and imparting hands-on practice on synthetic/semi synthetic models, live anesthetized animals and cadaver parts using highly advanced equipment and technology creating a neurosurgical operation room environment. http://aiimsnets.org/workshops.asp Neurosurgery Education and Training School (NETS)Website: www.aiimsnets.org Neurosurgery Animation, Graphics and Video Editing Laboratory Tele-education Platform | ||||||||||||||||||||||||||||||||
| Research Fields: | Innovation based research and development.
Research in neurosurgery skills training.
Laboratory based neurosurgery focused research.
Clinical research | ||||||||||||||||||||||||||||||||
| Research Projects from Recognized National &International Agencies: | Completed Projects as Chief Investigator:ANTISENSE PHARMA Gmb Josef-Engert-StraBe9D-93053 Regensburg Germany A multi-national, multi-center, open-label, active-controlled, randomized parallel-group dose-finding study to evaluate the efficacy and safety of two doses of AP 12009 in adult patients with recurrent high-grade glioma, administered intratumorally as continuous high-flow microperfusion over a 7-day period every other week. International Society of Pediatric Neurosurgery, (ISPN), International Study Group on Neuro-endoscopy, (ISGNE). The International Infant Hydrocephalus Study (IIHS) is an international multi-center, prospective, controlled, randomized study of the treatment of newly diagnosed obstructive hydrocephalus in infants below 2 years of age. Dept. of Science and Technology: FIST (DST-FIST), Ministry of Science and Technology, Govt. of India. FIST sponsored AIIMS Neurosurgery Skills Training Facility and Experimental Laboratory (Cadaver Dissection Facility) Department of Biotechnology (DBT), Ministry of Science and Technology, Govt of India. Collaborative Indo-German Program for Bilateral Workshops, Seminars and Tele-education in Training Microsurgical and Endoscopic Techniques in Neurosurgery Ongoing Projects as Chief Investigator:Indian Council of Medical Research (ICMR), MinistryofHealth& Family Welfare, Govt. of India, AIIMS+ CSE- IIT-D Evaluation of development of neurosurgery skills by hands - on skills training and interactive virtual training modules (web based, tele-education and real time simulation). Department of Health and Research (DHR), Indian Council of Medical Research, MinistryofHealth& Family Welfare, Govt of India, AIIMS+ CSE- IIT-D Expansion of DST + DBT Sponsored Neurosurgery Skills Training Facility and Development of Stereoscopic (3 Dimensional - 3D) Virtual Training Modules for Neurosurgery Skills Training Department of Science and Technology - Instrumentation Development Program (DST- IDP), India. AIIMS+ BME- IIT-D: Development of Low-Cost Versatile Neurosurgery Equipment System for Neurosurgery Dept. of Science and Technology: (DST-FIST Level II), Ministry of Science and Technology, Govt. of India. DST- for Neurosurgery Skills Training Facility (Cadaver Dissection Stations) and 3D Surgical Endoscopic and 3D Microscopic Integrated Digital Neurosurgery OR’s and Central Repository Server for Archival , Streaming and Teleconferencing. Research projects as Co-investigator:Codman (J & J) A Registry for Comparing Catheter-Related Infection Among various Shunt-systems in the Treatment of Hydrocephalus Indian Council of Medical Research (ICMR)MinistryofHealth& Family Welfare, Govt of India. Study of the role of bone marrow derived mononuclear cells in peripheral nerve repair of adult rats. Actelion Pharmaceuticals Ltd.Gewerbestrasse 16, CH-4123 Allschwil, Switzerland. A Prospective, Multi-centre, double-blind, randomized, placebo-controlled,parallel-group study to assess the efficacy and safety of clazosentan in reducing vasospasm-related morbidity and all cause mortality in adult patients with aneurismal subarachnoid hemorrhage treated by surgical clipping. London School of Hygiene and Tropical Medicine, London, UK. CRASH-2 (Project NI-774) Clinical Randomization of Antifibrinolytic (Tranaexemic acid) in trauma pts with or at risk of Significant Hemorrhage (death / tranfusion requirement) Peregrine Pharmaceuticals,Inc.14272 Franklin Avenue Suite100, Tustin , CA 92780-7017, 714-508-6000. Open label, dose confirmation study of Interstial I131-ch TNTA/B MAb (COTARAR ) for the treatment of Recurrent GlioblastomaMultiforme (GBM) at first relapse.
Department of Biotechnology (DBT), Ministry of Science and Technology, Govt of India.
Hypoxia and p53-HIC1 axis in stemness of glial tumors and cell lines Indian Council of Medical Research (ICMR)MinistryofHealth& Family Welfare, Govt of India. Glioblastomas in children and adults: A comparative study with special reference to molecular pathways and MGMT methylation status. ANTISENSE PHARMA Gmb Josef-Engert-StraBe9D-93053 Regensburg Germany Efficacy and Safety of AP 12009 in Adult Patients with Recurrent or Refractory Anaplastic Astrocytoma (WHO grade III) as Compared to Standard Treatment with Temozolomide or BCNU: A Randomized, Actively Controlled, Open Label Clinical Phase III Study. Ministry of Communication and Information Technology, Department of Electronics and Information Technology.
Foundation of Trusted and Scalable: Last Mile Healthcare, Indo-US joint R & D PROJECT BY IIT-Delhi, All India Institute of Medical Sciences (AIIMS –Delhi) C-DAC-Chennai, Dartmouth College & Rice University, USA. | ||||||||||||||||||||||||||||||||
TEACHING EXPERIENCE |
Invited speaker in numerous Continuing Medical Education (CME) programs, seminars, workshops and conferences. TOTAL NO. OF PUBLICATIONS
Awards to Students for Research Work carried out under guidance :
Research Guidance:Number of scholars who have been awarded M.Ch. / M.D./Ph.D degrees under supervision as guide \ co-guide:
| ||||||||||||||||||||||||||||||||
| Indexed Papers: 2005 to 2012 October | PUBLICATIONS
Indexed Abstracts
Chapters:
|

| Address: | Room No: 3013 (Seminar Room), Department of Biochemistry, 3rd Floor Teaching Block, AIIMS, New Delhi – 110029 |
| Email: | karthi.dr[at]gmail[dot]com, karthikeyan_p[at]aiims[dot]edu |
| Public profiles: | Orcid | Google Scholar | Research Gate | YouTube | Goodreads |
| Research focus | Leukemia Biology, Bioinformatics, Medical Education |
| Sr. No. | Degree | Year | Subject | University/Institution |
|---|---|---|---|---|
| 1. | MBBS | 2010 | All Subjects | Kanyakumari Government Medical College |
| 2. | MD | 2015 | Biochemistry | Maulana Azad Medical College |
| 3. | DNB | 2016 | Biochemistry | National Board of Examinations |
| 4. | PhD | 2022 | Biochemistry | AIIMS, New Delhi |
| Sr. No. | Positions held | Name of the Institute | Period |
|---|---|---|---|
| 1 | Junior Resident | Maulana Azad Medical College | 2012 - 2015 |
| 2 | Senior Resident | AIIMS, New Delhi | 2015 - 2018 |
| 3 | Research Associate II | AIIMS, New Delhi | 2019 - 2022 |
| 4 | Assistant Professor | Maulana Azad Medical College | May 2022 – Jan 2023 |
| Sr. No | Name of Award | Awarding Agency | Year |
|---|---|---|---|
| 1 | FIRST PRIZE in Biochemistry Quiz Competition | Association of Medical Biochemists of India | 2014 |
| 2 | Certificate for BEST JOURNAL CLUB PRESENTATION | Dept. of Biochemistry, AIIMS, Delhi | 2017 |
| 3 | Acknowledgement in Harper illustrated Biochemistry, 31st edition for suggestions and corrections | Victor W. Rodwell (chief editor) | 2018 |
| 4 | Research Associate Fellowship | Indian Council of Medical Research | 2019 |
| 5 | Certificate for Quiz Master | Indian Immunology Society | 2020, 2021, 2022 |
| Sr. No | Author(s) | Title | Name of Journal | Volume | Page | Year |
|---|---|---|---|---|---|---|
| 1 | Pethusamy K, Seethy A, Dhar R, Karmakar A, Chaudhary S, Bakhshi S, P JK, Chopra A et al. | Loss of TET2 with reduced genomic 5-hmC is associated with adverse-risk AML | Leukemia & lymphoma | 63(14) | 3426-3432 | 2022 |
| 2 | Sahoo OS, Pethusamy K, Srivastava TP, Talukdar J et al. | The metabolic addiction of cancer stem cells. | Frontiers in oncology | 12:955892. | eCollection | 2022 |
| 3 | Chattopadhyay I, Dhar R, Pethusamy K, Seethy A et al. | Exploring the Role of Gut Microbiome in Colon Cancer | Applied Biochemistry and Biotechnology | 193(6) | 1780-1799 | 2021 |
| 4 | Seethy A, Pethusamy K, Chattopadhyay I, Sah R et al. | TETology: Epigenetic Mastermind in Action | Applied Biochemistry and Biotechnology | 193(6) | 1701-1726 | 2021 |
| 5 | Dhar R, Seethy A, Singh S, Pethusamy K, Srivastava T et al. | Cancer immunotherapy: Recent advances and challenges. | Journal of Cancer Research and Therapeutics | 17(4) | 834-844 | 2021 |
| 6 | Dhar R, Singh S, Mukherjee I, Pethusamy K, Purkayastha K et al. | EMTiness in pseudo-malignant behavior of trophoblasts during embryo implantation. | Frontiers in Bioscience-Landmark | 26(4) | 717-743 | 2021 |
| 7 | Seethy AA, Singh S, Mukherjee I, Pethusamy K et al. | Potential SARS-CoV-2 interactions with proteins involved in trophoblast functions - An in-silico study. | Placenta | 103 | 141-151 | 2021 |
| 8 | Chakraborty M, Singh P, Dsouza JMP, Pethusamy K et al. | Fasting and postprandial lipid parameters: A comparative evaluation of cardiovascular risk assessment in prediabetes and diabetes. | J Family Med Prim Care | 28;9(1) | 287-292 | 2020 |
| 9 | Dhar R, Pethusamy K, Singh S, Mukherjee I et al. | Draft genome of Ompok bimaculatus (Pabda fish). | BMC Research Notes | 26;12(1) | 825 | 2019 |
| 10 | Dhar R, Seethy A, Pethusamy K, Singh S et al. | De novo assembly of the Indian blue peacock (Pavo cristatus) genome using Oxford Nanopore technology and Illumina sequencing. | Gigascience | 1;8(5) | giz038 | 2019 |
If you are interested in working on similar projects as ours or have a unique idea in any field that you wish to pursue, please send an email to karthikeyan_p[at]aiims[dot]edu.People with independent fellowships are welcomed. Let's explore opportunities for collaboration and growth together.
(Content provider: Dr. Achal K Srivastava)
Neurology is one of the earliest super – specialty at the Institute. Dr. James Austin, a Neurologist from Oregon, USA started a nucleus of Neurology service in the department of Medicine in 1962-63. In 1965, Dr Sushila Nayar, then Union health minister, invited Prof. Baldev Singh (one of the founder members of NSI, Neurological Society of India) to start a department of Neurology at AIIMS. When Prof Baldev Singh (also called ‘father of neurology’ in India and lovingly called "Papa Neuron") moved to neurophysiology on his retirement, the department was headed by Dr S N Pathak and then by Dr Vimla Virmani in 1975. After Prof. Vimla Virmani, Prof. M C Maheshwari took charge of the department in 1978. The department was shifted to the Cardiothoracic and Neurosciences Centre in the year 1985. In the year 2001, Prof. M.Behari took over the mantle of leadership. She retired in June 2016. Prof Kameshwar Prasad became the head of the department in October 2013. He retired on 31st January 2019. Prof. MV Padma Srivastava took over the leadership on 1st February 2019. From its inception, the emphasis of the department has been on quality patient care, research and to achieve academic excellence. Though the department started with 25 in patient beds, now there are 75 beds including neurointensive care. Out patient services and inpatient care has been incessantly on the rise over the years. The department has tried to maintain impeccable record of comprehensive patient care, teaching and training of students as well as contribute significantly to the scientific literature in terms of research. The department actively pursues clinical care and research activities in the sub-specialities of Movement Disorders, Neuroinfections and immunology, Stroke, Intractable epilepsy, Neuro-muscular Disorders, Sleep, Headache, Dementia amongst others. The department is equipped with the latest modalities for the diagnosis and management of various neurological disorders. The department has been in the forefront of medical research since its formation and is renowned internationally for quality clinical and basic research, particularly in the field of stem cells, Parkinson’s disease, stroke, epilepsy, neuromuscular disorders, sleep and headache. Regular patient information programs and scientific deliberations are conducted by the department. The faculty of the department routinely participates in the public awareness programs on television, and radio etc. and are active in various national and international CME programs.
Dr. Ramesh Doddamani,  MBBS, MS (General Surgery), MCh (Neurosurgery) |
| Consultant and Additional Professor Dept. of Neurosurgery, CN Centre, All India Institute of Medical Sciences and Gamma Knife Centre, Jai Prakash Narayan Apex Trauma Centre, New Delhi, India – 110029 Email:drsdramesh[at]aiims[dot]edu Phone No: 011-26593291 | Neurosurgery Unit – 1 OPD (Consultation): CN Tower; Room:19 Days:Monday (9am – 1 pm); Thursday (2pm – 5 pm) |
Dr Ramesh Doddamani is currently holding the academic position of Additional Professor in the department of neurosurgery, All India Institute of Medical Sciences, New Delhi. He completed his graduation (MBBS) from the prestigious Mysore Medical College. Later, went on to accomplish his Post-graduation (MS, General Surgery), followed by Super-specialization (MCh Neurosurgery) both from the reputed premier institute of the country, Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh. After completion of the residency program, He joined as a Faculty of neurosurgery at AIIMS, New Delhi in 2015.
He is highly experienced and skilled in performing all the neurosurgical procedures. His area of special interests being: Epilepsy Surgery, Stereotactic and Functional Neurosurgery, Robotic Neurosurgery, Pain procedures, Neurosurgery for Psychiatric disorders, Neuro-Oncology, Endovascular Neurosurgery. He has published high quality research in several high impact journals in these fields. He is on the editorial board of the “Neurology India” (official journal of Neurological Society of India) as an Assistant Editor, Section Editor for “World Neurosurgery” (official journal of World Federation of Neurosurgery) for ‘Epilepsy’ and ‘Pain’ Sections. He is an invited editor for the journal “Neurosurgical Focus” (Official journal of American Association of Neurological Surgeons) on the topic of Neurocutaneous disorders. He is also the founding member and Secretary of the “Society for Epilepsy Neurobiology and Neuromodulation Surgery” (SENNS). He is the member of various national neurosurgical societies and has delivered lectures at numerous national and international conferences.
| Degree | Specialty | Institution | Duration |
|---|---|---|---|
| MS | General Surgery | PGIMER, Chandigarh, India | 2006-2009 |
| MCh | Neurosurgery | PGIMER, Chandigarh, India | 2011 - 2013 |
| Position | Specialty | Institution | Duration |
|---|---|---|---|
| Additional Professor | Neurosurgery | All India Institute of Medical Sciences (AIIMS), New Delhi, India | 2021 – Till date |
| Associate Professor | Neurosurgery | All India Institute of Medical Sciences (AIIMS), New Delhi, India | 2018 - 2021 |
| Assistant Professor | Neurosurgery | All India Institute of Medical Sciences (AIIMS), New Delhi, India | 2015 - 2018 |
| Consultant | Neurosurgery | BGS Global Superspecialty Hospital, Bangalore, India | 2014 - 2015 |
| Senior Resident | Neurosurgery | Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India | 2011-2013 |
| Junior Resident | General Surgery | Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India | 2009 - 2011 |
“Deciphering the role of HDACs in patients of Temporal Lobe Epilepsy”
Doddamani RS, Meena RK, Selvam MM, Venkataramanaa NK, Tophkhane M, Garg SK. IntraventricularGliosarcomas: Literature Review and a Case Description. World Neurosurg. 2016; 90:707.e5-707.e12.
PhD and MTech programs in Biomedical Engineering.
PhD and MTech programs in Biomedical Engineering.
| Incharge | Dr.T.Velpandian, Prof. of Ocul Pharmacology |
| Faculty | Dr. Nabanita Halder, Prof. of Ocul Pharmacology |
Facilities Established HPBAF - High Precision Bio-analytical Lab (DST-FIST grant) MolDyne – Molecular Dynamics Lab OcuCel- Cell culture facility for invitro drug screening NODDL – Novel Ocular Drug Development Lab ADD-FOND – Adv.DrugDelv. Fac. For Ocu. Neovascular Dis. GLP-Disp - Pharmacy (IV-Parentral dispensing Facility) Patient Care
Community Services
PhD Scholars
| Student’s name | Research topics |
| MadhuNath | Evaluation of the Role of Retinal Renin Angiotensin System (RAS) in the Animal Model of Retinopathy of Prematurity (ROP) |
| Hanuman Sharma | Functional Importance of Nucleoside Transporters in the Ocular Disposition of their Substrates |
| AnkitaKotnala | Evaluation of A2E Biological Functions Relevant to the Pathology of Age Related Macular Degeneration |
| Moksha Laxmi | Understanding the Drug Transporter Functions in Blood Ocular Barriers during ocular inflammation in the Experimental Models of Uveitis |
| Ujjwalkumar Das | Developing and validating QSPR model to define enhanced drug penetration across blood ocular barriers |
State-of-the-Art Facilities Available at Ocular Pharmacology and Pharmacy
HPBAF  Neo-vasular research
Neo-vasular research  NODDL-Sterile facility
NODDL-Sterile facility  MOLDYN
MOLDYN 

| Address: | 3027B, Department of Biochemistry, AIIMS, New Delhi – 110029 |
| Email: | siddhartha_kundu[at]yahoo[dot]co[dot]in siddhartha_kundu[at]aiims[dot]edu |
| Telephone: | +91-11-26546514 |
| Public profiles: | Orcid || Loop-Frontiers || Exaly || ResearchGate || GoogleScholar || |
| Research focus | Mathematical and Computational Biochemistry |
| Areas of Interest | Mathematical analyses of biochemical reactions & metabolic networks Mathematical modelling and simulations of complex biochemical systems Algorithms for molecular biology |
| Hyperlink | Description |
|---|---|
| http://doi.org//10.1142/S0219720022500184 https://cran.r-project.org/package=TemporalGSSA | [Siddhartha_kundu_img1.png] |
| http://doi.org//10.3389/fmolb.2023.1206502 https://cran.r-project.org/package=ReDirection | [Siddhartha_kundu_img2.png] |
| http://doi.org//10.1177/11779322211045878 http://178.63.18.214/ProTG4.html | [Siddhartha_kundu_img2.png] |
| http://doi.org/10.1186/s13104-021-05477-z http://178.63.18.214/Fe2OG.html | [Siddhartha_kundu_img2.png] |
| Degree | Subject | University/Institution | Year |
|---|---|---|---|
| PhD | Computational Biology & Bioinformatics | School of Computational and Integrative Sciences (SCIS), Jawaharlal Nehru University, New Mehrauli Road, New Delhi 110067 | 2014-2018 |
| MD | Biochemistry | All India Institute of Medical Sciences (AIIMS), Ansari Nagar, New Delhi 110029 | 1999-2001 |
| MBBS | Pre-&Para-/Medical/ Surgical subjects | University College of Medical Sciences (UCMS), Dilshad Garden, New Delhi 110095 | 1992-1996 |
| 1. | Society for Mathematical Biology (SMB): Life member (ID:36503496) |
| 2. | European Society for Mathematical and Theoretical Biology (ESMTB) : Life member ID: 50143836 |
| 3. | Elected member Sigma Xi society ( Scientific Research Honors Society) |
| 1. | 2022 | Kundu S#*. TemporalGSSA: a numerically robust R-wrapper to facilitate computation of a metabolite-specific and simulation time-dependent trajectory from stochastic simulation algorithm (SSA)-generated datasets. Jour Bioinf. Comp. Biol. 2022, 20(4):2250018. PMID: 35941839 JBCB2022 (Additional Material). |
| 2. | 2021 | Kundu S#*. Mathematical modeling and stochastic simulations suggest that low-affinity peptides can bisect MHC1-mediated export of high-affinity peptides into “early”- and “late”-phases. Heliyon. 2021, 7(7):e07466. PMID: 34286133 [HYON2021] (Additional Material). |
| 2024 |
|
| 2023 |
|
| 2022 |
|
| 2021 |
|
| 2020 |
|
| 2019 |
|
| 2018 |
|
| 2017 |
|
| 2016 |
|
| 2015 |
|
| 2012 |
|
| 2011 |
|
| 2002 |
|
| (#) Single author; (*)Corresponding author |
| Position | Subject/Work | University/Institution | Year |
|---|---|---|---|
| Associate Professor Assistant Professor | Biochemistry | All India Institute of Medical Sciences (AIIMS), Ansari Nagar, New Delhi 110029 | 2023-2019-2023 |
| Associate Professor | Biochemistry | Army College of Medical Sciences (ACMS), Dr. Baba SahebAmbedkar Medical College and Hospital (BSAMCH), Govt. of NCT of Delhi, Rohini, Delhi 110085 | 2015-2018 2018-2019 |
| Assistant Professor | Biochemistry | Army College of Medical Sciences (ACMS), Brar Square, Delhi Cantt.,New Delhi – 110010 | 2009-2014 |
| Scientist ‘D’ (Medical) | Program Officer | Indian Council of Medical Research (ICMR), V. RamalingaswamiBhawan, Ansari Nagar, New Delhi 110029 | 07-10/2019 |
| Senior Level Consultant | Program Director | Information Technology Research Academy (ITRA), Digital India Corporation (formerly Media Lab Asia), Ministry of Electronics and Information Technology, C-DOT campus, New Delhi 110030 | 2016-2017 |
| Research Consultant | Computational Biology | India Research Labs (IRL) IBM | 2002-2003 |
Research Associate/Fellow/Scientist
| PostDoctoral work | International Center for Genetic Engineering and Biotechnology (ICGEB) National Institute of Immunology (NII) ICMR-National Institute of Pathology (NIOP) Indian Institute of Technology Delhi (IITD) | 05-10/2014 2005-2008 2003-2004 01-05/2002 |
| Title | Download |
|---|---|
| In Charge | Dr.Jasbir Kaur -Prof. of Ocul.Biochem. |
| Dr. Alok kr. Ravi, Prof. of Ocul.Biochem. | |
| PhD Scholars | |
| Parul Saxena | |
| Arpna Srivastava | |
| Ocular biochemistry section is engaged in research on biochemical, immunological and genetic aspects of eye diseases. Section has handled the Indo-US Case Control Study on risk factors in age related senile Cataract. Research work is being carried out in Uveitis, Optic neuritis, Corneal ulcer etc. Several TOKEN programmes including WHO workshop programmes have been organized. | |
| Tissue and cell culture/Stem cell culture facility has been established in the section. Research work on stem cell culture is in progress. The lab is focusing to understand the molecular basis of ocular diseases, mainly Ocular tumors and Glaucoma. The focus is also on developing of microquantitative procedures for analysis of ocular fluids like aqueous and vitreous humors and tears. | |
| The beneficial effects of certain Ayurvedic drugs are also being evaluated for research purposes. The section continues to render clinical laboratory services, besides teaching and training to undergraduates and postgraduates. Section had produced Ph.Ds and MDs. | |
| Sr. No. | Name | Partner CBOs |
|---|---|---|
| 1 | Nangli Dairy | SSMI |
| 2 | Trilokpuri | AIIMS |
| 3 | Jath khod | DDJS |
| 4 | Madipur | SSMI |
| 5 | Nangal Raya | MCD Delhi |
| 6 | Dakshinpuri | Delhi Government |
| 7 | Chirag Delhi | Delhi Government |
| 8 | Mahipalpur | Delhi Government |
| 9 | Jaunapur | Delhi Government |
| 10 | Fatehpur Beri | MCD Delhi |
| 11 | Basant Gaon | Delhi Government |
| 12 | Mehrauli | Delhi Government |
| 13 | Budh Nagar | Delhi Government |
| 14 | Rajokri | Delhi Government |
| 15 | Sagarpur | Delhi Government |
| 16 | Neb Sarai | Delhi Government |
| 17 | Railway Colony | Railway Dispensary |
| 18 | Ayanagar | Delhi Government |
| 19 | Batla House | Delhi Government |
| 20 | Sarai Kalekhan | Delhi Government |
| 21 | Dharuhera | Hero Motors |
| 22 | Garhi, East of Kailash | Delhi Government |
| 23 | Tauru | Deepalaya |
| 24 | Patel gardan | Deepalaya |
| 25 | Janakpuri | Deepalaya |
| 26 | Sanjay Colony | Deepalaya |
| 27 | Sohna | Deepalaya |
Courses relevant to Biomedical Engineering is offered at IIT Delhi and include Introduction to Basic Medical Sciences for Engineers, Industrial Biomaterial Technology, Research Techniques in Biomedical Engineering, Medical Imaging, Tissue engineering, Biomaterials, Biosensor Technology, Biomedical Signal and Image Processing, Emerging Biomedical Technology Health Care, Vascular Bioengineering, Mathematics for Biomedical Engineers, Biomechanical Design of Medical Devices.The centre has recently its M.Tech. programin 2017.
Courses relevant to Biomedical Engineering is offered at IIT Delhi and include Introduction to Basic Medical Sciences for Engineers, Industrial Biomaterial Technology, Research Techniques in Biomedical Engineering, Medical Imaging, Tissue engineering, Biomaterials, Biosensor Technology, Biomedical Signal and Image Processing, Emerging Biomedical Technology Health Care, Vascular Bioengineering, Mathematics for Biomedical Engineers, Biomechanical Design of Medical Devices.The centre has recently its M.Tech. programin 2017.
List of students is available on following link: http://cbme.iitd.ac.in/content/onroll-phd-students
| S.No. | Name | Room No. (IIT-Delhi) | Tel. No (011-2659-) |
|---|---|---|---|
| 1 | Mr. Rajesh Kumar, JLA | III/399 | 6132,6396 |
| 2 | Ms. Pushp Lata, PA to Head, | III/399 | 6132,6396 |
| 3 | Mr. Yash Pal Sharma, Store Incharge | III/398 | 6233 |
| 4 | Sh. Jagdish, Attendant (C) | III/399 | 6132,6396 |
| 5 | Mr. Anil Pandey, Tech. Asstt. | III/399 | 6132,6396 |
| S.No. | Name | Room No. (IIT-Delhi) | Tel. No (011-2659-) |
|---|---|---|---|
| 1 | Mr. Rajesh Kumar, JLA | III/399 | 6132,6396 |
| 2 | Ms. Pushp Lata, PA to Head, | III/399 | 6132,6396 |
| 3 | Mr. Yash Pal Sharma, Store Incharge | III/398 | 6233 |
| 4 | Sh. Jagdish, Attendant (C) | III/399 | 6132,6396 |
| 5 | Mr. Anil Pandey, Tech. Asstt. | III/399 | 6132,6396 |
Associate Professor
Room No. 3040; 3rd Floor, Teaching Block, Department of Biochemistry, AIIMS; New Delhi-29
Email id: rakheeyadav[at]aiims[dot]edu, rakheeyadav79[at]gmail[dot]com
| Degree | University/ Institution | Year of Passing |
|---|---|---|
| MBBS | Pt BD Sharma PGIMS, MD University, Rohtak (Haryana) | 2002 |
| MD (Biochemistry) | Pt BD Sharma PGIMS, Pt BD Sharma UHS, Rohtak (Haryana) | 2011 |
Positions held (starting from the most recent):
| Position | Department | University/ Institution | Period |
|---|---|---|---|
| Associate Professor | Biochemistry | AIIMS Delhi | 2020 onwards |
| Assistant Professor | Biochemistry | AIIMS Delhi | 2016-2020 |
| Assistant Professor | Biochemistry | SGT Medical College & Hospital, Gurgaon (Haryana) | 2014-2016 |
| Senior Resident | Biochemistry | VMMC & Safdarjung Hospital Delhi | 2011-2014 |
Research Focus of the Lab/ Key Areas: Adipocyte Biology, Insulin Resistance, Obesity & metabolic syndrome
Projects & Funding: ICMR Extramural and AIIMS Intramural Grants
List of Lab members:
Mr Blessed Raj has done MSc in Medical Biochemistry from JIPMER Puducherry and got registered as PhD scholar at AIIMS in Nov 2020. His proposed work is to elucidate the role of ECM-Adipocyte communication in obesity induced adipose tissue dysfunctions
Has done MD Thesis under my supervision titled, “Study of ECM Remodeling in adipose tissue dysfunctions in obesity” and presently working in ongoing lab projects.
She has won Mrs. Dwarka Prasad Trust Travel Grant in 2019 to present her work at 15th Asia Pacific Federation for Clinical Biochemistry and Laboratory Medicine (APFCB) Congress; Jaipur in Nov 2019
Also won best oral paper award in AMBION 2020: National Postgraduate Update cum CME, Chandigarh, November, 2020 (Online Presentation)
Thesis title “A prospective study of changes in human Gut Microbiota (GM) and its association with insulin sensitivity in obese individuals undergoing Bariatric Surgery”
He has been awarded ICMR financial support for his MD thesis (Dec 2020)
Thesis title “Study of the expression of vascular endothelial growth factor (VEGF-A) and its isoforms, in Obesity and their association with insulin sensitivity”
Thesis titled “Assessment of Amphiregulin and CRISPLD1 as visceral adipose tissue derived modulators of cardiovascular health in obesity”
NPCB National Trachoma Prevalence Survery Report, India 2014-17
Manual on Training of Trainers for Volunteers in Primary Eye Care

Dr. Pramod Kumar Gautam
Additional Professor
Room No. 3040, 3rd Floor, Teaching Block,
Department of Biochemistry
All India Institute of Medical Sciences
Ansari Nagar, New Delhi-110029
Official Phone: (O) 011-26594682; (Ext) 4682
Email id:pramodgautam_13[at]yahoo[dot]com,gautam[at]aiims[dot]edu
I am currently working as an additional professor in the Department of Biochemistry. My PhD and post-doctoral fellowship from Banaras Hindu University, Varanasi, India
UG, PG teaching, and research
The immune system can be likened to a sophisticated army, equipped with various tools and mechanisms to protect the body from infections and cancers. However, during tumor development, cancer cells release substances that suppress the immune system, allowing the tumor to grow and spread. To combat this, researchers are focusing on developing immunotherapies that enhance the body's natural defenses against cancer. These immunotherapies target specific pathways involved in tumor growth, angiogenesis, and immune suppression. By discovering and studying the effects of natural compounds and plant extracts, scientists hope to develop safe and effective treatments for cancer that can be used in combination with existing therapies. The goal is to improve cancer management, early detection, and targeted drug delivery to prevent the progression of the disease. Our research lab utilizes advanced molecular & immunological techniques.
Current lab members: Miss Anita (CSIR-JRF); Rupinder Kaur (CSIR-SRF, NET), Dr. Sreekar; Dr. Neha Singh; Dr. Soni Kumari (Research Scientist-II); Ankit Kumar; and Bharta Sinha (DEO, AIIMS, New Delhi).
Anita submitted her thesis in the year 2024. Her title of thesis is to elucidate the immunomodulatory and anti-tumor role of m1 macrophage on bone marrow derived mesenchymal stem cells: implications in breast cancer. Anita has been qualified CSIR-JRF and currently working as a research scientist in the Dept. of Pharmacology at AIIMS, New Delhi.
ORCID: 0000-0002-0158-8307
Rupinder Kaur, a 4th year Ph.D. student (2020-present) and CSIR-SRF (Direct) fellow, delves into the fascinating world of cancer-immunology. Her research focuses on unraveling the immunomodulatory effects of tumor-derived exosomes on Gamma-Delta T cells. By exploring this intricate interaction, she aims to uncover potential therapeutic strategies for cancer treatment. Rupinder's work primarily consists of the analysis of differential micro-RNA cargo in extracellular vesicles in peripheral blood of cancer patients. She is also working on elucidating the mysteries of the change in polarity of gamma delta T cells under the effect of tumor derived extracellular vesicles. She completed her Master in Biochemistry in 2019 from Punjab Agricultural University, Ludhiana.
Thesis Title: “To study the immunomodulatory effect of tumor derived exosomes in Gamma-Delta T cells.”
Myself, Ankit Kumar and I have done my B.Sc. in Zoology (Hons) from St. Xavier College Ranchi in 2018–21. and currently I have joined as M.Sc student and am working on a thesis titled "Differentially expressed exosomal miRNA derived from Pancreatic Ductal AdenoCarcionoma (PDAC)".
Qualification- PhD in Microbiology
ORCID-https://orcid.org/0000-0001-9802-0445
Current affiliation- Project Student, Department of Biochemistry, All India Institute of Medical Sciences
Project Title-Elucidating the targeted therapeutic role of docetaxel- loaded- HSP70 peptide complex in PDX mouse models.
Expertise- Expert in microbiology, medicinal plants, and cancer biology. Skilled in analyzing microbial interactions, identifying medicinal compounds in plants, and studying cancer cell signaling pathways. Proficient in microbiological techniques, plant extraction methods, and cancer cell culture assays. Experience in research, drug discovery, and contributing to advancements in medical science.
PhD in Biochemistry
ORCID ID: 0000-0002-9743-3202
I am currently working as a Research Scientist II on an ICMR-funded project titled “Elucidating the Therapeutic Role of Docetaxel-Loaded HSP Peptide Complex in PDX Mouse Model.”
He has a strong interest in cancer and cancer immunology and is about to embark on research in breast cancer immunology. His focus will be on developing new methods to detect novel biomarkers that can aid in the early diagnosis of breast cancer. He has finished his M.B.B.S. from Dr. NTR university of health sciences, Andhra Pradesh.
Dr. Sonam Agarwal (ICMR- RA);Dr.. Khuswant Singh (CSIR-JRF); Dr. Kunal Kumar; Dr. Vijay Mohan (Post Doc Fellow); Pavit Singh (MBBS-STS student).
Publication Details
https://scholar.google.co.in/citations?user=PBcBKhwAAAAJ&hl=en
The eye health education unit of department is pro-actively engaged in developing IEC materials of common eye problem. Various IEC materials like small booklets, pamphlets, posters, Audio-visual movie pertaining to eye care have been developed. Community leaders, parents and guardians, school teachers are main target for eye health education. Community ophthalmology has initiated health education activities for patients utilizing out-patient and inpatient services at the institute. This is in addition to the already ongoing health education activities at the primary eye care clinics. The topics for health education are wide ranging such as general eye care, care of spectacles, refractive error, care after cataract surgery, glaucoma, retinoblastoma, retinopathy of prematurity etc. These are undertaken in conjunction with faculty and residents from respective sub-specialties, optometrists, nurses and medical social workers of RP Centre. Faculty from the department were involved in the NPCB program on sensitization of Doctors/Paramedics about the eye donation and its importance as well as the vital information related to eye donation and delivered talks on the same during the Eye Donation Fortnight 2020. Posters :- Cataract, Refractive Error, Presbyopia, General Eye Care, Conjunctivitis, Vitamin 'A', Eye Donation Magnitude of Trachoma NPCB Survey (2014-2015) NSU SSU 2015 Recent Contributions in Community Eye Health Research RPC Model of Low Vision & Rehabilitation Services UVR Poster 2015 Excellence in Primary Eye Care Vision Delhi- A Primary Eye Cate Initiative (1st April to 31st March) DR Screening Poster Health Education Pamphlets on Primary eye care: Health education booklet on PEC (http://www.aiims.edu/images/depart/RPC/Books/Booklet%20RPC-28%20June%202014%20Output.pdf) General Eye Care Glaucoma Presbyopia Diabetic Retinopathy Refractive Error Eye Donation Training Manuals on Primary eye care 1. Training of School Teachers for School Vision Screening to Prevent and Control Childhood Visual Impairment and Blindness 2. Manual on Training of Trainers for Volunteers in Primary Eye Care 3. Vision Screening Card for Schools 4. Vision Screening Card for Primary Eye Care
The eye health education unit of department is pro-actively engaged in developing IEC materials of common eye problem. Various IEC materials like small booklets, pamphlets, posters, Audio-visual movie pertaining to eye care have been developed. Community leaders, parents and guardians, school teachers are main target for eye health education. Community ophthalmology has initiated health education activities for patients utilizing out-patient and inpatient services at the institute. This is in addition to the already ongoing health education activities at the primary eye care clinics. The topics for health education are wide ranging such as general eye care, care of spectacles, refractive error, care after cataract surgery, glaucoma, retinoblastoma, retinopathy of prematurity etc. These are undertaken in conjunction with faculty and residents from respective sub-specialties, optometrists, nurses and medical social workers of RP Centre. Faculty from the department were involved in the NPCB program on sensitization of Doctors/Paramedics about the eye donation and its importance as well as the vital information related to eye donation and delivered talks on the same during the Eye Donation Fortnight 2020.
Cataract, Refractive Error, Presbyopia, General Eye Care, Conjunctivitis, Vitamin 'A', Eye Donation

Magnitude of Trachoma NPCB Survey (2014-2015)
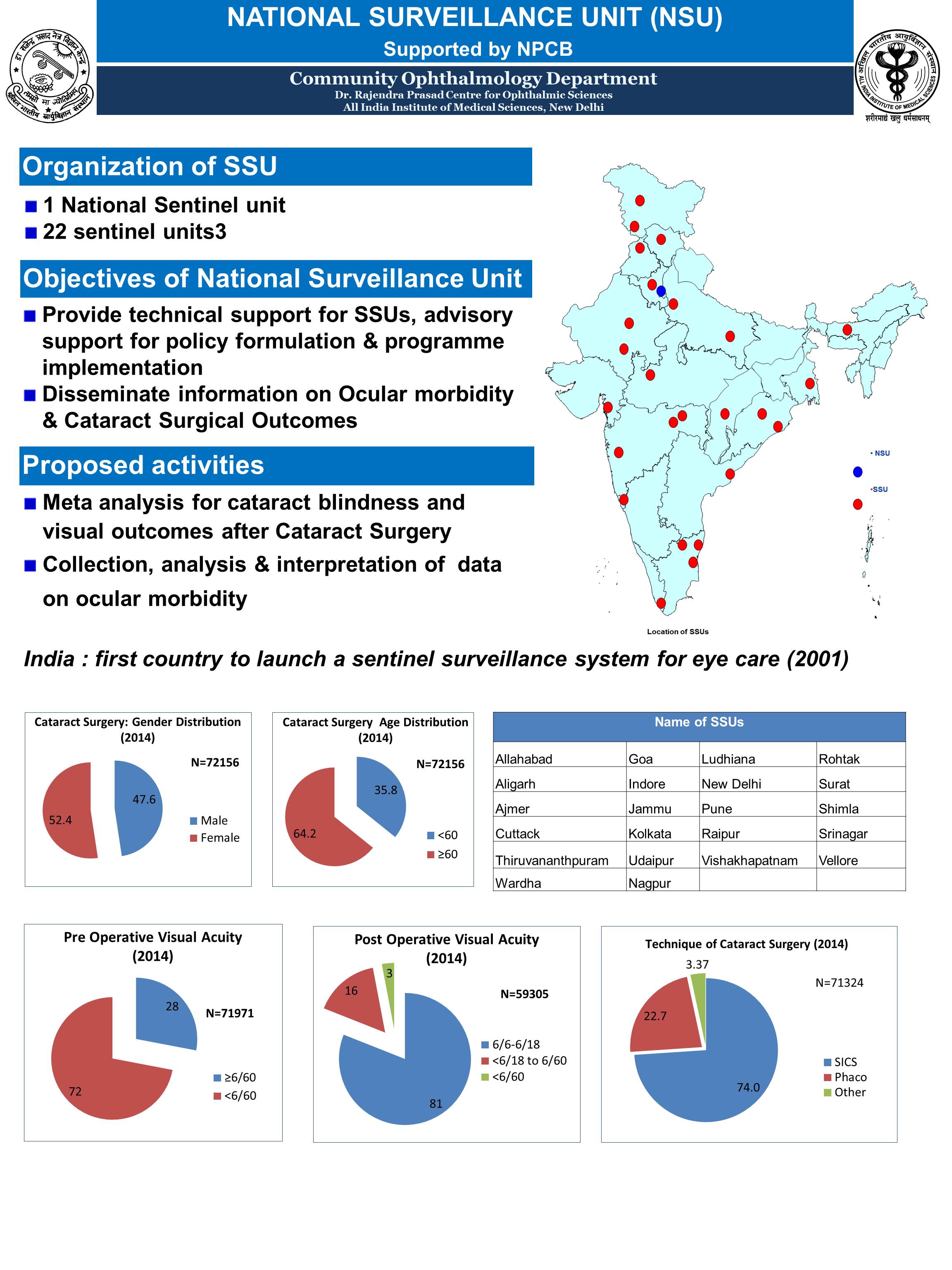
NSU SSU 2015
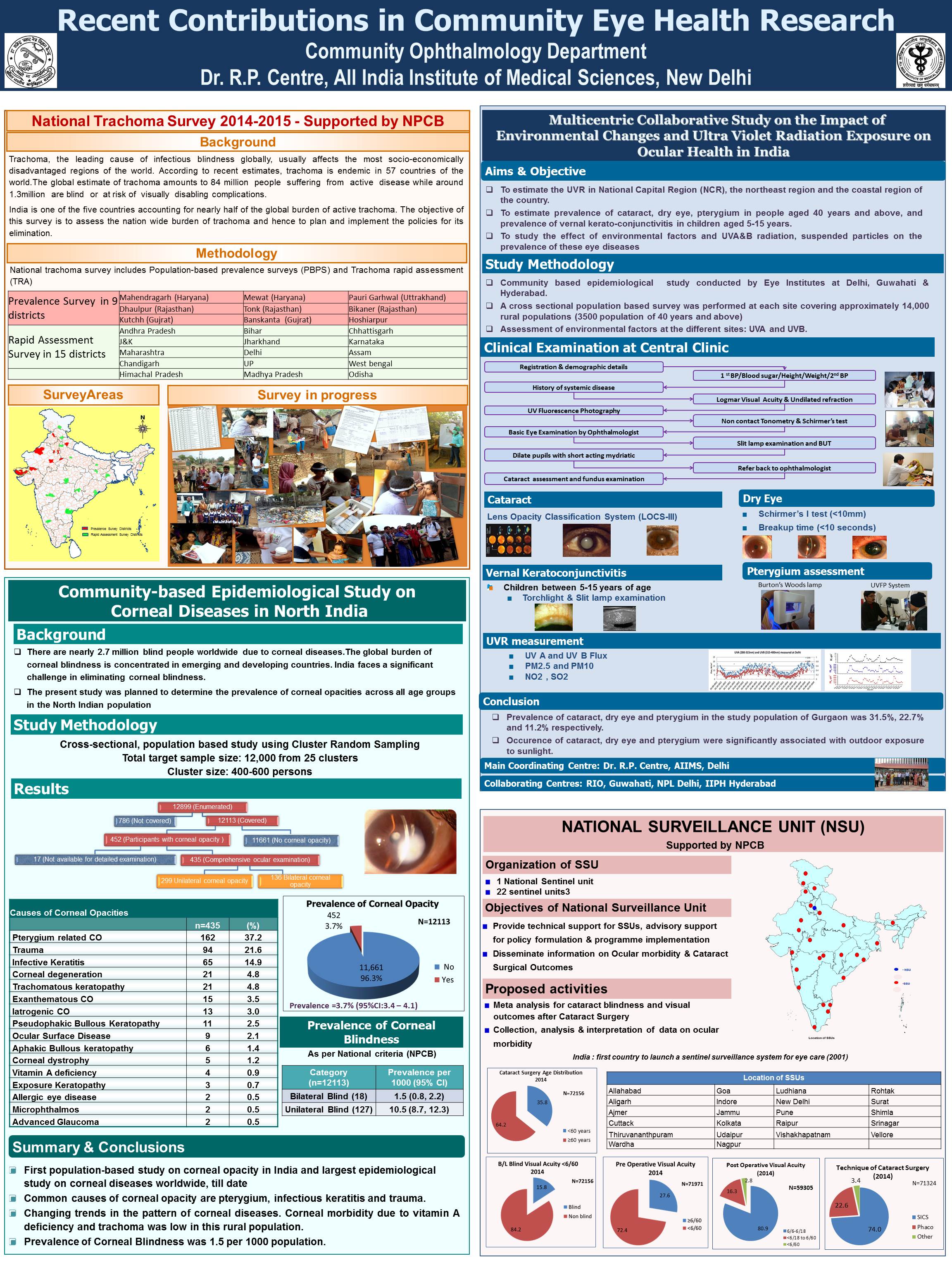
Recent Contributions in Community Eye Health Research
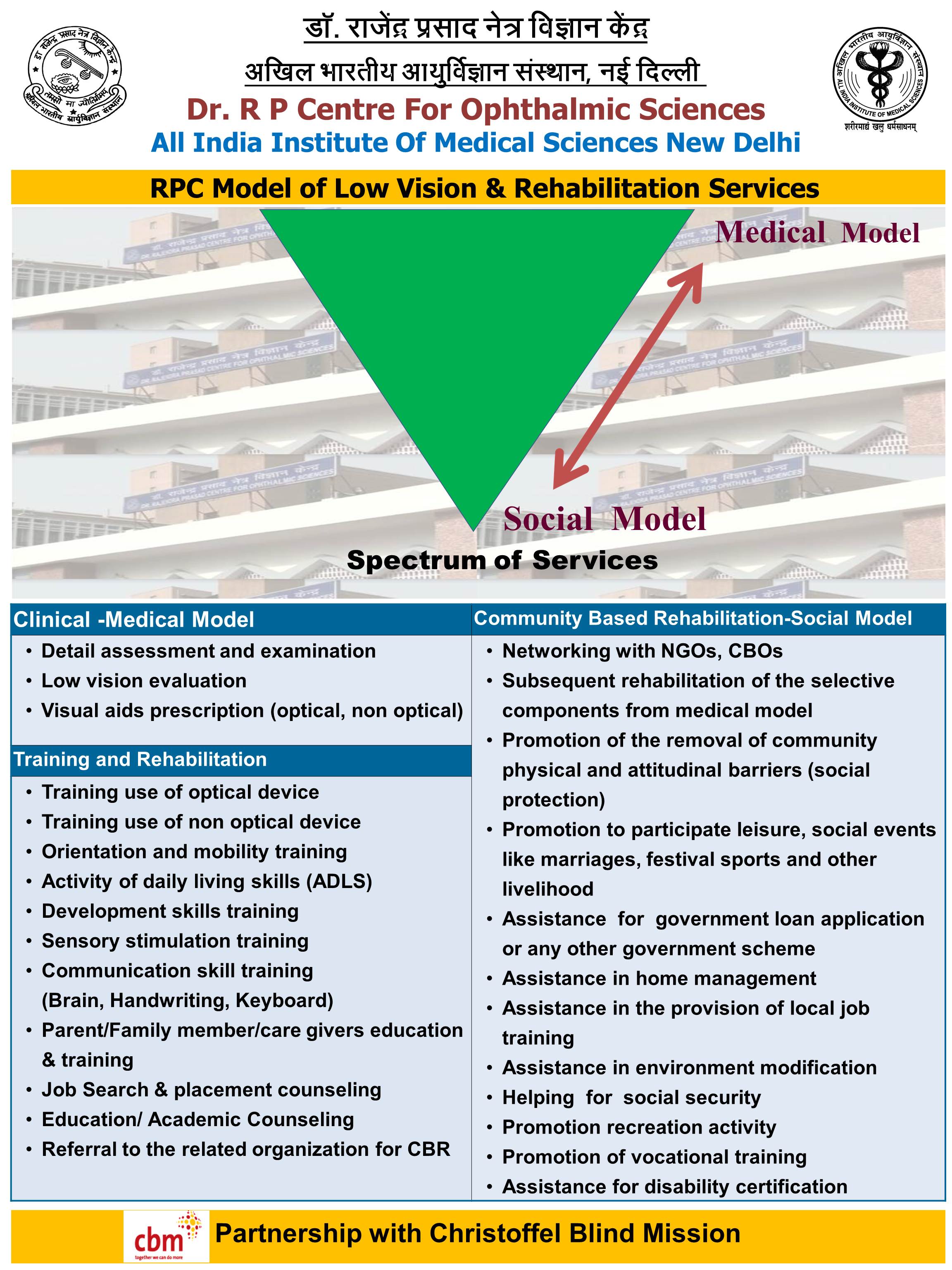
RPC Model of Low Vision & Rehabilitation Services
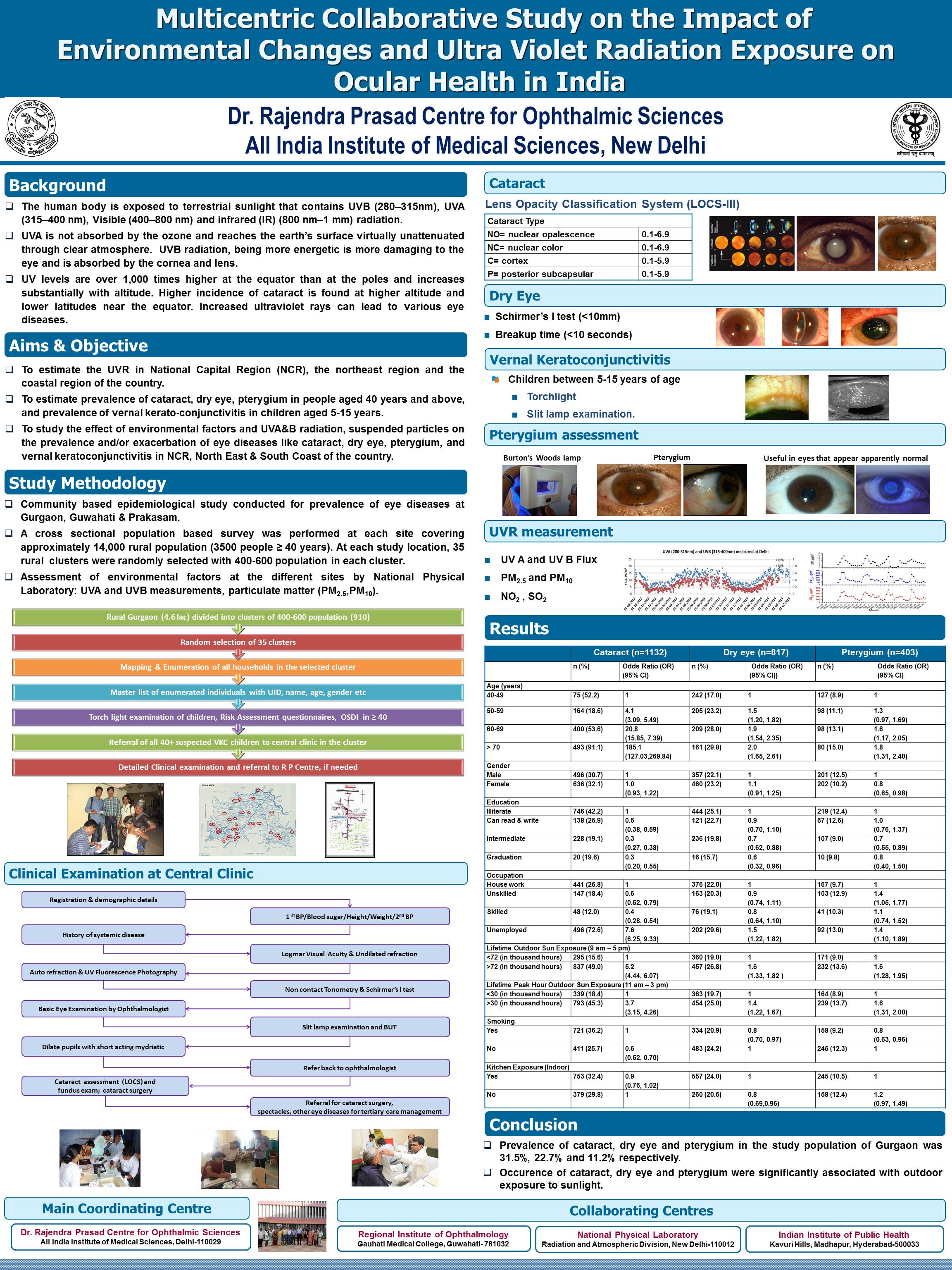
UVR Poster 2015
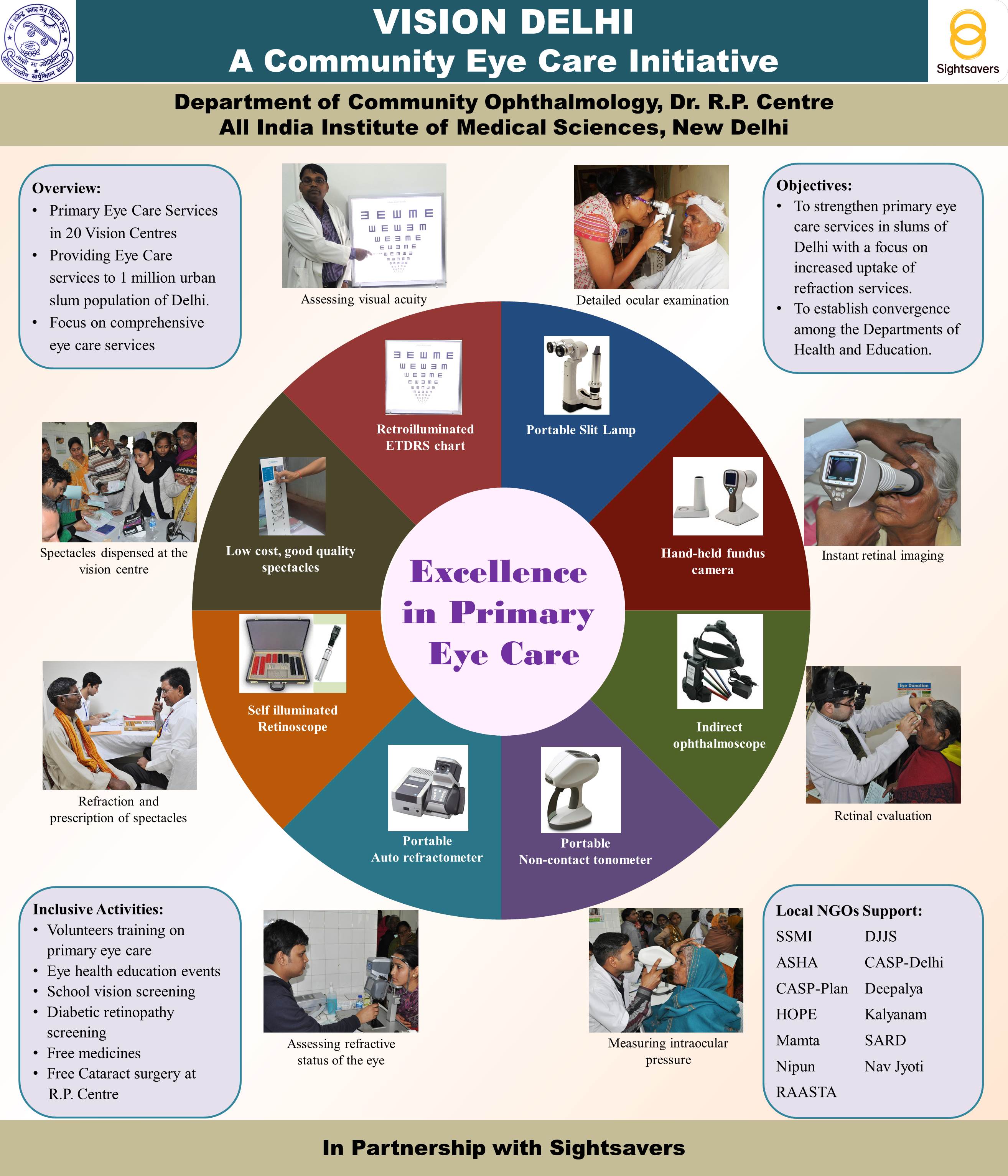
Excellence in Primary Eye Care
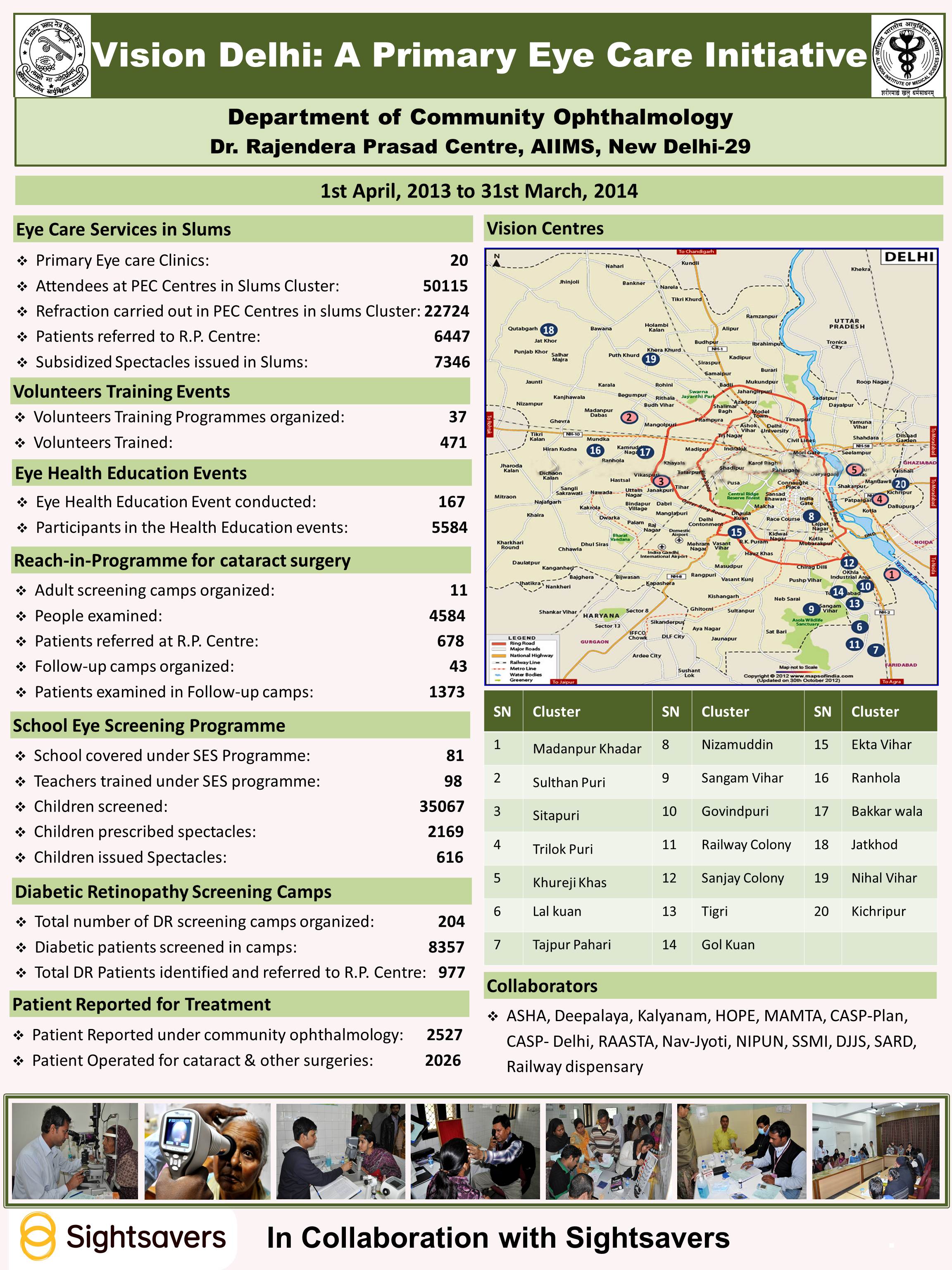
Vision Delhi- A Primary Eye Cate Initiative (1st April to 31st March)
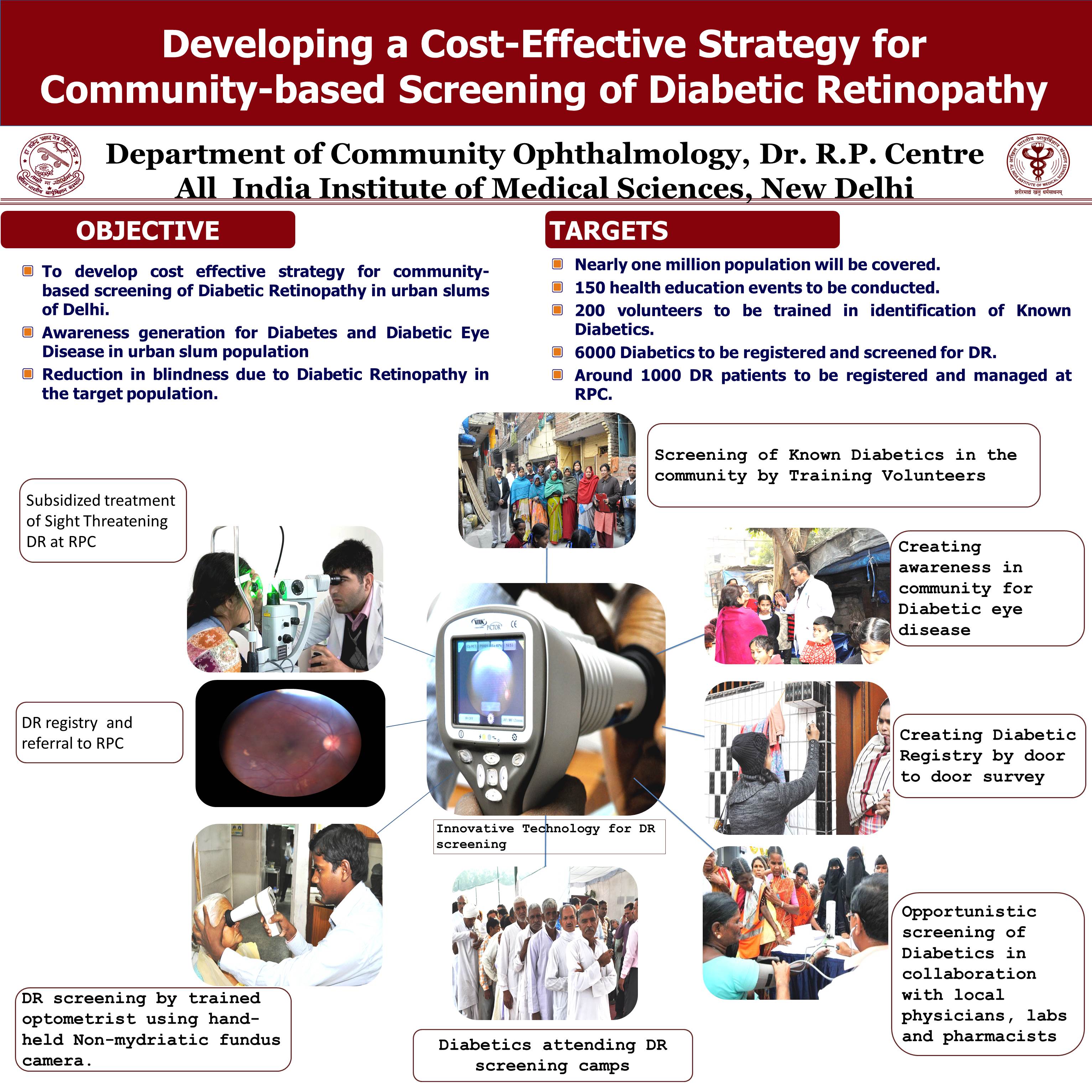
DR Screening Poster
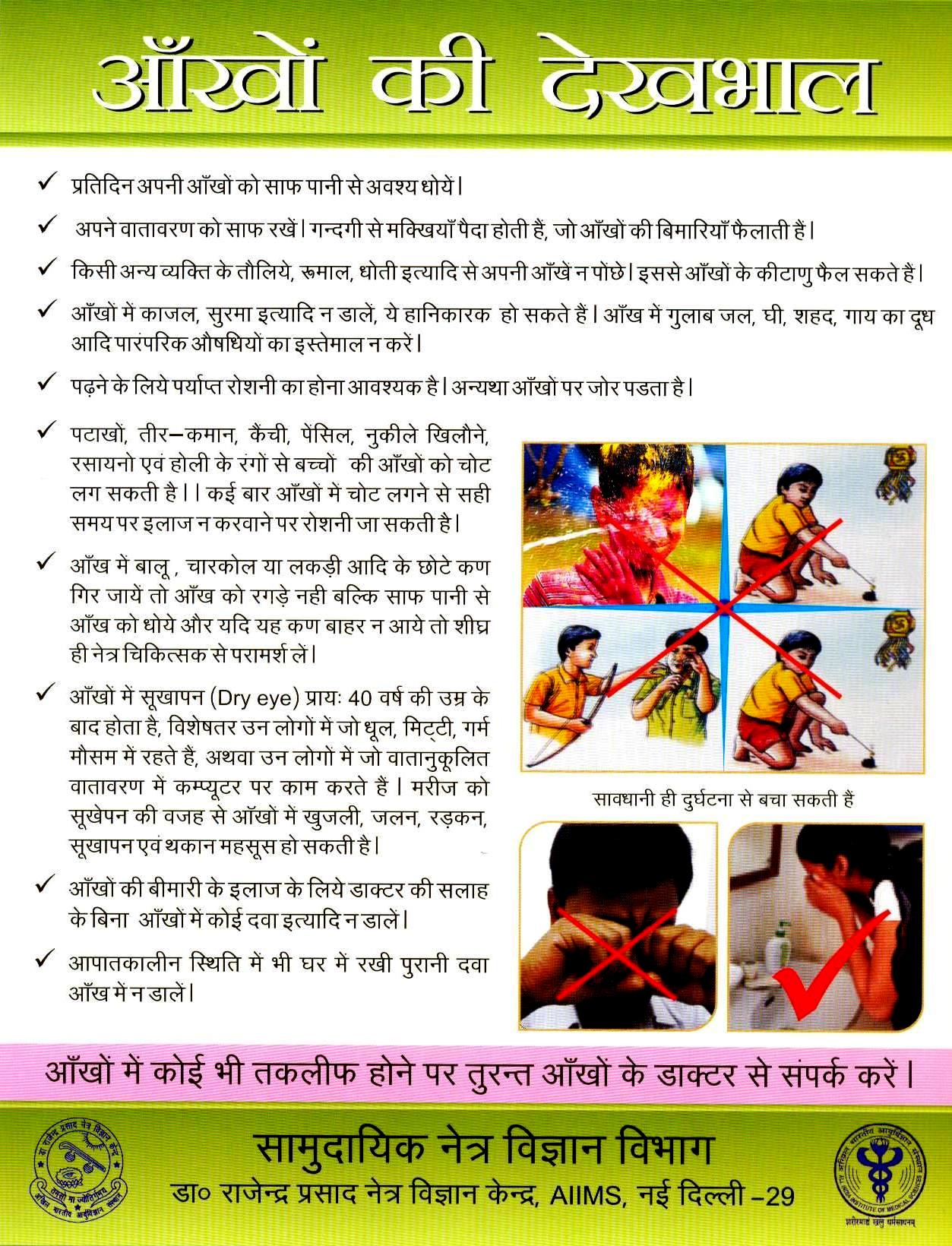
General Eye Care
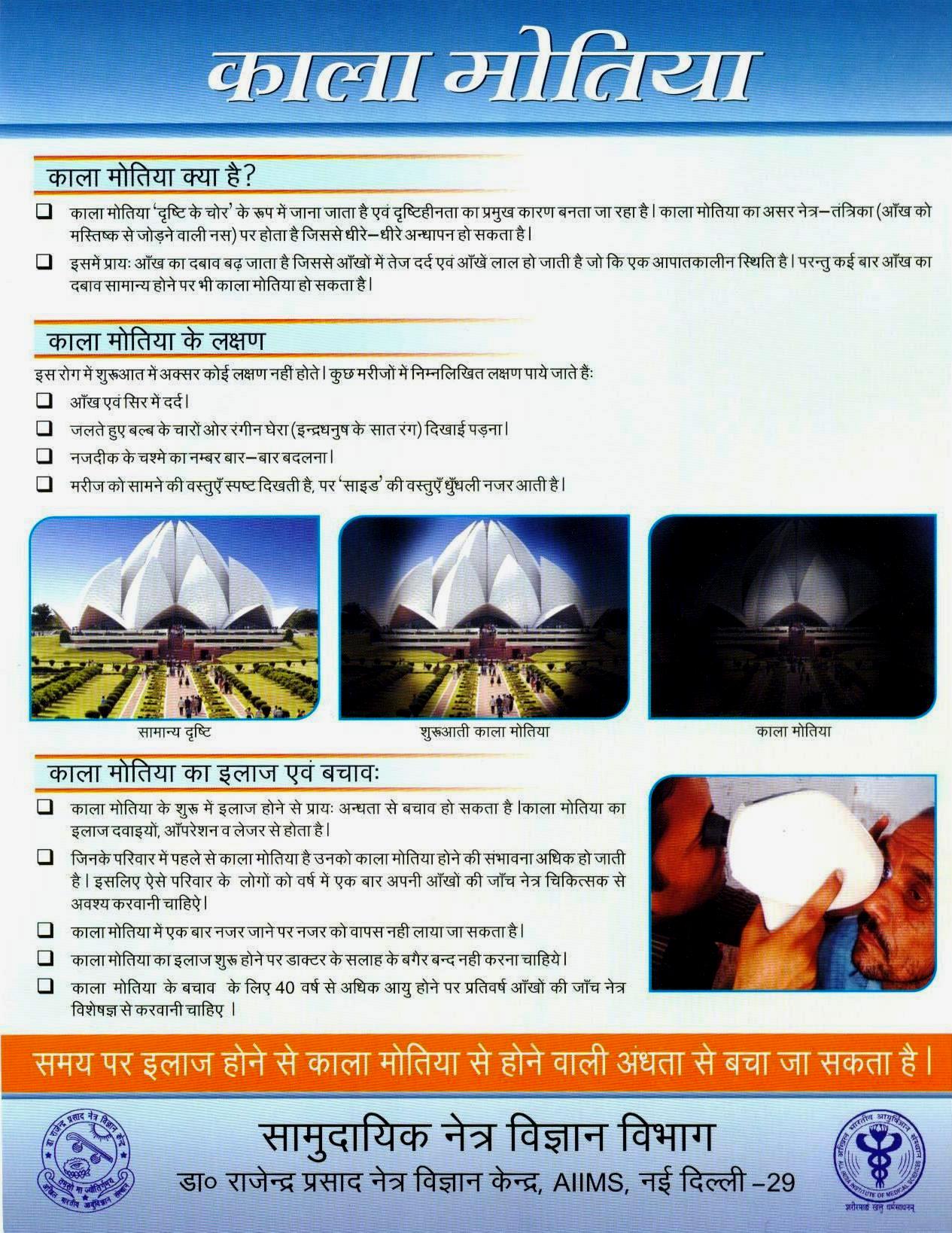
Glaucoma
Presbyopia
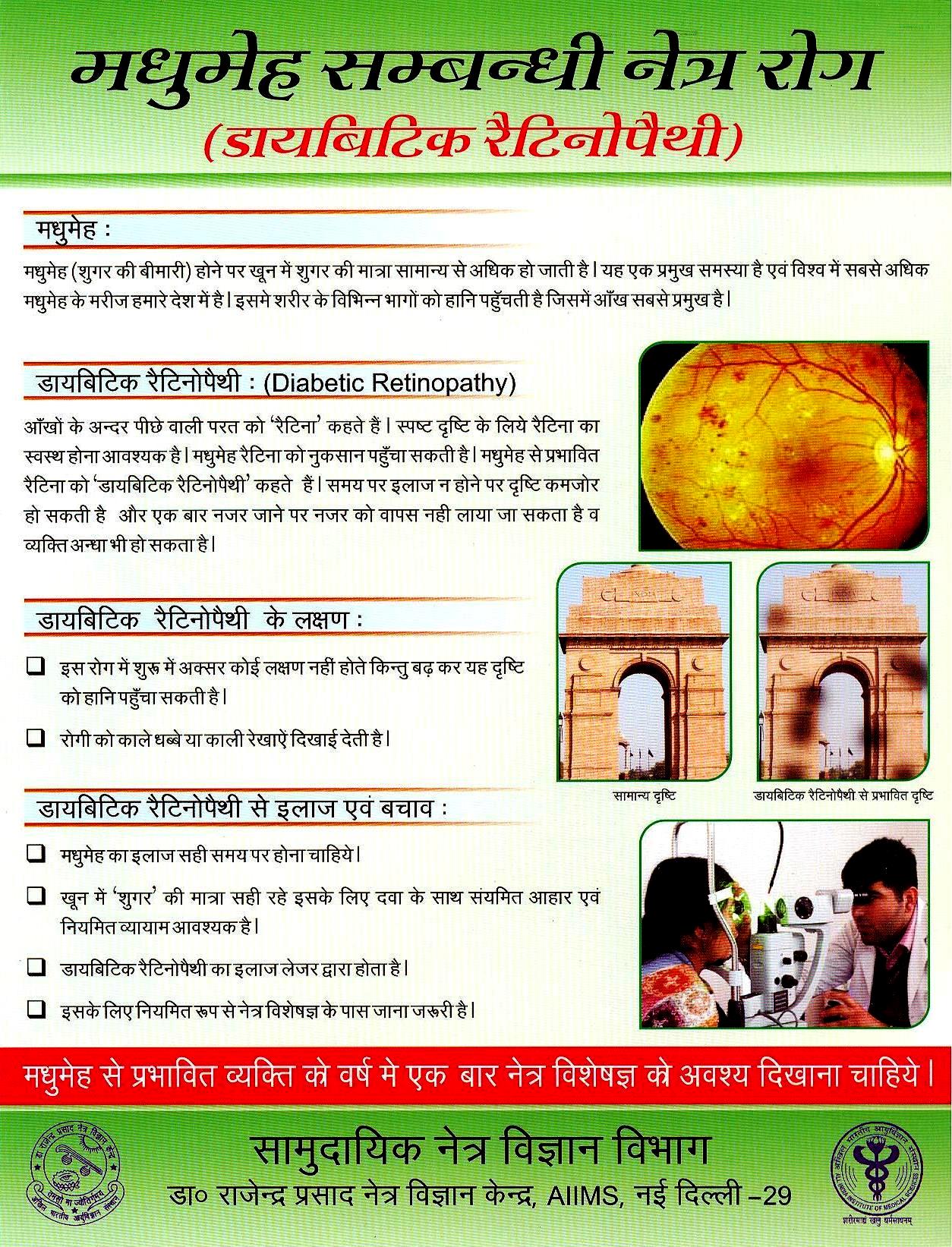
Diabetic Retinopathy
Refractive Error
Eye Donation
The eye health education unit of department is pro-actively engaged in developing IEC materials of common eye problem. Various IEC materials like small booklets, pamphlets, posters, Audio-visual movie pertaining to eye care have been developed. Community leaders, parents and guardians, school teachers are main target for eye health education. Community ophthalmology has initiated health education activities for patients utilizing out-patient and inpatient services at the institute. This is in addition to the already ongoing health education activities at the primary eye care clinics. The topics for health education are wide ranging such as general eye care, care of spectacles, refractive error, care after cataract surgery, glaucoma, retinoblastoma, retinopathy of prematurity etc. These are undertaken in conjunction with faculty and residents from respective sub-specialties, optometrists, nurses and medical social workers of RP Centre. Faculty from the department were involved in the NPCB program on sensitization of Doctors/Paramedics about the eye donation and its importance as well as the vital information related to eye donation and delivered talks on the same during the Eye Donation Fortnight 2020. Posters :- Cataract, Refractive Error, Presbyopia, General Eye Care, Conjunctivitis, Vitamin 'A', Eye Donation Magnitude of Trachoma NPCB Survey (2014-2015) NSU SSU 2015 Recent Contributions in Community Eye Health Research RPC Model of Low Vision Rehabilitation Services UVR Poster 2015 Excellence in Primary Eye Care Vision Delhi- A Primary Eye Cate Initiative (1st April to 31st March) DR Screening Poster Health Education Pamphlets on Primary eye care: Health education booklet on PEC (http://www.aiims.edu/images/depart/RPC/Books/Booklet%20RPC-28%20June%202014%20Output.pdf) General Eye Care Glaucoma Presbyopia Diabetic Retinopathy Refractive Error Eye Donation Training Manuals on Primary eye care 1. Training of School Teachers for School Vision Screening to Prevent and Control Childhood Visual Impairment and Blindness 2. Manual on Training of Trainers for Volunteers in Primary Eye Care 3. Vision Screening Card for Schools 4. Vision Screening Card for Primary Eye Care
The department is currently involved in The National Survey on Human Resources & Infrastructure for Paediatric Eye Care Services in India. As on 15th October 2020, there are nearly 10303 eye institutes in the entire country, out of which 8125 (78.9%) institutes have been contacted telephonically for participation in the HR survey. Out of them, completed responses have been received from 7200 institutes (Response Rate 88.6%) & about 2000 institutes were found to have paediatric oriented services (defined as paediatric OT facilities under general anaesthesia).
National Blindness Survey was completed in 30 districts and National Trachoma Survey in 24 districts in the country with support from National Programme for Control Blindness (NPCB), Government of India. Under the NBS and in each district, a sample of 3000 participants aged 50 years and above were enumerated and at-least 90% of them were examined across 50 clusters spread throughout the district. A GIS based map of each cluster covered was also being prepared. It was for the first time that an assessment of diabetic status and evaluation of patients (either newly diagnosed or previously diagnosed) for presence of Diabetic Retinopathy was also being done in a nation-wide manner. Each survey was facilitated and closely monitored by faculty from RP Centre at initiation, interim and towards the end of the survey which required 10-18 days of continuous field work. Emphasis was given for involvement of local medical colleges or renowned non-profit centres of Ophthalmology when doing the survey in a district. Over 93,000 participants were enrolled in the National Blindness Survey and over 25,00 children and 55,000 adults in the National Trachoma Survey.
Historically, the Community Ophthalmology department has been engaged in various national level blindness surveys, INDEYE and INDGEN studies on age related eye diseases and its genetic component in collaboration with LSH&TM, manpower and management training with Lions Club International Foundation, operational research studies with ORBIS, situational assessment of eye care infrastructure, Corneal Opacity Rural Epidemiological (CORE) study, North India Myopia Study (NIMS), training programs in primary eye care. Innovative tools such as the IND-VFQ, a National Surveillance Unit to assess the cataract surgical outcomes in country, IEC material on primary eye care were also developed and put into practice by the department. National agencies like ICMR, DST have been collaborated with in community based research work. Close collaborations have been developed with international agencies like World Health Organization, London School of Hygiene and Tropical Medicine UK, Wellcome trust, ORBIS, Sightsavers, Operation Eyesight Universal, CBM, Lions Clubs International Foundation etc.
Harpal Singh, PhD, Professor, Head Areas of Interest: Medical diagnostics, Drug Delivery Systems, Antimicrobial Polymers, Polymeric Hydrogels, Nanobiotechnology, Polymer based implants Medical devices Email: harpal [at] cbme.iitd.ac.in; Phone: +91-11-2659-1149 (O) |  | Arnab Chanda, PhD, Assistant Professor Areas of Interest: Biomimetics, Gait, Wearable Technologies, Soft Tissue Mechanics, Entrepreneurship Email: arnabchanda[at]cbme.iitd.ac.in; Phone: 011-2659-1086 | |
S. M. K. Rahman, Assistant Professor Areas of Interest: Computer architecture, embedded systems, microprocessor based industrial control, digital hardware design and medical electronics Email: rahman [at] cbme.iitd.ac.in; Phone: +91-11-2659-1152 (O) | Sandeep Kumar Jha, PhD, Associate Professor Areas of Interest: Biosensors (optical, piezoelectric, capacitive, electrochemical); nanoparticle sensing; microfluidic lab-on-a-chip; capillary electrophoresis microchip; immobilization and stabilization of biomolecules Email: sandeepjha [at] cbme.iitd.ac.in; Phone: +91-11-2659-1119 (O); | ||
Dinesh Kalyanasundaram, PhD, Associate Professor Areas of Interest: Laser based micromachining of composites; Finite Element Modelling; Orthopaedics/ Orthodontic implants; DNA based diagnostic devices; Lab-on-chip devices Email: dineshk [at] cbme.iitd.ac.in; Phone: +91-11-2659-7344 (O) | Anup Singh, PhD, Associate Professor Areas of Interest: Medical Imaging, image/signal processing, quantitative multi-parametric MRI, application of Machine Learning, development of methods/software for medical image/signal processing and data analysis. Email: anupsm [at] cbme.iitd.ac.in; Phone: +91-11-2659-1055 (O); | ||
Neetu Singh, PhD, Associate Professor Areas of Interest: Design and synthesis of nano-structured materials for biomedical implants, cancer diagnostics, tissue engineering and drug delivery. Systematic understanding of the bio-activity of nanostructures and developing specific "structure-bioactivity" relationships. Email: sneetu [at] cbme.iitd.ac.in; Phone: +91-11-2659-1422 (O); | Dr Amit Mehndiratta, MBBS, DPhil (Oxon), Assistant Professor Areas of Interest: Medical imaging, Image processing, Physiological modeling and Quantitative image analysis, Mobile assisted healthcare (m-Health), Email: amehndiratta [at] cbme.iitd.ac.in; Phone: +91-11-2659-6230 | ||
 | Dr. Deepak Joshi, PhD, Assistant Professor Areas of Interest: Brain-Computer Interface (BCI), Development of Intelligent Prosthesis, Signal Processing and Machine Learning for Neuroprostheses, Neuromusculoskeletal modelling. Email: joshid [at] cbme.iitd.ac.in; Phone: +91-11-2659-1155 (O) | Dr. Jayanta Bhattacharyya, PhD, Assistant Professor Areas of Interest: Bio-materials, Nanoparticles, Genetically engineered polypeptides, Drug delivery, Healthcare. Development of bioinspired and bio-derived materials to meet unmet needs in treating and diagnosing disease. Email: jayanta [at] cbme.iitd.ac.in; Phone: +91-11-2659-1337 (O) | |
| Biswarup Mukherjee, PhD, Assistant professor Areas of Interest: Ultrasound imaging, Bioinstrumentation, Biomechatronics, Prosthetics and Rehabilitation, Haptics Email: bmukherjee[at] cbme.iitd.ac.in; Phone: --- |
Veena Koul, PhD,Professor, Areas of Interest: Biomedical nanotechnology ,Biomaterials, Medical Devices, Soft Tissue regeneration and Drug Delivery Systems Email: veenak [at] cbme.iitd.ac.in; veenak_iitd [at] yahoo.com Phone: +91-11-2659-1041 (O)/6132/ 6396 (PA) |
Prof. S.K Guha, Honorary Professor Indian Institute of Technology Delhi Areas of Interest: Biomedical Engineering. Email: ; Phone: --- (O) |
Harpal Singh, PhD, Professor, Head Areas of Interest: Medical diagnostics, Drug Delivery Systems, Antimicrobial Polymers, Polymeric Hydrogels, Nanobiotechnology, Polymer based implants Medical devices Email: harpal [at] cbme.iitd.ac.in; Phone: +91-11-2659-1149 (O) | | Arnab Chanda, PhD, Assistant Professor Areas of Interest: Biomimetics, Gait, Wearable Technologies, Soft Tissue Mechanics, Entrepreneurship Email: arnabchanda[at]cbme.iitd.ac.in; Phone: 011-2659-1086 | |
S. M. K. Rahman, Assistant Professor Areas of Interest: Computer architecture, embedded systems, microprocessor based industrial control, digital hardware design and medical electronics Email: rahman [at] cbme.iitd.ac.in; Phone: +91-11-2659-1152 (O) | Sandeep Kumar Jha, PhD, Associate Professor Areas of Interest: Biosensors (optical, piezoelectric, capacitive, electrochemical); nanoparticle sensing; microfluidic lab-on-a-chip; capillary electrophoresis microchip; immobilization and stabilization of biomolecules Email: sandeepjha [at] cbme.iitd.ac.in; Phone: +91-11-2659-1119 (O); | ||
Dinesh Kalyanasundaram, PhD, Associate Professor Areas of Interest: Laser based micromachining of composites; Finite Element Modelling; Orthopaedics/ Orthodontic implants; DNA based diagnostic devices; Lab-on-chip devices Email: dineshk [at] cbme.iitd.ac.in; Phone: +91-11-2659-7344 (O) | Anup Singh, PhD, Associate Professor Areas of Interest: Medical Imaging, image/signal processing, quantitative multi-parametric MRI, application of Machine Learning, development of methods/software for medical image/signal processing and data analysis. Email: anupsm [at] cbme.iitd.ac.in; Phone: +91-11-2659-1055 (O); | ||
Neetu Singh, PhD, Associate Professor Areas of Interest: Design and synthesis of nano-structured materials for biomedical implants, cancer diagnostics, tissue engineering and drug delivery. Systematic understanding of the bio-activity of nanostructures and developing specific "structure-bioactivity" relationships. Email: sneetu[at]cbme.iitd.ac.in; Phone: +91-11-2659-1422 (O); | Dr Amit Mehndiratta, MBBS, DPhil (Oxon), Assistant Professor Areas of Interest: Medical imaging, Image processing, Physiological modeling and Quantitative image analysis, Mobile assisted healthcare (m-Health), Email: amehndiratta [at] cbme.iitd.ac.in; Phone: +91-11-2659-6230 | ||
| Dr. Deepak Joshi, PhD, Assistant Professor Areas of Interest: Brain-Computer Interface (BCI), Development of Intelligent Prosthesis, Signal Processing and Machine Learning for Neuroprostheses, Neuromusculoskeletal modelling. Email: joshid [at] cbme.iitd.ac.in; Phone: +91-11-2659-1155 (O) | Dr. Jayanta Bhattacharyya, PhD, Assistant Professor Areas of Interest: Bio-materials, Nanoparticles, Genetically engineered polypeptides, Drug delivery, Healthcare. Development of bioinspired and bio-derived materials to meet unmet needs in treating and diagnosing disease. Email: jayanta [at] cbme.iitd.ac.in; Phone: +91-11-2659-1337 (O) | |
Biswarup Mukherjee, PhD, Assistant professor Areas of Interest: Ultrasound imaging, Bioinstrumentation, Biomechatronics, Prosthetics and Rehabilitation, Haptics Email: bmukherjee[at] cbme.iitd.ac.in; Phone: --- | - | - |
Veena Koul, PhD,Professor, Areas of Interest: Biomedical nanotechnology ,Biomaterials, Medical Devices, Soft Tissue regeneration and Drug Delivery Systems Email: veenak [at] cbme.iitd.ac.in; veenak_iitd [at] yahoo.com Phone: +91-11-2659-1041 (O)/6132/ 6396 (PA) |
Prof. S.K Guha, Honorary Professor Indian Institute of Technology Delhi Areas of Interest: Biomedical Engineering. Email: ; Phone: --- (O) |
Prof. Sneh Anand, Prof Nivedita Karmakar Gohil,Prof S.K Guha, Prof S.N Tandon,Prof K.B. Sahay, Prof. Ray AlokRanjan, Prof. Dinesh Mohan
Primary eye care services: As a part of routine outreach eye care services, it runs twenty-eight Primary Eye Care Clinics in urban slums and underprivileged community of Delhi and National Capital Region in collaboration with Delhi Government and various NGOs. primary eye care services to poor and vulnerable communities as identified locations in Delhi. Patients requiring cataract surgery are transported to RP Centre and get admitted and operated free of charge.
Low Vision Rehabilitation Services: Under this initiative, vision rehabilitation services are being provided to people with visual disability by a rehabilitation team of Community Ophthalmology. Orientation & mobility, reading and writing rehabilitation services, low vision evaluation, counselling on vocational training, activities of daily living (ADL), Instrumental ADL, issuance of disability certificates, advice for environmental and lighting modification are various components of services being offered to the needy patients and family members. All the information about various government schemes and assistance to avail them are also provided. Young patients needing admission to schools for the blind are also helped. Community based rehabilitation is also run through networking system with various NGOs. Patients are being referred for vocation training to such NGOs.
Volunteers training: Community ophthalmology provide training to the volunteers in primary eye care and involve volunteers in the vision centres and camp activities.
Health education on Primary eye care: Regular eye health education events are conducted to create awareness on eye health.
School based screening: The department also involved in screening school children of Delhi for refractive errors and trains school-teachers. Screening is done through existing vision centers of department and also by involving and training teachers in school-based screening activities.
Reach In Programme (RIP): Reach in Programme is astrategy to capture unreached and vulnerable population of cataract patients through partnerships with community based organizations. Through it, screening camps are organized in surrounding areas of Delhi and free cataract surgical services are done through community eye care ward at R.P. Centre. There are more than 10 NGOs which involved in Reach in Programme.
Diabetic Retinopathy (DR) screening in urban slums: daily one campsorganized with support of local NGOs. Known diabetic patient are identified through house to house visits with the support of volunteers. These patients are invited in the DR screening camps in the local areas. A low cost non mydriatic fundus camera is used for screening of DR cases. All suspected DR cases are referred to RP Centre for further management.
Outputs of activities of Community Ophthalmology Department in relation to patient care during the period March 2019 to March 2020:-
| Title | Download |
|---|---|
| Primary Eye Care Services through Vision Centres | |
| Number of Vision Centres | 28 |
| Attendees at Vision Centres | 82166 |
| Refractions Conducted | 34293 |
| Spectacles prescribed | 33497 |
| Patients referred to R.P. Centre | 9816 |
| Primary Eye Care Volunteer training events | |
| Volunteers Training Programmes organized | 42 |
| Volunteers Trained | 414 |
| Eye Health Education Events | |
| Eye Health Education Events conducted in Vision Centres | 1106 |
| Eye Health Education Events conducted in RPC | 184 |
| Reach-in-Programme for cataract surgery in Rural and remote areas | |
| Cataract screening camps organized | Nil |
| People examined | Nil |
| Refraction | Nil |
| Patients referred to R.P. Centre | Nil |
| School Eye Screening (SES) Programme | |
| Schools covered under SES Programme | 67 |
| Numbers of Children screened | 58110 |
| Refractions Conducted | 5838 |
| Spectacles Prescribed | 5142 |
| Spectacles Booked | 5142 |
| Diabetic Retinopathy Screening Camps | |
| Total number of DR screening camps organized | 257 |
| Diabetic patients screened in camps | 3405 |
| Total DR Patients identified | 409 |
| Total DR Patients referred to R.P Centre | 405 |
| Patient Reported for treatment at Dr. R.P. Centre under Community Ophthalmology | |
| Total Patient Reported under community ophthalmology: | 5251 |
| Total Patient Operated for cataract surgeries under community ophthalmology | 2156 |
| Follow-up camps organized | 48 |
| Patients examined in Follow-up camps | 1437 |
| Total Patient Reported under community ophthalmology: | 5251 |
| Low Vision Rehabilitation | |
| Total Enrolled | 1207 |
| Mobility Training | 581 |
| ADL Counselling | 1085 |
| Visual Disability Certification | 388 |
| Vocational Training | 45 |
| Special School Admission | 49 |
Additional Professor
Address: Room No 3040, 3rd Floor, Teaching block,
Department of Biochemistry
All India Institute of Medical Sciences
Ansari Nagar, New Delhi-110029
Official Phone: (O) 011-26593706 (Ext) 3706
Email id: riyazmir[at]aiims[dot]edu,riyaz978[at]gmail[dot]com
| Additional Professor | Biochemistry, AIIMS, New Delhi | 2023- present |
| Associate Professor | Biochemistry, AIIMS, New Delhi | 2020-2022 |
| Assistant Professor | Biochemistry, AIIMS, New Delhi | 2016-2020 |
| Postdoc Fellow | University of Nebraska Medical Center, USA | 2011-2016 |
| PhD | Biochemistry, AIIMS, New Delhi | 2005-2011 |
Editorial board member Clinical pathology and research Journal
We are a dedicated team of researchers focused on understanding the role of the R2TP complex in malignancy. The R2TP complex is a co-chaperone of Hsp90, involved in the assembly and stabilization of various macromolecular complexes in the cell. The interactions and collaborative functions of the R2TP complex with its clients remain poorly understood and unexplored. Our research delves into the molecular associations of the complex whilst cancer progression and how it can potentially be targeted for therapeutic interventions.
Additionally, we explore the functions of tumour suppressors, crucial proteins that play a pivotal role in preventing the uncontrolled growth of cancer cells. Understanding how these proteins operate and how they can be manipulated is a key aspect of our work.
Furthermore, our lab is also interested in the effects of genetic manipulation in mammalian inner ear cells. This area of research is important for understanding hearing loss and other inner ear disorders, and it has implications for the development of potential treatments.
We are committed to advancing knowledge in these areas and contributing to the development of novel strategies for treatment. To learn more about our ongoing projects and recent discoveries, please email

L to R: Ayesha, Pankaj, Hema, Dr Riyaz, Dhiraj and Mahaiwon
Present Lab members:
Mahaiwon is investigating the molecular associations and clinical significance of the R2TP complex in cervical cancer. She joined the lab in August 2017 and completed her M.Sc. Medical Biochemistry in AIIMS, New Delhi in 2019 with a thesis that analyses the expression of the R2TP complex in Diffuse Large B Cell Lymphoma. She qualified for the CSIR NET JRF in 2017.
Dhiraj started work at AIIMS as JRF in 2018 and enrolled as a PhD student in 2019. He studies the role of PIH1D1 (a subunit of the R2TP complex) in various phases of the cell cycle. He has completed his M.Sc. Bioinformatics from Jamia Millia Islamia University. He also qualified for the CSIR JRF in 2017 with AIR-63.
Pankaj’s work studies the trans-differentiation of inner ear supporting cells. This will provide insight into the development and function of supporting cells, leading to a better understanding of the biological roles these cells play.
Hema studies the role of the R2TP complex in the etiology of thyroid cancer. She completed her M.Sc. Medical Biochemistry in AIIMS, New Delhi in 2021. Her Master's thesis explored the role of B cells in a spectrum of Tuberculosis. She has qualified CSIR JRF and DBT JRF.
Ayesha joined in October 2022 and works on “Effect of genetic manipulation in mammalian inner ear cells”. She completed her M.Sc. Biosciences from Jamia Millia Islamia University. She qualified ICMR JRF(AIR-51).
Dr. Praveen Vashist, Dr. Suraj Singh Senjam, Dr. Vivek Gupta
Community Ophthalmology department of Dr. Rajendra Prasad Centre for Ophthalmic Sciences AIIMS is involved in community based activities like comprehensive primary eye care services, camps, school vision screening, low vision rehabilitation, and in epidemiological research and surveys, training and capacity building, community awareness and mobilization apart from academic activities. As a part of routine outreach eye care services, it runs fifteen integrated Primary Eye Care Clinics in urban slums and underprivileged community of Delhi. Since 2015, in collaboration with the Government of Delhi and with the support of Sightsavers NGO, services are being provided in the Delhi government and municipal health dispensaries / centres. There is a 30-bedded dedicated ward under community ophthalmology inside the centre. Outreach services also include screening of diabetic retinopathy in the underserved populations. Currently, there are three dedicated faculty members. Dr Suraj was awarded ACOIN Gold Medal for the year 2015-16 for excellence in Community Eye care. A team of 50+ supporting staff includes ophthalmologists, optometrists, research scholars, field investigator, health workers and data managers etc. The department has a PhD program and during 2019, three scholars were in various stages of their PhD program. The department was established in 1992 and is celebrating its silver jubilee in 2017.
Community Ophthalmology is involved in the activities like comprehensive primary eye care services, outreach eye camps in community as well as schools for the blind, school vision screening, low vision rehabilitation, and in epidemiological research and surveys, training and capacity building, community awareness and mobilization apart from academic activities. Outreach services also include screening of diabetic retinopathy in the underserved populations. Community ophthalmology is currently running 20 projects on eye care research & services in partnership with National agencies like NPCB&VI, DHR, ICMR, DST. Close collaborations have been developed with international agencies like World Health Organization, London School of Hygiene and Tropical Medicine UK, ORBIS, Sightsavers, Visionspring, Operation Eyesight Universal, CBM etc. Community Ophthalmology completed National Blindness and Visual Impairment (NB&VI) Survey2015-19 in 31 districts across the country with support from National Programme for Control Blindness and Visual Impairment (NPCB & VI), Government of India. The executive summaries of the National Blindness and visual Impairment Survey reports were released by the Hon’ble Minister of Health and Family Welfare of India, Dr Harsh Vardhan on 10-11 October 2019. Community Ophthalmology is collaborating with CARE department, IIT-Delhi for developing artificial intelligence, neural network, and vision computing based tools to detect glaucoma and diabetic retinopathy in patients receiving primary eye care services. Conducted anoperational research on involvement of Accredited Social Health Activists (ASHA) in delivery of primary eye care amongst urban poor population.
The department has dedicated teams that provide primary eye care services to poor and vulnerable communities as identified locations all over Delhi. These centres have been identified in collaboration with the local state government and with the various collaborative NGOs to ensure maximum benefit to the communities. The department conducts comprehensive eye camps under the Reach-In-Program in areas around Delhi (in NCR region). Patients that can be managed with these centres / camps are provided medicines and refraction services on the spot. Patients requiring cataract surgery are transported to RP Centre and get admitted and operated free of charge. Special arrangements are made to support the management of patients requiring management under various ophthalmic sub-specialties at RP Centre. Under Low Vision Rehabilitation services organized by the department, people with visual disability are being provided with low vision aids and visual rehabilitation services in the form of counseling, issuance of disability certificates, mobility & orientation training, activities of daily living training and advise for environmental and lighting modification etc. Community based rehabilitation is also run through networking system with various NGOs.
| In Charge | Dr.D.R.Shende - Professor |
| Faculty Member | Dr. Renu Sinha - Associate Professor |
This department is keenly involved in the newer techniques of providing safe and complication free anesthesia to children. The faculty has been involved in research activity to decrease the pain intra and post operatively and ease the recovery in all types of surgeries especially in squint surgery. The operation theatre at the R P Centre can run up to 4 tables simultaneously for general anesthesia patients. The department also provides emergency anesthesia facilities for trauma cases after routine OT. Anesthesia facilities are provided once a week in the OPD where minor OPD procedures and pediatric examination can be carried out.
| In-charge | Dr.Sanjay Sharma - Additional Professor |
|---|
Dr. R.P.Centre has its own radiology section which is equipped to carry out ocular radiological investigations using X-ray and ophthalmic ultrasound. Procedures performed include macrodacryocystography, orbital phlebography, evaluation of orbital fractures and foreign body localization on X-ray. There are 5 ultrasound machines available at different parts of the hospital including the OPD, casualty, wards and operation theatre and USG facility is available round the clock. For special investigations including CT scan with and without contrast, spiral CT, MRI, MR angiography, Colour Doppler and many other investigations the Department of Radiology, AIIMS provides support. All these investigations are available at a very subsidized rate to the patient and free services can also be provided to the needy.
About the Principal Investigator:
https://in.linkedin.com/in/pragyan-acharya-40599b16
@Acharya3Dr
https://www.researchgate.net/profile/Pragyan-Acharya
Organ Dysfunction- Mechanisms, Signaling and Biomarkers
The broad interest of the lab focuses on the pathogenesis of liver disease, particularly complications of liver cirrhosis such as acute-on-chronic liver failure (ACLF) and on non-alcoholic fatty liver disease (NAFLD). Our work centers around interactions and cross-talk between the immune system and the liver. Recent studies by our group has demonstrated the expansion of CD177+ neutrophils in ACLF and its relationship with patient mortality. Students in the lab are currently investigating the basis of such immune regulation and the potential of harnessing this information in developing new therapeutic approaches. In addition to immune- liver cross talk, a major interest of our group is to carry out systematic and rigorous biomarker discovery studies using mass spectrometry driven omics approaches (proteomics and metabolomics) and recent work by our group has uncovered novel biomarkers of acute kidney injury in ACLF. Our approach is to combine clinical observations in liver disease with mechanistic studies in lab cell culture and animal models.
Notable Awards and Society Memberships
Front : Dr. Pragyan Acharya
Back row (L to R): Nidhi Gauniyal, Shalini Sharma, Swati Srijaya Samantaray, Ditam Chakraborty, Rohini Saha, Aditya Roshan, Souvik Roy
WHAT THEY DO:
Rohini Saha- Studies neutrophil heterogeneity and its role in the Pathogenesis of Acute-on-Chronic Liver failure (ACLF). Rohini has also led some of the biomarker discovery projects in the lab.
Shalini Sharma- Studies the relationship between reactive oxygen species generation and organ dysfunctions
Ditam Chakaraborty- Studies the effect of ayurvedic formulation on the SARS-COV2 main protease in various cellular systems
Swati Srijaya Samantaray- Is involved in omics- driven biomarker discovery in organ dysfunctions and validation by various methods.
Nidhi Gauniyal- Is involved in establishing novel diagnostic methodologies for inherited liver disorders.
Aditya Roshan and Souvik Roy- are the newest additions to the lab and will be involved in studying neutrophil transmigration and NETosis respectively.
| PUBLICATIONS |
# As Corresponding author; * As First Author
Book Chapters
Cornea, Lens, Refractive Surgery, Low Vision Aids and Ocular Oncology
| S.No. | Name | Designation |
|---|---|---|
| 1 | Prof. Radhika Tandon | Professor and Officer-In-Charge |
| 2 | Prof. M. Vanathi | Professor of Ophthalmology |
| 3 | Prof. Bhavna Chawla | Professor of Ophthalmology |
| 4 | Dr. Noopur Gupta | Additional Professor of Ophthalmology |
| 5 | Dr. Neiwete Lomi | Associate Professor of Ophthalmology |
Dr. Amol Raheja
M.B.B.S, M.Ch., Skull Base and Cerebrovascular Fellow
Consultant and Assistant Professor, Neurosurgery
All India Institute of Medical Sciences and Jai Prakash Narain Apex Trauma Center
New Delhi, India; Phone: 91-11-26593291; Email: dramolraheja[at]aiims[dot]edu
Brief Profile –
Dr. Amol Raheja has been an AIIMS alumnus throughout his academic carrer. He joined the most prestigious and competitive medical school in India (AIIMS, New Delhi)in 2003. He was awarded a prestigious scholarshipunder the Kishore Vaigyanik Protsahan Yojana scheme in 2004 for best original research in medicine stream, which was conducted nationwide by Indian Institute of Science, Bangalore under the aegis of Department of Science and Technology, Government of India. After completing his medical schoolingin 2008; he joined M.Ch. Neurosurgery residency (6 years) in 2009. He had an excellent academic and surgical record throughout his residency training, with several publications in both national and international journals. He has also presented his work at various scientific meetings in India and abroad, which has resulted in best paper awards. He has won“Hindustan Ciba Geigy Epilepsy Award”for his work in the field of epilepsy surgery in 2014. At the largest international neurosurgical platform, he was awarded the prestigious “World Federation of Neurosurgical Societies – Young Neurosurgeon Award” in the year 2015for his original research in the field of traumatic brain injury. For his impeccable surgical skills, he has also won the first prize for “microsuturing and microneural anastamosis” atthe 15th Neurosurgery skills training workshop held at AIIMS. After completing his neurosurgical residency in 2015, he joined a 1 year clincial fellowship“Skull Base and Cerebrovascular Neurosurgery” at the University of Utah Medical Center, Salt Lake City, Utah, USA; under the mentorship of one of the world’s renowned skull base neurosurgeon – Professor William T. Couldwell. Subsequently he has joined as a faculty at AIIMS in the year 2016. He is well versed in all aspects of neurosurgery with special interest in Skull Base and Cerebrovascular Neurosurgery, and is currently working on many national and international research projects.
Areas of Interest – Neurosurgery (with special reference to) -
| 1. | ||
2. Designation | Dr ASHWANI KUMAR MISHRA Professor of Biostatistics (NDDTC) | |
| 3. Qualifications | PhD Statistics, MSc Statistics, BSc: Statistic and Mathematics | |
| 4. Email ID | akmaiims[at]gmail[dot]com, ashwanikm[at]aiims[dot]edu | |
| 5. Field of Interest | Broad Domain: Epidemiology, Biostatistics Sub-Domain: Substance Abuse, Clinical Epidemiology, Medical Epidemiology, Dimension Reduction Techniques, Computational Statistics | |
| 6. Total number of publications till date |
Total 159 | |
| 7. Details of publications since 2000 onwards (the full citation)- these should be divided into journal articles (peer reviewed publications) and books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications) | Thesis
Official Statistics
Theoretical Statistics
Epidemiology of Drug Use
Applied Statistics-Public Mental Health
Applied Statistics-Clinical Sciences
Applied Statistics-Scientometrics
Applied Statistics-Cancer Epidemiology & Population Genetics
Edited Manuscript-Associate Editor
Book Chapters
Technical Reports, Manual, Reports
| |
| 8. Presentations made at scientific meetings/ conferences/ workshops | Organisation of symposium/workshops/conference
Invited talks in conference, Symposium, Workshops
| |
| 9. Investigator in funded projects along with year and title (completed) |
| |
| 10. Investigator in funded projects along with year and title (ongoing) |
| |
| 11. Investigator in non-funded projects along with year and title (completed) |
| |
| 12. Investigator in non-funded projects along with year and title (ongoing) |
| |
| 13. Co-investigator in funded projects along with year and title (completed) |
| |
| 14. Co- investigator in non-funded projects along with year and title completed |
| |
| 15. Co- investigator in funded projects along with year and title (ongoing) |
| |
| 17 Co- investigator in non-funded projects along with year and title (ongoing) |
| |
| 18. Thesis supervised for MD/ PhD | - as guide (number only | 04 |
| -as co-guide (number only | 39 | |
| -as member of doctoral committee | 08 | |
| 19. Significant events |
| |
| 20. other relevant information | Awards and Honours Education 1999:FirstClassFirstforPost-GraduateExamination (GOLDMEDAL) 2001:FellowshipinBiostatistics fromSGPGIMS,Lucknow 2003: Received Post Graduate Education Certificate for Advanced Course inBiostatisticsandEpidemiologyfromNordicSchoolofPublicHealth,Goteborg andRDGardi MedicalCollege,Ujjain 2004: Faculty for the International Course on Health Intervention Studies,in collaborationwith Nordic SchoolofPublicHealth 2005: Faculty for the International Course in Research Methodology incollaboration with Nordic School of Public Health and RD Gardi MedicalCollege,Ujjain 2013: Awarded Certificate of Accomplishment with Distinction for the courseMathematicalBiostatisticsBootCamp,offeringofJohnHopkin'sUniversity,USA 2020:Receivedcertificationofcompletionwith91.2%MarksforthesuccessfulcompletionofthecourseonSystematicReviewandMeta-Analysis,fromJohnHopkinsUniversity,USA 2020: Letter of Commemoration from Vice-Chancellor, HNB UttarakhandMedicalEducationUniversityforeffectiveplanning,managementoftheONLINEcourseinResearchMethodologyasCourseCoordinator 2020: Received DSTGrantfrom DepartmentofScience andTechnology(DST) under the Accelerate Vigyan Scheme through Scientific and EngineeringResearch Board (SERB) for organizing 9 days online workshop on AnalyticalTechniques for StatisticalAnalysis inMentalHealth 2021:ElectedMemberEducationSubcommitteeforInternationalSocietyforClinicalBiostatistics(ISCB).ThishonourisquiteprestigiousinthesensethatI happen to be not only the member from India, or Asia but the only memberfrom the Developing world. In total there are 15 [14+1] members in thiscommittee. The other 14 members belong developed/high income countries [1Member each from Australia (AU), Canada (CA), France (FR), Romania (RO),3 Members from New Zealand (NZ), 5 Members from United Kingdom (UK),and2MembersfromUSA(US).Thiscommitteesupportsandorganizeeducationalactivities,suchasshort-courses,webinars,andseminarsoncontemporary methodsin Clinical Biostatistics. 2021:SuccessfullyCompletedPaidCoursewithExaminationonDataScienceandMachineLearning:MakingDataDrivenDecisionconductedbyMassachusetts Institute of Technology (MIT) and MIT Institute for Data,Systems,andSociety(MIT-IDSS). 2022: Nominated as the Board Member by Department of Medical EducationandResearch(DMER)byGovernmentofHaryana,forPromotionofResearchinMedicalUniversities. Research Awards 2007:WorldBankTravelgrantforattending56thInternationalStatisticalInstitute Conference held at Lisboa-Portugal, for thesis research paper SomeEpidemiologicalModelsforparasiticInfections:Comparisonbetweentraditionaland hierarchicallogisticregressionmethods 2014: World Bank Travel grant for attending 9th International Conference onTeaching Statistics for the research paper Challenges in Teaching of MedicalStatistics inDevelopingCountry 2017:AwardfromAIIMS,DelhifortheresearchpaperPatternofDrugUseandassociated behaviors among Female Injecting Drug Users from Northeast India:AMulti-Centric,Cross-Sectional,ComparativeStudy.SubstanceUse&Misuse Associate Editor 2022-till date: Statistical Editor, International Journal of Health Research and Medico-legal practice (IJHRMLP); Official publication of the Academy of Health research and Medical Education (AHRME) 2020-tilldate:AssociateEditor,FrontiersinPublicHealth for the Speciality Section Public Mental Health 2017-tilldate:AssociateEditorTobaccoandRegulatorySciences Reviewer
Membership of the Scientific Societies
|
Oculoplasty, Ocular oncology, Strabismus Neuro-ophthalmology
| S.No. | Name | Designation |
|---|---|---|
| 1 | Prof. Mandeep.S. Bajaj | Professor and Officer-In-Charge msbajaj32[at]hotmail[dot]com |
| 2 | Prof. Neelam Pushker | Professor of Ophthalmology pushkern[at]hotmail[dot]com |
| 3 | Prof Rohit Saxena | Professor of Ophthalmology rohitsaxena80[at]yahoo[dot]com |
| 4 | Dr.Swati Phujihele Aalok | Additional Professor of Ophthalmology |
| 5 | Dr.Rachna Meel | Additional Professor of Ophthalmology dr[dot]rachnameel[at]gmail[dot]com |
| 6 | Dr.Rebika | Assistant Professor of Ophthalmology |
| 7 | Dr. Sahil Agrawal | Assistant Professor of Ophthalmology |
The Oculoplasty and Oncology Services of Unit 5 have pioneered several surgical techniques including ptosis correction via conjunctival route, novel eyelid reconstruction methods and socket reconstruction using cultivated amniotic membrane graft. The unit has also conducted noteworthy research activities including genetic studies on congenital eyelid anomalies, use of minimally invasive technique for canalicular obstruction, anti-metabolites in contracted socket and lacrimal drainage system, to name a few.
The Unit provides state of art orbital, eyelid, lacrimal and ocular oncology care for cancers including orbital rhabdomyosarcoma, eyelid carcinomas, lacrimal gland adenoid cystic carcinomas, ocular surface malignancies, melanoma and retinoblastoma in coordination with paediatric, medical and radiation oncology teams of AIIMS. The unit is one of the few centres in the world to publish studies on sentinel lymph node biopsy in high-risk eyelid cancers which helps in better prognostication and treatment outcome. Both intramural and extramural research projects are ongoing in the field of clinical and molecular oncopathology. Tumour DNA sampling in retinoblastoma, molecular markers in retinoblastoma, ocular surface neoplasia, eyelid malignancies, lacrimal adenoid cystic carcinoma and ocular melanoma are some of basic research that is ongoing in close collaboration with ocular pathology team.
The Unit provides Ophthalmic Plastic and Reconstructive Surgery for a wide variety of disorders including ptosis, congenital structural anomalies including use of expanders in congenital contracted socket, cosmetic blepharoplasty, eyelid retraction surgery, problems related to lacrimal drainage system, trauma-related orbital and periorbital deformities. Procedures such as orbital decompression surgeries, evisceration, enucleation, exenteration, placement of implant, botulinum toxin injections and scar revision surgeries etc are also routinely performed in the unit.
During COVID-19 pandemic, the Oculoplasty Team was at the forefront in the management of cases with rhino-orbital mucormycosis during the epidemic of mucormycosis in the second wave of COVID-19 infection. We formed the AIIMS-RPC Guidelines for Early Detection and Prevention of Mucormycosis for the community and doctors which was also released by the press. In collaboration with Community Ophthalmology, we released the posters for awareness of patients and community mentioning the red flags for early detection and overall management and care of patients which included the follow-up advice also. Screening Guidelines were laid down by the Oculoplasty team and intensive screening for development of early signs of mucormycosis in indoor patients affected by COVID-19 infection on ventilator or any form of oxygen therapy with high-risk features was conducted by our team at various COVID wards in AIIMS for prompt treatment. Active participation of Faculty in Webinars on mucormycosis, including lectures, was conducted for teaching the residents on the early detection and treatment of mucormycosis. Studies related to impact of COVID-19 pandemic were initiated with the focus on the delayed presentations of mucormycosis and role of trans-cutaneous intra-orbital amphotericin B injections in early or recurrent cases of mucormycosis as a funded project. Psychosocial impact of destructive procedure, delayed presentations of cancer patients and change in pattern of orbital and periorbital infections during the COVID-19 pandemic are some of the ongoing studies. We have an active ongoing collaboration with the basic sciences on various projects related to mucormycosis.
Over the past few years, in the field of Oculoplasty, there has been a paradigm shift from invasive surgery to non-surgical and minimally invasive therapeutic procedures with aesthetically pleasing and promising results. Some of the important ongoing studies in line with this concept are - nonsurgical management of peri-orbital veno-lymphatic malformation by intralesional sclerotherapy, role of oral sildenafil, topical medication for ptosis pyogenic granuloma, abdominal fat transfer for the correction of cicatricial ectropion, use of botulinum toxin in thyroid eye disease and sutureless technique in skin grafting procedure. Some pioneering studies that are under publication are on single-stage surgery for eyelid reconstruction procedure, novel approach for protection of ocular surface in severe burn or trauma cases, ocular surface reconstruction using collagen matrix in patients with ocular surface chemical burns etc.
More recently we have worked on role of biomarkers in fungal infection, use of fat graft in orbital volume augmentation, intralesional sclerotherapy in periocular and adnexal veno-lymphatic malformation, innovations in ptosis surgery, antimetabolites in contracted socket, intravitreal chemotherapy in retinoblastoma, orbital implants in enucleated socket, etc and published some of these studies in eminent journals.
The unit has been at the forefront of ocular cancer research, including clinical trials into new and better treatments. Publications in indexed journals, constant teaching and participation of resident doctors in ongoing CME programs, workshops and conferences are part of the training program. The Unit Faculty published more than 20 research articles in the year 2021-22 and presented their work through several webinars and online conferences. Our resident doctors received 5 awards in National and Internationalconferences. The unit annually conducts the Oculoplasty and Ocular Oncology workshop, maintaining its tradition of the year round workshops in the challenging times of the pandemic. A comprehensive overview of diagnostic and management techniques in Oculoplasty and Oncology is showcased, and the event is attended by delegates from all over the country. There are special sessions on video based surgical skill transfer, approach to complex orbital and periorbital diseases, ocular pathology and insight into diagnostic and management of selected challenging cases. Recent advances at the centre are highlighted and delegates are given an opportunity for hands-on experience.he aim of the unit is to serve the patients in a compassionate and professional manner providing comprehensive care with a holistic team approach.
The unit 5 also provides strabismus and neuro ophthalmology services. Patients with ocular misalignment, amblyopia, binocular visual problems and neuro-ophthalmic disorders are treated here. The unique protocols for clinical diagnosis, management, and advanced surgical facilities makes it one of the aspired places for strabismus care in India and abroad. In the field of amblyopia, the specialists now offer the novel dichoptic therapies for young children. In paediatric and in adult subjects, the basic as well as complex strabismic disorders are addressed in a systematic manner. The detailed preoperative orthoptic evaluation, centre specific treatment algorithm and the diverse expertise profile tries to provide the novel care here.
Resident training is one of the major programs at our centre. To impart quality diagnostic and surgical skills to budding surgeons, the strabismus section conducts regular wet lab exercises, the common as well as complex case scenarios are simulated in wet lab, and under the direct guidance of an expert the skills are transferred with monitored hands on surgical training. The residents regularly participate in state level and national level conferences to present centres work and innovations in the field of strabismus. Recognizing which many awards and recognitions have been conferred in last few years. To address the existing lacunae in clinical as well as basic research areas, novel surgical techniques, randomised controlled trials and multicentric trials are conducted here. The effect of atropine eye drops in halting myopia progression, signs of vascular anomalies in amblyopic eyes (on optical coherence tomography angiography) and newer surgical techniques to provide better care are currently being explored here. To improve training patterns the animal modules are also being created here. To address surgical limitations, newer surgeries in unusual types of strabismus, modifications in existing technique, and newer concepts are also being explored.
Short CV of NAME : Nishkarsh Gupta
POSITION TITLE : Associate Professor of Onco-anaesthesia & Palliative Medicine
| INSTITUTION AND LOCATION | DEGREE(if applicable) | Completion Date MM/YYYY | FIELD OF STUDY |
|---|---|---|---|
| MAMC, New Delhi, India | M.B.B.S | 12/2000 | Medicine |
| MAMC, New Delhi, India | M.D. | 05/2005 | Anaesthesiology |
| IAPC at AIIMS Dr BRAIRCH, AIIMS | CCEPC IAPC | 05/2013 | Palliative Care |
| Basic Life Support and Advanced Cardiac Life Support Course accredited by American Heart Association, USA. | BLS and ACLS (instructor) | 2008 | Instructor |
| Fellowship in palliative Medicine | NFPM, Kozhikode, India | 2016 | Completed |
| PGCCHM | NIHFW, Munirka, Delhi, | 2011 | Hospital administration |
I have the expertise, leadership, training, and motivation necessary to successfully carry out the proposed research project. I have a broad background in, with specific training and expertise in anesthesiology, cancer pain and palliative care research. As PI or co-Investigator, I have been involved in difficult airway management, perioperative anaesthesia management, cancer pain and palliative care of terminally ill cancer patients. I have been able to recruit and track participants over time as required in these projects. In addition, I successfully administered the projects (e.g. staffing, research protections, budget), collaborated with other researchers, and produced several peer-reviewed publications. I am also aware of the importance of frequent communication among project members and of constructing a realistic research plan, timeline, and budget.
B. Positions and Honors
| Grade of Post | Hospital | Period |
|---|---|---|
| Associate Professor Assistant Professor (Onco-anaesthesia & Palliative Medicine) | DrBRAIRCH, AIIMS, Delhi, India | 1.07.2015-till date 08.06.2012-30.06.2015 |
| Assistant Professor | PGIMER & Dr RML hospital, Delhi | 21-11-2009 to 7.06.2012 |
| Attending consultant | Max, superspeciality Hospital, Saket | 06-06-08 – 20/11/09 |
| Registrar | LNH, Delhi, India | 06-Jun-2005 to 5-06-08 |
| Post graduate | MAMC, Delhi, India | 1-Jul-02 to 30-Apr-05 |
Member, Indian Society of Anesthesiologists (ISA)
Member, Indian Society of Palliative Care
Member, Research Society of Anesthesiology & Clinical Pharmacology
Member, Airway Management Foundation
Member, All India Difficult Airway Association
Member Indian Society of Critical Care Medicine
Member APCC
Member Asian Achieves
ACLS and BLS instructor
PTC Instructor
Airway management skills
Nishkarsh Gupta (PI)
Comparative evaluation of Nasotracheal intubation with Glidescope Videolaryngosocope and conventional Macintosh laryngoscope using cuff inflation technique in patients undergoing head and neck cancer surgeries: A prospective randomized study
Comparative evaluation of forced air warming and infusion of amino Acid enriched solution on intraoperative hypothermia in patients undergoing head and neck cancer surgeries: A prospective randomized study. The study was funded by AIIMS intramural grant. (patient enrollment over, presently analyzing data) as PI
| Type of publication | Published | Under publication | 1st/ communicating author |
|---|---|---|---|
| Papers | 50 | 8 | 30 |
| Book chapters | 2 | 2 | 3 |
| Abstracts | 5 | 0 | 2 |
Cornea, Cataract, Refractive and Glaucoma services
| S.No. | Name | Designation |
|---|---|---|
| 1 | Prof. Namrata Sharma | Professor and Officer-in-Charge namrata[dot]sharma[at]gmail[dot]com |
| 2 | Prof. Tanuj Dada | Professor of Ophthalmology tanujdada[at]gmail[dot]com |
| 3 | Dr Prafulla Kumar Maharana | Associate Professor of Ophthalmology drpraful13[at]gmail[dot]com |
| 4 | Dr Dewang Angmo | Associate Professor of Ophthalmology dewang45[at]gmail[dot]com |
| 5 | Dr.Anu Malik | Asstt. Prof. of Ophth. |
| 6 | Dr. Karthikeyan M. | Asstt. Prof. of Ophth. |
The unit provides comprehensive services for management of pediatric and adult cataract, refractive surgeries, corneal transplantation, medical, laser and surgical management of pediatric and adult glaucoma. Unit runs specialty clinics that include cornea clinic, refractive surgery clinic and glaucoma clinic.
All kinds of adult cataract and pediatric cataract are seen and managed in this unit. The pediatric cataracts include congenital cataract, syndromic cataract, traumatic cataract and other complicated cataracts. Adult cataracts such as senile cataracts and complicated cataract cases, such as those with subluxated and dislocated cataracts are also seen and managed. Modern cataract surgery such as femtosecond laser assisted cataract surgery (FLACS) and Premium intraocular lens surgery such as trifocal, multifocal and toric intraocular lens are routinely done in this unit. Besides this, challenging cases such as aniridic IOL implantation, intralenticular lens aspiration (ILLA), capsular support devices with IOL placement are also done. Secondary intraocular lens placement and glued scleral fixated intraocular lens (SFIOL) surgery are done to rehabilitate aphakic patients.
The unit also runs a state of the art refractive clinic. It deals with all the refractive cases for correction of myopia, hyperopia and astigmatism. All modern refractive surgery such a small incision lenticule extraction (SMILE), femtosecond LASIK are carried out in this unit. Other refractive procedures such as implantable collamer lens (ICL) surgery, implantable phakic contact lens (IPCL) surgery, photorefractive keratectomy (PRK) and intrastromal corneal ring segments (ICRS) are also performed in this unit.
The aim of cornea clinic is to evaluate patients with corneal problems and plan their appropriate management. Patients of microbial keratitis including bacterial, fungal and viral keratitis are evaluated and managed. Other corneal conditions such as corneal dystrophy, corneal decompensation, corneal opacity and keratoconus are evaluated in the cornea clinic. Various corneal procedure such as corneal collagen cross linking with Riboflavin(C3R), penetrating keratoplasty are performed in this unit. Anterior lamellar procedure such anterior lamellar therapeutic keratoplasty (ALTK), superficial anterior lamellar keratoplasty (SALK) and deep anterior lamellar keratoplasty (DALK) and endothelial keratoplasty procedure such as Descemet stripping automated endothelial keratoplasty (DSAEK), and Descemet membrane endothelial keratoplasty (DMEK) are also performed. Recently we have started corneal transplantation using biosynthetic cornea. Amniotic membrane transplantation (AMT), mucous membrane transplantation (MMT), cultivated limbal epithelial transplant (CLET), simple limbal epithelial transplant (SLET), minor salivary gland transplantation (MSGT), keratoprosthesis (KPRO) are also performed for various ocular surface disorders.
The aim of the glaucoma clinic is to evaluate patients with raised IOP with optic neuropathy and plan their appropriate management. We have a glaucoma laboratory for high end research and clinical purposes. Glaucoma laboratory is equipped with Casia AS-OCT, Spectralis OCT for RNFL and GCC, HRT, UBM and tonometers like Tonopen, I Care and Perkins for IOP measurements in patients with scarred cornea, pediatric and uncooperative patients. High volume of patients allow us to undertake long term outcome studies on standard techniques and different surgical modifications which enhances our knowledge and understanding of the disease in general.
We provide laser treatments like Laser Peripheral Iridotomy, Selective Laser Trabeculoplasty for early Glaucoma, Trans-scleral DLCP, Micropulse laser therapy for refractory glaucoma. Surgical cases include pediatric glaucoma and adult glaucoma with uncontrolled IOP. Pediatric glaucoma managed with Goniotomy, Trabeculotomy, Trabeculotomy with trabeculectomy with Mitomycin C. Adult glaucoma managed with Phacoemulsification with ICG guided BANG (Bent Ab interno Needle Goniectomy), Phacoemulsification with ECP (EndoCyclo Photocoagulation), Trabeculectomy with Mitomycin C, Trabeculectomy with deep sclerectomy, Glaucoma Drainage Devices.

Ashok Sharma, Ph.D
Additional Professor
DBT-Ramalingaswami Fellow, DST-Ramanujan Fellowship Awardee
Room No-3029, Department of Biochemistry,
Posted: National Cancer Institute/AIIMS
Jhajjar Campus, Haryana, Bharat (India)
Phone: +91-(11)-2659-3545(off.); 09818665092 (M)
Email : ashok[dot]sharma[at]aiims[dot]edu
http://scholar.google.com/citations?user=3ac275cAAAAJ&hl=en
https://www.researchgate.net/profile/Ashok_Sharma12/
Dr. Sharma is an Additional Professor in the Department of Biochemistry and Posted in NCI-India/AIIMS Jhajjar Campus, AIIMS, New Delhi.He received Ph.D. in Cancer Biology at the Department of Biochemistry at All India Institute of Medical Sciences (AIIMS), New Delhi, in 2009. He is the recipient of multiple awards, including the prestigious “DBT-Ramalingaswami fellowship” and “DST-Ramanujan fellowship” awards from Govt. of India and “Outstanding Immunologist Award”, Immunocon, Indian Immunologist Society, BHU.
In 2009, he joined the Vanderbilt Medical Center, Vanderbilt University, Nashville, TN USA as a postdoctoral fellow. He worked on tight junction proteins (claudins) and their role in regulating cell migration and epithelial-mesenchymal transition (EMT). In 2012, he joined the group of Adam R Karpf at Eppley Institute, UNMC, as a senior postdoc. He is working on the epigenetics & regulation of Cancer-Testis/germline antigen POTE and its biomarkers/therapeutic potential. He has published multiple research articles and abstracts in national and international journals. He is actively involved in ePG-Pathshala, an MHRD, National Mission on Education through ICT (NME-ICT) venture to develop e-content at the postgraduate level that will help to improve the education system in India. Dr. Sharma has been the principal investigator and co-investigator in multiple projects for gynecological cancer. Dr. Sharma has been actively involved in establishing the “DBT-AIIMS/NCI-India Translational & Clinical Research Partnership Center” as PI with the help of DBT, GOI, and Early Detection Research Network (EDRN) at NCI-India with collaboration with EDRN-NCI-USA.
Assertive discoveries have been carried out during the past decade to explore the role of epigenetic mechanisms in regulating cellular phenotype. This regulation provides the software that packages DNA, and modifications in gene expression without changing the DNA sequence of a gene. These are called epigenetic alterations. These alterations include methylation, acetylation, phosphorylation, and ubiquitylation of DNA and histone proteins (nucleosomes) as well as chromatin remodeling. "Epigenetics" refers to heritable changes in gene expression patterns without changing the primary DNA sequence. Technological advancements in genome-wide DNA sequencing, RNA sequencing for coding and non-coding expression patterns, DNA methylation and chromatin assay and assessment of all of the above with advanced bioinformatics tools are facilitating to delineate the cancer epigenome and permit key insights for developing personalized therapeutics. Our lab focuses on cancer epigenetics and is trying to decipher the epigenome regulation that may lead to the development of new epigenetic therapeutic drugs. The recent discovery of Cancer Testis/Germline (CT/CG) antigen expression in cancer suggests a strong link between gametogenesis and carcinogenesis.CG antigens can serve as biomarkers for cancer stem cells and potential targets in cancer metastatic processes as well as in the recurrence of cancer after chemotherapy. We are indulging in opening new avenues for novel Cancer Testis/Germline (CT/CG) POTE antigens to be used for cancer immunotherapy for treating gynecological cancer patients for better reproductive health. POTE (Prostate, Placenta, Ovary, and Testis-expressed) is a recently discovered gene family consisting of 14 autosomal and pericentromeric localized cancer-testis/germline antigen genes. The POTE paralogs gene family encodes proteins with cysteine-rich (CRR) domains, ankyrin repeat motifs, and α-helical regions. It is established that epigenetic mechanisms control the expression of CT/CG antigens. Epigenetic modulatory agents robustly promote the expression of CG antigens and the class-1 histocompatibility complex (MHCI).Thus, we emphasize the possible clinical use of epigenetic modulators to augment the immunotherapeutic potential of POTE family antigens and how this will ultimately improve cancer detection and treatment strategies.
Towards the mechanistic part, we are working on chromatin dynamics to be applied for answering key questions of alteration in pericentromeric localized gene expression during cancer. POTEs gene families are localized in pericentromeric regions, where duplicated genes are often abundant. Still, it is unclear how POTE paralogs escape pericentromeric repression and become expressed in cancer. Chromatin has a defined 3-D organization inside the nucleus, which guides gene expression. Although this 3D Genome organization is just recently being defined to the molecular levels, there is much to be answered in this area. Our lab is working to correlate the established molecular mechanisms for gene regulation e.g DNA methylation to be linked to the 3D genome organization inside the nucleus. It is known that there are several repressive compartments inside the nucleus where genes are dynamically located as a whole. Therefore what is the relation of epigenetic gene regulation to the gene localization and arrangement inside the nucleus? This is an inevitable question here. One such repressive compartment is nuclear lamina, where the associated sequences, called "Lamina-associated domains (LADs)" and "pericentromeric-associated domains (PADs)" are dynamically placed. We are trying to find factors responsible for these LADs /PADs formation and regulation to be applied for cancer biology. Altogether this is an entirely new area in the field of cancer biology, and studies are coming up with new fascinating facts; we are trying to be part of these strategies, with an ultimate goal to combat cancer. For further details, please visit "Laboratory of Chromatin and Cancer Epigenetics", the URL of which is at my researchgate profile.
| July 2021- Present Aug. 2020-June, 2021 | : Additional Professor- Department of Biochemistry, National Cancer Institute, Jhajjar Campus, Haryana : Associate Professor- Posted at National Cancer Institute, Jhajjar Campus, Haryana |
| July 2018- June, 2021 | : Associate Professor- Department of Biochemistry |
| Dec. 2015- Aug 2020 | : Faculty In-Charge, Biochemistry Diagnostic lab |
| Jun 2015 - Jun 2018 | : Assistant Professor- Department of Biochemistry |
| April 2015- Jun 2015 | : DBT-Ramalingaswami Fellow- Dept. of Obstetrics & Gynaecology |
| Oct.2012-March 2015 | : Postdoctoral Research Associate - Eppley Institute for Research in Cancer, UNMC, Omaha, Nebraska, USA Project focus: Mechanisms of DNA hypomethylation in ovarian cancer and evaluating its contribution to tumour progression and potential as a biomarker for the disease. ⮚ Understand the role of DNA methylation changes in cancer, with a current emphasis on epithelial ovarian cancer (EOC) ⮚ Understand the role of Lamina Associated Domain (LADs) in genomic instability ⮚ Define the mechanisms leading to activation of Cancer-Germline POTE genes in cancer ⮚ Mechanisms under the current study include DNA methylation, histone modifications, nucleosome positioning, and the interaction of epigenetic factors with transcription factor-driven oncogenic signalling mechanisms. |
| Jan. 2009-Oct. 2012 | : VUMC Research Fellow - Department of Surgical Oncology, Vanderbilt University, Nashville, TN, USA Research focuses on "Elaborate the mechanism underlying the role of claudin 1 as a tumour promoter and metastasis in Colon cancer". ⮚ Epigenetic regulation of claudin 1 expression and role of ELAV family proteins in modulation of mRNA stability. ⮚ Explore the signalling and molecular mechanisms using anoikis as the study model, potentially applying to the in-vivo model of colon cancer metastasis and invasion. ⮚ Determine the role of APC and NOTCH signalling pathway in DSS/AOM induced IBD and cancer in claudin-1 overexpressed transgenic mice ⮚ Elaborating the mechanisms underlying using the different PKC and PKA inhibitors on the novel nuclear localization of claudin-1 in colon metastasis. |
| Jun.2005–Jan. 2009 | Senior Research Fellow: Project:Effect of Bleomycin on the Expression of High Mobility Group Proteins in Benzo(a)pyrene Induced Skin Tumour "awarded & funded by Indian Council of Medical Research (ICMR- PHA/BMS/2006). |
| Aug. 2003-May, 2005 | Junior Research Fellow: Project: Studies on Expression of HMGA Chromosomal Proteins In Cancer and Their Interaction with DNA ". Project funded by Department of Science & Technology (DST) (SP/SO/AS-55/2002), India |
| Aug. 2002-July 2003 | Research Assistant: Project: Preferential Binding of Quinolones to DNA with Alternating G, C/A, T Sequences: A Spectroscopic Study" funded by Indian Council of Medical Research (ICMR- 58/4/97-BMS-II). |
The University of Melbourne, Australia, Jun 2014
Advanced Certificate courses in “Epigenetic Control of Gene Expression."
This course addresses the basic principles of epigenetics, the role of epigenetics in biological phenomena such as imprinting, X-inactivation, cellular identity, cellular reprogramming in several organisms, and a focus on mammals. It also deciphers the interplay between epigenetic control and the environment, the role of aberrant epigenetic mechanisms in human diseases, and finally, the development of epigenetically effective drugs. The program's objective is to provide a solid foundation of information, enabling participants to design experiments when returning to their own research lab.
All India Institute of Medical Sciences (AIIMS), New Delhi, India
Ph.D. Department of Biochemistry, September 2008.
Thesis: Effect of Anticancer Agents on the Expression of High Mobility Group (HMG) Proteins in Skin Cancer”
Examined the mechanism of various anticancer agents like cisplatin, doxorubicin, Bleomycin through the expression of DNA binding high mobility group (HMGs) proteins in benzo(a)pyrene-induced squamous cell carcinoma of the skin.
I used various molecular and biochemical techniques, both In-vitro and In-vivo models, and basic microbiological and biochemical techniques and data corroborate with Magnetic Resonance Imaging in an animal model.
Results help in elucidation of the molecular mechanisms that mediate cisplatin. Doxorubicin resistance holds promise for the design of pharmacological strategies for preventing, overcoming, or reversing this form of drug resistance.
Maharshi Dayanand University, Rohtak, HR, India
Master of Science (M.Sc.) Specialization: Biochemistry, September 2001.
Dissertation: Effect of NaCl Salinity on Oxalate Metabolism in Shoot of Barley during Early Phase of Growth “. Results published in 'India Journal.'
Pt. B.D.S Post Graduate Institute of Medical Sciences, Rohtak, HR, India
Key Publications (Selected):
(http://scholar.google.com/citations?hl=en&user=3ac275cAAAAJ
Highly motivated and interested fellows and students are encouraged to inquire regarding the availability of research positions. We are seeking applications from motivated, goal-oriented individuals with excellent academic backgrounds and having their ownCSIR/DBT/ICMR/BINC/DST fellowships.Candidates with experience in Molecular Biology/Bioinformatics or other multidisciplinary are encouraged to contact and send their CV along with a cover letter at ashok[dot]sharma[at]aiims[dot]edu
Cornea, Cataract Refractive Surgery Services
| S.No. | Name | Designation |
|---|---|---|
| 1 | Prof. Jeewan S. Titiyal | Professor and Unit Head titiyal[at]gmail[dot]com |
| 2 | Prof. Tushar Agarwal | Professor of Ophthalmology drtushar[at]gmail[dot]com |
| 3 | Prof. Rajesh Sinha | Professor of Ophthalmology sinharaj1[at]gmail[dot]com |
| 4 | Dr. Manpreet Kaur | Assistant Professor of Ophthalmology manpreet[dot]aiims[at]gmail[dot]com |
| 5 | Dr. Sridevi Nair | Assistant Professor of Ophthalmology srideviaiims[at]gmail[dot]com |
The unit provides state of the art services in the field of cornea, cataract, and refractive surgery to patients from all over the country. A comprehensive resident training programme that comprises academic lectures, bed-side teaching, and stepwise surgical training is undertaken. Clinical research is given major importance and innovative techniques are constantly being developed to improve the clinical care of patients.
The unit offers various advanced, cutting-edge surgical techniques to treat cataract, corneal pathologies, and refractive errors at a minimal cost. High precision, bladeless femtosecond laser assisted cataract surgery (FLACS) that uses laser to perform steps such as incision creation, capsulotomy, and nuclear fragmentation is also available. FLACS is particularly useful in challenging case scenarios such as white cataract where it helps create a circular, adequately sized capsulotomy, or advanced posterior polar cataract where the hybrid pattern of nucleotomy enhances surgical safety. The use of three-dimensional heads-up display microscopes (ARTEVO 800) is a novel addition to the cataract surgical armamentarium. It provides greater magnification and enhanced visibility of the surgical field as compared with the conventional binocular operating microscopes, thus facilitating better surgical outcomes. It is also a valuable tool in the pandemic era for teaching and demonstration of surgical techniques to trainee residents while adhering to social distancing norms.
The latest premium intraocular lenses are routinely being implanted, such as multifocal intraocular lens (IOL) and toric IOLs. Toric IOLs not only help in management of cases with high astigmatism but are also customized for specific cases such as corneal ectasia. Multifocal IOLs are also routinely implanted to cater to the needs of patients who wish to be spectacle free post-surgery.
The unit also provides highly specialised care to paediatric patients with cataract. Special emphasis is placed on timely surgical interventional and regular follow-up with proper amblyopia management to optimise visual outcomes.
The unit has a dedicated contact lens clinic conducted once a week, which caters to optical and cosmetic rehabilitation of a variety of cases, including corneal ectasia with irregular astigmatism, aphakia, corneal opacity and post-keratoplasty astigmatism. In cases of progressive corneal ectasia, corneal collagen crosslinking is done as a minimally invasive procedure to halt disease progression. Various customizations are available to cater to the individual needs of the patient like lenticule-assisted crosslinking and contact lens assisted crosslinking. Newer techniques like oxygen-assisted crosslinking are being evaluated to improve the efficacy of the procedure. Limbal stem cell transplantation is also done for management of limbal stem cell deficiency and ocular surface rehabilitation.
The residents are provided training in eye banking as well as performing keratoplasties. Newer specular microscopes available in the National Eye Bank aid in better assessment of the donor corneas. Hundreds of corneal transplantation surgeries are performed each year under the unit. Optical keratoplasties are done to provide sight to those who are disabled due to corneal opacities, while therapeutic keratoplasties are performed to debulk the infective load in patients presenting with recalcitrant corneal infections. Lamellar keratoplasty that involves the selective replacement of the diseased corneal tissue is also routinely performed. The newer automated microkeratomes have facilitated the creation of donor lenticules with increased precision, for use in both anterior lamellar and endothelial keratoplasties. The use of advanced microscopes with integrated optical coherence tomography (OCT) that allow in-vivo visualisation of donor and host cornea have enhanced the safety and precision of lamellar keratoplasty. Femtosecond laser is also being used for donor as well as host corneal tissue preparation during keratoplasty.
paediatric patients with cataract. Special emphasis is placed on timely surgical interventional and regular follow-up with proper amblyopia management to optimise visual outcomes.
The most advanced technology is used in refractive surgeries, with patients being offered all types of procedures including laser assisted in situ keratomileusis (LASIK), photorefractive keratectomy (PRK) and small incision lenticule extraction (SMILE). Customized corneal laser refractive procedures that tailor the treatment based on the corneal topography or ocular wavefront profile are also offered to the patients. Different types of phakic IOLs are available to meet the need of the patients of all age groups, including Implantable Collamer Lens (ICL), Refractive Implantable Lens (RIL) and presbyopic phakic IOL.
The unit faculty members and senior residents have been enthusiastically involved in all the academic activities, teaching programmes, surgical skill training classes, research work and purpose-driven initiatives.
Vitreoretina, Glaucoma, Uvea & ROP
| S.No. | Name | Designation |
|---|---|---|
| 1 | Prof. Rajpal | Professor & Officer-In-Charge |
| 2 | Prof. Viney Gupta | Professor of Ophthalmology |
| 3 | Prof. Parijat Chandra | Professor of Ophthalmology |
| 4 | Dr. Rohan Chawla | Additional Professor of Ophthalmology |
| 5 | Dr. Vinod Kumar | Additional Professor of Ophthalmology |
| 6 | Dr. Shikha Gupta | Associate Professor of Ophthalmology |
The unit provides services for effective diagnosis, treatment and also research in Vitreoretinal diseases, Glaucoma, Uvea and Retinopathy of Prematurity (ROP)
The unit has contributed considerably in the field of vitreoretinal diseases, especially diabetic retinopathy, vein occlusions, central serous retinopathy, age related macular degeneration, ROP, trauma etc. With a huge range of latest investigative and treatment tools like microperimetry, wide-field digital fundus angiography, Spectralis OCT, OCT Angiography, video angiography, high resolution ocular coherence tomography, lasers, photodynamic therapy, PASCAL laser, MFERG etc, the unit continues to provide excellent ophthalmic care to patients.
The unit is engaged in cutting edge modern vitreoretinal surgery with the use of wide angle viewing systems, 23G/25G/27G small gauge sutureless vitrectomy, modern surgical microscopes and other advanced vitreoretinal surgery equipment that have revolutionised surgery techniques and have outcomes comparable to best in the world. We operate on complex retinal detachments, tractional retinal detachments, giant retinal tears and macular disorders with high quality surgery and excellent outcomes.
The unit is an apex referral center for screening, laser treatment and surgery of retinopathy of prematurity (ROP), an important cause of childhood blindness in premature babies. We now have a dedicated Paediatric high dependency unit (HDU) manned by SR Paediatrics to provide pre and post operative support.
Active research is ongoing on stem cells for use in retinal degenerative diseases and macular hole surgery. The unit also actively engages in collaborating with ocular pharmacology and ocular biochemistry to study various retinal diseases in animal models.
The glaucoma faculty and senior residents cater to Adult and Paediatric glaucoma cases. Their research encompasses novel surgical techniques, Imaging in glaucoma to Glaucoma genetics. Apart from conventional trabeculectomy and glaucoma drainage devices , the unit offers modern surgical procedures like angle surgeries namely goniotomy, BANG (bent ab interno needle goniectomy) and GATT(Gonioscopy assisted transluminal trabeculotomy). Laser procedures like YAG iridotomy, iridoplasty, Selective laser trabeculoplasty, Endocyclophotocoagulation, Diode laser cyclophotocoagulation, Micropulse are done routinely.
They have published new surgical techniques in managing complex cases of Malignant glaucoma.The unit faculty and senior residents are devoted to good long term patient care. The faculty have published their 2 decades of experience in managing children with Congenital glaucomas.
Dr. Kokkula Praneeth
M.B.B.S, M.S., M.Ch., Vascular Neurosurgery Fellow
Consultant and Assistant Professor, Neurosurgery
All India Institute of Medical Sciences and Jai Prakash Narain Apex Trauma Center
New Delhi, India; Phone: 91-11-26593291; Email: praneethkokkula[at]aiims[dot]edu
Brief Profile
Dr. Kokkula Praneethis an undergraduate from Osmania Medical College and joined as Junior Resident in Department of Surgical Disciplines at AIIMS, New Delhi in 2012. Later he did his M.Ch. Neurosurgery from PGIMER, Chandigarh in 2018, he continued as Post-Doctoral Fellow in Vascular Neurosurgery at PGIMER till 2019. For 3 months duration he worked as Assistant Professor, Neurosurgery at Jodhpur. In October 2019, he joined Department of Neurosurgery, AIIMS New Delhi as an Assistant Professor. He had an excellent academic and surgical record throughout his residency training, with several publications in both national and international journals. He is well versed in all aspects of neurosurgery with special interest in Neurotrauma, Skull Base, Cerebrovascular Neurosurgery, Neurooncology and Gamma Knife Radiosurgery, and is currently working on many national and international research projects.
Areas of interest and expertise
Academic record
| College/University | Duration | |
|---|---|---|
| M.B.B.S. | Osmania Medical College | Aug 2006 - Apr 2011 |
| Internship | Osmania Medical College | Apr 2011 – Apr 2012 |
| M.S. (Surgery) | AIIMS, New Delhi | July 2012 – June 2015 |
| M.Ch. (Neurosurgery) | PGIMER, Chandigarh | July 2015 - June 2018 |
| Post-Doctoral Fellowship - Vascular Neurosurgery (1 year) | PGIMER, Chandigarh | July 2018 - June 2019 |
Work Experience Post M.Ch.
| Post-Doctoral Fellowship - Vascular Neurosurgery | PGIMER, Chandigarh July 2018 – June 2019 | 1 year |
| Assistant Professor (Neurosurgery) | AIIMS, Jodhpur July 2019 – Oct 2019 | 3 months |
Assistant Professor (Neurosurgery) | AIIMS, New Delhi Oct 2019 – till date | 3yrs 1months (till date) |
Awards and Achievements
Professional Memberships –
Clinics and inpatient services:
Trauma OPD: Tuesday, 14.00-17.00 hrs, Room number 104, First Floor, JPNATC
TC3 ICU, TC3A ICU, TC5 - JPNATC
Trauma OT4, 5 - JPNATC
Research and Publications
Chapters in books
Funded projects
| S. No. | Title of the project | Role | Funded by (Name of funding agency) | Duration (years) | Start year- End year |
|---|---|---|---|---|---|
| 1 | Role of Biomarkers in Predicting Evolution of Cerebral Edema following Traumatic Brain Injury | Principal Investigator | AIIMS | 2 yrs | 2020-2022 |
| 2 | Evaluation of Cathepsin B in peripheral blood of Isolated Traumatic Brain Injury patients and its correlation. | Co-Investigator | ICMR | 3yrs | 2020-2023 |
Cataract, Refractive surgery, Vitreoretina, Uvea, Squint and Neuro-ophthalmology
| S.No. | Unit-I |
|---|---|
| 1 | Dr. S.K. Khokhar, Prof. of Ophth. |
| 2 | Dr. Pradeep Venkatesh, Prof. of Ophth |
| 3 | Dr. Shorya Vardhan Azad, Assoc. Prof. of Ophth |
| 4 | Dr. Amar Pujari, Asstt. Prof. of Ophth |
| 5 | Dr. Saurabh Verma Asstt. Prof of Ophth |
| 6 | Dr. Devesh Kumawat, Asstt. Prof. Ophth |
The unit provides comprehensive services for management of paediatric and adult cataracts, refractive errors (surgical management) vitreo-retinal disorders, strabismus and neuro-ophthalmic disorders. The unit runs many specialty clinics such as Lens clinic, Retina clinic, Uveitis clinic, Squint Clinic and Neuro-ophthalmology Clinic.
All kinds of paediatric cataract cases are seen and managed in the lens clinic. These include bilateral congenital cataracts, syndromic cataracts, metabolic, complicated and unilateral cataracts. Long term post operative care including needed refractive correction and amblyopia treatment is also provided. Complicated adult cataract cases, such as those with subluxated cataracts are also seen and managed. The lens clinic is run on every Thursday at 2pm for all lens cases dealing with both pediatric and complicated adult cataracts.
The unit also carries out state-of-the-art refractive procedures. It deals with all the refractive cases for correction of myopia, hyperopia and astigmatism. All modern cataract and refractive surgeries using the latest lasers like femtosecond LASIK, femtosecond laser-assisted cataract surgery (FLACS) and small incision lenticule extraction (SMILE) are carried out at very nominal cost. Other refractive procedures such as ICL surgery, Photorefractive keratectomy (PRK), and intrastromal corneal ring segments (ICRS) are also performed as indicated.
The aim of the Retina clinic is to evaluate patients with medical and surgical retinal problems and plan their appropriate management. Certain key areas of specialization in medical retina are management of Diabetic Retinopathy, Age Related Macular Degeneration, Vascular Occlusions and Retinal Degenerations and Dystrophies. Surgical retina cases such as those with simple or complex retinal detachments, macular hole, intraocular foreign body and endophthalmitis etc are managed with most modern micro-incision vitreo-retinal surgical platforms. The surgeons of the unit are adept at managing all these complex cases using the latest microsurgical techniques and lasers. Laser treatment of various disorders and Anti-VEGF injections are also carried out in this unit. The retina clinic runs on two days i.e., Thursday and Friday from 2pm that caters to various new and old follow up cases related to retina.
The Uvea clinic deals with cases of intraocular inflammation. These could be of infective or autoimmune aetiology. Long term treatment strategies for these chronic disorders are worked out with the help of state-of-the-art ophthalmic diagnostic equipment. The uvea clinic runs on Monday from 2pm.
Simple and complex squint surgeries including inferior oblique, superior oblique surgeries and surgeries for nerve palsies are carried out in this unit. The squint clinic runs every Wednesday from 2 pm where various ocular motility disorders are diagnosed and advised for proper management. The unit also has a dedicated Neuro-ophthalmology clinic where referrals from different units and also other departments are evaluated, and appropriate management strategies implemented.
Quality post graduate education, training and research are our other focus areas. Regular assessments, academic exercises and group teaching exercises including ward rounds are carried out regularly for proper education and training of the residents.

Left to right: Dr.Shaikh Abdul Mubeen, Deepak Vats, Diravyaseelan M, Hema Yadav,Archana Singh, Dr. Sudhasini Panda, Alisha Arora, Faisal Shah
Dr. Archana Singh
Additional Professor
Address: Room no. 3022, Dept. of Biochemistry, III floor, Teaching Block, AIIMS, Ansari Nagar, Delhi
Official Phone: 011-26593467
Email id: archanasinghmamc[at]gmail[dot]com, archanasinghaiims[at]gmail[dot]com
| Degree | Subject | University/ Institution | Year |
|---|---|---|---|
| M.B.B.S. | Bachelor of Medicine and Surgery | Maulana Azad Medical College, Delhi University | 1998-2003 |
| M.D. | Biochemistry | Lady Hardinge Medical College, Delhi University | 2005-2008 |
| Position | Department | University/ Institution | Dates |
|---|---|---|---|
| Senior Resident | Biochemistry | Lady Hardinge Medical College | 27 May 2008 - 30 Dec 2009 |
| Assistant Professor | Biochemistry | University College of Medical Sciences | 31 Dec 2009 - 13 June 2014 |
| Assistant Professor | Biochemistry | All India Institute of Medical Sciences | 14 June 2014 – 30 June 2017 |
| Associate Professor | Biochemistry | All India Institute of Medical Sciences | 1 July 2017 – 30 June 2020 |
| Additional Professor | Biochemistry | All India Institute of Medical Sciences | 1 July 2020- till date |
Life member of the Association of the Medical Biochemist of India (AMBI), Association of the Clinical Biochemists of India (ACBI), Indian Society for Atherosclerosis Research (ISAR), Indian Immunology Society
We have worked on the genetics and immunology of pre-eclampsia and intra uterine growth restriction. We are developing new treatment modalities with respect to nitric oxide. We have published about seven original studies so far on this aspect. Her work on various aspect of complicated pregnancy has won three awards as mentioned above.
We are elucidating the biochemical, genetic and immunological host factors of tuberculosis in understanding disease pathophysiology and development of diagnostic biomarkers for identification of latent TB among household contacts. For the last seven years, we have been actively working on understanding the host factors like vitamin D, nitric oxide and iron regulatory proteins that could influence the pathophysiology of pulmonary tuberculosis (TB) with respect to the latency of infection by studying closed household contacts of TB patients. We have completed one SERB funded project “Study of vitamin D receptor (VDR) and cathelicidin expression and their correlation with Fok1 VDR polymorphism in Tuberculosis” and established a cohort of 200 pulmonary TB patients and their household contacts studying these host factors which was published as three independent research articles (Scientific Reports 2019, J Steroid Biochem Mol Biol 2019 and Ind J Clin Biochem 2021).
We are also working on the adaptive immune responses and the genetic correlates in the household contacts of active pulmonary TB patients. It would be interesting to understand why some of the household contacts do not develop tuberculosis and what are the immunological basis for the same. Thus, the findings will add bulk to the global scientific library of tuberculosis regarding the same.
We are also interested in understanding why diabetic individuals are more prone to develop tuberculosis and are studying the role of macrophage effector function in hyperglycemia to understand the same. The article regarding this work has got recently accepted for publication in the European Journal of Immunology.
We are exploring various adjunct therapies for tuberculosis treatment.
Tuberculosis
Involved as co-Investigator and Co-guide in other interdepartmental Extramural and Intramural projects and DM/Mch/PhD/MD/MS/MSc/MBBS thesis and research work.

Current Affiliation: Postdoctoral fellow, La Jolla Institute for Immunology, San Diego, California
3, Dr. Diravyaseelan M (M.D)

Current Affiliation: Senior Resident, Department of Biochemistry, AIIMS, Delhi
4 Mr. Faisal Shah (MSc)

Current Affiliation: PhD Scholar, Friedrich-Loeffler-Institute, University of Griefswald, Griefswald, Germany
5 Ms. Hema Yadav (MSc)

Current Affiliation: PhD Scholar, Department of Biochemistry, AIIMS, Delhi
Interested in taking JRF/research trainees/ MBBS summer fellows as and when funds are available
* Communicating Author
Patient Care: Presently In - charge of clinical chemistry laboratory, Department of Biochemistry, All India Institute of Medical Sciences, Delhi. Is also in charge for porphyria testing in the department.
Students presently working in Laboratory

Alisha completed her B.Sc.(H) in Zoology from Daulat Ram College, University of Delhi in 2017. She has completed her M.Sc. in Zoology from Hansraj College, University of Delhi in 2019. She qualified CSIR-UGC-JRF in 2017. Currently she is a third year PhD student under the guidance of Dr. Archana Singh. She is working on “Influence of different grades of hyperglycemia on innate immune responses in pathophysiology of active tuberculosis
2. Mr. Deepak Vats (PhD student)

Deepak completed his B.Sc. (H) in Zoology from Panjab University in 2017. He did his M.Sc. in Zoology from CCS Haryana Agricultural University in 2019. He qualified CSIR-NET-JRF in December 2020. Currently he is a second year PhD student under the guidance of Dr. Archana Singh. His PhD thesis is on “Study of immune response in TST (Tuberculin Skin Test) and IGRA (Interferon Gamma Release Assay) negative household contacts compared to latent TB infected household contacts of adult pulmonary tuberculosis patients
3. Ms. Vidushi Sharma (MSc student)

Vidushi completed her B.Sc.(H) in Biochemistry from Sri Venkateswara College, University of Delhi in 2021. She is the Delhi University Gold Medalist in the year 2021 for securing the highest marks in the B.Sc. (H) Biochemistry examinations. She had secured an All India Rank 1 in both AIIMS Biochemistry and Biotechnology entrance exams. She qualified GATE 2022 in both Biotechnology and Life Science. She is a first year M.Sc student and under the supervision of Dr. Archana Singh, she is working on her thesis titled “Study of Bdellovibrio bacteriovorus as a live antibiotic against Mycobacterium tuberculosis.”
4. Dr. Shaikh Abdul Mubeen (Junior Resident)

Dr. Mubeen did his MBBS from Government Medical College and Hospital, Aurangabad. Currently he is the first year M.D. student under the guidance of Dr. Archana Singh. His thesis is focused on the “Study of Immunophenotypes of monocyte subsets in TST and IGRA negative household contacts of adult pulmonary Tuberculosis Patients.”
MD, DNB, FICA, FIMSA, MNAMS, PGCCHM, CCEPC,
Fellowship in Palliative Medicine
Fellowship in Clinical Research Methodology & Evidence-Based Medicine
Mobile: 9810394950
Email: drrgarg[at]hotmail[dot]com
Twitter: @DrRakeshGarg8
Additional Professor,
Anesthesiology, Critical Care, Pain and Palliative Medicine, DR BRAIRCH,
All India Institute of Medical Sciences, New Delhi, India.
MBBS:University College of Medical Sciences.
MD (Anesthesiology):Maulana Azad Medical College.
Senior Residency:All India Institute of Medical Sciences (AIIMS), New Delhi
Total of 250 publications (International and National).
Authored 25 chapters in Books.
Editor of 2 books.
Onco-Anaesthesiology, Acute and Chronic Pain, Airway, Resuscitation, Research
Editors: Pubmed Indexed Journals
Editorial Board member of 12 International and National journals.
Journals reviewer: Reviewed over 1000 manuscript for International, and National Journals
Substance use has been Major challenge faced by health professionals and policymakers all across the world. The pattern of drug use varies from time to time depending on the availability of new illicit drugs. And increased witness of newer psychoactive substances. Called new psychoactive substances (NPS). Or in the form of preparations, that are not controlled under the Single Convention on Narcotic Drugs of 1961 or the convention on psychotropic Substances of 1971, but that may pose a threat of public health.
A total of 1127 such substances have been identified by the national authorities and forensic laboratories from 134 countries.
In the above background, the present study was planned by the National Drug Dependence treatment center (NDDTC) at the All India Institute of Medical Science (AIIMS), New Delhi, with objective to assess the extent and pattern of NPS use among treatment- seeking substance users and to develop and establish urine testing procedure for “New Psychoactive Substances” among treatment- seeking substance users. The study was supported by the department of Revenue, Ministry of Finance, and Government of India.
This report is the first attempt in establishing objective evidence of the occurrence of NPS among treatment seekers in India. It is important to highlight that the current study began in 2017, and some of the compounds detected in patients’ urine samples were later placed under international control. A novel finding of this study is that some of the identified substances are currently not under international control.
This report addresses a mixed group of readers such as medicinal chemists, forensic scientists, toxicologists, clinicians, healthcare professional, law enforcement agencies, and policymakers. It is hoped that findings and recommendations form this report to ne informative and meaningful in addressing the challenges posed by newer psychoactive drug in the country. We recommend that future research and policy interventions should be geared toward addressing this emerging problem of the NPS.
Coordinating Centre
National Drug Dependence Treatment Centre, All India Institute of Medical Sciences, New Delhi
Participating Centers
Government Medical College, Amritsar, Punjab
Regional Institute of Medical Sciences, Imphal, Manipur
All India Institute of Medical Sciences, Bhubaneswar, Orissa
All India Institute of Medical Sciences, Rishikesh, Uttarakhand
Research Staff
Arun Kumar
Substance use has been Major challenge faced by health professionals and policymakers all across the world. The pattern of drug use varies from time to time depending on the availability of new illicit drugs. And increased witness of newer psychoactive substances. Called new psychoactive substances (NPS). Or in the form of preparations, that are not controlled under the Single Convention on Narcotic Drugs of 1961 or the convention on psychotropic Substances of 1971, but that may pose a threat of public health.
A total of 1127 such substances have been identified by the national authorities and forensic laboratories from 134 countries.
In the above background, the present study was planned by the National Drug Dependence treatment center (NDDTC) at the All India Institute of Medical Science (AIIMS), New Delhi, with objective to assess the extent and pattern of NPS use among treatment- seeking substance users and to develop and establish urine testing procedure for “New Psychoactive Substances” among treatment- seeking substance users. The study was supported by the department of Revenue, Ministry of Finance, and Government of India.
This report is the first attempt in establishing objective evidence of the occurrence of NPS among treatment seekers in India. It is important to highlight that the current study began in 2017, and some of the compounds detected in patients’ urine samples were later placed under international control. A novel finding of this study is that some of the identified substances are currently not under international control.
This report addresses a mixed group of readers such as medicinal chemists, forensic scientists, toxicologists, clinicians, healthcare professional, law enforcement agencies, and policymakers. It is hoped that findings and recommendations form this report to ne informative and meaningful in addressing the challenges posed by newer psychoactive drug in the country. We recommend that future research and policy interventions should be geared toward addressing this emerging problem of the NPS.
DR. SUSHMA BHATNAGAR
Professor & Head Department of Onco-Ansesthesia,Pain and Palliative care
Editor, Indian Journal of Palliative Care
Room No-242, 2nd Floor
Institute Rotary Cancer Hospital
All India Institute of Medical Sciences
New Delhi 110029, India
Tel 091-11- 26565457, Mobile9811326453, Telefax 91-11-26588227
E-mail shumob[at]yahoo[dot]com ,sushmabhatnagar1[at]gmail[dot]com
| DATE | DESIGNATION | INSTITUTE |
|---|---|---|
| 2011-till date | Professor and Head | Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi |
| 2007-2011 | Additional Professor | Institute Rotary Cancer Hospital, All India Institute of Medical Sciences,New Delhi |
| 2003 – 2007 | Associate Professor | Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi |
| 1999 – 2003 | Assistant Professor | Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi |
| Oct 1995 – Dec 1998 | Associate Professor | Rajawadi Municipal Hospital, Mumbai |
| Sept 1991– Oct 1995 | Assistant Professor | Rajawadi Municipal Hospital, Mumbai |
| DATE | COLLEGE | FROM |
|---|---|---|
| 1986 – 1991 | SMS Medical college, MD (Anaesthesiology) | Jaipur |
| 1981 – 1986 | SMS Medical College, MBBS | Jaipur |
| 2011 – 2013 | Cardiff University, MSc in Palliative Medicine | Cardiff.UK |
Ph D # 7
MD/MS # 8
MSc Nursing # 2
Supervised Ms. Caroline Barry medical student from Hull York Medical School, University of York, Heslington, York, UK, Y010 5DD. as observership from 1ST Oct.2007 to 7th Oct.2007.
Supervised PhD thesis of Theology Student from Belgium.
Supervised PhD thesis of Psychology student from Delhi University.
Ongoing Phd – 4
How to start and Run a Pain Clinic “Palliative care in Pain Management” Sushma Bhatnagar 252-257,Wiley India Pvt Ltd.,New Delhi
Freedom from Pain. 2009, IK International House Pvt. Ltd. New Delhi
A hand book on Cancer Pain Management from developing countries perspective by IASP PRESS
Dr. Rajendra Prasad Centre for Ophthalmic Sciences is an integral part of AIIMS and was created in 1967 as a National Institute of Ophthalmology within the precincts of the AIIMS to ensure maximized interdisciplinary benefits and holistic patient care. As the Apex Institution under the National Programme for Control of Blindness ( NPCB ), it was the first Centre of its kind started at the AIIMS more than 38 years ago, followed by the other super-speciality Centres later at the Institute. The diverse patient and therefore the ancillary work load at Dr. R. P. Centre (a WHO Collaborating Centre for Prevention of Blindness) has been steadily and continuously increasing especially so in the last few years with the advent and application of latest technologies in sophisticated investigative and operative ophthalmology so important for overall patient care, both in the erstwhile laboratories as well as in our newer facilities at the Centre. To promote research in all directions of Ophthalmology this centre is having super-specialty departments to support extensive basic and applied research in ophthalmic sciences.
To know about the individual departments in detail please follow the link on the left side panel.
 |
Dr. Satish Verma
Additional Professor
Department Of Neurosurgery and Gamma Knife
Neurosciences Centreand
Jai Prakash Narayan Apex Trauma Centre
AIIMS, New Delhi.
E-mail - drsatishsx[at]aiims[dot]edu
Phone - 01126593291
Office - 606 CN Centre
Out-Patient days
CNC (Room# 16) - Monday (Forenoon), Thursday (Afternoon)
JPNA Trauma Centre - Thursday (Forenoon)
Dr Satish Verma joined as Assistant Professor in the Department of Neurosurgery at AIIMS, New Delhi, in November 2016. He did his graduation (MBBS) in 2008 from Motilal Nehru Medical College, Allahabad and post-graduation (MS General Surgery) in 2011 from King George’s Medical University, Lucknow. He worked as Senior Resident, Neurosurgery at Maulana Azad Medical College, New Delhi from 2011-2012. In 2012 he joined as MCh Neurosurgery resident at AIIMS, New Delhi. After completing MCh in July 2012, he worked as Chief Resident, Neurosurgery, at JPN Apex Trauma Centre, AIIMS till December 2015. Thereafter he worked as Senior Research Associate on a CSIR (Council for Scientific and Industrial Research) funded project, based on Endoscopic keyhole approaches for anterior circulation intracranial aneurysms from Jan 2016 to Oct 2016.
Academic Record
| S.No | Position Held | Duration |
|---|---|---|
| 1 | MBBS (Undergraduate), MLNMC, Allahabad | 01.10.2002 – 31.03.2008 |
| 2 | Junior Resident (General Surgery), KGMU, Lucknow | 31.05.2008 – 30.05.2011 |
| 3 | Senior Resident (Neurosurgery Non-Acad), LNH, New Delhi | 04.07.2011 – 08.12.2011 |
| 4 | Senior Resident (Neurosurgery Academic), AIIMS, New Delhi | 02.07.2012 – 01.07.2015 |
| 5 | Senior Resident (Neurosurgery Post MCh), AIIMS, New Delhi | 12.08.2015 – 02.01.2016 |
| 6 | Senior Research Associate (Neurosurgery), AIIMS, New Delhi | 03.01.2016 – 02.11.2016 |
| 7 | Assistant Professor (Neurosurgery), AIIMS, New Delhi | 03.11.2016 - 30.06.2020 |
| 8 | Associate Professor (Neurosurgery), AIIMS, New Delhi | 01.07.2020 - 30.06.2023 |
| 9 | Additional Professor (Neurosurgery), AIIMS, New Delhi | 01.07.2023 - Present |
Areas of interest-
Short-term Courses/ Observerships/ Fellowships -
Professional Memberships-
Details of Pubmed Indexed Publications-
1. Verma, S.K., et al., Correction of pediatric cervical kyphosis with standalone posterior approach-a single-center experience of seven cases. Childs Nerv Syst, 2023. 39(1): p. 239-247.
2. Verma, S.K., et al., Gamma Knife Stereotactic Radiosurgery for Giant Intracranial Tumors - A Series of 70 Patients. Neurol India, 2023. 71(Supplement): p. S123-s132.
3. Verma, S., D. Agrawal, and M. Singh, Role of Gamma Knife Radiosurgery in the Management of Functional Disorders - A Literature Review. Neurol India, 2023. 71(Supplement): p. S49-s58.
4. Chandra, P.S., et al., Technique of Distraction, Compression, Extension, Reduction to Reduce and Realign Old Displaced Odontoid Fracture from Posterior Approach: A Novel Technique. Neurospine, 2023. 20(1): p. 393-404.
5. Verma, S., et al., Use of Intraoperative Imaging to Preserve C1-C2 Mobility in Complex Atlas-Hangman Fractures. Neurology India, 2022. 70(1): p. 209-214.
6. Varshney, G., et al., Single-Stage Posterior Only Approach for Unilateral Atlantoaxial Spondyloptosis with type-II odontoid Fracture in Pediatric Patients. Neurol India, 2022. 70(Supplement): p. S129-s134.
7. Sharma, D., et al., Determination of Availability of Safety Margin for Placement of C3-C6 Pedicle Screw on CT Angiography. World Neurosurg, 2022. 157: p. e22-e28.
8. Sawarkar, D.P., et al., O-Arm Assisted Anterior Odontoid Screw Fixation in Type II and Rostral Type III Odontoid Fractures: Single Center Surgical Series of 50 Patients. Neurol India, 2022. 70(Supplement): p. S135-s143.
9. Kumari, S., S.K. Verma, and P.K. Singh, Crouzon’s Syndrome With A Dominant Sinus Pericranii Draining Transverse Sinus- Report Of A Rare Association And Review Of Literature. Pediatric Neurosurgery, 2022.
10. Garg, K., et al., Hybrid Workshops During the COVID-19 Pandemic-Dawn of a New Era in Neurosurgical Learning Platforms. World Neurosurg, 2022. 157: p. e198-e206.
11. Bisht, M., et al., Evaluation of Dural Parameters at C1 Level in Patients with Chiari 1 Malformation Following Foramen Magnum and C1 Posterior Arch Removal: Introduction of a Novel Concept to Decompress without Affecting Stability. Neurol India, 2022. 70(Supplement): p. S160-s165.
12. Verma, S., M. Tripathi, and P.S. Chandra, Cervicogenic Headache: Current Perspectives. Neurol India, 2021. 69(Supplement): p. S194-s198.
13. Verma, S. and S. Kumari, Orbitofrontal Extradural Hematoma: Unusual Cause of Proptosis. Pediatr Neurosurg, 2021.
14. Singh, S. and S. Verma, Letter: Protective Effects of Obstructive Sleep Apnea on Outcomes After Subarachnoid Hemorrhage: A Nationwide Analysis. Neurosurgery, 2021. 88(5): p. E486-e487.
15. Singh, P.K., et al., Management of myelopathy due to anterior soft tissue compression in vertebral hemangioma. World Neurosurgery, 2021.
16. Sawarkar, D., et al., Evolution to Pedicle Reformation Technique in Surgical Management of Hangman's Fracture. World Neurosurg, 2021. 149: p. e481-e490.
17. Paramanand, S.D., et al., Anterior odontoid screw fixation for pediatric and adolescent odontoid fractures: Single center experience over a decade. World Neurosurgery, 2021.
18. Garg, K., et al., Effect of External Ventricular Drain Tunnel Length on Cerebrospinal Fluid Infection Rates-A Bayesian Network Meta-Analysis. World Neurosurg, 2021.
19. Doddamani, R.S., et al., Microscissor DREZotomy for post brachial plexus avulsion neuralgia: A single center experience. Clin Neurol Neurosurg, 2021. 208: p. 106840.
20. Verma, S.K., et al., Video Section-Operative Nuances: Step by Step - Donning and Doffing in Neurosurgical Operating Room. Neurol India, 2020. 68(4): p. 796-799.
21. Singh, P.K., et al., Long-Term Outcome of Surgical Management in Symptomatic Pediatric Vertebral Hemangiomas Presenting With Myelopathy. Neurosurgery, 2020.
22. Singh, P.K., et al., Management of neglected complex hangman's fracture by reforming the C2 pedicle: new innovative technique of motion preservation at the C1-2 joint in 2 cases. J Neurosurg Spine, 2020: p. 1-8.
23. Singh, P.K., et al., Management of C2 Body Giant Cell Tumor by Innovatively Fashioned Iliac Crest Graft and Modified Cervical Mesh Cage Used as Plate. World Neurosurg, 2020. 140: p. 241-246.
24. Choudhary, K.S., et al., Feasibility of Double Anterior Odontoid Screw: A CT-Based Morphometric Analysis of the Axis in Adult Indian Population. Neurol India, 2020. 68(6): p. 1361-1366.
25. Verma, S.K. and P.K. Singh, Letter to Editor. Giant intracranial aneurysms of the posterior circulation. J Neurosurg, 2019. 132(3): p. 984-985.
26. Sharma, B.S., D.P. Sawarkar, and S.K. Verma, Endoscopic Management of Fourth Ventricle Neurocysticercosis: Description of the New Technique in a Case Series of 5 Cases and Review of the Literature. World Neurosurg, 2019. 122: p. e647-e654.
27. Bora, S., et al., Intracranial aspergillosis amongst immunocompetent patients: An experience with combined surgical and medical management of 18 patients. Clin Neurol Neurosurg, 2019. 186: p. 105511.
28. Verma, S.K., et al., Traumatic Posterior Fossa Extradural Hematoma: Experience at Level I Trauma Center. Asian J Neurosurg, 2018. 13(2): p. 227-232.
29. Satyarthee G D, V.S., Giant pituitary adenoma associated with extra diaphragmatic extension as multiple nubbin into subarachnoid space: Uncommon entity. Biomedical Research and Clinical Practice, 2018. 3(3): p. 1-2.
30. Mankotia, D.S., et al., Rare Case of Cerebrospinal Fluid Proctorrhea Caused by Anterior Sacral Meningocele with Recto-thecal Fistula. World Neurosurg, 2018. 114: p. 323-325.
31. Verma, S.K., et al., Pediatric cemento-ossifying fibroma of the orbital roof: Rare pathology at a rare location. Neurol India, 2017. 65(4): p. 902-903.
32. Singh, P.K., et al., Evaluation of Correction of Radiologic Parameters (Angulation and Displacement) and Accuracy of C2 Pedicle Screw Placement in Unstable Hangman's Fracture with Intraoperative Computed Tomography-Based Navigation. World Neurosurg, 2017. 107: p. 795-802.
33. Verma, S.K., et al., Medial sphenoid wing meningiomas: Experience with microsurgical resection over 5 years and a review of literature. Neurol India, 2016. 64(3): p. 465-75.
34. Verma, S.K., et al., O-arm with navigation versus C-arm: a review of screw placement over 3 years at a major trauma center. British Journal of Neurosurgery, 2016. 30(6): p. 658-661.
35. Sawarkar, D.P., et al., Fatal Superior Sagittal Sinus and Torcular Thrombosis After Vestibular Schwannoma Surgery: Report of a Rare Complication and Review of the Literature. World Neurosurg, 2016. 96: p. 607.e19-607.e24.
36. Verma, S.K., et al., Giant calvarial cavernous hemangioma. J Pediatr Neurosci, 2015. 10(1): p. 41-4.
37. Verma, S.K., et al., Orbital roof intradiploic meningioma in a 16-year-old girl. J Pediatr Neurosci, 2015. 10(1): p. 51-4.
38. Verma, S.K., G.D. Satyarthee, and B.S. Sharma, Giant intradiploic arachnoid cyst for 13 years. J Pediatr Neurosci, 2014. 9(2): p. 139-41.
39. Verma, S.K., G.D. Satyarthee, and B.S. Sharma, Giant choroid plexus papilloma of the lateral ventricle in fetus. J Pediatr Neurosci, 2014. 9(2): p. 185-7.
40. Verma, S.K., et al., Torcular occipital encephalocele in infant: Report of two cases and review of literature. J Pediatr Neurosci, 2013. 8(3): p. 207-9.
41. Verma, S.K., et al., Glioblastoma multiforme presenting as a fungating mass extending through the previous craniotomy site. Neurol India, 2013. 61(3): p. 325-6.
Chapters in Books -
Research Papers Presented in Conferences
International
| S.No. | Conference | Year | Topic | Travel Grants |
|---|---|---|---|---|
| 1 | WSSFN (World Society for Stereotactic and Functional Neurosurgery) Interim Meeting, Dubai | 2023 | Gamma-Knife Stereotactic Radiosurgery for Large Jugular Paragangliomas - Series of 18 patients | WSSFN Travel Grant |
| 2 | WSSFN (World Society for Stereotactic and Functional Neurosurgery) Interim Meeting, Dubai | 2023 | Gamma-Knife Stereotactic Radiosurgery for Giant Meningiomas - Series of 28 patients | WSSFN Travel Grant |
| 3 | 8th World Congress of IFNE (International Federation for Neuroendoscopy), Capetown, South Africa | 2017 | Endoscopic controlled keyhole approaches for clipping of anterior circulation aneurysms : A single centre experience over 2 years | Scholarship Educational Grant from IFNE |
| 4 | EANS (European Association of Neurosurgical Societies ) Athens, Greece | 2016 | Evaluation of surgical correction of radiological parameters (angulation and displacement) and accuracy of C2 pedicle screw placement in unstable hangman’s fracture with intraoperative CT based navigation. | EANS Travel grant |
| 5 | Annual meeting of ISPN (International Society of Pediatric Neurosurgery), Rio de Janeiro, Brazil. | 2014 | Evolution in management and outcome of Craniosynostosis : A single centre experience of 128 cases at AIIMS, New Delhi | ISPN International travel grant |
National
| S.No. | Conference | Year | Topic |
|---|---|---|---|
| 1 | NSSA (Neuro Spinal Surgeons Association) Annual Meeting 2023, 16-18 September, New Delhi | 2023 | How I do it - Surgical Management of Vertebral Hemangiomas - A Three Pronged Approach. |
| 2 | 11th Combined meeting of Asia Pacific Spine Society (APSS) & Asia Pacific Paediatric Orthopaedic Society (APPOS), Goa, India, from September 22nd to 24th, 2017 | 2017 | Evaluation of correction of radiological parameters (angulation and displacement) and accuracy of C2 pedicle screw placement in unstable Hangman’s fracture with intraoperative CT based navigation. |
| 3 | Neurocon UK/UP, Nainital, Uttarakhand. | 2016 | O-arm with navigation versus C-arm: A review of screw placement over 3 years at a major trauma centre. |
| 4 | IndSPNCON (Indian Society for Pediatric Neurosurgery), Bhubaneswar, Odisha | 2014 | Evolution in management and outcome of Craniosynostosis : A single centre experience of 128 cases at AIIMS, New Delhi. |
| 5 | IndSPNCON (Indian Society for Pediatric Neurosurgery), Bhubaneswar, Odisha | 2014 | Giant Calvarial Cavernous Hemangioma – A case report. |

National Survey on Extent and Pattern of Substance Use in India’ 2019
While psychoactive substance use often tends to be framed as a problem or menace in the public-health or social-welfare discourse, the exact dimensions of substance use in India have not been assessed adequately, so far. A wide variety of entities – policy makers, researchers, service-providers, law-enforcers – need reliable and credible estimates of how many people in India use addictive substances and how many of them suffer from substance use disorders.
This report presents the major findings of the survey in terms of proportion of Indian population using various substances and those affected by substance use disorders. Representing a culmination of efforts of a large number of organizations and individuals, this is the first attempt in the history of India to provide detailed estimates of substance use in the country as well at the level of each states. It should now be possible to answer the questions like, which states of the country has the largest population of people affected by drug use? Or which substance is consumed by most Indian people who use drugs? After providing a snap-shot of the intricate and robust scientific research methodology, we provide the results of the survey in terms of each of the major categories of psychoactive substances, at the national as well as at the level of states. We also provide a broad framework of recommendations on how should the country move ahead in terms of mounting an effective response to the drug use epidemic. This comprehensive survey had multiple components. Considering the complex phenomenon of substance use and its consequences a number of issues need to be explored and studied in depth.
Photo 1 ( Hon Cabinet Minister. Shri Thaawar Chand Gehlot. Shri Thaawarchand Gehlot. Minister for Social Justice & Empowerment along with Hon Minister of State, Shri Vijay Sampla for MSJ&E, Chief, NDDTC, Prof Rakesh Kumar Chadda & Prof Atul Ambekar (Prinicipal Invetigator of the National Survey at the launch of "Magnitude of Substance Use in India, 2019" report)
Prof Atul Ambekar,
Principal Investigator,
Professor, National Drug Dependence Treatment Centre, AIIMS, New Delhi
atul.ambekar[at]gmail[dot]com
Prof Rakesh Kumar Chadda, Chief, National Drug Dependence Treatment Centre (NDDTC), AIIMS, New Delhi
Prof Sudhir K. Khandelwal, Ex-Chief, National Drug Dependence Treatment Centre (NDDTC), AIIMS, New Delhi
Ravindra Rao, Associate Professor, National Drug Dependence Treatment Centre (NDDTC), AIIMS, New Delhi
Ashwani Kumar Mishra, Associate Professor, National Drug Dependence Treatment Centre (NDDTC), AIIMS, New Delhi
Alok Agrawal, Assistant Professor, National Drug Dependence Treatment Centre (NDDTC), AIIMS, New Delhi
Please click here for detailed report
National Survey on Extent and Pattern of Substance Use in India’ 2019
While psychoactive substance use often tends to be framed as a problem or menace in the public-health or social-welfare discourse, the exact dimensions of substance use in India have not been assessed adequately, so far. A wide variety of entities – policy makers, researchers, service-providers, law-enforcers – need reliable and credible estimates of how many people in India use addictive substances and how many of them suffer from substance use disorders.
This report presents the major findings of the survey in terms of proportion of Indian population using various substances and those affected by substance use disorders. Representing a culmination of efforts of a large number of organizations and individuals, this is the first attempt in the history of India to provide detailed estimates of substance use in the country as well at the level of each states. It should now be possible to answer the questions like, which states of the country has the largest population of people affected by drug use? Or which substance is consumed by most Indian people who use drugs? After providing a snap-shot of the intricate and robust scientific research methodology, we provide the results of the survey in terms of each of the major categories of psychoactive substances, at the national as well as at the level of states. We also provide a broad framework of recommendations on how should the country move ahead in terms of mounting an effective response to the drug use epidemic. This comprehensive survey had multiple components. Considering the complex phenomenon of substance use and its consequences a number of issues need to be explored and studied in depth.
Photo 1 ( Hon Cabinet Minister. Shri Thaawar Chand Gehlot. Shri Thaawarchand Gehlot. Minister for Social Justice & Empowerment along with Hon Minister of State, Shri Vijay Sampla for MSJ&E, Chief, NDDTC, Prof Rakesh Kumar Chadda & Prof Atul Ambekar (Prinicipal Invetigator of the National Survey at the launch of "Magnitude of Substance Use in India, 2019" report)
Principal Investigator,
Professor, National Drug Dependence Treatment Centre, AIIMS, New Delhi
atul.ambekar[at]gmail[dot]com
Chief, National Drug Dependence Treatment Centre (NDDTC), AIIMS, New Delhi
atul.ambekar[at]gmail[dot]com
Ex-Chief, National Drug Dependence Treatment Centre (NDDTC), AIIMS, New Delhi
atul.ambekar[at]gmail[dot]com
Associate Professor, National Drug Dependence Treatment Centre (NDDTC), AIIMS, New Delhi
atul.ambekar[at]gmail[dot]com
Associate Professor,
National Drug Dependence Treatment Centre (NDDTC), AIIMS, New Delhi
atul.ambekar[at]gmail[dot]com
Assistant Professor,
National Drug Dependence Treatment Centre (NDDTC), AIIMS, New Delhi
Please click here for detailed report
| Public information officer (PIO) | Prof Raka Jain
|
Assistant public information officer (PIO)
| Dr Monika Mongia
|
Appellate authoity
| Prof R K Chadda
|
Public information officer (PIO)
Assistant public information officer (APIO)
Appellate authoity
Designation: Additional Professor
Address: Room No. 3020, Department of Biochemistry, Third Floor, Teaching Block, AIIMS, New Delhi
Official phone: +91-11-2659 4027
Email ID:
| Position held | Department | University/Institution | Duration |
|---|---|---|---|
| Additional Professor | Biochemistry | AIIMS, New Delhi | 2020 onwards |
| Associate Professor | Biochemistry | AIIMS, New Delhi | 2017 to 2020 |
| Assistant Professor | Biochemistry | AIIMS, New Delhi | 2014 to 2017 |
| Staff Scientist | Hem & Oncology | University of Chicago, USA | 2011 to 2014 |
| Research Associate | Geno & Sys Biology | University of Chicago, USA | 2009 to 2011 |
| Sr Post Doc | Genetics | Yale University | 2005 to 2009 |
| Degree | Department | University/Institution | Year | Remarks |
|---|---|---|---|---|
| PhD | Biochemistry | AIIMS, New Delhi | 2004 | Best Postgraduate in Clinical research |
| MSc | Medical Biochemistry | JIPMER, Pondicherry | 1998 | Honour of Merit for University 1st Rank in Masters |
| BSc (Hons.) | Chemistry | Calcutta University | 1995 |
The laboratory employs classic molecular biology tools assisted with in silico tools to elucidate pathogenesis of various cancer including Breast Cancer, Gall Bladder Cancer, AML etc. The breast cancer project studies the cellular and molecular events pertaining to the Androgen Receptor-mediated events in Breast Cancer cell lines and validating the same in tumor obtained post-surgery. In GBC, we are exploring the role of Nuclear Receptors in the pathophysiology of gallbladder cancer and its implication in the severity of the disease. We are also investigating tumor infiltrating lymphocytes in the same. In vitro study on gallbladder cancer cell lines alteration of different phenotypic properties like migration, invasion, proliferation, apoptosis etc following treatment with different drugs targeting nuclear receptors.
Placenta is a highly specialised multifaceted organ that supports the life of growing fetus throughout the pregnancy and also serves as a source of nutrient, gaseous and waste products exchange between the mother and the fetal circulation. During the course of gestation, the placenta undergoes multiple changes which are crucial for establishing a healthy pregnancy. Placental research is aimed to identify and analyse the effect of toxic pollutants such as Sulphur dioxide and Particulate matter on the trophoblast cells and thus pregnancy. A part of my research work also warrants to identify the transgenerational effect of these pollutants on the fetal health and growth which would be achieved by performing in-silico analysis and animal experiments.
PhD scholars
| Sl. No. | Personnel | Date of registration | Research area |
|---|---|---|---|
| Sl. No. | Personnel | Date of registration | Research area |
| 1 | Tryambak P. Srivastava | 31-03-2018 | Breast Cancer |
| 2 | Sunil Singh | 13-11-2018 | Placental Biology |
| 3 | Dr. Sajib Kumar Sarkar | 14-11-2018 | Gall Bladder Cancer |
| 4 | Neha Kashyap | 24-06-2021 | Placental Biology |
MSc Student
| Sl. No. | Personnel | Date of registration | Research area |
|---|---|---|---|
| 5 | Lavanya Gupta | 08-09-2021 | Placental Biology |
Post Doc Fellows
| Sl. No. | Personnel | Date of registration | Research area |
|---|---|---|---|
| 6 | Dr. Arnab Nayek | Bioinformatics | |
| 7 | Dr. Joyeeta Talukdar | Cancer Biology | |
| 8 | Dr. Rashmi | Patient derived tumor organoid cultures | |
| 9 | Dr. Isha Goel | Bioinformatics |
| Sl. No. | Personnel | Research area |
|---|---|---|
| 10 | Indrani Mukherjee | Placental Biology |
| 11 | Abhibroto Karmakar | Autoimmune disorders |
| 12 | Swati Ajmeriya | Bioinformatics |
| 13 | Aman Saifi | Renal cell carcinoma |
| Sl. No. | Personnel | Research area |
|---|---|---|
| 14 | Vivak Kumar | Documentation and laboratory assistance |
| 15 | Deepak Kumar | Laboratory assistance |
Tryambak is a final-year PhD scholar in Dr. Karmakar’s laboratory. He is working on elucidating the role of the Androgen Receptor in the pathogenesis of Breast Cancer. This prospective study is carried out simultaneously in cell lines and the subjects with breast cancer undergoing surgical interventions at AIIMS, New Delhi. His doctoral research is assisted by a group of basic scientists, pathologists, surgeons; medical, surgical, and laboratory oncologists. He remains grateful to the generous funding support from the ICMR, DHR, and SERB for laboratory funding and CSIR-UGC in terms of senior research fellowship.
Tryambak obtained his B.Sc. B.Ed. dual degrees from the Regional Institute of Education, Bhubaneswar, a constituent unit of NCERT, New Delhi. Following his graduation, he joined South Asian University (SAU), New Delhi for an M.Sc. in Biotechnology. In his masters’ dissertation, he checked the efficacy of a Pfizer drug against the HIV-1 subtype C.
Tryambak advocates open access to knowledge and information. An amateur linguist, he communicates his science, blogs, and thoughts on his website and Twitter. His profile, contact information, and other relevant details can be fetched from his website.
Mr. Sunil Singh has completed his Bachelor’s in 2015 from Deshbandhu College, University of Delhi, New Delhi. After B.Sc. he joined All India Institute of Medical Sciences (AIIMS), New Delhi as master’s Student and completed it in 2017. During M.Sc. he did his thesis under the mentorship of Dr. Subhradip Karmakar on the “Role of Peroxisome Proliferator Activated Receptor alpha (PPAR-α) in Human Trophoblast Invasion”. In 2018 he joined Dr. Subhradip Karmakar, Asst. Professor, Dept. of Biochemistry, AIIMS, New Delhi as PhD student and has started his work on understanding the role of toxic pollutants such as Sulphur dioxide and Particulate matter on the trophoblast cells and thus pregnancy and placentation. A part of his research work also warrants to identify the
transgenerational effect of these pollutants on the fetal health and growth which would be achieved by performing RNA-Seq and ChIP-Seq followed by depth in-silico analysis and animal experiments.
Dr Sajib Kumar Sarkar (MBBS, MD, DNB) is a 4th year PhD scholar with Dr Karmakar. He did his MD in Biochemistry from MAMC, New Delhi. As a part of MD thesis he worked on in vitro and animal models of insulin resistance and observed the ameliorating effect of extract of Jamun (Syzigium cumini) seed. He completed 3 years of Senior Residency from department of Biochemistry, AIIMS, New Delhi. Presently he is exploring the molecular pathogenesis of gallbladder cancer with special focus on nuclear receptors.
Ms. Neha Kashyap, first year Ph.D. Scholar has completed her Bachelors in Zoology Honours from “Ravenshaw University” Cuttack, Odisha. She has done her Masters in Life Sciences (Specialization in Biochemistry) from Central University of Punjab, Bhatinda. Her M.Sc. dissertation work was on the topic "miRNA mediated pathway modulation by phytochemicals: An In-silico approach" under the guidance of Dr. Shashank Kumar, Assistant Professor in the Department of Biochemistry. She got selected for the Indian Academy of Sciences “Summer Research Fellowship” project sponsored by the Indian Academy of Sciences, Bengaluru, during her graduation where she worked on the project "Analysis of Phytochemical constituents and amino acids present in green
seaweeds from South East Coast of India” under Dr.George Seghal Kiran,Assistant Professor in Pondicherry University. Later, she worked as a Junior Research Fellow (JRF) in Structural Parasitology lab, International Centre for Genetic Engineering and Biotechnology (I.C.G.E.B), New Delhi under eminent Principal Scientist Dr. Amit Sharma, Director of ICMR-NIMR in the Project "Development and validation of Hyponozite biomarkers for detecting Plasmodium vivax infection" .She also worked there on “Malarial culture and parasite proteins crystallography” .She qualified for ICMR-JRF 2020. Currently, she is working as a Ph.D. Scholar, under Dr. Subhradip Karmakar, Additional Professor in the Department of Biochemistry in All India Institute of Medical Sciences (AIIMS), New Delhi. She is working with the placenta group. Her tentative thesis is " Molecular insights into the chromatin dynamics and epigenetic changes during trophoblast fusion.”.
Ms Lavanya Gupta has completed her Bachelors from Sri Venkateswara College, University of Delhi in the year 2018-2021. She has done a summer internship project on “Applications of Bioinformatics in Cardiovascular Disorders for Novel Therapeutics Design under ”SRI VENKATESWARA INTERNSHIP PROGRAM FOR RESEARCH IN
ACADEMICS(SRI-VIPRA 2020) “ which included: Identification of target receptors implicated in cardiovascular diseases , compilation of ligand libraries ,Study of ADMET properties for drug-likeness and Virtual screening by docking followed by evaluation of docking energy to find best hit. She has done ADD ON COURSE -
1) “The Science of Stem cells “
2) "Fundamentals of Immunology: Innate Immunity and B-Cell Function"
3) "Understanding the Brain: The Neurobiology of Everyday Life An online course authorized by American Museum.
She was also involved in drug and development project (VISTAAR) , a science Popularisation Event organised by SVC .
Also, she was a part of mindspar ideathon event organised in Sri Venkateswara college, where she was awarded with the best presentation.
Currently, she is working as a Msc student, under Dr. Subhradip Karmakar, Additional Professor in the Department of Biochemistry in All India Institute of Medical Sciences (AIIMS), New Delhi. She is working with the placenta group. Her tentative thesis is "To study the role of estrogen regulated miRNA involved in the process of Human
Dr. Arnab is working as a Research Associate (Bioinformatician), in the department of Biochemistry, All India Institute of Medical Sciences, New Delhi, under the guidance of Dr. Subhradip Karmakar, Additional Professor, Department of Biochemistry. He is associated with the transcriptomics (RNA-seq) data analysis from RNA sequencing data generated from the lab as well as publicly available data from the The Cancer Genome Atlas (TCGA) database, development of integrated pipelines for NGS data analysis etc. His research credentials supported with 13 publications in referred journals and his research interest includes Next generation sequencing (NGS) data analysis from human samples to improve the disease diagnosis for clinicians, development of integrated pipelines for
NGS data analysis, protein structure modelling, protein engineering, Molecular dynamics simulations.
Dr. Rashmi
Works on Cancer Research Related to Understand the Altruistic Mechanism and Metastasis. My focus is to understand the mechanism of cancer recurrence, and the complex biological systems that underlie its development. Further, if possible to identify new ways of treating the disease by taking a close-up look at the fundamental mechanisms at work within cells.
Dr. Rashmi Minocha has completed her Ph.D. in Biochemistry from the Ludwig Maximilian University of Munich (LMU), Germany. During the course of her Ph.D., she carried out her research work at the Gene Center, LMU Munich and at the Institute of Biochemistry, University of Gießen (Germany). The overall aim of her doctoral work was to understand how gene expression is regulated by the cross communication between its single steps using yeast as a model organism. Specifically, she worked on the biochemical and functional characterization of splicing proteins Mud2 and Prp19 complex (Prp19C).
After her Ph.D., she moved back to India and joined All India Institute
of Medical Sciences (AIIMS) in the Department of Biochemistry to pursue her interests in medical and health-based research. She is presently working as a Young Scientist Awardee (a fellowship and research grant funded by Department of Health Research). Her major research interests are:
Her on-going focus is to apply these 3D culture systems to investigate into the molecular mechanisms which drive gallbladder carcinogenesis.
Ms. Indrani Mukherjee completed her Bachelor’s degree from Bethune College, Kolkata, the oldest women’s college in Asia with first division in Zoology. She pursued her Master’s degree in Zoology with first class from Asutosh College, University of Calcutta. Ms. Indrani completed her research training during M.Sc on the “Role of nanocapsulated flavonoidal antioxidants in combating age related cerebral ischemia-reperfusion (CIR) induced oxidative injury in rat brain” under the guidance of Dr. Nirmalendu Das, Emeritus Scientist, CSIR-Indian Institute of Chemical Biology, Kolkata. She formulated nano-encapsulated antioxidants and applied them orally to Sprague Dawley rats as a pre-treatment prior to CIR insult. She studied the rat brains for histological examinations and
expression of cellular apoptotic factors. Later, she worked under the guidance of Dr. Parasuraman Jaisankar, Senior Principal Scientist, CSIR-Indian Institute of Chemical Biology, Kolkata, in two projects. One project was entitled “A molecular docking approach to study the possible interactions between Yeast 1,4-α glucosidase and some synthetic inhibitors” where she used molecular docking to analyse the interactions between various proteins and their ligands. The second project was entitled “Isolation of enzymes from natural resources” where she used column chromatography, thin layer chromatography and HPLC for the extraction and chemical purification of phosphatases from natural resources. Ms. Indrani then worked as a Project Fellow under the guidance of Dr. Shantanu Chowdhury, Senior Principal Scientist, Functional Genomics, CSIR-Institute of Genomics and Integrative Biology, New Delhi. She focussed on learning the basic molecular biology techniques. She was involved in the amplification of pGL3 basic vector in Stbl2 strain of E.coli and its transient transfection and analysis of protein expression profile in HT 1080 cells. Currently, she is working as a PhD student under the guidance of Dr. Subhradip Karmakar, Additional Professor, Department of Biochemistry, All India Institute of Medical Sciences, New Delhi. She is a registered Ph.D scholar of Amity University, Noida, Uttar Pradesh. Her tentative thesis is entitled as “To Investigate the Role of Reactive Oxygen Species in Development of Pre-eclampsia”. Pre- eclampsia is a leading cause of maternal and neonatal mortality and morbidity and is usually diagnosed during the last trimester of pregnancy (after 20 weeks of gestation). During Pre-eclampsia, trophoblast cell migration and invasion into the maternal decidua, and vessels are typically incomplete, and thus angiogenesis and trophoblast cell proliferation are impaired. The shallow trophoblastic invasion induces placental ischemic reperfusion injury due to irregular uterine blood flow which results in the generation of reactive oxygen species (ROS). Therefore, her hypothesis is that excessive ROS generation along with an alteration of cytokine and hormonal levels in the uterine microenvironment, might contribute to the pathogenesis of Pre-eclampsia. Ms. Indrani was also awarded with CSIR-Senior Research Fellowship in the year 2019 and served as the Cultural Secretary of Society of Young Scientists (SYS), AIIMS, New Delhi, for the year 2020-2021.
Systemic Lupus Erythematosus is a chronic, autoimmune disease with wide clinical presentation. Lupus widely affects many organs and system with no cure. The main area of our study is understanding the genomic stratification and drug responds between the patients with lupus. We keen to explore the molecular aspect of patients during lupus flare and remission. We are also looking at single nucleotide polymorphism in SLE patients focusing on Indian population. Apart from my PhD we are looking at the role of nuclear receptor in pathogenesis of gall bladder cancer.
Apart from science I love teaching dance, recitation and writing poems. I love to do solo travelling and cooking give me zeal to life. I believe education is important for all in this regard I made an YouTube channel
creating medical awareness and do career counselling in field of life sciences.
Swati Ajmeriya is working as Senior Research fellow at Department of Biochemistry, AIIMS under Dr. Subhradip Karmakar. She did her masters in Biotechnology. She does research in the area of genomics using bioinformatic tools and techniques. She has worked on high-throughput exome, transcriptome and metagenomics data. She has good command over linux scripting, R and python programming. She also develops pipelines for rapid processing of genomics data. Swati's research work is primarily involved in transcriptomics and statistical genomics with applications to the identification of differentially expressed genes and genetic variants conferring susceptibility to diseases by discovering variants, genes and pathways from high-throughput data.
Mr Aman Saifi is working as a Junior Research Fellow on a project called "Molecular Analysis to explore resistance against receptor tyrosine kinase inhibitors (RTKI) in Renal Cell Carcinoma (RCC) and the prognostic role of circulating tumour cells in patients with metastatic RCC (mRCC). He has completed his Bachelor's and Master's Integrated Degree in Biotechnology from Amity University, Uttar Pradesh. He qualified GATE exam in 2021 as well as in 2022. His university awarded him a merit scholarship during his coursework. He was selected for the summer internship program at Jawaharlal Nehru University. He worked on the project "standardizing the IR64 rice seeds tissue culture protocol for the plant transformation with Agrobacterium tumefaciens harbouring pCAMBIA1304 vector". Later, for his master's thesis, he worked on the project "standardization of differentiation of bone cell precursors (macrophages and mesenchymal stem cells) into mature bone cells (osteoclast and osteoblast cells)" in the department of Biotechnology, AIIMS
| Sl. No. | Personnel | Duration | Work |
|---|---|---|---|
| MD-PhD graduates | |||
| 1 | Dr. Karthikeyan Pethusamy | 2016-2022 | AML |
| 2 | Dr. Ashikh Seethy | 2017-2022 | MDS |
| MD graduate | |||
| 3 | Dr. Ankita Raj | 2015-2018 | Placental Biology |
| Senior Resident | |||
| 4 | Dr. Ashok Kumar Ahirwar | 2014-2017 | Placental Biology |
NDDTC, AIIMS to celebrate 17th Annual Day in April 2020 (TBA)
NDDTC, AIIMS celebrates its 16th Annual Day on 15th April 2019
1st National Conference on Addiction Psychiatry (November 27-29, 2017)
NDDTC, AIIMS to celebrate 17th Annual Day in April 2020 (TBA)
NDDTC, AIIMS celebrates its 16th Annual Day on 15th April 2019
1st National Conference on Addiction Psychiatry (November 27-29, 2017)
NDDTC, AIIMS celebrates its 16th Annual Day on 15th April 2019
The 16th Annual Day of National Drug Dependence Treatment Centre (NDDTC), All India Institute of Medical Sciences (AIIMS), New Delhi was celebrated at NDDTC, Ghaziabad on 16th April 2019. Mr. Deves Deval, Director, DDAP, MOH&FW; Prof.RandeepGuleria, Director, AIIMS, New Delhi, Dr. DK Sharma, MS, AIIMS, New Delhi. Mr. Veerendra Mishra, Director, NISD were the dignitaries for the function. Prof (Dr.) Rakesh Chadda, Chief NDDTC and Head Department of Psychiatry, AIIMS presented the Annual Report for the year 2018- 2019 highlighting the achievements of the centre. Organizing Secretary, Prof(Dr.) Atul Ambekar presented the findings of recently conducted 2nd“National Drug Use Survey of India”. Textbook of “Basics of Addiction Psychology” was also released on this occasion.










NAUGRATION OF CIMR BY SH J P NADDA (FORMER HEALTH MINISTER)

A. IDY GALLERY (2017-18)

A. IDY GALLERY (2017-18)

DR H R NAGENDRA, DR S C MANCHANDA WITH DR RANDEEP GULERIA DURING IDY 2017

B.IDY GALLERY (2018-19)

B.IDY GALLERY (2018-19)

Training Program on “Self Management of Excessive Tension (SMET)” for AIIMS Faculty Members

Training programme on “Self Management of Excessive Tension (SMET)” for AIIMS Scholars & Research Fellows

BASIC YOGA TRAINING FOR SCHOOL STUDENTS ON “INSTITUTE DAY"
BASIC YOGA TRAINING FOR SCHOOL STUDENTS ON “INSTITUTE DAY"
ON LINE SESSIONS DURING PANDEMIC

EXPERT GROUP MEETING ON INTEGRATIVE MEDICINE

Dr Gautam Sharma, CIMR and Robert Svoboda, Ramkumar, Hansaji J Yogendra in conversation with Michael Menezes during “JAIPUR LITERATURE FESTIVAL”

VISIT AT CIMR BY SECRETARY, MINISTRY OF AYUSH

DURING ORIENTATION PROGRAMME FOR AYURVEDA RESEARCHERS WITH PROFESSOR TANUJA NESHRI,DIRECTOR , ALL INDIA INSTITUTE OF AYURVEDA NEW DELHI

VISIT BY DELEGATES FROM AUSTARLIA AT CIMR ,AIIMS NEW DELHI

NATIONAL AYURVEDA DAY CELEBERATION

Tree plantation (Saraca asoca Roxb.) planted by Prof. Randeep Guleria ( Director, AIIMS, New Delhi) on 19th June 2022
Inter-institutional Yoga Quiz competition -2022

Mass Yoga practice on 8th International day of Yoga 21st June 2022

Mass Yoga practice on 8th International day of Yoga 21st June 2022

SWAYAM Workshop for Nursing Staff of AIIMS, New Delhi -2022

1. GLIMPSES OF CIMR VISIT BY SMT ANUPRIYA PATEL, MINISTER OF STATE FOR HEALTH AND FAMILY WELFARE-2024

2. MASS COMMON YOGA PROTOCOL DEMONSTRATION IN IDY-2024
NDDTC, AIIMS celebrates its 16th Annual Day on 15th April 2019
The 16th Annual Day of National Drug Dependence Treatment Centre (NDDTC), All India Institute of Medical Sciences (AIIMS), New Delhi was celebrated at NDDTC, Ghaziabad on 16th April 2019. Mr. Deves Deval, Director, DDAP, MOH&FW; Prof.RandeepGuleria, Director, AIIMS, New Delhi, Dr. DK Sharma, MS, AIIMS, New Delhi. Mr. Veerendra Mishra, Director, NISD were the dignitaries for the function. Prof (Dr.) Rakesh Chadda, Chief NDDTC and Head Department of Psychiatry, AIIMS presented the Annual Report for the year 2018- 2019 highlighting the achievements of the centre. Organizing Secretary, Prof(Dr.) Atul Ambekar presented the findings of recently conducted 2nd“National Drug Use Survey of India”. Textbook of “Basics of Addiction Psychology” was also released on this occasion.
21st Annual Meeting of International Society of Addiction Medicine to be held in New Delhi, India from 13th to 16th November 2019. The theme of the conference is "Addiction in a Rapidly Changing World". We look forward to this opportunity to meet colleagues for shared learning, and a rich social and cultural experience. The conference is being organised by the Department of Psychiatry & National Drug Dependence Treatment Centre (NDDTC), All India Institute of Medical Sciences (AIIMS), New Delhi, India.
Key dates
Proposal Submission deadline for Symposium/ Workshop: 30th April, 2019 (Midnight; Indian Standard Time)
Abstract Submission deadline for Oral Communication / Posters: 30th June, 2019 (Midnight; Indian Standard Time)
Please click here for detail
21st Annual Meeting of International Society of Addiction Medicine to be held in New Delhi, India from 13th to 16th November 2019. The theme of the conference is "Addiction in a Rapidly Changing World". We look forward to this opportunity to meet colleagues for shared learning, and a rich social and cultural experience. The conference is being organised by the Department of Psychiatry & National Drug Dependence Treatment Centre (NDDTC), All India Institute of Medical Sciences (AIIMS), New Delhi, India.
Key dates
Proposal Submission deadline for Symposium/ Workshop: 30th April, 2019 (Midnight; Indian Standard Time)
Abstract Submission deadline for Oral Communication / Posters: 30th June, 2019 (Midnight; Indian Standard Time)
Please click here for detail
| Substance use disorders: Handbook for physicians |  |
| Substance use disorders: Manual for paramedical personnel |  |
| Substance use disorders: A manual for facilitators |  |
| Substance use disorders: Case book |  |
| Substance use disorders: Manual for physicians |  |
| Substance use disorders: Manual for nursing personnel |  |
| Screening and brief intervention for drug use: Resource Guide |  |
| Manual for long term pharmacotherapy |  |
| Psychosocial interventions for persons with substance abuse: Theory and practice (Developed by NIMHANS Bangalore, REPRINT) |  |
| -- | -- |
|---|---|
| Substance use disorders: Handbook for physicians | |
| Substance use disorders: Manual for paramedical personnel | |
| Substance use disorders: A manual for facilitators | |
| Substance use disorders: Case book | |
| Substance use disorders: Manual for physicians | |
| Substance use disorders: Manual for nursing personnel | |
| Screening and brief intervention for drug use: Resource Guide | |
| Manual for long term pharmacotherapy | |
| Psychosocial interventions for persons with substance abuse: Theory and practice (Developed by NIMHANS Bangalore, REPRINT) | |
The Faculty members have carried out several research projects funded by national and internationally recognized agencies like Indian Council of Medical Research (ICMR), Ministry of Health and Family Welfare, Ministry of Social Justice and Empowerment, Ministry of Finance, Council of Scientific and Industrial Research (CSIR), Department of Science and Technology (DST), WHO (India), WHO (Geneva), and United Nations Office of Drugs and Crime (UNODC). Some of the research projects have resulted in Publications by the centre.
Some of the important research and public health projects are listed below.
Some Ongoing Projects
Completed Projects

Dr. Jayanth Kumar, Additional Professor
Address: Room No. 4008, Convergence Block, AIIMS, New Delhi.
Email id: drjayanth[at]aiims[dot]edu
MBBS, Medicine and Surgery (2000-2006)
Government Stanley Medical College,
Chennai, Tamilnadu
MD, Biochemistry, (2007-2010)
All India Institute of Medical Sciences (AIIMS), New Delhi.
Senior Demonstrator (2010-2012)
Department of Biochemistry, AIIMS, New Delhi
Postdoctoral Research Fellowship (2012-2014)
Department of Pathology and Lab Medicine
David Geffen School of Medicine at UCLA, Los Angeles, California
Assistant Professor (2014-2017)
Department of Biochemistry, AIIMS, New Delhi
Associate Professor (2017-2020)
Department of Biochemistry, AIIMS, New Delhi
Additional Professor (2020-Present)
Department of Biochemistry, AIIMS, New Delhi
Our lab focusses on multiple research questions whose answers hopefully will lead to a translational utility.
We are always on the lookout for excellent postdoctoral/graduate students. If you are interested in the type of work which we do and have an idea which you wish to work on, please drop an email to drjayanth[at]aiims[dot]edu.
MBBS students for summer fellowships and short-term training are always welcome if you are willing to put in the hard work
The Faculty members have carried out several research projects funded by national and internationally recognized agencies like Indian Council of Medical Research (ICMR), Ministry of Health and Family Welfare, Ministry of Social Justice and Empowerment, Ministry of Finance, Council of Scientific and Industrial Research (CSIR), Department of Science and Technology (DST), WHO (India), WHO (Geneva), and United Nations Office of Drugs and Crime (UNODC). Some of the research projects have resulted in Publications by the centre.
Some of the important research and public health projects are listed below.
It is the online portal of Tele Medicine Facility of National Drug Dependence Treatment Center (NDDTC), All India Institute of Medical Sciences (AIIMS), New Delhi.
Faculty-in-charge: Dr Yatan Pal Singh Balhara
It is the online portal of Tele Medicine Facility of National Drug Dependence Treatment Center (NDDTC), All India Institute of Medical Sciences (AIIMS), New Delhi.
Faculty-in-charge: Dr Yatan Pal Singh Balhara
Click here to access eNDDTC
Dr Kanwaljeet Garg
MBBS (AIIMS), M.CH (AIIMS), DNB, MNAMS, FACS
Complex Spine Surgery Fellowship
Additional Professor, Department of Neurosurgery and Gamma Knife,
All India Institute of Medical Sciences and JPN apex Trauma Centre
New Delhi, India; Phone: 91-11-26593291
Email: kanwaljeet[at]aiims[dot]edu
Brief Profile
Dr Kanwaljeet Garg is an AIIMS alumnus. He joined AIIMS, New Delhi, the most prestigious and competitive medical school in India in 2001. He further completed M.Ch. Neurosurgery residency (6 years) from AIIMS, New Delhi itself. He had an excellent academic and surgical record throughout his residency training with many publications in both national and international journals in residency. He has also presented his work at various scientific meetings in India and abroad. He was awarded the ISPN travelling fellowship to present his research. He has also won the first prize for “micro suturing and microneural anastomosis” and “high speed drilling” at the 13th Neurosurgery skills training workshop held at AIIMS.
After completing his neurosurgical residency, he joined a one year long clinical fellowship “Combined Spine Surgery” at the Cumming School of Medicine, University of Calgary, Calgary (Canada), under the mentorship of world-renowned spine surgeons like Prof John Hurlbert and Prof Jacques Bouchard. He refined his skills in spine surgery during this fellowship and also learned the art of minimal invasive spine surgery at a high-volume centre. He was about to start another fellowship in spine surgery with Prof Richard Fessler at Rush University, Chicago (USA) but he got selected and joined as an Assistant Professor, Department of Neurosurgery at AIIMS in July 2015. Currently, he is working as an Additional Professor in the same department. He is well versed in all aspects of neurosurgery with special interest in Spine surgery, surgery for Movement disorders and Stereotactic Radiosurgery (Gamma Knife). He has keen research interest and has been working on many projects. He has keen interest in research and has about 250 publications in renowned international and national journals. Considering this, he was invited to be a Section Editor for the journal World Neurosurgery. He is also an Associate Editor for the Frontiers in Surgery,Neurology India and Indian Journal of Neurotrauma.
Areas of Interest –
Spine surgery
Functional neurosurgery
Gamma knife Radiosurgery
Pediatric neurosurgery
Skull base and Cerebrovascular surgery
Endoscopic neurosurgery
Neuro-oncology
Research Interests :
Professional Memberships –12 national and international societies
Clinics and inpatient services:
Neurosurgery Unit I
OPD days : Monday 9 am – 1 pm and Thursday 2 pm – 5 pm, Room number 16, Ground Floor, CNC OPD (For OPD appointment, contact 011-26593291)
Gamma Knife Clinic: Tuesday 9 am – 11 am, Gamma Knife Center, AIIMS, New Delhi
DBS Clinic: Saturday 9 am – 10 am, Room number 12, Ground Floor, CNC OPD, AIIMS, New Delhi
Spine Clinic: Saturday 10 am – 12 pm, Room number 10, Ground Floor, CNC OPD, AIIMS, New Delhi
Inpatient : NSICU-B, NSICU-C 1stfloor, CN Center; NS-3 ward – 3rd floor, CN Center
Operation theatre : NS-OT, 1stfloor, CN Center
Publications
Total number of publications – 270 1 (February 2023)
Pubmed link -https://pubmed.ncbi.nlm.nih.gov/?term=kanwaljeet+garg
Following are some of his selected publications –
Functional
Spine
Radiosurgery
Peripheral nerve
Trauma
Vascular
Hydrocephalous
Resident Training
Oncology
Philosophy of community-based treatment
Community based drug treatment approach is a key strategy to reach out to individuals using alcohol and/or drugs, afflicted families and vulnerable groups who may not be able to avail these facilities on account of difficulty in access, social stigma and other factors. The advantage of community-based treatment is that treatment is available at the doorstep and flexibility can be maintained in delivery of services. It also facilitates family and community participation. Community based drug treatment is provided on an outpatient basis, and is managed with minimal staff with a ‘low threshold’ approach. The treatment services are located closer to the community, which makes it easy for the community to access the services needed for individuals in-need.
Treatment goals
The goals of these services are:
NDDTC has been implementing community-based treatment programmes at three locations in Delhi.
A. Community Clinic, Trilokpuri, New Delhi
(Faculty in-charge: Dr. Biswadip Chatterjee; Dr. Siddharth Sarkar)
Timings of clinic: 8.00 AM to 3.00 PM everyday
(Closed on Sunday & Holidays)
Address:
Community Drug Treatment Clinic
MIT Rotary Eye Hospital
All India Institute of Medical Sciences
Block 2, Trilokpuri
New Delhi – 110 091
Community Clinic, Trilokpuri, New Delhi was started in December 2003 as part of community drug treatment services of the National Drug Dependence Treatment Centre (NDDTC). The clinic was started to develop a model for low-cost, low-threshold treatment through availability of limited manpower and resources. Initially, a needs assessment survey was conducted. Awareness in the community was spread through locally acceptable methods such as drum announcements, information in the cable television and meetings with local leaders. The clinic in located in the heart of Trilokpuri and is easily accessible to people from Trilokpuri and adjoining areas.
Staff Team
A qualified and committed multidisciplinary team is managing the community clinic. The clinical staff includes faculty in charge (currently Dr Biswadip Chatterjee), one more faculty members, senior resident doctor (academic-pursuing DM (addiction psychiatry), Senior resident (non-academic) and junior resident doctor (pursuing MD, psychiatry), two staff nurses and a Medical Social Service Officer (MSSO). The ancillary staff includes medical record peon, an orderly and a guard and support staff. The doctors and the MSSO are available on two days in a week (Wednesday & Saturday). The other staff is available on all six working days.
Services at the clinic
The clinical staff assesses the new patients attending the clinic and formulates a management plan with immediate, short-term and long-term goals and objectives. Screening for the co-morbid medical illnesses is performed. Patients are referred to the nearest multi-specialty hospital for investigations for co-morbid physical illness, if required. In follow-up visits, patients are evaluated regularly and feedback is taken from the family members as well. In a few cases requiring admission, referral to NDDTC for admission is made.
The MSSOs are trained in psychosocial interventions including brief intervention, motivation enhancement, relapse prevention and family interventions. Home visits are made as and when required. The staff nurses in the Community Clinic, Trilokpuridispense medications to the patient, participate in psychosocial rehabilitation and provide support and care to patient and family members.
People served / catchment area
The catchment area of ‘Community Clinic, Trilokpuri, New Delhi’ includes the area in the radius of 5 kilometers. The patients and family members from these areas can seek advice and treatment for drug / alcohol problems at ‘Community Clinic, Trilokpuri’
Additional Activities that have been carried out so far
Profile of patients
On an average each month approximately 2000 patient visits are made in‘Community Clinic, Trilokpuri New Delhi’, that includes around 20 new patients and the rest are follow up cases. Approximately 70 patients visit daily. The majority of the follow up patients are Opioid dependent patients receiving agonist maintenance treatment (also known as Opioid Substitution Therapy, OST). For this purpose, various pharmacological options are used: buprenorphine, buprenorphine-naloxone, Slow Release Oral Morphine (SROM) etc. There are some opioid dependent patients on antagonist maintenance (Naltrexone) as well. Patients with Alcohol dependence are also treated using appropriate combination of psychosocial services and long-term medications (such as Disulfiram).
Services and facilities available
Ø Alcohol Dependence
o Outpatient detoxification (using benzodiazepines)
o Inpatient detoxification at NDDTC (referral)
o Long term pharmacotherapy
§ Deterrent medication: Disulfiram (dispensed free of cost)
§ Anticraving medication: Acamprosate (to be purchased by patient), Naltrexone
o Psychosocial interventions
Ø Opioid Dependence
o Outpatient detoxification
o Inpatient detoxification at NDDTC (referral)
o Long term pharmacotherapy (Free of cost)
§ Agonist maintenance: Buprenorphine (directly observed therapy), Morphine SR (directly observed therapy), Buprenorphine-naloxone
§ Antagonist: Naltrexone (directly observed therapy)
o Psychosocial interventions
Ø Nicotine Dependence
o Nicotine replacement therapy: Nicotine gum (to be purchased by patient)
o Bupropion and nortryptilline (to be purchased by patient)
o Psychosocial interventions
Ø Other drugs (benzodiazepine, inhalants, cannabis, etc.)
o Outpatient detoxification
o Inpatient detoxification at NDDTC (referral)
o Psychosocial interventions
Ø HIV/AIDS
o Pre and post test counseling
o Referral to nearest centre for testing (HIV, CD4, etc.) and antiretroviral medication (ART)
o Counseling and behavioral interventions with focus on harm reduction, condom usage and other safer practices
Ø Non-pharmacological interventions
o Instillation of hope
o Psychoeducation
o Motivational enhancement therapy
o Relapse prevention therapy
o Alternative therapies: Yoga
Ø Family interventions
o Psychoeducation
o Family counseling
Ø Social/community interventions
o Occupational rehabilitation facilities. Attempts are also made sometimes to facilitate provision of small financial help in the form of micro-credit to the needy patients.
o School based awareness
o Interactions with NGOs, local authorities (bank, post office, etc.), community leaders, etc.
Ø Other activities
o Training of doctors from government dispensaries
B. Community Outreach Clinic, SunderNagari, New Delhi
(Faculty in-charge: Dr. Ravindra Rao; Dr Roshan Bhad)
Timings of clinic: 8.00 AM to 3.00 PM everyday
(8.00 AM to 1.00 PM on Sunday & Holidays)
Address:
Community Drug Treatment Clinic,
Community Centre, DUSUB
F2 Block, Sunder Nagari
New Delhi - 110093
As a part of its community-based treatment program, NDDTC is also running a community buprenorphine based opioid substitution therapy clinic at Sunder Nagari, in New Delhi. The clinic was started in year 2003. This area is inhabited largely by people from lower socio-economic strata. The clinic is currently located in the premises of a community marriage hall managed by the Delhi Urban Shelter Improvement Board (DUSIB).
A unique feature of the clinic is that it is co-located with Methadone Clinic run by NDDTC as well as a Drop-in-Centre managed by a NGO implementing Targeted Interventions for Injecting Drug Users supported by National AIDS Control Organization through Delhi State AIDS Control Society. Currently, the clinic offers services to those individuals residing in 5 km radius of Sunder Nagari area only.
The clinic is managed by a doctor (senior resident), two nursing staff, and a MSSO, along with ancillary support staff, besides the faculty in-charge. The doctor and MSSO is available for three days (Monday, Thursday & Saturday), while other staff is available on all weekdays including public holidays.
The treatment philosophy and modality is similar to that followed in Trilokpuri community clinic, except for the fact that only opioid dependent individuals requiring long-term agonist maintenance treatment are catered to in this clinic. Both Buprenorphine and Methadone are available as a form of Opioid Substitution Therapy (OST) in this clinic. The doctor conducts an initial assessment and community-based services are provided to those requiring long-term agonist maintenance treatment. Other patients are referred to NDDTC, AIIMS for further treatment. Buprenorphine & Methadone is dispensed to the patients daily on a ‘Daily-Observed-Treatment’ basis.
Patients requiring other health related services such as general medical care, HIV testing, anti-retroviral treatment, tuberculosis diagnosis and treatment, etc. are referred to the nearest health facilities located in the vicinity. Similarly, tie-up with the NGO working in the premises is also done to ensure provision of harm reduction services as and when required.
The clinic has registered more than 1200 patients till date, and about 600 patients visit the clinic on a daily basis for their Buprenorphine & Methadone dose.
B1: Methadone Maintenance Treatment (MMT) Clinic, Sunder Nagari
(Faculty in-charge: Dr. Ravindra Rao, Dr Roshan Bhad)
Timings of clinic: 8.00 AM to 3.00 PM everyday
(8.00 AM to 1.00 PM on Sunday & Holidays)
Another new initiative at the Sunder Nagari Community, New Delhi is a Methadone Maintenance Treatment (MMT) clinic. This was initially a part of the project “Methadone Maintenance Treatment in India: A multi-site feasibility and effectiveness study” started. This treatment service has been initiated in India in August 2012 in five government hospitals (NDDTC, AIIMS; Civil Hospital Kapurthala; Civil Hospital, Bathinda; King Edward Memorial (KEM) Hospital, Mumbai and Regional Institute of Medical Sciences (RIMS), Imphal) with support from United Nations Office on Drugs and Crime (UNODC). This multi-site initiatives being coordinated by the National Drug Dependence Treatment Centre (NDDTC), AIIMS. MMT increases the treatment option for opioid dependent patients as this medication has been widely used across the world as an effective treatment and HIV risk reduction strategy. Through this initiative, procedures required for scale-up of Methadone Maintenance Treatment in the country will be documented.
The MMT clinic at Sunder Nagari has since been functional since August 2012. The clinic is located in the premises of a community marriage hall managed by the Delhi Urban Shelter Improvement Board (DUSIB). A doctor and MSSO are available for two days a week. The staff nurse, on the other hand, is available for all the days of the week, including Sundays, for dispensing of medicines at the clinic. Other ancillary staff is available on weekdays, while a guard is posted round-the-clock in the clinic premises.
Opioid dependent patients who require long-term agonist medication are catered to in this clinic. The doctor conducts assessment of the patients for their suitability to methadone, and prescribes methadone. Methadone is dispensed as a liquid by the nursing staff. The patients have to visit the clinic daily for their dose of methadone. The counselor conducts psychosocial assessment, motivation enhancement, family intervention, relapse prevention, psycho-education, and home visits, as required. A unique feature of the clinic is that it operates with an active collaboration with a NGO working with Injecting Drug Users, which provides the outreach services. Apart from direct services, referral services to other healthcare facilities in the vicinity are provided by the MMT clinic.
Since its inception in August 2012, the clinic has registered more than 1000 clients.
B2: Mobile Methadone Dispensing Units
Mobile dispensing units (Mobile Van) model has been implemented since March 2019 and currently services are being provided at two locations at different timings. Both the clinics are attended by 60-100 patients daily for Methadone Maintenance Programme
1. Seemapuri Location, East Delhi every day 8.30 AM-10.30 AM
2. Gokulpuri/Babarpur Location, East Delhi every day 11.00 AM-13.00 PM
C. Community Drug Treatment Clinic, Kotla Mubarakpur, New Delhi (Temporarily shifted to Sarai Kale Khan Night Shelter run by SPYM NGO)
This clinic was started as a part of DTC scheme under Drug De-Addiction Programme (DDAP) of Ministry of Health & Family Welfare, Government of India. The clinic was started in March 2017 and currently runs on Tuesday & Friday.
(Faculty in-charge:Prof Atul Ambekar; Dr. Alok Agrawal)
Timings of clinic: 8.00 AM to 3.00 PM everyday
(Closed on Sunday & Holidays)

Left to right(Standing): Shikha Roy, Ram Vikas Yadav, Mudassir Ali, Archna Singh, Dolly Rathore, Bhanupriya Awasthi, Sabiha Khan, Megha Suresh
Front(L to R): Nidhi Bailwal, Bindiya Jindal, Sakshi Shukla, Adeeba Malik.
Address: Room Nos. 3044 and 3046a,
Department of Biochemistry,
AIIMS, New Delhi.
Phone: 011-26593635; 26593478
Email id: arch_singh[at]ymail[dot]com, arch2574[at]gmail[dot]com
| Degree | University | Subject | Year |
|---|---|---|---|
| MBBS | Nalanda Medical College, Patna, India | Medicine, Surgery, Gynecology | 1998 |
| M.D. | All India Institute of Medical Sciences, Delhi, India | Biochemistry | 2004 |
| Ph. D | All India Institute of Medical Sciences, Delhi, India | Biochemistry | 2008 |
| MPH | University of Michigan, Ann Arbor, US | Environmental Health (Nutrition concentration) | 2008 |
| Sr. No. | Position held | Name of Institution/Place | From | To |
|---|---|---|---|---|
| 1 | Professor | All India Institute of Medical Sciences, New Delhi, India. | July 2023 | Present |
| 2 | Additional Professor | All India Institute of Medical Sciences, New Delhi, India. | July 2019 | June 2023 |
| 3 | Associate Professor | All India Institute of Medical Sciences, New Delhi, India. | July 2016 | June 2019 |
| 4 | Assistant Professor. | All India Institute of Medical Sciences, New Delhi, India | Nov 2012 | June 2015 |
| 5 | Assistant Professor | IIPH-D, Public Health Foundation of India, New Delhi, India. | Jan 2009 | Oct 2012 |
| 6 | Senior Resident | All India Institute of Medical Sciences, New Delhi, India | August 2004 | July 2007 |
| 7 | Junior Resident | All India Institute of Medical Sciences, New Delhi, India. | July 2001 | June 2004 |
1. Life Member of the Society for Mitochondrial Research and Medicine, India.
2. Life Member, Indian Association for Cancer Research.
3. Life Member of Immunology Society of India.
4. Life member of Association of Medical Biochemists of India
The broad research focus of my laboratory is on different aspects of lipid metabolism in cancer and obesity. Some of our research revolves around the role of ABCA1, involved in lipid efflux, in maintaining adipocyte homeostasis in obesity since we observed a lower gene expression of this transporter in the visceral adipose tissue of obese individuals. We are looking at pathways related to adipocyte ABCA1 and some lipid species like ceramides that could drive insulin resistance in obesity. We have also studied HDL’s function and quality concerning its key physiological roles i.e., in reverse cholesterol transport, antioxidative capacity, endothelial reactivity etc. We aim to understand the implications of changes in the quality of various HDL-associated molecules such as ApoA1 and Sphingosine-1-phosphate. Our cancer research focuses on analysing various aspects of metabolic reprogramming in pediatric B-ALL. We have recently found inter-tumor heterogeneity in the expression of lipid metabolism enzymes like ACSM3, and ACSL1 among pediatric B-ALL cases and we are planning to apply various approaches to understand the biological implications of this differential expression. Other avenues of interest include bioenergetics, mitochondrial biogenesis and factors regulating mitochondrial DNA copy number in leukemia.
The nutrition research in the lab extends into both the biochemical and public health domains in the context of the dietary quality and nutritional status of indigenous tribal communities of India. Our work among these communities encompasses food systems sustainability research and I am a collaborator on a recently awarded Team Science Grant on this theme in which my role is to develop successful diagnostic technologies for micronutrient assessment that can be feasible and cost-effective for assessing micronutrient status in these vulnerable communities. My interest extends to exploring the nutrient profiles of unique indigenous varieties of foods like mushrooms and indigenous rice varieties. We have also recently started work on a collaborative project with the Department of Cardiology and TGI, India for understanding the effect of foods on inflammatory biomarkers among CAD patients.
We are ably supported in our research work by experienced and sincere laboratory technicians. We are an enthusiastic research group, promoting collaborative work with various departments at AIIMS and between Institutes like IGIB and TGI, India. We endeavour to publish and disseminate our work across the global research community.
In keeping with our interest in metabolism, we enjoy experimenting with various cuisines and enjoy varied culinary experiences to rejuvenate ourselves occasionally.
We have a vibrant and enthusiastic team in the lab that is always striving to enhance their academic and extra-curricular skills.
Positions Available: Expected in January 2024.
Some Key publications:
Community based drug treatment approach is a key strategy to reach out to individuals using alcohol and/or drugs, afflicted families and vulnerable groups who may not be able to avail these facilities on account of difficulty in access, social stigma and other factors. The advantage of community-based treatment is that treatment is available at the doorstep and flexibility can be maintained in delivery of services. It also facilitates family and community participation. Community based drug treatment is provided on an outpatient basis, and is managed with minimal staff with a ‘low threshold’ approach. The treatment services are located closer to the community, which makes it easy for the community to access the services needed for individuals in-need.
The goals of these services are:
NDDTC has been implementing community-based treatment programmes at three locations in Delhi.
(Faculty in-charge: Dr. Biswadip Chatterjee; Dr. Siddharth Sarkar)
Timings of clinic: 8.00 AM to 3.00 PM everyday
(Closed on Sunday & Holidays)
Address:
Community Drug Treatment Clinic
MIT Rotary Eye Hospital
All India Institute of Medical Sciences
Block 2, Trilokpuri
New Delhi – 110 091
Community Clinic, Trilokpuri, New Delhi was started in December 2003 as part of community drug treatment services of the National Drug Dependence Treatment Centre (NDDTC). The clinic was started to develop a model for low-cost, low-threshold treatment through availability of limited manpower and resources. Initially, a needs assessment survey was conducted. Awareness in the community was spread through locally acceptable methods such as drum announcements, information in the cable television and meetings with local leaders. The clinic in located in the heart of Trilokpuri and is easily accessible to people from Trilokpuri and adjoining areas.
A qualified and committed multidisciplinary team is managing the community clinic. The clinical staff includes faculty in charge (currently Dr Biswadip Chatterjee), one more faculty members, senior resident doctor (academic-pursuing DM (addiction psychiatry), Senior resident (non-academic) and junior resident doctor (pursuing MD, psychiatry), two staff nurses and a Medical Social Service Officer (MSSO). The ancillary staff includes medical record peon, an orderly and a guard and support staff. The doctors and the MSSO are available on two days in a week (Wednesday & Saturday). The other staff is available on all six working days.
The clinical staff assesses the new patients attending the clinic and formulates a management plan with immediate, short-term and long-term goals and objectives. Screening for the co-morbid medical illnesses is performed. Patients are referred to the nearest multi-specialty hospital for investigations for co-morbid physical illness, if required. In follow-up visits, patients are evaluated regularly and feedback is taken from the family members as well. In a few cases requiring admission, referral to NDDTC for admission is made.
The MSSOs are trained in psychosocial interventions including brief intervention, motivation enhancement, relapse prevention and family interventions. Home visits are made as and when required. The staff nurses in the Community Clinic, Trilokpuridispense medications to the patient, participate in psychosocial rehabilitation and provide support and care to patient and family members.
The catchment area of ‘Community Clinic, Trilokpuri, New Delhi’ includes the area in the radius of 5 kilometers. The patients and family members from these areas can seek advice and treatment for drug / alcohol problems at ‘Community Clinic, Trilokpuri’
On an average each month approximately 2000 patient visits are made in‘Community Clinic, Trilokpuri New Delhi’, that includes around 20 new patients and the rest are follow up cases. Approximately 70 patients visit daily. The majority of the follow up patients are Opioid dependent patients receiving agonist maintenance treatment (also known as Opioid Substitution Therapy, OST). For this purpose, various pharmacological options are used: buprenorphine, buprenorphine-naloxone, Slow Release Oral Morphine (SROM) etc. There are some opioid dependent patients on antagonist maintenance (Naltrexone) as well. Patients with Alcohol dependence are also treated using appropriate combination of psychosocial services and long-term medications (such as Disulfiram).
Alcohol Dependence
Opioid Dependence
Nicotine Dependence
Other drugs (benzodiazepine, inhalants, cannabis, etc.)
HIV/AIDS
Non-pharmacological interventions
Family interventions
Social/community interventions
Other activities
(Faculty in-charge: Dr. Ravindra Rao; Dr Roshan Bhad)
Timings of clinic: 8.00 AM to 3.00 PM everyday
(8.00 AM to 1.00 PM on Sunday & Holidays)
Address:
Community Drug Treatment Clinic,
Community Centre, DUSUB
F2 Block, Sunder Nagari
New Delhi - 110093
As a part of its community-based treatment program, NDDTC is also running a community buprenorphine based opioid substitution therapy clinic at Sunder Nagari, in New Delhi. The clinic was started in year 2003. This area is inhabited largely by people from lower socio-economic strata. The clinic is currently located in the premises of a community marriage hall managed by the Delhi Urban Shelter Improvement Board (DUSIB).
A unique feature of the clinic is that it is co-located with Methadone Clinic run by NDDTC as well as a Drop-in-Centre managed by a NGO implementing Targeted Interventions for Injecting Drug Users supported by National AIDS Control Organization through Delhi State AIDS Control Society. Currently, the clinic offers services to those individuals residing in 5 km radius of Sunder Nagari area only.
The clinic is managed by a doctor (senior resident), two nursing staff, and a MSSO, along with ancillary support staff, besides the faculty in-charge. The doctor and MSSO is available for three days (Monday, Thursday & Saturday), while other staff is available on all weekdays including public holidays.
The treatment philosophy and modality is similar to that followed in Trilokpuri community clinic, except for the fact that only opioid dependent individuals requiring long-term agonist maintenance treatment are catered to in this clinic. Both Buprenorphine and Methadone are available as a form of Opioid Substitution Therapy (OST) in this clinic. The doctor conducts an initial assessment and community-based services are provided to those requiring long-term agonist maintenance treatment. Other patients are referred to NDDTC, AIIMS for further treatment. Buprenorphine & Methadone is dispensed to the patients daily on a ‘Daily-Observed-Treatment’ basis.
Patients requiring other health related services such as general medical care, HIV testing, anti-retroviral treatment, tuberculosis diagnosis and treatment, etc. are referred to the nearest health facilities located in the vicinity. Similarly, tie-up with the NGO working in the premises is also done to ensure provision of harm reduction services as and when required.
The clinic has registered more than 1200 patients till date, and about 600 patients visit the clinic on a daily basis for their Buprenorphine & Methadone dose.
B1: Methadone Maintenance Treatment (MMT) Clinic, Sunder Nagari
(Faculty in-charge: Dr. Ravindra Rao, Dr Roshan Bhad)
Timings of clinic: 8.00 AM to 3.00 PM everyday
(8.00 AM to 1.00 PM on Sunday & Holidays)
Another new initiative at the Sunder Nagari Community, New Delhi is a Methadone Maintenance Treatment (MMT) clinic. This was initially a part of the project “Methadone Maintenance Treatment in India: A multi-site feasibility and effectiveness study” started. This treatment service has been initiated in India in August 2012 in five government hospitals (NDDTC, AIIMS; Civil Hospital Kapurthala; Civil Hospital, Bathinda; King Edward Memorial (KEM) Hospital, Mumbai and Regional Institute of Medical Sciences (RIMS), Imphal) with support from United Nations Office on Drugs and Crime (UNODC) . This multi-site initiatives being coordinated by the National Drug Dependence Treatment Centre (NDDTC), AIIMS. MMT increases the treatment option for opioid dependent patients as this medication has been widely used across the world as an effective treatment and HIV risk reduction strategy. Through this initiative, procedures required for scale-up of Methadone Maintenance Treatment in the country will be documented.
support from United Nations Office on Drugs and Crime (UNODC)
The MMT clinic at Sunder Nagari has since been functional since August 2012. The clinic is located in the premises of a community marriage hall managed by the Delhi Urban Shelter Improvement Board (DUSIB). A doctor and MSSO are available for two days a week. The staff nurse, on the other hand, is available for all the days of the week, including Sundays, for dispensing of medicines at the clinic. Other ancillary staff is available on weekdays, while a guard is posted round-the-clock in the clinic premises.
Opioid dependent patients who require long-term agonist medication are catered to in this clinic. The doctor conducts assessment of the patients for their suitability to methadone, and prescribes methadone. Methadone is dispensed as a liquid by the nursing staff. The patients have to visit the clinic daily for their dose of methadone. The counselor conducts psychosocial assessment, motivation enhancement, family intervention, relapse prevention, psycho-education, and home visits, as required. A unique feature of the clinic is that it operates with an active collaboration with a NGO working with Injecting Drug Users, which provides the outreach services. Apart from direct services, referral services to other healthcare facilities in the vicinity are provided by the MMT clinic.
Since its inception in August 2012, the clinic has registered more than 1000 clients.
B2: Mobile Methadone Dispensing Units
Mobile dispensing units (Mobile Van) model has been implemented since March 2019 and currently services are being provided at two locations at different timings. Both the clinics are attended by 60-100 patients daily for Methadone Maintenance Programme
1. Seemapuri Location, East Delhi every day 8.30 AM-10.30 AM
2. Gokulpuri/Babarpur Location, East Delhi every day 11.00 AM-13.00 PM
This clinic was started as a part of DTC scheme under Drug De-Addiction Programme (DDAP) of Ministry of Health & Family Welfare, Government of India. The clinic was started in March 2017 and currently runs on Tuesday & Friday.
(Faculty in-charge:Prof Atul Ambekar; Dr. Alok Agrawal)
Timings of clinic: 8.00 AM to 3.00 PM everyday
(Closed on Sunday & Holidays)

Address: Room No. 3027A,
Department of Biochemistry,
AIIMS, New Delhi - 110029
Phone: +91-11-2659-4945
Email id: sudipsen665[at]gmail[dot]com
| Degree | Subject | University/ Institution | Year |
|---|---|---|---|
| Ph.D. | Biochemistry | AIIMS, New Delhi | 2007 |
| M.D. | Biochemistry | AIIMS, New Delhi | 2002 |
| M.B.B.S. | N.A. | N.R.S. Medical College, Calcutta | 1995 |
| Position | Department | University/ Institution | Dates |
|---|---|---|---|
| Professor | Biochemistry | AIIMS, New Delhi | 2022 – till date |
| Additional Professor | Biochemistry | AIIMS, New Delhi | 2018 – 2022 |
| Associate Professor | Biochemistry | AIIMS, New Delhi | 2015 – 2018 |
| Assistant Professor | Biochemistry | AIIMS, New Delhi | 2012 – 2015 |
| Assistant Professor | Biochemistry | UCMS, Delhi | 2009 – 2012 |
| DST Fast Track Fellow | Biochemistry & Ophthalmology | AIIMS, New Delhi | 2006 – 2009 |
We have developed an in-vitro model of cerebral palsy using fetal neural stem cells (FNSCs), in collaboration with NBRC, Manesar. This model is helping us identify the changes that occur during the disease process, and determine better ways by which we can prevent/treat cerebral palsy.
Currently enrolled Ph.D. scholars:
Positions Available: Contact by email to get the latest information.
The centre is also active in educating the public on substance use related issues and spreading awareness. Following are some of the activities in this area in the recent past:
Awareness generation programmes among industrial workers and management:
A symposium for general public on ‘workplace substance use and its management’ was organised by the centre in April 2006
Health education material has been published by the centre, in the form of pamphlets containing information about various substances of abuse, their consequences as well as treatment.
Besides these, the centre has also published health educational material for free distribution and download.



The centre is also active in educating the public on substance use related issues and spreading awareness. Following are some of the activities in this area in the recent past:
Awareness generation programmes among industrial workers and management:
A symposium for general public on ‘workplace substance use and its management’ was organised by the centre in April 2006
Health education material has been published by the centre, in the form of pamphlets containing information about various substances of abuse, their consequences as well as treatment.
Besides these, the centre has also published health educational material for free distribution and download.
Address: Room no 4007,
4th Floor, Convergence Block,
Department of Biochemistry,
All India Institute of medical Sciences, New Delhi
Phone: +91-11-26549235
Email id: kchosdol[at]gmail[dot]com, kunzangchosdol[at]yahoo[dot]com
| Degree | Subject | University/ Institution | Year |
|---|---|---|---|
| PhD | Biochemistry | AIIMS, New Delhi | 2007 |
| MD | Biochemistry | AIIMS, New Delhi | 1999 |
| MBBS & Internship | Medicine | Bundhelkhand University, Jhansi, UP | 1995 |
| Position | Department | University/ Institution | Dates |
|---|---|---|---|
| Professor | Biochemistry | All India Institute of Medical Science, New Delhi | 2014- Till date |
| Additional Professor | Biochemistry | All India Institute of Medical Science, New Delhi | 2010-2014 |
| Associate Professor | Biochemistry | All India Institute of Medical Science, New Delhi | 2007-2010 |
| Assistant Professor | Biochemistry | All India Institute of Medical Science, New Delhi | 2003-2007 |
| Senior Demonstrator | Biochemistry | All India Institute of Medical Science, New Delhi | 2000-2003 |
1. Indian Patent Application No. 1400/DEL/2013: Sinha S, Khan I, Zakaria MK, Chosdol K, Chattopadhyay P for the invention entitled “Placental like Alkaline Phosphatase (PLAP) Promoter Mediated Cell Targeting”
2. Indian patent, PCT-1282 (PCT/IB2013/05008): Chosdol K, Dikshit B and Sinha S: For the “Use of FAT1 gene and its products including RNA, protein and the derivatives of the same, as suitable molecules for either inflammation or cancer and the associated phenotype and the processes linking the same and also as a biomarker for the above processes”. International patent filed, PCT in process.
Research Funding Agencies: DST; DRDO; DBT; IMRG (AIIMS).
1.Dr. Khushboo Irshad, PhD - DST-SERB Young Scientist
Dr. Khushboo Irshad completed her PhD at the Department of Biochemistry, AIIMS, New Delhi, in 2013 under the supervision of Prof. Kunzang Chosdol, Prof. Subrata Sinha and Prof. P. Chattopadhyay. Her thesis involved the study of correlation between hypoxia and Notch signaling pathway in glioblastoma and identification of a combined gene signature to predict the survival of glioblastoma patients. Her work derived a key prognostic molecular cluster characteristic of the Notch pathway response in hypoxic glioblastoma tumors and gliomasphere cultures (PLoS One (2015); 10(3):e0118201; felicitated with AIIMS Excellence Research Award-2015 that was awarded to Prof. Chosdol). Presently, her research focuses on deciphering the role of FAT1, a novel gene implicated in glioma, in regulating the hallmark features of glioma like stemness and invasiveness, as well as in maintenance of the balance between pro-inflammatory and anti-inflammatory signaling in glioma. She was awarded the DST-SERB Start-Up Research Grant in March 2016, for the project aimed at elucidation of FAT1 function in modulating pro-inflammatory signaling and anti-inflammatory / immunosuppressive signaling pathways in glioma.
2.Dr. SRINIVAS H, MD,DNB (PhD)
Dr. Srinivas H done MBBS from Bangalore Medical college, Rajiv gandhi university of health sciences Karnataka and MD from MAULANA AZAD Medical College, Delhi university, New Delhi. His MD thesis was on procalcitonin, IL 6, TNFalpha and urinary isoprostane in sepsis patients under the guidance of ex HOD and director professor Dr TK Mishra. He has completed one year of senior residency in PGIMER, Chandigarh and two year of senior residency in AIIMS, New Delhi. He has published his work in national and international papers in the various field of sciences and medical education. He is working now on pathway analysis of interaction between FAT1 with p53, HIF 1alpha and beta catenin in glioma as a PhD research scholar under the guidance of Dr KUNZANG CHOSDOL and Dr SUBRATA SINHA. He has done DNB from Diplomate of National Board in biochemistry and certification course in industry program, clinical trials and administration from bioinformatics institute of India. He is a Life member of Association of Medical Biochemistry of India since 2008
Life member of Society for Tissue Engineering and Regenerative Medicine (India), Thiruvananthapuram since 2010 and Indian Association of Cancer Research.
3.Ms. Chitrangda Srivastava - PhD scholar
Ms. Chitrangda Srivastava is currently in her final year of PhD. She is working on the characterization of FAT1 gene promoter. In addition, she is analyzing the functional role of FAT1 with EMT and stemness in hypoxic glioma. She completed her M.Sc. from the department of Biochemistry, AIIMS, in 2012. Her M.Sc. thesis involved the study of the role of Notch signalling pathway with EMT and stemness in pathogenesis of glioma under hypoxia. She has won several awards during her PhD tenure, including Best Oral Presentation Award in ACOS-2016, European Young Scientist Travel Award-2015, G.P. Talwar Foundation Travel Award-2015, etc. She is an Associate Member of the American Association of Cancer Research since 2011 and an Associate Member of the European Society of Neuro-Oncology since 2016.
4.Nargis Malik, PhD. Scholar
Nargis Malik completed her M.Sc. in toxicology from Meerut University, Currently she is a second year PhD. student working on the “Role of FAT1 gene on the regulation of microRNAs in glioma”
5.Ms. AKANKSHA KANOJIA, M.Sc. student
Akanksha Kanojia has completed her B.Sc.(H) in Biomedical Sciences from Acharya Narendra Dev College, University of Delhi in 2016. She is currently pursuing M.Sc. in Biochemistry from All India Institute of Medical Science, Delhi under the guidance of Dr. Kunzang Chosdol.
Mukesh Kumar (Laboratory Attendant Gr. II)
Mukesh Kumar is working as a Laboratory Attendant Gr.-II in the Department of Biochemistry since August 2011. He help in the research related work for M.Sc., Ph.D. and M.D. Students in Research Laboratory of Dr. Parthaprasad Chattopadhyay & Dr. Kunzang Chosdol. His nature of duties includes, culture work, DEPC treatment and assistance of UG/PG examination.
The centre has well equipped laboratories for detecting health consequences of substance use as well as detecting presence of various drugs of abuse in the body fluids. Screening of Urine to detect presence of drugs of abuse is routinely performed as a part of the patient-care in the centre. Following are some of the statistics on laboratory tests conducted in the centre in the recent past.
Yearly record of Biochemistry Laboratory (April 2015 to March 2016)
1.) Biochemistry Tests = 24994
2.) Hematological = 7393
3.) HIV Investigations = 91
| Drugs | Nos. | |
|---|---|---|
| Morphine Test | 3781 | |
| Codeine Test | 2536 | |
| Buprenorphine Test | 3301 | |
| Proxyvon Test | 2721 | |
| Avil Test | 2536 | |
| Naltrexone Test | 2536 | |
| Pentazocine Test | 2736 | |
| Benzodiazépines Test | 6372 | |
| Barbiturates Test | 40 | |
| Cocaine Test | 40 | |
| Cannabis Test | 935 | |
| Cotinine Test | 40 | |
| Inhalants | 25 | |
| Total number of drugs tested in urine | 27624 | |
CURRICULUM VITAE
Name : Dr. Hitesh kumar Gurjar
Permanent Address : 522, Masjid moth Doctors Hostel,
AIIMS, NewDelhi-110049
Phone - +91-11-26258219/+91-9968582218
E-mail :hieshgurjar[at]gmail[dot]com
hitesh_gurjar[at]yahoo[dot]com
Academic Qualifications : M.B.B.S.
M.Ch (Neurosurgery)
Current Position : Assistant Professor, Department of Neurosurgery,
All India Institute of Medical Sciences, New Delhi, India
Academic Record
| College/University | Year of Passing | Distinction/Honours | |
|---|---|---|---|
| M.B.B.S. | All India Institute of Medical Sciences | Dec.2004 | Gold Medal in Microbiology |
| M.Ch.(Neurosurgery) | All India Institute of Medical Sciences | Dec.2009 | - |
Professional/Clinical Experience:
Courses Attended:
4. midas rex training course held at aiims in March 2010
Research Papers / Dissertations:
Publication
Papers Published :
1. Role of Invasive ICP Monitoring in Patients with Traumatic Brain Injury: An Experience of 98 Cases (2006)
Deepak Kumar Gupta , Hitesh Kumar, AK Mahapatra,
Indian Journal of Neurotrauma (IJN3T1), 2006, Vol. 3, No. 1, pp. 31-36
2. Cerebellar hemorrhage following endoscopic third ventricular colloid cyst decompression.
Gurjar H, Dwarakanath S, Sharma BS, Chandra S, Neurol India, 2008 April-Jun;56(2):218-20
3. Large Pontine Tubercular Abscess Treated Surgically
Gurjar HK, Joshua SP, Agrawal D, Mahapatra AK Br J Neurosurg. 2012 Jul 17.
4. Multicentric intracranial epidermoid or epi/dermoid cysts?
Goyal N, Sharma MS, Gurjar H, Mahapatra AK. Acta Neurochir (Wien). 2012 Jul;154(7):1285-6. Epub 2012 Apr 29
5. Cranioplasty following decompressive craniectomy in traumatic brain injury: Experience at Level — I apex trauma centre Noufal Basheer, Deepak Gupta, AK Mahapatra, Hitesh Gurjar
The Indian Journal of Neurotrauma December 2010(Vol. 7, Issue 2,Pages 139-144)
6. Survival after a penetrating injury traversing midbrain - case report
Br J Neurosurg. 2010 Aug;24(4):477-8
Papers and Posters Presented:
1. Prolactinomas: surgical management and controversies. Oral presentation at NSI conference held at Agra(U.P.) in dec. 2007
2. Os Odontoideum: experience of 34 cases. Oral presentation at “spine 2010”-an International conference of Neuro Spinal Surgeons Foundation of India, held at Indore India
3. Rare CPA lesions: report of 4 cases. Poster presentation at 9th Annual Conference of SBSSI and WFNS Skull Base study group Workshop, Hands on Cadaveric workshop at AIIMS, New Delhi, October 2007.
Conferences and Workshops Attended:
The centre has well equipped laboratories for detecting health consequences of substance use as well as detecting presence of various drugs of abuse in the body fluids. Screening of Urine to detect presence of drugs of abuse is routinely performed as a part of the patient-care in the centre. Following are some of the statistics on laboratory tests conducted in the centre in the recent past.
1. Biochemistry Tests = 24994
2. Hematological = 7393
3. HIV Investigations = 91
| Drugs | Nos. | |
|---|---|---|
| Morphine Test | 3781 | |
| Codeine Test | 2536 | |
| Buprenorphine Test | 3301 | |
| Proxyvon Test | 2721 | |
| Avil Test | 2536 | |
| Naltrexone Test | 2536 | |
| Pentazocine Test | 2736 | |
| Benzodiazépines Test | 6372 | |
| Barbiturates Test | 40 | |
| Cocaine Test | 40 | |
| Cannabis Test | 935 | |
| Cotinine Test | 40 | |
| Inhalants | 25 | |
| Total number of drugs tested in urine | 27624 | |
| Sr No | Image | Name | Description |
|---|---|---|---|
| 1 |  | DR. SUSHMA BHATNAGAR, MD | Professor and HeadAreas of Interest
Email: sushmabhatnagar1[at]gmail[dot]com Mobile: +91-9811326453 OPD Days (PAC and Pain Clinic):
|
| 2 |  | Dr. Seema Mishra, MD | ProfessorAreas of Interest
Email: seemamishra2003[at]gmail[dot]com Office:Office: Room No. 249, Second Floor, Dr BRAIRCH, AIIMS OPD Days (PAC and Pain Clinic):
|
| 3 | | Dr Rakesh Garg, MD, DNB, MNAMS, PGCCHM, FICCM, FIMSA, FICA, NFPM, | ProfessorAreas of Interest
Contact : drrgarg[at]hotmail[dot]com Mobile: +91-9810394950 OPD Days (PAC and Pain Clinic):
|
| 4 |  | Dr. Nishkarsh Gupta, MD, DNB, MNAMS, PGCCHM | ProfessorAreas of Interest
Contact : drnishkarsh[at]rediffmail[dot]com Mobile: +91-9868398338 Office: Room No. 139, First Floor, Dr BRAIRCH, AIIMS OPD Days (PAC and Pain Clinic):
|
| 5 |  | Dr Sachidanand Jee Bharati, MD, DM (Neuroanaesthesia) | ProfessorAreas of Interest
Contact : sacidadr[at]yahoo[dot]co[dot]in Mobile: +91-9868398337 Office: Office: Room No. 139, First Floor, Dr BRA IRCH, AIIMS OPD Days (PAC and Pain Clinic):
|
| 6 |  | Dr. Vinod Kumar, MD | ProfessorAreas of Interest
Contact : vkchanpadia[at]gmail[dot]com Mobile: +91-9868398336 Office: Room No. 139, First Floor, Dr BRA IRCH, AIIMS. OPD Days (PAC and Pain Clinic):
|
| 7 |  | Dr. Brijesh Kr. Ratre, MD | Assistant ProfessorAreas of Interest
Contact : brajesh.ratre[at]gmail[dot]com Mobile: +91-8696156799 Office: Room No. 135, First Floor, Dr BRA IRCH, AIIMS OPD Days (PAC and Pain Clinic): |
| 8 |  | Dr. Shweta Arun Bhopale, MD | Assistant ProfessorAreas of Interest
Contact : dr.shweta610ab[at]gmail[dot]com Mobile: +91-9028900479 Office: Room no. 18, First Floor Academic Block, NCI-AIIMS, Jhajjar Phone: 01251274769 OPD Days (PAC and Pain Clinic):
|
| 9 |  | Dr. Anuja Pandit, MD (Gold medalist), DM (Onco-Anaesthesia) | Assistant ProfessorAreas of Interest
Contact : anujapandit[at]yahoo[dot]co[dot]in Mobile: +91-9710030457 Office: Room No. 4, First Floor, Academic Block, National Cancer Institute, AIIMS, Jhajjar OPD Days (PAC and Pain Clinic):
|
| 10 |  | Dr Balbir Kumar, MD | Assistant ProfessorAreas of Interest
Contact : drbalbir10[at]gmail[dot]com Mobile : +91-7087432124 Office : Room No.19, First Floor Academic Block NCI-AIIMS New Delhi Phone : 01251274769 OPD Days (PAC and Pain Clinic and DMG):
|
| 11 |  | Dr. Saurabh Vig, MD, DM (Onco-Anaesthesia) | Assistant ProfessorAreas of Interest
Contact : saurabh377[at]yahoo[dot]com Office: Room No 10, first floor, Academic block, National Cancer Institute, AIIMS, Jhajjar OPD Days (PAC and Pain Clinic):
|
| 12 |  | Dr. Raghav Gupta, MBBS, DNB (Anesthesia), MNAMS, DM (Onco-Anesthesia), A.FAMS, IDRA | Assistant ProfessorAreas of Interest
Contact : raghavgupta88[at]gmail[dot]com Mobile: +91-8130622963, +918860297649 Office: Room No. 126, First Floor, Academic Block, National Cancer Institute (Jhajjar) AIIMS, New Delhi |
| 13 |  | Dr. Prashant Sirohiya, MD, DNB | Assistant ProfessorAreas of Interest
Mobile: +91-8824090277 Office: Room No. 177, First Floor Academic Block, National Cancer Institute, Badsa, Jhajjar |
In-Patient Services
Ø The centre has a well-equipped 50-bedded hospital.
Ø The hospital has provisions for admitting patients with all kinds of substance use disorders.
Ø There is also provision for treatment of those with special needs such as women drug users, adolescent drug users, drug users with dual-diagnosis (substance use disorder along with a psychiatric illness) etc.
Ø The hospital is adequately staffed with round the clock availability of doctors, nurses as well as paramedical staff.
Ø During the inpatient stay the patients receive comprehensive care and treatment from staff trained in medical, nursing, psychological and social-services background.
Ø The admission is purely on a voluntary basis and only with the consent of the patient.
Ø The hospital is strictly a no-smoking zone.
Ø The hospitalisation charges are approximately Rs. 37/- per day (to be deposited at the time of admission for 15 days, i.e. a sum of Rs. 550/-). For poor patients, these charges can be waived-off.
Ø The outpatient clinic of the centre functions from Monday to Friday.
Ø Both, new as well as old patients are seen in the outpatient department.
Ø TheOPD registration timings are from 9:00 AM to 11:30 AM.
Ø No referral from anywhere is required. The patients are expected to get registered at the registration counter and wait for their turn in the waiting area.
Ø The registration fee for new patients is Rs. 10/- only (valid for the duration of one year). There is no fee for subsequent (follow-up) visits.
Click here for our Clinical care statistics
Recently the centre has introduced three specialty clinics. These are
(i) Tobacco Use Cessation,
(ii) Adolescent Drug Use Clinic
(iii) Dual Diagnosis Clinic (Substance Use Disorder and Psychiatric Illness)
Tobacco Cessation Clinic (TCC) (Faculty in-charge:Dr. S. Jhanjee; Dr.PrabhuDayal; Dr Gauri ShankerKaloiya)
Tobacco is a powerfully addictive drug and is a major preventable cause of
morbidity and mortality. A focused approach on tobacco cessation greatly
helps patients to quit this harmful addiction. To help patients quit tobacco use, NDDTC offers Tobacco cessation clinic in the OPD on every Monday at 9.00 A.M. This clinic offers pharmacotherapy, psycho-education and counseling services.
Adolescent Clinic (Faculty in-charge:Dr. Anju Dhawan; Dr Rachana Bhargava; DrBiswadip Chatterjee; DrPiyali Mandal)
A growing number of adolescents are falling prey to substance use. Since this group of population has special treatment needs the centre offers a specialty clinic the Adolescent Drug Use Clinic, every Tuesday at 9:00 AM in the OPD.
Dual Diagnosis Clinic (Faculty in-charge: Dr. Rakesh Lal; Dr. Yatan Pal Singh Balhara; Dr Siddharth Sarkar)
Many people who are dependent on psychoactive drugs suffer simultaneously from mental (psychiatric) disorders. “Dual Diagnosis” is the term commonly used to describe this group of patients. Since this group has special needs for treatment, a specialty clinic is functional to cater to this group of patients, every Wednesday at 9:00 AM at NDDTCOPD
Women Clinic (Faculty-in-charge: Dr AtulAmbekar; DrPiyali Mandal)
Substance use disorders are increasingly being recognized among women. Keeping in mind the special needs of women substance users a clinic has been started at NDDTCOPD on Saturdays from 9:00 am onwards.
Behavioural Addictions Clinic (BAC) (Faculty in-charge: Dr. Yatan Pal Singh Balhara; Dr Rachana Bhargava)
The Behavioral Addictions Clinic (BAC) is aimed at catering to those experiencing behavioral addictions. This includes various conditions including Internet addiction, (video) gaming addiction, smartphone addiction, screen addiction, excessive use of social media, pathological gambling among others. The clinic offers treatment services for the behavioral addictions and the co-occurring psychiatric and substance use disorders that are commonly observed in this population.
Dual Diagnosis Clinic at AIIMS, New Delhi campus (Faculty in-charge: Dr. Yatan Pal Singh Balhara)
The Dual Diagnosis Clinic is aimed at catering to the needs of those suffering from co-occurring disorders. This includes those who have medical disorder or psychiatric disorder in addition to the substance use (addictive) disorders. Some of the commonly seen co-occurring disorders in the clinic include alcoholic liver disease, diabetes, viral hepatitis, cancers, depression, anxiety disorders, psychosis, co-occurring with alcohol, cannabis, opioids (heroin and prescription opioids), tobacco and benzodiazepine use disorders. The clinic offers medicine based (pharmacological) as well as psycho-social treatment for the co-occurring disorders.
| Days | OPD Services | Ward | ||
|---|---|---|---|---|
Unit 1 Prof Rakesh Chadda, Chief, NDDTC Prof Atul Ambekar Dr Prabhu Dayal Dr Alok Agrawal Dr Piyali Mandal Walk-in Admission Days: Wednesday & Saturday | Unit II Prof Rakesh Lal Prof Sonali Jhanjee Dr Ravindra Rao Dr Roshan Bhad Dr Shalini Singh Walk-in Admission Days: Tuesday & Friday | Unit III Prof Anju Dhawan Dr Yatan Pal Singh Balhara Dr. Biswadip Chatterjee Dr. Siddharth Sarkar
Walk-in Admission Days: Monday & Thursday | ||
| General OPD | Specialty OPD | Community Clinic | Rounds | |
| Monday | Unit III | Tobacco Cessation Clinic (TCC)
| Sundernagari Community Outreach Clinic | Unit III (Service Rounds : |
Prof Anju Dhawan Dr Biswadip Chatterjee | Prof Sonali Jhanjee (In-charge) Dr Prabhu Dayal Dr Gauri Shanker Kaloiya | Dr Roshan Bhad | ||
| Tuesday | UNIT II | Adolescent Clinic | Sarai Kale Khan Community Clinic | Unit I (Service Rounds : |
Prof Rakesh Lal Dr Ravindra Rao | Prof Anju Dhawan (In-charge) Dr Rachna Bhargava Dr Biswadip Chatterjee Dr Piyali Mandal | Dr Alok Aggarwal | ||
| Consultation Liaison Addiction Psychiatry (CLAP) Clinic at AIIMS, New Delhi | ||||
| Dr Roshan Bhad | ||||
| Wednesday | UNIT I | Dual Diagnosis Clinic (DDC) | Trilokpuri Community Clinic | Unit II Grand Rounds |
Dr Prabhu Dayal Dr Gauri Shanker Kaloiya Dr Alok Agrawal Dr Piyali Mandal | Dr Yatan Pal Singh Balhara Dr Siddharth Sarkar | Dr Biswadip Chatterjee | ||
| Consultation Liaison Addiction Psychiatry (CLAP) Clinic at AIIMS, New Delhi | ||||
| Dr Shalini Singh | ||||
| Thursday | Unit III | Family Empowerment Clinic (FEC) | Sundernagari Community Outreach Clinic | Unit I Grand Rounds |
Dr Yatan Pal Singh Balhara Dr Siddharth Sarkar | Dr Gauri Shanker Kaloiya Dr Siddharth Sarkar | Dr Ravindra Rao | ||
| Friday | UNIT II | Sarai Kale Khan Community Clinic | Unit III Grand Rounds | |
Prof Rakesh Lal Prof Sonali Jhanjee Dr Rachna Bhargava Dr Roshan Bhad Dr Shalini Singh | Prof Atul Ambekar (In-charge) | |||
| Saturday | UNIT I | Women’s Clinic | Trilokpuri Community Clinic | Unit II (Service Rounds : |
Prof Atul Ambekar Dr Prabhu Dayal Dr Alok Agrawal | Prof Atul Ambekar Dr Piyali Mandal | Dr Siddharth Sarkar | ||
| Behavioral Addictions Clinic (at AIIMS, New Delhi) | ||||
Dr Yatan Pal Singh Balhara Dr Rachna Bhargava | ||||
| Consultation Liaison Addiction Psychiatry (CLAP) Clinic at AIIMS, New Delhi | ||||
| Dr Ravindra Rao | ||||
| Psychology clinical services: Referral to a clinical psychology faculty to be decided based upon the corresponding F/U day of the treating psychiatry faculty: Mon / Wed / Thu for Dr. Kaloiya and Tue / Fri/Sat for Dr. Bhargava | ||||
Methadone Mobile Dispensing Unit will be stationed at *
*Timings and locations are subject to change | ||||
Click here for our Clinical care statistics
Recently the centre has introduced three specialty clinics. These are
(1) Tobacco Use Cessation,
(2) Adolescent Drug Use Clinic
(3) Dual Diagnosis Clinic (Substance Use Disorder and Psychiatric Illness)
(Faculty in-charge:Dr. S. Jhanjee; Dr.PrabhuDayal; Dr Gauri ShankerKaloiya)
Tobacco is a powerfully addictive drug and is a major preventable cause of
morbidity and mortality. A focused approach on tobacco cessation greatly
helps patients to quit this harmful addiction. To help patients quit tobacco use, NDDTC offers Tobacco cessation clinic in the OPD on every Monday at 9.00 A.M. This clinic offers pharmacotherapy, psycho-education and counseling services.
(Faculty in-charge:Dr. Anju Dhawan; Dr Rachana Bhargava; DrBiswadip Chatterjee; DrPiyali Mandal)
A growing number of adolescents are falling prey to substance use. Since this group of population has special treatment needs the centre offers a specialty clinic the Adolescent Drug Use Clinic, every Tuesday at 9:00 AM in the OPD.
(Faculty in-charge: Dr. Rakesh Lal; Dr. Yatan Pal Singh Balhara; Dr Siddharth Sarkar)
Many people who are dependent on psychoactive drugs suffer simultaneously from mental (psychiatric) disorders. “Dual Diagnosis” is the term commonly used to describe this group of patients. Since this group has special needs for treatment, a specialty clinic is functional to cater to this group of patients, every Wednesday at 9:00 AM at NDDTCOPD
(Faculty-in-charge: Dr AtulAmbekar; DrPiyali Mandal)
Substance use disorders are increasingly being recognized among women. Keeping in mind the special needs of women substance users a clinic has been started at NDDTCOPD on Saturdays from 9:00 am onwards.
(Faculty in-charge: Dr. Yatan Pal Singh Balhara; Dr Rachana Bhargava)
The Behavioral Addictions Clinic (BAC) is aimed at catering to those experiencing behavioral addictions. This includes various conditions including Internet addiction, (video) gaming addiction, smartphone addiction, screen addiction, excessive use of social media, pathological gambling among others. The clinic offers treatment services for the behavioral addictions and the co-occurring psychiatric and substance use disorders that are commonly observed in this population.
(Faculty in-charge: Dr. Yatan Pal Singh Balhara)
The Dual Diagnosis Clinic is aimed at catering to the needs of those suffering from co-occurring disorders. This includes those who have medical disorder or psychiatric disorder in addition to the substance use (addictive) disorders. Some of the commonly seen co-occurring disorders in the clinic include alcoholic liver disease, diabetes, viral hepatitis, cancers, depression, anxiety disorders, psychosis, co-occurring with alcohol, cannabis, opioids (heroin and prescription opioids), tobacco and benzodiazepine use disorders. The clinic offers medicine based (pharmacological) as well as psycho-social treatment for the co-occurring disorders.
| Days | OPD Services | Ward | ||
|---|---|---|---|---|
Unit 1 Prof Rakesh Chadda, Chief, NDDTC Prof Atul Ambekar Dr Prabhu Dayal Dr Alok Agrawal Dr Piyali Mandal Walk-in Admission Days: Wednesday & Saturday | Unit II Prof Rakesh Lal Prof Sonali Jhanjee Dr Ravindra Rao Dr Roshan Bhad Dr Shalini Singh Walk-in Admission Days: Tuesday & Friday | Unit III Prof Anju Dhawan Dr Yatan Pal Singh Balhara Dr. Biswadip Chatterjee Dr. Siddharth Sarkar
Walk-in Admission Days: Monday & Thursday | ||
| General OPD | Specialty OPD | Community Clinic | Rounds | |
| Monday | Unit III | Tobacco Cessation Clinic (TCC)
| Sundernagari Community Outreach Clinic | Unit III (Service Rounds : |
Prof Anju Dhawan Dr Biswadip Chatterjee | Prof Sonali Jhanjee (In-charge) Dr Prabhu Dayal Dr Gauri Shanker Kaloiya | Dr Roshan Bhad | ||
| Tuesday | UNIT II | Adolescent Clinic | Sarai Kale Khan Community Clinic | Unit I (Service Rounds : |
Prof Rakesh Lal Dr Ravindra Rao | Prof Anju Dhawan (In-charge) Dr Rachna Bhargava Dr Biswadip Chatterjee Dr Piyali Mandal | Dr Alok Aggarwal | ||
| Consultation Liaison Addiction Psychiatry (CLAP) Clinic at AIIMS, New Delhi | ||||
| Dr Roshan Bhad | ||||
| Wednesday | UNIT I | Dual Diagnosis Clinic (DDC) | Trilokpuri Community Clinic | Unit II Grand Rounds |
Dr Prabhu Dayal Dr Gauri Shanker Kaloiya Dr Alok Agrawal Dr Piyali Mandal | Dr Yatan Pal Singh Balhara Dr Siddharth Sarkar | Dr Biswadip Chatterjee | ||
| Consultation Liaison Addiction Psychiatry (CLAP) Clinic at AIIMS, New Delhi | ||||
| Dr Shalini Singh | ||||
| Thursday | Unit III | Family Empowerment Clinic (FEC) | Sundernagari Community Outreach Clinic | Unit I Grand Rounds |
Dr Yatan Pal Singh Balhara Dr Siddharth Sarkar | Dr Gauri Shanker Kaloiya Dr Siddharth Sarkar | Dr Ravindra Rao | ||
| Friday | UNIT II | Sarai Kale Khan Community Clinic | Unit III Grand Rounds | |
Prof Rakesh Lal Prof Sonali Jhanjee Dr Rachna Bhargava Dr Roshan Bhad Dr Shalini Singh | Prof Atul Ambekar (In-charge) | |||
| Saturday | UNIT I | Women’s Clinic | Trilokpuri Community Clinic | Unit II (Service Rounds : |
Prof Atul Ambekar Dr Prabhu Dayal Dr Alok Agrawal | Prof Atul Ambekar Dr Piyali Mandal | Dr Siddharth Sarkar | ||
| Behavioral Addictions Clinic (at AIIMS, New Delhi) | ||||
Dr Yatan Pal Singh Balhara Dr Rachna Bhargava | ||||
| Consultation Liaison Addiction Psychiatry (CLAP) Clinic at AIIMS, New Delhi | ||||
| Dr Ravindra Rao | ||||
| Psychology clinical services: Referral to a clinical psychology faculty to be decided based upon the corresponding F/U day of the treating psychiatry faculty: Mon / Wed / Thu for Dr. Kaloiya and Tue / Fri/Sat for Dr. Bhargava | ||||
Methadone Mobile Dispensing Unit will be stationed at *
*Timings and locations are subject to change | ||||
The centre provides training to the medical, nursing and psychology students of the All India Institute of Medical Sciences. Clinical posting to the centre is a part of the curricula for the following courses:
Besides these the centre has also been involved in providing training to various categories of staff throughout the country and out-side the country through its training programmes. Manuals for doctors have also been developed and are available for free download.
| Account Name | Director, AIIMS New Delhi |
| Bank Name | State Bank of India |
| Branch | Ansari Nagar, New Delhi 110029, India |
| Account Number | 10874584010 |
| IFSC Code | SBIN0001536 |
| MICR Code | 110002005000085 |
The centre provides training to the medical, nursing and psychology students of the All India Institute of Medical Sciences. Clinical posting to the centre is a part of the curricula for the following courses:
Besides these the centre has also been involved in providing training to various categories of staff throughout the country and out-side the country through its training programmes. Manuals for doctors have also been developed and are available for free download.
One of the primary mandates of the centre is to build capacities of human resources in the country in the area of substance use disorders. The centre has been involved in providing training to doctors and other categories of staff members since 1989. The centre has developed curricula, training schedules, modalities and resource materials for training of trainers, Medical Doctors (GDMOs), nurses and laboratory personnel. The training programmes have been reviewed and modified through workshops of resource persons. Some of the training programmes organised by the centre in the recent past include:
Note: The resource persons for all these training programmes include the faculty and staff members of NDDTC. Faculty members from other institutes are also sometimes invited as resource persons for the training.
The centre has completed project focused on training of doctors in the area of substance use disorders. The project envisaged imparting training to at least one doctor in each of the district hospital in the country, so that close to 350 doctors of country received training over a period of three years. This project was funded by the National Fund for Control of Drug Abuse (NFCDA), Department of Revenue, Ministry of Finance, Government of India. Other institutes collaborating with NDDTC, AIIMS in this venture included:
Besides these, the faculty from the centre has also been involved in providing training to doctors, nurses, project managers and counsellors from various other organisations. These include the NGOs supported by the Ministry of Social Justice and Empowerment, National Institute of Social Defence, Regional Resource and Training Centres, National Institute of Criminology and Forensic Sciences, National AIDS Control Organisation, State AIDS Control Societies etc.
The centre has also produced resource material in the form of manuals for training. These manuals are distributed to the participants during training programmes. In addition these manuals are also available for free download.
The centre has been involved in providing training to doctors and other categories of staff members since 1989. The centre has developed curricula, training schedules, modalities and resource materials for training of trainers, Medical Doctors (GDMOs), nurses and laboratory personnel. Between January 1989 and October 2007, about 40 courses for doctors have been organised. Various manuals are available. The training programmes have been reviewed and modified through workshops of resource persons.
NAUGRATION OF CIMR BY SH J P NADDA (FORMER HEALTH MINISTER)
A. IDY GALLERY (2017-18)
A. IDY GALLERY (2017-18)
DR H R NAGENDRA, DR S C MANCHANDA WITH DR RANDEEP GULERIA DURING IDY 2017
B.IDY GALLERY (2018-19)
B.IDY GALLERY (2018-19)
Training Program on “Self Management of Excessive Tension (SMET)” for AIIMS Faculty Members
Training programme on “Self Management of Excessive Tension (SMET)” for AIIMS Scholars & Research Fellows
BASIC YOGA TRAINING FOR SCHOOL STUDENTS ON “INSTITUTE DAY"
BASIC YOGA TRAINING FOR SCHOOL STUDENTS ON “INSTITUTE DAY"
ON LINE SESSIONS DURING PANDEMIC
EXPERT GROUP MEETING ON INTEGRATIVE MEDICINE
Dr Gautam Sharma, CIMR and Robert Svoboda, Ramkumar, Hansaji J Yogendra in conversation with Michael Menezes during “JAIPUR LITERATURE FESTIVAL”
VISIT AT CIMR BY SECRETARY, MINISTRY OF AYUSH
DURING ORIENTATION PROGRAMME FOR AYURVEDA RESEARCHERS WITH PROFESSOR TANUJA NESHRI,DIRECTOR , ALL INDIA INSTITUTE OF AYURVEDA NEW DELHI
VISIT BY DELEGATES FROM AUSTARLIA AT CIMR ,AIIMS NEW DELHI
NATIONAL AYURVEDA DAY CELEBERATION
Tree plantation (Saraca asoca Roxb.) planted by Prof. Randeep Guleria ( Director, AIIMS, New Delhi) on 19th June 2022
Inter-institutional Yoga Quiz competition -2022
Mass Yoga practice on 8th International day of Yoga 21st June 2022
Mass Yoga practice on 8th International day of Yoga 21st June 2022
SWAYAM Workshop for Nursing Staff of AIIMS, New Delhi -2022
1. GLIMPSES OF CIMR VISIT BY SMT ANUPRIYA PATEL, MINISTER OF STATE FOR HEALTH AND FAMILY WELFARE-2024
2. MASS COMMON YOGA PROTOCOL DEMONSTRATION IN IDY-2024
One of the primary mandates of the centre is to build capacities of human resources in the country in the area of substance use disorders. The centre has been involved in providing training to doctors and other categories of staff members since 1989. The centre has developed curricula, training schedules, modalities and resource materials for training of trainers, Medical Doctors (GDMOs), nurses and laboratory personnel. The training programmes have been reviewed and modified through workshops of resource persons. Some of the training programmes organised by the centre in the recent past include:
Note: The resource persons for all these training programmes include the faculty and staff members of NDDTC. Faculty members from other institutes are also sometimes invited as resource persons for the training.
The centre has completed project focused on training of doctors in the area of substance use disorders. The project envisaged imparting training to at least one doctor in each of the district hospital in the country, so that close to 350 doctors of country received training over a period of three years. This project was funded by the National Fund for Control of Drug Abuse (NFCDA), Department of Revenue, Ministry of Finance, Government of India. Other institutes collaborating with NDDTC, AIIMS in this venture included:
Besides these, the faculty from the centre has also been involved in providing training to doctors, nurses, project managers and counsellors from various other organisations. These include the NGOs supported by the Ministry of Social Justice and Empowerment, National Institute of Social Defence, Regional Resource and Training Centres, National Institute of Criminology and Forensic Sciences, National AIDS Control Organisation, State AIDS Control Societies etc.
The centre has also produced resource material in the form of manuals for training. These manuals are distributed to the participants during training programmes. In addition these manuals are also available for free download.
The centre has been involved in providing training to doctors and other categories of staff members since 1989. The centre has developed curricula, training schedules, modalities and resource materials for training of trainers, Medical Doctors (GDMOs), nurses and laboratory personnel. Between January 1989 and October 2007, about 40 courses for doctors have been organised. Various manuals are available. The training programmes have been reviewed and modified through workshops of resource persons.
DR. RAJEEV SHARMA
M.B.B.S., M.S., M.Ch.
Assistant Professor, Neurosurgery,
All India Institute of Medical Sciences
New Delhi, India.
Brief Profile -
Dr Rajeev Sharma has an excellent academic and surgical record. After completing his MS, surgery from Government Medical College & Hospital, Nagpur, in 2007; he worked as Senior Resident, Neurosurgery for 1 year in Dr RML Hospital, New Delhi; GB Pant Hospital, New Delhi; and Lok Nayak Hospital, New Delhi. In August 2008, he joined M.Ch. Neurosurgery residency( 3 years) course at National Institute of Mental Health and Neurosciences, (NIMHANS), Bangalore, India. After finishing his M Ch residency in July 2011, he has worked as Senior Resident, Neurosurgery in NIMHANS, Bangalore, India for 1 year. He has worked as faculty in PGIMER, Dr RML Hospital, New Delhi for 17 months before joining as Neurosurgery faculty at AIIMS, New Delhi. He is well versed in all aspects of Neurosurgical care. He has presented his work at various meetings in India and has several publications to his credit in various national and international journals.
Education & Training:
Areas of Interest -
Clinical Interests:
Surgery Research Interests:
Clinics :
Publications:
1) Rajeev Sharma, Praveen Saligouda, Dhananjaya I Bhat, B Indira Devi. Compound elevated skull fracture mimicking a frontotemporoorbitozygomatic craniotomy flap. Neurology India 2012;60(4):448-9.
2) Rajeev Sharma, Arun Kumar, Dhananjaya I Bhat, B Indira Devi. Compound elevated skull fractures in adults: a series of five patients and review of literature. Indian Journal of Neurotrauma 2012;9:112-6.
3) Rajeev Sharma, B A Chandramouli, Ravi Mohan Rao. Ventral foramen magnum neurenteric cyst presenting as acute rapidly progressive quadriparesis and respiratory compromise: a case report and review of literature. Neurology India 2013;61(2):187-9.
4) Dhaval Shukla, Rajeev Sharma, Bhagavatula Indira Devi, Somanna Sampath. Rostral basilar artery syndrome following transsphenoidal surgery- a report of 4 cases. Acta neurochirurgica 2013;155:1633-6.
5) Rajeev Sharma, B A Chandramouli, Prateek Nayak. Nasal encephalocele with herniated anterior cerebral arteries in an adult- a technical case report with special emphasis on technique of management of herniated cerebral vessels. Neurology India 2013;61(5):80-1.
6) Rajeev Sharma, Dwarakanath Srinivas, Somanna Sampath. Giant cerebral cavernous malformation causing raised intracranial pressure in an adult: Case report and review of literature. Indian Journal of Neurosurgery 2013;2(3):42-4.
7) Rajeev Sharma, Harisha Poomagame Narasimhamurthy, Somanna Sampath. Intradural extramedullary dorsal spinal tuberculoma: a manifestation of paradoxical response to antitubercular chemotherapy. Indian Journal of Neurosurgery 2013;2(3):58-9.
8) Rajeev Sharma, Banwari Lal Bairwa, Meenakshi Bhardwaj, Laxmi Naraian Gupta. Primary intracranial mesenchymal chondrosarcoma mimicking meningioma. Indian Journal of Neurosurgery 2014;3(2):132-4.
Guest Lectures:
1) Low back pain- myths and misbelieves- evidence based. presented in Neuro CME organised by Shakti Neurosciences centre at Bluebird resort, Hisar on 19 October, 2013.
Public Lectures:
1) Head injury awareness lecture in Dept of social work, Bhim Rao Ambedkar College, YamunaVihar, Delhi on 28 October, 2014.
Professional Memberships:
1) Life member of Neurological society of India. 2) Life member of Delhi Neurological association. 3) Member of Bangalore Neurological society.
The SET (Skills, e-Learning, Telemedicine) Facility is a state of art facility set up to modernise and update medical education at the institute. It imparts skill based learning to medical undergraduates, postgraduates and nursing staff so that they are better prepared when managing patients in wards and clinics. The facility has active involvement of faculty members from various clinical and non-clinical departments who develop the training modules and teaching content and impart hands-on teaching to the students. The skill lab provides a stress free environment to learn skills. The other aspects of the facility are to develop e-learning modules and to impart education through telemedicine linkages with medical colleges and hospitals across India.
The facility has a Dry Skill Lab equipped to impart several basic and advanced medical skills through in-house developed modules. It has a Wet Lab hosting cadaveric and other surgical skill development workshops in various surgical specialties. In addition there are three modern studios hosting telemedicine classes regularly with capability to link with over 50 medical institutions across India.
The SET Facility is an example of the vision of the institute’s leadership at continuous innovation in the field of medical education....
1. Ghati, N., Killa, A. K., Sharma, G., Karunakaran, B., Agarwal, A., Mohanty, S., Nivethitha, L., Siddharthan, D., Pandey, R. M. (2020). A randomized trial of the immediate effect of bee-humming breathing exercise on blood pressure and heart rate variability in patients with essential hypertension. EXPLORE. https://doi.org/10.1016/j.explore.2020.03.009
2. Gupta, U., Gupta, Y., Jose, D., Mani, K., Jyotsna, V. P., Sharma, G., Tandon, N. (2020a). Effectiveness of a Video-Based Lifestyle Education Program Compared to Usual Care in Improving HbA1c and Other Metabolic Parameters in Individuals with Type 2 Diabetes: An Open-Label Parallel Arm Randomized Control Trial (RCT). Diabetes Therapy, 11(3), 667–679. https://doi.org/10.1007/s13300-020-00769-2
3. Gupta, U., Gupta, Y., Jose, D., Mani, K., Jyotsna, V., Sharma, G., Tandon, N. (2020b). Effectiveness of yoga-based exercise program compared to usual care, in improving HbA1c in individuals with type 2 diabetes: A randomized control trial. International Journal of Yoga, 13(3), 233. https://doi.org/10.4103/ijoy.IJOY_33_20
4. Kaur, H., Chaudhary, S., Mohanty, S., Sharma, G., Kumaran, S. S., Ghati, N., Bhatia, R., Nehra, A., Pandey, R. (2022). Comparing cognition, coping skills and vedic personality of individuals practicing yoga, physical exercise or sedentary lifestyle: a cross-sectional fMRI study. Integrative Medicine Research, 11(1), 100750. https://doi.org/10.1016/j.imr.2021.100750
5. Kumar, A., Bhatia, R., Sharma, G., Dhanlika, D., Vishnubhatla, S., Singh, R. K., Dash, D., Tripathi, M., Srivastava, M. V. P. (2020). Effect of yoga as add-on therapy in migraine (CONTAIN). Neurology, 94(21), e2203–e2212. https://doi.org/10.1212/WNL.0000000000009473
6. Mandal, S., Misra, P., Sharma, G., Sagar, R., Kant, S., Dwivedi, S. N., Lakshmy, R., Goswami, K. (2021). Effect of Structured Yoga Program on Stress and Professional Quality of Life Among Nursing Staff in a Tertiary Care Hospital of Delhi—A Small Scale Phase-II Trial. Journal of Evidence-Based Integrative Medicine, 26(30), 1–10. https://doi.org/10.1177/2515690X21991998
7. Mohanty, S., Sharma, P., Sharma, G. (2020). Yoga for infirmity in geriatric population amidst COVID-19 pandemic. Asian Journal of Psychiatry, 53, 102199. https://doi.org/10.1016/j.ajp.2020.102199
8. Neyaz, O., Sumila, L., Nanda, S., Wadhwa, S. (2019). Effectiveness of Hatha Yoga Versus Conventional Therapeutic Exercises for Chronic Nonspecific Low-Back Pain. The Journal of Alternative and Complementary Medicine, 25(9), 938–945. https://doi.org/10.1089/acm.2019.0140
9. Sahar Qazi, Soumi Das, Bharat Krushna Khuntia, Vandana Sharma, Shruti Sharma, Gautam Sharma, K. R. (2021). In silico molecular docking and molecular dynamic simulation analysis of phytochemicals from Indian foods as potential inhibitors of SARS-CoV-2 RdRp and 3CLpro. Natural Product Communications.
10. Sharma, G. (2020). Exploring Knowledge, Attitude and Practice regarding Yoga among patients attending Cardiology and Neurology clinics in a tertiary care hospital in Northern India. National Medical Journal of India.
11. Sharma, G. (2021). Knowledge, Attitude and Practice towards Ayurveda among patients attending specialty clinics at a tertiary care institute in India. National Medical Journal of India.
12. Sharma, G., A, M., Naik, G., Nivethitha, L. (2021). A review on role of yoga in the management of patients with cardiac arrhythmias. International Journal of Yoga, 14(1), 26. https://doi.org/10.4103/ijoy.ijoy_7_20
1. “Yoga as Lifestyle Medicine” on 4 th Jan 2020 at 23 rd International Conference on Frontiers in Yoga Research and its publications (INCOFYRA) organized by V-YASA, Bengaluru.
2. Title- Differences in Cognitive Function and Emotional Processing among Yoga Practitioners, Physically Active Individuals, and Sedentary Lifestyle Individuals: A Functional Magnetic Resonance Imaging Study. Vanue: World's First Symposium on "Role of Meditation for Prevention And Treatment Of Cardiovascular Diseases." AIIMS, Rishikesh, Uttarakhand, India. Date: 9th 10th March, 2019
3. Title: Effects of a different non-pharmacological interventions involving mindfulness based yoga and comprehensive neuropsychological rehabilitation with aphasia therapy on post-stroke: A PROBE trial
Venue: World Stroke Congress, Canada. Date November 2018
4. Yoga: A Potential adjunct therapy for patients with Cardiac Arrhythmia” as an Invited speaker in Worlds First Symposium on “Role of Meditation for prevention and treatment of Cardiovascular Diseases” Integrated approach to prevention of cardiovascular diseases held on March 9-10, 2019 at All India Institute of Medical Sciences (AIIMS), Rishikesh, Uttarakhand,
Cell Regulation & Trafficking Lab
Dr. Parthaprasad Chattopadhyay, Professor
Address: Room No. 4007, Convergence Block, AIIMS, New Delhi.
Phone:011-26549238
Email: parthoaiims[at]hotmail[dot]com
EDUCATION
MBBS, (1981-1987) R G Kar Medical College,Calcutta University, Kolkata
MD, Biochemistry, (1989-1991) All India Institute of Medical Sciences, New Delhi.
PhD, Biochemistry (1992-1996) All India Institute of Medical Sciences, New Delhi.
Senior Demonstrator (1992-1995) Department of Biochemistry, AIIMS, New Delhi
Assistant Professor (1997-2003) Department of Biochemistry, AIIMS, New Delhi
Associate Professor (2003-2007) Department of Biochemistry, AIIMS, New Delhi
Additional Professor (2007-2011) Department of Biochemistry, AIIMS, New Delhi
Professor (2011- till date) Department of Biochemistry, AIIMS, New Delhi
a) Nanoparticle trafficking within the cell: Tracing the path of nanoparticles within the cell and attempting to modulate their intracellular travel to prolong their stay within the cell for increased unloading of their cargo (drug).
b) Site-directed epigenetic modulation: Using modified CRISPR based techniques to modulate CpG methylation and Histone methylation/acetylation for altering gene expression of tumor suppressor and promoter genes
Department of Biotechnology and Department of Science & Technology, Ministry of Science & Technology, GOI.
| Name | Designation | Date of Superannuation |
|---|---|---|
| Dr.Davinder Mohan | Professor and Programme In-charge | September2002 |
| Prof Rajat Ray | Professor and Chief & Member INCB | September2013 |
| Prof S K Khandelwal | Professor and Chief | December 2016 |
| Dr Meera Vaswani | Professor | February2012 |
| Dr B. M. Tripathi | Professor | |
| Dr.N.G.Desai | Additional Professor | |
| Dr.H.P.Jhingan | Additional Professor | |
| Dr.B.S.Chavan | Associate Professor | |
| Dr.Kishore Chandiramani | Associate Professor | |
| Dr.Vinay Kapoor | Associate Professor | |
| Dr Hem Raj Pal | Associate Professor | |
| Dr Nanaji Kaw | Associate Professor | May 2014 |
| Dr. Raka Jain | Professor | October 2022 |
Professor and Programme In-charge
Date of Superannuation: September2002
Professor
Date of Superannuation: February2012
Professor
Date of Superannuation: --
Additional Professor
Date of Superannuation: --
Additional Professor
Date of Superannuation: --
Associate Professor
Date of Superannuation: --
Associate Professor
Date of Superannuation: --
Associate Professor
Date of Superannuation: --
Associate Professor
Date of Superannuation: --
Associate Professor
Date of Superannuation: May 2014
Professor
Date of Superannuation: October 2022
Prof S K Khandelwal is Ex-Professor and Head of the department of Psychiatry and Second Chief, National Drug Dependence Treatment Centre (NDDTC) between 2013-2016.
Prof Rajat Ray is Ex-Professor and Head of the Department of Psychiatry and First Chief, National Drug Dependence Treatment Centre (NDDTC) between 2003-2013.
Prof S K Khandelwal is Ex-Professor and Head of the department of Psychiatry and Second Chief, National Drug Dependence Treatment Centre (NDDTC) between 2013-2016.
1. Sharma, V., Khuntia, B. K., Gupta, A., Rathore, S., Srivastava, A. K., Sharma, G. (2022). Shirodhara (Indian traditional oil flow therapy) Integrated with Brief Behavioural Therapy for unresolved Chronic Insomnia Disorder: A Case Report. Psychiatry Research Case Reports. 15:100057.
2.Rathore, S., Khuntia, B. K., Wadhawan, M., Sharma, V., Sharma, G. (2022). Herbal adaptogens: An integrative approach for enhancing performance and resilience in athletes. Phytotherapy research : PTR, 10.1002/ptr.7529. https://doi.org/10.1002/ptr.75293.
3. Sharma, V., Khuntia, B. K., Soneja, M., Huddar, V. G., Ramakrishnan, S., Sharma, P., Rathore, S., Valliappan, V., Wadhawan, M., Chhabra, V., Agarwal, A., Jat, M., Kumar, A., Nesari, T. M., Sharma, G. (2022). Efficacy of add-on Ayurveda and Yoga intervention in health care workers of tertiary care hospital during COVID-19: Randomized controlled trial. Complementary therapies in clinical practice, 48, 101601. https://doi.org/10.1016/j.ctcp.2022.101601
4.Khuntia, B. K., Agarwal, A., Sharma, G. (2022). Letter to Editor on "A randomized, controlled, blinded, parallel-group, clinical trial to study the role of Ayurcov (AyurCoro3), a one-day regimen as an adjuvant therapy for COVID-19 disease management, at dedicated Covid Hospital (DCH) in India". Complementary therapies in medicine, 68, 102838. https://doi.org/10.1016/j.ctim.2022.102838
5. Sharma, G., Sharma, P., Mohan, B., Agarwal, A., Lama, S., Jat, M., Biju, K. C., Upadhyay, P., Gupta, A., Mohanty, S., Miglani, M., Sharma, S., Sagar, R., Prabhakaran, D., Pandey, R. M. (2022). Prevalence of psychological outcomes and its associated factors in healthcare personnel working during COVID-19 outbreak in India. Indian journal of psychiatry, 64(2), 151–158. https://doi.org/10.4103/indianjpsychiatry.indianjpsychiatry_60_21
6. Khuntia, B. K., Sharma, V., Wadhawan, M., Chhabra, V., Kidambi, B., Rathore, S., ... Sharma, G. (2022). Antiviral Potential of Indian Medicinal Plants Against Influenza and SARS-CoV: A Systematic Review. Natural Product Communications, 17(3), 1934578X221086988.
7. Sharma, G., Gujral, J. S., Agarwal, A., Jat, M., Mohanty, S., Pandey, R. M. (2021). Exploring knowledge, attitude and practice regarding yoga among patients attending cardiology and neurology clinics in a tertiary care hospital in northern India. The National medical journal of India, 34(4), 201–205. https://doi.org/10.25259/NMJI_11_20
8. Khuntia, B. K., Sharma, V., Qazi, S., Das, S., Sharma, S., Raza, K. and Sharma, G. (2021). Ayurvedic medicinal plants against COVID-19: an in silico analysis. Natural Product Communications, 16(11), p.1934578X211056753.
9. Sharma, G., Ramakumar, V., Sharique, M., Bhatia, R., Naik, N., Mohanty, S., Agarwal, A., Meti, M., Shukla, A., Deepti, S., Bansal, R., Gupta, A., Ahmed, A. S., Pandey, R. M., Narang, R., Mishra, S., Saxena, A., Juneja, R., LIVE-Yoga Investigators (2022). Effect of Yoga on Clinical Outcomes and Quality of Life in Patients With Vasovagal Syncope (LIVE-Yoga). JACC. Clinical electrophysiology, 8(2), 141–149. https://doi.org/10.1016/j.jacep.2021.09.007
10. Qazi, S., Das, S., Khuntia, B. K., Sharma, V., Sharma, S., Sharma, G. and Raza, K. (2021). In silico molecular docking and molecular dynamic simulation analysis of phytochemicals from Indian foods as potential inhibitors of SARS-CoV-2 RdRp and 3CLpro. Natural Product Communications, 16(9), p.1934578X211031707.
11. Ghati, N., Killa, A. K., Sharma, G., Karunakaran, B., Agarwal, A., Mohanty, S., Nivethitha, L., Siddharthan, D., Pandey, R. M. (2021). A randomized trial of the immediate effect of Bee-Humming Breathing exercise on blood pressure and heart rate variability in patients with essential hypertension. Explore (New York, N.Y.), 17(4), 312–319. https://doi.org/10.1016/j.explore.2020.03.009
12. Kaur, H., Chaudhary, S., Mohanty, S., Sharma, G., Kumaran, S. S., Ghati, N., Bhatia, R., Nehra, A., Pandey, R. M. (2022). Comparing cognition, coping skills and vedic personality of individuals practicing yoga, physical exercise or sedentary lifestyle: a cross-sectional fMRI study. Integrative medicine research, 11(1), 100750. https://doi.org/10.1016/j.imr.2021.100750
13. Ramakumar, V., Sharma, G., Naik, N., Sharique, M., Agarwal, A., Kailath, D., Bansal, R. and Saxena, A. (2021). Effect of yoga on clinical outcomes and quality of life in patients with vasovagal syncope-a randomised control trial. Journal of the American College of Cardiology, 77, pp.221-221.
14. Sharma, G., Mooventhan, A., Naik, G., Nivethitha, L. (2021). A Review on Role of Yoga in the Management of Patients with Cardiac Arrhythmias. International journal of yoga, 14(1), 26–35. https://doi.org/10.4103/ijoy.IJOY_7_20
15. Mandal, S., Misra, P., Sharma, G., Sagar, R., Kant, S., Dwivedi, S. N., Lakshmy, R., Goswami, K. (2021). Effect of Structured Yoga Program on Stress and Professional Quality of Life Among Nursing Staff in a Tertiary Care Hospital of Delhi-A Small Scale Phase-II Trial. Journal of evidence-based integrative medicine, 26, 2515690X21991998. https://doi.org/10.1177/2515690X21991998
16. Gupta, U., Gupta, Y., Jose, D., Mani, K., Jyotsna, V. P., Sharma, G., Tandon, N. (2020). Effectiveness of Yoga-based Exercise Program Compared to Usual Care, in Improving HbA1c in Individuals with Type 2 Diabetes: A Randomized Control Trial. International journal of yoga, 13(3), 233–238. https://doi.org/10.4103/ijoy.IJOY_33_20
17. Mohanty, S., Sharma, P., Sharma, G. (2020). Yoga for infirmity in geriatric population amidst COVID-19 pandemic: Comment on "Age and Ageism in COVID-19: Elderly mental health-care vulnerabilities and needs". Asian journal of psychiatry, 53, 102199. https://doi.org/10.1016/j.ajp.2020.102199
18. Kumar, A., Bhatia, R., Sharma, G., Dhanlika, D., Vishnubhatla, S., Singh, R. K., Dash, D., Tripathi, M., Srivastava, M. (2020). Effect of yoga as add-on therapy in migraine (CONTAIN): A randomized clinical trial. Neurology, 94(21), e2203–e2212. https://doi.org/10.1212/WNL.0000000000009473
19. Gupta, U., Gupta, Y., Jose, D., Mani, K., Jyotsna, V. P., Sharma, G., Tandon, N. (2020). Effectiveness of a Video-Based Lifestyle Education Program Compared to Usual Care in Improving HbA1c and Other Metabolic Parameters in Individuals with Type 2 Diabetes: An Open-Label Parallel Arm Randomized Control Trial (RCT). Diabetes therapy : research, treatment and education of diabetes and related disorders, 11(3), 667–679. https://doi.org/10.1007/s13300-020-00769-2.
20. Neyaz, O., Sumila, L., Nanda, S., Wadhwa, S. (2019). Effectiveness of Hatha Yoga Versus Conventional Therapeutic Exercises for Chronic Nonspecific Low-Back Pain. Journal of alternative and complementary medicine (New York, N.Y.), 25(9), 938–945. https://doi.org/10.1089/acm.2019.0140
Dr. Gautam Sharma, Prof. In-charge
Participated as a mentor in the meeting of the 2nd CIMER (Centre for Integrative Medicine, Education, and Research) committee. (Virtual participation), organized by AIIMS, Raipur. (29th March 2022)
Title: Newer evidence of Yoga in Medicine at the Cardiology Update and Cardio-Imaging Conference organized under the aegis of Society of Image-guided therapy at Dayanand Medical College and Hospital campus, Ludhiana, Punjab, India. (5th-6th March 2022)
Title: How Yoga Promotes Faster Recovery in Cardiac Rehabilitation” in the 5th Asian Yoga Therapy Association Hybrid Webinar, organized and hosted by VYASA Yoga, Singapore. (25th September 2021)
Title: Yoga for Wellbeing as guest speaker at DD News channel. (20th June 2021)
Title: Effect of Yoga on Clinical Outcomes and Quality of Life in Patients with Vasovagal Syncope (LIVE-YOGA). Venue: International YOGACON USA 2021 organized by American Academy of Yoga Meditation and All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India. (Virtual participation) (13th June 2021)
Participated in the first virtual committee meeting of “Yoga for Productivity”. (24th March 2021)
Participated in a committee meeting for “Formulation of Integrative Health Policy”, NITI Aayog, New Delhi, India. ( 8th October 2020)
Participated in “Rashtriya Arogya Nidhi” meeting. Venue: Directorate General of Health Services (DGHS), Nirman Bhawan, New Delhi. (1st September 2020)
Title: Yoga as Lifestyle Medicine. Venue: “23rd International Conference on Frontiers in Yoga Research and its publications (INCOFYRA)”organized by S-VYASA University, Bengaluru, Karnataka, India. (4th January 2020)
Panel discussion, Title: Back to the Future. Venue: Zee Jaipur Literature Festival. (23rd January 2020)
Panel discussion. Title: Opportunities and Challenges in Integrative Medicine. Venue: All India Institute of Ayurveda (AIIA), New Delhi, India. (22nd November 2019)
Title: Yoga: A Potential adjunct therapy for patients with Cardiac Arrhythmia”. Venue: First symposium on “Role of Meditation for prevention and treatment of Cardiovascular Diseases” Integrated approach to prevention of cardiovascular diseases, All India Institute of Medical Sciences (AIIMS), Rishikesh, Uttarakhand, India. (9th-10th March 2019)
2nd Round Table on “Integrative Medicine”. Venue: NITI Aayog. (6th February 2019)
Title: Integrative Research-Opportunities and Future Directions. Venue: Orientation program conducted for PG scholars at All India Institute of Ayurveda (AIIA), New Delhi. (21st January 2019)
Chairperson of the 10th Annual Conference of the Indian Heart Rhythm Society (IHRS). Venue: The Lalit Hotel, Jaipur, Rajasthan, India. (8th December 2018)
Title: Yoga and Cardiovascular health. Venue: Indian Council of Medical Research (ICMR), New Delhi, India. (21st June 2018)
Sudha Lama (Nursing Officer)
Title: A study to assess parenting stress and psychological health of women having single parenting experience in Delhi-NCR. Venue: Geriatric Nursing: A multidisciplinary approach towards active ageing organized by Rajkumari Amrit Kaur College of Nursing, New Delhi, India. (24th March 2022)
Dr Bharat Krushna Khuptia (Scientist C)
Title: Healthy Ageing: Complementary Medicine insights evidence. Venue: Geriatric Nursing: A multidisciplinary approach towards active ageing Rajkumari Amrit Kaur College of Nursing, New Delhi, India. (23rd March 2022)
Dr. Anupama Gupta (Sr. Medical Officer)
Title: Sleep and the autonomic nervous system: A bidirectional relationship: Restless legs Syndrome and Autonomic function. Venue: World Sleep Congress 2022, Rome, Italy. (15th March 2022)
Dr. Vandna Sharma (Scientist C)
Title: Evaluation of the prophylactic effect of Comprehensive Ayurveda and Mindfulness-based Yoga regimen among health care workers (HCW) of a tertiary care hospital in Delhi during COVID-19 Pandemic: A randomized controlled trial. Venue: international Virtual Convention on Ayurveda and Research advances on COVID-19, organized by Ayurveda College Coimbatore and Diskha E- learning, Coimbatore, Tamil Nadu, India. (Virtual participation) (20th June 2021)
Dr. Shubhangi Rathore (Medical Officer)
Title: Paediatric Developmental Disorders. Venue: Global Ayurveda Medical Travel organized by Confederation of Indian Industry(CII) (Virtual participation). (18th February 2021)
Dr Guru Dutta Satyarthee
Professor, Department of Neurosurgery AIIMS, New Delhi
Publication:
http://doi.org/10.5256/f1000research.7698.r13750.
http://doi.org/10.5256/f1000research.7566.r16091.
Prof Rajat Ray is Ex-Professor and Head of the Department of Psychiatry and First Chief, National Drug Dependence Treatment Centre (NDDTC) between 2003-2013.
| Designation | Name of the staff member(s) |
|---|---|
| Senior Administrative officer | NA |
| Assistant Administrative Officer | Sh. Ashok Kumar |
| Finance and Chief Accounts Officer | Sh Vijay Pal |
| ANS Nursing Superintendent | Ms. Betty Donna Rawat |
| Store Officer | NA |
| Asstt. Store Officer | Sh Ram Pal Singh |
| AE Civil | Sh Shabad Ali |
| AE Electrical | Sh Satbir Kumar |
| AE (AC & R) | Sh Hem Singh |
| JE ( Civil) | Sh Rakesh Kumar |
| JE (Elec.) | Sh Prashant Kumar |
| JE (AC & R) | Sh Satya Prakash |
| Scientist | NA |
| Medical Social Service Officer | Dr. Brahm Prakash Mr. Deepak Yadav Mr. Dinesh Kumar |
| Biochemist | NA |
| Medical Record Officer | Mr. Harish Chandra |
| Librarian Gr-I | Mr. Pramod Kumar |
| Security Cum Fire Guard Gr.-II | Sh. Pradeep Sh Amit Chillar Sh. Gautam Malik |
Dr. Kalpana Luthra
Professor & Head
Department of Biochemistry
Room No-4001, 4thFloor
Convergence Block,
All India Institute of Medical Sciences,
New Delhi-110029
Phone: 011-26549242
Email Id: kalpanaluthra[at]gmail[dot]com
Dr. Kalpana Luthra is a Professor & Head in the Department of Biochemistry, All India Institute of Medical Sciences (AIIMS), New Delhi, India. She completed her PhD at AIIMS in 1994 and joined as faculty at AIIMS in 1998. She was awarded Shakuntala Amir Chand Prizeby Indian Council of Medical Research (ICMR) for the year 2003 & Fogarty fellowship in 2002 and availed training in HIV-1 antibody related work at New York University. She is a Fellow of The National Academy of Medical Sciences India (NAMS), National Academy of Sciences, India (NASI) & Indian National Science Academy (INSA).
HIV Immunology: Coevolution of virus and antibody responses, generation and characterization of human recombinant anti-HIV-1 monoclonal antibodies
HIV-1 is a complex virus with a remarkable ability to protect itself from our intricate network of immune system. This is achieved by masking itself from the immune recognition by acquiring the host proteins or by escaping the humoral response by virtue of its extraordinary ability to mutate. This leads to generation of diverse strains of HIV-1 virus, making the treatment and prevention a complicated process. More than 90% of the HIV-1 infections in India are caused by clade C viruses. Our lab focuses on studying various aspects of HIV-1 infection which includes:
HIV-1C primary isolates generated in our lab from select infected children showed resistance to neutralization by majority of the known second generation bNAbs (Makhdoomi et al,Virology2016). We followed up antiretroviral naïve chronically infected children and mapped their plasma for presence of bnAbs (Makhdoomi et al.J Gen Virol. 2017 Jul;98(7):1879-189) and identified a pair of identical twins AIIMS_329 and AIIMS_330. The plasma from both donors showed the evolvement of bnAbs targeting common epitopes in the V2 and V3 regions of the envelope, suggesting bnAb development in these twins may perhaps be determined by specific sequences in the shared virus that can guide development of immunogens aimed at eliciting V2 and V3 bNAbs. Characterization of the neutralization sensitive and resistant viruses coevolving with bNAbs in the contemporaneous AIIMS_330 plasma provides information towards understanding viral alterations that may have contributed to the development of resistance to bnAbs. (Mishra N. J Virolhttps://doi.org/10.1128/JVI.00654-19).
Our work on circulating HIV-1 in perinatally infected infants defined viral factors associated with early bnAb responses, supportive of polyvalent vaccination approaches capable of inducing bnAbs against HIV-1 (Mishra N. Nat.Commun.,2020) 11:4409https://doi.org/10.1038/s41467-020-18225-x). As in the case of monozygotic twins, we identified that the antibody response in infants primarily targets the V2 region of HIV-1, making it an attractive target for immunogen design to elicit antibodies.
Using the high throughput technology of HIV-1 specific single B cell sorting, we isolated a bNAb AIIMS-P01 from a pediatric elite neutralizer (Kumar et al,JVI, 2019). This mAb has shown 67% breadth at a potency of 0.5 µg/ml, and shows good neutralizing activity against Indian clade C viruses and needs to be tested in future for in vivo protection against HIV-1 infection.
Recently, we generated and structurally analyzed a heavy chain matured linage antibody 44m of the parental anti-HIV-1 human monoclonal AIIMS P01, that demonstrated improved neutralization potential against globally diverse viruses, as compared to the parent antibody (Kumar Set al. iScience. 2023)
During the COVID-19 pandemic, neutralizing antibodies have been shown to be a critical feature of recovered patients. Given the unique nature of HIV-1 bnAbs and their ability to recognize and/or accommodate viral glycans, we reasoned that the glycan shield of SARS-CoV-2 spike protein can be targeted by HIV-1 specific bnAbs. We showed that HIV-1 specific monoclonal antibodies as well as polyclonal plasma antibodies cross-react and neutralize SARS-CoV-2. (Mishra N. PLoS Pathog 2021. 17(9): e1009958 https://doi.org/10.1371/journal.ppat.1009958.
Publications (Selected publications since last 5 years)
Chapter on DNA Fingerprinting for class XI-XII ‘Textbook in Biology (supplementary material) published by the Central Board of Secondary Education (CBSE) in December 2000. Chapter on “Basic concept of Clinical Biochemistry” in e book “Clinical Biochemistry”, 18thSeptember 2006. (Revised 5thMay 2008).
http://nsdl.niscair.res.in/jspui/bitstream/123456789/691/1/ClinicalBiochem_Concepts.pdf
Patents
Dr. Swarandeep Singh, Research Associate:
D r. Swarandeep Singh, is a Research Associate, working on a project entitled "Development of therapeutic broadly neutralizing monoclonal antibodies against circulating HIV-1 clade C in children and adults." He earned his Ph.D. in the HIV-1 Immunology Laboratory at AIIMS New Delhi under the chief guidance of Professor Kalpana Luthra. During his Ph.D., he developed expertise in designing and characterizing HIV-1 vaccines and recombinant monoclonal antibodies. Dr. Singh's primary research interest lies in HIV-1 vaccine design, with a focus on testing designed immunogens in preclinical animal models. Additionally, he actively explores the generation and modification of novel monoclonal antibodies from chronically HIV-1 infected patients for therapeutic purposes. During the COVID-19 pandemic, he has showcased the unique nature of HIV-1 broadly neutralizing antibodies (bnAbs) & polyclonal plasma antibodies cross-reacted and effectively neutralized SARS-CoV-2, showcasing the potential dual application of HIV research insights in combating other viral infections. Through the esteemed HIV-1 Research Trust Fellowship Award (United Kingdom), Dr. Swarandeep Singh has gained advanced skills in the design of self-assembling protein nanoparticles as a platform for HIV vaccines & other innovative vaccine strategies
Recipient of prestigious HIVResearchTrustsScholarship Award,UK, to pursue the training on self-
Antara Malik, PhD scholar:
Ms. Antara Malik is a fifth year PhD student currently working in the lab of Dr. Kalpana Luthra. Primarily, her thesis work is aimed at understanding the status of the immune responses and the role of macrophages and T cells in the immunopathology of Chronic Pancreatitis. The second part of her thesis work involves theelucidation of metabolic alterations associated with the progression of Chronic Pancreatitis.
She completed her Masters in Biotechnology from Jamia Millia Islamia, New Delhi. Her master’s dissertation was conducted in NIPGR (National Institute of Plant Genome Research), New Delhi where her project work involved cloning of Sucrose Transporters and Expression Analysis of Genes in Rice plants. She graduated in Biochemistry (Hons.) from University of Delhi.
Research Focus of the Lab:
Apart from the ongoing research work involving HIV-1, Prof. Kalpana Luthra has also collaborated with Prof. Pramod K. Garg, Department of Gastroenterology and the group recently started working on Chronic Pancreatitis.
Chronic Pancreatitis is an inflammatory disease of the pancreas which results in the slow destruction of pancreatic parenchyma, severe abdominal pain, subsequent fibrosis leading to poor quality of life. The mechanism of inflammation, tissue destruction and fibrosis is not well understood.
Patients commonly experience recurrent exacerbations with painful attacks interspersed by relatively quiescent phases. Also, some patients present with chronic continuous pain. This may be driven by either or both innate and adaptive immune responses on which there are several contradictory studies/lacunae in the existing literature.
Hereby, there arises a need to understand the inflammatory processes in Chronic Pancreatitis with regard to the initiating and effector cells that are involved, and the inflammatory mediators driving the process. The translational significance lies in the possibility of repurposing some of the known anti-inflammatory/immunosuppressive drugs that may be tested in these patients.
Post her Masters, she continued as a JRF in NIPGR, where she was working on the characterization of tissue specific expression pattern of PIF transcription factors in rice and tomato plants in response to high temperature, drought and salt stress via quantitative PCR and generation of PIF regulatory network via transcriptome profiling of over expression and knock out/down lines using RNA Seq librarypreparation.
Further, she joined IARI (Indian Agricultural Research Institute), New Delhi as a JRF where her project was based on the integration of plant and parasite omics to decipher the interactions and identify molecular targets for the management of root knot disease of rice.
Later on, she shifted her research focus to human sciences and joined Dr. B.R. Ambedkar Center for Biomedical Research (ACBR), University of Delhi as a JRF where she was studying the genetic polymorphism of Growth Differentiation Factor15 (GDF15) in patients with Coronary Artery Disease in Asian Indian population followed by the differential expression of GDF15 in these patients at mRNA and protein level.
Association with professional bodies
Life member of Indian Immunology society since January 2023.
Shaifali Sharma, Ph.D. Scholar
Ms. Shaifali Sharma is a Ph.D. Scholar in Prof. Luthra’s Laboratory since February 2020. As a part of her thesis, she is generating HIV-1 envelope immunogen which binds to germline version of known anti-HIV-1 broadly neutralizing antibodies from early HIV-1 infected donors.
She earned her Master’s degree in Medical Biochemistry from AIIMS, New Delhi in 2019. As a part of her M.Sc. thesis dissertation, she studied the HIV-1 envelope glycoprotein by generating pseudoviruses from a chronically infected long term non-progressor, in order to identify envelope features of the virus circulating in patient. After completing her M.Sc., she continued being a part the Lab as a Junior Research Fellow (joined in October 2019) and later registered for Ph.D. in February 2020.
Association with professional bodies
Life member of Indian Immunology society since April 2018.
Dr. Sanket Katpara, Ph.D. Scholar
Dr. Sanket Katpara is a second year PhD student at the department of biochemistry working under the chief supervision of Professor Kalpana Luthra in the HIV immunology lab. As part of his PhD thesis, he is working on “Generation and Characterization of recombinant anti-HIV-1 human monoclonal antibodies from HIV-1 infected individuals”. He is interested in generation of monoclonal antibodies that can target different epitopes on the HIV-1 envelope which can be used as a combinatorial therapy for the treatment of drug resistant HIV-1 infected individuals.
Earlier he has also completed his M.D. under the supervision of Dr Kalpana Luthra at the Department of Biochemistry, AIIMS. (2017-2020) and worked as a senior resident at the Dept. of Biochemistry, AIIMS, New Delhi (2020-2023)
Harsh Bhakhri, PhD Scholar:
Mr. Harsh Bhakhri is a PhD scholar (Dec 2021-present) currently in third year, is working on the characterization of the B cell receptor repertoire in HIV-1 subtype C infected individuals and also in generation of human anti-HIV-1 monoclonal antibodies from infected individuals. He has interest in studying the BCR sequences and their association to neutralization response in a cohort of HIV-1 infected individuals. He is also looking into the neutralizing plasma antibody response against various SARS-COV2 variants in different vaccinees for assessment of the protective response of the vaccination drive in Indian population.
He has also completed his M.Sc. in Biochemistry from AIIMS in 2021. His masters dissertation thesis work was to the role of M6A writer METTL3 and readers (IGF2BP1/3) in hematopoietic development and leukemogenesis. He has done his graduation in B.Sc. (Hons) Biochemistry from Sri Venkateswara College, University of Delhi in 2019.
Skills: Generation of pseudo-viruses, Generation of stable cell line, FACS, Neutralization assays, Single B-cell sorting, Single cell PCR, Molecular cloning, Site Directed Mutagenesis, Freestyle mammalian protein expression and purification, Size exclusion chromatography, Genomic data analysis using Galaxy server, R and Python.
Favorite hobbies: Generation of lots of viruses, learning new skills, a little bit of graphic designing, music and badminton.
Dr. Aradhana Sarma
Dr. Aradhana Sarma is a first year M.D. student at the Department of Biochemistry and is working under the chief supervision of Professor Kalpana Luthra. She is currently working on infectious molecular clones for her M.D. thesis titled “Generation and characterization of infectious molecular clones from HIV-1 viral envelopes derived from infected children”. With the help of this study, she intends to use the lab generated IMCs as potential tools in HIV-1 vaccine and entry inhibitor research.
She has completed her MBBS from Jorhat Medical College and Hospital, Assam.
Anil Kumar (Masalchi/Bearer Gd.II)
Mr. Anil Kumar previously worked as a Lab Attendant in Prof. Luthra’s lab in a research project since May, 2003. He was responsible for smooth functioning and maintenance of the lab, which included packing of tips, autoclaving and sterilization of plastic/glasswares, washing of equipment and cleaning of culture lab. He has completed his 12th standard Delhi in 2013. He is employed as Masalchi/Bearer Gd.II from January 2020.
Mr. Ajeesh T. Gangadharan (Junior Administrative Assistant)
Mr. Ajeesh T. Gangadharan joined Dr.K Luthra’s Lab as a Data Entry Operator in a research project on 1st October, 2005. He completed his B.Com from MG University, Kerala in 2002 & Computer Diploma From NIIT, New Delhi in 2004. After the completion of 15 years of service in various research projects, in September 2021 he joined the same lab as a Junior Administrative Assistant. His nature of work includes entering and systematic maintenance of patient data in Excel sheet, to contact and sent written communications for getting quotations for chemicals, preparing supply orders, processing bills, maintaining Accounts of the project, preparing Utilization certificates & Statement of expenditure, maintaining stock register, compilation of the project reports etc..
Mr. Abdul Wahid Hussain, Lab Technician
Mr. Abdul Wahid Hussain is working as a Lab Technician in Dr. Kalpana Luthra’s lab in a research project since January, 2010. He is an expert phlebotomist. His nature of works are cell culture (mammalian and bacterial) media preparation, Buffers preparation etc., PCR, DNA isolation, Patient sample collection, PBMCs isolation, Protein purification, Biological substance distribution to collaborators, Procurement/ordering of chemicals and lab instruments maintenance. He has completed his M.Sc.MLT from NIMS university Jaipur, Rajasthan in year 2020.
Suraj Kumar, Lab Technician
Mr. Suraj Kumar joined Prof. Luthra’s lab in the Chronic Pancreatitis research project as a lab technician in June 2022. He completed his Bachelor of Science (Hons) in Chemistry in the year 2022 through distance learning programme from Indira Gandhi National Open University (IGNOU), New Delhi. Also, he has a Diploma in Medical Lab Technology (2022) from DPMI (Delhi Paramedical Management of Institute) and a Diploma in Information Technology (2019). He is an expert phlebotomist and a quick learner.
His job duties include patient’s sample collection from OPD,Wards, OT’s, ICU (both adults and paediatrics), maintaining records of patient’s clinical data files, sample and reagents/consumable records, patient counselling, PBMC isolation, gel electrophoresis, cell culture media and buffer preparation. He is well versed in the sample processing steps of flow cytometry, macrophage culture, magnetic cell sorting, ELISA and Plasmid isolation (Mini and Midi kits) and is able to carry out flow cytometric data acquisition.
In addition, he is also well trained in the usage of BSL-1 cabinet, Lyophilizer, Multi ELISA reader, Automated cell counter, inverted/ upright microscope, homogenizer, Nanodrop spectrophotometer, cell washer, pH meter, Weighing balance, Autoclave, water bath, hot air oven, centrifuge machines and CO2 Incubator shaker. Currently, he is in the process of learning the data analysis of Flow Cytometry and Mass Spectrometry.
He has previously worked in Sir Ganga Ram Hospital, New Delhi and two other diagnostic centres where he had hands on experience in conducting routine laboratory tests along with RTPCR, ESR,H&E staining, Urine,stool,sputum culture, Leishman, Giemsa,Gram positive and negative staining, Blood group testing, Serology testing (Typhoid, HIV, HCV,HBSAg,Syphilis,Malaria,Dengue IgM/IgG) , BTCT testing and skin test. Apart from this, he gained operational knowledge of instruments like HPLC for HbA1C,ERBA Chem5X(semi-automated),Urinometer (fully automated),Sysmax Coulter, Hemoglobinometer,Fibrometer coagulation and Microtome.
| Designation | Name of the staff member(s) |
|---|---|
| Senior Administrative officer | NA |
| Assistant Administrative Officer | Sh. Ashok Kumar |
| Finance and Chief Accounts Officer | Sh Vijay Pal |
| ANS Nursing Superintendent | Ms. Betty Donna Rawat |
| Store Officer | NA |
| Asstt. Store Officer | Sh Ram Pal Singh |
| AE Civil | Sh Shabad Ali |
| AE Electrical | Sh Satbir Kumar |
| AE (AC & R) | Sh Hem Singh |
| JE ( Civil) | Sh Rakesh Kumar |
| JE (Elec.) | Sh Prashant Kumar |
| JE (AC & R) | Sh Satya Prakash |
| Scientist | NA |
| Medical Social Service Officer | Dr. Brahm Prakash Mr. Deepak Yadav Mr. Dinesh Kumar |
| Biochemist | NA |
| Medical Record Officer | Mr. Harish Chandra |
| Librarian Gr-I | Mr. Pramod Kumar |
| Security Cum Fire Guard Gr.-II | Sh. Pradeep Sh Amit Chillar Sh. Gautam Malik |
| Name | Designation | Contact Address at AIIMS, New Delhi | Clinical Services Schedule |
|---|---|---|---|
| Prof. Anju Dhawan डॉअंजुधवन | Professor & Chief, NDDTC प्राध्यापकएवंप्रमुख राष्ट्रीयव्यसनउपचारकेंद्र | Room No. 4091 Tel: 01126594336 | Monday (General OPD) Wednesday (Administrative rounds) Thursday (Adolescent Clinic) Friday (Ward Rounds) |
| Prof. Sonali Jhanjee डॉसोनालीझांजी | Professor प्राध्यापक | Room No. 4086A Tel: 01126594997 | Monday (Tobacco Cessation Clinic, NDDTC) Wednesday (Ward Rounds) Thursday (Patient education facility) Friday (General OPD) |
| Prof. Atul Ambekar डॉ अतुल अंबेकर | Professor प्राध्यापक | Room No. 4090-B Tel: 01126594094 | Tuesday (DTC, Kotla Mubarakpur) Thursdays (Ward Rounds) Friday (Women’s Clinic) Saturday (General OPD) |
| Dr Yatan Pal Singh Balhara डॉयतनपाल सिंह बल्हारा | Professor प्राध्यापक | Room No 4080-C Tel: 01126593236 | Tuesday (Dual Diagnosis Clinic) Thursday (General OPD) Friday (Ward Rounds) Saturday (Behavioral Addictions Clinic & Dual Diagnosis Clinic), AIIMS, New Delhi |
| Dr Ravindra Rao डॉरविन्द्रराव | Professor प्राध्यापक | Room No 12, Fifth Floor, Port Cabin Tel: 01126593236 | Tuesday (General OPD) Wednesday (Ward Rounds) Thursday (Community Clinic, Sundarnagri) Friday (Consultation Liaison Addiction Psychiatry-CLAP at AIIMS, Delhi) |
| Dr. Ashwani Kumar Mishra डॉअश्वनीकुमारमिश्रा | Professor प्राध्यापक | Room No 4085-D Tel: 01126593236 | A-306 (Tuesday) A-306 (Wednesday) A-306 (Friday) |
| Dr.Rachna Bhargava डॉरचनाभार्गव | Professor प्राध्यापक | Room No 4085-D Tel: 01126593236 | Tuesday (General OPD) Wednesday (Child Guidance Clinic, AIIMS New Delhi) Thursday (Adolescent Clinic, NDDTC) Saturday (Behavioral Addictions Clinic, AIIMS, New Delhi) |
| Dr. Gauri Shanker Kaloiya डॉगौरीशंकरकलोईया | Professor प्राध्यापक | Room No 4085-D Tel: 01126593236 | Monday (Tobacco Cessation Clinic, NDDTC) Tuesday (Tobacco Cessation Clinic, AIIMS, New Delhi) Wednesday (General OPD) Thursdays (Family Empowerment Clinic) |
| Dr Prabhu Dayal डॉप्रभूदयाल | Professor प्राध्यापक | Room No 4085-D Tel: 01126593236 | Tuesday (Tobacco Cessation Clinic, AIIMS New Delhi) Wednesday (General OPD) Thursday (Ward Rounds) Saturday (General OPD) |
| Dr Alok Agrawal डॉआलोकअग्रवाल | Additional Professor अपरआचार्य | Tel: 01126593236 | Wednesday (General OPD) Thursday (Ward Rounds) Friday (DTC, Kotla Mubarakpur/Sarai Kale Khan) Saturday (General OPD) |
| Dr. Biswadip Chatterjee डॉ विश्र्वदीप चटर्जी | Additional Professor अपरआचार्य | Tel: 01126593236 | Monday (General OPD) Wednesday (Community Clinic Trilokpuri) Thursday (Adolescent Clinic) Friday (Ward Rounds) |
| Dr. Rizwana Quraishi डॉरिज़वानाकुरैशी | Additional Professor अपरआचार्य | Tel: 01126593236 | Tuesday (NDDTC Lab) Wednesday (NDDTC Lab) Friday (NDDTC Lab) Saturday (NDDTC Lab) |
| Dr Siddharth Sarkar डॉ सिद्धार्थसरकार | Additional Professor अपरआचार्य | Tel: 01126593236 | Tuesday (Dual Diagnosis Clinic) Thursday (General OPD & Family Empowerment Clinic) Friday (Ward Rounds) Saturday (Community Clinic Trilokpuri) |
| Dr Piyali Mandal डॉ पियालीमंडल | Additional Professor अपरआचार्य | Tel: 01126593236 | Tuesday (Service rounds/Pardabagh Women Clinic) Wednesday (General OPD) Thursday (Ward Rounds) Friday (Women’s Clinic) |
| Dr. Roshan Bhad डॉरोशनभड़ | Additional Professor सहयोगीआचार्य | Tel: 01126593236 | Monday (Community Clinic, Sundernagari) Tuesday (General OPD) Wednesday (Ward Rounds) Thursday (Consultation Liaison Addiction Psychiatry- CLAP), AIIMS, New Delhi |
| Dr Shalini Singh डॉशालिनी सिहं | Associate Professor सहायकआचार्य | Tel: 01126593236 | Monday (Service rounds) Tuesday (Consultation Liaison Addiction Psychiatry-CLAP at AIIMS, New Delhi Wednesday (Ward Rounds) Friday (General OPD) |
As of August 2024
Several faculty members of the centre have served as experts (Members or Chairperson) in national bodies to strengthen drug dependence related activities in the country. These include-
| Name | Designation | Contact Address at AIIMS, New Delhi | Clinical Services Schedule |
|---|---|---|---|
| Prof. Anju Dhawan डॉअंजुधवन | Professor & Chief, NDDTC प्राध्यापकएवंप्रमुख राष्ट्रीयव्यसनउपचारकेंद्र | Room No. 4091 Tel: 01126594336 | Monday (General OPD) Wednesday (Administrative rounds) Thursday (Adolescent Clinic) Friday (Ward Rounds) |
| Prof. Sonali Jhanjee डॉसोनालीझांजी | Professor प्राध्यापक | Room No. 4086A Tel: 01126594997 | Monday (Tobacco Cessation Clinic, NDDTC) Wednesday (Ward Rounds) Thursday (Patient education facility) Friday (General OPD) |
| Prof. Atul Ambekar डॉ अतुल अंबेकर | Professor प्राध्यापक | Room No. 4090-B Tel: 01126594094 | Tuesday (DTC, Kotla Mubarakpur) Thursdays (Ward Rounds) Friday (Women’s Clinic) Saturday (General OPD) |
| Dr Yatan Pal Singh Balhara डॉयतनपाल सिंह बल्हारा | Professor प्राध्यापक | Room No 4080-C Tel: 01126593236 | Tuesday (Dual Diagnosis Clinic) Thursday (General OPD) Friday (Ward Rounds) Saturday (Behavioral Addictions Clinic & Dual Diagnosis Clinic), AIIMS, New Delhi |
| Dr Ravindra Rao डॉरविन्द्रराव | Professor प्राध्यापक | Room No 12, Fifth Floor, Port Cabin Tel: 01126593236 | Tuesday (General OPD) Wednesday (Ward Rounds) Thursday (Community Clinic, Sundarnagri) Friday (Consultation Liaison Addiction Psychiatry-CLAP at AIIMS, Delhi) |
| Dr. Ashwani Kumar Mishra डॉअश्वनीकुमारमिश्रा | Professor प्राध्यापक | Room No 4085-D Tel: 01126593236 | A-306 (Tuesday) A-306 (Wednesday) A-306 (Friday) |
| Dr.Rachna Bhargava डॉरचनाभार्गव | Professor प्राध्यापक | Room No 4085-D Tel: 01126593236 | Tuesday (General OPD) Wednesday (Child Guidance Clinic, AIIMS New Delhi) Thursday (Adolescent Clinic, NDDTC) Saturday (Behavioral Addictions Clinic, AIIMS, New Delhi) |
| Dr. Gauri Shanker Kaloiya डॉगौरीशंकरकलोईया | Professor प्राध्यापक | Room No 4085-D Tel: 01126593236 | Monday (Tobacco Cessation Clinic, NDDTC) Tuesday (Tobacco Cessation Clinic, AIIMS, New Delhi) Wednesday (General OPD) Thursdays (Family Empowerment Clinic) |
| Dr Prabhu Dayal डॉप्रभूदयाल | Professor प्राध्यापक | Room No 4085-D Tel: 01126593236 | Tuesday (Tobacco Cessation Clinic, AIIMS New Delhi) Wednesday (General OPD) Thursday (Ward Rounds) Saturday (General OPD) |
| Dr Alok Agrawal डॉआलोकअग्रवाल | Additional Professor अपरआचार्य | Tel: 01126593236 | Wednesday (General OPD) Thursday (Ward Rounds) Friday (DTC, Kotla Mubarakpur/Sarai Kale Khan) Saturday (General OPD) |
| Dr. Biswadip Chatterjee डॉ विश्र्वदीप चटर्जी | Additional Professor अपरआचार्य | Tel: 01126593236 | Monday (General OPD) Wednesday (Community Clinic Trilokpuri) Thursday (Adolescent Clinic) Friday (Ward Rounds) |
| Dr. Rizwana Quraishi डॉरिज़वानाकुरैशी | Additional Professor अपरआचार्य | Tel: 01126593236 | Tuesday (NDDTC Lab) Wednesday (NDDTC Lab) Friday (NDDTC Lab) Saturday (NDDTC Lab) |
| Dr Siddharth Sarkar डॉ सिद्धार्थसरकार | Additional Professor अपरआचार्य | Tel: 01126593236 | Tuesday (Dual Diagnosis Clinic) Thursday (General OPD & Family Empowerment Clinic) Friday (Ward Rounds) Saturday (Community Clinic Trilokpuri) |
| Dr Piyali Mandal डॉ पियालीमंडल | Additional Professor अपरआचार्य | Tel: 01126593236 | Tuesday (Service rounds/Pardabagh Women Clinic) Wednesday (General OPD) Thursday (Ward Rounds) Friday (Women’s Clinic) |
| Dr. Roshan Bhad डॉरोशनभड़ | Additional Professor सहयोगीआचार्य | Tel: 01126593236 | Monday (Community Clinic, Sundernagari) Tuesday (General OPD) Wednesday (Ward Rounds) Thursday (Consultation Liaison Addiction Psychiatry- CLAP), AIIMS, New Delhi |
| Dr Shalini Singh डॉशालिनी सिहं | Associate Professor सहायकआचार्य | Tel: 01126593236 | Monday (Service rounds) Tuesday (Consultation Liaison Addiction Psychiatry-CLAP at AIIMS, New Delhi Wednesday (Ward Rounds) Friday (General OPD) |
Several faculty members of the centre have served as experts (Members or Chairperson) in national bodies to strengthen drug dependence related activities in the country. These include-
Dr. Gautam Sharma, Prof. In-charge
Participated as a mentor in the meeting of the 2nd CIMER (Centre for Integrative Medicine, Education, and Research) committee. (Virtual participation), organized by AIIMS, Raipur. (29th March 2022)
Title: Newer evidence of Yoga in Medicine at the Cardiology Update and Cardio-Imaging Conference organized under the aegis of Society of Image-guided therapy at Dayanand Medical College and Hospital campus, Ludhiana, Punjab, India. (5th-6th March 2022)
Title: How Yoga Promotes Faster Recovery in Cardiac Rehabilitation” in the 5th Asian Yoga Therapy Association Hybrid Webinar, organized and hosted by VYASA Yoga, Singapore. (25th September 2021)
Title: Yoga for Wellbeing as guest speaker at DD News channel. (20th June 2021)
Title: Effect of Yoga on Clinical Outcomes and Quality of Life in Patients with Vasovagal Syncope (LIVE-YOGA). Venue: International YOGACON USA 2021 organized by American Academy of Yoga Meditation and All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India. (Virtual participation) (13th June 2021)
Participated in the first virtual committee meeting of “Yoga for Productivity”. (24th March 2021)
Participated in a committee meeting for “Formulation of Integrative Health Policy”, NITI Aayog, New Delhi, India. ( 8th October 2020)
Participated in “Rashtriya Arogya Nidhi” meeting. Venue: Directorate General of Health Services (DGHS), Nirman Bhawan, New Delhi. (1st September 2020)
Title: Yoga as Lifestyle Medicine. Venue: “23rd International Conference on Frontiers in Yoga Research and its publications (INCOFYRA)”organized by S-VYASA University, Bengaluru, Karnataka, India. (4th January 2020)
Panel discussion, Title: Back to the Future. Venue: Zee Jaipur Literature Festival. (23rd January 2020)
Panel discussion. Title: Opportunities and Challenges in Integrative Medicine. Venue: All India Institute of Ayurveda (AIIA), New Delhi, India. (22nd November 2019)
Title: Yoga: A Potential adjunct therapy for patients with Cardiac Arrhythmia”. Venue: First symposium on “Role of Meditation for prevention and treatment of Cardiovascular Diseases” Integrated approach to prevention of cardiovascular diseases, All India Institute of Medical Sciences (AIIMS), Rishikesh, Uttarakhand, India. (9th-10th March 2019)
2nd Round Table on “Integrative Medicine”. Venue: NITI Aayog. (6th February 2019)
Title: Integrative Research-Opportunities and Future Directions. Venue: Orientation program conducted for PG scholars at All India Institute of Ayurveda (AIIA), New Delhi. (21st January 2019)
Chairperson of the 10th Annual Conference of the Indian Heart Rhythm Society (IHRS). Venue: The Lalit Hotel, Jaipur, Rajasthan, India. (8th December 2018)
Title: Yoga and Cardiovascular health. Venue: Indian Council of Medical Research (ICMR), New Delhi, India. (21st June 2018)
Sudha Lama (Nursing Officer)
Title: A study to assess parenting stress and psychological health of women having single parenting experience in Delhi-NCR. Venue: Geriatric Nursing: A multidisciplinary approach towards active ageing organized by Rajkumari Amrit Kaur College of Nursing, New Delhi, India. (24th March 2022)
Dr Bharat Krushna Khuptia (Scientist C)
Title: Healthy Ageing: Complementary Medicine insights evidence. Venue: Geriatric Nursing: A multidisciplinary approach towards active ageing Rajkumari Amrit Kaur College of Nursing, New Delhi, India. (23rd March 2022)
Dr. Anupama Gupta (Sr. Medical Officer)
Title: Sleep and the autonomic nervous system: A bidirectional relationship: Restless legs Syndrome and Autonomic function. Venue: World Sleep Congress 2022, Rome, Italy. (15th March 2022)
Dr. Vandna Sharma (Scientist C)
Title: Evaluation of the prophylactic effect of Comprehensive Ayurveda and Mindfulness-based Yoga regimen among health care workers (HCW) of a tertiary care hospital in Delhi during COVID-19 Pandemic: A randomized controlled trial. Venue: international Virtual Convention on Ayurveda and Research advances on COVID-19, organized by Ayurveda College Coimbatore and Diskha E- learning, Coimbatore, Tamil Nadu, India. (Virtual participation) (20th June 2021)
Dr. Shubhangi Rathore (Medical Officer)
Title: Paediatric Developmental Disorders. Venue: Global Ayurveda Medical Travel organized by Confederation of Indian Industry(CII) (Virtual participation). (18th February 2021)
As a part of the 9th IDY week-long celebrations 2023, several events were organized:
A New Approach to Nurture Dynamic Awareness with Mindfulness (ANANDAM) workshops for AIIMS, New Delhi employees:
2023
2022
As a part of the 8th IDY week-long celebrations 2022, several events were organized:
3. Mass yoga practice on IDY (21 st June 2022) at the central lawn, AIIMS, New Delhi (https://www.youtube.com/watch?v=geXHnSxhtpg)
2021
The 7 th IDY was celebrated virtually at AIIMS, New Delhi on 21st June 2021(https://www.youtube.com/watch?v=DZjzIZriSPQt=1564s)
2020
The 6th IDY was celebrated virtually at AIIMS, New Delhi on 21st June 2020 (https://www.youtube.com/watch?v=1pDq-kbj95M)
2019
As a part of the 5th IDY week-long celebrations 2019, several events were organized:
2018
As a part of the 4th IDY week-long celebrations 2018, several events were organized:
2017
As a part of the 3rd IDY week-long celebrations 2017, several events were organized:
1. Self Management of Excessive Tension (SMET) workshops for employees of AIIMS, New Delhi:
2. Mass yoga practice on 21st June 2017 at the central lawn, AIIMS, New Delhi
3. Yoga training program at the Indian Council of Medical Research (ICMR) on 21st June 2017
Training programs
2022
2021
2020
2018
2020
2018
| Name | Designation | Research theme(s)/Laboratory name | |
|---|---|---|---|
| Dr. Kalpana Luthra | Prof. & HOD | kalpanaluthra[at]gmail[dot]com | Laboratory of HIV Immunology |
| Dr.Parthaprasad Chattopadhyay | Professor | parthoaiims[at]hotmail[dot]com | Laboratory of Cell Regulation and Intracellular Trafficking |
| Dr.Kunzang Chosdol | Professor | kunzangchosdol[at]yahoo[dot]com | Laboratory of Cancer Biology and Hypoxia |
| Dr. Sudip Sen | Professor | sudipsen665[at]gmail[dot]com | Stem Cells and Disease Modeling Laboratory |
| Dr.Archna Singh | Professor | arch2574[at]gmail[dot]com | Laboratory of Molecular Nutrition and Mitochondrial Biology |
| Dr.Jayanth Kumar | Additional Professor | jayanth[dot]aiims[at]gmail[dot]com | Translational Molecular Medicine Laboratory |
| Dr. Subhradip Karmakar | Additional Professor | subhradipaiims[at]gmail[dot]com subhradip[dot]k[at]aiims[dot]edu | Laboratory for Placenta Biology and Molecular Oncology |
| Dr.Archana Singh | Additional Professor | archanasinghmamc[at]gmail[dot]com | Laboratory of Tuberculosis Immunology and Clinical Chemistry |
| Dr.Ashok Sharma | Additional Professor (Neurobiochemistry) | ashoksharma1202[at]gmail[dot]com | Laboratory of Chromatin and Cancer Epigenetics |
| Dr. Pragyan Acharya | Additional Professor | Dr.pragyan[dot]acharya[at]gmail[dot]com | Laboratory of Liver Disease Signaling and Immunology |
| Dr.Riyaz Ahmad Mir | Additional Professor | riyaz978[at]gmail[dot]com | Cancer Biology and Regenerative Medicine |
| Dr. Pramod Kumar Gautam | Additional Professor | pramodgautam_13[at]yahoo[dot]com | Laboratory of Immunology and Cancer Immunotherapy |
| Dr.Rakhee Yadav | Additional Professor | rakheeyadav79[at]gmail[dot]com | Laboratory of Adipocyte Biology and Insulin Resistance |
| Dr.Siddhartha Kundu | Associate Professor | siddhartha_kundu[at]yahoo[dot]co[dot]in | Mathematical and Computational Biochemistry |
| Dr. Karthikeyan P. | Assistant Professor | karthi[dot]dr[at]gmail[dot]com |

2. Name: Dr Shalini Singh
3. Designation:
| Name of institute | Designation | From | To |
|---|---|---|---|
| All India Institute of Medical Sciences, Delhi | Assistant Professor, National Drug Dependence Treatment Centre | September 2019 | Ongoing |
| Institute of Liver Biliary Sciences, Delhi | Assistant Professor, Psychiatry | January 2019 | September 2019 |
| All India Institute of Medical Sciences, Delhi | Senior Resident, Psychiatry | February 2015 | December 2018 |
| Vardhman Mahavir Medical College, Delhi | Senior Resident, Psychiatry | August 2014 | February 2015 |
| Lady Hardinge Medical College, Delhi | Junior Resident, Psychiatry | May 2011 | April 2014 |
| Mayo Clinic | Research trainee, Gastroenterology Division | May 2009 | December 2009 |
4. Qualifications :
| Name of institute | Qualification | From | To |
|---|---|---|---|
| All India Institute of Medical Sciences, Delhi | DM, Addiction Psychiatry | 2016 | 2018 |
| Lady Hardinge Medical College, Delhi | MD Psychiatry | 2011 | 2014 |
| Maulana Azad Medical College, Delhi | MBBS | 2003 | 2009 |
5. Email ID :- shalin.achra@gmail.com
6. Field of Interest
Consultation Liaison Addiction Psychiatry
Management of alcohol dependence in those with alcohol related liver disease
Safe use of opioids for management of chronic non-cancer pain
Viral hepatitis in those who inject drugs: improved screening protocols
Prevention of substance use disorders
Student wellness
Training of healthcare professionals in management of substance use disorders
7. Total number of publications till date: >40
8. Details of publications since 2010 onwards (the full citation)- these should be divided into journal articles (peer reviewed publications) and books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications)
Journal articles:
Book chapters:
Books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications)
9. Presentations made at scientific meetings/ conferences/ workshops
| S. No. | Title of the talk | Name of the CME/conference | Date | City |
|---|---|---|---|---|
| Drug use among students, how to prevent and what are the harms? | Wellness symposia for Undergraduate and postgraduate students: “MATE (Mind Activation Through Education)” AIIMS | 14th January, 2023 | AIIMS, Delhi | |
| Prevention and Management of substance Misuse | Training of Prospective Resource Person for roll out of School Health and Wellness Programme in CBSE affiliated schools in collaboration with UNESCO | August, 2022 | NCERT, Delhi | |
Making the Medical Curriculum Queer affirmative
| INSIGHT 2020 | 15th April 2022 | AIIMS, Delhi | |
| Screening, Assessment and Diagnosis of Substance Use Disorders | Online training program for clinical staff of Ministry of Social Justice and Empowerment (MoSJE) supported IRCAs and ODICs | 31st March, 2022 | Delhi (online) | |
| Interviewing a Patient with Substance Use Disorder – Attitude And Skills | Online training program for clinical staff of Ministry of Social Justice and Empowerment (MoSJE) supported IRCAs and ODICs | 31st March, 2022 | Delhi (online) | |
| Overview of Opioid Use Disorders | Online training program for clinical staff of Ministry of Social Justice and Empowerment (MoSJE) supported IRCAs and ODICs | 21st December, 2021 | Delhi (online) | |
| Management of Tobacco Dependence | 21st December, 2021 | Delhi (online) | ||
| Management of Cannabis Dependence and associated conditions | 29th November, 2021 | Delhi (online) | ||
| Management of Benzodiazepine Dependence | 29th November, 2021 | Delhi (online) | ||
| Operational aspects of medical treatment for substance use disorders | 9th April, 2021 | Delhi (online) | ||
| Can a neighborhood fall sick? Opioid addiction, collective violence, and currents of death in contemporary India. | Lecture series organized by Centre for Study of Developing Societies, India | 29th January, 2021 | Delhi (online) | |
| Opioid dependence syndrome: concepts and treatment | Substance Use Disorder Nursing Training Program, Lady Hardinge Medical College | 21 January 2020 | Delhi | |
Clinical communication with patients and overcoming challenges
| Workshop for junior nursing officers working in AIIMS Main Hospital to enhance soft skills
| 21 February 2020 | Delhi | |
| Epidemiology of behavioral addictions | Nurses’ training of trainers program on behavioral addictions, AIIMS Delhi College of Nursing | 9 March 2020 | Delhi | |
Naltrexone Implant in Addiction Psychiatry
| XXI Annual Conference of the International Society of Addiction Medicine
| 13 November 2019 | Delhi | |
Super- Specialty course in Addiction Psychiatry in India
| XXI Annual Conference of the International Society of Addiction Medicine
| 16 November 2019 | Delhi | |
| Pharmacological management of opioid dependence syndrome | Nurses training of trainers program on substance use disorders, AIIMS Delhi College of Nursing | 30 November 2019 | Delhi |
10. Investigator/ Co-investigator in funded projects along with year completed/ongoing
As principal investigator:
| S. No. | Title of the project | Funded by (Name of funding agency) | Duration (years) | Start year | End year | Total funds sanctioned (Rs) |
|---|---|---|---|---|---|---|
| A Cross-Sectional Study to Screen for Psycho-sexual Health Disorders and Measure Neurochemical Correlates in Gynaecology Cancer Survivors | Intramural Collaborative Research Project for the year 2020 – 2021 | 2 years | 2021 | 2023 | 14,24,000 | |
| HIV, Hepatitis B and C testing in individuals receiving agonist treatment for injecting drug use at a community clinic in Delhi: a cross sectional assessment of risk factors and seroprevalence. | AIIMS Early Career Intramural Research Project for the year 2021 – 2022 | 18 months | 2022 | 2023 | 4,44,000 |
As co-investigator
| S. No. | Title of the project | Funded by (Name of funding agency) | Duration (years) | Start year | End year | Total funds sanctioned (Rs) |
|---|---|---|---|---|---|---|
| An exploratory case- control study to assess the protective genetic factors against alcoholic liver disease among population from northern part of India | AIIMS-Intramural | 3 years | 2017 | 2021 | 5 Lakh | |
| Establishing and Implementing capacity building mechanisms for addiction treatment facilities in India | Ministry of Health and Family Welfare | 5 years | 2019 | 2024 | 12 Crore | |
Setting up of a TeleMedicine and online resource hub on mental health and addictive disorders for South East Asia
| World Health Organisation-SEAR | 1 year | 2020 | 2021 | 10 Lakh | |
Development of module on prevention of substance use and addiction among students for the teachers from the state of Chhattisgarh
| Government of Chhattisgarh | 1 year | 2020 | 2021 | 10 Lakh | |
Development and evaluation of service delivery models for management of substance use disorders among the homeless population receiving urban shelter services in Delhi
| Department of Women and Children (WCD), Ministry of Health and Family Welfare, Government of Delhi | 2 years | 2020 | 2022 | 30 Lakh |
| S. No. | Title of the project |
|---|---|
| A cross sectional study to measure the frequency of the BDNF gene polymorphism (Val66Met) in patients seeking treatment for Alcohol Dependence syndrome (ADS) | |
| Feasibility of ecological momentary assessment to measure associations between perceived control over alcohol use, craving, mood and daily alcohol consumption in treatment-seeking patients of alcohol dependence syndrome | |
| Association of the galanin and galanin receptor gene polymorphism (rs948854) and opioid dependence: A case control observational study | |
| Substance use among homeless women receiving services from shelter homes in Delhi | |
| Prevalence and correlates of neurological and neurocognitive disorder in HIV positive patients on ART |
12. Thesis supervised for MD/ DM/PhD
- as guide 1
-as co-guide 5
13. Awards and Honours
14. Any other relevant information
| Title |
| Submission of Ph.D seat requirements for January 2025 session |
| Allocation of thesis CHIEF GUIDE in respect of students who are pursuing M.D.(Biochemistry)for JULY-2024 SESSION-Modification regarding |
| Allocation of thesis CHIEF GUIDE in respect of students who are pursuing MDS(Paediatrics and Preventive Dentistry) for July-2024 SESSION-Modifications regarding |
| Re-allocation/revision of MD thesis CHIEF GUIDE in respect of following students who are pursuing MD (Medicine) - Modification regarding. |
| Arrangement for TWO MONTHS Extension for submission of THESIS PROTOCOL in respect of Jr. Resident (MD/MS/MDS/DM/MCH)(6 Years Course) & Sr. Residents (DM/MCH (3 Years Course) enrolled in JANUARY-2024 Session at AIIMS, New Delhi - reg. |
| Mutual exchange of MS/MCH thesis CHIEF GUIDE in respect of following students who are pursuing MS/MCH - Modification reg. |
| Allocation of thesis CHIEF GUIDE in respect of student who are pursuing (Forensic Medicine) for JULY-2023 SESSION - Modifications regarding. |
| Allocation of thesis CHIEF GUIDE in respect of student who are pursuing M.S.(Otorhinolarngology) for JANUARY -2024 SESSION - Modifications regarding. |
| Allocation of thesis CHIEF GUIDE in respect of student who are pursuing (Hospital Administration) for JANUARY -2024 SESSION - regarding. |
| Allocation of thesis CHIEF GUIDE in respect of student pursuing M.D. (Radiodiagnosis) for JANUARY -2024 SESSION - Modifications regarding. |
| Matter regarding non-allotment of MSc/M.Biotechnology/M.Sc Nursing students to all Faculty at AIIMS, New Delhi - reg. |
| Allocation of Thesis Chief Guide in respect of Sr. Resident/Sponsored Trainee DM/M.Ch) for the July,2023 session - reg. |
| Addtional extension for submission of THESIS deadline in respect of the students pursuing MD/MS/MDS t AIIMS, New Delhi - Final examination is due in MAY-2023 - reg. |
| Academic guidelines/rules for submission of Thesis Protocol/Thesis in respect of the Resident (PG) pursuing MD/MS/MDS/DM/MCH course at AIIMS, NEw Delhi - reg. |
| Arrengement for TWO MONTHS Extension for sumbission of THESIS PROTOCOL in respect of J.R (MD/MS/MDS/& DM/MCH (3 years Course) encolled in JULY 2023 Session, AIIMS, New Delhi - reg. |
| Allocation of thesis Chief Guide in respect of Student Pursing MD/MS/MDS/DM/MCH (6 years) course for July,2023 session.- reg. |
| Allocation of thesis Chief Guide in respect of Dr. Asmita Gautam, Pursuing (Anaesthesiology) for July-23 Session - Revised list of thesis Chief Guide reg. |
| Allocation of thesis Chief Guide in respect of Student Pursing MD/MS/MDS/DM/MCH (6 years) course for July,2023 session.- reg. |
| Allocation of thesis Chief Guide in respect of Student Pursing MD/MS/MDS/DM/MCH (6 years) course for July,2023 session.- reg. |
| Allocation of thesis Chief Guide in respect of Student Pursing MD/MS/MDS/DM/MCH (6 years) course for July,2023 session.- reg. |
| Allocation of thesis Chief Guide in respect of Sr. Resident/Sponsored Trainee DM/M.Ch for July,2023 session. reg. |
| Allocation of thesis Chief Guide in respect of Sr. Resident/Sponsored Trainee DM/M.Ch for July,2023 session. reg. |
| Extenstion of submission of THESIS deadline in respect of the MD/MS/MDS students of January -2021 at AIIMS, New Delhi - Final Professional examination is due in December-2023 - reg.. |
| Arrangement for Two Months extension for submission of Thesis Protocol in respect of Jr. Residents ( Acad.)/Sr. Residents ( Acad.) enrolled in January-23 session for MD/MS/MDS/DM/MCH course at AIIMS, New Delhi- reg. |
| Allocation of thesis Chief Guide in respect of students pursuing MD/MS/MDS.DM/MCH ( 6 years) course for January-2023 Session - reg. |
| Allocation of thesis Chief Guide in respect of students pursuing MD/MS/MDS.DM/MCH ( 6 years) course for January-2023 Session - reg. |
| To streamline the procedure regarding allocation of thesis chief guide in respect of Senior Resident/Sponsored Trainee DM/M.Ch- regarding. |
| To streamline the procedure regarding allocation of thesis chief guide in respect of Senior Resident/Sponsored Trainee DM/M.Ch- regarding. |
| Allocation of thesis Chief Guide in respect of students pursuing MD/MS/MDS.DM/MCH ( 6 years) course for January-2023 Session - reg. |
| Allocation of thesis Chief Guide in respect of students pursuing MD/MS/MDS.DM/MCH ( 6 years) course for January-2023 Session - reg. |
| Extionsion of rsubmission of thesis/dissertation deadline in respect of the Sr. Residents/Sponsored Trainee pursuing DM/M.Ch course at AIIMs, New Delhi in view of COVID-19 Pandemic - Final examination is due in May2023 - reg.. |
| Request for retaiing Deptt. Allotted Thesis Guide for 2nd Thesis for 6 year M.Ch candidates Deptt. of Neurosurgery. |
| To streamline the procedure regarding allocation of thesis chief guide in respect of Senior Resident/Sponsored Trainee DM/M.Ch-regarding. |
| To streamline the procedure regarding allocation of thesis chief guide in respect of Senior Resident/Sponsored Trainee DM/M.Ch-regarding. |
| Arrangement for Two Months extension for submission of Thesis Protocol in respect of the students enrolled in July 2022 Session for MD/MS/MDS/DM/MCH course at AIIMS, New Delhi-regarding. |
| Arrangement for Two Months extension for submission of Thesis Protocol in respect of the students enrolled in July 2022 Session for MD/MS/MDS/DM/MCH course at AIIMS, New Delhi-regarding. |
| Arrangement for Two Months extension for submission of Thesis Protocol in respect of the students enrolled in July 2022 Session for MD/MS/MDS/DM/MCH course at AIIMS, New Delhi-regarding. |
| To streamline the procedure regarding allocation of thesis chief guide in respect of Senior Resident/Sponsored Trainee DM/M.Ch-regarding. |
| Allocation of thesis Chief Guide in respect of students pursuing MD (Psychiatry)- regarding. |
| Allocation of thesis Chief Guide in respect of students pursuing MD/MS/MDS & DM/MCH (6 years Course)- regarding. |
| Implementation of Top Class College Education Scheme for OBC, EBC, DNT during the year 2022-23. |
| Grant of Temporary Permission under section 14 (1) of the IMC, Act 1956 read with section 61(2) of the Naitonal Medical Commission Act-2019 Mandatory compliance of the National Medical Commission oACt-2019 by all the Foreign nationals Residents reg. |
| To Streamline othe procedure regarding allocation of Thesis Chief guide in respect of Sr. Resident/Sponsored Trainee DM/M.Ch) reg.. |
| State/UT/Community-wise physical allocation of scholarship and Timeline Activities under the Two scholarship Schemes viz. Post-Matric and Merit cum means Scholarship schemes for minorities Communities for the year 2022-23. |
| To streamline the procedure regarding allocation of thesis CHIEF Guide in respect of students pursuing MD/MS/MDS/DM/MCH - reg. |
| To streamline the procedure regarding allocation of thesis CHIEF Guide in respect of students pursuing MD/MS/MDS/DM/MCH - reg. |
| To streamline the procedure regarding allocation of thesis CHIEF Guide in respect of students pursuing MD/MS/MDS/DM/MCH - reg. |
| To streamline the procedure regarding allocation of thesis CHIEF Guide in respect of students pursuing MD/MS/MDS/DM/MCH - reg. |
| Standard Operating Procedure for MSc/M. Biotechnology/MSc Nursing Courses at AIIMS, New Delhi - reg. |
| Anti Ragging Squad Duty roster for Gents & Ladies Hostels form 14th Feb. to 14th March, 2022. |
| Suspension of Sort term & Elecctive Training - reg. |
| Arrangement for Academic activities in view of recent spurt of COVID-19 cases. |
| Training in "Infection Control Managements" for Resident Doctors - Mandatory compliance of training reg.. |
| Arrangement for Academic activities in view of recent spurt of COVID-19 cases. |
| E-Training in "COVID-19 Managements" for Resident Doctors - Mandatory compliance of training regarding |
| Addition extension for submission of thesis deadline in respect of the students pursuing MD/MS/MDS at AIIMS, New Delhi in view of COVID-19 Pandemic-Final examination due in May 2022 |
| Clarification regarding deadline for submission of THESIS in respect of the students pursuing DM/M.Ch (6 years Course) at AIIMS, New Delhi - Final examination is due in MAY-2022. |
| Additional extension for submission of THESIS deadline in respect of the students pursuing MD/MS/MDS at AIIMS, New Delhi in view of COVID-19 pandemic - Final examination is due in MAY-2-22 - reg.. |
| Nomination/addition of any Regular Faculty in place of Contractual Faculty a thesis Co-Guide in respect of Resident Doctors - reg. |
| Extension for submission of Thesis deadline in respect of the students pursuing MD/MS/MDS/DM/M.Ch 6yeras course at AIIMS, New Delhi in view of COVID-19 Pandemic-Final examination is due in May-2022-Regarding |
| < Reimbursement to student for ATLS/ACLS/BLS courses conducted by the outside agencies / societies |
| < Endorsement of advice / prescription putting clear signature and rubber stamp by Resident Doctors in respect of OPD /IPD patients at AIIMS, New Delhi - Regarding |
| < Modification in Protocol, Thesis submission and final examination thereof in respect of M.Biotechnology and M.Sc. students enrolled in August 2020 Session in various courses at AIIMS, New Delhi in view of COVID-19 Pandemic-Regarding |
| < Recommencement of Short Term/LongTerm & Elective Training Programmes for Foreign Nationals - reg |
| < रेजीडेटं चिकित्सकों हेतु कोविड-19 प्रबंधन में ई-सटिंफिकेट पाठ्यक्रम प्रशिक्षण- प्रशिक्षण पाठ्य़क्रम के अनिवार्य अनुपालन संबंधी/Training for “E-Certificate Course in COVID-19 Managements” for Resident Doctors – Mandatory complance of training couse regarding |
| < Additional extension of deadline for submission of THESIS PROTOCOL in respect of thestudents enrolled in january-21 session in various courses at AIIMS, New Delhi in view of COVID-19 Pandemic - reg. |
| < Inviting nomninations for Orations - reg. |
| < अल्प अवधि /दीर्ध अवधि एवं वैकल्पिक प्रशिक्षण को पुन: आंरभ करने संबंधी. |
| < अल्प अवधि /दीर्ध अवधि एवं वैकल्पिक प्रशिक्षण को पुन: आंरभ करने संबंधी. |
| < एम्स, ऩई दिल्ली में जुलाई-2020 तथा जनवरी 2021 सत्र के लिए स्नातकोत्तर पाठ्यक्रम ( एमडी /एमएम /एमडीएस) की नामावली में परिवर्तन संबंधी/Change of nomenclature for PG course ( MD/MS/MDS) for July 2020 & January-2021 Session at AIIMS, New Delhi – reg. |
| < Recommencment of Short/Term/Long Term & Elective Training - reg. |
| < Revised schedule of Pre-Professional Examination of IX semester from 1st Dec. to 24th Dec. 2020 |
| < Implementation of Three Scholarship Schemes : Progress and Monitoring in FY 2020-21 |
| < Cancellation of Short Term & Elective Training - reg. |
| < आपातकालीन चिकित्सा विभाग में जूनियर रेजिडेटों ( शैक्षिक) की रोटेशन निति तैयार करके आपातकालीन चिकित्सा विभाग में रोगी उपचार सेंवाएं सुद्धढ करने के लिए जूनियर रेजिडेटों की संख्या बढाने संबंधी/ Augmentation of manpower to strengthen the patient care services in the Deptt. Of Emergency Medicine by formulating rotation policy of Jr. Residents ( Academic) to the Deptt. Of Emergency Medicine – Reg. |
| < अ.भा.आ.सं. ऩई दिल्ली में कुछ रेजीडेट चिकित्सकों का प्राईवेट प्रैक्टिस/प्राईवेट कार्य में शामिल होने तथा कोचिंग संस्थानों के साथ संल्गन होने पर निषेधात्मक आदेश संबंधी/Involvement of some of the Resident Doctors, AIIMS in private practice/Private work & attachment with Coaching Institutions – Prohibition order reg. |
| < Revision of tution fee for the undergraduate Programmes |
| < Re-activation of the National Scholarship Portal (NSP 2.0) for inviting applications ( fresh and renewal both) under National Scholarship for Higher Education for ST students for the financial year 2020-21 |
| < Insturctions for Students for filling the Application form in NSP 2020-21 |
| < FAQ's for Students for NSP 2020-21 |
| < Re-activation of the National Scholarship Portal (NSP 2.0) for inviting applications ( fresh and renewal both) under National Scholarship for Higher Education for ST students for the financial year 2020-21 |
| < Implementation of Centrally Sponsored Schemes/Central Sector Schemes in NCT of Delhi |
| < Submission of Ph.D seat details for Ph.D Prospectus for the July, 2020 session. |
| < Submission of Thesis by students enrolled in various courses at AIIMS, New Delhi in view of the COVID-19 Pandemic |
| < स्नातकोत्रर पाठ्यक्रमों हेतु मूल्यांकनकर्ताओं की सूची को अपडेट करनें संबंधी/ Updating Assessor’s list for postgraduate course |
| < NIRF, M/o HRD- Data Capture System - Medical |
| < थीसीस/डीसर्टेशन को दोनों तरफ से मुद्रित किए जाने संबंधी।/Printing of Thesis/Dissertation in both side-regarding |
| < अ.भा.आ.सं. ऩई दिल्ली में विभिन्न एम.एस.सी./मास्टर डिग्री पाठ्यक्रमों की नामावली में परिवर्तन/Change of Nomenclature in respect of various M.Sc/Master Degree Courses at the AIIMS, New Delhi |
| < Regarding two Scholarship Schemes for minority communities viz Post matric and Merit-cum-Means for the year 2019-20 |
| < ऱेजीडेन्ट चिकित्सकों के संबंध में थिसिस के सह-गाइड के रुप में नियमित संकाय-सदस्च के नामांकन संबंधी/ Nomination of Regular Faculty as thesis Co-Guide in respect of Resident Doctors – reg. |
| < रेजीडेट डांक्टर्स के संबंध में सबमिशन-त्यागपत्र की सूचना-अनुपस्थिति रिपोर्ट एवं अवकाश प्रार्थना पत्र संबंधी/ Submission intimation of resignation/absentee report and leave application in respect of Resident Doctors – reg. |
| < कनिष्ठ रेजीडेट ( शेक्षिक) को शैक्षिक छुट्टियों आंन ड्यूटी छुट्टियों के दौरान सीएमई/ सम्मेलन/ संगौष्टी /कार्यशाला इत्यादि ( देश में या विदेश में) में भाग लेने के लिए दिशा-निर्देश/ Guidelines for attending CME/Conference/Symposium/Workshop/etc. (within country or abroad) on Academic leaves/On duty leaves in respect of Jr. Residents (Academic) – reg. |
| < आपात चिकित्सा विभाग में अपात चिकित्सा विभाग के रेजीडेट के लिए रोटेशन नीति बनाकर रोगी उपचार सेंवाओं को सशक्त करने के लिए कर्मचारियों की सख्या बढानें संबंधी/ Augmentation of Manpower to strengthen the patient care services in the Dptt. Of Emergency Medicine by formulating Rotation policy of Jr. Residents to the Deptt. Of Emergency Medicine – Reg. |
| < Internship Programme of Intern from 01.01.2019 to 31.12.2019 |
| < Guidelines for leaves to Jr. Residents (Academic) Pursing MD/MS/MDS/M.Ch - reg |
| < Mandatory Postgraduate Research Methodology Course and Qualifying Exam from Academic Session January 2019 onward regarding |
| < Section 15(6) of Delhi Medical Council Act 1997 - Mandatory compliance of the Delhi Medical Council Act by all the Resident Doctors regarding |
| < Training Programme on "Deceased organ and Tissue Donation" by ORBO for all Residents Doctors - Mandatory compliance of Training Program and submission of certificate regarding |
| < Section 15(6) of Delhi Medical Council Act 1997 - Mandatory compliance of the Delhi Medical Council Act by all the Resident Doctors regarding |
| < Guidelines for submission of thesis protocol/ thesis and eligibility for Chief Guide in respect of Jr/Sr. Residents (Academic) pursuing MD/MS/MDS/DM/M.Ch- regarding |
| < Submission of thesis protocol/thesis in respect of Junior Resident (PG) regarding |
| < Rotation of Senior Residents in different Departments/Centres - reg |
| < Request for grant of permission to attend the various meetings/Conferences/Symposium/Training and workshop etc. in India and abroad for students -reg. |







The Department of Biochemistry was set up when the Institute was established as a center of national importance for teaching, research and patient care in 1956 by an Act of Parliament. The department is globally recognized for its quality of teaching (undergraduate, postgraduate), medical research, patient care, and training. We conduct lectures and practical exercises for the under (MBBS)- and post (MD)-graduate medical, basic and applied courses (M.Sc., M. Biotechnology) as well as undergraduate Nursing (B.Sc.) classes. In undergraduate teaching we employ innovative teaching techniques such as Problem Based Learning. The postgraduate (M.D., M.Sc.) and doctoral (Ph.D.) candidates undertake their thesis work under the supervision of the faculty. A recent development is the conduct of practical classes for the D.M. program (Medical genetics). Our department is located on the third floor of the Old teaching block and the fourth floor of the Convergence block. Our laboratories (UG, PG) are well equipped and can accommodate several students simultaneously. We have several central/shared instrumentation rooms which the faculty, residents and students utilize for research, teaching and training activities. Presentations, are regularly held in the demonstration- and seminar-rooms.
| Sr. No. | Group | Strength |
|---|---|---|
| 1. | Faculty | 15 |
| 2. | Staff | 23 |
| 3. | Scientists | NA |
| 4. | Senior Residents | 09 |
| 5. | Enrolled students (M.D., M.Sc.) and research scholars (Ph.D.) | 63 |
| 6. | Pre-and postdoctoral research scholars (associates, assistants, fellows) | NA |
Our faculty are well trained and have worked in research laboratories (national, international) of repute. Our faculty are engaged extensively in research related to basic, clinical and translational biomedical research. The funding for research is obtained from intra- and extra-mural research grants and is drawn from national (Department of Biotechnology, DBT; Wellcome-DBT India Alliance, Indian Council of Medical Research, ICMR; Department of Science and Technology, DST; Defence Research and Development Organization, DRDO; Ayush; Ministry of Electronics and Information Technology, MEiTY) and international (National Institutes of Health, NIH) funding agencies. Our faculty actively participates in mentoring undergraduates (ICMR-Short term studentship, AIIMS undergraduate mentorship program, KVPY). Undergraduate students are also actively encouraged to join the faculty as part of their summer fellowship.
The research work of the faculty is diverse and includes classical Biochemistry in association with “omics’-based protocols and analytics. A detailed introduction to each faculty member’s research work and laboratory is available at their individual URLs. A generic classification of the current faculty includes biochemical and immunological alterations during cancer progression (Kunzang Chosdol, Subhradip Karmakar, Jayanth Kumar, Ashok Sharma, Riyaz Mir, Pramod Gautam), infection, inflammation and immunological mechanisms (Alpana Sharma, Kalpana Luthra, Archana Singh, Ashok Sharma, Pragyan Acharya), nanoparticles and drug-delivery systems (Parthaprasad Chattopadhyay), metabolic and nutritional basis of obesity (Archna Singh, Rakhee Yadav), stem cell biology (Sudip Sen), mathematical and computational analysis of biochemical systems (Siddhartha Kundu). Faculty members are encouraged to participate in collaborative work.
The department has initiated a Guest Lecture Series wherein external faculty members who have made significant contribution(s) to their research domains are invited to present and discuss their work with faculty members, students and research fellows. The presentations are meant to be informal, interactive and informative and the speakers are encouraged to share their scientific journey with the attendees. Several prominent scientists such as Sivaprakash Ramalingam (IGIB, New Delhi), Pawan Dhar (JNU, New Delhi), Arpan Banerjee (NBRC, New Delhi), Soumen Basak (NII, New Delhi), Sheetal Gandotra (IGIB, New Delhi), Sujatha Sunil (ICGEB, New Delhi), Rama Akondy (Ashoka University, New Delhi), Raviraj Venkalaya (IIT, Jodhpur), Bushra Ateeq (IIT Kanpur), Manidipa Banerjee (IIT Delhi) have already done so. Our students and faculty have also benefitted from interactions with speakers such as Prof. Anil K Bamezai (Villanova University, USA), Drs.Vijay Reddy Peddareddigari, Imran Khan (Bristol Myers Squibb) and Vivek TN (IGIB, New Delhi).
The curricula is vibrant with regular opportunities for students to interact with faculty and other members. These include journal club presentations and seminars. Newly enrolled students (M.D., M.Sc.) undergo a departmental rotation with all faculty members. They are then required to join a faculty under whose supervision they will work on a research problem, present their protocol and submit their dissertation. Several new modules have been introduced for the newly enrolled students. These include microteaching (innovative teaching methods, problem-based learning), an introduction to “R”-driven data analytics and soft-skill training. Additionally, the students are examined for their proficiency in general Biochemistry through regular assessments. The Ph.D. program, includes course work which is spread over two semesters. This is composed of didactic classes and includes generalized and specialized Biochemistry, biomedical waste management, ethics, and Biostatistics. Practical training via hands-on laboratory work is practiced. This is aimed at orienting and equipping the scholars with the knowledge and means to undertake full-time research work. The scholars are issued a completion certificate at the end of this.
E-mail: shalin.achra@gmail.com
| Name of institute | Designation | From | To |
|---|---|---|---|
| All India Institute of Medical Sciences, Delhi | Assistant Professor, National Drug Dependence Treatment Centre | September 2019 | Ongoing |
| Institute of Liver Biliary Sciences, Delhi | Assistant Professor, Psychiatry | January 2019 | September 2019 |
| All India Institute of Medical Sciences, Delhi | Senior Resident, Psychiatry | February 2015 | December 2018 |
| Vardhman Mahavir Medical College, Delhi | Senior Resident, Psychiatry | August 2014 | February 2015 |
| Lady Hardinge Medical College, Delhi | Junior Resident, Psychiatry | May 2011 | April 2014 |
| Mayo Clinic | Research trainee, Gastroenterology Division | May 2009 | December 2009 |
| Name of institute | Qualification | From | To |
|---|---|---|---|
| All India Institute of Medical Sciences, Delhi | DM, Addiction Psychiatry | 2016 | 2018 |
| Lady Hardinge Medical College, Delhi | MD Psychiatry | 2011 | 2014 |
| Maulana Azad Medical College, Delhi | MBBS | 2003 | 2009 |
Total number of publications till date: >40
Details of publications since 2010 onwards (the full citation)- these should be divided into journal articles (peer reviewed publications) and books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications)
Shalini Singh, and Yatan Pal Singh Balhara. “A Review of Indian Research on Co- Occurring Cannabis use Disorders & psychiatryc Disorders " Indian Journal of Medical Research 146 no. 2( Feb.1, 2017) 186 .
Yatan Pal Singh Balhara, Ashwani Mishra, Hem Sethi, Shalini Singh, and Sudhir Kumar Khandelwal. “Time Trends of Cannabis Use Among Treatment-Seeking Individuals at Government De-Addiction Centers Across India Over a Period of 7 Years.” Indian Journal of Psychological Medicine 38, no. 4 (2016): 331–35.
Yatan Pal Singh Balhara, Shaul Lev-Ran, José Martínez-Raga, Amine Benyamina, Shalini Singh, Lisa Blecha, and Nestor Szerman. “State of Training, Clinical Services, and Research on Dual Disorders Across France, India, Israel, and Spain.” Journal of Dual Diagnosis 12, no. 3–4 (October 1, 2016): 252–60.
Mina, Shaily, Masarat Jabeen, Shalini Singh, and Rohit Verma. “Gender Differences in Depression and Anxiety Among Atopic Dermatitis Patients.” Indian Journal of Dermatology 60, no. 2 (2015): 211.
Budania, Satish Kumar, Monika Rathi, Shalini Singh, and Suresh Yadav. “Serum Cholesterol and Depression: A Puzzle Never Finished.” Journal of the Scientific Society 42, no. 2 (May 1, 2015): 59.
Shruti, Aggarwal, Shalini Singh, and Dinesh Kataria. “Knowledge, Attitude and Social Distance Practices of Young Undergraduates towards Mental Illness in India: A Comparative Analysis.” Asian Journal of Psychiatry 23 (October 1, 2016): 64–69.
Shalini Singh, Shruti Aggarwal, Suman Kumar Sinha, and Dinesh Kataria. "How are you feeing today doctor? Mental wellbeing of young medical professionals: A cross- sectional analysis. Free papers (posters).” Indian Journal of Psychiatry 56, no. Suppl 1 (January 2014): S63–96.
Buttar, Navtej S., Cathrine J. DeMars, Gwen Lomberk, Sumera Rizvi, Juliana Bonilla-Velez, Shalini Achra, Shahrooz Rashtak, Kenneth K. Wang, Martin E. Fernandez- Zapico, and Raul Urrutia. “Distinct Role of Kruppel-like Factor 11 in the Regulation of Prostaglandin E2 Biosynthesis.” The Journal of Biological Chemistry 285, no. 15 (April 9, 2010): 11433–44.
| S. No. | Title of the talk | Name of the CME/conference | Date | City |
|---|---|---|---|---|
| 1 | Drug use among students, how to prevent and what are the harms? | Wellness symposia for Undergraduate and postgraduate students: “MATE (Mind Activation Through Education)” AIIMS | 14th January, 2023 | AIIMS, Delhi |
| 2 | Prevention and Management of substance Misuse | Training of Prospective Resource Person for roll out of School Health and Wellness Programme in CBSE affiliated schools in collaboration with UNESCO | August, 2022 | NCERT, Delhi |
| 3 | Making the Medical Curriculum Queer affirmative | INSIGHT 2020 | 15th April 2022 | AIIMS, Delhi |
| 4 | Screening, Assessment and Diagnosis of Substance Use Disorders | Online training program for clinical staff of Ministry of Social Justice and Empowerment (MoSJE) supported IRCAs and ODICs | 31st March, 2022 | Delhi (online) |
| 5 | Interviewing a Patient with Substance Use Disorder – Attitude And Skills | Online training program for clinical staff of Ministry of Social Justice and Empowerment (MoSJE) supported IRCAs and ODICs | 31st March, 2022 | Delhi (online) |
| 6 | Overview of Opioid Use Disorders | Online training program for clinical staff of Ministry of Social Justice and Empowerment (MoSJE) supported IRCAs and ODICs | 21st December, 2021 | Delhi (online) |
| 7 | Management of Tobacco Dependence | - | 21st December, 2021 | Delhi (online) |
| 8 | Management of Cannabis Dependence and associated conditions | - | 29th November, 2021 | Delhi (online) |
| 9 | Management of Benzodiazepine Dependence | - | 29th November, 2021 | Delhi (online) |
| 10 | Operational aspects of medical treatment for substance use disorders | - | 9th April, 2021 | Delhi (online) |
| 11 | Can a neighborhood fall sick? Opioid addiction, collective violence, and currents of death in contemporary India. | Lecture series organized by Centre for Study of Developing Societies, India | 29th January, 2021 | Delhi (online) |
| 12 | Opioid dependence syndrome: concepts and treatment | Substance Use Disorder Nursing Training Program, Lady Hardinge Medical College | 21 January 2020 | Delhi |
| 13 | Clinical communication with patients and overcoming challenges | Workshop for junior nursing officers working in AIIMS Main Hospital to enhance soft skills | 21 February 2020 | Delhi |
| 14 | Epidemiology of behavioral addictions | Nurses’ training of trainers program on behavioral addictions, AIIMS Delhi College of Nursing | 9 March 2020 | Delhi |
| 15 | Naltrexone Implant in Addiction Psychiatry | XXI Annual Conference of the International Society of Addiction Medicine | 13 November 2019 | Delhi |
| 16 | Super-Specialty course in Addiction Psychiatry in Psychiatry in India | XXI Annual Conference of the International Society of Addiction Medicine | 16 November 2019 | Delhi |
| 17 | Pharmacological management of opioid dependence syndrome | Nurses training of trainers program on substance use disorders, AIIMS Delhi College of Nursing | 30 November 2019 | Delhi |
Investigator/ Co-investigator in funded projects along with year completed/ongoing
| S. No. | Title of the project | Funded by (Name of funding agency) | Duration (years) | Start year | End year | Total funds sanctioned (Rs) |
|---|---|---|---|---|---|---|
| 1 | A Cross-Sectional Study to Screen for Psycho-sexual Health Disorders and Measure Neurochemical Correlates in Gynaecology Cancer Survivors | Intramural Collaborative Research Project for the year 2020 – 2021 | 2 years | 2021 | 2023 | 14,24,000 |
| 2 | HIV, Hepatitis B and C testing in individuals receiving agonist treatment for injecting drug use at a community clinic in Delhi: a cross sectional assessment of risk factors and seroprevalence. | AIIMS Early Career Intramural Research Project for the year 2021 – 2022 | 18 months | 2022 | 2023 | 4,44,000 |
| S. No. | Title of the project | Funded by (Name of funding agency) | Duration (years) | Start year | End year | Total funds sanctioned (Rs) |
|---|---|---|---|---|---|---|
| 1 | An exploratory case- control study to assess the protective genetic factors against alcoholic liver disease among population from northern part of India | AIIMS-Intramural | 3 years | 2017 | 201 | 5 Lakh |
| 2 | Establishing and Implementing capacity building mechanisms for addiction treatment facilities in India | Ministry of Health and Family Welfare | 5 years | 2019 | 2024 | 12 Crore |
| 3 | Setting up of a TeleMedicine and online resource hub on mental health and addictive disorders for South East Asia | World Health Organisation-SEAR | 1 years | 2020 | 2021 | 10 Lakh |
| 4 | Development of module on prevention of substance use and addiction among students for the teachers from the state of Chhattisgarh | Government of Chhattisgarh | 1 years | 2020 | 2021 | 10 Lakh |
| 5 | Development and evaluation of service delivery models for management of substance use disorders among the homeless population receiving urban shelter services in Delhi | Department of Women and Children (WCD), Ministry of Health and Family Welfare, Government of Delhi | 2 years | 2020 | 2022 | 30 Lakh |
| S. No. | Title of the project | Funded by (Name of funding agency) | Duration (years) | Start year | End year | Total funds sanctioned (Rs) |
|---|---|---|---|---|---|---|
| 1 | An exploratory case- control study to assess the protective genetic factors against alcoholic liver disease among population from northern part of India | AIIMS-Intramural | 3 years | 2017 | 2021 | 5 Lakh |
| 2 | Establishing and Implementing capacity building mechanisms for addiction treatment facilities in India | Ministry of Health and Family Welfare | 5 years | 2019 | 2024 | 12 Crore |
| 3 | Setting up of a TeleMedicine and online resource hub on mental health and addictive disorders for South East Asia | World Health Organisation-SEAR | 1 year | 2020 | 2021 | 10 Lakh |
| 4 | Development of module on prevention of substance use and addiction among students for the teachers from the state of Chhattisgarh | Government of Chhattisgarh | 1 year | 2020 | 2021 | 10 Lakh |
| 5 | Development and evaluation of service delivery models for management of substance use disorders among the homeless population receiving urban shelter services in Delhi | Department of Women and Children (WCD), Ministry of Health and Family Welfare, Government of Delhi | 2 years | 2020 | 2022 | 30 Lakh |
| S. No. | Title of the project |
|---|---|
| 1 | A cross sectional study to measure the frequency of the BDNF gene polymorphism (Val66Met) in patients seeking treatment for Alcohol Dependence syndrome (ADS) |
| 2 | Feasibility of ecological momentary assessment to measure associations between perceived control over alcohol use, craving, mood and daily alcohol consumption in treatment-seeking patients of alcohol dependence syndrome |
| 3 | Association of the galanin and galanin receptor gene polymorphism (rs948854) and opioid dependence: A case control observational study |
| 4 | Substance use among homeless women receiving services from shelter homes in Delhi |
| 5 | Prevalence and correlates of neurological and neurocognitive disorder in HIV positive patients on ART |
- as guide 1
-as co-guide 5
Medals/Book Prizes For Institute Foundation Day Celebration & Convocation – 2022
Medals/Book Prizes For Institute Foundation Day Celebration & Convocation – 2021
Medals/Book Prizes For Institute Foundation Day Celebration & Convocation – 2020
Medals/Book Prizes For Institute Foundation Day Celebration & Convocation – 2019
Medals/Book Prizes For Institute Foundation Day Celebration & Convocation – 2018
Medals/Book Prizes For Institute Foundation Day Celebration & Convocation – 2017
Medals/Book Prizes For Institute Foundation Day Celebration & Convocation – 2016
Medals/Book Prizes For Institute Foundation Day Celebration & Convocation – 2015
Medals/Book Prizes For Institute Foundation Day Celebration & Convocation – 2014
Medals/Book Prizes For Institute Foundation Day Celebration & Convocation – 2013
Medals/Book Prizes For Institute Foundation Day Celebration & Convocation – 2012
Medals/Book Prizes For Institute Foundation Day Celebration & Convocation – 2011
Desh Ka Prakriti Parikshan Abhiyan : Transforming Healthcare with Ayurveda
All India Institute of Medical Sciences, New Delhi joins the ‘Desh Ka Prakriti Parikshan Abhiyan’ to help employees and patients understand their unique Prakriti and adopt personalized preventive health practices.
The Centre for Integrative Medicine and Research (CIMR) at AIIMS, New Delhi, initiated the Desh Ka Prakriti Parikshan Abhiyan (DKPP), a visionary campaign launched by Hon’ble Prime Minister Shri Narendra Modi on October 29, 2024. This initiative, led by the Ministry of Ayush, aims to identify individuals' unique mind-body constitutions, known as Prakriti and provide customized health recommendations, encompassing diet, sleep, and exercise, for health promotion and disease prevention.
This campaign at CIMR, AIIMS, New Delhi was inaugurated by Dr. M. Srinivas, Director, who became the lead participant in the Prakriti assessment drive. A total of 4,500 plus Prakriti assessments were accomplished. The campaign’s success is attributed to guidance and leadership of Dr. Gautam Sharma, Professor, Dept. of Cardiology, Founder and Professor In-charge of CIMR, AIIMS, New Delhi.
CIMR Ayurveda physicians have conducted the Prakriti assessments of AIIMS patients, staff and citizens of Delhi-NCR in association with CSIR-Institute of Genomics and Integrative Biology (IGIB) and the All India Institute of Ayurveda (AIIA), New Delhi. Participants were educated on the significance of Prakriti in personalized healthcare, highlighting its role in disease prevention and holistic well-being.
AIIMS has been integrating Prakriti-based research into clinical practices for over five years. Studies conducted include assessments of post-CABG patients, multiple sclerosis and neuromyelitis optica cases, and bronchial asthma patients.
The Desh Ka Prakriti Parikshan Abhiyan demonstrates India’s innovative approach to healthcare by integrating Ayurveda with digital technology acting as a cornerstone to a global research in near future by generating valuable scientific data.
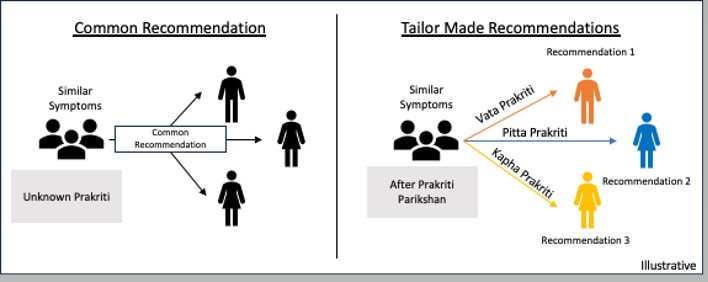
As a part of the 9th IDY week-long celebrations 2023, several events were organized:
A New Approach to Nurture Dynamic Awareness with Mindfulness (ANANDAM) workshops for AIIMS, New Delhi employees:
2023
2022
As a part of the 8th IDY week-long celebrations 2022, several events were organized:
3. Mass yoga practice on IDY (21 st June 2022) at the central lawn, AIIMS, New Delhi (https://www.youtube.com/watch?v=geXHnSxhtpg)
2021
The 7 th IDY was celebrated virtually at AIIMS, New Delhi on 21st June 2021(https://www.youtube.com/watch?v=DZjzIZriSPQt=1564s)
2020
The 6th IDY was celebrated virtually at AIIMS, New Delhi on 21st June 2020 (https://www.youtube.com/watch?v=1pDq-kbj95M)
2019
As a part of the 5th IDY week-long celebrations 2019, several events were organized:
2018
As a part of the 4th IDY week-long celebrations 2018, several events were organized:
2017
As a part of the 3rd IDY week-long celebrations 2017, several events were organized:
1. Self Management of Excessive Tension (SMET) workshops for employees of AIIMS, New Delhi:
2. Mass yoga practice on 21st June 2017 at the central lawn, AIIMS, New Delhi
3. Yoga training program at the Indian Council of Medical Research (ICMR) on 21st June 2017
2022
2021
2020
2018
2020
2018
CURRICULUM VITAE
Dr. Deepak Kumar Gupta
Professor and Consultant Neurosurgeon
Department of Neurosurgery, AIIMS and associated JPN Apex Trauma Centre New Delhi, India
Chair-Pediatric Neurosurgery Fellowship, Program & Services
AREAS OF INTEREST
ACADEMIC QUALIFICATION (Baccalaureate to Postdoctoral)
| DEGREE | INSTITUTION | YEAR |
|---|---|---|
| MBBS | University College of Medical Sciences Delhi,New Delhi, India | 1993 (Dec) |
MS (General Surgery) | Medical Science Lady Hardinge Medical College and Associated Dr.RML Hospital, New Delhi, In | 1998 (Apr) |
| MCh (Neurosurgery) | All India Institute of Medical Sciences (AIIMS), New Delhi, India | 2004 (May) |
| PhD (Neurosurgery) | All India Institute of Medical Sciences (AIIMS), New Delhi, India | Completed |
ACADEMIC POSITIONS:
| July 2017-till present | Professor, AIIMS | ||
| July 2011-June 2016 | Additional Professor Neurosurgery, AIIMS | ||
| July 2008-July 2011 | Associate Professor Neurosurgery, AIIMS | ||
| September 2005- July 2008 | Assistant Professor Neurosurgery, AIIMS | ||
| June 2004- September 2005 | Senior Research Officer, Department of Neurosurgery, AIIMS |
HONORS
| 2015 | Core committee inventor of International Head Injury Guidelines Core Committee member of International Consensus Guidelines for Decompressive Craniectomy in TBI |
| 2013 | Prof. Ming-Chien Kao’s Award World federation of Neurological Surgeons Conference Seoul, South Korea |
| 2012 | Award by International Society for Pediatric Neurosurgery for Work on Craniopharyngiomas during 40th Annual Meeting of ISPN 2012, Sydney, Australia |
| 2012 | Received on behalf of JPN Apex Trauma Centre: Institutional Award for the Best Neurotrauma Centre from Neurotrauma Society for India |
| 2011 | Young Investigator Award, National Neurotrauma conference, Shanghai, China |
| 2011 | International Travelling Fellowship Award, WFNS (International) at Cape town, South Africa |
RESEARCH SUPPORT
| As Principal | Title | Role |
|---|---|---|
| Investigator Ongoing | ||
| Research | ||
| 2012 -2015 | European Society of Intensive Care Medicine | PI |
| study of therapeutic hypothermia (32-35°C) for | ||
| ICP reduction after traumatic brain injury | ||
| (EUROTHERM) | ||
| 2015-2020 | Approaches and Decisions in Acute Pediatric | PI |
| TBI Trial, (ADAPT) USA | ||
| 2015-2020 | Collaborative European Neurotrauma | PI |
| Effectiveness research in TBI Collaborative | ||
| Indian Neurotrauma Effectiveness research in | ||
| TBI (CENTER TBI) | ||
| 2015-2020 | The POLAR-RCT: The Prophylactic | PI |
| hypothermia trial to Lessen traumatic brain | ||
| injury-Randomised Controlled Trial | ||
| 2017-2020 | Randomised Evaluation of Surgery with | PI |
| Craniectomy for patients undergoing | ||
| Evacuation of Acute Subdural Haematoma | ||
| (RESCUE-ASDH) | ||
| 2017-2019 | Asia Coma Electrical Stimulation Trial (ACES) | PI |
| Completed Research | Title | Role |
| 2008-2013 | COTARA: Intratumoral radioimmuno therapy | PI |
| with radiolabelled I -131 in recurrent | ||
| glioblastoma multiforme CRASH 2 | ||
| 2011-2015 | Indo-US Project: Collaborative Head Injury and | PI |
| Adherence to Guidelines (CHIRAG) | ||
| 2013-2015 | Role of cerebral microdialysis in Ischemia vs. | PI |
| Mitochondrial dysfunction in severe Traumatic | ||
| Brain injury | ||
PUBLICATIONS(total):147
Books: 15 chapters Research Papers, Reports: 50 General articles: 82
AWARDS: 23
WORKSHOPS AND CONFERENCES ORGANIZED
COURSES/WORKSHOPS CONDUCTED AS COURSE DIRECTOR
1. ICP monitoring in TBI: 16th April 2012, JPNATC, AIIMS, Delhi
SOCIETY POSITIONS HELD/HOLDING
EDITORIAL CONTRIBUTIONS
1.
2. Designation: Associate Professor of Psychiatry
3. Qualifications: MD DNB (Psychiatry) MNAMS
International Certification in Addiction Medicine
4. Email ID: roshan[at]aiims[dot]edu, drroshansindia[at]gmail[dot]com
5. Field of Interest: Addictive disorders among adolescents and youth
Consultation Liaison in Addiction Psychiatry
Community Psychiatry
Drug Policy
Public Health
6. Speciality Clinics: Community drug treatment clinic at Sundernagri; Mobile Methadone Dispensing; Consultation Liaison Addiction Psychiatry
7. Total number of publications till date 50
8. Details of publications since 2010 onwards
9. Presentations made at scientific meetings/ conferences/ workshops 25
10. Co-investigator in funded/non funded projects 15
11. Funded/Non funded projects:
1. Comparative assessment of stress and coping among adolescent with recent inhalant abuse: A case control study (Funded by AIIMS Intramural research grant)
2. Field Testing of the International Standards for the Treatment Drug Use Disorders (The Standards) in India (Funded by WHO-UNODC grant)
3. Service -based field testing of ICD-11:Public Health/Clinical Utility and Comparability with ICD-10 in India (Funded by WHO, Geneva)
4. “Alcohol e-Help” – A Study to explore the efficacy of the World Health Organization Internet self-help intervention for the reduction of alcohol consumption (Funded by WHO, Geneva)
5. Rates and pattern of psychoactive substance use among prisoners in India(Funded by Ministry of Social Justice & Empowerment, GOI)
6. An explorative study of knowledge, perceived attitude and risk of addiction potential among different stakeholders concerning recreational cannabis use among youth in India (Funded by AIIMS Intramural research grant)
7. Development and validation of an Indian scale to assess severity of substance related problems(Funded by Indian Council of Medical Research-ICMR)
8. A pilot study of assessment of behavioral markers for treatment seeking substance use disorder patients through digital phenotyping: A cross sectional comparative study from Delhi-NCR, India
12. Memberships of professional bodies
13. Important awards & honours
14: Other relevant information: Currently Board of Director of International Society of Addiction Medicine (ISAM) and Chair Person, ISAM NExT (2020-23)
International Certification in Addiction Medicine
E-mail: roshan[at]aiims[dot]edu, drroshansindia[at]gmail[dot]com
2. Designation: Associate Professor of Psychiatry
3. Qualifications: MD DNB (Psychiatry) MNAMS
International Certification in Addiction Medicine
4. Email ID: roshan[at]aiims[dot]edu, drroshansindia[at]gmail[dot]com
Community drug treatment clinic at Sundernagri; Mobile Methadone Dispensing; Consultation Liaison Addiction Psychiatry
Total number of publications till date 50
Parmar A, Gupta P, Bhad R. An exploratory study of clinical profile, stigma and pathways to care among primary cannabis use disorder patients in India . J Sbst Use, 2021; https://doi.org/10.1080/14659891.2021.1897695
Kathiresan P, Bhad R, Rao R. What's in a name? Nosological issues in substance use and addictive disorders: Perspective from ICD-11. Asian J Psychiatr, 2021; DOI: 10.1016/j.ajp.2021.102585
Parmar A, Gupta P, Panda U, Bhad R. An observational study assessing the pathways to care among treatment seeking users of natural opiates. Drugs: Education, Prevention & Policy. 2019. https://doi.org/10.1080/09687637.2019.1649363
Presentations made at scientific meetings/ conferences/ workshops 25
Co-investigator in funded/non funded projects 15
Currently Board of Director of International Society of Addiction Medicine (ISAM) and Chair Person, ISAM NExT (2020-23)
| -- | -- | -- | -- |
|---|---|---|---|
| UNDERGRADUATE | M.B.B.S | B.Sc (HONS.) NURSING | B.Sc NURSING POST BASIC |
| B.Sc. (Hons) in Medical Technology in Radiography | Bachelor of Optometry | - | |
| POSTGRADUATE | MD/MS/MDS/DM/Mch ( 6yrs) | M.Sc Nursing | M.Sc Courses |
| M. Biotech | - | - | |
| SUPERSPECIALTY | DM/M.Ch | - | - |
| DOCTORAL | Fellowship | - | Ph.D |
| RESIDENCY | Junior Resident | Senior Resident | Senior Demonstrator |
Current designation :
Additional professor ( Since July 2021)
National Drug Dependence Treatment Centre &Department of Psychiatry
All India Institute of Medical Sciences
New Delhi-110029
Contact information :
Contact address 4th floor academic building
Department of Psychiatry &NDDTC
AIIMS, New Delhi-110029
Email piyum2008[at]gmail[dot]com
Telephone +919899620279, Contact no: 011-26593236
M.D. ( Doctor of Medicine) in Psychiatry, All India Institute of Medical Sciences, New Delhi
D.Ch (Diploma in Child Health) in Paediatrics, Institute of child Health, Kolkata
M.B.B.S from Medical College, Kolkata
| S.No | Name of Award | Awarding Agency | Year |
|---|---|---|---|
| 1 | ICMR financial assistance for MD thesis | ICMR | 2009 |
| 2 | International travel award | National Institute of Drug Abuse | 2013 |
| 3 | Early career investigator poster award | World Congress of Asian Psychiatry | 2013 |
| 4 | Travel award | CSIR | 2013 |
| 5 | Travel award | ICMR | 2013 |
| 6 | Travel award | DST | 2014 |
| 7 | WHO-ISAM Grants-In-Aid-Of-Travel Fellowship
| International Society of Addiction Medicine | 2014
|
| 8 | International travel award | National Institute of Drug Abuse | 2020 |
Area of interest: Substance use among women ,Adolescent substance use
Principal investigator for the project titled
Peer reviewer for
Book chapter
International
The electron microscopy facility (Sophisticated Analytical Instrumentation Facility-New Delhi, supported by DST-SAIF program) conducts national training programs on biological electron microscopy for
1. Scientific investigators (PhD/MD and MSc students in life sciences with 2-3 years of research experience after joining a PhD program; November-December, 12 days) and
2. Summer training for Laboratory technicians, graduate and postgraduate students and scientists working in Govt. recognised Institutions/ National Laboratories (May-June,1 month).
The aim of both training is to provide with the detailed hands-on comprehensive technical knowledge on the tissue preparation, ultramicrotomy, imaging, and elemental detection under transmission and scanning electron microscope, and tissue antigen localisation under transmission electron microscope (Immunogold electron microscopy).
Cancer Registry is an institution which is responsible for the collection, storage, analysis and interpretation of data on persons with cancer.
Cancer Registration is a process of continuing, systematic collection of data on the occurrence, characteristics and outcome of reportable neoplasms with the purpose of helping to assess and control the impact of malignant disease in the community. Broadly there are two types of cancer Registries-Population Based (PBCR) and Hospital Based (HBCR).
The HBCR records all cases of cancer treated in a given hospital irrespective of the population from which the cases has come. The main interest is clinical care in hospital setting.
The primary concern of PBCR is cancer in the community. The PBCR collects information on all new cancer in a defined population and provide information on cancer incidence, mortality and trends over time in the defined population/geographic area covered by the registry.
The Delhi Cancer Registry is a Population Based Cancer Registry established in January 1986 with the aim of obtaining reliable morbidity and mortality data on cancer occurring among the Delhi Urban residents.
The Delhi PBCR covers an urban area of 1113.65 square kilometers of Delhi Municipal Corporation, New Delhi Municipal Committee and Delhi Cantonment and 29 census towns with a population of 16,368,899 (Males : 8,761,005, Females:7,607,894) as per 2011 census.
The sources of cancer data are various departments viz. Radiotherapy, Pathology, Hematology, Radiology and Medical records of more than 175 major Government hospital centers, 250 private hospitals and nursing homes and Department of Vital Statistics of New Delhi Municipal Committee and Delhi Municipal Corporation.
The Delhi Cancer Registry also established Hospital Based Cancer Registry (HBCR) at Dr. BRAIRCH, AIIMS, New Delhi as an extra mural research project under National Cancer Registry Programme funded by National Center for Disease Informatics and Research, ICMR, Bangalore since 2014.
Email: piyum2008[at]gmail[dot]com
Telephone +919899620279, Contact no: 011-26593236
Contact address 4th floor academic building
Department of Psychiatry &NDDTC
AIIMS, New Delhi-110029

M.D. ( Doctor of Medicine) in Psychiatry, All India Institute of Medical Sciences, New Delhi
D.Ch (Diploma in Child Health) in Paediatrics, Institute of child Health, Kolkata
M.B.B.S from Medical College, Kolkata
| S.No | Name of Award | Awarding Agency | Year |
|---|---|---|---|
| 1 | ICMR financial assistance for MD thesis | ICMR | 2009 |
| 2 | International travel award | National Institute of Drug Abuse | 2013 |
| 3 | Early career investigator poster award | World Congress of Asian Psychiatry | 2013 |
| 4 | Travel award | CSIR | 2013 |
| 5 | Travel award | ICMR | 2013 |
| 6 | Travel award | DST | 2014 |
| 7 | WHO-ISAM Grants-In-Aid-Of-Travel Fellowship | International Society of Addiction Medicine | 2014 |
| 8 | International travel award | National Institute of Drug Abuse | 2020 |
Area of interest: Substance use among women ,Adolescent substance use
Principal investigator for the project titled
Peer reviewer for
Book chapter
Mandal P , Parmar A , Ambekar A, Dhawan A . Substance use among treatment seeking Indian adolescent girls: Are they unique? Asian J Psychiatr. 2019;41:17-9. doi: 10.1016/j.ajp.2019.03.007. Epub 2019 Mar 6.
Gupta P, Mandal P, Singh D, Pattanayak RD, Bhargava R, Anju Dhawan A. Detection of Optic Neuropathy and 3-month Follow-up of an Adolescent Inhalant User: Are we Paying Enough Attention? Indian J Psychol Med. 2016; 38(5): 486–88.doi: 10.4103/0253-7176.191390
Rao R, Mandal P , Gupta R, Ramshankar P , Mishra A , Ambekar A , Jhanjee S, Dhawan A. Factors Affecting Drug Use During Incarceration: A Cross-Sectional Study of Opioid-Dependent Persons from India. J Subst Abuse Treat . 2016;(61 ):13–7 Mandal P, Prakash S."Tramadol: a good option for management of opioid withdrawal syndrome in developing countries." J Subst Use, 2016,21(4) : 339–40
Mandal P, Jain R, Jhanjee S, Sreenivas V. Psychological Barriers to Tobacco Cessation in Indian Buprenorphine-Naloxone Maintained Patients: A Pilot Study. Indian J Psychol Med. 2015 Jul-Sep; 37(3): 299–304. doi: 10.4103/0253-7176.162944
Prakash S, Mandal P. Is the DSM-5 position on dhat syndrome justified?Asian J Psychiatry. 2014; 12:155-57.DOI: http://dx.doi.org/10.1016/j.ajp.2014.08.006
Gupta A, Mandal P, Rachna Bhargava R, Pattanayak RD, Sagar R, Dhawan A.Marked Exacerbation of ADHD After Onset of Inhalant Use: A Case Report. J Neuropsychiatry Clin Neurosci. 2014 26(4) : E6-E7
Mandal P, Prakash S. Stigma of mental disorders and role of nursing professionals: A developing country perspective. J nursing & care. 2014; 3(5):190. http://dx.doi.org/10.4172/2167-1168.1000190
Thapa R, Mallick D, Mandal P, Ghosh A. Neuroblastoma masquerading as juvenile idiopathic arthritis. Indian J Pediatrics . 2007; 74(4 ): 421-422
International
| Postgraduate | Courses |
|---|---|
| Ph. D. | Doctor of Philosophy |
| M.D.,(Anatomy) | Doctor of Medicine in Anatomy [Previously Master of Surgery (M.S.,) in Anatomy] |
| M.Sc.,(Anatomy) | Master of Science in Anatomy |
| Sr. no. | Name of the Test & Developed by: |
|---|---|
| 1. | AIIMS COMPREHENSVE NEUROPSYCHOLOGICAL BATTERY IN HINDI (ADULT FORM) Surya Gupta et al. |
| 2 | AIIMS COMPREHENSVE NEUROPSYCHOLOGICAL BATTERY IN HINDI (CHILDREN’S FORM) Surya Gupta et al. |
| 3 | AIIMS COMPREHENSVE DEMENTIA ASSESSMENT SCALE IN HINDI Surya Gupta et al. |
| Sr. no. | Name | Copyrights (In process) |
|---|---|---|
| 1. | Indian Aphasia Battery (IAB) Ashima Nehra& Dwarka Pershad | Diary No. 56414/2014-CO/L |
| 2. | Cognitive rehabilitation of response inhibition ability (CRRIA) Ashima Nehra & Swati Bajpai | Diary No. 55474/2014-CO/L |
| 3. | Computerized Opus in Neuropsychological testing using E-application of multitasking paradigm (CONTEMP). Ashima Nehra & Swati Bajpai | Diary No. 56421/2014-CO/SW |
| 4. | Dementia Assessment By Rapid Test (DART) Swati Bajpai & Ashima Nehra | Diary No. 55472/2014-CO/L |
| 5. | Neuropsychological Evaluation Screening Tool (NEST) Sakshi Chopra, Harsimarpreet Kaur,Ashima Nehra | Diary No. 55476/2014-CO/L |
| 6. | Rehabilitation of Cognition Using Restorative Exercises & Activities Targeted For Elderly (RECREATE) Swati Bajpai & Ashima Nehra | Diary No. 11397/2017-CO/L |
| 7. | Rehabilitation of Electric Cognitive Functioning Post Traumatic Brain Injury to Retrain and Restore Attention, Concentration, Memory And Functions (RETRACE) Sakshi Chopra & Ashima Nehra | Diary No. 11400/2017-CO/L |
| 8. | “Rehabilitation of Everyday Language and Cognitive Functioning post Stroke for Aphasia Rehabilitation: An Indian Rehabilitation Program (REPAIR) Harsimar Preet Kaur & Ashima Nehra | Diary No. 11402/2017-CO/L |
Cancer is emerging as a major public health problem globally. As per WHO GLOBOCAN 2020, 1.32 million new cases of cancer are detected each year in India and 0.85 million succumb to this deadly disease. Cancer treatment requires a multimodal management approach. Surgery is one of the main modalities for treating cancer and 90 % of cancer patients need some surgical intervention. The surgical specialty dealing with cancer management is known as Surgical Oncology.
Dr. B. R. Ambedkar Institute Rotary Cancer Hospital (Dr. BRA-IRCH), AIIMS, New Delhi was established in the year 1984 with an aim to provide comprehensive cancer care services in Northern India. Dedicated surgical oncology services were started in 1988 and subsequently a 20 bedded surgical Oncology ward with major OT and ICU were built with a philanthropic donation by Shri Kanhayalal Punj. Prof NK Shukla was the first faculty to initiate cancer surgical services and Dr. SVS Deo joined as second faculty in 1995. The unit was recognized as an independent Department of Surgical Oncology in the year 2001 and IRCH was expanded to a 182 bedded comprehensive cancer center with 46 Surgical beds, 6 bedded ICU and 3 major Operation theaters in 2005. MCh Surgical Oncology program was started in 2012. The department took a leadership role in the planning and establishment of state of art surgical oncology services at National Cancer Institute (NCI) Jhajjar and started cancer surgical services at NCI in 2019.Currently the department has 10 faculty members,18 MCh trainees and 12 Senior residents.
The three major activities of the department include Patient Care, Teaching & Training and Research.
The department leads in introducing advanced and cutting edge surgical programs including Minimally Invasive Surgery (Lap & VATS), Peritoneal Surface Malignancies (Cytoreductive Surgery, HIPEC & PIPAC), Oncoplastic & Microvascular surgery, Risk Reducing Surgery, Navigational Surgery, Organ Conservation and Intra-operative Radiation Therapy and Palliative Surgical Oncology at AIIMS.
Teaching and Training: The department runs MCh Surgical Oncology program, which is one of the leading and popular MCh programs in India. In addition, the department offers long term and short-term training to general surgeons. The department has trained more than 150 cancer surgeons during last 25 years, who are in leadership positions in different parts of the country.
Research : The faculty members of the department are actively engaged in a number of collaborative basic and clinical research projects including multicentric international trials. The department has developed a computerized comprehensive oncology clinical data base and currently has comprehensive clinical data related to more than 10,000 cancer patients operated in the department. The faculty has published more than 300 scientific papers in prestigious national and international journals.
Other Activities: The faculty of the department are actively involved as members, experts and advisors for various organizations and scientific bodies like NBE, ICMR, DBT, DS, Ministry of Health, IASO, ISPSM, ABSI and BSI. The department regularly conducts workshops and organizes major conferences (ICC 2013, NATCON 21, ABSICON18 and INDO-UK Oncoplasty course, ISPSM-ESSO cadaver courses on CRS & HIPEC etc).
1983 - Dr. BRA-IRCH was established as a comprehensive cancer center of AIIMS
1988 - Dr. NK Shukla joined as first faculty and established a Unit of Surgical Oncology to offer basic cancer surgical services.
1991 – Senior Residency training program was started, and major cancer surgical services initiated.
1995 – Dr SVS Deo joined as second full-time faculty.
1996 – A dedicated 20 bedded Surgical Oncology ward along with a major OT and ICU were established with a philanthropic donation from Shri. Kanhayalal Punj.
2001 – Unit of Surgical Oncology was upgraded as a full-fledged independent Department
2005 – IRCH expanded to 182 bedded regional cancer Center including 48 Surgical Oncology beds and 3 major operation theaters.
2012 – M.Ch. course in Surgical Oncology was started with an annual intake of 5 students.
2012 – Dr. Sunil Kumar and Dr. MD Ray joined as full-time faculty
2017 – Prof. SVS Deo assumed the role of Head of Department after Prof. NK Shukla’s superannuation.
2018 – Three more faculty members Dr Sandeep Bhoriwal, Dr Ashutosh Mishra and Dr Jyoti Sharma joined the Department.
2019 – Inauguration of National Cancer Institute, AIIMS, Jhajjar campus by Honorable Prime Minister and launch of Surgical Oncology services at NCI campus.
2020 – Four more faculty members joined the department Dr. Naveen, Dr. Babul Bansal, Dr. Jyoutishman Saikia and Dr Raghuram K.
| S NO | NAME AND DESIGNATION | DEPARTMENT |
|---|---|---|
| 1 | Prof. Randeep Guleria |
Pulmonary Medicine |
2 |
Prof. Nikhil Tandon |
Dept of Endocrinology |
3 |
Prof. S. K. Choudhary.
|
Dept. of CTVS |
4 |
Prof. Rohit Bhatia |
Dept. of Neurology |
5 |
Prof. Gautam Sharma |
Dept. of Cardiology |
6 |
Dr. Maneesh Singhal Addl. Prof.
|
Department Of Surgery |
| S NO | NAME AND DESIGNATION | DEPARTMENT |
|---|---|---|
| 1 | Prof. Randeep Guleria |
Pulmonary Medicine |
2 |
Prof. Nikhil Tandon |
Dept of Endocrinology |
3 |
Prof. S. K. Choudhary.
|
Dept. of CTVS |
4 |
Prof. Rohit Bhatia |
Dept. of Neurology |
5 |
Prof. Gautam Sharma |
Dept. of Cardiology |
6 |
Dr. Maneesh Singhal Addl. Prof.
|
Department Of Surgery |
| Sr.No | Name | Designation |
|---|---|---|
| 1 | Ms. Srishty Raman | PhD |
| 2 | Ms.Priya K Gorai | PhD |
| 3 | Ms. Shivani | PhD |
| 4 | Ms. Arti Joshi | PhD |
| 5 | Ms. Devyani Sharma | PhD |
| 6 | Ms.Sania Yasmin | PhD |
| 7 | Ms. Anjali Yadav | PhD |
| 8 | Ms. Anjali Maurya | PhD |
| 9 | Ms. Akanksha Mishra | PhD |
| 10 | Mr. Amit Kumar | PhD |
| 11 | Bhaskar Sharma | PhD |
| 12 | Deepika Kumari | PhD |
| 13 | Yogesh Sharma | PhD |
| 14 | Dr. Filgy George | PhD |
| 15 | Supriya Verma | PhD |
| 16 | Sumant Kumar | PhD |
| Sr.No | Name | Designation |
|---|---|---|
| 1 | Dr.Dibakar Borthakur | Senior Resident |
| 2 | Dr. R. Jayshree | Senior Resident |
| 3 | Dr.Namaschivayam G.R | Senior Resident |
| 4 | Dr. Silka Agarwal | Senior Resident |
| 5 | Dr Jayant Biswas | Senior Resident |
| 6 | Dr. S. Kamalesh | Senior Resident |
| 7 | Dr. Dravida Chemmal M | Senior Resident |
| 8 | Dr. Hari Hara Hanusun N | Senior Resident |
| 9 | Dr. Pooja Poddar | Senior Resident |
| 10 | Dr. Filgy George | Senior Resident |
| Sr.No. | Name | Position |
|---|---|---|
| 1 | Dr Sumit Daitan | Junior Resident |
| 2 | Dr Surbhi A S | Junior Resident |
| 3 | Dr Shubhankar Roy | Junior Resident |
| 4 | Dr Akhila M. S | Junior Resident |
| 5 | Dr Neelam Devi | Junior Resident |
| 6 | Dr Madhur Binda | Junior Resident |
| 7 | Dr Sukanya | Junior Resident |
| 8 | Dr Dharani D | Junior Resident |
| 9 | Dr Kirthi Ravi | Junior Resident |
| 10 | Dr Ajay Kumar Kujur | Junior Resident |
| 11 | Dr Krishna Rao | Junior Resident |
| 12 | Dr Anusha Prasad | Junior Resident |
| 13 | Dr Krishna Prasad Sharma | Junior Resident |
| 14 | Dr D. Hari Prasad | Junior Resident |
| Sr.No. | Name | Position |
|---|---|---|
| 1 | Deepika Drall | M.Sc |
| 2 | Mudavath Gopi Naik | M.Sc |
| 3 | Tooba Tahreem Khan | M.Sc |
| 4 | Robin Saini | M.Sc |
| 5 | Shristhi Jain | M.Sc |
| 6 | Swarna Tomar | M.Sc |
| 7 | AMR Suresh | M.Sc |
| 8 | Sanskriti Singh | M.Sc |
| 9 | Neeti Saini | M.Sc |
| 10 | Jasmine Kaur Saini | M.Sc |
| 11 | Deepak Kr. Rao | M.Sc |
| 12 | Ankit Panchal | M.Sc |

2. Name: Dr Siddharth Sarkar
3. Designation: Additional Professor
4. Qualifications: MD
5. Email ID:sidsarkar22[at]gmail[dot]com
6. Field of Interest: Addiction Psychiatry, Medical Education, Consultation Psychiatry
7. Total number of publications till date: 225
8. Details of publications since 2010 onwards (the full citation)- these should be divided into journal articles (peer reviewed publications) and books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications)
Sagar R, Sarkar S. Drug Therapy for Psychiatric Disorders 1st Edition, Jaypee Brothers Medical Publishers, 2019.
Chadda S, Kumar V, Sarkar S, editors. Social Psychiatry: Principles and Clinical Perspectives. Jaypee Brothers, New Delhi; 2018
https://pubmed.ncbi.nlm.nih.gov/?term=siddharth+sarkar&sort=date
https://scholar.google.co.in/citations?hl=en&user=h7j6D4sAAAAJ
9. Presentations made at scientific meetings/ conferences/ workshops:
10. Investigator/ Co-investigator in funded projects along with year completed/ongoing:
11. Investigator/Co-investigator in non-funded projects along with year and title completed/ongoing
12. Thesis supervised for MD/ DM/PhD
- as guide - 2
-as co-guide - 10
13. Awards and Honours:
Sarada Menon Gold Medal for DNB, Psychiatry
Young Psychiatrist Award of Indian Psychiatric Society 2016
Bhagwat Award of Indian Psychiatric Society 2015
Balint Award of Indian Association for Social Psychiatry 2017
NIDA Young Investigator Awardee for ISAM 2022
14. Any other relevant information:
Deputy Editor of Indian Journal of Social Psychiatry
Assistant Editor of Indian Journal of Psychiatry
Email: sidsarkar22[at]gmail[dot]com
Addiction Psychiatry, Medical Education, Consultation Psychiatry
number of publications till date: 225
Details of publications since 2010 onwards (the full citation)- these should be divided into journal articles (peer reviewed publications) and books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications)
Sagar R, Sarkar S. Drug Therapy for Psychiatric Disorders 1st Edition, Jaypee Brothers Medical Publishers, 2019.
Chadda S, Kumar V, Sarkar S, editors. Social Psychiatry: Principles and Clinical Perspectives. Jaypee Brothers, New Delhi; 2018
https://pubmed.ncbi.nlm.nih.gov/?term=siddharth+sarkar&sort=date
https://scholar.google.co.in/citations?hl=en&user=h7j6D4sAAAAJ
- as guide - 2
-as co-guide - 10
Sarada Menon Gold Medal for DNB, Psychiatry
Young Psychiatrist Award of Indian Psychiatric Society 2016
Bhagwat Award of Indian Psychiatric Society 2015
Balint Award of Indian Association for Social Psychiatry 2017
NIDA Young Investigator Awardee for ISAM 2022
Deputy Editor of Indian Journal of Social Psychiatry
Assistant Editor of Indian Journal of Psychiatry
1.
2. Name: Dr. Rizwana Quraishi
3. Designation: Additional Professor (Clinical Chemistry), Faculty In-charge, Laboratory Services, National Drug dependence Treatment Center, Department of Psychiatry, AIIMS, New Delhi.
4. Qualifications: M.Sc. (Biochemistry), Ph.D. (Clinical Chemistry)
5. Email ID: rizwanaquraishi[at]gmail[dot]com
6. Field of Interest:
7. Total number of publications till date: 40
- as guide (number only): 2 MD
-as co-guide (number only): 2 DM, 5 MD, 2 Ph.D. (Member)
Email: rizwanaquraishi[at]gmail[dot]com
Total number of publications till date: 40
- as guide (number only): 2 MD
-as co-guide (number only): 2 DM, 5 MD, 2 Ph.D. (Member)
Located on the 7th floor of the convergence block, the Centre for Integrative Medicine and Research (CIMR) consists of a research area, clinics, therapy rooms, yoga hall and conference hall.
1. Research area: Well-equipped area accommodating 16 workstations meant exclusively for Scientists engaged in research work.
2. Research clinics: The clinics operate daily from Monday to Saturday from 9 am to 5 pm for evaluation of patients enrolled in research projects.
3. Therapy rooms: There are two therapy rooms meant for Ayurvedic therapies such as Shirodhara for the enrolled patients.
4. Yoga hall: The yoga hall has been specially designed for an ideal holistic yoga experience. It can accommodate upto 35 participants at a time.
5. Conference hall: Equipped with a high-end projector with an interactive smart board, the conference hall is used to conduct seminars, workshops, journal clubs, project presentations, and meetings.
6. Video conferencing facility: Equipped with a video conferencing facility that is used for virtual yoga therapy, and counseling sessions.
The Neuropathology laboratory, AIIMS was established by Professor Subimal Roy in mid 1970s. As the doyen of Neuropathology, he was one of those who introduced the specialty of Neuropathology in this country at a time when the branch was still evolving in other parts of the world. The Neuropathology laboratory delivers a wide range of diagnostic and research services with a particular expertise in neuro-oncology, epilepsy, inflammatory diseases of the CNS, neurodegenerative diseases, peripheral nerve and adult and paediatric muscle diseases. The research activities in this section have been widely cited and put on the global map of Neuropathology.
Guidelines for organization of Conferences/ Courses/ Workshops/CME/Symposiums etc.
Elective Training Undergraduate Medical Students (Foreign only)
| Sr.No. | Name | Designation |
|---|---|---|
| 1 | Mrs. Pratibha | Sr. Technical Officer |
| 2 | Mr. Dinesh Tomer | Sr. Technical Officer |
| 3 | Mr. Bhupinder Kumar | Sr. Technical Officer |
| 4 | Mr. Arvind Dabas | Technical Officer |
| 5 | Mr. Mahesh Dutt | Technical Officer |
| 6 | Mrs. Bhawna Satija | Technical Officer |
| 7 | Mr. K.P. Singh | Medical Laboratory Technologist |
| 8 | Mr. Ajay Kumar | Medical Laboratory Technologist |
| 9 | Mr. Punit Kumar | Medical Laboratory Technologist |
| 10 | Mrs. Vimla Joy | Medical Laboratory Technologist |
| 11 | Mrs. Jyoti Aneja | Medical Laboratory Technologist |
| 12 | Mrs. Sharda Devi | Junior Medical Laboratory Technologist |
| 13 | Mr. Rajendra Singh | Junior Medical Laboratory Technology |
| 14 | Mr. R.P. Manjhi | Animal Attendant |
| 15 | Mrs. N. Veena | Personal Assistant |
| 16 | Mrs. Kanta Kadyan | Personal Assistant |
| 17 | Mr. Harish | Junior Administrative Assistant |
| 18 | Mr. Praveen Kumar | Office Attendant |
| 19 | Mr. Vikas Kumar | Office Attendant |
| 20 | Mr. Inder Singh | Office Attendant |
| 21 | Mr. Ram Kumar-II | Sanitary Attendant |
| 22 | Mr. Shish Pal | Sanitary Attendant |
| 23 | Mr. Vinod Kumar | Sanitary Attendant |
| 24 | Mr. Sandeep Arya | Chief Technical Officer |
| 25 | Mrs. Chanda Panwar | Sr.Technical Officer |
| 26 | Mr. Anurag Singh | Technical Officer |
| 27 | Mr. Meharban Singh | Medical Laboratory Technologist |
| 28 | Mr. Madan Mohan | Medical Laboratory Technologist |
| 29 | Mr. Pardeep K. Vaishnav | Medical Laboratory Technologist |
| 30 | Mrs. Vidhyashree M | Medical Laboratory Technologist |
| 31 | Mr. Chitranjan Patra | Junior Administrative Assistant |
| 32 | Mr. Anoop Nair | Data Entry Operator |
| 33 | Mr. Vinay | Lab Attendant |
| 34 | Ms. Laxmi | Data Entry Operator |
| 35 | Ms. Chetna | Data Entry Operator |
| 36 | Mr. Ankit Kumar | Data Entry Operator |
| 37 | Ms Samriti Sharma | Personal Assistant |
| 38 | Mr Sachin | Lab Attendant |
| 39 | Mr Mantesh | Lab Attendant |
The department is actively engaged in teaching, research and patient care activities since its inception (1965). Various radiotherapy services offered to the patients are External beam radiotherapy, brachytherapy, stereo-tactic radiotherapy (SRT) and intensity modulated radiotherapy (IMRT) Every year Approximately 4000 new patients consult department for various treatments by radiotherapy and nearly 10,000 patients are on follow up after treatment by the departments. etc. New patients are usually registered on referral after pathological confirmation of neoplasm/malignancy. The department has the comprehensive set up for treatment of various cancers, in combination with surgery and chemotherapy. This department has post-graduate programme (MD in Radiothearpy) and doctoral programme (Ph-D).
Radiology unit at Dr BRAIRCH was established in 1983 with x-ray and mammography facility. It has gradually expanded since then. This was the first facility in AIIMS to acquire ultrasound, whole body CT scan, mammography and multidetector CT. This unit provides diagnostic and interventional radiology services to all clinical units of Dr BRAIRCH.

Department of Medical Oncology excels in clinical, teaching and research activities. From its inception in 1984, work-load has consistently increased: currently out of about 70,000 cases registered at IRCH per year, medical oncology manages about 37,000 by itself. In addition, medical oncology department is involved in patient care services in different clinics – including breast, Gastroenterology, Head & Neck Surgery & ENT, Pediatric oncology, Pediatric Surgery, lung cancer, ophthalmic Ca, Bone & soft tissue & Urology clinic. It has a very busy day care service where around 60 patients are managed per day. In addition, patients are admitted in the regular ward also, more than 7000 patients get chemotherapy on an outpatient basis and OPD based procedures are carried out 3 times a week.
Medical Oncology department is running a DM and PhD programme
This department has its own laboratory where many of the technologies such as RT- PCR, FISH, cytogenetics, tissue culture, and Flowcytometry etc. have already been standardized. Stem cell storage is carried out; routinely also blood component therapy is provided with the help of cell separator.
This is one of the few centres in the country to have established hematopoietic stem cell transplant programme. About 350 transplants have already been carried out to treat malignant and non-malignant hematological disorders. In collaboration with Department of CTVS, stem cell transplant program has been extended to treat myocardial Ischemia also. Currently, phase II studies are also being performed in collaboration with Dr. R.P. Centre and paediatric surgery to explore role of stem cells in the treatment of Retinitis pigmentosa and spina bifida.
We have also investigated an alternative source of hematopoietic stem cells namely fetal liver. Here in, we have demonstrated the secretion of certain cytokines which induce recovery in aplastic anemia patients.In addition, Department has spearheaded a program to reach out to the communities for cancer awareness and cancer detection. Doctors and paramedical staff of neighbouring states and Delhi have been trained. Screening program for common cancers in Urban slum dwellers have been conducted and over 10,000 people have been screened.
Medical Oncology has been actively working with various NGO’s to increase cancer awareness in schools and in the communities. Medical oncology faculty has been participating in many Continuing education programs/workshops/symposia conducted by Medical Oncology on various topics regularly over the last several years including hemato-oncology, cancer screening and awareness, lung cancer, cancer team management, colorectal cancers, hematopoietic stem cell transplants etc. Many of these program were funded by WHO.
Medical Oncology has also taken the initiative to carry out research in our traditional methods, namely Pranayam, yoga, meditation and Sudershan Kriya. Research has shown beneficial effects of these techniques on brain, endocrine system and immune system. Antioxidant defence also improved following these practices. International Symposium was organized in 2002 at AIIMS to discuss these findings. Several faculty from within and outside country made their presentations, program was attended by more than 1000 participants. An International Conference on ‘Expanding Paradigms: Science, Consciousness and Spirituality’ was also organized in February, 2006 at New Delhi on this subject. Several faculty members within and outside country made their presentations and there were approximately 1500 participants.
Medical Oncology has also investigated the role of antioxidant vitamins to treat lung cancer. This is a rather innovative area of research; part of the work has already been published.

Medical Physics Unit at IRCH is looking after radiation related research in medical imaging, image quality in mammography, CT scan, ultrasound, radiography, fluoroscopy and angiography, radiation dosimetry in patient in imaging, reduction of dose without compromising diagnostic information, radiation protection and measurement of radiation dose to staff and attendants, irradiation of blood bag before blood transfusion to patients, radiation protection survey for radiological imaging installation (CT scanner, x-rays, mammography) all over AIIMS, Quality Assurance of medical film processors, darkrooms, x-ray units, x-ray reporting rooms, film illuminators and continuous quality improvement in radiological services to patients and doctors. Our activity includes staff and public education regarding radiation safety, besides imparting knowledge (in form of regular classes) in the field of Medical Physics and Radiation Safety to MD (radiology), MBBS students, B.Sc. Radiography, Human biology students, nursing students and other interested groups and individuals- which includes trainees from other hospitals not only from India but abroad as well. The unit provides consultation in any untoward accidental radiation exposure to patient, public or staff. Our endeavour make radiation installations safe for public, staff and public for which there is a great concern now-a-days. Optimisation and maximum utilization of images and development of ways to reduce patient and public radiation doses are going to be touch-stone for comparison of services provided by different hospitals in medical imaging. Medical Physics Unit, therefore, is working for quality in medical imaging at AIIMS.
The Laboratory Oncology Unit is the laboratory division of the Dr. BRAIRCH. It was started in October 1991, in order to give the IRCH its own laboratory so as to meet its highly specialized laboratory needs in the best possible manner. This was formalized by including a laboratory devoted exclusively to cancer, in the IRCH Development Plan of 1992-93. Its focus so far, mainly, but not exclusively, has been Hemato-oncopathology.
Starting from hemogram, bone marrow and peripheral blood smear studies in 1992, laboratory has grown multidimensional with new investigations being introduced at regular intervals. Multi-parametric flowcytometry with emphasis on minimal residual disease detection, Molecular studies including state of art molecular cytogenetics using array CGH and next-generation sequencing and Multiple Myeloma laboratories of this department are some of the unique laboratory sections of this department.
The laboratory conducts around 1,11,831 tests per year. Due to its fast and expert handling of difficult and challenging cases and because of some expertise being uniquely available here, Laboratory Oncology serves as referral laboratory not only for IRCH, but for other departments and Centers of the AIIMS main hospital.
1. NAME: Dr. BISWADIP CHATTERJEE

2. NAME in HINDI: डॉ. विश्वदीप चटर्जी
3. Designation: Additional Professor of Psychiatry, NDDTC and Department of Psychiatry
4. Designation in Hindi: अपर प्रोफ़ेसर, राष्ट्रीय व्यसन उपचार केंद्र
5. Qualifications: MBBS; M.D. (PSYCHIATRY)
6. Email ID: biswadip[dot]c[at]gmail[dot]com; biswadip[dot]c[at]aiims[dot]edu
7. Field of interest:
8. Speciality clinics and services:
9. Total number of publications: 47
9. Presentations made at scientific meetings/ conferences/ workshops:
10. Funded projects
11. Non funded projects
12. Thesis supervised for MD/ DM:
13. Significant events/achievements/awards
Email: biswadip[dot]c[at]gmail[dot]com; biswadip[dot]c[at]aiims[dot]edu
Total number of publications: 47
Singh VV, Gupta S, Sarkar S, Chatterjee B. Problematic dicyclomine use: A case report and narrative review. Asian Journal of Psychiatry 2020;48:101891. doi: 10.1016/j.ajp.2019.101891
Located on the 7th floor of the convergence block, the Centre for Integrative Medicine and Research (CIMR) consists of a research area, clinics, therapy rooms, yoga hall and conference hall.
1. Research area: Well-equipped area accommodating 16 workstations meant exclusively for Scientists engaged in research work.
2. Research clinics: The clinics operate daily from Monday to Saturday from 9 am to 5 pm for evaluation of patients enrolled in research projects.
3. Therapy rooms: There are two therapy rooms meant for Ayurvedic therapies such as Shirodhara for the enrolled patients.
4. Yoga hall: The yoga hall has been specially designed for an ideal holistic yoga experience. It can accommodate upto 35 participants at a time.
5. Conference hall: Equipped with a high-end projector with an interactive smart board, the conference hall is used to conduct seminars, workshops, journal clubs, project presentations, and meetings.
6. Video conferencing facility: Equipped with a video conferencing facility that is used for virtual yoga therapy, and counseling sessions.

Prof. Shariff is an MBBS graduate and MS (Anatomy) from JIPMER in Pondicherry. He joined AIIMS as senior demonstrator and later joined as Assistant Professor.His research focuses on the Enteric Nervous System.
He has also been instrumental in establishing the blended learning facility in the department of Anatomy.
M.S. (BHU), D.N.B., M.N.A.M.S

Professor
Address : Room No. 1009, Ist Floor
PC Block
Deptt of Anatomy
AIIMS, N. Delhi
Phone : 011-26593216
Research Focus: Pain arising from burn injury is a devastating experience for patients. Results of our research in rodents show that blocking the B2 subtype of bradykinin receptor produces significant relief from burn-induced pain. An attempt to test this alternative hypothesis in a clinical trial to be conducted in the largest burn unit in the country could not be done, due to lack of funds. Other putative drugs, which have shown efficacy in rodents are the cannabinoid type 1 receptor and the somatostatin type 2A receptor agonist. These could relieve specific parameters of pain like pain-at-rest but not touch-induced allodynia.
1. George J. et al. 2014. J Burn Care Res 35:e391-398 (Published by American Burn Association)
2. Kumar R. et al. 2016. Indian J Med Res 144:730-740.
3. Kumar R. et al. 2018. Eur J Anaesthesiol 35:955-965.

Intrathecal catheterization with drug administration in rodents is a novel technique for simulating intraspinal administration of drugs during cardiac surgery. I underwent training at the Anesthesia Research Laboratory of University of California at San Diego for 3 months in 2008. It was supported by an International biomedical associateship grant from Indian Council of Medical Research, N. Delhi.
Substance P receptor antagonists when administered through catheters in rodents proved effective in ameliorating post-operative pain. A more potent effect was obtained when it was combined with local peripheral administration.
1. Gautam M et al. 2016. Spinal Cord 54:172-182.
2. Gupta S et al 2018. Ann Neurosci 25:268-276.
Current research work is focused on developing rat models of (1) Neuropathic pain by partial sciatic nerve ligation (2) Osteoarthritis by intra-articular injection of monoiodoacetate. Both are chronic diseases which compromises the quality of life.
Assistant Prof at B. P. Koirala Institute of Health Sciences, Nepal in 1997.

Prof. Rima Dada did her MBBS from Delhi University at Maulana Azad Medical College. Thereafter, she joined the MD programme in Anatomy at the University College of Medical Sciences, again under Delhi University. She completed her Senior Residency and her Ph.D. studies in Genetics at AIIMS, New Delhi. Later, she joined AIIMS as an Assistant Professor in the Department of Anatomy.
Teaching, Research, Training and Genetic (Human Cytogenetic and Molecular) Diagnostic servicesGenetic Diagnostic and patient care services: Both cytogenetic and molecular techniques used for analysis of various genetic disorders eg-Reproductive disorders (premature ovarian failure, Recurrent spontaneous abortion, various endocrinal disorders, infertility, congenital malformations, Glaucoma, Congenital cataract, BPES,Retinoblastoma and various hematological disorders and cancers.Also offering Sperm DNA damage and seminal ROS assessment facility to couples with idiopathic infertility and cases with recurrent ART failure.
Research interests: Genetics of reproductive disorders, ocular disorders and various childhood cancers. Also studying impact of lifestyle interventions on markers of aging.
Prof. Rima Dada is on the editorial board of several national and international journals and member of various scientific bodies.She has been awarded several prestigious national and international awards and has several international and national indexed papers and book chapters.

Prof. Arundhati Sharma did her graduation (B. Sc) and post graduation (M. Sc) in Genetics and Molecular Biology from Osmania and Pune University, respectively. She did her Ph D in Human Genetics from Nizam’s Institute of Medical Sciences and did her subsequent post doctoral work in the Department of Medical Genetics, SGPGIMS, Lucknow. Later, she joined as Assistant Professor of Genetics in the Department of Anatomy, AIIMS.Her work includes teaching, training and providing diagnostic facilities in the field of Human genetics. Her laboratory provides the following:
Diagnostic and patient care services-conventional cytogenetic services (Karyotyping) and other chromosomal studies. Molecular cytogenetic services using fluorescent in-situ hybridization (FISH) for various genetic numerical and structural abnormalities, cancers and other genetic conditions. Research interests include genetics of various endocrine and eye disorders, identification of biomarkers for prognostic and diagnostic purposes for various cancers and adverse drug reactions, and studies of Addiction genetics, i.e. identification of the genetic contribution to alcohol and drug dependence.
8. Bansal M, Tandon R, Saxena R,Sharma A, Sen S, Kishore A, Venkatesh P, Maiti S, Chakraborty D. Ophthalmic genetics practice and research in India: Vision in 2020. Am J Med Genet C Semin Med Genet. 2020 Sep;184(3):718-727
9. Kathpalia P, Nag TC, Chattopadhyay P, Sharma A, Bhat MA, Roy TS, Wadhwa S. In ovo Sound Stimulation Mediated Regulation of BDNF in the Auditory Cortex and Hippocampus of Neonatal Chicks. Neuroscience. 2019; 408: 293-307. doi: 10.1016/j.neuroscience. 2019.04.014. Epub 2019 Apr 24.

Dr Renu Dhingra joined BSc (Hons) Human Biology at AIIMS, then completed her MSc (Anatomy) at AIIMS, followed by a PhD. She further worked as a Senior Demonstrator in the Department of Anatomy, AIIMS. Later, she joined University College of Medical Sciences, New Delhi as a Lecturer and thereafter at Gulf Medical College Ajman, UAE. Subsequently, she joined the department of Anatomy at AIIMS as an Assistant Professor.
Her research interest is in placental biology. At present, she is working on ‘apoptotic, oxidative endoplasmic reticulum stressand angiogenetic markers in pre –eclampsia . Her current research also focuses on migration and invasion studies on trophoblastic cells. The laboratory has the infrastructure for handling cell lines, conducting in-vitro assays, apoptotic, cytotoxic assays and other molecular biology techniques like ELISA, Immunofluorescence, Western Blot and PCR.
She has established the Plastination laboratoryin the department. The plastinated specimens serve as valuable adjuncts for teaching Anatomy to undergraduate and postgraduate students.

Dr TC Nag received his doctoral degree (1991) from the University of Calcutta, Kolkata. He was a postdoctoral fellow in the Department of Biology, University of Montréal, Canada (1993) and later worked as a research associate and Pool Officer in Neurobiology Laboratory at the Department of Anatomy, AIIMS, New Delhi (1995-1998). He also worked as a lecturer in West Bengal Educational Service (1998-2001) after which he joined as an assistant professor in the electron microscopy section of the department (2001). He is a recipient of Shakuntala Amir Chand Prize of ICMR (1999), SS Parmar Foundation Award and JR Bhattacharjee Award of Indian Academy of Neurosciences and AIIMS Research excellence award (2015) and is a member of National Academy of Sciences, Allahabad and Associate Editor, Journal of Biochemical and Molecular Toxicology (Wiley).
Major research interest: Age-related structural and neurochemical changes in the human retina and factors associated with them, and the impact of iron accumulation through aging, and various effects of exposure to bright prolonged light on the retina in animal models (chicks and rodents).

Dr. Ritu Sehgal graduated from Maulana Azad Medical College (MAMC) and completed her MS Anatomy and Senior Residency from the same institution. She was awarded the‘Pyare Lal Sharma & Bishan Devi Gold Medal’forBest thesis/student in Pre & Paraclinical Subjects. She joined AIIMS as Assistant Professor of Anatomy after working for a brief period as Assistant Professor at VMMC, New Delhi
Research interest:receptors expression in breast cancer and medical education

Dr. Saroj Kaler Jhajhria joined as assistant professor in the Anatomy department (AIIMS) in 2012.She did herM.B.B.S. from S.M.S. Medical College, Jaipur (Rajasthan). She completed MD and senior residency in Anatomy from the All India Institute of Medical Sciences (AIIMS), Delhi in 2008 and 2011 respectively. She is an active participant for Medical Education workshops & seminars and cadaveric workshops. Her interest includes neurobiology, toxicology and gross anatomy. She has administrative charge of the Gross Anatomy Lab (Dissection Hall).

Tony joined AIIMS as faculty in 2014. He is continuing his work on the pathogenesis of pancreatitis.Now, he and his team have also established two surgical models of acute pancreatitis in rats at the Institute, which also measures organ dysfunction.He is also working on two models of chronic pancreatitis.His work includes the role of autophagy, cell death and inflammation in the pathogenesis of acute and chronic pancreatitis. He also studies the development and effect of aging on the various components of the human auditory system.
He is interested in teaching various aspects of anatomy and has a special interest in history, especially that of medical education.He is also a resource person for Mentoring, Interpersonal Communication Skills and Personality Development in the Health Sector and also for medical research, writing a manuscript and the process of reviewing and editing.
a) Changing populations of neurons and glia in human cochlear nucleus with aging- Chapter 12
b) Morphology of the human pancreas during development and aging- Chapter 4 P.C Rath, R. Sharma, S. Prasad Eds: Topics in Biomedical Gerontology.
c) Parija SC, Adkoli BV Eds: Effective Medical Communication- the ABCD of it. Chapter: Jacob TG, Sahni P: Publishing effectively and ethically. Springer Singapore. 2020. pp 123-130. doi: 10.1007/978-981-15-3409-6.

Dr. Neerja Rani is a graduate (BSc. Hons Human Biology) and postgraduate (MSc. Anatomy) and Ph D fromAll India Institute of Medical Sciences, New Delhi. She worked on ‘Apoptotic changes in placenta of preeclamptic patients’ for her Ph D. Her work received an award at theInternational Federation for Placental Association in 2007.
She worked as a Senior Demonstrator in the Department of Anatomy, AIIMS,as Assistant Professor at PGIMS, Rohtak andas Assistant Professor at Lady Hardinge Medical College. At present she is working as an Additional Professor in the Department of Anatomy, AIIMS. Her area of interest in research is preeclampsia in humans.
1.Mochan S , Bhatla N, Rani N, Gupta SK , Saxena S ,Arora P andDhingra R.sFLT-1 induces endoplasmic reticulum stress by activating perk pathway in BeWo cells.Abstracts/Placenta.Mar2017; 51:130-131.
2.Gupta SK, Bhatla N, Rani N, Mochan S, Saxena S, Arora P andDhingra R.Hydrogen sulphide producing enzymes are decreased in placentas from preeclampsia.Abstracts/Placenta.Mar2017; 51:131.
3.Arora P, Khetrapal P, Bhatla N, Rani N, Mochan S, Gupta SK, Saxena S and Dhingra R.Matrix metalloproteinase 2 and tissue inhibitor of metalloproteinase 2 mRNA levels in early onset preeclampsia.Abstracts/Placenta.Mar2017; 51:131.
4.Deshmukh VR, Mandal RP, Kusuma H and Rani N.Accessory upper subscapular Nerve-The Neurotization tool.J Clin Diagn Res.2016Sep; 10(9):AD01–AD02
5.Jain P, Raza K, Singh S, Kumari C, Kaler S, Rani N.Lumbar sympathetic chain:anatomical variation and clinical perspectives.Clin Ter 2016; 167(6):185-187

Dr. Seema Singh is aMBBSgraduatefrom KMC Mangalore. She completed her MD and senior residency in Anatomy from AIIMS, New Delhi. She joined Lady Hardinge Medical College as assistant professor (Contractual basis) in 2013.Presently, she is anAdditional professorin the Department of Anatomy, AIIMS. Her interest includes enteric nervous system, medical Education and gross anatomy.

Dr. Subhash Chandra Yadav did Ph.D. (2007) in Molecular Biology from Banaras Hindu University (BHU), Varanasi, India. He was visiting researcher (from 2005 to 2006) at the Institute of Crystallography, Free University (FU) Berlin, Germany. He was a postdoctoral fellow at Molecular Biophysics Unit, Indian Institute of Science (IISc), Bangalore Karnataka (2007-08) India and Medical Center, University of Tennessee, Knoxville, TN USA (2008). He worked as a Scientist In charge of nanobiology and electron microscopy facility at the Institute of Himalayan Bioresource Technology (CSIR-IHBT) Palampur H.P. India from 2008 to 2011. He was employed as a Fellow at TERI-Deakin University (Australia) Nanobiotechnology Centre (TDNBC), New Delhi, from 2011 to 2015. He joined the Electron Microscope Facility, Department of Anatomy, AIIMS, New Delhi, as an Assistant Professor in 2015, Associate Professor in 2018, and currently an Additional Professor since 2021 of 3D Electron Tomography, Electron Microscopy, and Nanotechnology. He was visiting professor at Stanford University, the USA, in 2019-20.
Electron Tomography and Nanobiology, Development of nanotechnology-based diagnostics system, Targeted drug delivery vehicles and therapeutic efficacy improvement of biomolecules.
Raman S, Tanwar P, Bhatla N, Yadav SC. An Immuno-Nano-Fluorescence Assay, Antibodies and a Kit Thereof for Detection of Human Papillomavirus (HPV) Infection Associated Cervical Cancer. Indian Patent 2021, 202111035011 (Filed 03.08.2021)
Tiwari M, Dinda A, Yadav SC, Bhat M. Cancer Detection System, Patent Number; 400170, Application Number: 201611011074, dated 28.06.2022 (Indian patent granted)

Duration: Three (03) years Residency training programme in Neuroanaesthesiology and Critical Care
Eligibility A candidate must possess MD / DNB (Anaesthesia) degree of a University recognized by Medical Council of India. The entrance exams are conducted in December and May every year.
For further information contact Examination Cell, AIIMS
Procedure of selection
For this program the candidate is selected through 2 step competitive examination held at national level.
Final selection of the candidate is made on the bases of combined evaluation of step-I, and II
The candidates selected work as Senior Resident (non-DM) in the department. They are supposed to do all clinical work of OR, ICUs, and emergency both independently and also under supervision.
Teaching Program
Rotational Policy
There is a compulsory rotational policy for clinical exposure of the candidates to various sub-specialities of Anaesthesia and Intensive Care apart from Neuroanaesthesia, Neurotrauma, and Neurocritical Care. It is the only sub-speciality of Anaesthesia at AIIMS, New Delhi where the Senior Residents are exposed to most of the sub-specilalities of Anaesthesia. During the three years tenure the candidates are rotated to Trauma Anaesthesia (General, Ortho, and Neurotrauma) and Plastic Surgery at JPNA Trauma Centre, Onco-anaesthesia at BRA IRCH, General Anaesthesia including Laparoscopy, Transplant Surgery, Paediatric, Gynaecologic, ENT, and Ophthalmologic Anaesthesia at RPC.
Guidelines for Short-Term/Long-Term Training/Visiting Fellow in respect of Indian and Foreign National candidates
A. SHORT-TERM TRAINING UPTO PERIOD OF SIX MONTHS
Training will be provided to the candidates sponsored by the Government/Autonomous Bodies or Institutions/Public Health Sector Organizations / MCI approved medical colleges and Government / Defence Services. The short-term training may not be allowed to the private practitioners.
B. SHORT-TERM TRAINING UPTO THE PERIOD OF SIX MONTHS TO THE FOREIGN NATIONALS CANDIDATES
The short-term training may be provided to the foreign national candidates sponsored by the foreign Government / Autonomous Bodies / Medical Institutions duly recommended by the Dean or any other competent authority of the concerned College / University / Institution.
C. LONG-TERM TRAINING SIX MONTHS TO TWO YEARS
This training will be provided to the candidates sponsored by the Government of India / Semi-Government / Autonomous Bodies / Institutions / Public Sector Organizations / Public Defense Services only. The long-term training is not allowed to the private practitioners / NGOs.
The persons with postgraduate degree and working on regular basis will be given preference.
The department of Neuroanaesthesiology and Critical Care at AIIMS is committed for advancement and promotion of Neuroanaesthesia and Neurocritical Care in India and abroad. The department regularly organizes a scientific event the “AIIMS Neuroanaesthesia Update”, every year starting from 2013. Eminent faculties of National and International repute along with AIIMS faculty participate in the meeting. It is a unique event where the anaesthetic procedures are telecasted live from the operation theatres and the delegates directly communicate with the anaesthesiologists and operating neurosurgeon as a part of the discussion. The department also started regular courses such as Cadaveric Hands-on Workshop on Airway Management and AIIMS Neurological Life Support (ANLS) with the target audience which includes emergency physicians, neurosurgeons, and neurologists apart from the anaesthesiologists. The department encourages faculty of national repute to deliver talks in the Neurosciences Centre based on recent neurosciences issues. The department also encourages faculty of International repute to be part of the departmental academic and research activities as a Visiting Professor.
For more details contact Dean / Registrar, Academic Section - II, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110 029, India
The Services of Onco-Anaesthesiology, Critical Care, Pain and Palliative Medicine is an integral part of Dr BR Amedkaer Institute Rotary Cancer Hospital and National cancer Institute, All India Institute of Medical Sciences, New Delhi. The unit has grown over the years to provide holistic pain management of the whole of this cancer centre in addition to providing anesthesia, Intensive care and Palliative Medicine services. The Unit of Anesthesiology was upgraded to Department of Onco-Anaesthesia and Palliative Medicine in June 2015. The Department is headed by Dr (Prof) Sushma Bhatnagar. The department have well trained faculty (Dr Sushma Bhatnagar, Dr Seema Mishra, Dr Rakesh Garg, Dr Nishkarsh Gupta, Dr Vinod Kumar, Dr SachidanandJeeBharati, Dr BrajeshRatre) and provide services to anesthesiology, intensive care, pain and palliative care. All of them are professionally qualified anesthesiologists and critical care physicians and have gained experience as palliative care personnel in the advanced cancer patients referred for pain and other symptom management.
The mission of the Department is to provide state-of-art and comprehensive care for patients with cancer with both curative and palliative intent. It includes services for various diagnostic interventions, surgical procedures, pain and palliative procedures. The department provides round the clock services for acute and chronic pain management as well. The department has six bedded intensive care unit which provides care for critically ill patients and six bedded palliative care ward for palliative care of oncology patients.
Since the inception of the unit way back in 1990s, the unit has grown in all aspects of the care including anaesthesia, intensive care, pain and palliative care. Because of the holistic contribution and increase in faculty strength, unit was upgraded to department. The Department has its regular academic activities and also pursuing various research activities in the fields of Cancer Pain, Palliative Care and Perioperative Medicine for proposed benefits for the patient. These research activities provides beneficial. The department has developed protocol and has structured SOPs for better patient management. The department organizes CMEs, conferences and workshops on regular basis. The unit also organizes certificate course in Palliative Care twice a year in the month of June and November and Foundation course on Palliative care once in a year in the month of February.
The department provides comprehensive care for the surgical procedures. We have pre-anaesthetic clinic for preoperative evaluation and optimization for surgical interventions. The operating rooms are well equipped with state-of-art infrastructure including anesthesia workstations and other ancillary equipments like invasive monitoring devices, intubating fiberscope, ultrasound machines etc. The centre has well equipped recovery area providing immediate care to postsurgical patients. All surgical patients receives acute pain management services round the clock supervised by the faculty. Our department provides point of care technology with ultrasound for diagnostic (vascular access, nerve blocks, volume responsiveness assessment, and for therapeutic purposes (pleurocentesis, optimization of cardiovascular function in various types of shock) in the operating room, palliative care ward and Intensive care
The department provide emergency services including airway management and ventilatory support to patients admitted with other specialties like surgical oncology, medical oncology and radiation oncology. The services for management of pain due to chemotherapy or radiation therapy are also provided to these departments round the clock.
The intensive care unit is six bedded and provide care for patients after the surgery and critically ill patients from surgical oncology, medical oncology and radiation oncology departments. The ICU is well equipped with state-of-art technology and human manpower. The nursing staff and physiotherapist are well trained and provide care round the clock.
We have also run OPDs 6 days in a week where we examine and treat cancer pain patients and admit patients if required to the palliative care. In theses OPDs we also patients for pre anesthesia check ups. The six bedded palliative care unit provides total in-hospital care to cancer patients for palliative care management. The ward has an adjoining procedure room which provides well equipped place for interventions in palliative care patients for symptom and pain management. The ward has well trained nursing staff and physiotherapist for improving the quality of life for cancer palliative care.
The department has been sanctioned two academic courses - and first batch of these DM and MD candidates started from January 2016. The department also organizes certificate course in Palliative care every six months.
The department has been designated as WHO collaborating centre for Training and and Education in Palliative Care (WHO CC IND-163).
The department had been designated as ESMO Designated Centre of Integrative Oncology and Palliative Care.
Dr. Sushma Bhatnagar, MD
Professor and Head
Email : sushmabhatnagar1[at]gmail[dot]com
Mobile : +91-9811326453
For website related queries:
Dr Rakesh Garg
Mobile : 9810394950
Email: drrgarg[at]hotmail[dot]com

Institute Rotary Cancer Hospital (DR. B.R.A. Institute Rotary Cancer Hospital) started functioning in 1983-84 on 35 beds with infrastructure of 2 floors. Recently it has been converted into a 200 bedded, 7th floor building. Prime Minister of India Sh. Atal Bihari Vajpayee, inaugurated this centre on October 5, 2003.
Best of radiodiagnostic and radiotherapy machines including state of art linear accelerator, brachytherapy, stereotactic radiotherapy and intensity modulated radiotherapy are available at this centre. Vaccum assisted advanced mammography unit, first of its kind in India, has made stereotactic breast biopsy possible. Prostate cancer can be diagnosed at an early stage with help of tranrectal sextant biopsy. Radio frequency ablation of liver cancer has also been initiated.
DR. B.R.A. Institute Rotary Cancer Hospital is one of the few centres in the country to have established hematopoietic stem cell bone marrow transplant programme; more than 250 transplants have been performed. In collaboration with dept. of CTVS, stem cell transplant programme has been extended to treat myocardial ischemia also.
Medical Oncology has established modern techniques utilizing FISH and polymerase chain reaction (PCR) to prognosticate cancer patients. Also, innovative research by this department has demonstrated the liberation of hematopoietic cytokines from fetal liver, with the potential to treat aplastic anemia. This department has researched into our ancient wisdom also and has discovered that combination of yoga, pranayam, meditation and sudershan kriya-a rhythmic breating process induces positive changes in brain. These processes enhance antioxidant defence and immune functions of body, and thus may prevent onset and/or progression of cancer.
Preventive oncology programme to bring awareness about cancer masses has been initiated, also screening programme to detect cancer early, over 10,000 people have been screened so far.

Name: Dr. Gauri Shanker Kaloiya
Designation: Professor of Clinical Psychology
Qualification: Ph.D., M.Phil. (CIP)
E-mail: gkaloiya@aiims.edu
Telephone: 26593236 (off)
Rehabilitation Council of India (RCI) registration (CRR) No.- A01630
Feld of Interest: Addiction, Psychosocial interventions, Cognitive Behaviour Therapy, Family Therapy, Group Therapy, Life Skills,
Total No. of Publication: 90
THESIS SUPERVISION:
Guide: 5 (Ph,D.-2, MD- 3)
Co-Guide: 24 (Ph,D.-6, DM- 5, MD- 13)
AWARDS & HONOURS
Email: kaloiya@aiims.edu
Telephone: 26593236 (off)
Rehabilitation Council of India (RCI) registration (CRR) No.- A01630
Feld of Interest: Addiction, Psychosocial interventions, Cognitive Behaviour Therapy, Family Therapy, Group Therapy, Life Skills,
Total No. of Publication: 90
Ranjan P, Vikram NK, Chournar A, Pradeep Y, < Ahuja M, Puri MM, Malhotra A, Kumari A,Chopra S, Batra A, Balsalkar G, Goswami D, Guleria K, Sarkar S, Kachhawa G, Verma A, Kumari MK, Madan J, Dabral A, Kamat S, Mittal A,Kumar R, Venkataraman S, Kaloiya GS, Bhatla N, Kumar SS, Baitha U, Prakash A, Tiwaskar M, Tewary K, Misra A, Guleria R (2022). Executive summary of evidence and consensus-based clinical practice guideline for management of obesity and overweight in postpartum women: An AIIMS-DST initiative. Diabetes & Metabolic Syndrome: Clinical Research & Reviews, 16 (3).
Ranjan P, Vikram NK, Chournar A, Pradeep Y, < Ahuja M, Puri MM, Malhotra A, Kumari A,Chopra S, Batra A, Balsalkar G, Goswami D, Guleria K, Sarkar S, Kachhawa G, Verma A, Kumari MK, Madan J, Dabral A, Kamat S, Mittal A,Kumar R, Venkataraman S, Kaloiya GS, Bhatla N, Kumar SS, Baitha U, Prakash A, Tiwaskar M, Tewary K, Misra A, Guleria R (2022). Executive summary of evidence and consensus-based clinical practice guideline for management of obesity and overweight in midlife women: An AIIMS-DST initiative. Diabetes & Metabolic Syndrome: Clinical Research & Reviews, 16 (3).
Jhanjee S., Varshney M., Panda U.K., Kaloiya G.S., Dayal P., Yadav D (2018). Evaluation of a training workshop on tobacco cessation: capacity building initiative in India. Tobacco Induced Diseases,16.( 1), A65. doi:10.18332/tid/84169
Thesis Supervision:
Guide: 5 (Ph,D.-2, MD- 3)
Co-Guide: 24 (Ph,D.-6, DM- 5, MD- 13)
awards & Honours
Email: akmaiims[at]gmail[dot]com, ashwanikm[at]aiims[dot]edu
Broad Domain: Epidemiology, Biostatistics
Sub-Domain: Substance Abuse, Clinical Epidemiology, Medical Epidemiology, Dimension Reduction Techniques, Computational Statistics
Total 159
Thesis
Official Statistics
Theoretical Statistics
Epidemiology of Drug Use
Applied Statistics-Public Mental Health
Applied Statistics-Clinical Sciences
Applied Statistics-Scientometrics
Applied Statistics-Cancer Epidemiology & Population Genetics
Edited Manuscript-Associate Editor
Book Chapters
Technical Reports, Manual, Reports
Organization of symposium/workshops/conference
Invited talks in conference, Symposium, Workshops
Awards and Honours
Education
1999: First Class First for Post-GraduateExamination (GOLDMEDAL)
2001: Fellowship in Biostatistics from SGPGIMS, Lucknow
2003: Received Post Graduate Education Certificate for Advanced Course in Biostatistics and Epidemiology from Nordic School of Public Health, Goteborg and RD Gardi Medical College, Ujjain
2004: Faculty for the International Course on Health Intervention Studies, in collaboration with Nordic School of Public Health
2005: Faculty for the International Course in Research Methodology in collaboration with Nordic School of Public Health and RD Gardi Medical College, Ujjain
2013: Awarded Certificate of Accomplishment with Distinction for the course Mathematical Biostatistics Boot Camp, offering of John Hopkin's University, USA
2020: Received certification of completion with 91.2%Marks for the successful completion of the course on Systematic Review and Meta-Analysis, from John Hopkins University, USA
2020: Letter of Commemoration from Vice-Chancellor, HNB Uttarakhand Medical Education University for effective planning, management of the ONLINE course in Research Methodology as Course Coordinator
2020: Received DST Grant from Department of Science and Technology (DST) under the Accelerate Vigyan Scheme through Scientific and Engineering Research Board (SERB) for organizing 9 days online workshop on Analytical Techniques for Statistical Analysis in Mental Health
2021: Elected Member Education Subcommittee for International Society for Clinical Biostatistics (ISCB). This honour is quite prestigious in the sense that I happen to be not only the member from India, or Asia but the only member from the Developing world. In total there are 15 [14+1] members in this committee. The other 14 members belong developed/high income countries [1Member each from Australia (AU), Canada (CA), France (FR), Romania (RO),3 Members from New Zealand (NZ), 5 Members from United Kingdom (UK), and 2 Members from USA (US).This committee supports and organize education al activities, such as short-courses, webinars, and seminar son contemporary methods in Clinical Biostatistics.
2021: Successfully Completed Paid Course with Examination on Data Science and Machine Learning: Making Data Driven Decision conducted by Massachusetts Institute of Technology (MIT) and MIT Institute for Data, Systems, and Society (MIT-IDSS).
2022: Nominated as the Board Member by Department of Medical Education and Research (DMER) by Government of Haryana, for Promotion of Research in Medical Universities.
Research Awards
2007: World Bank Travel grant for attending 56th International Statistical Institute Conference held at Lisboa-Portugal, for thesis research paper Some Epidemiological Models for Parasitic Infections: Comparison between traditional and Hierarchical Logistic Regression Methods
2014: World Bank Travel grant for attending 9th International Conference on Teaching Statistics for the research paper Challenges in Teaching of Medical Statistics in Developing Country
2017: Award from AIIMS, Delhi forthe research paper Pattern of Drug Use and associated behaviors among Female Injecting Drug Users from Northeast India: A Multi-Centric, Cross-Sectional, Comparative Study. Substance Use & Misuse
Associate Editor
2022-till date: Statistical Editor, International Journal of Health Research and Medico-legal practice (IJHRMLP); Official publication of the Academy of Health research and Medical Education (AHRME)
2020-tilldate: Associate Editor, Frontiers in Public Health for the Speciality Section Public Mental Health
2017-tilldate: Associate Editor Tobacco and Regulatory Sciences
Reviewer
Membership of the Scientific Societies

2. Name: Dr Ravindra Rao
3. Designation: Professor (Psychiatry)
4. Qualifications: MD (Psychiatry)
5. Email ID: dr[dot]rvenkatrao[at]aiims[dot]gov[dot]in, drrvrao[at]gmail[dot]com
6. Field of Interest: Addiction Psychiatry; Public Health related to substance use disorder; Community-based treatment for substance use disorder; Consultation Liaison Addiction Psychiatry
7. Total number of publications till date: 87
8. Details of publications since 2010 onwards (the full citation)- these should be divided into journal articles (peer reviewed publications) and books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications)
9. Presentations made at scientific meetings/ conferences/ workshops
10. Investigator/ Co-investigator in funded projects along with year completed/ongoing
11. Investigator/Co-investigator in non-funded projects along with year and title completed/ongoing
12. Thesis supervised for MD/ DM/PhD
- as guide (number only): 6
-as co-guide (number only): 12
 |  |  |  |  |
TRAINED Dr Deepak Agrawal completed his neurosurgical residency training from All India Institute of Medical Sciences (AIIMS), following which he did year long fellowship training in endoscopic and pediatric neurosurgery under Prof Steinbok in Vancouver, Canada. | GAMMA KNIFE Trained in Gamma Knife Surgery from Cleveland Clinic, USA and has performed more than 1000 Gamma knife surgeries till date. | SPINE AND SPINAL He is also especially trained in spinal surgery and spinal interumentation and has recieved the prestigous AO spine fellowship from BAsel, Switzerland. | TRAUMA Dr Agrawal has also been trained in trauma in Critical care and has been a fellow at University of Michigan, USA | TATA DBT Dr Agrawal has been Awarded the TATA DBT Innovation fellowship for a period of 3 years. |
| Dr. Gautam Sharma | Professor In-charge |
| Dr. Jitender Sodhi | Faculty |
| Dr. Anupama Gupta | Senior Medical Officer |
| Dr. Bharat Krushna Khuntia | Scientist C |
| Dr. Varun V. | Senior Medical Officer |
| Dr. Akriti Shukla | Medical Officer |
| Dr. Shubhangi Rathore | Medical Officer |
| Mr. Mohd. Sharique | Research Associate |
| Dr. Sriloy Mohanty | Research Associate |
| Mr. Aman Agarwal | Research Associate |
| Dr. Varun Chhabra | Senior Research Fellow |
| Dr. Mohit Wadhawan | Senior Research Fellow |
| Dr. Khushpreet Kaur | Senior Research Fellow |
| Mr. Amit Kashyap | Junior research Fellow |
| Mr. Kamal | Medical Social Worker |
| Mr. Ashish Panwar | Senior Technical Assistant |
| Ms. Bushra | Senior Technical Assistant |
| Mr. Vinay Sharma | Yoga Therapist |
| Ms. Divya Singh | Yoga Therapist |
| Ms. Alka Arya | Yoga Therapist |
| Mr. Deepak Kumar | Ayurveda Therapist |
| Mrs. Arti | Ayurveda Therapist |
| Mrs. Sarita | Ayurveda Therapist |
| Mr. Ishwar Singh | Ayurveda Therapist |
| Mr. Harsh Kumar | Multipurpose Worker |
| Ms. Priti | Multipurpose Worker |
| Mr. Kapil | Multipurpose Worker |
| Mrs. Shrabani Mondal | Senior Nursing Officer |
| Mr. Man Singh Jat | Senior Nursing Officer |
| Mrs. Sudha Lama | Nursing Officer |
| Mrs. Anu James | Nursing Officer |
| Mr. Arun EV | Nursing Officer |
| Mrs. Parul | Nursing Officer |
| Mrs. Sudha Sharma | Nursing Officer |
| Mr. Ram Teerath | Personal Assistant |
| Mr. Sushant Kumar | Singh Junior Administrative Assistant |
| Mr. Vishal Saroj | Field Investigator |
| Mrs. Veena | Data Entry Operator |
| Mr. Mark Daniel Baxla | Data Entry Operator |
E-mail: dr[dot]rvenkatrao[at]aiims[dot]gov[dot]in, drrvrao[at]gmail[dot]com
Addiction Psychiatry; Public Health related to substance use disorder; Community-based treatment for substance use disorder; Consultation Liaison Addiction Psychiatry
Total number of publications till date: 87
Details of publications since 2010 onwards (the full citation)- these should be divided into journal articles (peer reviewed publications) and books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications)
Ghosh S, Jain R, Rao R, Mishra AK, Jhanjee S. Does ethyl glucuronide in hair correlates with alcohol consumption? A comparative study with other traditional biomarkers among individuals with alcohol dependence syndrome. Alcohol, Nov 2022.
Singh B, Rao R. Is there an opioid epidemic in India? Journal of Public Health, 2021;43 (Suppl 2).
Ganesh R, Rao R, Deb KS, Bhad R, Yadav D. Digital Capacity and Interest in mHealth Interventions Among Individuals on Opioid Agonist Maintenance Treatment: A Cross-Sectional Community-Based Study. Indian Journal of Psychological Medicine. July 2021.
Ghosh S, Jain R, Singh S, Rao R, Mishra AK, Jhanjee S. A simplified approach for determination of urinary ethyl glucuronide by gas chromatography–mass spectrometry. Journal of Analytic Science and Technology, 2021;12:35.
Singh A, Rao R, Chatterjee B, Mishra AK, Kaloiya G, Ambekar A. Cognitive functioning in patients maintained on buprenorphine at peak and trough buprenorphine levels: An experimental study. Asian Journal of Psychiatry, 2021.
Rao R, Yadav D, Bhad R, Rajhans P. Mobile Methadone Dispensing – Experience of a new model of methadone delivery from India: An Implementation Research. Bulletin of the World Health Organization, 2021;99:422–28 doi:
Kathiresan P, Rao R, Narnoli S, Hans G, Sharan P. Adjuvant Trazodone for management of Protracted Delirium Tremens. Indian Journal of Psychological Medicine, 2020.
Rao R, Tripathi R. Stimulants and Sleep. In: Gupta R., Neubauer D.N., Pandi-Perumal S.R. (eds) Sleep and Neuropsychiatric Disorders. Springer, Singapore.
Investigator/ Co-investigator in funded projects along with year completed/ongoing
Investigator/Co-investigator in non-funded projects along with year and title completed/ongoing
- as guide (number only): 6
-as co-guide (number only): 12

Dr. Deepak Agrawal
Professor, Neurosurgery,
AIIMS, New Delhi-110029
Phone: 9868398242
E-mail: drdeepak@aiims.edu
Website: http://www.drdeepakagrawal.com
Dr Deepak Agrawal completed his neurosurgical residency training from All India Institute of Medical Sciences, following which he did year long fellowship training in endoscopic and pediatric neurosurgery under Prof Steinbok in Vancouver, Canada. He returned back to India to join AIIMS as faculty.
Dr Agrawal has received training in Gamma-Knife surgery and is a part of the gamma-knife team at AIIMS. He is also trained in stereotactic and image guided neurosurgery and is credited for indigenization of a key component of image-guided neurosurgery which has resulted in more than 99% savings in the cost of disposables used in image-guidance
Dr Agrawal has a keen interest in research and has been instrumental in securing the ‘DST-FIST’ grant for the department of neurosurgery at AIIMS. He is presently involved in a multinational, muticentric shunt registry and in an autopsy study on diffuse axonal injury which is funded by AIIMS. He has won several national and international awards for his research and has more than 10 chapters in neurosurgical texts and more than 50 publications (including 15 original research articles) which have been published in international publications. His specific research interests are shunt infection and pathogenesis of severe head injury.

Dr Yatan Pal Singh Balhara
MD, DNB (Psychiatry), MNAMS, Masters in Addiction Studies (King’s College London, UK; University of Adelaide, Australia; Virginia Commonwealth University, USA), International Masters in Mental Health Policy and Services
ypsbalhara[at]gmail[dot]com
Professor of Psychiatry, NDDTC and Department of Psychiatry, AIIMS, New Delhi
Visiting Faculty, AIIMS, Rishikesh
Global Master Trainer, UNODC and The Colombo Plan
Mental health (including addictive disorders) policy and services; Co-occurring disorders (Interface of psychiatric disorders, medical disorders, Addictive disorders- dual disorders); Behavioral Addictions (Internet addiction, gaming addiction etc.); eHealth
Total number of publications: 350
E-mail: ypsbalhara[at]gmail[dot]com
Visiting Faculty, AIIMS, Rishikesh
Global Master Trainer, UNODC and The Colombo Plan
Mental health (including addictive disorders) policy and services; Co-occurring disorders (Interface of psychiatric disorders, medical disorders, Addictive disorders- dual disorders); Behavioral Addictions (Internet addiction, gaming addiction etc.); eHealth
Total number of publications: 350
Bhutani, J., Bhutani, S., Balhara, Y. P. S., & Kalra, S. (2012). Compassion fatigue and burnout amongst clinicians: A medical exploratory study. Indian Journal of Psychological Medicine, 34(4), 332–337.https://doi.org/10.4103/0253-7176.108206
Dr Manmohan Singh
Assistant Professor, Neurosurgery
Office Phone No. : 011-26588700-ext 4914
E-mail mehaknoor@hotmail.com
Personal Profile: Born on 9th October 1972. Graduated from Govt. Medical College Amritsar in 1993. Completed internship in 1994 in the same institute.Achieved M.S. (Surgery) degree in 1997 from Post Graduate Institute of Medical Education and Research (PGIMER) Chandigarh and received Silver Medal for topping M.S (Surgery) exam. Thereafter worked as Senior Resident (General Surgery) in PGIMER. Joined AIIMS as MCh Neurosurgery candidate in July 1999 and finished in 2002 May. In June 2003 Joined AIIMS as Assistant Professor Neurosurgery.
Primary area of interest: Skull base, Vascular and Brachial Plexus surgery apart from Neuro-oncology and spine.
Unit: Neurosurgery unit-II
OPD Schedule: Tuesday and Saturday 9.00 am-1.00pm
Research Project:
1.Principal investigator in ongoing international multicentric multinational trial: CRASH-2 (A large randomized placebo controlled trail among trauma patients with or at risk of significant haemorrhage, of the effect of antifibrinolytic treatment on death and transfusion requirement)
Till now have enrolled 21 patients
2.AP12009-G004 in Recurrent Grade III-IV glioma-A multinational and multicentric double blind randomized trial. Sponsored by Antisense Pharma-Germany. Period Dec. 2003 – June 2006 Mahapatra AK, Julka PK, Suri A, Kale SS, Singh Manmohan
Publications:

2. Name: ATUL AMBEKAR
3. Designation: Professor
4. Qualifications :- MBBS, MD
5. Email ID- atul.ambekar[at]gmail[dot]com, atul.ambekar[at]aiims[dot]edu
6. Field of Interest:
• Public Health Issues related to Alcohol and Drug Use
• Opioid Substitution Therapy (OST) and Harm Reduction
• Training and human resource development
• Gender and drug use
• Drug Policies and Programs
• Epidemiology of drug use
• Community based research to facilitate access to services
• Use of Information and Communication Technology in addiction-related issues
7. Total number of publications till date: 185
8. Details of publications since 2010 onwards (the full citation)- these should be divided into journal articles (peer reviewed publications) and books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications):
9. Presentations made at scientific meetings/ conferences/ workshops (2017 onwards)
10. Investigator/ Co-investigator in funded projects along with year completed/ongoing
11. Investigator/Co-investigator in non-funded projects along with year and title completed/ongoing
12. Thesis supervised for MD/ DM/PhD
- as guide: 12
-as co-guide: 23
13. Awards and Honours
• Addiction Psychiatry Society of India (APSI) – Secretary General
• American Society of Addiction Medicine (ASAM)
• Asia Pacific Society for Alcohol and Addiction Research (APSAAR) – Board of Directors (2017-21)
• Harm Reduction International (HRI)
• Indian Association for Social Psychiatry (IASP) – Elected Member, Executive Council (2017-20)
• Indian Association of Private Psychiatry (IAPP) – Member, National Advisory Board
• Indian Psychiatric Society (IPS) – Member, Certification and course committee
• International AIDS Society (IAS)
• International Doctors for Healthier Drug Policies (IDHDP)
• International Society for Substance Use Treatment & Prevention Professionals (ISSUP)
• International Society for the Study of Drug Policy (ISSDP)
• International Society of Addiction Medicine (ISAM) – Member, Board of Directors
Training and Capacity Building Consultancies
Research and Evaluation Consultancies
Dr. Rajinder Kumar
Asstt. Prof Neurosurgery
Office phone No.:Ext 4914
E mail ID :rklaythalling@rediffmail.com
Areas of Interest: Spine Surgery, Pediatric, Endoscopy Functional neurosurgery
OPD Schedule: Unit- 1 Mondays morning Thursdays evening need to take prior appointment for OPD consultation
In patient services daily rounds , operations, consultations.
Research Projects
Role of VIIa in contusive Brain Injury - A Phase II Trial
CSF Proteomics study in Health and Disease
In Vitro study of MHC and TGF and role of interferon gamma in culture of GBM cells
Long term comparative study of ant versus post approach in degenerative cervical spondylosis
Publications Four
E-mail: atul.ambekar[at]gmail[dot]com, atul.ambekar[at]aiims[dot]edu
number of publications till date: 185
Details of publications since 2010 onwards (the full citation)- these should be divided into journal articles (peer reviewed publications) and books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications):
Singh A, Rao R, Chatterjee B, Mishra AK, Kaloiya G, Ambekar A (2021). Cognitive functioning in patients maintained on buprenorphine at peak and trough buprenorphine levels: An experimental study, Asian Journal of Psychiatry, 61, 102697,
Singh et al (India State-Level Disease Burden Initiative Neurological Disorders Collaborators) (2021). The burden of neurological disorders across the states of India: the Global Burden of Disease Study 1990–2019. The Lancet Global Health,
Castro‐Calvo, J., King, D. L., Stein, D. J., Brand, M., Carmi, L., Chamberlain, S. R., Demetrovics, Z., Fineberg, N. A., Rumpf, H.‐J., Yücel, M., Achab, S., Ambekar, A., Bahar, N., Blaszczynski, A., Bowden‐Jones, H., Carbonell, X., Chan, E. M. L., Ko, C.‐H., de Timary, P., Dufour, M., Grall‐Bronnec, M., Lee, H. K., Higuchi, S., Jimenez‐Murcia, S., Király, O., Kuss, D. J., Long, J., Müller, A., Pallanti, S., Potenza, M. N., Rahimi‐Movaghar, A., Saunders, J. B., Schimmenti, A., Lee, S.‐Y., Siste, K., Spritzer, D. T., Starcevic, V., Weinstein, A. M., Wölfling, K., and Billieux, J. (2021) Expert appraisal of criteria for assessing gaming disorder: An international Delphi study. Addiction,
Vishwakarma A, Tarwani J, Chawla N, Dayal P, Agrawal A, Mandal P & Ambekar A (2020) Mephentermine dependence with induced psychosis: a series of two cases, Journal of Substance Use, 25:6, 569-571, DOI: 10.1080/14659891.2020.1749949
Rao R, Gupta SK, Swaminathan P, Gupta V, Dhawan A, Agrawal A & Ambekar A (2020) Predictors of long-term retention on opioid agonist treatment with buprenorphine: a 6-year, community-based retrospective cohort study in India, Journal of Substance Use, 25:5, 489-494, DOI: 10.1080/14659891.2020.1736666
National Drug Law Enforcement Agency (2021) [lead authors: Ambekar A & Kedia S]. Standard Policy and Practice Guidelines for NDLEA counselling centres . Lagos: United Nations Office on Drugs and Crime and National Drug Law Enforcement Agency (NDLEA), Government of Nigeria
Standard Policy and Practice Guidelines for NDLEA counselling centres
Ambekar A & Mohan A (2019). Guidelines:Treatment of Opioid Dependence using Opioid Agonists (Buprenorphine),with focus on operational procedures Gurugram:Indian Psychiatric Society
Ambekar A et al (2018) Dealing with Substance Abuse (Block 1), MCFTE-003, Substance Abuse Counselling and Therapy, New Delhi: Indira Gandhi National Open University
Ambekar A et al (2018) Therapeutic Interventions (Block 2), MCFTE-003, Substance Abuse Counselling and Therapy. New Delhi: Indira Gandhi National Open University
Rao R, Agrawal A & Ambekar A (2014), Opioid Substitution Therapy under National AIDS Control Programme: Clinical Practice Guidelines for treatment with Buprenorphine . New Delhi: National AIDS Control Organisation, India.
Ambekar A (2012). Capacity Building Needs Assessment in the context of IDU Interventions in India. New Delhi: United Nations Office on Drugs and Crime (UNODC) Regional Office for South Asia, and National AIDS Control Organisation
Capacity Building Needs Assessment in the context of IDU Interventions in India
Ambekar A (2010), Reaching out to female partners of Injecting Drug Users: A Training manual for service providers. New Delhi: United Nations Office on Drugs and Crime, Regional Office for South Asia
Reaching out to female partners of Injecting Drug Users: A Training manual for service providers
Ambekar A, Rao R, Kedia S & Mukherjee D (2011), A manual for counsellors in the context of Injecting Drug Use – Targeted Intervention . New Delhi: United Nations Office on Drugs and Crime (UNODC) Regional Office for South Asia, New Delhi and the Tata Institute of Social Sciences (TISS)
A manual for counsellors in the context of Injecting Drug Use – Targeted Intervention
Ambekar A, Agrawal A, Rao R, Mishra AK, Khandelwal SK, Chadda RK on behalf of the group of investigators for the National Survey on Extent and Pattern of Substance Use in India (2019). Magnitude of Substance Use in India . New Delhi: Ministry of Social Justice and Empowerment, Government of India
Atul Ambekar, Viswanathan Arumugam, Umesh Sharma, Rajkumar Raju, Shalini Singh (2014), Drug Use Patterns among Clients Receiving Services from Targeted Interventions for People Who Inject Drugs: Findings from Bihar, Haryana, Jammu and Uttarakhand, New Delhi: India HIV/AIDS Alliance, 2014.
Anju Dhawan, Ravindra Rao, Atul Ambekar, Anita Chopra, Raka Jain, Deepak Yadav, Rajat Ray, (2014). Methadone Maintenance Treatment in India: A Feasibility and Effectiveness Report . New Delhi: United Nations Office on Drugs and Crime (UNODC) Regional Office for South Asia
Methadone Maintenance Treatment in India: A Feasibility and Effectiveness Report
Atul Ambekar (2012), Factors Influencing the performance of Targeted Interventions among IDUs. New Delhi: United Nations Office on Drugs and Crime (UNODC) Regional Office for South Asia, and National AIDS Control Organisation, India
Factors Influencing the performance of Targeted Interventions among IDUs
Atul Ambekar (2012), Association of Drug Use Pattern with vulnerability and service uptake among IDUs, New Delhi: United Nations Office on Drugs and Crime (UNODC) Regional Office for South Asia, and National AIDS Control Organisation
Association of Drug Use Pattern with vulnerability and service uptake among IDUs
United Nations Office on Drugs and Crime (multiple contributors) (2012) National Drug Use Survey in Maldives Male’: UNODC, Maldives Project Office
Atul Ambekar (2012), HIV Prevention among IDUs and their female sex partners – Implementation Gaps and Barriers: A Study in Punjab, Haryana and Chandigarh . New Delhi: United Nations Office on Drugs and Crime (UNODC) Regional Office for South Asia
Dabholkar H, Ambekar A & Benegal V,(2017) “Psychiatric Emergencies in Substance Abuse” in Thara R, Vijayakumar L (eds), Emergencies in Psychiatry in Low and Middle Income countries, Edition - II, New York: Routledge
Emergencies in Psychiatry in Low and Middle Income countries
Ambekar A & Deb KS , (2013). “Import of Narcotics for Clinical Trial Supplies”, in Kshirsagar N, Kulkarni T, Desai A, Shah J (eds), Regulatory requirements for Drug Development and Clinical Research , New Delhi: Indian Council of Medical Research (ICMR)
Regulatory requirements for Drug Development and Clinical Research
Dabholkar H, Ambekar A & Benegal V, “Psychiatric Emergencies in Substance Abuse” in Thara R, Vijayakumar L (eds), Emergencies in Psychiatry in Low and Middle Income countries , (2012), Manipal: Byword Books
Emergencies in Psychiatry in Low and Middle Income countries
Investigator/ Co-investigator in funded projects along with year completed/ongoing
Investigator/Co-investigator in non-funded projects along with year and title completed/ongoing
- as guide: 12
-as co-guide: 23
Awarded “ Venus International Medical Award 2019 (VIMA 2019)” for Excellence in Psychiatry, April 2019
Winner of “ BMJ Awards South Asia 2016” for the category, “Non-Communicable Disease Initiative of the Year”, November 2016
International Journal of Drug Policy
International Journal of Mental Health and Addiction
Journal of Addiction and Dependence
Journal of HIV for Clinical and Scientific Research
Journal of Drug Safety and Toxicology
Journal of Mental Health and Human Behaviour
Drafting thematic chapter of INCB Annual Report 2017 (“Treatment & rehabilitation of drug use disorders: Essential component of demand reduction ”).International Narcotics Control Board (INCB), Vienna (2017)
Treatment & rehabilitation of drug use disorders: Essential component of demand reduction
Developing (a) “ Standard Policy and Practice Guidelines ” and “Training Manual” and (b) conducting training programmes for Counsellors. National Drug Law Enforcement Agency (NDLEA), Government of Nigeria andUNODC, Vienna (2015-2017)
Developing a E-health portal on Problem alcohol use in India, [ https://www.alcoholwebindia.in ]WHO, Geneva (2010-13)
National Drug Use Survey in Maldives. UNODC, Maldives Project Office (2011-2012)
Training and Capacity Building Consultancies
andstudy of Capacity Building Needs Assessment (CBNA) Factors Influencing Performance of IDU Targeted Interventions in India.UNODC, ROSA, under GFATM Round 9 (2011)
Factors Influencing Performance of IDU Targeted Interventions in India
Developing a Training Manual for reaching out to female sex partners of male IDUs , and conducting TOT Programme. UNODC, ROSA (2010-2011)
Training Manual for reaching out to female sex partners of male IDUs
Developing a training manual for counsellors in the context of Injecting Drug Use – Targeted Intervention, Consultancy forUNODC, ROSA (2010-2011)
Drug Use Pattern Assessment among People Who Inject Drugs (PWID) in Haryana, Bihar and Uttarakhand ,India HIV/AIDS Alliance and NACO (2013-2014)
Drug Use Pattern Assessment among People Who Inject Drugs (PWID) in Haryana, Bihar and Uttarakhand
Association of Drug Use pattern with Vulnerability and Service uptake among Injecting Drug Users in India ,UNODC, ROSA, (2012)
Gaps and Barriers in implementing and scaling up services for HIV Prevention among IDUs in Punjab and Haryana . UNODC, ROSA (2009)
In-charge: Implementation of the scheme “Strengthening Drug De-Addiction Programme: Establishing Drug Treatment Clinics (DTCs)”, Ministry of Health and Family Welfare, Government of India. Details at: http://dtc-scheme.in/
In-charge: Implementation of the scheme “Establishing Addiction Treatment Facilities (ATFs) in government hospitals in India”, Ministry of Social Justice and Empowerment, Government of India. Details at: https://atf-scheme.in/
The Centre for Integrative Medicine and Research is a pioneering initiative by AIIMS, New Delhi in the quest for convergence of contemporary medicine with India’s ancient and traditional medical practices. The centre at the premier institute of the country shall be dedicated to research, documentation and delivery of holistic healthcare. It has been envisioned as a “state of the art” research centre where top experts from various disciplines of contemporary medicine will collaborate with Yoga and Ayurveda specialists, both for disease treatment, and for preventive healthcare. The Centre for Integrative Medicine and Research was inaugurated on 22nd of June 2016 by Shri J.P Nadda, honourable Union Minister for Health and Family Welfare and president AIIMS, in the presence of Prof M.C. Mishra, director, AIIMS, New Delhi and Dr H.R. Nagendra, chancellor, Swami Vivekananda Yoga AnusandhanaSamsthana, Banglore.
Prof. A K Banerji
(1965-1995) presently Emeritus Professor Neurosurgery
“It was May 1965 that I came to Delhi from Vellore where I was a lecturer, to appear for a Union Public Service Commission interview for the job of Reader at G. B. Pant hospital, Delhi and All India Institute of Mental Health, Bangalore (later to become NIMHANS). I was the only candidate and was asked at the end as to which place would I prefer. I chose Bangalore. Just before leaving for the interview, I had gone to see Dr. Baldev Singh and Dr P. N. Tandon (PNT) at AIIMS to pay a courtesy call. They were sharing an office and I suspect eagerly waiting like spiders, to catch a victim in neurosurgery, who could stick on at AIIMS, which at that time had actually nothing no space, equipment or staff. After a little talking about general things, suddenly, Dr. Baldev Singh asked me to think whether I at all wanted to go for the interview, as AIIMS could possibly offer me a job, I of course declined the proposal as a bird in hand was better than two in the bush. Then Dr. Tandon asked me to come home for tea that evening. I left for the Union Public Service Commission office. Today when I see large number of candidates for a job interview my own experience seems miraculous.
Coming back after the interview I recounted what happened to Gopal and his wife Radha (Dr. G.K. Vishwakarma was then Asst. Professor Orthopaedics and later became D.G.H.S. of Government of India) Insidious pressure started from them to come to AIIMS and forget about Bangalore. Incidentally Bangalore had a working, full fledged department with Prof. RM. Verma and he tried hard to get me there even after I joined AIIMS.
That evening I spent at Tandons. Dr. P. N. Tandon had been my Anatomy demonstrator in 1952 while Mrs. Leela Tandon was my lecturer in Obstetrics and Gynaecology at Medical College, Lucknow. I had met Dr. P.N. Tandon in 1963 at the annual Neurological Society of India meeting in Calcutta. For both of us it was the very first meeting that we had attended of NSI. Dr. P. N. Tandon had established the department of neurosurgery at AlIMS 2 months before in March 65. He had been promised equipment but nothing had arrived in the two months. He was eager that I should join but was frank to say he did not know how things would eventually develop. After returning to Gopal's house, Radha and Gopal took me to see 'My Fair Lady' at Sheila Theatre which then was the best in Delhi, if not India. After returning well past midnight we slept on the roof and went on talking about what I should do. I think it was near the break of dawn that I finally succumbed to pressures from Gopal and Radha and said OK I'll come to Delhi if the job was offered. Next morning before I left Delhi Dr. Baldev Singh took me to meet Prof. K. L. Wig then Director AIIMS. Our liking for each other was instantaneous and the bond carried throughout.
I joined as adhoc Assistant Professor in June'65. There was one office of Dr. Baldev Singh in which in addition to Dr. P. N. Tandon another chair and a small table was put for me. The process of starting a department began really from scratch. Space was allotted on the first floor by the side of anatomy lecture theatre. I and Dr. V. Virmani (my opposite number in Neurology) sat down to draw maps and carve out rooms in the large halls. At that moment, our vibes were bristly to say the least. Dr. Virmani was considerably senior in age plus she had known Dr. Baldev Singh since Amritsar days and she also held the trump card of being Punjabi speaking which was then the lingua franca of AIIMS. Over the years our relationship mellowed and we did develop mutual admiration and respect for each other. I hit upon the strategy in our dealings at that time of building the departments, of saying exactly opposite of what I wanted. Dr. Virmani would of course, reverse my suggestions much to my advantage. Today when I look back it all appears so childish. But then it was great fun. Slowly collecting items like pins, chairs, tables, almirahs and make real offices was a new challenge for which I was not trained. Anyway we built the office cubicles, laboratories and got the OPD on the 4th floor in ship shape. It was so gratifying after two years of joining that we had a place of our own.
We started with surgical instruments which actually were of World War II vintage which included an operation table. Burr holes had to be made by a brace in 4 stages and both Dr. Tandon and I developed the art to perfection. To begin with we had no beds. Both for Neurology and Neurosurgery, Prof. K.L. Wig and the Pediatricians generously allowed us use of their beds in what is now the nurses hostel. There was so little clinical work that it was terribly frustrating in the beginning. I started taking clinics for the MD students of medicine, pediatrics and radiology. I slowly became quite popular to the extent that one day Dr. Wig called me to see one of his patients in his office. I must have impressed him no end as after that on several occasions he would ask for my opinion on patients. This was a small matter for him but a great boost for my confidence for which my gratitude goes to him.
By 1968 we were having a ward in the OPD block (ward IX) and we were well settled. The operation theaters were in the College of Nursing Block. Radiology to begin with was in the nurses hostel, and only in 1968 shifted to its present location. That was the time when we had Dr. S. K. Ghosh in radiology from 1965 to 1968 and he was a great help. Very often we started the day at 7.30 A.M. with ward rounds, dressings and stitch removals, followed by neuroradiology (ventriculograms angiograms etc) and then this was followed by surgery which would invariably end by 7 or 8 P.M., particularly if it was a posterior fossa tumour. At night one of us i.e. PNT or myself would sleep in the doctors room adjacent to the main O.T. block. From 1966 onwards Dr. B.B. Sawhney and Dr. M. Gourie Devi, now Director and Vice Chancellor NIMHANS who were residents in neurology would help us out by doing night duties and also assist in surgery as we did not have regular residents of our own. The role played by Col. G.C. Tandon, the Professor of Anaesthesia, was unforgettable. Dr. Hattangdi's lectures in anaesthesia helped us enormously and he also shared our burden in looking after patients, sometimes relieving us of our daily chores. The two films I saw with Anjali, my wife, during the time was courtesy of Hattangadi. Before I proceed I must tell of my first day in the operation theatre block (MOT) in the consultants changing room, where I went on my own apprehensively, to discover its ambience. The only person there in OT dress was reading an Agatha Christie paperback with great seriousness. On entering he asked me as to who I was and then got up with great cordiality and shook me by the hands. That was Dr. Satish Nayyar, Assistant Professor in Surgery well known as he was a Hallet medalist in the primary FRCS examination. Dr. Satish Nayyar gave me a cup of tea and then said that I must cultivate some hobby (his was reading mystery novels) as Assistant Professors had nothing to do as the Professor usurped all the work which was worthwhile, while all the minor work was done by the Registrars (later called residents). I went into depression from which it took me a long time to come out. Within a week I took courage in my hands and went to talk it over with PNT. We decided that alternate cases would be operated by us while the other would assist. Matters went on well but I was perturbed over the fact that if he assisted, he would go out and talk to the patients attendants before I could come out. Again I went to him in 1968 and PNT graciously agreed he wouldn't do so. This was a remarkable thing at AIIMS. My struggle for identity of Assistant Professors went on to the faculty over such oligarchy and it was ultimately in 1970 that I was able to change the nomenclature of hospital units which hitherto were identified with the head, to that of the departments. Thus Prof. P.N.T's unit changed to Neurosurgery unit-a practice which continues today. I have always felt that to obtain the best from colleagues a measure of democracy and participation should be the prime substance PNT's contribution towards this was immense which allowed me to put my heart and soul in developing the department and later the Neurosciences Centre. I guess the role of wives is also very great. Our families (Tandon and Banerji) were close to each other and even today no major decision in the Banerji family takes place without Tandons consultation. I guess this meeting was lucky for both of us.
In 1969 Dr. S.K. Ghosh left for Goa on promotion as Professor and Neuroradiology was taken over by Dr. R.K. Goulatia for whom a separate post was created in neuroradiology. In mid 70's Dr. S.S. Saini was persuaded to join Neuroanaesthesia and this started the nucleus of a comprehensive clinical setup. Fortunately we were able to persuade (Mrs. D. Saini to join as our OT sister incharge and thus there was a feeling of family and belonging, so important in the development phases of any new venture. Dr. Subimal Roy was spending considerable time in Neuropathology to complete the picture. I had a vision of Neurosciences Centre akin to PNT, however I knew that basic neurosciences can never develop on its own because of economic compulsions. My emphasis was on developing clinical neurosciences and bring in basic neurosciences within its umbrella.
By mid 70's both neurosurgery and neurology had relocated itself on the main hospitals 4th floor and we were lucky to have separate independent wards. Mrs. M. Bindra joined us as sister I/C of neurosurgery ward and her dedication eventually made our ward the talking point of nursing care in the Institute. She eventually rose to become the Nursing Superintendent of the Neurosciences Centre.
In 1966 one day, walked into my office Dr. Brahm Prakash, who had resigned his Short Service Commission in the army and had married recently. He was at loose ends, asking my advise as to what he should do. He had earlier worked as my junior resident in general surgery at Medical College, Lucknow and the association was about 10 yrs. old. I persuaded him to join neurosurgery.We were able to rustle up the required formalities for starting MCh course with bare facilities but boundless enthusiasm. He was the first trainee and later joined our faculty and went on to become the Director Professor at G.B. Pant Hospital and started his own MCh programme. The AlIMS MCh course went from strength to strength and eventually we were having both the 5 yr and 3 yr streams. Neurology D.M. had started already in 1965. Now AlIMS trainees are spread all over India. Several headed departments e.g? Dr. Gourie Devi became Director Vice Chancellor of NIMHANS, Dr. B. Prakash at G.B. Pant Hospital Delhi, Dr. B.S. Das at NIMHANS, Dr. S. Mohanty at IMS, BHU Varanasi, Dr. A. K. Reddy at NIMS Hyderabad, and Dr. M.A. Wani at SKIMS Srinagar. Many hold important positions in teaching as well as private sector. We i.e. PNT and I are inordinately proud of all who trained themselves with us and wish them all the best in their future endeavors. Our wish is that they better us in their achievements. A major breakthrough in our clinical services occurred in 1976 with the coming of Prof. H.W. Pia who did a course in laboratory microsurgery. In the next few years we started a microsurgery laboratory and operative microsurgery was initiated. In the Indian scenario we stole the lead. In late 60's with the help of our ENT surgeon Dr. S.K. Kacker we started trans-sphenoidal pituitary surgery which consolidated in the 70's and became a routine procedure.
The process of development of the Neurosciences Centre in collaboration with the Cardiothoracic Sciences Centre started in real earnest in early 70's. Dr. N. Gopinath of Cardiothoracic Surgery and PNT were the architects. Land allocation was done by Prof. V. Ramalingaswami, the then Director AIIMS. Ghosh and Pradhan Associates were appointed architects and their started the planning for the basement, ground floor and the operation theatre block of our centre. Hours and hours of meetings with the architects-designing and tearing plans, it went on and on. I heard my wife say that I started talking of planning even in my sleep. We were about ready to have the foundation stone laying. This was 1977 and Mrs. Indira Gandhi's infamous emergency was coming to an end. One afternoon, in PNT's office, Dr. N. Gopinath suddenly said it would be nice to have Mrs. Gandhi lay the foundation stone. I had recently treated Mr. Dhawan's (then the personal secretary to Mrs. Indira Gandhi) nephew and I said shall I try. I rang him up on the phone from PNTs office. Mr. Dhawan immediately said yes and wanted probable days and times so that it could be confirmed taking into account Mrs. Gandhi's tour programmes. Elections were round the corner and Dr. Ramalingaswami wisely asked us to go slow. Mrs. Gandhi lost the elections and it is possible that the Janata Government which followed may have taken offence and delayed the start of the Centre had we got Mrs.lndira Gandhi to lay our foundation stone. Eventually, President Mr.Neelam Sanjeeva Reddy lay the foundation stone in 1978. When the building started many problems surfaced e.g. we suddenly discovered that there were very few toilets while most of the patients of cardiology were on diuretics and required use of toilets frequently. Again to the drawing boardbreaking of walls, laying of new sewer lines and so new toilets came into being. I know the OPD and of course the toilets have today become too inadequate with increasing number of patients coming to the Centre.
The brief period of Janata regime from 1977 and 1979 saw the irrepressible Mr. Raj Narain come as the Health Minister. All work in the Ministry came to a halt as also our Centre which bore the backlash of erratic ways of Mr. Raj Narain. The only thing I remember was meeting him near the present Community Medicine Department late in the evening,Mr. Raj Narain was coming to inaugurate, if I remember correctly, the Centre of Community Medicine. As usual he was hours late and the then Director Dr. L.P. Agarwal was standing with 3to4 faculty members. I tried slinking away but Dr. L.P. Agarwal called me and more or less forced me to stay on awaiting Mr. Raj Narain. He eventually came when the numbers of people waiting was not more than half a dozen. Before going to cut the ribbon he was introduced to all of us. He was highly intrigued with me and asked what would I find if I did have an opportunity to see the inside of the head of Mrs. Indira Gandhi. I made some polite comments though I was sure Mrs. Gandhi had a better quality brain than Mr. Raj Narain. Anyway he went on to narrate it with great gusto during a special convocation to award an Honorary D. Litt to Dr. Sewoosagar Ramgoolam of Mauritius. It was in such bad taste that Morarji Desai who was chairing frowned and all of us in the auditorium hung our head with embarrassment.
My two stints as Chief of Neurosciences Centre were significant in the development of the Centre. The first was a 2 year term as acting Chief of Centre while Dr. PNT was on Nehru Fellowship between 1984-86. This was the time when after the first phase of building (OPD, radiology wing, basement and OT block) we had reached a dead end as far as expansion of the Centre was concerned. Prof. M. L. Bhatia was the Chief of Cardiothoracie Sciences Centre. Our formal requests for funds were stiffly rebuffed by the then Joint Secretary Finance Adviser (JSFA) of Health Ministry. Ms. Sarla Grewal, widely nick named 'hunterwali' by her unkind colleagues, was the Secretary. We were advised not to try and influence her which could cause an unpredictable antagonism to our proposal. Anyway we went to meet her, placed before her, the developments till date, including our mounting clinical load, increasing public expectations, and the blockades experienced by us for expanding our Centres to what was originally planned. Ms. Grewal quietly listened to us, occasionally interjecting for a clarification. After we completed she asked for the JSFA who was the main stumbling block, to come and join the meeting. The moment he saw us his hackles were raised. On being asked by Ms.Grewal as to what were the problems in giving us the grant he started off with a long list of financial mismanagement by AlIMS in which our Centres had no role to play. (Most of the problems recounted were exaggerated to say the least). Ms. Grewal asked as to why our Centres were being penalised for what AlIMS had done. To this the JSFA said that this is a part of financial management for which he was responsible. Then we saw the legendary Ms. Sarla Grewal come into her elements. In chaste Punjabi she asked the JSFA as to who was the Secretary of the Ministry and how dare he speak to her like that. The poor JSFA spluttered and stuttered and tried to put in a word edgeways. Ms. Grewal asked him to leave the office and we knew that our battle was half won. However after leaving her office both Prof. M.L. Bhatia and I, as a matter of diplomacy, went to the JSFA's office. He was in the dumps. We nursed his hurt ego by asking for his help as we knew that he was quite capable of going to the Finance (Expenditure) Secretary and derail our proposals. I think the strategy worked as he did become a supporter. Of course things were helped as a few close relations of the JSFA fell conveniently ill at the same time requiring cardiac and neurosurgery. Funds eventually came though it took another year and in 1986 the remainder of the present Centre's building was started. Prof. P. Venugopal was a constant source of support in our endeavours. In the same period the next Union Health Secretary was Mr. Srinivasan, who was unenthusiastic about our Centres. His general impression was that we were overstaffed, our equipment underutilized and our clinical output low compared to other hospitals e.g. G. B. Pant Hospital Delhi, Christian Medical College Vellore, and certainly Apollo Hospital Madras which to him was the ultimate in financial management and output. Incidentally he was involved with the starting of Escorts Heart Institute which he clearly told us is a 'better bet than us'. Prof. Bhatia, Venugopal and I went through our records as well as what we could gather from the other institutions which Mr. Srinivasan thought had better quality and quantity of work. He had a meeting separately with our Neurosciences group to take stock. I had taken Dr. Baldev Singh and Dr. P.N. Tandon for the presentation made by me. By the end Mr. Srinivasan was convinced of the genuineness of our proposals. My plea at that time was to get financial grant equal to G.B. Pant Hospital whose output was half of ours. It was a landmark victory as our grants immediately increased, a trend which continued in the future.
My next stint as Chief of Centre was between 1988-95. Finances were forthcoming in good measure We had a CT scan and state of art angiography equipment. Our ICU was the best in the country. What we lacked was a MRI Scanner. I must pay special thanks to Mr. R.L. Mishra who was the Union Health Secretary in the latter part of my assignment. We had an excellent relationship and he was always positive in his approach. It is through his help that we got the NMR department setup at AIIMS, which was far more than merely obtaining MRI equipment. Incidentally even today the NMR Department has the only 2 Tesla machine capable of MR Scan and also MR Spectroscopy. The NMR department also has chemical NMR and the only experimental NMR in India today. It was an unique experience to create a whole department with the help of the then director Dr. S. K. Kacker who was always supportive.
It is during my tenure that proposals were sent to the Government for making the Centre the best equipped not only in India but in the Asian region. The Gamma Knife has started after I retired and I am sure PET scan and other newer equipment would come in due course.
I am often asked as to whether I have any regrets. My special regret is our offices being removed from the main Institute. It was originally envisaged that offices would remain where they were located i.e., adjacent to Anatomy dissection hall. The translocation has severed the umbilical cord to the other specialties in the Institute. This isolation does not augur well for the future of our Centre, as any branch of medicine to flourish requires interaction with sister disciplines. My other regret is the inability to have nonclinical neurosciences to come and establish themselves in our Centers new building. I had tried, even to the extent of keeping a floor vacant for one year under various pretexts.
My greatest gains were the colleagues I had - friends for life. I know I left alive vibrant active Centre which will only grow from strength to strength. Even today for anything I always say Neurosciences Centre, AIIMS is the best and with every breath only wish it the very best in its future endeavors.”
The Centre for Integrative Medicine and Research is a pioneering initiative by AIIMS, New Delhi in the quest for convergence of contemporary medicine with India’s ancient and traditional medical practices. The centre at the premier institute of the country shall be dedicated to research, documentation and delivery of holistic healthcare. It has been envisioned as a “state of the art” research centre where top experts from various disciplines of contemporary medicine will collaborate with Yoga and Ayurveda specialists, both for disease treatment, and for preventive healthcare. The Centre for Integrative Medicine and Research was inaugurated on 22nd of June 2016 by Shri J.P Nadda, honourable Union Minister for Health and Family Welfare and president AIIMS, in the presence of Prof M.C. Mishra, director, AIIMS, New Delhi and Dr H.R. Nagendra, chancellor, Swami Vivekananda Yoga AnusandhanaSamsthana, Banglore.
Dr.SonaliJhanjee (nee Arora)
Professor
MD, DNB(Psychiatry)
Certificate in Global tobacco Control from Institute of Global tobacco control, Johns Hopkins Bloomberg School of Public Health (JHSPH), Baltimore, USA.
sonalijhanjee[at]gmail[dot]com
Interventional (both pharmacological and psychosocial) research in tobacco cessation, Teaching/Training/Capacity building for treatment of nicotine dependence and substance abuse treatment,Yoga and meditation in stress reduction and treatment of drug abuse, Opioid substitution treatment, community based treatment of drug use
Total number of publications till date 65
Details of publications since 2004 onwards (the full citation)- these should be divided into journal articles (peer reviewed publications) and books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications)
1.Rolling out of Opioid Substitution Treatment (OST) in Tihar prisons, India-A collaborative project of AIIMS,UNODC-ROSA & TIHAR PRISONS.(PI) Funded by UNODC ROSA)(2008-12)
2.Community based brief intervention vs simple advice for women tobacco users.(PI) Funded by ICMR 2013-14
1. Efficacy of Varenicline for smokeless tobacco use.Funded by National Institute of Health(NIH), U.S.A 2011- 13
2.Cognitive Behavioural based Intervention in Group Setting for Tobacco Cessation in tertiary de-addiction center in Northern India. Funded by ICMR,2015-2016
3.Impact of a package of intensive smoking-cessation interventions versus basic smoking-cessation advice on outcomes in smear-positive patients with pulmonary tuberculosis. Funded by EU FP7 Programme & ICMR (2009- 16)
4. Oral substitution with buprenorphine Co-I Funded by UNODC- ROSA(2007-2008)
5. Developing a network of De-addiction services from the government, NGO and private sector. (funded by WHO,2011)
- as guide (number only) 4
-as co-guide (number only) 10
1. Part of the SRNT Global Curriculum Review Board
2. Resource person for WHO-ERS “Train the trainer” tobacco cessation workshop in Dhaka, Bangladesh on 8th-9th January,2017
3.Part of an Roundtable discussion in 2014 held under National Tobacco Control Programme to discuss the current evidence around the existing and potential impact Of Electronic Nicotine Delivery Systems (ENDS) on public health and discuss regulation of e-cigarettes under existing legislative framework
4. Expert Groups
◦Finalizing course modules on “Tobacco Quit Line Services” under MOH&FW,2016
◦Finalizing modules of the project “mHealth for Tobacco Cessation” under MOH&FW, 2015
◦Meeting dealing with ‘Development of Training module / Strategy’ under NTCP, MOH&FW
5.Part of ICMR task force on proposal for ICMR-funded task force project on epidemiology of substance abuse in the state of Punjab (esasp)(2013-14)
6. Part of an expert team convened by UNODC (United Nations Office of Drugs and Crime, Regional Office for South Asia, New Delhi) to evaluate oral substitution(with buprenorphine) sites in India in 2007.
7. As desired by Standing Parliamentary committee on demand for grants, was part of AIIMS team to carry out site visits to Ministry Of Health funded drug deaddiction centres for evaluation of number of cases in treatment and outcome following treatment in 2008.
| 1 | Dr. Avinash Kanodia | DM | 2001-2004 |
| 2 | Dr. Ashwani Sharma | DM | 2002-2005 |
| 3 | Dr. Jasmeet Singh | DM | 2002-2005 |
| 4 | Dr. T. Rizvi | DM | 2002-2005 |
| 5 | Dr. Ajit Singh Puri | DM | 2004-2007 |
| 6 | Dr. Edmond Moses | DM | 2006-2009 |
| 7 | Dr. Subhash Kumar | DM | 2007-2010 |
| 8 | Dr. Sandeep Sharma | DM | 2007-2010 |
| 9 | Dr. Leve Joseph | DM | 2010-2012 |
| 10 | Dr. Vishal Goyal | DM | 2010-2013 |
| 11 | Dr. Ravi Chetan | DM | 2011-2014 |
| 12 | Dr. Himanshu Agarwal | DM | 2012-2015 |
| 13 | Dr. Anshul Jain | DM | 2013-2016 |
| 14 | Dr. Kavita Vani | DM | 2013-2016 |
| 15 | Dr. Nishchint Jain | DM | 2014-2017 |
| 16 | Dr. Somerender Singh | DM | 2015-2017 |
| 17 | Dr. Partiban B | DM | 2016-2018 |
| 18 | Dr. Subhash Phuyal | DM | 2016-2018 |
| 19 | Dr.Madan Mohan Gupta | DM | 2016-2018 |
| 20 | Dr. Jeysellan | DM | 2016-2018 |
| 21 | Dr. PUneeth K.T. | DM | 2017-2019 |
| 22 | Dr. Nishant Mishra | DM | 2018-2020 |
| 23 | Dr. Sushant Agarwal | DM | 2018-2020 |
| 24 | Dr. Kalyan Sarma | DM | 2018-2020 |
| 25 | Dr. Manoj Nayak | DM | 2019-2021 |
Prof. P.N. Tandon (1965-1990) presently Emeritus Professor Neurosurgery
“The Departments of Neurology and Neurosurgery at the All India Institute of Medical Sciences were initiated in March 1965 with the appointment of Prof. Baldev Singh and myself as the first Professors. A neurology service in the Department of Medicine started by Dr. Jim Austin from the USA and later under care of Dr. Vimla Virmani was already in existence at that time. Significantly enough the Institute was, from its very inception, an important centre of neuroscience research. The first two Professors in Department of Physiology (Prof. B.K. Anand and Prof. A.S. Paintal) were undisputable leaders of neurophysiology in the country. Dr. Paintal had, however, already moved to Patel Chest Institute a year earlier, the remaining faculty members of the department were all pursuing neurophysiology research. Prof. Keswani, the Chief of Anatomy, was primarily interested in neuroanatomy. Prof. G. P. Talwar, at that stage, was enthusiastically involved in researches in neurochemistry This was of course before his shift to immunology. Acknowledging these strengths International Brain Research Organization (IBRO) had already held one of its earlier workshops in the Institute. Dr. Sriramachari, Deputy Director of Indian Council of Medical Research, though not on the faculty of the Institute freely provided his services for all neuropathological work till several years later when Dr. Subimal Roy took over the responsibility fully. While clinical neurology and neurosurgery departments existed at several centers in the country much earlier; even the oldest such centers at Vellore, Madras, Bombay and Calcutta, did not have such broad base of neuroscience as we were fortunate to have at the Institute. Given the overall milieu of rapid growth and development in the institute at that time, the clinical departments also expanded rapidly. It will be hard for the current staff and students of the Institute to visualize how close interaction existed among all these departments and units in the earlier years. This was in no small measure due to the all pervading influence of Prof. Baldev Singh real father figure for all of us.
The idea of establishing a "Brain Research Centre" at the Institute had already been envisaged by Prof. B.K. Anand even before the clinical departments came into existence. No doubt this was primarily thought of as a basic research centre. Thus on 1st December 1964, Dr. Anand vide his letter No. Phy/64/1235 requested the Director for initiating steps for developing a Brain Research Centre" with the existing ICMR Neurophysiology unit as its nucleus. Unfortunately no action was taken on his request.
In 1968, when the Institute was to formulate its development plans for the Fourth Five Year plan of the Government, Prof. Anand, Prof. Baldev Singh and I had several informal discussions to once again revive the proposal for a Brain Research Centre. It may be mentioned that, not surprisingly, this proposal was heavily loaded in favour of creating research laboratories including a couple for neurology and neurosurgery. While we were heavily constrained in our clinical work due to limited diagnostic and operative facilities at this time we went along with Prof. Anand in supporting this proposal hoping to strengthen the patient care services through the development plan for the Institute hospital which was to be commissioned
The Development Committee approved the proposal in principle, but owing to financial constraints no concrete steps were taken. The Institute Body ultimately agreed to create a few staff positions so that "Centre can make a start as early as the Financial Year 1970/71. In practical terms it amounted to absorbing some of the staff of the Indian Council of Medical Research Neurophysiology Unit and nothing more.
When we finally shifted to the new hospital the Neurosurgery Department had 22 beds allotted to it. We had one operation theatre, but no specialized neurosurgical operation table and no intensive care unit. The neuroradiology set up consisted of a skull table without automatic changer for angiography, no facilities for tomography nor a dedicated unit for myelography. Isotope encephalometry then a routine diagnostic investigation abroad was nonexistent. We had an EEG machine but no facilities for EMG or nerve conduction. Nonetheless we were facing increasing demands for patient care from all over the country and also our neighboring countries. Waiting lists for admission and surgery were a constant source of worry for us and frustration for the suffering patients. We had already started the M. Ch. course.
Similar problems were being faced by the Cardiology and Cardiothoracic Surgery Departments. One day in 1971 when Prof. Gopinath and I were scrubbing for surgery in the common scrub room between our two theatres, he informed me that they have submitted a proposal for a Cardiothoracic Centre "Why don't you also do so, otherwise we will never progress". I, therefore, once again took up this matter with Prof. Anand who was now also the Dean and sounded the Director, Prof. V. Ramalingaswami. On receiving a favorable response, it was decided that, unlike in the past, our proposal this time should be a comprehensive one, including parallel development of basic neurosciences and clinical disciplines. Dr. Manchanda along with Prof. Anand formulated the proposal in respect to basic neurosciences. I, in consultation with Prof. Sumedha Pathak, the then Professor and Head of Department of Neurology and on the advice of Prof. Baldev Singh and Dr. Banerji prepared the plan for the clinical centre. A draft proposal was thus submitted on 16`" July 1971 to the Dean with the comments "in view of the present extent of development at the Institute to start with emphasis will be on neurophysiology, neurology and neurosurgery. Nucleus for the following will be established with a view to development of these into fully fledged specialties, as integral part of the centre, as personnel and fiscal resources were available". These included neuroanatomy, neurochemistry, neuropathology. This proposal was discussed by Prof. Baldev Singh (who was now an Emeritus Professor) with Prof. B.K. Anand who agreed with it fully and desired to "go ahead and fill up all the details regarding space, equipment, personnel etc. working out the cost" etc. We agreed to change the name from Brain Research Centre to Neurosciences Centre. We had a detailed and somewhat ambitious plan formulated. Though the plans were ready there was no obvious source for funding it. Was it going to be another document for the archives? This thought remained a constant worry, Prof. Ramalingaswami was fully in agreement but was finding it difficult to find funds for it.
Several months passed. One day while casually discussing our mounting frustrations with lack of any progress with my elder brother, who was then a Jt. Secretary in the Prime Minister's office, I initially got a cautious reply, "Prakash, officially I do not wish to get involved in any thing that may be considered as a favour to my brother. The only thing I can do is to arrange a meeting for you with the PS to the Hon'ble Minister of Health Shri Uma Shanker Dixit. Even before that, first take the permission from your Director to do so". It was easy to obtain Director's permission and shortly afterwards a meeting was held with Shri Rajgopal, who was more than sympathetic to our request for establishing the Neurosciences Centre. At the end of the meeting he told me that it was not possible to get such a major scheme funded in the middle of a plan period but "may be we could get advanced action initiated which can then be formalized in the next plan". He promised to discuss this with Dixitji at an appropriate time. The meeting ended with encouraging but cautious note, "I promise nothing but I am convinced it is a genuine need. You are asking nothing for yourself? you are willing to provide more and better service to those knocking at your door".
Not expecting any prompt action I was pleasantly surprised to receive a call from the Director later that evening, "Health Secretary Shri K.K. Dass wants us to include the matter related to the establishment of the Neurosciences Centre in the agenda for the next meeting of the Institute Body due shortly. He wants a copy of the proposal sent to him in advance". On 2nd August 1972, a copy of the formal proposal was duly sent to the Shri K.K. Dass by the Director. At the Institute Body meeting held on 12'" September 1972, the Institute decided, "The Institute considered that it was fortunate that expertise in several fields of Neurosciences exists at the institute both in basic and clinical areas. The Institute considered the scheme put up for its consideration as possible, desirable and in the larger interests of the country. Recognizing the strengths already built in the various departments in respect of the neurosciences, the Institute approved the proposal in principle to set up a Centre for Neurological Sciences at the AIIMS and decided that not only it be included in the proposals for the Fifth Five year Plan of the AIIMS but, the possibility of advance action in the Fourth Five Year Plan itself, should also be seriously explored. It was accordingly decided that the matter be considered by the Finance Committee in greater detail". We felt happy but not jubilant, fully conscious of the harder battles ahead
The Proposal was duly put up to the Finance Committee meetings held on 4th January 1973, 8th February 1973 and 5th April 1973 and as feared owing to "financial constraints" no funds could be made available. The real reason was no doubt that Shri K.K. Dass had retired by now and his successor Shri Ramachandran had his own antipathies against the Institute as future events confirmed.
However, without waiting for a formal decision of the Finance Committee, Prof. Ramalingaswami forwarded the proposal to Dr. Banwari Lall, Chief, Health Division, Planning Commission for his consideration. Dr. Lail was a close friend of Prof. Anand who arranged a meeting with him in the Planning Commission after Dr. Lall had opportunity to scrutinize the proposal. With high hopes Prof. Anand and I attended the meeting. To our surprise Dr. Lall, after a brief discussion, said, "Bal (B.K. Anand), I am sorry this proposal as it stands is unlikely to be approved owing to severe financial constraints. The only component that may be favorably looked at is the patient care part". He also made several suggestions for curtailing the budgetary demands even for the clinical component. It was with a sense of disappointment that we walked out of his office. I was, in addition assailed with the fear of losing Prof. Anand's interest and support for the project. Probably sensing my thoughts, on our way to the exit he suddenly stopped said, "Prakash, it is too bad to have things take a turn this way, but let us be practical. We should take whatever we can get and keep trying for the rest. You will have my full support". Few in his place could have been so generous and even more so the enthusiastic support we continued to get from him later on provided enough proof of the genuineness of these sentiments. For all this he no doubt, got the flak of his colleagues in the Physiology Department.
In pursuance of the decision of the Institute Body and the informal advice received from Dr. Lall we carried out another detailed exercise to draft a formal EFC (Expenditure Finance Committee) memo. In the meanwhile Prof. Gopinath had carried out a similar exercise for the Cardio-thoracic Centre. As a matter of fact, these exercises were mostly done with the constant consultations with each other. Combined these two proposals required considerable financial support. Dr. Ramalingaswami advised us that we should seek the views of the new Health Minister Shri Khadilkar. After a patient hearing of our individual proposals, he pointed out the difficult financial situation and advised that we should try and economize by establishing some common facilities and sharing whatever can be shared thus bringing down the total cost of two proposals. He promised to get the demands included in the Fifth Five Year Plan proposals of the Institute. Thus Prof. Gopinath and I carried out another exercise maintaining the basic character of two independent centers, yet having some common areas and support laboratories. On 2nd August 1973, a new draft proposal was forwarded to the Director with a note, "In view of the difficult economics situation, we (Profs. Anand, Gopinath and Tandon) have also reviewed the projects with an idea to prune these without undue detriment to the utility of the projects". And further, "Following this review, if we could get a total of Rs. 350 lakhs (Rs. 200 lakhs for Cardiothoracic and Rs. 150 lacs for Neurosciences Centre), we could still make a worthwhile contribution".
The Planning Commission, discussed the proposals of the Health Ministry (which included those of AIIMS) on 31st August 1973. The bias of the Health Secretary, Shri Ramachandran against the institute was too obvious. He had proposed a total of Rs. 150 lakhs for the whole Institute. As a matter of fact it was specially emphasized that the Ministry "did not favor that all the specialties should be concentrated in one place in the country". Following strong pleadings by the Director, one of the members of the Planning Commission, Member (M), pointed out that "the Ministry had proposed Rs. 1.50 crores for the AlIMS as against the Fourth Plan provision of Rs. 3.33 crores, and since this was a premier Institute in the country, the Ministry may explore the possibility of providing some additional funds for the Fifth Five Year Plan. With regards to the proposals for the two centers, the Planning Commission ultimately decided to allocate separate funds for "the development of super-specialties: a total of 236 lakhs, without specifically mentioning our proposals. This was a typical bureaucratic stroke by the Health Secretary to scuttle our proposal. Before implementing the program, the Ministry of Health decided to enquire from all medical institutions in the country to submit their proposals for "development of super-specialties", notwithstanding the fact that the Central Government is supposed to directly fund only the national institutes. As expected proposals were received from several places and interestingly even Orthopaedics was considered a super-specialty. The Health Ministry, obviously under the instructions from its Secretary put the whole matter in the cold storage with the usual excuse, "the matter is under consideration": even though the Fifth Plan had already begun from April 1974.
One day Dr. Karan Singh, who was now the Minister of Health, desired to see me for some unconnected reason. At the end of our meeting, I enquired about our proposals for the centers. Only then the cat came out of the bag. He frankly informed me that the Secretary was sitting on the file on the excuse of collecting information mentioned above. Dr. Karan Singh recognized the futility of the exercise. Since in the limited funds allocated for super specialities it would be impossible to meet the needs of even a few. He promptly took the initiative and in August 1974 appointed a committee under the Chairmanship of Dr. Srivastava, the Director General Health Services, to assess the existing potentials and future possibilities of strengthening superspecialities in the centrally funded institutions only. The Committee included experts in the concerned disciplines from all over the country. It collected the necessary information from various institutions and finally paid site-visits to each of these before recommending our two proposals alongwith some allocations to a couple of others. Thus from a total of Rs. 236 lacs allocation for super specialities the two Centres at the AIIMS, was provided Rs. 188.37 lacs.
On March 26, 1975, even before we received a formal approval of the Government to establish the Centre, a letter addressed to the Director, AlIMS received from Dr. Sharad Kumar, DDG(M), indicating that, "Under the Purely Central Scheme of "Development of Superspecialities', the Government of India has sanctioned a provision of Rs. 10 lakhs for the development of the Departments of (1) Neurosurgery and Neurology; and (2) Cardiology and Cardiothoracic Surgery...............”
This communication, though not mentioning anything about the Centers, was the first indication that the Government had selected AIIMS; for development of these super-specialties. Two weeks later on 11th April 1975, the recommendations of the "Expert Committee on Establishment of Cardiothoracic and Neurosciences Centre at the Institute", were ultimately received, setting at rest all uncertainties about the two proposals. It would be worth reproducing the extracts of this communication with respect to Neurosciences Centre (see Dr. Sharad Kumar's letter dated 11th April 1975). Shortly afterwards on 22"d July 1975 a formal letter from the Ministry of Health and F.W. No. V. 16020/54/ME (PG), communicated to the Institute an allocation of Rs. 188.37 lacs for the super-specialties (including both centers) for the 5th Five Year Plan. It needs to be recorded that the fullest understanding between Prof. Gopinath and myself and the cooperation of the rest of the faculty of the concerned departments made it possible for us to keep on revising and redrafting the proposals as per the bureaucratic needs of the Government, without sacrificing the basic objectives. No hidden rivalries, personal egos or unjustified interests of individuals ever cast any shadow as we pursued the planning and implementation of the projects through various administrative channels. For me it was a rare experience of trust and camaraderie not so common in our institutions.
As expected it was not smooth sailing from now onwards. We had to wait till March 1976 for the first release of funds, a paltry sum of Rs. 3 lacs. At one stage the Financial Advisor to Ministry of Health, whose main grudge against the Institute happened to be "misuse of funds for erecting black marble columns in the foyer" without any justification reduced the total allocation for the Fifth Plan by nearly Rs. 40 lacs, probably worrying that we would waste it on black marble columns. When no explanation and assurances from Dr. Gopinath and myself failed to convince him, we had to approach the office of the Finance Minister (Shri C. Subrramanayam) and the Planning Commission Deputy Chairman Shri P.N. Haksar, two of the most progressive policy makers of the country has known. Let me hasten to add that Prof. Gopinath and I approached them with the approval of our Director.
In July 1976, the Estate Committee formally appointed M/s. Pradhan Ghosh and Associates as the architects. However, between 1976 and 1978 repeated revisions of the building plan were required due to pruning of the budget allocations and rising cost of the building. At last on 14th April 1978, the President of India Shri Neelam Sanjiva Reddy laid the foundation stone of the twin centers. In his welcome address Dr. Ramalingaswami stated, "Our vision of the Centers is that they will be Centers both of public service and of higher learning at the same time". Their philosophy is that in which the patients and their needs come first, everything else is subordinate and subservient to this: He pointed out that, "The greatest and deepest need of a Centre is to be needed by Society". Quoting the famous economist Francis Delaisi, he said that. "the purpose of an Institution is to supply stability needed for long term operations. At the same time, Institutions must be able to adjust to change. It is our hope that stability, adjustability and continuity will mix in the centers in appropriate balance". Rashtrapatiji in his address expressed his happiness on the establishment of these Centers. While emphasizing that, "Our most urgent need is Primary Health Care" which should be pursued with all energy and resources at our command." He pointed out that, "we cannot altogether neglect the setting up and improvement of more advanced levels of health care at District, State and national levels. We need to have a few Centers of excellence in a large country like ours where the most advanced levels of care can be provided; specialists and researchers can be trained and the most complex problems may be referred for appropriate management" For him, "It is not a question of this or that" but a "proper balance in the developments of these various levels of health care". He was equally concerned about the scientific community which must be able to discover, adopt and innovate suitable methods not only in dealing with our current problems but also in coping with changing trends and changing needs of the future". I have quoted these excerpts from the speeches because I believe that as long as we pursue these ideals the Centre would continue to justify the generous resources provided by the government and enjoy the trust of the people.
Five years later, in March 1983, out patient clinics for Neurology, Neurosurgery (as also Cardiology and Cardiothoracic Surgery) moved to the new building, while the work continued to complete the rest. Progressively as the work progressed we continued to occupy the areas already completed. By July 1984, the built up area included basement, OPD, receiving station, noninvasive laboratories, radiology wing, 8 operation theatres (Neuro 3, Cardiac 4, Common 1) along with ICUs and postoperative wards. It was only in 1988-89 that the Centres became fully functional in their new abode. At this time Neurosciences centre had a total of 180 beds, 3 fully equipped operation theatres, 30 bedded ICUs, Intermediate care wards, fully fledged departments of Neuroradiology, Neuroanaesthesia, within this complex. The offices of the faculty and supportive staff, Neurochemistry laboratories continued to remain in the old building and by mutual agreement the Neuropathology still continues to be in parent Department of Pathology. This may be compared to the facilities available to us before we moved to the Centre. The combined strength of beds for Neurology and Neurosurgery including a half baked ICU was only 72, scattered in different parts of the old hospital.
There was only one dedicated operation theatre for neurosurgery and we shared another one with Cardiothoracic Department three days a week. There were four members on the faculty of Neurosurgery. I have been informed that there will be separate write-up's about the development of Neurology, Neuroradiology, Neuroanaesthesia, Neuropathology, Neurochemistry etc. hence I shall restrict myself in the remaining part of this review on Neurosurgery only. Nonetheless it should be mentioned that once the scheme for creating the Centre was approved, in the interval before its complete occupation we were permitted to augment the overall facilities and staff strength in a progressive manner with a view to improve the quality and maximise output of all our activities-patient care service and education in particular. Funds for research had, as even now, to be obtained on competitive basis from the grant giving agencies. During this interval we were able to obtain a munificent grant from the Swedish International Development Agency (SIDA) which modernized our diagnostic and clinical facilities including those for operation theatres and ICU. The first CT Scan in the country was installed under this grant. It was not just a coincidence that this was inaugurated by the President of India on the same day as the foundation of the Centre(s) was laid.
Coming back to the growth of neurosurgical services, in the first full year of our work i.e. 1966 we admitted 140 patients, attended to 540 in the OPD and performed 111 major and 89 minor surgical procedures. It may be mentioned that at that time many of our patients were admitted, operated upon and discharged from the emergency ward. Five years later in 1971 these numbers were 422 admitted, 1044 attended in OPD and 535 (303 major and 232 minor operations performed. In 1976, the year when the first token grant was received for the Centre we admitted 1094 patients, attended to 3784 (1960 new and 1824 old) patients in the OPD, and performed 520 major and 785 minor surgical operations. It may be recalled that at that time neuroradiological investigations pneumoencephalography ventriculography, angiography and myelography were performed by. the clinical team and hence were included as minor operations. In 1986, prior to shifting to the Centre 1898 patients were admitted, 11.225 (3406 new and 7918 old) patients seen in the OPD and 735 and 257 major or minor operations were performed. Starting with only two faculty members in 1965 - Dr. Banerji and myself, it was only in 1971 that we added one more lecturer. Dr B. Prakash. The next person to join was Dr R. Bhatia as Lecturer in 1974 The first faculty position in the Department of Neurosurgery after the Centre came into existence, was 1979 with Dr. Banerji taking over as a Professor. A little known episode in this connection needs mention to illustrate the prevailing team spirit at that time. When we got the first position of a Professor sanctioned for the Centre, I had in my mind wanted it for Dr. Banerji. The day the matter was to be finalized in the Academic Committee I was indisposed and requested Dr. Banerji to attend the meeting and briefed him about my plan. His immediate response was that it should be alloted to Neuropathology, "Dr. Subimal Roy should be given a chance before me". Dr. V.S. Mehta then joined as a Lecturer in 1981 followed by Dr. A.K. Mahapatra in 1983. In the meanwhile Dr. B. Prakash left for G.B. Pant Hospital in 1980. Thus even after fully commissioning the Centre in 1988, the Department had a total strength of 5 faculty members; who continued to share the ever increasing service load as indicated by the figures provided above.
Education
Besides the full fledged in-service M.Ch. course (3 years for post MS (surgery) and a direct 5+1 year after MBBS), the department has been participating in undergraduate education as well as collaborating with basic science department for Ph.D. program. From 1968 when our first trainee obtained his M.Ch. degree, till 1988, twenty eight persons obtained their postgraduate degrees. Since 1988 up to date an additional 31 have qualified. Most of these are serving the country. Several of them became chiefs of their departments at Delhi, Varanasi, Srinagar, Bangalore, Cuttack and Hyderabad, thus fulfilling an important objective for which the Centre was created. From its inception the Department has been actively engaged in CME programs both intramural and extramural. Short-term training programs are organized regularly on recent advances like CT scanning, Microsurgery, Neural Transplantation, Vascular Surgery, Skull base surgery etc. An yearly course on Neurobiology for Clinicians was organized (4 at the AIIMS and 1 at NIMHANS, Bangalore). National level Hands-on Workshops were organized from time to time with the help of international faculty as for example on microneurosurgery, skull-base surgery, neural transplantation etc. A microneurosurgical laboratory, the first of its kind in the country, was established for training in microsurgical techniques, not only for neurosurgeons but for others specialities also from all over the country. The first National Neural Transplantation Facility was established in collaboration with the Department of Anatomy. The first Text Book of Neurosurgery in the country was the result of a joint effort between Madras Neurological Institute and AlIMS in 1980. This has been completely revised and updated in 1996. Four monographs "Lectures in neurobiology" were brought out in collaboration with the Department of Anatomy, AIIMS. The faculty has made contributions to several national and international text books including Tropical Neurology, Handbook of Neurology and Techniques in Neurosurgery.
Research
AlIMS provided a unique milieu for advancing frontiers of knowledge. The Neurosurgery Department fully participated in this effort The major areas of research contributions of the Department involved collaboration of other departments in the Institute and outside included;
1. Head Injury: epidemiology, intracranial hematomas and temporal lobe lesions, brainstem injuries, growing skull factures, outcome of severe head injury. Those studies included a collaborative investigation with Institute of Neurology, Madras and another with University of Charllotesville, Virginia, USA. With in the Institute departments of ENT, Ophthalmology, Pathology, Radiology and Medical Jurisprudence were parts of the investigations at various stages.
2. CNS Tuberculosis experimental studies on pathogenesis, clinical manifestations, etiology and management of post meningitic sequelae, neuroimaging. evaluation of therapeutic modalities (These studies were carried out in collaboration with the Departments of Microbiology, Pathology and Radiology and Nuclear Medicine).
3. Brain Abscesses: Etiopathology, clinical manifestations, brain abscess in cyanotic heart disease, subdural abscesses, management strategies.
4. Cysticercosis: its clinical manifestations, diagnostic dilemmas, CT imaging, role of surgery.
5. Brachial Plexus injuries: a series of investigations as one of the largest in the world, included problems of diagnosis, evaluation of surgical procedures. These studies have been carried out in collaboration with Department of Neurology.
6. Optic nerve injuries are a subject of prospective investigations for more than a decade. Clinical manifestations, visual evoked potentials, role of surgery have been evaluated in collaboration with the department of ENT and as a part of an international multicentric study.
7 Subarachnoid hemorrhage and Intracranial aneurysms specially epidemiological, etiopathological investigations and studies to evaluate various management strategies. The initiation of these studies was done as a part of a multicentric national study which proved the fallacy of the prevailing view of rarity of intracranial aneurysms in India
8. Pituitary Tumours: Immunohistochemical classification, correlation of clinical-pathological and hormonal profile, tissue culture studies (These studies were carried out in collaboration with the Departments of Endocrinology and Neuropathology). Most of these studies were initiated after Trans sphenoid surgery had been established, for the first time in India, in collaboration with ENT department.
9. Gliomas: were a subject of a series of investigations on pathology, classification, evaluation of growth potentials, prognostic factors etc. Surgery for gliomas of the dominant hemisphere constituted a major thrust. A large number of investigations including EM, immunohistochemistry, in-vivo and in in-vitro labeling index studies, tissue culture and molecular markers have been carried out by the neuropathology department.
10. Experimental studies on intracranial hypertension elaborated the patho-physiological mechanisms based on a biomechanical model. These studies were carried out in collaboration with the Department of Physiology at AlIMS and Biomedical Engineering at Indian Institute of Technology, Delhi. In another series of investigations with the Department of Pharmacology the pathogenetic mechanism of pulmonary oedema in raised ICP was elaborated.
11. Experimental neural Transplantation: A national fetal Neural Transplantation Unit (supported by Department of Science and technology) was established in collaboration with the Department of Anatomy. A number of original contributions were made through a series of papers.
The above account will testify that much has been accomplished, no doubt a lot more needs to be. For me personally it has been a rewarding experience and source of great satisfaction, not just the physical growth of the Centre but the years of affection and friendship of the team who really made this happen. The only regret that continues to haunt me is our failure to see a parallel growth of the basic neurosciences as an integral part of the Neurosciences Centre. Individually these disciplines in the Institute have made very outstanding contributions. It has been stated that an institution is the lengthened shadow of an individual. If there is one example to disprove this adage, the Neurosciences Centre is one. It was born in the dreams of several, nurtured with the selfless, dedicated services of many who submerged their egoes for a cause greater than themselves, working as a team the parallel of which could hardly be found any where. In the true spirit of Gita, their sole concern was duty and not the reward. No sacrifice was great enough for establishing a centre of excellence. Posterity will judge whether they succeeded on not but no one would deny that they attempted. Unlike many other such centres in our country, even after the departure of those who initiated it, the Centre continues its journey to greater heights as will be obvious from the story told by those who succeeded. I hope and pray that the Centre will continue to live up to the foundation stone. "In the ultimate analysis, it is not the budget, nor the number of staff positions that makes a truly great centre of public service and higher learning. It is the presence of thoughtful, imaginative, humanistic, loyal and devoted faculty and students that is vital". The Centre continues to be endowed with them and I can only wish them greater heights in years ahead.
Recommendations of The Committee on Establishment of Neurology and Neurosurgery Centre at the AIIMS and Safdarjang Complex
This Centre has been chosen for the following reasons :
i) The excellent staff that are in position and the very good record of patient care, teaching and research, particularly at the AlIMS.
ii) The existence of the supporting departments of basic sciences which are fully equipped and which can provide initially the nucleus for each ancillary department of the proposed Neurosciences Centre.
iii) The proximity of the department of Neurology at the Safdarjang Hospital which can serve as a trauma and emergency unit for this proposed centre.
The needs of this proposed Neuro-centre are indicated in Appendix I and may be seen to be economical and the minimum required.
This recommendation to make the neurology complex of the AlIMS and Safdarjang Hospital into a Neuro Centre is based on the following requirements.
a) Enthusiastic cooperation from the Departments of Anatomy, Physiology, Biochemistry, Pathology, Microbiology, Endocrinology, Genetics, Immunology and Experimental Medicine and Surgery of the AlIMS and their capacity to provide the necessary staff and equipment to develop these special aspects like neuro-anatomy, neuro-physiology, neuro-pathology, neuro-chemistry etc. that is, a pooling of the resources already available. As this Neuro-centre develops and the national resources improve, each one of these sub-specialities may develop its section in a new building to be constructed.
b) Expansion of the bed strength facilities will need space not available in the present building. A piece of land has already been earmarked to build a Neurocentre which has to be taken up on a priority basis.
c) Till such times as the building is ready, the rest of the recommendations may be given effect to immediately.
Neurology and Neurosurgery Centre cont.
The Committee has further observed that
1. Minimum arrangements have to be made to coordinate the emergency and head injury service of the Safdarjung Hospital with the Neuro-centre by:
a) according mutual and appropriate designations for the staff of each institution in the other; and
b) arranging full clinical coverage of these beds by the combined staff of the Neuro-Centre and delineating mutual responsibilities.
2. The Neuro-radiological facilities already available in the Safdarjung Hospital, including one Mimer X-ray machine, must be made available for this Neuro-Centre immediately, alongwith early sanction of the recommended neuro radiology staff.
3. Experienced Neuro-pathologists being very few in the country, the Committee strongly recommends the immediate appointment of Dr. S. Sriramachari, Director, Registry of Pathology, New Delhi, as the Hony. Professor of Neuro pathology in this Neuro-centre.
4. The various sub-sections collaborating from the parent departments in the AlIMS should. in course of time, become full-fledged departments of the sub-speciality - e.g. neuro-pathology, neuro-radiology, neuro-physiology, neuro-chemistry, neuro-psychology etc.”
E-mail: sonalijhanjee[at]gmail[dot]com
Certificate in Global tobacco Control from Institute of Global tobacco control, Johns Hopkins Bloomberg School of Public Health (JHSPH), Baltimore, USA.
Interventional (both pharmacological and psychosocial) research in tobacco cessation, Teaching/Training/Capacity building for treatment of nicotine dependence and substance abuse treatment,Yoga and meditation in stress reduction and treatment of drug abuse, Opioid substitution treatment, community based treatment of drug use
Total number of publications till date 65
Details of publications since 2004 onwards (the full citation)- these should be divided into journal articles (peer reviewed publications) and books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications)
1.Rolling out of Opioid Substitution Treatment (OST) in Tihar prisons, India-A collaborative project of AIIMS,UNODC-ROSA & TIHAR PRISONS.(PI) Funded by UNODC ROSA)(2008-12)
2.Community based brief intervention vs simple advice for women tobacco users.(PI) Funded by ICMR 2013-14
Name- Anju Dhawan

3. Designation- Professor, National Drug Dependence Treatment Centre (NDDTC)
4. Qualifications- MBBS, MD Psychiatry
5. Email ID- dranjudhawan[at]gmail[dot]com
6. Field of Interest- Adolescent Substance Use, Meditation Research
7. Total number of publications till date- 144
8. Details of publications since 2010 onwards (the full citation)- these should be divided into journal articles (peer reviewed publications) and books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications)
10. Investigator/ Co-investigator in funded projects along with year completed/ongoing
| Projects as Chief Investigator | Source of funding | Year |
|---|---|---|
| Psychotropic substance abuse | United Nations Drug Control Programme, Regional Office for South Asia (UNDCP ROSA) | 2001-02 |
| Evaluation of functioning of de-addiction centres in the country | WHO (India) | 2001-2002 |
| Opioid Substitution Treatment with Buprenorphine | United Nations Office on Drugs and Crime, Regional Office for South Asia (UNODC-ROSA) | 2006-2009 |
| Assessment of feasibility and effectiveness of Methadone Maintenance Treatment in India | UNODC (ROSA) | 2011-2013 |
| Effectiveness of Yoga in patients of Opioid Dependence | Central Council for Research in Yoga and Naturopathy, AYUSH, Ministry of Health and Family Welfare | 2009-2011 |
| Assessment of pattern, profile and correlates of substance use in children | NCPCR | 2012-2013 |
| Training of doctors on Substance Use Disorders | Department of Revenue, Ministry of Finance | 2010-15 |
| Mapping and Size Estimation of Street Children Who Use Drugs in Delhi | Department of Women and Child development, Delhi Govt | 2015-16 |
| Extent of Mental Health issues & Addictive Behavior among Adolescents seeking help in Adolescent Friendly Health Clinics in Delhi | Adolescent Health Division, Directorate of Family Welfare, Govt of NCT of Delhi | 2019-2020 |
| Survey on Substance use among School and College Students | Ministry of Social Justice and Empowerment, Government of India | 2019-20 |
| Screening and Intervention for Drug/Substance Use among Secondary School going Children | UEE Mission, Education Department Delhi | 2020-21 |
| A prospective double blind, randomized clinical study to evaluate the antibody response after Covid-19 vaccine when provided along with KabasuraKudineer, a siddha medicine | SSIAR | 2021-22 |
| A prospective double blind, randomized clinical study to evaluate the antibody response after Covid-19 vaccine when provided along with NOQ19, an Ayurvedic medicine | SSIAR | 2022 |
Research Projects as co-investigator-
| Projects as Co-Investigator | Source of funding | Year |
|---|---|---|
| Rapid Assessment Survey Project on Alcohol, Tobacco and other substances in Districts of Darjeeling, Kohima, Aizwal | WHO (India) | 1999 |
| Rapid Assessment Survey Project on Alcohol, Tobacco and other substances in Districts of North Goa, Jodhpur, Madras | WHO (India) | 2000 |
| Buprenorphine maintenance programme in Kohima district | WHO (India) | 2000 |
| Global study on illegal drug markets | UNDCP and UNICRI | 2000-2001 |
| A survey of prevalence of drug dependence and comorbidity in the general population of Thrissur | WHO (India) | 2001-2002 |
| Advance Statistical Analysis of National Survey Data using new methodologies without the addition of data | WHO (India) | 2001-2002 |
| To undertake a study to examine the relationship of tobacco as a gateway drug and to determine the prevalence of substance use behavioural disorders including tobacco in Metropolis Delhi | WHO (India) | 2002-2003 |
| Database on Drug Abuse and HIV/AIDS | UNODC (ROSA) | 2005-2009 |
| Assessment of drug use in out of School Adolescents | WHO (India) | 2008 |
| Development of intervention for drug use in out of school adolescents | WHO (India) | 2008-2009 |
| Coordination & convergence of Delhi District Health Services programmes & drug use intervention for the out of school children | WHO (India) | 2010-2011 |
| Developing a network of de-addiction services from the Government, NGO & Private sector | WHO (India) | 2010-2011 |
| Extent of internet use amongst adolescents with non-psychotic disorders: A case control study | AIIMS | 2016 |
| Validation of Teen Addiction Severity Index | AIIMS | 2016 |
| Screening and Intervention for Drug/Substance Use among Elementary School going Children | UEE Mission, Education Department Delhi | 2020-21 |
| A study to examine dependence, harm perception and motivation to quit amongst Indian areca nut users and pilot test an intervention module | WHO (India) | 2020-22 |
| Real World Effectiveness of add-on Yoga for patients with opioid dependence stabilized on treatment | DST SATYAM | 2022-23 |
| A study to examine psych-social and behavioral domains among school going adolescents during covid-19 pandemic: Mixed study design | ICMR | 2022-24 |
11. Investigator/Co-investigator in non-funded projects along with year and title completed/ongoing
Substance use among adolescents seeking treatment at NDDTC (2014-15)
Adult attention-deficit hyperactivity disorders and its correlates in patients with opioid dependence (2018-19)
Retrospective study to analyze the profile, the pattern of substance
use and outcome of treatment of adolescent patients who sought
treatment for opioid use (on-going)
To assess the effect of intervention of yoga and meditation-based structured programme for youth on the psychological functioning of medical students (on-going)
12. Thesis supervised for MD/ DM/PhD
- as guide (number only)- 8
-as co-guide (number only)-PhD thesis-8, MD and DM thesis-16
13. Awards and Honors
NATIONAL
INTERNATIONAL
Duration: Three (03) years Residency training programme in Neuroanaesthesiology and Critical Care
Eligibility A candidate must possess MD / DNB (Anaesthesia) degree of a University recognized by Medical Council of India. The entrance exams are conducted in December and May every year.
For further information contact Examination Cell, AIIMS
Procedure of selection
For this program the candidate is selected through 2 step competitive examination held at national level.
Step-I Written examination of multiple choice questions based on MD (Anaesthesia), Critical Care and Basic Neuroanaesthesia. The candidates are short listed for step-II.
Step-II There is a departmental interview where candidates are examined to evaluate their clinical acumen and aptitude.
Final selection of the candidate is made on the bases of combined evaluation of step-I, and II
The candidates selected work as Senior Resident (non-DM) in the department. They are supposed to do all clinical work of OR, ICUs, and emergency both independently and also under supervision.
Teaching Program
1. Seminar
2. Journal Club
3 Clinical Case Presentations
Rotational Policy
There is a compulsory rotational policy for clinical exposure of the candidates to various sub-specialities of Anaesthesia and Intensive Care apart from Neuroanaesthesia, Neurotrauma, and Neurocritical Care. It is the only sub-speciality of Anaesthesia at AIIMS, New Delhi where the Senior Residents are exposed to most of the sub-specilalities of Anaesthesia. During the three years tenure the candidates are rotated to Trauma Anaesthesia (General, Ortho, and Neurotrauma) and Plastic Surgery at JPNA Trauma Centre, Onco-anaesthesia at BRA IRCH, General Anaesthesia including Laparoscopy, Transplant Surgery, Paediatric, Gynaecologic, ENT, and Ophthalmologic Anaesthesia at RPC.
Guidelines for Short-Term/Long-Term Training/Visiting Fellow in respect of Indian and Foreign National candidates
Training will be provided to the candidates sponsored by the Government/Autonomous Bodies or Institutions/Public Health Sector Organizations / MCI approved medical colleges and Government / Defence Services. The short-term training may not be allowed to the private practitioners.
· Fee: - A fee of Rs.1, 000/- per month will be charged from the trainees (Indian citizens) and a fee of Indian Rupees equivalent to US $200 will be charged from the foreign nationals/citizens. However, the candidates sponsored by the Defence Services only will not be charged any fee.
· At a given time the number of long-term / short-term trainees in a particular department should not exceed 50% of the sanctioned strength of faculty of that department.
The short-term training may be provided to the foreign national candidates sponsored by the foreign Government / Autonomous Bodies / Medical Institutions duly recommended by the Dean or any other competent authority of the concerned College / University / Institution.
· A fee of US $ 200 per month will be charged from the foreign national candidates.
· There will be no financial obligations on the part of the Institute / Govt. of India.
· No accommodation etc. will be provided to the trainees.
· If the foreign nationals want hands on training, approval of MCI is necessary.
This training will be provided to the candidates sponsored by the Government of India / Semi-Government / Autonomous Bodies / Institutions / Public Sector Organizations / Public Defense Services only. The long-term training is not allowed to the private practitioners / NGOs.
The persons with postgraduate degree and working on regular basis will be given preference.
· Fee: - A fee of Rs.1,000/- per month will be charged from the trainees (Indian citizens) and a fee of Indian Rupees equivalent to US $200 will be charged from the foreign nationals/citizens. However, the candidates sponsored by the Defence Services only will not be charged any fee.
· At a given time the number of long-term/short-term trainees in a particular department should not exceed 50% of the sanctioned strength of faculty of that department.
· The foreign nationals / citizens trainees will be treated as Observers and not allowed hands on training without prior permission of the Medical Council of India. If the foreign national trainees want hands on training then the approval of the MCI is necessary.
The department of Neuroanaesthesiology and Critical Care at AIIMS is committed for advancement and promotion of Neuroanaesthesia and Neurocritical Care in India and abroad. The department regularly organizes a scientific event the “AIIMS Neuroanaesthesia Update”, every year starting from 2013. Eminent faculties of National and International repute along with AIIMS faculty participate in the meeting. It is a unique event where the anaesthetic procedures are telecasted live from the operation theatres and the delegates directly communicate with the anaesthesiologists and operating neurosurgeon as a part of the discussion. The department also started regular courses such as Cadaveric Hands-on Workshop on Airway Management and AIIMS Neurological Life Support (ANLS) with the target audience which includes emergency physicians, neurosurgeons, and neurologists apart from the anaesthesiologists. The department encourages faculty of national repute to deliver talks in the Neurosciences Centre based on recent neurosciences issues. The department also encourages faculty of International repute to be part of the departmental academic and research activities as a Visiting Professor.
For more details contact Dean / Registrar, Academic Section - II, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110 029, India
| S.No. | Publications | Year Published |
|---|---|---|
| 1 | Agarwal H, Sebastian LJD, Gaikwad SB, Ajay Garg, Nalini K Mishra: Vein of Galen aneurysmal malformation—clinical and angiographic spectrum with management perspective: an institutional experience J NeuroIntervent Surg 2016;0:1–6 | 2016 |
| 2 | Kakkar A, Baghmar S, Garg A, Suri V, Raina V, Sarkar C, Sharma MC. Recurrent rhabdoid meningioma with lymph node, pulmonary and bone metastases: A diagnostic and therapeutic challenge. Brain Tumor Pathol 2016, Feb 13. | 2016 |
| 3 | Malhotra V, Chandra SP, Dash D, Garg A, Tripathi M, Bal CS, Tripathi M. A screening tool to identify surgical candidates with drug refractory epilepsy in a resource limited settings. Epilepsy Res 2016, Mar;121:14-20. | 2016 |
| 4 | Vivek Shete , Amandeep Kumar, Leve Joseph Devarajan, Bhawani S. Sharma- Delayed appearance and rupture of a post-traumatic supraclinoid aneurysm in a 2-year-old child. Neurology India / January 2015/ Volume 63/ 112-114. | 2015 |
| 5 | Deepa Dash, Kameshwar Prasad, Leve Joseph: Cerebral venous thrombosis: An Indian perspective. Neurology India / May 2015/ Volume 63/ 318-328 | 2015 |
| 6 | Himanshu Agarwal, Leve Joseph Devarajan Sebastian, Shailesh B Gaikwad, Ajay Garg, And Nalini Kant Mishra: Spinal cord involvement and contrast enhancement in posterior reversible encephalopathy syndrome. BJR Case Rep 2015; 1: 20150326 | 2015 |
| 7 | Sahoo SS, Suri A, Bansal S, Devarajan SL, Sharma BS. Outcome of revascularization in moya-moya disease: Evaluation of a new angiographic scoring system. Asian J Neurosurg 2015;10:252‑9. | 2015 |
| 8 | Kurwale NS, Chandra SP, Chouksey P, Arora A, Garg A, Sarkar C, et al. Impact of intraoperative MRI on outcomes in epilepsy surgery: Preliminary experience of two years. Br J Neurosurg 2015, Jun;29(3):380-5. | 2015 |
| 9 | Kakkar A, Sable M, Suri V, Sarkar C, Garg A, Satyarthee GD, Sharma MC. Cerebellar liponeurocytoma, an unusual tumor of the central nervous system - ultrastructural examination. Ultrastruct Pathol 2015, Jun 24:1-5. | 2015 |
| 10 | Naik V, Ahmed FU, Gupta A, Garg A, Sarkar C, Sharma B, Mahapatra AK. Intracranial fungal granulomas: A single institutional clinicopathologic study of 66 patients and review of the literature. World Neurosurg 2015, Jun; 83(6): 1166-72. | 2015 |
| 11 | Kurwale NS, Chandra SP, Chouksey P, Arora A, Garg A, Sarkar C, et al. Impact of intraoperative MRI on outcomes in epilepsy surgery: Preliminary experience of two years. Br J Neurosurg 2015, Feb 7:1-6. | 2015 |
| 12 | Chandra PS, Kurwale N, Garg A, Dwivedi R, Malviya SV, Tripathi M. Endoscopy-Assisted interhemispheric transcallosal hemispherotomy: Preliminary description of a novel technique. Neurosurgery 2015, Feb 12. | 2015 |
| 13 | Chandra PS, Prabhu M, Goyal N, Garg A, Chauhan A, Sharma BS. Distraction, compression, extension, and reduction combined with joint remodeling and extra-articular distraction: Description of 2 new modifications for its application in basilar invagination and atlantoaxial dislocation: Prospective study in 79 cases. Neurosurgery 2015, Mar 19. | 2015 |
| 14 | Naik V, Ahmed FU, Gupta A, Garg A, Sarkar C, Sharma B, Mahapatra AK. Intracranial fungal granulomas: A single instituitional clinico-pathological study of 66 patients and review of literature. World Neurosurg 2015, Feb 17. | 2015 |
| 15 | Kumar A, Chandra PS, Sharma BS, Garg A, Rath GK, Bithal PK, Tripathi M. The role of neuronavigation-guided functional MRI and diffusion tensor tractography along with cortical stimulation in patients with eloquent cortex lesions. Br J Neurosurg 2014, Apr;28(2):226-33. | 2014 |
| 16 | Faruq M, Narang A, Kumari R, Pandey R, Garg A, Behari M, et al. Novel mutations in typical and atypical genetic loci through exome sequencing in autosomal recessive cerebellar ataxia families. Clin Genet 2014, Oct;86(4):335-41. | 2014 |
| 17 | Desai S, Shukla G, Goyal V, Srivastava A, Srivastava MV, Tripathi M, et al. Changes in psychiatric comorbidity during early postsurgical period in patients operated for medically refractory epilepsy-a mini-based follow-up study. Epilepsy Behav 2014, Jan 23;32C:29-33. | 2014 |
| 18 | Chandra PS, Vaghania G, Bal CS, Tripathi M, Kuruwale N, Arora A, et al. Role of concordance between ictal-subtracted SPECT and PET in predicting long-term outcomes after epilepsy surgery. Epilepsy Res 2014, Dec;108(10):1782-9. | 2014 |
| 19 | Garg K, Singh PK, Sharma BS, Chandra PS, Suri A, Singh M, Kumar R, Kale SS, Mishra NK, Gaikwad SK, Mahapatra AK. Pediatric intracranial aneurysms--our experience and review of literature. Childs Nerv Syst. 2014 May;30(5):873-83. | 2014 |
| 20 | Suri V, Kakkar A, Sharma M, Padma M, Garg A, Sarkar C. Primary angiitis of the central nervous system: A study of histopathological patterns and review of the literature. Folia Neuropathol 2014;52(2):187-96. | 2014 |
| 21 | Kumar A, Krishna G, Singh PK, Garg A, Sharma BS. Spontaneously disappearing pineal region mass: A rare manifestation of vein of galen malformation. Indian J Pediatr 2014, Aug 8. | 2014 |
| 22 | Kakkar A, Sharma MC, Goyal N, Sarkar C, Suri V, Garg A, et al. Meningeal fibroma: A rare meningioma mimic. J Neurosurg Pediatr 2014, Aug;14(2):155-9. | 2014 |
| 23 | Sable MN, Nalwa A, Suri V, Singh PK, Garg A, Sharma MC, Sarkar C. Gangliocytic paraganglioma of filum terminale: Report of a rare case. Neurol India 2014;62(5):543-5. | 2014 |
| 24 | Kakkar A, Sharma MC, Suri V, Kaushal S, Chandra SP, Garg A, Sarkar C. Angiocentric glioma: A treatable cause of epilepsy: Report of a rare case. Neurol India 2014;62(6):677-9. | 2014 |
| 25 | Sable M, Kakkar A, Ranjan R, Garg A, Bakhshi S, Sharma MC. Yolk sac tumor of the temporal bone: An unusual presentation as hydrocephalus. Neurol India 2014;62(6):679-81. | 2014 |
| 26 | Faruq M, Srivastava AK, Suroliya V, Kumar D, Garg A, Shukla G, Behari M. Identification of FXTAS presenting with SCA 12 like phenotype in india. Parkinsonism Relat Disord 2014, Jul 17;20(10):1089-93. | 2014 |
| 27 | Chandra PS, Ramdurg SR, Kurwale N, Chauhan A, Ansari A, Garg A, et al. Extended costo-transversectomy to achieve circumferential fusion for pathologies causing thoracic instability. Spine J 2014, Jan 18. | 2014 |
| 28 | Prasad K, Sharma A, Garg A, Mohanty S, Bhatnagar S, Johri S, et al. Intravenous autologous bone marrow mononuclear stem cell therapy for ischemic stroke: A multicentric, randomized trial. Stroke 2014, Dec;45(12):3618-24. | 2014 |
| 29 | Garg A. Non-multiple sclerosis demyelinating diseases. In: Gupta RK, Kumar S, editors. Magnetic Resonance Imaging of Neurological Diseases In tropics. New Delhi: Jaypee Brothers Medical Publishers; 2014b. p. 281-91.1019 | 2014 |
| 30 | Third ventricular tuberculoma: Garg Kanwaljeet, Gurjar Hitesh Kumar, Joseph S, Shashikant Ravi Chetan, Sharma Bhawani Shankar: Neurology India,Year : 2014 | Volume: 62 | Issue Number:1 | Page: 73-75 | 2014 |
| 31 | Multiple intraventricular neurocysticerci: Deepti Vibha, MD, DM,Vipin Ola, MD,Madhuri Behari, MD, DM,Vinay Goyal, MD, DM,Garima Shukla, MD, DM andS. Leve Joseph Devarajan, MD, DM. NeurologySeptember 3, 2013vol. 81no. 10936-937 | 2013 |
| 32 | >Chandra P.S., Kumar A., Ansari A., Mishra N.K., Sharma B.S. : Distraction compression extension reduction of basilar invagination & atlanto-axial dislocation: a novel pilot technique: Neurosurgery 72 (6); 1040-1053; June 2013 | 2013 |
| 33 | >Kakkar A, Sharma MC, Garg A, Goyal N, Suri V, Sarkar C, Mahapatra AK. Uterus-Like mass in association with neural tube defect: A case report and review of the literature. Pediatr Neurosurg 2013, Apr 4 | 2013 |
| 34 | Chandra SP, Bal CS, Jain S, Joshua SP, Gaikwad S, Garg A, et al. Intra-Operative co-registration of MRI, PET and electrocorticographic data for neocortical lesional epilepsies may improve the localization of the epileptogenic focus: A pilot study. World Neurosurg 2013, Feb 21. | 2013 |
| 35 | Chandra SP, Singh A, Goyal N, Laythalling RK, Singh M, Kale SS, et al. Analysis of changing paradigms of management in 179 patients with spinal tuberculosis over a 12-year period and proposal of a new management algorithm. World Neurosurg 2013, Jan 22. | 2013 |
| 36 | Chandra SP, Singh A, Goyal N, Laythalling RK, Singh M, Kale SS, et al. Analysis of changing paradigms of management in 179 patients over 12 year period & proposal of A new management algorithm. World Neurosurg 2013, Jan 21. | 2013 |
| 37 | Singh G, Sharma MC, Suri V, Sarkar C, Garg A, Singh M. Alveolar soft part sarcoma of the paranasal sinuses masquerading as a giant invasive pituitary adenoma. Ann Diagn Pathol 2012, Aug 24. | 2012 |
| 38 | Singh G, Sharma MC, Agarwal S, Prasad GL, Mishra S, Singh MM, et al. Epithelial-myoepithelial carcinoma of the lacrimal gland: A rare case. Ann Diagn Pathol 2012, Aug;16(4):292-7. | 2012 |
| 39 | Agarwal S, Sharma MC, Singh G, Suri V, Sarkar C, Garg A, et al. Papillary glioneuronal tumor-a rare entity: Report of four cases and brief review of literature. Childs Nerv Syst 2012, Aug 7;28(11):1897-904. | 2012 |
| 40 | Singh G, Agarwal S, Sharma MC, Suri V, Sarkar C, Garg A, Kale SS. Spindle cell oncocytoma of the adenohypophysis: Report of a rare case and review of literature. Clin Neurol Neurosurg 2012, Apr;114(3):267-71. | 2012 |
| 41 | Prasad K, Mohanty S, Bhatia R, Srivastava MV, Garg A, Srivastava A, et al. Autologous intravenous bone marrow mononuclear cell therapy for patients with subacute ischaemic stroke: A pilot study. Indian J Med Res 2012, Aug;136(2):221-8. | 2012 |
| 42 | Padma Srivastava MV, Bhasin A, Bhatia R, Garg A, Gaikwad S, Prasad K, et al. Efficacy of minocycline in acute ischemic stroke: A single-blinded, placebo-controlled trial. Neurol India 2012;60(1):23-8. | 2012 |
| 43 | Ahuja A, Suri V, Suri A, Sharma MC, Prakash G, Bakhshi S, et al. Unusual central nervous system presentation of alk-positive anaplastic large cell lymphoma in a child. Neurol India 2012;60(5):522-4. | 2012 |
| 44 | Zanzmera P, Srivastava P, Garg A, Bhatia R, Singh M, Tripathi M, Prasad K. Prediction of stroke outcome in relation to alberta stroke program early CT score (ASPECTS) at admission in acute ischemic stroke: A prospective study from tertiary care hospital in north india. Neurology Asia 2012;17(2):101-7. | 2012 |
| 45 | Padma Srivastava MV, Bhasin A, Bhatia R, Garg A, Gaikwad S, Prasad K, et al. Efficacy of minocycline in acute ischemic stroke: A single-blinded, placebo-controlled trial. Neurol India 2012;60(1):23-8. | 2012 |
| 46 | Kumar A, Chandra PS, Bisht A, Garg A, Mahapatra AK, Sharma MC. Successful surgical excision of a nondysraphic holodorsal intramedullary lipoma in a 14-month-old child. Pediatr Neurosurg 2012, Feb 22. | 2012 |
| 47 | Rathore YS, Chandra PS, Kumar R, Singh M, Sharma MS, Suri A, Mishra NK, Gaikwad S, Garg A, Sharma BS, Mahapatra AK.: Monitored gradual occlusion of the internal carotid artery followed by ligation for giant internal carotid artery aneurysms. Neurol India. 2012, Mar-April; 60(2): 174-9. | 2012 |
| 48 | Chandra PS, Kumar A, Chauhan A, Ansari A, Mishra NK, Sharma BS.: “Distraction, compression and extension reduction of basilar invagination and atlanto-axial dislocation: A novel pilot Technique. Neurosurgery, published ahead of print DOI 10.1227/NEU.0b013e31828bf342, 2013, Feb 19. | 2012 |
| 49 | Kasliwal MK, Garg A, and Sharma BS. Midline intracranial hyperdense epidermoid tumor radiologically masquerading a neurenteric cyst. Clin Neurol Neurosurg. 2011;113(1):81-2. | 2011 |
| 50 | Subhash Kumar, Mishra NK.: “Middle meningeal artery arising from the basilar artery: report of a case and its probable embryological mechanism” – Accepted for publication Journal of NeuroInterventional Surgery, 2011. | 2011 |
| 51 | Ahuja A, Sharma MC, Suri V, Sarkar C, Sharma BS, and Garg A. Pineal anlage tumour - a rare entity with divergent histology. J Clin Neurosci. 2011. | 2011 |
| 52 | Gaikwad SB, S Sharma. S Kumar. Successful Embolization of a conus medullaris arteriovenous malformation using Onyx. Published Neurology India 2010, Vol 58, 817-818 | 2010 |
| 53 | Sharma S, S Kumar, Mishra NK, Gaikwad SB. Cerebral miliary micro aneurysms in polyarteritis nodosa: Report of two cases. Neurology India 2010, May-June, vol. 58: 457-459 | 2010 |
| 54 | Padma MV, Bhasin A, Bhatia R, et al. Normobaric oxygen therapy in acute ischemic stroke: A pilot study in Indian patients. Ann Indian Acad Neurol. 2010;13(4):284-8. | 2010 |
| 55 | Chandra PS, Bal C, Garg A, et al. Surgery for medically intractable epilepsy due to postinfectious etiologies. Epilepsia. 2010;51(6):1097-100. | 2010 |
| 56 | Sharma MC, Jain D, Sarkar C, Suri V, Garg A, Singh M, Mahapatra AK, Sharma BS: Spinal teratomas: a clinico-pathological study of 27 patients. Acta Neurochir (Wien) 2009, 151(3):245-252; discussion 252. | 2009 |
| 57 | Sharma MC, Jain D, Sarkar C, Suri V, Garg A, Singh M, Mahapatra AK, Sharma BS: Spinal teratomas: a clinico-pathological study of 27 patients. Acta Neurochir (Wien) 2009, 151(3):245-252; discussion 252. | 2009 |
| 58 | Sharma MC, Jain D, Sarkar C, Suri V, Garg A, Singh M, Mahapatra AK, Sharma BS: Spinal teratomas: a clinico-pathological study of 27 patients. Acta Neurochir (Wien) 2009, 151(3):245-252; discussion 252. | 2009 |
| 59 | Sharma MC, Jain D, Gupta A, Sarkar C, Suri V, Garg A, Gaikwad SB, Chandra PS: Dysembryoplastic neuroepithelial tumor: a clinicopathological study of 32 cases. Neurosurg Rev 2009, 32(2):161-170. | 2009 |
| 60 | Agarwal S, Suri V, Rishi A, Shukla B, Garg A, Sharma MC, Sinha S, Sarkar C: Glioneuronal tumor with neuropil-like islands: a new entity. Neuropathology 2009, 29(1):96-100. | 2009 |
| 61 | Suri V, Shukla B, Garg A, Singh M, Rishi A, Sharma MC, Sarkar C: Intracranial inflammatory pseudotumor: report of a rare case. Neuropathology 2008, 28(4):444-447. | 2008 |
| 62 | Suri V, Sharma MC, Suri A, Karak AK, Garg A, Sarkar C, Jain D: Myelolipomatous change in an interhemispheric lipoma associated with corpus callosum agenesis: case report. Neurosurgery 2008, 62(3):E745; discussion E745 | 2008 |
| 63 | Sharma S, Sankhyan N, Kalra V, Garg A: Thalamic Changes in Tay-Sachs’ Disease Arch Neurol 2008, 65(12):1669. | 2008 |
| 64 | Sharma AK, Gaikwad S, Gupta V, Garg A, Mishra NK. Measurement of peak CSF flow velocity at cerebral aqueduct, before and after lumbar CSF drainage, by use of phase-contrast MRI: Utility in the management of idiopathic normal pressure hydrocephalus. Clin Neurol Neurosurg 2008; 110:363-368. | 2008 |
| 65 | Sankhyan N, Sharma S, Kalra V, Garg A, Balkrishnan P: Cystic white-matter changes in childhood Wilson's disease. Pediatric Neurology 2008, 39(4):281-282. | 2008 |
| 66 | Prasad K, Bhatia R, Srivastava MV, Pardasani V, Garg A, Rishi A: Fatal subacute necrotising brainstem encephalitis in a young man due to a rare parasitic (Balamuthia) infection. Practical neurology 2008, 8(2):112-117. | 2008 |
| 67 | Kiran NA, Suri A, Kasliwal MK, Garg A, Ahmad FU, Mahapatra AK. Gross total excision of pediatric giant cystic craniopharyngioma with huge retroclival extension to the level of foramen magnum by anterior trans petrous approach: report of two cases and review of literature. Childs Nerv Syst 2008; 24:385-391. | 2008 |
| 68 | Jain D, Sharma MC, Sarkar C, Suri V, Rishi A, Garg A, Vaishya S. Chordoid glioma: report of two rare examples with unusual features. Acta neurochirurgica 2008;150(3):295-300; discussion | 2008 |
| 69 | Jain D, Sharma MC, Sarkar C, Suri V, Garg A, Mahapatra AK, Kumar L. Pituitary gland involvement by a gamma delta hepatosplenic lymphoma, a mimicker of pituitary adenoma: report of a rare case. J Neurooncol 2008. | 2008 |
| 70 | Jain D, Sharma MC, Sarkar C, Rishi A, Suri V, Garg A, Mahapatra AK. Spinal teratoma with renal differentiation-A rare phenomenon: Report of two patients. Clin Neurol Neurosurg 2008;110(3):265-9. | 2008 |
| 71 | Gupta R, Rishi A, Suri V, Sharma MC, Gupta A, Garg A, Sarkar C. Sacral myxopapillary ependymoma with extensive osteolysis. J Neurooncol 2008;86(3):349-52 | 2008 |
| 72 | Bhatia R, Desai S, Garg A, Padma MV, Prasad K, Tripathi M. Isolated facial myokymia as a presenting feature of pontine neurocysticercosis. Mov Disord 2008; 23:135-137. | 2008 |
| 73 | Sharma AK, Gaikwad S, Gupta V, Garg A, Mishra NK. Measurement of peak CSF flow velocity at cerebral aqueduct, before and after lumbar CSF drainage, by use of phase-contrast MRI: Utility in the management of idiopathic normal pressure hydrocephalus. Clin Neurol Neurosurg 2008; 110:363-368. | 2008 |
| 74 | Kiran NA, Suri A, Kasliwal MK, Garg A, Ahmad FU, Mahapatra AK. Gross total excision of pediatric giant cystic craniopharyngioma with huge retroclival extension to the level of foramen magnum by anterior trans petrous approach: report of two cases and review of literature. Childs Nerv Syst 2008; 24:385-391. | 2008 |
| 75 | Jain D, Sharma MC, Sarkar C, Suri V, Rishi A, Garg A, Vaishya S. Chordoid glioma: report of two rare examples with unusual features. Acta neurochirurgica 2008;150(3):295-300; discussion | 2008 |
| 76 | Jain D, Sharma MC, Sarkar C, Suri V, Garg A, Mahapatra AK, Kumar L. Pituitary gland involvement by a gamma delta hepatosplenic lymphoma, a mimicker of pituitary adenoma: report of a rare case. J Neurooncol 2008 | 2008 |
| 77 | Bhatia R, Desai S, Garg A, Padma MV, Prasad K, Tripathi M. Isolated facial myokymia as a presenting feature of pontine neurocysticercosis. Mov Disord 2008; 23:135-137 | 2008 |
| 78 | Shah H, Garg A, Mishra NK, Kale SS, Gaikwad SB. Delayed symptomatic cyst formation following gamma-knife radiosurgery. A case report. The Neuroradiology Journal. 2007;19:727-732 | 2007 |
| 79 | Puri AS, Garg A, Mishra NK, Gaikwad SB, Mehta VS. Bilateral cerebellar dysplastic gangliocytomas (lhermitteduclos disease) with cerebellar ectopia and presyrinx cord changes. A case report. The Neuroradiology Journal. 2007;19:717-721 | 2007 |
| 80 | Garg A, Mishra NK, Gaikwad SB, Gupta V. Bilateral internal carotid artery segmental agenesis associated with persistent trigeminal artery, vascular ectasia, abnormal configuration of brain stem and cerebellum. A case report. The Neuroradiology Journal. 2007;20:25-29 | 2007 |
| 81 | Garg A, Sridhar MR, Gulati S. Autosomal recessive type 1 lissencephaly. Indian J Pediatr. 2007;74:199-201 | 2007 |
| 82 | Gupta V, Tanvir R, Garg A, Gaikwad SB, Mishra NK. Heparin-Induced Thrombocytopenia in a Case of Endovascular Aneurysm Coiling. AJNR Am J Neuroradiol 2007 28: 155-158 | 2007 |
| 83 | Sharma MC, Sarkar C, Jain D, Suri V, Garg A, Vaishya S. Uterus-like mass of mullerian origin in the lumbosacral region causing cord tethering. Report of two cases. J Neurosurg Spine. 2007;6:73-76 | 2007 |
| 84 | Jain D, Sharma MC, Sarkar C, Suri V, Garg A, Singh M, Sharma BS, Mahapatra AK. Clear cell meningioma, an uncommon variant of meningioma: A clinicopathologic study of nine cases. J Neurooncol. 2007;81:315-321 | 2007 |
| 85 | Atri S, Sharma MC, Sarkar C, Garg A, Suri A. Papillary glioneuronaltumour: A report of a rare case and review of literature. Childs Nerv Syst. 2007;23:349-353 | 2007 |
| 86 | Mridha AR, Sharma MC, Sarkar C, Garg A, Singh MM, Suri V. Anaplastic ependymoma with cartilaginous and osseous metaplasia: Report of a rare case and review of literature. J Neurooncol. 2007;82:75-80 | 2007 |
| 87 | Rizvi T, Garg A, Mishra NK, Gaikwad SB, Gupta V. Metachronous double spinal duralarteriovenous fistulas. Case report and review of the literature. J Neurosurg Spine 2006; 4: 503-5 | 2006 |
| 88 | Epari S, Sharma MC, Sarkar C, Garg A, Gupta A, Mehta VS. Chordoid meningioma, an uncommon variant of meningioma: A clinicopathologic study of 12 cases. J Neurooncol. 2006; 78:263-269 | 2006 |
| 89 | Gupta DK, Suri A, Mahapatra AK, Mehta VS, Garg A, Sarkar C, Ahmad FU. Intracranial Rosai-Dorfman disease in a child mimicking bilateral giant petroclivalmeningiomas: a case report and review of literature. Childs NervSyst 2006; 22:1194-1200 | 2006 |
| 90 | Deb P, Sarkar C, Garg A, Singh VP, Kale SS, Sharma MC. Intracranial gliofibroma mimicking a meningioma: a case report and review of literature. ClinNeurolNeurosurg. 2006; 108:178-86 | 2006 |
| 91 | Ahmad FU, Pandey P, Sharma BS, Garg A. Foot drop after spinal anesthesia in a patient with a low-lying cord. Int J ObstetAnesth 2006;15:233-236 | 2006 |
| 92 | Sarkar C, Sharma MC, Deb P, Singh VP, Chandra PS, Gupta A, Tripathi M, Bhatia M, Gaikwad S, Bal CS, Jain S (2006) Neuropath logical spectrum of lesions associated with intractable epilepsies: a 10-year experience with a series of 153 resections. Neurol India 54:144-150; discussion 150-141 | 2006 |
| 93 | Gupta A, Ahmad FU, Kumar A, Gaikwad S, Vaishya S (2006) Umbilical CSF fistula: a rare complication of ventriculoperitoneal shunt. ActaNeurochir (Wien) 148:1205-1207 | 2006 |
| 94 | Dwarakanath S, Suri A, Mahapatra AK, Mehta VS, Gaikwad S, Sarkar C (2006) Endoscopic assisted excision of a retroclival arachnoid cyst presenting as hysterical breathlessness. Childs NervSyst 22:424-427 | 2006 |
| 95 | Deb P, Gupta A, Sharma MC, Gaikwad S, Singh VP, Sarkar C (2006) Meningioangiomatosis with meningioma: an uncommon association of a rare entity--report of a case and review of the literature. Childs NervSyst 22:78-83 | 2006 |
| 96 | Shukla G, Bhatia M, Padma Srivastava MV, Tripathi M, Srivastava A, Singh VP, Saratchandra P, Gupta A, Gaikwad S, Bal CS, Jain S (2005) Unidirectional whole body turning: a new lateralising sign in complex partial seizures. J NeurolNeurosurg Psychiatry 76:1726-1729 | 2005 |
| 97 | Ahmad FU, Suri A, Mahapatra AK, Mehta VS, Garg A, Sharma MC, Sridhar E. Intraventricularrhabdoid tumor. Indian J Pediatr. 2005 Aug;72(8):693-6 | 2005 |
| 98 | Ahmad FU, Chandra PS, Sanyal S, Garg A, Mehta VS. SellarTuberculoma: an Unusual Infection. Indian J Tuberc 2005; 52:215-217. | 2005 |
| 99 | Jaiswal AK, Garg A, Mahapatra AK. Spinal ossifying lipoma. J ClinNeurosci 2005; 12:714-717 | 2005 |
| 100 | Singh NP, Sarkar C, Sharma MC, Garg A, Gaikwad SB, Kale SS, Mehta VS. Paraganglioma of caudaequina: report of seven cases. Brain Tumor Pathol 2005; 22:15-20 | 2005 |
| 101 | Sharma A, Garg A, Mishra NK, Gaikwad SB, Sharma MC, Gupta V, Suri A. Primary Ewing's sarcoma of the sphenoid bone with unusual imaging features: a case report. ClinNeurolNeurosurg 2005; 107:528-531 | 2005 |
| 102 | Rizvi T, Garg A, Singh M, Sharma MC. Large intracranial mass with a calcified rim - is it a brain abscess? PediatrNeurosurg. 2005; 41:112-114 | 2005 |
| 103 | Gupta V, Rizvi T, Garg A, Gaikwad SB, Mishra NK. Postangiographic thrombosis of a spinal arteriovenous malformation: case report. J Neurosurg Spine 2005;2(4):486-490. | 2005 |
| 104 | Rizvi T, Garg A, Singh M, Sharma MC. Large intracranial mass with a calcified rim - is it a brain abscess? PediatrNeurosurg. 2005; 41:112-114 | 2005 |
| 105 | Dwarakanath S, Suri A, Garg A, Mahapatra AK, Mehta VS. Adult complex spinal dysraphism with situsinversustotalis: a rare association and review. Spine 2005; 30:E225-228 | 2005 |
| 106 | Sharma MC, Epari S, Gaikwad S, Verma A, Sarkar C. Orbital paraganglioma: report of a rare case. Can J Ophthalmol 2005;40:640-644 | 2005 |
| 107 | Deb P, Sharma MC, Gaikwad S, Gupta A, Mehta VS, Sarkar C. Cerebellopontine angle paraganglioma - report of a case and review of literature. J Neurooncol 2005; 74:65-69 | 2005 |
| 108 | Sharma S, Sarkar C, Gaikwad S, Suri A, Sharma MC. Primary neurocytoma of the spinal cord: a case report and review of literature. J Neurooncol 2005; 74:47-52 | 2005 |
| 109 | Deb P, Sharma MC, Gaikwad S, Tripathi M, Chandra PS, Jain S, Sarkar C (2005) Neuropathological spectrum of Rasmussen encephalitis. Neurol India 2005; 53:156-160; discussion 160-151 | 2005 |
| 110 | Suri A, Mahapatra AK, Gaikwad S, Sarkar C. Giant mucoceles of the frontal sinus: a series and review. J ClinNeurosci 2005; 11:214-218 | 2004 |
| 111 | Garg A, Chugh M, Gaikwad SB, et al. Juvenile pilocytic astrocytoma presenting with subarachnoid hemorrhage. Case report and review of the literature. J Neurosurg 2004; 100:525-529 | 2004 |
| 112 | Garg, A, Gulati S, Gupta V, Kalra V. Congenital muscular dystrophy with characteristic radiological findings similar to those with Fukuyama congenital muscular dystrophy. Neurol India 2004; 52:496-498 | 2004 |
| 113 | Garg A, Gupta V, Gaikwad SB, et al. Scalp malignant peripheral nerve sheath tumor (MPNST) with bony involvement and new bone formation: case report. ClinNeurolNeurosurg 2004; 106:340-344 | 2004 |
| 114 | Garg A, Gaikwad SB, Kanodia A, Suri A, Gupta V, Mishra NK. Positional occlusion/stasis of vertebral arteries in a case of cervical rheumatoid arthritis presenting with multiple posterior circulation infarcts: a case report with angiographic demonstration. Spine 2004; 29:E321-325. Erratum in: Spine 2004 Oct 15; 29(20):2341. | 2004 |
| 115 | Garg A, Gaikwad S, Gupta V, Mishra NK, Vaish S, Ralte AM. Malignant rhabdoidtumour of the third ventricle. AustralasRadiol 2004; 48:80-83 | 2004 |
| 116 | Garg A, Gaikwad SB, Gupta V, Mishra NK, Kale SS, Singh J. Bipartite atlas with osodontoideum: case report. Spine 2004; 29:E35-38 | 2004 |
| 117 | Garg A, Suri A, Gupta V. Cyst with a mural nodule: unusual case of brain metastasis. Neurol India 2004; 52:136 | 2004 |
| 118 | Agarwal PP, Gaikwad SB, Garg A, Gupta V, Mishra NK, Mehta VS. Giant intraparenchymalneurocysticercosis: unusual MRI findings. Neurol India 2004; 52:259-260 | 2004 |
| 119 | Ahmad FU, Suri S, Mahapatra AK, Ralte A, Sarkar C, Garg A. Giant calvarial Ewing's sarcoma. PediatrNeurosurg 2004; 40:44-46 | 2004 |
| 120 | Rizvi T, Garg A, Gupta V, Gaikwad S, Mishra NK. Role of CISS MR Sequence in Detection of Spinal Dural Arteriovenous Fistula- Case report. Clinical Radiology Extra 2004; 59:78-82. | 2004 |
| 121 | Ralte AM, Rao S, Sharma MC, Suri A, Gaikwad S, Sarkar C. Myxopapillaryependymoma of the temporal lobe--report of a rare case of temporal lobe epilepsy. ClinNeuropathol 2004;23:53-58 | 2004 |
| 122 | Jagia P, Gulati GS, Sharma S, Goyal NK, Gaikwad S, Saxena A. MRI features of tuberculoma of the right atrial myocardium. PediatrRadiol 2004; 34:904-907 | 2004 |
| 123 | Tripathi M, Goel V, Padma MV, Jain S, Maheshwari MC, Gaikwad S, Gupta V, Chandra PS, Mehta VS. Fenestration of the posterior communicating artery. Neurol India 2003;51:75-76 | 2003 |
| 124 | Gaikwad SB, Garg A, Mishra NK, Gupta V, Srivastava A, Sarkar C. Cerebrotendinousxanthomatosis: Neuroimaging findings in two siblings from an Indian family. Neurol India 2003 Sep; 51(3): 401-3. | 2003 |
| 125 | Prabhakar H, Bithal PK, Garg A. Tension pneumocephalus following craniotomy in the supine position. J NeurosurgAnesthesiol 2003; 15:278-81 | 2003 |
| 126 | Garg A, Gupta V, Gaikwad S, et al. Isolated central canal rupture of spinal dermoid: report of two cases. AustralasRadiol 2003; 47:194-197 | 2003 |
| 127 | Suri A, Chabbra RP, Mehta VS, Gaikwad S, Pandey RM. Effect of intramedullary signal changes on the surgical outcome of patients with cervical spondylotic myelopathy. Spine J 2003; 3:33-45 | 2003 |
| 128 | Suri A, Singh VP, Kale SS, Mehta VS, Gaikwad S. Multifocal intracranial rhabdoid tumor. Neurol India 2003; 51:297-298 | 2003 |
| 129 | Gupta V, Garg A, Behari M, Thomas R, Gaikwad SB, Mishra NK. Intramedullary Tuberculoma: MR findings in 13 cases. Rivista di Neuroradiologia 2003; 16:1359 | 2003 |
| 130 | Gupta V, Garg A, Chandra S, Sharma MC, Gaikwad SB, Gulati S. Cerebellar epilepsy- A case report of a cerebellar gangliomatoushamartomaRivisita di Neuroradiologia 2003; 16:784-707 | 2003 |
| 131 | Gaikwad SB, Garg A, Deol PS, Sharma MC, Bhatia M, Gupta A, Gupta V, Mishra NK. Dysembryoplasticneuroepithelial tumors- Neuroimaging findings. Rivisita di Neuroradiologia 2003; 16:877-882 | 2003 |
| 132 | Mishra NK, Gupta V, Garg A., Gaikwad S.B. Vein of Galen Malformations - AIIMS experience. Rivista di Neuroradiologia 2003; 16:1308 | 2003 |
| 133 | Gaikwad SB, Gupta V, K Avinash, Garg A, Suri A, Kale S, Mishra NK. Craniovertebral junction abnormalities with vertebrobasilarischaemia. Rivisita di Neuroradiologia 2003; 16:1349 | 2003 |
| 134 | Gupta V, Kumar A, Garg A, Gaikwad SB, Singh VP, Sharma MC, Kumar R, Mishra NK. Radiological analysis of lateral and third ventricular tumors – A retrospective study. Rivisita di Neuroradiologia 2003; 16:865-868 | 2003 |
| 135 | Srivastava AK, Tripathi M, Gaikwad SB, Padma MV, Jain S Internuclearophthalmoplegia and torsional nystagmus: an MRI correlate. Neurol India 2003;51:271-272 | 2003 |
| 136 | Shukla G, Bhatia M, Singh VP, Jaiswal A, Tripathi M, Gaikwad S, Bal CS, Sarker C, Jain S. Successful selection of patients with intractable extratemporal epilepsy using non-invasive investigations. Seizure 2003;12:573-576 | 2003 |
| 137 | Sarkar C, Mukhopadhyay S, Ralte AM, Sharma MC, Gupta A, Gaikwad S, Mehta VS. Intramedullary subependymoma of the spinal cord: a case report and review of literature. ClinNeurolNeurosurg 2003; 106:63-68 | 2003 |
| 138 | Sarkar C, Sharma MC, Arora R, Gaikwad S, Mehta VS. 21-year-old male with cystic intracerebral tumor. Brain Pathol 2003; 13:113-114, 117 | 2003 |
| 139 | Gaikwad SB, Garg A, Mishra NK, Gupta V, Srivastava A, Sarkar C. Cerebrotendinousxanthomatosis: neuroimaging findings in two siblings from an Indian family. Neurol India 2003; 51:401-403 | 2003 |
| 140 | Pandey G, Kapur M, Khan MI, Gaikwad SM. A new access to polyhydroxypiperidines of the azasugar class: synthesis and glycosidase inhibition studies. Org BiomolChem 2003; 1:3321-3326 | 2003 |
| 141 | Thomas R, Bhatia M, Bal CS, Gaikwad S, Singh VP, Jain S. Correlation of ictal EEG and SPECT studies in patients of intractable epilepsy with normal MRI. Neurol India 2002; 50:440-443 | 2002 |
| 142 | Thomas R, Behari M, Gaikwad SB, Prasad K. An unusual case of paroxysmal kinesigenic dyskinesia. J ClinNeurosci 2002; 9:94-97 | 2002 |
| 143 | Sharma MC, Agarwal M, Suri A, Gaikwad S, Mukhopadhyay P, Sarkar C (2002) A melanoticdesmoplasticmedulloblastoma: report of a rare case and review of the literature. Brain Tumor Pathol 2002; 19:93-96 | 2002 |
| 144 | Garg A, Gupta V, Gaikwad S, et al. Spinal angiolipoma: report of three cases and review of MRI features. AustralasRadiol 2002; 46:84-90 | 2002 |
| 145 | Sharma MC, Agarwal M, Suri A, Gaikwad S, Mukhopadhyay P, Sarkar C. Lipomedulloblastoma in a child: a controversial entity. Hum Pathol 2002;33:564-569 | 2002 |
| 146 | Jayasundar R, Sahani AK, Gaikwad S, Singh S, Behari M. Proton MR spectroscopy of basal ganglia in Wilson's disease: case report and review of literature. MagnReson Imaging 2002; 20:131-135 | 2002 |
| 147 | Deol PS, Mishra NK, Gaikwad SB, Garg A, Gupta V, Sharma MC. Cavernous Hemangioma of the Gasserian Ganglion MR Appearance. vista di Neuroradiologia 2001;14:333 | 2001 |
| 148 | Deol PS, Mishra NK, Gupta V, Gaikwad SB, Garg A, Singh N. Post Traumatic Cavernous Fistula fed by Persistent Trigeminal artery: Treatment by GDC Embolisation. Interventional Neuroradiology 2001; 7: 47-50 | 2001 |
| 149 | Sharma MC, Vaish S, Arora R, Gaikwad S, Sarkar C. Composite pituitary adenoma and intrasellartuberculoma: report of a rare case. PatholOncol Res 2001; 7:74-76 | 2001 |
| 150 | Sharma A, Gaikwad SB, Deol PS, Mishra NK, Kale SS. Partial aplasia of the posterior arch of the atlas with an isolated posterior arch remnant: findings in three cases. AJNR Am J Neuroradiol 2000; 21:1167-1171 | 2000 |
| 151 | Sharma A, Gaikwad SB, Deol PS, Mishra NK, Kale SS. Partial aplasia of the posterior arch of the atlas with an isolated posterior arch remnant: findings in three cases. AJNR Am J Neuroradiol. 2000 Jun-Jul; 21(6): 1167-71 | 2000 |
| 152 | Sharma MC, Arora R, Mahapatra AK, Sarat-Chandra P, Gaikwad SB, Sarkar C. Intrasellartuberculoma--an enigmatic pituitary infection: a series of 18 cases. ClinNeurolNeurosurg 2000; 102:72-77 | 2000 |
| 153 | Chandra S, Goyal M, Mishra NK, Gaikwad SB. Invasive aspergillosis presenting as a cavernous sinus mass in immuno competent individuals; report of 3 cases. Neuroradiology 2000; 42:108-111 | 2000 |
| 154 | Sharma MC, Sarkar C, Karak AK, Gaikwad S, Mahapatra AK, Mehta VS. Intraventricularneurocytoma: a clinicopathological study of 20 cases with review of the literature. J ClinNeurosci 1999; 6:319-323 | 1999 |
| 155 | Goyal M, Mishra NK, Sharma A, Gaikwad SB, Mohanty BK, Sharma S. Alcohol ablation of symptomatic vertebral hemangiomas. AJNR Am J Neuroradiol. 1999 Jun-Jul; 20(6): 1091-6 | 1999 |
| 156 | Sharma MC, Kanse M, Mahapatra AK, Gaikwad S, Sarkar C. Case of the month: September 1998 - 18 year old male with large cystic orbital tumor. Brain Pathol 1999; 9:191-192 | 1999 |
| 157 | Sarkar C, Sharma MC, Gaikwad S, Sharma C, Singh VP. Choroid plexus papilloma: a clinicopathological study of 23 cases. SurgNeurol 1999; 52:37-39 | 1999 |
| 158 | Goyal M, Mishra NK, Sharma A, Gaikwad SB, Mohanty BK, Sharma S. Alcohol ablation of symptomatic vertebral hemangiomas. AJNR Am J Neuroradiol 1999; 20:1091-1096 | 1999 |
| 159 | Goyal M, Malik A, Mishra NK, Chandra S, Gaikwad SB, Jain K. Congenital maldevelopment of intervertebral disc simulating a neurofibroma. Skeletal Radiol. 1998; 27:388-91 | 1998 |
| 160 | Sharma A, Gaikwad SB, Goyal M, Mishra NK, Sharma MC. Calcified filumterminaleparaganglioma causing superficial siderosis. AJR Am J Roentgenol. 1998; 170:1650-1652 | 1998 |
| 161 | Sharma MC, Singh A, Verma A, Gaikwad S, Sarkar C. Diagnostic yield in computed tomography guided stereotactic biopsies. J Assoc Physicians India 1998; 46:427-430 | 1998 |
| 162 | Sharma MC, Gaikwad S, Mahapatra AK, Menon PS, Sarkar C. Hypothalamic hamartoma: report of a case with unusual histologic features. Am J SurgPathol 1998; 22:1538-1541 | 1998 |
| 163 | Sharma MC, Gaikwad S, Mehta VS, Dhar J, Sarkar C. Gliofibroma: mixed glial and mesenchymaltumour. Report of three cases. ClinNeurolNeurosurg 1998; 100:153-159 | 1998 |
| 164 | Sharma A, Gaikwad SB, Goyal M, Mishra NK, Sharma MC. Calcified filumterminaleparaganglioma causing superficial siderosis. AJR Am J Roentgenol 1998; 170:1650-1652 | 1998 |
| 165 | Sharma MC, Mahapatra AK, Gaikwad S, Jain AK, Sarkar C. Pigmented medulloepithelioma: report of a case and review of the literature. Childs NervSyst 1998; 14:74-78 | 1998 |
| 166 | Goyal M, Malik A, Mishra NK, Chandra S, Gaikwad SB, Jain K. Congenital maldevelopment of intervertebral disc simulating a neurofibroma. Skeletal Radiol 1998; 27:388-391 | 1998 |
| 167 | Sharma MC, Sarkar C, Gaikwad S, Mahapatra AK, Bahadur S. Congenital orbital teratoma: a report of two cases. Indian J Ophthalmol 1997; 45:49-52 | 1997 |
| 168 | Sharma MC, Mahapatra AK, Gaikwad SB, Sarkar C. Solitary giant skull base schwannomas--report of four cases. SurgNeurol 1997; 48:382-387; discussion 387-388 | 1997 |
| 169 | Sharma A, Goyal M, Mishra NK, Gupta V, Gaikwad SB. MR imaging of tubercular spinal arachnoiditis. AJR Am J Roentgenol 1997; 168:807-812 | 1997 |
| 170 | Sarkar C, Sharma MC, Sudha K, Gaikwad S, Varma A. A clinico-pathological study of 29 cases of gliosarcoma with special reference to two unique variants. Indian J Med Res 1997;106:229-235 | 1997 |
| 171 | Padma MV, Gaikwad S, Jain S, Maheshwari MC, Misra NK. Distribution of vascular lesions in ischaemic stroke: a magnetic resonance angiographic study. Natl Med J India 1997; 10:217-220 | 1997 |
| 172 | Malik A, Goyal M, Mishra NK, Gaikwad SB, Padma V. Intracerebralhaematoma formation in herpes simplex encephalitis: a case report. AustralasRadiol 1997; 41:303-305 | 1997 |
| 173 | Gupta V, Goyal M, Mishra NK, Sharma A, Gaikwad SB. Positional MRI: a technique for confirming the site of leakage in cerebrospinal fluid rhinorrhoea. Neuroradiology 1997; 39:818-820 | 1997 |
| 174 | Gupta V, Goyal M, Mishra N, Gaikwad S, Sharma A. MR evaluation of CSF fistulae. ActaRadiol 1997; 38:603-609 | 1997 |
| 175 | Goyal M, Sharma A, Mishra NK, Gaikwad SB, Sharma MC. Imaging appearance of pachymeningeal tuberculosis. AJR Am J Roentgenol 1997; 169:1421-1424 | 1997 |
| 176 | Goyal M, Malik A, Mishra NK, Gaikwad SB. Idiopathic hypertrophic pachymeningitis: spectrum of the disease. Neuroradiology 1997; 39:619-623 | 1997 |
| 177 | Sharma MC, Sudha K, Rathore A, Sarkar C, Gaikwad S, Patir R, Karak AK. Two rare parasites of the human brain--Gnathostomaspinigerum and sparganum (Spirometra). J Assoc Physicians India 1996; 44:824-828 | 1996 |
| 178 | Sharma MC, Mahapatra AK, Sudha K, Gaikwad S. Melanoticneuroectodermaltumour of infancy: immunohistochemical and histogenetic consideration. J Assoc Physicians India 1996; 44:278-280 | 1996 |
| 179 | Sharma MC, Mahapatra AK, Gaikwad S, Biswal A. Primary extramedullary orbital plasmacytoma in a child. Childs NervSyst 1996; 12:470-472 | 1996 |
| 180 | Sharma MC, Karak AK, Gaikwad SB, Mahapatra AK, Mehta VS, Sudha K. Intracranial intraparenchymalschwannomas: a series of eight cases. J NeurolNeurosurg Psychiatry 1996; 60:200-203 | 1996 |
| 181 | Goyal M, Mishra NK, Gaikwad S, Jayasundar R. Cervical intramedullary lipoma with unusual MRI features: case report. Neuroradiology 1996; 38 Suppl 1:S117-119 | 1996 |
| 182 | Padma MV, Sharma AK, Gaikwad S, Maheshwari MC. The myopathic variety of arthrogryposis multiplex congenita. J Assoc Physicians India 1995; 43:291-292 | 1995 |
E-mail: dranjudhawan[at]gmail[dot]com
Details of publications since 2010 onwards (the full citation)- these should be divided into journal articles (peer reviewed publications) and books/monographs/project reports/ proceedings from workshops (non-peer reviewed publications)
Quraishi R, Pattanayak R, Jain R, Dhawan A (2013). A descriptive study of clinical, hematological, and biochemical parameters of inhalant users seeking treatment at a tertiary care center in India. Indian J Psychol Med Apr, 35(2):174-9.
Gupta A, Mandal P, Bhargava R, Pattanayak RD, Sagar R, Dhawan A (2014). Marked exacerbation of ADHD after onset of inhalant use: a case report. J Neuropsychiatry Clin Neurosci, 26(4):E6-7.
Marked exacerbation of ADHD after onset of inhalant use: a case report.
Balhara YP, Ranjan R, Dhawan A, Yadav D (2014). Experiences from a community based substance use treatment centre in an urban resettlement colony in India. J Addict, 98:20-28.
Ranjan R, Pattanayak RD, Dhawan A (2014). Long-term agonist and antagonist therapy for adolescent opioid dependence: a description of two cases. Indian J Psychol Med, 36(4):439-43.
Jyotsna VP, Dhawan A, Sreenivas V, Deepak KK, Singla R (2014). Completion report: Effect of Comprehensive Yogic Breathing program on type 2 diabetes: A randomized control trial. Indian J EndocrinolMetab, 18(4):582-4.
Dhawan A, Chopra A, Ambekar A, Ray R (2015). Treatment Seeking Behavior of Inhalant Using Street Children: Are We Prepared to Meet Their Treatment Needs. Indian J Psychol Med, 37(3): 282-287.
Dhawan A, Chopra A, Jain R, Yadav D, Vedamurthachar (2015). Effectiveness of yogic breathing intervention on quality of life of opioid dependent users. Int J Yoga, 8(2): 144-147.
Effectiveness of yogic breathing intervention on quality of life of opioid dependent users.
Rao R, Mandal P, Gupta R, Ramshankar P, Mishra A, Ambekar A, Jhanjee S, Dhawan A (2016). Factors Affecting Drug Use During Incarceration: A Cross-Sectional Study of Opioid-Dependent Persons from India. J Subst Abuse Treat, 61: 13-17.
Gupta P, Mandal P, Singh D,Pattanyak R, Bhargava R, Dhawan A (2016). Detection of Optic Neuropathy and 3-month Follow-up of an Adolescent Inhalant User: Are we Paying Enough Attention? Indian J Psychol Med , 38(5): 486–488.doi: 10.4103/0253-7176.191390
Das M, Jain R, Dhawan A, Kaur A (2016). Assessment of abuse liability of Tramadol among experienced drug users: Double-blind crossover randomized controlled trial. J Opioid Manag, 12(6):421-430.
Singh G, Kaloiya GS, Dhawan A, Balhara YPS, Mishra AK (2018) Need for evaluation of underlying dysfunctional cognition in problem drinkers. Asian Journal of Psychiatry 31: 71-72.
Raghav R, Jain R, Dhawan A, Ray TS, Kumar P (2018). Chronic co-administration of nalbuphine attenuates the development of opioid dependence. Pharmacology Biochemistry and Behavior 175: 130-138.
Dhawan A, Modak T, Sarkar S (2019). Transdermal buprenorphine patch : Potential for role in management of opioid dependence. Asian J Psychiatr 40:88-91.
Mandal P, Parmar A, Ambekar A, Dhawan A (2019). Substance use among treatment seeking Indian adolescent girls: Are they unique? Asian J Psychiatr
Gupta, S., Dhawan, A. (2022). Methodological issues in conducting yoga- and meditation-based research: A narrative review and research implications. Journal of Ayurveda and integrative medicine, 13(3), 100620. https://doi.org/10.1016/j.jaim.2022.100620
Singh, V. V., Sarkar, S., Chadda, R. K., Mishra, A. K., & Dhawan, A. (2022). Reasons for leaving treatment among patients with opioid dependence: A 3-month prospective follow-up study. Journal of opioid management, 18(5), 455–466. https://doi.org/10.5055/jom.2022.0739
Dhawan A, Chopra A, Balhara YPS. Building National Capacity For Management Of Substance Use Disorders. Alcohol and Alcoholism. 2014; 49 (suppl 1): i12 DOI: http://dx.doi.org/10.1093/alcalc/agu052.51
Dhawan A., Patil V., Gupta S., Chugh G. Mindfulness and Mental Health. In: Okpaku S.O.(eds) Innovations in Global Mental Health. Springer, Cham, 2021. https://doi.org/10.1007/978-3-319-70134-
Investigator/ Co-investigator in funded projects along with year completed/ongoing
| Projects as Chief Investigator | Source of funding | Year |
|---|---|---|
| Psychotropic substance abuse | United Nations Drug Control Programme, Regional Office for South Asia (UNDCP ROSA) | 2001-02 |
| Evaluation of functioning of de-addiction centres in the country | WHO (India) | 2001-2002 |
| Opioid Substitution Treatment with Buprenorphine | United Nations Office on Drugs and Crime, Regional Office for South Asia (UNODC-ROSA) | 2006-2009 |
| Assessment of feasibility and effectiveness of Methadone Maintenance Treatment in India | UNODC (ROSA) | 2011-2013 |
| Effectiveness of Yoga in patients of Opioid Dependence | Central Council for Research in Yoga and Naturopathy, AYUSH, Ministry of Health and Family Welfare | 2009-2011 |
| Assessment of pattern, profile and correlates of substance use in children | NCPCR | 2012-2013 |
| Training of doctors on Substance Use Disorders | Department of Revenue, Ministry of Finance | 2010-15 |
| Mapping and Size Estimation of Street Children Who Use Drugs in Delhi | Department of Women and Child development, Delhi Govt | 2015-16 |
| Extent of Mental Health issues & Addictive Behavior among Adolescents seeking help in Adolescent Friendly Health Clinics in Delhi | Adolescent Health Division, Directorate of Family Welfare, Govt of NCT of Delhi | 2019-2020 |
| Survey on Substance use among School and College Students | Ministry of Social Justice and Empowerment, Government of India | 2019-20 |
| Screening and Intervention for Drug/Substance Use among Secondary School going Children | UEE Mission, Education Department Delhi | 2020-21 |
| A prospective double blind, randomized clinical study to evaluate the antibody response after Covid-19 vaccine when provided along with KabasuraKudineer, a siddha medicine | SSIAR | 2021-22 |
| A prospective double blind, randomized clinical study to evaluate the antibody response after Covid-19 vaccine when provided along with NOQ19, an Ayurvedic medicine | SSIAR | 2022 |
| Projects as Co-Investigator | Source of funding | Year |
|---|---|---|
| Rapid Assessment Survey Project on Alcohol, Tobacco and other substances in Districts of Darjeeling, Kohima, Aizwal | WHO (India) | 1999 |
| Rapid Assessment Survey Project on Alcohol, Tobacco and other substances in Districts of North Goa, Jodhpur, Madras | WHO (India) | 2000 |
| Buprenorphine maintenance programme in Kohima district | WHO (India) | 2000 |
| Global study on illegal drug markets | UNDCP and UNICRI | 2000-2001 |
| A survey of prevalence of drug dependence and comorbidity in the general population of Thrissur | WHO (India) | 2001-2002 |
| Advance Statistical Analysis of National Survey Data using new methodologies without the addition of data | WHO (India) | 2001-2002 |
| To undertake a study to examine the relationship of tobacco as a gateway drug and to determine the prevalence of substance use behavioural disorders including tobacco in Metropolis Delhi | WHO (India) | 2002-2003 |
| Database on Drug Abuse and HIV/AIDS | UNODC (ROSA) | 2005-2009 |
| Assessment of drug use in out of School Adolescents | WHO (India) | 2008 |
| Development of intervention for drug use in out of school adolescents | WHO (India) | 2008-2009 |
| Coordination & convergence of Delhi District Health Services programmes & drug use intervention for the out of school children | WHO (India) | 2010-2011 |
| Developing a network of de-addiction services from the Government, NGO & Private sector | WHO (India) | 2010-2011 |
| Extent of internet use amongst adolescents with non-psychotic disorders: A case control study | AIIMS | 2016 |
| Validation of Teen Addiction Severity Index | AIIMS | 2016 |
| Screening and Intervention for Drug/Substance Use among Elementary School going Children | UEE Mission, Education Department Delhi | 2020-21 |
| A study to examine dependence, harm perception and motivation to quit amongst Indian areca nut users and pilot test an intervention module | WHO (India) | 2020-22 |
| Real World Effectiveness of add-on Yoga for patients with opioid dependence stabilized on treatment | DST SATYAM | 2022-23 |
| A study to examine psych-social and behavioral domains among school going adolescents during covid-19 pandemic: Mixed study design | ICMR | 2022-24 |
Adult attention-deficit hyperactivity disorders and its correlates in patients with opioid dependence (2018-19)
Retrospective study to analyze the profile, the pattern of substance
use and outcome of treatment of adolescent patients who sought
treatment for opioid use (on-going)
To assess the effect of intervention of yoga and meditation-based structured programme for youth on the psychological functioning of medical students (on-going)
- as guide (number only)- 8
-as co-guide (number only)-PhD thesis-8, MD and DM thesis-16
13. Awards and Honors
Year of Completion: 1977
Area of Interest: --
Current Affiliation: --
Year of Completion: 1983
Area of Interest: --
Current Affiliation: --
Year of Completion: 1984
Area of Interest:--
Current Affiliation: --
Year of Completion: 1986
Area of Interest: --
Current Affiliation: --
Year of Completion: 1986
Area of Interest: --
Current Affiliation: --
Year of Completion: 2006
Area of Interest: --
Current Affiliation: --
Year of Completion: 2009
drcgicmr[at]gmail[dot]com
Area of Interest: Movement Disorder
Current Affiliation: Scientist E, ICMR, New Delhi

Year of Completion: 2011
saima_aiims[at]rediffmail[dot]com
Area of Interest: Genetics/ Molecular Biology
Current Affiliation: Women Scientist (BioCARe- DBT), Department Of Anatomy, AIIMS, New Delhi
Year of Completion: 2011
ashu.bhasin[at]gmail[dot]com
Area of Interest: Stroke, regenerative medicine and neuorehabilitation
Current Affiliation: Project Research Officer, Department of Neurology, AIIMS, New Delhi
Year of Completion: 2012
neha.karlupia[at]gmail[dot]com
Area of Interest: Stem Cell therapy in rodents
Current Affiliation: --

Year of Completion: 2013
mohit.saxena.aiims[at]gmail[dot]com
Area of Interest: Neuroimaging, Movement Disorders
Current Affiliation: Clinical Post Doc, Cleveland Clinic, Ohio, USA
Year of Completion: 2013
singhi.aiims[at]gmail[dot]com
Area of Interest: Ataxia
Current Affiliation: Project Scientist C, Department of Neurology, AIIMS, New Delhi

Year of Completion: 2014
amits52003[at]gmail[dot]com
Area of Interest: Stroke Genetics, Meta-analysis, Epidemiology
Current Affiliation: Project Scientist C, Department of Neurology, AIIMS, New Delhi

Year of Completion: 2014
farooq[at]igib.[dot]es.in
Area of Interest: Ataxia Genomics
Current Affiliation: Scientist E, CSIR Institute of Genomics and Integrative Biology, Mall Road, Delhi

Year of Completion: 2015
anupmaguptaa[at]live.[dot]om
Area of Research: Sleep Medicine
Current Affiliation: Project Scientist B, Department of Neurology, AIIMS, New Delhi

Year of Completion: 2016
kchaudhary84[at]redif[dot]mail.com
Area of Research: functional neuroimaging in drug refractory epilepsy
Current Affiliation: Project SRO, Department of Neurology, AIIMS, New Delhi

Year of Completion: 2016
pradeepguptaneuro[at]gmail[dot]com
Area of Interest: Stroke Genetics, Neuroimaging
Current Affiliation: Research Associate, Department of Paediatrics. RR Hospital, New Delhi

Year of Completion: 2017
deepak5sep[at]gmail[dot]com
Ataxia Genetics
Current Affiliation: Research Associate, CSIR-IGIB Delhi
Year of Completion: 2017
vibhuti_bms[at]yahoo[dot]co.in
Area of Interest: Stroke Genetics
Current Affiliation: Postdoctoral fellow, Cleveland Clinics, Ohio, USA

Year of Completion: 2017
rekha.dwivedi2006[at]gmail[dot]com
Area of Research: Epilepsy
Current Affiliation: National Post-Doctoral Fellow (N-PDF)
Department of Neurology, AIIMS, New Delhi.

Year of Completion: 2018
kavishls[at]gmail[dot]com
Area of Research: Genetic and Immunological mechanisms in persons with epilepsy.
Current Affiliation: Project Senior Research Officer,
Department of Neurology, AIIMS, New Delhi.

Year of Completion: 2018
sunilshakya21[at]gmail[dot]com
Area of Interest: Genetics Ataxia
Current Affiliation: Project Scientist-C, Department of Nuclear Medicine, AIIMS, New Delhi

Year of Completion: 2018
hinasharma09.hs[at]gmail[dot]com
Area of Interest: Neurophysiology, Acute Stroke Intervention
Current Affiliation: Executive director at National Network of Depression Center India Foundation, US Affiliate

Year of Completion: 2019
mahisagar87[at]gmail[dot]com
Area of Interest: Stroke genetics/Biomarker Analysis/Epidemiology
Current Affiliation: Project Senior Research Officer
Department of Neurology, AIIMS, New Delhi.
| S. No. | Title of the project |
|---|---|
| 1 | Role of Dynamic Susceptibility Perfusion and Dynamic Contrast Enhanced Perfusion Magnetic Resonance Imaging in characterization and grading of Gliomas |
| 2 | Role of Computed Tomography Perfusion in differentiation of post treatment effects from Tumor Recurrence in patients with high grade Gliomas: A Prospective descriptive Study. |
| 3 | Cerebral Pial Arteriovenous Fistulae: A Retrospective Analysis |
| S. No. | Title of the project |
|---|---|
| 1 | Role of Imaging in managing of Acute Ischemic Stroke: A Retrospective Analysis |
| 2 | Spinal Cord Diffusion Tensor Imaging in Intramedullary Neoplastic and Neoplastic Lesions: A Feasibility Study |
| 3 | Intracranial Dural Arteriovenous Fistulae: A Retrospective Analysis |
| 4 | Evaluation of findings on Magnetic Resonance imaging of Spinal Dural Arteriovenous Fistulae: A Retrospective Analysis |
| S. No. | Title of the project | Collaborating department/institution |
|---|---|---|
| 1 | Unraveling the causes of Stroke and Cognitive decline in the General Population- A cross-cultural perspective study | Dept. of Neurology, AIIMS, New Delhi |
| 2 | Prevalence of Symptomatic and asymptomatic coronary artery disease in patients with stroke and transient ischemic attacks | Dept. of Neurology, AIIMS, New Delhi |
| 3 | Intra-arterial chemotherapy for Retinoblastoma | Dept. of Opthalmology, RPC, AIIMS |
| S. No. | Title of the project | Collaborating department/institution |
|---|---|---|
| 1 | Assessment of white matter integrity through diffusion tensor imaging in schizophrenia patients with auditory hallucinations | Dept. of Psychiatry, AIIMS, New Delhi |
| 2 | Predictors of poor visual outcome at six months in patients with Idiopathic Intracranial hypertension | Dept. of Neurology, AIIMS, New Delhi |
| 3 | Randomized Two Arm Parallel Group Clinical trial to evaluate efficacy of trans-sphenoidal microscopic/endoscopic surgery using high field intra-operative magnetic resonance imaging guided resection as compared to two dimensional fluoroscopic guidance in extent of tumor resection in Non-functioning Pituitary macro-adenoma | Department of Neurosurgery, AIIMS, New Delhi |
| 4 | Distraction, Compression, Extension, Reduction (DCER) Combined With Joint Re-modelling and Extra-articular Distraction: Description of 2 New Modifications for Its Application in Basilar Invagination and Atlanto-Axial Dislocation: Prospective Study. | Department of Neurosurgery, AIIMS, New Delhi |
| 5 | Diffusion Tensor Imaging (DTI) tractography for prediction of facial nerve position in vestibular schwannoma and its intra-operative correlation. | Department of Neurosurgery, AIIMS, New Delhi |
| 6 | Cervical rotation before and after hinge-door cervical laminoplasty for cervical spondylotic myelopathy and its relation to post-operative axial neck symptoms. | Department of Neurosurgery, AIIMS, New Delhi |
| 7 | Outcome of Patients Undergoing Obliteration of Spinal Dural Arteriovenous Fistula and Role of Intra-operative Indocyanine Green Angiography | Department of Neurosurgery, AIIMS, New Delhi |
| S. No. | Title of the project | Name of Principal Investigator | Funded by (Name of funding agency) | Duration (years) | Start year–End year | Total funds sanctioned (Rs) |
|---|---|---|---|---|---|---|
| 1 | Efficacy of imaging assessment of neoangiogenesis and permeability to differentiate treatment related changes from tumor recurrence in high–grade glioma | Ajay Garg | ICMR | 3 | 2014-17 | 14 lacs |
| S. No. | Title of the project | Name of Principal Investigator | Funded by (Name of funding agency) | Duration (years) | Start year–End year | Total funds sanctioned (Rs) |
|---|---|---|---|---|---|---|
| 1 | Efficacy of Imaging Assessment of Neoangiogenesis and Permeability to Pre-operatively Grade Cerebral Glioma | Ajay Garg | Intramural Project | 2 | 2013-14 | 4.8 lacs |
| S. No. | Title of the project |
|---|---|
| 1 | Carotid Plaque Imaging in acute stroke |
| S. No. | Title of the project |
|---|---|
| 1 | Vein of Galen Aneurysmal Malformation -A Retrospective Study |
| 2 | Spinal Cord Arteriovenous Shunts-A Retrospective Analysis |
| S. No. | Title of the project | Collaborating department/institution |
|---|---|---|
| 1 | fMRI for memory evaluation in patients with Obstructive Sleep Apnea | Dept. of Medicine, AIIMS, New Delhi |
| 2 | Predictors of poor visual outcome at six months in patients with Idiopathic Intracranial hypertension | Dept. of Neurology, AIIMS, New Delhi |
| 3 | Unraveling the causes of Stroke and Cognitive decline in the General Population - A cross-cultural perspective study | Dept. of Neurology, AIIMS, New Delhi |
| 4 | Prevalence of Symptomatic and asymptomatic coronary artery disease in patients with stroke and transient ischemic attacks | Dept. of Neurology, AIIMS, New Delhi |
| 5 | Randomized Two Arm Parallel Group Clinical trial to evaluate efficacy of trans-sphenoidal microscopic/endoscopic surgery using high field intra-operative magnetic resonance imaging guided resection as compared to two dimensional fluoroscopic guidance in extent of tumor resection in Non-functioning Pituitary macro-adenoma | Department of Neurosurgery, AIIMS, New Delhi |
| 6 | Distraction, Compression, Extension, Reduction (DCER) Combined With Joint Re-modelling and Extra-articular Distraction: Description of 2 New Modifications for Its Application in Basilar Invagination and Atlanto-Axial Dislocation: Prospective Study. | Department of Neurosurgery, AIIMS, New Delhi |
| 7 | Assessment of white matter integrity through diffusion tensor imaging in schizophrenia patients with auditory hallucinations | Dept. of Psychiatry, AIIMS, New Delhi |
| 8 | Predictors of poor visual outcome at six months in patients with Idiopathic Intracranial hypertension | Dept. of Neurology, AIIMS, New Delhi |
| 9 | Intra-arterial chemotherapy for Retinoblastoma | Dept. of Opthalmology, RPC, AIIMS |
| S. No. | Title of the project | Collaborating department/institution |
|---|---|---|
| 1 | Arteriovenous malformations of Brain: Factors associated with post gamma knife radiation changes | Department of Neurosurgery, AIIMS, New Delhi |
| 2 | Intra medullary Spinal cord Tumours: Our experience of 100 cases and review of literature | Department of Neurosurgery, AIIMS, New Delhi |
| 3 | Primary Intradural extra medullary lesions: Five year experience at a tertiary care hospital- A retrospective study | Department of Neurosurgery, AIIMS, New Delhi |
| 4 | Retrospective analysis of operated cases of Giant Pituitary adenoma : An institutional experience | Department of Neurosurgery, AIIMS, New Delhi |
Duration: Three (03) years Residency training programme in Neuroanaesthesiology and Critical Care
Eligibility A candidate must possess MD / DNB (Anaesthesia) degree of a University recognized by Medical Council of India. The entrance exams are conducted in December and May every year.
For further information contact Examination Cell, AIIMS
Procedure of selection
For this program the candidate is selected through 2 step competitive examination held at national level.
Step-I Written examination of multiple choice questions based on MD (Anaesthesia), Critical Care and Basic Neuroanaesthesia. The candidates are short listed for step-II.
Step-II There is a departmental interview where candidates are examined to evaluate their clinical acumen and aptitude.
Final selection of the candidate is made on the bases of combined evaluation of step-I, and II
The candidates selected work as Senior Resident (non-DM) in the department. They are supposed to do all clinical work of OR, ICUs, and emergency both independently and also under supervision.
Teaching Program
Rotational Policy
There is a compulsory rotational policy for clinical exposure of the candidates to various sub-specialities of Anaesthesia and Intensive Care apart from Neuroanaesthesia, Neurotrauma, and Neurocritical Care. It is the only sub-speciality of Anaesthesia at AIIMS, New Delhi where the Senior Residents are exposed to most of the sub-specilalities of Anaesthesia. During the three years tenure the candidates are rotated to Trauma Anaesthesia (General, Ortho, and Neurotrauma) and Plastic Surgery at JPNA Trauma Centre, Onco-anaesthesia at BRA IRCH, General Anaesthesia including Laparoscopy, Transplant Surgery, Paediatric, Gynaecologic, ENT, and Ophthalmologic Anaesthesia at RPC.
A. SHORT-TERM TRAINING UPTO PERIOD OF SIX MONTHS
Training will be provided to the candidates sponsored by the Government/Autonomous Bodies or Institutions/Public Health Sector Organizations / MCI approved medical colleges and Government / Defence Services. The short-term training may not be allowed to the private practitioners.
B. SHORT-TERM TRAINING UPTO THE PERIOD OF SIX MONTHS TO THE FOREIGN NATIONALS CANDIDATES
The short-term training may be provided to the foreign national candidates sponsored by the foreign Government / Autonomous Bodies / Medical Institutions duly recommended by the Dean or any other competent authority of the concerned College / University / Institution.
C. LONG-TERM TRAINING SIX MONTHS TO TWO YEARS
This training will be provided to the candidates sponsored by the Government of India / Semi-Government / Autonomous Bodies / Institutions / Public Sector Organizations / Public Defense Services only. The long-term training is not allowed to the private practitioners / NGOs.
The persons with postgraduate degree and working on regular basis will be given preference.
The department of Neuroanaesthesiology and Critical Care at AIIMS is committed for advancement and promotion of Neuroanaesthesia and Neurocritical Care in India and abroad. The department regularly organizes a scientific event the “AIIMS Neuroanaesthesia Update”, every year starting from 2013. Eminent faculties of National and International repute along with AIIMS faculty participate in the meeting. It is a unique event where the anaesthetic procedures are telecasted live from the operation theatres and the delegates directly communicate with the anaesthesiologists and operating neurosurgeon as a part of the discussion. The department also started regular courses such as Cadaveric Hands-on Workshop on Airway Management and AIIMS Neurological Life Support (ANLS) with the target audience which includes emergency physicians, neurosurgeons, and neurologists apart from the anaesthesiologists. The department encourages faculty of national repute to deliver talks in the Neurosciences Centre based on recent neurosciences issues. The department also encourages faculty of International repute to be part of the departmental academic and research activities as a Visiting Professor.
For more details contact Dean / Registrar, Academic Section - II, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110 029, India
The department caters to the need of serious patients by admitting them. There are two general wards, one private ward and one ICU for neurology patients. There are 34 beds in each of the general wards located on the fourth floor (NS4) and the fifth floor (NS 5) and there are 12 beds in the private wards. For seeking admission in the general wards the patients are given dates by the senior resident incharge - admissions for admitting the patient. The patients are required to report at the prescribed date to the admitting resident at the mentioned time and place. They are then given admission slips which are presented at the central admissions and enquiry station. The charges are Rs. 375 (rupees three hundred and seventy five only) for ten days inclusive of food of the general wards. The admissions in the private wards are managed by the office of the Neurosciences centre and a probable date for admission is taken from this office. The patients are thereafter required to report to the central admissions for getting a room for admission. The private wards of neurology are in the cardio – neuro tower, a building which is next to the neurosciences centre. The charges of room in private wards are rupees twelve thousand and five hundred only(12,500/= for a period of ten days, food charges extra). Patients in general ward can also avail the food of the private wards by making the required payment.
| UNIT | NUMBER OF BEDS | SPECIALITY |
|---|---|---|
| UNIT I | 34 | Neurology |
| UNIT II | 34 | Neurology |
| ICU | 5 | Neurology |
| PRIVATE WARD | 7 | Neurology |
For entry into the DM and PhD courses the students can gather information from the website and the advertisements in the leading news Papers. The DM courses are three year courses and the entrance examination are conducted on an yearly or twice yearly basis depending on the number of seats.
The Department does not offer any special training apart from the DM courses, and the PhD Programs. Students from various teaching institutions outside and within India can apply for observer ship in the department through the academic section.
26.05.1965 to 26.02.1968
25.01.1969 to 24.09.1975
27.02.1968 to 03.07.1979
Jan 1976 to 01.11.1995
04.07.1979 to 30.04.2001
17.12.1979 to 17.12.1982
18.04.1984 to 30.06.2015
13.06.1984 to 19.07.1994
09.01.1985 to 31.08.2002
Sep 1992 to Sep 1993
16.07.1993 to 01.09.2003
Dec 1993 to May 1994
15.04.1996 to 07.04.1998
22.08.1998 to 11.10.1999
21.01.2000 to 01.10.2009
22.03.2001 to 14.01.2020
04.04.2001 to 27.01.2002
17.04.2001 to 12.05.2005
02.11.2016 to 31.07.2019
Dr. Rajendra Prasad Centre for Ophthalmic Sciences, named after the first President of India, Dr. Rajendra Prasad, was established on the 10th of March, 1967 as a National centre for ophthalmic science, to provide state of the art patient care, expand human resources for medical education and undertake research to find solutions to eye health problems of national importance.
Prof L P Agarwal was the visionary, who envisaged an eye center that would be at the fore front of eye health planning, academics and clinical care. It was designed keeping in mind the specific needs of India, and included the best features of leading ophthalmic centers around the world.
Prof L PAgarwal and the RPC were instrumental in making India the first country to start a National Programme for Prevention of visual impairment and Control of Blindness. The Centre formed the apex of the pyramid of Ophthalmic services in India, under this programme.
RPC has been recognized over the years, as a center of excellence by policy makers, professionals and the discerning public. All its expertise is available to the common man at highly subsidized rates or free.
The Centre is a constituent unit of the All India Institute of Medical Sciences, wherein it retains the fullest autonomy, while still keeping it within the mainstream of medical education and health care.
Dr.R.P. Centre continues to play a pivotal role in the National Programme for Control of Blindness. Faculty members of the Centre provide technical inputs at various forums that deliberate on policy planning and programme implementation. We have contributed our share in various blindness surveys and rapid assessments that have been conducted under the National Programme. As part of the Working Group, we have assisted in the framing of the Plan of Action under the Vision 2020 initiative. The Plan of Action shall guide the National Programme for Control of Blindness in the years to come. The Centre continues to foster partnerships with nongovernmental organizations engaged in the field of eye care. The centre has developed software for the National Registry of Eye Care infrastructure and human resources in India” this was done to support vision 2020 activities in India. This will be of immense use for policy planning in future.
Chiefs of Dr. R.P. Centre
| Prof. L.P. Agarwal (Founder) | 1967-79 |
| Prof. Madan Mohan | 1979-89 |
| Prof. P.K. Khosla | 1989-93 |
| Prof. Prem Prakash | 1993-96 |
| Prof. V.K. Dada | 1996-2001 |
| Prof. H.K. Tewari | 2001-04 |
| Prof. S. Ghose | 2004 - 5.10.2011 |
| Prof. R.V. Azad | Oct 2011-March 2014 |
| Prof. Y.R. Sharma | March 2014 -December 2015 |
| Prof. Atul Kumar | January 2016 to Aug 2021 |
| Prof. J.S. Titiyal | Sep 2021 to Date |
DM (Neuroanaesthesiology and Critical Care)
Duration: Three (03) years course
Eligibility A candidate must possess MD (Anaesthesia) degree of a University recognized by Medical Council of India. The entrance exams are conducted in December and May every year.
For further information contact Examination Cell, AIIMS
Procedure of selection
For this program the candidate is selected through 2 step competitive examination held at national level.
Step-I Written examination of multiple choice questions based on MD (Anaesthesia), Critical Care and Basic Neuroanaesthesia. The candidates are short listed for step-II.
Step-II There is a departmental interview where candidates are examined to evaluate their clinical acumen and aptitude.
Final selection of the candidate is made on the bases of combined evaluation of step-I, and II
The selected candidates work as Senior Resident (DM) in the department. They are supposed to do all clinical work of OR, ICUs, and emergency both independently and also under supervision. The candidate is expected to maintain a log book of all anaesthetic, postoperative, and critical care experience. They are supposed to write one dissertation to qualify to appear in final DM exam. The final DM examination to award the degree takes place after the end of 3rd year.
Teaching Program
1. Seminar
2. Journal Club
3 Clinical Case Presentations
Final Examination
The final examination to award the degree of DM (Neuroanaesthesiology and Critical Care) consists of following steps
1. Theory examination
a. Paper - 1
b. Paper - 2
c. Paper - 3
2. Practical
a. One long case
b. Two short cases
c. Grand Viva (Includes Drugs, Equipments, and Radiology)
Duration: One (01) year course
Eligibility A candidate must possess MD / DNB (Anaesthesia, Medicine) or MS (Surgery) degree of a University recognized by Medical Council of India with three years’ post PG experience in Neurosciences or having a degree of DM (Neuroanaesthesiology, Neurology), MCh (Neurosurgery). The entrance exams are conducted in December and May every year.
For further information contact Examination Cell, AIIMS
Procedure of selection
For this program the candidate is selected through 2 step competitive examination held at national level.
Step-I Written examination of multiple choice questions based on Neurocritical Care, Critical Care and Basic Neurosciences. The candidates are short listed for step-II.
Step-II There is a departmental interview where candidates are examined to evaluate their clinical acumen and aptitude.
Final selection of the candidate is made on the bases of combined evaluation of step-I, and II
The selected candidates work as Neurocritical Care Fellow in the Neuro ICUs. They are supposed to do all clinical work of Neurosurgery ICUs, Neurology ICU, Stroke Unit at Neurosciences centre and Neurotrauma ICU at JPNA Trauma Centre, both independently and also under supervision. The candidate is expected to maintain a log book of all critical care experience. The final fellowship examination to award the degree takes place after the end of one year.
Teaching Program
1. Seminar
2. Journal Club
3 Clinical Case Presentations
Final Examination
The final examination to award the degree of Post-Doctoral Fellowship (Neurocritical Care) consists of following steps
Practical Exam
a. One long case
b. Two short cases
c. Grand Viva (Includes Drugs, Equipments, and Radiology)
Year of admission: Feb. 2014
Course enrolled: Ph. D under Dr. K. Prasad
Year of admission: Feb. 2015
Course enrolled: Ph. D under Dr. K. Prasad
Year of admission: Aug. 2014
Course enrolled: Ph. D under Dr. K. Prasad
Year of admission: Aug. 2014
Course enrolled: Ph. D under Dr. K. Prasad
Year of admission: Aug. 2014
Course enrolled: Ph. D under Dr. K. Prasad
Year of admission: July 2014
Course enrolled: Ph. D under Dr. M.V. Padma
Year of admission: Feb. 2014
Course enrolled: Ph. D under Dr. M. Tripathi
Year of admission: Feb. 2015
Course enrolled: Ph. D under Dr. M. Tripathi
Year of admission: Feb. 2013
Course enrolled: Ph. D under Dr. Vinay Goyal
Year of admission: Feb. 2013
Course enrolled: Ph. D under Dr. Achal
Year of admission: Feb. 2014
Course enrolled: Ph. D under Dr. Achal
Year of admission: Feb. 2014
Course enrolled: Ph. D under Dr. Achal
Year of admission: Aug. 2014
Course enrolled: Ph. D under Dr. Achal
Year of admission: Aug.2014
Course enrolled: Ph. D under Dr. Achal
Year of admission: Feb. 2014
Course enrolled: Ph. D under Dr. Rohit Bhatia
Year of admission: Feb. 2016
Course enrolled: Ph. D under Dr. Rohit Bhatia
Year of admission: Aug. 2016
Course enrolled: Ph. D under Dr. Deepti Vibha
Year of admission: July. 2019
Course enrolled: Ph. D under Dr. Vishnu V.Y
Year of admission: July. 2019
Course enrolled: Ph. D under Dr. Roopa Rajan
Year of admission: July. 2019
Course enrolled: Ph. D under Dr. Roopa Rajan
Substance Use Prevention: Resource Material for Parents and Adolescents

The Drug Dependence Treatment Centre, AIIMS was established in the year 1988 and was functional from the premises of the Deen Dayal Upadhyay Hospital, New Delhi. In 2003 it was upgraded as the National Centre (National Drug Dependence Treatment Centre) and is fully operational from its new premises in Ghaziabad, Delhi-NCR since April 2003.
The National Drug Treatment Centre, Ghaziabad (NDDTC), AIIMS has been established as the apex centre for treatment of drugs and substance abuse disorders in the country. It provides a state of art model for de‐addiction treatments. This centre has full range of specialists & facilities. The NDDTC is situated on 10 acre beautiful campus near CGO Complex at Ghaziabad, Delhi-NCR. It is presently having 50 bedded treatment facilities with expansion plan for the future.
The centre has well qualified multi-disciplinary faculty and staff (medical doctors, pre-clinical scientists, social scientists, research staff, nursing staff, laboratory personnel and administrative staff) to render various modalities of care. Clinical care is provided through outpatient, inpatient settings and community clinics. Help is available for the treatment of disorders related to use of all the substances i.e. Alcohol, Opioids, Cannabis, Tobacco etc. and behavioral addictions. Treatment modalities include both pharmacological (i.e. with medications) and non-pharmacological (i.e. psychological / social) treatments. Both medically assisted and drug-free treatment related to drug use, and long-term supervised medications (Buprenorphine/Methadone/Naltrexone maintenance therapy) are provided. The centre carries out the relevant hematological, biochemical laboratory tests to monitor health damage. Further, several drugs of abuse are screened simultaneously through analysis of patients’ urine sample.
The centre has been involved in:
The centre provides clinical care to about 4000 new patients and about 35000 old patients every year. It also provides clinical care to about 33000 patients in its community clinic. In addition, every year about 600 patients are seen in Tobacco use cessation clinic, about 40 patients in adolescent clinic and about 300 patients in dual diagnosis clinic.
The years 1999-2012 saw much growth and many achievements for the centre. The centre has developed curricula, training schedules, modalities and resource materials for training of trainers, Medical Doctors (GDMOs), nurses and laboratory personnel. Between January 1989 and October 2007, about 40 courses for doctors have been organized. Various manuals for doctors are available. The training programmes have been reviewed and modified through workshops of resource persons.
Besides clinical care, NDDTC has been involved in a multitude of other areas. Right from its inception, NDDTC has played a leadership role in the country and has worked on development of various replicable models of care, training of post-graduate psychiatry students and health professionals, development of resource materials, research and policy planning.
Following is a brief overview of recent contributions:
Faculty members from NDDTC are members of various expert committees and technical groups at regional and international level, and contributing to policy development. The Ex-Chief of the Centre was a member of the International Narcotics Control Board (INCB), the monitoring body for the implementation of the United Nations international drug control conventions.
Other significant achievements of the centre are:
| Officer Name | Contact |
|---|---|
| Mr. Gopal Datt Sharma Jr. Administrative Officer & P.S. (Officiating) | (+91-11-26589695) (+91-11-26593101) Fax: 91-11-26588919 Email: ps.chiefrpc[at]gmail[dot]com |
| Mr. Narender Kumar Nagar Sr. Administrative Assistant |
Dr. Rajendra Prasad Centre for Ophthalmic Sciences
All India Institute of Medical Sciences (AIIMS)
Ansari Nagar
New Delhi – 110029 (India)
| Reception & Inquiry Number | Address |
|---|---|
| +91-11-26593012) | Dr. Rajendra Prasad Centre for Ophthalmic Sciences All India Institute of Medical Sciences (AIIMS) Ansari Nagar New Delhi – 110029 (India) |
Substance Use Prevention: Resource Material for Parents and Adolescents
The Drug Dependence Treatment Centre, AIIMS was established in the year 1988 and was functional from the premises of the Deen Dayal Upadhyay Hospital, New Delhi. In 2003 it was upgraded as the National Centre (National Drug Dependence Treatment Centre) and is fully operational from its new premises in Ghaziabad, Delhi-NCR since April 2003.
The National Drug Treatment Centre, Ghaziabad (NDDTC), AIIMS has been established as the apex centre for treatment of drugs and substance abuse disorders in the country. It provides a state of art model for de‐addiction treatments. This centre has full range of specialists & facilities. The NDDTC is situated on 10 acre beautiful campus near CGO Complex at Ghaziabad, Delhi-NCR. It is presently having 50 bedded treatment facilities with expansion plan for the future.
The centre has well qualified multi-disciplinary faculty and staff (medical doctors, pre-clinical scientists, social scientists, research staff, nursing staff, laboratory personnel and administrative staff) to render various modalities of care. Clinical care is provided through outpatient, inpatient settings and community clinics. Help is available for the treatment of disorders related to use of all the substances i.e. Alcohol, Opioids, Cannabis, Tobacco etc. and behavioral addictions. Treatment modalities include both pharmacological (i.e. with medications) and non-pharmacological (i.e. psychological / social) treatments. Both medically assisted and drug-free treatment related to drug use, and long-term supervised medications (Buprenorphine/Methadone/Naltrexone maintenance therapy) are provided. The centre carries out the relevant hematological, biochemical laboratory tests to monitor health damage. Further, several drugs of abuse are screened simultaneously through analysis of patients’ urine sample.
The centre has been involved in:
The centre provides clinical care to about 4000 new patients and about 35000 old patients every year. It also provides clinical care to about 33000 patients in its community clinic. In addition, every year about 600 patients are seen in Tobacco use cessation clinic, about 40 patients in adolescent clinic and about 300 patients in dual diagnosis clinic.
The years 1999-2012 saw much growth and many achievements for the centre. The centre has developed curricula, training schedules, modalities and resource materials for training of trainers, Medical Doctors (GDMOs), nurses and laboratory personnel. Between January 1989 and October 2007, about 40 courses for doctors have been organized. Various manuals for doctors are available. The training programmes have been reviewed and modified through workshops of resource persons.
Besides clinical care, NDDTC has been involved in a multitude of other areas. Right from its inception, NDDTC has played a leadership role in the country and has worked on development of various replicable models of care, training of post-graduate psychiatry students and health professionals, development of resource materials, research and policy planning.
Following is a brief overview of recent contributions:
Faculty members from NDDTC are members of various expert committees and technical groups at regional and international level, and contributing to policy development. The Ex-Chief of the Centre was a member of the International Narcotics Control Board (INCB), the monitoring body for the implementation of the United Nations international drug control conventions.
Other significant achievements of the centre are:
Duration: Three (03) years course
Eligibility A candidate must possess MD (Anaesthesia) degree of a University recognized by Medical Council of India. The entrance exams are conducted in December and May every year.
For further information contact Examination Cell, AIIMS
Procedure of selection
For this program the candidate is selected through 2 step competitive examination held at national level.
Step-I Written examination of multiple choice questions based on MD (Anaesthesia), Critical Care and Basic Neuroanaesthesia. The candidates are short listed for step-II.
Step-II There is a departmental interview where candidates are examined to evaluate their clinical acumen and aptitude.
Final selection of the candidate is made on the bases of combined evaluation of step-I, and II
The selected candidates work as Senior Resident (DM) in the department. They are supposed to do all clinical work of OR, ICUs, and emergency both independently and also under supervision. The candidate is expected to maintain a log book of all anaesthetic, postoperative, and critical care experience. They are supposed to write one dissertation to qualify to appear in final DM exam. The final DM examination to award the degree takes place after the end of 3rd year.
Teaching Program
Final Examination
The final examination to award the degree of DM (Neuroanaesthesiology and Critical Care) consists of following steps
Duration: One (01) year course
Eligibility A candidate must possess MD / DNB (Anaesthesia, Medicine) or MS (Surgery) degree of a University recognized by Medical Council of India with three years’ post PG experience in Neurosciences or having a degree of DM (Neuroanaesthesiology, Neurology), MCh (Neurosurgery). The entrance exams are conducted in December and May every year.
For further information contact Examination Cell, AIIMS
Procedure of selection
For this program the candidate is selected through 2 step competitive examination held at national level.
Final selection of the candidate is made on the bases of combined evaluation of step-I, and II
The selected candidates work as Neurocritical Care Fellow in the Neuro ICUs. They are supposed to do all clinical work of Neurosurgery ICUs, Neurology ICU, Stroke Unit at Neurosciences centre and Neurotrauma ICU at JPNA Trauma Centre, both independently and also under supervision. The candidate is expected to maintain a log book of all critical care experience. The final fellowship examination to award the degree takes place after the end of one year.
Teaching Program
Final Examination
The final examination to award the degree of Post-Doctoral Fellowship (Neurocritical Care) consists of following steps
Practical Exam
| Chief, Dr.R.P.Centre |
| Prof Jeewan Singh Titiyal |
| Medical Superintendent |
| Dr. D.K.Sharma |
| Sr. Administrative Officer |
| Ms. Saroj Pant |
| Accounts Officer |
| Shri Shivanand Thakur |
| Stores Officer |
| Mrs. Archana Sharma |
| July 2022 | Jan 2022 |
|---|---|
Dr. Sahaj Agarwal, Dr. Kanukuntala Saikrishna, Dr. Yamini Priyanka, Dr. Siddharth S, Dr. Farsana Mustafa, Dr. Ashem Thoibisana, Dr. Punith SB | Dr. Vedang Desai, Dr. Shiny Joy, Dr. Prachi Mohapatra, Dr. Abhishek Vaigankar, Dr. Sampurna Chowdhury |
| July 2021 | Jan 2021 |
|---|---|
Dr. Pinki Chatterpal, Dr. Chandu Meena, Dr. Manda Goveen, Dr. Sohini Chakraborty, Dr. Chitrangada Yadav | Dr. Ashfak Alam, Dr. Pooja Anand, Dr. Mohit Mann, Dr. Abutahir Shaikh, Dr. Abhishek Anand, Dr. Baikuntha Panigrahi |
| July 2020 | Jan 2020 |
|---|---|
Dr. Jerry George, Dr. Pritam Majumdar, Dr. Rahul Chawla, Dr. Aminu Aliyar | Dr. Billa Srujana, Dr. Kamalesh Tayede, Dr. Saman Fatima, Dr. Ayush Mohan Makkar, Dr. Parkipandala Sathish, Dr. Saranya B. Gomathy |
| Name | Month/Year of Completion | |
|---|---|---|
| Dr. Girija Prasad Rath | June 2005 | girijarath@yahoo.co.in |
| Dr. M. Radhakrishnan | June 2005 | mrks1973@yahoo.com |
| Dr. Indranil Ghosh | June 2006 | ghoshindranilghosh@rediffmail.com |
| Dr. Mukesh Mohan Gupta | June 2006 | drmukeshmohangupta@yahoo.co.in |
| Dr. Deepak Sharma | December 2006 | dsharma@u.washington.edu |
| Dr. Hemant Bhagat | December 2006 | drhemantbhagat@rediffmail.com |
| Dr. Virendra Jain | June 2008 | vjain_01@yahoo.com |
| Dr. Pradeep Kumar Lai (S) | December 2008 | drlaithangba@gmail.com |
| Dr. Deepak Singh | December 2008 | drdeepakaims@gmail.com |
| Dr. Zulfiqar Ali (S) | December 2008 | zulfiqaraliiii@yahoo.com |
| Dr. Prasanna Bidkar | June 2009 | drprasannabidkar@gmail.com |
| Dr. Manish Kumar Marda | December 2009 | drmmarda@gmail.com |
| Dr. Gyaninder Pal Singh | June 2010 | drsingh_gp@yahoo.co.in |
| Dr. Rahul Yadav (S) | June 2011 | docrahulyadav@gmail.com |
| Dr. Ashish Bindra | December 2011 | dr_ashi2208@yahoo.com |
| Dr. Sachidanand Jee Bharti | December 2011 | sachidadr@yahoo.co.in |
| Dr. Tumul Chowdhury | December 2011 | tumulthunder@gmail.com |
| Dr. Keshav Goyal | December 2011 | keshavgoyal@yahoo.co.in |
| Dr. Charu Mahajan | June 2012 | charushrikul@gmail.com |
| Dr. B. Kiran Reddy | June 2012 | reddykiranb@rediffmail.com |
| Dr. Navdeep Sokhal | December 2012 | drnavdeep_kumar@yahoo.com |
| Dr. Nidhi Gupta | June 2013 | neurodmrenu@yahoo.com |
| Dr. Vivek Bharti Sharma | June 2013 | drnidhisrivastava2@gmail.com |
| Dr. Renu Bala (S) | December 2013 | vbs_rashmi@yahoo.co.in |
| Dr. Surya Kumar Dube | June 2014 | surya.dube@gmail.com |
| Dr. Bhavna Hooda (S) | December 2014 | bhavnahooda2007@rediffmail.com |
| Dr. Vanitha Rajagopalan | December 2014 | varun2202@yahoo.com |
| Dr. Varun Jain | December 2014 | varun2202@yahoo.com |
| Dr. Priyanka Gupta | December 2014 | drpriyankagupta84@gmail.com |
| Dr. Ankur Luthra | December 2014 | anki_979@yahoo.co.in |
| Dr. Shailendra Kumar | June 2015 | drshail.kumar@gmail.com |
| Dr. Sujoy Banik | December 2015 | drsujoyb@gmail.com |
| Dr. Ranadhir Mitra | June 2016 | ranascb@yahoo.com |
| Dr. Nayani Radhakrishna | June 2017 | nayani.rk@gmail.com |
| Dr. Vikash Chauhan | December 2017 | vikas.max@gmail.com |
| Dr. Gaurav Singh Tomar | December 2017 | spunkygst@gmail.com |
| Dr. Shalendra Singh | December 2017 | drsinghafmc@yahoo.co.in |
| Dr. Devika Bhardwaj | December 2018 | devika0204@gmail.com |
| Dr. Barkha Bindu | December 2018 | barkha.gmh@yahoo.co.in |
| Dr. Suman Sokhal | December 2018 | drsokhal@yahoo.co.in |
| Dr. Nitasha Mishra | December 2018 | nitsmishra@gmail.com |
Dr. Rajendra Prasad Centre for Ophthalmic Sciences has been recognized as the Apex Organisation by the Government of India under the National Programme for the Control of Blindness.
This programme was launched in 1976 to combat blindness problem in India with the objectives of:
The Centre also assists the Ministry of Health in short term and long term planning and evaluation of the programme. It undertakes and plans epidemiological investigations and provides technical leadership to the entire nation.
The Centre is actively collaborating with various National and International agencies like ICMR, WHO and others in various fields of clinical, applied and basic research. It has also been designated as a WHO Collaborating Centre.
NEURO ANAESTHESIA OPD
| Name of the Lab | Test Done | Details & Rates in Indian Rupees (INR) | |
|---|---|---|---|
| FD20-FD20 (LAB-2) | Digital Subtraction Angiography, Neurovascular interventions | Consumables to be brought by the patient | |
| Gamma Knife Angiogram | Payment included in gamma knife package | ||
| ARTIZEE (LAB-1) | Flat panel DSA system | Consumables to be brought by the patient | |
| DEFINITION EDGE (Room No 21, Cath lab complex) | CT Emergency | Free in first 24-hours | |
| CT Routine | General Ward | Private ward | |
| Head | 200* | 500* | |
| Chest or abdomen | 750* | 1500* | |
| Spine | 750* | 1500* | |
| * Consumables to be brought by the patient | |||
| Portable Ultrasound (CX30, CX 50) | Ultrasound | 200 | |
| Doppler examination | 300 | ||
| NMR (GK FACILITY) | MRI head or Spine | 2500 (IPD) & 3000 (OPD) | |
| MR Angiography | 2500 (IPD) & 3000 (OPD) | ||
| Additional Study | 1500 | ||
| Contrast | 2000 for >12 years | ||
| MR (Gamma Knife & X-Knife) | Payment included in gamma knife package | ||
| DIGITAL X-RAYS Room No.56 | Plain X-rays OPD/indoor | Rs 30 for each X-ray film | |
| AGRGOMETER | DSA LAB | Nil | |
| CREATINE METER | DSA LAB | Nil | |
Duration: Three (03) years Residency training programme in Neuroanaesthesiology and Critical Care
Eligibility A candidate must possess MD / DNB (Anaesthesia) degree of a University recognized by Medical Council of India. The entrance exams are conducted in December and May every year.
For further information contact Examination Cell, AIIMS
For this program the candidate is selected through 2 step competitive examination held at national level.
Step-I Written examination of multiple choice questions based on MD (Anaesthesia), Critical Care and Basic Neuroanaesthesia. The candidates are short listed for step-II.
Step-II There is a departmental interview where candidates are examined to evaluate their clinical acumen and aptitude.
Final selection of the candidate is made on the bases of combined evaluation of step-I, and II
The candidates selected work as Senior Resident (non-DM) in the department. They are supposed to do all clinical work of OR, ICUs, and emergency both independently and also under supervision.
1. Seminar
2. Journal Club
3 Clinical Case Presentations
There is a compulsory rotational policy for clinical exposure of the candidates to various sub-specialities of Anaesthesia and Intensive Care apart from Neuroanaesthesia, Neurotrauma, and Neurocritical Care. It is the only sub-speciality of Anaesthesia at AIIMS, New Delhi where the Senior Residents are exposed to most of the sub-specilalities of Anaesthesia. During the three years tenure the candidates are rotated to Trauma Anaesthesia (General, Ortho, and Neurotrauma) and Plastic Surgery at JPNA Trauma Centre, Onco-anaesthesia at BRA IRCH, General Anaesthesia including Laparoscopy, Transplant Surgery, Paediatric, Gynaecologic, ENT, and Ophthalmologic Anaesthesia at RPC.
Training will be provided to the candidates sponsored by the Government/Autonomous Bodies or Institutions/Public Health Sector Organizations / MCI approved medical colleges and Government / Defence Services. The short-term training may not be allowed to the private practitioners.
·Fee: - A fee of Rs.1, 000/- per month will be charged from the trainees (Indian citizens) and a fee of Indian Rupees equivalent to US $200 will be charged from the foreign nationals/citizens. However, the candidates sponsored by the Defence Services only will not be charged any fee.
·At a given time the number of long-term / short-term trainees in a particular department should not exceed 50% of the sanctioned strength of faculty of that department.
The short-term training may be provided to the foreign national candidates sponsored by the foreign Government / Autonomous Bodies / Medical Institutions duly recommended by the Dean or any other competent authority of the concerned College / University / Institution.
·A fee of US $ 200 per month will be charged from the foreign national candidates.
·There will be no financial obligations on the part of the Institute / Govt. of India.
·No accommodation etc. will be provided to the trainees.
·If the foreign nationals want hands on training, approval of MCI is necessary.
This training will be provided to the candidates sponsored by the Government of India / Semi-Government / Autonomous Bodies / Institutions / Public Sector Organizations / Public Defense Services only. The long-term training is not allowed to the private practitioners / NGOs.
The persons with postgraduate degree and working on regular basis will be given preference.
·Fee: - A fee of Rs.1,000/- per month will be charged from the trainees (Indian citizens) and a fee of Indian Rupees equivalent to US $200 will be charged from the foreign nationals/citizens. However, the candidates sponsored by the Defence Services only will not be charged any fee.
·At a given time the number of long-term/short-term trainees in a particular department should not exceed 50% of the sanctioned strength of faculty of that department.
·The foreign nationals / citizens trainees will be treated as Observers and not allowed hands on training without prior permission of the Medical Council of India. If the foreign national trainees want hands on training then the approval of the MCI is necessary.
The department of Neuroanaesthesiology and Critical Care at AIIMS is committed for advancement and promotion of Neuroanaesthesia and Neurocritical Care in India and abroad. The department regularly organizes a scientific event the “AIIMS Neuroanaesthesia Update”, every year starting from 2013. Eminent faculties of National and International repute along with AIIMS faculty participate in the meeting. It is a unique event where the anaesthetic procedures are telecasted live from the operation theatres and the delegates directly communicate with the anaesthesiologists and operating neurosurgeon as a part of the discussion. The department also started regular courses such as Cadaveric Hands-on Workshop on Airway Management and AIIMS Neurological Life Support (ANLS) with the target audience which includes emergency physicians, neurosurgeons, and neurologists apart from the anaesthesiologists. The department encourages faculty of national repute to deliver talks in the Neurosciences Centre based on recent neurosciences issues. The department also encourages faculty of International repute to be part of the departmental academic and research activities as a Visiting Professor.
For more details contact Dean / Registrar, Academic Section - II, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110 029, India
Duration: Three (03) years Residency training programme in Neuroanaesthesiology and Critical Care
Eligibility A candidate must possess MD / DNB (Anaesthesia) degree of a University recognized by Medical Council of India. The entrance exams are conducted in December and May every year.
For further information contact Examination Cell, AIIMS
For this program the candidate is selected through 2 step competitive examination held at national level.
Step-I Written examination of multiple choice questions based on MD (Anaesthesia), Critical Care and Basic Neuroanaesthesia. The candidates are short listed for step-II.
Step-II There is a departmental interview where candidates are examined to evaluate their clinical acumen and aptitude.
Final selection of the candidate is made on the bases of combined evaluation of step-I, and II
The candidates selected work as Senior Resident (non-DM) in the department. They are supposed to do all clinical work of OR, ICUs, and emergency both independently and also under supervision.
1. Seminar
2. Journal Club
3 Clinical Case Presentations
There is a compulsory rotational policy for clinical exposure of the candidates to various sub-specialities of Anaesthesia and Intensive Care apart from Neuroanaesthesia, Neurotrauma, and Neurocritical Care. It is the only sub-speciality of Anaesthesia at AIIMS, New Delhi where the Senior Residents are exposed to most of the sub-specilalities of Anaesthesia. During the three years tenure the candidates are rotated to Trauma Anaesthesia (General, Ortho, and Neurotrauma) and Plastic Surgery at JPNA Trauma Centre, Onco-anaesthesia at BRA IRCH, General Anaesthesia including Laparoscopy, Transplant Surgery, Paediatric, Gynaecologic, ENT, and Ophthalmologic Anaesthesia at RPC.
Training will be provided to the candidates sponsored by the Government/Autonomous Bodies or Institutions/Public Health Sector Organizations / MCI approved medical colleges and Government / Defence Services. The short-term training may not be allowed to the private practitioners.
·Fee: - A fee of Rs.1, 000/- per month will be charged from the trainees (Indian citizens) and a fee of Indian Rupees equivalent to US $200 will be charged from the foreign nationals/citizens. However, the candidates sponsored by the Defence Services only will not be charged any fee.
·At a given time the number of long-term / short-term trainees in a particular department should not exceed 50% of the sanctioned strength of faculty of that department.
The short-term training may be provided to the foreign national candidates sponsored by the foreign Government / Autonomous Bodies / Medical Institutions duly recommended by the Dean or any other competent authority of the concerned College / University / Institution.
·A fee of US $ 200 per month will be charged from the foreign national candidates.
·There will be no financial obligations on the part of the Institute / Govt. of India.
·No accommodation etc. will be provided to the trainees.
·If the foreign nationals want hands on training, approval of MCI is necessary.
This training will be provided to the candidates sponsored by the Government of India / Semi-Government / Autonomous Bodies / Institutions / Public Sector Organizations / Public Defense Services only. The long-term training is not allowed to the private practitioners / NGOs.
The persons with postgraduate degree and working on regular basis will be given preference.
·Fee: - A fee of Rs.1,000/- per month will be charged from the trainees (Indian citizens) and a fee of Indian Rupees equivalent to US $200 will be charged from the foreign nationals/citizens. However, the candidates sponsored by the Defence Services only will not be charged any fee.
·At a given time the number of long-term/short-term trainees in a particular department should not exceed 50% of the sanctioned strength of faculty of that department.
·The foreign nationals / citizens trainees will be treated as Observers and not allowed hands on training without prior permission of the Medical Council of India. If the foreign national trainees want hands on training then the approval of the MCI is necessary.
The department of Neuroanaesthesiology and Critical Care at AIIMS is committed for advancement and promotion of Neuroanaesthesia and Neurocritical Care in India and abroad. The department regularly organizes a scientific event the “AIIMS Neuroanaesthesia Update”, every year starting from 2013. Eminent faculties of National and International repute along with AIIMS faculty participate in the meeting. It is a unique event where the anaesthetic procedures are telecasted live from the operation theatres and the delegates directly communicate with the anaesthesiologists and operating neurosurgeon as a part of the discussion. The department also started regular courses such as Cadaveric Hands-on Workshop on Airway Management and AIIMS Neurological Life Support (ANLS) with the target audience which includes emergency physicians, neurosurgeons, and neurologists apart from the anaesthesiologists. The department encourages faculty of national repute to deliver talks in the Neurosciences Centre based on recent neurosciences issues. The department also encourages faculty of International repute to be part of the departmental academic and research activities as a Visiting Professor.
For more details contact Dean / Registrar, Academic Section - II, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110 029, India
| S. No | Name of the Course | Details of Admission |
|---|---|---|
| 1. | D.M. (Neuroimaging & Interventional Neuroradiology) One general seat every 6-months; one sponsored seat every year | Eligibility: M D in Radiology or its equivalent from a recognized institution Upper Age Limit: 35 years Duration of the course: Three years Selection Criteria a) All India advertisement b) Screening of application for compliance of basic qualification & career grading c) Objectives test for grading aptitude & merit. (90 minutes examination, 100 multiple choice questions) d) Departmental interview for assessment of past performance, curricular ability to imbibe training & interactive abilities e) Final interview by institutional board headed by the Director |
Dr. Shashank Sharad Kale
Professor Neurosurgery
Office Phone number: 26594888
Email address: skale67@gmail.com
Striving to provide comprehensive spine care at the Neurosurgery Department AIIMS by dealing with complex cervical, occipito-cervical, thoracic, lumbar and sacral pathologies, tumors, and fusion and fixation, operations has been a constant endeavor. The department is now fully equipped to deal with complex spinal problems with the latest technological advances including Image guided workstation. The minimal access system for spinal surgery is being procured. A research laboratory with facility for cadaver dissection and spinal operations on experimental animals with drill, microscope and computer aids is under development has been developed.
My special area of interest is the cranio-vertebral junction. I have documented one of the largest series of patients in the world on developmental CVJunction anomalies and their management- almost 800 patients. Research on TB of the CV Junction – experience of 75 patients is under consideration for publication. Research of spinal TB with severe neurological deficits in 45 patients has been accepted for publication in Journal of Neurosurgery Spine. In the last 3years I have been invited to lecture/chair sessions/seminars on spine surgery topics all over the country and in international meetings. I have been nominated the Course Chairman for the AOSpine courses at Davos Switzerland attended by more than 300 spine surgeons from 80 countries in the world.
OPD Schedule: Neurosurgery Unit II Tuesday 9 AM to 12 AM, Saturday 9 AM to 12 AM
Inpatients: NS2 ward
Operation Theatre: NSOT First Floor CN Centre
Unit: Neurosurgery Unit II
Number of Beds: 47 + Private Wards
Research Projects: Intra-tumoral drug delivery for anaplastic astrocytoma trial; Cervical spondylotic myelopathy
multi-centric trial
Stenographer with The HOD Neurology
LDC (Ad - hoc)
Attendent
LDC
LDC (Ad Hoc)
Data entry operator (Under Project)
Lab Attendent
Stenographer with Prof. Kameshwar Prasad
Data entry operator with Dr K. Prasad
Project assistant with Prof K Prasad
Field investigator with Prof K Prasad.
Project assistant with Prof MV Padma
Field Worker with Dr. M.Tripathi (Project)
Technical Officer (EPS Lab)
Technical Assistant (EPS Lab)
Lab Technician (EPS Lab)
Lab Technician (EPS Lab)
Lab Technician (EPS Lab)
Lab Technician
LDC (EPS Lab)
Attendent (EPS Lab)
Hospital Attendant
Professor & Head of the Department
Professor
Professor
Professor
Professor
Associate Professor
Associate Professor
Associate Professor
Associate Professor
Assistant Professor
Assistant Professor
Assistant Professor
Assistant Professor
Assistant Professor (Contract)
Senior resident (DM student)
Date of Joining: 10.7.2014
Senior resident (DM student)
Date of Joining: 1.1.2015
Senior resident
Date of Joining: 24.8.2015
Senior resident
Date of Joining: 1.9.2015
Senior resident
Date of Joining: 28.2.2015
Senior resident
Date of Joining: 9.10.2015
Senior resident (DM student)
Date of Joining: 1.1.2016
Senior resident (DM student)
Date of Joining: 30.1.2016
The following academic courses are conducted by the department:
Duration: Three (03) years course
Eligibility A candidate must possess MD (Anaesthesia) degree of a University recognized by Medical Council of India. The entrance exams are conducted in December and May every year.
For further information contact Examination Cell, AIIMS
For this program the candidate is selected through 2 step competitive examination held at national level.
Step-I Written examination of multiple choice questions based on MD (Anaesthesia), Critical Care and Basic Neuroanaesthesia. The candidates are short listed for step-II.
Step-II There is a departmental interview where candidates are examined to evaluate their clinical acumen and aptitude.
Final selection of the candidate is made on the bases of combined evaluation of step-I, and II
The selected candidates work as Senior Resident (DM) in the department. They are supposed to do all clinical work of OR, ICUs, and emergency both independently and also under supervision. The candidate is expected to maintain a log book of all anaesthetic, postoperative, and critical care experience. They are supposed to write one dissertation to qualify to appear in final DM exam. The final DM examination to award the degree takes place after the end of 3rd year.
1. Seminar
2. Journal Club
3 Clinical Case Presentations
The final examination to award the degree of DM (Neuroanaesthesiology and Critical Care) consists of following steps
a. Paper - 1
b. Paper - 2
c. Paper - 3
a. One long case
b. Two short cases
c. Grand Viva (Includes Drugs, Equipments, and Radiology)
Duration: One (01) year course
Eligibility A candidate must possess MD / DNB (Anaesthesia, Medicine) or MS (Surgery) degree of a University recognized by Medical Council of India with three years’ post PG experience in Neurosciences or having a degree of DM (Neuroanaesthesiology, Neurology), MCh (Neurosurgery). The entrance exams are conducted in December and May every year.
For further information contact Examination Cell, AIIMS
For this program the candidate is selected through 2 step competitive examination held at national level.
Step-I Written examination of multiple choice questions based on Neurocritical Care, Critical Care and Basic Neurosciences. The candidates are short listed for step-II.
Step-II There is a departmental interview where candidates are examined to evaluate their clinical acumen and aptitude.
Final selection of the candidate is made on the bases of combined evaluation of step-I, and II
The selected candidates work as Neurocritical Care Fellow in the Neuro ICUs. They are supposed to do all clinical work of Neurosurgery ICUs, Neurology ICU, Stroke Unit at Neurosciences centre and Neurotrauma ICU at JPNA Trauma Centre, both independently and also under supervision. The candidate is expected to maintain a log book of all critical care experience. The final fellowship examination to award the degree takes place after the end of one year.
1. Seminar
2. Journal Club
3 Clinical Case Presentations
The final examination to award the degree of Post-Doctoral Fellowship (Neurocritical Care) consists of following steps
a. One long case
b. Two short cases
c. Grand Viva (Includes Drugs, Equipments, and Radiology)
Professor & Head
1957-1994
Asstt. Professor
1987-1994
Asstt. Professor
1997-1999
Asstt. Professor
1995-1997
Assoc. Professor
2001-2005
Professor & Head
1979-2016
Asstt. Professor
2016-2017
Year of Completion: June 2005
girijarath[at]yahoo[dot]co[dot]in
Year of Completion: June 2005
mrks1973[at]yahoo[dot]com
Year of Completion: June 2006
ghoshindranilghosh[at]rediffmail[dot]com
Year of Completion: June 2006
drmukeshmohangupta[at]yahoo[dot]co[dot]in
Year of Completion: December 2006
dsharma@u.washington.edu
Year of Completion: December 2006
drhemantbhagat[at]rediffmail[dot]com
Year of Completion: June 2008
vjain_01[at]yahoo[dot]com
Year of Completion: December 2008
drlaithangba[at]gmail[dot]com
Year of Completion: December 2008
drdeepakaims[at]gmail[dot]com
Year of Completion: December 2008
zulfiqaraliiii[at]yahoo[dot]com
Year of Completion: June 2009
drprasannabidkar[at]gmail[dot]com
Year of Completion: December 2009
drmmarda[at]gmail[dot]com
Year of Completion: June 2010
drsingh_gp[at]yahoo[dot]co[dot]in
Year of Completion: June 2011
docrahulyadav[at]gmail[dot]com
Year of Completion: December 2011
dr_ashi2208[at]yahoo[dot]com
Year of Completion: December 2011
sachidadr[at]yahoo[dot]co[dot]in
Year of Completion: December 2011
tumulthunder[at]gmail[dot]com
Year of Completion: December 2011
keshavgoyal[at]yahoo[dot]co[dot]in
Year of Completion: June 2012
charushrikul[at]gmail[dot]com
Year of Completion: June 2012
reddykiranb[at]rediffmail[dot]com
Year of Completion: December 2012
drnavdeep_kumar[at]yahoo[dot]com
Year of Completion: June 2013
neurodmrenu[at]yahoo[dot]com
Year of Completion: June 2013
drnidhisrivastava2[at]gmail[dot]com
Year of Completion: December 2013
vbs_rashmi[at]yahoo[dot]co[dot]in
Year of Completion: June 2014
surya.dube[at]gmail[dot]com
Year of Completion: December 2014
bhavnahooda2007[at]rediffmail[dot]com
Year of Completion: December 2014
varun2202[at]yahoo[dot]com
Year of Completion: December 2014
varun2202[at]yahoo[dot]com
Year of Completion: December 2014
drpriyankagupta84[at]gmail[dot]com
Year of Completion: December 2014
anki_979[at]yahoo[dot]co[dot]in
Year of Completion: June 2015
drshail.kumar[at]gmail[dot]com
Year of Completion: December 2015
drsujoyb[at]gmail[dot]com
Year of Completion: June 2016
ranascb[at]yahoo[dot]com
Year of Completion: June 2017
nayani.rk[at]gmail[dot]com
Year of Completion: December 2017
vikas.max[at]gmail[dot]com
Year of Completion: December 2017
spunkygst[at]gmail[dot]com
Year of Completion: December 2017
drsinghafmc[at]yahoo[dot]co[dot]in
Year of Completion: December 2018
devika0204[at]gmail[dot]com
Year of Completion: December 2018
barkha.gmh[at]yahoo[dot]co[dot]in
Year of Completion: December 2018
drsokhal[at]yahoo[dot]co[dot]in
Year of Completion: December 2018
nitsmishra[at]gmail[dot]com
Chief Technical Officer
Technical Officer
Technical Officer
Technical Officer
Technical Officer
Technical Officer
Technical Officer
Technician Radiology Gr. I
Technical Officer
Technician Radiology Gr. I
Technical Officer
Technical Officer
Technical Officer
Technician Radiology Gr. I
Technician Radiology Gr. I
Technician Radiology Gr. I
Technician Radiology Gr. I
Technician Radiology Gr. I
Technician Radiology Gr. I
Technician Radiology Gr. I
Technician Radiology Gr. II (Contract)
Dart Room Asstt.
Dart Room Asstt.
Dart Room Asstt.
Sister Gd II
Sister Gd II
Brother Gd. II
Brother Gd. II
Brother Gd. II
Sister Gd. II
Brother Gd. II
PS
Junior Administrative Assistant
Junior Administrative Assistant (PACS room)
Junior Administrative Assistant (Record room)
PTSG
PTSG
Data Entry Operator
Lab Technician
Lab Technician
Hospital Attendant
Gamma Knife, Hospital Attendant
Hospital Attendant
Hospital Attendant
Hospital Attendant
MTS
Hospital Attendant
MTS
The following academic courses are conducted by the department:
Duration: Three (03) years course
Eligibility A candidate must possess MD (Anaesthesia) degree of a University recognized by Medical Council of India. The entrance exams are conducted in December and May every year.
For further information contact Examination Cell, AIIMS
Procedure of selection
For this program the candidate is selected through 2 step competitive examination held at national level.
Final selection of the candidate is made on the bases of combined evaluation of step-I, and II
The selected candidates work as Senior Resident (DM) in the department. They are supposed to do all clinical work of OR, ICUs, and emergency both independently and also under supervision. The candidate is expected to maintain a log book of all anaesthetic, postoperative, and critical care experience. They are supposed to write one dissertation to qualify to appear in final DM exam. The final DM examination to award the degree takes place after the end of 3rd year.
Teaching Program
Final Examination
The final examination to award the degree of DM (Neuroanaesthesiology and Critical Care) consists of following steps
Duration: One (01) year course
Eligibility A candidate must possess MD / DNB (Anaesthesia, Medicine) or MS (Surgery) degree of a University recognized by Medical Council of India with three years’ post PG experience in Neurosciences or having a degree of DM (Neuroanaesthesiology, Neurology), MCh (Neurosurgery). The entrance exams are conducted in December and May every year.
For further information contact Examination Cell, AIIMS
Procedure of selection
For this program the candidate is selected through 2 step competitive examination held at national level.
Final selection of the candidate is made on the bases of combined evaluation of step-I, and II
The selected candidates work as Neurocritical Care Fellow in the Neuro ICUs. They are supposed to do all clinical work of Neurosurgery ICUs, Neurology ICU, Stroke Unit at Neurosciences centre and Neurotrauma ICU at JPNA Trauma Centre, both independently and also under supervision. The candidate is expected to maintain a log book of all critical care experience. The final fellowship examination to award the degree takes place after the end of one year.
Teaching Program
Final Examination
The final examination to award the degree of Post-Doctoral Fellowship (Neurocritical Care) consists of following steps
Practical Exam
Past Faculty
Name | Designation | Period | |
|---|---|---|---|
| Dr. Surinder Singh Saini | Professor & Head | 1987-1992 | saini_surindar[at]yahoo[dot]com |
| Dr. Hari Hara Dash | Professor & Head; Chief, NSC | 1987-2012 | dr.harihardash[at]gmail[dot]com |
| Dr Pramod Kumar Bithal | Professor & Head | 1987-2016 | bithal.pramod[at]gmail[dot]com |
| Dr. Neeraj Vishnoi | Associate Professor | 1993 | nvishnoi[at]me[dot]com |
| Dr. Ajit Kumar Kayal | Assistant Professor | 1993-1996 | --- |
| Dr. Anju Romino Bhalotra | Assistant Professor | 1997 | drakgk[at]yahoo.co.in |
| Late Dr. Bibekananda Mohanty | Assistant Professor | 1998-2000 | --- |
| Dr. Gyanendra Upamanyu | Assistant Professor | 1998 | gyan64[at]hotmail[dot]com |
| Dr. Prabhat Kumar Sinha | Assistant Professor | 2000-2001 | pksinha02[at]yahoo[dot]com |
| Name | Month/Year of Completion | |
|---|---|---|
| Dr. Girija Prasad Rath | June 2005 | girijarath[at]yahoo[dot]co[dot]in |
| Dr. M. Radhakrishnan | June 2005 | mrks1973[at]yahoo[dot]com |
| Dr. Indranil Ghosh | June 2006 | ghoshindranilghosh[at]rediffmail[dot]com |
| Dr. Mukesh Mohan Gupta | June 2006 | drmukeshmohangupta[at]yahoo[dot]co[dot]in |
| Dr. Deepak Sharma | December 2006 | dsharma[at]u[dot]washington[dot]edu |
| Dr. Hemant Bhagat | December 2006 | drhemantbhagat[at]rediffmail[dot]com |
| Dr. Virendra Jain | June 2008 | vjain_01[at]yahoo[dot]com |
| Dr. Pradeep Kumar Lai (S) | December 2008 | drlaithangba[at]gmail[dot]com |
| Dr. Deepak Singh | December 2008 | drdeepakaims[at]gmail[dot]com |
| Dr. Zulfiqar Ali (S) | December 2008 | zulfiqaraliiii[at]yahoo[dot]com |
| Dr. Prasanna Bidkar | June 2009 | drprasannabidkar[at]gmail[dot]com |
| Dr. Manish Kumar Marda | December 2009 | drmmarda[at]gmail[dot]com |
| Dr. Gyaninder Pal Singh | June 2010 | drsingh_gp[at]yahoo[dot]co[dot]in |
| Dr. Rahul Yadav (S) | June 2011 | docrahulyadav[at]gmail[dot]com |
| Dr. Ashish Bindra | December 2011 | dr_ashi2208[at]yahoo[dot]com |
| Dr. Sachidanand Jee Bharti | December 2011 | >sachidadr[at]yahoo[dot]co[dot]in |
| Dr. Tumul Chowdhury | December 2011 | tumulthunder[at]gmail[dot]com |
| Dr. Keshav Goyal | December 2011 | keshavgoyal[at]yahoo[dot]co[dot]in |
| Dr. Charu Mahajan | June 2012 | charushrikul[at]gmail[dot]com |
| Dr. B. Kiran Reddy | June 2012 | reddykiranb[at]rediffmail[dot]com |
| Dr. Navdeep Sokhal | December 2012 | drnavdeep_kumar[at]yahoo[dot]com |
| Dr. Nidhi Gupta | June 2013 | neurodmrenu[at]yahoo[dot]com |
| Dr. Vivek Bharti Sharma | June 2013 | drnidhisrivastava2[at]gmail.com |
| Dr. Renu Bala (S) | December 2013 | vbs_rashmi[at]yahoo[dot]co[dot]in |
| Dr. Surya Kumar Dube | June 2014 | surya.dube[at]gmail[dot]com |
| Dr. Bhavna Hooda (S) | December 2014 | bhavnahooda2007[at]rediffmail[dot]com |
| Dr. Vanitha Rajagopalan | December 2014 | varun2202[at]yahoo[dot]com |
| Dr. Varun Jain | December 2014 | varun2202[at]yahoo[dot]com |
| Dr. Priyanka Gupta | December 2014 | drpriyankagupta84[at]gmail[dot]com |
| Dr. Ankur Luthra | December 2014 | anki_979[at]yahoo[dot]co[dot]in |
| Dr. Shailendra Kumar | June 2015 | drshail.kumar[at]gmail.com |
| Dr. Sujoy Banik | December 2015 | drsujoyb[at]gmail.com |
| Dr. Ranadhir Mitra | June 2016 | ranascb[at]yahoo[dot]com |
| Dr. Nayani Radhakrishna | June 2017 | nayani[dot]rk[at]gmail.com |
| Dr. Vikash Chauhan | December 2017 | vikas[dot]max[at]gmail.com |
| Dr. Gaurav Singh Tomar | December 2017 | spunkygst[at]gmail.com |
| Dr. Shalendra Singh | December 2017 | drsinghafmc[at]yahoo[dot]co[dot]in |
| Dr. Devika Bhardwaj | December 2018 | devika0204[at]gmail.com |
| Dr. Barkha Bindu | December 2018 | barkha[dot]gmh[at]yahoo[dot]co[dot]in |
| Dr. Suman Sokhal | December 2018 | drsokhal[at]yahoo[dot]co[dot]in |
| Dr. Nitasha Mishra | December 2018 | nitsmishra[at]gmail.com |

Dr Animesh Das
MBBS, MD, DM
Assistant Professor
Department of Neurology
Room number, 7th floor, Neurosciences Centre
Email- animeshdas05[at]gmail[dot]com
OPD: Wednesday/ Saturday (forenoon), Room no-6, Ground Floor, Neurosciences Centre
Dr Animesh Das has joined as Assistant Professor of Neurology at the All India Institute of Medical Sciences, New Delhi, India in 2019. He has special interest in demyelinating diseases, movement disorders and clinical electrophysiology.
Dr. Das graduated from BRD Medical College, Uttar Pradesh in 2011 and completed his postgraduate degree (MD) in Pediatrics from All India Institute of Medical Sciences, New Delhi in 2014. He did his 1-year senior residency in the Department of Pediatrics at All India Institute of Medical Sciences, New Delhi from 2014-2015. Subsequently, he did his DM (Neurology) in 2018 from Sanjay Gandhi Post Gradute Institute of Medical Sciences and Post-Doctorate fellowship in Neurophysiology from the same Institute.
Publications:
D.M. Students
| Name | Expected Month & Year of Completion | |
| Dr. Devjyoti Sharma | July 2021 | drwrizu[at]gmail[dot]com |
| Dr. Sunil Routaray | July 2021 | drsunilroutaray[at]gmail[dot]com |
| Dr. Arohan Gupta | July 2021 | arohangupta[at]gmail[dot]com |
| Dr. Chandrakant Prasad | July 2021 | chandrakant.vems[at]gmail[dot]com |
| Dr. Vikas Chauhan | December 2017 | vikas.max[at]gmail[dot]com |
| Dr. Ashutosh Kaushal | December 2018 | drashutosh.kaushal[at]gmail[dot]com |
| Dr. Subodh Kumar | December 2018 | subodh.kgmc[at]gmail[dot]com |
| Dr. Ritesh Lamsal | December 2018 | riteshlamsal[at]gmail[dot]com |
| Dr Bhagya Ranjan Jena | June 2019 | drbhagya.j3100[at]gmail[dot]com |
| Dr. Ruhi Mamualiya | June 2019 | dr.ruhi[at]gmail[dot]com |
| Dr. Hirok Ray | June 2019 | hirokroy85[at]gmail[dot]com |
| Dr. Ankur Dhanda | December 2019 | ankurdhanda[at]gmail[dot]com |
| Dr. Ratnesh Shukla | June 2020 | ratneshafmc[at]gmail[dot]com |
| Dr. Sidharth Srinivas Chaveli | December 2019 | sid.chavali[at]gmail[dot]com |
| Dr. Ankur Khandewal | June 2020 | ankurchintus[at]gmail[dot]com |
| Dr. V.Sameera | December 2020 | sameera1v[at]gmail[dot]com |
| Dr. Rashmi Rani Mahapatra | December 2020 | dr.rashmimahapatra[at]yahoo.com |
| Dr. Saurabh Barman | December 2020 | wowsourav[at]gmail[dot]com |
| Dr. Deep Sengupta | December 2020 | langdon88[at]gmail[dot]com |
Post- Doctoral Fellows
| Name | Expected Month & Year of Completion | |
| Dr. Sneha Singh | January 2018 | drss_india[at]yahoo.com |
| Dr Vineet Choudhary | July 2019 | Vin.chowdhary[at]gmail[dot]com |
Professor Head
1987-1992
saini_surindar[at]yahoo[dot]com
Professor & Head; Chief, NSC
1987-2012
dr.harihardash[at]gmail[dot]com
Professor & Head
1987-2016
bithal.pramod[at]gmail[dot]com
Associate Professor
1993
nvishnoi[at]me[dot]com
Assistant Professor
1993-1996
---
Assistant Professor
1997
drakgk[at]yahoo.co.in
Assistant Professor
1998-2000
---
Assistant Professor
1998
gyan64[at]hotmail[dot]com
Assistant Professor
2000-2001
pksinha02[at]yahoo[dot]com
Year of Completion: June 2005
girijarath[at]yahoo[dot]co[dot]in
Year of Completion: June 2005
mrks1973[at]yahoo[dot]com
Year of Completion: June 2006
ghoshindranilghosh[at]rediffmail[dot]com
Year of Completion: June 2006
drmukeshmohangupta[at]yahoo[dot]co[dot]in
Year of Completion: December 2006
dsharma[at]u[dot]washington[dot]edu
Year of Completion: December 2006
drhemantbhagat[at]rediffmail[dot]com
Year of Completion: June 2008
vjain_01[at]yahoo[dot]com
Year of Completion: December 2008
drlaithangba[at]gmail[dot]com
Year of Completion: December 2008
drdeepakaims[at]gmail[dot]com
Year of Completion: December 2008
zulfiqaraliiii[at]yahoo[dot]com
Year of Completion: June 2009
drprasannabidkar[at]gmail[dot]com
Year of Completion: December 2009
drmmarda[at]gmail[dot]com
Year of Completion: June 2010
drsingh_gp[at]yahoo[dot]co[dot]in
Year of Completion: June 2011
docrahulyadav[at]gmail[dot]com
Year of Completion: December 2011
dr_ashi2208[at]yahoo[dot]com
Year of Completion: December 2011
sachidadr[at]yahoo[dot]co[dot]in
Year of Completion: December 2011
tumulthunder[at]gmail[dot]com
Year of Completion: December 2011
keshavgoyal[at]yahoo[dot]co[dot]in
Year of Completion: June 2012
charushrikul[at]gmail[dot]com
Year of Completion: June 2012
reddykiranb[at]rediffmail[dot]com
Year of Completion: December 2012
drnavdeep_kumar[at]yahoo[dot]com
Year of Completion: June 2013
neurodmrenu[at]yahoo[dot]com
Year of Completion: June 2013
drnidhisrivastava2[at]gmail.com
Year of Completion: December 2013
vbs_rashmi[at]yahoo[dot]co[dot]in
Year of Completion: June 2014
surya.dube[at]gmail[dot]com
Year of Completion: December 2014
bhavnahooda2007[at]rediffmail[dot]com
Year of Completion: December 2014
varun2202[at]yahoo[dot]com
Year of Completion: December 2014
varun2202[at]yahoo[dot]com
Year of Completion: December 2014
drpriyankagupta84[at]gmail[dot]com
Year of Completion: December 2014
anki_979[at]yahoo[dot]co[dot]in
Year of Completion: June 2015
drshail.kumar[at]gmail.com
Year of Completion: December 2015
drsujoyb[at]gmail.com
Year of Completion: June 2016
ranascb[at]yahoo[dot]com
Year of Completion: June 2017
nayani[dot]rk[at]gmail.com
Year of Completion: December 2017
vikas[dot]max[at]gmail.com
Year of Completion: December 2017
spunkygst[at]gmail.com
Year of Completion: December 2017
drsinghafmc[at]yahoo[dot]co[dot]in
Year of Completion: December 2018
devika0204[at]gmail.com
Year of Completion: December 2018
barkha[dot]gmh[at]yahoo[dot]co[dot]in
Year of Completion: December 2018
drsokhal[at]yahoo[dot]co[dot]in
Year of Completion: December 2018
nitsmishra[at]gmail.com
MBBS, MD, DM
Professor, Department of Neurology,
Head, Unit III
Room #60, Ground Floor, Neurosciences Center, AIIMS , New Delhi
Phone: +91 11 26546688
Email: achalsrivastava[at]hotmail[dot]com
Outpatients clinic ( General Neurology including Ataxia Clinic - Movement Disorder Clinic)
Wednesday and Saturday (forenoon)
For appointments: +91 11 26594656 or email to ataxiaclinicaiims[at]gmail[dot]com
Dr. Achal Kumar Srivastava is Professor of Clinical Neurophysiology in the Department of Neurology at the All India Institute of Medical Sciences, New Delhi, India. He heads the Clinical Neurophysiology facility and Ataxia clinic at the center and is a member of the Comprehensive Epilepsy care team here. He has special interest in ataxias, epilepsy and genetics of movement disorders. He is a recipient of more than 25 paper presentation awards and has more than 100 publications to his credit.
Dr. Srivastava graduated from MLN Medical College, Allahabad, Uttar Pradesh in 1991 and completed his postgraduate degree (MD) in Medicine (1994) from the same college. Subsequently he obtained post-doctoral specialist certification in DM (Neurology) in 1998 from the Department of Neurology, All India Institute of Medical Sciences, New Delhi. He worked as Senior Scientist grade scientist fellow for over a year at CSIR Institute of Genomics and Integrative Biology (formerly known as Center for Biochemical technology) and then joined as Assistant Professor in the Department of Neurology in March 2001. He has keen interest in teaching and has provided guidance and training to more than 70 DM and PhD students in their research work.
Dr. Srivastava has received academic awards at National and International scientific forums, mainly for his work in the field of ataxias and genetics of neurological disorders. Many of his students (both DM and PhD) have also won academic awards and honours, under his guidance. He was invited by Molecular Biology Division at John Hopkins USA for presentation of his work on spinocerebellar ataxia type 12. He has received outstanding paper presentation award from AINA at American Academy of Neurology conference at San Francisco in 2004 and the best paper award at Neurological Society of India conference at Hyderabad in 1998. He has received many travel fellowships to attend international conferences. He has received Young investigator award for CAG triplet repeat disorder conferences at USA and Italy. He has collaborative projects with many universities and research institutes. He is on the editorial board of Journal of Clinical Neuroscience and many other journals of repute.
Name | Designation | Period | |
|---|---|---|---|
| Dr. Surinder Singh Saini | Professor & Head | 1987-1992 | saini_surindar[at]yahoo[dot]com |
| Dr. Hari Hara Dash | Professor & Head; Chief, NSC | 1987-2012 | dr.harihardash[at]gmail[dot]com |
| Dr Pramod Kumar Bithal | Professor & Head | 1987-2016 | bithal.pramod[at]gmail[dot]com |
| Dr. Neeraj Vishnoi | Associate Professor | 1993 | nvishnoi[at]me[dot]com |
| Dr. Ajit Kumar Kayal | Assistant Professor | 1993-1996 | --- |
| Dr. Anju Romino Bhalotra | Assistant Professor | 1997 | drakgk[at]yahoo[dot]co[dot]in |
| Late Dr. Bibekananda Mohanty | Assistant Professor | 1998-2000 | --- |
| Dr. Gyanendra Upamanyu | Assistant Professor | 1998 | gyan64[at]hotmail[dot]com |
| Dr. Prabhat Kumar Sinha | Assistant Professor | 2000-2001 | pksinha02[at]yahoo[dot]com |
Professor & Head
1987-1992
saini_surindar[at]yahoo[dot]com
Professor & Head; Chief, NSC
1987-2012
dr.harihardash[at]gmail[dot]com
Professor & Head
1987-2016
bithal.pramod[at]gmail[dot]com
Associate Professor
1993
nvishnoi[at]me[dot]com
Assistant Professor
1993-1996
Assistant Professor
1997
drakgk[at]yahoo[dot]co[dot]in
Assistant Professor
1998-2000
Assistant Professor
1998
gyan64[at]hotmail[dot]com
Assistant Professor
2000-2001
pksinha02[at]yahoo[dot]com
| S.No. | Name | Designation | Office address | Office tel | |
|---|---|---|---|---|---|
| 1 | Dr S S Kale | Professor and Head | skale67[at]yahoo[dot]com | ||
| 2 | Prof P N Tandon | Emeritus Professor | 716, CN Centre, AIIMS | tandon[at]nbrc[dot]ac[dot]in | |
| 3 | Prof A K Banerji | Emeritus Professor | 716, CN Centre, AIIMS | akb1935[at]yahoo[dot]com | |
| 4 | Dr P S Chandra | Professor | 607, 6th floor, CN Centre, AIIMS | saratpchandra[at]gmail[dot]com | |
| 5 | Dr Ashish Suri | Professor | 712, CN Centre, AIIMS | 26593538 | surineuro[at]gmail[dot]com |
| 6 | Dr Rajinder Kur | Professor | 605 6th floor, NSC, AIIMS | rklaythalling[at]rediffmail[dot]com | |
| 7 | Dr Manmohan Sih | Professor | 715,CN center, AIIMS | manmohan1972[at]gmail[dot]com mehaknoor[at]hotmail[dot]com | |
| 8 | Dr Deepak Agwal | Professor (Trauma Centre) | 713, C N Centre, AIIMS | ved[at]vsnl[dot]com | |
| 9 | Dr Deepak K. Gupta | Professor (Trauma Centre) | 714, C N Centre, AIIMS | drdeepakgupta[at]gmail[dot]com | |
| 10 | Dr G D Saarthi | Associate Professor (Trauma Centre) | 714, C N Centre, AIIMS | duttaguru2002[at]yahoo[dot]com | |
| 11 | Dr Pankaj Kumar Singh | Associate Professor(Trauma Centre) | 717, CN Center, AIIMS | pankajsingh11[at]gmail[dot]com | |
| 12 | Dr Vivek Tandon | Addittional Professor | 608 6th floor, NSC, AIIMS | drvivektandon[at]gmail[dot]com | |
| 13 | Dr Sachin A rkar | Professor | 717, CN Center, AIIMS | drsachinb81[at]gmail[dot]com | |
| 14 | Dr. Shashwat Mishra | Associate Professor | gyrusrectus[at]gmail[dot]com | ||
| 15 | Dr. Amandeep Jagdevan | Associate Professor | aman_jagdevan[at]yahoo[dot]co[dot]in | ||
| 16 | Dr Rajeev Sharma | Associate Professor | rajubd79[at]rediffmail[dot]com | ||
| 17 | Dr. Shweta Kedia | Associate Professor | drshwetakedia[at]gmail[dot]com | ||
| 18 | Dr Hitesh Kumar | Associate Professor | 608 6th floor, NSC, AIIMS | hiteshgurjar[at]gmail[dot]com | |
| 19 | Dr. Manoj Phalak | Associate Professor | - | ||
| 20 | Dr. Kanwaljeet Garg | Associate Professor | - | ||
| 21 | Dr Ramesh Doddamani | Addittional Professor | - | ||
| 22 | Dr Dattaraj Sawarkar | Associate Professor | - | ||
| 23 | Dr. Amol Raheja | Assistant Professor | dramolraheja[at]aiims[dot]edu | ||
| 24 | Dr Satish Kumar Verma | Additional Professor | drsatishsx[at]gmail[dot]com | ||
| 25 | Dr. Rajesh Kr. Meena | Assistant Professor | - | ||
| 26 | Dr. Kokkula Praneeth | Assistant Professor | praneethkokkula[at]aiims[dot]edu | ||
| 27 | Dr Ravi ShmaDr Ravi Shma | Assistant Professor | - |
| Name | Expected Month & Year of Completion | |
|---|---|---|
| Dr. Devjyoti Sharma | July 2021 | drwrizu[at]gmail[dot]com |
| Dr. Sunil Routaray | July 2021 | drsunilroutaray[at]gmail[dot]com |
| Dr. Arohan Gupta | July 2021 | arohangupta[at]gmail[dot]com |
| Dr. Chandrakant Prasad | July 2021 | chandrakant.vems[at]gmail[dot]com |
| Dr. Vikas Chauhan | December 2017 | vikas.max[at]gmail[dot]com |
| Dr. Ashutosh Kaushal | December 2018 | drashutosh.kaushal[at]gmail[dot]com |
| Dr. Subodh Kumar | December 2018 | subodh.kgmc[at]gmail[dot]com |
| Dr. Ritesh Lamsal | December 2018 | riteshlamsal[at]gmail[dot]com |
| Dr Bhagya Ranjan Jena | June 2019 | drbhagya.j3100[at]gmail[dot]com |
| Dr. Ruhi Mamualiya | June 2019 | dr.ruhi[at]gmail[dot]com |
| Dr. Hirok Ray | June 2019 | hirokroy85[at]gmail[dot]com |
| Dr. Ankur Dhanda | December 2019 | ankurdhanda[at]gmail[dot]com |
| Dr. Ratnesh Shukla | June 2020 | ratneshafmc[at]gmail[dot]com |
| Dr. Sidharth Srinivas Chaveli | December 2019 | sid.chavali[at]gmail[dot]com |
| Dr. Ankur Khandewal | June 2020 | ankurchintus[at]gmail[dot]com |
| Dr. V.Sameera | December 2020 | sameera1v[at]gmail[dot]com |
| Dr. Rashmi Rani Mahapatra | December 2020 | dr.rashmimahapatra[at]yahoo[dot]com |
| Dr. Saurabh Barman | December 2020 | wowsourav[at]gmail[dot]com |
| Dr. Deep Sengupta | December 2020 | langdon88[at]gmail[dot]com |
| Name | Expected Month & Year of Completion | |
|---|---|---|
| Dr. Sneha Singh | January 2018 | drss_india[at]yahoo[dot]com |
| Dr Vineet Choudhary | July 2019 | Vin.chowdhary[at]gmail[dot]com |
Year of Completion: July 2021
drwrizu[at]gmail[dot]com
Year of Completion: July 2021
drsunilroutaray[at]gmail[dot]com
Year of Completion: July 2021
arohangupta[at]gmail[dot]com
Year of Completion: July 2021
chandrakant.vems[at]gmail[dot]com
Year of Completion: December 2017
vikas.max[at]gmail[dot]com
Year of Completion: December 2018
drashutosh.kaushal[at]gmail[dot]com
Year of Completion: December 2018
subodh.kgmc[at]gmail[dot]com
Year of Completion: December 2018
riteshlamsal[at]gmail[dot]com
Year of Completion: June 2019
drbhagya.j3100[at]gmail[dot]com
Year of Completion: June 2019
dr.ruhi[at]gmail[dot]com
Year of Completion: June 2019
hirokroy85[at]gmail[dot]com
Year of Completion: December 2019
ankurdhanda[at]gmail[dot]com
Year of Completion: June 2020
ratneshafmc[at]gmail[dot]com
Year of Completion: December 2019
sid.chavali[at]gmail[dot]com
Year of Completion: June 2020
ankurchintus[at]gmail[dot]com
Year of Completion: December 2020
sameera1v[at]gmail[dot]com
Year of Completion: December 2020
dr.rashmimahapatra[at]yahoo[dot]com
Year of Completion: December 2020
wowsourav[at]gmail[dot]com
Year of Completion: December 2020
langdon88[at]gmail[dot]com
Year of Completion: January 2018
drss_india[at]yahoo[dot]com
Year of Completion: July 2019
Vin.chowdhary[at]gmail[dot]com
Email: sgaikwad_63[at]yahoo[dot]com | sbgaikwad1112[at]gmail[dot]com
Contact No: 9971237573

Year of Completion: July 2021
drwrizu[at]gmail[dot]com
Year of Completion: July 2021
drsunilroutaray[at]gmail[dot]com
Year of Completion: July 2021
arohangupta[at]gmail[dot]com
Year of Completion: July 2021
chandrakant.vems[at]gmail[dot]com
Year of Completion: December 2017
vikas.max[at]gmail[dot]com
Year of Completion: December 2018
drashutosh.kaushal[at]gmail[dot]com
Year of Completion: December 2018
subodh.kgmc[at]gmail[dot]com
Year of Completion: December 2018
riteshlamsal[at]gmail[dot]com
Year of Completion: June 2019
drbhagya.j3100[at]gmail[dot]com
Year of Completion: June 2019
dr.ruhi[at]gmail[dot]com
Year of Completion: June 2019
hirokroy85[at]gmail[dot]com
Year of Completion: December 2019
ankurdhanda[at]gmail[dot]com
Year of Completion: June 2020
ratneshafmc[at]gmail[dot]com
Year of Completion: December 2019
sid.chavali[at]gmail[dot]com
Year of Completion: June 2020
ankurchintus[at]gmail[dot]com
Year of Completion: December 2020
sameera1v[at]gmail[dot]com
Year of Completion: December 2020
dr.rashmimahapatra[at]yahoo.com
Year of Completion: December 2020
wowsourav[at]gmail[dot]com
Year of Completion: December 2020
langdon88[at]gmail[dot]com
Year of Completion: January 2018
drss_india[at]yahoo.com
Year of Completion: July 2019
Vin.chowdhary[at]gmail[dot]com
| Office Staff | |
| Mrs. Alka Khanna | Personal Assistant |
| Mr. Lalit Saraswat | UDC |
| Mr. Varun Vashist | UDC |
| Mr. Ashok Kumar | Office Assistant |
| Ms. Vimla Bist |
Neuro-OT/ Neuro Cath-Lab/ CT Scan & MRI/ Gamma Knife Technical Staff
| |
| Mr. Sarda Ram | Technical Assistant |
| Mr. S .K. Mehto | Technical Assistant |
| Mr. Purshottam Mathpal | Technical Assistant |
| Mr. Anil Kumar Rana | Technical Assistant |
| Mr. Lakhvir Singh | Technical Assistant |
| Mr. Pratap Singh | Technical Assistant |
| Mr. S.R. Mishra | OT Technician |
| Mr. Gopal Adhikari | OT Technician |
| Mr. Ram Asrey | OT Technician |
| Mr. Narender Singh | OT Technician |
| Mr. Devi Prasad | OT Assistant |
| Mr. Balam Singh Bisht | OT Assistant |
| Mr. Mahesh Sharma | OT Assistant |
| Mr. Bijender Singh | OT Assistant |
| Mr. Hukam Singh | OT Assistant |
| Mr. Laxman Singh | OT Assistant |
| Mr. Bablu | OT Assistant |
| Mr. Davender Kumar | OT Assistant |
| Mr. Chakleshwar Verma | OT Assistant |
| Miss. Neha Kaushik | OT Assistant |
| Mr. Abhay Kumar Gautam | OT Assistant |
| Mr. Praveen Kumar | OT Assistant |
| Mr. Pramod Kumar Sharma | OT Assistant |
| Mr. Ved Mitra | OT Assistant |
| Mr. Manoj Kumar | OT Assistant |
| Mr. Prem Das | OT Assistant |
| Mr. Dhirender Kishore | OT Assistant |
| Mr. Jitender Kumar | OT Assistant |
| Mr. Prem Shanker Sahu | OT Assistant |
| Mr. Ram Swaroop Meena | OT Assistant |
| Mr. Dharmender Kumar | OT Assistant |
| Mr. Saddam Hussain | OT Assistant |
| Mrs. Sujata Gupta | OT Assistant |
| Mrs.Githa G.S | OT Assistant |
| Mr. Suman Gowala | OT Assistant |
| Mr. Rupak Kumar | OT Assistant |
| Mr. Santanu Maity | OT Assistant |
| Ms. Shivani Sharma | OT Assistant |
| Ms. Renu Sharma | OT Assistant |
| Mr. Satyajeet | OT Assistant |
| Mr. Rakesh Kumar | OT Assistant |
| Mr. Sunder Singh | H/A |
ICU (Neurology/ Neurosurgery) and Ward Technical Staff
| |
| Mr. Devender Kapoor | Technical Officer |
| Mr. Duli Chand | Technical Assistant |
| Mr. Nihal Singh | OT Technician |
| Mr. Janak Raj | OT Technician |
| Mr. Lalit Prasad | OT Technician |
| Mr. Chandan Singh | OT Assistant |
| Mr. Mozam Ali | OT Assistant |
| Mr. Ram Swaroop Meena | OT Assistant |
| Mr. Dharmpal | OT Assistant |
| Mr.Bijender Singh | OT Assistant |
| Mr. Pramod Kumar Sharma | OT Assistant |
| Mr. Marpu Giribabu | OT Assistant |
| Mr. Nitin | OT Assistant |
| Mr. Nishi Kumar | H/A |
| Mr. Virender Kumar | H/A |
| Mr. Anand | H/A |
| S. No. | Name | Designation | Office Address | Office telephone | |
|---|---|---|---|---|---|
| 1. | Dr. S. B. Gaikwad | Professor & Head | Room no.11, 6th floor CNC Room No.15, Cath Lab Complex, CNC | Ext. 3457 Ext.4418 | sgaikwad_63[at]yahoo[dot]com |
| 2. | Dr. Ajay Garg | Professor | Room No.14, Cath Lab Complex | Ext 6449 | ajaygarg[at]aiims[dot]ac[dot]in drajaygarg@gmail.com |
| 3. | Dr. Leve Joseph Devarajan S. | Additional Professor | Room No.17, Cath Lab Complex | Ext.3844 | leve_s[at]yahoo[dot]com |
| Sno. | Name of the Test & Developed by: |
|---|---|
| 1. | AIIMS COMPREHENSVE NEUROPSYCHOLOGICAL BATTERY IN HINDI (ADULT FORM) Surya Gupta et al. |
| 2. | AIIMS COMPREHENSVE NEUROPSYCHOLOGICAL BATTERY IN HINDI (CHILDREN’S FORM) Surya Gupta et al. |
| 3. | AIIMS COMPREHENSVE DEMENTIA ASSESSMENT SCALE IN HINDI Surya Gupta et al. |
Personal Assistant
UDC
UDC
Office Assistant
Technical Assistant
Technical Assistant
Technical Assistant
Technical Assistant
Technical Assistant
Technical Assistant
OT Technician
OT Technician
OT Technician
OT Technician
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
H/A
Technical Officer
Technical Assistant
OT Technician
OT Technician
OT Technician
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
H/A
H/A
H/A
| Mrs. Alka Khanna | Personal Assistant |
| Mr. Lalit Saraswat | UDC |
| Mr. Varun Vashist | UDC |
| Mr. Ashok Kumar | Office Assistant |
| Ms. Vimla Bist |
| Mr. Sarda Ram | Technical Assistant |
| Mr. S .K. Mehto | Technical Assistant |
| Mr. Purshottam Mathpal | Technical Assistant |
| Mr. Anil Kumar Rana | Technical Assistant |
| Mr. Lakhvir Singh | Technical Assistant |
| Mr. Pratap Singh | Technical Assistant |
| Mr. S.R. Mishra | OT Technician |
| Mr. Gopal Adhikari | OT Technician |
| Mr. Ram Asrey | OT Technician |
| Mr. Narender Singh | OT Technician |
| Mr. Devi Prasad | OT Assistant |
| Mr. Balam Singh Bisht | OT Assistant |
| Mr. Mahesh Sharma | OT Assistant |
| Mr. Bijender Singh | OT Assistant |
| Mr. Hukam Singh | OT Assistant |
| Mr. Laxman Singh | OT Assistant |
| Mr. Bablu | OT Assistant |
| Mr. Davender Kumar | OT Assistant |
| Mr. Chakleshwar Verma | OT Assistant |
| Miss. Neha Kaushik | OT Assistant |
| Mr. Abhay Kumar Gautam | OT Assistant |
| Mr. Praveen Kumar | OT Assistant |
| Mr. Pramod Kumar Sharma | OT Assistant |
| Mr. Ved Mitra | OT Assistant |
| Mr. Manoj Kumar | OT Assistant |
| Mr. Prem Das | OT Assistant |
| Mr. Dhirender Kishore | OT Assistant |
| Mr. Jitender Kumar | OT Assistant |
| Mr. Prem Shanker Sahu | OT Assistant |
| Mr. Ram Swaroop Meena | OT Assistant |
| Mr. Dharmender Kumar | OT Assistant |
| Mr. Saddam Hussain | OT Assistant |
| Mrs. Sujata Gupta | OT Assistant |
| Mrs.Githa G.S | OT Assistant |
| Mr. Suman Gowala | OT Assistant |
| Mr. Rupak Kumar | OT Assistant |
| Mr. Santanu Maity | OT Assistant |
| Ms. Shivani Sharma | OT Assistant |
| Ms. Renu Sharma | OT Assistant |
| Mr. Satyajeet | OT Assistant |
| Mr. Rakesh Kumar | OT Assistant |
| Mr. Sunder Singh | H/A |
| Mr. Devender Kapoor | Technical Officer |
| Mr. Duli Chand | Technical Assistant |
| Mr. Nihal Singh | OT Technician |
| Mr. Janak Raj | OT Technician |
| Mr. Lalit Prasad | OT Technician |
| Mr. Chandan Singh | OT Assistant |
| Mr. Mozam Ali | OT Assistant |
| Mr. Ram Swaroop Meena | OT Assistant |
| Mr. Dharmpal | OT Assistant |
| Mr.Bijender Singh | OT Assistant |
| Mr. Pramod Kumar Sharma | OT Assistant |
| Mr. Marpu Giribabu | OT Assistant |
| Mr. Nitin | OT Assistant |
| Mr. Nishi Kumar | H/A |
| Mr. Virender Kumar | H/A |
| Mr. Anand | H/A |
The department of Neuroimaging & Interventional Neuroradiology at All India institute of Medical Sciences is dedicated to the highest quality patient care, education, research, and community service. The department provides imaging and interpretation services to Neurosciences Centre.
The objectives of the Neuroimaging & Interventional Neuroradiology Department are:
The department is currently equipped with two Digital Subtraction Angiography systems (the biplane ‘Siemens ARTZEE’ & Philips FD 20/20 with facilities for rotational angiography & 3-D reconstruction. One 1.5T MR system (GE 450w), one CT scanner (Siemens Definition Edge 128-slice CT scanner and one color Doppler unit (HP ‘Sonos 4500’) serves as mainstays of diagnostic studies. These units cater to the requirements of the Neurosciences centre.
Personal Assistant
UDC
UDC
Office Assistant
Technical Assistant
Technical Assistant
Technical Assistant
Technical Assistant
Technical Assistant
Technical Assistant
OT Technician
OT Technician
OT Technician
OT Technician
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
H/A
Technical Officer
Technical Assistant
OT Technician
OT Technician
OT Technician
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
OT Assistant
H/A
H/A
H/A
STAFF
Office Staff
Mrs. Alka Khanna
Personal Assistant
Mr. Lalit Saraswat
UDC
Mr. Varun Vashist
UDC
Mr. Ashok Kumar
Office Assistant
Ms. Vimla Bist
Neuro-OT/ Neuro Cath-Lab/ CT Scan & MRI/ Gamma Knife Technical Staff
Mr. Sarda Ram
Technical Assistant
Mr. S .K. Mehto
Technical Assistant
Mr. Purshottam Mathpal
Technical Assistant
Mr. Anil Kumar Rana
Technical Assistant
Mr. Lakhvir Singh
Technical Assistant
Mr. Pratap Singh
Technical Assistant
Mr. S.R. Mishra
OT Technician
Mr. Gopal Adhikari
OT Technician
Mr. Ram Asrey
OT Technician
Mr. Narender Singh
OT Technician
Mr. Devi Prasad
OT Assistant
Mr. Balam Singh Bisht
OT Assistant
Mr. Mahesh Sharma
OT Assistant
Mr. Bijender Singh
OT Assistant
Mr. Hukam Singh
OT Assistant
Mr. Laxman Singh
OT Assistant
Mr. Bablu
OT Assistant
Mr. Davender Kumar
OT Assistant
Mr. Chakleshwar Verma
OT Assistant
Miss. Neha Kaushik
OT Assistant
Mr. Abhay Kumar Gautam
OT Assistant
Mr. Praveen Kumar
OT Assistant
Mr. Pramod Kumar Sharma
OT Assistant
Mr. Ved Mitra
OT Assistant
Mr. Manoj Kumar
OT Assistant
Mr. Prem Das
OT Assistant
Mr. Dhirender Kishore
OT Assistant
Mr. Jitender Kumar
OT Assistant
Mr. Prem Shanker Sahu
OT Assistant
Mr. Ram Swaroop Meena
OT Assistant
Mr. Dharmender Kumar
OT Assistant
Mr. Saddam Hussain
OT Assistant
Mrs. Sujata Gupta
OT Assistant
Mrs.Githa G.S
OT Assistant
Mr. Suman Gowala
OT Assistant
Mr. Rupak Kumar
OT Assistant
Mr. Santanu Maity
OT Assistant
Ms. Shivani Sharma
OT Assistant
Ms. Renu Sharma
OT Assistant
Mr. Satyajeet
OT Assistant
Mr. Rakesh Kumar
OT Assistant
Mr. Sunder Singh
H/A
ICU (Neurology/ Neurosurgery) and Ward Technical Staff
Mr. Devender Kapoor
Technical Officer
Mr. Duli Chand
Technical Assistant
Mr. Nihal Singh
OT Technician
Mr. Janak Raj
OT Technician
Mr. Lalit Prasad
OT Technician
Mr. Chandan Singh
OT Assistant
Mr. Mozam Ali
OT Assistant
Mr. Ram Swaroop Meena
OT Assistant
Mr. Dharmpal
OT Assistant
Mr.Bijender Singh
OT Assistant
Mr. Pramod Kumar Sharma
OT Assistant
Mr. Marpu Giribabu
OT Assistant
Mr. Nitin
OT Assistant
Mr. Nishi Kumar
H/A
Mr. Virender Kumar
H/A
Mr. Anand
H/A
In India, the concept of “Neuroanaesthesia as a subspeciality” of Anaesthesia was recognized, way back in 1968, when Dr. Surinder Singh Saini volunteered to anaesthetize the neurosurgical patients at All India Institute of Medical Sciences (AIIMS), New Delhi, on a regular basis. Formal training in Neuroanaesthesia, for post-graduate degree holders (MD) of Anaesthesia, for trainees from all over India, was started in 1982. In 1987, an independent Department of Neuroanaesthesia was established under the leadership of Prof. S S Saini as the Head along with two more faculties, Dr. Hari Hara Dash as Assistant Professor and Dr. Parmod Kumar Bithal as Lecturer. Five Senior Resident (SR) doctors joined them for assisting the clinical activities of the department.
In August 1989, the Department was shifted to the newly built the Cardiothoracic and Neurosciences Centre (CNC) of AIIMS (present location) along with other sister departments. Facilities during that time included three well-equipped operation theatres (OTs), one emergency (septic) OT, which was shared with the cardiothoracic centre, five-bedded intensive care unit (ICU), and twenty beds for postoperative patients.
In 1995, a process to start three years superspeciality degree course (DM) in Neuroanaesthesiology was initiated under stewardship of Prof. H. H. Dash. It was materialized in 2001, when DM (SR) posts (Six direct and three sponsored) were sanctioned by the Institute body. In 2002, two direct candidates were enrolled, for the first time in India, through a common entrance test. After the JPNA Trauma Centre was established by AIIMS, in 2006, 10 more post of non-DM SR was added to the existing 10 posts. In the subsequent year (2007), two more posts of SR (DM) were again sanctioned making the final tally of open category DM (SR) seats as eight. At present, the department is located in the Neurosciences Centre, at 6/7th floor, with the office operated from room no. 709A. One personal assistant and two office assistants look after the smooth management official activities.
Currently, the Department of Neuroanaesthesiology has expanded its horizon; caters clinical service to six well-equipped neurosurgical OTs, a brain suite (MRI- OT), two neuro-cath Labs, two MRI facilities, One GammaKnife facility, one pain clinic, a pre-anaesthetic check-up (PAC) clinic, two neurosurgical ICUs (total 26 beds), one neurology ICU of five beds, more than two OTs for trauma patients, a twenty-bedded ICU for neurotrauma patients apart from providing resuscitation measures for neurological and neurosurgical ward patients. To meet with the demand of workload, the faculty strength now has been increased to sixteen which includes two professors, four additional professors, and ten assistant professors.
This department has been actively involved with training of Indian defense service personnel and overseas trainees apart from the DM and Non-DM trainees (SRs) of Neuroanaesthesia. So far, 25 candidates have been awarded the DM degree in Neuroanaesthesiology. The department plans to start Neurocritical Care programme in coming years, and to establish this super-speciality in India, the need for which is being realized, nation-wide. The faculty and staff of this department strive hard to ensure that the ‘Department of Neuroanaesthesiology’ continues to be the torch-bearer of perioperative neurosciences, and serve as a role model in this field.
| Name | Designation | ||
|---|---|---|---|
 | Dr Mihir Prakash Pandia | Professor & HOD | pandiamihir[at]gmail[dot]com |
 | Dr Hari Hara Dash | Emeritus Professor | dr.harihardash[at]gmail[dot]com |
 | Dr Parmod Kumar Bithal | Emeritus Professor | bithal.parmod[at]gmail[dot]com |
 | Dr Rajendra Singh Chouhan | Professor | chouhanrs[at]hotmail[dot]com |
 | Dr Girija Prasad Rath | Professor | girijarath[at]yahoo[dot]co[dot]in |
 | Dr Hemanshu Prabhakar | Professor | prabhakaraiims[at]yahoo[dot]co[dot]in |
 | Dr Gyaninder Pal Singh | Professor | drsingh_gp[at]yahoo[dot]co[dot]in |
 | Dr Ashish Bindra | Professor | dr_ashi2208[at]yahoo[dot]com |
 | Dr Niraj Kumar | Professor | drnirajaiims[at]gmail[dot]com |
 | Dr Keshav Goyal | Professor | keshavgoyal[at]yahoo[dot]co[dot]in |
| Dr Navdeep Sokhal | Professor | drnavdeep_kumar[at]yahoo[dot]com | |
 | Dr Charu Mahajan | Additional Professor | charushrikul[at]gmail[dot]com |
 | Dr Indu Kapoor | Additional Professor | dr.indu.me[at]gmail[dot]com |
| Dr Surya Kumar Dube | Additional Professor | surya.dube[at]gmail[dot]com | |
 | Dr Suman Gupta | Associate Professor | sumansokhal82[at]gmail[dot]com |
 | Dr Hirok Roy | Assistant Professor | hirokroy85[at]gmail[dot]com |
Prof. & Head
sharmamehar[at]yahoo[dot]co[dot]in
+919717739755
011-26549205
Professor
Surivaishali[at]yahoo[dot]co[dot]in
+919810254964
011-26544656
| Name | Designation | ||
|---|---|---|---|
| Dr Mihir Prakash Pandia | Professor & HOD | pandiamihir[at]gmail[dot]com |
| Dr Hari Hara Dash | Emeritus Professor | dr.harihardash[at]gmail[dot]com |
| Dr Parmod Kumar Bithal | Emeritus Professor | bithal.parmod[at]gmail[dot]com |
| Dr Rajendra Singh Chouhan | Professor | chouhanrs[at]hotmail[dot]com |
| Dr Girija Prasad Rath | Professor | girijarath[at]yahoo[dot]co[dot]in |
| Dr Hemanshu Prabhakar | Professor | prabhakaraiims[at]yahoo[dot]co[dot]in |
| Dr Gyaninder Pal Singh | Professor | drsingh_gp[at]yahoo[dot]co[dot]in |
| Dr Ashish Bindra | Professor | dr_ashi2208[at]yahoo[dot]com |
| Dr Niraj Kumar | Professor | drnirajaiims[at]gmail[dot]com |
| Dr Keshav Goyal | Professor | keshavgoyal[at]yahoo[dot]co[dot]in |
| Dr Navdeep Sokhal | Professor | drnavdeep_kumar[at]yahoo[dot]com | |
| Dr Charu Mahajan | Additional Professor | charushrikul[at]gmail[dot]com |
| Dr Indu Kapoor | Additional Professor | dr.indu.me[at]gmail[dot]com |
| Dr Surya Kumar Dube | Additional Professor | surya.dube[at]gmail[dot]com | |
| Dr Suman Gupta | Associate Professor | sumansokhal82[at]gmail[dot]com |
| Dr Hirok Roy | Assistant Professor | hirokroy85[at]gmail[dot]com |
<div class="row nmt-30 row-col">
<div class="mt-30 col-sm-6 col-md-4 col-lg-4 col-xl-3 col-15">
<div class="ShadowBox rounded-8 position-relative d-flex flex-wrap PDFBox">
<div class="w-100">
<div class="PDFIcon">
</div>
<h3 class="Heading18 Font600 Color-323232 Heading">
AIIMS Act Rules & Regulations
</h3>
</div>
<p class="pb-0">
<a class="FullLink Font-0 PDFDocIcon" href="/files/inline-document/Introduction.pdf" title="AIIMS Act Rules & Regulations" target="_blank">Introduction</a>
</p>
</div>
</div>
</div>
The Neuropathology laboratory, AIIMS was established by Professor Subimal Roy in mid 1970s. As the doyen of Neuropathology, he was one of those who introduced the specialty of Neuropathology in this country at a time when the branch was still evolving in other parts of the world. The Neuropathology laboratory delivers a wide range of diagnostic and research services with a particular expertise in neuro-oncology, epilepsy, inflammatory diseases of the CNS, neurodegenerative diseases, peripheral nerve and adult and paediatric muscle diseases. The research activities in this section have been widely cited and put on the global map of Neuropathology.
In India, the concept of “Neuroanaesthesia as a subspeciality” of Anaesthesia was recognized, way back in 1968, when Dr. Surinder Singh Saini volunteered to anaesthetize the neurosurgical patients at All India Institute of Medical Sciences (AIIMS), New Delhi, on a regular basis. Formal training in Neuroanaesthesia, for post-graduate degree holders (MD) of Anaesthesia, for trainees from all over India, was started in 1982. In 1987, an independent Department of Neuroanaesthesia was established under the leadership of Prof. S S Saini as the Head along with two more faculties, Dr. Hari Hara Dash as Assistant Professor and Dr. Parmod Kumar Bithal as Lecturer. Five Senior Resident (SR) doctors joined them for assisting the clinical activities of the department.
In August 1989, the Department was shifted to the newly built the Cardiothoracic and Neurosciences Centre (CNC) of AIIMS (present location) along with other sister departments. Facilities during that time included three well-equipped operation theatres (OTs), one emergency (septic) OT, which was shared with the cardiothoracic centre, five-bedded intensive care unit (ICU), and twenty beds for postoperative patients.
In 1995, a process to start three years superspeciality degree course (DM) in Neuroanaesthesiology was initiated under stewardship of Prof. H. H. Dash. It was materialized in 2001, when DM (SR) posts (Six direct and three sponsored) were sanctioned by the Institute body. In 2002, two direct candidates were enrolled, for the first time in India, through a common entrance test. After the JPNA Trauma Centre was established by AIIMS, in 2006, 10 more post of non-DM SR was added to the existing 10 posts. In the subsequent year (2007), two more posts of SR (DM) were again sanctioned making the final tally of open category DM (SR) seats as eight. At present, the department is located in the Neurosciences Centre, at 6/7th floor, with the office operated from room no. 709A. One personal assistant and two office assistants look after the smooth management official activities.
Currently, the Department of Neuroanaesthesiology has expanded its horizon; caters clinical service to six well-equipped neurosurgical OTs, a brain suite (MRI- OT), two neuro-cath Labs, two MRI facilities, One GammaKnife facility, one pain clinic, a pre-anaesthetic check-up (PAC) clinic, two neurosurgical ICUs (total 26 beds), one neurology ICU of five beds, more than two OTs for trauma patients, a twenty-bedded ICU for neurotrauma patients apart from providing resuscitation measures for neurological and neurosurgical ward patients. To meet with the demand of workload, the faculty strength now has been increased to sixteen which includes two professors, four additional professors, and ten assistant professors.
This department has been actively involved with training of Indian defense service personnel and overseas trainees apart from the DM and Non-DM trainees (SRs) of Neuroanaesthesia. So far, 25 candidates have been awarded the DM degree in Neuroanaesthesiology. The department plans to start Neurocritical Care programme in coming years, and to establish this super-speciality in India, the need for which is being realized, nation-wide. The faculty and staff of this department strive hard to ensure that the ‘Department of Neuroanaesthesiology’ continues to be the torch-bearer of perioperative neurosciences, and serve as a role model in this field.
In India, the concept of “Neuroanaesthesia as a subspeciality” of Anaesthesia was recognized, way back in 1968, when Dr. Surinder Singh Saini volunteered to anaesthetize the neurosurgical patients at All India Institute of Medical Sciences (AIIMS), New Delhi, on a regular basis. Formal training in Neuroanaesthesia, for post-graduate degree holders (MD) of Anaesthesia, for trainees from all over India, was started in 1982. In 1987, an independent Department of Neuroanaesthesia was established under the leadership of Prof. S S Saini as the Head along with two more faculties, Dr. Hari Hara Dash as Assistant Professor and Dr. Parmod Kumar Bithal as Lecturer. Five Senior Resident (SR) doctors joined them for assisting the clinical activities of the department.
In August 1989, the Department was shifted to the newly built the Cardiothoracic and Neurosciences Centre (CNC) of AIIMS (present location) along with other sister departments. Facilities during that time included three well-equipped operation theatres (OTs), one emergency (septic) OT, which was shared with the cardiothoracic centre, five-bedded intensive care unit (ICU), and twenty beds for postoperative patients.
In 1995, a process to start three years superspeciality degree course (DM) in Neuroanaesthesiology was initiated under stewardship of Prof. H. H. Dash. It was materialized in 2001, when DM (SR) posts (Six direct and three sponsored) were sanctioned by the Institute body. In 2002, two direct candidates were enrolled, for the first time in India, through a common entrance test. After the JPNA Trauma Centre was established by AIIMS, in 2006, 10 more post of non-DM SR was added to the existing 10 posts. In the subsequent year (2007), two more posts of SR (DM) were again sanctioned making the final tally of open category DM (SR) seats as eight. At present, the department is located in the Neurosciences Centre, at 6/7th floor, with the office operated from room no. 709A. One personal assistant and two office assistants look after the smooth management official activities.
Currently, the Department of Neuroanaesthesiology has expanded its horizon; caters clinical service to six well-equipped neurosurgical OTs, a brain suite (MRI- OT), two neuro-cath Labs, two MRI facilities, One GammaKnife facility, one pain clinic, a pre-anaesthetic check-up (PAC) clinic, two neurosurgical ICUs (total 26 beds), one neurology ICU of five beds, more than two OTs for trauma patients, a twenty-bedded ICU for neurotrauma patients apart from providing resuscitation measures for neurological and neurosurgical ward patients. To meet with the demand of workload, the faculty strength now has been increased to sixteen which includes two professors, four additional professors, and ten assistant professors.
This department has been actively involved with training of Indian defense service personnel and overseas trainees apart from the DM and Non-DM trainees (SRs) of Neuroanaesthesia. So far, 25 candidates have been awarded the DM degree in Neuroanaesthesiology. The department plans to start Neurocritical Care programme in coming years, and to establish this super-speciality in India, the need for which is being realized, nation-wide. The faculty and staff of this department strive hard to ensure that the ‘Department of Neuroanaesthesiology’ continues to be the torch-bearer of perioperative neurosciences, and serve as a role model in this field.

MBBS, MD, DM
Associate Professor
Department of Neurology
Room number 704, 7thFloor,Neurosciences Centre
Phone No – 01126593662
Email : vishnuvy16[at]aiims[dot]edu
OPD: Tuesday/Friday Room No. 5, Neurosciences Centre, Ground Floor
Comprehensive Neuromuscular Disorders (CNMD) Clinic: Tuesday, Room No. 5, Neurosciences Centre, Ground Floor
Comprehensive Stroke clinic: Saturday, Room No.20, Neurosciences Centre, Ground Floor
Dr. Vishnu was born in Southern-most state of India, Kerala. He is currently working as Associate Professor, Neurology at the All India Institute of Medical Sciences (AIIMS), New Delhi, India.
Training:He completed his medical school (under graduation – MBBS) at Government Medical College, Thiruvananthapuram, Kerala, India. Following this he pursued his MD residency in Internal medicine from JIPMER, Puducherry and three-year residency (DM) in Neurology at PGIMER Chandigarh. He is currently pursuing an MRC funded split-site fellowship in Neuromuscular Genomic Medicine with UK supervising centre being Queen Square Institute of Neurology. He is also selected for the inaugural World Stroke Organisation Future Leaders Programme. He has received training in Cochrane systematic reviews and meta-analysis at Cochrane South Asia.
Research Interests: His research areas include Neuromuscular disorders, Stroke, Primary CNS vasculitis, Machine learning and Evidence based medicine. He has established a GBS Consortium of more than 30 centres. Dr.Vishnu is Incharge of AIIMS Comprehensive Neuromuscular disorders clinic (AIIMS-CNMD). He runs the multinational ICGNMD project in AIIMS New Delhi. In stroke, currently he is involved as PI in an investigator-initiated RCT on role of prophylactic levetiracetam for primary prevention of post stroke seizures. He is a co-PI in an on-going machine learning project on early diagnosis of stroke in resource limited settings in collaboration with IIT Delhi. He is the PI of the AIIMS Primary CNS Vasculitis Registry and has an ongoing funded project on CSF and blood biomarkers in PCNSV. He is also involved in two Cochrane systematic reviews on HIV related neuropathy. He is the co-creator of a machine-learning based ios app for neurological differential diagnosis which was subsequently validated in multicentre study.
Dr. Vishnu has a group of passionate researchers who believe in multidisciplinary collaborative research to find innovative solutions to problems that Neurologists face in our part of the world. The team’s research ethics is strongly based on adherence to principles of Evidence Based Medicine. The team believes that their greatest strength lies in adherence to the core values of scientific integrity, accountability, honesty, racial and gender equality in all situations.
Ongoing projects as PI
1. A randomised double blind study of prophylactic levetiracetam for the prevention of post stroke seizures (PROLEVIS) – A multicentre Investigator initiated academic trial (Funded by SERB, Department of Science and Technology, Government of India)
2. Machine Learning model for early diagnosis of stroke in resource limited settings: Pilot study: A collaborative project with IIT Delhi (Funded by DBT, Government of India)
3. Identification of pathobiological and disease activity markers in Primary CNS Vasculitis (Funded by ICMR, Government of India)
4.Prevention of post-stroke seizures with Levetiracetam in Intracranial Cerebral Venous Sinus Thrombosis (PROLEVIS-CVT): A Randomized Placebo-Controlled Trial (Funded by DHR)
5. Identification of genetic vasculopathies among a cohort of Primary CNS Vasculitis using whole-exome sequencing (Intramural grant)
6. AIIMS Primary CNS Vasculitis Registry>
7. GBS Consortium
8. The first investigation of the genetic causes of Facioscapulohumeral muscular dystrophy (FSHD) in the Indian population: AIIMS-UCL Intramural grant
Ongoing projects as Co-PI
1. Smartphone based Telestroke Vs ‘Stroke Physician’ led Acute Stroke Management (SMART INDIA): A cluster randomised trial (Funded by DHR, Government of India)
2. International Centre for Genomic Medicine in Neuromuscular Diseases (ICGNMD)"- Funded by the Medical Research Council, UK (PI: Prof. MV Padma Srivastava, AIIMS New Delhi)
3. WSO FLP Grant- Establishing Organized Stroke Care In Low-And-Middle Income Countries: From Training of Non-Specialist to Implementation
1. Citicoline in Acute Ischemic Stroke undergoing revascularisation therapy- Investigator initiated academic trial- Funded by Intramural grant from AIIMS, New Delhi
2. International Neuromuscular COVID database
3. BRAHMI (Bacopa Monnieri) for Dementia due to Alzheimer’s Disease- Systematic Review and Meta-analysis (Funded by ICMR, Government of India)
4. Comparison of diagnostic accuracy between neurology residents and a novel neurology App on an iOS platform: A multi-centre cross sectional observational study
1. American Academy of Neurology Young Investigator: International scholarship award – 2015
2. World Stroke Congress: Young Investigator Award: 2018
3. Department of Science and Technology- SERB- Early career award- 2017
4. International travel grant for World Congress of Neurology, Kyoto, 2017
5. David Sackett Memorial Award for Outstanding Performance at International course in Health Research methods and Evidence based medicine, St John’s Hospital in collaboration with Macmaster’s University, Canada
6. First Prize in group presentations at International course in Health Research methods and Evidence based medicine, St John’s Hospital in collaboration with Macmaster’s University, Canada
Total publications: 150
Top 25 publications
2022
2021
2020
2019
2018
2017
2016
2015
2014
2013
2012
Ms. Jyoti Sharma
Book chapter
Chapters
In India, the concept of “Neuroanaesthesia as a subspeciality” of Anaesthesia was recognized, way back in 1968, when Dr. Surinder Singh Saini volunteered to anaesthetize the neurosurgical patients at All India Institute of Medical Sciences (AIIMS), New Delhi, on a regular basis. Formal training in Neuroanaesthesia, for post-graduate degree holders (MD) of Anaesthesia, for trainees from all over India, was started in 1982. In 1987, an independent Department of Neuroanaesthesia was established under the leadership of Prof. S S Saini as the Head along with two more faculties, Dr. Hari Hara Dash as Assistant Professor and Dr. Parmod Kumar Bithal as Lecturer. Five Senior Resident (SR) doctors joined them for assisting the clinical activities of the department.
In August 1989, the Department was shifted to the newly built the Cardiothoracic and Neurosciences Centre (CNC) of AIIMS (present location) along with other sister departments. Facilities during that time included three well-equipped operation theatres (OTs), one emergency (septic) OT, which was shared with the cardiothoracic centre, five-bedded intensive care unit (ICU), and twenty beds for postoperative patients.
In 1995, a process to start three years superspeciality degree course (DM) in Neuroanaesthesiology was initiated under stewardship of Prof. H. H. Dash. It was materialized in 2001, when DM (SR) posts (Six direct and three sponsored) were sanctioned by the Institute body. In 2002, two direct candidates were enrolled, for the first time in India, through a common entrance test. After the JPNA Trauma Centre was established by AIIMS, in 2006, 10 more post of non-DM SR was added to the existing 10 posts. In the subsequent year (2007), two more posts of SR (DM) were again sanctioned making the final tally of open category DM (SR) seats as eight. At present, the department is located in the Neurosciences Centre, at 6/7th floor, with the office operated from room no. 709A. One personal assistant and two office assistants look after the smooth management official activities.
Currently, the Department of Neuroanaesthesiology has expanded its horizon; caters clinical service to six well-equipped neurosurgical OTs, a brain suite (MRI- OT), two neuro-cath Labs, two MRI facilities, One GammaKnife facility, one pain clinic, a pre-anaesthetic check-up (PAC) clinic, two neurosurgical ICUs (total 26 beds), one neurology ICU of five beds, more than two OTs for trauma patients, a twenty-bedded ICU for neurotrauma patients apart from providing resuscitation measures for neurological and neurosurgical ward patients. To meet with the demand of workload, the faculty strength now has been increased to sixteen which includes two professors, four additional professors, and ten assistant professors.
This department has been actively involved with training of Indian defense service personnel and overseas trainees apart from the DM and Non-DM trainees (SRs) of Neuroanaesthesia. So far, 25 candidates have been awarded the DM degree in Neuroanaesthesiology. The department plans to start Neurocritical Care programme in coming years, and to establish this super-speciality in India, the need for which is being realized, nation-wide. The faculty and staff of this department strive hard to ensure that the ‘Department of Neuroanaesthesiology’ continues to be the torch-bearer of perioperative neurosciences, and serve as a role model in this field.
कोविड-19 मानसिक स्वास्थ्य हेल्पलाइन - एम्स संकाय, रेजीडेंट और कर्मचारी

AIIMS First Prize winner of kaya kalp

Bio Medical Waste Trolleys

Card board boxes for glassware


Kaya Kalp Inspection

Resource Material

Sewage Treament Plant

STP Sludge

Temporary Storage Facility

Training Session for Bio Medical Waste mgmt workers

Training session

Trial Access of "MedOne Plastic Surgery Platform" through BBD Library
All India Institute of Medical Sciences (AIIMS), New Delhi
Bhalchandra Babaji Dikshit
Bhalchandra Babaji Dikshit was an Indian physician, specialist in Pharmacology & Physiology. He has done research in Tropical Diseases (Plague, Malaria etc.). Toured U.S.A. & Western Europe. Author of about 35 articles and research papers. Bhalchandra Babaji Dikshit was born on the 2nd of September, 1902 in Amravati, India. Bhalchandra Babaji Dikshit studied at Bombay University and received Bachelor of Medicine and Bachelor of Surgery degrees. In 1926 he graduated from Calcutta University - Doctor of Public Health; in 1934 - Edinburgh University - Doctor of Philosophy. Fellow: Royal College of Physicians (Edinburgh.), Royal Society (Edinburgh), National Institute of Sciences of India. Bhalchandra Babaji Dikshit was the first director of All India Institute of Medical Sciences in New Delhi.
Email :- refquery@aiims.edu
Email :- refquery@aiims.edu
| eISBN | Author | Title | Year | Hyperlink |
| 9781498710343 | Sherif Emil | Clinical Pediatric Surgery: A Case-Based Interactive Approach: A Case-Based Interactive Approach | 2020 | http://www.taylorfrancis.com/books/9781498710343 |
| 9781351250801 | Mark Davenport; James D. Geiger; Nigel J. Hall; Steven S. Rothenberg | Operative Pediatric Surgery | 2021 | http://www.taylorfrancis.com/books/9781351250801 |
| 9780429027789 | Alejandra Vilanova-Sánchez; Marc A. Levitt | Pediatric Colorectal and Pelvic Reconstructive Surgery | 2020 | http://www.taylorfrancis.com/books/9780429027789 |
| 9781315113746 | David E. Wesson; Bindi Naik-Mathuria | Pediatric Trauma: Pathophysiology, Diagnosis, and Treatment | 2017 | http://www.taylorfrancis.com/books/9781315113746 |
| eISBN | Author | Title | Year | Hyperlink |
| 9781498710343 | Sherif Emil | Clinical Pediatric Surgery: A Case-Based Interactive Approach: A Case-Based Interactive Approach | 2020 | http://www.taylorfrancis.com/books/9781498710343 |
| 9781351250801 | Mark Davenport; James D. Geiger; Nigel J. Hall; Steven S. Rothenberg | Operative Pediatric Surgery | 2021 | http://www.taylorfrancis.com/books/9781351250801 |
| 9780429027789 | Alejandra Vilanova-Sánchez; Marc A. Levitt | Pediatric Colorectal and Pelvic Reconstructive Surgery | 2020 | http://www.taylorfrancis.com/books/9780429027789 |
| 9781315113746 | David E. Wesson; Bindi Naik-Mathuria | Pediatric Trauma: Pathophysiology, Diagnosis, and Treatment | 2017 | http://www.taylorfrancis.com/books/9781315113746 |
 | Access Medicine |
 | JAMAevidence |
 | Oxford Medicine Online (Oxford's Textbooks) |
| Ovid E- book collection | |
| E- Books of Clinical & Laboratory Standards Institute (CLSI) Standards and Guidelines for Medical Professionals | Book List |
| Taylor and Francis books | Book List |
| Access Medicine |
| JAMAevidence |
| Oxford Medicine Online (Oxford's Textbooks) |
| Ovid E- book collection | |
| E- Books of Clinical & Laboratory Standards Institute (CLSI) Standards and Guidelines for Medical Professionals | Book List |
| Taylor and Francis books | Book List |
| 1. | Alphabetical List-2024 |
| 2. | Publisher Wise list-2024 |
| 3. | NDDTC Library Subscribed Journals List |
| 1. | Alphabetical List-2024 |
| 2. | Publisher Wise list-2024 |
| 3. | NDDTC Library Subscribed Journals List |
| 1. | Alphabetical List |
| 2. | Publisher Wise list |
| 1. | Alphabetical List |
| 2. | Publisher Wise list |
 | BMJ Best Practice |
 | BMJ Case Reports |
 | BMJ Learning |
 | BMJ Research to Publication |
 | EMBASE |
 | UpToDate |
 | Web of Science |
| S.No. | Title |
| 1 | Knimbus Remote Access |
| 2 | OpenAthens (Faculty Only) |
Trial Access of "MedOne Plastic Surgery Platform" through BBD Library
All India Institute of Medical Sciences (AIIMS), New Delhi
Bhalchandra Babaji Dikshit
Bhalchandra Babaji Dikshit was an Indian physician, specialist in Pharmacology & Physiology. He has done research in Tropical Diseases (Plague, Malaria etc.). Toured U.S.A. & Western Europe. Author of about 35 articles and research papers. Bhalchandra Babaji Dikshit was born on the 2nd of September, 1902 in Amravati, India. Bhalchandra Babaji Dikshit studied at Bombay University and received Bachelor of Medicine and Bachelor of Surgery degrees. In 1926 he graduated from Calcutta University - Doctor of Public Health; in 1934 - Edinburgh University - Doctor of Philosophy. Fellow: Royal College of Physicians (Edinburgh.), Royal Society (Edinburgh), National Institute of Sciences of India. Bhalchandra Babaji Dikshit was the first director of All India Institute of Medical Sciences in New Delhi.
All India Institute of Medical Sciences (AIIMS) was established by the Act of Parliament in 1956 as anautonomous institute to set patterns in Undergraduate and Postgraduate Medical Education in all its branches to demonstrate a high standard of medical education. This is the only institute outside the jurisdiction of Medical Council of India to encourage experiments in the curriculum. New AIIMS are also created on the pattern of AIIMS. New Delhi. It mainly follows a disciplinary structure. However, since inception, AIIMS has been constantly upgrading its course content in tunewith the changing needs.
Courses at AIIMS New Delhi at a glance
| UNDERGRADUATE | MBBS | B.Sc. Nursing (Hons.) | B.Sc. Nursing Post Basic |
| B.Sc. (Hons) in Medical Technology in Radiography | Bachelor of Optometry
| B.Sc. (OTT)
| |
| B.Sc. (Dental Room Asstt.) | B.Sc. (Dental Hygiene) | ||
| POSTGRADUATE (M.Sc Nursing/Biotech) | M.Biotech | M.Sc. Courses | M.Sc. Nursing |
| POSTGRADUATE | MD/MS/MDS | DM (6 yrs.) | M.Ch (6 yrs.)
|
| MD Hospital Administration | |||
| SUPERSPECIALTY | DM | M.Ch | |
| DOCTORAL | Fellowship | Ph.D | |
| RESIDENCY | Junior Resident | Senior Resident | Senior Demonstrator |
Syllabus of Various Academic Courses and Residents' Manual
| Guidelines for Academic Courses, Awards and Orations at AIIMS - IInd Edition |
| ALL ABOUT M.B.B.S. COURSE AT AIIMS |
| Syllabus for MBBS |
| Syllabus for B.Sc. Nursing (Hons) and B.Sc. (Post Basic)Nursing |
| Syllabus for B.Sc Ophthalmic/Radio. Techniques |
| Syllabus for MD/MS/MDS/MHA |
| Syllabus for M.Sc & M.Biotech |
| Syllabus for M.Sc (Nursing) |
| Syllabus for DM/M.Ch |
| Residents' Manual |
| Format for submission of thesis and dissertation/projects involving research in human subjects for clearance by Ethics Committee of AIIMS |
| Syllabus for M.Sc. (Reproductive Biology & Clinical Embryology) |
Guidelines for Academic Courses, Awards and Orations at AIIMS - IInd Edition
Syllabus for M.Sc. (Reproductive Biology & Clinical Embryology)
Format for submission of thesis and dissertation/projects involving research in human subjects for clearance by Ethics Committee of AIIMS
CONSTITUTION OF INSTITUTE ETHICS COMMITTEE |
| FORMAT FOR SUBMISSION OF PROJECTS INVOLVING RESEARCH IN HUMAN SUBJECTS FOR CLEARANCE BY ETHICS COMMITTEE OF AIIMS |
| FORMAT FOR SUBMISSION OF PROTOCOL INVOLVING RESEARCH IN HUMAN SUBJECTS FOR CLEARANCE BY ETHICS SUB-COMMITTEE AND COMMITTEE OF AIIMS FOR DM / M.Ch / Ph.D/ MD / MS / MHA / M.Sc / M.Biotech. STUDENTS (FOR THESIS OR DISSERTATION) |
Format for submission of thesis and dissertation/projects involving research in human subjects for clearance by Ethics Committee of AIIMS
1. Perioperative monitoring and anaesthetic issues during robotic surgery. Symposium on Anaesthesia for Robotic Surgery.PGIMER Chandigarh. 18th April 2015
2. Management of a 2year old child with Pierre Robin sequence who develops acute airway edema following tonsillectomy. 7th National Conference of the Indian Association of Paediatric Anaesthesiologists. PGIMER Chandigarh. 22nd Feb 2015
3. Malignant Hyperthermia in India. 6th Annual Conference of the Indian College of Anaesthesiologists. Narayan Hridyalaya. Bengaluru on 21st Nov 2014.
4. Perioperative fluid therapy in Paediatric patients. Comprehensive Review in Anaesthesiology & Critical care. SN Medical College Agra on 8th Nov 2014.
5. Paravertebral block- nerve block of promise. Principles and practice of Pediatric Anaesthesia.PGIMER Chandigarh 28th Sept 2014.
6. Anticoagulants and antiplatelets implications for the regionalists. 4th National Conference of Academy of Regional Anaesthesia (AORA) of India. New Delhi, 20th Sep 2014.
7. Pro-con debate on “Regional anaesthesia for Bronchitic vasculopath on antiplatelets. Cadence 2014 (Cardiovascular disease in Noncardiac surgery);Medanta, the Medicity on 13th September 2014.
1. Perioperative monitoring and anaesthetic issues during robotic surgery. Symposium on Anaesthesia for Robotic Surgery.PGIMER Chandigarh. 18th April 2015
2. Management of a 2year old child with Pierre Robin sequence who develops acute airway edema following tonsillectomy. 7th National Conference of the Indian Association of Paediatric Anaesthesiologists. PGIMER Chandigarh. 22nd Feb 2015
3. Malignant Hyperthermia in India. 6th Annual Conference of the Indian College of Anaesthesiologists. Narayan Hridyalaya. Bengaluru on 21st Nov 2014.
4. Perioperative fluid therapy in Paediatric patients. Comprehensive Review in Anaesthesiology & Critical care. SN Medical College Agra on 8th Nov 2014.
5. Paravertebral block- nerve block of promise. Principles and practice of Pediatric Anaesthesia.PGIMER Chandigarh 28th Sept 2014.
6. Anticoagulants and antiplatelets implications for the regionalists. 4th National Conference of Academy of Regional Anaesthesia (AORA) of India. New Delhi, 20th Sep 2014.
7. Pro-con debate on “Regional anaesthesia for Bronchitic vasculopath on antiplatelets. Cadence 2014 (Cardiovascular disease in Noncardiac surgery);Medanta, the Medicity on 13th September 2014.
You are welcome to AIIMS, the premier Medical Institute of India. AIIMS is committed to provide quality services and medical care to each and every citizen coming to AIIMS. In line with our mandate. We, at AIIMS, strive hard to provide comprehensive, high quality tertiary care services (specialty and super-specialty services) to our users. However, there may be some deficiencies due to extreme patient load and limited resources.
This charter seeks to provide a frame work, which enables our users to know:
Please Help Us Serve You Better Facilities Available Are Subject To Change Without Any Prior Notice
You are welcome to AIIMS, the premier Medical Institute of India. AIIMS is committed to provide quality services and medical care to each and every citizen coming to AIIMS. In line with our mandate. We, at AIIMS, strive hard to provide comprehensive, high quality tertiary care services (specialty and super-specialty services) to our users. However, there may be some deficiencies due to extreme patient load and limited resources.
This charter seeks to provide a frame work, which enables our users to know:
Please Help Us Serve You Better Facilities Available Are Subject To Change Without Any Prior Notice
Verification of documents and certificates issued by the Academic Section, AIIMS, New Delhi
MOM of Dean Committee
MoM of Academic Committee
The SET (Skills, e-Learning, Telemedicine) Facility is a state of art facility set up to modernise and update medical education at the institute. It imparts skill based learning to medical undergraduates, postgraduates and nursing staff so that they are better prepared when managing patients in wards and clinics. The facility has active involvement of faculty members from various clinical and non-clinical departments who develop the training modules and teaching content and impart hands-on teaching to the students. The skill lab provides a stress free environment to learn skills. The other aspects of the facility are to develop e-learning modules and to impart education through telemedicine linkages with medical colleges and hospitals across India.
The patient welfare services are in the continuum of hospital services extending to the identification and removing barriers that may be limiting effective engagement of patients with healthcare services.
For poor & indigent patients with BPL Ration Card, low income certificate and those who fall into BPL category as per the latest State/UT-wise threshold poverty line for Rural & Urban areas (Revised per capita threshold income per month w.e.f. 01.01.2019 under Umbrella Scheme of Rashtriya Arogya Nidhi - MoHFW, [DOWNLOAD] following services are given by competent authority:
In addition to the above mentioned, following services are also extended for patient welfare:
Patients and their care-givers may contact their concerned Medical Social Service Officer for availing these services.
The patient welfare services are in the continuum of hospital services extending to the identification and removing barriers that may be limiting effective engagement of patients with healthcare services.
For poor & indigent patients with BPL Ration Card, low income certificate and those who fall into BPL category as per the latest State/UT-wise threshold poverty line for Rural & Urban areas (Revised per capita threshold income per month w.e.f. 01.01.2019 under Umbrella Scheme of Rashtriya Arogya Nidhi - MoHFW, [DOWNLOAD] following services are given by competent authority:
In addition to the above mentioned, following services are also extended for patient welfare:
Patients and their care-givers may contact their concerned Medical Social Service Officer for availing these services.
Orations/Guest Lecture
The success of this charter depends on the support we receive from our users.
Please try to appreciate the various constraints under which the hospital is functioning. On an average, 7200 patients attend the OPD daily & more than 400-500 patients visit Casualty daily.
Please follow the rules and regulations of the hospital while inside the hospital campus.
Please do not cause inconvenience to other patients by crowding or making noise unnecessarily.
Please help us in keeping the hospital and its surroundings neat and clean.
Please don't argue with security guards, show your passes when asked for & help maintain the order and peace inside the hospital premises.
Please use the facilities of this hospital with care and do not damage/ spoil hospital property.
Beware of Touts & unauthorized persons. Don't indulge in any money transactions with them.
The Hospital is a No Smoking Zone. Please don't indulge in any money transactions with them.
Please refrain from demanding under favours from the staff and officials.
Please provide useful feedback and constructive suggestions. These may be addressed to the Medical Superintendent of the Hospital.
Academic Awards for Students
The success of this charter depends on the support we receive from our users.
Please try to appreciate the various constraints under which the hospital is functioning. On an average, 7200 patients attend the OPD daily & more than 400-500 patients visit Casualty daily.
Please follow the rules and regulations of the hospital while inside the hospital campus.
Please do not cause inconvenience to other patients by crowding or making noise unnecessarily.
Please help us in keeping the hospital and its surroundings neat and clean.
Please don't argue with security guards, show your passes when asked for & help maintain the order and peace inside the hospital premises.
Please use the facilities of this hospital with care and do not damage/ spoil hospital property.
Beware of Touts & unauthorized persons. Don't indulge in any money transactions with them.
The Hospital is a No Smoking Zone. Please don't indulge in any money transactions with them.
Please refrain from demanding under favours from the staff and officials.
Please provide useful feedback and constructive suggestions. These may be addressed to the Medical Superintendent of the Hospital.
There will be occasions when our services will not be up to your expectations.
Please do not hesitate to register your complaints. It will only help as serve you better.
You may lodge your complaints to the Duty Officer in Control Room. Every complaint will be duly acknowledged and sincere attempt will be made to solve your problem.
Anti Ragging Duty Roster
There will be occasions when our services will not be up to your expectations.
Please do not hesitate to register your complaints. It will only help as serve you better.
You may lodge your complaints to the Duty Officer in Control Room. Every complaint will be duly acknowledged and sincere attempt will be made to solve your problem.
Patients admitted in General Ward of AIIMS have to deposit bed charges in advance of 10 days at the rates approved by Government time to time (currently Rs. 375). This entitles them for doctor consultations, certain basic investigations, life saving medicines and surgical items, diet, linen, I.V. fluids etc.
For allotment inPrivate Wards, after recommendation by the treating doctor, patient should contact the Medical Superintendent Office. A waiting list is maintained and the private room is allotted as per the witting list. The hospitalization charges of private room are as under:-
Deluxe (A Class) - Room rent Rs. 6300/- per day( + Diet Charges Rs.300/- per in addition)
Semi Deluxe(B Class) - Rs. 3000 per day ( + Diet Charges Rs.300/- per in addition)
Private ward patients are charged additionally for specific investigations, procedures, operations etc.
All in-patients receive treatment by team of Resident Doctors and Nurses, available round the clock, under the supervision and guidance of Faculty Members of AIIMS.
Hospital Attendantsare available in different wards to help in patient care and related activities.
All the wards are fully equipped with modern gadgets & equipments e.g. ventilators, monitors, defibrillators, nebulisers; central O2& suction supply etc. to provide top quality medical care.
Indoor services have central air conditioning, hot and cold water, toilets, portable X-ray machines, ECG services - (2nd floor, C2ward), Generator back up, emergency lights, internal telephone, chairs for attendants etc.
Waste disposalis done as per the established rules (Biomedical waste management and handling rules, 1998) and utmost care is taken to keep the premises neat and clean.
Every inpatient is provided with two attendant passes.
Visitors are allowed only during notified visiting hours i.e.4:00 p.m. to 6:00 p.m.
Special Investigations likeUSG, CT, MRIetc. are changed as per the rates approved by Government and revised from time to time.
For very poor patients, on recommendation of treating Doctor, the hospital charges may be waived off by Med. Supdt./ his nominee and costly drugs/surgical items may be provided by the hospital.
Financial assistance is also available through Prime Minister's Relief Fund, NIAF and other suchfunds. You may contact Medical Social Service Dept. & Welfare Officer in this regard.
Bed linenis changed at the time of admission, thereafter on every alternate day and also whenever required.
Foodis served three times a day. Also,Teais provided in the morning.
Facilities provided in private ward- Each room has - attached toilets & bath room, T.V. with cable connection, Refrigerator, A.C., sofas, bed for attendant, chairs and table, geyser, emergency light, phone with incoming facility etc.
Destitute unattended patientsare provided with attendants from hospital, drugs & surgical items are provided from hospital and all hospital charges are waived. Medical Social Service Officers help in location and calling the relatives/family members of unattended/unknown patients Destitute patients are relocated to some destitute home after discharge from hospital.
Short Admissionsrequiring stay for less than 24 hours are done for minor illness/some investigations/Interventions. At present the admission charges for this are Rs. 60/-
Day care facilityis available for certain types of operations. e.g. laproscopic surgery; day care chemotherapy; blood transfusion, dialysis, endoscopies and similar interventions.
Operation Theratres
The institute has fully equipped modern Operation Theatres, where all kinds of major and minor surgeries are performed using the latest techniques and technology.
For routine surgeries, the respective departments maintain waiting list. Patients are called and operated upon as per the waiting list. But, in case of emergencies/urgencies, the out of turn surgeries are also performed, at the discretion at the treating doctors.
The patient should get his Pre-Anaesthetic check up done in PAC Room on 5th floor OPD Block during afternoon before getting admitted for operation and follow the instructions given by the treating Doctors.
ICUsThe hospital has fully equipped Main ICU at 8th Floor, AB wing to provide expert ICU care. There are ICUs/HDUs in few wards of main hospital and CTVS ICU & NS ICU in CN Centre. Patients requiring urgent ICU care are admitted to ICUs at the discretion of treating Doctors.
Laboratory Services
Emergency Lab - 24 hours, throughout the year, for all emergency investigations.
Routine Lab - Sample Collection Timings:- Weeks Days - 8:30 a.m. to 10:30 a.m.
Saturday - 8:30 a.m. to 10:00 a.m.
All type of routine and special investigations incl. Biochemical, microbiological, pathology, immunology and genetic studies are done at AIIMS.
Blood Bank:-AIIMS has a licensed modern, state of the art Blood Bank that functions 24 hours a day and provides facilities for blood donation, storage, issue of blood and its components. Strict precautions are taken and testing is done to prevent any borne infection. If your patient requires blood transfusions, then you are requested to arrange healthy blood donors for donating blood in order to reduce shortage of blood.
Miscellaneous Facilities
Ambulance facility is available to transfer patients to other hospitals or meet any exigency/disaster situation.
If required, patients' attendants may stay in Raj Gharia Dharamshala / Sureka Vishram Sadanafter paying the prevailing charges situated near the East Campus of AIIMS.
Free battery operated vans(Parikrama Sewa)are available for transporting patients and attendants with in the campus.
Enrollment List at AIIMS New Delhi
Patients admitted in General Ward of AIIMS have to deposit bed charges in advance of 10 days at the rates approved by Government time to time (currently Rs. 375). This entitles them for doctor consultations, certain basic investigations, life saving medicines and surgical items, diet, linen, I.V. fluids etc.
For allotment inPrivate Wards, after recommendation by the treating doctor, patient should contact the Medical Superintendent Office. A waiting list is maintained and the private room is allotted as per the witting list. The hospitalization charges of private room are as under:-
Deluxe (A Class) - Room rent Rs. 6300/- per day( + Diet Charges Rs.300/- per in addition)
Semi Deluxe(B Class) - Rs. 3000 per day ( + Diet Charges Rs.300/- per in addition)
Private ward patients are charged additionally for specific investigations, procedures, operations etc.
All in-patients receive treatment by team of Resident Doctors and Nurses, available round the clock, under the supervision and guidance of Faculty Members of AIIMS.
Hospital Attendantsare available in different wards to help in patient care and related activities.
All the wards are fully equipped with modern gadgets & equipments e.g. ventilators, monitors, defibrillators, nebulisers; central O2& suction supply etc. to provide top quality medical care.
Indoor services have central air conditioning, hot and cold water, toilets, portable X-ray machines, ECG services - (2nd floor, C2ward), Generator back up, emergency lights, internal telephone, chairs for attendants etc.
Waste disposalis done as per the established rules (Biomedical waste management and handling rules, 1998) and utmost care is taken to keep the premises neat and clean.
Every inpatient is provided with two attendant passes.
Visitors are allowed only during notified visiting hours i.e.4:00 p.m. to 6:00 p.m.
Special Investigations likeUSG, CT, MRIetc. are changed as per the rates approved by Government and revised from time to time.
For very poor patients, on recommendation of treating Doctor, the hospital charges may be waived off by Med. Supdt./ his nominee and costly drugs/surgical items may be provided by the hospital.
Financial assistance is also available through Prime Minister's Relief Fund, NIAF and other suchfunds. You may contact Medical Social Service Dept. & Welfare Officer in this regard.
Bed linenis changed at the time of admission, thereafter on every alternate day and also whenever required.
Foodis served three times a day. Also,Teais provided in the morning.
Facilities provided in private ward- Each room has - attached toilets & bath room, T.V. with cable connection, Refrigerator, A.C., sofas, bed for attendant, chairs and table, geyser, emergency light, phone with incoming facility etc.
Destitute unattended patientsare provided with attendants from hospital, drugs & surgical items are provided from hospital and all hospital charges are waived. Medical Social Service Officers help in location and calling the relatives/family members of unattended/unknown patients Destitute patients are relocated to some destitute home after discharge from hospital.
Short Admissionsrequiring stay for less than 24 hours are done for minor illness/some investigations/Interventions. At present the admission charges for this are Rs. 60/-
Day care facilityis available for certain types of operations. e.g. laproscopic surgery; day care chemotherapy; blood transfusion, dialysis, endoscopies and similar interventions.
Operation Theratres
The institute has fully equipped modern Operation Theatres, where all kinds of major and minor surgeries are performed using the latest techniques and technology.
For routine surgeries, the respective departments maintain waiting list. Patients are called and operated upon as per the waiting list. But, in case of emergencies/urgencies, the out of turn surgeries are also performed, at the discretion at the treating doctors.
The patient should get his Pre-Anaesthetic check up done in PAC Room on 5th floor OPD Block during afternoon before getting admitted for operation and follow the instructions given by the treating Doctors.
ICUsThe hospital has fully equipped Main ICU at 8th Floor, AB wing to provide expert ICU care. There are ICUs/HDUs in few wards of main hospital and CTVS ICU & NS ICU in CN Centre. Patients requiring urgent ICU care are admitted to ICUs at the discretion of treating Doctors.
Laboratory Services
Emergency Lab - 24 hours, throughout the year, for all emergency investigations.
Routine Lab - Sample Collection Timings:- Weeks Days - 8:30 a.m. to 10:30 a.m.
Saturday - 8:30 a.m. to 10:00 a.m.
All type of routine and special investigations incl. Biochemical, microbiological, pathology, immunology and genetic studies are done at AIIMS.
Blood Bank:-AIIMS has a licensed modern, state of the art Blood Bank that functions 24 hours a day and provides facilities for blood donation, storage, issue of blood and its components. Strict precautions are taken and testing is done to prevent any borne infection. If your patient requires blood transfusions, then you are requested to arrange healthy blood donors for donating blood in order to reduce shortage of blood.
Miscellaneous Facilities
Ambulance facility is available to transfer patients to other hospitals or meet any exigency/disaster situation.
If required, patients' attendants may stay in Raj Gharia Dharamshala / Sureka Vishram Sadanafter paying the prevailing charges situated near the East Campus of AIIMS.
Free battery operated vans(Parikrama Sewa)are available for transporting patients and attendants with in the campus.
OPD services are situated in Raj Kumari Amrit Kaur (RAK) OPD Block and adjoining extended OPD building for Medicine and Pediatrics OPD.
| Registration Time | Consultation Time | |
|---|---|---|
| General OPD | 8:30 a.m. to 10:30 a.m. | 8.30 a.m. to 1:00 p.m. |
| Speciality Clinics | 1:00 p.m. to 2:00 p.m. | 1:00 p.m. to 6:00 p.m. |
OPD Card costing Rs. 10/- can be purchased from main counter, OPD ground floor. After this, you should get yourself registered at the counter of respective OPDs.
You have right to consult any doctor/ consultant. For seeking appointment with any consultant on his OPD days, you may contact his/her office.
Patients are seen on first come first serve basis. However, out of turn consultation may be provided in case of emergency or to senior citizens.
For consultation in Speciality and Super-speciality clinics, you need to have referred from general OPD of AIIMS or any Government Institution.
Speciality Clinics - (for details see OPD brochure available at enquiry counter in OPD)
Super Speciality Services:- following Centres provide these services-
Cardio Thoracic and Neuro Sciences Centre.
Dr. Rajendra Prasad Centre for Ophthalmic Sciences.
Dr. B.R. Ambedkar Institute Rotary Cancer Hospital.
National Drugs Dependency Treatment Centre, Ghaziabad.
Investigations: After OPD consultation, the treating doctor will fill up the requisition forms for various investigations & direct/guide you to the concerned lab /dept.
Sample collection centre for Blood, Urine, Stool etc. - Room No. 27, RAK OPD Ground Floor and Room No. 14A in Extended OPD Block.
Sample Collection Timings are:- 8:00 a.m. to 10:00 a.m.
Certain specialized investigations are done on particular days only.
The report normally reaches the concerned OPD on the next OPD day.
Certain investigations are done free of charge while others are charged as per the prevailing norms fixed by Government. Patients should Deposit the money only at the designated hospital Cash Counters and obtain the proper receipt.
Due to excess work load, waiting period exists for certain investigations like MRI, CT, USG etc. Patients are given future dates by the concerned departments. However, these may be done out of turn in urgent situations, on recommendation of the treating doctor.
Many facilities are provided at OPD level e.g. ECG, Plaster, Injection and Immunization Room, Contraception and MTP Services, Minor Surgical Intervention, Physiotherapy, Bronchoscopy, Endoscopy etc.
Medical fitness / Medical examination and other such certificates are issued after paying the requisite fees. For this purpose contact the central registration office, ground floor OPD.
The decision to admit a patient rests with the treating doctor. The patient will be admitted only if a vacant bed is available. But, in case of emergency, out of turn admission may be done.
Wheel chairs, patient trolleys etc. are available free of charge at the entrance of OPD.
OPDs have waiting hall with chairs, STD booth, TVs, lifts, ramp for Ortho OPD, public utilities like drinking water & toilets etc. at each floor.
You should park your vehicle in the paid parking only otherwise it is likely to be towed away.
To meet day-to-day needs of patients, there is canteen and grocery shop in front of the private ward block; medical stores, book shops, general store and STD booths in the subway nearby.
The AIIMS offers various Trainings at different levels
All India Institute of Medical Sciences (AIIMS) was established by the Act of Parliament in 1956 as anautonomous institute to set patterns in Undergraduate and Postgraduate Medical Education in all its branches to demonstrate a high standard of medical education. This is the only institute outside the jurisdiction of Medical Council of India to encourage experiments in the curriculum. New AIIMS are also created on the pattern of AIIMS. New Delhi. It mainly follows a disciplinary structure. However, since inception, AIIMS has been constantly upgrading its course content in tunewith the changing needs.
Courses at AIIMS New Delhi at a glance
| -- | -- | -- | Download |
|---|---|---|---|
| MBBS | B.Sc. Nursing (Hons.) | B.Sc. Nursing Post Basic | Undergraduate |
| B.Sc. (Hons) in Medical Technology in Radiography | Bachelor of Optometry | B.Sc. (OTT) | |
| B.Sc. (Dental Room Asstt.) | B.Sc. (Dental Hygiene) | ||
| M.Biotech | M.Sc. Courses | M.Sc. Nursing | Postgraduate (M.Sc Nursing/Biotech) |
| MD/MS/MDS | DM (6 yrs.) | M.Ch (6 yrs.)
| Postgraduate |
| MD Hospital Administration | |||
| DM | M.Ch | Superspecialty | |
| Fellowship | Ph.D | Doctoral | |
| RESIDENCY | Junior Resident | Senior Resident | Senior Demonstrator |
OPD services are situated in Raj Kumari Amrit Kaur (RAK) OPD Block and adjoining extended OPD building for Medicine and Pediatrics OPD.
| Registration Time | Consultation Time | |
|---|---|---|
| General OPD | 8:30 a.m. to 10:30 a.m. | 8.30 a.m. to 1:00 p.m. |
| Speciality Clinics | 1:00 p.m. to 2:00 p.m. | 1:00 p.m. to 6:00 p.m. |
OPD Card costing Rs. 10/- can be purchased from main counter, OPD ground floor. After this, you should get yourself registered at the counter of respective OPDs.
You have right to consult any doctor/ consultant. For seeking appointment with any consultant on his OPD days, you may contact his/her office.
Patients are seen on first come first serve basis. However, out of turn consultation may be provided in case of emergency or to senior citizens.
For consultation in Speciality and Super-speciality clinics, you need to have referred from general OPD of AIIMS or any Government Institution.
Speciality Clinics - (for details see OPD brochure available at enquiry counter in OPD)
Super Speciality Services:- following Centres provide these services-
Cardio Thoracic and Neuro Sciences Centre.
Dr. Rajendra Prasad Centre for Ophthalmic Sciences.
Dr. B.R. Ambedkar Institute Rotary Cancer Hospital.
National Drugs Dependency Treatment Centre, Ghaziabad.
Investigations: After OPD consultation, the treating doctor will fill up the requisition forms for various investigations & direct/guide you to the concerned lab /dept.
Sample collection centre for Blood, Urine, Stool etc. - Room No. 27, RAK OPD Ground Floor and Room No. 14A in Extended OPD Block.
Sample Collection Timings are:- 8:00 a.m. to 10:00 a.m.
Certain specialized investigations are done on particular days only.
The report normally reaches the concerned OPD on the next OPD day.
Certain investigations are done free of charge while others are charged as per the prevailing norms fixed by Government. Patients should Deposit the money only at the designated hospital Cash Counters and obtain the proper receipt.
Due to excess work load, waiting period exists for certain investigations like MRI, CT, USG etc. Patients are given future dates by the concerned departments. However, these may be done out of turn in urgent situations, on recommendation of the treating doctor.
Many facilities are provided at OPD level e.g. ECG, Plaster, Injection and Immunization Room, Contraception and MTP Services, Minor Surgical Intervention, Physiotherapy, Bronchoscopy, Endoscopy etc.
Medical fitness / Medical examination and other such certificates are issued after paying the requisite fees. For this purpose contact the central registration office, ground floor OPD.
The decision to admit a patient rests with the treating doctor. The patient will be admitted only if a vacant bed is available. But, in case of emergency, out of turn admission may be done.
Wheel chairs, patient trolleys etc. are available free of charge at the entrance of OPD.
OPDs have waiting hall with chairs, STD booth, TVs, lifts, ramp for Ortho OPD, public utilities like drinking water & toilets etc. at each floor.
You should park your vehicle in the paid parking only otherwise it is likely to be towed away.
To meet day-to-day needs of patients, there is canteen and grocery shop in front of the private ward block; medical stores, book shops, general store and STD booths in the subway nearby.
Phone Number of Emergency :- 26594405, 26594706 ( round the clock)
Phone Number of Neurosurgery Resident on Call for all emergencies/Casualty : 8929936770
Location :- Ground floor, AB wing, easily accessible from AIIMS entrance on Aurobindo Marg.
These services are available 24 hour a day, throughout the year.
Anyone with urgent medical problem can seek consultation/treatment in the Emergency.
If Doctors decide that you need urgent medical intervention, you will be registered at the Emergency registration counter, free of charge and proper medical care will be provided promptly.
Emergency has dedicated team of Senior Residents from major specialties (i.e.Emergency Medicine, Surgery & Pediatrics) and Junior Residents, Nurses, Paramedics and Hospital Attendants etc. to provide urgent medical services.
We endeavor to provide medical care (incl. Investigation & treatment) at the earliest possible time.
However, in view of extreme workload in Emergency (more than 450 patients seek consultation per day) those cases that are not so urgent may have to wait for some time.
The treating doctors will call any specialist/super-specialist, who is available on call for urgent consultation as and when required.
In serious cases treatment/management gets priority over paper work like Registration/Medico- Legal requirements.
Emergency has fully equipped Operation Theatre for any urgent surgery etc.
The Emergency is fully equipped with all modern gadgets like monitors, ventilators, nebulisers, defibrillators, central O2 and suction supply etc.
All urgent investigations like Hemogram, Blood Biochemistry, Urine toxicology, Cardiac Biomarker, Blood Gas Analysis, ECG, USG, X-ray, C.T. Scan, etc. are available for casualty patients round the clock.
All medicines and surgical items available in Emergency are provided free of cost.
For any guidance/ assistance including financial help for poor and indigent patients, Social Guides and M.S.S.O are available at the entrance of Emergency should be approached.
Facilities like patient trolleys are available ate the entrance of Emergency.
Public utilities like toilets, waiting area with Tea/Coffee/Snacks, fans, chairs etc. are available.
Phone Number of Emergency :- 26594405, 26594706 ( round the clock)
Phone Number of Neurosurgery Resident on Call for all emergencies/Casualty : 8929936770
Location :- Ground floor, AB wing, easily accessible from AIIMS entrance on Aurobindo Marg.
These services are available 24 hour a day, throughout the year.
Anyone with urgent medical problem can seek consultation/treatment in the Emergency.
If Doctors decide that you need urgent medical intervention, you will be registered at the Emergency registration counter, free of charge and proper medical care will be provided promptly.
Emergency has dedicated team of Senior Residents from major specialties (i.e.Emergency Medicine, Surgery & Pediatrics) and Junior Residents, Nurses, Paramedics and Hospital Attendants etc. to provide urgent medical services.
We endeavor to provide medical care (incl. Investigation & treatment) at the earliest possible time.
However, in view of extreme workload in Emergency (more than 450 patients seek consultation per day) those cases that are not so urgent may have to wait for some time.
The treating doctors will call any specialist/super-specialist, who is available on call for urgent consultation as and when required.
In serious cases treatment/management gets priority over paper work like Registration/Medico- Legal requirements.
Emergency has fully equipped Operation Theatre for any urgent surgery etc.
The Emergency is fully equipped with all modern gadgets like monitors, ventilators, nebulisers, defibrillators, central O2 and suction supply etc.
All urgent investigations like Hemogram, Blood Biochemistry, Urine toxicology, Cardiac Biomarker, Blood Gas Analysis, ECG, USG, X-ray, C.T. Scan, etc. are available for casualty patients round the clock.
All medicines and surgical items available in Emergency are provided free of cost.
For any guidance/ assistance including financial help for poor and indigent patients, Social Guides and M.S.S.O are available at the entrance of Emergency should be approached.
Facilities like patient trolleys are available ate the entrance of Emergency.
Public utilities like toilets, waiting area with Tea/Coffee/Snacks, fans, chairs etc. are available.
Dr. Rajendra Prasad Centre for Ophthalmic Sciences, named after the first President of India, Dr. Rajendra Prasad, was established on the 10th of March, 1967 as a National centre for ophthalmic science, to provide state of the art patient care, expand human resources for medical education and undertake research to find solutions to eye health problems of national importance.
Prof L P Agarwal was the visionary, who envisaged an eye center that would be at the fore front of eye health planning, academics and clinical care. It was designed keeping in mind the specific needs of India, and included the best features of leading ophthalmic centers around the world.
Prof L PAgarwal and the RPC were instrumental in making India the first country to start a National Programme for Prevention of visual impairment and Control of Blindness. The Centre formed the apex of the pyramid of Ophthalmic services in India, under this programme.
RPC has been recognized over the years, as a center of excellence by policy makers, professionals and the discerning public. All its expertise is available to the common man at highly subsidized rates or free.
The Centre is a constituent unit of the All India Institute of Medical Sciences, wherein it retains the fullest autonomy, while still keeping it within the mainstream of medical education and health care.
Dr.R.P. Centre continues to play a pivotal role in the National Programme for Control of Blindness. Faculty members of the Centre provide technical inputs at various forums that deliberate on policy planning and programme implementation. We have contributed our share in various blindness surveys and rapid assessments that have been conducted under the National Programme. As part of the Working Group, we have assisted in the framing of the Plan of Action under the Vision 2020 initiative. The Plan of Action shall guide the National Programme for Control of Blindness in the years to come. The Centre continues to foster partnerships with nongovernmental organizations engaged in the field of eye care. The centre has developed software for the National Registry of Eye Care infrastructure and human resources in India” this was done to support vision 2020 activities in India. This will be of immense use for policy planning in future.
| Name | Period |
|---|---|
| Prof. L.P. Agarwal (Founder) | 1967-79 |
| Prof. Madan Mohan | 1979-89 |
| Prof. P.K. Khosla | 1989-93 |
| Prof. Prem Prakash | 1993-96 |
| Prof. V.K. Dada | 1996-2001 |
| Prof. H.K. Tewari | 2001-04 |
| Prof. S. Ghose | 2004 - 5.10.2011 |
| Prof. R.V. Azad | Oct 2011-March 2014 |
| Prof. Y.R. Sharma | March 2014 -December 2015 |
| Prof. Atul Kumar | January 2016 to Aug 2021 |
| Prof. J.S. Titiyal | Sep 2021 to Date |
Prof Jeewan Singh Titiyal
Dr. D.K.Sharma
Ms.Nirmala Jacinta Kujur
Shri Shivanand Thakur
Mrs. Archana Sharma
Patents presenting with Fever (body temperature of 38o Celsius or high) with one of the following symptoms:
Muscle ache, cough, abnormal breathing (unusual breathing difficulty) or suspected pneumonia by the physician, or influenza
in addition to
History of direct contact with infected / dead birds in past 7 days or
Occurrence of unusual death of birds in the community within the past 14 days; or
Contact with a pneumonia patient or another patient suspected of avian influenza
Case definition of probable case:symptoms of suspected case and Preliminary test shows infection of influenza group A, but cannot yet be confirmed whether it is from human or birds or
Respiratory failure or
Death
Case definition of Confirmed cases: A suspected or probable case with at least one of the following:
Obtain NP swabs from all the patients (see annexure 1)
Assess severity of illness: Look for presence of following:
Respiratory distress as indicated by: increased respiratory rates, chest indrawing, dehydration, hypotension, altered sensorium or oxygen saturation of less than 93% in room air. If any of these are present patient should be admitted to ward in designated area and manage on following principles
If patient is stable: (absence of above clinical features): take NP aspirate from all the patients and isolate them in the designated area identified for them and Start on Oseltamivir
Obtain lab results and see clinical course. If lab tests negative: discontinue Oseltamivir and provide supportive care, shift them to regular wards if hospitalization indicated otherwise send them home
If lab test is positive: Transfer to designated in patient area and continue supportive care and oseltamivir
Adult patients: Infection control precautions for 7 days after resolution of fever
Children: Infection control measures for 21 days after onset of illness.
If discharged earlier: child should not attend school and parents should be educated to observe infection control measures at home.
Chemoprophylaxis:
For close contacts: Oseltamivir 75 mg daily for 7 days
Persons at risk: Oseltamivir 75 mg daily for the entire epidemic
Annexure 1
Collection and transport of samples
Samples from upper respiratory tract include
From lower respiratory tract samples >include :
Specimens for the laboratory diagnosis of avian influenza A should be collected in the following order of priority:
The sample collection should be done with all the necessary biosafety precautions including use of gowns, gloves and masks
The samples should be kept on ice and transported to virology laboratory as soon as possible
Antiviral drugs and their doses
Oseltamivir: is the only drug effective against H5N1 virus Doses are:
Children weighing
< 15 Kg: 30 mg twice a day
15-23 Kgs: 45 mg twice a day
23-40 kgs: 60 mg twice a day
> 40 kg: 75 mg twice a day
Nausea and vomiting: transient and occur in the beginning and are self limiting
Abdominal pain, epistaxis, conjuctivitis
Should be used in pregnancy with caution
Contraindications:Hypersensitivity to drug
(Patents presenting with Fever (body temperature of 38o Celsius or high) with one of the following symptoms: Muscle ache, cough, abnormal breathing (unusual breathing difficulty) or suspected pneumonia by the physician, or influenza in addition to History of direct contact with infected / dead birds in past 7 days >or Occurrence of unusual death of birds in the community within the past 14 days; or Contact with a pneumonia patient or another patient suspected of avian influenza)
![]()
![]()
(Look for presence of following Respiratory distress as indicated by: increased respiratory rates, chest indrawing, dehydration, hypotension, altered sensorium or oxygen saturation of less than 93% in room air)
Any one of the above present
![]()
Admit in designated area and treat as follows
Isolate cases
Monitor vital signs every 1-2 hours
Maintain air way breathing and circulation (ABC)
Maintain hydration, electrolyte balance, and nutrition
Provide oxygen and assisted ventilation when indicated
Manage fever with paracetamol
Give antiviral Oseltamivir (For doses see annexure 2)
Broad spectrum antibiotics for treatment of secondary pulmonary infection
Avoid giving nebulized medications: chances of spread
None of the above present
![]()
Keep the patient in designated out patient area, start oseltamivir and collect lab report reportresults

![]()
Send home with supportive care
![]()
Transfer to general ward and manage according to
What is Avian Influenza?
Avian influenza, or “bird flu” or “avian flu” is an infection caused by avian (bird) influenza (flu) viruses. These flu viruses occur naturally among birds. Wild birds worldwide carry the viruses in their intestines, but usually do not get sick from them. However, bird flu is very contagious among birds and can make some domesticated birds, including chickens and ducks, very sick and kill them.
Do avian flu viruses infect humans?
Bird flu viruses do not usually infect humans, but several cases of human infection with bird flu viruses have occurred since 1997.
How does avian flu spread in birds?
Infected birds shed flu virus in their saliva, nasal secretions, and feces (droppings). Susceptible birds become infected when they have contact with contaminated excretions or surfaces that are contaminated with excretions.
How does avian flu spread in humans?
It is believed that most cases of bird flu infection in humans have resulted from contact with infected poultry or contaminated surfaces. There is no evidence of human-to-human transmission so far.
What is a pandemic?
A pandemic is an epidemic that usually affects a large proportion of the population, occurring over a wide geographic area such as a section of a nation, the entire nation, a continent or the world.
should be done if migratory birds are sighted near one’s house?
Migratory birds may or may not carry the avian flu virus. It depends on whether these birds have flown from a region where avian flu is prevalent. This can be determined only by an expert. Therefore in case a migratory bird is sighted, it should not be killed. However, as a precaution, one should stay away from these birds and their droppings. The municipal authorities should be informed immediately.
What should be done if one sight’s a dead bird?
If the cause of death of the bird is not certain, the municipal authorities should be informed immediately. They may send the bird for testing to find out whether or not it was infected with the avian influenza virus.In case of unusual death of poultry, the civic authorities must be informed immediately.
Can avian flu be contracted by visiting a shop that is next to a shop that sells chicken?
In the event of a pandemic of avian flu, it is possible
Is it safe to eat poultry and poultry products?
Poultry and poultry products can be prepared and consumed as usual, with no fear of acquiring infection with the avian flu virus.One should continue to follow good hygienic and cooking practices.The virus is destroyed at a temperature of 70o C for 30 minutes. After handling poultry and eggs, one should wash hands and other exposed parts with soap and water.
Are the chicken droppings on eggs infective?
As it is likely that the eggs that reach the consumer were laid several hours ago, the likelihood of infection is low, even if the droppings were carrying the avian flu virus. The avian flu virus is destroyed by drying, and exposure to sunlight for a few hours.
However, in the event of a pandemic, recent droppings are to be considered infective unless proven otherwise.
Is it safe to use chicken-droppings as manure?
During a pandemic, do not come in contact with fresh droppings. Use some other manure until such time the pandemic has cleared
How can avian flu be controlled in poultry?
At present, culling is the only way to contain avian flu in poultry.
Can domestic normal-appearing ducks spread avian flu?
Yes they can. In fact, waterfowls are known to be reservoirs of infection. The avian flu virus does not harm these waterfowls. However the waterfowls can spread the avian flu virus to humans. These waterfowls are therefore “carriers” of avian flu.
Can a person suffering from influenza suffer from avian flu at the same time?
Yes, it is possible. Neither suffering from influenza, nor vaccination against human influenza offers protection against avian flu. However, health care providers and others who are at high risk of infection should get themselves vaccinated against human influenza virus so that they are at least protected against one of them.
What are the symptoms and signs of avian flu in humans?
Cough, fever, sore throat, muscle aches, pneumonia and other complications
What is the test for avian flu?
A throat swab is taken from the patient to test for avian flu.
Which are the places where such testing is done?
The testing facilities are currently available at All India Institute of Medical Sciences, New Delhi, and National Institute of Virology, Pune.
Is there a vaccine for humans against avian flu?
There is no vaccine for humans against avian flu. The vaccine against human influenza virus does not protect against avian flu.
Are any medicines available to prevent bird flu in humans?
There is no recommendation for the routine use of medicines for the prevention of bird flu in humans.
Patents presenting with Fever (body temperature of 38o Celsius or high) with one of the following symptoms:
Muscle ache, cough, abnormal breathing (unusual breathing difficulty) or suspected pneumonia by the physician, or influenza
in addition to
History of direct contact with infected / dead birds in past 7 days or
Occurrence of unusual death of birds in the community within the past 14 days; or
Contact with a pneumonia patient or another patient suspected of avian influenza
Case definition of probable case:symptoms of suspected case and Preliminary test shows infection of influenza group A, but cannot yet be confirmed whether it is from human or birds or
Respiratory failure or
Death
Case definition of Confirmed cases: A suspected or probable case with at least one of the following:
Obtain NP swabs from all the patients (see annexure 1)
Assess severity of illness: Look for presence of following:
Respiratory distress as indicated by: increased respiratory rates, chest indrawing, dehydration, hypotension, altered sensorium or oxygen saturation of less than 93% in room air. If any of these are present patient should be admitted to ward in designated area and manage on following principles
If patient is stable: (absence of above clinical features): take NP aspirate from all the patients and isolate them in the designated area identified for them and Start on Oseltamivir
Obtain lab results and see clinical course. If lab tests negative: discontinue Oseltamivir and provide supportive care, shift them to regular wards if hospitalization indicated otherwise send them home
If lab test is positive: Transfer to designated in patient area and continue supportive care and oseltamivir
Adult patients: Infection control precautions for 7 days after resolution of fever
Children: Infection control measures for 21 days after onset of illness.
If discharged earlier: child should not attend school and parents should be educated to observe infection control measures at home.
Chemoprophylaxis:
For close contacts: Oseltamivir 75 mg daily for 7 days
Persons at risk: Oseltamivir 75 mg daily for the entire epidemic
Annexure 1
Collection and transport of samples
Samples from upper respiratory tract include
From lower respiratory tract samples >include :
Specimens for the laboratory diagnosis of avian influenza A should be collected in the following order of priority:
The sample collection should be done with all the necessary biosafety precautions including use of gowns, gloves and masks
The samples should be kept on ice and transported to virology laboratory as soon as possible
Antiviral drugs and their doses
Oseltamivir: is the only drug effective against H5N1 virus Doses are:
Children weighing
< 15 Kg: 30 mg twice a day
15-23 Kgs: 45 mg twice a day
23-40 kgs: 60 mg twice a day
> 40 kg: 75 mg twice a day
Nausea and vomiting: transient and occur in the beginning and are self limiting
Abdominal pain, epistaxis, conjuctivitis
Should be used in pregnancy with caution
Contraindications:Hypersensitivity to drug
(Patents presenting with Fever (body temperature of 38o Celsius or high) with one of the following symptoms: Muscle ache, cough, abnormal breathing (unusual breathing difficulty) or suspected pneumonia by the physician, or influenza in addition to History of direct contact with infected / dead birds in past 7 days >or Occurrence of unusual death of birds in the community within the past 14 days; or Contact with a pneumonia patient or another patient suspected of avian influenza)
![]()
![]()
(Look for presence of following Respiratory distress as indicated by: increased respiratory rates, chest indrawing, dehydration, hypotension, altered sensorium or oxygen saturation of less than 93% in room air)
Any one of the above present
![]()
Admit in designated area and treat as follows
Isolate cases
Monitor vital signs every 1-2 hours
Maintain air way breathing and circulation (ABC)
Maintain hydration, electrolyte balance, and nutrition
Provide oxygen and assisted ventilation when indicated
Manage fever with paracetamol
Give antiviral Oseltamivir (For doses see annexure 2)
Broad spectrum antibiotics for treatment of secondary pulmonary infection
Avoid giving nebulized medications: chances of spread
None of the above present
![]()
Keep the patient in designated out patient area, start oseltamivir and collect lab report reportresults
![]()
Send home with supportive care
![]()
Transfer to general ward and manage according to
What is Avian Influenza?
Avian influenza, or “bird flu” or “avian flu” is an infection caused by avian (bird) influenza (flu) viruses. These flu viruses occur naturally among birds. Wild birds worldwide carry the viruses in their intestines, but usually do not get sick from them. However, bird flu is very contagious among birds and can make some domesticated birds, including chickens and ducks, very sick and kill them.
Do avian flu viruses infect humans?
Bird flu viruses do not usually infect humans, but several cases of human infection with bird flu viruses have occurred since 1997.
How does avian flu spread in birds?
Infected birds shed flu virus in their saliva, nasal secretions, and feces (droppings). Susceptible birds become infected when they have contact with contaminated excretions or surfaces that are contaminated with excretions.
How does avian flu spread in humans?
It is believed that most cases of bird flu infection in humans have resulted from contact with infected poultry or contaminated surfaces. There is no evidence of human-to-human transmission so far.
What is a pandemic?
A pandemic is an epidemic that usually affects a large proportion of the population, occurring over a wide geographic area such as a section of a nation, the entire nation, a continent or the world.
should be done if migratory birds are sighted near one’s house?
Migratory birds may or may not carry the avian flu virus. It depends on whether these birds have flown from a region where avian flu is prevalent. This can be determined only by an expert. Therefore in case a migratory bird is sighted, it should not be killed. However, as a precaution, one should stay away from these birds and their droppings. The municipal authorities should be informed immediately.
What should be done if one sight’s a dead bird?
If the cause of death of the bird is not certain, the municipal authorities should be informed immediately. They may send the bird for testing to find out whether or not it was infected with the avian influenza virus.In case of unusual death of poultry, the civic authorities must be informed immediately.
Can avian flu be contracted by visiting a shop that is next to a shop that sells chicken?
In the event of a pandemic of avian flu, it is possible
Is it safe to eat poultry and poultry products?
Poultry and poultry products can be prepared and consumed as usual, with no fear of acquiring infection with the avian flu virus.One should continue to follow good hygienic and cooking practices.The virus is destroyed at a temperature of 70o C for 30 minutes. After handling poultry and eggs, one should wash hands and other exposed parts with soap and water.
Are the chicken droppings on eggs infective?
As it is likely that the eggs that reach the consumer were laid several hours ago, the likelihood of infection is low, even if the droppings were carrying the avian flu virus. The avian flu virus is destroyed by drying, and exposure to sunlight for a few hours.
However, in the event of a pandemic, recent droppings are to be considered infective unless proven otherwise.
Is it safe to use chicken-droppings as manure?
During a pandemic, do not come in contact with fresh droppings. Use some other manure until such time the pandemic has cleared
How can avian flu be controlled in poultry?
At present, culling is the only way to contain avian flu in poultry.
Can domestic normal-appearing ducks spread avian flu?
Yes they can. In fact, waterfowls are known to be reservoirs of infection. The avian flu virus does not harm these waterfowls. However the waterfowls can spread the avian flu virus to humans. These waterfowls are therefore “carriers” of avian flu.
Can a person suffering from influenza suffer from avian flu at the same time?
Yes, it is possible. Neither suffering from influenza, nor vaccination against human influenza offers protection against avian flu. However, health care providers and others who are at high risk of infection should get themselves vaccinated against human influenza virus so that they are at least protected against one of them.
What are the symptoms and signs of avian flu in humans?
Cough, fever, sore throat, muscle aches, pneumonia and other complications
What is the test for avian flu?
A throat swab is taken from the patient to test for avian flu.
Which are the places where such testing is done?
The testing facilities are currently available at All India Institute of Medical Sciences, New Delhi, and National Institute of Virology, Pune.
Is there a vaccine for humans against avian flu?
There is no vaccine for humans against avian flu. The vaccine against human influenza virus does not protect against avian flu.
Are any medicines available to prevent bird flu in humans?
There is no recommendation for the routine use of medicines for the prevention of bird flu in humans.
This web page is for the patients undergoing Coronary Artery Bypass Grafting (CABG). This web page attempts to explain the cause of the disease, the risk factors, the effects of disease and possible treatment options. It tells about the surgery, preoperative preparation and postoperative care in hospital and at home. Lastly, an effort has been made to spread preventive awareness about the coronary artery disease. For better understanding, at the cost of technical perfection, language has been made as simple as possible.
This web page is for the patients undergoing Coronary Artery Bypass Grafting (CABG). This web page attempts to explain the cause of the disease, the risk factors, the effects of disease and possible treatment options. It tells about the surgery, preoperative preparation and postoperative care in hospital and at home. Lastly, an effort has been made to spread preventive awareness about the coronary artery disease. For better understanding, at the cost of technical perfection, language has been made as simple as possible.
This web page is for the patient who has a heart valve problem and who seeks treatment for the same. The web page describes in various chapters some of the fundamentals of blood circulation through the heart and the function of the valves and the effects of the disease. The web page also tells about the symptoms, tests that are used for diagnosis and after care. It tells about the surgery and postoperative care while the patient is in hospital. Finally it explains the aftercare when the patient is at home. For the purpose of better understanding, language has been made as simple as possible and efforts have been made to explain the facts in common language.
This web page is for the patient who has a heart valve problem and who seeks treatment for the same. The web page describes in various chapters some of the fundamentals of blood circulation through the heart and the function of the valves and the effects of the disease. The web page also tells about the symptoms, tests that are used for diagnosis and after care. It tells about the surgery and postoperative care while the patient is in hospital. Finally it explains the aftercare when the patient is at home. For the purpose of better understanding, language has been made as simple as possible and efforts have been made to explain the facts in common language.
* Organized two training programmes on HIV/AIDS prevention for the Delhi University College students in December1998 and January 1999'.
* Organized an AIDS awareness programme and Blood Donation Camp at BITS, Pilani (Rajasthan) in March - April 1999.
* IEC material in the form of books and booklets is being produced
* `Shubchintak' AIDS helpline - drawing a very good response from public.
* Traning Programmes on HIV/AIDS prevention will be held in the coming months for the
- Workers of NGOs
- Workers of NGOs
- Teachers
- Secondary School Students * Educational Materoa; os being planned on STDs, use of condoms etc.
When you need help...
The Experience of the AIDS Helpline of AIIMS New Delhi
The AIIMS experiene In November 1998, the All India Institute of Medical Sciences (AIIMS), New Delhi established an AIDS Education & Training Cell to create awareness about HIV/AIDS in the General Public. On of the schemes Iaunched to achieve this foal was a free telephone help line called `Shubhchintak' (`well-wisher' in Hindi). This hep line launched on December 1998 has answered the queries of many callers. `Shubhchintak' works from 10:00am to 5:00pm on all working days from Monday to Friday and on Saturdays from 10:00am to 1:00pm. All calls are handled by person with counselling skills. The hame, age, gender, address, phone number or any other identification of the caller is not asked for so that the caller remains totally anonymous and can ask any type of question without fear or anxiety. The significant difference between this help line and others is that it is interactive and caters to the specific personal problems of the callers.On an average `Shubhchintak' recives about 32 calls per day. However, whenever a writ-up appears in the press or an announcement is made on All India Radio, the number of calls go up on that day and a few days thereafter. It is found that 87.9% of the callers are males while 12.1% are females. Though we cannot comment on the age of the callers, they seemed to by young persons (approximately 15-30 years age group). Some of the questions asked by the calllers:
Writhe is AIDS? What causes AIDS?
Difference between HIV & AIDS?
Modes of transmission
Windows period
Methods to prevent AIDS?
There were also questions regarding the blood test for HIV (such as when and where it could be done, cost of the test, time taken for reporting and reliability of FLISAtest;) some of the callers were curious to know whether `oral sec' causes AIDS. Many callers asked about the risk of getting HIV/AIDS quoting personal experiences and problems. The AIIMS experience points out that given an opportunity the grneral punblic, especially young people, want to know about HIV/AIDS and opportunityes nedd to be created to address these queries in a scientific and cost effective manner. In this situation interactive help line have an Important role to play. (Dr Bir Singh, Additional Professor & Dr V.P. Reddaiah, Professor & Head, Centre for Community Midicine, AIIMS, New Delhi)
(Health Dialogue Issue No. 16. June 1999).
* Organized two training programmes on HIV/AIDS prevention for the Delhi University College students in December1998 and January 1999'.
* Organized an AIDS awareness programme and Blood Donation Camp at BITS, Pilani (Rajasthan) in March - April 1999.
* IEC material in the form of books and booklets is being produced
* `Shubchintak' AIDS helpline - drawing a very good response from public.
* Traning Programmes on HIV/AIDS prevention will be held in the coming months for the
- Workers of NGOs
- Workers of NGOs
- Teachers
- Secondary School Students * Educational Materoa; os being planned on STDs, use of condoms etc.
When you need help...
The Experience of the AIDS Helpline of AIIMS New Delhi
The AIIMS experiene In November 1998, the All India Institute of Medical Sciences (AIIMS), New Delhi established an AIDS Education & Training Cell to create awareness about HIV/AIDS in the General Public. On of the schemes Iaunched to achieve this foal was a free telephone help line called `Shubhchintak' (`well-wisher' in Hindi). This hep line launched on December 1998 has answered the queries of many callers. `Shubhchintak' works from 10:00am to 5:00pm on all working days from Monday to Friday and on Saturdays from 10:00am to 1:00pm. All calls are handled by person with counselling skills. The hame, age, gender, address, phone number or any other identification of the caller is not asked for so that the caller remains totally anonymous and can ask any type of question without fear or anxiety. The significant difference between this help line and others is that it is interactive and caters to the specific personal problems of the callers.On an average `Shubhchintak' recives about 32 calls per day. However, whenever a writ-up appears in the press or an announcement is made on All India Radio, the number of calls go up on that day and a few days thereafter. It is found that 87.9% of the callers are males while 12.1% are females. Though we cannot comment on the age of the callers, they seemed to by young persons (approximately 15-30 years age group). Some of the questions asked by the calllers:
Writhe is AIDS? What causes AIDS?
Difference between HIV & AIDS?
Modes of transmission
Windows period
Methods to prevent AIDS?
There were also questions regarding the blood test for HIV (such as when and where it could be done, cost of the test, time taken for reporting and reliability of FLISAtest;) some of the callers were curious to know whether `oral sec' causes AIDS. Many callers asked about the risk of getting HIV/AIDS quoting personal experiences and problems. The AIIMS experience points out that given an opportunity the grneral punblic, especially young people, want to know about HIV/AIDS and opportunityes nedd to be created to address these queries in a scientific and cost effective manner. In this situation interactive help line have an Important role to play. (Dr Bir Singh, Additional Professor & Dr V.P. Reddaiah, Professor & Head, Centre for Community Midicine, AIIMS, New Delhi)
(Health Dialogue Issue No. 16. June 1999).
Book: All You Wanted to Know About AIDS/HIV Language: Bilingual: Hindi and English Autors(s): Dr. Bir Singh & Dr. V.P. Reddaiah Year of Publication: 1999, 2003, 2005, 2008 (Revised 4th Edition) Published by: AIDS Education & Training Cell, AIIMS, New Delhi Can be had from: AIDS Education & Training Cell, New Delhi Available : Free of Cost |  |
Booklet: Know About AIDS / HIV Language: English Author(s): Dr. Bir Singh & V.P. Reddaiah Year of Publication: 1999, 2003, 2005 and 2008 Published by: AIDS Education & Training Cell, AIIMS, New Delhi Can be had from: AIDS Education & Training Cell, AIIMS, New Delhi Available: Free of Cost |  |
Booklet: HIV/AIDS Ke Baare Mein Jaaniye Language : Hindi Author(s): Dr. Bir Singh & Dr. V.P. Reddaiah Year of Publication: 1999, 2003, 2005 and 2008 Published by: AIDS Education & Training Cell, AIIMS, New Delhi Can be had from: AIDS Education & Training Cell, AIIMS, New Delhi Available : Free of Cost |  |
Book: A Handy Guide for Good Sex & Family Life Language: English Author(s): Dr. Bir Singh & Dr. V.P. Reddaiah Year of Publication: 2000, 2008 Published by: AIDS Education & Training Cell, AIIMS, New Delhi Can be had from: AIDS Education & Training Cell, AIIMS, New Delhi Available : Free of Cost |  |
All these books are mainly targetted for the general public ( Youth, Parents, Students, Teachers , NGO Workers and Health Care workers) . These are not text books. These have got limited usefulness for Medical Doctors but are quite useful for Paramedicals and General public.
Bulk copies( Minimum Order : 50 copies) of ALL these books can be had DIRECTLY from the printer at the printing cost of the books. We can help in that process. The payment has to be made DIRECTLY to the printer by a cheque paid in advance. For details about the printer, cost etc., please contact the by E mail: eshubhchintak@gmail.com or at phone number 91-011-265 88 333 between 10 AM to 5 PM on working Mondays to Fridays.
Please send your request to :
Dr Bir Singh, Professor,
Centre for Community Medicine,
AIIMS, New Delhi-110029.
Or email to: eshubhchintak@gmail.com Please write your complete postal address with PIN code in these requests.
Book: All You Wanted to Know About AIDS/HIV Language: Bilingual: Hindi and English Autors(s): Dr. Bir Singh & Dr. V.P. Reddaiah Year of Publication: 1999, 2003, 2005, 2008 (Revised 4th Edition) Published by: AIDS Education & Training Cell, AIIMS, New Delhi Can be had from: AIDS Education & Training Cell, New Delhi Available : Free of Cost | |
Booklet: Know About AIDS / HIV Language: English Author(s): Dr. Bir Singh & V.P. Reddaiah Year of Publication: 1999, 2003, 2005 and 2008 Published by: AIDS Education & Training Cell, AIIMS, New Delhi Can be had from: AIDS Education & Training Cell, AIIMS, New Delhi Available: Free of Cost | |
Booklet: HIV/AIDS Ke Baare Mein Jaaniye Language : Hindi Author(s): Dr. Bir Singh & Dr. V.P. Reddaiah Year of Publication: 1999, 2003, 2005 and 2008 Published by: AIDS Education & Training Cell, AIIMS, New Delhi Can be had from: AIDS Education & Training Cell, AIIMS, New Delhi Available : Free of Cost | |
Book: A Handy Guide for Good Sex & Family Life Language: English Author(s): Dr. Bir Singh & Dr. V.P. Reddaiah Year of Publication: 2000, 2008 Published by: AIDS Education & Training Cell, AIIMS, New Delhi Can be had from: AIDS Education & Training Cell, AIIMS, New Delhi Available : Free of Cost | |
All these books are mainly targetted for the general public ( Youth, Parents, Students, Teachers , NGO Workers and Health Care workers) . These are not text books. These have got limited usefulness for Medical Doctors but are quite useful for Paramedicals and General public.
Bulk copies( Minimum Order : 50 copies) of ALL these books can be had DIRECTLY from the printer at the printing cost of the books. We can help in that process. The payment has to be made DIRECTLY to the printer by a cheque paid in advance. For details about the printer, cost etc., please contact the by E mail: eshubhchintak@gmail.com or at phone number 91-011-265 88 333 between 10 AM to 5 PM on working Mondays to Fridays.
Please send your request to :
Dr Bir Singh, Professor,
Centre for Community Medicine,
AIIMS, New Delhi-110029.
Or email to: eshubhchintak@gmail.com Please write your complete postal address with PIN code in these requests.
"AIDS Education & Training Cell" was established at Center for Community Medicine in November 1998. This cell is in continuation of the erstwhile NGO-AIDS cell which has ceased to exit w.e.f. September-October 1998.
"AIDS Education & Training Cell" works in the areas of HIV/AIDS prevention, education, training and counselling.
Dr. Bir Singh, Additional Professor of Community Medicine is the Co-ordinator of this Cell.
This Cell runs a Telephonic Helpline called "Shubhchintak" (Phone No. 91-11- 265 88 333) which works from 10AM to 5PM on all working days and answers queries of the clients about HIV/AIDS, sexuality issues and problems and family-life education. This service came into force from December 1, i.e. World AIDS Day, 1998.
Apart from the telephonic AIDS helpline “Shubhchintak”, the AETC also launched an internet based helpline AIDS “e-Shubhchintak”.
"AIDS Education & Training Cell" was established at Center for Community Medicine in November 1998. This cell is in continuation of the erstwhile NGO-AIDS cell which has ceased to exit w.e.f. September-October 1998.
"AIDS Education & Training Cell" works in the areas of HIV/AIDS prevention, education, training and counselling.
Dr. Bir Singh, Additional Professor of Community Medicine is the Co-ordinator of this Cell.
This Cell runs a Telephonic Helpline called "Shubhchintak" (Phone No. 91-11- 265 88 333) which works from 10AM to 5PM on all working days and answers queries of the clients about HIV/AIDS, sexuality issues and problems and family-life education. This service came into force from December 1, i.e. World AIDS Day, 1998.
Apart from the telephonic AIDS helpline “Shubhchintak”, the AETC also launched an internet based helpline AIDS “e-Shubhchintak”.
"AIDS Education & Training Cell" was established at Center for Community Medicine in November 1998. This cell is in continuation of the erstwhile NGO-AIDS cell which has ceased to exist w.e.f. September-October 1998.
The "AIDS Education & Training Cell" works in the areas of HIV/AIDS prevention, education, training and counselling. Dr. Bir Singh, Professor of Community Medicine is the Co-ordinator of this Cell.
This Cell runs a Telephonic Helpline called "Shubhchintak"(Phone No. 91-11- 265 88 333) which works from 10AM to 5PM on all working days and answers queries of the clients about HIV/AIDS, sexuality issues and problems and family-life education. This service came into force from December 1, i.e. World AIDS Day, 1998.
Recently we have launched an Internet based helpline called "e-Shubhchintak". This can be accessed by visiting the web site www.aiims.edu
With effect from December 1, (World AIDS Day), 1998 this cell has also started a Helpline called Shubhchintak (Phone No. 91-11-265 88 333) which works from 10.00 AM to 5.00 PM and answers queries of clients about HIV/AIDS, Sexuality issues & problems and family life education. This helpline being individualised and interactive has already become hugely popular and on an average receives 32 calls per day. Recently we have launched an Internet based helpline called "e-Shubhchintak". This can be accessed by visiting the web site www.aiims.edu
Four of the latest publications of the AIDS Education & Training Cell are shown in the AIDS CELL main page:
These booklets are free of cost. Please contact Dr. Bir Singh, Coordinator of AETC at eshubhchintak@gmail.com for your copy.
If you have any query on HIV/AIDS prevention, blood tests for HIV etc., you can also ask the same at this e-mail address :
eshubhchintak@gmail.com
Paper Books
Report of the Activities for the ear 2007-2008
Professor of Community Medicine
AIIMS , New Delhi-110029
Phones: Office - 011-2659 4985
011-265 88 333
011-265 89 815, 265 88 663
E-mail: birsingh43@gmail.com , birsingh43@hotmail.com
Public Health Nurse / Counsellor
Ms. Sosamma Shyam
Secretary
Ms. Manju Sidhu
"AIDS Education & Training Cell" was established at Center for Community Medicine in November 1998. This cell is in continuation of the erstwhile NGO-AIDS cell which has ceased to exist w.e.f. September-October 1998.
The "AIDS Education & Training Cell" works in the areas of HIV/AIDS prevention, education, training and counselling.Dr. Bir Singh (birsingh43@hotmail.com), Professor of Community Medicine is the Co-ordinator of this Cell.
This Cell runs a Telephonic Helpline called "Shubhchintak"(Phone No. 91-11- 265 88 333) which works from 10AM to 5PM on all working days and answers queries of the clients about HIV/AIDS, sexuality issues and problems and family-life education. This service came into force from December 1, i.e. World AIDS Day, 1998.
Recently we have launched an Internet based helpline called "e-Shubhchintak". This can be accessed by visiting the web site www.aiims.edu
With effect from December 1, (World AIDS Day), 1998 this cell has also started a Helpline called Shubhchintak (Phone No. 91-11-265 88 333) which works from 10.00 AM to 5.00 PM and answers queries of clients about HIV/AIDS, Sexuality issues & problems and family life education. This helpline being individualised and interactive has already become hugely popular and on an average receives 32 calls per day. Recently we have launched an Internet based helpline called "e-Shubhchintak". This can be accessed by visiting the web site www.aiims.edu
Four of the latest publications of the AIDS Education & Training Cell are shown in the AIDS CELL main page:
These booklets are free of cost. Please contact Dr. Bir Singh, Coordinator of AETC at eshubhchintak@gmail.com for your copy.
If you have any query on HIV/AIDS prevention, blood tests for HIV etc., you can also ask the same at this e-mail address : eshubhchintak@gmail.com
Paper Books
Report of the Activities for the ear 2007-2008
Professor of Community Medicine
AIIMS , New Delhi-110029
Phones: Office - 011-2659 4985
011-265 88 333
011-265 89 815, 265 88 663
E-mail: birsingh43@gmail.com , birsingh43@hotmail.com
Public Health Nurse / Counsellor
Ms. Sosamma Shyam
Secretary
Ms. Manju Sidhu

Director AIIMS

Union Minister M/o Health and Family Welfare
Minister of State

Minister of State
All India Institute Of Medical Sciences, New Delhi website complies with World Wide Web Consortium (W3C) Web Content Accessibility Guidelines (WCAG) 2.0 level AA. This will enable people with visual impairments access the website using assistive technologies, such as screen readers. The information of the website is accessible with different screen readers.
| Screen Reader | Website | Free / Commercial |
|---|---|---|
| Various Screen Readers to choose from | ||
| Non Visual Desktop Access (NVDA) | http://www.nvda-project.org/ | Free |
| System Access To Go | http://www.satogo.com/ | Free |
| Thunder | http://www.screenreader.net/index.php?pageid=11 | Free |
| WebAnywhere | http://webanywhere.cs.washington.edu/wa.php | Free |
| Hal | http://www.yourdolphin.co.uk/productdetail.asp?id=5 | Commercial |
| JAWS | http://www.freedomscientific.com/jaws-hq.asp | Commercial |
| Supernova | http://www.yourdolphin.co.uk/productdetail.asp?id=1 | Commercial |
| Window-Eyes | http://www.gwmicro.com/Window-Eyes/ | Commercial |
Anti-Ragging Squad Duty Roster from 1st August to 31st August, 2017
Anti-Ragging Squad Duty Roster for Gents/Ladies Hostels from 12th July to 31st August, 2016
Anti-Ragging Squad Duty Roster for Gents / Ladies Hostels from 15th July to 31st August, 2013
Anti-Ragging Squad Duty Roster for Gents / Ladies Hostels from 1st August 2014 to 31st August, 2014
Anti-Ragging Squad Duty Roster for Gents/Ladies Hostels from 15th July to 31st August, 2015
Attendance Register of the Vth Semester Students of MBBS Student

Professor, Neuro-Anaesthesiology & Critical Care
Email : registrar@aiims.edu
Tel. No : 011-26594832
| Sr. No. | Name | From | To |
|---|---|---|---|
| 1 | Dr. Sanjeev Lalwani | 11.01.2015 | 19.09.2023 |
| 2 | Dr. Sanjay Arya | 01.02.2012 | 11.01.2015 |
| 3 | Dr. L.R. Murmu | 15.03.2008 | 07.07.2008 |
| 4 | Dr. Sunil Chumber | 04.02.2008 | 14.03.2008 |
| 5 | Dr. Sandeep Agarwala | 13.03.2007 | 04.02.2008 |

Professor, Deptt. of Pediatrics
Email : associatedeanacad@aiims.edu, rakesh_lodha@aiims.edu
Tel. No : 011-26594622
| Sr. No. | Name | From | To |
|---|---|---|---|
| 1 | Prof. Rajeev Kumar | Apr. 2017 | July 2024 |
| 2 | Prof. Virinder Kumar Bansal | Aug. 2016 | Apr. 2017 |
| Sr. No. | Name | From | To |
|---|---|---|---|
| 1 | Dr. Virinder Kumar Bansal | Nov. 2013 | Aug. 2016 |
| 2 | Dr. Rakesh Yadav | Jul. 2010 | Nov. 2013 |
| 3 | Dr. Sandeep Guleria | Nov. 2006 | Jul. 2007 |
| 4 | Dr. Sunil Chumber | Jul. 2006 | Jun. 2010 |
| 5 | Dr. Neerja Bhatla | Apr. 2006 | Jun. 2006 |
| 6 | Dr. Nikhil Tandon | Apr. 2004 | Mar. 2006 |
| 7 | Dr. Y. K. Joshi | Jun. 2001 | Apr. 2004 |
| 8 | Dr. R. B. Vajpayee | Nov. 1996 | May. 2001 |
| 9 | Dr. B. K. Kapoor | May. 1996 | Oct. 1996 |
| 10 | Dr. R. K. Pandhi | Feb. 1996 | May. 1996 |
| 11 | Dr. B. K. Kapoor | Sep. 1995 | Feb. 1996 |
| 12 | Dr. R. K. Pandhi | Jan. 1993 | Sep. 1995 |
| 13 | Dr. D. Takkar | Jan. 1991 | Dec. 1992 |
| 14 | Dr. K. K. talwar | May. 1989 | Dec. 1990 |
| 15 | Dr. Rakesh Tandon | Aug. 1987 | May. 1989 |
| 16 | Dr. Kusum Verma | Sep. 1985 | Sep. 1989 |
| 17 | Dr. N. C. Madan | Jul. 1984 | Sep. 1984 |
| 18 | Dr. Usha Nayar | Jul. 1981 | Jul. 1984 |
| 19 | Dr. Ramesh Kumar | Apr. 1979 | Jul. 1981 |
| 20 | Dr. I.K. Dhawan | Jan. 1977 | Mar. 1979 |
| 21 | Dr. M.M. Kapoor | Jan. 1975 | Jan. 1977 |
| 22 | Dr. J.S. Bajaj | Jan. 1974 | Dec. 1974 |
| 23 | Dr. M.M. Kapoor | May. 1973 | Dec. 1973 |
| 24 | Dr. J.S. Bajaj | Apr. 1972 | May. 1973 |

Email : dean@aiims.edu
Tel. No : 011-26594833
| Sr. No. | Name | From | To |
|---|---|---|---|
| 1 | Dr. Neena Khanna | 1st Dec.2021 | 30th June 2022 |
| 2 | Prof. Anita Saxena | 29th Aug.2020 | 30th Oct. 2021 |
| 3 | Dr.Chitra Sarkar | 3rdAug 2020 | 28thAug 2020 |
| 4 | Dr. V. K. Bahl | 11th Jun 2018 | 31st Jul 2020 |
| 5 | Dr. Y .K.Gupta | Jan. 2018 | 30th April 2018 |
| 6 | Dr. Balram Airan | Jun. 2015 | 31st Dec. 2017 |
| 7 | Dr. P. K. Julka | Oct. 2013 | May 2015 |
| 8 | Dr. Shashi Wadhwa | May. 2012 | July 2013 |
| 9 | Dr. Rani Kumar | Mar. 2009 | April 2012 |
| 10 | Dr. R. C. Deka | May. 2006 | March 2009 |
| 11 | Dr. Kusum Verma | Aug. 2004 | Sep. 2005 |
| 12 | Dr. H. K. Tewari | Jul. 2003 | July 2004 |
| 13 | Dr. P. VenuGopal | Jan. 2002 | July 2003 |
| 14 | Dr. R. B. Vajpayee | Nov. 2001 | Jan. 2002 |
| 15 | Dr. P. K. Dave | May. 2001 | Nov. 2001 |
| 16 | Dr. M. C. Maheshwari | Oct. 1996 | Apr. 2001 |
| 17 | Dr. L. K. Bhutani | Apr. 1996 | Sep. 1996 |
| 18 | Dr. L. M. Nath | Jun. 1993 | Mar. 1996 |
| 19 | Dr. P. K. Khosla | Sep. 1992 | Mar. 1993 |
| 20 | Dr. U. Sharma | Oct. 1990 | Aug. 1992 |
| 21 | Dr. B. N. Tandon | Sep. 1989 | Sep. 1990 |
| 22 | Dr. M. M. S. Ahuja | May. 1988 | Aug.1989 |
| 23 | Dr. O. P. Ghai | Jul. 1987 | Apr, 1988 |
| 24 | Dr. J. S. Guleria | Mar. 1985 | May. 1987 |
| 25 | Dr. L. N. Mahapatra | Apr. 1984 | Feb. 1985 |
| 26 | Dr. P. Chandra | Mar. 1979 | Mar. 1984 |
| 27 | Dr. L. P. Agarwal | Nov. 1977 | Mar. 1979 |
| 28 | Dr. N. H. Keswani | Feb. 1974 | Nov. 1977 |
| 29 | Dr. B. K. Anand | Sep. 1969 | Feb. 1974 |
| 30 | Dr. K. L. Wig | Jul. 1962 | Aug. 1969 |
All India Institute Of Medical Sciences, New Delhi website complies with World Wide Web Consortium (W3C) Web Content Accessibility Guidelines (WCAG) 2.0 level AA. This will enable people with visual impairments access the website using assistive technologies, such as screen readers. The information of the website is accessible with different screen readers.
| Screen Reader | Website | Free / Commercial |
|---|---|---|
| Various Screen Readers to choose from | ||
| Non Visual Desktop Access (NVDA) | http://www.nvda-project.org/ | Free |
| System Access To Go | http://www.satogo.com/ | Free |
| Thunder | http://www.screenreader.net/index.php?pageid=11 | Free |
| WebAnywhere | http://webanywhere.cs.washington.edu/wa.php | Free |
| Hal | http://www.yourdolphin.co.uk/productdetail.asp?id=5 | Commercial |
| JAWS | http://www.freedomscientific.com/jaws-hq.asp | Commercial |
| Supernova | http://www.yourdolphin.co.uk/productdetail.asp?id=1 | Commercial |
| Window-Eyes | http://www.gwmicro.com/Window-Eyes/ | Commercial |
The faculty of the Department has been participating in Community health camps frequently.

Prof. Nagarur Gopinath who established the dept of Cardiothoracic surgery at the AIIMS in 1964, passed away on Sunday,3rd june, 2007 at Bangalore. He was 84.
He began open heart surgery at the AIIMS in 1964, and began a training program in CTVS, leading to the M.Ch degree in 1966.He has trained a large number of students including half the faculty at the AIIMS. His students are now heading many of the departments in the country.He received the padma Shri from the govt. of India, and the wockhardt lifetime achievement award in 2004,and the lifetime achievement award from the Indian Association of cardiovascular-Thoracic surgeons in 2000.
Following his retirement in 1982 he continued to serve the AIIMS as Emeritus professor and contributed many monographs and papers on preventive aspects of heart disease. He is survived by Mrs. Gopinath, one daughter and two sons. The cardiothoracic centre will certainly feel the void left behind by Prof.Gopinath which will be difficult to fill.
| S.No. | Name | Designation |
|---|---|---|
| 1 | Mr. Ashok Kumar | PS |
| 2 | Ms. Rachna | PA |
| a | New patient with appointment | C wing, Ground Floor |
| b | New patient without appointment | B wing, Ground Floor |
| c | Follow up patient with appointment | 3rd Floor counter |
| d | Follow up patient without appointment | A wing 3rd Floor and C wing Ground floor |
| e | All clinics appointment | 3rd Floor counter |
| f | Advance appointment | 3rd Floor counter |
Anti-Ragging Squad Duty Roster from 1st August to 31st August, 2017
Anti-Ragging Squad Duty Roster for Gents/Ladies Hostels from 12th July to 31st August, 2016
Anti-Ragging Squad Duty Roster for Gents / Ladies Hostels from 15th July to 31st August, 2013
Anti-Ragging Squad Duty Roster for Gents / Ladies Hostels from 1st August 2014 to 31st August, 2014
Anti-Ragging Squad Duty Roster for Gents/Ladies Hostels from 15th July to 31st August, 2015
Attendance Register of the Vth Semester Students of MBBS Student
Professor, Neuro-Anaesthesiology & Critical Care
Email : registrar@aiims.edu
Tel. No : 011-26594832
| Sr. No. | Name | From | To |
|---|---|---|---|
| 1 | Dr. Sanjeev Lalwani | 11.01.2015 | 19.09.2023 |
| 2 | Dr. Sanjay Arya | 01.02.2012 | 11.01.2015 |
| 3 | Dr. L.R. Murmu | 15.03.2008 | 07.07.2008 |
| 4 | Dr. Sunil Chumber | 04.02.2008 | 14.03.2008 |
| 5 | Dr. Sandeep Agarwala | 13.03.2007 | 04.02.2008 |
Professor, Deptt. of Pediatrics
Email : associatedeanacad@aiims.edu, rakesh_lodha@aiims.edu
Tel. No : 011-26594622
| Sr. No. | Name | From | To |
|---|---|---|---|
| 1 | Prof. Rajeev Kumar | Apr. 2017 | July 2024 |
| 2 | Prof. Virinder Kumar Bansal | Aug. 2016 | Apr. 2017 |
| Sr. No. | Name | From | To |
|---|---|---|---|
| 1 | Dr. Virinder Kumar Bansal | Nov. 2013 | Aug. 2016 |
| 2 | Dr. Rakesh Yadav | Jul. 2010 | Nov. 2013 |
| 3 | Dr. Sandeep Guleria | Nov. 2006 | Jul. 2007 |
| 4 | Dr. Sunil Chumber | Jul. 2006 | Jun. 2010 |
| 5 | Dr. Neerja Bhatla | Apr. 2006 | Jun. 2006 |
| 6 | Dr. Nikhil Tandon | Apr. 2004 | Mar. 2006 |
| 7 | Dr. Y. K. Joshi | Jun. 2001 | Apr. 2004 |
| 8 | Dr. R. B. Vajpayee | Nov. 1996 | May. 2001 |
| 9 | Dr. B. K. Kapoor | May. 1996 | Oct. 1996 |
| 10 | Dr. R. K. Pandhi | Feb. 1996 | May. 1996 |
| 11 | Dr. B. K. Kapoor | Sep. 1995 | Feb. 1996 |
| 12 | Dr. R. K. Pandhi | Jan. 1993 | Sep. 1995 |
| 13 | Dr. D. Takkar | Jan. 1991 | Dec. 1992 |
| 14 | Dr. K. K. talwar | May. 1989 | Dec. 1990 |
| 15 | Dr. Rakesh Tandon | Aug. 1987 | May. 1989 |
| 16 | Dr. Kusum Verma | Sep. 1985 | Sep. 1989 |
| 17 | Dr. N. C. Madan | Jul. 1984 | Sep. 1984 |
| 18 | Dr. Usha Nayar | Jul. 1981 | Jul. 1984 |
| 19 | Dr. Ramesh Kumar | Apr. 1979 | Jul. 1981 |
| 20 | Dr. I.K. Dhawan | Jan. 1977 | Mar. 1979 |
| 21 | Dr. M.M. Kapoor | Jan. 1975 | Jan. 1977 |
| 22 | Dr. J.S. Bajaj | Jan. 1974 | Dec. 1974 |
| 23 | Dr. M.M. Kapoor | May. 1973 | Dec. 1973 |
| 24 | Dr. J.S. Bajaj | Apr. 1972 | May. 1973 |
Email : dean@aiims.edu
Tel. No : 011-26594833
| Sr. No. | Name | From | To |
|---|---|---|---|
| 1 | Dr. Neena Khanna | 1st Dec.2021 | 30th June 2022 |
| 2 | Prof. Anita Saxena | 29th Aug.2020 | 30th Oct. 2021 |
| 3 | Dr.Chitra Sarkar | 3rdAug 2020 | 28thAug 2020 |
| 4 | Dr. V. K. Bahl | 11th Jun 2018 | 31st Jul 2020 |
| 5 | Dr. Y .K.Gupta | Jan. 2018 | 30th April 2018 |
| 6 | Dr. Balram Airan | Jun. 2015 | 31st Dec. 2017 |
| 7 | Dr. P. K. Julka | Oct. 2013 | May 2015 |
| 8 | Dr. Shashi Wadhwa | May. 2012 | July 2013 |
| 9 | Dr. Rani Kumar | Mar. 2009 | April 2012 |
| 10 | Dr. R. C. Deka | May. 2006 | March 2009 |
| 11 | Dr. Kusum Verma | Aug. 2004 | Sep. 2005 |
| 12 | Dr. H. K. Tewari | Jul. 2003 | July 2004 |
| 13 | Dr. P. VenuGopal | Jan. 2002 | July 2003 |
| 14 | Dr. R. B. Vajpayee | Nov. 2001 | Jan. 2002 |
| 15 | Dr. P. K. Dave | May. 2001 | Nov. 2001 |
| 16 | Dr. M. C. Maheshwari | Oct. 1996 | Apr. 2001 |
| 17 | Dr. L. K. Bhutani | Apr. 1996 | Sep. 1996 |
| 18 | Dr. L. M. Nath | Jun. 1993 | Mar. 1996 |
| 19 | Dr. P. K. Khosla | Sep. 1992 | Mar. 1993 |
| 20 | Dr. U. Sharma | Oct. 1990 | Aug. 1992 |
| 21 | Dr. B. N. Tandon | Sep. 1989 | Sep. 1990 |
| 22 | Dr. M. M. S. Ahuja | May. 1988 | Aug.1989 |
| 23 | Dr. O. P. Ghai | Jul. 1987 | Apr, 1988 |
| 24 | Dr. J. S. Guleria | Mar. 1985 | May. 1987 |
| 25 | Dr. L. N. Mahapatra | Apr. 1984 | Feb. 1985 |
| 26 | Dr. P. Chandra | Mar. 1979 | Mar. 1984 |
| 27 | Dr. L. P. Agarwal | Nov. 1977 | Mar. 1979 |
| 28 | Dr. N. H. Keswani | Feb. 1974 | Nov. 1977 |
| 29 | Dr. B. K. Anand | Sep. 1969 | Feb. 1974 |
| 30 | Dr. K. L. Wig | Jul. 1962 | Aug. 1969 |
Focus areas of clinical care and research of the Department.
The department of Cardiac Anaesthesia maintains its records, duly catalogued indexed and computerized (Since Oct 2006) using SPSS software. The headings under which the records are categorized are as under:
These records are registered daily in operation theatre on a medical record sheet and register and also computerized. Annual report of department records is submitted annually.
The normal functioning of the department is according to the rules and regulations laid down by CN Centre, AIIMS. Seven Theatres function everyday with 2 or 3 cases in each theatre daily. One Emergency heart surgery may be taken up anytime in the day/night. One consultant and one or two seniors residents round the clock emergency duty for postoperative care of cardiac patients as well as intensive and ventilatory/resuscitative management in coronary care unit. One consultant on round the clock call for emergency operations. Anaesthesia is given for a total of 14-20 heart operations everyday with postop and coronary ventrilatory care. General anesthesia or monitored anaesthesia care is given in cath. Lab and computerized angiography and MRI in Cardiac patients.Two senior residents are on emergency call-attending calls from CCU, ICU, CTVS wards, Cath. Lab. and Operation Theatres. Bedside pre anaesthetic check up is done daily.
2 academic sessions held per week as part of department’s academic activity – where seminars/Tutorials/Journal Clubs/Examinations are held by faculty & residents. The department has access to the AIIMS Dr. B.B.Dixit Library and National Medical Library at all times. Internet access is available via computer facility in all consultant’s rooms.
एआईआईएमएस में हृदयरोगविज्ञान विभाग, प्रो. सुजॉय बी. रॉय के नेतृत्व में स्थापित किया गया। इस विभाग ने चिकित्सीय देखभाल की उत्कृष्ट सुविधाएं विकसित की है और यहाँ पर वयस्कों तथा बाल चिकित्सा की पूर्णत: विकसित सुविधाएं उपलब्ध हैं जैसे कि कोरोनरी हस्तक्षेप, वॉल्वुलोप्लास्टी, जन्मजात शंटों का डिवाइज़ क्लोज़र और इलेक्ट्रोफिसियोलॉजी सेवाएं (जिसमें रेडियोफ्रिक्वेन्सी पृथक्करण, पेसमेकर, बाय-वेंट्रिकुलर पेसमेकर और कार्डिर्योवर्टर डिफाइब्रिलेटर आरोपण शामिल है)। प्रयोगशाला परीक्षण सुविधाओं में ट्रेडमिल परीक्षण, होल्टर रिकॉर्डिंग, इकोकार्डियोग्राफी (ट्रान्सथोरासीक, ट्रान्सइसोफिगल, थ्री-डी और भ्रूण इकोकार्डियोग्राफी समेत), सिन्कोप हेतु टिल्ट परीक्षण तथा कार्टो प्रणाली मैपिंग समेत इलेक्ट्रोफिसियोलॉजी परीक्षण शामिल हैं। इस विभाग ने वातज्वर और वात हृदयरोग के क्षेत्र में उल्लेखनीय कार्य किया है जैसे कि किशोर-संबंधी माइट्रल स्टेनोसिस, एंजियोप्लास्टी, एरिथमिया, कार्डियोमायोपैथी तथा जन्मजात हृदयरोग।
हृदयरोग (कार्डियोलॉजी) विभाग की स्थापना के समय से ही विभागाध्यक्षों के नाम निम्नलिखित हैं:
| नाम |
|---|
| प्रो. सुजॉय बी रॉय |
| प्रो मदन लाल भाटिया |
| प्रो. राजन टंडन |
| प्रो. हरबंस सिंह वसीर |
| प्रो. सुभाष चंद मनचंदा |
| प्रो. केवल कृष्ण तलवार |
| प्रो. के. श्रीनाथ रेड्डी |
| प्रो. विनय कुमार बहल |
| प्रो. अनीता सक्सेना |
| प्रो. श्याम सुंदर कोठारी |
| Prof. Balram Bhargava |
| प्रो. राजीव नारंग (वर्तमान विभागाध्यक्ष) |
This web page is for the patients undergoing Coronary Artery Bypass Grafting (CABG). This web page attempts to explain the cause of the disease, the risk factors, the effects of disease and possible treatment options. It tells about the surgery, preoperative preparation and postoperative care in hospital and at home. Lastly, an effort has been made to spread preventive awareness about the coronary artery disease. For better understanding, at the cost of technical perfection, language has been made as simple as possible.
This web page is for the patient who has a heart valve problem and who seeks treatment for the same. The web page describes in various chapters some of the fundamentals of blood circulation through the heart and the function of the valves and the effects of the disease. The web page also tells about the symptoms, tests that are used for diagnosis and after care. It tells about the surgery and postoperative care while the patient is in hospital. Finally it explains the aftercare when the patient is at home. For the purpose of better understanding, language has been made as simple as possible and efforts have been made to explain the facts in common language.
A need was felt by the nursing administrators that a planned nursing in-service education needs to be started so as to increase the knowledge base of practicing nurses in order to improve & maintain high standard of nursing care at the AIIMS Hospital.
To increase the existing knowledge base of nurses practicing clinical nursing.
To improve and maintain high standard of nursing care to patients at the AIIMS Hospital., which would increase the satisfaction level of patients / relatives.
To improve communication skills among nursing personnel at AIIMS.
To update knowledge regarding handling / upkeep of latest & sophisticated instruments and gadgets.
To enable nurses to secure credit points for renewing their nursing license by the DNC.
Nursing in-service education is one of the cornerstones in professional development of nursing personnel working in AIIMS. A need based nursing in-service program has been started w.e.f. January 2011. This is started with the aim of updating clinical nursing knowledge on the premise of continuing nursing education. The program is well structured with thrice a week classes.( Two classes for bedside nurses and one class for Sister in-charges and above)
This is done for practicing nurses to increase their knowledge base in order to improve the standard of nursing care at the AIIMS. Once a week classes are conducted for middle level managers focusing on Nursing Administration and Management. In the month of January 2011, a well organized induction & orientation program was conducted for 133 newly recruited nurses at the main hospital by the In-service nursing educator.
In 2012, a total of 297 newly recruited nurses got oriented by designated nursing personnel in two sessions, regarding various aspects viz. hospital layout, various departments, OPD schedules and their professional duties and responsibilities.
| Facilitator | : | Mrs. B.D Prema H Kumar, Chief Nursing Officer (acting) [RN, RM & B.Sc (PC)] |
| Officer In-charge & Mentor | : | Mrs. Ansamma Neelakantan, Deputy Nursing Superintendent [RN, RM & B.Sc (PC)] |
| Educator/ Co-ordinator | : | Mrs. Rebecca J. Herald, Sister Grade I(HR) [RN, RM, B.Sc.(N), Masters in Nursing (Gold Medalist)] |
| Mrs.Merin Lisa Kuriakose, Sister Grade II [RN, RM, B.Sc.(N), M.Sc (N)] |
The following C.N.E.classes were conducted for the year 2012 in the Main Hospital.
Classes for Sister Incharges/ANS/DNS/NS/CNO
Materiel Management
Ethical and Legal issues in clinical nursing
Conflict Management
Stress Management
Nursing Administration
Classes for bedside nurses
Patient safety
Nursing Process
Ethical and Legal issues in clinical nursing
Pre and post operative Nursing Management
Stress Management
Medication Administration Safety
Asstt. Nursing Supdt, is responsible to Deputy Nursing Supdt. for the total nursing care of patients, management and development of the unit assigned to her: -
Assist the total needs of patients in the unit and prepare planned nursing care.
Demonstrate and Supervise the nursing care of patients in the unit.
Attend regular round in the unit with the medical and nursing personnel.
Reviewing reports from Sr. Gr. I regarding the nursing care of patients in each shifts.
Give counseling and health education to the patients and their attendants.
Plan and arrange duty for nursing personnel posted under her.
To ensure availability of adequate nursing staff in all shifts.
Maintain cleanliness of unit its annexes and environment.
Interact with the engineering service department for proper up keep of the unit.
Keeping Deputy Nursing Supdt., Nursing Supdt. informed of the needs of the patient care areas and bring it to their notice any special problems.
Guide the Sister Grade-I to ensure supplies and equipments of different stores, and re-checking their use and care.
Daily check of emergency and dangerous drugs, life saving equipments i.e.monitors, ventilators, defibrillators, suction machines and O2 points etc., to ensure their proper functioning.
Periodical check of all stocks and supplies.
Maintain good inter-personnel relationship with all categories of staff, patients and their relatives.
Maintain good public relation with patients relatives and the public, and project positive image of the hospital.
Maintain disciple of nursing and domestic staff.
Interpretation of Hospital policies, rules and regulations.
Daily check of attendance and reporting the lapses.
Investigate complaints if any.
Work evaluation and confidential reports.
Guidance and counseling of nursing staff in the unit.
Project the annual requirements of drugs supplies and equipments for the units.
Take care of legal aspects and report about the medico legal cases in the ward.
Plan and implement a proper orientation programme for new nursing staff, student nurse and domestic staff.
Participate in In-service education of nursing personnel and attend the meetings.
Give incidental and planned teaching to nursing personnel in the unit, as well as domestic staff.
Participate in clinical teaching for student nurses in Co-operation with the nursing tutor.
Perform any other duties assigned to her for time to time.
Deputy Nursing Superintendent is responsible to the Nursing Supdt. and assist her in the administration of nursing services in the hospital.
Supervise the nursing care given to the patients in various departments by taking regolar round of her area.
Act as a liasion officer between Nursing Supdt. and the nursing staff of the hospital.
Interpret the pliicies and procedures of the Nursing service department to sub-oradinate staff and others.
Attend the emergency calls concerning nursing services or hostel problems.
Receive evening and night reports from the Assistant Nursing Supdt./Supervisors.
Keep records and reports of Nursing Services.
Maintain the records of attendance of nursing staff and leave of any kind.
Conduct regolar physical verification of hospital stocks, i.e. drugs, equipments etc.
Initiate procedure for condemnation and procurement of hospital equipment/linen etc.
Maintain the confidential report and records of nursing personnel.
Assist the nursing supdt. in making master duty roster of nursing personnel.
Assist the nursing superintendent in Recruitment of nursing staff.
Assist the nursing supdt. on planning and organising nursing services in the hospital.
Officiate in the absence of nursing supdt.
Attend the official meetings.
Keep the senior nursing Officials (CNO & NS) informed of the happenings in the wards.
Assist in planning/organising and implementing staff development programmes.
Ensure clinical experience facilities for student nurses in various clinical areas of the hospital.
Provide guidance and counseling to nursing staff.
Arrange orientation programmes for new nursing staff.
Maintain discipline among nursing personnel.
Organise educational programmes for graduate/post graduate students from different hospitals with the co-ordiantion of clinical instructor/lecturer clilege of nursing.
Escorts special visitors, Nursing Superintendent, Medical Superintendent for hospital rounds.
Arranges and participates in professional and social functions of the staff and students.
Maintains good public relations.
Any other duties assigned to her from time to time.
Nursing Superintendent is responsible to the C.N.O. for planning organisation and development of nursing services in the hospital in consultation with Medical Supdt./Chief of centres.
She/he will be responsible for efficient running of Nursing Services of the Main hospital and various centres of AIIMS.
She will assist the Director in formulating broad policies concerning Nursing Services.
She will disseminate the AIM, objectives and policies regarding patient care to all cadres of nursing services.
She will implement policies and procedures of Institute regarding nursing services.
She/he will plan future requirements of nurses and carry out recruitment of nurses from time to time.
She/he will plan and disseminate programmes for continuting education re-orientation programmes for nurses.
She/he will closely interact with other hospitals regarding improvement of patient care.
She/he will encourage research by nurses in their work areas.
She/he will guide and conunsel the sub-ordinate nursing staff.
She/he will keep herself abreast of latest happenings in nursing care by attending National / International conferences.
She will strive to implement standard nursing practices and maintain highest quality of care.
She will critically analyse the budgets for nursing services from Main hospital and various centers before being forwarded to Director.
Evaluate confidential reports of higher level nursing officers and recommend for promotion.
She will be assisted in her duties by nursing Supdt.’s, of Main Hospital and from the centres.
She will keep the Director informed about the happening concerning the hospital.
Head of Departments (Independent) | |
| Department | Name of the Head |
| Deptt. of Anaesthesiology | Dr. Lokesh Kashyap |
| Deptt. of Anatomy | Dr. A.Sharrif |
| Deptt. of Biochemistry | Dr.Kalpana Luthra |
| Deptt. of Biophysics | Dr. Punit Kaur |
| Deptt. of Biostatistics | Dr. Maroof Ahmad Khan |
| Deptt. of Biotechnology | Dr. Anushree Gupta |
| Centre for Community Med. | Dr. Kiran Goswami |
| Deptt. of Derm. & Vene. | Dr Kaushal K Verma |
| Deptt. of Endo. & Metab. | Dr. Nikhil Tandon |
| Deptt. of Emergency Medicine | Dr. Rakesh Yadav |
| Deptt. of Forensic Medicine & Toxicology. | Dr. Sudhir Kumar Gupta |
| Deptt. of Gastro. & HNU | Dr. Pramod kr. Garg |
| Deptt. of G.I. Surgery & Liver Transplantation | Dr. Sujoy Pal |
| Deptt. of Haematology | Dr.M.Mahapatra |
| Deptt. of Transplant Immunology & Immunogenetics | Dr. D.K. Mitra |
| Deptt. of Hospital Administration | Dr. Sidhartha Satpathy |
| Deptt. of Lab. Med. | Dr. Sudip Kr. Dutta |
| Deptt. of Medicine | Dr. Naveet Wig |
| Deptt. of Pulmonary Medicine & Sleep Disorders | Dr. Anant Mohan |
| Deptt. of Geriatric Medicine | Dr. Naveet Wig |
| Deptt. of Microbiology | Dr. Lalit Dhar |
| Deptt. of Nephrology | Dr. D.Bhowmik |
| Deptt. of Nuclear Magnetic Resonance | Dr. Rama Jayasunder |
| Deptt. of Nuclear Medicine | Dr. C.S. Bal |
| Deptt. of Obst. & Gynae. | Dr. Neena Malhotra |
| Deptt. of Orthopaedics | Dr. |
| Deptt. of E.N.T. | Dr. Alok Thakkar |
| Deptt. of Paediatrics | Dr. Madhulika Kabra |
| Deptt. of Paediatric Surgery | Dr.Sandeep Agarwala |
| Deptt. of Pathology | Dr. V.K.Iyer |
| Deptt. of Pharmacology | Dr. D.V.S.Arya |
| Deptt. of Physical Medicine & Rehabilitation | Dr. Sanjay Wadhwa |
| Deptt. of Physiology | Dr. K.P. Kochhar |
| Deptt. of Psychiatry | Dr. Pratap Sharan |
| Deptt. of Radiodiagnosis | Dr. Deep N.Srivastava |
| Deptt. of Reprod. Biology | Dr. A.Haldar |
| Deptt. of Surgical Disciplines | Dr. Sunil Chumber |
| Deptt. of Urology | Dr. Amlesh Seth |
| Principal, College of Nursing | Dr. Latha Venkatescan |
Head of Departments (Under the Chief of Centres) | |
| Deptt. of Cardiology | Dr. Rajiv Narang |
| Deptt. of Cardiac Anaesthesia | Dr. Neeti Makhija |
| Deptt. of Cardiac Radiology | Dr. Sanjiv Sharma |
| Deptt. of Medical Oncology | Dr. Lalit Kumar |
| Deptt. of Surgical Oncology | Dr. S.V.S.Deo |
| Deptt. of Neurology | Dr. Manjari Tripathi |
| Deptt. of Neurosurgery | Dr. S.S.Kale |
| Deptt. of Neuro Anaesthesia | Dr. Arvind |
NURSING SERVICES AT A.I.I.M.S.
A glance at Nursing Services at AIIMS, New Delhi...
Nursing services forms an integral part of any health care facility. These \services aim at high quality nursing care to the patients and community. The professional nurses work in an environment that encourages professionalism and expertise in providing holistic patient care with the members of allied disciplines in the hospital. The nurses at AIIMS conduct themselves within the boundary of ethical and legal framework.
Indeed, on any given day, nursing professionals handle a wide array of responsibilities ranging from patient care, ward management, humanre sources management, facilities management, as well as attendant’s management.
Importance of values in nursing
When working in healthcare, nurses often handle fast-paced situations that require quick decisions and specific skills, so having a value system in place is fundamental. Not only do they provide a frame work of behavior and help to influence important decision, they;
Core Values in Delivering Patient Care
ORGANIZATION OF NURSING SERVICES
Chief Nursing Officer - Nursing Superintendent - Dy. Nursing Superintendent - Asstt. Nursing Superintendent - Senior Nursing Officer - Nursing Officer
SIU Norms
One of the major challenges in nursing administration is staffing nursing units. Staffing in AIIMS, New Delhi is based on SIU Norms which are as follows :
Nursing Superintendent is responsible to the C.N.O. for planning organisation and development of nursing services in the hospital in consultation with Medical Supdt./Chief of centres.
Deputy Nursing Superintendent is responsible to the Nursing Supdt. and assist her in the administration of nursing services in the hospital.
NURSING ADMINISTRATION
EDUCATIONAL ACTIVITIES
GENERAL DUTIES
Asstt. Nursing Supdt, is responsible to Deputy Nursing Supdt. for the total nursing care of patients, management and development of the unit assigned to her :
NURSING CARE
WARD MANAGEMENT
TEACHING AND SUPERVISION

Address : Room No. 1009, Ist Floor, PC Block Deptt of Anatomy AIIMS, N. Delhi
Phone : 011-26593216
Research Focus: Pain arising from burn injury is a devastating experience for patients. Results of our research in rodents show that blocking the B2 subtype of bradykinin receptor produces significant relief from burn-induced pain. An attempt to test this alternative hypothesis in a clinical trial to be conducted in the largest burn unit in the country could not be done, due to lack of funds. Other putative drugs, which have shown efficacy in rodents are the cannabinoid type 1 receptor and the somatostatin type 2A receptor agonist. These could relieve specific parameters of pain like pain-at-rest but not touch-induced allodynia.
1. George J. et al. 2014. J Burn Care Res 35:e391-398 (Published by American Burn Association)
2. Kumar R. et al. 2016. Indian J Med Res 144:730-740.
3. Kumar R. et al. 2018. Eur J Anaesthesiol 35:955-965.
Intrathecal catheterization with drug administration in rodents is a novel technique for simulating intraspinal administration of drugs during cardiac surgery. I underwent training at the Anesthesia Research Laboratory of University of California at San Diego for 3 months in 2008. It was supported by an International biomedical associateship grant from Indian Council of Medical Research, N. Delhi.
Substance P receptor antagonists when administered through catheters in rodents proved effective in ameliorating post-operative pain. A more potent effect was obtained when it was combined with local peripheral administration.
1. Gautam M et al. 2016. Spinal Cord 54:172-182.
2. Gupta S et al 2018. Ann Neurosci 25:268-276.
Current research work is focused on developing rat models of (1) Neuropathic pain by partial sciatic nerve ligation (2) Osteoarthritis by intra-articular injection of monoiodoacetate. Both are chronic diseases which compromises the quality of life.
Assistant Prof at B. P. Koirala Institute of Health Sciences, Nepal in 1997.
Address : Room No. 1009, Ist Floor, PC Block Deptt of Anatomy AIIMS, N. Delhi
Phone : 011-26593216
Research Focus: Pain arising from burn injury is a devastating experience for patients. Results of our research in rodents show that blocking the B2 subtype of bradykinin receptor produces significant relief from burn-induced pain. An attempt to test this alternative hypothesis in a clinical trial to be conducted in the largest burn unit in the country could not be done, due to lack of funds. Other putative drugs, which have shown efficacy in rodents are the cannabinoid type 1 receptor and the somatostatin type 2A receptor agonist. These could relieve specific parameters of pain like pain-at-rest but not touch-induced allodynia.
1. George J. et al. 2014. J Burn Care Res 35:e391-398 (Published by American Burn Association)
2. Kumar R. et al. 2016. Indian J Med Res 144:730-740.
3. Kumar R. et al. 2018. Eur J Anaesthesiol 35:955-965.
Intrathecal catheterization with drug administration in rodents is a novel technique for simulating intraspinal administration of drugs during cardiac surgery. I underwent training at the Anesthesia Research Laboratory of University of California at San Diego for 3 months in 2008. It was supported by an International biomedical associateship grant from Indian Council of Medical Research, N. Delhi.
Substance P receptor antagonists when administered through catheters in rodents proved effective in ameliorating post-operative pain. A more potent effect was obtained when it was combined with local peripheral administration.
1. Gautam M et al. 2016. Spinal Cord 54:172-182.
2. Gupta S et al 2018. Ann Neurosci 25:268-276.
Current research work is focused on developing rat models of (1) Neuropathic pain by partial sciatic nerve ligation (2) Osteoarthritis by intra-articular injection of monoiodoacetate. Both are chronic diseases which compromises the quality of life.
Assistant Prof at B. P. Koirala Institute of Health Sciences, Nepal in 1997.
As part of the Department Hospital Administration, AIIMS Delhi, various training and courses are imparted. For further details,
The Department of Pathology at A.I.I.M.S, founded in 1957, has been a pioneer in the field of pathology since its inception. The Department is a leading innovator in research, service and education. It has established a lead in medical research involving nutrition, cell differentiation, epidemiology, virology, various malignancies and neuro-sciences. Department of pathology is providing specialised pathology and Oncopathology services to whole of AIIMS and Dr.B .R.A IRCH (Dr. B. R. Ambedkar Institute Rotary Cancer Hospital) for many years.
The department of Oncopathology at NCI Jhajjar forms the backbone of all Oncology services provided at our center. Since its inception, the department has grown from strength to strength and aims to set up the Units of Histopathology, Cytology, Immunohistochemistry, Cytogenetics and Molecular pathology. Working in close coordination with teams from AIIMS Delhi, we strive to establish a world class diagnostic center dedicated to care and management of cancer patients.
Department of pathology is also providing full Oncopathology services to NCI Jhajjar with full involvement of all specialities as detailed below
Nuclear Medicine is a specialized branch of medicine that encompasses arrays of radiopharmaceuticals for both diagnostic and therapeutic purposes throughout the patient care continuum. The department at NCI has state-of- art facilities such as a digital ready 128 slice PET/CT and 16 Slice SPECT/CT, and currently offers the most commonly performed oncological studies.


Medical Physics Unit at IRCH and NCI is instrumental in providing licensing and compliance with the regulations of Atomic Energy Regulatory Board (AERB) to all x-ray imaging machines, radiation safety and quality in imaging related services to all those departments which uses radiation in imaging, patient services and research activities. We look after radiation related research in medical radiological imaging in mammography, CT, ultrasound, radiography, fluoroscopy and angiography, radiation dosimetry in patient in imaging, reduction of dose without compromising diagnostic information, radiation protection and measurement of radiation dose to staff and attendants, irradiation of blood bag before blood transfusion to patients, radiation protection survey for radiological imaging installation all over AIIMS and NCI. Our activity includes staff and public education regarding radiation safety, besides imparting knowledge (in form of regular classes) in the field of Medical Physics and Radiation Safety to MD (radiology), MBBS students, B.Sc. Radiography, M.Sc. Biophysics, M.Sc. Cardio-radiology, nursing students and other interested groups and individuals which includes trainees from other hospitals. The unit provides consultation in any untoward accidental radiation exposure to patient, public or staff. Our endeavour makes radiation installations safe for patient, staff and public for which there is a great concern now-a-days. We have a viable PhD programme in Medical Physics running in the department.
The Department started functioning in 1983 with help of x-ray and mammography unit. It developed gradually. Today, the department, along with NCI Jhajjar has 3 CT machines, 1 MRI, 2 DSA, 2 mammography units with digital breast Tomosynthesis and Contrast enhanced mammography, in addition to numerous ultrasound and radiography units, including fluoroscopy and portable radiography. The department provides services to inpatients and outpatients of BRA-IRCH and NCI Jhajjar
| Equipment | BRA-IRCH | NCI Jhajjar |
|---|---|---|
| CT | 1 | 2 |
| MRI | 0 | 1 +1 (in process) |
| DSA | 1 | 1 |
The department provides diagnostic as well as interventional radiology services to cancer patients. Diagnostic CT scans, MRI, Ultrasound, Xray, Mammography are performed. Interventional procedures include biopsy and fine needle aspiration cytology under CT, Ultrasound and mammography guidance, percutaneous transhepatic biliary drainage, percutaneous nephrostomy, transarterial angioembolisation, Nerve blocks for pain relief, NG tube insertion, percutaneous gastrostomy, tumor ablative proVacuum assisted biopsy, clip placement and wire localisation of breast masses and vascular procedures such as peripherally inserted central line catheter and angioembolisation procedures.
The department boasts of turn-around report times of 24 hours. Dates for routine imaging (CT and Ultrasound) of all in-patients are given the next working day.
CThe Department of Head and Neck Oncology at the National Cancer Institute, Jhajjar, strives to offer affordable and quality service to patients with head and neck cancer. The department currently provides daily outpatient services (Monday to Friday), including various office-based procedures. We ensure optimal and quality clinical in-patient services in the current 20-bedded ward on the 5th floor. Additionally, we run a multidisciplinary disease management group twice a week (Tuesday and Friday) and a swallowing clinic with a facility for Functional endoscopic evaluation of swallowing (FEES) for appropriate rehabilitation of the patients after surgery in the OPD setting. Emergency services (management of airway and bleeding in relation to head and neck cancers) are offered round the clock. We are equipped with nasal endoscopy and fiberoptic laryngoscopy for clinical oncologic examination.
The department runs eight operation theaters weekly (Monday to Friday). It offers surgical treatment of cancer related to the domain of Otorhinolaryngology (maxillectomy, laryngectomy, neck dissection, glossectomy, thyroidectomies, mandibulectomy, etc.) for early and advanced oral, laryngeal, and other head and neck cancers.
In addition to clinical care, the department has also been playing a prominent role in academic and research activities. Residents training (MS {ENT} and MCh {Head and Neck Cancer Surgery}) is being undertaken with an emphasis on clinical care, research, and teaching aspects. The teaching courses in the subspecialties of Head and neck oncology are being conducted regularly.
Cancer is emerging as a major public health problem globally. As per WHO GLOBOCAN 2020, 1.32 million new cases of cancer are detected each year in India and 0.85 million succumb to this deadly disease. Cancer treatment requires a multimodal management approach. Surgery is one of the main modalities for treating cancer and 90 % of cancer patients need some surgical intervention. The surgical specialty dealing with cancer management is known as Surgical Oncology.
Background: Dedicated surgical oncology services at Dr. BRA-IRCH were started in 1988. Prof NK Shukla was the first faculty to initiate cancer surgical services and Dr. SVS Deo joined as second faculty in 1995. The unit was recognized as an independent Department of Surgical Oncology in the year 2001 and the services were further expanded to 46 Surgical beds, 6 bedded ICU and 3 major Operation theaters in 2005. MCh Surgical Oncology program was started in 2012. The department took a leadership role in the planning and establishment of state of art surgical oncology services at National Cancer Institute (NCI) Jhajjar and started cancer surgical services at NCI-AIIMS in 2019. Currently the department has 10 faculty members,18 MCh trainees and 12 Senior residents.
The three major activities of the department include Patient Care, Teaching & Training and Research.
The department leads in introducing advanced and cutting-edge surgical programs including Minimally Invasive Surgery (Lap & VATS), Peritoneal Surface Malignancies (Cytoreductive Surgery, HIPEC & PIPAC), Oncoplastic & Microvascular surgery, Risk Reducing Surgery, Navigational Surgery, Organ Conservation and Intra-operative Radiation Therapy and Palliative Surgical Oncology at AIIMS.
Teaching and Training: The department runs MCh Surgical Oncology program, which is one of the leading and popular MCh programs in India. In addition, the department offers long term and short-term training to general surgeons. The department has trained more than 150 cancer surgeons during last 25 years, who are in leadership positions in different parts of the country.
Research: The faculty members of the departmentare actively engaged in a number of collaborative basic and clinical research projects including multicentric international trials. The department has developed a computerized comprehensive oncology clinical data base and currently has comprehensive clinical data related to more than 10,000 cancer patients operated in the department. The faculty has published more than 300 scientific papers in prestigious national and international journals.
Other Activities: The faculty of the department are actively involved as members, experts and advisors for various organizations and scientific bodies like NBE, ICMR, DBT, DS, Ministry of Health, IASO, ISPSM, ABSI and BSI. The department regularly conducts workshops and organizes major conferences (ICC 2013, NATCON 21, ABSICON18 and INDO-UK Oncoplasty course, ISPSM-ESSO cadaver courses on CRS & HIPEC etc.)
History of Dept of Surgical Oncology
Major Landmarks & Timelines –
1983 - Dr. BRA-IRCH was established as a comprehensive cancer center of AIIMS
1988 - Dr. NK Shukla joined as first faculty and established a Unit of Surgical Oncology to offer basic cancer surgical services.
1991 – Senior Residency training program was started, and major cancer surgical services initiated.
1995 – Dr SVS Deo joined as second full-time faculty.
1996 – A dedicated 20 bedded Surgical Oncology ward along with a major OT and ICU were established with a philanthropic donation from Shri. Kanhayalal Punj.
2001 – Unit of Surgical Oncology was upgraded as a full-fledged independent Department
2005 – IRCH expanded to 182 bedded regional cancer Center including 48 Surgical Oncology beds and 3 major operation theaters.
2012 – M.Ch. course in Surgical Oncology was started with an annual intake of 5 students.
2012 – Dr. Sunil Kumar and Dr. MD Ray joined as full-time faculty
2017 – Prof. SVS Deo assumed the role of Head of Department after Prof. NK Shukla’s superannuation.
2018 – Three more faculty members Dr Sandeep Bhoriwal, Dr Ashutosh Mishra and Dr Jyoti Sharma joined the Department.
2019 – Inauguration of National Cancer Institute, AIIMS, Jhajjar campus by Honorable Prime Minister and launch of Surgical Oncology services at NCI campus.
2020 – Four more faculty members joined the department Dr. Naveen, Dr. Babul Bansal, Dr. Jyoutishman Saikia and Dr Raghuram K.
External Beam Radiotherapy Brachytherapy
| 4D-CT Simulation | ICRT |
| IMRT | ILRT |
| IGRT | Mould Brachytherapy |
| SGRT | Image Guided Brachytherapy |
| VMAT | Interstitial Brachytherapy |
| SBRT | - |
| SRT | - |
| TSET | - |
| TBI | - |
| Vision RT | - |
| Radiation under Anaesthesia | - |
1. Varian Trubeam 2.7 (2)

2. Flexitron (1)

3. 4D-CT Simulator (1)

Department of Radiation Oncology at NCI Jhajjar started functioning on May 29th, 2019 with brachytherapy. Subsequently, Linear Accelerator facilities were Inaugurated on 14th November 2019 in the presence of Director AIIMS Delhi Dr. Randeep Guleria, Head-NCI Dr. GK Rath, and Head of Department Dr. DN Sharma. Since thenaround 33,399 radiation fractions have been delivered via Linear Accelerator and 1108 patientstreated with brachytherapy. Apart from Radiation Treatment delivery, we are also running OPD and IPD services.OPD services are running since November 2019 site and organ-specific in collaboration with other departments. We have fully functional IPD services with 24 Bedded ward. Our effort toward patient care is reflected in the fact that during the COVID-era when all the regular services were affected Department of Radiation Oncology provided its services to the patients without hampering patient care.
Preventive Oncology NCI:

Preventive oncology includes measures that are taken to prevent the development or delay progression of cancer. Cancer prevention is taken on three major levels:
(A). Primary Cancer Prevention: It focuses on health promotion, identifying causative factors and reducing the risk of cancer. For example, alcohol and tobacco cessation, weight reduction, vaccination, healthy lifestyle, etc.
(B) Secondary Cancer Prevention: It focuses on early cancer detection through screening before the onset of symptoms when the cancers are likely to be treated successfully. For example, mammography, HPV-DNA test, oral visual inspection, PSA test, etc.
(C) Tertiary Cancer Prevention: It focuses on delaying the progression and preventing the complications like secondary malignancies after cancer diagnosis.
Why it's important:
Cancer prevention is done at both individual and community level for reducing the risk and incidence of cancer. By preventing cancer, the number of new cases of cancer will be lowered and thus reducing overall cancer burden. Early diagnosis will lead to optimal cancer management and improved survival.
Preventive Oncology at NCI-Jhajjar envisages to
develop evidence-based approaches and technical resources for cancer prevention and control in India through:
A need was felt by the nursing administrators that a planned nursing in-service education needs to be started so as to increase the knowledge base of practicing nurses in order to improve & maintain high standard of nursing care at the AIIMS Hospital.
To increase the existing knowledge base of nurses practicing clinical nursing.
To improve and maintain high standard of nursing care to patients at the AIIMS Hospital., which would increase the satisfaction level of patients / relatives.
To improve communication skills among nursing personnel at AIIMS.
To update knowledge regarding handling / upkeep of latest & sophisticated instruments and gadgets.
To enable nurses to secure credit points for renewing their nursing license by the DNC.
Nursing in-service education is one of the cornerstones in professional development of nursing personnel working in AIIMS. A need based nursing in-service program has been started w.e.f. January 2011. This is started with the aim of updating clinical nursing knowledge on the premise of continuing nursing education. The program is well structured with thrice a week classes.( Two classes for bedside nurses and one class for Sister in-charges and above)
This is done for practicing nurses to increase their knowledge base in order to improve the standard of nursing care at the AIIMS. Once a week classes are conducted for middle level managers focusing on Nursing Administration and Management. In the month of January 2011, a well organized induction & orientation program was conducted for 133 newly recruited nurses at the main hospital by the In-service nursing educator.
In 2012, a total of 297 newly recruited nurses got oriented by designated nursing personnel in two sessions, regarding various aspects viz. hospital layout, various departments, OPD schedules and their professional duties and responsibilities.
| Facilitator | : | Mrs. B.D Prema H Kumar, Chief Nursing Officer (acting) [RN, RM & B.Sc (PC)] |
| Officer In-charge & Mentor | : | Mrs. Ansamma Neelakantan, Deputy Nursing Superintendent [RN, RM & B.Sc (PC)] |
| Educator/ Co-ordinator | : | Mrs. Rebecca J. Herald, Sister Grade I(HR) [RN, RM, B.Sc.(N), Masters in Nursing (Gold Medalist)] |
| Mrs.Merin Lisa Kuriakose, Sister Grade II [RN, RM, B.Sc.(N), M.Sc (N)] |
The following C.N.E.classes were conducted for the year 2012 in the Main Hospital.
Classes for Sister Incharges/ANS/DNS/NS/CNO
Materiel Management
Ethical and Legal issues in clinical nursing
Conflict Management
Stress Management
Nursing Administration
Classes for bedside nurses
Patient safety
Nursing Process
Ethical and Legal issues in clinical nursing
Pre and post operative Nursing Management
Stress Management
Medication Administration Safety
Asstt. Nursing Supdt, is responsible to Deputy Nursing Supdt. for the total nursing care of patients, management and development of the unit assigned to her: -
Assist the total needs of patients in the unit and prepare planned nursing care.
Demonstrate and Supervise the nursing care of patients in the unit.
Attend regular round in the unit with the medical and nursing personnel.
Reviewing reports from Sr. Gr. I regarding the nursing care of patients in each shifts.
Give counseling and health education to the patients and their attendants.
Plan and arrange duty for nursing personnel posted under her.
To ensure availability of adequate nursing staff in all shifts.
Maintain cleanliness of unit its annexes and environment.
Interact with the engineering service department for proper up keep of the unit.
Keeping Deputy Nursing Supdt., Nursing Supdt. informed of the needs of the patient care areas and bring it to their notice any special problems.
Guide the Sister Grade-I to ensure supplies and equipments of different stores, and re-checking their use and care.
Daily check of emergency and dangerous drugs, life saving equipments i.e.monitors, ventilators, defibrillators, suction machines and O2 points etc., to ensure their proper functioning.
Periodical check of all stocks and supplies.
Maintain good inter-personnel relationship with all categories of staff, patients and their relatives.
Maintain good public relation with patients relatives and the public, and project positive image of the hospital.
Maintain disciple of nursing and domestic staff.
Interpretation of Hospital policies, rules and regulations.
Daily check of attendance and reporting the lapses.
Investigate complaints if any.
Work evaluation and confidential reports.
Guidance and counseling of nursing staff in the unit.
Project the annual requirements of drugs supplies and equipments for the units.
Take care of legal aspects and report about the medico legal cases in the ward.
Plan and implement a proper orientation programme for new nursing staff, student nurse and domestic staff.
Participate in In-service education of nursing personnel and attend the meetings.
Give incidental and planned teaching to nursing personnel in the unit, as well as domestic staff.
Participate in clinical teaching for student nurses in Co-operation with the nursing tutor.
Perform any other duties assigned to her for time to time.
Deputy Nursing Superintendent is responsible to the Nursing Supdt. and assist her in the administration of nursing services in the hospital.
Supervise the nursing care given to the patients in various departments by taking regolar round of her area.
Act as a liasion officer between Nursing Supdt. and the nursing staff of the hospital.
Interpret the pliicies and procedures of the Nursing service department to sub-oradinate staff and others.
Attend the emergency calls concerning nursing services or hostel problems.
Receive evening and night reports from the Assistant Nursing Supdt./Supervisors.
Keep records and reports of Nursing Services.
Maintain the records of attendance of nursing staff and leave of any kind.
Conduct regolar physical verification of hospital stocks, i.e. drugs, equipments etc.
Initiate procedure for condemnation and procurement of hospital equipment/linen etc.
Maintain the confidential report and records of nursing personnel.
Assist the nursing supdt. in making master duty roster of nursing personnel.
Assist the nursing superintendent in Recruitment of nursing staff.
Assist the nursing supdt. on planning and organising nursing services in the hospital.
Officiate in the absence of nursing supdt.
Attend the official meetings.
Keep the senior nursing Officials (CNO & NS) informed of the happenings in the wards.
Assist in planning/organising and implementing staff development programmes.
Ensure clinical experience facilities for student nurses in various clinical areas of the hospital.
Provide guidance and counseling to nursing staff.
Arrange orientation programmes for new nursing staff.
Maintain discipline among nursing personnel.
Organise educational programmes for graduate/post graduate students from different hospitals with the co-ordiantion of clinical instructor/lecturer clilege of nursing.
Escorts special visitors, Nursing Superintendent, Medical Superintendent for hospital rounds.
Arranges and participates in professional and social functions of the staff and students.
Maintains good public relations.
Any other duties assigned to her from time to time.
Nursing Superintendent is responsible to the C.N.O. for planning organisation and development of nursing services in the hospital in consultation with Medical Supdt./Chief of centres.
She/he will be responsible for efficient running of Nursing Services of the Main hospital and various centres of AIIMS.
She will assist the Director in formulating broad policies concerning Nursing Services.
She will disseminate the AIM, objectives and policies regarding patient care to all cadres of nursing services.
She will implement policies and procedures of Institute regarding nursing services.
She/he will plan future requirements of nurses and carry out recruitment of nurses from time to time.
She/he will plan and disseminate programmes for continuting education re-orientation programmes for nurses.
She/he will closely interact with other hospitals regarding improvement of patient care.
She/he will encourage research by nurses in their work areas.
She/he will guide and conunsel the sub-ordinate nursing staff.
She/he will keep herself abreast of latest happenings in nursing care by attending National / International conferences.
She will strive to implement standard nursing practices and maintain highest quality of care.
She will critically analyse the budgets for nursing services from Main hospital and various centers before being forwarded to Director.
Evaluate confidential reports of higher level nursing officers and recommend for promotion.
She will be assisted in her duties by nursing Supdt.’s, of Main Hospital and from the centres.
She will keep the Director informed about the happening concerning the hospital.
Organizational Structure
| Institute Body | |||||||||
| Governing Body | |||||||||
| Academic Committee | Standing Finance Committee | Standing Selection Committee | Estate Committee | Hospital Affairs Committee | |||||
| President AIIMS/Chairman Governing Body | |||||||||
| (Director AIIMS) | |||||||||
| Dean (Academic) | Dean (Research) | Dean (Examination) | Medical Supdt. | Chief of Centers | Head of Deptt's | Addl. Director (Admn.) | Sr. F.A. | ||
| Associate Dean (Academic) | Associate Dean (Research) | Associate Dean(Examination) | Main Hospital | Faculty Members | Dy. Secretary Chief Security Officer Dy. Director (Computer Facility) Sr. Store Officer Chief Admn. Officer Supdt. Engineer | Financial Advisor | |||
| Registrar | Admn. Officer | Asstt. Controller of Examination | |||||||
Organizational Structure
| Institute Body | |||||||||
| Governing Body | |||||||||
| Academic Committee | Standing Finance Committee | Standing Selection Committee | Estate Committee | Hospital Affairs Committee | |||||
| President AIIMS/Chairman Governing Body | |||||||||
| (Director AIIMS) | |||||||||
| Dean (Academic) | Dean (Research) | Dean (Examination) | Medical Supdt. | Chief of Centers | Head of Deptt's | Addl. Director (Admn.) | Sr. F.A. | ||
| Associate Dean (Academic) | Associate Dean (Research) | Associate Dean(Examination) | Main Hospital | Faculty Members | Dy. Secretary Chief Security Officer Dy. Director (Computer Facility) Sr. Store Officer Chief Admn. Officer Supdt. Engineer | Financial Advisor | |||
| Registrar | Admn. Officer | Asstt. Controller of Examination | |||||||
Welcome to the Computer Facility at the All India Institute of Medical Sciences (AIIMS), New Delhi. As a pioneering institution in healthcare and medical education, AIIMS is committed to leveraging cutting-edge technology to advance research, education, and patient care. Starting its humble journey in 1978 as a unit in the Department of Biophysics, it became a Specialty Centre in Jan'1989. All these years, our Computer Facility has stood as a testament to this commitment, providing state-of-the-art infrastructure and support services to meet the evolving needs of our esteemed faculty, researchers, students, and healthcare professionals.
In today's digital age, information technology plays a vital role in every aspect of healthcare, from research and education to clinical practice and administration. The Computer Facility at AIIMS New Delhi serves as the technological backbone, facilitating the seamless integration of IT solutions into various facets of our institution.
Services Offered: Our Computer Facility offers a comprehensive range of services tailored to meet the diverse needs of our stakeholders :
The Computer Facility, is dedicated to providing technological support and resources to facilitate excellence in education, research, and patient care. By harnessing the power of technology, we aim to drive innovation, foster collaboration, and empower the AIIMS community to address the most pressing challenges in healthcare.
NURSING SERVICES AT A.I.I.M.S.
A glance at Nursing Services at AIIMS, New Delhi...
Nursing services forms an integral part of any health care facility. These \services aim at high quality nursing care to the patients and community. The professional nurses work in an environment that encourages professionalism and expertise in providing holistic patient care with the members of allied disciplines in the hospital. The nurses at AIIMS conduct themselves within the boundary of ethical and legal framework.
Indeed, on any given day, nursing professionals handle a wide array of responsibilities ranging from patient care, ward management, humanre sources management, facilities management, as well as attendant’s management.
Importance of values in nursing
When working in healthcare, nurses often handle fast-paced situations that require quick decisions and specific skills, so having a value system in place is fundamental. Not only do they provide a frame work of behavior and help to influence important decision, they;
Core Values in Delivering Patient Care
ORGANIZATION OF NURSING SERVICES
Chief Nursing Officer - Nursing Superintendent - Dy. Nursing Superintendent - Asstt. Nursing Superintendent - Senior Nursing Officer - Nursing Officer
SIU Norms
One of the major challenges in nursing administration is staffing nursing units. Staffing in AIIMS, New Delhi is based on SIU Norms which are as follows :
Nursing Superintendent is responsible to the C.N.O. for planning organisation and development of nursing services in the hospital in consultation with Medical Supdt./Chief of centres.
Deputy Nursing Superintendent is responsible to the Nursing Supdt. and assist her in the administration of nursing services in the hospital.
NURSING ADMINISTRATION
EDUCATIONAL ACTIVITIES
GENERAL DUTIES
Asstt. Nursing Supdt, is responsible to Deputy Nursing Supdt. for the total nursing care of patients, management and development of the unit assigned to her :
NURSING CARE
WARD MANAGEMENT
TEACHING AND SUPERVISION
| Department | Name of the Head |
|---|---|
| Deptt. of Anaesthesiology | Dr. Lokesh Kashyap |
| Deptt. of Anatomy | Dr. A.Sharrif |
| Deptt. of Biochemistry | Dr.Kalpana Luthra |
| Deptt. of Biophysics | Dr. Punit Kaur |
| Deptt. of Biostatistics | Dr. Maroof Ahmad Khan |
| Deptt. of Biotechnology | Dr. Anushree Gupta |
| Centre for Community Med. | Dr. Kiran Goswami |
| Deptt. of Derm. & Vene. | Dr Kaushal K Verma |
| Deptt. of Endo. & Metab. | Dr. Nikhil Tandon |
| Deptt. of Emergency Medicine | Dr. Rakesh Yadav |
| Deptt. of Forensic Medicine & Toxicology. | Dr. Sudhir Kumar Gupta |
| Deptt. of Gastro. & HNU | Dr. Pramod kr. Garg |
| Deptt. of G.I. Surgery & Liver Transplantation | Dr. Sujoy Pal |
| Deptt. of Haematology | Dr.M.Mahapatra |
| Deptt. of Transplant Immunology & Immunogenetics | Dr. D.K. Mitra |
| Deptt. of Hospital Administration | Dr. Sidhartha Satpathy |
| Deptt. of Lab. Med. | Dr. Sudip Kr. Dutta |
| Deptt. of Medicine | Dr. Naveet Wig |
| Deptt. of Pulmonary Medicine & Sleep Disorders | Dr. Anant Mohan |
| Deptt. of Geriatric Medicine | Dr. Naveet Wig |
| Deptt. of Microbiology | Dr. Lalit Dhar |
| Deptt. of Nephrology | Dr. D.Bhowmik |
| Deptt. of Nuclear Magnetic Resonance | Dr. Rama Jayasunder |
| Deptt. of Nuclear Medicine | Dr. C.S. Bal |
| Deptt. of Obst. & Gynae. | Dr. Neena Malhotra |
| Deptt. of Orthopaedics | Dr. |
| Deptt. of E.N.T. | Dr. Alok Thakkar |
| Deptt. of Paediatrics | Dr. Madhulika Kabra |
| Deptt. of Paediatric Surgery | Dr.Sandeep Agarwala |
| Deptt. of Pathology | Dr. V.K.Iyer |
| Deptt. of Pharmacology | Dr. D.V.S.Arya |
| Deptt. of Physical Medicine & Rehabilitation | Dr. Sanjay Wadhwa |
| Deptt. of Physiology | Dr. K.P. Kochhar |
| Deptt. of Psychiatry | Dr. Pratap Sharan |
| Deptt. of Radiodiagnosis | Dr. Deep N.Srivastava |
| Deptt. of Reprod. Biology | Dr. A.Haldar |
| Deptt. of Surgical Disciplines | Dr. Sunil Chumber |
| Deptt. of Urology | Dr. Amlesh Seth |
| Principal, College of Nursing | Dr. Latha Venkatescan |
| Department | Name of the Head |
|---|---|
| Deptt. of Cardiology | Dr. Rajiv Narang |
| Deptt. of Cardiac Anaesthesia | Dr. Neeti Makhija |
| Deptt. of Cardiac Radiology | Dr. Sanjiv Sharma |
| Deptt. of Medical Oncology | Dr. Lalit Kumar |
| Deptt. of Surgical Oncology | Dr. S.V.S.Deo |
| Deptt. of Neurology | Dr. Manjari Tripathi |
| Deptt. of Neurosurgery | Dr. S.S.Kale |
| Deptt. of Neuro Anaesthesia | Dr. Arvind |
| Senior Financial Advisor | |
|---|---|
| Smt. Divya Yanamadala |
| Financial Advisor |
|---|
| - |
| F & CAOs |
|---|
| Shri Vijay Pal Singh |
| Shri Padam Singh |
| Ms. Rakesh Kumari |
| Accounts Officers | ||
|---|---|---|
| Sh. Trilok Chand | Sh. Prem Pal | Smt. Meenakshi Dabral |
| Sh. Prakash Kumar Giri | Sh. Bharat Bhushan | Sh. Joginder Singh |
| Sh. Anil Kumar | Shri Satish Kumar Yadav | Sh. Upendra Kumar |
| Sh. Yogesh Kumar | Sh. Shivanand Thakur | Smt. Snehlata |
| Shri Rajesh Kr. Bairwa | - | - |
| Asstt. Accounts Officers | ||
|---|---|---|
| Smt. Meena Gupta | Shri Braham Singh | Smt.. Rashu Kabtiyal |
| Smt. S. Tanveer | Smt. Sushil Kumari | Sh. Satya Dev Sharma |
| Sh. Nagender | Sh. Arvind Kumar | Ms. Veena Gaba |
| Ms. Urmila | - | - |
| Jr. Account Officers |
|---|
| Vacant |
PROTOCOL
POST-HIV EXPOSURE MANAGEMENT / PROPHYLAXIS (PEP)
Occupational exposure:
Occupational exposure refers to exposure to potential blood-borne infections (HIV, HBV and HCV) that occurs during performance of job duties.
“Exposure” which may place an HCP at risk of blood-borne infection is defined as:
What is infectious and what is not?
| TABLE 12.3.4 POTENTIALLY INFECTIOUS BODY FLUIDS | ||
Exposure to body fluids considered ‘at risk’ | Exposure to body fluids considered ‘not at risk’ | |
| Blood | Tears | Unless these secretions contain visible blood |
| Semen | Sweat | |
| Vaginal secretions | Urine and Faeces | |
| Cerebrospinal fluid | Saliva | |
| Synovial, pleural, peritoneal, pericardial fluid | ||
| Amniotic fluid | ||
| Other body fluids contaminated with visible blood | ||
Protocol:
It is necessary to determine the status of the exposure and the HIV status of the exposure source
before starting post exposure prophylaxis (PEP).
Step 1: Immediate measures
For skin — if the skin is broken after a needle-stick or sharp instrument:
· Immediately wash the wound and surrounding skin with water and soap, and rinse. Do not scrub.
· Do not use antiseptics or skin washes (bleach, chlorine, alcohol, betadine).
After a splash of blood or body fluids on unbroken skin:
· Wash the area immediately
· Do not use antiseptics
For the eye:
· Irrigate exposed eye immediately with water or normal saline. Sit in a chair, tilt head back and ask a colleague to gently pour water or normal saline over the eye.
· If wearing contact lens, leave them in place while irrigating, as they form a barrier over the eye and will help protect it. Once the eye is cleaned, remove the contact lens and clean them in the normal manner. This will make them safe to wear again
· Do not use soap or disinfectant on the eye.
For mouth:
· Spit fluid out immediately
· Rinse the mouth thoroughly, using water or saline and spit again. Repeat this process several times
· Do not use soap or disinfectant in the mouth
· Consult the designated physician of the institution for management of the exposure immediately.
Don’ts
· Do not panic
· Do not squeeze wound to bleed it
· Do not use bleach, chlorine, alcohol, betadine, iodine or any antiseptic or detergent
Step II: Prompt reporting:
a) All needle-stick/sharp injuries should be reported to the immediate supervisor, and then to the Casualty Medical Officer.
b) An entry is made in the Needle-Stick Injury Register in the Casualty.
Step III: Post exposure treatment:
The decision to start PEP is made on the basis of degree of exposure to HIV and the HIV statusof the source from where the exposure/infection has occurred. More so, it should begin as soon as possible preferably within two hours, and is notrecommended after 72 hours.
PEP is not needed for all types of exposures:The HIV seroconversion rate of 0.3% after an AEB (accidental exposure to blood) (for percutaneous exposure) is an average rate. The risk of infection transmission is proportional to the amount of HIV transmitted, which depends on the nature of exposure and the status of the source patient. A baseline rapid HIV testing of exposed and source person must be done for PEP. However, initiation of PEP should not be delayed while waiting for the results of HIV testing of the source of exposure. Informed consent should be obtained before testing of the source as per national HIV testing guidelines.
First PEP dose within 72 hours
A designated person/trained doctor must assess the risk of HIV and HBV transmission following an AEB. This evaluation must be quick so as to start treatment without any delay, ideally within two hours but certainly within 72 hours; PEP is not effective when given more than 72 hours after exposure. The first dose of PEP should be administered within the first 72 hours of exposure. If the risk is insignificant, PEP could be discontinued, if already commenced.
Step IV: Counselling for PEP
Exposed persons (clients) should receive appropriate information about what PEP is about and the risk and benefits of PEP in order to provide informed consent for taking PEP. It should be clear that PEP is not mandatory.
Step V: Psychological support
Many people feel anxious after exposure. Every exposed person needs to be informed about the risks, and the measures that can be taken. This will help to relieve part of the anxiety. Some clients may require further specialised psychological support.
Step VI: Documentation of exposure
Documentation of exposureis essential. Special leave from workshould be considered initially for a period of two weeks. Subsequently, it can be extended based on the assessment of the exposed person’s mental state, side effects and requirements.
IMPORTANT: Seek expert opinion in case of
· Delay in reporting exposure (> 72 hours).
· Unknown source
· Known or suspected pregnancy, but initiate PEP
· Breastfeeding mothers, but initiate PEP
· Source patient is on ART
· Major toxicity of PEP regimen.
Step VII: Follow-up of an exposed person
Whether or not post-exposure prophylaxis is started, a follow up is needed to monitor for possible infections and to provide psychological support.
Clinical follow-up
In the weeks following an AEB, the exposed person must be monitored for the eventual appearance of signs indicating an HIV seroconversion: acute fever, generalized lymphadenopathy, cutaneous eruption, pharyngitis, non-specific flu symptoms and ulcers of the mouth or genital area. These symptoms appear in 50%-70% of individuals with an HIV primary (acute) infection and almost always within 3 to 6 weeks after exposure. When a primary (acute) infection is suspected, referral to an ART centre or for expert opinion should be arranged rapidly.
An exposed person should be advised to use precautions (e.g., avoid blood or tissue donations, breastfeeding, unprotected sexual relations or pregnancy) to prevent secondary transmission, especially during the first 6–12 weeks following exposure. Condom use is essential.Drug adherence and side effect counselling should be provided and reinforced at every follow-up visit. Psychological support and mental health counselling is often required.
Laboratory follow-up
Exposed persons should have post-PEP HIV tests. HIV-test at 3 months and again at 6 months is recommended. If the test at 6 months is negative, no further testing is recommended.
1) TRAINING
| S. No. | Category of staff | Trained |
| 1 | Doctors | 79 |
| 2 | Nurses | 211 |
| 3 | Paramedical staff | 414 |
| 4 | Sanitation staff (SA/HA) | 56 |
| TOTAL | 760 | |
2) VACCINATION
| S.No. | Category of staff | For Hepatitis B Vaccinated( first and second dose) |
| 1 | Biotec(CMBWTF) | 21 |
| 2 | Sanitary / Hospital attendants | 324 |
| TOTAL | 345 | |
| S No | Name | Designation | Office Address | Office telephone | |
|---|---|---|---|---|---|
| 01 | Dr. S. B. Gaikwad | Professor & Head | Room no.11, 6th floor CNC Room No.15, Cath Lab Complex, CNC | Ext. 3457 Ext.4418 | sgaikwad_63@yahoo.com |
| 02 | Dr. Ajay Garg | Professor | Room No.14, Cath Lab Complex | Ext 6449 | ajaygarg@aiims.ac.in drajaygarg@gmail.com |
| 03 | Dr. Leve Joseph Devarajan S. | Additional Professor | Room No.17, Cath Lab Complex | Ext.3844 | leve_s@yahoo.com |

Dr. Shailesh B Gaikwad, MD, FNAMS, CCST
Professor & Head, Department of Neuroimaging & Interventional Neuroradiology, Neurosciences centre
All India Institute of Medical Sciences (A.I.I.M.S), New Delhi
Chairman, AIIMS Gymkhana
Email id: sgaikwad_63@yahoo.com | sbgaikwad1112@gmail.com
Contact No : 9971237573
Reviewer for following journal
Awarded WHO Fellowship in Neurointervention, 2001
Hands-on-training workshop on GDC treatment of Intracranial aneurysms, held on 1-4 June 2000, Seoul National University Hospital, Seoul, South Korea, Program proctor Prof. In Sup Choi, Chairman, Department of Interventional Neuroradiology, MGH, Boston, USA.
Hands-on-training on Carotid Angioplasty and Stenting, , Organized by Prof Kieren Murphy, Neuroradiology, John Hopkins University, Baltimore, USA, September 7-10, 2000.
Course on “International Master Degree in Neurovascular diseases”, 2001, Course director - Prof P Lausjaunias, Bicetre, France, co-organized by Paris Sud University, and Mahidol University.
Attended 12th & 13th Zurich workshop on interventional Neuroradiology, March 2004 & 2005. Course conducted by Prof. A Valavanis, Professor and Head of Neuroradiology department, Zurich University Hospital, Switzerland
Visiting Fellowship for “Advanced training in neurointerventional techniques” at Hacetteppe University Hospital, Ankara, Turkey, May 2006. Course director-Prof Saruhan Cekirge, Isiil Satchi. This centre is the primary site for hands-on-training in Onyx embolization of AVMs and advanced neurointervention procedures including FLOW DIVERTERS.
Visiting Professor-Department of Neuroradiology, South Carolina, Duke University, USA (December 2007).
Attended “3rd Anatolian International Workshop on Interventional Neuroradiology”, 8-11th May, 2008 , Istanbul, Turkey
Visiting Professor & Research Associate: BWH, Harvard Medical School, Boston, USA-31/1/2009-30th June 2009
Hands-on training on Flow diverters
Hands-on training on: Penumbra and Merci devices, n-BCA Liquid Embolic System Advanced Training Course (for AVM embolization) at the University of Massachusetts Medical School, Worcester, MA, USA. Course director-Prof. Ajay Wakhloo –June 13, 2009
Hands-on training workshop for advanced training in Perfexion Gamma knife for treatment of brain tumours and AVMs, 28th November-2nd December, 2011, at Cleveland Clinic, Ohio, USA
Awarded Fellowship by National Academy of Medical Sciences-27/10/2017
Member of expert group on “National Stroke Registry”: Expert group meeting on PBSR, HSBR, “To review PBSR & HSBR Training workshop for HSBR centers”, 12th December, 2019 NCDIR, ICMR, Bangalore, Karnataka
Expert of “Skill Development Initiative for Emerging World Countries”, Republic of Maldives, January 2020 onwards.
Attended World Live Neurovascular Conference, held on 23-24 October 2020, Live Virtual Experience.
Chief Coordinator for “Conducting Neuroradiology Workshop”, National Institute of Neurosciences & Hospital, Dhaka, Republic of Bangladesh.
Clinical Neuropsychology at the Neurosciences Centre, AIIMS in New Delhi, India, provides para-clinical services following the terminology outlined by the Sneh Bhargava Commission (2012) This specialized service encompasses a comprehensive range of neuropsychological services, including psycho-diagnostics (which involves clinical history taking, psychometric assessment, and clinical observation), remediation (involving counseling and rehabilitation), and neuropsychological disability evaluations. These services address both cognitive and non-cognitive aspects for individuals with neurological and neurosurgical conditions. Established in 1969 with the appointment of Dr. Surya Gupta, this discipline has played a significant role in advancing clinical neuropsychology in the country, aiming to deliver services in line with international standards for the benefit of patients at the Neurosciences Centre at AllMS.
Furthermore, the discipline has been enriched through clinical neuropsychological educational programs in neuropsychology for M.B.B.S., Nursing, DM (Neurology), MCh (Neurosurgery), and MD (Psychiatry) students. Presently, it also supervises research projects for postgraduate students from these departments, focusing on neuropsychological psychometric assessments. The creation of distinctive neuropsychological test batteries, such as the 'AIIMS Neuropsychological Battery,' represents a significant achievement in assessing organicity, lateralization, and lobar functions across various age groups, including Adults, Children, and the Elderly. These efforts have been supported by three research projects funded by the ICMR.
Since 2005, our research and clinical services have expanded to include the development of neuropsychological screening tools for clinicians to use in their practices, history taking forms, tests, and a variety of neuropsychological rehabilitation programs for neurological and neurosurgical conditions. Committed to enhancing patient care, we provide advanced Neuropsychological services tailored to individuals with neurological disorders. By closely collaborating with clinicians at AIIMS, New Delhi, who act as primary healthcare providers in a hospital setting, we adhere to the World Health Organization's Continuum of Care Model to address the specific needs that prompt referrals.
Sneh Bhargav Commission (2012). Work Standards for Faculty of Autonomous Institutions of Medical Education under the Department of Health and Family Welfare, Govt of India. Memo. no. V-16020/57/2008-ME-I (Pt.) pp 165-174.
| S No | Faculty Member | Designation | Email ID | Contact no |
|---|---|---|---|---|
| 01 | Dr. MC Sharma | Prof. & Head | sharmamehar@yahoo.co.in | +919717739755, 011-26549205 |
| 02 | Dr. Vaishali Suri | Professor | Surivaishali@yahoo.co.in | +919810254964, 011-26544656 |
In India, the concept of “Neuroanaesthesia as a subspeciality” of Anaesthesia was recognized, way back in 1968, when Dr. Surinder Singh Saini volunteered to anaesthetize the neurosurgical patients at All India Institute of Medical Sciences (AIIMS), New Delhi, on a regular basis. Formal training in Neuroanaesthesia, for post-graduate degree holders (MD) of Anaesthesia, for trainees from all over India, was started in 1982. In 1987, an independent Department of Neuroanaesthesia was established under the leadership of Prof. S S Saini as the Head along with two more faculties, Dr. Hari Hara Dash as Assistant Professor and Dr. Parmod Kumar Bithal as Lecturer. Five Senior Resident (SR) doctors joined them for assisting the clinical activities of the department.
In August 1989, the Department was shifted to the newly built the Cardiothoracic and Neurosciences Centre (CNC) of AIIMS (present location) along with other sister departments. Facilities during that time included three well-equipped operation theatres (OTs), one emergency (septic) OT, which was shared with the cardiothoracic centre, five-bedded intensive care unit (ICU), and twenty beds for postoperative patients.
In 1995, a process to start three years superspeciality degree course (DM) in Neuroanaesthesiology was initiated under stewardship of Prof. H. H. Dash. It was materialized in 2001, when DM (SR) posts (Six direct and three sponsored) were sanctioned by the Institute body. In 2002, two direct candidates were enrolled, for the first time in India, through a common entrance test. After the JPNA Trauma Centre was established by AIIMS, in 2006, 10 more post of non-DM SR was added to the existing 10 posts. In the subsequent year (2007), two more posts of SR (DM) were again sanctioned making the final tally of open category DM (SR) seats as eight. At present, the department is located in the Neurosciences Centre, at 6/7th floor, with the office operated from room no. 709A. One personal assistant and two office assistants look after the smooth management official activities.
Currently, the Department of Neuroanaesthesiology has expanded its horizon; caters clinical service to six well-equipped neurosurgical OTs, a brain suite (MRI- OT), two neuro-cath Labs, two MRI facilities, One GammaKnife facility, one pain clinic, a pre-anaesthetic check-up (PAC) clinic, two neurosurgical ICUs (total 26 beds), one neurology ICU of five beds, more than two OTs for trauma patients, a twenty-bedded ICU for neurotrauma patients apart from providing resuscitation measures for neurological and neurosurgical ward patients. To meet with the demand of workload, the faculty strength now has been increased to sixteen which includes two professors, four additional professors, and ten assistant professors.
This department has been actively involved with training of Indian defense service personnel and overseas trainees apart from the DM and Non-DM trainees (SRs) of Neuroanaesthesia. So far, 25 candidates have been awarded the DM degree in Neuroanaesthesiology. The department plans to start Neurocritical Care programme in coming years, and to establish this super-speciality in India, the need for which is being realized, nation-wide. The faculty and staff of this department strive hard to ensure that the ‘Department of Neuroanaesthesiology’ continues to be the torch-bearer of perioperative neurosciences, and serve as a role model in this field.
In India, the concept of “Neuroanaesthesia as a subspeciality” of Anaesthesia was recognized, way back in 1968, when Dr. Surinder Singh Saini volunteered to anaesthetize the neurosurgical patients at All India Institute of Medical Sciences (AIIMS), New Delhi, on a regular basis. Formal training in Neuroanaesthesia, for post-graduate degree holders (MD) of Anaesthesia, for trainees from all over India, was started in 1982. In 1987, an independent Department of Neuroanaesthesia was established under the leadership of Prof. S S Saini as the Head along with two more faculties, Dr. Hari Hara Dash as Assistant Professor and Dr. Parmod Kumar Bithal as Lecturer. Five Senior Resident (SR) doctors joined them for assisting the clinical activities of the department.
In August 1989, the Department was shifted to the newly built the Cardiothoracic and Neurosciences Centre (CNC) of AIIMS (present location) along with other sister departments. Facilities during that time included three well-equipped operation theatres (OTs), one emergency (septic) OT, which was shared with the cardiothoracic centre, five-bedded intensive care unit (ICU), and twenty beds for postoperative patients.
In 1995, a process to start three years superspeciality degree course (DM) in Neuroanaesthesiology was initiated under stewardship of Prof. H. H. Dash. It was materialized in 2001, when DM (SR) posts (Six direct and three sponsored) were sanctioned by the Institute body. In 2002, two direct candidates were enrolled, for the first time in India, through a common entrance test. After the JPNA Trauma Centre was established by AIIMS, in 2006, 10 more post of non-DM SR was added to the existing 10 posts. In the subsequent year (2007), two more posts of SR (DM) were again sanctioned making the final tally of open category DM (SR) seats as eight. At present, the department is located in the Neurosciences Centre, at 6/7th floor, with the office operated from room no. 709A. One personal assistant and two office assistants look after the smooth management official activities.
Currently, the Department of Neuroanaesthesiology has expanded its horizon; caters clinical service to six well-equipped neurosurgical OTs, a brain suite (MRI- OT), two neuro-cath Labs, two MRI facilities, One GammaKnife facility, one pain clinic, a pre-anaesthetic check-up (PAC) clinic, two neurosurgical ICUs (total 26 beds), one neurology ICU of five beds, more than two OTs for trauma patients, a twenty-bedded ICU for neurotrauma patients apart from providing resuscitation measures for neurological and neurosurgical ward patients. To meet with the demand of workload, the faculty strength now has been increased to sixteen which includes two professors, four additional professors, and ten assistant professors.
This department has been actively involved with training of Indian defense service personnel and overseas trainees apart from the DM and Non-DM trainees (SRs) of Neuroanaesthesia. So far, 25 candidates have been awarded the DM degree in Neuroanaesthesiology. The department plans to start Neurocritical Care programme in coming years, and to establish this super-speciality in India, the need for which is being realized, nation-wide. The faculty and staff of this department strive hard to ensure that the ‘Department of Neuroanaesthesiology’ continues to be the torch-bearer of perioperative neurosciences, and serve as a role model in this field.

“It was May 1965 that I came to Delhi from Vellore where I was a lecturer, to appear for a Union Public Service Commission interview for the job of Reader at G. B. Pant hospital, Delhi and All India Institute of Mental Health, Bangalore (later to become NIMHANS). I was the only candidate and was asked at the end as to which place would I prefer. I chose Bangalore. Just before leaving for the interview, I had gone to see Dr. Baldev Singh and Dr P. N. Tandon (PNT) at AIIMS to pay a courtesy call. They were sharing an office and I suspect eagerly waiting like spiders, to catch a victim in neurosurgery, who could stick on at AIIMS, which at that time had actually nothing no space, equipment or staff. After a little talking about general things, suddenly, Dr. Baldev Singh asked me to think whether I at all wanted to go for the interview, as AIIMS could possibly offer me a job, I of course declined the proposal as a bird in hand was better than two in the bush. Then Dr. Tandon asked me to come home for tea that evening. I left for the Union Public Service Commission office. Today when I see large number of candidates for a job interview my own experience seems miraculous.
Coming back after the interview I recounted what happened to Gopal and his wife Radha (Dr. G.K. Vishwakarma was then Asst. Professor Orthopaedics and later became D.G.H.S. of Government of India) Insidious pressure started from them to come to AIIMS and forget about Bangalore. Incidentally Bangalore had a working, full fledged department with Prof. RM. Verma and he tried hard to get me there even after I joined AIIMS.
That evening I spent at Tandons. Dr. P. N. Tandon had been my Anatomy demonstrator in 1952 while Mrs. Leela Tandon was my lecturer in Obstetrics and Gynaecology at Medical College, Lucknow. I had met Dr. P.N. Tandon in 1963 at the annual Neurological Society of India meeting in Calcutta. For both of us it was the very first meeting that we had attended of NSI. Dr. P. N. Tandon had established the department of neurosurgery at AlIMS 2 months before in March 65. He had been promised equipment but nothing had arrived in the two months. He was eager that I should join but was frank to say he did not know how things would eventually develop. After returning to Gopal's house, Radha and Gopal took me to see 'My Fair Lady' at Sheila Theatre which then was the best in Delhi, if not India. After returning well past midnight we slept on the roof and went on talking about what I should do. I think it was near the break of dawn that I finally succumbed to pressures from Gopal and Radha and said OK I'll come to Delhi if the job was offered. Next morning before I left Delhi Dr. Baldev Singh took me to meet Prof. K. L. Wig then Director AIIMS. Our liking for each other was instantaneous and the bond carried throughout.
I joined as adhoc Assistant Professor in June'65. There was one office of Dr. Baldev Singh in which in addition to Dr. P. N. Tandon another chair and a small table was put for me. The process of starting a department began really from scratch. Space was allotted on the first floor by the side of anatomy lecture theatre. I and Dr. V. Virmani (my opposite number in Neurology) sat down to draw maps and carve out rooms in the large halls. At that moment, our vibes were bristly to say the least. Dr. Virmani was considerably senior in age plus she had known Dr. Baldev Singh since Amritsar days and she also held the trump card of being Punjabi speaking which was then the lingua franca of AIIMS. Over the years our relationship mellowed and we did develop mutual admiration and respect for each other. I hit upon the strategy in our dealings at that time of building the departments, of saying exactly opposite of what I wanted. Dr. Virmani would of course, reverse my suggestions much to my advantage. Today when I look back it all appears so childish. But then it was great fun. Slowly collecting items like pins, chairs, tables, almirahs and make real offices was a new challenge for which I was not trained. Anyway we built the office cubicles, laboratories and got the OPD on the 4th floor in ship shape. It was so gratifying after two years of joining that we had a place of our own.
We started with surgical instruments which actually were of World War II vintage which included an operation table. Burr holes had to be made by a brace in 4 stages and both Dr. Tandon and I developed the art to perfection. To begin with we had no beds. Both for Neurology and Neurosurgery, Prof. K.L. Wig and the Pediatricians generously allowed us use of their beds in what is now the nurses hostel. There was so little clinical work that it was terribly frustrating in the beginning. I started taking clinics for the MD students of medicine, pediatrics and radiology. I slowly became quite popular to the extent that one day Dr. Wig called me to see one of his patients in his office. I must have impressed him no end as after that on several occasions he would ask for my opinion on patients. This was a small matter for him but a great boost for my confidence for which my gratitude goes to him.
By 1968 we were having a ward in the OPD block (ward IX) and we were well settled. The operation theaters were in the College of Nursing Block. Radiology to begin with was in the nurses hostel, and only in 1968 shifted to its present location. That was the time when we had Dr. S. K. Ghosh in radiology from 1965 to 1968 and he was a great help. Very often we started the day at 7.30 A.M. with ward rounds, dressings and stitch removals, followed by neuroradiology (ventriculograms angiograms etc) and then this was followed by surgery which would invariably end by 7 or 8 P.M., particularly if it was a posterior fossa tumour. At night one of us i.e. PNT or myself would sleep in the doctors room adjacent to the main O.T. block. From 1966 onwards Dr. B.B. Sawhney and Dr. M. Gourie Devi, now Director and Vice Chancellor NIMHANS who were residents in neurology would help us out by doing night duties and also assist in surgery as we did not have regular residents of our own. The role played by Col. G.C. Tandon, the Professor of Anaesthesia, was unforgettable. Dr. Hattangdi's lectures in anaesthesia helped us enormously and he also shared our burden in looking after patients, sometimes relieving us of our daily chores. The two films I saw with Anjali, my wife, during the time was courtesy of Hattangadi. Before I proceed I must tell of my first day in the operation theatre block (MOT) in the consultants changing room, where I went on my own apprehensively, to discover its ambience. The only person there in OT dress was reading an Agatha Christie paperback with great seriousness. On entering he asked me as to who I was and then got up with great cordiality and shook me by the hands. That was Dr. Satish Nayyar, Assistant Professor in Surgery well known as he was a Hallet medalist in the primary FRCS examination. Dr. Satish Nayyar gave me a cup of tea and then said that I must cultivate some hobby (his was reading mystery novels) as Assistant Professors had nothing to do as the Professor usurped all the work which was worthwhile, while all the minor work was done by the Registrars (later called residents). I went into depression from which it took me a long time to come out. Within a week I took courage in my hands and went to talk it over with PNT. We decided that alternate cases would be operated by us while the other would assist. Matters went on well but I was perturbed over the fact that if he assisted, he would go out and talk to the patients attendants before I could come out. Again I went to him in 1968 and PNT graciously agreed he wouldn't do so. This was a remarkable thing at AIIMS. My struggle for identity of Assistant Professors went on to the faculty over such oligarchy and it was ultimately in 1970 that I was able to change the nomenclature of hospital units which hitherto were identified with the head, to that of the departments. Thus Prof. P.N.T's unit changed to Neurosurgery unit-a practice which continues today. I have always felt that to obtain the best from colleagues a measure of democracy and participation should be the prime substance PNT's contribution towards this was immense which allowed me to put my heart and soul in developing the department and later the Neurosciences Centre. I guess the role of wives is also very great. Our families (Tandon and Banerji) were close to each other and even today no major decision in the Banerji family takes place without Tandons consultation. I guess this meeting was lucky for both of us.
In 1969 Dr. S.K. Ghosh left for Goa on promotion as Professor and Neuroradiology was taken over by Dr. R.K. Goulatia for whom a separate post was created in neuroradiology. In mid 70's Dr. S.S. Saini was persuaded to join Neuroanaesthesia and this started the nucleus of a comprehensive clinical setup. Fortunately we were able to persuade (Mrs. D. Saini to join as our OT sister incharge and thus there was a feeling of family and belonging, so important in the development phases of any new venture. Dr. Subimal Roy was spending considerable time in Neuropathology to complete the picture. I had a vision of Neurosciences Centre akin to PNT, however I knew that basic neurosciences can never develop on its own because of economic compulsions. My emphasis was on developing clinical neurosciences and bring in basic neurosciences within its umbrella.
By mid 70's both neurosurgery and neurology had relocated itself on the main hospitals 4th floor and we were lucky to have separate independent wards. Mrs. M. Bindra joined us as sister I/C of neurosurgery ward and her dedication eventually made our ward the talking point of nursing care in the Institute. She eventually rose to become the Nursing Superintendent of the Neurosciences Centre.
In 1966 one day, walked into my office Dr. Brahm Prakash, who had resigned his Short Service Commission in the army and had married recently. He was at loose ends, asking my advise as to what he should do. He had earlier worked as my junior resident in general surgery at Medical College, Lucknow and the association was about 10 yrs. old. I persuaded him to join neurosurgery. We were able to rustle up the required formalities for starting MCh course with bare facilities but boundless enthusiasm. He was the first trainee and later joined our faculty and went on to become the Director Professor at G.B. Pant Hospital and started his own MCh programme. The AlIMS MCh course went from strength to strength and eventually we were having both the 5 yr and 3 yr streams. Neurology D.M. had started already in 1965. Now AlIMS trainees are spread all over India. Several headed departments e.g? Dr. Gourie Devi became Director Vice Chancellor of NIMHANS, Dr. B. Prakash at G.B. Pant Hospital Delhi, Dr. B.S. Das at NIMHANS, Dr. S. Mohanty at IMS, BHU Varanasi, Dr. A. K. Reddy at NIMS Hyderabad, and Dr. M.A. Wani at SKIMS Srinagar. Many hold important positions in teaching as well as private sector. We i.e. PNT and I are inordinately proud of all who trained themselves with us and wish them all the best in their future endeavors. Our wish is that they better us in their achievements. A major breakthrough in our clinical services occurred in 1976 with the coming of Prof. H.W. Pia who did a course in laboratory microsurgery. In the next few years we started a microsurgery laboratory and operative microsurgery was initiated. In the Indian scenario we stole the lead. In late 60's with the help of our ENT surgeon Dr. S.K. Kacker we started trans-sphenoidal pituitary surgery which consolidated in the 70's and became a routine procedure.
The process of development of the Neurosciences Centre in collaboration with the Cardiothoracic Sciences Centre started in real earnest in early 70's. Dr. N. Gopinath of Cardiothoracic Surgery and PNT were the architects. Land allocation was done by Prof. V. Ramalingaswami, the then Director AIIMS. Ghosh and Pradhan Associates were appointed architects and their started the planning for the basement, ground floor and the operation theatre block of our centre. Hours and hours of meetings with the architects-designing and tearing plans, it went on and on. I heard my wife say that I started talking of planning even in my sleep. We were about ready to have the foundation stone laying. This was 1977 and Mrs. Indira Gandhi's infamous emergency was coming to an end. One afternoon, in PNT's office, Dr. N. Gopinath suddenly said it would be nice to have Mrs. Gandhi lay the foundation stone. I had recently treated Mr. Dhawan's (then the personal secretary to Mrs. Indira Gandhi) nephew and I said shall I try. I rang him up on the phone from PNTs office. Mr. Dhawan immediately said yes and wanted probable days and times so that it could be confirmed taking into account Mrs. Gandhi's tour programmes. Elections were round the corner and Dr. Ramalingaswami wisely asked us to go slow. Mrs. Gandhi lost the elections and it is possible that the Janata Government which followed may have taken offence and delayed the start of the Centre had we got Mrs.lndira Gandhi to lay our foundation stone. Eventually, President Mr.Neelam Sanjeeva Reddy lay the foundation stone in 1978. When the building started many problems surfaced e.g. we suddenly discovered that there were very few toilets while most of the patients of cardiology were on diuretics and required use of toilets frequently. Again to the drawing boardbreaking of walls, laying of new sewer lines and so new toilets came into being. I know the OPD and of course the toilets have today become too inadequate with increasing number of patients coming to the Centre.
The brief period of Janata regime from 1977 and 1979 saw the irrepressible Mr. Raj Narain come as the Health Minister. All work in the Ministry came to a halt as also our Centre which bore the backlash of erratic ways of Mr. Raj Narain. The only thing I remember was meeting him near the present Community Medicine Department late in the evening, Mr. Raj Narain was coming to inaugurate, if I remember correctly, the Centre of Community Medicine. As usual he was hours late and the then Director Dr. L.P. Agarwal was standing with 3to4 faculty members. I tried slinking away but Dr. L.P. Agarwal called me and more or less forced me to stay on awaiting Mr. Raj Narain. He eventually came when the numbers of people waiting was not more than half a dozen. Before going to cut the ribbon he was introduced to all of us. He was highly intrigued with me and asked what would I find if I did have an opportunity to see the inside of the head of Mrs. Indira Gandhi. I made some polite comments though I was sure Mrs. Gandhi had a better quality brain than Mr. Raj Narain. Anyway he went on to narrate it with great gusto during a special convocation to award an Honorary D. Litt to Dr. Sewoosagar Ramgoolam of Mauritius. It was in such bad taste that Morarji Desai who was chairing frowned and all of us in the auditorium hung our head with embarrassment.
My two stints as Chief of Neurosciences Centre were significant in the development of the Centre. The first was a 2 year term as acting Chief of Centre while Dr. PNT was on Nehru Fellowship between 1984-86. This was the time when after the first phase of building (OPD, radiology wing, basement and OT block) we had reached a dead end as far as expansion of the Centre was concerned. Prof. M. L. Bhatia was the Chief of Cardiothoracie Sciences Centre. Our formal requests for funds were stiffly rebuffed by the then Joint Secretary Finance Adviser (JSFA) of Health Ministry. Ms. Sarla Grewal, widely nick named 'hunterwali' by her unkind colleagues, was the Secretary. We were advised not to try and influence her which could cause an unpredictable antagonism to our proposal. Anyway we went to meet her, placed before her, the developments till date, including our mounting clinical load, increasing public expectations, and the blockades experienced by us for expanding our Centres to what was originally planned. Ms. Grewal quietly listened to us, occasionally interjecting for a clarification. After we completed she asked for the JSFA who was the main stumbling block, to come and join the meeting. The moment he saw us his hackles were raised. On being asked by Ms.Grewal as to what were the problems in giving us the grant he started off with a long list of financial mismanagement by AlIMS in which our Centres had no role to play. (Most of the problems recounted were exaggerated to say the least). Ms. Grewal asked as to why our Centres were being penalised for what AlIMS had done. To this the JSFA said that this is a part of financial management for which he was responsible. Then we saw the legendary Ms. Sarla Grewal come into her elements. In chaste Punjabi she asked the JSFA as to who was the Secretary of the Ministry and how dare he speak to her like that. The poor JSFA spluttered and stuttered and tried to put in a word edgeways. Ms. Grewal asked him to leave the office and we knew that our battle was half won. However after leaving her office both Prof. M.L. Bhatia and I, as a matter of diplomacy, went to the JSFA's office. He was in the dumps. We nursed his hurt ego by asking for his help as we knew that he was quite capable of going to the Finance (Expenditure) Secretary and derail our proposals. I think the strategy worked as he did become a supporter. Of course things were helped as a few close relations of the JSFA fell conveniently ill at the same time requiring cardiac and neurosurgery. Funds eventually came though it took another year and in 1986 the remainder of the present Centre's building was started. Prof. P. Venugopal was a constant source of support in our endeavours. In the same period the next Union Health Secretary was Mr. Srinivasan, who was unenthusiastic about our Centres. His general impression was that we were overstaffed, our equipment underutilized and our clinical output low compared to other hospitals e.g. G. B. Pant Hospital Delhi, Christian Medical College Vellore, and certainly Apollo Hospital Madras which to him was the ultimate in financial management and output. Incidentally he was involved with the starting of Escorts Heart Institute which he clearly told us is a 'better bet than us'. Prof. Bhatia, Venugopal and I went through our records as well as what we could gather from the other institutions which Mr. Srinivasan thought had better quality and quantity of work. He had a meeting separately with our Neurosciences group to take stock. I had taken Dr. Baldev Singh and Dr. P.N. Tandon for the presentation made by me. By the end Mr. Srinivasan was convinced of the genuineness of our proposals. My plea at that time was to get financial grant equal to G.B. Pant Hospital whose output was half of ours. It was a landmark victory as our grants immediately increased, a trend which continued in the future.
My next stint as Chief of Centre was between 1988-95. Finances were forthcoming in good measure We had a CT scan and state of art angiography equipment. Our ICU was the best in the country. What we lacked was a MRI Scanner. I must pay special thanks to Mr. R.L. Mishra who was the Union Health Secretary in the latter part of my assignment. We had an excellent relationship and he was always positive in his approach. It is through his help that we got the NMR department setup at AIIMS, which was far more than merely obtaining MRI equipment. Incidentally even today the NMR Department has the only 2 Tesla machine capable of MR Scan and also MR Spectroscopy. The NMR department also has chemical NMR and the only experimental NMR in India today. It was an unique experience to create a whole department with the help of the then director Dr. S. K. Kacker who was always supportive.
It is during my tenure that proposals were sent to the Government for making the Centre the best equipped not only in India but in the Asian region. The Gamma Knife has started after I retired and I am sure PET scan and other newer equipment would come in due course.
I am often asked as to whether I have any regrets. My special regret is our offices being removed from the main Institute. It was originally envisaged that offices would remain where they were located i.e., adjacent to Anatomy dissection hall. The translocation has severed the umbilical cord to the other specialties in the Institute. This isolation does not augur well for the future of our Centre, as any branch of medicine to flourish requires interaction with sister disciplines. My other regret is the inability to have nonclinical neurosciences to come and establish themselves in our Centers new building. I had tried, even to the extent of keeping a floor vacant for one year under various pretexts.
My greatest gains were the colleagues I had - friends for life. I know I left alive vibrant active Centre which will only grow from strength to strength. Even today for anything I always say Neurosciences Centre, AIIMS is the best and with every breath only wish it the very best in its future endeavors.”
(Content provider: Dr. Achal K Srivastava)
Neurology is one of the earliest super – specialty at the Institute. Dr. James Austin, a Neurologist from Oregon, USA started a nucleus of Neurology service in the department of Medicine in 1962-63. In 1965, Dr Sushila Nayar, then Union health minister, invited Prof. Baldev Singh (one of the founder members of NSI, Neurological Society of India) to start a department of Neurology at AIIMS. When Prof Baldev Singh (also called ‘father of neurology’ in India and lovingly called "Papa Neuron") moved to neurophysiology on his retirement, the department was headed by Dr S N Pathak and then by Dr Vimla Virmani in 1975. After Prof. Vimla Virmani, Prof. M C Maheshwari took charge of the department in 1978. The department was shifted to the Cardiothoracic and Neurosciences Centre in the year 1985. In the year 2001, Prof. M.Behari took over the mantle of leadership. She retired in June 2016. Prof Kameshwar Prasad became the head of the department in October 2013. He retired on 31st January 2019. Prof. MV Padma Srivastava took over the leadership on 1st February 2019. From its inception, the emphasis of the department has been on quality patient care, research and to achieve academic excellence. Though the department started with 25 in patient beds, now there are 75 beds including neurointensive care. Out patient services and inpatient care has been incessantly on the rise over the years. The department has tried to maintain impeccable record of comprehensive patient care, teaching and training of students as well as contribute significantly to the scientific literature in terms of research. The department actively pursues clinical care and research activities in the sub-specialities of Movement Disorders, Neuroinfections and immunology, Stroke, Intractable epilepsy, Neuro-muscular Disorders, Sleep, Headache, Dementia amongst others. The department is equipped with the latest modalities for the diagnosis and management of various neurological disorders. The department has been in the forefront of medical research since its formation and is renowned internationally for quality clinical and basic research, particularly in the field of stem cells, Parkinson’s disease, stroke, epilepsy, neuromuscular disorders, sleep and headache. Regular patient information programs and scientific deliberations are conducted by the department. The faculty of the department routinely participates in the public awareness programs on television, and radio etc. and are active in various national and international CME programs.
“The Departments of Neurology and Neurosurgery at the All India Institute of Medical Sciences were initiated in March 1965 with the appointment of Prof. Baldev Singh and myself as the first Professors. A neurology service in the Department of Medicine started by Dr. Jim Austin from the USA and later under care of Dr. Vimla Virmani was already in existence at that time. Significantly enough the Institute was, from its very inception, an important centre of neuroscience research. The first two Professors in Department of Physiology (Prof. B.K. Anand and Prof. A.S. Paintal) were undisputable leaders of neurophysiology in the country. Dr. Paintal had, however, already moved to Patel Chest Institute a year earlier, the remaining faculty members of the department were all pursuing neurophysiology research. Prof. Keswani, the Chief of Anatomy, was primarily interested in neuroanatomy. Prof. G. P. Talwar, at that stage, was enthusiastically involved in researches in neurochemistry This was of course before his shift to immunology. Acknowledging these strengths International Brain Research Organization (IBRO) had already held one of its earlier workshops in the Institute. Dr. Sriramachari, Deputy Director of Indian Council of Medical Research, though not on the faculty of the Institute freely provided his services for all neuropathological work till several years later when Dr. Subimal Roy took over the responsibility fully. While clinical neurology and neurosurgery departments existed at several centers in the country much earlier; even the oldest such centers at Vellore, Madras, Bombay and Calcutta, did not have such broad base of neuroscience as we were fortunate to have at the Institute. Given the overall milieu of rapid growth and development in the institute at that time, the clinical departments also expanded rapidly. It will be hard for the current staff and students of the Institute to visualize how close interaction existed among all these departments and units in the earlier years. This was in no small measure due to the all pervading influence of Prof. Baldev Singh real father figure for all of us.
The idea of establishing a "Brain Research Centre" at the Institute had already been envisaged by Prof. B.K. Anand even before the clinical departments came into existence. No doubt this was primarily thought of as a basic research centre. Thus on 1st December 1964, Dr. Anand vide his letter No. Phy/64/1235 requested the Director for initiating steps for developing a Brain Research Centre" with the existing ICMR Neurophysiology unit as its nucleus. Unfortunately no action was taken on his request.
In 1968, when the Institute was to formulate its development plans for the Fourth Five Year plan of the Government, Prof. Anand, Prof. Baldev Singh and I had several informal discussions to once again revive the proposal for a Brain Research Centre. It may be mentioned that, not surprisingly, this proposal was heavily loaded in favour of creating research laboratories including a couple for neurology and neurosurgery. While we were heavily constrained in our clinical work due to limited diagnostic and operative facilities at this time we went along with Prof. Anand in supporting this proposal hoping to strengthen the patient care services through the development plan for the Institute hospital which was to be commissioned
The Development Committee approved the proposal in principle, but owing to financial constraints no concrete steps were taken. The Institute Body ultimately agreed to create a few staff positions so that "Centre can make a start as early as the Financial Year 1970/71. In practical terms it amounted to absorbing some of the staff of the Indian Council of Medical Research Neurophysiology Unit and nothing more.
When we finally shifted to the new hospital the Neurosurgery Department had 22 beds allotted to it. We had one operation theatre, but no specialized neurosurgical operation table and no intensive care unit. The neuroradiology set up consisted of a skull table without automatic changer for angiography, no facilities for tomography nor a dedicated unit for myelography. Isotope encephalometry then a routine diagnostic investigation abroad was nonexistent. We had an EEG machine but no facilities for EMG or nerve conduction. Nonetheless we were facing increasing demands for patient care from all over the country and also our neighboring countries. Waiting lists for admission and surgery were a constant source of worry for us and frustration for the suffering patients. We had already started the M. Ch. course.
Similar problems were being faced by the Cardiology and Cardiothoracic Surgery Departments. One day in 1971 when Prof. Gopinath and I were scrubbing for surgery in the common scrub room between our two theatres, he informed me that they have submitted a proposal for a Cardiothoracic Centre "Why don't you also do so, otherwise we will never progress". I, therefore, once again took up this matter with Prof. Anand who was now also the Dean and sounded the Director, Prof. V. Ramalingaswami. On receiving a favorable response, it was decided that, unlike in the past, our proposal this time should be a comprehensive one, including parallel development of basic neurosciences and clinical disciplines. Dr. Manchanda along with Prof. Anand formulated the proposal in respect to basic neurosciences. I, in consultation with Prof. Sumedha Pathak, the then Professor and Head of Department of Neurology and on the advice of Prof. Baldev Singh and Dr. Banerji prepared the plan for the clinical centre. A draft proposal was thus submitted on 16`" July 1971 to the Dean with the comments "in view of the present extent of development at the Institute to start with emphasis will be on neurophysiology, neurology and neurosurgery. Nucleus for the following will be established with a view to development of these into fully fledged specialties, as integral part of the centre, as personnel and fiscal resources were available". These included neuroanatomy, neurochemistry, neuropathology. This proposal was discussed by Prof. Baldev Singh (who was now an Emeritus Professor) with Prof. B.K. Anand who agreed with it fully and desired to "go ahead and fill up all the details regarding space, equipment, personnel etc. working out the cost" etc. We agreed to change the name from Brain Research Centre to Neurosciences Centre. We had a detailed and somewhat ambitious plan formulated. Though the plans were ready there was no obvious source for funding it. Was it going to be another document for the archives? This thought remained a constant worry, Prof. Ramalingaswami was fully in agreement but was finding it difficult to find funds for it.
Several months passed. One day while casually discussing our mounting frustrations with lack of any progress with my elder brother, who was then a Jt. Secretary in the Prime Minister's office, I initially got a cautious reply, "Prakash, officially I do not wish to get involved in any thing that may be considered as a favour to my brother. The only thing I can do is to arrange a meeting for you with the PS to the Hon'ble Minister of Health Shri Uma Shanker Dixit. Even before that, first take the permission from your Director to do so". It was easy to obtain Director's permission and shortly afterwards a meeting was held with Shri Rajgopal, who was more than sympathetic to our request for establishing the Neurosciences Centre. At the end of the meeting he told me that it was not possible to get such a major scheme funded in the middle of a plan period but "may be we could get advanced action initiated which can then be formalized in the next plan". He promised to discuss this with Dixitji at an appropriate time. The meeting ended with encouraging but cautious note, "I promise nothing but I am convinced it is a genuine need. You are asking nothing for yourself? you are willing to provide more and better service to those knocking at your door".
Not expecting any prompt action I was pleasantly surprised to receive a call from the Director later that evening, "Health Secretary Shri K.K. Dass wants us to include the matter related to the establishment of the Neurosciences Centre in the agenda for the next meeting of the Institute Body due shortly. He wants a copy of the proposal sent to him in advance". On 2nd August 1972, a copy of the formal proposal was duly sent to the Shri K.K. Dass by the Director. At the Institute Body meeting held on 12'" September 1972, the Institute decided, "The Institute considered that it was fortunate that expertise in several fields of Neurosciences exists at the institute both in basic and clinical areas. The Institute considered the scheme put up for its consideration as possible, desirable and in the larger interests of the country. Recognizing the strengths already built in the various departments in respect of the neurosciences, the Institute approved the proposal in principle to set up a Centre for Neurological Sciences at the AIIMS and decided that not only it be included in the proposals for the Fifth Five year Plan of the AIIMS but, the possibility of advance action in the Fourth Five Year Plan itself, should also be seriously explored. It was accordingly decided that the matter be considered by the Finance Committee in greater detail". We felt happy but not jubilant, fully conscious of the harder battles ahead
The Proposal was duly put up to the Finance Committee meetings held on 4th January 1973, 8th February 1973 and 5th April 1973 and as feared owing to "financial constraints" no funds could be made available. The real reason was no doubt that Shri K.K. Dass had retired by now and his successor Shri Ramachandran had his own antipathies against the Institute as future events confirmed.
However, without waiting for a formal decision of the Finance Committee, Prof. Ramalingaswami forwarded the proposal to Dr. Banwari Lall, Chief, Health Division, Planning Commission for his consideration. Dr. Lail was a close friend of Prof. Anand who arranged a meeting with him in the Planning Commission after Dr. Lall had opportunity to scrutinize the proposal. With high hopes Prof. Anand and I attended the meeting. To our surprise Dr. Lall, after a brief discussion, said, "Bal (B.K. Anand), I am sorry this proposal as it stands is unlikely to be approved owing to severe financial constraints. The only component that may be favorably looked at is the patient care part". He also made several suggestions for curtailing the budgetary demands even for the clinical component. It was with a sense of disappointment that we walked out of his office. I was, in addition assailed with the fear of losing Prof. Anand's interest and support for the project. Probably sensing my thoughts, on our way to the exit he suddenly stopped said, "Prakash, it is too bad to have things take a turn this way, but let us be practical. We should take whatever we can get and keep trying for the rest. You will have my full support". Few in his place could have been so generous and even more so the enthusiastic support we continued to get from him later on provided enough proof of the genuineness of these sentiments. For all this he no doubt, got the flak of his colleagues in the Physiology Department.
In pursuance of the decision of the Institute Body and the informal advice received from Dr. Lall we carried out another detailed exercise to draft a formal EFC (Expenditure Finance Committee) memo. In the meanwhile Prof. Gopinath had carried out a similar exercise for the Cardio-thoracic Centre. As a matter of fact, these exercises were mostly done with the constant consultations with each other. Combined these two proposals required considerable financial support. Dr. Ramalingaswami advised us that we should seek the views of the new Health Minister Shri Khadilkar. After a patient hearing of our individual proposals, he pointed out the difficult financial situation and advised that we should try and economize by establishing some common facilities and sharing whatever can be shared thus bringing down the total cost of two proposals. He promised to get the demands included in the Fifth Five Year Plan proposals of the Institute. Thus Prof. Gopinath and I carried out another exercise maintaining the basic character of two independent centers, yet having some common areas and support laboratories. On 2nd August 1973, a new draft proposal was forwarded to the Director with a note, "In view of the difficult economics situation, we (Profs. Anand, Gopinath and Tandon) have also reviewed the projects with an idea to prune these without undue detriment to the utility of the projects". And further, "Following this review, if we could get a total of Rs. 350 lakhs (Rs. 200 lakhs for Cardiothoracic and Rs. 150 lacs for Neurosciences Centre), we could still make a worthwhile contribution".
The Planning Commission, discussed the proposals of the Health Ministry (which included those of AIIMS) on 31st August 1973. The bias of the Health Secretary, Shri Ramachandran against the institute was too obvious. He had proposed a total of Rs. 150 lakhs for the whole Institute. As a matter of fact it was specially emphasized that the Ministry "did not favor that all the specialties should be concentrated in one place in the country". Following strong pleadings by the Director, one of the members of the Planning Commission, Member (M), pointed out that "the Ministry had proposed Rs. 1.50 crores for the AlIMS as against the Fourth Plan provision of Rs. 3.33 crores, and since this was a premier Institute in the country, the Ministry may explore the possibility of providing some additional funds for the Fifth Five Year Plan. With regards to the proposals for the two centers, the Planning Commission ultimately decided to allocate separate funds for "the development of super-specialties: a total of 236 lakhs, without specifically mentioning our proposals. This was a typical bureaucratic stroke by the Health Secretary to scuttle our proposal. Before implementing the program, the Ministry of Health decided to enquire from all medical institutions in the country to submit their proposals for "development of super-specialties", notwithstanding the fact that the Central Government is supposed to directly fund only the national institutes. As expected proposals were received from several places and interestingly even Orthopaedics was considered a super-specialty. The Health Ministry, obviously under the instructions from its Secretary put the whole matter in the cold storage with the usual excuse, "the matter is under consideration": even though the Fifth Plan had already begun from April 1974.
One day Dr. Karan Singh, who was now the Minister of Health, desired to see me for some unconnected reason. At the end of our meeting, I enquired about our proposals for the centers. Only then the cat came out of the bag. He frankly informed me that the Secretary was sitting on the file on the excuse of collecting information mentioned above. Dr. Karan Singh recognized the futility of the exercise. Since in the limited funds allocated for super specialities it would be impossible to meet the needs of even a few. He promptly took the initiative and in August 1974 appointed a committee under the Chairmanship of Dr. Srivastava, the Director General Health Services, to assess the existing potentials and future possibilities of strengthening superspecialities in the centrally funded institutions only. The Committee included experts in the concerned disciplines from all over the country. It collected the necessary information from various institutions and finally paid site-visits to each of these before recommending our two proposals alongwith some allocations to a couple of others. Thus from a total of Rs. 236 lacs allocation for super specialities the two Centres at the AIIMS, was provided Rs. 188.37 lacs.
On March 26, 1975, even before we received a formal approval of the Government to establish the Centre, a letter addressed to the Director, AlIMS received from Dr. Sharad Kumar, DDG(M), indicating that, "Under the Purely Central Scheme of "Development of Superspecialities', the Government of India has sanctioned a provision of Rs. 10 lakhs for the development of the Departments of (1) Neurosurgery and Neurology; and (2) Cardiology and Cardiothoracic Surgery...............”
This communication, though not mentioning anything about the Centers, was the first indication that the Government had selected AIIMS; for development of these super-specialties. Two weeks later on 11th April 1975, the recommendations of the "Expert Committee on Establishment of Cardiothoracic and Neurosciences Centre at the Institute", were ultimately received, setting at rest all uncertainties about the two proposals. It would be worth reproducing the extracts of this communication with respect to Neurosciences Centre (see Dr. Sharad Kumar's letter dated 11th April 1975). Shortly afterwards on 22"d July 1975 a formal letter from the Ministry of Health and F.W. No. V. 16020/54/ME (PG), communicated to the Institute an allocation of Rs. 188.37 lacs for the super-specialties (including both centers) for the 5th Five Year Plan. It needs to be recorded that the fullest understanding between Prof. Gopinath and myself and the cooperation of the rest of the faculty of the concerned departments made it possible for us to keep on revising and redrafting the proposals as per the bureaucratic needs of the Government, without sacrificing the basic objectives. No hidden rivalries, personal egos or unjustified interests of individuals ever cast any shadow as we pursued the planning and implementation of the projects through various administrative channels. For me it was a rare experience of trust and camaraderie not so common in our institutions.
As expected it was not smooth sailing from now onwards. We had to wait till March 1976 for the first release of funds, a paltry sum of Rs. 3 lacs. At one stage the Financial Advisor to Ministry of Health, whose main grudge against the Institute happened to be "misuse of funds for erecting black marble columns in the foyer" without any justification reduced the total allocation for the Fifth Plan by nearly Rs. 40 lacs, probably worrying that we would waste it on black marble columns. When no explanation and assurances from Dr. Gopinath and myself failed to convince him, we had to approach the office of the Finance Minister (Shri C. Subrramanayam) and the Planning Commission Deputy Chairman Shri P.N. Haksar, two of the most progressive policy makers of the country has known. Let me hasten to add that Prof. Gopinath and I approached them with the approval of our Director.
In July 1976, the Estate Committee formally appointed M/s. Pradhan Ghosh and Associates as the architects. However, between 1976 and 1978 repeated revisions of the building plan were required due to pruning of the budget allocations and rising cost of the building. At last on 14th April 1978, the President of India Shri Neelam Sanjiva Reddy laid the foundation stone of the twin centers. In his welcome address Dr. Ramalingaswami stated, "Our vision of the Centers is that they will be Centers both of public service and of higher learning at the same time". Their philosophy is that in which the patients and their needs come first, everything else is subordinate and subservient to this: He pointed out that, "The greatest and deepest need of a Centre is to be needed by Society". Quoting the famous economist Francis Delaisi, he said that. "the purpose of an Institution is to supply stability needed for long term operations. At the same time, Institutions must be able to adjust to change. It is our hope that stability, adjustability and continuity will mix in the centers in appropriate balance". Rashtrapatiji in his address expressed his happiness on the establishment of these Centers. While emphasizing that, "Our most urgent need is Primary Health Care" which should be pursued with all energy and resources at our command." He pointed out that, "we cannot altogether neglect the setting up and improvement of more advanced levels of health care at District, State and national levels. We need to have a few Centers of excellence in a large country like ours where the most advanced levels of care can be provided; specialists and researchers can be trained and the most complex problems may be referred for appropriate management" For him, "It is not a question of this or that" but a "proper balance in the developments of these various levels of health care". He was equally concerned about the scientific community which must be able to discover, adopt and innovate suitable methods not only in dealing with our current problems but also in coping with changing trends and changing needs of the future". I have quoted these excerpts from the speeches because I believe that as long as we pursue these ideals the Centre would continue to justify the generous resources provided by the government and enjoy the trust of the people.
Five years later, in March 1983, out patient clinics for Neurology, Neurosurgery (as also Cardiology and Cardiothoracic Surgery) moved to the new building, while the work continued to complete the rest. Progressively as the work progressed we continued to occupy the areas already completed. By July 1984, the built up area included basement, OPD, receiving station, noninvasive laboratories, radiology wing, 8 operation theatres (Neuro 3, Cardiac 4, Common 1) along with ICUs and postoperative wards. It was only in 1988-89 that the Centres became fully functional in their new abode. At this time Neurosciences centre had a total of 180 beds, 3 fully equipped operation theatres, 30 bedded ICUs, Intermediate care wards, fully fledged departments of Neuroradiology, Neuroanaesthesia, within this complex. The offices of the faculty and supportive staff, Neurochemistry laboratories continued to remain in the old building and by mutual agreement the Neuropathology still continues to be in parent Department of Pathology. This may be compared to the facilities available to us before we moved to the Centre. The combined strength of beds for Neurology and Neurosurgery including a half baked ICU was only 72, scattered in different parts of the old hospital.
There was only one dedicated operation theatre for neurosurgery and we shared another one with Cardiothoracic Department three days a week. There were four members on the faculty of Neurosurgery. I have been informed that there will be separate write-up's about the development of Neurology, Neuroradiology, Neuroanaesthesia, Neuropathology, Neurochemistry etc. hence I shall restrict myself in the remaining part of this review on Neurosurgery only. Nonetheless it should be mentioned that once the scheme for creating the Centre was approved, in the interval before its complete occupation we were permitted to augment the overall facilities and staff strength in a progressive manner with a view to improve the quality and maximise output of all our activities-patient care service and education in particular. Funds for research had, as even now, to be obtained on competitive basis from the grant giving agencies. During this interval we were able to obtain a munificent grant from the Swedish International Development Agency (SIDA) which modernized our diagnostic and clinical facilities including those for operation theatres and ICU. The first CT Scan in the country was installed under this grant. It was not just a coincidence that this was inaugurated by the President of India on the same day as the foundation of the Centre(s) was laid.
Coming back to the growth of neurosurgical services, in the first full year of our work i.e. 1966 we admitted 140 patients, attended to 540 in the OPD and performed 111 major and 89 minor surgical procedures. It may be mentioned that at that time many of our patients were admitted, operated upon and discharged from the emergency ward. Five years later in 1971 these numbers were 422 admitted, 1044 attended in OPD and 535 (303 major and 232 minor operations performed. In 1976, the year when the first token grant was received for the Centre we admitted 1094 patients, attended to 3784 (1960 new and 1824 old) patients in the OPD, and performed 520 major and 785 minor surgical operations. It may be recalled that at that time neuroradiological investigations pneumoencephalography ventriculography, angiography and myelography were performed by. the clinical team and hence were included as minor operations. In 1986, prior to shifting to the Centre 1898 patients were admitted, 11.225 (3406 new and 7918 old) patients seen in the OPD and 735 and 257 major or minor operations were performed. Starting with only two faculty members in 1965 - Dr. Banerji and myself, it was only in 1971 that we added one more lecturer. Dr B. Prakash. The next person to join was Dr R. Bhatia as Lecturer in 1974 The first faculty position in the Department of Neurosurgery after the Centre came into existence, was 1979 with Dr. Banerji taking over as a Professor. A little known episode in this connection needs mention to illustrate the prevailing team spirit at that time. When we got the first position of a Professor sanctioned for the Centre, I had in my mind wanted it for Dr. Banerji. The day the matter was to be finalized in the Academic Committee I was indisposed and requested Dr. Banerji to attend the meeting and briefed him about my plan. His immediate response was that it should be alloted to Neuropathology, "Dr. Subimal Roy should be given a chance before me". Dr. V.S. Mehta then joined as a Lecturer in 1981 followed by Dr. A.K. Mahapatra in 1983. In the meanwhile Dr. B. Prakash left for G.B. Pant Hospital in 1980. Thus even after fully commissioning the Centre in 1988, the Department had a total strength of 5 faculty members; who continued to share the ever increasing service load as indicated by the figures provided above.
Besides the full fledged in-service M.Ch. course (3 years for post MS (surgery) and a direct 5+1 year after MBBS), the department has been participating in undergraduate education as well as collaborating with basic science department for Ph.D. program. From 1968 when our first trainee obtained his M.Ch. degree, till 1988, twenty eight persons obtained their postgraduate degrees. Since 1988 up to date an additional 31 have qualified. Most of these are serving the country. Several of them became chiefs of their departments at Delhi, Varanasi, Srinagar, Bangalore, Cuttack and Hyderabad, thus fulfilling an important objective for which the Centre was created. From its inception the Department has been actively engaged in CME programs both intramural and extramural. Short-term training programs are organized regularly on recent advances like CT scanning, Microsurgery, Neural Transplantation, Vascular Surgery, Skull base surgery etc. An yearly course on Neurobiology for Clinicians was organized (4 at the AIIMS and 1 at NIMHANS, Bangalore). National level Hands-on Workshops were organized from time to time with the help of international faculty as for example on microneurosurgery, skull-base surgery, neural transplantation etc. A microneurosurgical laboratory, the first of its kind in the country, was established for training in microsurgical techniques, not only for neurosurgeons but for others specialities also from all over the country. The first National Neural Transplantation Facility was established in collaboration with the Department of Anatomy. The first Text Book of Neurosurgery in the country was the result of a joint effort between Madras Neurological Institute and AlIMS in 1980. This has been completely revised and updated in 1996. Four monographs "Lectures in neurobiology" were brought out in collaboration with the Department of Anatomy, AIIMS. The faculty has made contributions to several national and international text books including Tropical Neurology, Handbook of Neurology and Techniques in Neurosurgery.
AlIMS provided a unique milieu for advancing frontiers of knowledge. The Neurosurgery Department fully participated in this effort The major areas of research contributions of the Department involved collaboration of other departments in the Institute and outside included;
The above account will testify that much has been accomplished, no doubt a lot more needs to be. For me personally it has been a rewarding experience and source of great satisfaction, not just the physical growth of the Centre but the years of affection and friendship of the team who really made this happen. The only regret that continues to haunt me is our failure to see a parallel growth of the basic neurosciences as an integral part of the Neurosciences Centre. Individually these disciplines in the Institute have made very outstanding contributions. It has been stated that an institution is the lengthened shadow of an individual. If there is one example to disprove this adage, the Neurosciences Centre is one. It was born in the dreams of several, nurtured with the selfless, dedicated services of many who submerged their egoes for a cause greater than themselves, working as a team the parallel of which could hardly be found any where. In the true spirit of Gita, their sole concern was duty and not the reward. No sacrifice was great enough for establishing a centre of excellence. Posterity will judge whether they succeeded on not but no one would deny that they attempted. Unlike many other such centres in our country, even after the departure of those who initiated it, the Centre continues its journey to greater heights as will be obvious from the story told by those who succeeded. I hope and pray that the Centre will continue to live up to the foundation stone. "In the ultimate analysis, it is not the budget, nor the number of staff positions that makes a truly great centre of public service and higher learning. It is the presence of thoughtful, imaginative, humanistic, loyal and devoted faculty and students that is vital". The Centre continues to be endowed with them and I can only wish them greater heights in years ahead.
Recommendations of The Committee on Establishment of Neurology and Neurosurgery Centre at the AIIMS and Safdarjang Complex
This Centre has been chosen for the following reasons :
The needs of this proposed Neuro-centre are indicated in Appendix I and may be seen to be economical and the minimum required.
This recommendation to make the neurology complex of the AlIMS and Safdarjang Hospital into a Neuro Centre is based on the following requirements.
The Committee has further observed that
Department of Neurosurgery started a humble beginning in March 1965, with only two faculty members and a few beds. However, with dedicated efforts and sincerity of Prof. P.N. Tandon and Prof. A.K. Banerji, M.Ch training program could be initiated in 1967, when Dr. Brahm Prakash joined as M.Ch. student. In the last 45 years, Department has made a long journey in training over 140 neurosurgeons. The training provided here is considered the best in the country, as evaluated by independent assessment system.
The department is a Mecca for Neurosurgical patient care in India. It is equipped with ultra-modern technology and equipments from time to time i.e. operating microscope, Laser, CUSA, Ultrasound, Intra-operative MRI, Gamma Knife and Image Guidance System, which are necessary to provide state of the art care at par with the best neurosurgical centers any where in the world. With a moderate beginning in 1965, when only 50 patients were operated upon, today we operate around 3000 cases annually at AIIMS. With the inception of Trauma Centre in 2007, where we deal with all types of cranio-spinal trauma, our department, in addition, operates around 1500 trauma cases annually. There are in addition over 250 patients treated with Gamma Knife Radiosurgery annually (Total number till date around3000).
The Department has always been in the forefront in the areas of research and academic activities. There has been research on evidence based clinical practice and laboratory based work. These include clinico-pathological research on head injury, neuro-tuberculosis, glioma, pituitary tumors, peripheral nerve and brachial plexus injury & intracranial aneurysms. Laboratory based studies include (a) Neural transplant was developed as a national facility by DST (1984-1990), (b) Evoked potentials as diagnostic and prognostic tool, (c) Study of genetic and molecular aspect of glioma, (d) Study of cerebral blood flow using SPECT scan in brain tumor, minor head injury and craniostenosis (e) Near infrared spectroscopy and (f) MR spectroscopy etc. The Department has participated in a large number of multi-centric studies at National and International levels.
Feelings of the architects of Neurosurgery AIIMS
| Name | Designation |
|---|---|
| Dr. Chetan D.Patal | Professor & Head |
| Name | Designation |
|---|---|
| Dr. Aarti Vij | Professor |
| Name | Designation |
|---|---|
| Dr. Aarti Vij | Addl. Prof. |
| Name | Designation |
|---|---|
| Dr. Sujata Mohanty | Asstt. Prof. |
| S.No. | Name | Designation | |
|---|---|---|---|
| 1 | Dr R.Lakshmy | Professor | lakshmy_ram@yahoo.com Area of interest:
|
| Name | Designation | |
|---|---|---|
| Dr. A. K. BISOI | drakbisoi@gmail.com | Professor and Head of the Department(CTVS) |
| Dr. V.DEVAGOUROU | vdeva@hotmail.com | Professor (CTVS) |
| Dr. SACHIN TALWAR | sachintalwar@hotmail.com, drsachintalwar@gmail.com | Professor (CTVS) |
| Dr. P. RAJASHEKAR | praja@aiims.edu | Professor (CTVS) |
| Dr. MANOJ SAHU | drmanojsahu@gmail.com | Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SARVESH PAL SINGH | sarveshpalsingh@gmail.com | Additional Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr.P.RAMESH MENON | rpmpgi@gmail.com | Additional Professor Pediatrics (Neonatalogy) in CTVS |
| Dr. PRADEEP RAMAKRISHNAN | pradeep.r.reddy85@gmail.com | Associate Professor (CTVS) |
| Dr. UMMED SINGH | drusd@yahoo.com | Associate Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SUSHAMA GAYATRI B | sushama.gayatri@gmail.com | Assistant Professor (CTVS) |
| Dr. NAVNITA KISKU | navnita.kisku@gmail.com | Assistant Professor (CTVS) |
| Dr. AMITABH SATSANGI | indiactvs@gmail.com | Assistant Professor (CTVS) |
| Dr. MAYANK YADAV | drmayankctvs@gmail.com | Assistant Professor (CTVS) |
| Dr.BHARATH.V | drbharathv@gmail.com | Assistant Professor (CTVS) |
| Name | Designation |
|---|---|
| Dr. Ruma Ray | Professor |
As part of the Department Hospital Administration, AIIMS Delhi, various training and courses are imparted. For further details,
The Department of Pathology at A.I.I.M.S, founded in 1957, has been a pioneer in the field of pathology since its inception. The Department is a leading innovator in research, service and education. It has established a lead in medical research involving nutrition, cell differentiation, epidemiology, virology, various malignancies and neuro-sciences. Department of pathology is providing specialised pathology and Oncopathology services to whole of AIIMS and Dr.B .R.A IRCH (Dr. B. R. Ambedkar Institute Rotary Cancer Hospital) for many years.
The department of Oncopathology at NCI Jhajjar forms the backbone of all Oncology services provided at our center. Since its inception, the department has grown from strength to strength and aims to set up the Units of Histopathology, Cytology, Immunohistochemistry, Cytogenetics and Molecular pathology. Working in close coordination with teams from AIIMS Delhi, we strive to establish a world class diagnostic center dedicated to care and management of cancer patients.
Department of pathology is also providing full Oncopathology services to NCI Jhajjar with full involvement of all specialities as detailed below
Nuclear Medicine is a specialized branch of medicine that encompasses arrays of radiopharmaceuticals for both diagnostic and therapeutic purposes throughout the patient care continuum. The department at NCI has state-of- art facilities such as a digital ready 128 slice PET/CT and 16 Slice SPECT/CT, and currently offers the most commonly performed oncological studies.
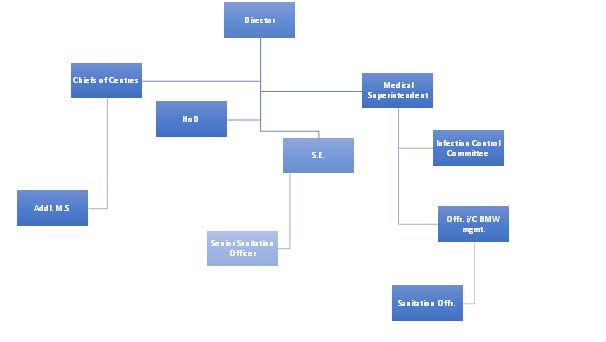
Preventive Oncology NCI:
Preventive oncology includes measures that are taken to prevent the development or delay progression of cancer. Cancer prevention is taken on three major levels:
(A). Primary Cancer Prevention: It focuses on health promotion, identifying causative factors and reducing the risk of cancer. For example, alcohol and tobacco cessation, weight reduction, vaccination, healthy lifestyle, etc.
(B) Secondary Cancer Prevention: It focuses on early cancer detection through screening before the onset of symptoms when the cancers are likely to be treated successfully. For example, mammography, HPV-DNA test, oral visual inspection, PSA test, etc.
(C) Tertiary Cancer Prevention: It focuses on delaying the progression and preventing the complications like secondary malignancies after cancer diagnosis.
Why it's important:
Cancer prevention is done at both individual and community level for reducing the risk and incidence of cancer. By preventing cancer, the number of new cases of cancer will be lowered and thus reducing overall cancer burden. Early diagnosis will lead to optimal cancer management and improved survival.
Preventive Oncology at NCI-Jhajjar envisages to
develop evidence-based approaches and technical resources for cancer prevention and control in India through:
Medical Physics Unit at IRCH and NCI is instrumental in providing licensing and compliance with the regulations of Atomic Energy Regulatory Board (AERB) to all x-ray imaging machines, radiation safety and quality in imaging related services to all those departments which uses radiation in imaging, patient services and research activities. We look after radiation related research in medical radiological imaging in mammography, CT, ultrasound, radiography, fluoroscopy and angiography, radiation dosimetry in patient in imaging, reduction of dose without compromising diagnostic information, radiation protection and measurement of radiation dose to staff and attendants, irradiation of blood bag before blood transfusion to patients, radiation protection survey for radiological imaging installation all over AIIMS and NCI. Our activity includes staff and public education regarding radiation safety, besides imparting knowledge (in form of regular classes) in the field of Medical Physics and Radiation Safety to MD (radiology), MBBS students, B.Sc. Radiography, M.Sc. Biophysics, M.Sc. Cardio-radiology, nursing students and other interested groups and individuals which includes trainees from other hospitals. The unit provides consultation in any untoward accidental radiation exposure to patient, public or staff. Our endeavour makes radiation installations safe for patient, staff and public for which there is a great concern now-a-days. We have a viable PhD programme in Medical Physics running in the department.
The Department started functioning in 1983 with help of x-ray and mammography unit. It developed gradually. Today, the department, along with NCI Jhajjar has 3 CT machines, 1 MRI, 2 DSA, 2 mammography units with digital breast Tomosynthesis and Contrast enhanced mammography, in addition to numerous ultrasound and radiography units, including fluoroscopy and portable radiography. The department provides services to inpatients and outpatients of BRA-IRCH and NCI Jhajjar
| Equipment | BRA-IRCH | NCI Jhajjar |
|---|---|---|
| CT | 1 | 2 |
| MRI | 0 | 1 +1 (in process) |
| DSA | 1 | 1 |
The department provides diagnostic as well as interventional radiology services to cancer patients. Diagnostic CT scans, MRI, Ultrasound, Xray, Mammography are performed. Interventional procedures include biopsy and fine needle aspiration cytology under CT, Ultrasound and mammography guidance, percutaneous transhepatic biliary drainage, percutaneous nephrostomy, transarterial angioembolisation, Nerve blocks for pain relief, NG tube insertion, percutaneous gastrostomy, tumor ablative proVacuum assisted biopsy, clip placement and wire localisation of breast masses and vascular procedures such as peripherally inserted central line catheter and angioembolisation procedures.
The department boasts of turn-around report times of 24 hours. Dates for routine imaging (CT and Ultrasound) of all in-patients are given the next working day.
External Beam Radiotherapy Brachytherapy
| 4D-CT Simulation | ICRT |
| IMRT | ILRT |
| IGRT | Mould Brachytherapy |
| SGRT | Image Guided Brachytherapy |
| VMAT | Interstitial Brachytherapy |
| SBRT | - |
| SRT | - |
| TSET | - |
| TBI | - |
| Vision RT | - |
| Radiation under Anaesthesia | - |
1. Varian Trubeam 2.7 (2)
2. Flexitron (1)
3. 4D-CT Simulator (1)
Department of Radiation Oncology at NCI Jhajjar started functioning on May 29th, 2019 with brachytherapy. Subsequently, Linear Accelerator facilities were Inaugurated on 14th November 2019 in the presence of Director AIIMS Delhi Dr. Randeep Guleria, Head-NCI Dr. GK Rath, and Head of Department Dr. DN Sharma. Since thenaround 33,399 radiation fractions have been delivered via Linear Accelerator and 1108 patientstreated with brachytherapy. Apart from Radiation Treatment delivery, we are also running OPD and IPD services.OPD services are running since November 2019 site and organ-specific in collaboration with other departments. We have fully functional IPD services with 24 Bedded ward. Our effort toward patient care is reflected in the fact that during the COVID-era when all the regular services were affected Department of Radiation Oncology provided its services to the patients without hampering patient care.
CThe Department of Head and Neck Oncology at the National Cancer Institute, Jhajjar, strives to offer affordable and quality service to patients with head and neck cancer. The department currently provides daily outpatient services (Monday to Friday), including various office-based procedures. We ensure optimal and quality clinical in-patient services in the current 20-bedded ward on the 5th floor. Additionally, we run a multidisciplinary disease management group twice a week (Tuesday and Friday) and a swallowing clinic with a facility for Functional endoscopic evaluation of swallowing (FEES) for appropriate rehabilitation of the patients after surgery in the OPD setting. Emergency services (management of airway and bleeding in relation to head and neck cancers) are offered round the clock. We are equipped with nasal endoscopy and fiberoptic laryngoscopy for clinical oncologic examination.
The department runs eight operation theaters weekly (Monday to Friday). It offers surgical treatment of cancer related to the domain of Otorhinolaryngology (maxillectomy, laryngectomy, neck dissection, glossectomy, thyroidectomies, mandibulectomy, etc.) for early and advanced oral, laryngeal, and other head and neck cancers.
In addition to clinical care, the department has also been playing a prominent role in academic and research activities. Residents training (MS {ENT} and MCh {Head and Neck Cancer Surgery}) is being undertaken with an emphasis on clinical care, research, and teaching aspects. The teaching courses in the subspecialties of Head and neck oncology are being conducted regularly.
Cancer is emerging as a major public health problem globally. As per WHO GLOBOCAN 2020, 1.32 million new cases of cancer are detected each year in India and 0.85 million succumb to this deadly disease. Cancer treatment requires a multimodal management approach. Surgery is one of the main modalities for treating cancer and 90 % of cancer patients need some surgical intervention. The surgical specialty dealing with cancer management is known as Surgical Oncology.
Background: Dedicated surgical oncology services at Dr. BRA-IRCH were started in 1988. Prof NK Shukla was the first faculty to initiate cancer surgical services and Dr. SVS Deo joined as second faculty in 1995. The unit was recognized as an independent Department of Surgical Oncology in the year 2001 and the services were further expanded to 46 Surgical beds, 6 bedded ICU and 3 major Operation theaters in 2005. MCh Surgical Oncology program was started in 2012. The department took a leadership role in the planning and establishment of state of art surgical oncology services at National Cancer Institute (NCI) Jhajjar and started cancer surgical services at NCI-AIIMS in 2019. Currently the department has 10 faculty members,18 MCh trainees and 12 Senior residents.
The three major activities of the department include Patient Care, Teaching & Training and Research.
The department leads in introducing advanced and cutting-edge surgical programs including Minimally Invasive Surgery (Lap & VATS), Peritoneal Surface Malignancies (Cytoreductive Surgery, HIPEC & PIPAC), Oncoplastic & Microvascular surgery, Risk Reducing Surgery, Navigational Surgery, Organ Conservation and Intra-operative Radiation Therapy and Palliative Surgical Oncology at AIIMS.
Teaching and Training: The department runs MCh Surgical Oncology program, which is one of the leading and popular MCh programs in India. In addition, the department offers long term and short-term training to general surgeons. The department has trained more than 150 cancer surgeons during last 25 years, who are in leadership positions in different parts of the country.
Research: The faculty members of the departmentare actively engaged in a number of collaborative basic and clinical research projects including multicentric international trials. The department has developed a computerized comprehensive oncology clinical data base and currently has comprehensive clinical data related to more than 10,000 cancer patients operated in the department. The faculty has published more than 300 scientific papers in prestigious national and international journals.
Other Activities: The faculty of the department are actively involved as members, experts and advisors for various organizations and scientific bodies like NBE, ICMR, DBT, DS, Ministry of Health, IASO, ISPSM, ABSI and BSI. The department regularly conducts workshops and organizes major conferences (ICC 2013, NATCON 21, ABSICON18 and INDO-UK Oncoplasty course, ISPSM-ESSO cadaver courses on CRS & HIPEC etc.)
History of Dept of Surgical Oncology
Major Landmarks & Timelines –
1983 - Dr. BRA-IRCH was established as a comprehensive cancer center of AIIMS
1988 - Dr. NK Shukla joined as first faculty and established a Unit of Surgical Oncology to offer basic cancer surgical services.
1991 – Senior Residency training program was started, and major cancer surgical services initiated.
1995 – Dr SVS Deo joined as second full-time faculty.
1996 – A dedicated 20 bedded Surgical Oncology ward along with a major OT and ICU were established with a philanthropic donation from Shri. Kanhayalal Punj.
2001 – Unit of Surgical Oncology was upgraded as a full-fledged independent Department
2005 – IRCH expanded to 182 bedded regional cancer Center including 48 Surgical Oncology beds and 3 major operation theaters.
2012 – M.Ch. course in Surgical Oncology was started with an annual intake of 5 students.
2012 – Dr. Sunil Kumar and Dr. MD Ray joined as full-time faculty
2017 – Prof. SVS Deo assumed the role of Head of Department after Prof. NK Shukla’s superannuation.
2018 – Three more faculty members Dr Sandeep Bhoriwal, Dr Ashutosh Mishra and Dr Jyoti Sharma joined the Department.
2019 – Inauguration of National Cancer Institute, AIIMS, Jhajjar campus by Honorable Prime Minister and launch of Surgical Oncology services at NCI campus.
2020 – Four more faculty members joined the department Dr. Naveen, Dr. Babul Bansal, Dr. Jyoutishman Saikia and Dr Raghuram K.
Immediate
Reporting
Management
Follow-Up
Occupational exposure
Occupational exposure refers to exposure to potential blood-borne infections (HIV, HBV and HCV) that occurs during performance of job duties.
“Exposure” which may place an HCP at risk of blood-borne infection is defined as :
What is infectious and what is not?
| Exposure to body fluids considered ‘at risk’ | Exposure to body fluids considered ‘not at risk’ | |
|---|---|---|
| Blood | Tears | Unless these secretions contain visible blood |
| Semen | Sweat | |
| Vaginal secretions | Urine and Faeces | |
| Cerebrospinal fluid | Saliva | |
| Synovial, pleural, peritoneal, pericardial fluid | - | |
| Amniotic fluid | ||
| Other body fluids contaminated with visible blood | ||
It is necessary to determine the status of the exposure and the HIV status of the exposure source before starting post exposure prophylaxis (PEP).
Step-1 : Immediate measures
For skin - if the skin is broken after a needle-stick or sharp instrument :
After a splash of blood or body fluids on unbroken skin :
For the eye
For mouth
Don’ts
Step-II : Prompt reporting :
Step-III : Post exposure treatment :
The decision to start PEP is made on the basis of degree of exposure to HIV and the HIV statusof the source from where the exposure/infection has occurred. More so, it should begin as soon as possible preferably within two hours, and is notrecommended after 72 hours.
PEP is not needed for all types of exposures : The HIV seroconversion rate of 0.3% after an AEB (accidental exposure to blood) (for percutaneous exposure) is an average rate. The risk of infection transmission is proportional to the amount of HIV transmitted, which depends on the nature of exposure and the status of the source patient. A baseline rapid HIV testing of exposed and source person must be done for PEP. However, initiation of PEP should not be delayed while waiting for the results of HIV testing of the source of exposure. Informed consent should be obtained before testing of the source as per national HIV testing guidelines.
First PEP dose within 72 hours
A designated person/trained doctor must assess the risk of HIV and HBV transmission following an AEB. This evaluation must be quick so as to start treatment without any delay, ideally within two hours but certainly within 72 hours; PEP is not effective when given more than 72 hours after exposure. The first dose of PEP should be administered within the first 72 hours of exposure. If the risk is insignificant, PEP could be discontinued, if already commenced.
Step-IV : Counselling for PEP :
Exposed persons (clients) should receive appropriate information about what PEP is about and the risk and benefits of PEP in order to provide informed consent for taking PEP. It should be clear that PEP is not mandatory.
Step-V : Psychological support :
Many people feel anxious after exposure. Every exposed person needs to be informed about the risks, and the measures that can be taken. This will help to relieve part of the anxiety. Some clients may require further specialised psychological support.
Step-VI : Documentation of exposure :
Documentation of exposureis essential. Special leave from workshould be considered initially for a period of two weeks. Subsequently, it can be extended based on the assessment of the exposed person’s mental state, side effects and requirements.
IMPORTANT : Seek expert opinion in case of
Step-VII : Follow-up of an exposed person :
Whether or not post-exposure prophylaxis is started, a follow up is needed to monitor for possible infections and to provide psychological support.
Clinical follow-up
In the weeks following an AEB, the exposed person must be monitored for the eventual appearance of signs indicating an HIV seroconversion: acute fever, generalized lymphadenopathy, cutaneous eruption, pharyngitis, non-specific flu symptoms and ulcers of the mouth or genital area. These symptoms appear in 50%-70% of individuals with an HIV primary (acute) infection and almost always within 3 to 6 weeks after exposure. When a primary (acute) infection is suspected, referral to an ART centre or for expert opinion should be arranged rapidly.
An exposed person should be advised to use precautions (e.g., avoid blood or tissue donations, breastfeeding, unprotected sexual relations or pregnancy) to prevent secondary transmission, especially during the first 6–12 weeks following exposure. Condom use is essential.Drug adherence and side effect counselling should be provided and reinforced at every follow-up visit. Psychological support and mental health counselling is often required.
Laboratory follow-up
Exposed persons should have post-PEP HIV tests. HIV-test at 3 months and again at 6 months is recommended. If the test at 6 months is negative, no further testing is recommended.
| Sr. No. | Category of staff | Trained |
|---|---|---|
| 1 | Doctors | 79 |
| 2 | Nurses | 211 |
| 3 | Paramedical staff | 414 |
| 4 | Sanitation staff (SA/HA) | 56 |
| TOTAL | 760 | |
| Sr. No. | Category of staff | For Hepatitis B Vaccinated (first and second dose) |
|---|---|---|
| 1 | Biotec (CMBWTF) | 21 |
| 2 | Sanitary / Hospital attendants | 324 |
| TOTAL | 345 | |




The National Cancer Institute (NCI) is a specialty tertiary healthcare institute dedicated to cancer care. This is second campus of the AIIMS Delhi located at Jhajjar, Haryana.
National Cancer Institute is one of the largest public funded health care projects in independent India costing nearly 2035 crore rupees.
The institute is envisaged to bridge the gap in cancer healthcare, providing state-of-art facility to patients and play a pioneering role in the field of translational research.
It will concentrate on various unanswered questions through research prevention, early diagnosis and management of Indian cancers like the oral cancers, gall bladder cancers, cervical cancers etc.
Apex Centre for Translational Research in Prevention & Care for India Centric Cancers.
It is largest Public Funded Hospital Project at Rs 2035 Crores.
NCI is set in 60 acres within the Jhajjar campus of AIIMS and 2.5 Lakh Sq Meter built-up area. The National Cancer Institute has 700+ beds dedicated for cancer prevention, care and research, 350+ dwelling units and 600+ hostel rooms for doctors and staff . 3000+ career opportunities to tap the best brains in oncology. Dedicated PI based labs, tissue/bio-banking banking facility, etc.
National Cancer Institute has one of Asia’s 1st fully automated core-lab
Bhoomi pujan of NCI was performed by Hon’ble Union Minister for Health & Family Welfare on 12 th December, 2015.National Cancer Institute started with phase-I on December 2018 consisting of 250 beds, OPD and OT. In March 2019, services of Radiation Oncology and Nuclear Medicine began.
State of the art Medical Equipment & Facilities in plan.
Fully paperless ICU and OT System.
India’s 1st Public Sector Proton Facility which is a new paradigm in the treatment of cancer patients in the country with fully integrated and is well equipped with cutting edge technology
Modular 25 OT, 04 PET Scanners, 02 MRI Scanners, 05 Linear Accelerator, Intra-OP RT Facility, Oncology Emergency, 60 Intensive Care beds, 03 Brachytherapy, 20 Bedded Nuclear Medicine, 40 Bedded Palliative Care Unit with 14 PI Labs and approximately 500,000 patients in a year
National Cancer Institute comprises of 6 blocks: Hospital block (area -56324 Sqm), OPD block (area- 11252.26 sqm) which has 60+ consultant rooms along with waiting area for 1200 people, Diagnostic block and animal house(area -17757 sqm) consisting state-of-art Core Lab Facility & Animal house with nude mice facility, Administration & Research block (area- 14713 sqm) with Bio-Bank facility for sorting tissue samples for research purposes, Academic block & Research block (area- 13669 sqm) which comprises 12 PI based Research lab and Auditorium of 450 capacity, Guest House block with residential facilities (area- 7653 sqm) with approx. 90 rooms along with cafeteria, gymnasium, and seminar room etc
NCI is also collaborating with Department of AYUSH for research into the role of Indian Systems of Medicine in prevention and cure of cancers. NCI is collaborating with the National Institute of Cancer of USA, La Foundaton De I’ Academie de Medicine of France, Barts Cancer Institute in Queen Mary University of London in UK and many more national and international organizations to carry out high quality research

The DR. BRA-IRCH has the following departments:
Institute Rotary Cancer Hospital (DR. B.R.A. Institute Rotary Cancer Hospital) started functioning in 1983-84 on 35 beds with infrastructure of 2 floors. Recently it has been converted into a 200 bedded, 7th floor building. Prime Minister of India Sh. Atal Bihari Vajpayee, inaugurated this centre on October 5, 2003.
Best of radiodiagnostic and radiotherapy machines including state of art linear accelerator, brachytherapy, stereotactic radiotherapy and intensity modulated radiotherapy are available at this centre. Vaccum assisted advanced mammography unit, first of its kind in India, has made stereotactic breast biopsy possible. Prostate cancer can be diagnosed at an early stage with help of tranrectal sextant biopsy. Radio frequency ablation of liver cancer has also been initiated.
DR. B.R.A. Institute Rotary Cancer Hospital is one of the few centres in the country to have established hematopoietic stem cell bone marrow transplant programme; more than 250 transplants have been performed. In collaboration with dept. of CTVS, stem cell transplant programme has been extended to treat myocardial ischemia also.
Medical Oncology has established modern techniques utilizing FISH and polymerase chain reaction (PCR) to prognosticate cancer patients. Also, innovative research by this department has demonstrated the liberation of hematopoietic cytokines from fetal liver, with the potential to treat aplastic anemia. This department has researched into our ancient wisdom also and has discovered that combination of yoga, pranayam, meditation and sudershan kriya-a rhythmic breating process induces positive changes in brain. These processes enhance antioxidant defence and immune functions of body, and thus may prevent onset and/or progression of cancer.
Preventive oncology programme to bring awareness about cancer masses has been initiated, also screening programme to detect cancer early, over 10,000 people have been screened so far.
ई. एच. एस. (परिवार चिकित्सा विभाग) की स्थापना एम्स में केन्द्रीय सरकार की स्वास्थ्य सेवाओं के पैटर्न पर संस्थान के कर्मचारियों और उनके आश्रित व्यक्तियों की निवारक, संवर्धनात्मक और उपचारात्मक स्वास्थ्य देखभाल हेतु की गई थी।
बाह्य रोगी देखभाल का कार्य चिकित्सकों के द्वारा किया जाता है। यहां एक इंजेक्शन लगाने का कमरा, पट्टी बांधने का कमरा, इलाज कक्ष और दिवस देखभाल कक्ष हैं। दिवस देखभाल कक्ष में रोगी को अवलोकन के लिए किसी छोटी चिकित्सीय और शल्य चिकित्सा प्रक्रिया के बाद रखा जाता है। ईएचएस के आंतरिक रोगियों के लिए 52 बिस्तर हैं जो उनके लिए तय अलग अलग वॉर्डों में उपलब्ध हैं। यहां निजी कमरे हैं जो इन रोगियों के लिए तय किए गए हैं।
| year wise | UNDERGRADUATE Students List | POSTGRADUATE Students List | ||
|---|---|---|---|---|
| Senior Res. | Junior Res. | M.Sc | ||
| 2012 | Acad Non- Acad | Acad Non- Acad | Acad | |
| 2013 | Acad Non- Acad | Acad M.D/ M.D.S/ M.S / M.H.A from 2011 to 2013 Non- AcadJuly session only | Acad | |
| 2014 | Acad | Acad M.D/ M.D.S/ M.S / M.H.AJan Session Non AcadJan Session | ||
ONLINE HOSTEL APPLICATION SUBMISSION SYSTEM (for Post Graduate)
PROCEDURE TO APPLY FOR HOSTEL ACCOMODATION ONLINE (for Post Graduate)
ONLINE HOSTEL APPLICATION SUBMISSION SYSTEM(for Under Graduate)
PROCEDURE TO APPLY FOR HOSTEL ACCOMMODATION ONLINE(for Under Graduate)


The All India Institute of Medical Sciences has several hostels for its undergraduate and postgraduate students, PhD scholars and resident doctors. Conveniently located, hostellers do not have to travel long distances after a day of hard work and studies. These hostels are an essential component of the life at this institution wherein students, staff and faculty reside in the same campus. The life in hostels enables students to spend ample time in the hospital, departments utilizing library and other facilities to ensure they develop academically and acquire the necessary skills that can be obtained only through experience. In addition the hostel life allows students to interact with their colleagues and peers, make friends, and develop into good human beings capable of independent judgment and coping with the day to day pressures of life. Some students may leave their homes for the first time and they can be reassured these hostels would eventually turn out to be a home away from home!





कोविड-19 मानसिक स्वास्थ्य हेल्पलाइन - एम्स संकाय, रेजीडेंट और कर्मचारी
Dr. Shailesh B Gaikwad, MD, FNAMS, CCST
Professor & Head, Department of Neuroimaging & Interventional Neuroradiology, Neurosciences centre
All India Institute of Medical Sciences (A.I.I.M.S), New Delhi
Chairman, AIIMS Gymkhana
Email id: sgaikwad_63@yahoo.com | sbgaikwad1112@gmail.com
Contact No : 9971237573
Reviewer for following journal
Awarded WHO Fellowship in Neurointervention, 2001
Hands-on-training workshop on GDC treatment of Intracranial aneurysms, held on 1-4 June 2000, Seoul National University Hospital, Seoul, South Korea, Program proctor Prof. In Sup Choi, Chairman, Department of Interventional Neuroradiology, MGH, Boston, USA.
Hands-on-training on Carotid Angioplasty and Stenting, , Organized by Prof Kieren Murphy, Neuroradiology, John Hopkins University, Baltimore, USA, September 7-10, 2000.
Course on “International Master Degree in Neurovascular diseases”, 2001, Course director - Prof P Lausjaunias, Bicetre, France, co-organized by Paris Sud University, and Mahidol University.
Attended 12th & 13th Zurich workshop on interventional Neuroradiology, March 2004 & 2005. Course conducted by Prof. A Valavanis, Professor and Head of Neuroradiology department, Zurich University Hospital, Switzerland
Visiting Fellowship for “Advanced training in neurointerventional techniques” at Hacetteppe University Hospital, Ankara, Turkey, May 2006. Course director-Prof Saruhan Cekirge, Isiil Satchi. This centre is the primary site for hands-on-training in Onyx embolization of AVMs and advanced neurointervention procedures including FLOW DIVERTERS.
Visiting Professor-Department of Neuroradiology, South Carolina, Duke University, USA (December 2007).
Attended “3rd Anatolian International Workshop on Interventional Neuroradiology”, 8-11th May, 2008 , Istanbul, Turkey
Visiting Professor & Research Associate: BWH, Harvard Medical School, Boston, USA-31/1/2009-30th June 2009
Hands-on training on Flow diverters
Hands-on training on: Penumbra and Merci devices, n-BCA Liquid Embolic System Advanced Training Course (for AVM embolization) at the University of Massachusetts Medical School, Worcester, MA, USA. Course director-Prof. Ajay Wakhloo –June 13, 2009
Hands-on training workshop for advanced training in Perfexion Gamma knife for treatment of brain tumours and AVMs, 28th November-2nd December, 2011, at Cleveland Clinic, Ohio, USA
Awarded Fellowship by National Academy of Medical Sciences-27/10/2017
Member of expert group on “National Stroke Registry”: Expert group meeting on PBSR, HSBR, “To review PBSR & HSBR Training workshop for HSBR centers”, 12th December, 2019 NCDIR, ICMR, Bangalore, Karnataka
Expert of “Skill Development Initiative for Emerging World Countries”, Republic of Maldives, January 2020 onwards.
Attended World Live Neurovascular Conference, held on 23-24 October 2020, Live Virtual Experience.
Chief Coordinator for “Conducting Neuroradiology Workshop”, National Institute of Neurosciences & Hospital, Dhaka, Republic of Bangladesh.
| S No | Name | Designation | Office Address | Office telephone | |
|---|---|---|---|---|---|
| 01 | Dr. S. B. Gaikwad | Professor & Head | Room no.11, 6th floor CNC Room No.15, Cath Lab Complex, CNC | Ext. 3457 Ext.4418 | sgaikwad_63@yahoo.com |
| 02 | Dr. Ajay Garg | Professor | Room No.14, Cath Lab Complex | Ext 6449 | ajaygarg@aiims.ac.in drajaygarg@gmail.com |
| 03 | Dr. Leve Joseph Devarajan S. | Additional Professor | Room No.17, Cath Lab Complex | Ext.3844 | leve_s@yahoo.com |
ओपीडी अपॉइंटमेंट बुकिंग टेलीफोन पर-
011-26589142(इस टेलीफोन पर ओपीडी बुकिंग के लिए समय सुबह 8:00 बजे से रात 8:00 बजे (सभी कार्य दिवस में)।
मोबाइल ऐप: एम्स ऐप के अकार्यात्मक हो जाने के कारण इसे Google Play स्टोर से हटा दिया गया है। जिन उपयोगकर्ताओं ने इस ऐप को इंस्टॉल किया था, उन्हें अपने उपकरणों से इसे हटा देना चाहिए।.
में पोस्ट ऑपरेटिव कार्डिएक सर्जिकल रोगियों के प्रभावी फॉलोअप की सेवाओं के लिए, समर्पित हेल्पलाइन और व्हाट्सएप नंबर: 9999635940, 9999635425 सोमवार,बुधवार और शुक्रवार (यानी सामान्य ओपीडी घंटों से अन्यथा) दोपहर 2:00 बजे से शाम 6:00 बजे तक सक्रिय रहेंगे।.
नोट: - यदि ओ.आर.एस पोर्टल पर अपॉइंटमेंट उपलब्ध नहीं हैं, तो कृपया कॉल सेंटर को भी कॉल न करें, क्योंकि ओ.आर.एस पोर्टल तथा फोन के माध्यम से आपंइटमेंट एक ही पूल से मिलते हैं|
Clinical Neuropsychology at the Neurosciences Centre, AIIMS in New Delhi, India, provides para-clinical services following the terminology outlined by the Sneh Bhargava Commission (2012) This specialized service encompasses a comprehensive range of neuropsychological services, including psycho-diagnostics (which involves clinical history taking, psychometric assessment, and clinical observation), remediation (involving counseling and rehabilitation), and neuropsychological disability evaluations. These services address both cognitive and non-cognitive aspects for individuals with neurological and neurosurgical conditions. Established in 1969 with the appointment of Dr. Surya Gupta, this discipline has played a significant role in advancing clinical neuropsychology in the country, aiming to deliver services in line with international standards for the benefit of patients at the Neurosciences Centre at AllMS.
Furthermore, the discipline has been enriched through clinical neuropsychological educational programs in neuropsychology for M.B.B.S., Nursing, DM (Neurology), MCh (Neurosurgery), and MD (Psychiatry) students. Presently, it also supervises research projects for postgraduate students from these departments, focusing on neuropsychological psychometric assessments. The creation of distinctive neuropsychological test batteries, such as the 'AIIMS Neuropsychological Battery,' represents a significant achievement in assessing organicity, lateralization, and lobar functions across various age groups, including Adults, Children, and the Elderly. These efforts have been supported by three research projects funded by the ICMR.
Since 2005, our research and clinical services have expanded to include the development of neuropsychological screening tools for clinicians to use in their practices, history taking forms, tests, and a variety of neuropsychological rehabilitation programs for neurological and neurosurgical conditions. Committed to enhancing patient care, we provide advanced Neuropsychological services tailored to individuals with neurological disorders. By closely collaborating with clinicians at AIIMS, New Delhi, who act as primary healthcare providers in a hospital setting, we adhere to the World Health Organization's Continuum of Care Model to address the specific needs that prompt referrals.
Sneh Bhargav Commission (2012). Work Standards for Faculty of Autonomous Institutions of Medical Education under the Department of Health and Family Welfare, Govt of India. Memo. no. V-16020/57/2008-ME-I (Pt.) pp 165-174.
| S No | Faculty Member | Designation | Email ID | Contact no |
|---|---|---|---|---|
| 01 | Dr. MC Sharma | Prof. & Head | sharmamehar[at]yahoo[dot]co[dot]in | +919717739755, 011-26549205 |
| 02 | Dr. Vaishali Suri | Professor | Surivaishali[at]yahoo[dot]co[dot]in | +919810254964, 011-26544656 |
In India, the concept of “Neuroanaesthesia as a subspeciality” of Anaesthesia was recognized, way back in 1968, when Dr. Surinder Singh Saini volunteered to anaesthetize the neurosurgical patients at All India Institute of Medical Sciences (AIIMS), New Delhi, on a regular basis. Formal training in Neuroanaesthesia, for post-graduate degree holders (MD) of Anaesthesia, for trainees from all over India, was started in 1982. In 1987, an independent Department of Neuroanaesthesia was established under the leadership of Prof. S S Saini as the Head along with two more faculties, Dr. Hari Hara Dash as Assistant Professor and Dr. Parmod Kumar Bithal as Lecturer. Five Senior Resident (SR) doctors joined them for assisting the clinical activities of the department.
In August 1989, the Department was shifted to the newly built the Cardiothoracic and Neurosciences Centre (CNC) of AIIMS (present location) along with other sister departments. Facilities during that time included three well-equipped operation theatres (OTs), one emergency (septic) OT, which was shared with the cardiothoracic centre, five-bedded intensive care unit (ICU), and twenty beds for postoperative patients.
In 1995, a process to start three years superspeciality degree course (DM) in Neuroanaesthesiology was initiated under stewardship of Prof. H. H. Dash. It was materialized in 2001, when DM (SR) posts (Six direct and three sponsored) were sanctioned by the Institute body. In 2002, two direct candidates were enrolled, for the first time in India, through a common entrance test. After the JPNA Trauma Centre was established by AIIMS, in 2006, 10 more post of non-DM SR was added to the existing 10 posts. In the subsequent year (2007), two more posts of SR (DM) were again sanctioned making the final tally of open category DM (SR) seats as eight. At present, the department is located in the Neurosciences Centre, at 6/7th floor, with the office operated from room no. 709A. One personal assistant and two office assistants look after the smooth management official activities.
Currently, the Department of Neuroanaesthesiology has expanded its horizon; caters clinical service to six well-equipped neurosurgical OTs, a brain suite (MRI- OT), two neuro-cath Labs, two MRI facilities, One GammaKnife facility, one pain clinic, a pre-anaesthetic check-up (PAC) clinic, two neurosurgical ICUs (total 26 beds), one neurology ICU of five beds, more than two OTs for trauma patients, a twenty-bedded ICU for neurotrauma patients apart from providing resuscitation measures for neurological and neurosurgical ward patients. To meet with the demand of workload, the faculty strength now has been increased to sixteen which includes two professors, four additional professors, and ten assistant professors.
This department has been actively involved with training of Indian defense service personnel and overseas trainees apart from the DM and Non-DM trainees (SRs) of Neuroanaesthesia. So far, 25 candidates have been awarded the DM degree in Neuroanaesthesiology. The department plans to start Neurocritical Care programme in coming years, and to establish this super-speciality in India, the need for which is being realized, nation-wide. The faculty and staff of this department strive hard to ensure that the ‘Department of Neuroanaesthesiology’ continues to be the torch-bearer of perioperative neurosciences, and serve as a role model in this field.
In India, the concept of “Neuroanaesthesia as a subspeciality” of Anaesthesia was recognized, way back in 1968, when Dr. Surinder Singh Saini volunteered to anaesthetize the neurosurgical patients at All India Institute of Medical Sciences (AIIMS), New Delhi, on a regular basis. Formal training in Neuroanaesthesia, for post-graduate degree holders (MD) of Anaesthesia, for trainees from all over India, was started in 1982. In 1987, an independent Department of Neuroanaesthesia was established under the leadership of Prof. S S Saini as the Head along with two more faculties, Dr. Hari Hara Dash as Assistant Professor and Dr. Parmod Kumar Bithal as Lecturer. Five Senior Resident (SR) doctors joined them for assisting the clinical activities of the department.
In August 1989, the Department was shifted to the newly built the Cardiothoracic and Neurosciences Centre (CNC) of AIIMS (present location) along with other sister departments. Facilities during that time included three well-equipped operation theatres (OTs), one emergency (septic) OT, which was shared with the cardiothoracic centre, five-bedded intensive care unit (ICU), and twenty beds for postoperative patients.
In 1995, a process to start three years superspeciality degree course (DM) in Neuroanaesthesiology was initiated under stewardship of Prof. H. H. Dash. It was materialized in 2001, when DM (SR) posts (Six direct and three sponsored) were sanctioned by the Institute body. In 2002, two direct candidates were enrolled, for the first time in India, through a common entrance test. After the JPNA Trauma Centre was established by AIIMS, in 2006, 10 more post of non-DM SR was added to the existing 10 posts. In the subsequent year (2007), two more posts of SR (DM) were again sanctioned making the final tally of open category DM (SR) seats as eight. At present, the department is located in the Neurosciences Centre, at 6/7th floor, with the office operated from room no. 709A. One personal assistant and two office assistants look after the smooth management official activities.
Currently, the Department of Neuroanaesthesiology has expanded its horizon; caters clinical service to six well-equipped neurosurgical OTs, a brain suite (MRI- OT), two neuro-cath Labs, two MRI facilities, One GammaKnife facility, one pain clinic, a pre-anaesthetic check-up (PAC) clinic, two neurosurgical ICUs (total 26 beds), one neurology ICU of five beds, more than two OTs for trauma patients, a twenty-bedded ICU for neurotrauma patients apart from providing resuscitation measures for neurological and neurosurgical ward patients. To meet with the demand of workload, the faculty strength now has been increased to sixteen which includes two professors, four additional professors, and ten assistant professors.
This department has been actively involved with training of Indian defense service personnel and overseas trainees apart from the DM and Non-DM trainees (SRs) of Neuroanaesthesia. So far, 25 candidates have been awarded the DM degree in Neuroanaesthesiology. The department plans to start Neurocritical Care programme in coming years, and to establish this super-speciality in India, the need for which is being realized, nation-wide. The faculty and staff of this department strive hard to ensure that the ‘Department of Neuroanaesthesiology’ continues to be the torch-bearer of perioperative neurosciences, and serve as a role model in this field.
“It was May 1965 that I came to Delhi from Vellore where I was a lecturer, to appear for a Union Public Service Commission interview for the job of Reader at G. B. Pant hospital, Delhi and All India Institute of Mental Health, Bangalore (later to become NIMHANS). I was the only candidate and was asked at the end as to which place would I prefer. I chose Bangalore. Just before leaving for the interview, I had gone to see Dr. Baldev Singh and Dr P. N. Tandon (PNT) at AIIMS to pay a courtesy call. They were sharing an office and I suspect eagerly waiting like spiders, to catch a victim in neurosurgery, who could stick on at AIIMS, which at that time had actually nothing no space, equipment or staff. After a little talking about general things, suddenly, Dr. Baldev Singh asked me to think whether I at all wanted to go for the interview, as AIIMS could possibly offer me a job, I of course declined the proposal as a bird in hand was better than two in the bush. Then Dr. Tandon asked me to come home for tea that evening. I left for the Union Public Service Commission office. Today when I see large number of candidates for a job interview my own experience seems miraculous.
Coming back after the interview I recounted what happened to Gopal and his wife Radha (Dr. G.K. Vishwakarma was then Asst. Professor Orthopaedics and later became D.G.H.S. of Government of India) Insidious pressure started from them to come to AIIMS and forget about Bangalore. Incidentally Bangalore had a working, full fledged department with Prof. RM. Verma and he tried hard to get me there even after I joined AIIMS.
That evening I spent at Tandons. Dr. P. N. Tandon had been my Anatomy demonstrator in 1952 while Mrs. Leela Tandon was my lecturer in Obstetrics and Gynaecology at Medical College, Lucknow. I had met Dr. P.N. Tandon in 1963 at the annual Neurological Society of India meeting in Calcutta. For both of us it was the very first meeting that we had attended of NSI. Dr. P. N. Tandon had established the department of neurosurgery at AlIMS 2 months before in March 65. He had been promised equipment but nothing had arrived in the two months. He was eager that I should join but was frank to say he did not know how things would eventually develop. After returning to Gopal's house, Radha and Gopal took me to see 'My Fair Lady' at Sheila Theatre which then was the best in Delhi, if not India. After returning well past midnight we slept on the roof and went on talking about what I should do. I think it was near the break of dawn that I finally succumbed to pressures from Gopal and Radha and said OK I'll come to Delhi if the job was offered. Next morning before I left Delhi Dr. Baldev Singh took me to meet Prof. K. L. Wig then Director AIIMS. Our liking for each other was instantaneous and the bond carried throughout.
I joined as adhoc Assistant Professor in June'65. There was one office of Dr. Baldev Singh in which in addition to Dr. P. N. Tandon another chair and a small table was put for me. The process of starting a department began really from scratch. Space was allotted on the first floor by the side of anatomy lecture theatre. I and Dr. V. Virmani (my opposite number in Neurology) sat down to draw maps and carve out rooms in the large halls. At that moment, our vibes were bristly to say the least. Dr. Virmani was considerably senior in age plus she had known Dr. Baldev Singh since Amritsar days and she also held the trump card of being Punjabi speaking which was then the lingua franca of AIIMS. Over the years our relationship mellowed and we did develop mutual admiration and respect for each other. I hit upon the strategy in our dealings at that time of building the departments, of saying exactly opposite of what I wanted. Dr. Virmani would of course, reverse my suggestions much to my advantage. Today when I look back it all appears so childish. But then it was great fun. Slowly collecting items like pins, chairs, tables, almirahs and make real offices was a new challenge for which I was not trained. Anyway we built the office cubicles, laboratories and got the OPD on the 4th floor in ship shape. It was so gratifying after two years of joining that we had a place of our own.
We started with surgical instruments which actually were of World War II vintage which included an operation table. Burr holes had to be made by a brace in 4 stages and both Dr. Tandon and I developed the art to perfection. To begin with we had no beds. Both for Neurology and Neurosurgery, Prof. K.L. Wig and the Pediatricians generously allowed us use of their beds in what is now the nurses hostel. There was so little clinical work that it was terribly frustrating in the beginning. I started taking clinics for the MD students of medicine, pediatrics and radiology. I slowly became quite popular to the extent that one day Dr. Wig called me to see one of his patients in his office. I must have impressed him no end as after that on several occasions he would ask for my opinion on patients. This was a small matter for him but a great boost for my confidence for which my gratitude goes to him.
By 1968 we were having a ward in the OPD block (ward IX) and we were well settled. The operation theaters were in the College of Nursing Block. Radiology to begin with was in the nurses hostel, and only in 1968 shifted to its present location. That was the time when we had Dr. S. K. Ghosh in radiology from 1965 to 1968 and he was a great help. Very often we started the day at 7.30 A.M. with ward rounds, dressings and stitch removals, followed by neuroradiology (ventriculograms angiograms etc) and then this was followed by surgery which would invariably end by 7 or 8 P.M., particularly if it was a posterior fossa tumour. At night one of us i.e. PNT or myself would sleep in the doctors room adjacent to the main O.T. block. From 1966 onwards Dr. B.B. Sawhney and Dr. M. Gourie Devi, now Director and Vice Chancellor NIMHANS who were residents in neurology would help us out by doing night duties and also assist in surgery as we did not have regular residents of our own. The role played by Col. G.C. Tandon, the Professor of Anaesthesia, was unforgettable. Dr. Hattangdi's lectures in anaesthesia helped us enormously and he also shared our burden in looking after patients, sometimes relieving us of our daily chores. The two films I saw with Anjali, my wife, during the time was courtesy of Hattangadi. Before I proceed I must tell of my first day in the operation theatre block (MOT) in the consultants changing room, where I went on my own apprehensively, to discover its ambience. The only person there in OT dress was reading an Agatha Christie paperback with great seriousness. On entering he asked me as to who I was and then got up with great cordiality and shook me by the hands. That was Dr. Satish Nayyar, Assistant Professor in Surgery well known as he was a Hallet medalist in the primary FRCS examination. Dr. Satish Nayyar gave me a cup of tea and then said that I must cultivate some hobby (his was reading mystery novels) as Assistant Professors had nothing to do as the Professor usurped all the work which was worthwhile, while all the minor work was done by the Registrars (later called residents). I went into depression from which it took me a long time to come out. Within a week I took courage in my hands and went to talk it over with PNT. We decided that alternate cases would be operated by us while the other would assist. Matters went on well but I was perturbed over the fact that if he assisted, he would go out and talk to the patients attendants before I could come out. Again I went to him in 1968 and PNT graciously agreed he wouldn't do so. This was a remarkable thing at AIIMS. My struggle for identity of Assistant Professors went on to the faculty over such oligarchy and it was ultimately in 1970 that I was able to change the nomenclature of hospital units which hitherto were identified with the head, to that of the departments. Thus Prof. P.N.T's unit changed to Neurosurgery unit-a practice which continues today. I have always felt that to obtain the best from colleagues a measure of democracy and participation should be the prime substance PNT's contribution towards this was immense which allowed me to put my heart and soul in developing the department and later the Neurosciences Centre. I guess the role of wives is also very great. Our families (Tandon and Banerji) were close to each other and even today no major decision in the Banerji family takes place without Tandons consultation. I guess this meeting was lucky for both of us.
In 1969 Dr. S.K. Ghosh left for Goa on promotion as Professor and Neuroradiology was taken over by Dr. R.K. Goulatia for whom a separate post was created in neuroradiology. In mid 70's Dr. S.S. Saini was persuaded to join Neuroanaesthesia and this started the nucleus of a comprehensive clinical setup. Fortunately we were able to persuade (Mrs. D. Saini to join as our OT sister incharge and thus there was a feeling of family and belonging, so important in the development phases of any new venture. Dr. Subimal Roy was spending considerable time in Neuropathology to complete the picture. I had a vision of Neurosciences Centre akin to PNT, however I knew that basic neurosciences can never develop on its own because of economic compulsions. My emphasis was on developing clinical neurosciences and bring in basic neurosciences within its umbrella.
By mid 70's both neurosurgery and neurology had relocated itself on the main hospitals 4th floor and we were lucky to have separate independent wards. Mrs. M. Bindra joined us as sister I/C of neurosurgery ward and her dedication eventually made our ward the talking point of nursing care in the Institute. She eventually rose to become the Nursing Superintendent of the Neurosciences Centre.
In 1966 one day, walked into my office Dr. Brahm Prakash, who had resigned his Short Service Commission in the army and had married recently. He was at loose ends, asking my advise as to what he should do. He had earlier worked as my junior resident in general surgery at Medical College, Lucknow and the association was about 10 yrs. old. I persuaded him to join neurosurgery. We were able to rustle up the required formalities for starting MCh course with bare facilities but boundless enthusiasm. He was the first trainee and later joined our faculty and went on to become the Director Professor at G.B. Pant Hospital and started his own MCh programme. The AlIMS MCh course went from strength to strength and eventually we were having both the 5 yr and 3 yr streams. Neurology D.M. had started already in 1965. Now AlIMS trainees are spread all over India. Several headed departments e.g? Dr. Gourie Devi became Director Vice Chancellor of NIMHANS, Dr. B. Prakash at G.B. Pant Hospital Delhi, Dr. B.S. Das at NIMHANS, Dr. S. Mohanty at IMS, BHU Varanasi, Dr. A. K. Reddy at NIMS Hyderabad, and Dr. M.A. Wani at SKIMS Srinagar. Many hold important positions in teaching as well as private sector. We i.e. PNT and I are inordinately proud of all who trained themselves with us and wish them all the best in their future endeavors. Our wish is that they better us in their achievements. A major breakthrough in our clinical services occurred in 1976 with the coming of Prof. H.W. Pia who did a course in laboratory microsurgery. In the next few years we started a microsurgery laboratory and operative microsurgery was initiated. In the Indian scenario we stole the lead. In late 60's with the help of our ENT surgeon Dr. S.K. Kacker we started trans-sphenoidal pituitary surgery which consolidated in the 70's and became a routine procedure.
The process of development of the Neurosciences Centre in collaboration with the Cardiothoracic Sciences Centre started in real earnest in early 70's. Dr. N. Gopinath of Cardiothoracic Surgery and PNT were the architects. Land allocation was done by Prof. V. Ramalingaswami, the then Director AIIMS. Ghosh and Pradhan Associates were appointed architects and their started the planning for the basement, ground floor and the operation theatre block of our centre. Hours and hours of meetings with the architects-designing and tearing plans, it went on and on. I heard my wife say that I started talking of planning even in my sleep. We were about ready to have the foundation stone laying. This was 1977 and Mrs. Indira Gandhi's infamous emergency was coming to an end. One afternoon, in PNT's office, Dr. N. Gopinath suddenly said it would be nice to have Mrs. Gandhi lay the foundation stone. I had recently treated Mr. Dhawan's (then the personal secretary to Mrs. Indira Gandhi) nephew and I said shall I try. I rang him up on the phone from PNTs office. Mr. Dhawan immediately said yes and wanted probable days and times so that it could be confirmed taking into account Mrs. Gandhi's tour programmes. Elections were round the corner and Dr. Ramalingaswami wisely asked us to go slow. Mrs. Gandhi lost the elections and it is possible that the Janata Government which followed may have taken offence and delayed the start of the Centre had we got Mrs.lndira Gandhi to lay our foundation stone. Eventually, President Mr.Neelam Sanjeeva Reddy lay the foundation stone in 1978. When the building started many problems surfaced e.g. we suddenly discovered that there were very few toilets while most of the patients of cardiology were on diuretics and required use of toilets frequently. Again to the drawing boardbreaking of walls, laying of new sewer lines and so new toilets came into being. I know the OPD and of course the toilets have today become too inadequate with increasing number of patients coming to the Centre.
The brief period of Janata regime from 1977 and 1979 saw the irrepressible Mr. Raj Narain come as the Health Minister. All work in the Ministry came to a halt as also our Centre which bore the backlash of erratic ways of Mr. Raj Narain. The only thing I remember was meeting him near the present Community Medicine Department late in the evening, Mr. Raj Narain was coming to inaugurate, if I remember correctly, the Centre of Community Medicine. As usual he was hours late and the then Director Dr. L.P. Agarwal was standing with 3to4 faculty members. I tried slinking away but Dr. L.P. Agarwal called me and more or less forced me to stay on awaiting Mr. Raj Narain. He eventually came when the numbers of people waiting was not more than half a dozen. Before going to cut the ribbon he was introduced to all of us. He was highly intrigued with me and asked what would I find if I did have an opportunity to see the inside of the head of Mrs. Indira Gandhi. I made some polite comments though I was sure Mrs. Gandhi had a better quality brain than Mr. Raj Narain. Anyway he went on to narrate it with great gusto during a special convocation to award an Honorary D. Litt to Dr. Sewoosagar Ramgoolam of Mauritius. It was in such bad taste that Morarji Desai who was chairing frowned and all of us in the auditorium hung our head with embarrassment.
My two stints as Chief of Neurosciences Centre were significant in the development of the Centre. The first was a 2 year term as acting Chief of Centre while Dr. PNT was on Nehru Fellowship between 1984-86. This was the time when after the first phase of building (OPD, radiology wing, basement and OT block) we had reached a dead end as far as expansion of the Centre was concerned. Prof. M. L. Bhatia was the Chief of Cardiothoracie Sciences Centre. Our formal requests for funds were stiffly rebuffed by the then Joint Secretary Finance Adviser (JSFA) of Health Ministry. Ms. Sarla Grewal, widely nick named 'hunterwali' by her unkind colleagues, was the Secretary. We were advised not to try and influence her which could cause an unpredictable antagonism to our proposal. Anyway we went to meet her, placed before her, the developments till date, including our mounting clinical load, increasing public expectations, and the blockades experienced by us for expanding our Centres to what was originally planned. Ms. Grewal quietly listened to us, occasionally interjecting for a clarification. After we completed she asked for the JSFA who was the main stumbling block, to come and join the meeting. The moment he saw us his hackles were raised. On being asked by Ms.Grewal as to what were the problems in giving us the grant he started off with a long list of financial mismanagement by AlIMS in which our Centres had no role to play. (Most of the problems recounted were exaggerated to say the least). Ms. Grewal asked as to why our Centres were being penalised for what AlIMS had done. To this the JSFA said that this is a part of financial management for which he was responsible. Then we saw the legendary Ms. Sarla Grewal come into her elements. In chaste Punjabi she asked the JSFA as to who was the Secretary of the Ministry and how dare he speak to her like that. The poor JSFA spluttered and stuttered and tried to put in a word edgeways. Ms. Grewal asked him to leave the office and we knew that our battle was half won. However after leaving her office both Prof. M.L. Bhatia and I, as a matter of diplomacy, went to the JSFA's office. He was in the dumps. We nursed his hurt ego by asking for his help as we knew that he was quite capable of going to the Finance (Expenditure) Secretary and derail our proposals. I think the strategy worked as he did become a supporter. Of course things were helped as a few close relations of the JSFA fell conveniently ill at the same time requiring cardiac and neurosurgery. Funds eventually came though it took another year and in 1986 the remainder of the present Centre's building was started. Prof. P. Venugopal was a constant source of support in our endeavours. In the same period the next Union Health Secretary was Mr. Srinivasan, who was unenthusiastic about our Centres. His general impression was that we were overstaffed, our equipment underutilized and our clinical output low compared to other hospitals e.g. G. B. Pant Hospital Delhi, Christian Medical College Vellore, and certainly Apollo Hospital Madras which to him was the ultimate in financial management and output. Incidentally he was involved with the starting of Escorts Heart Institute which he clearly told us is a 'better bet than us'. Prof. Bhatia, Venugopal and I went through our records as well as what we could gather from the other institutions which Mr. Srinivasan thought had better quality and quantity of work. He had a meeting separately with our Neurosciences group to take stock. I had taken Dr. Baldev Singh and Dr. P.N. Tandon for the presentation made by me. By the end Mr. Srinivasan was convinced of the genuineness of our proposals. My plea at that time was to get financial grant equal to G.B. Pant Hospital whose output was half of ours. It was a landmark victory as our grants immediately increased, a trend which continued in the future.
My next stint as Chief of Centre was between 1988-95. Finances were forthcoming in good measure We had a CT scan and state of art angiography equipment. Our ICU was the best in the country. What we lacked was a MRI Scanner. I must pay special thanks to Mr. R.L. Mishra who was the Union Health Secretary in the latter part of my assignment. We had an excellent relationship and he was always positive in his approach. It is through his help that we got the NMR department setup at AIIMS, which was far more than merely obtaining MRI equipment. Incidentally even today the NMR Department has the only 2 Tesla machine capable of MR Scan and also MR Spectroscopy. The NMR department also has chemical NMR and the only experimental NMR in India today. It was an unique experience to create a whole department with the help of the then director Dr. S. K. Kacker who was always supportive.
It is during my tenure that proposals were sent to the Government for making the Centre the best equipped not only in India but in the Asian region. The Gamma Knife has started after I retired and I am sure PET scan and other newer equipment would come in due course.
I am often asked as to whether I have any regrets. My special regret is our offices being removed from the main Institute. It was originally envisaged that offices would remain where they were located i.e., adjacent to Anatomy dissection hall. The translocation has severed the umbilical cord to the other specialties in the Institute. This isolation does not augur well for the future of our Centre, as any branch of medicine to flourish requires interaction with sister disciplines. My other regret is the inability to have nonclinical neurosciences to come and establish themselves in our Centers new building. I had tried, even to the extent of keeping a floor vacant for one year under various pretexts.
My greatest gains were the colleagues I had - friends for life. I know I left alive vibrant active Centre which will only grow from strength to strength. Even today for anything I always say Neurosciences Centre, AIIMS is the best and with every breath only wish it the very best in its future endeavors.”
“The Departments of Neurology and Neurosurgery at the All India Institute of Medical Sciences were initiated in March 1965 with the appointment of Prof. Baldev Singh and myself as the first Professors. A neurology service in the Department of Medicine started by Dr. Jim Austin from the USA and later under care of Dr. Vimla Virmani was already in existence at that time. Significantly enough the Institute was, from its very inception, an important centre of neuroscience research. The first two Professors in Department of Physiology (Prof. B.K. Anand and Prof. A.S. Paintal) were undisputable leaders of neurophysiology in the country. Dr. Paintal had, however, already moved to Patel Chest Institute a year earlier, the remaining faculty members of the department were all pursuing neurophysiology research. Prof. Keswani, the Chief of Anatomy, was primarily interested in neuroanatomy. Prof. G. P. Talwar, at that stage, was enthusiastically involved in researches in neurochemistry This was of course before his shift to immunology. Acknowledging these strengths International Brain Research Organization (IBRO) had already held one of its earlier workshops in the Institute. Dr. Sriramachari, Deputy Director of Indian Council of Medical Research, though not on the faculty of the Institute freely provided his services for all neuropathological work till several years later when Dr. Subimal Roy took over the responsibility fully. While clinical neurology and neurosurgery departments existed at several centers in the country much earlier; even the oldest such centers at Vellore, Madras, Bombay and Calcutta, did not have such broad base of neuroscience as we were fortunate to have at the Institute. Given the overall milieu of rapid growth and development in the institute at that time, the clinical departments also expanded rapidly. It will be hard for the current staff and students of the Institute to visualize how close interaction existed among all these departments and units in the earlier years. This was in no small measure due to the all pervading influence of Prof. Baldev Singh real father figure for all of us.
The idea of establishing a "Brain Research Centre" at the Institute had already been envisaged by Prof. B.K. Anand even before the clinical departments came into existence. No doubt this was primarily thought of as a basic research centre. Thus on 1st December 1964, Dr. Anand vide his letter No. Phy/64/1235 requested the Director for initiating steps for developing a Brain Research Centre" with the existing ICMR Neurophysiology unit as its nucleus. Unfortunately no action was taken on his request.
In 1968, when the Institute was to formulate its development plans for the Fourth Five Year plan of the Government, Prof. Anand, Prof. Baldev Singh and I had several informal discussions to once again revive the proposal for a Brain Research Centre. It may be mentioned that, not surprisingly, this proposal was heavily loaded in favour of creating research laboratories including a couple for neurology and neurosurgery. While we were heavily constrained in our clinical work due to limited diagnostic and operative facilities at this time we went along with Prof. Anand in supporting this proposal hoping to strengthen the patient care services through the development plan for the Institute hospital which was to be commissioned
The Development Committee approved the proposal in principle, but owing to financial constraints no concrete steps were taken. The Institute Body ultimately agreed to create a few staff positions so that "Centre can make a start as early as the Financial Year 1970/71. In practical terms it amounted to absorbing some of the staff of the Indian Council of Medical Research Neurophysiology Unit and nothing more.
When we finally shifted to the new hospital the Neurosurgery Department had 22 beds allotted to it. We had one operation theatre, but no specialized neurosurgical operation table and no intensive care unit. The neuroradiology set up consisted of a skull table without automatic changer for angiography, no facilities for tomography nor a dedicated unit for myelography. Isotope encephalometry then a routine diagnostic investigation abroad was nonexistent. We had an EEG machine but no facilities for EMG or nerve conduction. Nonetheless we were facing increasing demands for patient care from all over the country and also our neighboring countries. Waiting lists for admission and surgery were a constant source of worry for us and frustration for the suffering patients. We had already started the M. Ch. course.
Similar problems were being faced by the Cardiology and Cardiothoracic Surgery Departments. One day in 1971 when Prof. Gopinath and I were scrubbing for surgery in the common scrub room between our two theatres, he informed me that they have submitted a proposal for a Cardiothoracic Centre "Why don't you also do so, otherwise we will never progress". I, therefore, once again took up this matter with Prof. Anand who was now also the Dean and sounded the Director, Prof. V. Ramalingaswami. On receiving a favorable response, it was decided that, unlike in the past, our proposal this time should be a comprehensive one, including parallel development of basic neurosciences and clinical disciplines. Dr. Manchanda along with Prof. Anand formulated the proposal in respect to basic neurosciences. I, in consultation with Prof. Sumedha Pathak, the then Professor and Head of Department of Neurology and on the advice of Prof. Baldev Singh and Dr. Banerji prepared the plan for the clinical centre. A draft proposal was thus submitted on 16`" July 1971 to the Dean with the comments "in view of the present extent of development at the Institute to start with emphasis will be on neurophysiology, neurology and neurosurgery. Nucleus for the following will be established with a view to development of these into fully fledged specialties, as integral part of the centre, as personnel and fiscal resources were available". These included neuroanatomy, neurochemistry, neuropathology. This proposal was discussed by Prof. Baldev Singh (who was now an Emeritus Professor) with Prof. B.K. Anand who agreed with it fully and desired to "go ahead and fill up all the details regarding space, equipment, personnel etc. working out the cost" etc. We agreed to change the name from Brain Research Centre to Neurosciences Centre. We had a detailed and somewhat ambitious plan formulated. Though the plans were ready there was no obvious source for funding it. Was it going to be another document for the archives? This thought remained a constant worry, Prof. Ramalingaswami was fully in agreement but was finding it difficult to find funds for it.
Several months passed. One day while casually discussing our mounting frustrations with lack of any progress with my elder brother, who was then a Jt. Secretary in the Prime Minister's office, I initially got a cautious reply, "Prakash, officially I do not wish to get involved in any thing that may be considered as a favour to my brother. The only thing I can do is to arrange a meeting for you with the PS to the Hon'ble Minister of Health Shri Uma Shanker Dixit. Even before that, first take the permission from your Director to do so". It was easy to obtain Director's permission and shortly afterwards a meeting was held with Shri Rajgopal, who was more than sympathetic to our request for establishing the Neurosciences Centre. At the end of the meeting he told me that it was not possible to get such a major scheme funded in the middle of a plan period but "may be we could get advanced action initiated which can then be formalized in the next plan". He promised to discuss this with Dixitji at an appropriate time. The meeting ended with encouraging but cautious note, "I promise nothing but I am convinced it is a genuine need. You are asking nothing for yourself? you are willing to provide more and better service to those knocking at your door".
Not expecting any prompt action I was pleasantly surprised to receive a call from the Director later that evening, "Health Secretary Shri K.K. Dass wants us to include the matter related to the establishment of the Neurosciences Centre in the agenda for the next meeting of the Institute Body due shortly. He wants a copy of the proposal sent to him in advance". On 2nd August 1972, a copy of the formal proposal was duly sent to the Shri K.K. Dass by the Director. At the Institute Body meeting held on 12'" September 1972, the Institute decided, "The Institute considered that it was fortunate that expertise in several fields of Neurosciences exists at the institute both in basic and clinical areas. The Institute considered the scheme put up for its consideration as possible, desirable and in the larger interests of the country. Recognizing the strengths already built in the various departments in respect of the neurosciences, the Institute approved the proposal in principle to set up a Centre for Neurological Sciences at the AIIMS and decided that not only it be included in the proposals for the Fifth Five year Plan of the AIIMS but, the possibility of advance action in the Fourth Five Year Plan itself, should also be seriously explored. It was accordingly decided that the matter be considered by the Finance Committee in greater detail". We felt happy but not jubilant, fully conscious of the harder battles ahead
The Proposal was duly put up to the Finance Committee meetings held on 4th January 1973, 8th February 1973 and 5th April 1973 and as feared owing to "financial constraints" no funds could be made available. The real reason was no doubt that Shri K.K. Dass had retired by now and his successor Shri Ramachandran had his own antipathies against the Institute as future events confirmed.
However, without waiting for a formal decision of the Finance Committee, Prof. Ramalingaswami forwarded the proposal to Dr. Banwari Lall, Chief, Health Division, Planning Commission for his consideration. Dr. Lail was a close friend of Prof. Anand who arranged a meeting with him in the Planning Commission after Dr. Lall had opportunity to scrutinize the proposal. With high hopes Prof. Anand and I attended the meeting. To our surprise Dr. Lall, after a brief discussion, said, "Bal (B.K. Anand), I am sorry this proposal as it stands is unlikely to be approved owing to severe financial constraints. The only component that may be favorably looked at is the patient care part". He also made several suggestions for curtailing the budgetary demands even for the clinical component. It was with a sense of disappointment that we walked out of his office. I was, in addition assailed with the fear of losing Prof. Anand's interest and support for the project. Probably sensing my thoughts, on our way to the exit he suddenly stopped said, "Prakash, it is too bad to have things take a turn this way, but let us be practical. We should take whatever we can get and keep trying for the rest. You will have my full support". Few in his place could have been so generous and even more so the enthusiastic support we continued to get from him later on provided enough proof of the genuineness of these sentiments. For all this he no doubt, got the flak of his colleagues in the Physiology Department.
In pursuance of the decision of the Institute Body and the informal advice received from Dr. Lall we carried out another detailed exercise to draft a formal EFC (Expenditure Finance Committee) memo. In the meanwhile Prof. Gopinath had carried out a similar exercise for the Cardio-thoracic Centre. As a matter of fact, these exercises were mostly done with the constant consultations with each other. Combined these two proposals required considerable financial support. Dr. Ramalingaswami advised us that we should seek the views of the new Health Minister Shri Khadilkar. After a patient hearing of our individual proposals, he pointed out the difficult financial situation and advised that we should try and economize by establishing some common facilities and sharing whatever can be shared thus bringing down the total cost of two proposals. He promised to get the demands included in the Fifth Five Year Plan proposals of the Institute. Thus Prof. Gopinath and I carried out another exercise maintaining the basic character of two independent centers, yet having some common areas and support laboratories. On 2nd August 1973, a new draft proposal was forwarded to the Director with a note, "In view of the difficult economics situation, we (Profs. Anand, Gopinath and Tandon) have also reviewed the projects with an idea to prune these without undue detriment to the utility of the projects". And further, "Following this review, if we could get a total of Rs. 350 lakhs (Rs. 200 lakhs for Cardiothoracic and Rs. 150 lacs for Neurosciences Centre), we could still make a worthwhile contribution".
The Planning Commission, discussed the proposals of the Health Ministry (which included those of AIIMS) on 31st August 1973. The bias of the Health Secretary, Shri Ramachandran against the institute was too obvious. He had proposed a total of Rs. 150 lakhs for the whole Institute. As a matter of fact it was specially emphasized that the Ministry "did not favor that all the specialties should be concentrated in one place in the country". Following strong pleadings by the Director, one of the members of the Planning Commission, Member (M), pointed out that "the Ministry had proposed Rs. 1.50 crores for the AlIMS as against the Fourth Plan provision of Rs. 3.33 crores, and since this was a premier Institute in the country, the Ministry may explore the possibility of providing some additional funds for the Fifth Five Year Plan. With regards to the proposals for the two centers, the Planning Commission ultimately decided to allocate separate funds for "the development of super-specialties: a total of 236 lakhs, without specifically mentioning our proposals. This was a typical bureaucratic stroke by the Health Secretary to scuttle our proposal. Before implementing the program, the Ministry of Health decided to enquire from all medical institutions in the country to submit their proposals for "development of super-specialties", notwithstanding the fact that the Central Government is supposed to directly fund only the national institutes. As expected proposals were received from several places and interestingly even Orthopaedics was considered a super-specialty. The Health Ministry, obviously under the instructions from its Secretary put the whole matter in the cold storage with the usual excuse, "the matter is under consideration": even though the Fifth Plan had already begun from April 1974.
One day Dr. Karan Singh, who was now the Minister of Health, desired to see me for some unconnected reason. At the end of our meeting, I enquired about our proposals for the centers. Only then the cat came out of the bag. He frankly informed me that the Secretary was sitting on the file on the excuse of collecting information mentioned above. Dr. Karan Singh recognized the futility of the exercise. Since in the limited funds allocated for super specialities it would be impossible to meet the needs of even a few. He promptly took the initiative and in August 1974 appointed a committee under the Chairmanship of Dr. Srivastava, the Director General Health Services, to assess the existing potentials and future possibilities of strengthening superspecialities in the centrally funded institutions only. The Committee included experts in the concerned disciplines from all over the country. It collected the necessary information from various institutions and finally paid site-visits to each of these before recommending our two proposals alongwith some allocations to a couple of others. Thus from a total of Rs. 236 lacs allocation for super specialities the two Centres at the AIIMS, was provided Rs. 188.37 lacs.
On March 26, 1975, even before we received a formal approval of the Government to establish the Centre, a letter addressed to the Director, AlIMS received from Dr. Sharad Kumar, DDG(M), indicating that, "Under the Purely Central Scheme of "Development of Superspecialities', the Government of India has sanctioned a provision of Rs. 10 lakhs for the development of the Departments of (1) Neurosurgery and Neurology; and (2) Cardiology and Cardiothoracic Surgery...............”
This communication, though not mentioning anything about the Centers, was the first indication that the Government had selected AIIMS; for development of these super-specialties. Two weeks later on 11th April 1975, the recommendations of the "Expert Committee on Establishment of Cardiothoracic and Neurosciences Centre at the Institute", were ultimately received, setting at rest all uncertainties about the two proposals. It would be worth reproducing the extracts of this communication with respect to Neurosciences Centre (see Dr. Sharad Kumar's letter dated 11th April 1975). Shortly afterwards on 22"d July 1975 a formal letter from the Ministry of Health and F.W. No. V. 16020/54/ME (PG), communicated to the Institute an allocation of Rs. 188.37 lacs for the super-specialties (including both centers) for the 5th Five Year Plan. It needs to be recorded that the fullest understanding between Prof. Gopinath and myself and the cooperation of the rest of the faculty of the concerned departments made it possible for us to keep on revising and redrafting the proposals as per the bureaucratic needs of the Government, without sacrificing the basic objectives. No hidden rivalries, personal egos or unjustified interests of individuals ever cast any shadow as we pursued the planning and implementation of the projects through various administrative channels. For me it was a rare experience of trust and camaraderie not so common in our institutions.
As expected it was not smooth sailing from now onwards. We had to wait till March 1976 for the first release of funds, a paltry sum of Rs. 3 lacs. At one stage the Financial Advisor to Ministry of Health, whose main grudge against the Institute happened to be "misuse of funds for erecting black marble columns in the foyer" without any justification reduced the total allocation for the Fifth Plan by nearly Rs. 40 lacs, probably worrying that we would waste it on black marble columns. When no explanation and assurances from Dr. Gopinath and myself failed to convince him, we had to approach the office of the Finance Minister (Shri C. Subrramanayam) and the Planning Commission Deputy Chairman Shri P.N. Haksar, two of the most progressive policy makers of the country has known. Let me hasten to add that Prof. Gopinath and I approached them with the approval of our Director.
In July 1976, the Estate Committee formally appointed M/s. Pradhan Ghosh and Associates as the architects. However, between 1976 and 1978 repeated revisions of the building plan were required due to pruning of the budget allocations and rising cost of the building. At last on 14th April 1978, the President of India Shri Neelam Sanjiva Reddy laid the foundation stone of the twin centers. In his welcome address Dr. Ramalingaswami stated, "Our vision of the Centers is that they will be Centers both of public service and of higher learning at the same time". Their philosophy is that in which the patients and their needs come first, everything else is subordinate and subservient to this: He pointed out that, "The greatest and deepest need of a Centre is to be needed by Society". Quoting the famous economist Francis Delaisi, he said that. "the purpose of an Institution is to supply stability needed for long term operations. At the same time, Institutions must be able to adjust to change. It is our hope that stability, adjustability and continuity will mix in the centers in appropriate balance". Rashtrapatiji in his address expressed his happiness on the establishment of these Centers. While emphasizing that, "Our most urgent need is Primary Health Care" which should be pursued with all energy and resources at our command." He pointed out that, "we cannot altogether neglect the setting up and improvement of more advanced levels of health care at District, State and national levels. We need to have a few Centers of excellence in a large country like ours where the most advanced levels of care can be provided; specialists and researchers can be trained and the most complex problems may be referred for appropriate management" For him, "It is not a question of this or that" but a "proper balance in the developments of these various levels of health care". He was equally concerned about the scientific community which must be able to discover, adopt and innovate suitable methods not only in dealing with our current problems but also in coping with changing trends and changing needs of the future". I have quoted these excerpts from the speeches because I believe that as long as we pursue these ideals the Centre would continue to justify the generous resources provided by the government and enjoy the trust of the people.
Five years later, in March 1983, out patient clinics for Neurology, Neurosurgery (as also Cardiology and Cardiothoracic Surgery) moved to the new building, while the work continued to complete the rest. Progressively as the work progressed we continued to occupy the areas already completed. By July 1984, the built up area included basement, OPD, receiving station, noninvasive laboratories, radiology wing, 8 operation theatres (Neuro 3, Cardiac 4, Common 1) along with ICUs and postoperative wards. It was only in 1988-89 that the Centres became fully functional in their new abode. At this time Neurosciences centre had a total of 180 beds, 3 fully equipped operation theatres, 30 bedded ICUs, Intermediate care wards, fully fledged departments of Neuroradiology, Neuroanaesthesia, within this complex. The offices of the faculty and supportive staff, Neurochemistry laboratories continued to remain in the old building and by mutual agreement the Neuropathology still continues to be in parent Department of Pathology. This may be compared to the facilities available to us before we moved to the Centre. The combined strength of beds for Neurology and Neurosurgery including a half baked ICU was only 72, scattered in different parts of the old hospital.
There was only one dedicated operation theatre for neurosurgery and we shared another one with Cardiothoracic Department three days a week. There were four members on the faculty of Neurosurgery. I have been informed that there will be separate write-up's about the development of Neurology, Neuroradiology, Neuroanaesthesia, Neuropathology, Neurochemistry etc. hence I shall restrict myself in the remaining part of this review on Neurosurgery only. Nonetheless it should be mentioned that once the scheme for creating the Centre was approved, in the interval before its complete occupation we were permitted to augment the overall facilities and staff strength in a progressive manner with a view to improve the quality and maximise output of all our activities-patient care service and education in particular. Funds for research had, as even now, to be obtained on competitive basis from the grant giving agencies. During this interval we were able to obtain a munificent grant from the Swedish International Development Agency (SIDA) which modernized our diagnostic and clinical facilities including those for operation theatres and ICU. The first CT Scan in the country was installed under this grant. It was not just a coincidence that this was inaugurated by the President of India on the same day as the foundation of the Centre(s) was laid.
Coming back to the growth of neurosurgical services, in the first full year of our work i.e. 1966 we admitted 140 patients, attended to 540 in the OPD and performed 111 major and 89 minor surgical procedures. It may be mentioned that at that time many of our patients were admitted, operated upon and discharged from the emergency ward. Five years later in 1971 these numbers were 422 admitted, 1044 attended in OPD and 535 (303 major and 232 minor operations performed. In 1976, the year when the first token grant was received for the Centre we admitted 1094 patients, attended to 3784 (1960 new and 1824 old) patients in the OPD, and performed 520 major and 785 minor surgical operations. It may be recalled that at that time neuroradiological investigations pneumoencephalography ventriculography, angiography and myelography were performed by. the clinical team and hence were included as minor operations. In 1986, prior to shifting to the Centre 1898 patients were admitted, 11.225 (3406 new and 7918 old) patients seen in the OPD and 735 and 257 major or minor operations were performed. Starting with only two faculty members in 1965 - Dr. Banerji and myself, it was only in 1971 that we added one more lecturer. Dr B. Prakash. The next person to join was Dr R. Bhatia as Lecturer in 1974 The first faculty position in the Department of Neurosurgery after the Centre came into existence, was 1979 with Dr. Banerji taking over as a Professor. A little known episode in this connection needs mention to illustrate the prevailing team spirit at that time. When we got the first position of a Professor sanctioned for the Centre, I had in my mind wanted it for Dr. Banerji. The day the matter was to be finalized in the Academic Committee I was indisposed and requested Dr. Banerji to attend the meeting and briefed him about my plan. His immediate response was that it should be alloted to Neuropathology, "Dr. Subimal Roy should be given a chance before me". Dr. V.S. Mehta then joined as a Lecturer in 1981 followed by Dr. A.K. Mahapatra in 1983. In the meanwhile Dr. B. Prakash left for G.B. Pant Hospital in 1980. Thus even after fully commissioning the Centre in 1988, the Department had a total strength of 5 faculty members; who continued to share the ever increasing service load as indicated by the figures provided above.
Besides the full fledged in-service M.Ch. course (3 years for post MS (surgery) and a direct 5+1 year after MBBS), the department has been participating in undergraduate education as well as collaborating with basic science department for Ph.D. program. From 1968 when our first trainee obtained his M.Ch. degree, till 1988, twenty eight persons obtained their postgraduate degrees. Since 1988 up to date an additional 31 have qualified. Most of these are serving the country. Several of them became chiefs of their departments at Delhi, Varanasi, Srinagar, Bangalore, Cuttack and Hyderabad, thus fulfilling an important objective for which the Centre was created. From its inception the Department has been actively engaged in CME programs both intramural and extramural. Short-term training programs are organized regularly on recent advances like CT scanning, Microsurgery, Neural Transplantation, Vascular Surgery, Skull base surgery etc. An yearly course on Neurobiology for Clinicians was organized (4 at the AIIMS and 1 at NIMHANS, Bangalore). National level Hands-on Workshops were organized from time to time with the help of international faculty as for example on microneurosurgery, skull-base surgery, neural transplantation etc. A microneurosurgical laboratory, the first of its kind in the country, was established for training in microsurgical techniques, not only for neurosurgeons but for others specialities also from all over the country. The first National Neural Transplantation Facility was established in collaboration with the Department of Anatomy. The first Text Book of Neurosurgery in the country was the result of a joint effort between Madras Neurological Institute and AlIMS in 1980. This has been completely revised and updated in 1996. Four monographs "Lectures in neurobiology" were brought out in collaboration with the Department of Anatomy, AIIMS. The faculty has made contributions to several national and international text books including Tropical Neurology, Handbook of Neurology and Techniques in Neurosurgery.
AlIMS provided a unique milieu for advancing frontiers of knowledge. The Neurosurgery Department fully participated in this effort The major areas of research contributions of the Department involved collaboration of other departments in the Institute and outside included;
The above account will testify that much has been accomplished, no doubt a lot more needs to be. For me personally it has been a rewarding experience and source of great satisfaction, not just the physical growth of the Centre but the years of affection and friendship of the team who really made this happen. The only regret that continues to haunt me is our failure to see a parallel growth of the basic neurosciences as an integral part of the Neurosciences Centre. Individually these disciplines in the Institute have made very outstanding contributions. It has been stated that an institution is the lengthened shadow of an individual. If there is one example to disprove this adage, the Neurosciences Centre is one. It was born in the dreams of several, nurtured with the selfless, dedicated services of many who submerged their egoes for a cause greater than themselves, working as a team the parallel of which could hardly be found any where. In the true spirit of Gita, their sole concern was duty and not the reward. No sacrifice was great enough for establishing a centre of excellence. Posterity will judge whether they succeeded on not but no one would deny that they attempted. Unlike many other such centres in our country, even after the departure of those who initiated it, the Centre continues its journey to greater heights as will be obvious from the story told by those who succeeded. I hope and pray that the Centre will continue to live up to the foundation stone. "In the ultimate analysis, it is not the budget, nor the number of staff positions that makes a truly great centre of public service and higher learning. It is the presence of thoughtful, imaginative, humanistic, loyal and devoted faculty and students that is vital". The Centre continues to be endowed with them and I can only wish them greater heights in years ahead.
Recommendations of The Committee on Establishment of Neurology and Neurosurgery Centre at the AIIMS and Safdarjang Complex
This Centre has been chosen for the following reasons :
The needs of this proposed Neuro-centre are indicated in Appendix I and may be seen to be economical and the minimum required.
This recommendation to make the neurology complex of the AlIMS and Safdarjang Hospital into a Neuro Centre is based on the following requirements.
The Committee has further observed that
Department of Neurosurgery started a humble beginning in March 1965, with only two faculty members and a few beds. However, with dedicated efforts and sincerity of Prof. P.N. Tandon and Prof. A.K. Banerji, M.Ch training program could be initiated in 1967, when Dr. Brahm Prakash joined as M.Ch. student. In the last 45 years, Department has made a long journey in training over 140 neurosurgeons. The training provided here is considered the best in the country, as evaluated by independent assessment system.
The department is a Mecca for Neurosurgical patient care in India. It is equipped with ultra-modern technology and equipments from time to time i.e. operating microscope, Laser, CUSA, Ultrasound, Intra-operative MRI, Gamma Knife and Image Guidance System, which are necessary to provide state of the art care at par with the best neurosurgical centers any where in the world. With a moderate beginning in 1965, when only 50 patients were operated upon, today we operate around 3000 cases annually at AIIMS. With the inception of Trauma Centre in 2007, where we deal with all types of cranio-spinal trauma, our department, in addition, operates around 1500 trauma cases annually. There are in addition over 250 patients treated with Gamma Knife Radiosurgery annually (Total number till date around3000).
The Department has always been in the forefront in the areas of research and academic activities. There has been research on evidence based clinical practice and laboratory based work. These include clinico-pathological research on head injury, neuro-tuberculosis, glioma, pituitary tumors, peripheral nerve and brachial plexus injury & intracranial aneurysms. Laboratory based studies include (a) Neural transplant was developed as a national facility by DST (1984-1990), (b) Evoked potentials as diagnostic and prognostic tool, (c) Study of genetic and molecular aspect of glioma, (d) Study of cerebral blood flow using SPECT scan in brain tumor, minor head injury and craniostenosis (e) Near infrared spectroscopy and (f) MR spectroscopy etc. The Department has participated in a large number of multi-centric studies at National and International levels.
Feelings of the architects of Neurosurgery AIIMS
(Content provider: Dr. Achal K Srivastava)
Neurology is one of the earliest super – specialty at the Institute. Dr. James Austin, a Neurologist from Oregon, USA started a nucleus of Neurology service in the department of Medicine in 1962-63. In 1965, Dr Sushila Nayar, then Union health minister, invited Prof. Baldev Singh (one of the founder members of NSI, Neurological Society of India) to start a department of Neurology at AIIMS. When Prof Baldev Singh (also called ‘father of neurology’ in India and lovingly called "Papa Neuron") moved to neurophysiology on his retirement, the department was headed by Dr S N Pathak and then by Dr Vimla Virmani in 1975. After Prof. Vimla Virmani, Prof. M C Maheshwari took charge of the department in 1978. The department was shifted to the Cardiothoracic and Neurosciences Centre in the year 1985. In the year 2001, Prof. M.Behari took over the mantle of leadership. She retired in June 2016. Prof Kameshwar Prasad became the head of the department in October 2013. He retired on 31st January 2019. Prof. MV Padma Srivastava took over the leadership on 1st February 2019. From its inception, the emphasis of the department has been on quality patient care, research and to achieve academic excellence. Though the department started with 25 in patient beds, now there are 75 beds including neurointensive care. Out patient services and inpatient care has been incessantly on the rise over the years. The department has tried to maintain impeccable record of comprehensive patient care, teaching and training of students as well as contribute significantly to the scientific literature in terms of research. The department actively pursues clinical care and research activities in the sub-specialities of Movement Disorders, Neuroinfections and immunology, Stroke, Intractable epilepsy, Neuro-muscular Disorders, Sleep, Headache, Dementia amongst others. The department is equipped with the latest modalities for the diagnosis and management of various neurological disorders. The department has been in the forefront of medical research since its formation and is renowned internationally for quality clinical and basic research, particularly in the field of stem cells, Parkinson’s disease, stroke, epilepsy, neuromuscular disorders, sleep and headache. Regular patient information programs and scientific deliberations are conducted by the department. The faculty of the department routinely participates in the public awareness programs on television, and radio etc. and are active in various national and international CME programs.
| Name | Designation |
|---|---|
| Dr. Chetan D.Patal | Professor & Head |
| Name | Designation |
|---|---|
| Dr. Aarti Vij | Professor |
| Name | Designation |
|---|---|
| Dr. Aarti Vij | Addl. Prof. |
| Name | Designation |
|---|---|
| Dr. Sujata Mohanty | Asstt. Prof. |
| S.No. | Name | Designation | |
|---|---|---|---|
| 1 | Dr R.Lakshmy | Professor | lakshmy_ram@yahoo.com Area of interest:
|
| Name | Designation | |
|---|---|---|
| Dr. A. K. BISOI | drakbisoi@gmail.com | Professor and Head of the Department(CTVS) |
| Dr. V.DEVAGOUROU | vdeva@hotmail.com | Professor (CTVS) |
| Dr. SACHIN TALWAR | sachintalwar@hotmail.com, drsachintalwar@gmail.com | Professor (CTVS) |
| Dr. P. RAJASHEKAR | praja@aiims.edu | Professor (CTVS) |
| Dr. MANOJ SAHU | drmanojsahu@gmail.com | Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SARVESH PAL SINGH | sarveshpalsingh@gmail.com | Additional Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr.P.RAMESH MENON | rpmpgi@gmail.com | Additional Professor Pediatrics (Neonatalogy) in CTVS |
| Dr. PRADEEP RAMAKRISHNAN | pradeep.r.reddy85@gmail.com | Associate Professor (CTVS) |
| Dr. UMMED SINGH | drusd@yahoo.com | Associate Professor (Cardiac Surgical Intensive Care under CTVS) |
| Dr. SUSHAMA GAYATRI B | sushama.gayatri@gmail.com | Assistant Professor (CTVS) |
| Dr. NAVNITA KISKU | navnita.kisku@gmail.com | Assistant Professor (CTVS) |
| Dr. AMITABH SATSANGI | indiactvs@gmail.com | Assistant Professor (CTVS) |
| Dr. MAYANK YADAV | drmayankctvs@gmail.com | Assistant Professor (CTVS) |
| Dr.BHARATH.V | drbharathv@gmail.com | Assistant Professor (CTVS) |
Professor
The faculty of the Department has been participating in Community health camps frequently.
अखिल भारतीय आयुर्विज्ञान संस्थान (एम्स)
अ. भ. आ. सं., नई दिल्ली-110029
टोल फ्री नंबर : 1800 116 117
टेलीफोन नंबर : 011-2658 9391, 011-2659 3677
ईमेल : npicaiims2010[at]gmail[dot]com

Focus areas of clinical care and research of the Department.
The department of Cardiac Anaesthesia maintains its records, duly catalogued indexed and computerized (Since Oct 2006) using SPSS software. The headings under which the records are categorized are as under:
These records are registered daily in operation theatre on a medical record sheet and register and also computerized. Annual report of department records is submitted annually.
The normal functioning of the department is according to the rules and regulations laid down by CN Centre, AIIMS. Seven Theatres function everyday with 2 or 3 cases in each theatre daily. One Emergency heart surgery may be taken up anytime in the day/night. One consultant and one or two seniors residents round the clock emergency duty for postoperative care of cardiac patients as well as intensive and ventilatory/resuscitative management in coronary care unit. One consultant on round the clock call for emergency operations. Anaesthesia is given for a total of 14-20 heart operations everyday with postop and coronary ventrilatory care. General anesthesia or monitored anaesthesia care is given in cath. Lab and computerized angiography and MRI in Cardiac patients.Two senior residents are on emergency call-attending calls from CCU, ICU, CTVS wards, Cath. Lab. and Operation Theatres. Bedside pre anaesthetic check up is done daily.
2 academic sessions held per week as part of department’s academic activity – where seminars/Tutorials/Journal Clubs/Examinations are held by faculty & residents. The department has access to the AIIMS Dr. B.B.Dixit Library and National Medical Library at all times. Internet access is available via computer facility in all consultant’s rooms.
The Department of Cardiology at AIIMS was established under the leadership of Prof. Sujoy B. Roy. The department has developed excellent facilities for clinical care and has fully developed facilities for adult and pediatric interventions including coronary interventions, valvuloplasty, device closure of congenital shunts and electrophysiology services (including radiofrequency ablation, pacemaker, bi-ventricular pacemaker and cardioverter defibrillator implantation). Laboratory testing facilities include treadmill testing, holter recording, echocardiography (including transthoracic, transesophageal, 3-D and fetal echocardiography), Tilt testing for syncope and electrophysiology testing including CARTO system mapping. The department has done pioneering work in the field of rheumatic fever and rheumatic heart disease including juvenile mitral stenosis, coronary artery disease including angioplasties, arrhythmias, cardiomyopathies and congenital heart diseases.
Following are the names of the Heads of the Department of Cardiology since its inception:
| Name |
|---|
| Prof. Sujoy B Roy |
| Prof. Madan Lal Bhatia |
| Prof. Rajan Tandon |
| Prof. Harbans Singh Wasir |
| Prof. Subhash Chand Manchanda |
| Prof. Kewal Krishan Talwar |
| Prof. K. Srinath Reddy |
| Prof. Vinay Kumar Bahl |
| Prof. Anita Saxena |
| Prof. Shyam Sunder Kothari |
| Prof. Balram Bhargava |
| Prof. Balram Bhargava |
| Prof. Rajiv Narang (current Head of Department) |
Prof. Nagarur Gopinath who established the dept of Cardiothoracic surgery at the AIIMS in 1964, passed away on Sunday,3rd june, 2007 at Bangalore. He was 84.
He began open heart surgery at the AIIMS in 1964, and began a training program in CTVS, leading to the M.Ch degree in 1966.He has trained a large number of students including half the faculty at the AIIMS. His students are now heading many of the departments in the country.He received the padma Shri from the govt. of India, and the wockhardt lifetime achievement award in 2004,and the lifetime achievement award from the Indian Association of cardiovascular-Thoracic surgeons in 2000.
Following his retirement in 1982 he continued to serve the AIIMS as Emeritus professor and contributed many monographs and papers on preventive aspects of heart disease. He is survived by Mrs. Gopinath, one daughter and two sons. The cardiothoracic centre will certainly feel the void left behind by Prof.Gopinath which will be difficult to fill.
This web page is for the patients undergoing Coronary Artery Bypass Grafting (CABG). This web page attempts to explain the cause of the disease, the risk factors, the effects of disease and possible treatment options. It tells about the surgery, preoperative preparation and postoperative care in hospital and at home. Lastly, an effort has been made to spread preventive awareness about the coronary artery disease. For better understanding, at the cost of technical perfection, language has been made as simple as possible.
This web page is for the patient who has a heart valve problem and who seeks treatment for the same. The web page describes in various chapters some of the fundamentals of blood circulation through the heart and the function of the valves and the effects of the disease. The web page also tells about the symptoms, tests that are used for diagnosis and after care. It tells about the surgery and postoperative care while the patient is in hospital. Finally it explains the aftercare when the patient is at home. For the purpose of better understanding, language has been made as simple as possible and efforts have been made to explain the facts in common language.
| S.No. | Name | Designation |
|---|---|---|
| 1 | Mr. Ashok Kumar | PS |
| 2 | Ms. Rachna | PA |
संस्थान/स्कूल के प्रमुख से प्रमाणपत्र (सीईए की प्रतिपूर्ति के लिए)
आधिकारिक बैग/ब्रीफ़केस/लेडीज़ पर्स की खरीद प्रतिपूर्ति दावा प्रपत्र
एम्स, नई दिल्ली में ई-पी.ए.आर प्रणाली ( स्पैरो) के कार्यन्वयन हेतु अपेक्षित सूचना
सेवानिवृत संकाय सदस्यो हेतु पैशन एवं चैक-लिस्ट संबंधी दस्तावेज
आवास किराया भत्ता प्रदान करने हेतु संस्थान कर्मचारियों द्वारा प्रवत्त प्रमाण पत्र
आवास किराया भत्ता प्रदान करने हेतु संस्थान कर्मचारियों द्वारा प्रदत्त प्रमाण-पत्र
Certificate From the Head of Institute/School ( For Reimbursement of CEA)
Purchase of Official bag/Briefcase/Ladies purse Reimbursement Claim Form
Application form for grant of Leave other than Casual Leave ( Office of the Chief Nursing Officer)
Information required for Implementation of E-OAR Mode ( Sparrow) at AIIMS, New Delhi
Certificate to be furnished by Institute Employees for Grant of HRA
Application from for an Advance for the Purchase of Personal Computer
Certificate to be Furnished by Institute Employee for Grant or HRA
Waiting List of students enrolled in various courses
| Year | Students Waiting List | |
| Senior Res. | Junior Res. | |
| 2013 | ( Non- Acad) January Session ( Non- Acad) July Session
| |
| 2014 | (Non Acad) Januaey Session | |
| year wise | UNDERGRADUATE Students List | POSTGRADUATE Students List | ||
|---|---|---|---|---|
| Senior Res. | Junior Res. | M.Sc | ||
| 2012 | Acad Non- Acad | Acad Non- Acad | Acad | |
| 2013 | Acad Non- Acad | Acad M.D/ M.D.S/ M.S / M.H.A from 2011 to 2013 Non- AcadJuly session only | Acad | |
| 2014 | Acad | Acad M.D/ M.D.S/ M.S / M.H.AJan Session Non AcadJan Session | ||
ONLINE HOSTEL APPLICATION SUBMISSION SYSTEM (for Post Graduate)
PROCEDURE TO APPLY FOR HOSTEL ACCOMODATION ONLINE (for Post Graduate)
ONLINE HOSTEL APPLICATION SUBMISSION SYSTEM(for Under Graduate)
PROCEDURE TO APPLY FOR HOSTEL ACCOMMODATION ONLINE(for Under Graduate)
The All India Institute of Medical Sciences has several hostels for its undergraduate and postgraduate students, PhD scholars and resident doctors. Conveniently located, hostellers do not have to travel long distances after a day of hard work and studies. These hostels are an essential component of the life at this institution wherein students, staff and faculty reside in the same campus. The life in hostels enables students to spend ample time in the hospital, departments utilizing library and other facilities to ensure they develop academically and acquire the necessary skills that can be obtained only through experience. In addition the hostel life allows students to interact with their colleagues and peers, make friends, and develop into good human beings capable of independent judgment and coping with the day to day pressures of life. Some students may leave their homes for the first time and they can be reassured these hostels would eventually turn out to be a home away from home!
DIRECTIVES OF THE HONOURABLE SUPREME COURT ON THE MENACE OF RAGGING
In view of the increasing incidents of ragging in colleges and elsewhere that reached proportions unbecoming of a civilised society the Hon’ble Supreme court admitted and heard the SLP No (s) 24295 of 2006 University of Kerala Vs Council, Principals’, Colleges, Kerala & Ors (with SLP(C) No.24296-99/2004 & W.P. (Crl) No. 173/2006 and SLP(C) No.14356/2005).
Pursuant to an order of Hon’ble Supreme Court of India dated November 27, 2006, the Ministry of Human Resource Development has constituted a Committee under the Chairmanship of Shri R.K. Raghavan (former Director, CBI) to look into the issue of ragging and suggest means of prevention of ragging in educational institutions.
The Committee primarily examined the following broad aspects of ragging:
The Committee had carried out a very detailed study with the help of voluntary organizations including CURE (Coalition for Uprooting Ragging from Education) and SPACE (Society for Peoples Action Change and Enforcement) and collected voluminous public opinion on the various factors contributing for ragging. Noted psychologists and educationists assisted the committee. The National Informatics Centre at the Ministry of Human Resources hosted a guest book in their website. Nearly eleven press releases were made during this period of evaluation and committee visited several cities in the country. A subcommittee of the Medical Council of India was also constituted for this purpose. A questionnaire was prepared that elicited over 12500 responses. In short a wide cross-section of the society provided the necessary background information, data and suggestions on tackling ragging in the country for consideration by the esteemed committee.
Subsequently the committee submitted a detailed report with suitable recommendations and measures required to effectively curb the menace. The recommendations of the Committee were duly accepted and the following directives have been issued to all the educational institutions for necessary implementation by the Hon’ble Supreme Court on 16 May 2007.
The All India Institute of Medical Sciences requests all students, parents and guardians to go through these directives and co-operate in the implementation of the directives of the Honourable Supreme Court of India. It is hoped that this will signal an end to the menace of ragging. Strict action shall be taken in accordance with the directives in case any student is found to indulge in ragging.
Application for Advance/Withdrawal form the General Provident Fund
Covid-19 Mental Health Helpline - AIIMS Faculty, Residents and Staff
Covid-19 Mental Health Helpline - AIIMS Faculty, Residents and Staff
011-26589142 (Timing for OPD booking on this Telephone is from 8:00 AM to 8:00 PM (All Working Days)
Mobile App : The AIIMS App has been removed from the Google Play store due to issues with the app rendering it non-functional. Users who had installed that app should remove it from their devices
For effective follow-up of post operative cardiac surgical patients at CTVS -OPD services, dedicated Helpline & Whatsapp numbers: 9999635940, 9999635425 will be active from 2:00pm to 6:00pm on Monday, Wednesday and Friday (i.e. otherwise usual OPD hours)/CTVS –OPD
Note:- If appointments are not available on O.R.S portal, then please do not call the call centre, as appointment through ORS portal and phone is from same pool.
23-12-2021
23-12-2021
23-12-2021
23-12-2021
23-12-2021
23-12-2021
23-12-2021
23-12-2021
You are not authorized to access this page.
ALL INDIA INSTITUTE OF MEDICAL SCIENCES (AIIMS)
NEW DELHI-110029
Toll Free No. : 1800 116 117
Tel No. : 011-2658 9391, 011-2659 3677
Mail : npicaiims2010[at]gmail[dot]com
जल्द आ रहा है
जल्द आ रहा है
जल्द आ रहा है
जल्द आ रहा है
Comming Soon
एम्स की स्थापना 1956 में स्वास्थ्य देखभाल के सभी पहलुओं में उत्कृष्टता को बढ़ावा देने के लिए एक केंद्र के रूप में की गई थी।

जवाहर लाल नेहरू जी ने देश को वैज्ञानिक संस्कृति से ओत प्रोत करने का सपना देखा था और स्वतंत्रता के तुरंत बाद उन्होंने इसे प्राप्त करने के लिए एक विशाल डिजाइन तैयार की। आधुनिक भारत के मंदिरों में से एक, जिन्हें उनकी कंल्पना से बनाया गया, चिकित्सा विज्ञान का एक उत्कृष्टता केन्द्र था। नेहरु जी का सपना यह था कि दक्षिण पूर्वी एशिया में चिकित्सा चिकित्सा और अनुसंधान की गति बनाए रखने के लिए एक केन्द्र होना चाहिए और इसमें उन्होंने अपनी तत्कालीन स्वास्थ्य मंत्री राजकुमारी अमृत कौर का पूरा सहयोग पाया।
एक भारतीय लोक सेवक, सर जोसेफ भोर, की अध्यक्षता में 1946 के दौरान स्वास्थ्य सर्वेक्षण और विकास समिति द्वारा एक राष्ट्रीय चिकित्सा केन्द्र की स्थापना की पहले ही सिफारिश की गई थी, जो राष्ट्र की बढ़ती स्वास्थ्य देखभाल गतिविधियों को संभालने के लिए उच्च योग्यता प्राप्त जनशक्ति की जरूरत पूरी कर सकें। पंडित नेहरु और अमृत कौर के सपने तथा भोर समिति की सिफारिशों को मिलाकर एक प्रस्ताव बनाया गया जिसे न्यूज़ीलैंड की सरकार का समर्थन मिला। न्यूज़ीलैंड का उदारतापूर्वक दिया गया दान कोलोम्बो योजना के तहत आया जिससे अखिल भारतीय आयुर्विज्ञान संस्थान (एम्स) की आधारशिला 1952 में रखी गई। अंत में एम्स का सृजन 1956 में संसद के एक अधिनियम के माध्यम से एक स्वायत्त संस्थान के रूप में स्वास्थ्य देखभाल के सभी पक्षों में उत्कृष्टता को पोषण देने के केन्द्र के रूप में कार्य करने हेतु किया गया था।

अखिल भारतीय आयुर्विज्ञान संस्थान की स्थापना सभी शाखाओं में स्नातक और स्नातकोत्तर चिकित्सा शिक्षा में अध्यापन के पैटर्न विकसित करने के उद्देश्य से संसद के अधिनियम द्वारा राष्ट्रीय महत्व के एक संस्थान के रूप में की गई थी, ताकि भारत में चिकित्सा शिक्षा के उच्च मानक प्रदर्शित किए जा सकें, स्वास्थ्य गतिविधि की सभी महत्वपूर्ण शाखाओं में कार्मिकों के प्रशिक्षण हेतु उच्चतम स्तर की शैक्षिक सुविधाएं एक ही स्थान पर लाने और स्नातकोत्तर चिकित्सा शिक्षा में आत्मनिर्भरता पाई जा सके।
संस्थान में अध्यापन, अनुसंधान और रोगियों की देखभाल के लिए व्यापक सुविधाएं हैं। जैसा कि अधिनियम में बताया गया है, एम्स द्वारा स्नातक और स्नातकोत्तर दोनों ही स्तरों पर चिकित्सा तथा पैरामेडिकल पाठ्यक्रमों में अध्यापन कार्यक्रम चलाए जाते हैं और यह छात्रों को अपनी ही डिग्री देता है। यहां 42 विषयों में अध्यापन और अनुसंधान आयोजित किए जाते हैं। चिकित्सा अनुसंधान के क्षेत्र में एम्स अग्रणी है, जहां एक वर्ष में इसके संकाय और अनुसंधानकर्ताओं द्वारा 600 से अधिक अनुसंधान प्रकाशन प्रस्तुत किए जाते हैं। एम्स में एक नर्सिंग महाविद्यालय भी चलाया जाता है और यहां बी. एससी. (ऑन) नर्सिंग पोस्ट प्रमाण पत्र डिग्री के लिए छात्रों को प्रशिक्षण भी दिया जाता है।
चार सुपर स्पेशियलिटी केन्द्रों के साथ 25 क्लिनिकल विभाग व्यावहारिक रूप से पूर्व और पैराक्लिनिकल विभागों की सहायता से रोग की सभी परिस्थितियों का प्रबंधन करते हैं। जबकि जलने के मामलों, कुत्ते के काटने के मामलों और संक्रामक रोगों से पीडित रोगियों को एम्स अस्पताल में उपचार नहीं दिया जाता है। एम्स द्वारा हरियाणा के वल्लभ गढ़ में व्यापक ग्रामीण स्वास्थ्य देखभाल केन्द्र में 60 बिस्तरों वाले अस्पताल का भी प्रबंधन किया जा रहा है और यहां सामुदायिक उपचार के लिए केन्द्र के माध्यम से लगभग 2.5 लाख आबादी को स्वास्थ्य सुविधाएं दी जाती हैं।








Information Pertaining to Academic Section for the year 2013-2014
No. of students On-Roll in various courses at AIIMS as on 31/3/2014: | |||
| 1 | MBBS Students | - | 383 |
| 2 | B.Sc. (Hons.)Nursing Students
| - | 393 |
| 3 | MD,MS,MDS,MHA & M.Ch.(6 years) Students | - | 655 |
| 4 | DM & MCH Students | - | 224 |
| 5 | Ph. D. Students | - | 419 |
| 6 | M.Sc., M.Sc. Nursing & M.Biotechnology Students | - | 109 |
No. of students who have been awarded degrees till 41st Convocation held in 2013: | |||
| 1 | MBBS | - | 2646 |
| 2 | B.Sc.(Hons.) Nursing, | - | 2674 |
| 3 | MD,MS,MDS,MHA & M.Ch. (6 years) | - | 5198 |
| 4 | DM & MCH | - | 1344 |
| 5 | Ph. D. | - | 996 |
| 6 | M.Sc., M.Sc. Nursing & M. Biotechnology | - | 764 |
एम्स द्वारा काय चिकित्सा, नर्सिंग और संबंधित क्षेत्रों में स्नातक स्तर के विभिन्न पाठ्यक्रम चलाए जाते हैं और लगभग सभी मूलभूत और क्लिनिकल चिकित्सा विशेषज्ञताओं और सुपर स्पेशियलिटीज में स्नातकोत्तर पाठ्यक्रम चलाए जाते हैं। इन पाठ्यक्रमों में प्रवेश पूरे देश में आयोजित प्रवेश परीक्षाओं के आधार पर दिया जाता है।
The section handles post-admission formalities for new students, develops and revises curricula and administers teaching programmes including internal assessment of undergraduate students admitted to various courses. The courses include MBBS, BSc (Hons) Medical Technology in Radiography, Ophthalmic Techniques, Operation Theatre Technology, BSc Dental Hygiene, BSc Dental Operating Room Assistant (DORA), BSc Nursing (Post-certificate) and BSc (Hons) Nursing courses.
The pattern of education in MBBS course was reviewed and re-structured in July 2004. The MBBS course is of 5½ years duration and comprises of 3 phases and internship. The details are as follows:
| Phase | Duration (years) | Training |
|---|---|---|
| First | One | Pre-Clinical |
| second | One-and-a-half second | Para-clinical second |
| Third | Two | Clinical |
| Internship | One | Compulsory rotation in various departments |
At present, 125 Indian students are admitted every year to the MBBS course (51 General category, 34 Other Backward Classes, 12 Economically Weaker Section (EWS) category, 19 Scheduled Caste and 9 Scheduled Tribe). For persons with disabilities (PWD), 5% reservation was provided on a horizontal basis. Seven foreign national students are also admitted each year. Beginning 2020, these admissions are made based on merit through the National Eligibility Entrance Test (NEET) conducted by the National Testing Agency.
As on 31 March 2021, 523 MBBS students including 73 interns were on rolls. Nine meritorious MBBS students were awarded scholarships for securing first, second and third positions in the first, second and final phase of professional examinations.
In 2020–2021, 98 students (38 General category, 10 EWS Category, 15 Scheduled Caste, 7 Scheduled Tribe and 26 Other Backward Classes, 2 Foreign Nationals) were admitted in BSc (Hons) Nursing course. For BSc Nursing (Post-certificate) course, 45 students (21 General category, 8 Scheduled Caste, 3 Scheduled Tribe, 9 Other Backward Classes, 3 EWS and 1 foreign national candidates) were admitted.
Students admitted to various BSc courses were:
| Course | General | SC | ST | OBC | EWS | Total |
|---|---|---|---|---|---|---|
| Opthalmic Techniques | 9 | 2 | 2 | 5 | 2 | 20 |
| Medical Technology in Radiology | 5 | 1 | 1 | 3 | 1 | 11 |
| Operation Theatre Technology | 1 | 1 | 1 | 2 | 1 | 6 |
| Dental Hygiene | 1 | 1 | 0 | 2 | 1 | 5 |
| Dental Operating Room Assistant | 2 | 2 | 1 | 3 | 2 | 10 |
The number of students on rolls in these courses as on 31st March 2021 were:
| Course | Number of Students |
|---|---|
| Nursing | |
| B.Sc Nursing (Post -basic) | 78 |
| B.Sc (Hons) Nursing | 323 |
| Paramedical | |
| B.Sc (Hons) Ophthalmic Techniques | 74 |
| B.Sc (Hons) Medical Technology in Radiology | 39 |
| B.Sc Operation Theatre Technology | 31 |
| B.Sc Dental Hygiene | 11 |
| B.Sc Dental Operating Room Assistant | 22 |
The Academic Section looks after all activities pertaining to admission and training of postgraduate students including junior and senior residents. It handles all activities related to Fellowship, PhD, DM, MCh, MD, MS, MDS, MCh/DM (Direct 6 years course), M Biotechnology (MBiotech) and MSc courses in different disciplines.
Admissions to all postgraduate courses for Indian nationals as well as sponsored candidates are made through an All-India Entrance Examination held twice a year for all postgraduate courses except MSc, MSc Nursing and MBiotechnology courses, for which the examination is held once a year. Foreign nationals are admitted under the sponsored category through the same entrance examination. In 2020–21, 748 students were admitted in various courses. The number of postgraduate and doctoral students on roll on 31 March 2021 was 1966.
Admissions in various courses
| Sr. No. | Name of Course | July 2020 | January 2021 | Total |
|---|---|---|---|---|
| 1 | MSc /MBiotech/ MSc Nursing (August) | 76 | * | 76 |
| 2 | MD / MS/ MDS/ MCh/ DM (Direct 6 Years) second | 260 | 186 | 446 |
| 3 | DM / MCh | 96 | 105 | 201 |
| 4 | PhD | 53 | 37 | 90 |
| 5 | Fellowship | 17 | 22 | 39 |
| Total | 502 | 350 | 852 |
*Admissions are done once in a year.
Postgraduate students on rolls
| Sr. No. | Name of Course | Number of Students on roll |
|---|---|---|
| 1 | PhD | 295 |
| 2 | DM | 363 |
| 3 | MCh | 174 |
| 4 | Fellowship programme | 49 |
| 5 | MD | 766 |
| 6 | MS | 115 |
| 7 | MDS | 67 |
| 8 | MSc / MBiotech / MSC Nursing | 156 |
| Total | 1985 |
यह विज्ञान है। यह एक सम्पन्न देश में अकेला ही भूख और गरीबी, अस्वच्छता और निरक्षरता की समस्याओं को सुलझा सकता है, यह परम्पराओं और रीति रिवाजों के डर तथा भय को समाप्त कर सकता है, संसाधनों की बर्बादी को रोक सकता है, जहां भूख से तड़पते लोग हैं।
जवाहरलाल नेहरू
एम्स का अनुसंधान केवल नियमित गतिविधि नहीं है बल्कि यह तीन उद्देश्यों के साथ एक मिशन है। कहीं अन्यत्र भी अनुसंधान का प्रयोजन अनुशासनिक गतिविधि द्वारा जिज्ञासा को शांत करना होता है और इस प्रकार नए ज्ञान का सृजन होता है। परन्तु एम्स में हम अपनी अनुसंधान भूमिका के प्रति सचेत हैं जो हम अध्यापन की गुणवत्ता को सुधारने में निभा सकते हैं। एक अध्यापक यदि अनुसंधान में संलग्न है तो उसके पास नवीनतम जानकारी होनी चाहिए और वह अपने छात्रों में पूछताछ की भावना और आजादी भी पैदा कर सकता है। अंत में एम्स का अनुसंधान हमारे राष्ट्रीय प्रयास के अलावा हमारे समाज में एक वैज्ञानिक सोच उत्पन्न करने के लिए है तथा हम अपने समाज से प्राधिकार और अंधविश्वास समाप्त करना चाहते हैं।
एम्स का अनुसंधान हमारे राष्ट्रीय प्रयास के अलावा हमारे समाज में एक वैज्ञानिक सोच उत्पन्न करने के लिए है तथा हम अपने समाज से प्राधिकार और अंधविश्वास समाप्त करना चाहते हैं।
एम्स को राष्ट्रीय और अंतरराष्ट्रीय एजेंसियों से विशाल अनुसंधान प्राप्त होते हैं, संस्थान अपनी ओर से मध्यम दर्जे के अनुसंधान अनुदान भी प्रदान करता है। ये अनुदान परियोजनाओं को जमा करने के बाद समितियों के जरिए उनकी छानबीन के बाद प्रदान किए जाते हैं और ये कनिष्ठ संकाय को अनुसंधान की प्रेरणा देने के प्राथमिक साधन है। इस प्रकार अन्य बातों के समान होने पर युवा वर्ग के आवेदनों को प्राथमिकता दी जाती है। अन्वेषक द्वारा कुछ प्रगति होने पर अन्य एजेंसियों से बड़े अनुदान पाने के लिए आवेदन कर सकता है।
एम्स में अनेक प्रकार के अनुसंधान किए जाते हैं। एक ओर हम तंत्रिका विज्ञान, आनुवंशिकी और हार्मोग्राफी अंत:क्रिया के कम्प्यूटर उद्दीपन पर परिष्कृत अनुसंधान करते हैं, दूसरी ओर हम राष्ट्रीय स्वास्थ्य समस्याओं की रोकथाम और इलाज पर क्लिनिकल तथा जनसांख्यिकी अध्ययन करते हैं। हम उन्नत तकनीकों को लागू करने का प्रयास करते हैं जैसे डीएनए पुनर्योगज प्रौद्योगिकी, प्रतिरक्षा विज्ञान और इलेक्ट्रॉन माइक्रोस्कोपी, जिससे हमारे देश के सामान्य रोगों जैसे कुष्ठ, मलेरिया, तपेदिक, डायबिटीज़, डायरिया, हिपेटाइटिस, फ्लोरोसिस और आयोडीन की कमी। हमारे पास अनेक प्रकार के स्वीकृत गर्भ निरोधकों पर केन्द्रित प्रजनन के लक्ष्य उन्मुख अनुसंधान के लिए अन्य अंतरराष्ट्रीय निधिकृत विशाल कार्यक्रम हैं। संस्थान से निकलने वाले वैज्ञानिक प्रकाशन की संख्या भी प्रति संकाय सदस्य प्रति वर्ष लगभग 2 है और इनमें से आधे से अधिक प्रकाशनों में वैज्ञानिक उद्धरण सूचकांक होते हैं। एम्स ने 1980-88 के बीच 8 वर्ष की अवधि में भारत के मेडिकल कॉलेज में पहला स्थान बनाए रखा (औसत + एसडी)। 237.5 +37.3 विज्ञान उद्धरण सूचकांक सूचीबद्ध प्रकाशन प्रति वर्ष (रेड्डी आदि नेच. मे. इंडिया 1991, 4 : 90-92)। इस 7 वर्ष की अवधि में 1987 में 94 के दौरान 1630 मेड लाइन सूचीबद्ध प्रकाशनों में भारत के चिकित्सा अनुसंधान संस्थानों में संलग्न संस्थानों में सर्वोच्च रहा (अरुणाचलम, करंट साइंस, 1997, 72 : 912-922)।
एम्स में अनुसंधान की गुणवत्ता और रेंज निम्नलिखित प्रबलन क्षेत्रों के चयन से परखी जा सकती है।
डायरिया रोगों का नियंत्रण
1980 के दशक में अस्पतालों के 40 प्रतिशत बिस्तर डायरिया से होने वाली कमी के मामलों से भरे होते थे। वर्ष 1997 में भारत के अनेक हिस्सों में प्रदर्शन के लिए भी ऐसे मामलों का पता लगाना कठिन हो गया। एम्स में किए जाने वाले मूलभूत, अनुप्रयुक्त और प्रचालन अनुसंधान ने इस रुपांतरण में एक महत्वपूर्ण भूमिका निभाई। हाल ही में हमने दो प्रकार के सुपर ओरल रीहाइड्रेशन घोल विकसित किए हैं जो एमिनो सांद्रता पर आधारित हैं।
हम अपने देश में सामान्य रोगों के अध्ययन के लिए पुनर्योगज डीएनए प्रौद्योगिकी, प्रतिरक्षा विज्ञान और इलेक्ट्रॉन माइक्रोस्कोपी जैसी उन्नत तकनीकों का उपयोग करने की कोशिश कर रहे हैं।
डब्ल्यूएचओ द्वारा इस वर्ष वैश्विक डायरिया रोग नियंत्रण कार्यक्रम में इस नए सूत्र को लाया जाएगा। एम्स में लगातार होने वाले इस रोग के इलाज के लिए एक विधि का विकास किया है, जिसे 1994 में वैश्विक डायरिया रोग नियंत्रण कार्यक्रम में उपयोग किया जाएगा। लगातार होने वाले डायरिया के 50 प्रतिशत मामलों में जिम्मेदार यह बैक्टीरिया एम्स में खोज लिया गया है और अनंतिम रूप से इसे एंटेरोएग्रीगेटिव ई. कोलाई नाम दियरा गया है। डायरिया रोग में जिंक की कमी पर अनुसंधान हेतु एम्स की भूमिका के लिए इसे टाइम पत्रिका में 1996 में अच्छी खबर के तौर पर प्रकाशित किया गया था।
एम्स में रोटा वायरस को डायरिया रोग के लिए एक प्रमुख कारण बताया गया था। अब हमने जैव प्रौद्योगिकी के सहयोग से रोटा वायरस का टीका विकसित किया गया है, जिसके लिए इस वर्ष पहले चरण के परीक्षण तैयार हैं।
एम्स द्वारा तपेदिक के निदान के लिए एक पीसीआर जांच का विकास किया गया है। यह जांच खास तौर पर एक्स्ट्रा पल्मोनरी तपेदिक में उपयोगी है, जो नमूना प्राप्त होने के 24-48 घण्टों के अंदर इसका निदान करती है, जबकि पारंपरिक जांचों में 6-8 सप्ताह का समय लगता है।
एम्स द्वारा इस घातक रोग के प्रति किए गए अनुसंधान के योगदान इस प्रकार हैं :
एक व्यवहार शरीर क्रिया विज्ञान अध्ययन
एम्स में आधुनिक डीएनए प्रौद्योगिकियों का उपयोग करते हुए अब भारत में इस महामारी के लिए जिम्मेदार परजीवी के विभेदों का अध्ययन करना संभव हो गया है।
एम्स द्वारा एचआईवी एंटीबॉडी का पता लगाने के लिए उच्च संवेदनशील और विशिष्ट एलाइजा प्रणाली का विकास स्वदेशी रूप से किया गया गया है। इसकी कीमत आयात किए गए जांच किट से लगभग आधी है और आयात किए गए किट की तुलना में इससे कई शुरूआती मामलों में रोग का पता लगाया जा सकता है।
एम्स द्वारा एचआईवी एंटीबॉडी का पता लगाने के लिए उच्च संवेदनशील और विशिष्ट एलाइजा प्रणाली का विकास स्वदेशी रूप से किया गया गया है। इसकी कीमत आयात किए गए जांच किट से लगभग आधी है और आयात किए गए किट की तुलना में इससे कई शुरूआती मामलों में रोग का पता लगाया जा सकता है। एम्स 1986 से एचआईवी / एड्स के लिए संदर्भ केन्द्रों में से एक और 1992 से राष्ट्रीय एचआईवी संदर्भ केन्द्र है।
एम्स में जनसांख्यिकी, क्लिनिकल और मूल भूत अनुसंधन से समस्या के परिमाण का आकलन किया गया है, जिससे स्वदेशी जांच किट का विकास और प्रत्याशी टीके तैयार किए गए हैं, हिपेटाइटिस सी वायरस के लिए रक्तदाताओं की छानबीन हेतु एक नैदानिक आकलन प्रणाली भी तैयार की गई है।
प्लेग के लिए नैदानिक जांच
एम्स दुनिया का पहला स्थान है जहां फॉर्मेलिन में स्थिर किए गए शव पर पीसीआर के उपयोग से 1994 की महामारी के दौरान प्लेग का पता लगाने और इसकी पुष्टि की विधि ज्ञात की गई थी। इसे क्लोन किया गया, क्रम ज्ञात किया गया और एफ1 पर अभिव्यक्त किया गया है तथा यर्सिनिया पेस्टिस के पीएलए जीन पर, जो प्रतिरक्षी अभिक्रियात्मक हैं। इनका उपयोग प्लेग के सिरोलॉजिकल परीक्षण हेतु किया जा रहा है।
एम्स द्वारा वृद्धि और विकास पर आयोडीन की कमी के प्रभावों को परिभाषित किया गया है, खास तौर पर मानव भ्रूण में मस्तिष्क विकास के लिए थाइरॉक्सिन की भूमिका। एम्स में प्रयोगशाला और क्षेत्र अध्ययनों से 1986 में भारत सरकार के सार्वभौमिक नमक आयोडीनीकरण कार्यक्रम का मार्ग प्रशस्त हुआ। आयोडीन की कमी को नियंत्रित करने के लिए हमारे योगदान भूटान, नेपाल, बंगलादेश, मालदीव, इंडोनेशिया, थाइलैंड और मध्य पूर्व के अनेक देशों तथा कई अफ्रीकी देशों तक विस्तारित किए गए हैं
नमक में आयोडीन की कमी के आकलन हेतु टाइट्रेशन विधि। यह सरल किन्तु महत्वपूर्ण जांच के सार्वभौमीकरण की सफलता सुनिश्चित करती है
एम्स में प्रयोगशाला और क्षेत्र अध्ययनों से 1986 में भारत सरकार के सार्वभौमिक नमक आयोडीनीकरण कार्यक्रम का मार्ग प्रशस्त हुआ।
अधिकांश अनुसंधान पिछले 25 वर्षों में एंटी ह्यूमन कोरियोनिक गोनेडोट्रॉपिन (एचसीजी) टीके के विकास के प्रति किया गया जो आरंभ में एम्स में किए गए अनुसंधान के आधार पर आगे बढ़ाया गया।
प्रतिरक्षी कोशिका विज्ञान की दृष्टि से अभिरंजित एंडोमेट्रियम के मोर्फोमेट्रिक विश्लेषण और प्राइमेट इम्प्लांटेशन जीव विज्ञान प्रयोगशाला में फोटो माइक्रोग्राफी
गर्भावस्था में भ्रूण के रोपण की एंडोक्राइन और पेराक्राइन प्रक्रियाओं पर मूलभूत अनुसंधान तथा पोस्ट कोइटल, पोस्ट ओव्यूलेटरी गर्भ निरोध। हमारी प्राइमेट इम्प्लांटेशन जीव विज्ञान प्रयोगशाला में एक गैर अमेरिकी केन्द्र में गर्भ निरोध अनुसंधान और विकास कार्यक्रम को मान्यता दी है जो एंड्रू मेलन फाउंडेशन द्वारा चलाया गया है और यह रॉक फेलर फाउंडेशन द्वारा दीर्घ अवधि आधार पर समर्थित दुनिया के ऐसे 13 केन्द्रों में से भी एक है।
एम्स द्वारा एंटार्कर्टिका की खोज पर 1990 से भारतीय प्रयासों में भागीदारी की गई है। खोज अभियान पर जाने वाले सदस्यों को स्वास्थ्य देखभाल प्रदान करने के अलावा एम्स मानव जीव की क्रोनो बायोलॉजी, तनाव के प्रति शरीर क्रियात्मक प्रतिक्रिया और एंटार्कर्टिका के प्रतिकूल परिवेश में इसका प्रभाव तथा एंटार्कर्टिका की कठोर और अकेलेपन की परिस्थितियों में इनके निष्पादन पर अनुसंधान आयोजित किए गए हैं।
इस पुस्तकालय को संस्थान के प्रथम निदेशक के नाम पर दिया गया है, जहां 61423 पुस्तकें, 53547 पत्रिकाएं और 14008 रिपोर्ट जैव चिकित्सा विज्ञान के क्षेत्र में संग्रह की गई हैं। इस पुस्तकालय में हर वर्ष 490 पत्रिकाएं और 80 समाचार पत्रिकाएं आती हैं। यह पुस्तकाय सप्ताह के सातों दिन सुबह 8 बजे से दोपहर 2 बजे तक पाठकों के लिए खुला होता है। पुस्तकालय में कम्प्यूटर सुविधा, माइक्रो फील्म, पुस्तकालय रीडर और रीडर प्रिंटर सुविधाएं हैं। यहां की समृद्ध और दक्ष सामग्री हमारे अनुसंधान की गतिविधियों को नई ऊर्जा प्रदान करती हैं।
बी. बी. दीक्षित पुस्तकालय में खास तौर पर व्यस्त क्षण
This section states the "Disclaimer" under which you may use aiims.edu/aiims.ac.in (the “Web Site”). Please read this page carefully. If you do not understand the Disclaimer stated here, do not use this web site and our services and in such case its use may be at your own risk. By using the Web Site, you are indicating your acceptance of the following Disclaimer. AIIMS, New Delhi, (the “Institute”) may revise this Disclaimer at any time by updating this posting. You should visit this page periodically to review the Disclaimer, because it is binding on you.
The content available on AIIMS website may not be up-to-date as the website and its content is being revamped. The site may also be having bugs and glitches, lack of functionality and broken links. Please bear with us for any such inconvenience and give your opinion, suggestions and feedback on the same for improvement of the website. By using the Web Site, you assume all the risks associated with dealing with other users with whom you come in contact through the Web Site. The Institute cannot and does not confirm that each user is who they claim to be. In the event that you have a dispute with another user, you release the Institute, its Director, its Employees and agents from any claims, demands and damages (actual and consequential, direct and indirect) of every kind and nature, known and unknown, suspected and unsuspected, disclosed and undisclosed, arising out of or in any way connected with such disputes.
The Institute does not guarantee the accuracy, thoroughness, reliability, or quality of content at the Web Site, and will not be responsible for any errors, inaccuracies, typographical errors or omissions in articles or any other content. The Institute will not be liable of any loss or damage caused by a users reliance on information obtained from the Web Site. You should not use the Web Site if you cannot or do not accept this responsibility. Despite our efforts to provide timely and accurate information, we may have errors from time to time.
You should not rely solely upon the information or advice read at the Web Site. Since each individual’s purpose is unique and different, you should always consult with others as per need on your own before making any important decisions based on the contents of the website.
Links to Third Party Sites
The Web Site may contain links to third party web sites. These links are provided solely as a convenience to you and not as an endorsement by the Institute of the content on such third party web sites. This Institute is not responsible for the content of linked third party web sites and does not make any representations regarding the content or accuracy of materials on such sites.
Indemnity
By using the Web Site, you agree to indemnify, defend and hold harmless the Institute, its Director, Officers, Employees, Ex-Employees from and against any claims, actions or demands, including without limitation reasonable legal and accounting fees, alleging or resulting from your use of the Material or your breach of the Terms of Use.
Disclaimer of Warranties
You expressly agree that the use of the web site is at your own risk. The web site is provided on an “as is” and “as available” basis without warranties of any kind, express or implied, including but not limited to warranties of title, merchantability, reliability, accuracy, fitness for a particular purpose or non-infringement.
The institute makes no warranty that the web site will be uninterrupted, timely, or secure. Additionally, the institute does not warrant that the web site will operate error-free or that the web site and its server are free of computer viruses or other harmful mechanisms. The institute is not responsible for any consequential or incidental damage, whether foreseeable or not, which may have resulted from the unavailability or malfunction of the web site. If your use of the web site or the material results in the need for servicing or replacing equipment or data, the institute is not responsible for those costs.
You agree that any information or data downloaded through the use of the web site is at your own discretion and risk and that you will be solely responsible for any damage to your computer system or loss of data that results from the download of such material and/or data.
The institute is not responsible for content or other information outside this web site. The institute makes no representation as to the quality, accuracy, suitability, functionality, or legality of any sites to which we may provide links. You hereby waive any claim you might have against the institute with respect to such links and sites.
Limitation of Liability
In no event shall the institute, its director, officers, employees, parents, affiliates or third parties be liable for any damages whatsoever including, without limitation, incidental and consequential damages, lost profits, or damages resulting from lost data or business interruption resulting from the use or inability to use the web site and services, whether based on warranty or contract. You hereby waive any and all claims against the institute and its parents, affiliates, officers, or employees arising out of your use of the web site and the information or services available thereon.
The Apps are designed, developed and maintained by AIIMS, New Delhi. Though all efforts have been made to ensure the accuracy and currency of the content on this app, the same should not be construed as a statement of law or used for any legal purposes. In case of any ambiguity or doubts, users are advised to verify/check with the Department(s) and/or other source(s), and to obtain appropriate professional advice. Under no circumstances will this Department be liable for any expense, loss or damage including, without limitation, indirect or consequential loss or damage, or any expense, loss or damage whatsoever arising from use, or loss of use, of data, arising out of or in connection with the use of this app. These terms and conditions shall be governed by and construed in accordance with the Indian Laws. Any dispute arising under these terms and conditions shall
be subject to the jurisdiction of the courts of India.
You must comply with App T&Cs as these apply to your use of the Apps and the Service T&Cs apply to your use of the Service that you access and use through the Apps. Any violation of these Apps T&Cs or the Service T&Cs may result in the termination of your access to the Apps and/or the Service.
The Apps are for your own personal use only. Any commercial use will result in termination of your access to the app and service. You cannot distribute or copy or modify any part of it in any way.
You must not attempt to extract any source code from the Apps, disassemble it or make any derivative versions, or attempt to interrupt or decipher the transmissions between the Apps and our systems.
The user of the apps must not use the app for any the following
The Apps and all copyright, database rights, and other intellectual property rights related to them belong to AIIMS New Delhi.
Privacy Policy
This privacy policy governs your use of the mobile applications (Apps) that are hosted at AIIMS New Delhi Mobile App Account in Google Play Store and Apple App Store. The contents published on these Applications were provided by the concerned
Ministries/Departments of AIIMS New Delhi. This information provided through these applications may not
have any legal sanctity and are for general reference only, unless otherwise specified. However, every effort has been made to provide accurate and reliable information through these applications. Users are advised to verify the correctness
of the facts published here from the concerned authorities. AIIMS New Delhi will not be responsible for the accuracy and correctness of the contents available in the application.
AIIMS New Delhi has built multiple free mobile applications. These mobile applications are provided by AIIMS at no cost and is intended for use as is by the general public and the employees of the institute.
This page is used to inform visitors regarding our policies with the collection, use, and disclosure of Personal Information if anyone decides to use these services.
If you choose to use these services, then you agree to the collection and use of information in relation to this policy. The Personal Information that is collected is used for providing and improving the services. AIIMS will not use or share your information with anyone except as described in this Privacy Policy.
Information Collection and Use
The Applications may obtain the information you provide when you download and register the Application. Registration is optional. However, please keep in mind that you may not be able to use some of the features offered by an Application unless you register.
For a better experience, while using our Service, we may require you to provide us with certain personally identifiable information, including but not limited to the phone number. When you register and use the Application, you generally provide (a) your name, email address, age, user name, password and other registration information; (b) download or use applications from us; (c) information you provide when you contact us for help and (d) information you enter into our system when using the Application, such as contact information and other details.
The information you provided may be used to contact you from time to time to provide you with important information and required notices.
The app does use any third party services that may collect information used to identify you.
Automatically Collected Information
In addition, the Application may collect certain information automatically, including, but not limited to, the type of mobile device you use, your mobile devices unique device ID, the IP address of your mobile device, your mobile operating system, the type of mobile Internet browsers you use, and information about the way you use the Application.
When you visit the mobile application, it may use GPS technology (or other similar technology) to determine your current location in order to determine the city you are located within and display a location map. The location information
may be sent to authorities for taking necessary actions and making policy decisions.
If you do not want the app to use your location for the purposes set forth above, you should turn off the location services for the mobile application located in your account settings or in your mobile phone settings and/or within the mobile
application. However, if the service provided by the Application requires the location services using GPS technology, such services offered by the application will not be available to you.
We may disclose User provided and Automatically Collected Information as required by law, such as to comply with a subpoena, or similar legal process when we believe in good faith that disclosure is necessary to protect our rights, protect
your safety or the safety of others, investigate fraud, or respond to a government request with our trusted service providers who work on our behalf, do not have an independent use of the information we disclose to them, and have agreed to adhere to the rules set forth in this privacy statement.
You can stop all collection of information by the Application easily by uninstalling the Application. You may use the standard uninstall processes as may be available as part of your mobile device or via the mobile application marketplace or network.
Data Retention Policy, Managing Your Information
We will retain User provided data for as long as you use the Application and for a reasonable time thereafter. We will retain Automatically Collected information also for a reasonable period of time depending on the nature of application and
thereafter may store it in aggregate. Please note that some or all of the User Provided Data may be required in order for the Application to function properly.
Misuse by Non Targeted Users
All mobile apps are meant for use by the targeted audience only. Misuse by nontargeted users should be prevented by owner of the mobile.
Security
We are concerned about safeguarding the confidentiality of your information. We provide physical, electronic, and procedural safeguards to protect information we process and maintain. For example, we limit access to this information to authorized employees and contractors who need to know that information in order to operate, develop or improve our Application. Please be aware that, although we endeavour to provide reasonable security for information we process and maintain, no security system can prevent all potential security breaches.
Your Consent
By using the Application, you are consenting to our processing of your information as set forth in this Privacy Policy now and as amended by us.
Logging Data
We want to inform you that whenever you use this service, in a case of an error in the app we collect data and information (through third party products) on your phone called Log Data. This Log Data may include information such as your device Internet Protocol (“IP”) address, device name, operating system version, the configuration of the app when utilizing my Service, the time and date of your use of the Service, and other statistics.
Service Providers
We may employ third-party companies and individuals due to the following reasons:
We want to inform users of this Service that these third parties have access to your Personal Information. The reason is to perform the tasks assigned to them on our behalf. However, they are obligated not to disclose or use the information for any other purpose.
Links to Other Sites
This Service may contain links to other sites. If you click on a third-party link, you will be directed to that site. Note that these external sites are not operated by me. Therefore, we strongly advise you to review the Privacy Policy of these websites. We have no control over and assume no responsibility for the content, privacy policies, or practices of any third-party sites or services.
Children’s Privacy
These Services do not address anyone under the age of 13. We do not knowingly collect personally identifiable information from children under 13. In the case we discover that a child under 13 has provided us with personal information, we will immediately delete this from our servers. If you are a parent or guardian and you are aware that your child has provided us with personal information, please contact us so that we will be able to do necessary actions.
Changes to This Privacy Policy
We may update our Privacy Policy from time to time. Thus, you are advised to review this page periodically for any changes. We will notify you of any changes by posting the new Privacy Policy on this page. These changes are effective immediately after they are posted on this page.
Contact Us
If you have any questions or suggestions about my Privacy Policy, do not hesitate to contact us at
Email - picf@aiims.edu.
Phone - +91-011-26593800
Address - Computer Facility, AIIMS, Ansari Nagar, New Delhi 110029, India

हृद्वक्ष केन्द्र, एम्स में कोरोनरी बाइपास सर्जरी जारी है

श्री देवीराम भारत में प्रथम ह़दय प्रतिरोपण

डॉ. राजेन्द्र प्रसाद नेत्र रोग विज्ञान केन्द्र, एम्स में लेजर उपचार कराता हुआ एक रोगी
एम्स में हाइटेक सुविधाओं और नर्सिंग देखभाल से इन लोगों की उत्तरजीविता में योगदान मिला है
बीसीआर हरे संकेत एबीएल लाल संकेत तीर से इनके मिलने का संकेत दर्शाया गया है

हाल में लगाए गए गामा नाइफ से इलाज के लिए तंत्रिका शल्य चिकित्सा रोगी को तैयार करना

एम्स की आधुनिकतम चुम्बकीय अनुनाद इमेजिंग सुविधा में जांच कराता रोगी

एक मल्टी चैनल ऑटोएनाइलाइजर जो रक्त के छोटे से नमूने का इस्तेमाल करते हुए रक्त रसायन के अनेक पैरामीटरों का शीघ्रतापूर्वक आकलन कर सकता है।
एम्स भारत और पड़ोसी देशों के लाभवंचित लाखों नागरिकों को विश्व स्तरीय क्लिनिकल सेवाएं प्रदान करने के लिए कठिन प्रयास करता है। इसके भव्य भवन और हाइटेक सुविधाएं आभिजात्य वर्ग की सतही छवि मात्र बनाती हैं। एम्स में आने के बाद यह विभ्रम मिट जाता है।एम्स भारत और पड़ोसी देशों के लाभवंचित लाखों नागरिकों को विश्व स्तरीय क्लिनिकल सेवाएं प्रदान करने के लिए कठिन प्रयास करता है। इसके भव्य भवन और हाइटेक सुविधाएं आभिजात्य वर्ग की सतही छवि मात्र बनाती हैं। एम्स में आने के बाद यह विभ्रम मिट जाता है।
यहां के गलियारे रोगियों से भरे होते हैं, जिनमें से अधिकांश लोग इतने गरीब हैं कि वे कहीं और अच्छा इलाज नहीं करा सकते। यह यहां बड़ी उम्मीदे लेकर आते हैं क्योंकि एम्स ने अपनी ऐसी प्रतिष्ठा बनाई है। वर्तमान में एम्स केवल एक अस्पताल नहीं है बल्कि यह सुविधाओं का समूह है। यहां 1500 से अधिक क्षेत्रफल में फैला हुआ मुख्य अस्पताल, डॉ. राजेन्द्र प्रसाद नेत्र रोग विज्ञान केन्द्र, हृदवक्ष केन्द्र, तंत्रिका विज्ञान केन्द्र, इंस्टीट्यूट रोटरी सेंटर अस्पताल और नशा मुक्ति केन्द्र। सुविधाओं के इस संकुल में प्रतिवर्ष लगभग 1.5 मिलियन बाह्य रोगी और 80,000 आंतरिक रोगी आते हैं। एम्स में प्रति वर्ष की जाने वाली शल्य चिकित्सा की संख्या 100,000 से अधिक है।
जबकि एम्स की शक्ति अंकों में नहीं बल्कि एक ही स्थान पर सर्वोत्तम चिकित्सा और शल्य क्रिया विशेषज्ञों, आधुनिकतम उपकरणों का उपलब्ध होना और नैदानिक या सार्वजनिक स्वास्थ्य चुनौतियों को पूरा करने के लिए हमारी क्षमता बढ़ाने में भी है। चाहे यह ऑटोएनालाइजर या लीनियर एक्सिलरेटर, चुम्बकीय अनुनाद इमेजिंग या गामा नाइफ, एम्स के पास से सभी हैं। जैसे ही कोई नया उपकरण आता है, संस्थान में कोई न कोई इसे लेने का प्रयास करता है और अपने सभी साधन जुटाकर इसे प्राप्त कर लेता है।
एम्स द्वारा जिन क्षेत्रों में विशेषज्ञता प्राप्त की गई है वे हैं कार्डियक कैथेटराइजेशन, हृदय वॉल्व सर्जरी, पोर्टो-केवल सर्जरी, नवजात सर्जरी, जोड़ प्रतिस्थापन, कॉकलियर इम्प्लांट और बहु अंग प्रतिरोपण (कार्निया, गुर्दे, अस्थि मज्जा, हृदय और यकृत)। परिष्कृत चिकित्सा और सर्जिकल देखभाल में हमारे परिणाम दुनिया में सर्वोत्तम हैं। इस प्रयास का सबसे अधिक संतुष्टिकारक पक्ष यह है कि ये आधुनिकतम प्रौद्योगिकियां वास्तव में गरीबों के लिए इस्तेमाल की जा रही हैं।
एम्स में रोगी देखभाल की भूमिका केवल हमारे अस्पताल तक सीमित नहीं है। एम्स द्वारा ऐसे डॉक्टरों और सर्जनों को प्रशिक्षण दिया जाता है जो देश भर में फैले हुए हैं तथा विदेश में भी कार्यरत हैं। दशकों से तंत्रिका वैज्ञानिकों, तंत्रिका शल्य चिकित्सकों, हृदय शल्य चिकित्सकों, बाल रोग शल्य चिकित्सकों और गैस्ट्रोएंटेरोलॉजिस्ट की बड़ी संख्या एम्स में प्रशिक्षण आती है, क्योंकि हमारे संस्थान में पहली बार इन सुपर स्पेशियलिटीज़ को आरंभ किया गया। अब हमारे पास एंडोक्राइनोलॉजी और मेडिकल ओंकोलॉजी में डीएम पाठ्यक्रम हैं। राष्ट्र ने एम्स पर बहुत अधिक निवेश किया है और एम्स के पास उन लोगों की सर्वोत्तम संभव स्वास्थ्य देखभाल प्रदान करने के पर्याप्त साधन हैं, चाहे उनकी भुगतान क्षमता कुछ भी हो। कुछ लोगों ने अपनी वचनबद्धता पूरी की होती।
चिरकालिक माइलॉइड ल्यूकेमिया के फिलाडेलफिया गुणसूत्र धनात्मक रोगियों की एक इंटरफेस कोशिका। कोशिका में दर्शाया गया है बी सी आर / ए बी / काइमेरिक फ्यूजन जीन (ओंकोजीन)। पीले संकेत से बी सी आर हरे और ए बी / (लाल) संकेत का अतिव्यापन दर्शाया गया है।
व्यापक ग्रामीण स्वास्थ्य सेवा परियोजना (सीआरएचएसटी) की स्थापना एम्स से लगभग 35 कि. मी. की दूरी पर वल्लभ गढ़ में भारत के ग्रामों में स्वास्थ्य देखभाल की प्रदायगी के मॉडल के रूप में कार्य करने हेतु की गई है। इसमें उप संभागीय अस्पताल और प्राथमिक स्वास्थ्य केन्द्रों, उप केन्द्रों और स्वास्थ्य कामगारों का एक नेटवर्क है। इसकी अनोखी विशेषता समुदाय की ओर से अपनी भागीदारी का सशक्त तत्व शामिल है। इस परियोजना से मध्यम संसाधनों की सहायता से स्वास्थ्य में बड़े सुधार का प्रदर्शन किया गया है।

श्रीमती रेणुका चौधरी, स्वास्थ्य और परिवार कल्याण मंत्री तथा एम्स की अध्यक्षा, एम्स में 25 सितम्बर 1997 को जीवनशैली तथा स्वास्थ्य पर एक प्रदर्शनी के कुछ पोस्टर देखती हुई
समुदाय चिकित्सा केन्द्र, एम्स के शहरी सेवा विस्तार में झुग्गी से आए हुए रोगी बाह्य रोगी क्लिनिक में

भौतिक चिकित्सा और पुनर्वास विभाग में इलाज कराने के बाद अपने पैरों पर वापस खड़ा होने वाला रोगी
अधिकांश स्वास्थ्य सूचकांक देश में वर्ष 2000 के लिए तय किए गए, जिन्हें बल्लभगढ़ में पहले ही पूरा किया गया है। सीआरएचएसपी में शिशु मृत्यु दर राष्ट्रीय औसत के 74 की तुलना में प्रति हजार जीवित जन्म पर 54.6 है। इस आबादी में राष्ट्रीय आंकड़े के अनुसार प्रतिवर्ष 1,00,000 जीवित जन्म पर 200-400 की तुलना में माताओं की मृत्यु शून्य है। यहां बच्चों और गर्भवती महिलाओं के टीकाकरण का कवरेज 95 प्रतिशत से अधिक है और साथ ही यहां विटामिन ए, डायरिया के दौरान ओआरटी का उपयोग तथा बच्चों में निमोनिया का शीघ्र और उपयुक्त इलाज किया जाता है।
एम्स में अन्य विस्तार गतिविधियों में एक मॉडल समुदाय आधारित शहरी स्वास्थ्य परियोजना और नशा मुक्ति केन्द्र शामिल है।
On the 7th of September 1902, was born at Amravti in a family distinguished lawyers Bhalachandra Babaji Dikshit , Who was destined to play an important role in building up infrastructure in the medical arena in independent India(1) He deviated from the family tradition, and chose to become a doctor. He graduated from Grant Medical College, Bombay , in1925 .His nearly forty-year career had two almost exactly equal phases .During the first twenty years, he distinguished himself as a scientist ,and during the next twenty he revealed his remarkable human qualities as a loving teacher and ideal administrator. B.B. Dikshit, the scientist: 1926-1946
Dr Dikshit’s research career began in 1926, when he joined the Department of Pharmacology at the School of Tropical Medicine and Hygiene in Calcutta so that he could participate in the fascinating work being done there by Prof. R.N Chopra .Using what must appear today as simple equipment , he worked out the mechanism underlying the cardiovascular effects of anti malarial alkaloids, the efficacy of pseudo ephedrine present in the Indian variety of ephedra plants, and the reliability of narcotine as a substitute for morphine. He did all his within 3 years , and also earned a Diploma in Public Health in 1927.
In 1930m, at the young age of 28, Dr Dikshit was appointed Professor of Pharmacology at Medical College, Vishakhapatnam. There he evaluated one of the first anti-leprosy derivatives of chaulmoogra oil, and also studied the Efficacy and safety of pertain as a spinal anaesthetic. His work at Vishakapatnam was highly appreciated but he was relieved of his post unceremoniously in 1931 because as his termination letter clearly stated, an eligible pharmacologist belonging to the Madras Presidency had become available. The British apparently had no compunction in taking steps which would discourage feelings of national integration
In 1931,Dr.Dikshit left for Edinburgh with plans for obtaining membership of the Royal College of Physicians. He joined Prof. A.J Clark in the Department of Pharmacology. Prof. Clark was so impressed by Dr. Dikshit’s abilities that he offered him a teaching assistantship in Physiology-then a very unusual achievement for an Indian. Encouraged by this gesture, Dr. Diskhit obtained not only his M.R.C.P in 1933 but also his Ph.D. a year later. Dr. Dikshit’s work in Edinburgh was centered on acetylcholine as a central neurotransmitter: a topic not obsolete even today. He tackled it with simple techniques such as comparing the effects of stimulation of the central end of sectioned vagus nerve with those of injection of acetylcholine into lateral ventricles of the brain ,using agents such as atropine and physostigmine , and studying the effects of cerebrospinal fluid (CSF) obtained from animals whose cut vagi also studied the acetylcholine concentration in different parts of the brain, and interestingly found higher concentrations cortex. His work on acetylcholine is held in very high esteem, and is now a part of a classical literature in this area. At Edinburgh he also studied the relationship of hypothalamus to cardiac irregularities the effect of caffeine on this relationship and the effect of sodium barbitone on the cardiac irregularities. This work is relevant to the advice given to patients susceptible to cardiac arrhythmias regarding restriction of their intake of tea, coffee and cola drinks. Dr. Dikshit’s work done at Edinburgh was published in the Journal of Physiology (London) in the years 1933 and 1934. He returned to India in 1934.Soon after his return, he got married to Hirabai, a graduate and marathi poetess of distinction . She proved to be an able and understanding partner, stood by him through all the vicissitudes of life, and indirectly contributed to his achievements. After a short period of unemployment, he was offered a post at the Haffkine Institute in Bombay through a recommendation made by Dr. C.G. Pandit, who later become the first Indian Director of the Indian Research Fund Association (the precursor of ICMR)
At Haffkine Institute, Dr. Dikshit continued his work on acetylcholine, made a brief digression to immunology of malaria, did extensive studies on drugs used in malaria and plague , and also established a snake farm so that venoms and antivenoms could be studied .Since he was at Haffkine during World War II, he also got involved in work specially relevant to the armed forces. This work requires speed , originality and ingenuity because the problems are often queer, and no textbook formula holds. Dr. Dikshit proved himself equal to the task.
B.B. Dikshit, the teacher and administrator:1946-1964
In 1946, Dr. Dikshit was appointed Principal, and Professor of Physiology, at B.J Medical College ,Poona. The college ,which had earlier been training licentiates in medicine , was to be upgraded for training medical Graduates , and the task was entrusted to Dr. Dikshit. This assignment brought to the fore his abilities as a teacher and administrator, and his humane qualities .One responsibility handled well often brings another. In 1951 he was appointed Surgeon-General to the Government Of Bombay. His sphere widened to health care and medical education throughout the Bombay Presidency. But all for the greatest challenge yet to come-a challenge which none else in India could have faced the way he did. In 1956, the government established in New Delhi a center of excellence in medicine, which could serve as a model for the country and also supply research-oriented teachers for the rapidly growing number of medical colleges. The center was christened the All India Institute of Medical Sciences (AIIMS), and Dr. B.B Dikshit was invited to be its first Director. His appointment remains one of the best things that have happened to AIIMS since its inception.
At AIIMS, which was created as an autonomous institute outside the purview of the Medical Council Of India, Dr. Dikshit had the freedom to implement a curriculum which took into account the then latest advances in medical education and was at the same time relevant to national needs. Dr Dikshit’s inspiring leadership made some of the best Indian medical scientists working in different parts of the world give up attractive offers abroad to come and join the exciting experiment in innovative institution building going on at AIIMS. Establishments of Institutions like AIIMS was a part of nation building, a part of the vision Nehru had of an India that would rediscover and recover its greatness. The faculty, students, technicians , gardeners and sweepers , all worked as one family under the parental eye of Dr Dikshit to make AIIMS a name to reckon with in the medical arena.
As an administrator, Dr Dikshit was very clear headed . He refused to get entangled in extraneous or irrelevant factors. He would get to the core of the problem and given an un ambiguous, fair and just decision. His comments on files were characteristically brief-still remembered fondly as either ‘Yes, BBD’ or ‘No, BBD’. Moreover, he was one hundred percent genuine, absolutely without any pretensions. He would tell a person clearly on his face what he thought of an issue, and write exactly that on file. This is in clear contrast to a commonly held but erroneous view that administration is some sort of trickery or manipulation. Dr Dikshit had an intense regard for truth and justice. HE was violently allergic to falsehood, but entirely above prejudice. That made him very level headed. Even when he discovered something deplorable, he would size up the culprit, but within five minutes all will be forgotten. He would look at every issue, every file, afresh, on its own merits, absolutely without prejudice. He refused to let an event of yesterday affect his decision today. Even those whose demands he denied, respected and admired his writ because his decisions were base on principles, not on personal considerations.
Although Dr Dikshit was exceptional as an administrator, what ahs made him immortal is the love and respect with which he is remembered by many generations of students-at B.J Medical College and at AIIMS. He had enormous theoretical capabilities, admirable practical skills, and a highly developed talent for teaching. He also had a life-long love for sports, which gave him something in common with the youth . He was a university-level hockey player , and in later life took to tennis and badminton. But to attribute his popularity among students to how well he taught or played would do him gross injustice. He had an extremely genuine, intense and selfless paternal attitude to students, characterized by totally unconditional love, which did not expect anything I return. The result was that students were as sure of him as children below ten may or may not like everything about their parents , but one children below ten are of their parents. Children below ten may or may not like everything about their parents , but one thing they are totally sure about is that parents love them, have only their goods at heart , and will never ever deliberately do them any harm. Students felt exactly the same about Dr. Dikshit . Dr. C. G Pandit who got Dr Dikshit job at Haffkine Institute, and also recommended his name for the appointment at AIIMS, once confided that he was jealous of Dr. Dikshit for only one precious thing: he had been able to get from the students the type of love which Dr. Dikshit had received. Not just Dr. Pandit , hardly any teacher gets it because students are vary fair and choosy in bestowing their love on teachers.
It would be reasonable to ask what it was that made for him very natural a behaviour which most of us find very difficult. The answer comes form Prof. N.K. Bhide, his student at B.J Medical College in 1947 and later with him as a young faculty member at AIIMS: “Dr Dikshit had some deeply spiritual qualities. “ Only spirituality the ability and tendency to see a common spirit uniting us all-can fill a person with universal and selfless love of the kind Dr Dikshit had. It was this vision of oneness that made him obey and reward to a newly appointed guard who pointed to his cigarette when he was entering the library (a non-smoking area). He respected the guard’s authority with responsibility and detachment because in either case he looked at authority as a sacred duty entrusted by god rather than something to be relished as a power to subdue others. It was again made him deeply contented man. After he became the Director of AIIMS, he wanted nothing form anyone –the government, his friends, or his students. That is what made him fearless ,true and impartial . That is what made him refuse many invitations: he did not go abroad even once as Director of AIIMS. He preferred to be physically karmabhoomi so that he could give his maximum to the job carve out for him by destiny. Dr Dikshit epitomized the life-affirming brand of spirituality preached by the Gita:
He who is in Yoga, the pure soul, the master of his self who has conquered the senses, whose self becomes the self of all existences, even though he does works, he is not involved in them.
The end came exactly as it should for such a deeply spiritual man. He had a reasonably advance warning that the end was near, but remained physically mobile and mentally agile till the last day. His wife was hesitating to make a visit to her parental home in view of his unreliable coronaries but he encouraged her to take it easy and make the visit. She made a two-week visit, and he held on till she returned. The day after she returned, he said the final good bye to us all sharp, clear and quick, like all his decisions. A painless, prompt finale, and yet not so sudden end as to leave behind a trail of regrets and remorse. The hundredth’s birth anniversary of Dr B.B.Dikshit is an appropriate occasion for IJPP to salute this colossus among the architects of post-independence Indian renaissance.
I am grateful to Prof. Mohan B.Dikshit for providing invaluable material and to Prof. N.K Bhide for giving me an insight into the man that was Prof. B.B Dikshit
DEPARTMENT OF PHYSIOLOGY
ALL INDIA INSTITUTE OF MEDICAL SCIENCES
NEW DEHLI-110029
Coming soon
"The appointment for new case is available for one month ( depending upon the availability of OPD slots) from the date of applying for appointment and for the follow-up, the appointment is available for three months ( also depending upon the availability of OPD slots) from the date of applying for the appointment".
| Organizational Structure | ||||
| Notice for Constitution at AIIMS | ||||
| Institute Body (IB) | ||||
| Governing Body (GB) | ||||
| Finance Committee | Academic Committee | Selection Committee | Estate Committee | Hospital Affairs Committee |
| President I.B. (Shri. Jagat P. Nadda, Hon'ble Union Minister of health and Family Welfare) | |||||
| Administration | Finance | Dean | Hospital | Centres | Computer Facility |
| Additional Director (Administration) (Sh. Karan Singh) | Sr. Financial Advisor (Smt. Divya Yanamadala) | Dr. Kaushal Kr. Verma-- Dr. Jeewan Singh Titiyal-- Dr. C.S.Bal-- | Medical Superintendent Dr. Nirupam Madaan (Main Hospital) | Chief of the Centres | Prof-In-Charge Deputy Director |
| Administration | |||||
| Additional Director (Administration) | |||||
| Chief Administrative Officer | Dy. Secretary (Dr. R. Gopinath) | Chief Procurement Officer | Superintending Engg. (Sh Jeetendra Kr. Saxena) | Dy. Chief Security Officer | Public Relation Officer |
| Finance Division | ||||
| Sr. Financial Advisor (Sh. Mritunjaya Saini) | ||||
| Financial Advisor | F & CAO | Account Officer | Assistant Account Officer | Jr. Account Officer |
| Gr. A, B, C & D Staff | ||||
| Academics | |||||
| Dean | |||||
| Sub Dean | |||||
| Registrar (Dr. Girija Pd. Rath) | Examination Section Dean | Head of Departments | |||
| Academic Section | - | Faculty | |||
| Asstt. Prof. | Assoc. Prof. | Addl. Prof | Professor | ||
| Hospital | ||||||
| Medical Superintendent | ||||||
| Additional Medical Superintendent | ||||||
| Deputy Medical Superintendent | ||||||
| Duty Officers for OPD and Casualty | All Clinical Laboratories | Hospital Records | Wards, Private Wards & Operation | Hospital Peripheral Services Laundry, Blood Bank etc | Medical Stores | Nursing Service |
| Centres | ||||||
| Chiefs of Various Centres | ||||||
| Chief Dr. R. P. Centre (Dr. Jeevan S. Titiyal) | Chief N. S. Centre Dr. Shailesh B. Gaikwad | Chief C. T. Centre (Dr. Sandeep Chauhan) | Chief Dr. BRA,IRCH (Dr. Sushma Bhatnagar) | Chief JPNA Trauma Centre (Prof. Kamran Farooque) | Chief NDDTC, Ghaziabad (Dr. Rakesh Lal) | Chief CDER (Dr. Ritu Duggal) |
| Head of Departments | ||||||
| Faculty | ||||||
| Officers & Other Staff | ||||||
| Under Graduate students | ||||||
| Post Graduate students | ||||||
| Senior Resident, Junior Resident | ||||||
| SRF, JRF | ||||||
| Computer Facility |
| Prof-In-Charge Computer Facility |
| Dy. Director Computer Facility |
| System Analyst |
| Senior Programmer |
| Programmer |
| Shri. Jagat P.Nadda, Minister of Health and Family Welfare, Nirman Bhawan , N.D-110011 | President |
| Dr. Anil Jain, M.P (Rajya Sabha), D-244, Anupam Garden,Saiyad Ul Ajaib, New Delhi-68 | Member |
| Shri Ramesh Bidhuri, M.P (Lok Sabha) , H.No.179, Sunpath House,Village Tughlakabad, New Delhi-110044 | Member |
| Shri Manoj Kumar Tiwari, M.P (Lok Sabha) , 24, Mother Terrasa Crescent Marg,, New Delhi. | Member |
| Dr. K.Vijay Radhav, Former Principal Scientific Advisor | Member |
| Sh. K.Sanjay Murthy, Secretary to the Govt. of India, Dept. of Higher Education, M/o Human Resource Development, Shastri Bhawan, New Delhi-110001 | Member |
| Dr. Pranjal Modi, Vice Chancellor , Gujarat University of Transplantation Sciences, Opp. Trauma Centre, Civil Hospital Campus, Asarwa, Ahmedabad-380016, Gujarat | Member |
| Shri Rajesh Bhushan ,Secretary (H&FW),Govt. of India, Ministry of Health & Family Welfare ,Nirman Bhawan, New Delhi – 110011 | Member |
| Prof. Yogesh Singh, Vice Chancellor, University of Delhi, Delhi -110007 | Member (Ex-Officio) |
| Dr. Atul Goel, Director General of Health Services, Govt. of India, Nirman Bhawan, New Delhi-110011 | Member(Ex-Officio) |
| Prof. Vijay Kumar Shukla, Rector & Vice Chancellor, Banaras Hindu University, Varanasi-221005, U.P. | Member |
Dr. (Smt.) Vijay Laxmi Saxena ,Former General Secretary, Indian Sciences Congress Association, (ISCA), Kolkata, West Bengal-700017 Coordinator Bioinformatics, Infrastructure Facility Centre of DBT, (Govt. of India), Head of Department of Zoology, Dayanand, Girls P.G. College, Kanpur, 7/182, Swarup Nagar, Kanpur – 208002, U.P. | Member |
| Dr. Kameshwar Prasad, Director, Rajendra Institute of Medical Sciences, Bariatu, Ranchi-834009, Jharkhand | Member |
| Dr.Prem Nair, Medical Director, Amrita Institute of Medical Sciences, Elamakkara, P.O., Kochi-682041, Kerala | Member |
| Dr. S.Venkatesh, Principal Advisor, R.No.501, New Epidemiology Block, National Centre for Disease Control, 22, Sham Nath Marg, Delhi -110054 | Member |
| Sh. Ashish Srivastava, Addl. Secretary and Financial Adviser, Govt. of India, Ministry of Health & Family Welfare, Nirman Bhawan, New Delhi – 110011 | Member |
| Director, AIIMS | Member-Secretary |
| Shri Nilambuj Sharan, Economic Advisor, Govt. of India , Ministry of Health & Family Welfare, Nirman Bhawan, New Delhi – 110011 | Special Invitee |
| Dean, AIIMS | Special Invitee |
| Dr. D.K. Sharma ,Medical Supdt., AIIMS | Special Invitee |
| President of AIIMS | Chairman |
| Dr. Anil Jain, M.P (Rajya Sabha) | Member |
| Secretary (H&FW),GOI | Member |
| Secretary, Department of Higher Education, Ministry of Education, GOI | Member |
| Addl. Secretary & Financial Advisor, MoHFW, GOI | Member (Ex- Officio) |
| Director General of Health Services, GOI | Member (Ex- Officio) |
| Dr. Kameshwar Prasad, Director RIMS, Ranchi | Member |
| Dr. Pranjal Modi, Vice Chancellor, Gujarat University of Transplantation Sciences, Ahmadabad | Member |
| Vice Chancellor, Delhi University, New Delhi | Member |
| Prof. Vijay Kumar Shukla, Rector & Vice Chancellor, Banaras Hindu University | Member |
| Director, AIIMS, New Delhi | Member-Secretary |
| Secretary Ministry of Health & Family Welfare, Govt. Of India | Chairman |
| Shri Ramesh Bidhuri, Member of Parliament (Lok Sabha) | Member |
| Director General of Health Services, Min. Of Health & Family welfare , Govt. Of India | Member |
| Secretary, Department of Higher Education , Min. Of Education , Govt of India | Member |
| Dr. K Vijaya Raghvan, Principal Advisor to Govt. Of India | Member |
| Additional Secretary & Financial Advisor , Min. Of Health & Family welfare , Govt. Of India | Member |
| Dr. Pranjal Modi , Vice Chancellor , Gujarat University of Transplantation Sciences | Member |
| Director , AIIMS, New Delhi | Member Secretary |
Please note : this call center exclusively manages OPD appointments. We are unable to assist with any general hospital inquiries or other services."
11-26589141, 26589142, 26589143, 26589144
Timing for OPD booking on this Telephone is from 8:30 AM to 4:30 PM on Monday to Friday ( all working days). On Saturday (working day), the timing for OPD appointment booking is from 8:30 AM to 1:00 PM.
011-26589141, 26589142, 26589143, 26589144
"The appointment for new case is available for one month (depending upon the availability of OPD slots) from the date of applying for appointment and for the follow-up, the appointment is available for three months (also depending upon the availability of OPD slots) from the date of applying for the appointment".
Mobile App: The AIIMS App has been removed from the Google Play store due to issues with the app rendering it non-functional. Users who had installed that app should remove it from their devices.
For effective follow-up of post operative cardiac surgical patients at CTVS -OPD services, dedicated Helpline & Whatsapp numbers: 9999635940, 9999635425 will be active from 2:00pm to 6:00pm on Monday, Wednesday and Friday (i.e. otherwise usual OPD hours)/CTVS –OPD
Note:- If appointments are not available on O.R.S portal, then please do not call the call centre, as appointment through ORS portal and phone is from same pool.
Dr. Pranjal Modi, Vice Chancellor, Gujarat University of Transplantation Sciences | Chairman |
| Director General of Health Services,MoHFW, Govt. of India | Member |
| Vice Chancellor, Delhi University, New Delhi | Member |
| Secretary, Department of Higher Education, Ministry of Education, GOI | Member |
Prof. Vijay Kumar Shukla, Rector & Vice Chancellor, Banaras Hindu University, U.P. | Member |
Dr. Prem Nair, Medical Director, Amrita Institute of Medical Sciences, Kochi | Member |
Dr.(Smt.) Vijay Laxmi Saxena, Former General Secretary, Indian Science Congress Association, Kolkata | Member |
| Director, AIIMS, New Delhi | Member-Secretary |
Dr. Kameshwar Prasad, Director RIMS, Ranchi | Chairman |
| Director General of Health Services, MoHFW, Govt. of India | Member |
Prof. Vijay Kumar Shukla, Rector & Vice Chancellor, Banaras Hindu University, U.P. | Member |
Dr. S.Venkatesh, Principal Advisor, DGHS | Member |
| Vice Chancellor, Delhi University, New Delhi | Member |
Dr. Vijay Raghavan, Former Principal Scientific Advisor | Member |
Dr.Prem Nair, Medical Director, Amrita Institute of Medical Sciences, Kochi | Member |
| Director, AIIMS, New Delhi | Member-Secretary |
| Sh. Ramesh Bhiduri, M.P. ( Lok Sabha) | Chairman |
| Shri Manoj Kumar Tiwari, M.P (Lok Sabha) | Member |
Dr. (Smt.) Vijay Laxmi Saxena , Former General Secretary, Indian Sciences Congress Association, (ISCA), Kolkata | Member |
| Director General of Health Services, MoHFW,Govt. of India | Member |
| Vice Chancellor, Delhi University, New Delhi | Member |
| Addl. Secretary & Financial Advisor, MoHFW, GOI | Member |
Prof. Vijay Kumar Shukla, Rector & Vice Chancellor, Banaras Hindu University, U.P. | Member |
| Director, AIIMS | Member-Secretary |
| Sh. Ramesh Bhiduri, M.P. ( Lok Sabha) | Chairman |
| Shri Manoj Kumar Tiwari, M.P (Lok Sabha) | Member |
Dr. (Smt.) Vijay Laxmi Saxena , Former General Secretary, Indian Sciences Congress Association, (ISCA), Kolkata | Member |
| Director General of Health Services, MoHFW,Govt. of India | Member |
| Vice Chancellor, Delhi University, New Delhi | Member |
| Addl. Secretary & Financial Advisor, MoHFW, GOI | Member |
Prof. Vijay Kumar Shukla, Rector & Vice Chancellor, Banaras Hindu University, U.P. | Member |
| Director, AIIMS | Member-Secretary |
Dr. Kameshwar Prasad, Director RIMS, Ranchi | Chairman |
| Director General of Health Services, MoHFW, Govt. of India | Member |
Prof. Vijay Kumar Shukla, Rector & Vice Chancellor, Banaras Hindu University, U.P. | Member |
Dr. S.Venkatesh, Principal Advisor, DGHS | Member |
| Vice Chancellor, Delhi University, New Delhi | Member |
Dr. Vijay Raghavan, Former Principal Scientific Advisor | Member |
Dr.Prem Nair, Medical Director, Amrita Institute of Medical Sciences, Kochi | Member |
| Director, AIIMS, New Delhi | Member-Secretary |
Dr. Pranjal Modi, Vice Chancellor, Gujarat University of Transplantation Sciences | Chairman |
| Director General of Health Services,MoHFW, Govt. of India | Member |
| Vice Chancellor, Delhi University, New Delhi | Member |
| Secretary, Department of Higher Education, Ministry of Education, GOI | Member |
Prof. Vijay Kumar Shukla, Rector & Vice Chancellor, Banaras Hindu University, U.P. | Member |
Dr. Prem Nair, Medical Director, Amrita Institute of Medical Sciences, Kochi | Member |
Dr.(Smt.) Vijay Laxmi Saxena, Former General Secretary, Indian Science Congress Association, Kolkata | Member |
| Director, AIIMS, New Delhi | Member-Secretary |
Please note : this call center exclusively manages OPD appointments. We are unable to assist with any general hospital inquiries or other services."
11-26589141, 26589142, 26589143, 26589144
Timing for OPD booking on this Telephone is from 8:30 AM to 4:30 PM on Monday to Friday ( all working days). On Saturday (working day), the timing for OPD appointment booking is from 8:30 AM to 1:00 PM.
011-26589141, 26589142, 26589143, 26589144
"The appointment for new case is available for one month (depending upon the availability of OPD slots) from the date of applying for appointment and for the follow-up, the appointment is available for three months (also depending upon the availability of OPD slots) from the date of applying for the appointment".
Mobile App: The AIIMS App has been removed from the Google Play store due to issues with the app rendering it non-functional. Users who had installed that app should remove it from their devices.
For effective follow-up of post operative cardiac surgical patients at CTVS -OPD services, dedicated Helpline & Whatsapp numbers: 9999635940, 9999635425 will be active from 2:00pm to 6:00pm on Monday, Wednesday and Friday (i.e. otherwise usual OPD hours)/CTVS –OPD
Note:- If appointments are not available on O.R.S portal, then please do not call the call centre, as appointment through ORS portal and phone is from same pool.
| Secretary Ministry of Health & Family Welfare, Govt. Of India | Chairman |
| Shri Ramesh Bidhuri, Member of Parliament (Lok Sabha) | Member |
| Director General of Health Services, Min. Of Health & Family welfare , Govt. Of India | Member |
| Secretary, Department of Higher Education , Min. Of Education , Govt of India | Member |
| Dr. K Vijaya Raghvan, Principal Advisor to Govt. Of India | Member |
| Additional Secretary & Financial Advisor , Min. Of Health & Family welfare , Govt. Of India | Member |
| Dr. Pranjal Modi , Vice Chancellor , Gujarat University of Transplantation Sciences | Member |
| Director , AIIMS, New Delhi | Member Secretary |
| President of AIIMS | Chairman |
| Dr. Anil Jain, M.P (Rajya Sabha) | Member |
| Secretary (H&FW),GOI | Member |
| Secretary, Department of Higher Education, Ministry of Education, GOI | Member |
| Addl. Secretary & Financial Advisor, MoHFW, GOI | Member (Ex- Officio) |
| Director General of Health Services, GOI | Member (Ex- Officio) |
| Dr. Kameshwar Prasad, Director RIMS, Ranchi | Member |
| Dr. Pranjal Modi, Vice Chancellor, Gujarat University of Transplantation Sciences, Ahmadabad | Member |
| Vice Chancellor, Delhi University, New Delhi | Member |
| Prof. Vijay Kumar Shukla, Rector & Vice Chancellor, Banaras Hindu University | Member |
| Director, AIIMS, New Delhi | Member-Secretary |
| Shri. Jagat P.Nadda, Minister of Health and Family Welfare, Nirman Bhawan , N.D-110011 | President |
| Dr. Anil Jain, M.P (Rajya Sabha), D-244, Anupam Garden,Saiyad Ul Ajaib, New Delhi-68 | Member |
| Shri Ramesh Bidhuri, M.P (Lok Sabha) , H.No.179, Sunpath House,Village Tughlakabad, New Delhi-110044 | Member |
| Shri Manoj Kumar Tiwari, M.P (Lok Sabha) , 24, Mother Terrasa Crescent Marg,, New Delhi. | Member |
| Dr. K.Vijay Radhav, Former Principal Scientific Advisor | Member |
| Sh. K.Sanjay Murthy, Secretary to the Govt. of India, Dept. of Higher Education, M/o Human Resource Development, Shastri Bhawan, New Delhi-110001 | Member |
| Dr. Pranjal Modi, Vice Chancellor , Gujarat University of Transplantation Sciences, Opp. Trauma Centre, Civil Hospital Campus, Asarwa, Ahmedabad-380016, Gujarat | Member |
| Shri Rajesh Bhushan ,Secretary (H&FW),Govt. of India, Ministry of Health & Family Welfare ,Nirman Bhawan, New Delhi – 110011 | Member |
| Prof. Yogesh Singh, Vice Chancellor, University of Delhi, Delhi -110007 | Member (Ex-Officio) |
| Dr. Atul Goel, Director General of Health Services, Govt. of India, Nirman Bhawan, New Delhi-110011 | Member(Ex-Officio) |
| Prof. Vijay Kumar Shukla, Rector & Vice Chancellor, Banaras Hindu University, Varanasi-221005, U.P. | Member |
Dr. (Smt.) Vijay Laxmi Saxena ,Former General Secretary, Indian Sciences Congress Association, (ISCA), Kolkata, West Bengal-700017 Coordinator Bioinformatics, Infrastructure Facility Centre of DBT, (Govt. of India), Head of Department of Zoology, Dayanand, Girls P.G. College, Kanpur, 7/182, Swarup Nagar, Kanpur – 208002, U.P. | Member |
| Dr. Kameshwar Prasad, Director, Rajendra Institute of Medical Sciences, Bariatu, Ranchi-834009, Jharkhand | Member |
| Dr.Prem Nair, Medical Director, Amrita Institute of Medical Sciences, Elamakkara, P.O., Kochi-682041, Kerala | Member |
| Dr. S.Venkatesh, Principal Advisor, R.No.501, New Epidemiology Block, National Centre for Disease Control, 22, Sham Nath Marg, Delhi -110054 | Member |
| Sh. Ashish Srivastava, Addl. Secretary and Financial Adviser, Govt. of India, Ministry of Health & Family Welfare, Nirman Bhawan, New Delhi – 110011 | Member |
| Director, AIIMS | Member-Secretary |
| Shri Nilambuj Sharan, Economic Advisor, Govt. of India , Ministry of Health & Family Welfare, Nirman Bhawan, New Delhi – 110011 | Special Invitee |
| Dean, AIIMS | Special Invitee |
| Dr. D.K. Sharma ,Medical Supdt., AIIMS | Special Invitee |
"The appointment for new case is available for one month ( depending upon the availability of OPD slots) from the date of applying for appointment and for the follow-up, the appointment is available for three months ( also depending upon the availability of OPD slots) from the date of applying for the appointment".
| Notice for Constitution at AIIMS | ||||
| Institute Body (IB) | ||||
| Governing Body (GB) | ||||
| Finance Committee | Academic Committee | Selection Committee | Estate Committee | Hospital Affairs Committee |
| President I.B. (Shri. Jagat P. Nadda, Hon'ble Union Minister of health and Family Welfare) | |||||
| Administration | Finance | Dean | Hospital | Centres | Computer Facility |
| Additional Director (Administration) (Sh. Karan Singh) | Sr. Financial Advisor (Smt. Divya Yanamadala) | Dr. Kaushal Kr. Verma-- Dr. Jeewan Singh Titiyal-- Dr. C.S.Bal-- | Medical Superintendent Dr. Nirupam Madaan (Main Hospital) | Chief of the Centres | Prof-In-Charge Deputy Director |
| Administration | |||||
| Additional Director (Administration) | |||||
| Chief Administrative Officer | Dy. Secretary (Dr. R. Gopinath) | Chief Procurement Officer | Superintending Engg. (Sh Jeetendra Kr. Saxena) | Dy. Chief Security Officer | Public Relation Officer |
| Finance Division | ||||
| Sr. Financial Advisor (Sh. Mritunjaya Saini) | ||||
| Financial Advisor | F & CAO | Account Officer | Assistant Account Officer | Jr. Account Officer |
| Gr. A, B, C & D Staff | ||||
| Academics | |||||
| Dean | |||||
| Sub Dean | |||||
| Registrar (Dr. Girija Pd. Rath) | Examination Section Dean | Head of Departments | |||
| Academic Section | - | Faculty | |||
| Asstt. Prof. | Assoc. Prof. | Addl. Prof | Professor | ||
| Hospital | ||||||
| Medical Superintendent | ||||||
| Additional Medical Superintendent | ||||||
| Deputy Medical Superintendent | ||||||
| Duty Officers for OPD and Casualty | All Clinical Laboratories | Hospital Records | Wards, Private Wards & Operation | Hospital Peripheral Services Laundry, Blood Bank etc | Medical Stores | Nursing Service |
| Centres | ||||||
| Chiefs of Various Centres | ||||||
| Chief Dr. R. P. Centre (Dr. Jeevan S. Titiyal) | Chief N. S. Centre Dr. Shailesh B. Gaikwad | Chief C. T. Centre (Dr. Sandeep Chauhan) | Chief Dr. BRA,IRCH (Dr. Sushma Bhatnagar) | Chief JPNA Trauma Centre (Prof. Kamran Farooque) | Chief NDDTC, Ghaziabad (Dr. Rakesh Lal) | Chief CDER (Dr. Ritu Duggal) |
| Head of Departments | ||||||
| Faculty | ||||||
| Officers & Other Staff | ||||||
| Under Graduate students | ||||||
| Post Graduate students | ||||||
| Senior Resident, Junior Resident | ||||||
| SRF, JRF | ||||||
| Computer Facility |
| Prof-In-Charge Computer Facility |
| Dy. Director Computer Facility |
| System Analyst |
| Senior Programmer |
| Programmer |
Coming soon
On the 7th of September 1902, was born at Amravti in a family distinguished lawyers Bhalachandra Babaji Dikshit , Who was destined to play an important role in building up infrastructure in the medical arena in independent India(1) He deviated from the family tradition, and chose to become a doctor. He graduated from Grant Medical College, Bombay , in1925 .His nearly forty-year career had two almost exactly equal phases .During the first twenty years, he distinguished himself as a scientist ,and during the next twenty he revealed his remarkable human qualities as a loving teacher and ideal administrator. B.B. Dikshit, the scientist: 1926-1946
Dr Dikshit’s research career began in 1926, when he joined the Department of Pharmacology at the School of Tropical Medicine and Hygiene in Calcutta so that he could participate in the fascinating work being done there by Prof. R.N Chopra .Using what must appear today as simple equipment , he worked out the mechanism underlying the cardiovascular effects of anti malarial alkaloids, the efficacy of pseudo ephedrine present in the Indian variety of ephedra plants, and the reliability of narcotine as a substitute for morphine. He did all his within 3 years , and also earned a Diploma in Public Health in 1927.
In 1930m, at the young age of 28, Dr Dikshit was appointed Professor of Pharmacology at Medical College, Vishakhapatnam. There he evaluated one of the first anti-leprosy derivatives of chaulmoogra oil, and also studied the Efficacy and safety of pertain as a spinal anaesthetic. His work at Vishakapatnam was highly appreciated but he was relieved of his post unceremoniously in 1931 because as his termination letter clearly stated, an eligible pharmacologist belonging to the Madras Presidency had become available. The British apparently had no compunction in taking steps which would discourage feelings of national integration
In 1931,Dr.Dikshit left for Edinburgh with plans for obtaining membership of the Royal College of Physicians. He joined Prof. A.J Clark in the Department of Pharmacology. Prof. Clark was so impressed by Dr. Dikshit’s abilities that he offered him a teaching assistantship in Physiology-then a very unusual achievement for an Indian. Encouraged by this gesture, Dr. Diskhit obtained not only his M.R.C.P in 1933 but also his Ph.D. a year later. Dr. Dikshit’s work in Edinburgh was centered on acetylcholine as a central neurotransmitter: a topic not obsolete even today. He tackled it with simple techniques such as comparing the effects of stimulation of the central end of sectioned vagus nerve with those of injection of acetylcholine into lateral ventricles of the brain ,using agents such as atropine and physostigmine , and studying the effects of cerebrospinal fluid (CSF) obtained from animals whose cut vagi also studied the acetylcholine concentration in different parts of the brain, and interestingly found higher concentrations cortex. His work on acetylcholine is held in very high esteem, and is now a part of a classical literature in this area. At Edinburgh he also studied the relationship of hypothalamus to cardiac irregularities the effect of caffeine on this relationship and the effect of sodium barbitone on the cardiac irregularities. This work is relevant to the advice given to patients susceptible to cardiac arrhythmias regarding restriction of their intake of tea, coffee and cola drinks. Dr. Dikshit’s work done at Edinburgh was published in the Journal of Physiology (London) in the years 1933 and 1934. He returned to India in 1934.Soon after his return, he got married to Hirabai, a graduate and marathi poetess of distinction . She proved to be an able and understanding partner, stood by him through all the vicissitudes of life, and indirectly contributed to his achievements. After a short period of unemployment, he was offered a post at the Haffkine Institute in Bombay through a recommendation made by Dr. C.G. Pandit, who later become the first Indian Director of the Indian Research Fund Association (the precursor of ICMR)
At Haffkine Institute, Dr. Dikshit continued his work on acetylcholine, made a brief digression to immunology of malaria, did extensive studies on drugs used in malaria and plague , and also established a snake farm so that venoms and antivenoms could be studied .Since he was at Haffkine during World War II, he also got involved in work specially relevant to the armed forces. This work requires speed , originality and ingenuity because the problems are often queer, and no textbook formula holds. Dr. Dikshit proved himself equal to the task.
B.B. Dikshit, the teacher and administrator:1946-1964
In 1946, Dr. Dikshit was appointed Principal, and Professor of Physiology, at B.J Medical College ,Poona. The college ,which had earlier been training licentiates in medicine , was to be upgraded for training medical Graduates , and the task was entrusted to Dr. Dikshit. This assignment brought to the fore his abilities as a teacher and administrator, and his humane qualities .One responsibility handled well often brings another. In 1951 he was appointed Surgeon-General to the Government Of Bombay. His sphere widened to health care and medical education throughout the Bombay Presidency. But all for the greatest challenge yet to come-a challenge which none else in India could have faced the way he did. In 1956, the government established in New Delhi a center of excellence in medicine, which could serve as a model for the country and also supply research-oriented teachers for the rapidly growing number of medical colleges. The center was christened the All India Institute of Medical Sciences (AIIMS), and Dr. B.B Dikshit was invited to be its first Director. His appointment remains one of the best things that have happened to AIIMS since its inception.
At AIIMS, which was created as an autonomous institute outside the purview of the Medical Council Of India, Dr. Dikshit had the freedom to implement a curriculum which took into account the then latest advances in medical education and was at the same time relevant to national needs. Dr Dikshit’s inspiring leadership made some of the best Indian medical scientists working in different parts of the world give up attractive offers abroad to come and join the exciting experiment in innovative institution building going on at AIIMS. Establishments of Institutions like AIIMS was a part of nation building, a part of the vision Nehru had of an India that would rediscover and recover its greatness. The faculty, students, technicians , gardeners and sweepers , all worked as one family under the parental eye of Dr Dikshit to make AIIMS a name to reckon with in the medical arena.
As an administrator, Dr Dikshit was very clear headed . He refused to get entangled in extraneous or irrelevant factors. He would get to the core of the problem and given an un ambiguous, fair and just decision. His comments on files were characteristically brief-still remembered fondly as either ‘Yes, BBD’ or ‘No, BBD’. Moreover, he was one hundred percent genuine, absolutely without any pretensions. He would tell a person clearly on his face what he thought of an issue, and write exactly that on file. This is in clear contrast to a commonly held but erroneous view that administration is some sort of trickery or manipulation. Dr Dikshit had an intense regard for truth and justice. HE was violently allergic to falsehood, but entirely above prejudice. That made him very level headed. Even when he discovered something deplorable, he would size up the culprit, but within five minutes all will be forgotten. He would look at every issue, every file, afresh, on its own merits, absolutely without prejudice. He refused to let an event of yesterday affect his decision today. Even those whose demands he denied, respected and admired his writ because his decisions were base on principles, not on personal considerations.
Although Dr Dikshit was exceptional as an administrator, what ahs made him immortal is the love and respect with which he is remembered by many generations of students-at B.J Medical College and at AIIMS. He had enormous theoretical capabilities, admirable practical skills, and a highly developed talent for teaching. He also had a life-long love for sports, which gave him something in common with the youth . He was a university-level hockey player , and in later life took to tennis and badminton. But to attribute his popularity among students to how well he taught or played would do him gross injustice. He had an extremely genuine, intense and selfless paternal attitude to students, characterized by totally unconditional love, which did not expect anything I return. The result was that students were as sure of him as children below ten may or may not like everything about their parents , but one children below ten are of their parents. Children below ten may or may not like everything about their parents , but one thing they are totally sure about is that parents love them, have only their goods at heart , and will never ever deliberately do them any harm. Students felt exactly the same about Dr. Dikshit . Dr. C. G Pandit who got Dr Dikshit job at Haffkine Institute, and also recommended his name for the appointment at AIIMS, once confided that he was jealous of Dr. Dikshit for only one precious thing: he had been able to get from the students the type of love which Dr. Dikshit had received. Not just Dr. Pandit , hardly any teacher gets it because students are vary fair and choosy in bestowing their love on teachers.
It would be reasonable to ask what it was that made for him very natural a behaviour which most of us find very difficult. The answer comes form Prof. N.K. Bhide, his student at B.J Medical College in 1947 and later with him as a young faculty member at AIIMS: “Dr Dikshit had some deeply spiritual qualities. “ Only spirituality the ability and tendency to see a common spirit uniting us all-can fill a person with universal and selfless love of the kind Dr Dikshit had. It was this vision of oneness that made him obey and reward to a newly appointed guard who pointed to his cigarette when he was entering the library (a non-smoking area). He respected the guard’s authority with responsibility and detachment because in either case he looked at authority as a sacred duty entrusted by god rather than something to be relished as a power to subdue others. It was again made him deeply contented man. After he became the Director of AIIMS, he wanted nothing form anyone –the government, his friends, or his students. That is what made him fearless ,true and impartial . That is what made him refuse many invitations: he did not go abroad even once as Director of AIIMS. He preferred to be physically karmabhoomi so that he could give his maximum to the job carve out for him by destiny. Dr Dikshit epitomized the life-affirming brand of spirituality preached by the Gita:
He who is in Yoga, the pure soul, the master of his self who has conquered the senses, whose self becomes the self of all existences, even though he does works, he is not involved in them.
The end came exactly as it should for such a deeply spiritual man. He had a reasonably advance warning that the end was near, but remained physically mobile and mentally agile till the last day. His wife was hesitating to make a visit to her parental home in view of his unreliable coronaries but he encouraged her to take it easy and make the visit. She made a two-week visit, and he held on till she returned. The day after she returned, he said the final good bye to us all sharp, clear and quick, like all his decisions. A painless, prompt finale, and yet not so sudden end as to leave behind a trail of regrets and remorse. The hundredth’s birth anniversary of Dr B.B.Dikshit is an appropriate occasion for IJPP to salute this colossus among the architects of post-independence Indian renaissance.
I am grateful to Prof. Mohan B.Dikshit for providing invaluable material and to Prof. N.K Bhide for giving me an insight into the man that was Prof. B.B Dikshit
DEPARTMENT OF PHYSIOLOGY
ALL INDIA INSTITUTE OF MEDICAL SCIENCES
NEW DEHLI-110029
Coronary bypass surgery in progress at Cardiothoracic Centre, AIIMS
Shri Devi Ram, the first heart transplant patient in India, operated on 3 August 1994 at AIIMS.
A patient undergoing laser treatment at Dr.Rajendra Prasad Centre for Ophthalmic Sciences,AIIMS.
The hi-tech facilities and nursing care at AIIMS have contributed a lot to the survival of these quadruplets
BCR green signals ABL red signals Arrows show fusion signals
A neurosurgical patient being prepared for treatment with the recetly installed gamma knife
A patient undergoing investigation at the state-of-the-art Magnetic Resonance Imaging facility of AIIMS.
A multichannal autoanalyser which can give quick estimation of several parameters of blood chemistry using a very small blood sample.
AIIMS strives hard to make world class clinical care available to millions of underprivileged citizens of India and neighboring countries. While its magnificent buildings and hi-tech facilities may create a superficial image of elitism, a visit to AIIMS is enough to dispel any such illusion
Its corridors are thronged by patients, most of them too poor to afford quality treatment elsewhere. They come here with high hopes because of the reputation which AIIMS as built up. AIIMS is at present, not a single hospital but a conglomerate of facilities .It has over 1500 spread over the main hospital, Dr. Rajendra Prasad Centre for Ophthalmic sciences, Cardiothoracic Centre, Neurosciences Centre, Institute Rotary Centre Hospital and De-addiction Centre. This complex of facilities caters to about 1.5 million outpatients and 80,000 inpatients every year .The number of surgical operations performed at AIIMS last year was over 100,000.
However, the strength of AIIMS lies not in numbers, but in availability under one roof of the best team of medical and surgical experts, state-of-the-art equipment, and our capacity to rise to the occasion to meet diagnostic or public health challenges.Be it the autoanalyser or the linear accelerator,magnetic resonance imaging or the gamma knife, AIIMS has them all. Once something new arrives on the scene,someone, somewhere in the Institute takes the initiative and musters the energy and drive required to get it
Among the areas pioneered by AIIMS are cardiac catheterization,heart valve surgery, porto-caval surgery, neonatal surgery,jointreplacement, cochlear implant and multi organ transplants (cornea, kidney,bone marrow,heart and liver).Our results in sophisticated medical and surgical care are among the best in the world. The most satisfying aspect of this endeavour is that these cutting- edge modalities are being actually used for is that poor.
The role of AIIMS in patient care is not confined to our own hospital.AIIMS has trained physicians and surgeons who have fanned out across the country and abroad.For decades a large proportion of neurologists, neurosurgeons, cardiac surgeons, paediatric surgeons and gastroenterologists were from AIIMS,simply because we were the first to start courses in these superspecialities.New we have D M courses also in endocrinology and medical oncology.The nation has invested heavily in AIIMS from its doubt that AIIMS meager resources in an attempt to provide the best possible health care to its people irrespective of their paying capacity. Few would has fulfilled its commitment.
An interphase cell from a Philadelphia Chromosome positive patient having chronic myeloid leukemia.The cellshows b c r/ a b/chimeric fusion gene(oncogene). The yellow signal represents overlapping of b c r green)and a b/ (red) signals.
The comprehensive rural health services project (CRHSP) was at established, ballabgarh, about 35 km from AIIMS, to serve as a model for delivery of health care to the villages of india. It consist of a subdivisional hospitals and network of a primary health centres, subcentres and health workers. Its unique feature is a strong element of participation of the community in its own care. The project has demonstrated their major improvement in health can be achieved with modest resources.
Mrs.Renuka Chowdhury,Minister of Health & Family Welfare and President of AIIMS, looking at some posters at an exhibition on Lifestyle and Health after inaugurating it at AIIMS on 25 september 1997
An outdoor out patient clinic in a slum at the urbal extension service of Center for Community Medicine, AIIMS.
Back on his feet. A patient undergoing treatment in the Department of Physical Medicine and Rehabilitation
Most of the health indices set as a goals for the country for the year 2000 have already been achieved in the ballabgarh block. The infant morality rate in CRHSP is 54.6 per 1000 live births per year against the national average is 74.There are no maternal deaths in this population against a national figure of 200-400 per 1,00,000 live births per year. Immunization coverage of children and pregnant women is over 95% as is the coverage for vitamin A, ORT use during diarrhea and early appropriate treatment of pneumonia in children.
Extension activities of AIIMS include a model community-based urban health project and a De-addiction Centres.
It is science Alone that can solve the problems of hunger and poverty, insanitation and illiteracy, of superstition and deadening custom and tradition, of vast resourses running to waste, of a rich country inhabited by starving people.
Jawaharlal Nehru
At AIIMS research is not just a routine activity but rather a mission with three objectives. As anywhere else, the primary purpose of research is to gratify curiosity by disciplined activity, thereby leading to creation of new knowledge. But at AIIMS, we are also conscious of the role research can play in improving the quality of teaching. A teacher engaged in research is up to date with recent information, and can also inculcate a sprit of enquiry and freedom of thought into his/her students. Finally, research at AIIMS is apart of our national endeavor to cultivate a scientific temper and to eliminate from our society the way of authority and superstition.
Research at AIIMS is a part of our national endaeavour to cultivate a scientific temper and to eliminate from our society the sway of authority and superstition .
While AIIMS attracts sizeable grants from national and international agencies, the Institution itself also offers modest research grants. The grants are sanction after the projects submitted have been screened by a Committee and are primary meant to initiate the junior faculty into research. Thus, other things being equal, preference is given to younger application. After an investigator has made some progress, he or she can apply for bigger grants from other agencies.
There is a wide variety of research performed at AIIMS. On the one hand we do sophisticated investigations in the neurosciences, in genetics and on computer simulation of hormone-receptor interaction. On the other hand ,we undertake clinical and epidemiological studies on the prevention and treatment of national health problems. We are trying to apply advanced techniques such as DNA recombinant technology, immunology and electron microscopy to study the common diseases in our country such as leprosy, malaria , tuberculosis, diabetes, diarrhoea, hepatitis, fluorosis and iodine deficiency. We have large internationally funded programmes on goals-oriented research in reproduction aimed at widening the variety of acceptable contraceptives. The scientific publications emanating from the Institute have been quite steady at about 2 publications per faculty member per year. about half of these publications are in journals covered by the Science Citation Index. During the 8 year period from 1980-88, AIIMS topped the list of medical colleges in India with (mean ± SD) 237.5 ± 37.3 Science Citation index-listed publications per year (Reddy et al. Natl Med J India 1991; 4: 90-92).During the 7 year period from 1987-94, AIIMS topped the list of institutions engaged in medical research in India with 1630 Medline-listed publications (Arunachalam. Current Science 1997; 72:912-922).
The quality and range of research at AIIMS may be judged from the following highly selected assortment of some thrust areas.
Control of Diarrheal disease
In 1980s,40% of pediatric beds in hospitals were occupied by cases of diarrheal dehydration. In 1997 it is difficult to find such a case even for demonstration in many parts of India. Basic, applied and operational research done at AIIMS has played a pivotal role in achieving this transformation. Recently we have developed two types of super oral dehydration solutions based on amino concentration.
We are trying to apply advanced techniques such as DNA recombinant technology,immunology and electron microscopy to study the common diseases in our country.
WHO will formally introduce this new formulation in the Global Diarrheal Disease Control Programme this year. AIIMS has developed an algorithm for the treatment of persistent diarrhea, which the WHO introduced in the Global Diarrheal Disease Control Programme in 1994. The bacteriumresponsible for 50% of the cases of persistent diarrhea has been discovered at AIIMS and provisionally named Enteroaggregative E.coli.AIIMS research on the role of zinc deficiency in diarrheal disease was cited by the "Time Magazine" in 1996 as good news for child health.
Rotavirus was demonstrated at AIIMS to be the major cause of diarrheal disease. Now we have developed a rotavirus vaccine in collaboration with the Department of Biotechnology, which is ready for phase-1 trials to be started this year.
AIIMS has developed a PCR test for the diagnosis of tuberculosis. The test, which is specially useful for extrapulmonary tuberculosis, gives the diagnosis within 24-48 hours of receiving the sample in contrast with conventional tests which take 6-8 weeks.Leprosy
Contributions of AIIMS towards research on this dreaded disease include:
A behavioural physiology study in progress.
By using modern DNA technologies at AIIMS, it has now become possible for the first time in India to study the strains of the parasite responsible for an epidemic.
AIIMS has developed indigenously a highly sensitive and specific ELISA system for detecting HIV antibodies. It costs less than half the imported test kits, and has detected many early cases which the imported kits could not.
AIIMS has developed indigenously a highly sensitive and specific ELISA system for detecting HIV antibodies.It costs less than half the imported test kits, and has detected many early cases which the imported kits could not. AIIMS has been one of the Reference Centres for HIV/AIDS since 1986, and the National HIV Reference Centre since 1992.
Epidemiological, clinical and basic research at AIIMS has assessed the magnitude of the problem, led to the development of an indigenous diagnostic test and a candidate vaccine, and a diagnostic assay system for screening blood donors for hepatitis C virus.
Diagnostic Test For Plague
AIIMS was the first place in the world to use PCR on formaline fixed autopsy material to detect and confirm plague during the1994 outbreak. We have cloned, sequenced and expressed the f1 and pla genes of Yersinia pestis which are immunoreactive. These are being used for developing a serological test for plague.
AIIMS has defined the effect of iodine deficiency on growth and development, specially the role of thyroxine in brain development in human fetuses. Laboratory and field studies done at AIIMS paved the way for the 'Universal Salt Iodization Programme of the Government of India in 1986.Our Contributions to control of iodine deficiency extend to Bhutan, Nepal, Bangladesh, Maldives, Indonesia, Thailand and several countries of Africa and the middle east.
Titration method for estimation of iodine in salt.
This simple is very important for ensuring the success of the universal salt
Much of the research that has been carried out in the last 25 years towards the development of an anti-human chronic gonadotropin (hCG) vaccine began with research initially carried out at AIIMS.
Morphometric analysis of immuno cytochemically stained endometrium and photomicrography inprogres in the Primate Implantation Biology Laboratory.
Basic Research on the endocrine and paracrine mechanisms in embryo implantation of pregnancy and the development of post-coital and post-ovulatory contraceptives.Our Primate Implantation Biology Laboratory has been recognized as a non-US Centre for Contraceptive Research and Development Programme of the Andrew Mellon Foundation and is also one of the 13 such Centres in the world supported on a long-term basis by the Rockefeller Foundation.
AIIMS has been participating in India's efforts at exploration of Antarctica since 1990.Besides providing health care to members of the expedition, AIIMS has also been using the opportunity to conduct research on chronobiology of the human organism, physiological responses to the stress of the hostile antarctic environment, and performance under the harsh and lonely conditions prevailing in antarctica.
The library, named after the first Director of the Institute, is a treasure house having 61423 books, 53547 journals and 14008 reports in the field of Biomedical Sciences. The library receives 490 journals and 80 newsletters every year. The library is open to the readers from 8 a.m. to 2 a.m seven days a week. The Library has a computer facility, microfilm library reader and reader-printer facility The rich and efficient is a potent force for energizing our research activities.
A particulary busy hour in the B.B.Dikshit Library.
The Academic Section develops policy and plans and executes academic activities at AIIMS, New Delhi. These activities encompass the undergraduate, postgraduate and doctoral programmes for medical, nursing and paramedical courses. These activities are conducted by the undergraduate, postgraduate and paramedical cells.
The section handles post-admission formalities for new students, develops and revises curricula and administers teaching programmes including internal assessment of undergraduate students admitted to various courses. The courses include MBBS, BSc (Hons) Medical Technology in Radiography, Ophthalmic Techniques, Operation Theatre Technology, BSc Dental Hygiene, BSc Dental Operating Room Assistant (DORA), BSc Nursing (Post-certificate) and BSc (Hons) Nursing courses.
The pattern of education in MBBS course was reviewed and re-structured in July 2004. The MBBS course is of 5½ years duration and comprises of 3 phases and internship. The details are as follows:
| Phase | Duration (years) | Training |
|---|---|---|
| First | One | Pre-Clinical |
| Second | One-and-a-half | Para-clinical |
| Third | Two | Clinical |
| Internship | One | Compulsory rotation in various departments |
At present, 125 Indian students are admitted every year to the MBBS course (51 General category, 34 Other Backward Classes, 12 Economically Weaker Section (EWS) category, 19 Scheduled Caste and 9 Scheduled Tribe). For persons with disabilities (PWD), 5% reservation was provided on a horizontal basis. Seven foreign national students are also admitted each year. Beginning 2020, these admissions are made based on merit through the National Eligibility Entrance Test (NEET) conducted by the National Testing Agency.
As on 31 March 2021, 523 MBBS students including 73 interns were on rolls. Nine meritorious MBBS students were awarded scholarships for securing first, second and third positions in the first, second and final phase of professional examinations.
In 2020–2021, 98 students (38 General category, 10 EWS Category, 15 Scheduled Caste, 7 Scheduled Tribe and 26 Other Backward Classes, 2 Foreign Nationals) were admitted in BSc (Hons) Nursing course. For BSc Nursing (Post-certificate) course, 45 students (21 General category, 8 Scheduled Caste, 3 Scheduled Tribe, 9 Other Backward Classes, 3 EWS and 1 foreign national candidates) were admitted.
Students admitted to various BSc courses were:
| Course | General | SC | ST | OBC | EWS | Total |
|---|---|---|---|---|---|---|
| Opthalmic Techniques | 9 | 2 | 2 | 5 | 2 | 20 |
| Medical Technology in Radiology | 5 | 1 | 1 | 3 | 1 | 11 |
| Operation Theatre Technology | 1 | 1 | 1 | 2 | 1 | 6 |
| Dental Hygiene | 1 | 1 | 0 | 2 | 1 | 5 |
| Dental Operating Room Assistant | 2 | 2 | 1 | 3 | 2 | 10 |
The number of students on rolls in these courses as on 31st March 2021 were:
| Course | Number of Students |
|---|---|
| Nursing | - |
| B.Sc Nursing (Post -basic) | 78 |
| B.Sc (Hons) Nursing | 323 |
| Paramedical | - |
| B.Sc (Hons) Ophthalmic Techniques | 74 |
| B.Sc (Hons) Medical Technology in Radiology | 39 |
| B.Sc Operation Theatre Technology | 31 |
| B.Sc Dental Hygiene | 11 |
| B.Sc Dental Operating Room Assistant | 22 |
The Academic Section looks after all activities pertaining to admission and training of postgraduate students including junior and senior residents. It handles all activities related to Fellowship, PhD, DM, MCh, MD, MS, MDS, MCh/DM (Direct 6 years course), M Biotechnology (MBiotech) and MSc courses in different disciplines.
Admissions to all postgraduate courses for Indian nationals as well as sponsored candidates are made through an All-India Entrance Examination held twice a year for all postgraduate courses except MSc, MSc Nursing and MBiotechnology courses, for which the examination is held once a year. Foreign nationals are admitted under the sponsored category through the same entrance examination. In 2020–21, 748 students were admitted in various courses. The number of postgraduate and doctoral students on roll on 31 March 2021 was 1966.
Admissions in various courses
| Sr. No. | Name of Course | July 2020 | January 2021 | Total |
|---|---|---|---|---|
| 1 | MSc /MBiotech/ MSc Nursing (August) | 76 | * | 76 |
| 2 | MD / MS/ MDS/ MCh/ DM (Direct 6 Years) second | 260 | 186 | 446 |
| 3 | DM / MCh | 96 | 105 | 201 |
| 4 | PhD | 53 | 37 | 90 |
| 5 | Fellowship | 17 | 22 | 39 |
| Total | 502 | 350 | 852 |
*Admissions are done once in a year.
Postgraduate students on rolls
| Sr. No. | Name of Course | Number of Students on roll |
|---|---|---|
| 1 | PhD | 295 |
| 2 | DM | 363 |
| 3 | MCh | 174 |
| 4 | Fellowship programme | 49 |
| 5 | MD | 766 |
| 6 | MS | 115 |
| 7 | MDS | 67 |
| 8 | MSc / MBiotech / MSC Nursing | 156 |
| Total | 1985 |
Information Pertaining to Academic Section for the year 2013-2014
No. of students On-Roll in various courses at AIIMS as on 31/3/2014: | |||
| 1 | MBBS Students | - | 383 |
| 2 | B.Sc. (Hons.)Nursing Students
| - | 393 |
| 3 | MD,MS,MDS,MHA & M.Ch.(6 years) Students | - | 655 |
| 4 | DM & MCH Students | - | 224 |
| 5 | Ph. D. Students | - | 419 |
| 6 | M.Sc., M.Sc. Nursing & M.Biotechnology Students | - | 109 |
No. of students who have been awarded degrees till 41st Convocation held in 2013: | |||
| 1 | MBBS | - | 2646 |
| 2 | B.Sc.(Hons.) Nursing, | - | 2674 |
| 3 | MD,MS,MDS,MHA & M.Ch. (6 years) | - | 5198 |
| 4 | DM & MCH | - | 1344 |
| 5 | Ph. D. | - | 996 |
| 6 | M.Sc., M.Sc. Nursing & M. Biotechnology | - | 764 |
AIIMS was created in 1956 to serve as a nucleus for nurturing excellence in all aspects of health care
Creating a country imbued with a scientific culture was Jawaharlal Nehru's dream, and immediately after independence he prepared a grand design to achieve it. Among the temples of modern India which he designed, was a centre of excellence in the medical sciences. Nehru's dream was that such a centre would set the pace for medical education and research in Southeast Asia , and in this he had the wholehearted support of his Health Minister, Rajkumari Amrit Kaur.
The health survey and development committee ,chaired by Sir Joseph Bhore, an Indian Civil Servant ,had in 1946 already recommended the establishment of a national medical centre which would concentrate on meeting the need for highly qualified manpower to look after the nation's expanding health care activities . The dreams of Nehru and Amrit Kaur and the recommendations of the Bhore Committee converged to create a proposal which found favor with the government of New Zealand. A generous grant from New Zealand under the Colombo Plan made it possible to lay the foundation stone of All India Institute of Medical Sciences (AIIMS) in 1952.The AIIMS was finally created in 1956,as an autonomous institution through an Act of Parliament ,to serve as a nucleus for nurturing excellence in all aspect of health care.
All-India Institute of Medical Sciences was established as an institution of national importance by an Act of Parliament with the objects to develop patterns of teaching in Undergraduate and Post-graduate Medical Education in all its branches so as to demonstrate a high standard of Medical Education in India; to bring together in one place educational facilities of the highest order for the training of personnel in all important branches of health activity; and to attain self-sufficiency in Post-graduate Medical Education.
The Institute has comprehensive facilities for teaching, research and patient-care. As provided in the Act, AIIMS conducts teaching programs in medical and para-medical courses both at undergraduate and postgraduate levels and awards its own degrees. Teaching and research are conducted in 42 disciplines. In the field of medical research AIIMS is the lead, having more than 600 research publications by its faculty and researchers in a year. AIIMS also runs a College of Nursing and trains students for B.Sc.(Hons.) Nursing post-certificate degrees.
Twenty-five clinical departments including four super specialty centers manage practically all types of disease conditions with support from pre- and Para-clinical departments. However, burn cases, dog-bite cases and patients suffering from infectious diseases are not entertained in the AIIMS Hospital. AIIMS also manages a 60-beded hospital in the Comprehensive Rural Health Centre at Ballabgarh in Haryana and provides health cover to about 2.5 lakh population through the Centre for Community Medicine.
The Apps are designed, developed and maintained by AIIMS, New Delhi. Though all efforts have been made to ensure the accuracy and currency of the content on this app, the same should not be construed as a statement of law or used for any legal purposes. In case of any ambiguity or doubts, users are advised to verify/check with the Department(s) and/or other source(s), and to obtain appropriate professional advice. Under no circumstances will this Department be liable for any expense, loss or damage including, without limitation, indirect or consequential loss or damage, or any expense, loss or damage whatsoever arising from use, or loss of use, of data, arising out of or in connection with the use of this app. These terms and conditions shall be governed by and construed in accordance with the Indian Laws. Any dispute arising under these terms and conditions shall
be subject to the jurisdiction of the courts of India.
You must comply with App T&Cs as these apply to your use of the Apps and the Service T&Cs apply to your use of the Service that you access and use through the Apps. Any violation of these Apps T&Cs or the Service T&Cs may result in the termination of your access to the Apps and/or the Service.
The Apps are for your own personal use only. Any commercial use will result in termination of your access to the app and service. You cannot distribute or copy or modify any part of it in any way.
You must not attempt to extract any source code from the Apps, disassemble it or make any derivative versions, or attempt to interrupt or decipher the transmissions between the Apps and our systems.
The user of the apps must not use the app for any the following
The Apps and all copyright, database rights, and other intellectual property rights related to them belong to AIIMS New Delhi.
Privacy Policy
This privacy policy governs your use of the mobile applications (Apps) that are hosted at AIIMS New Delhi Mobile App Account in Google Play Store and Apple App Store. The contents published on these Applications were provided by the concerned
Ministries/Departments of AIIMS New Delhi. This information provided through these applications may not
have any legal sanctity and are for general reference only, unless otherwise specified. However, every effort has been made to provide accurate and reliable information through these applications. Users are advised to verify the correctness
of the facts published here from the concerned authorities. AIIMS New Delhi will not be responsible for the accuracy and correctness of the contents available in the application.
AIIMS New Delhi has built multiple free mobile applications. These mobile applications are provided by AIIMS at no cost and is intended for use as is by the general public and the employees of the institute.
This page is used to inform visitors regarding our policies with the collection, use, and disclosure of Personal Information if anyone decides to use these services.
If you choose to use these services, then you agree to the collection and use of information in relation to this policy. The Personal Information that is collected is used for providing and improving the services. AIIMS will not use or share your information with anyone except as described in this Privacy Policy.
Information Collection and Use
The Applications may obtain the information you provide when you download and register the Application. Registration is optional. However, please keep in mind that you may not be able to use some of the features offered by an Application unless you register.
For a better experience, while using our Service, we may require you to provide us with certain personally identifiable information, including but not limited to the phone number. When you register and use the Application, you generally provide (a) your name, email address, age, user name, password and other registration information; (b) download or use applications from us; (c) information you provide when you contact us for help and (d) information you enter into our system when using the Application, such as contact information and other details.
The information you provided may be used to contact you from time to time to provide you with important information and required notices.
The app does use any third party services that may collect information used to identify you.
Automatically Collected Information
In addition, the Application may collect certain information automatically, including, but not limited to, the type of mobile device you use, your mobile devices unique device ID, the IP address of your mobile device, your mobile operating system, the type of mobile Internet browsers you use, and information about the way you use the Application.
When you visit the mobile application, it may use GPS technology (or other similar technology) to determine your current location in order to determine the city you are located within and display a location map. The location information
may be sent to authorities for taking necessary actions and making policy decisions.
If you do not want the app to use your location for the purposes set forth above, you should turn off the location services for the mobile application located in your account settings or in your mobile phone settings and/or within the mobile
application. However, if the service provided by the Application requires the location services using GPS technology, such services offered by the application will not be available to you.
We may disclose User provided and Automatically Collected Information as required by law, such as to comply with a subpoena, or similar legal process when we believe in good faith that disclosure is necessary to protect our rights, protect
your safety or the safety of others, investigate fraud, or respond to a government request with our trusted service providers who work on our behalf, do not have an independent use of the information we disclose to them, and have agreed to adhere to the rules set forth in this privacy statement.
You can stop all collection of information by the Application easily by uninstalling the Application. You may use the standard uninstall processes as may be available as part of your mobile device or via the mobile application marketplace or network.
Data Retention Policy, Managing Your Information
We will retain User provided data for as long as you use the Application and for a reasonable time thereafter. We will retain Automatically Collected information also for a reasonable period of time depending on the nature of application and
thereafter may store it in aggregate. Please note that some or all of the User Provided Data may be required in order for the Application to function properly.
Misuse by Non Targeted Users
All mobile apps are meant for use by the targeted audience only. Misuse by nontargeted users should be prevented by owner of the mobile.
Security
We are concerned about safeguarding the confidentiality of your information. We provide physical, electronic, and procedural safeguards to protect information we process and maintain. For example, we limit access to this information to authorized employees and contractors who need to know that information in order to operate, develop or improve our Application. Please be aware that, although we endeavour to provide reasonable security for information we process and maintain, no security system can prevent all potential security breaches.
Your Consent
By using the Application, you are consenting to our processing of your information as set forth in this Privacy Policy now and as amended by us.
Logging Data
We want to inform you that whenever you use this service, in a case of an error in the app we collect data and information (through third party products) on your phone called Log Data. This Log Data may include information such as your device Internet Protocol (“IP”) address, device name, operating system version, the configuration of the app when utilizing my Service, the time and date of your use of the Service, and other statistics.
Service Providers
We may employ third-party companies and individuals due to the following reasons:
We want to inform users of this Service that these third parties have access to your Personal Information. The reason is to perform the tasks assigned to them on our behalf. However, they are obligated not to disclose or use the information for any other purpose.
Links to Other Sites
This Service may contain links to other sites. If you click on a third-party link, you will be directed to that site. Note that these external sites are not operated by me. Therefore, we strongly advise you to review the Privacy Policy of these websites. We have no control over and assume no responsibility for the content, privacy policies, or practices of any third-party sites or services.
Children’s Privacy
These Services do not address anyone under the age of 13. We do not knowingly collect personally identifiable information from children under 13. In the case we discover that a child under 13 has provided us with personal information, we will immediately delete this from our servers. If you are a parent or guardian and you are aware that your child has provided us with personal information, please contact us so that we will be able to do necessary actions.
Changes to This Privacy Policy
We may update our Privacy Policy from time to time. Thus, you are advised to review this page periodically for any changes. We will notify you of any changes by posting the new Privacy Policy on this page. These changes are effective immediately after they are posted on this page.
Contact Us
If you have any questions or suggestions about my Privacy Policy, do not hesitate to contact us at
Email - picf@aiims.edu.
Phone - +91-011-26593800
Address - Computer Facility, AIIMS, Ansari Nagar, New Delhi 110029, India
Comming Soon
Comming Soon
This section states the "Disclaimer" under which you may use aiims.edu/aiims.ac.in (the “Web Site”). Please read this page carefully. If you do not understand the Disclaimer stated here, do not use this web site and our services and in such case its use may be at your own risk. By using the Web Site, you are indicating your acceptance of the following Disclaimer. AIIMS, New Delhi, (the “Institute”) may revise this Disclaimer at any time by updating this posting. You should visit this page periodically to review the Disclaimer, because it is binding on you.
The content available on AIIMS website may not be up-to-date as the website and its content is being revamped. The site may also be having bugs and glitches, lack of functionality and broken links. Please bear with us for any such inconvenience and give your opinion, suggestions and feedback on the same for improvement of the website. By using the Web Site, you assume all the risks associated with dealing with other users with whom you come in contact through the Web Site. The Institute cannot and does not confirm that each user is who they claim to be. In the event that you have a dispute with another user, you release the Institute, its Director, its Employees and agents from any claims, demands and damages (actual and consequential, direct and indirect) of every kind and nature, known and unknown, suspected and unsuspected, disclosed and undisclosed, arising out of or in any way connected with such disputes.
The Institute does not guarantee the accuracy, thoroughness, reliability, or quality of content at the Web Site, and will not be responsible for any errors, inaccuracies, typographical errors or omissions in articles or any other content. The Institute will not be liable of any loss or damage caused by a users reliance on information obtained from the Web Site. You should not use the Web Site if you cannot or do not accept this responsibility. Despite our efforts to provide timely and accurate information, we may have errors from time to time.
You should not rely solely upon the information or advice read at the Web Site. Since each individual’s purpose is unique and different, you should always consult with others as per need on your own before making any important decisions based on the contents of the website.
Links to Third Party Sites
The Web Site may contain links to third party web sites. These links are provided solely as a convenience to you and not as an endorsement by the Institute of the content on such third party web sites. This Institute is not responsible for the content of linked third party web sites and does not make any representations regarding the content or accuracy of materials on such sites.
Indemnity
By using the Web Site, you agree to indemnify, defend and hold harmless the Institute, its Director, Officers, Employees, Ex-Employees from and against any claims, actions or demands, including without limitation reasonable legal and accounting fees, alleging or resulting from your use of the Material or your breach of the Terms of Use.
Disclaimer of Warranties
You expressly agree that the use of the web site is at your own risk. The web site is provided on an “as is” and “as available” basis without warranties of any kind, express or implied, including but not limited to warranties of title, merchantability, reliability, accuracy, fitness for a particular purpose or non-infringement.
The institute makes no warranty that the web site will be uninterrupted, timely, or secure. Additionally, the institute does not warrant that the web site will operate error-free or that the web site and its server are free of computer viruses or other harmful mechanisms. The institute is not responsible for any consequential or incidental damage, whether foreseeable or not, which may have resulted from the unavailability or malfunction of the web site. If your use of the web site or the material results in the need for servicing or replacing equipment or data, the institute is not responsible for those costs.
You agree that any information or data downloaded through the use of the web site is at your own discretion and risk and that you will be solely responsible for any damage to your computer system or loss of data that results from the download of such material and/or data.
The institute is not responsible for content or other information outside this web site. The institute makes no representation as to the quality, accuracy, suitability, functionality, or legality of any sites to which we may provide links. You hereby waive any claim you might have against the institute with respect to such links and sites.
Limitation of Liability
In no event shall the institute, its director, officers, employees, parents, affiliates or third parties be liable for any damages whatsoever including, without limitation, incidental and consequential damages, lost profits, or damages resulting from lost data or business interruption resulting from the use or inability to use the web site and services, whether based on warranty or contract. You hereby waive any and all claims against the institute and its parents, affiliates, officers, or employees arising out of your use of the web site and the information or services available thereon.
Comming Soon
Viewing Information in Various File Formats
Provides information on how to access different file formats for viewing the required information.
The information provided by this Web site is available in various file formats, such as Portable Document Format (PDF), Word, Excel and PowerPoint. To view the information properly, your browser need to have the required plug-ins or software. For example, the Adobe Flash software is required to view the Flash files. In case your system does not have this software, you can download it from the Internet for free. The table lists the required plug-ins needed to view the information in various file formats.
Plug-in for alternate document types
| Document Type | Plug-in for Download |
|---|---|
| Portable Document Format (PDF) files | |
| Word files | |
| Excel files | |
| PowerPoint presentations | |
| Flash content |
Comming Soon
Test




























































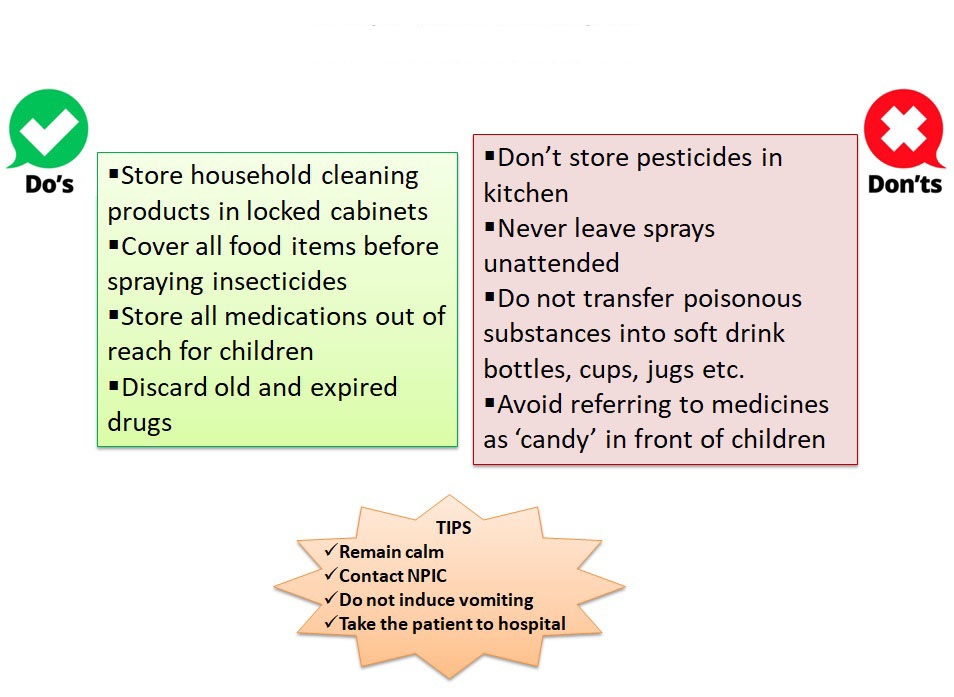



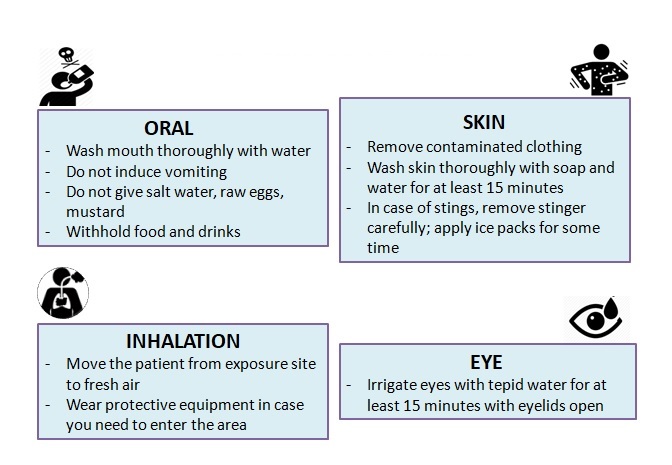


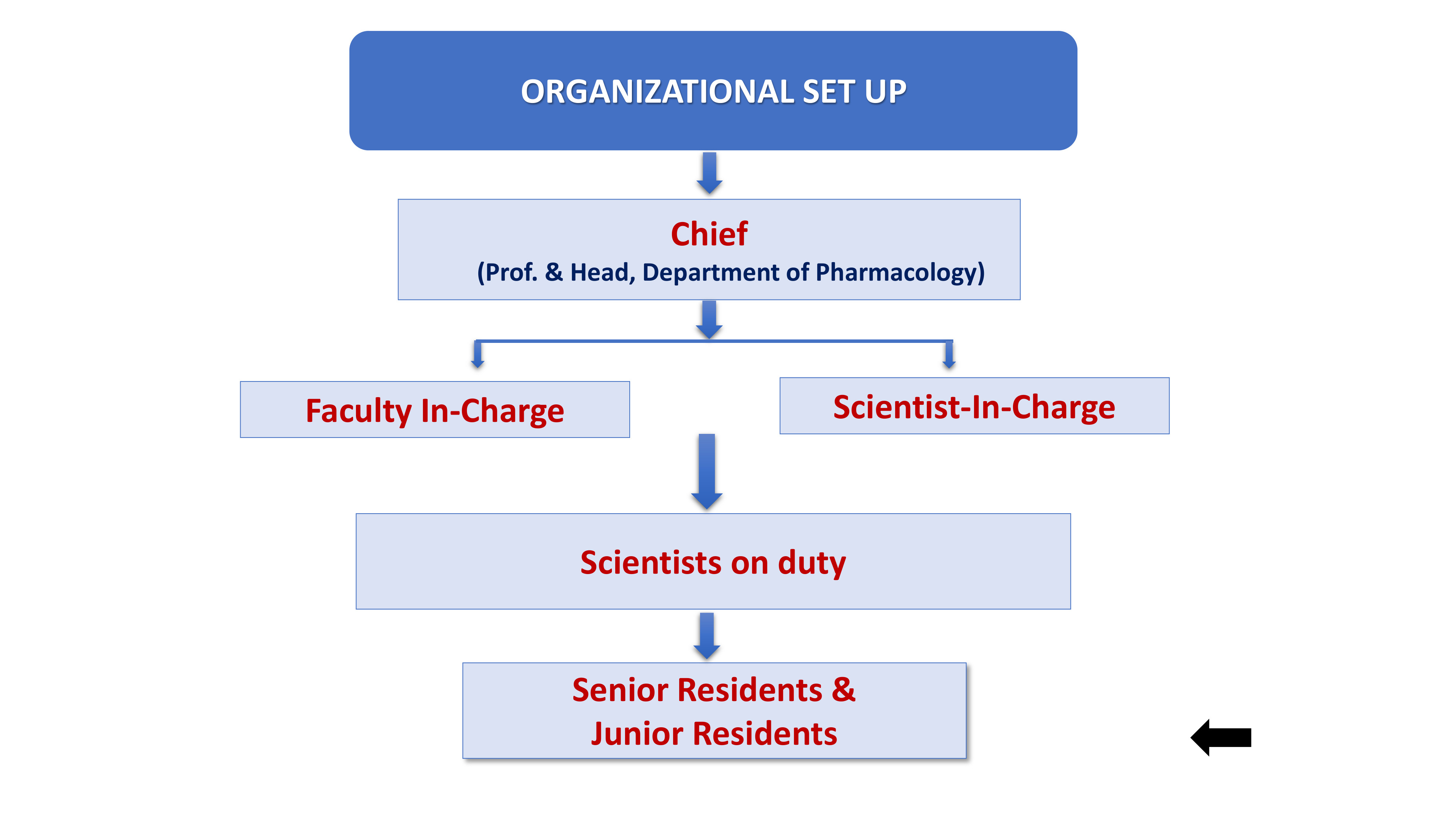
































































































































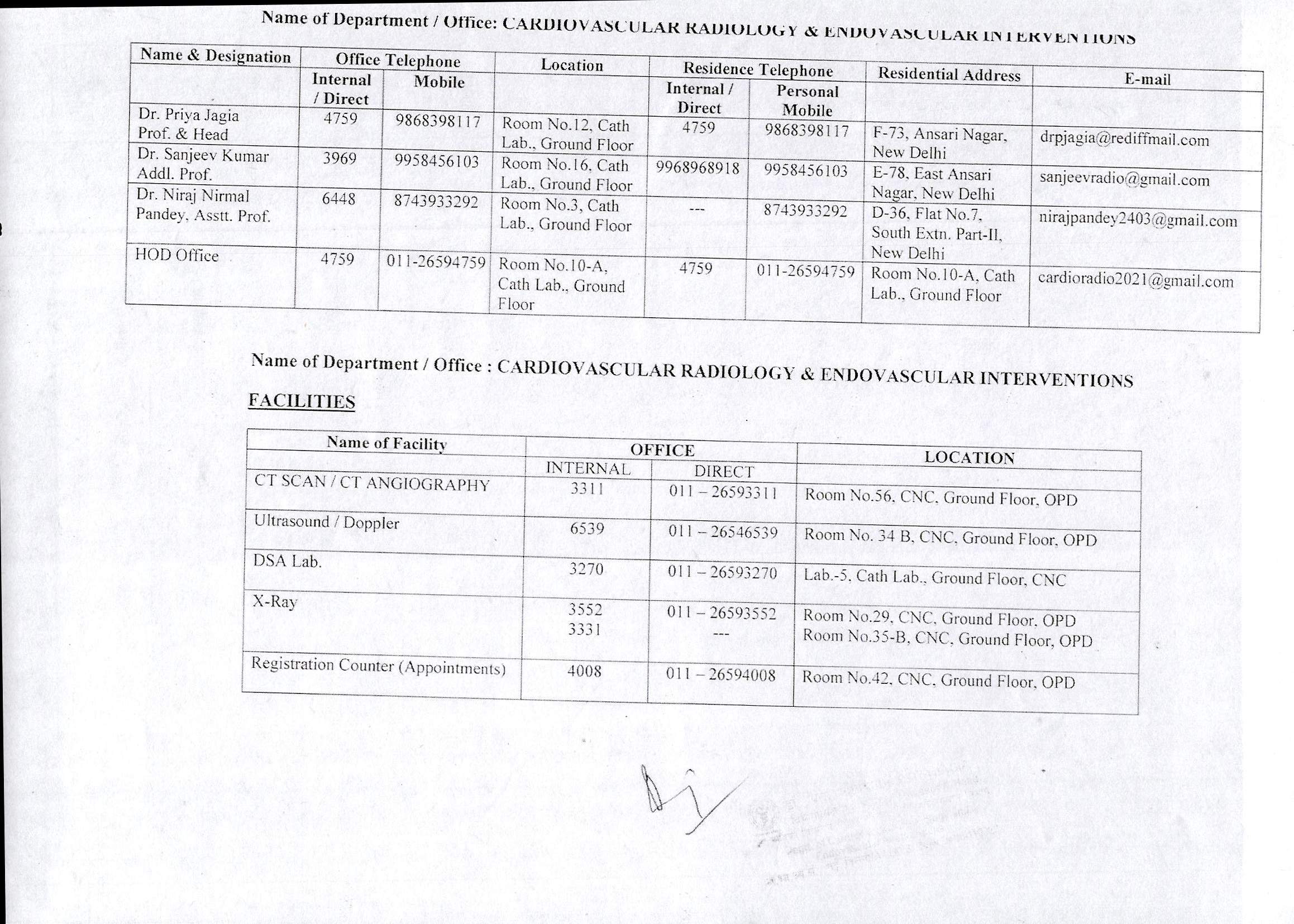





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}